Holistic Quota Management Michael Gilfix [email protected] November 6 th, 2002 LISA 2002.

OLD TESTS, NEW TESTS, AND WHAT DO WE MAKE OF
THEM? BrianM.Gilfix
MDCM,PhD,FRCPC,DABCC,FAACC
March26,2019
UPDATE — 1 June 2018, the IYPT2019 website is live … VISIT www.iypt2019.org
On 20 December 2017, during its 74th Plenary Meeting, the United Nations (UN) GeneralAssembly 72nd Session has proclaimed 2019 as the International Year of the Periodic Tableof Chemical Elements (IYPT 2019). In proclaiming an International Year focusing on thePeriodic Table of Chemical Elements and its applications, the United Nations hasrecognized the importance of raising global awareness of how chemistry promotessustainable development and provides solutions to global challenges in energy, education,agriculture and health. Indeed, the resolution was adopted as part of a more generalAgenda item on Science and technology for development. This International Year will bringtogether many different stakeholders including UNESCO, scientific societies and unions,educational and research institutions, technology platforms, non-profit organizations andprivate sector partners to promote and celebrate the significance of the Periodic Table ofElements and its applications to society during 2019.
The development of the Periodic Table of theElements is one of the most significantachievements in science and a uniting scientificconcept, with broad implications in Astronomy,Chemistry, Physics, Biology and other naturalsciences. The International Year of the PeriodicTable of Chemical Elements in 2019 will coincidewith the 150th anniversary of the discovery ofthe Periodic System by Dmitry Mendeleev in1869. It is a unique tool enabling scientists topredict the appearance and properties of matter on Earth and in the Universe. Manychemical elements are crucial to enhance the value and performance of productsnecessary for humankind, our planet, and industrial endeavors. The four most recentelements (113, 115, 117 and 118) were fully added into the Periodic Table, with theapproval of their names and symbols, on 28 November 2016.
The International Year of the Periodic Table of the Chemical Elements will coincide with theCentenary of IUPAC (IUPAC100). The events of IUPAC100 and of IYPT will enhance theunderstanding and appreciation of the Periodic Table and chemistry in general among thepublic. The 100th Anniversary of IUPAC will be on the UNESCO Calendar of Anniversarieson 28th July 2019.
“As the global organization that provides objective scientific expertise and develops the essential

Conflicts of Interest
• Ihavereceivedhonorariafrom:– AlnylamPharmaceuticals– Grifols,S.A.– RecordatiRareDiseasesCanada
2

Objectives
1. Tounderstandtheroleoftheclinicallaboratoryinmodernmedicine
2. Tounderstandwhysofewteststhatappearintheliteraturemakeitintoclinicalusage.
3. TounderstandtheprocessbywhichtestsnotavailableinQuebeccanbeordered.
3

Questions
1. Whatpercentageofteststhatappearintheliteraturemakeitintoclinicalusage?
2. Whatisthedifferencebetweencurrenttroponintestingandhigh-sensitivitytroponin?
3. NameonelimitationinapoBtesting?
4

Importance of This Year 2019 InternationalYearofthePeriodicTableof
ChemicalElements(150years)DimitryMendeleev
ThePeriodicTablebyPrimoLevi
(100thanniversaryofhisbirth)
Yiddish too. The links between obdurate matter and precarious survival become more intimate with time, as he graduates, begins a career, finds ways just to stay alive. The realization that zinc samples must be impure to yield to acid triggers an insight into the importance of difference and the new place of the Jewish people in fascist Italy under Benito Mussolini, who ruled from 1922 to 1943. “Dissension, diversity, the grain of salt and mustard are needed.” Fascism, however, “wants everybody to be the same and you are not”.
Resistance to fascism in Italy was something of a buffer against the country’s fascist racial laws. Levi achieved a first-class honours degree in chemistry. An unnamed military officer then gave him an enigmatic and ultimately futile job in faraway, unidenti-fied hills, to see if he could extract value from the tailings of an asbestos mine. In ‘Nickel’, this rooting in rubble prompts another hymn to matter. “The entrails of the earth swarm with gnomes,” he writes. The word nickel is even derived from the German for ‘little demon’ — creatures that might “let you find a treasure beneath the tip of your pickax, or deceive and bedazzle you, making modest pyrites glitter like gold”.
After the collapse of Italian fascism in 1943, Nazi divisions occupied Milan and Turin. Levi joined the partisans, and was betrayed. Imprisoned in Italy’s Repub-lic of Salò, a German puppet state, he was subsequently shipped to Auschwitz. Here, his chemistry degree and ability to speak German saved him — for slave work at the Buna rubber factory. To avoid starvation,
he secretly made fatty acids by oxidizing paraffin, tried to make fritters of cotton and forced himself to ingest glycerine. He identi-fied and stole iron–cerium rods found in the laboratory. Whittled down to make cigarette lighter flints, these were bartered: “This is how we won the bread which kept us alive until the arrival of the Russians.”
In his 1947 memoir If This Is A Man, Levi had written unforgettably of the crazy market forces in the camps, one of the great testaments of cruelty, shame and despair in mid-century Europe. The stories of The Periodic Table are poignant, acute and more shaped. In one casual sentence in ‘Vanadium’, he recounts how, decades after the war, when he was working with an industrial-varnish business, he found himself deal ing with a German from the Auschwitz factory. As he wrote, “real-ity is always more c o m p l e x t h a n invention: less kempt, cruder, less rounded out”. But crude, unkempt experience is trans-muted in this book. Literary alchemy is at work. In the 2002 biography Primo Levi, Ian Thompson notes that, in some ways, the clos-est Levi came to being a novelist was in the “daring and original” The Periodic Table, and nowhere more so than in ‘Vanadium’.
‘Silver’ exemplifies that originality, too. It includes a little detective story, told by a fellow chemist, of how intermittent batches of silver nitrate papers supplied for X-ray imagery were spoilt. Mystery solved, Levi
declares his ambition to seek more stories of luck, intuition and stratagems on which the working chemist relies, stories “in which stolid matter manifests a cunning intent upon evil and obstruction, as if revolted against the order dear to man”. In the post-war wreck-age of Italy, he finds plenty of obstruction. A down-at-heel factory manager in ‘Nitrogen’ commissions him to identify the unguent that renders lipstick ‘kiss proof ’. He decides the starting point must be uric acid. The search ends with Levi and his bride trying to amass urea from chicken dung and python excrement.
Such visceral realities are the lesson of the chemist’s trade, he writes. “Matter is matter, neither noble nor vile, infinitely transform-able, and its proximate origin is of no impor-tance whatsoever.” The book ends with the imagined odyssey of an atom of carbon, from calcium carbonate to carbon dioxide to leaf tissue, to glucose and ultimately to the pulse of energy in the hand that holds the pen.
Levi died in 1987, after falling from the third-storey landing of his Turin home. His book lives on, a chemist’s book, a hymn to the elements and a testament to what he calls “the strong and bitter flavour of our trade”.
I have four anthologies of science writ-ing on my shelves. Levi is in all four, and his matchless short story ‘Carbon’ in three. I think people will still be reading The Periodic Table in 2085. ■
Tim Radford is the author of The Consolations of Physics. He was science editor of The Guardian for 13 years. e-mail: [email protected]
“To avoid starvation, he secretly made fatty acids by oxidizing paraffin.”
Primo Levi, literary alchemist and Auschwitz survivor.
MAR
CEL
LO M
ENC
ARIN
I/B
RID
GEM
AN
3 1 J A N U A R Y 2 0 1 9 | V O L 5 6 5 | N A T U R E | 5 6 5ǟɥƐƎƏƙ
ɥ�/1(-%#1
ɥ��341#
ɥ�(,(3#"ƥ
ɥ�++
ɥ1(%'32
ɥ1#2#15#"ƥ ǟ
ɥƐƎƏƙ
ɥ�/1(-%#1
ɥ��341#
ɥ�(,(3#"ƥ
ɥ�++
ɥ1(%'32
ɥ1#2#15#"ƥ
5

McGill University Clinical Laboratories
• Locatedonthe4thand5thfloorsofPavilionEattheGlensite
• PartofOPTILABcluster(‘grappe”)• MUHC
– 5.3millionbillabletestsannually– 5,000-6000specimensperday
6

GRAPPE7:Montréal-CUSMLaboratoireserveur• CUSM(HGJimpliquéenpathologieetmicrobiologie)CentreuniversitairedesantéMcGill(CUSM)
• SiteGlen• HôpitalgénéraldeMontréal• HôpitaldeLachine
CIUSSSduCentre-Ouest-de-l'Île-de-Montréal• Hôpitalgénéraljuif
CIUSSSdel'Ouest-de-l'Île-de-Montréal• CentrehospitalierdeSaintMary's• HôpitalgénéralduLakeshore• HôpitaldeLaSalle
CISSSdel'Abitibi-Témiscamingue• HôpitaletCLSCdeVal-d’Or• CLSCdeSenneterre• HôpitaldeRouyn-Noranda• Hôpitald’Amos• CentredesoinsdecourteduréeLaSarre(CSCD)• PavillonSainte-Famille• PointdeservicedeTémiscaming-et-de-Kipawa
RégierégionaledelasantéetdesservicessociauxduNunavik
• CentredesantéInuulitsivik• CentredesantéTulattavikdel'Ungava
ConseilcridelasantéetdesservicessociauxdelaBaieJames
• HôpitaldeChisasibi• CMCMistissini
http://www.msss.gouv.qc.ca/professionnels/soins-et-services/optilab/montreal-cusm/
Mostcomplex“Grappe”• Onelaboratoryon
multiplesites• $99M• 850Employees• 120MDs
• GrappeLeadershipaccountabletoPDGofMUHC(fiduciary)
• Academicstrengths
7
MNIomitted&correctionrequested
Source:A.Dascal

Use of Diagnostic Tests in the Patient Pathway
8
in which laboratory medicine is used optimally to sup-port patient care, enhance patient safety, and improveoutcomes.
Definition and Purpose of LaboratoryMedicine
Laboratory medicine may be defined (Mosby’s MedicalDictionary) as “the branch of medicine in which samplesof tissue, fluid, or other body substance are examinedoutside of the person,” either in a laboratory or at thepoint of care (near-patient testing). It encompasses thetraditional disciplines of clinical chemistry, toxicology,hematology, immunology, microbiology (including se-rology and virology), anatomical pathology, cytology,molecular pathology, and cytogenetics. The global invitro diagnostics market was valued at $49.2 billion in2012, projected to grow at a rate of 7% from 2012–2017(2 ). This probably corresponds to 10–15 billion tests peryear worldwide (authors’ estimate).
Laboratory medicine supports the interaction be-tween patients and physicians by providing relevant data,increasing the likelihood of making the most appropriatedecisions for the optimum care of the individual.Gambino (3 ) and Lundberg (4 ) defined the interactionin terms of the total testing process (TTP)11 or “brain-to-brain loop.”
The Value of Laboratory Medicine
Isolating the value of the testing process from the overallprocess of patient management is complicated. Value canbe defined clinically or economically. Clinical value islinked to the improvement of health-related outcomes,whereas economic value is tied to cost-efficiency or-effectiveness (5 ). The former is not specific to individualcountries or healthcare systems, except insofar as it de-pends on the spectrum of patients presenting to thosesystems. The latter will depend on the specific setting in
which the testing process is to be deployed and the rangeand cost of diagnostic tools available. Economic analysesof value are thus difficult to transfer between settings. Wewill focus on clinical value in its broadest sense, becausethere is no such thing as cost-effectiveness for a clinicallyineffective process.
We propose an approach to measuring value inwhich the net value of a testing process is defined asdelivered benefits minus delivered harm (undesirable ef-fects of testing). In this model, net value is maximized byincreasing the benefits or reducing harm.
The benefits derive from the provision of objectivedata about patient health that enable screening of popu-lations for detection of asymptomatic disease, stratifica-tion of risk, specific diagnosis of a patient’s condition,selection and monitoring of appropriate therapy, predic-tion and early detection of adverse treatment outcomes,and assessment of prognosis (Fig. 1).
Existing Evidence of Value
It is outside the scope of this paper to offer a comprehen-sive review of all studies which address the value of labo-ratory medicine. Instead, we present examples that dem-onstrate benefit (Table 1). Further evidence can be foundin a US national status report (13 ).
POINT-OF-CARE TESTING
Point-of-care testing (POCT) is a specialized situation withunique attributes. “The close proximity of the patient, aclinical provider with a question, and the technology to rap-idly answer that question” leads to quicker decisions andactions compared to centralized testing (14). This has beendemonstrated with varied conditions, symptoms, and set-tings (15–18). These unique benefits are accompanied byunique concerns which are discussed later.
COST-EFFECTIVENESS
Although cost-effectiveness is not a primary focus of thisreview, a brief discussion of this topic is relevant. Thecost-effectiveness of laboratory testing has been studiedin various settings [reviewed by Hernandez et al. (19 ) andFang et al. (20 )].
11 Nonstandard abbreviations: TTP, total testing process; POCT, point-of-care testing; ICER,incremental cost-effectiveness ratio; QALY, quality-adjusted life year; Hb A1c, hemoglo-bin A1c; ICHCLR, International Consortium for Harmonization of Clinical Laboratory Re-sults; RCT, randomized controlled trial; PSA, prostate-specific antigen.
Screening RiskStratification Diagnosis Treatment
Selection Monitoring
Fig. 1. Uses of diagnostic tests in the patient pathway.
Review
590 Clinical Chemistry 61:4 (2015)
Hallworthetal.ClinChem2015;61:589-599.

9
OneTest=OneResult=OneAction

What we wish to avoid?

11
In a hospital chart, what percentage of the objective information is
generated by the hospital laboratory?
1. 80%2. 70%3. 50%4. 30%5. 10%

12
In a hospital chart, what percentage of the objective information is
generated by the hospital laboratory?
1. 80%
2. 70%3. 50%4. 30%5. 10%
Hallworth MJ. The 70% claim: what is the evidence base? Ann Clin Biochem 2011;48:487– 8.

13
Is it possible to know or be familiar with every test?
q Yesq No

14
No!
• TheMayoInterpretiveTestCatalogueisover700pageslong.
• In50years,thenumberoftestshasgrownfrom~250to>4000
• Newtestsareappearingfasterthanoldtestsaredisappearing,especiallyforMolDx(oneofthefastestgrowingsegments).

Problematic Tests
ObsoleteTests• CK-MB• Schillingtest• FTI• Prostaticacidphosphatase• Bence-Jonesprotein• LEcelltest• Fecalleukocytes• RBCfolate• Porphyrinscreeningtests
(Very)LimitedUtility• ESR• Serumfolate• Myoglobin• APCRratio• AST• MTHFR677C>T
15

Progress in Medicine = Progression of Analytical Tools An Example from Oncology
NATURE BIOTECHNOLOGY VOLUME 36 NUMBER 1 JANUARY 2018 47
R E V I E W
point for precision oncology11,12. For example, in a clinical trial that featured sequencing of ten cancer genes in lung adenocarcinoma tis-sues from 733 patients, one or more oncogenic mutations were identi-fied in 466 patients (64%), and 24 patients (3%) had mutations in two or more genes13. 260 patients received targeted therapy and achieved median survival of 3.5 years, compared with 2.4 years for 318 patients that did not receive matched therapy14.
Seizing the opportunity to make an immediate impact on patient care, the US National Cancer Institute (NCI) initiated several clini-cal trials to test the application of biomarker-driven therapeutic approaches16. These trials include the Lung Master Protocol (Lung-MAP, S1400), which aims to target therapies for lung squamous cell carcinoma (SCC). SCC has no approved targeted therapies, and the frequency of actionable somatic aberrations in these cancers is so low (5–20%) that traditional clinical trials are impractical17. In the Lung-MAP, next-generation sequencing (NGS) is used to identify actionable molecular abnormalities, and patients are randomized to targeted therapy or standard of care. Another example is the Adjuvant Lung Cancer Enrichment Marker Identification and Sequencing Trial
(ALCHEMIST), in which early-stage lung cancer patients are screened for epidermal growth factor receptor gene (EGFR) or anaplastic lymphoma kinase gene (ALK) mutations by sequencing18,19. In the Molecular Analysis for Therapy Choice (NCI-MATCH) clinical trial, biopsies of adult solid tumors and lymphomas are sequenced to screen for mutations in a panel of defined actionable genes, and patients are matched with either approved or investigational (phase 2) drugs20–23. The NCI-MATCH trial received such an enthusiastic response upon launch that enrollment had to be paused from January to April/May 2016 to allow expansion of laboratory capacity, as well as addition of more than a dozen new treatment arms15. Similar trials were initiated
Year Landmarks in the application of analytical tools to inform cancer diagnosis, prognosis, and therapy1847 Microscopy
Formal description of leukemia by Rudolf Virchow190,191
1941 CytopathologyHematoxylin and Eosin (H&E) staining of Papanicolaou-smear, cervical cancer192,193
1956 Improved karyotyping: accurate determination of human chromosome numbers194,195
1960s
Cytogenetics Philadelphia chromosome, chronic myeloid leukemia (CML)196
Electron microscopyEpstein–Barr Virus (EBV) associated with Burkitt’s lymphoma197
1970s
Chromosome bandingRecurrent translocations in hematological malignancies198–204
RadioimmunoassayCarcinoembryogenic antigen (CEA), colorectal cancer205,206
DNA sequencing207–209, molecular cloning210
1980s
Chromosome bandingRecurrent translocations in sarcomas/soft tissue tumors211–214
Radioactive probe hybridizationsDetection of BCR-ABL1, CML215; IgH-BCL2, B-cell lymphoma216; TcR-MYC,T-cell leukemia217; human papilloma virus (HPV) in cervical cancer218
Fluorescence in situ hybridization (FISH)219, 220
ERBB2 in breast cancer221
Flow cytometryAcute promyelocytic leukemia (APML)222, neuroblastoma223,myelodysplastic syndrome (MDS)224 , multiple myeloma225
Oncogenes and tumor suppressors: identification and characterization, e.g., RAS, MYC, RB1226-228
RadioimmunoassayEstrogen receptor229, prostate specific antigen230
ImmunohistochemistryEstrogen receptor229, 231, ERBB2232, 233
Invention of PCR234
Reverse transcriptase PCR (RT-PCR)BCR-ABL1 in CML235 , PML-RARA in APML236 , AML1/ETO in AML (acute myeloid leukemia)237
1990s
Human Genome Project238, 239
Positron emission tomography (PET), computed tomography (CT)240–242
Microarray profiling for high-throughput genomic and transcriptomic profiling of cancers243
Expression profiles of cancers244,245, diffuse large B-cell lymphoma (DLBCL) subtypes246,breast cancer prognosis247, hereditary breast cancer248, biomarkers of prostate cancer249,lung cancer250, gene fusions in prostate cancer251
2000s
PCR amplification and sequencing of “cancer genes”252 from tumor specimensGenomic landscapes of somatic aberrations in different cancers-breast, colorectal, pancreatic253–256
Massively parallel high-throughput/next-generation sequencing257–259
TCGA- The Cancer Genome Atlas260–264, https://cancergenome.nih.gov/Various modalities of precision oncology projects in research, clinical, and clinical trial settingsdiscussed in this review
Precision Medicine Initiative265,266
Cancer Breakthroughs 2020 (formerly, Cancer Moonshot), http://www.cancerbreakthroughs2020.org/
Figure 1 The progression of analytical tools in oncology. The historical timeline highlights key developments in the assessment of cancer cells and tumor tissue, starting from the microscopic description of leukemia cells by Rudolf Virchow, up to the futuristic Cancer Breakthroughs 2020 project. It may be noted that the modern tool kit for cancer analyses includes a range of old and new tools, and the high-throughput sequencing approaches add a highly informative component, complementary to other methods that include imaging, histopathology, and biochemical analyses. References are listed in the Supplementary Note.
Sequence dataTumor/ germline exome
Tumor transcriptome
Quality controlSequence alignment
Mapping
Library quality metrics- % on target; % PCR duplicates
Sequencing quality metrics-number of reads; percent alignment
mean coverage (exome) coverage of splice junctions (RNA)
Mutation signatures* Microsatellite instability (MSI)* Mutagen associated- tobacco, UV, temezolamide* Mutational process related- APOBEC, DNA repair defect
Detection of cancer viruses, e.g.,HPV, HTLV, EBV
Tumor mutanome9-mer neo-epitopes
(SNVs, indels, gene fusions)
Patient HLA typePHLAT/ HLA reporter
Neo-epitope-MHC binding affinities, in silico predictionIEDB consensus algorithm (IC50<500nM)
Mutant/wild-type MHC binding IC50 (fold change)
Neo-epitope expression, RNA-seq data
MHC binding /ELISPOT assayExperimental validation of candidate
immunogenic neo-epitopes
a
b
Exome (whole/ targeted panel)
Tumor content
Copy number aberrations* Focal amplifications/ deletions* Arm/ chromosomal level gains/ losses
Somatic/ germline mutations* Single nucleotide variants (SNVs)- mis-/ non-sense/ splice* Insertions/deletions (indels)- in frame/ frameshift* Zygosity/ clonality based on variant allele frequency and tumor content
Mutation burden* Number of mutations/Mb of human genome* (>10 mutations/Mb considered as hypermutated)
Transcriptome (capture/ poly a)
Gene expression*Cancer specific biomarkers*Expression of mutant/ amplified/ deleted genes*Outlier expression*Splicing aberrations
Cancers of unknown primary*Gene expression profiles (TCGA, MI_Oncoseq compendium, GTEX) --> *Predict tumor tissue of origin
Gene fusions*Recurrent gene fusions (diagnostic/ therapeutic targets)*Novel gene fusions, known oncogenes*Chimeric transcripts, tumor suppressors
Tumor-infiltrating immune cells profiles
Figure 2 Integrative sequencing analysis to define the spectrum of cancer aberrations. (a) Bioinformatic workflow and classes of cancer aberrations identified. The primary sequencing data are subjected to different quality control metrics and aligned to the reference genome to define the indicated genomic and transcriptomic aberrations. (b) Prediction of neo-antigens for immunotherapy. The flow chart indicates primary steps involved in in silico prediction of immunogenic cancer-specific neo-antigens in tumor samples, for potential use in developing personalized peptide vaccines.
NatureBiotechnology2018;36:46

BUT!
17

PeakofInflatedExpectations
(Hype)
TechnologyTrigger
PlateauofProductivity
TroughofDisillusionment
Gartner’s Hype Cycle

Trend in the Number of Biomarkers-related NIH-funded
Grants and Publications
19
often have not targeted critical decision points. Distin-guishing cancer patients, or other very sick people,from controls is apparently easy—it has been the sub-ject of thousands of papers. Far more difficult, how-
ever, is distinguishing rapidly growing from slowlygrowing prostate tumors (for example), which wouldprovide new information that would profoundly affecttreatment.
Fig. 1. Trend in the number of biomarker-related NIH-funded grants and related publications over 21⁄2 decades.
Fig. 2. FDA-cleared protein tests introduced since 1993 [updated from Anderson (1 )].HER-2, human epidermal growth factor receptor 2; TnT, troponin T; IL-2R, interleukin-2 receptor; IGFBP-3, insulin-like growthfactor–binding protein 3; IGFBP-1, insulin-like growth factor–binding protein 1; sMesothelin, soluble mesothelin-related peptide; sTfR,soluble transferrin receptor; Lp(a), lipoprotein(a); MPO, myeloperoxidase; PCT, procalcitonin; HE4, cancer antigen, human epididymisprotein 4; ST2, interleukin-1 receptor-like 1; CKfrag21-1, cytokeratin fragments 21-1; IGF-II, insulin-like growth factor 2; BNP, smallform of N-terminal pro–brain natriuretic peptide (introduced in 2002); LP-PLA2; lipoprotein-associated phospholipase A2; TnI, cardiactroponin I; CA15-3, cancer antigen 15-3 (same as CA27.29); Panc amylase, pancreatic amylase.
Opinions
Clinical Chemistry 59:1 (2013) 195
Andersonetal.ClinChem2013;59:194

FDA-cleared Protein Tests Introduced 1993-2013
20
often have not targeted critical decision points. Distin-guishing cancer patients, or other very sick people,from controls is apparently easy—it has been the sub-ject of thousands of papers. Far more difficult, how-
ever, is distinguishing rapidly growing from slowlygrowing prostate tumors (for example), which wouldprovide new information that would profoundly affecttreatment.
Fig. 1. Trend in the number of biomarker-related NIH-funded grants and related publications over 21⁄2 decades.
Fig. 2. FDA-cleared protein tests introduced since 1993 [updated from Anderson (1 )].HER-2, human epidermal growth factor receptor 2; TnT, troponin T; IL-2R, interleukin-2 receptor; IGFBP-3, insulin-like growthfactor–binding protein 3; IGFBP-1, insulin-like growth factor–binding protein 1; sMesothelin, soluble mesothelin-related peptide; sTfR,soluble transferrin receptor; Lp(a), lipoprotein(a); MPO, myeloperoxidase; PCT, procalcitonin; HE4, cancer antigen, human epididymisprotein 4; ST2, interleukin-1 receptor-like 1; CKfrag21-1, cytokeratin fragments 21-1; IGF-II, insulin-like growth factor 2; BNP, smallform of N-terminal pro–brain natriuretic peptide (introduced in 2002); LP-PLA2; lipoprotein-associated phospholipase A2; TnI, cardiactroponin I; CA15-3, cancer antigen 15-3 (same as CA27.29); Panc amylase, pancreatic amylase.
Opinions
Clinical Chemistry 59:1 (2013) 195
IoannidisJPA.ClinChem2013;59:202-4.

Association between biomarkers and disease often overstated
• Analysisof35ofthemosthighlycitedstudiespublishedbetween1991and2006in10well-regardedbiomedicaljournals
• Eachofthestudieshadbeenreferencedbyatleast400subsequentpapers;somehadcitationsnumberinginthethousands.
• Thestudiesanalyzedtherelationshipsbetweenbiomarkerssuchasthepresenceofspecificgenesorinfections,levelsofbloodproteinsandothermarkerswiththelikelihoodofdevelopingconditionssuchascancerandheartdisease.
• For29of35studiesincludedintheiranalysis,thesubsequentlypublishedmeta-analysisreportedalessoptimisticeffectsizeestimatethanthehighlycitedstudy.
21
IoannidisJPA,PangioyouOA.JAMA2011;305:2200-10.

22
publishing major discoveries leads toselective reporting from chasing sig-nificance. Half of the highly cited stud-ies were published early and this mayalso have given them a citation advan-tage (more time to accrue citations).However, half of the highly cited stud-ies were not published early in the ac-cumulation of evidence, and often theseattractive articles were among the late-appearing studies on the question of in-terest. There are some cases where thehighly cited studies were even pub-lished after the largest study in the field.More extreme estimates of associa-tions can be seen in both early studiesand late-appearing studies.
The potential exaggeration of ef-fects was seen in almost all cases thatwe analyzed, but some exceptions may
Figure. Relative Risks in the Highly Cited Studies vs the Corresponding Largest Studies and inthe Highly Cited Studies vs the Corresponding Meta-analyses
30
15
5
1
0.55 15 3010.5
Relative Risk in the Highly Cited Study
Rel
ativ
e R
isk
in th
e M
eta-
anal
ysis
30
15
5
1
0.55 15 3010.5
Relative Risk in the Highly Cited Study
Rel
ativ
e R
isk
in th
e La
rges
t Stu
dy Published early (first 2 y)Published late (after first 2 y)
A B
Diagonal lines represent equal effects between the highly cited study and the largest study (A) or the meta-analysis (B), respectively. A, Not shown are 3 topics whereby the highly cited study was the same as the largeststudy. B, Meta-analyses may include the data from the highly cited studies, but the latter are usually smallcompared with the corresponding meta-analyses (median, 5%; interquartile range, 2%-12%, of the meta-analysis sample size).
Table 3. Effect Sizes in Highly Cited Studies, Meta-analyses, and Largest Studies (continued)
Disease orOutcome Risk Factor
Relative Risk(95% CI) in
Meta-analysisa
Relative Risk(95% CI) in
Largest Study
Relative Risk(95% CI) in
Highly CitedStudy
Type of Estimate(Exposure Contrast)
Representationof the OriginalEffects in the
Meta-analysisb
Vascular disease Hyperhomocysteinemia 1.58 (1.49-1.68) 1.29 (1.09-1.58) 27.7 (3.20-240.0) OR (increased vsnormal levels)
Same
Deep veinthrombosis
Hyperhomocysteinemia 1.35 (1.11-1.66) 1.21 (1.04-1.40) 1.50 (1.06-2.11) OR (per 5-µmol/Lincrease)
DC
Venousthrombosis
Prothrombin gene,G20210A
3.17 (2.91-3.46) 3.45 (2.69-4.43) 2.76 (1.36-5.60) OR (AA!GA vs GG) Same
Type 2 diabetes TCF7L2 gene,DG10S478
1.38 (1.31-1.45) 1.34 (1.24-1.44) 1.52 (1.28-1.80) OR (T vs G allele ofrs12255372)c,d
DC
PPARG2 gene,Pro12Ala
1.18 (1.11-1.25) 1.14 (1.08-1.20) 4.55 (1.26-20.29) OR (C vs G allele) DC
Life-threateningbleeding withwarfarin
CYP2C9 gene, *2/*3polymorphism
2.26 (1.36-3.75) 2.29 (1.18-4.64) 2.39 (1.18-4.86) RR (*2 or *3 vs *1) Same
Interferonresponse inHCV infection
NS5A2209-2248 proteinmutations
5.53 (4.50-6.79) 7.94 (5.35-11.73) 7.94 (5.35-11.73) RR (mutant vsnonmutantisolates)
DC/DA
Pneumococcalpneumoniamortality
Penicillin resistance 1.37 (1.05-1.78) 1.50 (0.91-2.47) 1.00 (0.51-1.95) OR (PRSP vs PSSP) Same
Preterm delivery oflow-birth-weightinfant
Bacterial vaginosis 2.16 (1.56-3.00) 1.28 (0.98-1.68) 1.55 (1.20-2.01) OR (exposed vsnonexposed)
DA
Age-relatedmaculardegeneration
CFH gene, H1haplotype
2.43 (2.17-2.72) 2.05 (1.75-2.36) 2.41 (2.04-2.85) OR (Y402Hheterozygotes)
DC
Fracture Bone mineral density 1.45 (1.39-1.51) 1.54 (1.48-1.59) 1.54 (1.48-1.59) OR (per SD decrease) DC/DAAtrophic gastritis
and intestinalmetaplasia
H pylori 5.00 (3.10-8.30) 3.30 (1.30-6.60) 9.00 (1.90-41.3) RR (exposed vsnonexposed)
S!
Abbreviations: CI, confidence interval; CRP, C-reactive protein; DD, homozygous for the deletional (D) allele; DDE, l,l-dichloro-2,2-bis(p-chlorophenyl) ethylene; HCV, hepatitis C virus; Hpylori, Helicobacter pylori; DI, heterozygous for the D and I alleles; IGF-1, insulinlike growth factor 1; II, homozygous for the insertional (I) allele; NS5A2209-2248, amino acid sequence 2209to 2248 of nonstructural protein 5A; OR, odds ratio; PRSP, penicillin-resistant Staphylococcus pneumoniae; PSSP, penicillin-susceptible Staphylococcus pneumoniae; RR, risk ratio.
aAccording to random-effect calculations—except for hyperhomocysteinemia and vascular disease, and bone mineral density and fracture, where fixed-effect calculations have been used.bDC indicates different contrast of exposure between the highly cited study and the corresponding meta-analysis; DA indicates different adjustments for covariates between the highly cited
study and the corresponding meta-analysis; S! indicates the highly cited study was represented in the corresponding meta-analysis by another study with larger sample size; and S−indicates the highly cited study was represented in the corresponding meta-analysis by another study with smaller sample size.
cThe meta-analysis examined the association between type 2 diabetes and rs12255372, which is in high linkage disequilibrium (r2=0.95) with the marker DG10S478 reported in the highlycited study.
dThis is the summary OR for the 3 populations of the highly cited study, as they are reported in the meta-analysis.
EFFECT SIZES AND BIOMARKERS IN HIGHLY CITED ARTICLES
©2011 American Medical Association. All rights reserved. JAMA, June 1, 2011—Vol 305, No. 21 2207
at McGill University Libraries on July 11, 2011jama.ama-assn.orgDownloaded from
IoannidisJPA,PangioyouOA.JAMA2011;305:2200-10.

Diagnostic Biomarkers: Are We (actually) Moving from Discovery to
Clinical Application?
23
107• Numberofpreviouslyreviewedstudiespublishedin2006thatevaluatedthediagnosticvalueofamolecularor-omicsbasedtest
4259• Numberofarticlesreviewedcitingthesestudiesover10yearperiod2006-2016
118• Numberofstudiescontinuingresearchonthediagnosticvalueofthemolecularor–omics-basedtest
93• Numberofstudiesreportingprogressinvalidationofthetestforuseinclinicalpractice(or21%waste)
Parkeretal.ClinChem2018;64:1657-67.

How do you define progress?
24
BOX 1.
Types of progress in validation of molecular- or “-omics”-based diagnostic tests for use in clinical practice.
• Advance in the clinical validation: Further study report-ing the diagnostic accuracy of the test in an indepen-dent patient series comparable to the population onwhom the test would be used in practice.
• Technical improvement: Further study reporting modifi-cation of the assay or computational procedures toimprove diagnostic accuracy.
• Extended diagnostic application: Further study reportingapplication of the test to a different diagnostic questionin the same disease, independently of the study designused.
• Economic evaluationa: Further study performed specifi-cally to estimate the cost of using the test in clinicalpractice.
• Clinical use or implementationa: Further study evaluatingthe effect of using the test in practice or addressingquestions relevant to implementation of the test in practice(e.g., resources needed, training, turnover time).
a Only applicable if the clinical validity has previously beenestablished in an independent patient series comparable to thepopulation on whom the test would be used in practice
The definition of which studies constituted an ad-vance in clinical validation was heavily dependent on thedesign of the initial diagnostic study from 2006. Forexample, if the initial study used a healthy control or analternate-diagnosis control design, it automatically con-stituted progress when a new study used an independentpatient series comparable to the population on whom thetest would be used in practice. Studies comparing sickindividuals with controls could also be classified as anadvance in clinical validation, if the authors correctlyjustified the patient selection, for example, the evaluationof the likeliness of false-positive or false-negative resultsin certain patient groups in which we may suspect thediagnostic accuracy to be modified (comorbidities, preg-nancy, and such like). If both the initial diagnostic studyand the new study used independent patient series com-parable to those on whom the test would be used inpractice, the new study was only considered to constituteprogress if the authors justified why it was important tocarry out the new evaluation and indicated the additionalinformation relevant to the clinical application of the testthat is provided by the study.
Two authors independently classified each study ac-cording to whether or not it constituted progress and the
type of progress. Agreement in the classification of prog-ress was 91.5%; agreement in the classification of the typeof progress was 91%.
ANALYSIS
Using medians and interquartile ranges, we summarizedthe number of citations received by the 107 moleculardiagnostic studies published in 2006 in a 10-year period.Statistical comparisons between different subgroups weremade with a Kruskal–Wallis test. We considered that themolecular diagnostic tests published in 2006 had made astep toward clinical application if there was at least 1citation in the subsequent 10 years that we classified as“progress” according to the criteria established in Box 1.Citations from studies assessing the diagnostic value ofthe 107 tests could represent more than 1 type of progressas relevant. We calculated the proportion of studies thathad made progress and assessed the relationship betweenthese proportions and the characteristics of the initialstudy, using the Pearson !2 test, when possible, and theFisher exact test when the expected count in 1 of thesubgroups of analysis was less than 5. We performed thestatistical analysis using Stata SE version 12.
Results
We retrieved 4259 articles that cited the 107 molecular-or “-omics”-based diagnostic studies from 2006 throughDecember 2016. After screening abstracts and examiningthe full texts, we selected 118 (2.8%) for further analysis(Fig. 1) because they continued to evaluate the diagnosticvalue of 1 of the initial molecular- or “-omics”-based testsproposed. The total number of citations per study rangedfrom 3 to 282, with a median of 25 (Table 1). The num-ber of citations received was significantly associated withthe impact factor of the journal that published the initialstudy, with high-impact journals tending to receive morecitations (Table 1, P ! 0.004). There were also statisticaldifferences in the citations received according to the mo-lecular technology used (Table 1). Of the 118 diagnosticstudies analyzed in detail, 93 (78.8%) reflected progresstoward clinical application of the test, and the remaining25 (21.2%) did not constitute progress toward validationof the test for use in clinical practice and hence wereclassified as potential research waste. Although researchwaste was more frequent in lower impact journals (orjournals not indexed in Web of Science Journal CitationReports), the differences observed were not statisticallysignificant. Similarly, there were no significant differ-ences in the proportion of papers classified as waste overthe 10-year period studied (see Table 1 in the online DataSupplement).
Only 33 (30.8%) of the 107 molecular tests pub-lished in 2006 were the object of continued diagnosticresearch in the following 10 years, and 28 (26.2%) of
1660 Clinical Chemistry 64:11 (2018)
Parkeretal.ClinChem2018;64:1657-67.

Progress in the validation of 107 molecular diagnostic tests for use in clinical practice over a
10-year period
25
107moleculartestspublished
33PCRbasedtestssubjectedtocontinued
diagnosticresearch
28madeprogresstowardclinicalapplication
17clinicalvalidation13technicaladvance
44proteomicbasedtests
4madeprogressintowardclinicalapplication
Parkeretal.ClinChem2018;64:1657-67.

Limitation on the Acceptance of a Test:
Cholesterol versus ApoB-100 • Cholesterol
– CDCreferencemethod(Abell-Levy-Kendall-Brodie-Kendallmethod+IDMS)fortotalcholesterolisconsideredthe“goldstandard”forcholesterolmeasurement.
– ItservedastheaccuracybaseforalloftheepidemiologicstudiesandclinicaltrialsonwhichtherelationofincreasedbloodcholesteroltoCHDisbasedandthemedicaldecisionpointswerederived.
– Since1988,therehasbeenaprogramforstandardizationandtraceabilityofcholesterolmeasurementstotheNationalReferenceSystemforCholesterol(NRS/CHOL)
• OUTCOME:Improvedtestreliability
26MyersGLetal.ClinChem2000;46:1762-72

Limitation on the Acceptance of a Test: Cholesterol versus ApoB-100
• ApoB100– Calibrationstandards:CLSI-C37Anativeproteinwithassignedvalue(secondaryreferencematerial)
– apoBisfoundinotherparticles:VLDL,IDL,Lp(a),Chylomicronremnants
– LackstraceabilityandstandardizationtoaSystèmeinternationalunit(i.e.moles)
– CurrentobjectiveofaIFCCworkinggroupisapeptidebasedcalibrationMS-based(traceable)
27LangloisMRetal.ClinChem2018;64:1006-33

28
Precisionandaccuracyof10methodsfornon-HDL-Pdetermination
Delatoureral.ClinChem2018;

Errors In Databases?
• HGMD– Of239uniquevariantsdescribedasdiseasecausingonly7.5%fitthiscategory
• OMIM/HGMD– 27%ofannotationsforrecessivedisease-causingvariantsareincorrect
• ClinVar/ClinGen– Only56,742/172,870hadatleastone-starentry– variantsareclassifiedintoatleastthreeclinical-significancetiers,andthemethodsusedfortheassignmentandsupportingevidencemustbeprovided).
• Consequenceonmutationassessment?
NatureMethods2016;13:103

Liquid Biopsies: The Promise
• Whatitis?Analysisofcell-freecirculatingtumor(ct)DNAinblood
• ThePrize– Identifymetastaticdiseaseearlyon– Non-invasively– Cost-effectively
30M.Ratner.NatureBiotechnology2018;16:209-210.

31

Liquid Biopsies: The Reality
fusions (6 genes), and indels (23 genes) with high clinicalsensitivity rates (85% in stage III/IV solid tumors) and ultra-high specificity (>99.9%).2,4
PlasmaSELECT (Personal Genome Diagnostics, Inc) con-sists of a 64-gene panel with a reported sensitivity for single-base mutations and indels of 99.4% and a per base specificitygreater than 99.9%.2,5 Analytic sensitivity for indels and pointmutations is reported to be down to 0.1% mutant allele frac-tion in Guardant360 and 0.5% in PlasmaSELECT.2,4,5
Prostate-specific antigen (PSA) baseline serum levels weredetermined within 30 days of the genetic test for 90% of pa-tients, mean time from PSA blood work to the cfDNA test was16 days (range, 0-115 days). Written informed consent was ob-tained in accordance with Johns Hopkins University School ofMedicine institutional review board (IRB) guidelines, and thisstudy received IRB approval.
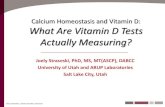
Results | The genetic alterations determined by cfDNA testingand baseline PSA serum levels in our cohort of patients withmetastatic prostate cancer are summarized in Figure 1. Par-ticipants were classified as complete congruence, 0 altera-tions if neither platform detected any alteration, (9/40 [22.5%])(Figure 2).
For the study of congruence among tests, only genetic al-terations in genes purportedly covered by both platforms wereconsidered (42 genes), thus patients with 1 or more altera-tions demonstrated by at least 1 platform (31/40 [77.5%]) whoseall cfDNA alterations were covered by only 1 of the tests wereexcluded (6/40 [15%]). Out of the 42 genes in the overlappingpanel, a total of 25 genes had reported alterations in our co-hort (60%); TP53 (n = 10), ATM (n = 6), ALK, BRCA1, and BRCA2(n = 5) were the most common.
Exome coverage for every gene in each sequencing paneldiffers between platforms. Congruence among tests was as-sessed on confirmation of exome coverage in the counterpartplatform for each alteration reported, excluding those altera-tions reported whose chromosomic location was not coveredby the other platform.
There were 25 of 40 (62.5%) patients with alterations inthe overlapping genes with confirmed coverage. Three (7.5%)of 40 patients had complete congruence with 1 or more altera-tions, 6 (15%) of 40 had partial congruence, and 16 (40%) of40 had no congruence. The remaining 15 patients either didnot have any reported alteration (complete congruence with0 alterations, 9/40 [22.5%]) or were not evaluable for patient-level congruence (6/40 [15%]).
Discussion | Despite the limited sample size, our data show verylow congruence for same patient-paired samples in 2 CLIA-certified commercially available tests with self-reported highaccuracy, specificity, and sensitivity to specifically detect andquantify tumor-specific alterations. These data cannot deter-mine which test is more accurate but suggest that reported genealterations will not be the same across different platforms, rais-ing the specter that patients could potentially receive differ-ent treatments depending on the cfDNA platform. Insuffi-cient genetic profiling congruence could jeopardize the clinicalbenefit of personalized medicine.1,6
Gonzalo Torga, MDKenneth J. Pienta, MD
Author Affiliations: The James Buchanan Brady Urological Institute, JohnsHopkins University School of Medicine, Baltimore, Maryland.
Corresponding Author: Gonzalo Torga, MD, Marburg 113 – UrologyDepartment, Johns Hopkins Hospital, 600 N Wolfe St, Baltimore, MD 21287([email protected]).
Accepted for Publication: September 14, 2017.
Published Online: December 14, 2017. doi:10.1001/jamaoncol.2017.4027
Author Contributions: Drs Torga and Pienta had full access to all of the data inthe study and take responsibility for the integrity of the data and the accuracyof the data analysis.Study concept and design: All authors.Acquisition, analysis, or interpretation of data: All authors.Drafting of the manuscript: All authors.Critical revision of the manuscript for important intellectual content: All authors.Statistical analysis: Torga.Obtained funding: Pienta.
Figure 2. Congruence Analysis of cfDNA-Targeted Next-Generation Sequencing in 2 Independent Commercial Platforms
0 4 6 8 8 12 14 16
Patients, No.2
No congruence
Partial congruence
Complete congruence, 1 or more alterations
Not evaluable for patient-level congruence,0 alterations covered by both panels
Complete congruence, 0 alterations
Patients negative for cell-free DNA (cfDNA) alterations in both tests wereclassified as complete congruence for 0 alterations (9/40 [22.5%]). Forcongruence analysis, patients who had 1 or more alterations reported, but nonewas covered by both tests, were excluded and classified as not evaluable for
patient-level congruence (6/40 [15%]). The proportion of patients withcomplete congruence for 1 or more alterations, partial, and no congruence was3 of 40 (7.5%), 6 of 40 (15%), and 16 of 40 (40%), respectively, among the2 platforms.
Letters
jamaoncology.com (Reprinted) JAMA Oncology June 2018 Volume 4, Number 6 869
© 2017 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a McGill University Libraries User on 03/25/2019
32
• Bloodsamplesfrom40patientswithprostatecancersenttotwodifferentclinicallaboratories:Guardant360&PersonalGenomeDiagnostics
• 65%ofspecimenshadonlypartialornocongruence
TorgaG,PientaKJ.JAMAOncology2018;4:868-869

Planned Introduction of Beckman hsTnI on March 28, 2019 at noon at all MUHC sites
33

Beckman hsTnI • HigherAnalyticalprecisionatlowerconcentrations-Improveslow-end
measuringrangewithademonstratedlimitofdetection(LoD)at2.3ng/L– Enablespreciseandreliablemeasurementoflowtroponinlevels
• Greaterclinicalsensitivityformyocardialinjury-Meetsallhighsensitivityrequirementsdefinedbyinternationalguidelines1– Measurescardiactroponin(cTn)valuesabovetheLoDin>50%ofahealthy
population– Demonstratesoptimalprecision:<10%CVimprecisionatthe99thpercentile
upperreferencelimit(URL)• Demonstratesexcellentcorrelationandconcordancewiththecurrent
AccuTnI+3assay(NOTIDENTICAL)• Accuraterecognitionofsmallchanges-Providesdeltavaluesandsex-
specific99thpercentileURLvalues• Reducesanalyticalfalsepositives• cTnIbiologyremainsthesame!
34

hsTnI: Some Key Points
• TheidealtesthashighbothsensitivityandNPV.• Anelevatedhs-cTnidentifiesthepresenceofmyocardialinjurybutnotthemechanismorunderlyingcause.
• MyocardialinjuryoutsidethatoccurringinthesettingofAMIcancreatediagnosticchallengesbutshouldnotbediscardedasanuisanceabnormality,becauseitisassociatedwithapoorcardiovascularprognosis.
• Termssuchas“troponinleak,”“troponinemia,”or“troponinitis”areunadvisablebecausesuchtermstrivializetheprognosticmeaningofmyocardialinjury.
35Januzzietal.JACC2019;73:1059

hsTnI: More Key Points
• TheabsolutechangeinTnhasgreaterdiagnosticaccuracyforAMIthanrelativechangecriteria.
• AcutoffsetatorneartheLoDofthehs-cTnIassayachievesveryhighNPVforAMI.
36

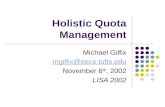
The Hope: A Clear Algorithm allowing Rapid Patient Disposition in the ER and
Only in the ER
37
Page 9 of 10
Figure 1: 0 hour/3 hour rule-in/rule-out algorithm for non-ST elevation acute coronary syndromes from ESC guidelines2
Contact information
For more information about the Access hsTnI assay or for reagent ordering information you can:
> Visit the Beckman Coulter website: http://www.beckmancoulter.com
> Contact your local Beckman Coulter representative
Acute Chest Pain
hs-cTn <URL hs-cTn >URL
Pain >6 hours Pain <6 hours
hs-cTn no change
Pain-free, GRACE <140,differential diagnoses excluded
Discharge/stress testing
∆ change* (l value >URL)
hs-cTn no change
Work-up differential diagnoses
Re-test hs-cTn: 3 hours
Hig
hly
abn
orm
al h
s-cT
n
+ C
linic
al p
rese
ntat
ion
G RACE = G loba l Reg ist ry of Acute Coronary Event s scorehs -cT n = h igh sensi t ivi t y card iac t ropon inURL = upper ref erence l imi t , 99 t h percent i le o f hea l t hy popula t ion* ∆ change dependent on assay. Highly abnormal hsT n def ines values beyond 5-f o ld t he URL.
Invasive management

Planned Guidance MYOCARDIALDAMAGE/INFARCTIONISRULEDOUTINPATIENTS:
presentingwithchestpaingreaterthan3hourssinceonsetwithoutclinicalevidenceofischemiaandhsTnIlessthanorequalto6ng/Lininitialsample
(LoD=2.3ng/L)OR:
hsTnIlessthanorequalto17.5ng/Lininitialsampleanddelta(change)lessthanorequalto5ng/L,3hourslater.
(PPV=66%&NPV=97%)CONSIDERMYOCARDIALDAMAGE/INFARCTIONIF:
hsTnIisgreaterthanorequalto87.5ng/LininitialsampleORdelta(change)greaterthanorequalto22ng/L3hourslater,withclinicalevidenceofischemia.
(PPV=90%&NPV=94%)
38

But, will we be seeing a lot more positives?
39
AccesshsTnI
AccuTnI+3 +ve>17.5ng/L -ve≤17.5ng/L
+ve>0.04µg/L 23 0
-ve≤0.04µg/L 6 31
Accuracy=54/60x100%=90%(79-96%CI)
B.Gilfix.Inhouseevaluationstudy-Lachine

WHATABOUTTESTSTHATARENOTDONEIN-HOUSE?
40

41
Send-Out Tests?
• OntheislandofMontreal– AsonApril1,2010,thesearenocharge.
• IntheProvinceofQuebec– UsuallydoesnotrequireapprovalbyaLaboratoryPhysician(MedicalBiochemistry,Hematology,Microbiology,MedicalGenetics)

42
Send-Out Tests?
• OutsideoftheProvinceofQuebec– AlwaysrequiresapprovalbyaLaboratoryPhysician(MedicalBiochemistry,Hematology,Microbiology,MedicalGenetics)
– RAMQAH-612formsignedbyrequestingphysicianANDLaboratoryPhysicianandsentbeforesampleisdrawn
– Why?• Istestjustified?• Whatisthesampletype?• Howisithandled&stored?• Whereistestdone?

43AUTORISATION POUR DES SERVICES DE BIOLOGIE MÉDICALE NON DISPONIBLES AU QUÉBEC
AH-612 DT9186 (rév. 2012-05)
DT9186
AUTORISATION POURDES SERVICES DE BIOLOGIE MÉDICALE
NON DISPONIBLES AU QUÉBEC
À REMPLIR PAR LE PROFESSIONNEL AUTORISÉ À PRESCRIREIdentité de l’usager
Nom de famille à la naissance Prénom Année Mois JourDate denaissance
Sexe Numéro d’assurance maladieNuméro
M F Nouveau-né de dossierNuméro Rue Appartement Ville
Adresse Province Code postal Ind. rég. N° de téléphone N° de poste Ind. rég. Autre téléphone N° de poste
Diagnostic et services demandésDiagnostic Code OMIM ou autre Grossesse en cours
Oui NonServices de biologie médicale demandés
Renseignements complémentaires concernant les services demandés
Si analyse génétique pour maladie héréditaire : confirmation d’absence de mutation familiale connue
Résumé du dossier clinique justifiant les services demandés et, s’il y a lieu, l’envoi simultané de plus d’un test pour un même usager.Si pertinent, joindre des documents supplémentaires (ex. : arbre généalogique)
Identité du professionnel autorisé à prescrireNom Prénom
Numérode permis
Spécialité Ind. rég. N° de téléphone N° de poste Ind. rég. N° de télécopieur
Nom de l’établissement
Numéro Rue
Adresse Ville Province Code postal
Personne-ressource à joindre pour informationNom Prénom Ind. rég. N° de téléphone N° de poste
Usager Professionnel Médecin Direction des ressources financières Régie de l’assurance maladieautorisé à prescrire approbateur de l’établissement désigné du Québec (RAMQ)
Année Mois JourSignature du professionnel Dateautorisé à prescrire
IMPORTANT: to ensure success in the process for external laboratory analysis requests, all requesting physicians must complete all highlighted fifields.
Note: if the RAMQ AH-612 is incomplete and/or illegible, the form will be returned to the requesting physician for completion.

44
Nom de l’usager N° d’assurance maladie N° de dossier
AH-612 DT9186 (rév. 2012-05)AUTORISATION POUR DES SERVICES
DE BIOLOGIE MÉDICALE NON DISPONIBLES AU QUÉBEC
J’atteste que, autant que je sache, les services de biologie médicale sont :
cliniquement requis;
non disponibles au Québec;
non disponibles au Canada (dans le cas d’une demande de services à l’extérieur du Canada).
Année Mois JourSignature du médecin approbateur Date
Année Mois JourSignature du directeur des ressources Datefinancières de l’établissement désigné
Nom PrénomNumérode permis
Spécialité Ind. rég. N° de téléphone N° de poste Ind. rég. N° de télécopieur
Établissement désigné :
CHU Sainte-Justine CHUS CHUM CHUQ CUSM HMR HGJ CHAUQ
Numéro Rue
Adresse Ville Province Code postal
À REMPLIR PAR LE MÉDECIN APPROBATEUR
Identité du médecin approbateur rattaché à un établissement désigné(médecin généticien ou médecin de laboratoire ayant une compétence officiellement reconnue par son établissementdans le domaine concerné par la demande d’analyse)
Coût réel des services ($ CAD)$
Établissement où les services de biologie médicale seront réalisésNom de l’hôpital ou du laboratoire Nom et prénom du médecin responsable Coût estimé des services ($ CAD)
$Numéro Rue Bureau
Adresse Ville Province/État Pays Code postal
La demande est :
autorisée annulée après discussion avec le professionnel prescripteur

45
Examples of Commonly Used Outside Laboratories
• Criteria:– Mustbeclinicallycertifiedlaboratory– Notresearchlaboratory– Canada1st
• Examples:– InCommonLaboratories(Ontario)– MayoMedicalLaboratories– ARUPLaboratories– QuestLaboratories– AthenaLaboratories– PreventionGenetics– GeneDx

46
AH-612 Form Received at Send-out bench
Sent for approval
DecisionApproved Not Approved
Typical reasons for not being approved:• test available in Quebec• test not available in a clinical lab• test not validated (e.g. available ina single commercial lab & all literature comes from that lab)• too broad or expensive in clinicalcontext (e.g. Is it AR, AD, or X-linked? Is testing for a common cause more efficient than testing for a rare cause?)
Reason written on 2nd page by approver. Initialed and dated.
Form stamped "Not approved".
Signed form faxed back to MD
requesting to have sample
drawn
Signed form filed.Request entered into data base.
BMGJan. 10, 2014; Updated Oct. 14, 2015
Process for Obtaining of Approval for
Out-of-province testing at MUHC
MUHC samples Yes
No
Signed form faxed back to Laboratory (non-
MUHC)MUHC
samplesYes
No
'BY�BQQSPWFE�SFGVTFE�3".2�")�����CBDL�UP�SFRVFTUJOH�QIZTJDJBO
3".2�")�����JT�SFHJTUFSFE�JO�3".2�EBUBTFU�3".2�SFRVFTU�JT�WBMJE�GPS���ZFBS
4BNQMFT�TPSUFE �MPHHFE�JO�BOE�TUPSFE�JO�GSJEHF�GSFF[FS�3".2�EBUBTFU�JT�VQEBUFE�BOE�TBNQMFT�BSF�TFOU�UP�FYUFSOBM�MBCPSBPUSZ�
'PSN�TUBNQMFE�h$BODFMMFE�"OOVMÏh

What to Expect in the Next 12 Months?
• Revisedlymphocytestimulationtest(finalstage)
• NT-ProBNP• Alzheimerdisease• VitaminB12metabolism• Alpha1-Antitrypsin
47