
October 2001 Volume 14 #1 - augcominc.com · 1 October 2001 Volume 13, #6 Volume 14 #1 Clinical...
16
1 October 2001 Volume 13, #6 Volume 14 #1 Clinical News Assessment protocol for SGDs Governmental Funding process for SGDs Equipment Medicare reimbursement for SGDs Case Example #1 Person with dysarthria Amyotrophic lateral sclerosis (ALS) Case Example #2 Person with dysarthria Developmental disability (DD) Case Example #3 Person with apraxia/aphasia Cerebral vascular accident (CVA) AAC-RERC State of the Science Conference on Communication Enhancement Continued on page 2 Assessment protocol for SGDs Medicare has renamed AAC devices Speech Generating Devices (SGDs), agreed to fund them and given the responsibility for recommending SGDs to ASHA certified speech- language pathologists (SLPs). SLPs rely on multi-faceted approaches to the SGD assessment process. Their strategies often include a review of medical records; interviews with the individual, caregivers and others; structured observations; formal assessments and equipment trials. Through a series of clinical decisions, SLPs ultimately make specific recommendations for an SGD and accessories. This process has not changed. However, Medicare funding requires a standardized report which covers specific areas, as discussed below. 1. Demographics. SLPs collect and report basic information about the beneficiary: • Beneficiary’s name, Medicare number, Date of birth, Primary medical diagnosis, Date of onset of disease/ condition, Communication diagnoses. Small groups of people, focused on a clear objective, can make a difference. In the fall of 1999, I reported on the (ultimately success- ful) effort by a working group of AAC professionals to convince Medicare, the largest health care program in the United States, to retreat from its decade-old policy of considering AAC devices merely as “convenience items,” which were not eligible for funding. 1 On January 1, 2001 Medicare finally agreed that AAC devices are “durable medical equipment,” named them Speech Generating Devices, or SGDs, and agreed to fund them. Now, as a secondary, but perhaps equally important product of Medicare’s momentous decision to fund AAC devices, we are witness- ing a sea change in the way in which speech-language pathologists (SLPs) in the United States must report the process of assessing an individual’s need for an SGD (i.e., AAC device). Medicare has decreed a new assessment protocol, which inevitably is becoming the de facto standard for AAC device assessment reports by other public and private insurers, as well. Once again, a small group of AAC advocates, clinicians, educa- tors, consumers, family members and researchers (contributing countless volunteer hours) worked together to develop an assessment protocol that was reviewed by 13 professional/consumer organizations (including the ALSA, AMA, ANA, ASHA, ISAAC, UCPA and USSAAC) and was then adopted by Medicare with no substantial changes. Other AAC device funders also are adopting the protocol. This series of events, while imposing a necessarily greater degree of uniformity on the AAC assessment process in the United States, has produced a validated and useful protocol that may very well provide SLPs in other countries and those who work with other popula- tions with useful guidance. Most of this newsletter describes aspects of the new SGD protocol. Clinical News describes the man- dated Medicare assessment process. Governmental summarizes the Medicare funding process; and Continued on page 2
-
Upload
truonglien -
Category
Documents
-
view
213 -
download
0
Transcript of October 2001 Volume 14 #1 - augcominc.com · 1 October 2001 Volume 13, #6 Volume 14 #1 Clinical...

1
October 2001
Volume 13, #6
Volume 14 #1
Clinical NewsAssessment protocol for SGDs
GovernmentalFunding process for SGDs
EquipmentMedicare reimbursement for SGDs
Case Example #1Person with dysarthriaAmyotrophic lateral sclerosis (ALS)
Case Example #2Person with dysarthriaDevelopmental disability (DD)
Case Example #3Person with apraxia/aphasiaCerebral vascular accident (CVA)
AAC-RERCState of the Science Conference onCommunication Enhancement
Continued on page 2
Assessment protocolfor SGDs
Medicare has renamed AAC devicesSpeech Generating Devices (SGDs),agreed to fund them and given theresponsibility for recommendingSGDs to ASHA certified speech-language pathologists (SLPs).
SLPs rely on multi-facetedapproaches to the SGD assessmentprocess. Their strategies ofteninclude a review of medical records;interviews with the individual,caregivers and others; structured
observations; formalassessments andequipment trials.Through a series of
clinical decisions, SLPsultimately make specific
recommendations for an SGD andaccessories. This process has notchanged. However, Medicarefunding requires a standardizedreport which covers specific areas,as discussed below.1. Demographics. SLPs collect andreport basic information about thebeneficiary:
• Beneficiary’s name, Medicarenumber, Date of birth, Primary medicaldiagnosis, Date of onset of disease/condition, Communication diagnoses.
Small groups of people, focused ona clear objective, can make adifference. In the fall of 1999, Ireported on the (ultimately success-ful) effort by a working group ofAAC professionals to convinceMedicare, the largest health careprogram in the United States, toretreat from its decade-old policy ofconsidering AAC devices merely as“convenience items,” which werenot eligible for funding.1 On January1, 2001 Medicare finally agreed thatAAC devices are “durable medicalequipment,” named them SpeechGenerating Devices, or SGDs, andagreed to fund them.
Now, as a secondary, but perhapsequally important product ofMedicare’s momentous decision tofund AAC devices, we are witness-ing a sea change in the way in whichspeech-language pathologists(SLPs) in the United States mustreport the process of assessing anindividual’s need for an SGD (i.e.,AAC device). Medicare has decreeda new assessment protocol, whichinevitably is becoming the de factostandard for AAC device assessmentreports by other public and privateinsurers, as well.
Once again, a small group ofAAC advocates, clinicians, educa-tors, consumers, family membersand researchers (contributingcountless volunteer hours) workedtogether to develop an assessmentprotocol that was reviewed by 13professional/consumer organizations
(including the ALSA,AMA, ANA, ASHA,ISAAC, UCPA andUSSAAC) and was thenadopted by Medicare
with no substantial changes.Other AAC device funders also areadopting the protocol.
This series of events, whileimposing a necessarily greaterdegree of uniformity on the AACassessment process in the UnitedStates, has produced a validated anduseful protocol that may very wellprovide SLPs in other countries andthose who work with other popula-tions with useful guidance.
Most of this newsletter describesaspects of the new SGD protocol.Clinical News describes the man-dated Medicare assessment process.Governmental summarizes theMedicare funding process; and
Continued on page 2

2
Upfront, Continued from page 1
[Note: ICD-9 codes for both medicaland communication diagnoses areincluded.2]
• Date(s) of SLP’s assessment.
• Contact information for the: Benefi-ciary (address, phone number);Physician (name, address, phonenumber, provider number); SLP (name,address, phone number; licensenumber); Primary support person(name, address, phone number).
2. Current communication impair-ment. SLPs assess the type andseverity of the individual’s speech/expressive communication impair-ment and the expected course of thedisease/condition.
a. Impairment type and severity.SLPs describe the person’s speechimpairment as:
• Dysarthria (often includes currentspeaking rate and intelligibilitymeasures)
• Aphasia (often includes scores onreceptive and expressive aphasia testsover time)
• Dyspraxia/apraxia (often focuses on
motor planning/execution scores onapraxia tests over time)
• Aphonia – Delineates the reasons forthe person’s inability to produce voicenaturally or to use a speech prosthesis(e.g., speaking valve, electrolarynx).[Note: In order to qualify for an SGD,aphonia must be due to a physicaldisability.]
b. Anticipated course of impair-ment. SLPs determine whether thespeech impairment is likely toimprove, deteriorate or remain stableover time. Table I illustrates StagingScales that can help document thecourse of the speech impairment.Figure 1 gives three examples ofstatements written about currentstatus and expected course.3. Comprehensive assessment.SLPs describe the person’s sensory,motor, language and cognitive statusand how these factors will likelyinfluence the person’s use of anSGD. This information often can beobtained from the existing medicalrecord and confirmed through theassessment process. SLPs with themost experience find few standard-
ized tests useful in determining howeffectively a person will use an SGDand SGD accessories.
a. Hearing status. SLPs reviewthe existing record and inquire aboutthe person’s hearing status. Consid-eration is given to:
• hearing acuity (along a continuumfrom normal hearing to deafness);
• any specifics regarding localization,understanding of natural speech ormachine-generated speech;
• hearing status of primary communica-tion partners, if relevant.
If an SGD is being recommended, the SLPreports, “[The person] possesses the hearingabilities to communicate effectively using anSGD.”
b. Vision status. SLPs review theexisting record and observe theperson’s visual abilities. The follow-ing parameters are considered:
• visual status (along a continuum fromnormal vision to blindness);
• any relevant information about acuity,visual tracking, visual fields, lightingneeds, angle of view, size of symbols,contrast (color, detail) and spacing.
If an SGD is being recommended, the SLPreports, “[The person] possesses the visualabilities to communicate effectively using anSGD,” or explains why someone withoutfunctional vision may require an SGD.
c. Physical status. SLPs provideinformation about the person’smotor skills and physical ability touse an SGD and accessories bydescribing:
Figure 1. Examples of current statusand expected course statements
1. Mr. X has a severe dysarthria due tocerebral palsy. The condition is stable andspeech intelligibility is not expected toimprove.
2. Mrs. B has severe dysarthria due toamyotrophic lateral sclerosis (ALS-Stage 3).Currently speech rate is 100 wpm (half ofnormal), indicating that speech intelligibilitywill deteriorate at a rapid rate. She willrequire the use of an SGD throughout thecourse of this disease (ALS-Stages 4 and 5).
3. Mr. P has moderate receptive aphasia andsevere apraxia. The condition is now chronicand stable. Speech intelligibility is notexpected to improve.
Equipment provides informationabout AAC device categories,Medicare codes, pricing andreimbursement. To illuminate theMedicare assessment process, thisissue presents three Case Ex-amples. These cases are beingpresented by their authors in NewOrleans at the ASHA Conventionin November, 2001. Finally, AAC-RERC reports on the State of theScience Conference in AAC andhighlights the AAC-RERCwebsite, which has valuable, up-to-date information on Medicareand the assessment protocol. Manythanks to those who contributed tothis issue. They are listed on page16.
Clinical News, Continued from page 1
14 years and beyond
This year begins my 14th year asauthor of Augmentative Communica-tion News. Time sure flies when youare having fun. I wish to announcethat ACN is now officially a quar-terly publication. Issues in eachvolume will vary from 8 to 16pages. Everything else will remainthe same (except we will all keepgetting older.)
Sarah W. Blackstone, Ph.D.,CCC-SLP,Author

3
Continued on page 4
• pertinent considerations regardingmotor skills, ambulatory status,wheelchair seating, positioning andmobility, endurance levels and fatigue;
• how the person will access an SGD(e.g., direct selection, scanning);
• specifics related to switch access,mouse control, other accesories andmounting systems;
• whether changes in physical accessare likely to occur over time and willrequire accommodations.
SLPs often consult with occupa-tional therapists (OTs), physicaltherapists (PTs) and rehabilitationengineers to determine motoricrequirements for SGD use.
If an SGD is being recommended, the SLPreports, “[The person] possesses the physicalabilities to use an SGD.”
d. Language status. SLPs deter-mine the person’s language andliteracy skills as they relate to usingan SGD and accessories. The reportdocuments the person’s languagestatus using the following param-eters:
• level of linguistic impairment (noimpairment to severe languageimpairment);
• performance on any language test(e.g., Boston Diagnostic AphasiaExamination-BDAE;Western AphasiaBattery-WAB; picture description);3,4
• type and level of symbolization theindividual can use to communicate;
• level of literacy skills (ability to read,write, spell);
• level of independence in formulatingmessages using symbols, words,spelling;
• whether changes in linguistic skillsare likely to occur over time.
If an SGD is being recommended, the SLPreports specifics about language skills and howthey affect the individual’s ability to use an SGDand SGD accessories effectively to achievefunctional communication goals.
e. Cognitive status. The SLP’sassessment provides informationabout the person’s cognitive skillsand abilities as they relate to theneed for and use of a SGD and mayinclude:
• level of cognitive impairment (noimpairment to significant cognitiveimpairment);
• functional attention, memory andproblem-solving skills.
Figure 2 is an example of a state-ment regarding cognitive status.
Figure 2. Example of cognitive statusstatement
Mr. S’s attention, memory and non-verbalproblem-solving skills are within functionallimits. He sustained attention for a two-hourevaluation and recalled symbol locations anddevice operations after brief instruction. Heused an SGD to initiate interactions andengage in conversation.
If an SGD is being recommended, the SLPreports, “[The person] possesses the cognitive/linguistic abilities to effectively use an SGD toachieve functional communication goals.”
4. Daily communication needs.SLPs document the individual’s dailycommunication needs and indicatewhether those needs can be metusing speech, signs, writing and/orlow-tech communication aids.
a. Specific daily functionalcommunication needs. In assessingcommunication needs, SLPs and
other team members take intoaccount daily situations, environ-ments, partners and specific mes-sages. Figure 3 gives examples thatdocument communication needs.
Figure 3. Examples of communicationneeds
• Communicate in emergency situations.
• Direct the behavior of caregivers.
• Advocate for self.
• Communicate with family, friends, employers,community personnel, medical personnel orclergy using the phone.
• Participate in family decision-making.
• Communicate while participating in activitiesrelated to employment.
• Attend and participate in support groups or daytreatment activities.
• Report medical status and complaints. Askquestions of medical providers and respond tomedical provider’s quetions.
• Discuss choices for end-of-life care.
b. Ability to meet communicationneeds with non-SGD treatmentapproaches. SLPs assess whether abeneficiary is able to fulfill his orher daily communication needsusing natural speech or speech aids,e.g., amplifier, valve, etc.) and othernon- SGD approaches. SLPs alsoconsider why an SGD may berequired in addition to, or instead of,low-tech strategies and naturalspeech. The report indicates:
• the types of non-SGD treatments thatwere considered (e.g., speech therapy,voice amplifier) and ruled out.
• the person’s ability to use low-techstrategies and natural modes of
Table 1. Examples of Staging Scales for assessing individuals withsevere speech impairments
Yorkston, K., Beukelman, D., Strand, E., & Bell, K. (1999). Clinical Management of Motor Speech Disorders in Children and Adults. Austin, TX: Pro-Ed

4
Clinical News, Continued from page 3
communication to meet daily commu-nication needs.
• issues related to communicating withprimary partners and caregivers inspecific contexts.
If an SGD is being recommended, the SLPreports, “[The person’s] daily communicationneeds cannot be met using natural communica-tion methods or low-tech/no-tech AACtechniques because of (bespecific).”
5. Functional communicationgoals. An important component ofthe assessment process is establish-ing functional treatment goals.Medicare guidance states thatfunctional goals for SLP treatmentshould be designed to achieve“optimum communication indepen-dence.” SLPs develop functionalgoals with the individual and family.Figure 4 lists examples of functionalcommunication goals.
Figure 4. Examples of functionalcommunication goals
• Within one week of receiving it, Mr. B willindependently communicate physical needs andemotional status to his wife on a daily basiswith 100% accuracy, using the recommendedSGD.
• Within 2 months, Ms. A will accurately andindependently describe her physical symptomsand ask questions when interacting with herphysician and other health care professionalswith 80% accuracy, using the recommendedSGD.
• Mrs. X will independently engage in socialexchanges on the telephone with immediatefamily (1 month) and extended family members(2 months), using the recommended SGD atleast twice daily.
• Within 4 months, Mr. Y will independentlyengage in face-to-face communicationexchanges with friends at home and in othersettings, using the recommended SGD.
• Within 6 months, Mrs. O will independentlyask questions and provide responses incommunity-based transactions (e.g., order in arestaurant) using the SGD.
If an SGD is being recommended, the SGDfunding request should list immediate, short andlong-term functional communication goals, anda timetable for completion of these goals.
6. Rationale for SGD selection.SLPs often work with OTs, PTs andrehabilitation engineers to match aperson’s needs and abilities to anappropriate SGD and accessories.
AAC teams often use SGD equip-ment (i.e., devices, software, acces-sories) to assess an individual’sability to learn and use specificdevice features, as well as to deter-mine any preferences a person mighthave for a device.
a. General features of recom-mended SGD and accessories. TableII gives examples of device featuresSLPs consider during the SGDassessment process.
• Input features: Type of access (directselection, scanning, Morse code). Howit turns on/off, etc.
• Message characteristics: Type ofsymbols and how much vocabularyperson will need. How vocabulary isorganized, stored and retrieved. Typesof rate enhancement features personwill need.
• Output features: Types of speechoutput (synthesized/digitized), displaycharacteristics (color, font size,dynamic vs. static) and feedbackmechanisms (visual, auditory (speech/sound) the person requires.
• SGD accessories: Need for mounts,switches, carrying case, protectivecovering, extra batteries, etc.
If an SGD is being recommended, the SLPreports, “[The person] will require a SGD andaccessories that have the following features toenable him/her to achieve his/her functionalcommunication goals.” (List required features)
b. Recommended Medicaredevice and accessory codes. SLPsidentify device and accessory codesthat match the features the personrequires before selecting a specificSGD. [See the Equipment sectionfor a discussion of SGD codes.]
If an SGD is being recommended, the SLPreports, “[This individual] requires an SGDfrom the ___ category (code) and SGDaccessories from the ___ and ___ categories(code) to meet his/her functional communica-tion goals.”
c. Description of the equipmentand procedures used during assess-ment process. SLPs will identify allequipment used in the assessmentprocess and the results of any devicetrials. Figure 5 gives an examplefrom an SLP report.
[Note: Medicare does not require that a trialperiod occur before a device recommendation ismade, but it does require the SLP to describeany trials in the report.]
Figure 5. Example of device trials
In addition to the XXXX, two other SGD’s wereconsidered during the assessment–-the ABCD(BBB Inc.) and the YY (a dynamic displaydevice). The ABCD was ruled out because it doesnot have a dynamic display. Ms. F. felt a dynamicdisplay was necessary so she could program andretrieve frequently needed messages. She did notwant to memorize codes or type in recurringmessages. The YY was eliminated because itdoes not have a keyboard. Ms. F is still able touse a keyboard. The XXXX offers both optionsand can accommodate her changing needs overthe course of the disease.
7. Recommended SGD andaccessories. After everyone agreeson a specific SGD and accessories,the SLP prepares a list of recom-mended equipment and a rationalefor including each item.
The report concludes, “(This individual)requires__(name/model number and companyof recommended SGD) and__ (names/modelnumber and company of all accessories) toachieve his/her functional communicationgoals.”
8. Patient/family support of SGD.SLPs determine the family/advo-cate/caregiver’s willingness tosupport the use of the recommendedSGD and accessories. The reportshould state:
The family/caregiver/advocate participated inthe assessment process and has/have agreed tosupport the recommended SGD and accessoriesand to assist the person to achieve statedfunctional communication goals.
9. Physician involvement state-ment. The SLP report also states thedate the assessment information wassent to the beneficiary’s physician torequest a prescription.
This report was forwarded to the treatingphysician (name, address, phone number) on______(date) so that (he/she) can write aprescription for the recommended SGD andaccessories.
10. Functional benefit of Upgrade.When requesting an upgrade of apreviously issued SGD, SLPsprovide information about the:
a) features or capabilities of theupgrade as compared to existingequipment,

5
Continued on page 6
b) additional daily functional commu-nication goals the patient can achievewith the upgrade as compared toexisting equipment, and
c) importance of the patient’s ability toachieve functional communicationgoals.
11. Assurance of financial inde-pendence and signature. SLPsmust write a disclaimer statementthat testifies to his/her financialindependence such as:
The speech-language pathologist performingthis evaluation is not an employee of and doesnot have a financial relationship with thesupplier of any SGD or SGD accessory.
After the assessment report isprepared, SLPs sign their name andprovide an ASHA certificationnumber and a state licensurenumber on the original report. Theoriginal is sent as part of thefunding packet to the supplier. [Seenext section.] Copies of the reportgo to the beneficiary, thebeneficiary’s physician and into theclinical record.
Table II. Assessment of features required for an SGDand SGD accessories
Funding Process forSGDs
This section describes the processfor submitting a claim to Medicarefor a speech generating device(SGD) and SGD accessories. Whensubmitting funding requests to anyagency, it is always important tofollow the guidelines and rules verycarefully. The requirements forMedicare funding are delineated intwo policy statements:
(1) Regional Medical Review Policy (RMRP-issued March 4, 2001), which describes the SLPassessment and reporting requirements tosupport a Medicare claim for an SGD, SGDsoftware and/or SGD accessories.
(2) National Coverage Decision, # 60-23 (NCD-issued November 30, 2000), which describes thescope of Medicare coverage for SGDs andaccessories.5
The funding packet
According to the RMRP, anASHA certified speech-languagepathologist (SLP) must conduct athorough assessment and prepare areport requesting specific equip-ment. The SLP then sends the report
to the beneficiary’s physician, alongwith a letter requesting that thephysician review the report andwrite a prescription for a SGD andSGD accessories.
It is advisable for the SLP tosend a “sample” prescription alongwith the report and letter. Figure 6on page 6 gives an example.
When the prescription is com-pleted, the SLP (or beneficiary)mails an original copy of the SLPreport, an original copy of thephysician’s prescription, the co-payment (or secondary/supplemen-tal insurance information) and the
supplier’s funding form to thesupplier for processing.
[Medicare requires thesupplier to have original(not faxed) signatures on all
documents.] The SLPcontacts the supplier
within one week ofmailing the documentation to makecertain it was received and allmaterials are in order.
Processing the request
After the supplier receives therequired funding materials, thefunding coordinator at the companymakes sure they are complete andadhere to all Medicare guidelines.Medicare holds the supplier respon-sible for documentation supplied bythe SLP and physician and has theright to audit the supplier at anytime to assure compliance with theirguidelines.
If necessary, the supplier willcontact the SLP to supply additionalinformation. It is important for SLPsto cooperate with the supplier inproviding requested information/modifications in a timely manner.
Once the supplier is satisfied thatthe funding materials are completeand in compliance, the SGD andaccessories are sent to the benefi-

6
ciary. Then the supplier bills Medi-care (and the secondary/supplemen-tal insurer, if applicable) for theremaining amount.
Seven easy (?) steps toSGD funding
To summarize, there are sevenstep to SGD funding:
Step #1. SLP conducts comprehensiveassessment for an SGD and SGDaccessories.
Step #2. SLP sends report to physician.
Step #3. Physician writes a prescriptionfor SGDs and SGD accessories.
Step #4. Original SLP report, originalphysician’s prescription, co-payment orsupplemental insurance informationand any required supplier forms aresent to the supplier.
Step #5. The supplier reviews and,when complete, processes the fundingrequest.
Step #6. The supplier ships the deviceand accessories to the beneficiary.
Step #7. The supplier bills Medicareand secondary/supplemental insurance(when applicable).
Governmental, Continued from page 5
Medicare reimburse-
ment for SGDs
Medicare is a cost reimbursementprogram. This means the beneficiarymust purchase or rent an item ofDurable Medicare Equipment(DME) before a Medicare claim canbe submitted. [Note: SGDs and accesso-
ries are considered DME.] Once a claimis submitted, Medicare then decideswhether an item is eligible and, if so,how much to reimbursement them.
Medicare uses “codes” to helpmake these decisions. Codes repre-sent groups of devices/equipmentthat have similar characteristics.
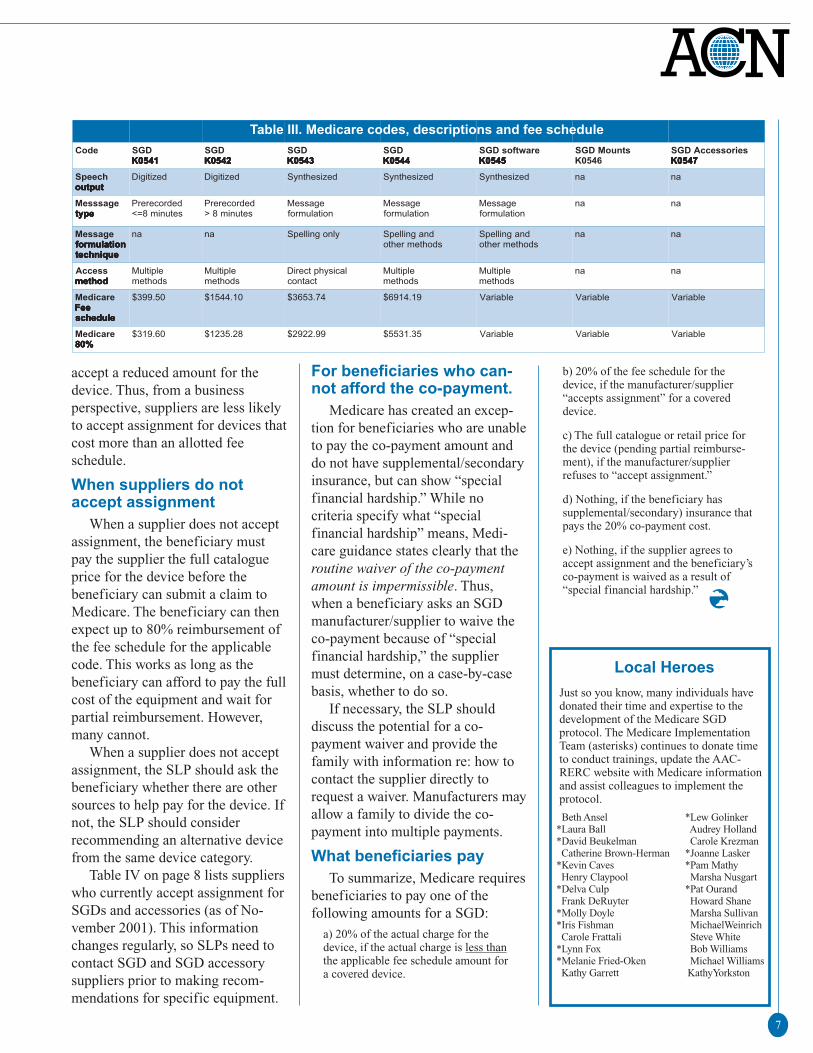
The Medicare guidance for SGDshas created seven codes: four forSGDs (K0541 to K0544) and oneeach for AAC software (K0545),SGD device mounts (K0546), ANDSGD device accessories (K0547).These codes are used in coveragedecisions. See Table III for descrip-tions.
Medicare uses two approaches indeciding how much to pay: (1) Feeschedules and (2) Individual consid-eration. Both approaches yield whatis called the “reasonable charge.”
(1) Fee schedules. The SGD codesK051-K054 have a fee schedule. Thismeans Medicare considers the“reasonable charge” the same for everydevice in the code.
(2) Individual consideration. The SGDcodes K055 - K057 are subject toindividual consideration. This meansthe “reasonable charge” is set sepa-rately for each item in the code.
Once Medicare sets the “reasonablecharge,” it will pay either 80% of theactual cost of the item or 80% of thefee schedule if one exists--which-ever is less.
Acceptingassignment
To make the servicedelivery and billing
processes easier andmore efficient for individual benefi-ciaries, some SGD manufacturersfollow a practice called “acceptingassignment.” This is a very commonbilling/claims procedure used bymost Medicare Durable MedicalEquipment (DME) suppliers.Accepting assignment means thesupplier collects only 20% from thebeneficiary (or supplemental/secondary insurer) and agrees to“bill” Medicare the remaining 80%of the allotted costs. Suppliers whoaccept assignment are helping tomake devices more affordable andreadily available to beneficiaries. Ifthe supplier does not accept assign-ment, the beneficiary must pay thefull fee schedule amount and waitfor Medicare reimbursement. SLPsshould confer with their clientsabout this issue beofre recommend-ing specific equipment.
How manufacturers decide
The manufacturer’s decision toaccept assignment is important froma business perspective. When asupplier accepts assignment, thecompany expects Medicare toreimburse it 80% of the fee scheduleamount, or 80% of the actual chargefor the device, whichever is less. Inaddition, the supplier can expect toreceive the other 20% from thebeneficiary or from thebeneficiary’s secondary/supplemen-tal insurance.
Medicare does not allow suppli-ers who accept assignment to billthe beneficiary for any “balance.”So if a device costs more than thefee schedule amount in a particularcategory, the supplier, by acceptingassignment, essentially agrees to
Figure 6. Example of aphysician’s prescription
7
accept a reduced amount for thedevice. Thus, from a businessperspective, suppliers are less likelyto accept assignment for devices thatcost more than an allotted feeschedule.
When suppliers do notaccept assignment
When a supplier does not acceptassignment, the beneficiary mustpay the supplier the full catalogueprice for the device before thebeneficiary can submit a claim toMedicare. The beneficiary can thenexpect up to 80% reimbursement ofthe fee schedule for the applicablecode. This works as long as thebeneficiary can afford to pay the fullcost of the equipment and wait forpartial reimbursement. However,many cannot.
When a supplier does not acceptassignment, the SLP should ask thebeneficiary whether there are othersources to help pay for the device. Ifnot, the SLP should considerrecommending an alternative devicefrom the same device category.
Table IV on page 8 lists supplierswho currently accept assignment forSGDs and accessories (as of No-vember 2001). This informationchanges regularly, so SLPs need tocontact SGD and SGD accessorysuppliers prior to making recom-mendations for specific equipment.
For beneficiaries who can-not afford the co-payment.
Medicare has created an excep-tion for beneficiaries who are unableto pay the co-payment amount anddo not have supplemental/secondaryinsurance, but can show “specialfinancial hardship.” While nocriteria specify what “specialfinancial hardship” means, Medi-care guidance states clearly that theroutine waiver of the co-paymentamount is impermissible. Thus,when a beneficiary asks an SGDmanufacturer/supplier to waive theco-payment because of “specialfinancial hardship,” the suppliermust determine, on a case-by-casebasis, whether to do so.
If necessary, the SLP shoulddiscuss the potential for a co-payment waiver and provide thefamily with information re: how tocontact the supplier directly torequest a waiver. Manufacturers mayallow a family to divide the co-payment into multiple payments.
What beneficiaries pay
To summarize, Medicare requiresbeneficiaries to pay one of thefollowing amounts for a SGD:
a) 20% of the actual charge for thedevice, if the actual charge is less thanthe applicable fee schedule amount fora covered device.
b) 20% of the fee schedule for thedevice, if the manufacturer/supplier“accepts assignment” for a covereddevice.
c) The full catalogue or retail price forthe device (pending partial reimburse-ment), if the manufacturer/supplierrefuses to “accept assignment.”
d) Nothing, if the beneficiary hassupplemental/secondary) insurance thatpays the 20% co-payment cost.
e) Nothing, if the supplier agrees toaccept assignment and the beneficiary’sco-payment is waived as a result of“special financial hardship.”
Table III. Medicare codes, descriptions and fee schedule
Local Heroes
Just so you know, many individuals havedonated their time and expertise to thedevelopment of the Medicare SGDprotocol. The Medicare ImplementationTeam (asterisks) continues to donate timeto conduct trainings, update the AAC-RERC website with Medicare informationand assist colleagues to implement theprotocol.
Beth Ansel *Lew Golinker*Laura Ball Audrey Holland*David Beukelman Carole Krezman Catherine Brown-Herman *Joanne Lasker*Kevin Caves *Pam Mathy Henry Claypool Marsha Nusgart*Delva Culp *Pat Ourand Frank DeRuyter Howard Shane*Molly Doyle Marsha Sullivan*Iris Fishman MichaelWeinrich Carole Frattali Steve White*Lynn Fox Bob Williams*Melanie Fried-Oken Michael Williams Kathy Garrett KathyYorkston

8
Table IV. Accepting assignment: Manufacturers of SGDs, SGD software and SGD accessories (11/01)

9
Continued on page 10
To illuminate the Medicareassessment process, this issuepresents three case examples. Weare all indebted to Laura Ball, PatOurand and Joanne Lasker fortaking the time to share these usefulillustrations of what goes into theassessment process.
Case #1: Person withdysarthria: ALSLaura J. Ball, Ph.D., CCC-SLP
Demographic informationAge & Gender: 41 year old male
Diagnoses: Amyotrophic LateralSclerosis (ICD-9 Diagnostic Code335); Dysarthria (ICD-9 DiagnosticCode 784.5)
Physical: Bulbar onset ALS. Ambulateswith a walker. Continues to exhibithand movement, although mildweakness with muscle wasting isapparent.
Communication: Mild dysarthria due toALS. Speech intelligibility is deterio-rating. This patient will require an SGDthroughout the course of this disease.
Life situationFamily: Currently lives at home withwife and three young children. Prior tothe illness, he enjoyed jogging, playingbasketball with his friends, playingcomputer games and cooking.
Academic: College graduate
Employment: Computer programmerand consultant, department manager.
Financial: Military benefits untilmedical discharge. Currently hasapplied for Medicare and has beenapproved. Has supplemental insuranceon his wife’s policy. Minimal privatefunds are available.
AssessmentThe SLP completed the SGD
assessment in one session. Thefollowing skills/abilities relate touse of an SGD.
Speech: Demonstrates milddysarthria. Speaking rate of101 wpm and intelligibilityof 91% on the SentenceIntelligibility Test.5
Note: Research has shownthat a person with ALS reaching a
speaking rate of approximately half of normal(100 wpm) will experience a rapid decline inintelligibility within 2 months.6
Primary means of communicationincludes slow, dysarthric naturalspeech, hand gestures and exaggeratedchanges in vocal intonation. Decreasedintelligibility places him at Stage 2 onthe ALS Severity Scale Speech Rating,indicating a need to supplement hisnatural speech with an SGD, in view ofthe imminent decline in intelligibility.[See Table I, page 3.]
Hearing: Attends and responds toauditory information presented atconversational loudness levels.Understands DECTalk synthesizedspeech as judged by appropriateresponses and reactions to messageoutput. Although slight sensori-neuralhearing loss was established, hediscriminated sentences on an SGDwith 100% accuracy.
Vision: He wears corrective lenses thatappropriately adjust his visual acuity.He located folders and words on SGDsand read orthographic symbols withfont size 10 using glasses, and font size14 without lenses.
Language and Cognition: Although noformal testing was conducted, herecalled extensive directions on how tolocate this clinic and recalled previousconversational interactions. He wasimmediately responsive to questionsand initiated interactions with the SGDafter only a very brief explanation. Noone observed or reported any cognitiveor linguistic changes.
Current communication statusand behaviors
• Slow, dysarthric natural speech.
• Independently uses multiple modali-ties to communicate, includinggestures, facial expressions, exagger-ated vocalizations and pointing.
• Unable to produce legible writtenmessages due to ALS affecting spinalmusculature, leaving hands and armsconsiderably weakened. As the diseaseprogresses, will become increasinglyparalyzed and therefore unable toaccess an SGD with a keyboard.
• Will benefit from an SGD andaccessories to compensate for hisdeteriorating speech and writing skills.
• Currently communicates needs &wants using speech; however, thedysarthria is rapidly progressive.
• Operates computer-based equipmentreadily, with extensive previouscomputer experience.
Communication needsFamily roles and psychosocial well-being: Because his children are young,he needs a system that enables him tocontinue in his role as father, discipli-narian and provider. Needs to commu-nicate with his spouse, relatingmessages to her as a caregiver and forintimacy. Needs a means of communi-cating with immediate family who liveat a distance. Needs a way to conversewith family, co-workers, and friends sohe does not become isolated.
Occupational Roles: His occupation asa computer consultant requirescommunication face-to-face and on thetelephone. He participates in adminis-trative meetings and is expected torapidly present detailed informationbefore a group.
Medical & Emergency: Needs aneffective means to call for assistance.Due to the progression of ALS, heneeds to convey changing medicalinformation and needs to his medicalproviders. Will need an SGD that offersmultiple methods of access over thecourse of the disease.
Functional communication goalsFunctional communication goals
are to use a synthesized SGD with atraditional orthographic display to:
1. Express needs/physical problems/pain with90+% accuracy.
2. Choose leisure activities with 90+% accuracy.
3. Express greetings and family rituals with90+% accuracy.
4. Offer information about recent events with90% accuracy.
5. Retell stories about past events and storelengthy messages for later retrieval with 90%accuracy.
6. Communicate effectively at work.
Rationale for device selectionThe assessment focused on
determining his needs regarding
10
Case Example #1, Continued from page 9
input, message characteristics,output and SGD access.
Input: Be able to use multiple accessmethods to accommodate changingneeds, fatigue and increasing paralysis:keyboard initially, switch for scanningand head-controlled input device fordirect selection when hands weakenand can’t use a keyboard.
Message characteristics: Formulatecomplex messages, store and retrievemessages using orthographic symbolsand rate acceleration techniques.
Output: Have synthesized voice output(DECTalk) so he can talk with hischildren, be understood in publicsettings, noisy environments and whentraveling in a car.
Other Features: Carry the SGD with ashoulder strap initially; battery powerfor up to 4 hours; mount it on wheel-chair as disease progresses.
The assessment determined he needs anSGD from category K0543 or K0544and accessories from categories K0546(mounts) and K0547 (switch,HeadMouse).
Specific device recommendationsHe was introduced to the Free-
dom 2000 (Words+, Inc.), Palmtop(Enkidu Research), Link (AssistiveTechnology), LightWriter (Zygo),DynaMyte (Dynavox), and theDynaVox 3100c (Dynavox). Duringthe assessment.
(1) He indicated an instant preferencefor the Freedom 2000.
(2) He immediately produced commu-nicative utterances using it with lessthan 5 minutes of instruction.
(3) The SGD increased his frequency ofcommunication attempts, attentionduring communicative interactions andsuccess in answering conversationalquestions.
(4) He used a HeadMouse to access theEZKeys onscreen keyboard and a specsswitch with scanning when he fatigued.
The following SGD and SGDaccessories were recommended
1. Freedom 2001-E Toughbook (F2001E-1D1),with Micro CommPac DECTalk speech outputand EZKeys for Windows.
2. Specs Switch (SPECS).
3. HeadMouse (HEADMOUSE) head-controlled input device.
4.HeadMouse Battery (HEADMOUSE-B1).Rechargeable battery to power the HeadMouse.
Note: All equipment is available from Words+,Inc.
Intervention/AcquisitionFunding was obtained (80% fromMedicare and 20% co-pay from thesupplemental policy.) Upon receipt ofthe SGD, he was scheduled to receive45 minutes of individual therapy ineach of 5 sessions. However, he usedthe device immediately and was onlyseen for one additional session to teachhim aspects of the rate-enhancingfeatures. He attained all of his func-tional communication goals in twotreatment sessions.
Impact of treatmentCurrently, he uses the SGD to
prepare stories and messages forphysicians during clinic visits and tostore agenda items for businessmeetings. He has maintained hisemployment by combining on-sitework and home consultation.
He now relies on the Freedom2000 to communicate. His wiferecently said their youngest childonly knows “Perfect Paul” as her
father’s voice. His friends tease himabout feeling “ordered” around bythe DECTalk. He participates incommunity activities and providesfrequent “consultative” assistance toindividuals with ALS regardingcommunication options.
Afterthoughts
This case example describeswhat occured for a person withbulbar onset ALS. Persons withspinal or mixed onset ALS mayrequire a different device profile.In either case, access is a vital issue.Individuals with progressiveneurodegenerative diseases requirean SGD that adapts to changes inneeds and abilities. It is importantto select an SGD that requiresminimal learning, since theseindividuals typically receive limitedintervention and many do notchoose to expend their valuable timeand limited energy learning acomplex SGD.
Case #2: Person withdysarthria: DDPat Ourand, M.S., CCC-SLP
Demographic informationAge & Gender: 43-year-old male
Diagnoses: Cerebral palsy (ICD-9Diagnostic Code 335), Severe Dysar-thria (ICD-9 Diagnostic Code 784.5)
Physical Status: Quadriplegia resultingin paralysis and significantly reducedstrength, force and range of motion inupper and lower extremities.
Communication Status: Current speechis limited to use of guttural soundsprimarily to answer yes/no questions.He has relied on an alphabet/wordboard to communicate since he was 12years old. He is literate.
Life situationFamily: Lives in his ownapartment. Has 24-hourstaff support for activitiesof daily living (ADLs) and
routine medical care. Hismother and sister, who live in aneighboring state, are able to under-stand his natural speech.
Academic: Completed high school.Earned Associates Degree in ComputerScience from a local communitycollege (1994).
Employment: Works part-time in asupported work environment. Does dataentry work and is paid at a piece rate.Also works on an advocacy project forthe ARC, assisting other adults withdevelopmental disabilities to completeinterviews.
Financial: Receives Social SecurityDisability Insurance, survivor benefitsas a disabled adult child. Since hereceives SSDI, his health insurance isMedicare. Because his monthly SSDI

11
Continued on page 12
benefits are sufficiently low, he alsoqualifies for Maryland’s MedicalAssistance (MA) program. Throughthis program, he is eligible for parallelhealth insurance benefits, but noadditional cash benefits.
Current communication statusand behavior
He is a very willing and ablecommunicator. He uses his voice toinitiate communication and respondto “yes/no” questions. Speechintelligibility is poor. Pragmaticskills are strong; his use of syntaxand semantics are intact. He uses hisalphabet/word board to expresslanguage and enhances his interac-tions using gestures, facial expres-sions and exaggerated vocalizations.He points to letters/words on theboard with his right index finger. Heis unable to write because of hisquadriplegia. He often uses a wholeword approach when constructingmessages. In the past, he used E ZKeys for Windows, a communica-tion software program, which ran ona laptop computer. However, he haddifficulty using the dynamic wordprediction program.Assessment
Sensory: Vision and hearing areadequate for his use of an SGD.
Motor: Has a power chair that hecontrols with a joystick positioned onthe right side of the wheelchair. He isunable to transfer independently to andfrom the wheelchair and other surfacesand requires physical assistance formost activities of daily living. Hisalphabet/word board is approximately17.5” inches by 13.5” inches. Heaccesses it using his right hand andright index finger.
Language and cognition: Review ofprevious SLP reports over the past 10years indicates his receptive language isrelatively intact and highly functional.He comprehends sophisticateddirections and engages in conversationswith both familiar and unfamiliarpartners. He likes to read newspapersand magazines.
During the assessment, he used avariety of SGDs and had no difficulty
learning to use the features on severaldevices, composing messages withminimal assistance. He clearly has thesensory, motor, cognitive and linguisticskills to use an SGD.
Communication needsHe identified the following
communication needs:
Home: Needs a way to make telephonecalls and provide instructions tocaregivers.
Occupational Roles: Needs a way totalk with peers, colleagues andsupervisors at work.
Psychosocial well being: Needs a wayto discuss current events with room-mates, staff and co-workers. Needs away to initiate and maintain a conversa-tion with unfamiliar partners in thecommunity.
Medical & Emergency: Needs a way tophone someone in case of an emer-gency and schedule appointments.Needs a way to notify workers at hisapartment of emergency situationsaffecting him and/or his roommates.
Functional communication goalsThe following treatment goals
were established.
• Signal a caregiver or roommate inanother room using an SGD, with100% accuracy.
• Using an SGD, converse with hismother, other family members andfriends on the telephone in case ofemergency and for other reasons atleast once weekly, with 90+% accuracy.
• Independently use an SGD in face-to-face interaction to communicate basicneeds and wants and to converse withcaregivers in his home daily, with 80%accuracy.
• Schedule medical appointments andspeak with medical professionals usingan SGD, with 90% accuracy.
• Express detailed needs, ideas,questions and answers to medicalprofessionals, caregivers, family andfriends using an SGD, with 90%accuracy.
• Ask questions and provide responsesin community-based interactions, suchas asking a clerk for help at a storeusing an SGD, with 90% accuracy.
Rationale for device selectionThe following device features
were identified as critical:
Input: Membrane sensitive keyboardwith up to 128 locations, positionedslightly to the right of midline, about 6-9” from the body at approximately a30-degree angle.
Message characteristics:Word prediction, word endings andfrequently used words list.
Enable stoage and retrieval of messagesprepared in advance.
Enable message formulation using acombination of words and/or letters.
Output: Intelligible synthesized speechoutput (DECtalk).
Auditory, tactile and kinestheticfeedback for targeting and access
Mounts and Accessories: Keyguard tooptimize accuracy of activations andincrease rate.
Specific SGD recommendationsAssessment information revealed
he requires an SGD from categoryK0544. Devices from the K0541and K0542 categories were deemedinappropriate because he has asignificant need to generate novelutterances. SGDs from K0543 donot offer him an appropriate rateenhancement technique (i.e., WordPower) or sufficient storage andretrieval options. Two SGDs fromK0544 were considered.
The Tablet Portable IMPACT wasoffered but ruled out because of its sizeand touch window. He needs a devicewith larger targets. Also, the IMPACThas a touch screen. His rate andaccuracy are better using a membranekeyboard.
The PathFinder has dynamic and staticdisplays, an alphabet/word softwareprogram known as WordPower anddimensions that approximate his non-electronic letter/word board. Themembrane keyboard has twokeyguards. He can select pre-pro-grammed and whole messages,customize messages and have intelli-gible speech output.

12
Lost driver’s license andwould like to re-apply forlicensure.
Financial: Has limitedinsurance through
workmen’s compensation.Some funding support through statevocational rehabilitation. Now ondisability and Medicare-eligible.
Current communication statusand behaviors
Current communication methodsare highly inefficient at conveyingnovel or complex information tocommunication partners. He occa-sionally initiates conversation abouta variety of topics with familymembers and therapists, but he isreluctant to attempt to speak to lessfamiliar communication partners,e.g., he no longer “chats” with otherparishioners after church. Hiscomments are often unintelligible tounfamiliar communication partners;and he is limited to responding tosimple questions. He cannot talk onthe phone.
Previous treatment: He participated ininpatient and outpatient treatment 2xweekly for a year after his stroke.Treatment focused on improving: (1)the effectiveness of his communicationby increasing verbal productions, (2)reading and writing skills and (3) oral-motor skills. His verbal productions didnot improve significantly.
Case Example #2, Continued from page 11
Case #3: Person withApraxia/Aphasia: CVAJoanne Lasker, Ph.D., CCC-SLP
Demographic information
Age & Gender: 51 year old male
Diagnoses: CVA (ICD-9 DiagnosticCode 436) sustained 3 years prior toevaluation, moderate receptive andexpressive aphasia (ICD-9 DiagnosticCode 784.3), moderate to severeapraxia of speech (ICD-9 DiagnosticCode 784.69).
Communication Status: Aphasia andapraxia are stable and not expected toimprove significantly. Speech islimited. Patient and his family arefrustrated. They heard about theUniversity Speech Clinic at a hospital-based Stroke Support Group. Theycame because they wanted him to “talkagain.” Prior to this assessment, theyhad not been exposed to speechgenerating devices.
Life situationFamily: Lives with wife, who works asan elementary schoolteacher. Has twoolder children (21 and 17 years old) anda two-year-old granddaughter
Academic: 2 years of college
Employment: Worked as mechanicalpress operator (computer-operatedmachine). Unable to work since stroke.
During a one-month trial period (four30-minute sessions/total of 2 hours), helearned to generate spontaneousutterances with appropriate content andformat the PathFinder without cueing(e.g., I will call you later. She shouldnot talk to him.). At the end of the trialhe stated, “I love this device!”
Based on the assessment andone-month trial period, the follow-ing equipment was recommended:
PathFinder with WordPower software(K0544).
This SGD is available from the Prentke RomichCompany.
Intervention/acquisitionThe evaluation was completed in
June 2001; final funding requestwas submitted in August 2001 andhe received the device in September2001. He obtained funding [80%from Medicare; 20% from theDivision of Rehabilitation Services(DORS). DORS also authorized 12treatment sessions with an SLP. Heis receiving weekly sessions at hiswork site to target stated functionalgoals.
Prognosis: Given the time post onsetand current severity of his apraxia andmoderate aphasia, his prognosis fordeveloping functional speech is poor. Inaddition, his needs cannot be met usingnatural communication methods (e.g.speech, gestures, writing) or low-technology speaking aids (e.g.communication book). He requires anSGD so he can interact effectively withboth familiar and unfamiliar communi-cation partners.
AssessmentThe current assessment consisted
of two 90-minute sessions andfocused on obtaining more informa-tion about his cognitive, speech,language and literacy skills (throughSGD trials) with the purpose ofselecting an appropriate SGD andaccessories so he could achievefunctional communication goals.
Language. Standardized tests con-firmed his aphasia and apraxia ofspeech. He has a moderate impairmentin language comprehension and asevere impairment in expressivecommunication. He is limited in hisability to initiate important topics ofconversation because he has word-retrieval difficulty (due to aphasia) andhas difficulty articulating (due toapraxia).
Western Aphasia Battery: OverallAphasia Quotient: 56.4/100; Spontane-ous Speech: 4/10 (Fluency, Grammati-cal Competence, and Paraphasias);Auditory Comprehension: 9.3/20;Repetition: 4.4/10; Naming: 5.5/10;Reading and Writing: 14.7/203
Impact of treatmentHe uses his device daily at work,
in his home and throughout thecommunity. He is currently attend-ing a 2-week vocational evaluationand uses the SGD with staff torequest appointment times, arrangetransportation and complete phonecalls to family and friends. He islearning to use the infrared featuresof the device to augment his writing.His supervisor at work is pleasedwith his use of the SGD. His motherstates “He has it all the time andloves it to death!”

13
Continued on page 14
Table V. Example of cognitive assessment for SGDs
Apraxia Battery for Adults: Scoresconsistent with severe to profoundapraxia of speech; however, resultswere confounded in part by thepresence of expressive languagedeficits.
Cognition: (assessed through devicetrials.) The assessment revealed he hasthe functional cognitive and linguisticabilities necessary to use an SGD. Hecan create, store and retrieve messagesrelated to a number of topics, usingboth text and pictorial representations.He could locate prestored messages aswell as generate new messages using akeyboard and word-prediction arraywith both text and symbols. See TableV for a summary of areas assessed.
Physical/Hearing/Vision: Walks slowlywith cane. Persistent weakness of hisright arm/hand which is splinted. Canuse direct selection to access a devicewith his left hand when he places thedevice on a table or when the devicehangs from a strap around his neck. Hishearing and vision are within normallimits and adequate for SGD use.
Communication needsThe patient and his wife identi-
fied the need for him to communi-cate in the following contexts:
Family Roles: Return to work so he canresume a “wage-earner” role within hisfamily. Interact with family members ofa variety of ages and literacy levels.Participate in marital counselingsessions. Discuss practical mattersrelated to home maintenance, behavior-management with children, financialmatters with his wife.
Psychosocial Well-being: Interact withchurch members. Conduct interactionswith familiar and unfamiliar communi-cation partners in the community.
Discuss house renovations with variousprofessionals. Pass the driver’slicensure exam.
Medical & Emergency: Talk on thephone in emergency situations when heis babysitting. Speak with medicalpersonnel and therapists (physical,psychological, speech). Deal withpersonnel involved with potential roademergencies when he regains hisdriver’s license.
Functional communication goalsThe following functional com-
munication goals were identified:
1. Formulate two-word sentences usingthe word-prediction spelling mode ofthe SGD in role-play situations takenfrom his daily activities with, 80%accuracy within 8 weeks.
2. Program a “news” message on theSGD and comunicate it to groupmembers weekly during 90% of allgroup sessions.
3. Use written instructions to indepen-dently program a new page on the SGDwith 12 messages and then link thepage to the keyboard page, within 3months.
4. Access pages of stored messages anduse these messages appropriately inconsumer-based transactions in personand on the telephone, 80% of the timewithin 3 months.
Rationale for device selection The following SGD features
were identified as necessary.
Input: Direct selection.
Message characteristics: Letter-based andsymbol-based; Word-prediction; Multiplelevels so messages can be stored and
organized in ways that are similar to whathe currently uses (communication book);Vocabulary that enables him to formulatenovel messages or use prestored phrases/sentences.
Output: Text-to-speech synthesis so hecan generate novel messages and spell;auditory feedback to improve auditorycomprehension; speech that is intelligibleto children and to unfamiliar listenersover the phone.
Other Features: Lightweight, so he cancarry it; battery life of at least 5 hours,so he can use it in a variety of settingsaway from electrical outlets.
Specific SGD recommendationsHe was introduced to a variety of
SGDs from categories of K0542(TechTalk 8 and MessageMate),K0543 (Lightwriter), and K0544(Dynamo, DynaMyte, DynaVox 3100).
Devices from multiple categorieswere presented during this evalua-tion because we were unsure abouthis SGD-based communicationskills, given the cognitive-linguisticaspects of his aphasia. By offeringtrials with several types of devices,we answered questions about hismessage capacity, formulationabilities and language representationskills as described:
K0542 -His needs and abilities exceedthe available vocabulary on theTechTalk8 and MessageMate.
K0543 - He was unable to spelladequately to generate novel messageson a purely text-based device.

14
Case Example #3, Continued from page 13
K0544 - The black/white symbols onthe Dynamo display were difficult todiscriminate and interfered with hissymbol selection accuracy and rate. TheDynaVox exceeded the size/weightcriteria for the patient to carryindependently/safely. During trials withthe DynaMyte, the following behaviorswere noted:
• He answered 20 questions regardingidentifying/biographical information,using preprogrammed screen andkeyboard;
• He expressed feelings and opinionsre: home repair, parenting issues, andchurch-related politics in conversationwith his wife;
• He participated successfully in 80%of conversational turns with anunfamiliar communication partner;
• He described a picture from amagazine (containing a scene of menon a boat) using specific language soan unfamiliar person could “sketch”picture without seeing it;
• He used the Adult User dictionary ontwo occasions to find vocabulary notavailable on custom screens;
• He typed functionally on the keyboardscreen and used word prediction sixtimes in conversation;
• He demonstrated the ability to use thecarrying case to transport the device.
As a result of the assessment, thefollowing equipment was recom-mended: (1) DynaMyte 3100(DMYT3100 (Category K0544)and (2) DynaMyte Carrying Case(CC-DMYT) (Category K0547).
All equipment is available from DynavoxSystems, Inc.
Intervention/AcquisitionThe device was funded in part by
Medicare (80%) and in part byvocational rehabilitation (20%). Ittook six months to acquire due toneed to educate vocational rehabili-tation personnel about the efficacyof SGDs in achieving communica-tion goals. [Editor’s note: Howfrustrating.]
Upon receipt of the recom-mended SGD, he attended oneindividual and one group SLPsession per week for 15 weeks toachieve functional communicationgoals. The SLP used a context-basedtreatment approach in which spe-cific skills were taught, practiced inexercises, practiced in role-play, andthen tried in “real life” situations.He made substantial progress on allgoals.
1. Formulating two-word sentenceswith 80% accuracy. Outcome: In atreatment session, he answeredquestions when the clinician acted as apotential employer in a job interview. Inreal life, he then successfully asked fora job application from a fast foodrestaurant and participated in aninterview with the manager.
2. Programming a “news” message onthe SGD during 90% of all groupsessions. Outcome: He programmedthese messages at home, practiced themin individual sessions and thencommunicated them each week inaphasia group.
3. Programming a new page on theSGD with 12 messages independentlyand linking the page to the keyboardpage. Outcome: Was accomplishedafter 4 weeks of treatment.
4. Accessing and using prestoredmessages appropriately 80% of thetime. Outcome: Completed 4 con-sumer-based transactions with theclinician present. He bought stampsfrom a post office, located an item withthe help of a sales clerk and purchasedit from Wal-Mart, bought hot cocoa atMcDonalds, and discussed the price ofroof shingles with a carpenter.
Impact of TreatmentFunctional outcomes and con-
sumer satisfaction measures were:
• His wife says, “The machine haschanged our life. He practices with it athome every day. Sometimes I have toremind him to take it with us when wego out. I just say, ‘I’m not doing yourtalking for you.’ The people in churchhave been real supportive, and want totalk to him with the machine.”
• He says, “The DynaMyte good helpBUT speech NO.” [The DynaMyte isgood, but my speech still hasn’t comeback.]
• He reapplied for his driver’s licenseand passed the written and practicaldriving tests.
• He is currently in the process oflooking for employment.
• He uses the device in church andcommunity.
• He uses it frequently as a “practicetool” at home.
Afterthoughts
Often people with aphasia are notconsidered “candidates” for SGDsdue to cognitive-linguistic deficits.However, this patient presented witha profile we see fairly frequently withyounger stroke patients. Specifically,his expressive communicationabilities were more impaired than hisreceptive abilities; he had usefulliteracy skills; he demonstrated anease with technology; his family wassupportive; and he possessed a“problem-solving” attitude towardhis chronic communication problem.Our assessment was highly personal-ized in order to obtain accuratemeasures of how he would use theSGD to communicate meaningfullyin daily activities. Based on thestructured tasks provided, we deter-mined that he could create and storemessages related to a number oftopics, using text as well as pictorialrepresentations.

15
Augmentative CommunicationNews (ISSN #0897-9278) ispublished quarterly. Copyright 2001by Augmentative Communication,Inc. 1 Surf Way, Suite 237,Monterey, CA 93940. Reproduceonly with written consent.Author: Sarah W. BlackstoneTechnical Editor: Carole KrezmanManaging Editor: Harvey PressmanOne Year Subscription: Personalcheck U.S. & Canada = $50 U.S.;Overseas = $62 U.S.Institutions, libraries, schools,hospitals, etc.: U.S. & Canada=$75U.S.; Overseas = $88 U.S. Single rate for this issue = $20.Special rates for consumers and full-time students. Periodicals Postagerate paid at Monterey, CA. POST-MASTER send address changes toAugmentative Communication, Inc.1 Surf Way, Suite 237, Monterey,CA 93940. Telephone: (831) 649-3050. FAX: (831) 646-5428.e-mail: [email protected]://www.AugComInc.com
State of the Science inAAC
On August 2-4, 2001, the AAC-RERC held its State of the ScienceConference (SOSC) on Communica-tion Enhancement, in conjunctionwith the 2001 USSAAC Conferencein St. Paul, MN. The NationalInstitute on Disability and Rehabili-tation Research (NIDRR), whichfunds the AAC-RERC, requires eachRERC to conduct a State of theScience Conference during the thirdyear of funding. In the area of AAC,this was the first time such an eventwas conducted since the 1990Visions conference.
The AAC-RERC partners invitedmembers of multiple stakeholdergroups to participate for three daysof presentations and discussions onvarious topic areas regarding AACand AAC technologies. A diversegroup of consumers and familymembers, manufacturers, research-ers, service providers, educators andother AAC experts arrived in St.Paul from the U.S. and Canada.AAC-RERC partners and theircollaborators prepared and pre-sented “white papers” on varioustopics. Several papers received inputfrom experts in Europe. In addition,the SOSC highlighted a presentationby consumer researchers who sharedpreliminary results from the AAC-RERC sponsored, consumer-ledresearch project, Tech 2010.
The main purpose of the presen-tations was to provide a “founda-tional base” about the current stateof the science in AAC technology,and about potential future directionsin AAC technology.
All participantsplayed active roles inthe process. Eachmorning, two papers
were presented as partof the USSAAC scientific
program. This made it possible forthe 200 plus USSAAC participants,as well as the 53 invited SOSCattendees, to hear the papers andcomment. After the morning presen-tations, the invited SOSC partici-pants reconvened for discussionsand brainstorming in an effort tocome to consensus about the issuesin the field related to the topic areas,which are listed below:
Future AAC Technology Needs.Consumer Perspectives. SarahBlackstone, Michael B. Williams andMick Joyce
Improving AAC Technologies for YoungChildren. Janice Light and KathrynDrager
Improving AAC Technologies for Adultswith Acquired Disabilities. DavidBeukelman and Laura Ball
AAC Performance and Usability Issues:The Effect of AAC Technology on theCommunicative Process. JefferyHigginbotham and Kevin Caves
Improving Connections Between AACTechnologies and the World. KevinCaves, Howard Shane and FrankDeRuyter
Enhancing Participation in Employ-ment though AAC Technologies. DavidMcNaughton, Diane Bryen andSolomon Rakhman
Enhancing Literacy DevelopmentThrough AAC Technologies. JanetSturm and David Yoder
Tech 2010: How do people learn to usean AAC device? Tracy Rackensperger,Michael B. Williams, Carole Krezmanand David McNaughton
Following the conference, thepapers were posted on the AAC-RERC website for additionalcomments. The Journal of theInternational Society for Augmenta-tive and Alternative Communica-
tion, Augmentative and AlternativeCommunication (AAC) will publishthe revised, peer-reviewed versionsof these white papers in the June2002 issue. This will serve as theofficial publication of the confer-ence outcomes.
For more information, go to: www.aac-rerc.comor contact Kevin Caves, Director, AAC-RERC,Duke University Medical Center, Box 3888,Durham, NC 27710. [email protected]
Log on to AAC-RERC Websitewww.aac-rerc.com
It has valuable, up-to-date informationabout the Medicare funding processand assessment protocol for AACdevices. It also has AAC-RERC projectupdates, white papers, ways to contactAAC-RERC partners and generalAACinformation.Go to www.aac-rerc.com.The rest is easy.

16
Periodicals
Augmentative Communication News
1 Surf Way, #237Monterey, CA 93940
Address Service Requested.
References1 Blackstone, S. (1999). Making a difference for
people who rely on AAC: The Medicare story.Augmentative Communication News. 12:4 and5: 1-16.
2 ICD-9 Code for communication diagnosis —Aphasia is 784.3; Verbal Apraxia is 784.69;Dysarthria is 784.5; Aphonia is 784.41.ICD stands for International Classification ofDiseases.
3 Goodglass, H., & Kaplan, E. (1983). Theassessment of aphasia and related disorders.Philadelphia: Lea & Febiger.
4 Kertesz, A. (1982). Western Aphasia BatteryOrlando, FL: Grune & Stratton, Inc.
5 Yorkston, K., Beukelman, D., & Tice, R. (1991).Sentence IntelligibilityTest. Lincoln, NE: Tice Technology Services,Inc.
6 Ball, L., Beukelman, D., & Pattee, G. (2001). Aprotocol for identificationof early bulbar signs in ALS. Journal ofNeurological Sciences, 191: 43-53.
ResourcesLaura J. Ball, Ph.D./CCC, Assistant Professor
Munroe-Meyer Institute for Genetics andRehabilitation, 985450, Nebraska MedicalCenter, University of Nebraska Medical Center,Omaha, NE 68198-5450Phone: 800-656-3937/[email protected]
Molly Doyle, Director, Las Floristas Center forApplied Rehabilitation Technology (CART),Rancho Los Amigos National RehabilitationCenter, 7601 E. Imperial Hwy, Downey CA90242, 562-401-6800, [email protected]
Lewis Golinker, Esq., Director, AssistiveTechnology Law Center, 202 East State Street,Suite 507, Ithaca, NY 14850. [email protected]
Joanne P. Lasker, Ph.D., CCC-SLP, AssistantProfessor, Florida State University, Departmentof Communication Disorders, 305 RegionalRehabilitation Center, Tallahassee, FL 32306.850-644-8465; [email protected]
Pamela Mathy, Director of Clinical Services,Department of Speech & Hearing ScienceArizona State University, PO Box 870102Tempe, AZ 85287, [email protected]
Patricia Ourand, M.S., CCC-SLP, AssociatedSpeech & Language Services, Inc., 100 E.Pennsylvania Avenue, Courtyard SuiteTowson, MD 21286, 410-825-9445,[email protected].

















