On-site clinical and management mentoring: Driving...
11
On-site clinical and management mentoring: Driving sustainable quality improvements in EmONC Nepali- German Support to the Health Sector Programme Valerie Broch Alvarez, Sept. 2016
Transcript of On-site clinical and management mentoring: Driving...

On-site clinical and management mentoring: Driving sustainable
quality improvements in EmONC
Nepali- German Support to the Health Sector Programme Valerie Broch Alvarez, Sept. 2016

Why still the focus on MNC?
539
281 229
170 190
258
0
100
200
300
400
500
600
1996 2006 2009 2012 2014 2015
Trends in maternal mortality, 1996-2015
50
39 33 33
23
0
10
20
30
40
50
60
1996 2001 2006 2011 2014
SDG target – 12 SDG target -‐ 70
Trends in neonatal mortality, 1996-2014
1. Nepal’s policies focused on access – quality was overlooked 2. Gaps in comprehensive quality of care: Met need for EmONC
(from 22% in 1998 to 41% in 2009) not adequately addressed 3. Centralized pre-service training, limited in-service supervision and
re-training 4. Lack of Midwives

Ø To address inefficiencies in current training and clinical practice - tailor made CD
Ø To retain HW in their communities
Ø To encourage greater continuity of care with focus on processes and organizational aspects (logistics, infrastructure, equipment etc.)
Ø To strengthen the HS, through better networking between public/public, public/private HFs and communities within each district – referral system strengthening
Why mentoring for QoC?

Mentoring for Improving MNHC
GDC support - improve care delivery with emphasis on EmONC through:
Ø On-site training/mentoring at the HF level Ø Developing capacity of the existing district supervisory
structure
Ø Initiation of a systems focus on a combined clinical and management mentoring of health centre teams
Ø Use of data for continuous quality improvement Ø Strengthening of effective referral systems for obstetric
emergencies

Clinical and management mentors (10)
CEONC BEONC BC
Health facility mentoring: Implementation
District 10 9
Districts CEONC
25 24 BEONC HP-BC
Referral system strengthening
321 322 Clinical Management
516 2/5d-4/6w Visits Frequency

Results: SBA-level clinical mentoring
#
MNC QI Tool (# standards)
# Mentees Average % standards met % Improvement
(D/B) Baseline
(B) Endline (E)
Average difference (D= E-‐B)
1 InfecMon prevenMon 128 45.6 85.6 40.0 88% 2 Antenatal care 119 44.2 84.5 40.3 91% 3 ComplicaMons of pregnancy 147 37.9 80.3 42.3 112% 4 Normal Delivery and Immediate
Newborn Care 116 42.5 82.3 40.6 95%
5 Postpartum care (PNC) 112 23.9 81.7 57.8 138% 6 Newborn care 141 31.2 77.6 46.5 149% 7 ComplicaMons of labour and
delivery 122 32.9 81.2 49.3 147%
8 Assessment of newborn with a problem
137 39.6 76.9 37.4 94%
Average % of standards met, baseline and endline

49.6
59.2
59.5
58.1
62.8
46.1
72.7
49.2
80.0
95.6
77.3
81.9
85.7
78.6
92.1
76.4
Tool 1: CommiJee structure and funcNon
Tool 2: Policies and guidelines
Tool 3: Facility management and support
services
Tool 4: Financial management
Tool 5: Human resource management
Tool 6: Hygiene, IP and waste management
Tool 7: InformaNon management and HMIS
Tool 8: TransportaNon and communicaNon
Baseline Endline
Results: Management mentoring
Average % of standards met, management tools (N=45)
Tools # of
standards Average % of standards met
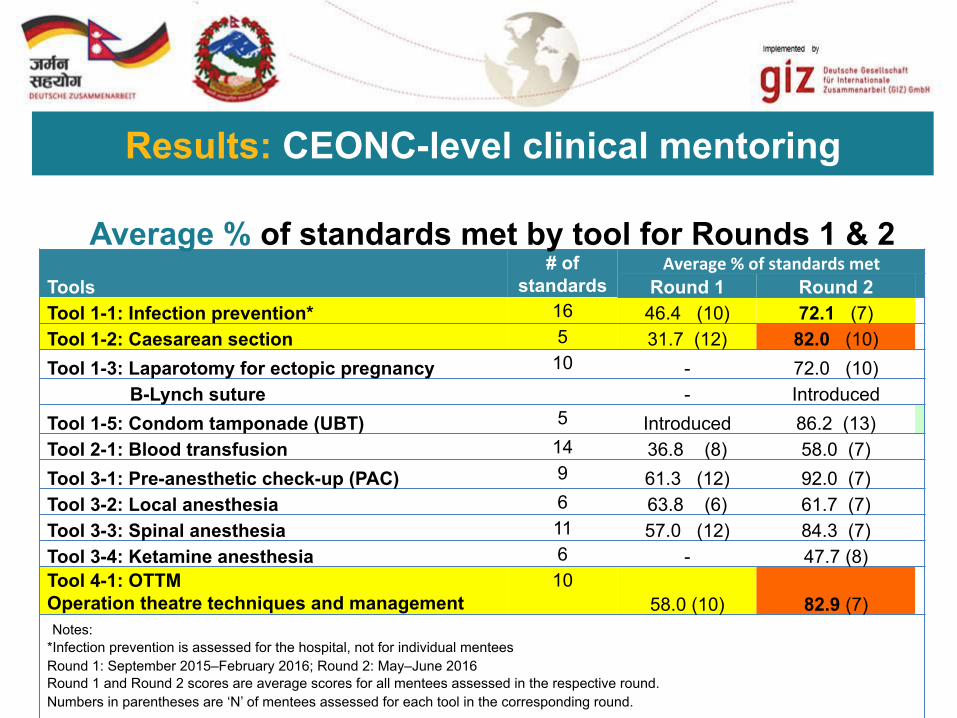
Round 1 Round 2 Tool 1-1: Infection prevention* 16 46.4 (10) 72.1 (7) Tool 1-2: Caesarean section 5 31.7 (12) 82.0 (10)
Tool 1-3: Laparotomy for ectopic pregnancy 10 - 72.0 (10) B-Lynch suture - Introduced
Tool 1-5: Condom tamponade (UBT) 5 Introduced 86.2 (13) Tool 2-1: Blood transfusion 14 36.8 (8) 58.0 (7)
Tool 3-1: Pre-anesthetic check-up (PAC) 9 61.3 (12) 92.0 (7) Tool 3-2: Local anesthesia 6 63.8 (6) 61.7 (7) Tool 3-3: Spinal anesthesia 11 57.0 (12) 84.3 (7) Tool 3-4: Ketamine anesthesia 6 - 47.7 (8) Tool 4-1: OTTM Operation theatre techniques and management
10 58.0 (10) 82.9 (7)
Notes: *Infection prevention is assessed for the hospital, not for individual mentees Round 1: September 2015–February 2016; Round 2: May–June 2016 Round 1 and Round 2 scores are average scores for all mentees assessed in the respective round. Numbers in parentheses are ‘N’ of mentees assessed for each tool in the corresponding round.
Results: CEONC-level clinical mentoring
Average % of standards met by tool for Rounds 1 & 2

Ø Difficult to ensure locally-driven process when funding comes from EDP but essential to drive real change
Ø Staff transfers and vacancies limit effectiveness, both of mentors and mentees
Ø Referral system needs to be fully functional to gain maximum benefit
Ø Learning may be limited in low case load locations and few opportunities to continue practising new skills
Ø Mentoring should be one element of continuous professional development (CPD)
Ø The real cost-effectiveness of mentoring versus other forms of supportive supervision is not yet known
Lessons learned and challenges

Conclusion and outlook
Ø Mentoring improves both clinicians and managers mentees’ motivation, confidence and adherence to MNCH protocols
Ø Mentoring checklists enable evidence-based feedback and continuous QI
Ø Mentorship integrates in-service training and systems improvement into routine care delivery
Ø Incorporation of the concept into NHSS (2015–2020) Ø Institutionalization of the mentorship approach for
continued QoC into the system – focus of next phase

THANK YOU!