Ocular Surface Review, Vol. 1, Issue 1
12
A guide to disease management in Asia-Pacific Dr. Hungwon Tchah Conducts a Battery of Dry Eye Tests - page 3 The Inflammatory Aspect of Dry Eye - page 11 REVIEW Which Of These Ocular Surfaces Is Not Like the Others? Which Of These Ocular Surfaces Is Not Like the Others? It’s Easy to Spot, but Meibomian Gland Dysfunction (MGD) Is Not - page 5 Vol. 1, Issue 1
-
Upload
media-mice -
Category
Documents
-
view
228 -
download
0
description
A guide to ocular surface disease management in Asia-Pacific
Transcript of Ocular Surface Review, Vol. 1, Issue 1

A guide to disease management in Asia-Pacific
Dr. Hungwon Tchah Conducts a Battery of Dry Eye Tests - page 3
The Inflammatory Aspect of Dry Eye - page 11
REVIEWWhich Of These Ocular Surfaces Is Not Like the Others?
Which Of These Ocular Surfaces Is Not Like the Others? It’s Easy to Spot, but Meibomian Gland Dysfunction (MGD) Is Not - page 5
Vol. 1, Issue 1

2
OCULAR SURFACE REVIEW
In this Issue
Challenges in the Diagnosis and Management of Dry Eye
Meibomian Gland Dysfunction and Ocular Irritation
Changing Dry Eye Diagnoses
Allergic Conjunctivitis is Increasing Globally
Demystifying Anti-inflammatory Therapy for Dry Eye Diseases
03
05
10
08
11
The incidence and prevalence of dry eye in Asia-Pacific are among
the highest rates in the world.Nowadays, more and more
people spend a lot of time in front of computers, iPads and TVs. Also, there are more international travelers in the region than before, who spend a great deal of time in airline cabins. These situations contribute to an increasing prevalence of dry eye, which has a great impact on normal life.
As a leader in providing solutions for dry eye management, Allergan feels that disease awareness is incredibly important.
Hence, with the publication of Ocular Surface Review, we would like to encourage eye care professionals to start sharing more of their experience and knowledge related to ocular surface disease. In fact, if you are an eye care professional, we invite you to share your ocular surface story in the next issue. You may do so by writing directly to the publisher Matt Young at [email protected].
Through this sharing, we hope to spread the right disease management concepts to break the vicious circle of inflammation and other problems on ocular surface at a very early stage.
In this issue, there are some wonderful new insights. In our cover story, Dr. Louis Tong, of Singapore National Eye Centre, discusses the revealing observations in his clinic and a practical application of international guidelines with a sensitivity to local characteristics and epidemiology.
Dr. Hungwon Tchah, of Seoul’s Asan Medical Center, writes about a “battery of tests” he conducts for dry eye to treat a condition that manifests with dryness in some cases, itchiness in others, and simply no clinical signs in some patients as well.
From the Philippines, Dr. Victor L. Caparas writes about the link between allergies and pollution, citing a telling example in Mongolia.
Other Asia-Pacific authors share their interesting views as well.
Allergan is your committed partner in ocular surface disease treatment, and we adhere to three principles in this regard:
1) Every patient has her/his unique disease profile and all deserve a safe and cost-effective medical care. Therefore individualized therapy is warranted.
2) Each drug/therapeutic approach needs an accurate positioning for a wise treatment paradigm.
3) To understand the pathogenesis of diseases, pharmaceutical rationales and health outcome measurement is the foundation of formulating a consensus on ocular surface health management.
Ocular Surface Review helps advance these missions, as do our organized roundtable discussions, seminars and other academic activities.
Also of note, Allergan has been continuously endeavoring to bring the breakthroughs of basic science and technology into daily practice, as well as help interpret evidences from large-scale randomized controlled trials for specific application to patients in real clinic settings. These translational medicine approaches from “bench” to “bedside” and “population” to “individuals” are committed to a vision of future human wellbeing and a safer practice environment.
We hope you enjoy this issue of Ocular Surface Review.
Sincerely,
Larry Li, M.D., M.S.C.Associate DirectorMedical and Scientific AffairsEye CareAsia-Pacific RegionAllergan Singapore Pte. Ltd.
Letter to Readers
Through Sharing, We Shall Overcome Ocular Surface Disease

3
OCULAR SURFACE REVIEW
By Hungwon Tchah, MD
It can be challenging to diagnose dry eye, because patients do
not always present with the same signs and symptoms. One patient may complain about dryness, while another patient may complain of itchiness. There are some patients who complain of many symptoms, but they have no clinical signs. Although there are some patients with obvious dryness based on clinical tests, these patients do not comprise a high number of our clinical population.
The diagnosis of dry eye is further complicated by coexisting diseases. For example, ocular allergy often is aggravated by dry eye, and vice versa. Additionally, meibomian gland dysfunction (MGD) is often seen in dry eye in Korea and the Asian population in general.1 Research has shown that the Asian population has a higher rate of MGD. We often have to treat patients’ MGD when we treat dry eye.
Sequence of Dry Eye Tests
When examining a patient for dry eye, I conduct a battery of tests. I begin with a slit-lamp examination. It is helpful to listen to a patient’s symptoms and complaints regarding dry eye, but one must consider that these reports are subjective. Symptoms do not always match the severity of the clinical signs. Even if there are no clinical signs of dry eye, if the patient complains, there is a problem, and we have to try to help to solve it.
Challenges in the Diagnosis and Management of Dry Eye
Nevertheless, some of these patients may need other kinds of medical care. I am also careful during repeat visits to listen for symptoms that are not improving, despite evidence of improved clinical signs. This may indicate the need for further analysis or a different treatment approach.
After the slit-lamp examination, I stain with fluorescein dye or lissamine green to look for erosions. I believe that lissamine green staining is more effective to spot epithelial defects and patterns that indicate dry eye, but the availability of this dye can vary from country to country. However, fluorescein dye has its advantages as well. For example, you can use fluorescein dye to check for epithelial defects and for the tear breakup time (TBUT) test.
Ocular Surface Review published by
PublisherMatt Young
EditorMary Archer
Editorial ConsultantsMichelle DaltonVanessa Caceres
DesignerWinson Chua
Published in consultation withAllergan Singapore Pte. Ltd.
Media MICE Pte Ltd6001 Beach Road, #19-06,
Golden Mile Tower, Singapore, 199589Phone: +65 8186 7677Fax: +65 6298 6316
E-mail: [email protected]
This publication is published by Media MICE Pte Ltd who is solely
responsible for its editorial content.
All rights reserved.
OCULAR SURFACE REVIEW

4
OCULAR SURFACE REVIEW
After staining, I will conduct a TBUT test. A TBUT test will assist in looking for evidence of evaporation, an important component in many dry eye cases that are seen nowadays. A breakup time of 10 seconds or more is considered normal, whereas 5 seconds or less is usually indicative of poor tear film, such as dry eye. This test can also aid in the evaluation of MGD signs.
The Schirmer’s test is commonly used for dry eye, but I find the results to be variable. If a patient has severe dry eye (5 mm or less), the test results may indicate this, but often it does not show evidence of dry eye in moderate patients. For these reasons, I will use the Schirmer’s test when necessary for research studies, but usually I do not use it otherwise.
Testing for MGD is an important part of dry eye testing in Asian patients. I will look for evidence of MGD via erosions and TBUT results. I also sometimes will express the glands to evaluate the kind of secretion that is produced. A video-meibography device for MGD diagnosis, which has an infrared light2,3 and which helps to illuminate the meibomian gland structures, appears to be a promising test, although I do not currently have it.
Testing in the Future
In a few more years, we may use more sophisticated tests for dry eye. Although the Luneau Cochet-Bonnet Aesthesiometer measures corneal sensation, it would be helpful to have a device that can more stringently connect these sensations with dry eye. It is also interesting to hear about research involving the correlations between higher-order aberrations and TBUT.
One device that can enhance dry eye diagnosis and that recently became available is the TearLab Osmolarity System (TearLab Corp., San Diego, California).4 With this test, ophthalmologists can measure the osmolarity of tears using a nanoliter-based sample from the patient. The device uses a pen to collect the tear sample and an LCD reading screen to show the results.
As mentioned previously, advancements to the current Schirmer’s test would be welcomed. The phenol red thread test, which uses special thread instead of the paper used with the Schirmer’s test, holds promise and may prove to be easier and more reliable.
Dry eye diagnosis continues to be a challenge. However, we can use the tests that are
References
1 Nichols KK, Foulks GN, Bron AJ, et al. International Workshop on Meibo-mian Gland Dysfunction: Executive Summary. Invest Ophthalmol Vis Sci. 2011;52(4):1922-1929.
2 Yokoi N, Komuro A, Yamada H Maruyama K, Kinoshita S. A newly developed video-meibography system featuring a newly designed probe. Jpn J Ophthalmol. 2007;51(1):53-56.
3 Arita R, Itoh K, Inoue K, Amano S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal popula-tion. Ophthalmology. 2008;115(5):911-915.
4 Sullivan BD, Whitmer D, Nichols KK, et al. An objective approach to dry eye disease severity. Invest Ophthalmol Vis Sci. 2010;51(12):6125-6130.
Images courtesy of Dr. Hungwon Tchah
Dry eye with MGD in a young patient. The image shows a clear lid margin
Dry eye with severe corneal erosion
Dry eye with MGD in old patient. This image shows a dirty lid margin
available — along with ones that will reach the market in the future — to properly measure dry eye severity and to provide patients with a solid treatment plan.
About the AuthorHungwon Tchah, MD, is Professor at Asan Medical Center, University of Ulsan, Seoul, Korea.

5
OCULAR SURFACE REVIEW
By Louis MG Tong, MBBS (S’pore), FRCS (Edin), DM (Nott), PhD (S’pore)
Meibomian gland dysfunction (MGD) is a
common occurrence in the Asia-Pacific region, yet many patients are unaware of its importance and prevalence. MGD disrupts the tear film and is likely a leading cause of evaporative dry eye.1,2 A major issue for clinicians is educating the patient about MGD. Patients at our clinic may not know what the meibomian gland is, what it does or why its health is important to their overall vision.
Symptoms
In MGD, patients present with numerous ocular surface complaints, including ocular itching or burning, watery/teary eyes, “crusty” eyelids upon waking and ocular redness. It is interesting to note that some of these same symptoms are present and are a primary complaint in patients with dry eye.
Further complicating matters is that clinically significant MGD can occur with or without anterior blepharitis or aqueous-deficient dry eye, which makes diagnosis especially difficult.
Prevalence Rates
MGD prevalence rates are consistently reported higher in the Asian population when compared with rates of their Western counterparts. A 56.3% age-standardized prevalence was found in a large cohort of urban Malay residents in Singapore.3 That same group of patients had almost a 40% prevalence rate when MGD was present with dry eye. Other groups in Asia have found similar rates of MGD in China and Beijing.2 Conversely, prevalence rates in the West are generally less than 20%.2
Those cohort studies are not ideal, however, because they only reported the number of people with MGD who had concurrent dry eye. Unless it is determined how many people in the population do not have dry eye but do have MGD, the odds of those with MGD also having dry eyes cannot be confirmed.
Further complicating diagno-sis is there is not an ideal test to diagnose dry eye; it is impossible to conclude that those patients without symptoms of dry eye do not have dry eye. Some researchers have shown that the force of the blink may correlate with lipid production and the ability to express lipids into tears.4
Factors Influencing MGD
There are numerous factors that could influence the higher rates reported in Asia-Pacific. At the Singapore National Eye Centre, many patients have neglected the hygiene of their lids. For example, these patients present with irritated eyelids and extremely clogged glands. This is a typical presentation especially with older patients. Without good lid hygiene, patients may be at increased risk for Demodex infestations. Anti-acne treatments have also been associated as a risk factor for MGD.
There may be some
Meibomian Gland Dysfunction and Ocular Irritation
“ Without good lid
hygiene, patients
may be at increased
risk for Demodex
infestations.” – Dr. Louis MG Tong
About the Author
Cover Story
OCULAR SURFACE REVIEW
5

6
OCULAR SURFACE REVIEW
genetic factors underlying lid inflammatory diseases but these are not well understood.5 For example, patients could be predisposed to MGD by risk factors, such as inconsistency of outflow of the secretions in the tear, decreased tear secretion or inspissation of the meibomian glands. Similarly, Shimizaki et al6 found a significantly higher rate of MGD in those with Sjögren’s syndrome (38.9%) than in dry eye patients without Sjögren’s (11.1%).
Another potentially confound-ing factor observed at our clinic is the postoperative glaucoma patient who has been taking drops for more than a year. Almost all of these eyes have some kind of epitheliopathy and dry eye, but they also seem to have debilitating MGD. At our clinic, studies are being conducted to investigate if MGD is a preexisting condition in these patients or if MGD occurs during the postoperative period because patients ignore proper care. Other
References 1. Nichols KK, Foulks GN, Bron AJ, et
al. International Workshop on Mei-bomian Gland Dysfunction: executive summary. Invest Ophthalmol Vis Sci. 2011;52(4):1922-1929.
2. Schaumberg DA, Nichols JJ, Papas EB, Tong L, Uchino M, Nichols KK.. The International Workshop on Meibomian Gland Dysfunction: Report of the Sub-committee on the Epidemiology of, and Associated Risk Factors for, MGD. Invest Ophthalmol Vis Sci. 2011;52(4):1994-2005.
3. Siak JJ, Tong L, Wong WL, et al. Preva-lence and risk factors of meibomian gland dysfunction: the Singapore Malay Eye Study. Presented at: Association for Research in Vision and Ophthalmology; Ft. Lauderdale, Fla.: May 3, 2010.
4. Personal correspondence from Don Korb, MD.
5. Vehof J, Kozareva D, Hysi PG, Ham-mond CJ. Heritability of dry eye disease. Presented at: Association for Research in Vision and Ophthalmology; Ft. Lauderdale, Fla.: May 7, 2012.
6. Shimazaki J, Goto E, Ono M, Shim-mura S, Tsubota K. Meibomian gland dysfunction in patients with Sjogren syndrome. Ophthalmology. 1998;105(8):1485-1488.
7. Viso E, Gude F, Rodriguez-Ares MT. The association of meibomian gland dys-function and other common ocular dis-eases with dry eye: a population-based study in Spain. Cornea. 2011;30(1):1-6.
Images courtesy of Dr. Louis MG Tong
About the AuthorDr. Louis MG Tong, MBBS(S’pore), FRCS(Edin), DM(Nott), PhD(S’pore), is Consultant and Clinician Scientist, Cornea and External Eye Disease Service, Singapore National Eye Centre; Assistant Director (Training and Education) and Head, Ocular Wound Healing and Therapeutics Laboratory, Singapore Eye Research Institute; and Adjunct Associate Professor, Duke-National University of Singapore, Graduate Medical School and Yong Loo Lin School of Medicine, National University of Singapore
population-based reports also have noted a relationship between glaucoma and dry eye.7
Treatment Options
Various treatments exist for MGD. For a mite infection, some clinicians use tea tree oil to clean the eyelids. Heating technologies also can treat the eyelid. Most heating techniques – such as using warm compresses – can be performed by the patient and do not necessitate a visit to the ophthalmologist.
Some physicians prescribe doxycycline or azithromycin, while others advocate probing the gland. The latter is a time-consuming and invasive treatment whereby, after administration of a local anesthesia, the clinician expresses each gland. Potential preventive measures may include prescribing oral omega-3 fatty acids.
At our clinic, we do not distinguish between dry eye and MGD for the purpose of treatment, because evaporative dry eye is extremely common. Therefore, dry eye and MGD usually are treated together. Meanwhile, the
recent International Workshop on Meibomian Gland Dysfunction, which involved more than 50 experts worldwide, resulted in an evidence-based approach to management of MGD. See Figure 1 on page 7.
Future Considerations
The meibomian glands play a role in the maintenance of the ocular surface system, and disrupting the balance will lead to one or more ocular surface diseases. Increased awareness of the dysfunction, early diagnosis and approaches to treatment are the best paradigm for patients.
An example of lid margin telangiectasia, one of the abnormalities used to evaluate MGD. This patient also underwent eyelid surgery
A typical example of blocked glands
Cover Story

7
OCULAR SURFACE REVIEW
STAGE CLINICAL DESCRIPTION TREATMENT
STAGE 1
No symptoms of ocular discomfort, itching or photophobia
Clinical signs of MGD based on gland expressionMinimally altered secretions: Grade ≥2 – <4Expressibility: 1
No ocular surface staining
Inform patient about MGD, the potential impact of diet and the effect of work/ home environments on tear evaporation, and the possible drying effect of certain systemic medications
Consider eyelid hygiene including warming/ expression as described below (±)
STAGE 2
Minimal to mild symptoms of ocular discomfort, itching or photophobia
Minimal to mild MGD clinical signsScattered lid margin featuresMildly altered secretions: Grade ≥4 – <8Expressibility: 1
None to limited ocular surface staining[DEWS grade 0–7; Oxford grade 0–3]
Advise patient on improving ambient humidity; optimizing workstations and increasing dietary omega-3 fatty acid intake (±)
Institute eyelid hygiene with eyelid warming (a minimum of four minutes, once or twice daily) followed by moderate to firm massage and expression of MG secretions (+)
All the above, plus (±)
Artificial lubricants (for frequent use, non-preserved preferred)Topical emollient lubricant or liposomal sprayTopical azithromycinConsider oral tetracycline derivatives
STAGE 3
Moderate symptoms of ocular discomfort, itching or photophobia with limitations of activities
Moderate MGD clinical signsh lid margin features: plugging, vascularityModerately altered secretions: Grade >8 – <13Expressibility: 2
Mild to moderate conjunctival and peripheral corneal staining, often inferior [DEWS grade 8–23; Oxford grade 4–10]
All the above, plus
Oral tetracycline derivatives (+)Lubricant ointment at bedtime (±)Anti-inflammatory therapy for dry eye as indicated (±)
STAGE 4
Marked symptoms of ocular discomfort, itching or photophobia with definite limitations of activities
Severe MGD clinical signsh lid margin features: dropout, displacementSeverely altered secretions: Grade ≥13Expressibility: 3
Increased conjunctival and corneal staining, including central staining [DEWS grade 24–33; Oxford grade 11–15]
h Signs of inflammation: e.g. ≥ moderate conjunctival hyperemia, phlyctenules
All the above, plus
Anti-inflammatory therapy for dry eye (+)
Key:
Meibum quality is assessed in each of 8 glands of the central third of the lower lid on a 0–3 scale for each gland: 0=clear meibum; 1=cloudy meibum; 2=cloudy with debris (granular); 3=thick, like toothpaste [range 0–24].
Expressibility of meibum is assessed from 5 glands: 0=all glands expressible; 1=3–4 glands expressible; 2=1–2 glands expressible; 3=no glands expressible. This can be assessed in the lower or upper lid.
Numerical staining scores refer to a summed score of staining of the exposed cornea and conjunctiva. The Oxford scheme has a scale range of 0–15 and the DEWS scale has a scale range of 0–33.
Figure 1
This chart details an evidence-based approach to MGD management. It was originally published (and data is reproduced here) in order to highlight findings of the recent International Workshop on Meibomian Gland Dysfunction (www.TearFilm.org). According to the Tear Film & Ocular Surface Society: “At each treatment level [in the chart], lack of response to therapy advances treatment to the next level. A [±] sign means that the evidence to support the use of the treatment at that level is limited or emerging, thus use should be based on clinical judgment. A [+] sign indicates the treatment is supported by the evidence at that stage of disease. The quality of expressed meibum and meibum expressibility are key features in the clinical assessment of MGD.”
Cover Story

8
OCULAR SURFACE REVIEW
By Victor L. Caparas, MD, MPH
Allergies are on the rise not just in the Asia-Pacific region but
all over the world. In Europe, the European Community Respiratory Health Survey (ECRHS) had reported a “continuous increase in sensitivity to common allergens among people born in each decade from the 1940s to the 1970s.”1 The International Study of Asthma and Allergies in Childhood (ISAAC) found a pattern of increasing prevalence worldwide, with a survey of 66 centers in 37 countries revealing that more centers had increases than decreases in prevalence after a mean of seven years between Phases One and Three of the study.2
This is not to downplay the significance of allergies and related conditions in the Asia-Pacific region. As the 2011 Global Asthma Report indicates, such conditions are not only increasing in prevalence but also tend to be more severe in low- to middle-income countries,3 many of which are found in the Asia-Pacific region.
‘Allergic rhinoconjunctivitis’
The rate of allergies, however, is difficult to quantify in the Asia-Pacific region. Few studies focus on the prevalence of allergies in the region. The number of studies dwindles further when we speak specifically of allergic conjunctivitis, a condition that appears to be generally associated with other conditions.
These studies tend to conflate these conditions into “allergic rhinoconjunctivitis.”
But here we begin to find some data to work with: ISAAC puts the prevalence of allergic rhinoconjunctivitis in the region within the range of 5% to 20% in the 6- to 7- and 13- to 14-year age groups.4 ISAAC has approximated the prevalence of allergic rhinoconjunctivitis at 5% in Indonesia, 7% in China and India and 15% in Singapore – this is compared with approximately 20% in Australia, the United Kingdom and the United States.5
Hypotheses
Several theories have attempted to explain the trend of increasing allergy worldwide. These theories were created from studies that associate allergies with free radicals and oxidative stress6, and CO2 and global warming as they affect pollen release.7 Allergies have also been associated with pollution, with studies demonstrating an increased IgE
response on exposure to vehicle exhaust8 and diesel particulate matter.9,10
Other studies further describe the ways pollutants may affect allergic disease. Pollutants have been found to modify antigen presentation.12 Airborn particles have been found to affect the allergenicity of pollen grains by altering their morphology, causing protein release and inducing protein changes while increasing total IgE production and blood eosinophil count.13
Hypotheses linking allergies to pollution seem particularly revelatory in light of one study conducted in Mongolia in 2005. In that study, allergic rhinoconjunctivitis progressively increased in prevalence as the researchers went from village (9.3%) to town (12.9%) to city (18.4%).14 The Mongolian study can be archetypal of the state of allergic conjunctivitis in the industrialized countries of the Asia-Pacific region – a region that, in addition, periodically experiences large-scale, air-quality disasters caused by forest fires.15
Meeting the Rise
The hallmark of allergic conjunctivitis is itchiness. Some will say that if there is no itchiness, it is not allergy. Other symptoms include inflammation, chemosis, stringy mucoid eye discharge, tearing, photophobia and foreign body sensation.
Allergy must be mediated by IgE, which results in the
Allergic Conjunctivitis is Increasing Globally
OCULAR SURFACE REVIEW

9
OCULAR SURFACE REVIEW
degranulation of mast cells and the release of histamine and inflammatory factors and vasoactive proteins. Here then is our repertoire of pharmaceutical agents to treat allergic conjunctivitis: antihistamines; mast cell stabilizers; and corticosteroids.
The clinician should aim for quick relief of symptoms, choosing a fast-acting agent calibrated to the severity of the episode, later tapered with cessation of symptoms. Antihistamines (eg, pheniramine, antazoline, emedastine) might be enough for occasional acute attacks. However, treatment also should include a plan to decrease further histamine and chemokine release, such as with mast cell stabilizers (eg, cromolyn sodium, pemirolast, lodoxamide).
The regimen will depend on the type of allergic conjunctivi-tis being treated. For perennial or seasonal allergic conjunctivi-tis (PAC/SAC), the regimen can include artificial tears (eg, hy-promellose, carboxymethylcel-lulose, polyethelene glycol), a mast cell stabilizer-antihistamine combination (eg, olopatadine, ketotifen, epinastine), and corti-costeroids (eg, fluorometholone, prednisolone, dexamethasone) in severe cases, shifting to a mast cell stabilizer if the condition is prolonged.
Cases of vernal keratocon-junctivitis (VKC) may be treated with a regimen, which includes artificial tears, corticosteroids for acute episodes and pulsed for exacerbations, concomitant with a mast cell stabilizer-antihista-mine combination. This regimen can be shifted to a mast cell sta-bilizer, if the case is prolonged. Additionally a topical cyclospo-rine can be used for refractive cases.
References
1. Global Asthma Report 2011. Paris, France: The International Union against Tuberculosis and Lung Disease. 2011:15.
2. Asher MI, Montefort S, Bjorksten B, et al, and the ISAAC Phase Three Study Group. Worldwide time trends in prevalence of symptoms of asth-ma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicoun-try cross-sectional surveys. Lancet. 2006;368(9537):733-743.
3. Global Asthma Report 2011. Paris, France: The International Union Against Tuberculosis and Lung Disease. 2011;10.
4. Garcia-Marcos L. Mapa Global de la prevalencia de Rinoconjuntivitis en niños (World-Wide Map of the Preva-lence of Rinoconjunctivitis in Children). ISAAC Symposium - Merida 2009. University of Yucatan, 28 Nov 2009. Lecture.
5. Strachan D, Sibbald B, Weiland S, et al. World-wide variations in prevalence of symptoms of allergic rhinoconjunctivi-tis in children: the International Study of Asthma and Allergies in Childhood (ISAAC). Pediatr Allergy Immunol. 1997;8(4):161-176.
6. Murr C, Schroecksnadel K, Winkler C, et al. Antioxidants may increase the probability of developing allergic disease and asthma. Med Hypotheses. 2005;64(5):973-977.
7. Ziska LH, Gebhard DE, Frenz DA, et al. Cities as harbingers of climate change: common ragweed, urbanization, and public health. J Allergy Clin Immunol. 2003;111(2):290-295.
About the AuthorDr. Victor L. Caparas, MD, MPH, is a Cataract, Cornea and Anterior Segment Specialist, Mandaluyong City, Philippines.
Atopic keratoconjunctivitis (AKC) may be treated with a regimen similar to that for VKC, with systemic immunotherapy for dermatitis.
The treatment of giant papillary conjunctivitis (GPC) includes artificial tears, cessation of contact lens use, and pulsed corticosteroids with concomitant mast cell stabilizer-antihistamine combination.
In addition, physicians need to see beyond medication in treating their allergic patients. Avoidance of allergens is key to a patient’s continued well-
being, but advice for controlling one’s physical environment is rarely touched on by doctors. Without this avoidance or at least minimization of exposure, patients suffer repeated episodes, which result in their graduation to stronger medications.
8. Riedl M, Diaz-Sanchez D. Biology of diesel exhaust effects on respira-tory function. J Allergy Clin Immunol. 2005;115(2):221-228.
9. Heo Y, Saxon A, Hankinson O. Effect of diesel exhaust particles and their components on the allergen-specific IgE and IgG1 response in mice. Toxicology. 2001;159(3):143-158.
10. Rusznak C, Devalia JL, Davies RJ. The impact of pollution on allergic disease. Allergy. 1994;49(18 Suppl):21-27.
11. Saxon A, Diaz-Sanchez D. Air pollution and allergy: you are what you breathe. Nat Immunol. 2005;6(3):223-226.
12. Takizawa H. Diesel exhaust particles and their effect on induced cytokine ex-pression in human bronchial epithelial cells. Curr Opin Allergy Clin Immunol. 2004;4(5):355-359.
13. Majd A, Chehregani A, Moin M, et al. The effects of air pollution on structures, proteins and allergenic-ity of pollen grains. Aerobiologia. 2004;20(2):111-118.
14. Viinanen A, Munhbayarlah S, Zevgee T, et al. Prevalence of asthma, al-lergic rhinoconjunctivitis and allergic sensitization in Mongolia. Allergy. 2005;60(11):1370-1377.
15. Wong-Anan N. Q+A – Why has South-east Asia’s Haze Returned? Reuters. Oct. 22, 2010. www.reuters.com. Ac-cessed Sept. 22, 2011.

10
OCULAR SURFACE REVIEW
By Kazuo Tsubota, MD, PhD
The Japanese Dry Eye Research Society developed
a dry eye diagnostic criteria in 1995 that differed from the U.S. and European classifications in that it included patients without symptoms.1 Since the criteria were published, numerous advances have been introduced in the diagnostics used to evaluate dry eye and in the medications used to treat the disease. The new definition, therefore, described dry eye as “a chronic disease of the cornea, conjunctiva and tears caused by various factors and associated with ocular discomfort and visual disturbance.” 2 A recent study3 evaluated the differences in the number of patients diagnosed with definite dry eye (DDE) or probable dry eye (PDE) using the old and new criteria.
It is important to recognize the number of dry eye patients in Japan is still large and prevalent in the elderly.4 In our comparative study,3 fewer patients were diagnosed with DDE or PDE under the new criteria.
The criteria state that patients without fluorescein or Rose Bengal staining would fall into the PDE classification rather than DDE, even with a short break-up time (BUT) of 5 seconds or less.
However, we also found those with short BUT-type dry eye seem to be very symptomatic and complain of severe problems. A prospective study to evaluate the discrepancy between the
References:
1. Shimazaki J. Definition and diagnosis of dry eye 1995. Ganka. 1995;37:765-770 (in Japanese).
2. Shimazaki J. Definition and diagnosis of dry eye 2006. Atarashii ganka. 2007;24:181-184 (in Japanese).
3. Uchino Y, Uchino M, Dogru M, Ward S, Yokoi N, Tsubota K. Changes in dry eye diagnostic status following implementation of revised Japanese dry eye diagnostic criteria. Jpn J Ophthalmol. DOI 10.1007/s10384-011-0099-y. Published online 15 Nov 2011.
4. Uchino M, Dogru M, Yagi Y, et al. The features of dry eye disease in a Japanese elderly population. Optom Vis Sci. 2006;83(11):797-802.
Changing Dry Eye DiagnosesComparing the new and old diagnostic criteria will yield more potential dry eye patients than confirmed.
About the AuthorDr. Kazuo Tsubota, MD, PhD, is Professor and Department Chair, Keio University School of Medicine in Tokyo, Japan.
“ In Japan, newer treatments, such as diquafosol sodium or rebamipide, are being used to stabilize the tear film rather than suppress inflammation. These types of treatments may provide additional insight on the mechanisms of dry eye for researchers and clinicians.” – Dr. Kazuo Tsubota
classification and the reported symptom(s) is necessary.
In Japan, newer treatments, such as diquafosol sodium or rebamipide, are being used to stabilize the tear film rather than suppress inflammation. These types of treatments may provide additional insight on the mechanisms of dry eye for researchers and clinicians.
Improving our ability to quantify a patient’s disease based on clinical signs and subjective symptoms will continue to help Japanese clinicians tailor appropriate treatments.
OCULAR SURFACE REVIEW

11
OCULAR SURFACE REVIEW
Demystifying Anti-inflammatory Therapy for Dry Eye Diseases
By Samar K. Basak, MBBS, MD, DNB, FRCS
Evidence has established the role of inflammation
in the pathogenesis of dry eye diseases.1-5 The focus of this article is to present a clinical perspective to available evidence, which may have a promising role for anti-inflammatory agents in the treatment of dry eye disease.
Cyclosporine A
Cyclosporine A, a US FDA-approved agent for treating dry eye disease, is an immune modulator, which decreases T-cell mediated inflam-matory cytokines.6,7 Cyclosporine A blocks molecular pathways that contribute to T-cell activation and may decrease apoptosis of conjunctival epithelium.7,8 Results of a study by Sall et al indicated that CsA (0.05% or 0.1%) significantly improved corneal staining and categorized Schirmer values (P < 0.05).9 Furthermore, CsA (0.05%) significantly improved subjective
Summary of Anti-inflammatory Therapy
• Artificial tears and surgical options, such as punctal occlusion devices, have been mainstays of dry eye treatment.4
• Recently, “inflammatory changes” have emerged as contributors to the pathogenesis of dry eye diseases.1,3
• Availability of effective anti-inflammatory options, such as cyclosporine A, corticosteroids and omega-3 fatty acids, have expanded the treatment landscape of dry eye diseases beyond treatment with artificial tears.1,5,9,13,14,16-18
• Although anti-inflammatory options may not be required for milder symptoms, they are effective options for moderate to severe dry eye diseases.9
• Cyclosporine A and corticosteroids are mainstay pharmacotherapeutic options for alleviating the inflammatory components of dry eye diseases.1,2,5,12-15
• Corticosteroids eye drops have limitations, such as rise in IOP, secondary glaucoma, cataract, delayed epithelial healing and risk of microbial keratitis.13
• While using anti-inflammatory options for treatment of dry eye diseases adequate care must be taken in terms of:• Long-term safety and• Improve compliance.11,13
• Surgical interventions, such as punctal occlusion, may be reserved for dry eye diseases that do not respond to anti-inflammatory pharmacotherapy.4
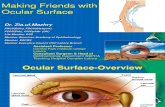
(1) Epithelial defect; (2) Epithelial defect after fluorescein staining; (3) Persistent epithelial defect in keratoplasty; (4) Rose Bengal staining in keratoconjunctivitis sicca; (5) Typical Rose Bengal staining in dry eye syndrome; (6) Lower tear meniscus height and Fluorescein staining of the cornea in dry eye
(1)
(4)
(2)
(5)
(3)
(6)
OCULAR SURFACE REVIEW

12
OCULAR SURFACE REVIEW
References
1. Brignole F, Pisella PJ, Goldschild M, et al. Flow cytometric analysis of inflammatory markers in conjunctival epithelial cells of patients with dry eyes. Invest Ophthalmol Vis Sci. 2000; 41(6):1356-1363.
2. Brignole F, Pisella PJ, De Saint Jean M, Goldschild M, Goquel A, Baudouin C. Flow cytometric analysis of inflamma-tory markers in KCS: 6-month treat-ment with topical cyclosporin A. Invest Ophthalmol Vis Sci. 2001;42(1):90-95.
3. Stern ME, Gao J, Schwalb TA, et al. Conjunctival T-cell subpopulations in Sjögren’s and non-Sjögren’s patients with dry eye. Invest Ophthalmol Vis Sci. 2002;43(8):2609-2614.
4. O’Brien PD, Collum LM. Dry eye: diag-nosis and current treatment strategies. Allergy Asthma Rep. 2004; 4(4):314-319.
5. McCabe E, Narayanan S. Advance-ments in anti-inflammatory therapy for dry eye syndrome. Optometry. 2009;80(10):555-566.
6. Drug Name: Restasis (cyclosporine oph-thalmic emulsion). Available at www.centerwatch.com. Accessed Oct 2011.
7. Matsuda S, Koyasu S. Mechanisms of action of cyclosporine. Immunophar-macology. 2000;47(2-3):119-125.
8. Gao J, Schwalb TA, Addeo JV, Ghosn CR, Stern ME. The role of apopto-sis in the pathogenesis of canine keratoconjunctivitis sicca: the effect of topical cyclosporin A therapy. Cornea. 1998;17(6):654-663.
9. Sall K, Stevenson OD, Mundorf TK, Reis BL. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease. CsA Phase 3 Study Group. Ophthalmol-ogy. 2000;107(4):631-639.
10. Pflugfelder SC, De Paiva CS, Villarreal AL, Stern ME. Effects of sequential artificial tear and cyclosporine emul-sion therapy on conjunctival goblet cell density and transforming growth factor-beta2 production. Cornea. 2008;27(1):64-69.
About the AuthorDr. Samar K. Basak is the Director & Head of the Department, Cornea and External Eye Diseases, Disha Eye Hospitals, Barrackpore, Kolkata, India.
11. Trattler W, Katsev D, Kerney D. Self-reported compliance with topical cyclo-sporine emulsion 0.05% and onset of the effects of increased tear production as assessed through patient surveys. Clin Ther. 2006; 28(11):1848-1856.
12. De Paiva CS, Corrales RM, Villarreal AL, et al. Corticosteroid and doxycycline suppress MMP-9 and inflammatory cytokine expression, MAPK activation in the corneal epithelium in experimental dry eye. Exp Eye Res. 2006;83(3):526-535.
13. Marsh P, Pflugfelder SC. Topical nonpreserved methylprednisolone therapy for keratoconjunctivitis sicca in Sjögren syndrome. Ophthalmology. 1999;106(4):811-816.
14. Pflugfelder SC, Maskin SL, Anderson B, et al. A randomized, double-masked, placebo-controlled, multicenter comparison of loteprednol etabonate ophthalmic suspension, 0.5%, and placebo for treatment of keratocon-junctivitissicca in patients with delayed tear clearance. Am J Ophthalmol. 2004;138(3):444-457.
15. Avunduk AM, Avunduk MC, Varnell ED, Kaufman HE. The comparison of efficacies of topical corticosteroids and nonsteroidal anti-inflammatory drops on dry eye patients: a clinical and immunocytochemical study. Am J Ophthalmol. 2003;136(4):593-602.
16. Miljanovic B, Trivedi KA, Dana MR, Gilbard JP, Buring JE, Schaumberg DA. Relation between dietary n-3 and n-6 fatty acids and clinically diagnosed dry eye syndrome in women. Am J Clin Nutr. 2005;82(4):887–893.
17. Brignole-Baudouin F, Baudouin C, Aragona P, et al. A multicentre, double-masked, randomized, controlled trial assessing the effect of oral supple-mentation of omega-3 and omega-6 fatty acids on a conjunctival inflamma-tory marker in dry eye patients. Acta Ophthalmol. 11 August 2011. doi: 10.1111/j.1755-3768.2011.02196.x.
18. Roncone M, Bartlett H, Eperjesi F. Es-sential fatty acids for dry eye: a review. Cont Lens Anterior Eye. 2010; 33(2):49-54.
measures, such as blurred vision. (P < 0.05).10 The most common adverse reactions following CsA are burning and stinging sensation upon instillation.9
Additionally, pharmacologic treatments for dry eye must effectively encompass treatment
adherence. Results of a survey from Trattler et al indicated that compliance was associated with higher rates of satisfaction, as compared with those who missed half or more of the prescribed dose.11
Corticosteroids
Dry eye symptoms, are associ-ated with increased concentra-tions of the pro-inflammatory cytokine IL-1 and enhanced ma-trix metalloproteinase-9 (MMP-9) activity.12 Several studies have reported that topical corticoste-roids, such as freshly prepared methylprednisolone, loteprednol etabonate and fluorometholone, significantly improved subjective and objective Schirmer scores in patients with moderate to severe dry eye diseases.13-15
Nevertheless, concerns of steroid-induced secondary glau-coma, for example, warrant ade-quate clinical consideration and monitoring.5 Furthermore, cor-ticosteroid therapy may not be justified in patients with milder dry eye symptoms.
Omega-3 Fatty Acids
Following anecdotal reports that indicated a role of omega-3 fat-ty acid supplementation in the treatment of dry eye disease, Miljanovi´c et al confirmed the association between the dietary intake of omega-3 fatty acids and the occurrence of dry eye disease.16 Omega-3 fatty acids block the gene transcription of pro-inflammatory cytokines TNF-alpha, IL-1a, and IL-1b.17,18
Conclusions
Identifying effective anti-inflammatory options may be crucial for addressing the causative factors of dry eye diseases. Available evidence indicates that cyclosporine A, corticosteroids and omega-3 fatty acids are effective pharmacotherapeutic choices.
ASIA/0038/2012