
Objectives Understand the basics of pediatric ophthalmology. Define the role of a pediatric...
52
Pediatric ophthalmology, strabismus and amblyopia Dr Mahmood Fauzi ASSIST PROF OPHTHALMOLOGY AL MAAREFA COLLEGE
-
Upload
laureen-poole -
Category
Documents
-
view
215 -
download
1
Transcript of Objectives Understand the basics of pediatric ophthalmology. Define the role of a pediatric...

Pediatric ophthalmology, strabismus and amblyopia
Dr Mahmood FauziASSIST PROF OPHTHALMOLOGY
AL MAAREFA COLLEGE

Objectives • Understand the basics of pediatric ophthalmology. • Define the role of a pediatric ophthalmologist.• Rationalize why children need a different structure for eye care.• Justify the Importance of pediatric vision screening• Review normal ophthalmic milestones.• Outline basic techniques for examining child's eye’s .• Outline age specific screening and Newer pediatric vision screening
technology.• Describe select pediatric ophthalmic conditions -Refractive errors, cataract,
coloboma, retinoblastoma, retinopathy of prematurity. • Describe etiology, risk factors, presentation ,diagnoses and management for
amblyopia and strabismus

Basics of Pediatric ophthalmology
• What is Pediatric ophthalmology?• It is a sub-speciality of ophthalmology concerned with eye
diseases, visual development, and vision care in children.
• What is the Role of Pediatric ophthalmologists?• They focus on the development of the visual system and the
various diseases that disrupt visual development in children.• Pediatric ophthalmologists also have expertise in managing the
various ocular diseases that affect children. Pediatric ophthalmologists are qualified to perform complex eye surgery as well as to manage children's eye problems using glasses and medications.

Children are Different & need a different structure for eye care
• Developing cortical connections• Window of opportunity for diagnosis and
treatment…just like with language development

Ophthalmic Milestones
• 30 weeks - Blink to light• 31 weeks - Pupils react• 2 to 3 weeks - Early fixation• Horizontal gaze - Birth• Vertical - 2 months• Fixate - Birth to 3
months• Follow - 3 months
• Color ? (3 months)
• Six Months Visual acuity 20/30–20/40 Binocularity well developed
• Field – Adult-like 1 year

Basic Techniques for Examining Children’s Eyes
• Age specific• Start with HISTORY– Moms are great
diagnosticians!• Common EXAM
components – Assessment of vision– External anatomy– Pupil function– Motility– Ocular fundus/Red
Reflex testing

Ocular History
• Does child appear to see well distance and near?• Any crossing?• Family history of eye disorders?• Recurrent discharge or redness?• Extreme photophobia?• NOT to worry about:– “Sits close to TV a lot”

External Examination
• Are eyelids symmetric?
• Pupil symmetry?
• Any redness, inflammation, or discharge?
• Cornea clear?
• Are the eyes aligned?

Pupil Exam
• Are the pupils round?
• Symmetric?
– If asymmetric, is it more asymmetric in dark or light?
• Reactive to light?

Motility Assessment
• Is the pupil light reflex central?
• Do the eyes move fully in all directions?
• Pseudostrabismus vs. true strabismus

Vision Assessment• Infants: Eye contact, follows face, smiles
• Toddlers: Cover each eye and follows objects (fix and follow)
• Verbal: Visual acuity screening with appropriate optotype (symbol/letters)
AAPOS Vision Screening Kit

Child abuse is a significant social problem which is associated with a high morbidity and mortality. “Shaken Baby Syndrome” (SBS) is one form of physical child abuse, a non-accidental traumatic brain injury. In 6% of reported cases of child abuse, an ophthalmologist is responsible for initially recognizing the abuse. Perhaps the greatest diagnostic clue is
a detailed history that is incompatible with the extent and severity of the injuries found on dilated fundus exam.

Newer / improved Pediatric Vision Screening Technology
• Photoscreening• Automated refractors• VEP screening• Retinal birefringence

The Importance of Pediatric Vision Screening
• Amblyopia affects up to 5% of thepopulation (>10 million Americans).
• In the first 4 decades of life amblyopiacauses more vision loss than all otherocular diseases combined!
• Amblyopia has a “window period” for treatment in early childhood.
• Screening can prevent otherwise fatal disorders such as retinoblastoma.

Periodicity Table for ScreeningPeriodicity Schedule for Visual System Assessment in Infants and Children
Newborn to 6 months
6 months to 12 months
1 to <3 years 3 to < 5 years 5 years and older
Ocular History x x X x x
External inspection of lids and eyes
x x x x x
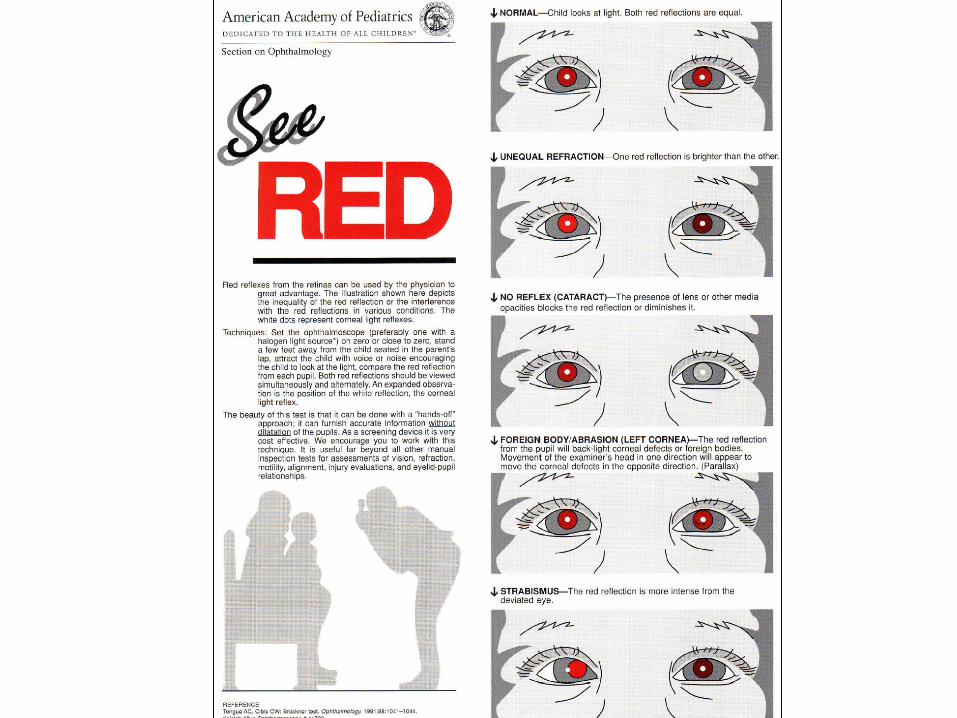
Red Reflex Testing x x x x x
Pupil examination x x x x
Ocular Motility Assessment x x x x
Instrument Based Screening x+
x+
*
Visual Acuity Fix and follow x x
Visual Acuity age-appropriate optotype assessment
x∆
x∆
+: Bill using CPT 99174∆: Bill using CPT 99173*: If unable to test visual acuity monocularly with age appropriate linear optotypes, instrument-based screening is suggested.
Age Specific Screening: NEWBORN
• External evaluation for obvious ocular malformations and infections– NOTE: Too young to evaluate alignment!!!
• RED REFLEX TEST—preferably prior to discharge from newborn nursery– Very important to r/o retinoblastoma or
congenital cataracts• If congenital cataracts not removed in first 2 to 3
months of life, permanent loss of sight occurs

Bruckner Reflex

Leukocoria is an Urgency! Diff Dx include cataract, glaucoma, PHPV,
Retinoblastoma, Retinal detachment, etc. In addition to sending a consult, CALL
ophthalmologist to make sure the patient is seen ASAP!

SELECT PEDIATRIC OPTHALMIC CONDITIONS
Pediatric Refractive Errors
• Nearsighted• Farsighted• Astigmatism• Anisometropia

Myopia (Near-sightedness)
Eyeball too long Can’t see far away Correct with specs,
contact lens, or excimer laser (older children)

Hyperopia (Far-sightedness)
The eyeball is too short “Accommodation” will
increase the effective lens power in the eye and focus at both near and far
Crossing may occur
GlassesAccommodation

Astigmatism
“Warpage” of the cornea like a football
Light rays in one axis are not focused the same as in opposite axis
Corrected with glasses

Congenital cataract refers to a lens opacity present at birth. Congenital cataracts cover a broad spectrum of severity: whereas some lens opacities do not progress and are visually insignificant, others can produce profound visual impairment.

Coloboma (from the Greek koloboma, meaning defect, is a hole
in one of the structures of the eye, such as the iris, retina, choroid, or optic disc. The hole is present from birth and can be caused when a gap called the choroid fissure, which is present during early stages of prenatal development, fails to close up completely before a child is born.

Retinoblastoma (Rb) is a rapidly developing cancer that develops from the immature cells of a retina, the light-detecting tissue of the eye and is the most common malignant tumor of the eye in children . The most common and obvious sign of retinoblastoma is an abnormal appearance of the pupil, leukocoria, also known as amaurotic cat's eye reflex
Leucokoria Cross eye

Retinopathy of prematurity (ROP) or Terry syndrome, previously known as retrolental fibroplasia (RLF), is a disease of the eye
affecting prematurely-born babies generally having received intensive neonatal care, in which oxygen therapy is often used and advantageous. It is thought to be caused by disorganized
growth of retinal blood vessels which may result in scarring and retinal detachment. ROP can be mild and may resolve spontaneously, but it may lead to blindness in serious cases. As such, all preterm babies are at risk for ROP, and very low birth weight is an additional risk factor. Both
oxygen toxicity and relative hypoxia can contribute to the development of ROP.
Dragged optic disc of ROP

Amblyopia
The Physician sees nothing and the Patient very little
What is Amblyopia?
Unilateral or bilateral decrease of visual acuity caused by form vision deprivation
and/or
Abnormal binocular interaction for which no organic cause can be detected

Amblyopia…In Other Words:
• The camera (eye) is capable of taking the picture but the computer (brain) doesn’t recognize that there is an image.
• “Either use it or lose it!”

Screen for Causes of Amblyopia
• Refractive errors• Obstruction of optical pathway (e.g. cataract
or corneal scar)• Strabismus• Other—anything that blocks input of
visual information to the brain
Remember in the pre-verbal child, the only way to detect amblyopia is to indirectly detect the risk factors.
(Refractive errors, Media opacities, Strabismus)

Treatment Amblyopia
• The clinician must first rule out an organic
cause and treat any obstacle to vision (eg,
cataract, occlusion of the eye from other
etiologies).
• Remove cataracts in the first 2 months of
life, and aphakic correction must occur
quickly
• Treatment of anisometropia and refractive errors must occur next
• The next step is forcing the use of the amblyopic eye by occlusion therapy

STRABISMUS• occurs when both eyes do not look at the same place at
the same time; the eyes are unable to align properly under normal conditions
• eye(s) may turn in, out, up, or down
• can be present in one or both eyes
• often referred to as: cross-eyed, crossed eyes, cockeye, weak eye, wall-eyed, wandering eyes, and/or eye turn

CAUSES OF STRABISMUS• lack of coordination between the muscles of the eye
responsible for eye movement and keeps both eyes from gazing at the same point
• problems with the nerves that transmit information to the eye muscles
• problems with the control center in the brain that directs eye movement
• in adults, can be caused by stroke, thyroid problems, brain injury, or other trauma
RISK FACTORS
• family
• refractive errors—extreme farsightedness (hyperopia) can develop strabismus due to the amount of eye focusing necessary to keep vision clear
• medical conditions—Down syndrome ,cerebral palsy ,stroke or head injury
from: Strabismus.com

TYPES OF STRABISMUS• Esotropia—inward turning of the eye
• Exotropia—outward turning of the eye
• Hypertropia—upward turning of the eye
• Hypotropia—downward turning of the eye
from: American Optometric Association
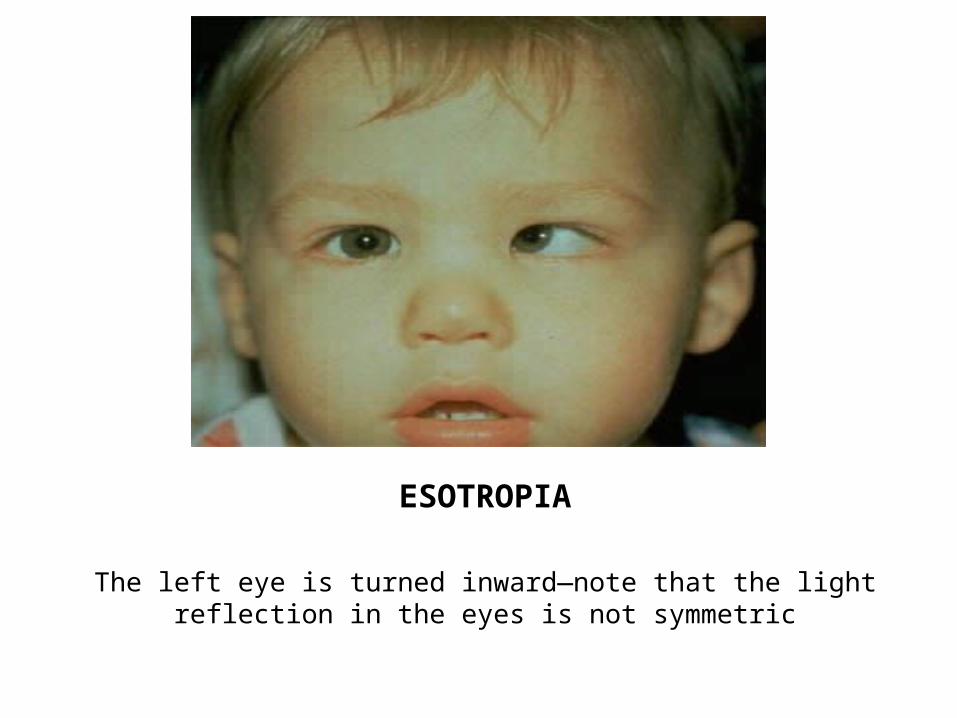
ESOTROPIA
The left eye is turned inward—note that the light reflection in the eyes is not symmetric

EXOTROPIA
The right eye is turned outward—again, not the light reflection in the eyes is not symmetrical

HYPERTROPIA
The right eye is turned upward—light reflection not symmetrical

HYPOTROPIA
The right eye is turned downward-light reflection in eyes is not symmetric

WHEN DOES IT OCCUR?
• congenital—developing during infancy; 50% of children with strabismus are born with it
• acquired—developing in adulthood
from: Strabismus.com

DIAGNOSIS•A comprehensive eye exam is necessary with
focus on the following:
•patient history•visual acuity•refraction•alignment and focusing•eye health exam
from: American Optometric Association

TREATMENT• there is no cure for strabismus
• with treatment, the effects of strabismus may be corrected
• the goal of treatment is to help the patient achieve as close to normal binocular vision as possible in every direction of gaze and at all distances

TREATMENT
Eye Patch
The stronger eye is patched to force the brain to interpret images from the strabismic eye. Eye patches will not change the angle of the strabismus. Typically, eye patching is used only if amblyopia is present.

TREATMENTEyeglass or
Contacts
Eyeglasses or Contacts are used to improved the positioning of the eye(s) by modifying the patient’s reaction to focus. Eyeglasses and Contacts can also redirect the line of sight, which can help straighten the eye.

TREATMENT
Prisms
Prisms are used to modify the way light and images hit the eye. The lenses provide comfort and can help prevent double vision from developing.

TREATMENTVision Therapy
A non-surgical method of therapy that treats the eye and the brain. An optometrist will oversee the therapy, which is designed to strengthen or develop visual skills. The optometrist may also use eyeglasses, prisms, eye patches and computerized medical devices during the therapy.

TREATMENTEye Surgery
Surgery may be necessary in an attempt to align the eyes by modifying one or more muscles in the eye. During surgery, the muscle positions will be changed or the length of the muscles will be changed. Surgery may follow a period of eye patching and then eyeglasses may be used after surgery to help treat strabismus.
Surgery on medial rectus muscle of the left eye.
UN- CONVENTIONAL-ALTERNATIVES

Primary care physicians are our
best line of defense for preventable
blindness!


















