
Omega-3 Fatty Acids for Cardiovascular Disease Prevention · Omega-3 Fatty Acids for Cardiovascular...
16
Current Treatment Options in Cardiovascular Medicine (2010) 12:365–380 DOI 10.1007/s11936-010-0079-4 Prevention Omega-3 Fatty Acids for Cardiovascular Disease Prevention Andrew Paul DeFilippis, MD, MSc * Michael J. Blaha, MD, MPH Terry A. Jacobson, MD Address *Johns Hopkins Ciccarone Center for the Prevention of Heart Disease, 600 North Wolfe Street, Carnegie 568, Baltimore, MD 21224, USA Email: [email protected] Published online: 28 May 2010 * Springer Science+Business Media, LLC 2010 Opinion statement Major dietary sources of omega-3 fatty acids are fish containing eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), as well as nuts, seeds, and vegetable oils con- taining α-linolenic acid (ALA). Omega-3 fatty acids, especially those derived from ma- rine sources, may be a useful tool for the primary and secondary prevention of cardiovascular disease. Omega-3s exert their cardioprotective effects through multiple mechanisms, including reducing arrhythmias and altering production of prostaglan- dins, which reduces inflammation and improves platelet and endothelial function. To date, no serious adverse effects of omega-3s have been identified, despite extensive study. In adults, any potential harm from mercury exposure from consuming fish rich in omega-3s is outweighed by the proven cardiovascular benefits of eating fish. Con- cerns over increased bleeding complications have not materialized despite the in- creased concomitant use of aspirin and clopidogrel. We recommend one serving (200–400 g) of fatty fish two times per week and a diet that includes foods rich in ALA for the primary prevention of cardiovascular disease. We recommend one serving (200–400 g) of fatty fish or a fish oil supplement containing 900 mg of EPA + DHA every day and a diet rich in ALA for patients with known cardiovascular disease or con- gestive heart failure. Introduction Interest in omega-3 fatty acids has grown steadily since the observation that Greenland Eskimos have a low in- cidence of cardiovascular disease (CVD) in the setting of a diet rich in fatty fish [1]. Over the past three dec- ades, epidemiologic and experimental data have pro- vided evidence for a beneficial effect of omega-3 fatty acids in preventing CVD [ 2–9•]. This article reviews recent studies that support or refute the notion that omega-3s can prevent CVD, as well as novel data that further our understanding of omega-3s’ mecha- nisms of action. New data support previous studies on the beneficial modulation of platelet activity, the
Transcript of Omega-3 Fatty Acids for Cardiovascular Disease Prevention · Omega-3 Fatty Acids for Cardiovascular...
Current Treatment Options in Cardiovascular Medicine (2010) 12:365–380DOI 10.1007/s11936-010-0079-4
Prevention
Omega-3 Fatty Acidsfor Cardiovascular DiseasePreventionAndrew Paul DeFilippis, MD, MSc*
Michael J. Blaha, MD, MPHTerry A. Jacobson, MD
Address*Johns Hopkins Ciccarone Center for the Prevention of Heart Disease,600 North Wolfe Street, Carnegie 568, Baltimore, MD 21224, USAEmail: [email protected]
Published online: 28 May 2010* Springer Science+Business Media, LLC 2010
Opinion statement
Major dietary sources of omega-3 fatty acids are fish containing eicosapentaenoic acid(EPA) and docosahexaenoic acid (DHA), as well as nuts, seeds, and vegetable oils con-taining α-linolenic acid (ALA). Omega-3 fatty acids, especially those derived from ma-rine sources, may be a useful tool for the primary and secondary prevention ofcardiovascular disease. Omega-3s exert their cardioprotective effects through multiplemechanisms, including reducing arrhythmias and altering production of prostaglan-dins, which reduces inflammation and improves platelet and endothelial function. Todate, no serious adverse effects of omega-3s have been identified, despite extensivestudy. In adults, any potential harm from mercury exposure from consuming fish richin omega-3s is outweighed by the proven cardiovascular benefits of eating fish. Con-cerns over increased bleeding complications have not materialized despite the in-creased concomitant use of aspirin and clopidogrel. We recommend one serving(200–400 g) of fatty fish two times per week and a diet that includes foods rich inALA for the primary prevention of cardiovascular disease. We recommend one serving(200–400 g) of fatty fish or a fish oil supplement containing 900 mg of EPA + DHAevery day and a diet rich in ALA for patients with known cardiovascular disease or con-gestive heart failure.
IntroductionInterest in omega-3 fatty acids has grown steadily sincethe observation that Greenland Eskimos have a low in-cidence of cardiovascular disease (CVD) in the settingof a diet rich in fatty fish [1]. Over the past three dec-ades, epidemiologic and experimental data have pro-vided evidence for a beneficial effect of omega-3
fatty acids in preventing CVD [2–9•]. This articlereviews recent studies that support or refute the notionthat omega-3s can prevent CVD, as well as novel datathat further our understanding of omega-3s’ mecha-nisms of action. New data support previous studieson the beneficial modulation of platelet activity, the

reduction in vascular inflammation, and the novelconcept of omega-3s preserving the “genetic youth”of individual cells [10–16]. In addition, we reviewthe balance of minimal versus optimal daily intake
of omega-3s for CVD prevention and discuss concernsregarding the impact of pollutants often found in fish(methyl mercury, polychlorinated biphenyls [PCBs],and dioxins) [17–19•, 20].
Source and metabolism of omega-3 fatty acids& There are three types of naturally occurring fats, classified by the number
of double covalent bonds present in their constituent fatty acids: satu-rated, monounsaturated, and polyunsaturated (Fig. 1). The food in-dustry created a fourth class, trans fats, by adding hydrogen ions topolyunsaturated fats through a process called hydrogenation (Fig. 1).
& Polyunsaturated fats may be classified further into two groups—omega-3 and omega-6 fatty acids—based on the position within thefatty acid of the first double bond (Fig. 1). The most prominentomega-6 fatty acids in the human diet are arachidonic acid (found inanimal meat) and linoleic acid (found in vegetable oils, seeds, andnuts), which may be converted into arachidonic acid by a desaturaseenzyme (Fig. 2). Major dietary sources of omega-3s are fish con-taining eicosapentaenoic acid (EPA) and docosahexaenoic acid(DHA), as well as nuts, seeds, and vegetable oils containing α-linolenic acid (ALA) (Table 1).
& ALA can be converted to EPA and then DHA by the same desaturaseenzyme that converts linoleic acid to arachidonic acid (Fig. 2). Theconversion of ALA to EPA + DHA is influenced by multiple factors,including competitive inhibition of desaturase by linoleic acid(Fig. 2), negative feedback inhibition of desaturase by EPA + DHA(Fig. 2), and gender differences; therefore, the conversion of ALA toEPA + DHA varies widely among different studies [21–28].
& In totality, most studies suggest that the conversion of ALA to EPA inhumans is inefficient. There is a paucity of epidemiologic and clinical
Figure 1. Classification of fats.
366 Prevention
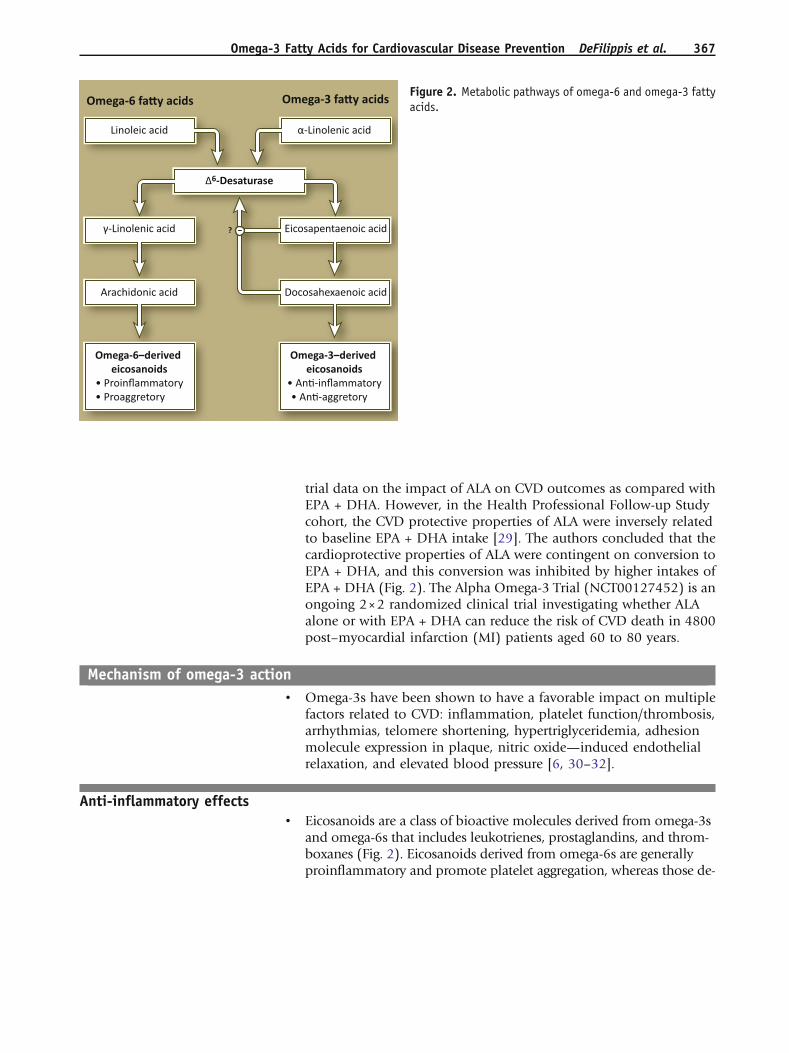
trial data on the impact of ALA on CVD outcomes as compared withEPA + DHA. However, in the Health Professional Follow-up Studycohort, the CVD protective properties of ALA were inversely relatedto baseline EPA + DHA intake [29]. The authors concluded that thecardioprotective properties of ALA were contingent on conversion toEPA + DHA, and this conversion was inhibited by higher intakes ofEPA + DHA (Fig. 2). The Alpha Omega-3 Trial (NCT00127452) is anongoing 2×2 randomized clinical trial investigating whether ALAalone or with EPA + DHA can reduce the risk of CVD death in 4800post–myocardial infarction (MI) patients aged 60 to 80 years.
Mechanism of omega-3 action& Omega-3s have been shown to have a favorable impact on multiple
factors related to CVD: inflammation, platelet function/thrombosis,arrhythmias, telomere shortening, hypertriglyceridemia, adhesionmolecule expression in plaque, nitric oxide—induced endothelialrelaxation, and elevated blood pressure [6, 30–32].
Anti-inflammatory effects& Eicosanoids are a class of bioactive molecules derived from omega-3s
and omega-6s that includes leukotrienes, prostaglandins, and throm-boxanes (Fig. 2). Eicosanoids derived from omega-6s are generallyproinflammatory and promote platelet aggregation, whereas those de-
Figure 2. Metabolic pathways of omega-6 and omega-3 fattyacids.
Omega-3 Fatty Acids for Cardiovascular Disease Prevention DeFilippis et al. 367
rived from omega-3s are predominately anti-inflammatory and inhibitplatelet aggregation [33]. This fundamental difference may account forsome of the cardioprotective effects of omega-3s, as inflammation andthrombosis are fundamental to the development of atherosclerosis andunstable coronary syndromes [34].
& Multiple studies have linked systemic markers of inflammation toCVD risk [35]. This past year, a study of 5677 participants from theMulti-Ethnic Study of Atherosclerosis (MESA) demonstrated an in-verse relationship between omega-3 fatty acid intake and markersof systemic inflammation: C-reactive protein (CRP), interleukin-6(IL-6), and matrix metalloproteinase 3 [13]. These findings wereindependent of age, body mass index, physical activity, smoking,alcohol, and other dietary variables. In another 2009 study of a
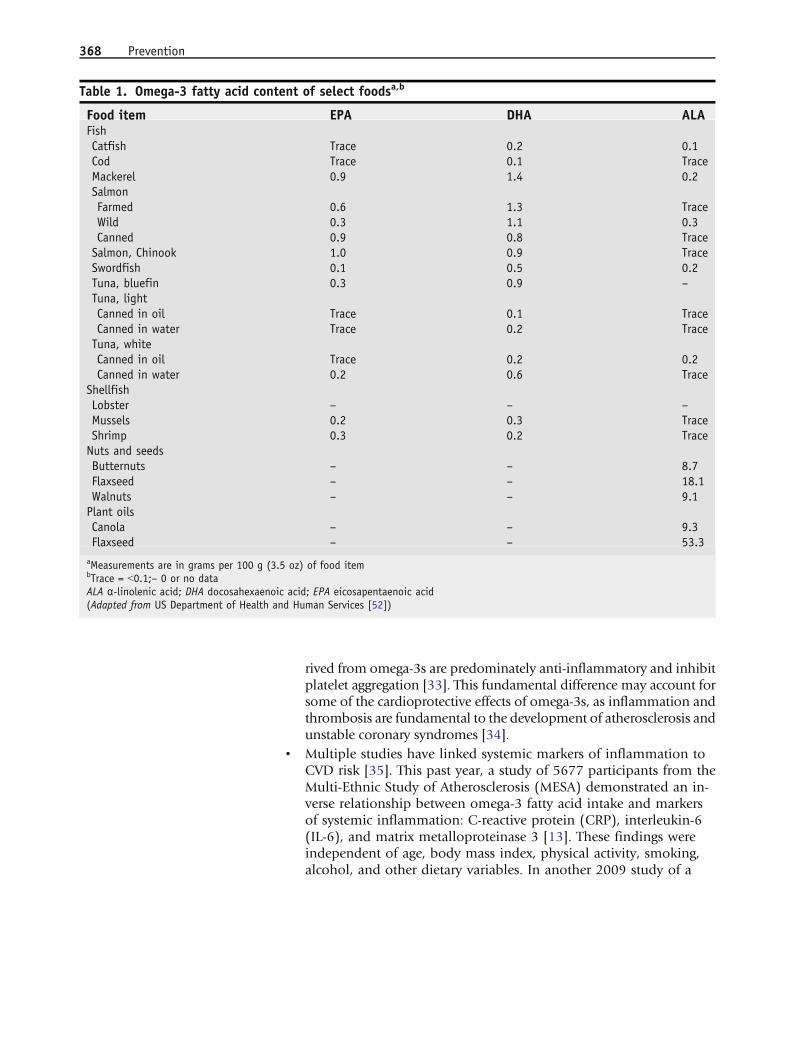
Table 1. Omega-3 fatty acid content of select foodsa,b
Food item EPA DHA ALAFishCatfish Trace 0.2 0.1Cod Trace 0.1 TraceMackerel 0.9 1.4 0.2SalmonFarmed 0.6 1.3 TraceWild 0.3 1.1 0.3Canned 0.9 0.8 TraceSalmon, Chinook 1.0 0.9 TraceSwordfish 0.1 0.5 0.2Tuna, bluefin 0.3 0.9 –Tuna, lightCanned in oil Trace 0.1 TraceCanned in water Trace 0.2 TraceTuna, whiteCanned in oil Trace 0.2 0.2Canned in water 0.2 0.6 Trace
ShellfishLobster – – –Mussels 0.2 0.3 TraceShrimp 0.3 0.2 TraceNuts and seedsButternuts – – 8.7Flaxseed – – 18.1Walnuts – – 9.1Plant oilsCanola – – 9.3Flaxseed – – 53.3
aMeasurements are in grams per 100 g (3.5 oz) of food itembTrace = G0.1;– 0 or no dataALA α-linolenic acid; DHA docosahexaenoic acid; EPA eicosapentaenoic acid(Adapted from US Department of Health and Human Services [52])
368 Prevention
population of 992 individuals with stable coronary heart disease(CHD), dietary omega-3s again were inversely related to CRP and IL-6 after multivariable adjustment [11]. These studies are consistentwith prior omega-3 fatty acid/inflammatory biomarker studies [14,16]. Although epidemiologic evidence suggests strong benefits ofomega-3s on reducing inflammatory markers, the clinical trial evi-dence also is very suggestive of consistent reductions in proinflam-matory cytokines such as IL-6 and tumor necrosis factor-α, with lessconsistent reductions in CRP [30]. Studies of the impact of ALA oninflammation have not shown consistent results, in contrast to theEPA + DHA studies.
Antiplatelet effects& The prostaglandin thromboxane A2 is a major stimulant of platelet
activation/atherothrombosis. Thromboxane is produced by the lib-eration of specific polyunsaturated fatty acids from cell membranes[36, 37]. The prostaglandins produced from omega-6 fatty acids(including thromboxane A2) generally are pro-aggregatory [6, 30]. Incontrast, prostaglandins produced from omega-3 fatty acids are rel-atively anti-aggregatory [30, 38]. Omega-3 fatty acids can displaceomega-6 fatty acid stores needed to produce thromboxane A2 in cellmembranes and act as competitors for the same metabolic pathways[38, 39].
& In vitro studies of human platelets demonstrate reductions inthromboxane A2 production in the presence of omega-3 fatty acids[40]. With omega-3 fatty acids acting as competitive inhibitors of theenzymes needed to produce thromboxane A2, some have hypothe-sized that individuals with higher membrane omega-3 content (highomega-3 intake) will produce less thrombosis-promoting throm-boxane A2 than individuals with lower membrane omega-3 levels.The antiplatelet effect of omega-3 fatty acids was supported by astudy of 62 patients with stable CVD and a laboratory assessmentconsistent with “aspirin resistance.” Omega-3 fatty acid supplemen-tation reduced the incidence of aspirin resistance by 80% in thispopulation [10].
Ventricular and atrial arrhythmias& The antiarrhythmic effects of omega-3s have been reviewed exten-
sively, with data suggesting a protective effect derived from bothbasic and clinical studies [41, 42]. Omega-3s have been shown toinhibit both the fast voltage-dependent sodium channels and the L-type calcium channels. In addition, omega-3s have been shown toinhibit some aspects of the repolarization portion of the potassiumcurrents. The results of these studies suggest that omega 3s maybe helpful in reducing ventricular arrhythmias as well as atrialfibrillation.
Omega-3 Fatty Acids for Cardiovascular Disease Prevention DeFilippis et al. 369

Telomere shortening& An analysis carried out in patients from the Heart and Soul Study has
demonstrated a novel mechanism for the protective effects of omega-3s [12]. Baseline plasma omega-3 levels were inversely related totelomere shortening over 5 years of follow-up in 608 patients withstable coronary artery disease. Telomeres are tandem repeats of DNAthat form a protective cap at the ends of chromosomes, and short-ening of telomeres is an emerging marker of biological age, whichhas been associated with CVD morbidity and mortality. Therefore,omega-3s may reduce CVD mortality by slowing “biological aging”via preserving telomere length.
Recent cardiovascular event outcome studies
Coronary heart disease prevention studies
GISSI-Prevenzione
Several trials were completed in the past few years that significantly addto our knowledge of omega-3s and CVD prevention. These trials build onprevious clinical trials of omega-3s and CVD events, most notably theGISSI-Prevenzione trial [4]. GISSI-Prevenzione was an open-label trialthat randomly assigned 11,324 post-MI patients to one of four groups: 1)1 g/d EPA + DHA, 2) 300 mg/d of a vitamin E supplement, 3) both, or 4)neither. All patients in the trial received appropriate intensive post-MIcare (circa 1993–1999) and had good adherence to a Mediterranean diet,with more than 70% of the participants eating fish at least once a week.Data were collected on 99.9% of participants during the 3.5 years ofintervention, and background medical care did not differ between theintervention and control groups. The EPA + DHA supplement group hada 15% reduction in the combined end point of death, nonfatal MI, andnonfatal stroke (P=0.023) compared with the control group (no sup-plement). Analysis of individual end points showed a 20% reduction intotal mortality (PG0.05), a 30% reduction in cardiovascular death (P=0.02), and a 45% reduction in sudden death (P=0.01). There was noreduction in nonfatal cardiovascular events in the fish oil group.
JELIS
The recent Japan EPA Lipid Intervention Study (JELIS) randomlyassigned 18,645 patients with hypercholesterolemia to receive a statinplus purified EPA (1800 mg/d) or a statin plus placebo [9•]. After anaverage of 4.6 years of follow-up, those randomly assigned to receivea statin plus purified EPA had a 19% relative risk reduction (absoluterisk reduction [ARR], 0.7%; P=0.011) in the combined primary out-come of sudden cardiac death, MI, unstable angina, and coronaryrevascularization compared with those treated with a statin and pla-cebo. Secondary analyses revealed statistically significant reductions inunstable angina and nonfatal coronary events but no significant re-duction in sudden cardiac deaths or coronary deaths in those treated
370 Prevention

with a statin and EPA compared with those treated with a statin andplacebo.
The purified EPA reduced first-time coronary events (primary pre-vention, n=14,981) by 18% and secondary coronary events (second-ary prevention, n=3664) by 19%, but only the secondary preventiongroup reached statistical significance. The lack of significance in theprimary prevention group may be secondary to the very low eventrates in the EPA and placebo groups, (1.4% and 1.7% over 5 years,respectively), or a high baseline level of omega-3 intake in thisJapanese population. Furthermore, the 95% confidence interval forthis 18% reduction in the primary prevention cohort overlappedwith the statistically significant reduction observed in the totalpopulation.
JELIS was the first primary prevention trial with omega-3s. In addition,JELIS was the first randomized controlled trial to show a benefit ofomega-3s beyond uniform statin treatment and the first to show abenefit with EPA supplementation alone (as opposed to EPA + DHA).Although the 18% reduction in the stratified analysis of first coronaryevents did not reach statistical significance, the point estimate of the riskreduction was not significantly different from that seen in the total studypopulation. Thus, the lack of statistically significant benefit most likely isa result of the lack of power in the secondary analyses rather than a truedifference from the significant reduction in CVD events found in thenonstratified study population.
OMEGA trial
The OMEGA trial enrolled 3851 patients within 2 weeks of an MI toreceive omega-3 fatty acids (∼850 mg/d EPA + DHA) or placebo inaddition to optimal medical care [43]. After 1 year of follow-up, nodifferences were seen between the omega-3 and placebo groups withrespect to the primary end point of sudden cardiac death, which wasvery low, 1.5%, in both groups. Incidence of the secondary endpoints also was very low, with no difference between the treatmentgroups. The results of this trial were presented in abstract formbut have not yet been published as a full-length peer-reviewedmanuscript.
The OMEGA trial is at odds with the larger GISSI-Prevenzione trial.The differences may be the result of more effective baseline treatment inthe OMEGA trial, lower-risk patients, or the shorter duration of theOMEGA trial. Limitations withstanding, the results call into questionwhether omega-3s are effective in the short term (1 year) in maximallytreated, low-risk acute coronary syndrome patients.
Congestive heart failure studies
GISSI Heart Failure
The GISSI Heart Failure trial was a randomized, double-blinded, place-bo-controlled 2×2 factorial trial of statins and omega-3 fatty acid sup-
Omega-3 Fatty Acids for Cardiovascular Disease Prevention DeFilippis et al. 371

plementation (∼850 mg/d EPA + DHA) in 6975 patients with chronic,stable heart failure already on optimal medical therapy (renin–angiotensin system and β-adrenergic blockade where indicated) [44•].After a median follow-up of 3.9 years, those assigned to omega-3 fattyacid supplementation experienced a 9% relative risk reduction (ARR,1.8%; PG0.05) in total mortality and an 8% relative risk reduction (ARR,2.3%; PG0.01) in mortality or cardiovascular hospital admissions. Sub-analyses examining the individual causes of mortality (worsening heartfailure, acute MI, sudden cardiac death) were consistent with the overallresult. In this trial, randomization to a statin had no impact on thecoprimary outcome of mortality and death or admission to hospital for acardiovascular reason.
The GISSI Heart Failure trial was the first omega-3 study performedspecifically in the heart failure population. Although the relative riskreduction was modest in this trial, it was additive to modern-day treat-ment with renin–angiotensin system and β-adrenergic blockade, withalmost no safety concerns. This trial led to recommendations of omega-3supplementation for all heart failure patients [18].
Antiarrhythmic studies
Implantable cardioverter-defibrillator studies
A meta-analysis of three double-blind, randomized interventional trialsof omega-3 fatty acids in patients with implantable cardioverter-defib-rillators (ICDs) found no difference in time to appropriate ICD inter-vention between the omega-3 treatment and placebo groups [45]. Thesenegative results contrast with some clinical trial data indicating preven-tion of sudden cardiac death as the major mechanism by which omega-3reduces cardiovascular events [6, 46]. This meta-analysis highlights theneed for more clinical trial data for the role of omega-3s in preventingventricular arrhythmias.
Atrial fibrillation
The use of omega-3s for preventing and treating atrial fibrillation issupported by recent epidemiologic and clinical trials. A prospectivecohort trial of 2174 men older than 18 years found an inverserelationship between serum omega-3 fatty acid levels and the inci-dence of hospital admission for atrial fibrillation [47]. In addition,in patients undergoing coronary artery bypass graft surgery, a 54%reduction in postoperative incidence of atrial fibrillation was seenin 160 patients given either placebo or 2 g/d of omega-3 startedpreoperatively and continued throughout the hospitalization [41].The impact of omega-3 supplementation on atrial fibrillation will bestudied further in two double-blind, randomized, controlled trials ofomega-3 fatty acids in the prevention of atrial fibrillation: theFORωARD trial and a study proposed by Pratt et al. [48, 49]. Ingeneral, these studies have been (or will be) performed largely withEPA + DHA.
372 Prevention
Safety
Adverse events and bleeding& In 2004, The USDepartment of Health andHuman Services Agency for
Healthcare Research and Quality reviewed 148 omega-3 fatty acidstudies reporting on adverse events in more than 20,000 subjects [50].In summary, gastrointestinal complaints were reported in 6.6% of thesubjects taking omega-3s, versus 4.3% in the placebo groups. Impor-tantly, an increased incidence of bleeding was not observed, and onlyone of the 148 studies reviewed reported such an association, and thisoccurred in patients randomly assigned to receive 6 g/d of omega-3.There are no reported deaths or life-threatening illnesses as a conse-quence of omega-3 consumption, and 77 of the studies reported noadverse events at all. The agency concluded that adverse events related toconsumption of fish oil or ALA supplements appear to be minor.
& In 2004, the US Food and Drug Administration (FDA) concludedthat up to 3 g/d of EPA + DHA is safe, although most data are limitedto less than 6 months [51]. These conclusions are supported furtherby a recent case-control study of 182 adults taking aspirin, clopi-dogrel, and high-dose omega-3 fatty acid supplementation (mean3 g/d) and 182 age- and gender-matched controls treated with as-pirin and clopidogrel alone [52]. After a mean treatment duration of33 months, no difference was found between cases and controls withregard to major bleeding (in only one subject taking omega-3) andminor bleeding (in four subjects taking omega-3 vs seven controls).Importantly, caution should be exercised when applying safety datagenerated in a clinical research setting to individual patients in thegeneral population.
Mercury and other contaminants& Concerns have been raised regarding contaminants found in fish,
namely methyl mercury dioxins and PCBs. Fortunately, dioxins andPCBs have been declining steadily since the 1970s, when govern-mental regulation of the production and emission of these pollutantsbegan. Unfortunately, these pollutants may persist in the environ-ment for years, and a 2004 report found higher levels of these con-taminants in farmed as opposed to wild salmon [53]. The fact thatfarmed salmon had higher levels of these pollutants than wildsalmon was widely publicized, but the main finding—that averagelevels of these pollutants were extremely low (farmed salmon atabout 2% of the FDA action level)—went unreported. Even the mostconservative estimates of the increased cancer risk imposed by dioxinand PBCs (24 cases per 100,000 over 70 years of exposure) are farless than the predicted 7000 CVD deaths that would be preventedfrom regular fish consumption during that period [19•]. Lastly, morethan 90% of dioxin and PCB exposure from food is from nonfishitems (meats, dairy, vegetables).
Omega-3 Fatty Acids for Cardiovascular Disease Prevention DeFilippis et al. 373

& Although there have been no cases of mercury poisoning related tofish consumption reported in the United States during the past35 years, subclinical neural damage in infants and an increase incardiovascular risk in adults from chronic exposure to low levels ofmercury found in fish may exist [19•]. One observational studyreported subtle neuropsychological changes in children who hadbeen exposed to high levels of mercury through frequent maternalconsumption of whale (1.6 µg of methyl mercury/g) during preg-nancy, but a similar study found no adverse effects in children whosemothers consumed an average of 12 servings of fish per week thatcontained average levels of methyl mercury (0.3 µg/g) [46].
& A comprehensive review of the data pertaining to methyl mercuryexposure and CVD was published in 2009 [19•]. Of the six studiesexamining the relationship between methyl mercury and CVD, onlytwo small studies (282 and 684 subjects) found an association be-tween methyl mercury levels and an increase in CVD. This risk wasobserved only in subjects who had methyl mercury levels 10 timesthose of the average American. The largest study, in more than87,000 adults, found no relationship between methyl mercury levelsand CVD. Even if methyl mercury does increase CVD, omega-3s re-duce this risk, and the average fish meal in the United States wouldlikely reduce CVD more than the most conservative estimate of harmfrom methyl mercury exposure.
& Although the risk posed by mercury exposure through fish con-sumption is speculative, the FDA recommends limiting consumptionof fish high in mercury (91 ppm or approximately 1 μg/g) to oneserving (7 oz) per week [51]. Because the fetal brain is more sus-ceptible than the adult brain to mercury-induced damage, the FDAand the Environmental Protection Agency recommend that pregnantwomen, nursing mothers, and young children avoid eating fish withhigh mercury content. The FDA maintains a Web page (http://www.cfsan.fda.gov) that currently lists shark, swordfish, king mackerel,and tilefish as having high mercury content.
& With the exception of Lovaza (GlaxoSmithKline, Research TrianglePark, NC), available by prescription, the FDA does not regulate fishoil supplements. A study examining five popular fish oil supple-ments found that three had undetectable levels of mercury (G6 μg/L)and two had levels between 10 and 12 μg/L of mercury by cold vaporatomic absorption spectroscopy [54]. This level of mercury is con-sidered negligible. An evaluation of 30 fish oil supplements mar-keted in Canada found detectable levels of PBCs in all thesupplements, but only one (shark oil) had a level greater than theFDA action level of 2 ppm [20].
Clinical utility: hypertriglyceridemia& In addition to being useful in preventing CVD events, the prescrip-
tion formulation of omega-3 fatty acids, Lovaza, has gained FDA
374 Prevention

approval, as an adjunct to diet, for reducing very high triglyceridelevels (9500 mg/dL) in adults. The dosage for this indication is 4 g/d,which is quite different from the dosages used in the previouslymentioned randomized trials for primary and secondary preventionof CVD events. In addition, prescription omega-3 fatty acid supple-mentation is considered a safe and effective adjunct to statin therapyfor further lowering triglycerides and non–high-density lipoproteincholesterol (HDL-C) [55]. Two recent studies evaluated the impact ofomega-3 supplementation in patients with residual hypertriglyceri-demia (200–400 mg/dL) on statin therapy. In both these studies,4 g/d of prescription omega-3 reduced elevated triglycerides andnon–HDL-C significantly more than either simvastatin or atorvasta-tin alone [56, 57]. Although prescription omega-3 is a useful adjunctin patients on statin therapy who have increased “residual risk” dueto elevated triglycerides and non–HDL-C, no clinical trial data areavailable on the impact of reducing triglycerides with omega-3s withrespect to CVD events.
Current and recommended omega-3 daily intake& Multiple federal, professional, and scientific agencies have made
recommendations for fish or omega-3 fatty acid (EPA + DHA) intakefor the primary prevention of coronary disease. Most of these agen-cies recommend two 4-oz servings of fish per week or approximately500 mg/d of EPA + DHA, without specific guidance for each fattyacid [17]. The Institute of Medicine of the National Academies set itsadequate ALA intake for adults older than 19 years at 1.6 g/d for menand 1.1 g/d for women [17]. These recommendations were echoed ina review published this year in the Journal of the American College ofCardiology that recommends “at least” 500 mg/d of EPA + DHA foradults without underlying overt CVD; however, the article went fur-ther by recommending 800 to 1000 mg/d for individuals withknown CHD or heart failure [18].
& Although dietary intake of omega-3 and omega-6 fatty acids varieswithin and between different populations, data suggest that mostAmericans receive less than the recommended intake for fish andtotal omega-3 fatty acids. Based on the National Health and Nutri-tion Examination Survey (NHANES III), the largest survey of nutrientconsumption in a representative American population, the medianintake of EPA + DHA is zero, the median intake of ALA is less than1 g/d, and the mean fish intake is 2.9 oz/wk [17, 50].
& Omega-3s are a unique group of polyunsaturated fats found mostabundantly in fatty fish, flaxseed, walnuts, soy, and canola oil(Table 2). The metabolism of omega-3s from fish (EPA + DHA) andvegetables (ALA) results in the production of potentially cardiopro-tective eicosanoids (3-series thromboxane, leukotrienes, prostaglan-dins) that reduce inflammation and thrombosis. Most prospectiverandomized trials demonstrate that omega-3s, particularly EPA and
Omega-3 Fatty Acids for Cardiovascular Disease Prevention DeFilippis et al. 375

DHA, have a favorable impact on cardiovascular health, and thishas been demonstrated most consistently with the use of fish oilsupplements. A prospective randomized control trial with ALA isongoing.
& To date, no serious adverse effects of omega-3s have been identified,despite trial data on more than 20,000 subjects. Any potential harmfrom mercury exposure is outweighed by the proven cardiovascularbenefits of eating fish in the adult population. The potential riskfrom methyl mercury can be mitigated further with prudent fish andfish oil supplement selection. To date, increased bleeding compli-cations have not materialized despite the increased use of aspirin andclopidogrel.
& It is recommended that patients with known CHD consume oneserving (200–400 g) of fatty fish (Table 1) or a fish oil supplementcontaining 900 mg of EPA + DHA every day and maintain a healthydiet rich in ALA (Tables 1 and 2). In addition, based on the GISSIHeart Failure trial, we recommend one serving (200–400 g) of fattyfish or a fish oil supplement containing 900 mg of EPA + DHA everyday for patients with congestive heart failure. Patents with a CHDrisk equivalent (eg, diabetes, peripheral vascular disease) also shouldconsider consuming a single serving of fatty fish several times a weekor a daily fish oil supplement containing 900 mg of EPA + DHA(Table 2). The latter recommendation is less evidence based andawaits further evaluation in ongoing trials. For patients without
Table 2. Summary of authors’ omega-3 fatty acid intake recommendation class and interpretation of levelsof evidence
Population Recommendation Class of recommendationand level of evidencea
Patients without documentedCHD
Eat a variety of (preferably fatty) fish at leasttwice per week
I-B
Include foods and oils rich in ALA in your dietPatients with documented CHDor CHF
Consume approximately 1 g of EPA + DHA per day,preferably from fatty fish. EPA + DHA supplementsmay be considered in consultation with the physician.
CHD: I-ACHF: I-B
Patients with CHD riskequivalents
IIa-C
Patients withhypertriglyceridemia
4 g/d of prescription omega-3 (Lovazab) for reductionof triglycerides
I-A for reduction of triglycerides(not for CVD event reduction)
aAuthors’ interpretation of levels of evidence is based on American College of Cardiology/American Heart Association level-of-evidenceguidelines [58]: class I—evidence and/or general agreement that a given procedure or treatment is useful and effective; class II—conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of a procedure or treatment; class IIa—weight of ev-idence/opinion is in favor of usefulness/efficacy; class IIb—usefulness/efficacy is less well established by evidence/opinion; class III—evidence and/or general agreement that the procedure/treatment is not useful/effective and in some cases may be harmful; evidence A—data derived from multiple randomized clinical trials or meta-analyses; evidence B—data derived from a single randomized trial or fromnonrandomized studies; evidence C—consensus opinion of experts, case studies, or standard of carebRegistered trademark of GlaxoSmithKline, Research Triangle Park, NCALA α-linolenic acid; CHD coronary heart disease; CHF congestive heart failure; CVD cardiovascular disease; DHA docosahexaenoic acid; EPAeicosapentaenoic acid
376 Prevention
known CHD, a single serving of fatty fish approximately once ortwice per week and a diet rich in ALA should be encouraged(Table 2). It is prudent to avoid fish containing high levels of methylmercury, as defined by the FDA. For patients with hypertriglyceri-demia, 4 g/d of prescription omega-3 is a recommended therapy toreduce triglycerides and non–HDL-C in both statin-treated and sta-tin-naïve patients. At this time, there is insufficient evidence to rec-ommend omega-3 therapy to reduce cardiac arrhythmias.
Acknowledgment
Dr. DeFilippis is supported by a National Research Service Award (NRSA) Training Grant (T32-HL-07227).
Disclosure
No potential conflicts of interest relevant to this article were reported.
References and Recommended ReadingPapers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. Dyerberg J, Bang HO, Stoffersen E, et al.: Eicosa-pentaenoic acid and prevention of thrombosis andatherosclerosis? Lancet 1978, 2(8081):117–119.
2. Albert CM, CamposH, StampferMJ, et al.:Blood levelsof long-chain n-3 fatty acids and the risk of suddendeath. N Engl J Med 2002, 346(15):1113–1118.
3. Albert CM, Hennekens CH, O’Donnell CJ, et al.: Fishconsumption and risk of sudden cardiac death.JAMA 1998, 279(1):23–28.
4. Dietary supplementation with n-3 polyunsaturatedfatty acids and vitamin E after myocardial infarction:results of the GISSI-Prevenzione trial. Gruppo Ital-iano per lo Studio della Sopravvivenza nell’Infartomiocardico. Lancet 1999, 354(9177):447–455[Published erratum appears in Lancet 2001, 357(9256):642].
5. Ascherio A, Rimm EB, Stampfer MJ, et al.: Dietaryintake of marine n-3 fatty acids, fish intake, and therisk of coronary disease among men. N Engl J Med1995, 332(15):977–982.
6. DeFilippis AP, Sperling LS: Understanding omega-3’s. Am Heart J 2006, 151(3):564–570.
7. Kris-Etherton PM, Harris WS, Appel LJ, AmericanHeart Association: Nutrition C: Fish consumption,
fish oil, omega-3 fatty acids, and cardiovasculardisease. Circulation 2002, 106(21):2747–2757[Published erratum appears in Circulation 2003, 107(3):512].
8. Kromhout D, Bosschieter EB, de LezenneCoulander C: The inverse relation between fishconsumption and 20-year mortality fromcoronary heart disease. N Engl J Med 1985, 312(19):1205–1209.
9.• Yokoyama M, Origasa H, Matsuzaki M, et al.; JapanEPA lipid intervention study (JELIS) Investigators:Effects of eicosapentaenoic acid on major coronaryevents in hypercholesterolaemic patients (JELIS): arandomised open-label, blinded endpoint analysis.Lancet 2007, 369(9567):1090–1098.
The JELIS trial randomly assigned 18,645 patients with hy-percholesterolemia to receive a statin plus purified EPA(1800 mg/d) or a statin plus placebo. After an average of4.6 years of follow-up, those assigned to a statin plus puri-fied EPA received a 19% relative risk reduction in the com-bined primary outcome of sudden cardiac death, fatal andnonfatal myocardial infarction, unstable angina, and coro-nary revascularization compared with those treated with astatin plus placebo. JELIS was the first omega-3 trial to in-clude subjects without known CVD, the first to show benefit
Omega-3 Fatty Acids for Cardiovascular Disease Prevention DeFilippis et al. 377

beyond uniform statin treatment, and the first to showbenefit with EPA supplementation alone (as opposed toEPA + DHA)10. Lev ES, Harel A, Mager N, et al.: Treatment of aspirin-
resistant patients with omega-3 fatty acids versusaspirin dose escalation. J Am Coll Cardiol 2010, 55(2):114.
11. Farzaneh-Far R, Harris WS, Garg S, et al.: Inverseassociation of erythrocyte n-3 fatty acid levels withinflammatory biomarkers in patients with stablecoronary artery disease: The Heart and Soul Study.Atherosclerosis 2009, 205(2):538–543.
12. Farzaneh-Far R, Lin J, Epel ES, et al.: Association ofmarine omega-3 fatty acid levels with telomericaging in patients with coronary heart disease. JAMA303(3):250–257
13. He K, Liu K, Daviglus ML, et al.: Associations of di-etary long-chain n-3 polyunsaturated fatty acidsand fish with biomarkers of inflammation andendothelial activation (from the Multi-Ethnic Studyof Atherosclerosis [MESA]). Am J Cardiol 2009, 103(9):1238–1243.
14. Lopez-Garcia E, Schulze MB, Manson JE, et al.:Consumption of (n-3) fatty acids is related toplasma biomarkers of inflammation and endothe-lial activation in women. J Nutr 2004, 134(7):1806–1811.
15. Micallef MA, Munro IA, Garg ML: An inverse rela-tionship between plasma n-3 fatty acids and C-re-active protein in healthy individuals. Eur J Clin Nutr2009, 63(9):1154–1156.
16. Pischon T, Hankinson SE, Hotamisligil GS, et al.:Habitual dietary intake of n-3 and n-6 fatty acids inrelation to inflammatory markers among US menand women. Circulation 2003, 108(2):155–160.
17. Kris-Etherton PM, Grieger JA, Etherton TD: Dietaryreference intakes for DHA and EPA. ProstaglandinsLeukot Essent Fat Acids 2009, 81(2–3):99–104.
18. Lavie CJ, Milani RV, Mehra MR, Ventura HO: Ome-ga-3 polyunsaturated fatty acids and cardiovasculardiseases. J Am Coll Cardiol 2009, 54(7):585–594.
19.• Mozaffarian D: Fish, mercury, selenium and car-diovascular risk: current evidence and unansweredquestions. Int J Environ Res Public Health 2009, 6(6):1894–1916.
This comprehensive review examines the evidence that con-taminants often found in fish (methyl mercury, PCBs, anddioxins) cause harm. The authors provide statistical analysisto compare the potential risk from these pollutants with theappreciable benefits of eating fish20. Rawn DF, Breakell K, Verigin V, et al.: Persistent or-
ganic pollutants in fish oil supplements on theCanadian market: polychlorinated biphenyls andorganochlorine insecticides. J Food Sci 2009, 74(1):T14–T19.
21. Burdge G: Alpha-linolenic acid metabolism in menand women: nutritional and biological implica-
tions. Curr Opin Clin Nutr Metab Care 2004, 7(2):137–144.
22. DeFilippis AP, Harper CR, Cotsonis GA, Jacobson TA:Effect of baseline plasma fatty acids on eicosapen-taenoic acid levels in individuals supplementedwith alpha-linolenic acid. Int J Food Sci Nutr 2009,60(Suppl 5):28–37.
23. Emken EA, Adlof RO, Gulley RM: Dietary linoleicacid influences desaturation and acylation of deu-terium-labeled linoleic and linolenic acids inyoung adult males. Biochim Biophys Acta 1994, 1213(3):277–288.
24. Gerster H: Can adults adequately convert alpha-linolenic acid (18:3n-3) to eicosapentaenoic acid(20:5n-3) and docosahexaenoic acid (22:6n-3)? IntJ Vitam Nutr Res 1998, 68(3):159–173.
25. Goyens PL, Spilker ME, Zock PL, et al.: Conversionof alpha-linolenic acid in humans is influenced bythe absolute amounts of alpha-linolenic acid andlinoleic acid in the diet and not by their ratio. Am JClin Nutr 2006, 84(1):44–53.
26. Harper CR, Edwards MJ, DeFilipis AP, Jacobson TA:Flaxseed oil increases the plasma concentrations ofcardioprotective (n-3) fatty acids in humans. J Nutr2006, 136(1):83–87.
27. Layne KS, Goh YK, Jumpsen JA, et al.: Normal sub-jects consuming physiological levels of 18:3(n-3)and 20:5(n-3) from flaxseed or fish oils havecharacteristic differences in plasma lipid and lipo-protein fatty acid levels. J Nutr 1996, 126(9):2130–2140.
28. Sprecher H: An update on the pathways of polyun-saturated fatty acid metabolism. Curr Opin Clin NutrMetab Care 1999, 2(2):135–138.
29. Mozaffarian D, Ascherio A, Hu FB, et al.: Interplaybetween different polyunsaturated fatty acids andrisk of coronary heart disease in men. Circulation2005, 111(2):157–164.
30. US Department of Health and Human Services Agencyfor Healthcare Research and Quality: Effects of omega-3 fatty acids on cardiovascular risk factors and inter-mediate markers of cardiovascular disease. EvidenceReport/Technology Assessment (Summary): Number93. Available at http://www.ahrq.gov/clinic/epcsums/o3cardrisksum.htm2004. Accessed May 2010.
31. Weber PC: Clinical studies on the effects of n-3 fattyacids on cells and eicosanoids in the cardiovascularsystem. J Intern Med Suppl 1989, 225(731):61–68.
32. Weber PC, Leaf A: Cardiovascular effects of omega 3fatty acids. Atherosclerosis risk factor modificationby omega 3 fatty acids. World Rev Nutr Diet 1991,66:218–232.
33. Simopoulos AP: Essential fatty acids in health andchronic disease. Am J Clin Nutr 1999, 70(3Suppl):560S–569S.
34. Ross R: Atherosclerosis—an inflammatory disease.N Engl J Med 1999, 340(2):115–126.
378 Prevention

35. Ridker PM, Hennekens CH, Buring JE, Rifai N: C-reactive protein and other markers of inflam-mation in the prediction of cardiovasculardisease in women. N Engl J Med 2000, 342(12):836–843.
36. Patrono C: The PGH-synthase system and isozyme-selective inhibition. J Cardiovasc Pharmacol 2006, 47(Suppl 1):S1–S6.
37. Patrono C, Falco A, Davi G: Isoprostane formationand inhibition in atherothrombosis. Curr OpinPharmacol 2005, 5(2):198–203.
38. Needleman P, Raz A, Minkes MS, et al.: Trieneprostaglandins: prostacyclin and thromboxanebiosynthesis and unique biological properties. ProcNatl Acad Sci U S A 1979, 76(2):944–948.
39. Engstrom K, Wallin R, Saldeen T: Effect of low-doseaspirin in combination with stable fish oil onwhole blood production of eicosanoids. Prosta-glandins Leukot Essent Fat Acids 2001, 64(6):291–297.
40. Kramer HJ, Stevens J, Grimminger F, Seeger W: Fishoil fatty acids and human platelets: dose-dependent decrease in dienoic and increase in tri-enoic thromboxane generation. Biochem Pharmacol1996, 52(8):1211–1217.
41. Calo L, Bianconi L, Colivicchi F, et al.: N-3 Fatty acidsfor the prevention of atrial fibrillation after coronaryartery bypass surgery: a randomized, controlled trial.J Am Coll Cardiol 2005, 45(10):1723–1728.
42. Reiffel JA, McDonald A: Antiarrhythmic effects ofomega-3 fatty acids.AmJCardiol2006,98(4A):50i–60i.
43. Senges S: Randomized trial of omega-3 fatty acidson top of modern therapy after acute myocardialinfarction: the OMEGA trial. Presented at theAmerican College of Cardiology 58th Annual Scien-tific Session. Orlando, FL: March 29–31, 2009.
44.• Tavazzi L, Maggioni AP, Marchioli R, et al.: Effect ofn-3 polyunsaturated fatty acids in patients withchronic heart failure (the GISSI-HF trial): a rando-mised, double-blind, placebo-controlled trial. Lan-cet 2008, 372(9645):1223–1230.
The GISSI Heart Failure trial randomly assigned 6975patients with chronic, stable heart failure on optimal medi-cal therapy to receive omega-3 fatty acid. After a medianfollow-up of 3.9 years, those assigned to omega-3 fatty acidsupplementation experienced a 9% relative risk reduction(ARR, 1.8%; PG0.05) in total mortality and an 8% relativerisk reduction (ARR, 2.3%; PG0.01) in mortality or cardio-vascular hospital admissions. This was the first omega-3 trialperformed specifically in the heart failure population andled some experts to recommend omega-3 supplementationfor heart failure patients45. Brouwer IA, Raitt MH, Dullemeijer C, et al.: Effect
of fish oil on ventricular tachyarrhythmia inthree studies in patients with implantable cardi-overter defibrillators. Eur Heart J 2009, 30(7):820–826.
46. Mozaffarian D, Rimm EB: Fish intake, contami-nants, and human health: evaluating the risks andthe benefits. JAMA 2006, 296(15):1885–1899.
47. Virtanen JK, Mursu J, Voutilainen S, Tuomainen TP:Serum long-chain n-3 polyunsaturated fatty acidsand risk of hospital diagnosis of atrial fibrillationin men. Circulation 2009, 120(23):2315–2321.
48. Macchia A, Varini S, Grancelli H, et al.: The rationaleanddesignof the FORomegaARDTrial: a randomized,double-blind, placebo-controlled, independent studyto test the efficacy of n-3 PUFA for the maintenance ofnormal sinus rhythm in patients with previous atrialfibrillation. Am Heart J 2009, 157(3):423–427.
49. Pratt CM, Reiffel JA, Ellenbogen KA, et al.: Efficacyand safety of prescription omega-3-acid ethyl estersfor the prevention of recurrent symptomatic atrialfibrillation: a prospective study. Am Heart J 2009,158(2):163–169.e161–163.
50. US Department of Health and Human Services Agencyfor Healthcare Research and Quality: Effects of omega-3 fatty acids on cardiovascular disease. Evidence Re-port/Technology Assessment: Number 94. Available athttp://www.ahrq.gov/downloads/pub/evidence/pdf/o3cardio/o3cardio.pdf. Accessed May 2010.
51. US Food and Drug Administration: Center for FoodSafety and Applied Nutrition. Washington, DC: De-partment of Health and Human Services; 2004.
52. Watson PD, Joy PS, Nkonde C, et al.: Comparison ofbleeding complications with omega-3 fatty acids +aspirin + clopidogrel—versus—aspirin + clopidog-rel in patients with cardiovascular disease. Am JCardiol 2009, 104(8):1052–1054.
53. Hites RA, Foran JA, Carpenter DO, et al.: Global as-sessment of organic contaminants in farmedsalmon. Science 2004, 303(5655):226–229.
54. Foran SE, Flood JG, Lewandrowski KB: Measurementof mercury levels in concentrated over-the-counterfish oil preparations: is fish oil healthier than fish?Arch Pathol Lab Med 2003, 127(12):1603–1605.
55. National Cholesterol Education Program (NCEP)Expert Panel on Detection, Evaluation, and Treat-ment of High Blood Cholesterol in Adults (AdultTreatment Panel III): Third Report of the NationalCholesterol Education Program (NCEP) ExpertPanel on Detection, Evaluation, and Treatment ofHigh Blood Cholesterol in Adults (Adult TreatmentPanel III) final report. Circulation 2002, 106(25):3143–3421.
56. Bays HE, McKenney J, Maki KC, et al.: Effects ofprescription omega-3-acid ethyl esters on non–high-density lipoprotein cholesterol when coad-ministered with escalating doses of atorvastatin.Mayo Clin Proc 2010, 85(2):122–128.
57. Davidson MH, Stein EA, Bays HE, et al.: Efficacy andtolerability of adding prescription omega-3 fattyacids 4 g/d to simvastatin 40 mg/d in hypertrigly-ceridemic patients: an 8-week, randomized,
Omega-3 Fatty Acids for Cardiovascular Disease Prevention DeFilippis et al. 379
double-blind, placebo-controlled study. Clin Ther2007, 29(7):1354–1367.
58. American Heart Association: Methodology Manualfor ACC/AHA Guideline Writing Committees:Methodologies and Policies from the ACC/AHA
Task Force on Practice Guidelines. Available athttp://www.acc.org/qualityandscience/clinical/manual/pdfs/methodology.pdf and http://circ.ahajournals.org/manual/. Accessed February 16,2010.
380 Prevention


















