
Observations on the mechanism of abdominal pain · Observations on the mechanismofabdominalpain the...
13
Gut, 1969, 10, 19-31 Observations on the mechanism of abdominal pain D. J. HOLDSTOCK, J. J. MISIEWICZ, AND SHEILA L. WALLER From the Medical Research Council Gastroenterology Research Unit, Central Middlesex Hospital, Park Royal, London Abdominal pain is one of the commonest presenting symptoms in gastroenterology. In some patients an organic lesion is responsible but in many others the cause of pain remains obscure, despite thorough investigation. There is some evidence, however, that the motor activity of the colon may be abnormal in patients with various alimentary disorders (Connell, 1959, 1962; Chaudhary and Truelove, 1961; Wangel and Deller, 1965; Misiewicz, Connell, and Pontes, 1966), but very little is known about the relationship between pain and changes of intraluminal pressure in individual patients (Connell, Jones, and Rowlands, 1965). In this paper we present the results of mano- metric studies in nine patients suffering from attacks of severe abdominal pain for which no cause was found after thorough investigation, including laparotomy in some cases. The attacks seemed to be related to changes in intraluminal pressures in either small or large intestine. METHODS AND PATIENTS Intraluminal pressure in the sigmoid and rectum was measured with small (7 x 10 mm) air-filled balloons (Atkinson, Edwards, Honour, and Rowlands, 1957) mounted on narrow tubes and placed through a sig- moidoscope at approximately 25, 20, and 15 cm proximal to the anal margin; the sigmoidoscope was then with- drawn. Pressure in the small intestine and proximal colon was recorded with radiotelemetering capsules (Rowlands and Wolff, 1960), which were located by fluoroscopy and by reference to the characteristics of the pressure record (Connell, McCall, Misiewicz, and Rowlands, 1963; Misiewicz, Waller, Fox, Goldsmith, and Hunt, 1968). The pressures were recorded on a multichannel pen writer; respiration and somatic movements were monitored in all the studies with a stethograph. In some patients measurements were carried out simultaneously in the distal colon and in the small intestine or proximal colon. Patients were asked to indicate the onset of abdominal pain by means of a signal switch which pro- duced an appropriate mark on the record; they were unable to see the pressure trace during the study. The tests were carried out in a quiet room with the subjects resting comfortably on a couch. Motor activity was measured in the fasting state, following the ingestion of a standard meal, and after the injection of 0.75 mg of prostigmine subcutaneously. Intravenous propantheline, 5 to 10 mg, was used to abolish motor activity. The nine patients described in this study were selected from a larger group referred for manometric investiga- tion of various abdominal symptoms, because abdominal pain, for which no definite cause could be found on routine investigation, was a prominent symptom in all of them. All the patients were normal on physical and sigmoidoscopic examination; their haemoglobin and ESR levels were within normal limits. Barium studies showed no evidence of organic disease. Relevant addi- tional investigations are listed below under individual patients and the findings are summarized in Table 1. TABLE I Patient Clinical Diagnosis No. 2 3 4 5 6 7 8 9 Postgastrectomy syndrome Postgastrectomy syndrome Constipation and abdominal pain Irritable colon syndrome Irritable colon syndrome Irritable colon syndrome Irritable colon syndrome Postdysenteric colon Irritable colon syndrome Correlation of Site of Pressure Intraluminal Activity Pressure with Pain + Small intestine + Small intestine and colon + Small intestine + + + + Colon Colon Colon Colon Colon Colon RESULTS PATIENT NO. 1 A 54-year-old man had had a Polya partial gastrectomy for duodenal ulcer 12 years previously. Postoperatively he suffered from dump- ing, diarrhoea, and steatorrhoea, but the most dis- abling symptom was abdominal pain which invari- ably followed the ingestion of food. The symptoms persisted despite a multiplicity of medical treatments and conversion of his gastrectomy to Billroth I four years after the original operation. Barium studies suggested that pain coincided with the entry of the contrast material into the small intestine. The patient was much disabled by the pain, which caused him to abstain from eating during the day; he had to lie down for one hour after the evening meal. Psychiatric assessment suggested an anxious person- ality with a low threshold to intestinal discomfort. 19 on December 29, 2019 by guest. Protected by copyright. http://gut.bmj.com/ Gut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Downloaded from
Transcript of Observations on the mechanism of abdominal pain · Observations on the mechanismofabdominalpain the...

Gut, 1969, 10, 19-31
Observations on the mechanism of abdominal painD. J. HOLDSTOCK, J. J. MISIEWICZ, AND SHEILA L. WALLER
From the Medical Research Council Gastroenterology Research Unit, Central MiddlesexHospital, Park Royal, London
Abdominal pain is one of the commonest presentingsymptoms in gastroenterology. In some patients anorganic lesion is responsible but in many others thecause of pain remains obscure, despite thoroughinvestigation. There is some evidence, however, thatthe motor activity of the colon may be abnormal inpatients with various alimentary disorders (Connell,1959, 1962; Chaudhary and Truelove, 1961; Wangeland Deller, 1965; Misiewicz, Connell, and Pontes,1966), but very little is known about the relationshipbetween pain and changes of intraluminal pressurein individual patients (Connell, Jones, and Rowlands,1965). In this paper we present the results of mano-metric studies in nine patients suffering from attacksof severe abdominal pain for which no cause wasfound after thorough investigation, includinglaparotomy in some cases. The attacks seemed to berelated to changes in intraluminal pressures in eithersmall or large intestine.
METHODS AND PATIENTS
Intraluminal pressure in the sigmoid and rectum wasmeasured with small (7 x 10 mm) air-filled balloons(Atkinson, Edwards, Honour, and Rowlands, 1957)mounted on narrow tubes and placed through a sig-moidoscope at approximately 25, 20, and 15 cm proximalto the anal margin; the sigmoidoscope was then with-drawn. Pressure in the small intestine and proximal colonwas recorded with radiotelemetering capsules (Rowlandsand Wolff, 1960), which were located by fluoroscopyand by reference to the characteristics of the pressurerecord (Connell, McCall, Misiewicz, and Rowlands,1963; Misiewicz, Waller, Fox, Goldsmith, and Hunt,1968). The pressures were recorded on a multichannelpen writer; respiration and somatic movements weremonitored in all the studies with a stethograph. In somepatients measurements were carried out simultaneouslyin the distal colon and in the small intestine or proximalcolon. Patients were asked to indicate the onset ofabdominal pain by means of a signal switch which pro-duced an appropriate mark on the record; they wereunable to see the pressure trace during the study. Thetests were carried out in a quiet room with the subjectsresting comfortably on a couch. Motor activity wasmeasured in the fasting state, following the ingestion ofa standard meal, and after the injection of 0.75 mg of
prostigmine subcutaneously. Intravenous propantheline,5 to 10 mg, was used to abolish motor activity.The nine patients described in this study were selected
from a larger group referred for manometric investiga-tion of various abdominal symptoms, because abdominalpain, for which no definite cause could be found onroutine investigation, was a prominent symptom in all ofthem. All the patients were normal on physical andsigmoidoscopic examination; their haemoglobin andESR levels were within normal limits. Barium studiesshowed no evidence of organic disease. Relevant addi-tional investigations are listed below under individualpatients and the findings are summarized in Table 1.
TABLE IPatient Clinical DiagnosisNo.
2
3
456789
Postgastrectomy syndromePostgastrectomy syndrome
Constipation and abdominalpainIrritable colon syndromeIrritable colon syndromeIrritable colon syndromeIrritable colon syndromePostdysenteric colonIrritable colon syndrome
Correlation of Site of PressureIntraluminal ActivityPressure withPain
+ Small intestine+ Small intestine
and colon+ Small intestine
++++
ColonColonColonColonColonColon
RESULTS
PATIENT NO. 1 A 54-year-old man had had a Polyapartial gastrectomy for duodenal ulcer 12 yearspreviously. Postoperatively he suffered from dump-ing, diarrhoea, and steatorrhoea, but the most dis-abling symptom was abdominal pain which invari-ably followed the ingestion of food. The symptomspersisted despite a multiplicity of medical treatmentsand conversion of his gastrectomy to Billroth I fouryears after the original operation. Barium studiessuggested that pain coincided with the entry of thecontrast material into the small intestine. Thepatient was much disabled by the pain, which causedhim to abstain from eating during the day; he hadto lie down for one hour after the evening meal.Psychiatric assessment suggested an anxious person-ality with a low threshold to intestinal discomfort.
19
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from

D. J. Holdstock, J. J. Misiewicz, and Sheila L. Waller
FIG. la.
FIG. 1. Patient no. 1. Smallintestinal pressure acivitycoinciding with symptoms after ameal (a) and after intravenous5-hydroxytryptamine, 0.5 mg ateach signal (b). (In this and allsubsequent figures calibration iin centimetres of water pressure.Stetho = stethograph.)
FIG. lb.
Pressure records from the small intestine areshown in Figure 1. The patient's pain coincided withbursts of small intestinal pressure activity afterfood (Fig. la), or with small intestinal activityinduced by intravenous injections of 5-hydroxy-tryptamine (Fig. lb), whilst intravenous saline
administered in identical circumstances had noeffect. Both motor activity and symptoms wereabolished by intravenous propantheline.
PATIENT NO. 2 This 49-year-old man's postgastrec-tomy symptoms were so disabling that prefrontal
20
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from

Observations on the mechanism of abdominal pain
Fioi. 2a.
FIG. Zb.FIG. 2. Patient no. 2. (a) High pressure waves in the rectal leadfollowing 0 75 mg ofprostigmine; dots mark the patientwincing. (b) Postprandial small intestinal motor activity coinciding with pain. (c) Marked motor activity in large and smallintestine after 0.75 mg ofprostigmine. Activity andpain abolished by 10 mg intravenous propantheline given at P. Verticalbar represents an interval offive minutes.
21
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from

D. J. Holdstock, J. J. Misiewicz, and Sheila L. Waller
FIG. 2c.
lobotomy was considered at one stage. Abdominalpain began at the age of 32. At the age of 38 a duo-denal ulcer was diagnosed, for which a Polya partialgastrectomy was performed two years later. Fromthen onwards he complained of postprandial upperabdominal pain and also of pain in the left iliacfossa which was associated with constipation: thesesymptoms were persistent and disabling. Repeatedinvestigations were negative and various treatments(including conversion of the gastrectomy to a Roux-en-y anastomosis three years after the originaloperation) produced only temporary benefit. Psy-chiatric opinion was that he suffered from a person-ality disorder with a marked propensity to anxiety.
Pressure records from this patient are shown inFigure 2. After 0.75 mg of subcutaneous prostigminevigorous contractions were present in the rectum,and each peak of pressure coincided with cramp-likelower abdominal pain likened by the patient to thepain he felt when constipated; he was seen to winceat the height of each pressure peak (Fig. 2a). Intra-venous propantheline stopped both the symptomsand the pressure activity.On another occasion, after starting a meal this
patient developed upper abdominal pain, whichcoincided with bursts of small intestinal pressureactivity (Fig. 2b). During a third study, an injectionof 075 mg of prostigmine produced both the lowerand the upper abdominal pain, with hyperactivity ofthe jejunum, sigmoid, and rectum. This activity wasabolished by intravenous propantheline with im-mediate relief of symptoms (Fig. 2c).
PATIENT NO. 3 A 49-year-old housewife presentedwith progressive constipation, vomiting, and severe
left-sided abdominal pain, during her first and onlypregnancy 22 years previously. Lumbar sympath-ectomy and subtotal colectomy with ileorectalanastomosis carried out elsewhere were ineffective.The constipation and abdominal pain were so severethat ileostomy was being considered. Examinationunder anaesthesia was normal and biopsy at 24 cmfrom the anal margin showed normal colonic mucosawith ganglion cells present in normal numbers.X-ray studies showed gaseous distension of thelarge bowel remnant.
Pressure activity of the small intestine before,during, and after a bout of pain is shown in Figures3a, b, and c. The resting record was normal (Fig. 3a)but during the pain small intestinal motor activitywas markedly increased (Fig. 3b), subsiding againwhen the pain abated (Fig. 3c). The symptoms andthe motor activity were abolished by intravenouspropantheline. Pressure activity in the colonicremnant did not increase during the episodes of pain.Because the evidence from the pressure studiessuggested that small intestinal activity was playinga part in the patient's symptoms, it was decided notto perform an ileostomy.
PATIENT NO. 4 This 23-year-old salesman had beensuffering during the previous six years from attacksof lower abdominal colic and diarrhoea: he hadbeen unable to work for nine months before admis-sion because of the severity of his symptoms. Twolaparotomies performed elsewhere had shown noabnormality apart from adhesions around thecaecum, and numerous other investigations werenegative. Sigmoidoscopy showed marked spasm ofthe sigmoid colon and his pain was triggered off by
22
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from

Observations on the mechanism of abdominal pain
FIo. 3a. FIG. 3D.
FIG. 3. Patient no. 3. Small intestinal pressure activity(a) before, (b) during, and (c) after an attack ofpain.
FIo. 4. Patient no. 4. Radiotelemetered pressure recordfrom lower descending colon. Onset of pain (P) coincidedwith high frequency motor activity.
FIo. 3c.
FIG. 4.
23
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from
D. J. Holdstock, J. J. Misiewicz, and Sheila L. Waller
FiG. Sa. FiG. Sb.
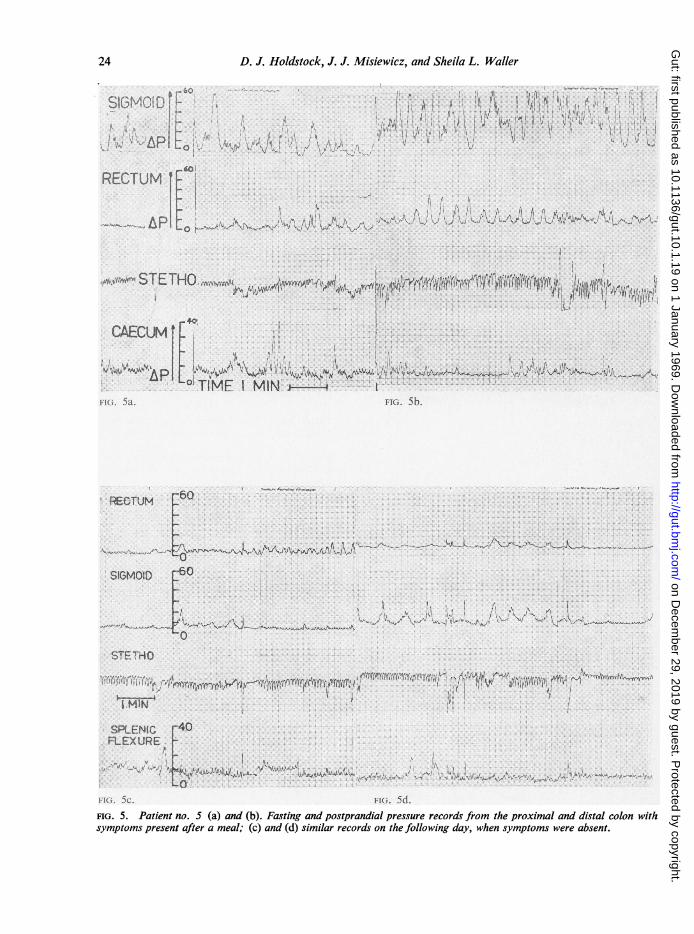
FIG. 5c. FIQ. 5d.FIG. 5. Patient no. 5 (a) and (b). Fasting and postprandial pressure records from the proximal and distal colon withsymptoms present after a meal; (c) and (d) similar records on the following day, when symptoms were absent.
24
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from

Observations on the mechanism of abdominal pain
the instrumentation. The spasm and the pain pre-vented the insertion of tubes to the usual extent andthe pressure record from the lower sigmoid andrectum was normal.As the relevant segment of the colon was not
accessible through the sigmoidoscope, a radio-telemetering capsule was given to the patient and itsposition followed fluoroscopically until it reachedthe lower descending colon. Intraluminal pressuresrecorded from that part of the colon included burstsof waves characterized by high amplitude andfrequency, which coincided with the patient's painindicated by point P in Figure 4. A barium enemacarried out subsequently without prior lavageshowed painful spasm of that area of the sigmoidfrom which pressure waves had been recorded. Boththe pain and the spasm were relieved by intravenouspropantheline.
PATIENT NO. 5 A 43-year-old priest complained fortwo years of pain in the left iliac fossa and theepigastrium, worse after meals or under stress,which was accompanied by the passage of 'rabbity'stools. His sigmoid colon was palpable and tender.A barium enema showed spasm of the sigmoid colonwhich was relieved by propantheline, but no ana-tomical abnormality. Studies of colonic motoractivity were performed on two successive days. Onthe first day his postprandial symptoms were presentand the sigmoid pressure record showed a high levelof basal activity followed by a marked response to ameal (Figs. 5a and b). On the second day the patientfelt well and experienced no discomfort following theingestion of an identical meal. On this occasion themotor activity of the sigmoid was much less both inthe basal and in the postcibal periods (Figs. 5c and d).
PATIENT NO. 6 A 35-year-old clerk suffered fromabdominal pain since the age of 15. While in theRAF a diagnosis of duodenal ulcer was considered,but antacids gave little relief. At the age of 22 hedeveloped achalasia of the cardia; a cardiomyotomyperformed three years later resulted in a completerelief of the dysphagia. However, the episodes ofabdominal pain persisted and eventually wereaccompanied by diarrhoea, with the passage of up toeight loose motions daily. Examination and sig-moidoscopy were always normal, though insufflationof the bowel with air sometimes reproduced his pain.Several barium meals and enema examinations andnumerous other investigations were normal, and avariety of treatments, including a milk drip during aperiod of inpatient investigations, were ineffective.
Studies on this patient were performed on twooccasions. On the first he had been free of symptomsfor several days and the colonic pressure response to
FIG. 6a. Patient no. 6. Pressure response of the left colonto prostigmine during remission.
prostigmine was not striking (Fig. 6a). The studieswere repeated several months later during a relapse.On this occasion right-sided abdominal pain beganin the postprandial period, but the pressure recordsfrom the sigmoid and rectum remained normal. Thepain spread to the left side following an injection ofprostigmine and this was accompanied by waveswith amplitudes exceeding 100 cm of water pressure(Fig. 6b). After intravenous propantheline the painwas relieved and the pressure activity abolished(Fig. 6c).
PATIENT NO. 7 A woman aged 58 suffered fromdiarrhoea for 20 years, becoming worse after anattack of gastroenteritis; the symptoms wereaggravated by fatty foods or fruit. She averagedabout six loose or watery motions daily with thepassage of mucus, but no blood, per rectum. Thediarrhoea was accompanied by lower abdominalpain which was worse before defaecation. She wasan anxious person with abdominal tenderness,especially on the left side. The rectal mucosa ap-peared oedematous at sigmoidoscopy, but biopsywas normal. Barium enema showed no evidence ofinflammatory disease of the colon, and otherrelevant investigations, including stool culture andlactose tolerance test, were normal.
25
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from

D. J. Holdstock, J. J. Misiewicz, and Sheila L. Waller
FIG. 6b.
FIG. 6c.FIGS. 6b and 6c. (b) Pressure response to the same dose ofprostigmine during relapse. High pressure waves in twoupper leads coincide with pain. Note change in pressure
scale. (c) Effect of 10 mg intravenous propantheline on theactivity in (b). Abolition of symptoms and of pressure
waves. (All the pressure waves in (c) are artefacts due tobody movement.) (R. sigmoid in this and remainingfigures indicates rectosigmoid.)
Her basal colonic pressure record was normal(Fig. 7a), but after a meal containing items of foodwhich sometimes upset her she developed markedleft-sided abdominal pain with an urge to defaecate.These symptoms coincided with the appearance onthe pressure record of waves at an increased fre-quency and amplitude (Fig. 7b). Following theinjection of prostigmine the severity of her symptomsincreased to such an extent that the test had to beterminated, and she passed five loose stools in thenext two hours.
PATIENT NO. 8 A 50-year-old naval surgeon hadrecurrent attacks of diarrhoea since an episode ofSonne dysentery during the war. The diarrhoea wasaccompanied by abdominal pain before each bowelmovement. All investigations, including bariumenema and repeated stool cultures, were negative.
Studies of colonic motor activity were performedduring a phase of active symptoms, when he waspassing up to five fluid motions daily. His basalpressure record was unusual, showing bursts ofactivity of high amplitude and frequency (Fig. 8a).These features became progressively more markedfollowing a meal (Fig. 8b), and the injection ofprostigmine (Fig. 8c); at no time were the wavespropulsive. Some of the pressure waves recordedreached the height of 97 mm Hg, which compareswith his blood pressure of 100/70 mm Hg. Despitethe active pressure record he had no abdominal painduring the period of study, although his bowels wereopened three times in the two hours afterwards.
PATIENT NO. 9 A 25-year-old girl suffered fromattacks of diarrhoea and lower abdominal painduring the previous four years. Symptoms beganfollowing the sudden death of her father. Amoebaewere said to have been found in the stools on oneoccasion, but previous specific antiamoebic chemo-therapy had no effect and extensive investigations ata specialist centre in this country showed no evidenceof amoebiasis. She was tender in the left iliac fossa;air insufflation during sigmoidoscopy precipitatedabdominal pain. At the time of the study she washaving up to six loose bowel movements daily.Her basal (Fig. 9a) and postprandial colonic
pressure records showed no unusual features, butafter subcutaneous prostigmine there was sustainedactivity, with waves up to 140 cm water (103 mm Hg)pressure: this compares with her arterial bloodpressure of 115/80 mm Hg. The waves were notpropulsive (Fig. 9b). In spite of this she felt no painat all, noticing only some gurgling in the lowerabdomen. There was no exacerbation of diarrhoeaafter the study.
26
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from

Observations on the mechanism ofabdominal pain
FIG. 7. Patient no. 7. Colonic pressurerecords: (a) basal; (b) 20 min after a mealwith left-sided abdominalpain and an urge todefaccate. High-frequency, high-pressuremotor activity in upper two leads.
FIG. 7a.
FIG. 7b.
27
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from

D. J. Holdstock, J. J. Misiewicz, and Sheila L. Waller
FIG. 8a.
Fio. 8b. FiG. 8c.FIG. 8. Patient no. 8. Colonic pressure records: (a) basal; (b) while eating, and (c) 12 min after prostigmine 0.75 mgintramuscularly. No symptoms, although high-frequency, high-pressure motor activity was present throughout. The wavesare not progressive.
28
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from

Observations on the mechanism ofabdominal pain
FIG. 9. Patient no. 9. Colonicpressure records: (a) basal; (b) 15min after prostigmine 0 75 mgintramuscularly. High pressurerapid waves produced nosymptoms; not progressive. Notechange ofpressure scale in uppertwo leads in (b).
FIG. 9a.
--. a.-
FiG. 9b.DISCUSSION
In this type of study assessment of pain must neces-sarily rely on subjective interpretation by the patient,and the normal range of intestinal response to thevarious stimuli used is not known. Nevertheless it
was felt that careful observation under standardconditions, combined with simultaneous measure-ments of intraluminal pressures, would result in ameaningful correlation between pain and motoractivity.
In all the nine patients described here abdominal
29
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from

D. J. Holdstock, J. J. Misiewicz, and Sheila L. Waller
pain was a prominent symptom. No organic diseaseof the small or large intestine was found, althoughthree patients (nos. 1, 2, and 3) had had previoussurgical procedures. Both postgastrectomy patientshad symptoms of dumping intermittently, but thesewere relatively mild and were absent during themanometric studies. Seven patients (nos. 1 to 7)developed typical attacks of abdominal pain duringthe manometric studies and in every case the symp-toms coincided with striking alterations in therecords of intraluminal pressure. Such alterationsoccurred in all the patients and were often the onlypositive finding on investigation.
Pain coincided with small intestinal pressureactivity in one of the patients with the postgastrec-tomy syndrome (patient no. 1) and in the patientwho had had a subtotal colectomy (patient no. 3).The other patient with the postgastrectomy syn-drome (no. 2) suffered from upper and lowerabdominal pain and in him changes in both smalland large intestinal motor activity were observed.Virtually nothing is known of the role of smallintestinal motor activity in the production ofabdominal pain in the absence of organic obstruc-tion. Horowitz and Farrar (1962) described twopatients in whom cramping pain coincided withbursts of jejunal pressure waves, and Connell et al(1965) found ileal hypermotility in one of theircases of postprandial abdominal pain. Many authorshave studied the motility of the small intestine duringdumping but no generally accepted conclusion hasemerged and attacks of dumping are not usuallyaccompanied by pain. Motor activity of the small;ntestine usually increases following the ingestion ofmeals, and distension of the intestine in animalsresults in the release of 5-hydroxytryptamine (5-HT)(Bulbring and Lin, 1958), which stimulates thehuman small bowel to contract, but inhibits themotor activity of the stomach and colon (Misiewicz,Waller, and Eisner, 1966). Since it is unlikely thatabdominal pain could result from relaxation ofsmooth muscle in the intestinal wall, it is possiblethat 5-HT could be used to localize the site of originof abdominal symptoms to the small intestine insome patients. In this context it is interesting thatintravenous 5-HT precipitated pain in patient no. 1.
In five patients (nos. 2 and 4 to 7) the onset ofabdominal pain coincided with a marked increasein the motor activity of the colon after a meal or aninjection of prostigmine. Two further patients(nos. 8 and 9) showed similar changes in colonicpressure but remained symptom-free. Of these sevenpatients, five had the irritable bowel syndrome,whilst the other two suffered from the post-dysentericbowel syndrome and postgastrectomy syndromerespectively (Table I).
Patients with the irritable bowel syndrome oftenshow a much greater increase of pressure in thedistal colon after food or prostigmine than donormal subjects (Chaudhary and Truelove, 1961;Wangel and Deller, 1965). Excessive pressureresponse was especially marked in the presence ofsymptoms (Chaudhary and Truelove, 1961), andthis is confirmed in our two patients (nos. 5 and 6)who were studied on separate occasions whensymptom-free and in relapse. Connell et al (1965)described in detail 12 patients with hypermotility ofthe pelvic colon associated with postprandialabdominal pain.The question arises as to how excessive motor
activity of intestinal smooth muscle can cause painin the absence of organic obstruction. Observationsmade at laparotomy under local anaesthesia indicatethat the intestine is sensitive only to distension, andrapid distension of a balloon in the small intestinecauses pain (Rowlands, 1952). It has been suggestedthat the pressure waves recorded from the coloniclumen represent dissociated segmenting contrac-tions which delay rather than accelerate the transitof colonic contents (Connell, 1962). Simultaneouscineradiography and pressure recording shows thatpressure waves can occur without movement ofcontents and vice versa (Ritchie, Ardran, and True-love, 1962). Excessive segmenting activity mightthus create a functional obstruction and cause painby distension of bowel proximal to the hyperseg-menting segment (Connell et al, 1965). However,the evidence (Connell, 1962; Wangel and Deller,1965) for a delaying effect of colonic pressure wavesis not conclusive and in five of our patients withmarked colonic activity diarrhoea, as well as pain,was a prominent symptom. It could be argued thatin the two patients (nos. 8 and 9) with excessivecolonic activity but no pain the recorded waves werepropulsive but there is no evidence of this on carefulinspection of the records. In the other patients it isdifficult to accept that pain due to functionalobstruction produced by hypersegmentation waspresent simultaneously with diarrhoea due toincreased propulsive activity.
If the hypothesis that pain is due to hyperseg-mentation causing functional obstruction is correct,the abnormal motor activity might well be focalrather than generalized. Circumstantial evidence infavour of the focal nature of abnormal colonicmotor function is provided by the clinical observa-tion that pain in the irritable colon syndrome isoften well localized to the left iliac fossa and that,as far as is known, the muscle abnormality indiverticular disease of the colon is limited to thesigmoid (Morson, 1963). Some further support forthis concept is provided by the present results. In
30
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from

Observations on the mechanism ofabdominalpain 31
two patients (nos. 3 and 4) rectal records werenormal, but at the same time small intestinal motoractivity in one (no. 3) and upper sigmoid activityin the other patient (no. 4) coincided with bouts ofpain. Another patient (no. 2) had pain coincidingwith high-amplitude pressure waves in the rectum,and synchronous pressure waves were recorded fromthe sigmoid lead but at a much lower amplitude,whilst a simultaneous record from the ileum wasnot abnormal (Fig. 2a). In patient no. 4 spasm ofthe sigmoid prevented the insertion of tubes to theirfull extent and pressures thus recorded were normal,whilst pressure records obtained from beyond thereach of the sigmoidoscope were judged to show anexcessive response (Fig. 4). It must be admitted,however, that knowledge of the extent of spread ofmotor abnormalities during bouts of pain is meagre,and the changes observed in patient no. 6 suggestthat they may progress from the proximal to thedistal colon.The often disappointing results of treatment with
oral propantheline and similar drugs in the clinicalmanagement of such cases are presumably due tothe difficulty of obtaining adequate dosage withoutintolerable side-effects. A trial of self-administeredsubcutaneous injection of propantheline in patients1 and 2 was unsuccessful for the same reason. How-ever, in the four patients given intravenous propan-theline, the simultaneous relief of pain and cessationof pressure activity were impressive, suggesting arelationship between symptoms and motor activity.On the other hand, the present results do not supportthe conclusion that this relationship is simple,because two patients (nos. 8 and 9), whose recordswere qualitatively similar to others in this study,remained free of pain throughout their tests, despitethe fact that pain was a feature of their illness. Inthese two patients the intraluminal pressures ap-proached the level of the arterial blood pressure,making it unlikely that ischaemia of the bowel wallis an important factor in the production of this typeof abdominal discomfort. Individual variations insensitivity to painful stimuli and in the threshold ofawareness to visceral sensations undoubtedly playa part, but are difficult to measure objectively. Forexample, it was our impression that patient no. 2was unusually aware of his visceral sensations andhad a low pain threshold, but that these featureswere much less marked in patient no. 1.
SUMMARY
Intraluminal pressures were measured in the smallor large intestine of nine patients suffering from re-current attacks of severe abdominal pain, for whichno cause was found after extensive investigation.
Abdominal pain was correlated with pressurechanges in the small or large intestine in sevenpatients; two patients remained symptom-freedespite excessive pressure activity.The relationship between abdominal pain and
intraluminal pressures is discussed in the light ofthese findings.
We are grateful to Dr F. Avery Jones and Dr T. D.Kellock, Central Middlesex Hospital, and Dr G. Watkin-son, York County Hospital, for allowing us to studypatients under their care, and to Dr Alan Young, StMark's Hospital, London, for radiological studies onpatients 4 and 5. We thank Mrs Moira Black for muchtechnical assistance and Mr A. Booker, F.P.S., of thePhotographic Department, Central Middlesex Hospital,for the illustrations.
REFERENCES
Atkinson, M., Edwards, D. A. W., Honour, A. J., and Rowlands,E. N. (1957). Comparison of cardiac and pyloric sphincters.A manometric study. Lancet, 2, 918-922.
Builbring, E., and Lin, R. C. Y. (1958). The effect of intraluminalapplication of 5-hydroxytryptamine and 5-hydroxytryptophanon peristalsis; the local production of 5-HT and its release inrelation to intraluminal pressure and propulsive activity.J. Physiol. (Lond.), 140, 381-407.
Chaudhary, N. A., and Truelove, S. C. (1961). Human colonicmotility: a comparative study of normal subjects, patients withulcerative colitis, and patients with the irritable colon syndrome.I. Resting patterns of motility. II. The effect of prostigmin.III. Effects of emotions. Gastroenterology, 40, 1-36.
Connell, A. M. (1959). Intraluminal pressures in the pelvic colon.Proc. roy. Soc. Med., 52, suppl., pp. 69-72.
(1962). The motility of the pelvic colon. II. Paradoxical motilityin diarrhoea and constipation. Gut, 3, 342-348.
-, Jones, F. A., and Rowlands, E. N. (1965). Motility of the pelviccolon. IV. Abdominal pain associated with colonic hyper-motility after meals. Ibid., 6, 105-112.
-, McCall, J., Misiewicz, J. J., and Rowlands, E. N. (1963).Observations on the clinical use of radio pills. Brit. med. J.,2, 771-774.
Horowitz, L., and Farrar, J. T. (1962). Intraluminal small intestinalpressures in normal patients and in patients with functionalgastrointestinal disorders. Gastroenterology, 42, 455-464.
Misiewicz, J. J., Connell, A. M., and Pontes, F. A. (1966). Comparisonof the effects of meals and prostigmine on the proximal anddistal colon in patients with and without diarrhoea. Gut, 7,468-473.Waller, S. L., and Eisner, M. (1966). Motor responses ofhumangastrointestinal tract to 5-hydroxytryptamine in vivo and invitro. Ibid., 7, 208-216.- , Fox, R. H., Goldsmith, R., and Hunt, T. J. (1968). Theeffect of elevated body temperature and of stress on the motilityof stomach and colon in man. Clin. Sci., 34, 149-159.
Morson, B. C. (1963). The muscle abnormality in diverticular diseaseof the sigmoid colon. Brit. J. Radiol., 36, 385-392.
Ritchie, J. A., Ardran, G. M., and Truelove, S. C. (1962). Motoractivity of the sigmoid colon of humans. A combined study byintraluminal pressure recording and cineradiography. Gastro-enterology, 43, 642-668.
Rowlands, E. N. (1952). Gastrointestinal motility in man. Functions ofextrinsic nerves. In Modern Trends in Gastroenterology, Series I,edited by F. Avery Jones, pp. 548-549. Butterworth, London.
, and Wolff, H. S. (1960). The radio pill. Telemetering from thedigestive tract. Brit. Commun. Electron., 7, 598-601.
Wangel, A. G., and Deller, D. J. (1965). Intestinal motility in man.III. Mechanisms of constipation and diarrhoea with particularreference to the irritable colon syndrome. Gastroenterology,48, 69-84.
on Decem
ber 29, 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.10.1.19 on 1 January 1969. Dow
nloaded from


















