Office Management of Pediatric Concussions · Office Management of Pediatric Concussions Donna K....
55
Office Management of Pediatric Concussions Donna K. Broshek, Ph.D., ABPP-CN Co-Director, Acute Concussion Evaluation Clinic Director, Neurocognitive Assessment Lab John Edward Fowler Professor Psychiatry & Neurobehavioral Sciences
Transcript of Office Management of Pediatric Concussions · Office Management of Pediatric Concussions Donna K....

Office Management of Pediatric
Concussions
Donna K. Broshek, Ph.D., ABPP-CN
Co-Director, Acute Concussion Evaluation Clinic
Director, Neurocognitive Assessment Lab
John Edward Fowler Professor
Psychiatry & Neurobehavioral Sciences

Disclosures• Funding from Virginia Department of Aging & Rehabilitative
Services for community TBI screening project
• Immediate Past President, Sports Neuropsychology Society
– The NFL & NHL are key sponsors of SNS conference.
– Not involved in our scientific program.
• Member of NBA/WNBA Concussion Committee
(uncompensated)
• Member of multiple concussion advisory panels for local schools
& UVA (uncompensated)

Objectives
• Understand the acute symptoms of concussion and typical
recovery for children & adolescents
• Become familiar with evidence based recommendations
for clinical management of concussion
• Understand the importance of identifying, diagnosing, &
treating specific prolonged post-concussion symptoms

Concussions…

Not just football…

Not just contact sports…

Not just males…

Not just sports…

Concussion definition (Berlin, 2017)
• Sport related concussion (SRC) is a traumatic brain injury
induced by biomechanical forces. Common features include:
– May be caused either by a direct blow to the head, face, neck or
elsewhere on the body with impulsive force transmitted to head.
– Typically results in rapid onset of short-lived impairment of
neurological function that resolves spontaneously. However, in
some cases, signs and symptoms evolve over a number of
minutes to hours.
– May result in neuropathological changes, but the acute clinical
signs and symptoms largely reflect a functional disturbance
rather than a structural injury and, as such, no abnormality is
seen on standard structural neuroimaging studies.

Concussion definition (Berlin, 2017)
• SRC results in a range of clinical signs and symptoms that
may or may not involve loss of consciousness.
• Resolution of the clinical and cognitive features typically
follows a sequential course. However, in some cases
symptoms may be prolonged.
• The clinical signs and symptoms cannot be explained by
drug, alcohol, or medication use, other injuries (such as
cervical injuries, peripheral vestibular dysfunction) or other
comorbidities (e.g., psychological factors or coexisting
medical conditions).

CDC Pediatric Guidelines (2018)
• Recommends the term mTBI
• One or more of:
– Confusion or disorientation
– LOC for 30 minutes or less
– Post-traumatic amnesia for less than 24 hours
– Other transient neuro findings: focal signs, symptoms,
or seizure
• Glasgow Coma Scale (GCS) score of 13-15

CDC mTBI Includes:
• GCS scores of 13-15
• “With or without the complication of
intracranial injury on neuroimaging”
• “Regardless of potentially requiring a
hospital admission and/or neurosurgical
intervention”
• Very different definition….

Expected Recovery• 70-80% of children with mTBI recover within 1-3
months (CDC)
• Vast majority recovery from SRC and return to
play or school within 1 month (Davis et al, 2017)
– Significant proportion experience symptoms > 1 month
– Adolescents may take longer to recover than younger
or older
• Individualized concussion management
for all ages is key.

AAN Guidelines (2013)
• Immediate removal from play if concussion
suspected
• Discarded concussion grading system:
• Focus on individual management
• No set timeline for return to play
• Concussion is a clinical diagnosis– Checklists, computerized testing, & balance assessments
are tools.

AAN Guidelines (2013)
• No return until assessed by a licensed health
care professional trained in concussion.
• Return to play slowly after acute symptoms
resolve.
• High school and younger – manage more
conservatively due to longer recovery.
• First 10 days after a concussion is the period of
greatest risk for another concussion.

Virginia Senate Bill 652 (2010)
• Mandates concussion education in all public high schools for coaches, student-athletes, & parents, as well as policies and procedures
• Student-athletes & parents to receive annual education
Virginia Senate Bill 652 (2010)
• Any athlete with suspected concussion shall be removed from play/activity– Shall not return the same day
– MUST be evaluated by health care professional• Licensed physician, physician assistant, osteopath, athletic trainer,
neuropsychologist, or nurse practitioner
– Must be asymptomatic with increasing exertion (Zurich)*
– Requires written clearance for return to activity

Virginia Senate Bill 172 (2014)
• Board of Education shall amend its
guidelines for school division policies
and procedures on concussions in
student-athletes to include a "Return to
Learn Protocol“

Virginia Board of Education
Guidelines for Policies on
Concussions in Student-Athletes
• Premature return to learn/play may
delay and/or impede recovery.
• Return-to-play should not occur before
the student-athlete has managed to
return to a full day of academic
activities.

Audience Question
• Should children with concussions
routinely undergo neuroimaging?
1. Yes
2. No

CDC Evidence Based Guidelines
for Pediatric mTBI (2018)

CDC Key Recommendations
1. Do not routinely image patients to diagnose mTBI.
2. Use validated, age-appropriate symptom scales to
diagnose mTBI.
3. Assess evidence-based risk factors for prolonged
recovery.
4. Provide patients with instructions on return to
activity customized to their symptoms.
5. Counsel patients to return gradually to non-sports
activities after no more than 2-3 days of rest.





Tipsheet for HCPs
• On Presentation/What are the red flags?
• On Discharge – What do we tell parents and/or caregivers?
• On Interim Assessment– When can the child or adolescent return to learn/play?
• On Re-Assessment after 1 month– What do we do next if symptoms still present.?

On Presentation – Red Flags
• Assess & treat symptoms
• Determine need for CT imaging or
observation/admission– Most do not need CT
• Treat acute headaches
• Prescribe physical & cognitive rest

On Presentation
• Headache (CDC/ONF)
– Nonopiod analgesia (ibuprofen, acetaminophen)
– Counsel family on analgesic overuse & rebound headaches
• Physical & cognitive rest– Initial 24/48 hour rest period; ask parents to check for
symptoms in 24 hour intervals (ONF)
– Observe more restrictive activity during the first several
days (CDC)
– Rest within first 3 days beneficial, but greater inactivity may
prolong symptoms (CDC)


Rehabilitation
StageAim Activity Goal of each step
1. Symptom-limited
activity
Daily activities that do not provoke symptoms Gradual reintroduction of work/school
activities
2. Light aerobic
exercise
Walking or stationary cycling at slow to medium
pace. No resistance trainingIncrease heart rate
3. Sport-specific
exercise
Running or skating drills. No head impact activities Add movement
4. Non-contact
training drills
Harder training drills, e.g., passing drills. May start
progressive resistance trainingExercise, coordination, and increased
thinking.
5. Full contact
practice
Following medical clearance, participate in normal
training activitiesRestore confidence and assess
functional skills by coaching staff
6. Return to play Normal game play

On Discharge
• Provide education & reassurance (ONF)
– Current symptoms are expected and common
– Expected positive recovery
• “Parents need to know that most patients recover
fully from concussion even though the recovery
rate is variable and unpredictable….Providing
information reduces anxiety and helps set realistic
expectations, promote recovery, and prevent re-
injury.”



“Post-Concussion Syndrome”
• Non-specific symptoms
• Unclear time frames
• Wide variability in use of term
• Does not provide diagnostic or
treatment information
• Not helpful to patient

Concussion & Post Concussion
Syndrome as Red Herring

• Many symptoms are misattributed to concussion
• Misattribution of symptoms results in inadequate
evaluation & treatment
• Treatable symptoms & conditions go untreated
• Post concussion syndrome is inappropriately
diagnosed at the time of initial concussion diagnosis or
within the expected recovery curve
• Over-prescription of cognitive & physical rest, causing
iatrogenic effects of isolation & inactivity



Time to Retire:
“Post-Concussion Syndrome”
• Non-specific symptoms & unclear time frames
• Wide variability in use of term
• Results in misattribution by health care providers
• Does not provide diagnostic or treatment information
– Delays or denies appropriate treatment
– Not helpful to patient

Audience Question
• Which of the following is the most
common symptom after concussion?
1. Drowsiness
2. Irritability
3. Headache
4. Dizziness

Common Factors Affecting
Recovery
• Headaches
• Visual Disturbance
• Vestibular Dysfunction
• Anxiety
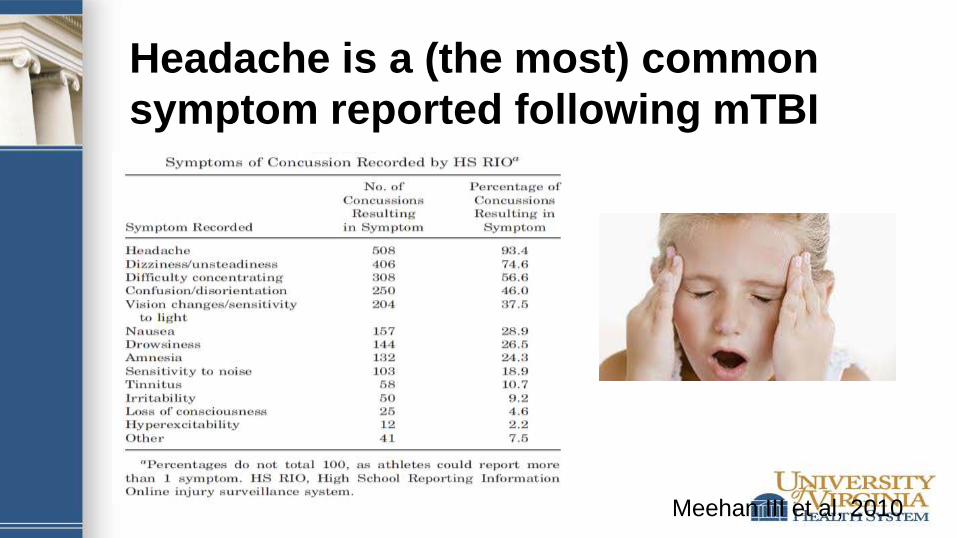
Headache is a (the most) common
symptom reported following mTBI
Meehan III et al, 2010

Vision: Convergence Insufficiency
• Common binocular vision disorder
– Eyestrain
– Headaches
– Blurred vision, diplopia [double vision]
– Sleepiness
– Difficulty concentrating
– Reading difficulties Archives of Ophthalmology. 2008;126(10):1336-1349

Vestibular Dysfunction
Vestibular system & central nervous system
work together to control eye, head & body
movements to maintain balance.
Symptoms of vestibular dysfunction:
• Vertigo
• Dizziness
• Imbalance
• Spatial disorientation
Predicting Psychological Distress
after Pediatric Concussion (Brooks et al., 2019)
• Prospective, multi-center study
– Ages 6-17, n=311
• Pre-injury anxiety is a significant predictor
of psychological distress at 4 weeks
• Screen for anxiety & manage proactively

A word about insomnia…
• Disrupted sleep is common
• Sleep deprivation can reduce reaction time,
cognitive processing speed
• Insomnia can further add to depression &
anxiety
• Poor sleep hygiene further exacerbates
insomnia and adds to lengthy recovery

Expectation as EtiologyMittenberg et al (1992, 1998)
“Beliefs about the probable effects of
concussion may well result in selective
attention to normal affective, cognitive, and
somatic responses to stress and reattribution
of those symptoms to brain injury.”

• “Most sports related head injury is minor,
and although most athletes who have a
concussion recover within a few days or
few weeks, a small number of individuals
develop long lasting or progressive
symptoms.”
• “The precise incidence of CTE after
repetitive head injury is unknown…”


The Benefits of Physical Activity
and Sport Powell et al. (2011)

Brief Interventions for Recovery

In Office Interventions
• Education & expectancy
– Symptoms are typical and expected
– You will get better
• Treat stress & sleep disturbance
– Prescribe phone apps: CBT-I Coach, Sleep
Genius, Calm, HeadSpace

In Office Interventions
• Anxiety:
• Education about anxiety as a risk factor
• Autonomic arousal in anxiety triggering
situations
• Focus on anxiety reduction
– Smart phone apps
· Diaphragmatic breathing (Breathe2Relax)
· Relaxation strategies/mindfulness
(Progressive Muscle Relaxation)

• Return to Activity • Return to Life
Concussion TreatmentDiagnose & Treat Specific Symptoms