OBEWS and MFTI - Synova Associates
16
10/3/2018 1 * * *I have nothing to disclose * Objectives for OBEWS: Define OBEWS Barriers to effective communication Goals of OBEWS Overview of criteria for scoring Identify the benefits of OB EWS * Objectives for MFTI: Define triage Benefits of standardized approach Explain the use of MFTI
Transcript of OBEWS and MFTI - Synova Associates

10/3/2018
1
*
*
*I have nothing to disclose
*Objectives for OBEWS:
Define OBEWS
Barriers to effective communication
Goals of OBEWS
Overview of criteria for scoring
Identify the benefits of OB EWS
*Objectives for MFTI:
Define triage
Benefits of standardized approach
Explain the use of MFTI

10/3/2018
2
*
*
*
Patient
Medical Staff
Nursing
Any Unit Specific
Staff members
Unit Secretary
Scrub Tech
10/3/2018
3
*Working Conditions
*Resources
*Team Composition
*
OB EWS Goals
Assist the bedside clinician with recognition of critical signs and
symptoms that a patient’s condition may be deteriorating
Increase escalation of patient’s potential worsening condition
Timely attendance to patient’s needs; theoretically reducing the
need for escalation in the emerging condition
*
A method of using routine physiological
measurements to identify maternal patients
who may be at risk for a decline in condition
or potential emergency and provides a
standards assessment and notification process
that prompts healthcare providers when
action is necessary.

10/3/2018
4
*
*Question data more effectively
*Respond with purpose and prepare for crisis
*Trigger tools are designed to encourage staff to
question parameters and critically think at the
bedside
*
*Reduction in clinical incidents
*Reduce patient LOS
*Higher Quality of Care
*Improved Outcomes
*Improved Patient Experience
*Lower nurse turnover
*
*Documentation is
required by nursing
staff every 4 hours or
with change in patient
condition regardless of
patient location.
*OBEWS applies to all
pregnant patients up
to 42 days postpartum.

10/3/2018
5
*
*Respiratory rate
*Heart rate
*Systolic BP
*Diastolic BP
*Temperature
*Pulse Oximetry
*LOC
*Urine output
*Fetal Heart rate
*Uterine activity
*Bleeding
*History of cesarean
section
*Gestational age
*
*
*Think and act
to the
situation
rather than
react to it.
the objective analysis and
evaluation of an issue in order to
form a judgment

10/3/2018
6
*
*Action plan is a guideline for
caring for your patient
*Action plans are NOT to replace
individual patient assessments
*Do NOT ignore the entire
clinical picture
*
*
*Artificial high scores
*Multiple charting systems
*Compliance of timing
*Other tools worth
evaluating

10/3/2018
7
* Supports safe clinical practice
* Provide opportunity for prompt response to patient score through
critical thinking
* Prevent further deterioration and delay of care
* Develop effective management plans and communicate effectively
* Reduce overall clinical risk
*
*
* RN evaluates patient, FHT
and calls provider
* Instructions/orders by
phone
* 24/7 physician coverage
* Reduced malpractice risk
* RN satisfaction: reduced turnover
* Provider satisfaction
* Patient satisfaction
* Reduced wait times and physician led care.
*

10/3/2018
8
*
Obstetric triage is the brief, thorough and
systematic maternal and fetal assessment
performed when a pregnant woman presents for
care to determine priority for full evaluation.
*
*Antenatal transfer is
associated with improved
neonatal outcomes
compared with neonatal
transfers.
EMTALA requirements relative to obstetric care-
1. Qualified medical person must perform an MSE to determine if the patient has a medical emergency; should include health of the women and the fetus.
2. Stabilize and/or transfer where the benefits outweigh the risk of transfer.
3. When necessary arrange transfer; patient may decline after being informed of risk/benefits of transfer.
4. MSE cannot be delayed to inquire about payment.
*No method to provide
consistent feedback to
clinicians compromised
patient safety and quality of
care
*
10/3/2018
9
*
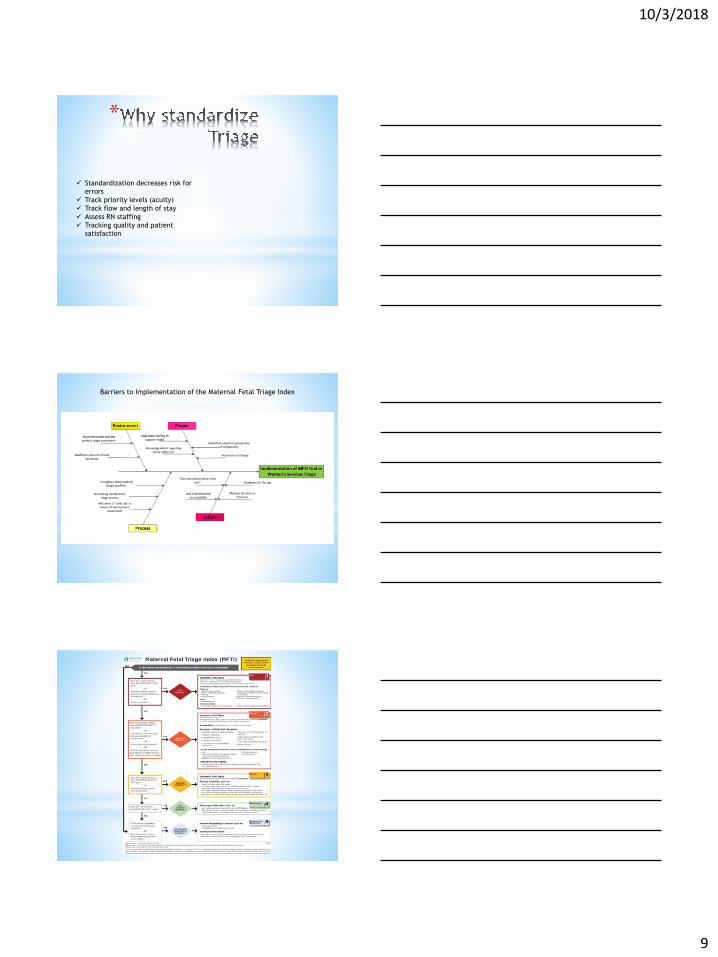
Standardization decreases risk for
errors
Track priority levels (acuity)
Track flow and length of stay
Assess RN staffing
Tracking quality and patient
satisfaction
Barriers to Implementation of the Maternal Fetal Triage Index

10/3/2018
10
*
o Use the first set of vitals
o FHR by auscultation or electronic fetal
monitoring
o Pulse oximetry
o PAY ATTENTION
All vital signs need to be assessed including
temperature. It has been shown that lack of
attention to abnormal vitals have a higher risk of
maternal death from preventable causes.
*
*With Contractions:
Coping is assessed
rather than using the
pain scale
*Pain unrelated to
contractions:
Use pain scale of 0-10
10/3/2018
11
*
*Urgency for assessment is based on relevant
history, high risk situations and need for
transfer
*Cervical exam is not included in the MFTI
*MFTI does not alter infectious disease control
processes for triage
*
*Does the woman or fetus have STAT vitals?
*Does mom or fetus require lifesaving intervention?
*Is birth imminent?
*
*Maternal HR <40 or >130
*Apneic
*SpO2 <93%
*SBP ≥ 160 or DBP ≥ 110 or <60/palpable
*No FHR detected by Doppler (unless previously
diagnosed fetal demise
*FHR <110bpm for >60 seconds

10/3/2018
12
*
*Urgent or priority 2 vitals?
*Severe pain w/o contractions?
*High risk situation?
*Will mom or newborn require higher level of care?
*
*Abnormal vital signs
oMaternal HR >120 or <50
oTemperature ≥ 101.0F (38.3C), R>26 or <12, SpO2
<95%,
oSBP ≥ 140 or DBP ≥ 90, symptomatic Or <80/40,
repeated
oFHR >160 bpm for > 60 seconds; decelerations
SEVERE PAIN: (no ctx) ≥ 7 on a 0-10 pain scale
*
- UNSTABLE HIGH RISK MEDICAL CONDITIONS
- DIFFICULTY BREATHING
- ALTERED MENTAL STATUS
- SUICIDAL/HOMICIDAL
- <34 weeks c/o detectable, uterine ctx
- <34 weeks c/o SROM/ leaking/spotting
- Active vaginal bleeding
- c/o decreased fetal movement
- Recent trauma

10/3/2018
13
*
-≥ 34 weeks with regular ctx, or SROM/leaking
with any of the following:
- HIV +
- Multiple gestation
- Planned, medically indicated cesarean
- Placenta Previa
- Breech or other malpresentation
- Active herpes
*
*Does the woman have priority 3 vital signs?
oTemperature >100.4F (38.0C)
oSBP ≥ 140 or DBP ≥ 90, asymptomatic
OR
*Does the women require prompt attention
*
*Signs of active labor ≥ 34 weeks
*c/o early labor signs and/or complaints of SROM/leaking 34-36.6 weeks
*≥ 34 weeks with regular ctx and HSV lesion
*≥ 34 weeks planned, elective, repeat cesarean w/ regular ctx
*≥ 34 weeks multiple gestation pregnancy with irregular ctx
*Woman is not coping with labor (per the Coping with Labor Algorithm v2©)

10/3/2018
14
*
*
*A complaint that is non urgent
o≥ 37 weeks early labor and/or SROM/leaking
oNon-urgent symptoms: common discomforts,
vaginal discharge, constipation, ligament pain,
nausea, anxiety
*
*Requesting service: NO COMPLAINT
*Scheduled procedure: NO COMPLAINT
oPrescription refills
oOutpatient service
oAny scheduled event formally or informally
NST
Version
Steroids

10/3/2018
15
*
Executive, administrative and clinical leadership
essential for implementation and sustainability
• Frontline team engagement imperative
• Don’t underestimate technological challenges
• It’s not all black and white
*
References:
1. American Academy of Pediatrics & American College of Obstetricians and Gynecologists
(2012). Guidelines for perinatal care (7th ed.). Washington, DC: Author.
2. American College of Obstetricians and gynecologists (2009). Intrapartum fetal heart rate
monitoring, nomenclature, interpretation and general management principles (ACOG Practice
Bulletin No. 106) Washington, D.C.
3. Association of Women’s Health Obstetric and Neonatal Nurses. (2009). Fetal heart monitoring
principles and practices (4th
ed.) Washington, DC: Author.
4. Cherouny PH, Federico FA, Haraden C, Leavitt Gullo S, Resar R. Idealized Design of Perinatal
Care. IHI Innovation Series white paper. Cambridge, MA: Institute for Healthcare Improvement;
2005. (Available on www.IHI.org)
5. Clark SL, Belfort MA, Byrum SL, et al. Improved outcomes, fewer cesarean deliveries, and
reduced litigation: results of a new paradigm in patient safety. American Journal of Obstetricians
and gynecologists, 2008;199:105.e1-105.e7.
6. Doyle, J., Kenny, T. H., Burkett, A. M., & von Gruenigen. (2011). A performance improvement
process to tackle tachysystole. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 40, 512–
519.
7. Nolan T, Resar R, Haraden C, Griffin FA. Improving the Reliability of Health Care. IHI
Innovation Series white paper. Boston: Institute for Healthcare Improvement; 2004. (Available
on www.IHI.org)
8. Merriel, A. Van der Nelson, H., Merriel, S., Bennett, J., Donald, F., Draycott, T., Siassakos, D.
(2015). Idnetifying deteriorating patients through multidisciplinary team training. American
Journal of Medical Quality.
9. Shields, L.E., Wisener, S., Klein, C., Pelletreau, B., and Hedriana, H.L. (2016). Use of maternal
early warning trigger tool reduces maternal morbidity. American Journal of Obstetricians and
Gynecologists, 2(1): 1-6.
10. Thorpe-Gardner, J., Love, N., Wrightson, J., Walsh, S. and Keeling, A. (2006). The value of
modified early warning score in surgical patients: a prospective observational study. Annals of
the Royal college of Surgeons of England, 88(6): 571-575.
11. The National Institute of Child Health and Human Development Workshop Report on Electronic
Fetal Heart Monitoring: Update on Definitions, Interpretation, and Research Guidelines (2008).
American Journal of Obstetricians and gynecologists, 112 (3), 661-666.
12. The National Institute of Child Health and Human Development Workshop Report on Electronic
Fetal Heart Monitoring: Update on Definitions, Interpretation, and Research Guidelines (2008).
Journal of Obstetrics, Gynecology and Neonatal Nursing. 37, 510-515.
13. Carle C1, Alexander P, Columb M, Johal J. 2013 Design and internal validation of an obstetric
early warning score: secondary analysis of the Intensive Care National Audit and Research
Centre Case Mix Programme database. Anaesthesia. Apr;68(4):354-67
14. Quinn AC1, Meek T, Waldmann C. 2016 Obstetric early warning systems to prevent bad
outcome Current Opinion Anaesthesiology. Jun;29(3):268-72.
15. Isaacs RA1, Wee MY, Bick DE, Beake S, Sheppard ZA, Thomas S, Hundley V, Smith GB, van
Teijlingen E, Thomas PW; Members of the Modified Obstetric Early Warning Systems Research
Group. 2014. A national survey of obstetric early warning systems in the United Kingdom: five
years on. Anaesthesia. Jul;69(7):687-92

10/3/2018
16
References
American college of obstetricians and gynecologists' committee on obstetric practice . (2016). Hospital-based triage of obstetric patients. Committee Opinion No.667. ACOG.
University of Utah College of Nursing and University of Utah Hospital & Clinics.
(n.d.). Birth tools . Retrieved June 29, 2018, from Coping with labor algorithm v2:
http://www.birthtools.org/birthtools/files/ccLibraryFiles/Filename/000000000067/Co
ping_Algorithm.pdf
Ruhl, C., Scheich, B., Onokpise, B., & Bingham, D. (2015). Content Validity Testing of the Maternal Fetal Triage Index. JOGNN, 701-716.