OncOlOgy - Amazon S3 to the 31% to 49% of patients reported with aprepitant.24 Aprepitant is a...
12
Perspectives on Improving the Prevention and Treatment of Chemotherapy-Induced Nausea and Vomiting (CINV) Developing Clinically and Economically Efficient Antiemetic Regimens To participate in this activity online, go to www.gotoper.com/CINV2013. Featuring Consultations With Mohammad Jahanzeb, MD Medical Oncologist Professor of Clinical Medicine, Hematology-Oncology Medical Director, Deerfield Beach Campus University of Miami Sylvester Comprehensive Cancer Center Deerfield Beach, FL Beverly Bell, MD Medical Director, Comprehensive Hematology Oncology Care Management inVentiv Medical Management Augusta, GA Medical Writer: Elizabeth Cameron, PhD A CME-Certified Activity ONCOLOGY CONSULTATIONS
Transcript of OncOlOgy - Amazon S3 to the 31% to 49% of patients reported with aprepitant.24 Aprepitant is a...

Perspectives on Improving the Prevention and Treatment of
Chemotherapy-Induced Nausea and Vomiting (CINV)
Developing Clinically and Economically Efficient Antiemetic Regimens
To participate in this activity online, go to www.gotoper.com/CINV2013.
Featuring Consultations With
Mohammad Jahanzeb, MD Medical Oncologist
Professor of Clinical Medicine, Hematology-OncologyMedical Director, Deerfield Beach Campus
University of Miami Sylvester Comprehensive Cancer CenterDeerfield Beach, FL
Beverly Bell, MDMedical Director, Comprehensive Hematology Oncology
Care ManagementinVentiv Medical Management
Augusta, GA
Medical Writer: Elizabeth Cameron, PhD
A CME-Certified Activity
OncOlOgyC o n s u lt a t i o n s

Initial release date: March 25, 2013Expiration date: March 25, 2014 Media Used: Print monograph with online posttest, evaluation, and request for credit Estimated time to complete this CME activity: 1 hour Copyright: 2013. Physicians’ Education Resource®, LLC.
Statement of NeedChemotherapy-induced nausea and vomiting (CINV) is a major side effect of many common chemotherapy regimens, and is often undertreated. CINV can adversely affect patients’ quality of life and may impair adherence to prescribed treatment regimens or even lead to withdrawal from potentially curative therapy. Expert guidelines on the prevention and management of CINV have recently been updated based on several new studies, and it is important for clinicians to remain current on the latest standards in order to further improve outcomes for their patients.
Learning Objectives• Review the recently updated clinical practice guidelines for
CINV• Identify the contributing factors that predispose patients to
developing CINV• Examine the managed care aspects of CINV• Evaluate clinical data regarding the efficacy and safety of avail-
able agents and combination strategies for the prevention and/or treatment of CINV
Target AudienceThis educational activity is directed toward hematologists, medical oncologists, fellows, and other health care professionals involved in the treatment and management of patients with cancer.
Accreditation and Designation of Credit StatementsPhysicians’ Education Resource®, LLC, is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Physicians’ Education Resource®, LLC, designates this live activity for a maximum of 1.0 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Commercial Support Acknowledgment This activity is supported by an educational grant from Eisai Inc.
FacultyMohammad Jahanzeb, MD Medical Oncologist Professor of Clinical Medicine, Hematology-OncologyMedical DirectorUniversity of Miami Sylvester Comprehensive Cancer CenterDeerfield Beach, FLBeverly Bell, MDMedical Director, Comprehensive Hematology Oncology Care ManagementinVentiv Medical ManagementAugusta, GA
The following individuals have no relevant financial relationships with commercial interests to disclose:Beverly Bell, MD; Elizabeth Cameron, PhD; Mohammad Jahanzeb, MD; and the PER Planning Staff (Alexis Mascitti, MD, and Emily Valko).
Off-Label/Investigational Use Disclosure and DisclaimerThis CME activity may contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. For additional information about approved uses, including approved indications, contraindications, and warnings, participants are advised to consult prescribing information and appropriate resources for all products/devices discussed or consult the Physicians’ Desk Reference.
The information provided in this CME activity is for continuing medical education purposes only and is not meant to substitute for the independent medical judgment of a physician relative to diagnostic and treatment options for a specific patient’s medical condition.
The opinions expressed in the content are solely those of the individual faculty members and do not reflect those of Physicians’ Education Resource, LLC, or the company that provided commercial support for this CME activity.
Method of Participation/How to Receive Credit1. Read the monograph in its entirety.2. Go to http://www.gotoper.com/CINV2013.3. Complete and submit the posttest, evaluation form, and request
for credit.4. Print your Certificate of Credit.
This activity is provided free of charge to participants.
Educational Partner Contact Information: For questions about this CME activity, please contact:Physicians’ Education Resource®, LLC666 Plainsboro Road, Ste 356Plainsboro, NJ 08536Phone: (888) 949-0045
Oncology consultations: Improving Outcomes in Chemotherapy-Induced Nausea and Vomiting (CINV)Developing Clinically and Economically Efficient Antiemetic Regimens

Oncology Consultations 3
Improving Outcomes in Chemotherapy-Induced Nausea and Vomiting (CINV)
Developing Clinically and Economically Efficient Antiemetic Regimens
in combination. Dopamine agonists such as metoclopramide or pro-chlorperazine are also used, especially for breakthrough emesis.1,4
Antiemetic medications are supportive agents, but they also have their own adverse-event potential, cautions, and contraindications. For example, the NK1 receptor antagonists, 5HT
3 receptor antagonists, and dexamethasone all are inducers of and/or metabolized by cytochrome p450 enzymes,5 so indirect drug-drug interactions with antineoplas-tics and other concomitant medications need to be considered.1,5-8
5HT3 Receptor AntagonistsThe 5HT3 receptor antagonists are selective inhibitors of a particular type of serotonin receptor known to be involved in the mechanism of nausea and vomiting. Serotonin acts through at least 15 different receptors located in the central nervous system and throughout the body.9 Approximately 95% of serotonin in the human body is located in the gastrointestinal tract, involved in intestinal physical mobility and secretions, among other functions.10
The first available 5HT3 receptor antagonists were dolasetron, granisetron, and ondansetron, and these agents are now available in multiple formulations: intravenous (IV), oral tablets, oral solution, and ondansetron is available as an oral rapidly disintegrating tablet, with granisetron available as a transdermal patch (Table 1). Oral for-mulations have been shown to be as effective as intravenous formula-tions,1,11 but may differ in cost (Table 1).4
These agents are generally considered equally effective at prevent-ing CINV, particularly acute emesis,1,11 but IV dolasetron is no longer recommended by National Comprehensive Cancer Network (NCCN) due to an association of IV (but not oral) dolasetron with an increased risk for cardiac arrhythmias.1 The efficacy of 5HT3 receptor antago-nists has a plateau in therapeutic efficacy (further dose escalations do not improve efficacy), but the efficacy of these agents is significantly improved when combined with glucocorticoids.11 A second-generation 5HT3 receptor antagonist became available in 2003: palonosetron for intravenous use.12 It has a higher affinity for the 5HT3 receptor than the first-generation agents, and has a significantly longer half-life13,14 (Table 2). Similar to the first-generation 5HT3 receptor antagonists, palonosetron also has increased efficacy when administered with dexamethasone.1
All 5HT3 receptor antagonists are metabolized by the cytochrome P450 system of enzymes (Table 2), and have reported electrocardio-gram interval changes (QT prolongation).1,12,15-18
The 5HT3 receptor antagonists are recommended by several agencies’ guidelines for the prophylactic treatment of acute and delayed CINV for chemotherapy with high emetogenic potential (HEC), including anthracyclines and cyclophosphamide (AC) combinations, and moder-ate emetogenic potential chemotherapy (MEC)1,4,19 (see the Developing Guidelines section below). These agents are generally well tolerated, with constipation and headache the most common adverse events.20
An additional formulation of granisetron, APF530, may be avail-able in the near future. It uses a unique drug delivery technology that allows efficacy for 5 days after a single subcutaneous injection.21 The drug company has resubmitted a New Drug Application to the FDA
OncOlOgyC o n s u lt a t i o n s
INTRODUCTION
Chemotherapy-induced nausea and vomiting (CINV) are among the most common and debilitating side effects of cancer treatment. The significant improvement in CINV prevention with the approval of new agents has helped reduce its severity and incidence, such that the modern clinician may not recognize the importance or predict the potential difficulties of successful prophylactic treatment of symptoms. Despite advances, CINV can still pose a significant clinical challenge.
Without effective prevention and control, CINV can result in metabolic imbalances, dehydration, esophageal tears/rupture, and nutritional deficiencies.1,2 In addition, uncontrolled side effects interfere with the delivery of potentially life-saving treatment by causing dose reductions or delays in administration.1 Controlling chemotherapy-induced emesis also facilitates decreasing the direct and indirect costs of managing cancer,3 including the costs for the patient—both psychologically and financially—of not being capable of returning to work. Successful prevention and control of chemotherapy-induced emesis can also contribute to the overall qual-ity of a patient’s treatment experience, in turn supporting compliance and adherence, preventing premature withdrawal from or cessation of treatment, and preventing side effects that decrease cancer patients’ functional performance status and quality of life.1,3
Question: In your experience, what are the challenges facing clinicians in effectively preventing and treating CINV? Dr. Mohammad Jahanzeb: Many factors can make effective treatment difficult. First and foremost are patient-based factors: those who are on highly emetogenic chemotherapy and/or very young patients. These can be challenging patients, especially if a clinician is not familiar with the available guidelines. Treating physicians also need to be cognizant of non-chemotherapy-related potential causes of nausea and vomiting in a patient such as brain metastases, an electrolyte imbalance, concomitant medications such as opiates, anticipatory CINV, etc.
Dr. Beverly Bell: When I started my fellowship more than 30 years ago, there were not very many effective antiemetics, and the hematology-oncology clinics and hospitals were just miserable. When serotonin inhibitors became available, it was like a night and day shift; the in-troduction of effective antiemetics changed the sociology of the hema-tology-oncology clinics. Patients could now speak to and interact with each other, the fear factor decreased, and new support systems formed. However, challenges remain, such as the delayed vomiting that occurs with platinum agents.
CLASSES OF ANTIEMETIC AGENTS Routine CINV prophylaxis generally involves 5-hydroxytryptamine type 3 (5HT
3) receptor antagonists, NK1 receptor antagonists (Table 1), and/or the corticosteroid dexamethasone used as single agents or

4 Oncology Consultations
for review, and a Prescription Drug User Fee Act (PDUFA) action date of March 27, 2013 has been announced.21
NK1 Receptor Antagonists Currently, only one NK1 receptor antagonist is available in the US, but it is available in two formulations: aprepitant and fosaprepitant, approved for use in the US in 2003 and 2008.7,8 Fosaprepitant is a parenteral water-soluble prodrug of the oral aprepitant,7 and it is effective as a one-day treatment.22 NK1 receptor antagonists are most effective when combined with a 5HT3 receptor antagonist and dexamethasone.11 When a pooled analysis of patients on aprepitant with ondansetron and dexa-methasone was compared with the same regimen without aprepitant, consistent efficacy was observed with the addition of aprepitant among various tumor types and HEC or MEC chemotherapies.23
Di Maio et al24 determined that approximately 20% of patients on HEC therapy are spared from emesis with the use of aprepitant, after com-paring trials where it was reported that 48% to 57% of patients experi-enced vomiting or required rescue therapy in regimens without aprepi-tant compared with the 27% to 37% of patients reported when aprepitant was included. Similarly, the authors also determined that about 10% of patients on MEC therapy are spared from emesis and possible rescue therapy with the use of aprepitant, after comparing the 44% to 58% of patients reported with vomiting or requiring rescue therapy without aprepitant to the 31% to 49% of patients reported with aprepitant.24
Aprepitant is a moderate CYP3A4 inhibitor, and its use requires a 50% dose reduction in dexamethasone dosages, and also affects the metabolism of warfarin and oral contraceptives, but does not clinically affect the dosages of 5HT
3 antagonists.5,7,8 Aprepitant and/or fosaprepi-tant are recommended by available guidelines for HEC and AC combi-nations, and some, but not all, guidelines include NK1 receptor antago-nists as an option in patients on MEC1,4,19 (see the Developing Guidelines section below). These agents are generally well tolerated, with fatigue or asthenia, hiccups, and dyspepsia the most common adverse events.20
Two new oral NK1 receptor antagonists are in development, netupitant (in a fixed-dose combination with palonosetron) and ro-
lapitant.25 Netupitant-palonosetron capsules recently completed two phase III clinical trials,26,27 and has a potential market launch in 2014.28 Rolapitant has also several phase III trials ongoing with an oral formulation,29-31 and results are expected in the second half of 2013,32 with a potential market launch of this product in 2014.28 An intravenous formulation of rolapitant is also in clinical trials.32 Another novel NK1 receptor antagonist, casopitant, was in develop-ment, and completed phase III clinical trials, but the pharmaceutical company withdrew the application for FDA approval after the FDA re-quested additional safety data that required further clinical trials.19,33
Dopamine AgonistsDopamine agonists were historically the drugs of choice for CINV, but these agents have a lower therapeutic index than the 5HT3 re-ceptor antagonists, NK1 receptor antagonists, and glucocorticoids for HEC or MEC.11 They are currently generally recommended for use in patients intolerant or refractory to these agents in patients on HEC or MEC, or on an as-needed basis for patients with minimally emeto-genic chemotherapy (MinEC).1,4 Metoclopramide, a 5HT receptor at high doses, can be co-administered with diphenhydramine to prevent the development of extrapyramidal symptoms such as dystonic move-ments, irritability, agitation, or somnolence.34 Metoclopramide comes in multiple dosage forms and has rapid onset of action (1-3 minutes after intravenous administration or 10-15 minutes after oral adminis-tration34).35 Prochlorperazine is an antipsychotic which has multiple effects on neurotransmitter systems, and as such, has some contrain-dications, including patients with severe liver or renal dysfunction, Parkinson’s disease, or hypothyroidism. It comes in oral, intrave-nous, and suppository formulations, and may cause drowsiness or lead to a mild leukopenia in patients if on a prolonged high dosage.36
AntipsychoticsOlanzapine, an antipsychotic with numerous mechanisms of action, including blocking dopamine, serotonin, catecholamines, acetylcho-line, and histamine receptors,37 has evidence of efficacy against em-
Table 1. 5HT3 and NK1 Receptor Antagonists
Class DrugGeneric
Company Brand NameBrand
CompanyCost per dose4,a
Total cost per HEC 3-day treatment cycle4,b
Serotonin (5HT3)
antagonistsGranisetron
Oral InjectionTransdermal
SeveralSeveral
NA
Kytrilc
Kytrilc
Sancuso
(Discontinued)(Discontinued)Prostrakan Inc.
0.6817.92NA
0.6817.92NA
Ondansetron ODTOral solution Inj and with
dextrose
SeveralSeveralSeveral
Zofran ODTZofranZofran
GlaxoSmithKlineGlaxoSmithKline GlaxoSmithKline
1.04NA
1.19
2.08NA
2.38
Dolasetron OralInjectiond
NANA
AnzemetAnzemet
sanofi-aventissanofi-aventis
65.21NA
65.21NA
Palonosetron Injection
Teva Pharma and Dr Reddys Labsc,e Aloxi Eisai 188.70 188.70
Neurokinin 1 (NK1) receptor antagonists
Aprepitant 125 mg oral 80 mg oral
Sandoz Pharmac Emend Merck 150.4596.29
343.03
Fosaprepitant Powder for IV NA Emend Merck 262.65 262.65
Inj=injection; NA=not available; ODT=oral disintegrating tablet; (x)=no longer available under this brand. a Drug prices determined by clear (non-shaded) boxes if both brand and generic available. Drug prices based on reimbursement rates from the Centers for Medicare & Medicaid Services as of the first quarter of 2011, computed at the manufacturer’s average sales price plus 6%. Other treatment-related direct and indirect costs were not considered. Actual treatment costs and reimbursement will most likely vary considerably across regions, payers, institutions, and practices, as well as over time, and the reader should consult current local cost information specific to the specific environment. b Per ASCO guidelines. c Not available as of publication. d Intravenous dolasetron not included in NCCN guidelines due to an association with an increased risk for cardiac arrhythmias.1
e Tentative approval by FDA.

Oncology Consultations 5
esis similar to other agents, but has a potentially superior response to nausea.38-43 Olanzapine is included in the current guidelines as an option for refractory and/or breakthrough CINV.1,4,19
DEVELOPING GUIDELINESQuestion: Are guidelines useful and applicable to real-life practice? What are the roadblocks to following these guide-lines encountered by clinicians?
Dr. Jahanzeb: Guidelines are useful, but gaps exist. They can be chal-lenging because the guidelines are more permissive than restrictive, with several options at every step. It is good in that we have all the options to work with, but the practitioner has no guidance on which option may be the best.
In my experience, you see both extremes: low-risk chemotherapies accompanying “big gun” antiemetic regimens, and some high-risk chemotherapy regimens being undertreated. Systems or pathways may bundle chemotherapies with antiemetics, but the patient may not get the right match due to a lack of leeway (or incentive) in pre-scribing practices to tailor to the individual patient. In some insti-tutions, the doctors only choose the chemotherapy regimen, and a nurse or pharmacist will add the antiemetics. It’s difficult to quantify the occurrence of these issues at a population level, and part of the overall challenge is variation in practice.
Dr. Bell: Guidelines are generalities. Though they are put together by some of the best authorities, they offer many options and are not specific. For practitioners not accustomed to using antiemetics, they are helpful.
Medical institutions may have their own pathways, algorithms of antiemetic supportive care, and/or have prewritten/computerized or-ders based on the chemotherapies ordered.
My role is to be an extension of the whole team: the patients, the providers, and the payers. Payers look at what chemotherapy the pa-tient is receiving. From an audit perspective it’s not always easy to evaluate the antiemetics, because, again, the guidelines are helpful but not very specific. Still, we have to ensure adequate supportive care, because once a patient starts vomiting, it is so difficult to stop.
Evidence shows that with the proper use of antiemetics, emesis can be prevented in the majority of patients. Several organizations have guidelines for the management of CINV, including the NCCN,1 the American Society of Clinical Oncology (ASCO),4 and the Multina-tional Association of Supportive Care in Cancer (MASCC)/European Society for Medical Oncology (ESMO) joint guidelines19,44 (Table 3), yet management of CINV continues to be a problem, and implementa-tion of these guidelines is suboptimal.45,46
It is generally recommended that the aggressiveness of treatment should correspond with the emetogenicity of chemotherapy agents used. This has resulted in the development of a grading system, with categories based on associated rates of CINV incidence. An agent is considered to be1,47,48:
• HEC if the incidence of CINV occurs in more than 90% of pa-tients
• MEC if CINV is reported in 30% to 90% of patients• Low emetogenic chemotherapy (LEC) if CINV is reported in 10%
to 30% of patients• MinEC if less than 10% of patients get CINV from the agent or
regimen For example, cisplatin is an antineoplastic drug classically associ-
ated with acute and delayed emesis potential, and the current NCCN guidelines list all doses of cisplatin as HEC,1 though previous versions divided the emetogenicity by the dose administered.49 In the case of combination chemotherapy, the recommended treatment is based on the most emetogenic agent.1,4 For example, the most appropriate an-tiemetics for patients on AC therapy are along the lines of the HEC (Table 3), even though each agent alone may be considered moderate risk.4,19,49 Chemotherapeutic agents in combination may potentiate each other’s emetogenicity50 and are not always recognized by the cur-rent grading systems.51,52 Furthermore, because of the design of the tri-als used to create the grading system, these categories describe acute emetogenicity that occurs within 24 hours of a single dose of the che-motherapy,52 and therefore may be unable to accurately account for an agent’s potential to cause nausea or delayed emetogenicity.
Even the best guidelines can only help if patients are receiving care based on them. The reported adherence to antiemetic guidelines is low, with a meaningful amount of both overtreatment and undertreatment, compared with guideline recommendations reported.45,46 The ASCO Quality Oncology Practice Initiative Programs of Excellence, which in 2012 performed institutional chart review of 12,621 charts at 289 in-stitutions desiring to be recognized as a Program of Excellence, found that less than 70% of patients were receiving aprepitant with HEC.53 Another study of US outpatient hospital facilities reported that apre-pitant was used in approximately 5.1% of patients receiving HEC (n = 3069) and 0.9% of patients receiving MEC (n = 16,070) between 2003 and 2007.54 Current guidelines recommend NK1 receptor antagonists for 100% of patients on HEC and AC,1,4,19 and ASCO and NCCN guide-lines include aprepitant or fosaprepitant as an option for patients on MEC.1,4 The reason for the underutilization of aprepitant may include unfamiliarity with the agent (first approved by the FDA on March 26, 2003) or the cost (especially considering it is an adjunct and not an alternative to 5HT
3 antagonists). A generic version of aprepitant has been approved in the US,55 and exclusivity for brand-name aprepitant expires on March 19, 2013.56 However, the pricing of the generic versus the branded formulation remains to be seen.
According to reports evaluating the rate of guideline adherence for members of their respective institutions, prophylaxis of acute CINV was nonadherent to guidelines in 39% to 45% of patients.45,46 For de-layed CINV, treatment was nonadherent to guidelines in 54% to 89% of patients,45,46 with a significant overuse of 5HT3 antagonists repor- ted for prophylaxis of delayed CINV.46 The odds for complete re-sponse, defined as no emesis and no use of rescue therapy, for both acute and delayed phases, were improved in the group following the guidelines.45 The rates for health care visits were lower in the guideline-following cohort, with statistically more patients in the guideline-inconsistent group requiring additional emergency de-partment (ED) and specialist visits in the 5 days after initiation of cycle 1 chemotherapy, but the number of hospital days was not statistically different between guideline-consistent and guideline-inconsistent cohorts.45
Although guidelines are valuable tools, they generalize treatment options, and CINV may demand a patient-tailored management ap-proach.25,57 Guidelines are what work best for most patients. They are not necessarily the best for all patients undergoing all regimens, and a percentage of patients do not respond to established antiemetics/antiemetic combinations despite consistency with guidelines.51
Practitioners and institutions need effective strategies to further reduce CINV, especially in the delayed phase, to reduce health care
Table 2. 5HT3 Receptor Antagonists5HT3 Receptor
Antagonist T1/2, hCytochrome P450
Metabolism
Dolasetron 7-815 CYP2D6, CYP3A415
Granisetron 5-918 CYP3A4,18 CYP1A1109
Ondansetron 3-616,17 CYP1A2, CYP2D6, CYP3A416,17
Palonosetron ~4012 CYP2D612
CYP=cytochrome P450; h=hours; T1/2
=half-life.

6 Oncology Consultations
utilization and costs.54 Any developed plans for effective CINV sup-portive care need frequent reevaluation, including careful consider-ation of agent efficacy and cost-effectiveness to limit the under- and overtreatment of patients in a practice setting, which can include the development of evidence-based pathways that are in line with estab-lished CINV guidelines.
COST CONSIDERATIONSDr. Jahanzeb: Many institutions also have their own pathways for clini-cians to adhere to, which use evidence-based guidelines as a starting point, and then take pharmacoeconomics into consideration.
Dr. Bell: We have to provide adequate supportive care because readmis-sion for delayed vomiting can become very expensive and troublesome for all concerned.
In managed care, we tend to be more concerned with whether the chemotherapy is appropriate, but we’re now seeing more questions regarding antiemetics. With the next-generation antiemetics, which are very effective and more expensive, we may begin to question the shotgun approach of dexamethasone, palonosetron, aprepitant, ondansetron, and whether it would be more cost-effective to stratify the way the NCCN guidelines try to do. Most companies will pay for antiemetics. They generally cost less than chemotherapy, although
Table 3. Summary of Recommended Antiemetic GuidelinesEmetogenic class and emetic
potential NCCN1 ASCO4 MASCC/ESMO (international)19,44
Acute CINV
High Paloa + Dex + NK1 (±Lorazepam) (±H
2 blocker or PPI)
5HT3 + Dex + NK1 5HT
3 + Dex + Apr
AC Paloa + Dex + NK1 (±Lorazepam) (±H
2 blocker or PPI)
5HT3 + Dex + NK1 5HT
3 + Dex + Aprc
Moderate (no AC) Paloa + Dex (±NK1)(±Lorazepam PRN) (±H
2 blocker or
PPI)
Paloa + Dex (±NK1b) Palo + Dex
High to moderate oral Granisetron or Ondansetron(±Lorazepam PRN) (±H
2 blocker or
PPI)
Classification not used, oral included with IV in ‘High’ or ‘Moderate’
Classification not used, oral included with IV in ‘High’ or ‘Moderate’
Low Dex or Metoclopramide or Prochlorperazine(±Lorazepam PRN) (±H
2 blocker or
PPI)
Dex Dex or 5HT3 or DRA
Minimal No routine prophylaxis No routine prophylaxis No routine prophylaxis
Low to minimal oral PRN Metoclopramide or PRN Prochlorperazine or PRN Haloperidol(±Lorazepam PRN) (±H
2 blocker or
PPI)
Classification not used, oral included with IV in ‘Low’ or ‘Minimal’
Classification not used, oral included with IV in ‘Low’ or ‘Minimal’
Delayed CINV
High (5HT3 for consideration if Palo not
used d1) + Dex + (Apr if Fos not used d1) (±Lorazepam) (±H
2 blocker or PPI)
Dex + (Apr if Fos not used d1)
Dex + Apr
AC (5HT3 for consideration if Palo not
used d1) + Dex + (Apr if Fos not used d1) (±Lorazepam) (±H
2 blocker or PPI)
Dex + (Apr if Fos not used d1)
Apr
Moderate (no AC) (5HT3 if Palo not used d1) or Dex
or Apr ± Dex (if Apr used d1) (±Lorazepam PRN) (±H
2 blocker or
PPI)
Dex Dex
High to moderate oral Not reported after stop chemotherapy
Classification not used, oral included with IV in ‘High’ or ‘Moderate’
Classification not used, oral included with IV in ‘High’ or ‘Moderate’
Low Metoclopramide or Prochlorperazine PRN
No routine prophylaxis No routine prophylaxis
Minimal No routine prophylaxis No routine prophylaxis No routine prophylaxis
Low to minimal oral Granisetron or Ondansetron Classification not used, oral included with IV in ‘Low’ or ‘Minimal’
Classification not used, oral included with IV in ‘Low’ or ‘Minimal’
5HT3=serotonin receptor antagonists (“setrons”); AC= anthracycline and cyclophosphamide; Apr=aprepitant; Dex=dexamethasone; DRA=dopamine receptor antagonist; Fos=fosaprepitant;
NK1=NK1 receptor antagonists (aprepitant or fosaprepitant); Palo=palonosetron; PPI=proton pump inhibitor; PRN=as needed. a If palonosetron is not available, use first-generation 5HT
3, though NCCN does not recommend IV dolasetron due to association with increased risk of cardiac arrhythmias.1
b If use NK1 receptor antagonist, any 5HT3 is allowed.
c If NK1 receptor antagonist is not available, palonosetron is preferred 5HT3 receptor antagonist.

Oncology Consultations 7
the antiemetics can be expensive. The conundrum is how liberal or tightly should we control the antiemetic options? Again, once a pa-tient starts vomiting, it is difficult to stop.
We should be reviewing the whole treatment package more con-sistently, keeping an eye on the cost-effectiveness of this type of symptom control. We can also do claims reviews, we know what the patients are getting upfront, and be sure they are getting antiemet-ics. Finally, compliance and adherence need to be looked at, risks of recurrence and resistance should be evaluated, and we need to look at the appropriateness of treatment as regards both cost and effectiveness. Engaging the patient in understanding the value of emotional, clinical, and financial investment in antiemetics is critical to effectiveness. Ultimately, if the patient does not recognize and feel a benefit from any therapy, it is difficult to overcome nonadherence.
An additional issue is that clinical trials are needed to further im-prove care, but individuals may be limited in enrollment due to costs and managed care stipulations. We have to do the trials to get the new agents to treat the diseases that are out there. We cannot and should not let patients suffer from CINV.
CINV results in a high amount of health care resource utilization. The direct costs of CINV include the costs of the antiemetic regimens, as well as administration devices, time from nurses and physicians for additional care, and potentially extended hospitalization or read-mission.24 Indirect costs of CINV can include reduced productivity at work and/or workdays lost for both patients and caregivers.24 The most frequently used health care resources for patients with uncon-trolled CINV in one study were rescue medication, additional office visits, or outpatient hospital visits.58
A report from Italy determined there was an 85% increase in over-all costs when CINV is not well controlled,59 and another from Aus-tralia found that 45% of unplanned presentations to the hospital for patients who had received chemotherapy in the previous 6 months were due to nausea and/or vomiting.60 A recent US report found that 13.8% of patients who had received HEC or MEC required a CINV-associated hospital visit; 0.2% were due to acute CINV, and 13.7% were delayed CINV.54 The hospital admissions associated with CINV were 64% inpatient (with a mean cost of over $7400), 26% outpatient (with a mean cost of just under $1500), and 10% ED visits (with a mean cost of over $900), with an overall mean hospital-reported cost of $5299 for a patient with CINV.54 Another recent US report determined that CINV events in a hospital setting cost approximately $1850 per day.61 Using data from before the nonclinical trial use of aprepitant and palonosetron, the cost of uncontrolled CINV was ap-proximately $1300 higher per patient of working age than that of a patient of working age with controlled CINV, with this report having 28% of patients defined as uncontrolled.62
As for the cost of antiemetics themselves, a recent market analy-sis estimated that the global CINV market for 2013 would be over 1.5 billion USD.28 An Italian group compared the cost of antiemetics with the cost of commonly used chemotherapy in Italy from 2011. The authors determined that maximal guideline-following antiemetics for prophylaxis cost 2.3% to 13.2% of frequently used chemotherapy regimens docetaxel, doxorubicin, cyclophosphamide (TAC), cisplatin with pemetrexed, cisplatin with gemcitabine and bevacizumab, or cisplatin with capecitabine and bevacizumab; however, with older regimens such as fluorouracil with epirubicin and cyclophospha-mide, the antiemetics were 42.5% to 82.8% the cost of the chemo-therapy.24
Other studies evaluated the cost-effectiveness of particular agents. 5HT
3 antagonists were found to be cost-effective in studies published in the late 1990s from both the United States63 and Canada.64 An analysis of the cost-effectiveness of aprepitant performed in Belgium found the drug costs to be worth the improvement in quality of life and improvement in CINV treatment-associated costs.65 Cost-effec-tiveness reports raise a number of vital questions24:
• How much is the health care system willing to pay to achieve a reduction in a distressing but time-limited side effect like CINV?
• How can we properly quantify the impact that CINV has on the physical and mental status of patients?
• What is the impact of these adverse events on the daily quality of life?
• How can all of the indirect costs (for the patient, the caregivers, the family, and society) deriving from the failure of antiemet-ics prophylaxis be adequately assessed and incorporated into a pharmacoeconomic model?
PERSONALIZING TREATMENTQuestion: How can clinicians best personalize treatment for CINV?
Dr. Jahanzeb: What I have found most productive for delayed CINV, which I see a fair amount of because I prescribe a lot of cisplatin and doxorubicin-based therapies, is to tailor and individualize the antiemet-ics to the patient; one size does not fit all.
Dr. Bell: I do not know how well algorithms and guidelines work for this problem when these are being used in practice. They are so impersonal when the clinician may need individualized treatment options. This is a problem. We want to be efficient yet get treatment that works. Still, it requires some art to customize the regimen to prevent breakthrough or anticipatory CINV. Patients must be assured that this intolerable side effect of cancer and treatment will be controlled.
Once CINV begins, it is generally more difficult to control; there-fore, it is much easier to prevent nausea and/or vomiting than to treat it.1 Although some health care practitioners and patients may believe that CINV is an indication that the chemotherapy is working,66 this relationship has never been demonstrated,52 and CINV should be pro-phylactically managed, if at all possible. Different factors may limit optimal antiemetic control regardless of the antiemetics the clinician prescribes.
The 2011 ASCO guidelines suggest that it might be prudent for a clinician and patient to have a discussion about cost and its impact on treatment compliance and patient finances4 to improve patient anxi-ety and treatment compliance. Clinicians may also need options for treatment choices if there is variability in renal or liver function, or if the patent has comorbidities (eg, preexisting arrhythmias or elec-trocardiogram abnormalities), in addition to financial and insurance considerations.67 If patient compliance is believed to be a problem, switching to a single dose of fosaprepitant and palonosetron admin-istered on the day of chemotherapy or use of the granisetron patch and/or the patient has a history of CINV (causing an inability to ef-fectively administer oral medications) may help minimize CINV risk on multi-day aprepitant and/or a first-generation 5HT
3 antagonist.Risk factors for CINV include patient characteristics such as age,
gender, alcohol use, history of motion sickness and/or morning sick-ness, and behavioral characteristics that may be influenced by previ-ous emesis with chemotherapy, anxiety, and expectations of chemo- and antiemetic therapies.68
An individual’s genetic and molecular characteristics, such as cy-tochrome P450 expression levels or presence of a 5HT3 receptor mu-tation, have also been identified as risk factors for CINV, making an individual more or less likely to experience these symptoms.51,68,69 Genetic polymorphisms have been reported for the cytochrome P450 metabolizing enzyme CYP2D6 that may be responsible for variation in responses to particular 5HT
3 receptor antagonists between individual patients. Depending on their genotype, individuals can be character-ized as extensive CYP2D6 metabolizers (the majority of the popula-tion), or poor, intermediate, or ultrarapid CYP2D6 metabolizers.70,71 Ultrarapid metabolizers given ondansetron or tropisetron had a sig-nificantly greater number of acute and delayed emesis episodes than

8 Oncology Consultations
non-ultrarapid metabolizers.71 Some of these risks can be eliminated with newer agents. Studies seem to suggest that gender does not affect CINV incidence once aprepitant is added to a patient’s regimen,72 and palonosetron has minimal variation in metabolism between poor and extensive CYP2D6 metabolizers.12
Even with the best antiemetics and following guidelines, 33% to 64% of patients still experience nausea.42,73-75 The precise role of NK1 antagonists in nausea prevention is still unclear. One study presented in 2008 shows an improvement in nausea when aprepi-tant is in the prophylaxis regimen,76 but there is still a significant amount of nausea despite aprepitant 3-drug regimens.42 Part of the issue may be due to differences between what patients experience and what clinicians believe is occurring, both in incidence and se-verity,77 a difference not nearly as vast with emesis.78 This is prob-ably due in part to the subjective nature of nausea and/or different reporting tools used to assess nausea, as well as a disconnect be-tween the definition of nausea in different cultures.79,80 Clinicians ruling out other things patients may interpret as nausea (eg, dys-pepsia) is encouraged.1,79
Although CINV is generally treated with antiemetics, nausea may be caused by different pathophysiologic mechanisms1 that may not respond to antiemetic therapy, or one antiemetic may be more effec-tive than another depending on the nausea’s root cause.68
ANATOMY AND PATHOPHYSIOLOGYDr. Bell: Right now we are treating symptoms, but there is still so much we do not understand about the process and the factors that influence nausea, so additional work can still be done. There has to be an objec-tive approach to what we are doing with these agents in an area with so much subjectivity.
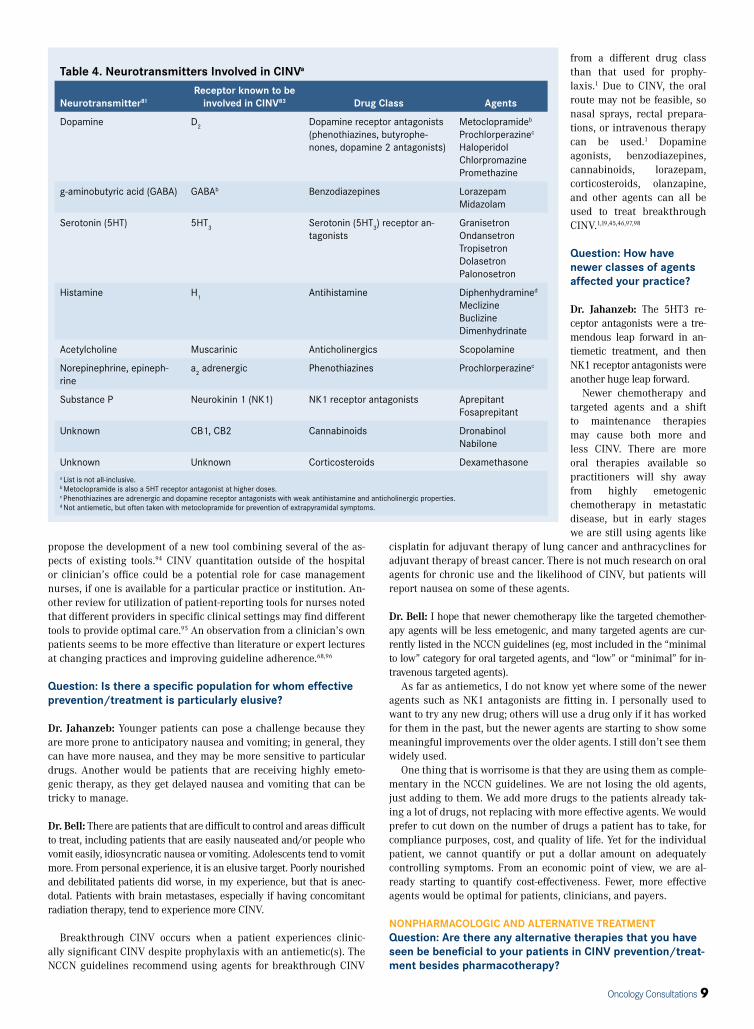
Understanding the pathophysiology of emesis has helped develop effective antiemetic agents that have revolutionized CINV manage-ment. However, the mechanisms behind CINV are varied and complex, involving more than two dozen neurotransmitter and receptor sets in-volved in initiating symptoms and chronic persistence of CINV.81 Vom-iting was historically been postulated to be caused by a distinct location (“vomiting center”) in the medulla,82 but is now believed to not be a “center” per se, but multiple connected neuronal areas in the medul-la.20,83 This area is stimulated by nerves from a chemoreceptor trigger zone (area postrema in the medulla), the pharynx and gastrointestinal tract, and cerebral cortex (sensory input, anxiety and memory).1,83,84 These afferent pathways use particular neurotransmitters, and efferent pathways going to the nerves in end organs causing the vomiting uti-lize some similar and some distinct neurotransmitters from those used in the afferent pathways. The pathways include interactions involving serotonin and its receptor 5HT
3 and substance P and its receptor neu-
rokinin 1 (NK1) (Table 4).83 Emesis is believed to involve85:• The brainstem “vomiting center” in the medulla which pre-
dominantly consists of substance P and NK1 receptors • Gastrointestinal vagal afferent nerve fibers that have a pre-
dominance of serotonin and 5HT3 receptors, but also contain
substance P and NK1 receptors The roles of these neurotransmitters have helped researchers
better understand and target the mechanisms that underlie the dif-ferent types of CINV. For example, serotonin seems to play the larg-est role during the initiation of symptoms and in the acute symp-toms, while the role of substance P is thought to be a major factor in delayed CINV.20,24,85-87 The biphasic curve of CINV (acute and delayed) is a relative description, and exactly where acute 5HT3-dominant phase ends and delayed substance P-dominant phase be-gins remains unclear.87
CINV CLASSIFICATIONSCINV is classified by the length of time it takes to occur after the administration of chemotherapy1:
• Acute nausea and/or vomiting occurs within minutes up to 24 hours, and generally peaks 5 to 6 hours after chemotherapy.
• Delayed nausea and/or vomiting occurs after 24 hours, and can persist for 5 to 7 days after chemotherapy.
• Anticipatory nausea and/or vomiting occurs before the adminis-tration of the chemotherapy and is thought to be a conditioned response occurring because of prior poor control of CINV.
• Breakthrough nausea and/or vomiting refers to nausea and vom-iting that occurs despite antiemetic prophylaxis and requires “rescue” medication.
• Refractory nausea and/or vomiting is the term used when patients have had failure of antiemetic prophylaxis and/or re-quired rescue medications in previous chemotherapy cycles, and have nausea and/or vomiting in subsequent cycles.
Question: How does your approach to delayed-onset CINV differ from acute-onset symptoms?
Dr. Jahanzeb: Of all the areas we have discussed, delayed-onset CINV is where more research would be the most beneficial. Addi-tional research areas should include the effect of chronic oral ther- apy with respect to CINV, controlling nausea induced by opiates, and radiation-induced nausea.
Clinicians can use NK1 receptor antagonists such as 3 days of aprepitant, or fosaprepitant on day 1 only for prevention of delayed CINV. Clinicians sometimes leave patients on 5HT3 receptor antago-nists for several days, or use dexamethasone, which can lead to blood sugar fluctuations in diabetics or to other side effects like thrush. If the patient is left on dexamethasone for longer than a few days, it can cause other adverse events and patients will need to be tapered off. A granisetron patch has been introduced, but patients may remove it for various reasons. We still do not have the ideal solution that works for all patients.
Dr. Bell: The NCCN Guidelines cite a Canadian meta-analysis that a 5HT3 antagonist (ie, ondansetron) on days 2 to 4 was not cost-effective for delayed emesis. However, when ondansetron was used alone, it did protect against delayed emesis in this meta-analysis. Delayed nausea and vomiting is difficult to stop. It also has social implications. Older patients in the hospital may not want to stay for extra days to receive the desired hydration required to flush out the platinums, even with ondansetron. Apart from experience with the patient and their chemotherapy, it is hard to predict who will have difficulty. The vomiting center and the individual patient response to chemotherapy or the antiemetics remains an enigma in many ways.
Delayed CINV may go underappreciated because it occurs after patients leave observation of medical personnel.52,53 The adminis-tration of prophylaxis for single-day chemotherapy occurs under medical supervision on day 1, but not on subsequent days when the patients are taking the prophylaxis at home.53 One study from Sing- apore showed that 42.1% of patients were not adherent to delayed (day 2-4) antiemetic regimens.88 Palonosetron has been shown to be more effective for delayed CINV than first-generation 5HT3 an-tagonists, potentially due to a long half-life, so it may be an option for a clinician when platinums and other agents known to cause delayed CINV are utilized,89-92 or alternatively, a granisetron patch (applied 24-48 hours prior to chemotherapy, can be worn up to 7 days total).93
Additional follow-up measures of a CINV “check” of a nausea and vomiting diary to share with the physician at the next visit, a phone call a few days after chemotherapy, or use of a reporting tool after the first dose of chemotherapy may provide a way to assess a need for changes for future delayed CINV prophylaxis.52 A review of patient-reporting CINV tools was published in 2008.94 The authors believe that none of the evaluated tools were optimal for clinical use, but
Oncology Consultations 9
propose the development of a new tool combining several of the as-pects of existing tools.94 CINV quantitation outside of the hospital or clinician’s office could be a potential role for case management nurses, if one is available for a particular practice or institution. An-other review for utilization of patient-reporting tools for nurses noted that different providers in specific clinical settings may find different tools to provide optimal care.95 An observation from a clinician’s own patients seems to be more effective than literature or expert lectures at changing practices and improving guideline adherence.68,96
Question: Is there a specific population for whom effective prevention/treatment is particularly elusive?
Dr. Jahanzeb: Younger patients can pose a challenge because they are more prone to anticipatory nausea and vomiting; in general, they can have more nausea, and they may be more sensitive to particular drugs. Another would be patients that are receiving highly emeto-genic therapy, as they get delayed nausea and vomiting that can be tricky to manage.
Dr. Bell: There are patients that are difficult to control and areas difficult to treat, including patients that are easily nauseated and/or people who vomit easily, idiosyncratic nausea or vomiting. Adolescents tend to vomit more. From personal experience, it is an elusive target. Poorly nourished and debilitated patients did worse, in my experience, but that is anec-dotal. Patients with brain metastases, especially if having concomitant radiation therapy, tend to experience more CINV.
Breakthrough CINV occurs when a patient experiences clinic- ally significant CINV despite prophylaxis with an antiemetic(s). The NCCN guidelines recommend using agents for breakthrough CINV
from a different drug class than that used for prophy-laxis.1 Due to CINV, the oral route may not be feasible, so nasal sprays, rectal prepara-tions, or intravenous therapy can be used.1 Dopamine agonists, benzodiazepines, cannabinoids, lorazepam, corticosteroids, olanzapine, and other agents can all be used to treat breakthrough CINV.1,19,45,46,97,98
Question: How have newer classes of agents affected your practice?
Dr. Jahanzeb: The 5HT3 re-ceptor antagonists were a tre-mendous leap forward in an-tiemetic treatment, and then NK1 receptor antagonists were another huge leap forward.
Newer chemotherapy and targeted agents and a shift to maintenance therapies may cause both more and less CINV. There are more oral therapies available so practitioners will shy away from highly emetogenic chemotherapy in metastatic disease, but in early stages we are still using agents like
cisplatin for adjuvant therapy of lung cancer and anthracyclines for adjuvant therapy of breast cancer. There is not much research on oral agents for chronic use and the likelihood of CINV, but patients will report nausea on some of these agents.
Dr. Bell: I hope that newer chemotherapy like the targeted chemother-apy agents will be less emetogenic, and many targeted agents are cur-rently listed in the NCCN guidelines (eg, most included in the “minimal to low” category for oral targeted agents, and “low” or “minimal” for in-travenous targeted agents).
As far as antiemetics, I do not know yet where some of the newer agents such as NK1 antagonists are fitting in. I personally used to want to try any new drug; others will use a drug only if it has worked for them in the past, but the newer agents are starting to show some meaningful improvements over the older agents. I still don’t see them widely used.
One thing that is worrisome is that they are using them as comple-mentary in the NCCN guidelines. We are not losing the old agents, just adding to them. We add more drugs to the patients already tak-ing a lot of drugs, not replacing with more effective agents. We would prefer to cut down on the number of drugs a patient has to take, for compliance purposes, cost, and quality of life. Yet for the individual patient, we cannot quantify or put a dollar amount on adequately controlling symptoms. From an economic point of view, we are al-ready starting to quantify cost-effectiveness. Fewer, more effective agents would be optimal for patients, clinicians, and payers.
NONPHARMACOLOGIC AND ALTERNATIVE TREATMENTQuestion: Are there any alternative therapies that you have seen be beneficial to your patients in CINV prevention/treat-ment besides pharmacotherapy?
Table 4. Neurotransmitters Involved in CINVa
Neurotransmitter81
Receptor known to be involved in CINV83 Drug Class Agents
Dopamine D2
Dopamine receptor antagonists (phenothiazines, butyrophe-nones, dopamine 2 antagonists)
Metoclopramideb
Prochlorperazinec
HaloperidolChlorpromazinePromethazine
g-aminobutyric acid (GABA) GABAb Benzodiazepines LorazepamMidazolam
Serotonin (5HT) 5HT3
Serotonin (5HT3) receptor an-
tagonistsGranisetronOndansetronTropisetronDolasetronPalonosetron
Histamine H1
Antihistamine Diphenhydramined
MeclizineBuclizineDimenhydrinate
Acetylcholine Muscarinic Anticholinergics Scopolamine
Norepinephrine, epineph-rine
a2 adrenergic Phenothiazines Prochlorperazinec
Substance P Neurokinin 1 (NK1) NK1 receptor antagonists AprepitantFosaprepitant
Unknown CB1, CB2 Cannabinoids Dronabinol Nabilone
Unknown Unknown Corticosteroids Dexamethasonea List is not all-inclusive.b Metoclopramide is also a 5HT receptor antagonist at higher doses.c Phenothiazines are adrenergic and dopamine receptor antagonists with weak antihistamine and anticholinergic properties.d Not antiemetic, but often taken with metoclopramide for prevention of extrapyramidal symptoms.

10 Oncology Consultations
Dr. Jahanzeb: I shy away from nonpharmaceutical approaches, and try to restrict myself to the evidence-based therapy. If a patient experiences breakthrough CINV, I may try dronabinol. If patients have questions about alternative therapies, I am lucky enough to be able to refer them to a colleague in my group who specializes in alternative and comple-mentary medicine.
Dr. Bell: Well, before the introduction of the more effective agents, pa-tients would try different things—not eating, running beforehand, etc—but nothing seemed to help. Further understanding about the vomiting center location and the communication with the gut and the targeting of the different agents could help. Recognizing that nausea and vomiting are different entities is important; some people have more of a problem with one or the other. It would be interesting to know if that has a physi-ological reason or not, as well.
We need more studies like those cited in the NCCN guidelines, head-to-head challenges of antiemetics versus antiemetics in the same tumors. This is the kind of work we need to go on in the future to determine comparative effectiveness.
Research on nonpharmacologic interventions has been conducted, but alternative therapies lack the empirical evidence seen with phar-macologic interventions. Acupressure,99,100 (electro)acupuncture,101-103 hypnosis, dietary management, cognitive behavioral interventions (for anticipatory nausea), scopolamine,104 grape juice and flavonoid-rich foods,105 ginger,106 and fennel seeds have been evaluated and shown some efficacy for some patients,51,107 but may be short-lived or not adequate for substantial improvement over available pharma-cologic antiemetics.51,108 Some experts recommend certain dietary interventions to help limit CINV, though there is limited evidence: having patients eat smaller, more frequent meals; reduce exposure to food aromas and other stimuli with strong odors; avoid foods that are spicy, fatty, or highly salty; take their antiemetics prior to meals so that the effect is present during and after meals; and/or repeating any previous measures or foods that minimize nausea.108
SUMMARYThe learning objectives of this activity were to review the recently up-dated clinical practice guidelines for CINV and their implementation, identify the contributing factors that predispose patients to developing CINV, examine the managed care aspects of CINV, and evaluate the clini-cal data regarding the efficacy and safety of available agents and combi-nation strategies for the prevention and/or treatment of CINV.
CINV, especially nausea and delayed CINV, can still pose a significant clinical challenge and needs to be managed prophylactically. The goals of prophylactic treatment are to create the optimal patient experience by ensuring the most effective and cost-efficient antiemetic administration. The benefits of effective antiemetic regimens include permitting the prescribed chemotherapy dose and duration to treat the cancer. 5HT3 receptor antagonists, NK1 receptor antagonists, and dopamine receptor antagonists target key neurotransmitter receptors involved in CINV, and are frequently used as prophylaxis of CINV and/or as needed for treat-ment of breakthrough CINV. Multiple guidelines exist for the prevention of CINV at different emetogenic potentials, but adherence to guidelines is generally low, and patient- and situation-specific factors may require tailoring the approach appropriately, especially when breakthrough CINV occurs.
References1. National Comprehensive Cancer Network (2013). Clinical Practice Guidelines in Oncology.
Antiemetics Version 1.2013. Available at http://www.nccn.org/professionals/physician_
gls/f_guidelines.asp. Accessed January 21, 2013.
2. Sepulveda-Vildosola AC, Betanzos-Cabrera Y, Lastiri GG, et al. Palonosetron hydrochlo-
ride is an effective and safe option to prevent chemotherapy-induced nausea and vomit-
ing in children. Archives of Medical Research. Aug 2008;39(6):601-606.
3. Pendergrass KB. Options in the treatment of chemotherapy-induced emesis. Cancer
Practice. Sep-Oct 1998;6(5):276-281.
4. Basch E, Prestrud AA, Hesketh PJ, et al. Antiemetics: American Society of Clinical Oncol-
ogy clinical practice guideline update. Journal of Clinical Oncology : Official Journal of the
American Society of Clinical Oncology. Nov 1 2011;29(31):4189-4198.
5. Aapro MS, Walko CM. Aprepitant: drug-drug interactions in perspective. Annals of
Oncology : Official Journal of the European Society for Medical Oncology / ESMO. Dec
2010;21(12):2316-2323.
6. Saylor MS, Smetana RF. Potential for drug-drug interactions in treating cancer-related
nausea and distress. Journal of Oncology Pharmacy Practice : Official Publication of the
International Society of Oncology Pharmacy Practitioners. Dec 2011;17(4):403-408.
7. Emend (fosaprepitant dimeglumine) for injection, for intravenous use [prescribing
information]. Whitehouse Station, NJ: Merck Sharp & Dohme Corp.; 2012.
8. Emend (aprepitant) capsules, for oral use [prescribing information]. Whitehouse Station,
NJ: Merck Sharp & Dohme Corp.; 2012.
9. Berger M, Gray JA, Roth BL. The expanded biology of serotonin. Annual Review of Medi-
cine. 2009;60:355-366.
10. Gershon MD, Tack J. The serotonin signaling system: from basic understanding to drug
development for functional GI disorders. Gastroenterology. Jan 2007;132(1):397-414.
11. Hesketh PJ. UpToDate website. Prevention and treatment of chemotherapy-induced
nausea and vomiting. Available at http://www.uptodate.com/contents/prevention-and-
treatment-of-chemotherapy-induced-nausea-and-vomiting. Accessed 2-2-13.
12. Aloxi (palonosetron HCl) [prescribing information]. Bloomington, MN: MGI Pharma, Inc.;
2007.
13. Grunberg SM, Koeller JM. Palonosetron: a unique 5-HT3-receptor antagonist for the
prevention of chemotherapy-induced emesis. Expert Opinion on Pharmacotherapy. Dec
2003;4(12):2297-2303.
14. Rojas C, Thomas AG, Alt J, et al. Palonosetron triggers 5-HT(3) receptor internalization
and causes prolonged inhibition of receptor function. European Journal of Pharmacology.
Jan 25 2010;626(2-3):193-199.
15. Anzemet (dolasetron mesylate) [prescribing information]. Bridewater, NJ: sanofi-aventis
US LLC; 2011.
16. Zofran (ondansetron HCl) [prescribing information]. Research Triangle Park, NC: Glaxo-
SmithKline; 2011.
17. Zofran (ondansetron HCl) injection for intravenous use [prescribing information]. Re-
search Triangle Park, NC: GlaxoSmithKline; 2012.
18. Granisetron HCl [prescribing information]. Sellersville, PA: Teva Pharmaceuticals USA;
2011.
19. Roila F, Herrstedt J, Aapro M, et al. Guideline update for MASCC and ESMO in the
prevention of chemotherapy- and radiotherapy-induced nausea and vomiting: results of
the Perugia consensus conference. Annals of Oncology : Official Journal of the European
Society for Medical Oncology / ESMO. May 2010;21 Suppl 5:v232-243.
20. Hesketh PJ. Chemotherapy-induced nausea and vomiting. The New England Journal of
Medicine. Jun 5 2008;358(23):2482-2494.
21. Drugs website. A.P. Pharma announces PDUFA action date for APF530 New Drug Ap-
plication resubmission. Available at http://www.drugs.com/nda/apf530_121016.html.
Accessed February 11, 2013.
22. Grunberg S, Chua D, Maru A, et al. Single-dose fosaprepitant for the prevention of
chemotherapy-induced nausea and vomiting associated with cisplatin therapy: random-
ized, double-blind study protocol--EASE. Journal of Clinical Oncology : Official Journal of
the American Society of Clinical Oncology. Apr 10 2011;29(11):1495-1501.
23. Aapro MS, Schmoll HJ, Jahn F, Carides AD, Webb RT. Review of the efficacy of aprepitant
for the prevention of chemotherapy-induced nausea and vomiting in a range of tumor
types. Cancer Treatment Reviews. Feb 2013;39(1):113-117.
24. Di Maio M, Bria E, Banna GL, et al. Prevention of chemotherapy-induced nausea and
vomiting and the role of neurokinin 1 inhibitors: from guidelines to clinical practice in
solid tumors. Anti-Cancer Drugs. Feb 2013;24(2):99-111.
25. Schwartz R, Kraft S, Schwartz J. Guideline Updates for Health System Pharmacists: Focus
on Chemotherapy-Induced Nausea and Vomiting. Value-Based Cancer Care. 2012;3(2
Supple 1):4-14.
26. ClinicalTrials.gov website. A safety study of oral netupitant and palonosetron for the
prevention of nausea and vomiting. Available at http://www.clinicaltrials.gov/ct2/show/
NCT01376297. Accessed February 11, 2013.
27. ClinicalTrials.gov website. An efficacy and safety study of oral netupitant and palonose-
tron for the prevention of nausea and vomiting. Available at http://www.clinicaltrials.
gov/ct2/show/NCT01339260. Accessed February 11, 2013.
28. Transparency Market Research website. CINV existing & pipeline drugs (Aloxi, Emend,

Oncology Consultations 11
netupitant-palonosetron fdc, APF530 & Rolapitant) - global market opportunity assess-
ment study, 2012 - 2018, free analysis. Available at http://www.transparencymarket-
research.com/cinv-market.html. Accessed February 11, 2013.
29. ClinicalTrials.gov website. A safety and efficacy study of rolapitant for the prevention of
chemotherapy-induced nausea and vomiting (CINV) in subjects receiving moderately
emetogenic chemotherapy (MEC). Available at http://www.clinicaltrials.gov/ct2/show/
NCT01500226. Accessed February 11, 2013.
30. ClinicalTrials.gov website. A safety and efficacy study of rolapitant for the prevention
of chemotherapy-induced nausea and vomiting (CINV) in subjects receiving highly
emetogenic chemotherapy (HEC). Available at http://www.clinicaltrials.gov/ct2/show/
NCT01500213. Accessed February 11, 2013.
31. ClinicalTrials.gov website. Phase 3 safety and efficacy study of rolapitant for the pre-
vention of chemotherapy-induced nausea and vomiting (CINV) in subjects receiving
highly emetogenic chemotherapy. Available at http://www.clinicaltrials.gov/ct2/show/
NCT01499849. Accessed February 11, 2013.
32. Tesaro website. Pipeline. Available at http://tesarobio.com/pipeline/. Accessed February
11, 2013.
33. Feyer P, Jordan K. Update and new trends in antiemetic therapy: the continuing need for
novel therapies. Annals of Oncology : Official Journal of the European Society for Medical
Oncology / ESMO. Jan 2011;22(1):30-38.
34. Metoclopramide [prescribing information]. Lake Forest, IL: Hospira, Inc.; 2012.
35. Smith HS, Cox LR, Smith BR. Dopamine receptor antagonists. Ann Palliat Med.
2012;1(2):137-142.
36. Prochlorperazine [prescribing information]. Bedford, OH: Bedford Laboratories; 2010.
37. Roila F, Garassino M, Fatigoni S. New anti-emetic treatments. Annals of Oncology : Of-
ficial Journal of the European Society for Medical Oncology / ESMO. Jul 2007;18 Suppl
9:ix43-47.
38. Navari RM, Nagy CK, Gray SE. The use of olanzapine versus metoclopramide for the
treatment of breakthrough chemotherapy-induced nausea and vomiting in patients
receiving highly emetogenic chemotherapy. Supportive Care in Cancer : Official Journal of
the Multinational Association of Supportive Care in Cancer. Jan 12 2013.
39. Navari RM, Brenner MC. Treatment of cancer-related anorexia with olanzapine and
megestrol acetate: a randomized trial. Supportive Care in Cancer : Official Journal of the
Multinational Association of Supportive Care in Cancer. Aug 2010;18(8):951-956.
40. Navari RM, Einhorn LH, Loehrer PJ, Sr., et al. A phase II trial of olanzapine, dexametha-
sone, and palonosetron for the prevention of chemotherapy-induced nausea and vomit-
ing: a Hoosier oncology group study. Supportive Care in Cancer : Official Journal of the
Multinational Association of Supportive Care in Cancer. Nov 2007;15(11):1285-1291.
41. Navari RM, Einhorn LH, Passik SD, et al. A phase II trial of olanzapine for the prevention
of chemotherapy-induced nausea and vomiting: a Hoosier Oncology Group study. Sup-
portive Care in Cancer : Official Journal of the Multinational Association of Supportive Care
in Cancer. Jul 2005;13(7):529-534.
42. Navari RM, Gray SE, Kerr AC. Olanzapine versus aprepitant for the prevention of
chemotherapy-induced nausea and vomiting: a randomized phase III trial. The Journal of
Supportive Oncology. Sep-Oct 2011;9(5):188-195.
43. Tan L, Liu J, Liu X, et al. Clinical research of Olanzapine for prevention of chemotherapy-
induced nausea and vomiting. Journal of Experimental & Clinical Cancer Research : CR.
2009;28:131.
44. Multinational Association of Supportive Care in Cancer website. MASCC Antiemetic
Guidelines. Available at http://www.mascc.org/index.php?option=com_content&view=
article&id=261. Accessed December 22, 2012.
45. Aapro M, Molassiotis A, Dicato M, et al. The effect of guideline-consistent antiemetic
therapy on chemotherapy-induced nausea and vomiting (CINV): the Pan European
Emesis Registry (PEER). Annals of Oncology : Official Journal of the European Society for
Medical Oncology / ESMO. Aug 2012;23(8):1986-1992.
46. Burmeister H, Aebi S, Studer C, Fey MF, Gautschi O. Adherence to ESMO clinical recom-
mendations for prophylaxis of chemotherapy-induced nausea and vomiting. Supportive
Care in Cancer : Official Journal of the Multinational Association of Supportive Care in
Cancer. Jan 2012;20(1):141-147.
47. Grunberg SM, Warr D, Gralla RJ, et al. Evaluation of new antiemetic agents and definition
of antineoplastic agent emetogenicity--state of the art. Supportive Care in Cancer : Official
Journal of the Multinational Association of Supportive Care in Cancer. Mar 2011;19 Suppl
1:S43-47.
48. Hesketh PJ, Kris MG, Grunberg SM, et al. Proposal for classifying the acute emetogenic-
ity of cancer chemotherapy. Journal of Clinical Oncology : Official Journal of the American
Society of Clinical Oncology. Jan 1997;15(1):103-109.
49. National Comprehensive Cancer Network (2012). Clinical Practice Guidelines in Oncology.
Antiemetics Version 1.2012. Available at http://www.nccn.org/professionals/physician_
gls/f_guidelines.asp. Accessed December 5, 2012.
50. Van Ryckeghem F, Van Belle S. Management of chemotherapy-induced nausea and
vomiting. Acta Clinica Belgica. Sep-Oct 2010;65(5):305-310.
51. Olver I, Molassiotis A, Aapro M, Herrstedt J, Grunberg S, Morrow G. Antiemetic research:
future directions. Supportive Care in Cancer : Official Journal of the Multinational Associa-
tion of Supportive Care in Cancer. Mar 2011;19 Suppl 1:S49-55.
52. Grunberg SM. Chemotherapy-Induced Nausea and Vomiting Incidence and Prevalence.
American Society of Clinical Oncology 2012 Educational Book. http://www.asco.org/AS-
COv2/Education+%26+Training/Educational+Book?&vmview=edbk_detail_view&confID
=114&abstractID=452012.
53. Aapro MS. The barriers related to implementing antiemetic guidelines into practice,
including cost and drug availability. Presented at: the Annual Meeting of the American
Society of Clinical Oncology; June 1-5, 2012; Chicago, IL.
54. Burke TA, Wisniewski T, Ernst FR. Resource utilization and costs associated with chemo-
therapy-induced nausea and vomiting (CINV) following highly or moderately emetogenic
chemotherapy administered in the US outpatient hospital setting. Supportive Care in
Cancer : Official Journal of the Multinational Association of Supportive Care in Cancer. Jan
2011;19(1):131-140.
55. U.S. Food and Drug Administration website. Drugs @ FDA, ANDA application
090999. Available at http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.
cfm?fuseaction=Search.DrugDetails or http://orange-book.findthedata.org/l/2479/Apre-
pitant. Accessed February 11, 2013.
56. U.S. Food and Drug Administration website. Orange Book: Approved Drug Products with
Therapeutic Equivalence Evaluations NO21549. Available at http://www.accessdata.fda.
gov/scripts/cder/ob/docs/patexclnew.cfm?Appl_No=021549&Product_No=001&table1=
OB_Rx. Accessed January 20, 2013.
57. Vidall C. Chemotherapy induced nausea and vomiting: a European perspective. British
journal of nursing. May 27-Jun 9 2011;20(10):S22, S25-28.
58. Ihbe-Heffinger A, Ehlken B, Bernard R, et al. The impact of delayed chemotherapy-in-
duced nausea and vomiting on patients, health resource utilization and costs in German
cancer centers. Annals of Oncology : Official Journal of the European Society for Medical
Oncology / ESMO. Mar 2004;15(3):526-536.
59. Ballatori E, Roila F, Ruggeri B, et al. The cost of chemotherapy-induced nausea and vomit-
ing in Italy. Supportive Care in Cancer : Official Journal of the Multinational Association of
Supportive Care in Cancer. Jan 2007;15(1):31-38.
60. McKenzie H, Hayes L, White K, et al. Chemotherapy outpatients’ unplanned presenta-
tions to hospital: a retrospective study. Supportive cCare in Cancer : Official Journal of the
Multinational Association of Supportive Care in Cancer. Jul 2011;19(7):963-969.
61. Craver C, Gayle J, Balu S, Buchner D. Clinical and economic burden of chemotherapy-in-
duced nausea and vomiting among patients with cancer in a hospital outpatient setting
in the United States. Journal of Medical Economics. 2011;14(1):87-98.
62. Tina Shih YC, Xu Y, Elting LS. Costs of uncontrolled chemotherapy-induced nausea and
vomiting among working-age cancer patients receiving highly or moderately emetogenic
chemotherapy. Cancer. Aug 1 2007;110(3):678-685.
63. Grunberg SM. Cost-effective use of antiemetics. Oncology. Mar 1998;12(3 Suppl 4):38-42.
64. Stewart DJ, Dahrouge S, Coyle D, Evans WK. Costs of treating and preventing nausea and
vomiting in patients receiving chemotherapy. Journal of Clinical Oncology : Official Jour-
nal of the American Society of Clinical Oncology. Jan 1999;17(1):344-351.
65. Annemans L, Strens D, Lox E, Petit C, Malonne H. Cost-effectiveness analysis of aprepi-
tant in the prevention of chemotherapy-induced nausea and vomiting in Belgium. Sup-
portive Care in Cancer : Official Journal of the Multinational Association of Supportive Care
in Cancer. Aug 2008;16(8):905-915.
66. Salsman JM, Grunberg SM, Beaumont JL, et al. Communicating about chemotherapy-
induced nausea and vomiting: a comparison of patient and provider perspectives. Journal
of the National Comprehensive Cancer Network : JNCCN. Feb 2012;10(2):149-157.
67. Natale JJ. Center of Excellence Media, LLC website. Optimizing antiemetic therapy: prog-
ress and ongoing challenges. Available at http://www.coexm.com/activities/print/0468-
9999-12-016-h01-p. Accessed 1-21-13.
68. Grunberg S. Patient-centered management of chemotherapy-induced nausea and vomit-
ing. Cancer Control : Journal of the Moffitt Cancer Center. Apr 2012;19(2 Suppl):10-15.
69. Tremblay PB, Kaiser R, Sezer O, et al. Variations in the 5-hydroxytryptamine type 3B
receptor gene as predictors of the efficacy of antiemetic treatment in cancer patients.
Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology.
Jun 1 2003;21(11):2147-2155.
12 Oncology Consultations
70. Bernard S, Neville KA, Nguyen AT, Flockhart DA. Interethnic differences in genetic
polymorphisms of CYP2D6 in the U.S. population: clinical implications. The Oncologist.
Feb 2006;11(2):126-135.
71. Kaiser R, Sezer O, Papies A, et al. Patient-tailored antiemetic treatment with 5-hydroxy-
tryptamine type 3 receptor antagonists according to cytochrome P-450 2D6 genotypes.
Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology.
Jun 15 2002;20(12):2805-2811.
72. Hesketh PJ, Grunberg SM, Herrstedt J, et al. Combined data from two phase III trials
of the NK1 antagonist aprepitant plus a 5HT 3 antagonist and a corticosteroid for pre-
vention of chemotherapy-induced nausea and vomiting: effect of gender on treatment
response. Supportive Care in Cancer : Official Journal of the Multinational Association of
Supportive Care in Cancer. Apr 2006;14(4):354-360.
73. Bloechl-Daum B, Deuson RR, Mavros P, Hansen M, Herrstedt J. Delayed nausea and vom-
iting continue to reduce patients’ quality of life after highly and moderately emetogenic
chemotherapy despite antiemetic treatment. Journal of Clinical Oncology : Official Journal
of the American Society of Clinical Oncology. Sep 20 2006;24(27):4472-4478.
74. Gralla RJ, Raftopoulos H. Progress in the control of chemotherapy-induced emesis: new
agents and new studies. J Oncol Pract. 2009;5(3):130-1333.
75. Grunberg SM, Deuson RR, Mavros P, et al. Incidence of chemotherapy-induced nausea
and emesis after modern antiemetics. Cancer. May 15 2004;100(10):2261-2268.
76. Gralla RJ, Raftopoulos H, Bria E, Hesketh PJ. Cisplatin in non-small cell lung cancer
(NSCLC)--Reducing the most prominent toxicity, emesis: Results of a meta-analysis with
1527 patients in randomized clinical trials (RCTs) testing the addition of an NK1 antago-
nist. Presented at: the Annual Meeting of the American Society of Clinical Oncology; May
30-June 5, 2008; Chicago, IL.
77. Basch EM. Summary of standard therapy for the management of nausea and vomiting
and review of newer approved therapies. Presented at: the Annual Meeting of the Ameri-
can Society of Clinical Oncology; June 1-5, 2012; Chicago, IL.
78. Basch E. The missing voice of patients in drug-safety reporting. The New England Journal
of Medicine. Mar 11 2010;362(10):865-869.
79. Aapro MS, Basch EM, Clark-Snow RA, Grunberg SM. Antiemetics: current standards,
emerging approaches, and persistent gaps: panel discussion. Presented at: the Annual
Meeting of the American Society of Clinical Oncology; June 1-5, 2012; Chicago, IL.
80. Grunberg SM. Chemotherapy-induced nausea and vomiting incidence and prevalence.
Presented at: the Annual Meeting of the American Society of Clinical Oncology; June 1-5,
2012; Chicago, IL.
81. Frame DG. Best practice management of CINV in oncology patients: I. Physiology and
treatment of CINV. Multiple neurotransmitters and receptors and the need for combina-
tion therapeutic approaches. The Journal of Supportive Oncology. Mar-Apr 2010;8(2 Suppl
1):5-9.
82. Wang SC, Borison HL. The vomiting center; a critical experimental analysis. Archives of
Neurology and Psychiatry. Jun 1950;63(6):928-941.
83. Hornby PJ. Central neurocircuitry associated with emesis. The American Journal of
Medicine. Dec 3 2001;111 Suppl 8A:106S-112S.
84. Roberts SM, Bezinover DS, Janicki PK. Reappraisal of the role of dolasetron in prevention
and treatment of nausea and vomiting associated with surgery or chemotherapy. Cancer
Management and Research. 2012;4:67-73.
85. Hesketh PJ, Van Belle S, Aapro M, et al. Differential involvement of neurotransmitters
through the time course of cisplatin-induced emesis as revealed by therapy with specific
receptor antagonists. European Journal of Cancer. May 2003;39(8):1074-1080.
86. ilder-Smith OH, Borgeat A, Chappuis P, Fathi M, Forni M. Urinary serotonin metabolite
excretion during cisplatin chemotherapy. Cancer. Oct 1 1993;72(7):2239-2241.
87. Hesketh PJ, Warr DG, Street JC, Carides AD. Differential time course of action of 5-HT3
and NK1 receptor antagonists when used with highly and moderately emetogenic chemo-
therapy (HEC and MEC). Supportive Care in Cancer : Official Journal of the Multinational
Association of Supportive Care in Cancer. Sep 2011;19(9):1297-1302.
88. Chan A, Low XH, Yap KY. Assessment of the relationship between adherence with
antiemetic drug therapy and control of nausea and vomiting in breast cancer patients
receiving anthracycline-based chemotherapy. Journal of Managed Care Pharmacy : JMCP.
Jun 2012;18(5):385-394.
89. Aapro MS, Grunberg SM, Manikhas GM, et al. A phase III, double-blind, randomized
trial of palonosetron compared with ondansetron in preventing chemotherapy-induced
nausea and vomiting following highly emetogenic chemotherapy. Annals of Oncology : Of-
ficial Journal of the European Society for Medical Oncology / ESMO. Sep 2006;17(9):1441-
1449.
90. Eisenberg P, Figueroa-Vadillo J, Zamora R, et al. Improved prevention of moderately
emetogenic chemotherapy-induced nausea and vomiting with palonosetron, a pharmaco-
logically novel 5-HT3 receptor antagonist: results of a phase III, single-dose trial versus
dolasetron. Cancer. Dec 1 2003;98(11):2473-2482.
91. Gralla R, Lichinitser M, Van Der Vegt S, et al. Palonosetron improves prevention of
chemotherapy-induced nausea and vomiting following moderately emetogenic chemo-
therapy: results of a double-blind randomized phase III trial comparing single doses of
palonosetron with ondansetron. Annals of Oncology : Official Journal of the European
Society for Medical Oncology / ESMO. Oct 2003;14(10):1570-1577.
92. Saito M, Aogi K, Sekine I, et al. Palonosetron plus dexamethasone versus granisetron
plus dexamethasone for prevention of nausea and vomiting during chemotherapy: a
double-blind, double-dummy, randomised, comparative phase III trial. The Lancet Oncol-
ogy. Feb 2009;10(2):115-124.
93. Granisetron Transdermal System [prescribing information]. Bedminster, NJ: ProStraken
Inc.; 2011.
94. Brearley SG, Clements CV, Molassiotis A. A review of patient self-report tools for chemo-
therapy-induced nausea and vomiting. Supportive Care in Cancer : Official Journal of the
Multinational Association of Supportive Care in Cancer. Nov 2008;16(11):1213-1229.
95. Wood JM, Chapman K, Eilers J. Tools for assessing nausea, vomiting, and retching.
Cancer nursing. Jan-Feb 2011;34(1):E14-24.
96. Mertens WC, Higby DJ, Brown D, et al. Improving the care of patients with regard to
chemotherapy-induced nausea and emesis: the effect of feedback to clinicians on adher-
ence to antiemetic prescribing guidelines. Journal of Clinical Oncology : Official Journal of
the American Society of Clinical Oncology. Apr 1 2003;21(7):1373-1378.
97. Feeney K, Cain M, Nowak AK. Chemotherapy induced nausea and vomiting--prevention
and treatment. Australian Family Physician. Sep 2007;36(9):702-706.
98. Storr MA, Sharkey KA. The endocannabinoid system and gut-brain signalling. Current
Opinion in Pharmacology. Dec 2007;7(6):575-582.
99. Molassiotis A, Helin AM, Dabbour R, Hummerston S. The effects of P6 acupressure in
the prophylaxis of chemotherapy-related nausea and vomiting in breast cancer patients.
Complementary Therapies in Medicine. Mar 2007;15(1):3-12.
100. Roscoe JA, Bushunow P, Jean-Pierre P, et al. Acupressure bands are effective in reduc-
ing radiation therapy-related nausea. Journal of Pain and Symptom Management. Sep
2009;38(3):381-389.
101. Bao T. Use of acupuncture in the control of chemotherapy-induced nausea and vomiting.
Journal of the National Comprehensive Cancer Network : JNCCN. May 2009;7(5):606-612.
102. Konno R. Cochrane review summary for cancer nursing: acupuncture-point stimulation
for chemotherapy-induced nausea or vomiting. Cancer Nursing. Nov-Dec 2010;33(6):479-
480.
103. Ezzo JM, Richardson MA, Vickers A, et al. Acupuncture-point stimulation for
chemotherapy-induced nausea or vomiting. Cochrane Database of Systematic Reviews.
2006(2):CD002285.
104. LeGrand SB, Walsh D. Scopolamine for cancer-related nausea and vomiting. Journal of
Pain and Symptom Management. Jul 2010;40(1):136-141.
105. Ingersoll GL, Wasilewski A, Haller M, et al. Effect of concord grape juice on chemother-
apy-induced nausea and vomiting: results of a pilot study. Oncology Nursing Forum. Mar
2010;37(2):213-221.
106. Ryan JL. Treatment of Chemotherapy-Induced Nausea in Cancer Patients. European
Oncology. 2010;6(2):14-16.
107. Mustian KM, Devine K, Ryan JL, et al. Treatment of nausea and vomiting during chemo-
therapy. US Oncol Hematol. 2011;4:91-97.
108. Tipton JM, McDaniel RW, Barbour L, et al. Putting evidence into practice: evidence-based
interventions to prevent, manage, and treat chemotherapy-induced nausea and vomiting.
Clinical Journal of Oncology Nursing. Feb 2007;11(1):69-78.
109. Nakamura H, Ariyoshi N, Okada K, Nakasa H, Nakazawa K, Kitada M. CYP1A1 is a major
enzyme responsible for the metabolism of granisetron in human liver microsomes. Cur-
rent Drug Metabolism. Oct 2005;6(5):469-480.