Online Chapter 20 · Handbook of Local Anesthesia. 1. Local Anesthesia. Injection is used to...
10
e130 Pain Control for Operative Dentistry Aldridge D. Wilder, Jr. maximum dose for a specific agent depending on the weight of the patient. These dosages are averages, however, and the dentist must be alert to adverse systemic effects when injected dosages approach the recommended limits. 1 Local anesthetics have different durations of action for pulpal and soft tissue anesthesia. Pulpal (deep) anesthesia varies from 30 to 90 or more minutes. Soft tissue anesthesia varies from 1 to 9 hours, depending on the specific agent and whether or not a vasoconstrictor is included. Local anesthetics are selected on the basis of the estimated length of the clinical procedure and the degree of anesthesia required (Online Box 20-1). Two (or more) anesthetic agents can be administered when needed. The total dose of both anesthetics should not exceed the lower of the two maximum doses for the individual agents. Anesthetics also are available in amide and ester types. Hypersensitivity and allergic reactions in affected patients are much less frequent with the amide type of local anesthetic. 1 Patient Factors CARDIOVASCULAR SYSTEM Before administering any drug, the condition of the cardio- vascular system (heart and blood vessels) must be assessed. At minimum, blood pressure, heart rate, and rhythm should be evaluated and recorded for all patients. According to the latest guidelines, patients with a systolic pressure less than 160 mm Hg and a diastolic pressure less than 100 mm Hg (stage 1 hypertension) are good candidates for all dental pro- cedures. Patients with blood pressure consistently greater than the aforementioned numbers (stage 2 hypertension) should be referred to their physicians, particularly if the elevation is greater than 20 mm Hg. 2 Malamed suggested that any resting patient with a pulse rate less than 60 beats per minute (beats/ min) or greater than 110 beats/min be questioned further. Athletes in good physical condition may have a lower heart rate, but without this information, the lower heart rate may indicate a heart block. Additionally, five or more “missed beats” (premature ventricular contractions) per minute with no obvious cause is an indication for medical consultation. Pain Control Historically, the public has associated dental treatment with pain. This association is no longer valid because techniques for the elimination of pain, including atraumatic injection, have been available for years and are essential to a successful dental practice. Local anesthesia for operative dentistry must be profound, often to depths required for pulpal anesthesia. The following information, if understood and practiced, should eliminate pain associated with dental procedures. For additional information the reader is referred to Malamed’s Handbook of Local Anesthesia. 1 Local Anesthesia Injection is used to achieve local anesthesia in restorative den- tistry. The administration of local anesthesia to all tissues in the operating site is recommended for most patients to elimi- nate pain and reduce salivation associated with tooth prepara- tion and restoration. To administer effective anesthesia, the dentist must have a thorough knowledge of the patient’s phys- ical and emotional status and an understanding of the effects of the drug to be injected and the advantages and disadvan- tages of adding vasoconstrictors. A therapeutic dose of a drug is the smallest amount that is effective when properly administered and does not cause adverse reactions. An overdose of a drug is an excessive amount that results in an overly elevated local accumulation or blood level of the drug, which causes adverse reactions. The normal healthy patient can safely receive five to eight cartridges of anesthetic per appointment. Each 1.8-mL cartridge contains anesthetic, with or without a vasoconstrictor (e.g., lidocaine 2% [anesthetic] with epinephrine 1 : 100,000 [vasoconstric- tor], lidocaine 2% plain [no vasoconstrictor]). The number of permissible cartridges increases as body weight increases. According to Malamed, the maximum recommended dose of 2% lidocaine with epinephrine 1 : 100,000 is 4.4 mg/kg, or 2 mg/lb, to an absolute maximum of 300 mg (Online Table 20-1). 1 Online Tables 20-1 and 20-2 will help calculate the Online Chapter 20 Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
Transcript of Online Chapter 20 · Handbook of Local Anesthesia. 1. Local Anesthesia. Injection is used to...

e130
Pain Control for Operative DentistryAldridge D. Wilder, Jr.
maximum dose for a specific agent depending on the weight of the patient. These dosages are averages, however, and the dentist must be alert to adverse systemic effects when injected dosages approach the recommended limits.1
Local anesthetics have different durations of action for pulpal and soft tissue anesthesia. Pulpal (deep) anesthesia varies from 30 to 90 or more minutes. Soft tissue anesthesia varies from 1 to 9 hours, depending on the specific agent and whether or not a vasoconstrictor is included. Local anesthetics are selected on the basis of the estimated length of the clinical procedure and the degree of anesthesia required (Online Box 20-1). Two (or more) anesthetic agents can be administered when needed. The total dose of both anesthetics should not exceed the lower of the two maximum doses for the individual agents. Anesthetics also are available in amide and ester types. Hypersensitivity and allergic reactions in affected patients are much less frequent with the amide type of local anesthetic.1
Patient FactorsCARDIOVASCULAR SYSTEMBefore administering any drug, the condition of the cardio-vascular system (heart and blood vessels) must be assessed. At minimum, blood pressure, heart rate, and rhythm should be evaluated and recorded for all patients. According to the latest guidelines, patients with a systolic pressure less than 160 mm Hg and a diastolic pressure less than 100 mm Hg (stage 1 hypertension) are good candidates for all dental pro-cedures. Patients with blood pressure consistently greater than the aforementioned numbers (stage 2 hypertension) should be referred to their physicians, particularly if the elevation is greater than 20 mm Hg.2 Malamed suggested that any resting patient with a pulse rate less than 60 beats per minute (beats/min) or greater than 110 beats/min be questioned further. Athletes in good physical condition may have a lower heart rate, but without this information, the lower heart rate may indicate a heart block. Additionally, five or more “missed beats” (premature ventricular contractions) per minute with no obvious cause is an indication for medical consultation.
Pain ControlHistorically, the public has associated dental treatment with pain. This association is no longer valid because techniques for the elimination of pain, including atraumatic injection, have been available for years and are essential to a successful dental practice. Local anesthesia for operative dentistry must be profound, often to depths required for pulpal anesthesia. The following information, if understood and practiced, should eliminate pain associated with dental procedures. For additional information the reader is referred to Malamed’s Handbook of Local Anesthesia.1
Local AnesthesiaInjection is used to achieve local anesthesia in restorative den-tistry. The administration of local anesthesia to all tissues in the operating site is recommended for most patients to elimi-nate pain and reduce salivation associated with tooth prepara-tion and restoration. To administer effective anesthesia, the dentist must have a thorough knowledge of the patient’s phys-ical and emotional status and an understanding of the effects of the drug to be injected and the advantages and disadvan-tages of adding vasoconstrictors.
A therapeutic dose of a drug is the smallest amount that is effective when properly administered and does not cause adverse reactions. An overdose of a drug is an excessive amount that results in an overly elevated local accumulation or blood level of the drug, which causes adverse reactions. The normal healthy patient can safely receive five to eight cartridges of anesthetic per appointment. Each 1.8-mL cartridge contains anesthetic, with or without a vasoconstrictor (e.g., lidocaine 2% [anesthetic] with epinephrine 1 : 100,000 [vasoconstric-tor], lidocaine 2% plain [no vasoconstrictor]). The number of permissible cartridges increases as body weight increases. According to Malamed, the maximum recommended dose of 2% lidocaine with epinephrine 1 : 100,000 is 4.4 mg/kg, or 2 mg/lb, to an absolute maximum of 300 mg (Online Table 20-1).1 Online Tables 20-1 and 20-2 will help calculate the
Onl ine Chapter 20
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.

Online Chapter 20—PainControlforOperativeDentistry e131
Patients with valvular heart disease or a predisposition to bacterial endocarditis should have prophylactic antibiotics prescribed before dental treatment; the American Heart Association defines the recommended regimen for these antibiotics.3
Overdose of any vasoconstrictor causes increased blood pressure, elevated heart rate, and possible dysrhythmias. These symptoms also may occur if a retraction cord treated with epinephrine is applied to abraded gingiva, which would result in the rapid uptake of the drug into the circulatory system. With careful operative dentistry, the gingiva should be mini-mally abraded, even in subgingival tooth preparations.
OnlineBox20-1 Approximate Duration of Action of Local Anesthetics*
Short Duration (Pulpal anesthesia approximately 30 minutes)
Mepivacaine, HCL 3%Prilocaine, HCL 4% (by infiltration)
Intermediate Duration (Pulpal anesthesia approximately 60 minutes)
Articaine, HCL 4% + epinephrine 1 : 100,000Articaine, HCL 4% + epinephrine 1 : 200,000Lidocaine, HCL 2% + epinephrine 1 : 50,000Lidocaine, HCL 2% + epinephrine 1 : 100,000Mepivacaine, HCL 2% + levonordefrin 1 : 20,000Mepivacaine, HCL 2% + epinephrine 1 : 200,000Prilocaine, HCL 4% (via nerve block only)Prilocaine, HCL 4% + epinephrine 1 : 200,000
Long Duration (Pulpal ≥90 minutes) anesthesia approximately 90+ minutes
Bupivacaine 0.5% + epinephrine 1 : 200,000
(From Malamed SF: Handbook of local anesthesia, ed 6, St. Louis, 2013, Mosby.)*These anesthetics all are from the amide category.
OnlineTable20-1 Maximum Recommended Dosages (MRDs) of Local Anesthetics Available in North America
MANUFACTURER’S AND FDA (MRD)
Local Anesthetic mg/kg mg/lb MRD, mg
ArticaineWith
vasoconstrictor7.0 3.2 Nonelisted
BupivacaineWith
vasoconstrictorNonelisted None
listed90
Withvasoconstrictor(Canada)
2.0 0.9 90
LidocaineWith
vasoconstrictor7.0 3.2 500
MepivacaineNo
vasoconstrictor6.6 3.0 400
Withvasoconstrictor
6.6 3.0 400
PrilocaineNo
vasoconstrictor8.0 3.6 600
Withvasoconstrictor
8.0 3.6 600
CALCULATION OF MILLIGRAMS OF LOCAL ANESTHETIC PER DENTAL CARTRIDGE (1.8 ml CARTRIDGE)
Local Anesthetic
Percent Concentration mg/ml
× 1.8 ml = mg/Cartridge
Articaine 4 40 72*
Bupivacaine 0.5 5 9
Lidocaine 2 20 36
Mepivacaine 2 20 36
3 30 54
Prilocaine 4 40 72
MRD, Maximum recommended dose.
*Cartridges of some drugs in the United States read, “1.7 ml. each” The actual volume of all local anesthetic cartridges is approximately 1.76 ml.
(From Malamed SF: Handbook of local anesthesia, ed 6, St. Louis, 2013, Mosby.)
CENTRAL NERVOUS AND RESPIRATORY SYSTEMSThe central nervous system (CNS) is more easily affected by overdose of injected anesthetic drugs compared with the car-diovascular system. Anesthetics depress the CNS, but when administered properly for local anesthesia, little or no clinical evidence of depression is encountered. At minimal to moder-ate overdose levels, depression is manifested in excitation (e.g., talkativeness, apprehension, sweating, elevated blood pressure and heart rate, elevated respiratory rate) or drowsiness. At moderate to high overdose levels, tonic-clonic seizure activity may occur, followed by generalized CNS depression, depressed blood pressure, reduced heart rate (<60 beats/min), depressed respiratory rate, and respiratory arrest. With lidocaine and procaine, the usual progression of excitatory signs and symp-toms described previously may not be seen, and the first clini-cal evidence of overdose may be mild sedation or drowsiness.1 The respiratory system is not affected by properly adminis-tered therapeutic doses of anesthetic drugs. The system may, however, be depressed and arrested by CNS depression result-ing from overdose.
ALLERGYMalamed stated that documented, reproducible allergy is an absolute contraindication for administration of local anes-thetic.1 When a patient reports a history of “sensitivity” or “reaction” to an injected dental anesthetic, the dentist must believe the patient until further investigation disproves the patient’s claim. Anaphylactic shock from an allergic reaction can be immediate and life threatening. Fast injection and intravascular injection of anesthetics are reasons for
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.

e132 Online Chapter 20—PainControlforOperativeDentistry
dental assistant is required to make the procedure more acceptable, and a positive approach is desirable with all patients during this phase of treatment. Probably the greatest positive effect is achieved through a caring manner, rather than by what is said. Words such as pain, sting, hurt, and inject should not be used because no matter what else is said, the patient will remember these potentially fear-invoking words. The operator must use a kind, considerate, and understanding approach. Every assurance should be made that the comfort of the patient is paramount and that the teeth and soft tissues will be treated with care. Such assurances, confidently and softly spoken, are welcomed during the administration of local anesthesia. One example is, “I may be taking longer than you expected, but we are giving the solution slowly to be kind to your tissues.” Patients who feel secure (safe from pain and in caring hands) gratefully accept local anesthesia. The art of tactfully keeping the syringe and needle from the view of the patient should be practiced. Here, the chairside assistant can be a tremendous help.
TECHNIQUE STEPS AND PRINCIPLESBecause profound, painless anesthesia of teeth and contiguous soft tissues is so important in operative dentistry, the salient features of a recommended technique for infiltration anesthe-sia of a maxillary canine are presented here. Technique instruc-tions for injection and infection control (particularly avoiding accidental needlestick injury) are described, and the following principles for the injection of a local anesthetic and epineph-rine are also applicable to infiltration and conduction anes-thesia. Infiltration anesthesia involves a supra-periosteal or field block, where deposition is near the nerve ends in the operating site. Conduction anesthesia involves a nerve block, where deposition is near a nerve trunk at a distance from the operating site.
In this example of infiltration anesthesia, the needle entry spot and direction are different from that presented in some textbooks on local anesthesia. Aspiration and slow deposition of solution are emphasized. For other local anesthesia injec-tions (inferior alveolar, Gow-Gates mandibular, posterosupe-rior alveolar, infraorbital, mental, and periodontal ligament), the reader is referred to a textbook on local anesthesia.
The routine supine position of the patient helps prevent vasodepressor syncope because it maintains blood supply and blood pressure to the brain. As a precaution, the upper torso should never be more than 10 degrees below the horizontal plane because this may cause respiratory distress secondary to the force of viscera against the diaphragm. Occasionally, patients may complain of breathing difficulty that is relieved only by sitting upright or standing (orthopnea), in which case a compromise in patient position is necessary. Another excep-tion to the supine position is when symptoms suggest an epinephrine overdose; in this case, a semi-erect or sitting position is best because it minimizes any further elevation in cerebral blood pressure. Symptoms of overdose include fear, perspiration, weakness, pallor, palpitations, anxiety, and restlessness.1
The syringe must have an aspirating feature. When anes-thetic is administered, aspiration is second in importance only to slow deposition of solution. For this purpose, the rod (piston) has a harpoon on its cartridge end and a thumb ring on the other end (Online Fig. 20-1, H). The harpoon engages the cartridge plunger, which results in its potential reverse
allergy-like reactions reported by patients. Some patients have proven allergy to bisulfite, an antioxidant used in anesthetic cartridges as a preservative for the vasoconstrictor.1
Any special condition of the patient should be recorded in the chart. The health status of the cardiovascular system, CNS, respiratory system, liver, kidneys, and thyroid gland should be noted, as well as the patient’s age, allergies, and pregnancy status. A medical history form must be completed and signed by the patient.
BenefitsCOOPERATIVE PATIENTWhen a local anesthetic appropriate for the procedure is pro-perly administered, patient anxiety and tension should be minimal. The appreciation and trust of the patient for the dentist (and dental assistant) are expressed in a more relaxed and cooperative attitude. Physically and emotionally, the patient and the dentist benefit from a relatively calm environment.
SALIVATION CONTROLSaliva control is a primary reason for the use of profound anesthesia in most patients. For years, it has been observed that complete anesthesia of all tissues (teeth and gingival tissues) in the dental operating site results in a marked re duction of salivation.4 Sometimes, a tooth is not sensitive and does not require anesthesia. If all other sensations from the operating site are eliminated, however, salivation is controlled.
HEMOSTASISThe term hemostasis, as used in operative dentistry, refers to the temporary reduction in blood flow and volume in tissue (ischemia) where a vasoconstrictor is used. The alpha effect of the vasoconstrictor causes constriction of the small blood vessels; the affected tissue bleeds less if cut or abraded. The principal function of a vasoconstrictor in operative dentistry is the prolongation of anesthesia because of reduced blood flow to and from the anesthetized site. Without epinephrine, anesthesia from 1 mL of lidocaine 2% lasts only 5 to 10 minutes; with epinephrine, the anesthesia lasts 40 to 60 minutes. Reduced blood flow helps keep the patient’s blood level of the anesthetic and the vasoconstrictor at a low level by reducing the rate of absorption into the circulatory system.
OPERATOR EFFICIENCYLocal anesthesia greatly benefits the dentist and the patient and is beneficial for successful tooth preparation and restora-tion. It improves operator efficiency, and usually, the patient is calmer and more cooperative. This increased cooperation may reinforce the dentist’s confidence and calmness, which may promote more efficient treatment. Without distractions or management problems from the patient, the dentist can focus on the treatment and its completion within a reasonable time frame.
AdministrationPSYCHOLOGYPatients have varying degrees of concern about receiving an intraoral injection. A concerted effort by the dentist and
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.

Online Chapter 20—PainControlforOperativeDentistry e133
ihs
r w c
DA
DA
DA
Operator’shand hard-stationary DA
A B
C D
E F
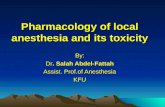
Online Fig. 20-1 A, Prop/guard (Stik-Shield) card. The periphery of the hole (h) is indexed (i) (four pairs of short cuts) to accept four external ridges (r) of the sheath (s) shown in B. B, The sheath (s) covers the injection portion of the needle, and the cap (c) covers the reverse end (cartridge needle). Sheath and cap are joined by spot plastic weld (w). Note the external ridge (r). C, With the fingers of one hand holding the prop/guard card printed-side up (and supporting it), the dental assistant (DA) uses the ends of the thumb, index, and middle fingers of the other hand to press the last one third of the sheath through the hole while lining up external ridges to align with the card indices. (Do not, at this time, jar the cap [on reverse end] loose with hand.) D, The dental assistant applies thumb pressure (arrow) on the end of the cap to insert sheath fully to its collar. (Do not, at this time, loosen the cap by any twisting motion.) E, The dental assistant’s left hand holds the sheath (card on sheath) and presses down on the countertop in a stationary position (left arrow), while the fingers of right hand “twist-break” plastic weld at cap/sheath union and deliberately move the cap off of the reverse-end needle. Note the horizontal right arrow depicting the movement of the hand (away from needle), which discards the cap. F, The dental assistant’s left hand, still holding the carded sheathed needle, now inserts the reverse-end needle into the hole in the threaded end of the syringe held by the other hand (kept at least 3 inches away from card).
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.

e134 Online Chapter 20—PainControlforOperativeDentistry
Operator
Operator’shand hard-stationary
Operator’shand remainsstationary oncountertop
OperatorI J
LK
DA
h
G H
G, The dental assistant’s left hand screws the sheathed needle clockwise onto the syringe threads to a full-seating position against the syringe nose. Note the protection of both hands by the guard card during such threading. The harpoon (h) is used later. H, The dental assistant lays the prepared syringe (minus anesthetic cartridge) on the countertop or tray behind the patient, propped up because of the guard card and ready for the operator. Note the harpoon (h) on the piston end. I and J, While fully retracting the spring-loaded, movable, rear cartridge seat of the syringe by hand retraction of the piston, the operator or assistant (behind the patient) inserts the cartridge, rearward end first (I), and “drops” the forward end (diaphragm end) of the cartridge into position (J) without dragging across or bending the reverse-end needle. The operator or the assistant slowly releases the piston retraction, moving the rear cartridge seat and the cartridge forward, allowing the reverse-end needle to pierce diaphragm. (Leakage of cartridge during later attempted deposition is usually caused by a bent reverse-end needle poorly centered on the diaphragm.) K and L, With the syringe propped by the card on countertop (or tray) behind the patient, the operator or assistant holds the sheath by the fingers of one hand (card protected) and the syringe by the other hand, which is kept stationary (K) as the sheath is loosened and removed away from the needle (L). M, The guard card now props the sheath.
Online Fig. 20-1, cont’d
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.

Online Chapter 20—PainControlforOperativeDentistry e135
sOperator
OperatorNM
O
N, The operator or the assistant sets the harpoon by gentle palm-thump of the thumb ring and then (O) tests the syringe for preparedness by thumb pressure moving the plunger forward 1 to 2 mm while verifying emission of solution (s) from the needle without leakage at the forward end of the syringe body.
Online Fig. 20-1, cont’d
movement to create negative pressure when the operator’s thumb (in the ring) pulls back gently.
Injection into infected tissue should be avoided because of the risk of spreading the infection. Also, the anesthetic becomes less effective because the infected tissue is acidic rather than basic. Alternative approaches such as nerve block should be used.
Disposable NeedleThe sheath covers the needle and the cap covers the reverse end (cartridge end) of the disposable needle (see s and c in Online Fig. 20-1, B). For each patient (appointment), the dental assistant selects a sheathed, capped, new disposable needle of the desired length and gauge. The sheathed needle comes sterile from the manufacturer. The needle remains sheathed except for setting the harpoon and testing the syringe preparedness (see the later discussion on principles), until the moment of entry at the injection site. This helps prevent acci-dental needlestick injury, which among other things indicates needle replacement. For each patient appointment, using a new, sterile needle contaminated only by that patient’s oral tissue eliminates cross-infection via the needle. Keeping the sheath in place ensures that the needle is sharp. When the needle contacts the firm periosteal tissue or bone, a minute barb can be formed that causes pain on withdrawal or during subsequent re-injection.
The needle must be sufficiently long that its full length is never out of sight (never completely within tissue). This means that in the unlikely event that a needle breaks at the hub junction, some of the needle is exposed for grasping and withdrawal. Needles of 27-gauge are generally recommended, although some operators prefer the 30-gauge, short needle for infiltration anesthesia of maxillary teeth. The 30-gauge needle may not allow aspiration, and some authorities believe that it does not pierce or move in tissue more easily than the 27-gauge needle. Also, the 30-gauge, long needle may deviate during injection for conduction anesthesia of the inferior alveolar nerve.
Prop/Guard CardThe dental assistant inserts the sheathed needle end into the prop/guard card (Stik-Shield; Tacoma, WA) (see Online Fig. 20-1, A through D) and removes the cap on the reverse end of the needle (see Online Fig. 20-1, E). The dental assistant inserts the reverse end of the needle into the hole at the threaded end of the syringe and screws the sheathed needle to a full seating position against the nose of the syringe (see Online Fig. 20-1, F and G). The guard card protects both hands. The card hits the nose of the syringe before the needle could injure the hand holding the syringe. The dental assistant inserts the cartridge and sets the harpoon or lays the propped (by card) syringe on a tray or countertop (see Online Fig. 20-1, H) behind the
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.

e136 Online Chapter 20—PainControlforOperativeDentistry
spring-loaded, retracted piston is slowly released. If the car-tridge needle is malpositioned or bent as the cartridge is loaded, leaking can occur as injection is initiated. The distaste-ful solution may drip freely into the patient’s mouth. If so, injection must be aborted, and another cartridge must be placed properly in the syringe.
The harpoon is set into the cartridge plunger by a light, quick thrust from the palm of the hand on the thumb ring (see Online Fig. 20-1, N). Too strong a blow may crack or break the cartridge.
The sheath should be removed out of the patient’s view, carefully moving it away from the hand holding the needle and syringe; the hand is held stationary on the tray or coun-tertop (see Online Fig. 20-1, K and L). The prop/guard card protects the hand during sheath removal (see Online Fig. 20-1, L). It also props the sheath, thus preventing contamination (see Online Fig. 20-1, M).
The assembled syringe is tested by pressing the plunger forward 1 to 2 mm to verify that it slides easily and to ensure that the solution is emitted from the needle tip without leakage (see Online Fig. 20-1, O). If preparation of the injection site has been accomplished previously by wiping of the entry site with gauze and the 1- to 2-minute placement of topical anes-thetic (see the next discussion on principles), the injection procedure follows.
Topical AnestheticBefore needle entry, the mucosa at the injection site should be wiped free of debris and saliva with a sterile gauze. After this, a lidocaine topical anesthetic ointment is applied for a minimum of 1 to 2 minutes to the selected entry spot (using a cotton-tipped swab, limiting the area of application to the swab dimension). This procedure often is started immediately after positioning the patient in the chair and following the wiping. The chairside assistant may perform the wiping and the application of the topical anesthetic. The use of a topical anesthetic is generally recommended. However, effective injection techniques, including a slow deposition rate (approximately 60 seconds per cartridge), a warmed car-tridge, and the use of sharp needles, are more important factors in achieving painless injection than the use of a topical anesthetic.
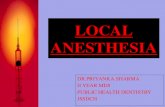
Injection SiteIf in place, the needle sheath should be removed in a one-person procedure, taking care to protect the hand with the shield (see Online Fig. 20-1, K and L). With the left hand, a right-handed operator gently raises the lip outward and upward to identify the vestibular fornix, or the mucogingival junction, where the attached gingiva joins the alveolar mucosa (Online Fig. 20-2). Holding the lip high enough, the operator visualizes the location of the root end and determines the injection site in the alveolar mucosa (1) as it is stretched per-pendicular, or nearly so, to the long axis of the tooth and (2) toward the periosteal target area, which is very near the root end of the tooth to be operated on (see Online Fig. 20-2). The injection site should be 5 to 10 mm lateral of the mucogingival line, allowing some freedom of needle movement and avoid-ing causing tissue tension. If the needle is held parallel to the tooth long axis, rather than at an angle as recommended, the needle tends to enter too close to the attached mucosa and thus to the sensitive periosteal lining, which would cause pain
patient for the operator to insert the cartridge, set the harpoon, remove the sheath, and test for preparedness.
Anesthetic CartridgeUsing a new cartridge for each patient is imperative. Because some ingredients do not have an extended shelf life, the anes-thetic cartridge should not be more than 18 months past the date of manufacture. The expiration date is printed on the packing container. Some manufacturers place an expiration date on the cartridge. The diaphragm end of the cartridge should not be contaminated by contact with potentially infected surfaces. The cartridge should not be immersed in a sterilizing solution (cold sterilizing solution or alcohol) because this can diffuse through the diaphragm and cause tissue damage. Cartridges should not be exposed to sunlight and should be stored at room temperature.1
Anesthetic SolutionThe weakest solution of anesthetic that will be effective should be used. Lidocaine 2% with 1 : 100,000 epinephrine is commonly used in operative dentistry and is generally recom-mended; 1 mL (half a cartridge) provides infiltration anesthe-sia for 40 to 60 minutes for anterior teeth. The addition of a vasoconstrictor to the anesthetic solution is necessary to prolong anesthesia by decreasing the rate of absorption of the anesthetic into blood. The vasoconstrictor may reduce the potential of anesthetic toxicity. As previously described, the vasoconstrictor in the anesthetic solution administered by infiltration is useful in reducing occasional hemorrhage by producing slight, transient ischemia of the cut or abraded soft tissue.
Before its use, the anesthetic solution should be warmed to approximately body temperature. Otherwise, the relatively cold solution contributes to the pain of injection. An approxi-mately 30°F difference exists between room temperature and body temperature. The anesthetic cartridge can be warmed in an anesthetic warmer, which is usually heated by a low-watt light bulb, or the cartridge can be held tightly in the palm of the hand for 10 to 15 seconds.
Anesthetic SyringeThe anesthetic syringe includes a rod (or piston) that has a harpoon (or barb) on the cartridge end and a thumb ring on the other end. The harpoon and thumb ring are features that allow the operator to aspirate during injection. The harpoon engages the cartridge plunger. During injection, the operator should use the thumb ring and periodically reverse the move-ment of the rod to create negative pressure causing aspiration. Periodic aspiration during injection is important to ensure that the solution is not being injected into a blood vessel. If the tip of the needle is in the vessel, blood is aspirated into the cartridge, indicating the need to reposition the needle. For patient safety and comfort, periodic aspiration is as important as slow deposition of the anesthetic solution.
Assembly of SyringeTo assemble the syringe, the assistant or operator picks up the syringe and, while holding the piston fully retracted, inserts the cartridge (see Online Fig. 20-1, I and J). The cartridge needle should be diaphragm centered. If it is not, the assistant or the operator guides the axial alignment of the cartridge such that the needle pierces the center of the diaphragm as the
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.

Online Chapter 20—PainControlforOperativeDentistry e137
30 seconds for 1.8 mL (one cartridge).1 This fast rate separates tissue and is too rapid to allow diffusion along normal tissue planes. If the injection is intravascular, it can lead to serious adverse reactions. Also, it is painful or at least uncomfortable. Malamed stated that a 1-minute rate for 1.8 mL of anesthetic (30 seconds for 1 mL, or half a cartridge) would not cause tissue damage and would not lead to serious overdose reactions, even if the anesthetic is accidentally injected intravascularly.1
An important principle is to deposit the smallest volume that will provide effective anesthesia. A common error is to deposit excessive anesthetic (with epinephrine) causing over-dose reactions.
After deposition, the needle is gently withdrawn and resheathed. A one-handed procedure is recommended. The operator inserts the needle partially into the propped sheath (remaining after the unsheathing procedure), uprights the sheath on the tray or countertop, and seats the needle fully into the sheath (Online Fig. 20-3, A and B). The sheathed syringe is left propped for possible reuse or for later removal and disposal (see Online Fig. 20-3, C). Resheathing is crucial in the prevention of needlestick injuries, which can cause cross-infection to the operator and other office personnel. The Occupational Safety and Health Administration (OSHA) stip-ulates that needle resheathing should be in a one-handed pro-cedure.5 It is also recommended that resheathing should be done by the same person who gave the injection; this elimi-nates the hazard of passing exposed needles. Even though multiple injections using the same needle for a patient creates no infection control concerns, multiple uses are discouraged because the used needle and the contents of its lumen may be infectious to dental personnel if accidental needlestick injury occurs.
It is important that the patient be continually observed during and after the administration of local anesthesia. An anesthetized patient should never be left unattended and unobserved. Adverse reactions, if they occur, demand imme-diate attention by the dentist.
Disposal of Needle and CartridgeProper disposal of the needle and cartridge is crucial. Removal and disposal of the sheathed, used needle is done by the dental assistant, who carefully unscrews the sheathed needle from the syringe (see Online Fig. 20-3, D) and moves it away from the syringe with a shield-protected hand (see Online Fig. 20-3, E). Tissue contact with the uncapped, exposed cartridge needle should be avoided. If the needle hub is too tight to remove with controlled finger pressure alone, a suture-needle holder (or similar instrument) should be used to loosen the needle hub. The reverse end of the used needle should never be manually recapped. The assistant’s hands should be gloved, preferably with utility gloves.
Disposal of the sheathed, used needle immediately follows its removal from the syringe. With the protective guard card still in place, the needle is placed in a nearby sharps disposal container by laying the attached card on the orifice rim (see Online Fig. 20-3, F). With the thumb pressing on the plastic, the sheathed needle is pushed out of the card into the con-tainer (see Online Fig. 20-3, G). The cartridge also should be disposed of in the sharps container. The sharps container must be leak-proof and hard walled and display an OSHA biohaz-ard label.5
from touching or stripping the periosteum from the bone. The needle tip should not be close to the periosteum until it has reached its target area.
InjectionWith the injection site identified and the needle directed prop-erly, two things are done simultaneously in preparation for injection: (1) A slight, gentle tug is applied to the lip (outward and upward) to have the entry spot tissue slightly taut, and (2) the needle is inserted about 3 mm into the mucosa (all the bevel under the epithelium). The slight, gentle tug while tensing the tissue, coupled with topical anesthesia, masks any sensation from the needle entry. After this, the lip may be relaxed, maintaining visibility of the needle. Initially, a small amount of solution is deposited slowly while observing and reassuring the patient. The operator waits several seconds for the anesthetic to take effect near the injection site before con-tinuing the injection. Still maintaining proper needle direc-tion, the operator gently continues inserting the needle toward the targeted periosteum. The operator needs to be careful to sense resistance when the needle tip touches the lining of the bone, at which time the needle immediately is withdrawn 1 to 2 mm.
The operator aspirates by slightly reversing the harpooned plunger a few millimeters by gentle backward movement of the thumb ring. Aspiration (negative pressure) verifies that the needle is not in a blood vessel. If blood appears in the car-tridge, the aspiration is positive; the needle immediately is withdrawn 1 to 2 mm, and the operator aspirates again until blood does not appear.
If aspiration is negative, the operator slowly deposits 1 mL (slightly more than half the cartridge) over the next 30 seconds, continually observing and reassuring the patient. A rate of deposition of 1 minute for 1 mL is a good rule of thumb. Slow deposition is the most important safety procedure for the prevention of adverse reactions from high blood levels of the anesthetic or epinephrine. Aspiration is second in importance. Malamed defined overly rapid deposition as taking less than
Online Fig. 20-2 Recommended entry spot (e), direction of needle (yn), and lip position (yl) for infiltration anesthesia of the maxillary canine. Direction of needle (xn) and lip position (xl) are not recommended. Ves-tibular fornix (vf) is the junction of the loose and fixed mucosa.
yl
yn
exl
vfxn
Lip position yl and needle direction yn recommended
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.

e138 Online Chapter 20—PainControlforOperativeDentistry
Online Fig. 20-3 A, Behind the patient, the operator (or individual who gave the injection), using only the syringe-holding hand, inserts the needle partially into the sheath propped by prop/guard card. B, The operator then places the syringe and sheath upright on the tray or countertop and presses the needle fully into the sheath. C, The operator lays the resheathed syringe propped by the card on the countertop.
Operator Operator
A
C
B
Emergency ProceduresThe importance of taking pretreatment vital signs cannot be overemphasized. The patient’s pretreatment blood pressure and pulse rate should be recorded in the chart. These vital signs are useful to uncover previously unknown cardiovascu-lar problems and to serve as a baseline if an adverse reaction occurs during treatment. Adverse reactions occurring during or after administration of local anesthesia can lead to serious complications that require emergency procedures. Foremost among these procedures are the following: (1) Place the patient in a supine position (note the exception below), (2) summon medical assistance, (3) monitor vital signs, and (4) apply basic life support (open the airway and use cardiopul-monary resuscitation [CPR], if needed). The supine position, with legs (only) slightly elevated, increases the volume of cir-culating blood and aids in increasing blood pressure. This procedure for a patient in syncope, or with syncopal symp-toms, should relieve hypoxia of the brain and return the patient to, or help maintain, consciousness. The supine posi-tion should not be used, however, when symptoms (e.g., fear, perspiration, weakness, pallor, palpitations) suggest an epi-nephrine overdose. In this case, a semi-erect or sitting position is best because it minimizes any further elevation in cerebral blood pressure.1
Analgesia (Inhalation Sedation)The most appropriate method of preventing pain is by block-ing the nerve pathways capable of conducting nerve impulses. For patients who have a low threshold of pain and are appre-hensive (hyper-responders), raising the threshold by inhala-tion sedation is an adjunctive aid to anesthesia by injection. The use of nitrous oxide and oxygen is one method of inhala-tion sedation. The reader is referred to a textbook on anesthe-sia that covers inhalation sedation in detail. The operator should understand that this method of pain control has defi-nite limitations. Analgesia should not be thought of as general anesthesia in any stage or depth. It is simply a condition in which the pain threshold is elevated. With inhalation sedation, the patient is conscious of the activities around him or her.
HypnosisThe fear of pain associated with dental procedures sometimes can be controlled by hypnosis. A favorable mental attitude may be established through suggestions of relaxation. The dentist and the patient may derive certain benefits through hypnosis. The dentist has the opportunity to work on a more relaxed and cooperative patient and has better control over patient habits such as talking and rinsing and oral tissue
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.

Online Chapter 20—PainControlforOperativeDentistry e139
References1. Malamed SF: Handbook of local anesthesia, ed 6, St. Louis, 2013, Mosby.2. Herman WW, Konzelman JL Jr, Prisant LM; Joint National Committee on
Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: New national guidelines on hypertension: A summary for dentistry. J Am Dent Assoc 135:576–584, 2004.
3. Dajani AS, Taubert KA, Wilson W, et al: Prevention of bacterial endocarditis: Recommendations by the American Heart Association. J Am Dent Assoc 128:1142–1151, 1997.
4. Sturdevant CM, et al, editors: The art and science of operative dentistry, ed 1, New York, 1968, McGraw-Hill.
5. Occupational Safety and Health Administration: Bloodborne pathogens (Federal Register 56: Section 1910, 1030 [26 U.S.C. 653], 64175–64182), Washington, D.C., 1991, OSHA.
6. Marcus HW: The role of hypnosis and suggestions in dentistry. J Am Dent Assoc 59:1149–1163, 1959.
tension. The patient who is relaxed is less fatigued at the end of the appointment and has no specific recollection of having experienced discomfort.
Hypnosis has some merit under certain circumstances and has produced satisfactory results for some practitioners when it is properly applied. Before hypnosis is attempted, the opera-tor must know how to recognize and cope with conditions associated with psychological, emotional, and mental factors and must be thoroughly familiar with all of the principles involved in hypnosis.
Hypnosis is not a way to eliminate all other accepted means of minimizing dental pain or discomfort, but it may be a valu-able adjunct in improving accepted procedures.6 Also, post-hypnotic suggestion has been found to be successful in alleviating certain noxious dental habits.
F G
DA
Hand hard-stationaryon countertop
DA
Hand remainsstationary
D E
DADA
D–G, The dental assistant, after patient dismissal, holds the syringe stationary with the fingers of one hand at least 2 inches away from guard card as the fingers of the stronger hand unscrew (counterclockwise) the sheathed, used needle from the syringe (D) and immediately move it (with reverse-end needle exposed) away from the syringe (distance from card to end of reverse-end needle is only 1 inch, and card stops needle from sticking syringe-holding fingers, which are ≥2 inches away) (E). The dental assistant continues to hold the sheathed needle and conveys it to a nearby (within a few feet) leak-proof, hard-walled, OSHA biohazard–labeled container with a suitable size orifice, gently laying (on the rim) the guard card with the reverse-end needle down (F), and steadies the card with fingers of one hand and presses (with the thumb of the other hand) the sheathed needle out of the card to free-fall into the container (G). The container should be kept upright, tightly closed between disposals of sharps, and out of the reach of children.
Online Fig. 20-3, cont’d
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.