Occupational radiation safety in Radiotherapy, Timothy Peace S
21
OCCUPATIONAL RADIATION SAFETY IN RADIOTHERAPY DEPARTMENT OF RADIOTHERAPY CHRISTIAN MEDICAL COLLEGE, VELLORE Timothy Peace S
-
Upload
ohscmcvellore -
Category
Health & Medicine
-
view
799 -
download
0
Transcript of Occupational radiation safety in Radiotherapy, Timothy Peace S

OCCUPATIONAL RADIATION SAFETY IN
RADIOTHERAPY
DEPARTMENT OF RADIOTHERAPY
CHRISTIAN MEDICAL COLLEGE, VELLORE
Timothy Peace S
PRESENTATION OUTLINE
• INTRODUCTION
• POTENTIAL AREAS OF RADIATION HAZARDS IN RT
• TELETHERAPY
– TELECOBALT
– MEDICAL LINEAR ACCELERATOR
• BRACHYTHERAPY
• GENERAL RADIATION SAFETY MEASURES
• RECOMMENDATIONS
INTRODUCTION
• Radiation therapy aims to
– Destroy the cancer
– using gamma rays, high-energy x-rays electrons, protons and heavy ions
– generated from radioisotopes, medical linear accelerators and synchrotrons
• Double-edged sword
– The cancer destroying radiation can also destroy normal cells
– Deterministic effects
• Gastrointestinal syndrome, CNS syndrome, cataract, pneumonitis, sterility, erythema, alopecia, cataract
– Stochastic effects
• Radiation carcinogenesis and genetic effects
POTENTIAL AREAS OF RADIATION HAZARDS IN RT
• Teletherapy
– Telecobalt treatment unit (1.25 MeV, gamma photons)
– Medical linear accelerator (6 & 15 MV high energy x-ray photons), electrons ranging from 4-21 MeV and neutrons arising from linear accelerators delivering more than 10 MV x-ray photons)
• Brachytherapy
– Pre-loaded system
– Manual after-loading system (only low dose rate brachytherapy)
– Remote after-loading system (also high dose rate brachytherapy)
• Simulator
– Diagnostic x-ray-based simulator unit

* The whole body dose limit is 20 mSv a year when averaged over 5 years with a maximum of 30 mSv in any one year (AERB)
Source: International Commission on Radiological Protection 26
Tissue or Organ Radiation Worker Member of Public
Whole of body 20* mSv /yr 1 mSv /yr
Lens of eye 150 mSv /yr 15 mSv /yr
Skin 500 mSv/yr 50 mSv /yr
Hands and feet 500 mSv /yr 50 mSv /yr
Pregnancy once declared
2 mSv to lower trunk
(1 mSv to foetus)
Foetus is considered to be member of public
ANNUAL DOSE LIMITS
TELETHERAPY TELECOBALT UNIT
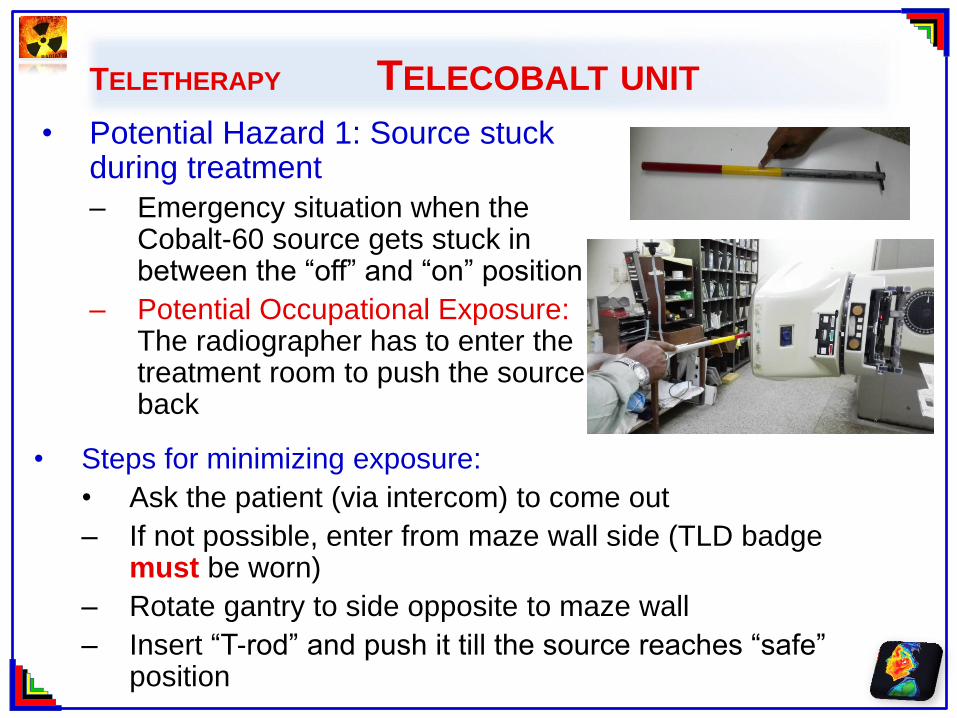
• Potential Hazard 1: Source stuck during treatment
– Emergency situation when the Cobalt-60 source gets stuck in between the “off” and “on” position
– Potential Occupational Exposure: The radiographer has to enter the treatment room to push the source back
• Steps for minimizing exposure:
• Ask the patient (via intercom) to come out
– If not possible, enter from maze wall side (TLD badge must be worn)
– Rotate gantry to side opposite to maze wall
– Insert “T-rod” and push it till the source reaches “safe” position
TELETHERAPY TELECOBALT UNIT
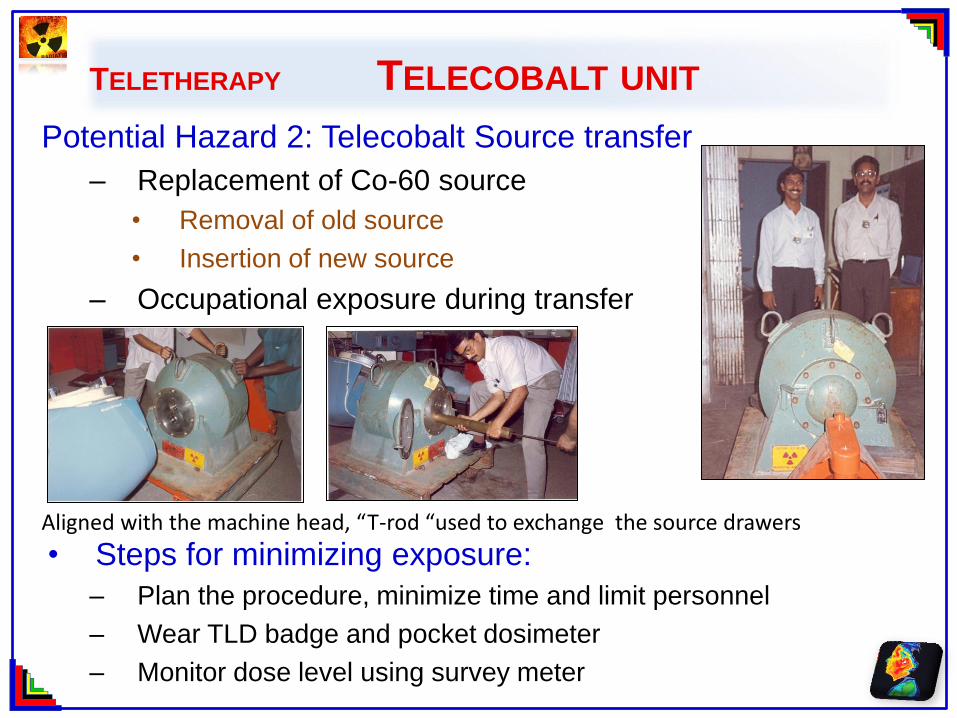
Potential Hazard 2: Telecobalt Source transfer
– Replacement of Co-60 source
• Removal of old source
• Insertion of new source
– Occupational exposure during transfer
• Steps for minimizing exposure:
– Plan the procedure, minimize time and limit personnel
– Wear TLD badge and pocket dosimeter
– Monitor dose level using survey meter
Aligned with the machine head, “T-rod “used to exchange the source drawers
TELETHERAPY TELECOBALT UNIT
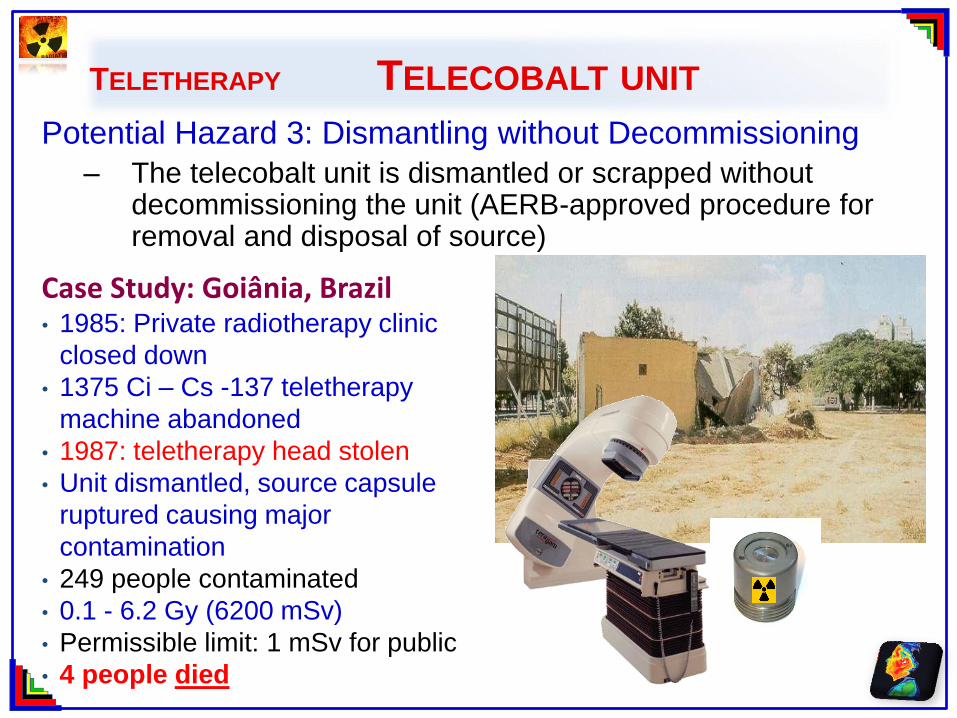
Potential Hazard 3: Dismantling without Decommissioning
– The telecobalt unit is dismantled or scrapped without decommissioning the unit (AERB-approved procedure for removal and disposal of source)
Case Study: Goiânia, Brazil • 1985: Private radiotherapy clinic
closed down
• 1375 Ci – Cs -137 teletherapy
machine abandoned
• 1987: teletherapy head stolen
• Unit dismantled, source capsule
ruptured causing major
contamination
• 249 people contaminated
• 0.1 - 6.2 Gy (6200 mSv)
• Permissible limit: 1 mSv for public
• 4 people died
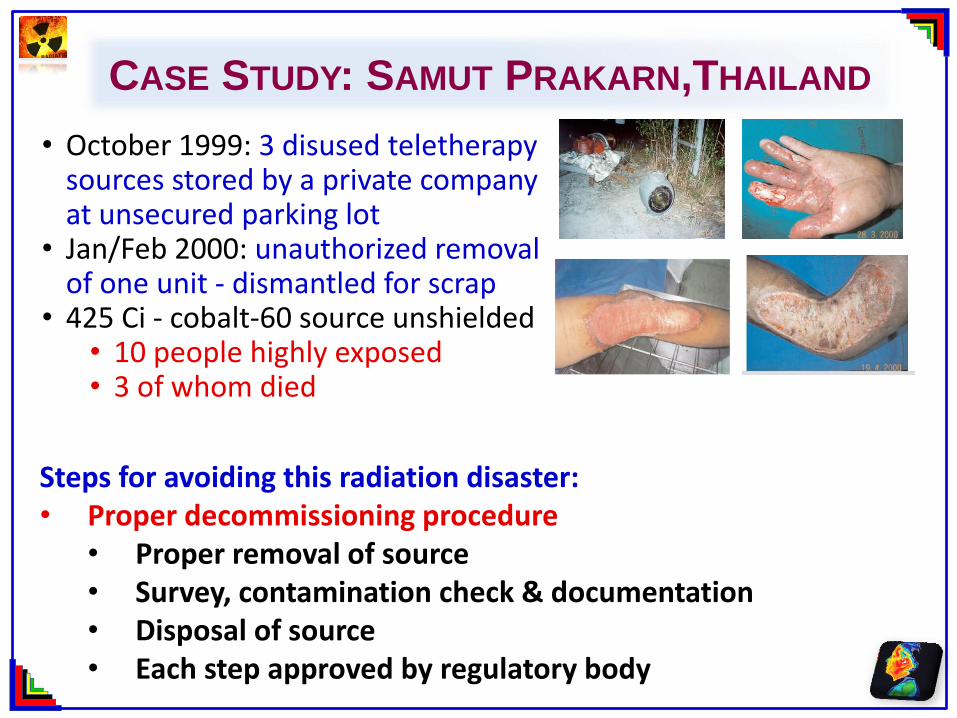
CASE STUDY: SAMUT PRAKARN,THAILAND
• October 1999: 3 disused teletherapy sources stored by a private company at unsecured parking lot
• Jan/Feb 2000: unauthorized removal of one unit - dismantled for scrap
• 425 Ci - cobalt-60 source unshielded • 10 people highly exposed • 3 of whom died
Steps for avoiding this radiation disaster: • Proper decommissioning procedure
• Proper removal of source • Survey, contamination check & documentation • Disposal of source • Each step approved by regulatory body
TELETHERAPY – MEDICAL LINEAR ACCELERATOR
• The linear accelerator does not consist of a radioactive
source and hence poses a lesser radiation hazard
• It generates high energy electrons (4-21 MeV) and x-rays
(6-15MV)
• Potential hazard: Personnel entering the room when the
radiation is „on‟ can potentially receive lifetime dose in a
single exposure
• Case study: St Teresa’s Hospital (STH), Hong Kong – Two physicists performed quality assurance check on a medical
linac
– discovered the accidental presence of a female ward assistant
– through the room's CCTV
– As for the affected female staff received 70 Sv (very low)
TELETHERAPY –LINEAR ACCELERATOR
• Case study: Industrial Accelerator – 15 MV food irradiation facility in Hanoi. – An individual entered the irradiation room without the operators‟
knowledge – unwittingly exposed his hands to the x-ray beam. – The individual received doses
• 10 - 25,000 mSv to the left hand • 20 - 50,000 mSv to the right hand.
– Within one month one hand had to be amputated as well as the fingers on the other hand.
• Simple steps that could have avoided these unnecessary exposures – Console to face treatment room door – Door interlock – “Last man out” switch – Check CCTV before starting exposure
Limit for hand: 500 mSv
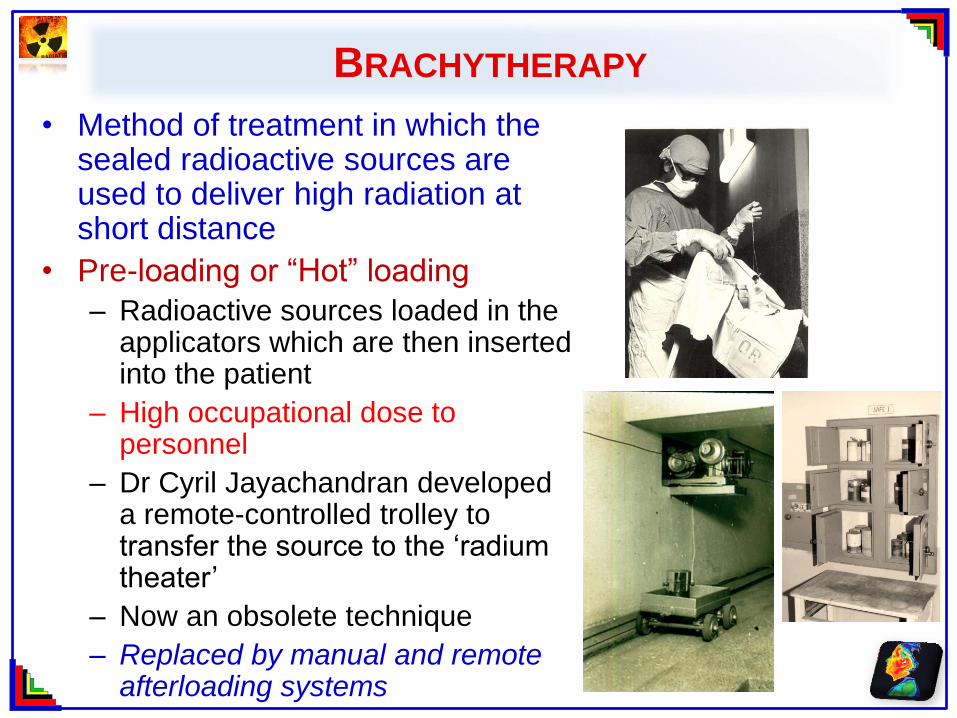
BRACHYTHERAPY
• Method of treatment in which the sealed radioactive sources are used to deliver high radiation at short distance
• Pre-loading or “Hot” loading
– Radioactive sources loaded in the applicators which are then inserted into the patient
– High occupational dose to personnel
– Dr Cyril Jayachandran developed a remote-controlled trolley to transfer the source to the „radium theater‟
– Now an obsolete technique
– Replaced by manual and remote afterloading systems
BRACHYTHERAPY - MANUAL AFTERLOADING
• Case study from another country:
Mishandling of source ribbons
– Patient scheduled for endobronchial
implant
• Ir 192 seeds: Activity- 2516 MBq.
– Staff mistakenly gave the attending
physician the inactive end of source
ribbon who inserted it into patient.
– Staff, assumed pieces of ribbon
contained no radioactive material,
coiled them and held them in her
hands.
– Dose to the staff‟s hand
• ~2.7 Gy (~2700 mSv – Allowed
500 mSv),
HDR BRACHYTHERAPY
• Case study from another country: Malfunction of high dose rate equipment – Patient was to be treated with a HDR
containing 159 GBq of Ir192
– The source wire had been broken and the source had remained in the patient.
– Personnel disregarded the alarm from an area radiation monitor because the unit console indicated 'safe'.
– The source remained in the patient for almost four days and the patient received 16,000 Gy at 1cm (Prescription: 18 Gy)
– The patient died shortly after removal of the source
– The loss of the source resulted in radiation exposure to 94 individuals
• Persons at the cancer clinic and the nursing home,
• Ambulance staff and workers at the waste disposal company
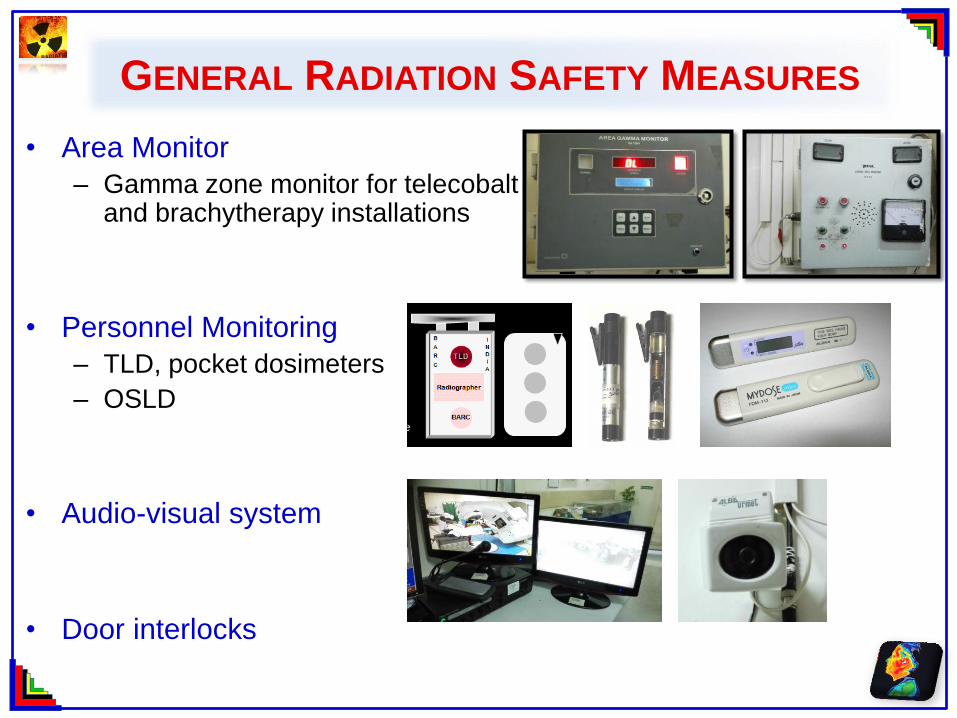
GENERAL RADIATION SAFETY MEASURES
• Area Monitor
– Gamma zone monitor for telecobalt and brachytherapy installations
• Personnel Monitoring
– TLD, pocket dosimeters
– OSLD
• Audio-visual system
• Door interlocks
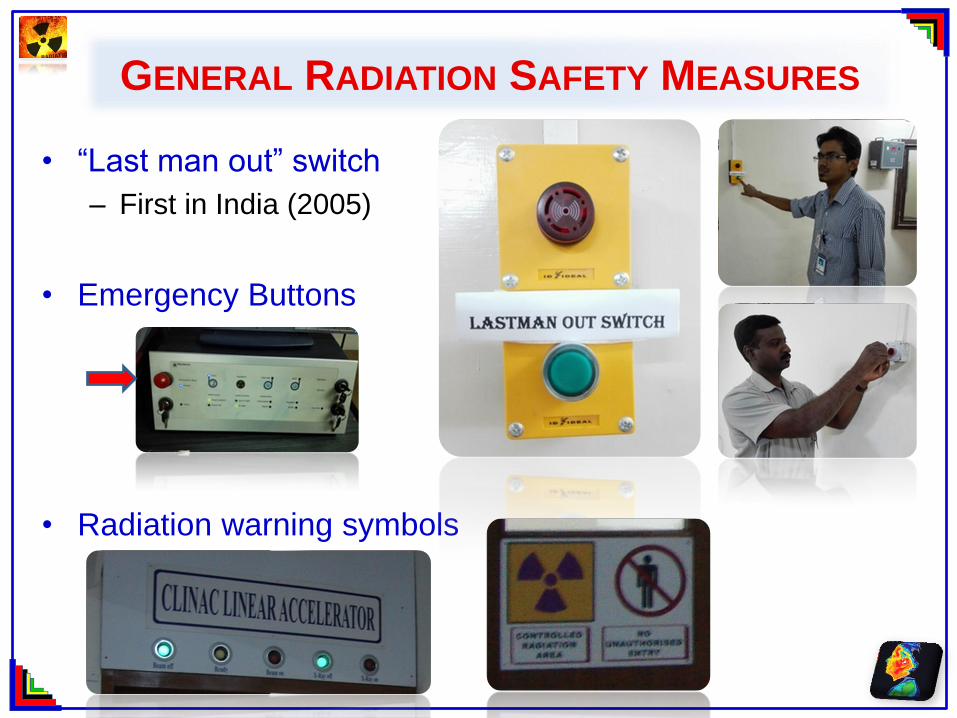
GENERAL RADIATION SAFETY MEASURES
• “Last man out” switch
– First in India (2005)
• Emergency Buttons
• Radiation warning symbols
DISCUSSION
• History shows that accidents rarely occur due to a single
equipment failure or a single human error. In most accident
cases there was a combination of elements such as:
– a) no prior safety assessment
– b) poor education and lack of training, especially when faced
with an unusual situation,
– c) management pressure (real or perceived) to continue work
even when safety systems were inoperable or deficient,
– d) poor maintenance programme or none at all, leading to a
reduction in layers of safety, and non-investigated false
alarms leading to persons ignoring warning systems.
RECOMMENDATIONS
• Each radiation professional in RT must cooperate with the Radiation Safety Officer to ensure
– Effective organisation of all radiotherapy practice
– Education, training and awareness
– Communication
– Follow-up of equipment faults
– Frequent Quality assurance
– General radiation safety measures (Area and personnel monitoring, routine survey, audio-visual system, safety interlocks and warning symbols)
– AERB guidelines must be followed for installation, commissioning and decommissioning of radiotherapy equipment
– AERB approved procedure for procurement, replacement and disposal of sources
– This will enable each radiation worker to handle radiation in a safe environment and limit the occupational exposure to “As Low as Reasonably Achievable - ALARA”
ACKNOWLEDGEMENTS
• Dr I Rabi Raja Singh, Radiation Safety Officer, CMC, Vellore
• Mr Jose Solomon Raj, Medical Physics Intern
• Mr Mohamathu Rafic, Lecturer in Medical Physics