A Gyimesek növényzete, a gyimesiek növényzetismerete Molnár Zsolt és Babai Dániel
description

Nutrition on the ICU
Zsolt Molnár
AITI

Basics
• Artificial nutrition
• Energy requirement:• 25-30 kcal/kg/day• Carbo-hydrates: 50-70%• Fat: 15-30 %• Proteins: 10-20% (1.2-1.5 g/kg/day amino acids)• Vitamins, trace elements
• Routes• Enteral• Parenteral

Routes

Patient satisfaction
„That tube went all the way to my stomach - and they put it in while I was conscious - nice! Made me feel better though ;-)”

What’s new? – 25 years of experience
• Better tools
• „All-in-one” preparations
• Glutamin
• Blood sugar controll
Wernerman J. In: 25 Years of Progress and Innovation in Intensive Care Medicine 2007

After 4 weeks of MSOF…

Blame/self blame?
≠

Introduction
• Feeding phylosophy 25 years ago• „Bigger is better” - „hyper-alimentation”
Wernerman J. In: 25 Years of Progress and Innovation in Intensive Care Medicine 2007
• Theoretical basis• Nitrogen balance
Munro HN, et al. Biochemical aspects of protein metablism, New York and London. Academic Press 1963
• Practical proof• High measured energy expenditure
Wilmore DW. The Metabolic Management of the Critically Ill. New York and London: Plenum Medical Books 1977

„Under-”, and „Overfeeding”
• Under feeding: – Prolonged ICU stay– Prolonged ventilation– Higher incidence of infection
Villet S, et al. Clin Nutr 2005; 24: 502-9Rubinson L, et al. Crit Care Med 2004; 32: 350-7
• Over feeding:– Prolonged ICU and hospital stay– Nausea, vomiting– Hyperlipidaemia, hyperglicaemia
Stapleton RD, et al. Proc AmThorac Soc 2006; 3: A737

PN - indications
• Not functioning or severely disabled GI-tractASPEN Task Force. J Parenter Enteral Nutr 2002; 26: 1SA–138SA
• EN contraindicated or <40% energy/5 days• Ethically acceptable: life expectancy ≥14 days
Nardo P, et al. Clin Nutr 2008; 27: 858-64
• Timing• ASAP: EN + PN after admission/surgery
Heidegger CP, et al. Curr Opin Crit Care. 2008; 14: 408-414

PN + adjuvant treatment
• Immuno-nutrition (glutamin)• Improved survival
Goeters C, et al. Crit Care Med 2002; 30: 2032-2037Griffiths R, et al. Nutrition 1997; 13: 295-302
• SafeBerg A, et al. In: Yearbook of ICEM 2009; pp: 705-715
• Water-, and lipid-soluble vitamins: 1 amp/day• Trace elements: 1 amp/day
Nardo P, et al. Clin Nutr 2008; 27: 858-64

Calory intake
How much?

Assessment
• Harris-Benedict formula• Gender, age, weight, height• Compensation factor
Long CL et al. JPEN 1979; 3: 452–6
• Ireton-Jones • Age, weight, gender, + burn + trauma
Ireton-Jones CS, et al. J Burn Care Rehabil 1992;13:330–3
• Frankenfield• Minute ventilation, Hb, Sepsis
Frankenfield DC, et al. J Trauma 1994;18:398–403
• Fusco• Age, height, weight
Fusco MA, et al. JPEN 1995;19(suppl):18S

Measurements
• Indirect calorimetry• O2 uptake/ CO2 production• „Gold standard”
Feurer I, et al. Nutr Clin Pract 1986;1:43–9
• Fick’s principle • PA-catheter• CO, Ca-vO2
Liggett SB, et al. Chest 1987;91:562–6

Assessment – shortcomings
• Harris-Benedict, Ireton-Jones, Frankenfield, Fusco• EE increases:
– Fever, shivering– Work of breathing– Pain, stress, physio, „realtives”, stb– Sepsis– Catecholamines
• EE decreases:– Hypothermia– Sedation, anaesthesia– IPPV/CPAP– MOF
McClave SA, et al. Nut Pract 1992; 9: 61-8
Only the patient is missing

Measurements – shortcomings
• Indirect calorimetry• Complicated, time consuming, expensive• Seal, FiO2<60%, „steady state” 60-120 minutes (!)• Snapshot only
Browning JA, et al. Crit Care Med 1982; 10: 82–5Hennenberg S, et al. Crit Care Med 1987; 15: 8–13
• Fick’s principle • P-A catheterisation• SvO2<60%, „flow-dependent O2 supply” (ARDS,sepsis) • „Mathematical coupling”
Vincent JL, et al. Am Rev Respir Dis 1990; 142: 2–7Tuchschmidt J, et al. Crit Care Med 1991; 19: 664–71

Caloric Intake in Medical ICU Patients: consistency of care with guidelines and relationship to clinical outcomes.
Krishnan JA, et al. Chest 2003; 124: 297-305
9-18 kcal/kg/day

Caloric Intake in Medical ICU Patients: consistency of care with guidelines and relationship to clinical outcomes.
• 33-66% (II) vs >66% (III)• Significantly better OR:
- Hospital survival- Spontaneous breathing – on discharge- No sepsis – on discharge
Krishnan JA, et al. Chest 2003; 124: 297-305
• 25% >• Significantly more:
- Nosocomial infectionRubinson L et al. CCM 2004; 32: 350

Sepsis, immobilisation

Fredriksson K, et al. Crit Care Med 2007; 35: S449-S453
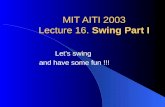
Mitochondrial function in sepsis: Respiratory versus leg muscle

Mitochondrial function in sepsis: Respiratory versus leg muscle
Fredriksson K, et al. Crit Care Med 2007; 35: S449-S453
Black: sepsis+MOFGrey: control (elective surgical patients)

Atrophy and Impaired Muscle Protein Synthesis during Prolonged Inactivity and Stress
Paddon-Jones D, et al. J Clin Endocrinol Metab. 2006 Dec;91(12):4836-41

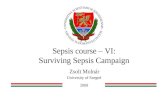
Atrophy and Impaired Muscle Protein Synthesis during Prolonged Inactivity and Stress
Variable Value
Age (yr) 27 ± 1Height (cm) 180 ± 3Body mass (prebed rest) (kg) 82.8 ± 4.0Body mass change (kg) –2.8 ± 0.6Upper body lean mass change (g) –679.8 ± 165.71
Lean leg mass change (g)2 –1325.4 ± 183.01
Body fat mass change (g) –95.6 ± 288.11RM leg ext strength change (%) –28.4 ± 4.41
1 Significant pre- to postbed rest change (P < 0.05).2 Loss of lean muscle mass (dual-energy x-ray absorptiometry) from both legs.
Paddon-Jones D, et al. J Clin Endocrinol Metab. 2006 Dec;91(12):4836-41

The way I did it till 2009…
• Supportive therapy• „Best standard care”• DO2/VO2 • Regular blood gases (arterial, central venous)• Tight blood sugar control 6-8 mmol/l
• Early, controlled enteral nutrition• 30 ml/h: NG aspirate 3-4 hours later• 50-60 ml/h ~ 1500 kcal/day
• Early tracheostomy• No sedation, active moving• Communication
• „Agressive” weaning• Passive moving: avoids contractures• Muscle strength: active excercise

…the way I will carry on
• Same, but…• Early EN +/- TPN
• 30 ml/h: NG aspirate 3-4 h later• 50-60 ml/h ~ 1500 kcal/day
• Blood sugar control• Target: 8-10 mmol/l (instead of 6-8 mmol/l)
Finfer S, et al. N Engl J Med 2009; 360: 1283-97
• Every patient on TPN will get:• Trace elements + vitamins (1amp/day)• Glutamin

• Chronic fasting ≠ critical illness muscle wasting• We treat patients differently now than 25 years ago
– ICU is more comfortable for patients
• Less often means more– 25-60% of calculated calory intake – not harmful, the opposite!– PRCTs are required
• Active moving is invaluable
Summary

Patients are always right:
if they are not hungry I don’t feed them.
Motto