Nutrition In Pediatric CRRT - Pediatric Continuous Renal ...
33
Nutrition In Pediatric CRRT Michael Zappitelli, MD, MSc Nutrition in AKI AND CRRT McGill University Health Center Montreal, Quebec, Canada
-
Upload
christina101 -
Category
Documents
-
view
1.371 -
download
0
description
Transcript of Nutrition In Pediatric CRRT - Pediatric Continuous Renal ...

NutritionIn Pediatric CRRT
Michael Zappitelli, MD, MScNutrition in AKI AND CRRT
McGill University Health CenterMontreal, Quebec, Canada

ObjectivesObjectives
Discuss the impact of nutrition in acute Discuss the impact of nutrition in acute kidney injury... and vice versakidney injury... and vice versa
Discuss clearance of nutrition and nutrition Discuss clearance of nutrition and nutrition adjustment in pediatric CRRT.adjustment in pediatric CRRT.

Critical Illness
Acute Kidney Injury
Poorer outcome, increased mortality
No real prevention/treatment
Left with:1) Modifying the negative effects of AKI
2) Providing adequate nutrition
??? Modify outcome???
X
X

Critical Illness
hormone changes-Acute: increase-Later: decrease
↑ cytokines Altered substrate utilizationCH2O: ↑hepatic gluconeogenesis (shift away from glycolysis) ↑lipogenesis- Inefficient glucose oxidation- Insulin resistance- Shift in use of amino acids: gluconeogenesis + APR’s
MALNUTRITION
Acute Kidney Injury
UremiaAcidosisAltered Glucose metab.
Cytokines
Impaired nutrient transportInefficient/inadequate supplyImpaired A.a. conversion↓lipid oxidation

Critical Illness and NutritionCritical Illness and Nutrition
Adequate nutrition needed for recovery + Adequate nutrition needed for recovery + normal functioning of growing child. normal functioning of growing child.
Tissue synthesis and immune function.Tissue synthesis and immune function.
Desire to avoid over- and under-feeding.Desire to avoid over- and under-feeding.
Underfeeding: increase morbidity, mortality, Underfeeding: increase morbidity, mortality, infection, wound healing, length of ventilation.infection, wound healing, length of ventilation.

Critical Illness and NutritionCritical Illness and Nutrition
Children: high risk of malnutrition.Children: high risk of malnutrition.
High basal metabolic rates.High basal metabolic rates.
Limited energy reserves.Limited energy reserves.
High (15-30%) baseline poor nutrition.High (15-30%) baseline poor nutrition.

Malnutrition AND AKIMalnutrition AND AKI Same difficulties/pathophysiology +Same difficulties/pathophysiology +
Increased difficulty in nutrition provision.Increased difficulty in nutrition provision.
Higher rate of baseline malnutrition/ comorbiditiesHigher rate of baseline malnutrition/ comorbidities
Metabolic changes of AKI.Metabolic changes of AKI.
Children with AKI – increased risk of malnutrition at PICU Children with AKI – increased risk of malnutrition at PICU discharge.discharge.
RRT – increases nutritional losses.RRT – increases nutritional losses.

Nutrition and AKINutrition and AKI
Problem: No evidence-based guidelines.Problem: No evidence-based guidelines.
Difficulty to show effect on hard outcomes.Difficulty to show effect on hard outcomes.
Recommendations based on Recommendations based on 1)1) Adult studiesAdult studies2)2) Known metabolic alterations with AKIKnown metabolic alterations with AKI3)3) Nutrition in critically ill childrenNutrition in critically ill children4)4) Measuring nutritional losses by RRT.Measuring nutritional losses by RRT.

Critical Illness – Energy needsCritical Illness – Energy needs
Metabolic needs vary according to the injury.Metabolic needs vary according to the injury.
RDA versus predictive equations vs direct RDA versus predictive equations vs direct measurement (indirect calorimetry).measurement (indirect calorimetry).
No single predictive equation shown to No single predictive equation shown to accurately estimate REE. accurately estimate REE.
Limitations to indirect calorimetry in critically ill Limitations to indirect calorimetry in critically ill patients.patients.

AKI and energy needsAKI and energy needs
Controversial – AKI per se may not affect Controversial – AKI per se may not affect energy expenditure.energy expenditure.
Affected more by coexisting conditions. Affected more by coexisting conditions.
Almost no data on pediatric AKI and Almost no data on pediatric AKI and energy needs. energy needs.

Indirect calorimetry AND CRRTIndirect calorimetry AND CRRT
IC: measure resting energy expenditure.IC: measure resting energy expenditure. Based on: Expired CO2 and O2 (O2 consumption + Based on: Expired CO2 and O2 (O2 consumption + CO2 production).CO2 production).
Potential problem with CRRTPotential problem with CRRT
Hemofilter
Dialysis fluidEffluent
HCO3/CO2 fluxes May affect ICmeasurements.
IC may not be reliable?

Critical Illness – Energy needsCritical Illness – Energy needs
Controversy: ? RDA ? 25-30% above REE.Controversy: ? RDA ? 25-30% above REE.
Mean REE in literature: 35 to 60 kcal/kg/day Mean REE in literature: 35 to 60 kcal/kg/day (0.15-0.27 MJ/kg/day)(0.15-0.27 MJ/kg/day)
Adults: 25-35 kcal/kg/day – probably need more Adults: 25-35 kcal/kg/day – probably need more in children.in children.
Almost no studies in AKI.Almost no studies in AKI.

CarbohydratesCarbohydrates
Patients become hyperglycemic.Patients become hyperglycemic.Insulin resistance, Insulin resistance, ↑↑hepatic hepatic gluconeogenesis.gluconeogenesis. Stress hormonesStress hormones Inflammatory mediators and cytokinesInflammatory mediators and cytokines Metabolic acidosisMetabolic acidosis Pre-existing hyperparathyroidismPre-existing hyperparathyroidism

Critical Illness - proteinCritical Illness - protein
Protein synthesis AND breakdown are Protein synthesis AND breakdown are increased: breakdown more increased. increased: breakdown more increased.
Manifestation: net negative nitrogen Manifestation: net negative nitrogen balance, skeletal muscle wasting. balance, skeletal muscle wasting.
Nitrogen balance = Nin – Nout. Nitrogen balance = Nin – Nout.

Critical Illness & AKI - proteinCritical Illness & AKI - protein
Protein metabolism abnormal:Protein metabolism abnormal:
- Reduced renal synthesis of amino acidsReduced renal synthesis of amino acids
- Altered amino acid uptakeAltered amino acid uptake
- Factors related to critical illness (elevated stress Factors related to critical illness (elevated stress hormones, increased hepatic gluconeogenesis, hormones, increased hepatic gluconeogenesis, relative insulin resistance). relative insulin resistance).

AKI and proteinAKI and protein
Protein synthesis CAN be increased by Protein synthesis CAN be increased by providing more amino acids.providing more amino acids.
Bellomo et al, Int J of Artif Organs, 2002Bellomo et al, Int J of Artif Organs, 2002Scheinkestel et al, Nutrition, 2003Scheinkestel et al, Nutrition, 2003
Still very difficult to achieve positive N Still very difficult to achieve positive N balance. balance.

Amino acid, trace metal and folate clearance by continuous renal replacement therapy in critically ill children. Zappitelli et al, submitted
Amino Acid
Day 2 (n=15) Day 5 (n=9)K1 CVVHD CVVHD Losses K Renal (n=2) K CVVHD CVVHD Losses K Renal (n=3)(ml/min/1.73m2) (mcg/kg/d) (ml/min/1.73m2) (ml/min/1.73m2) (mcg/kg/d) (ml/min/1.73m2) Mean±SD, Median Mean±SD, Median Mean Mean±SD, Median Mean±SD, Median Mean
TauAspThrSerAsnGluGlnProGlyAlaCitValCysMetIleLeuTyrPheOrnLysHisArg
104.5±179.0, 32.9 8.4±11.1, 4.8 1.0 77.8±111.2, 24.2 4.5±5.4, 1.8 2.1335.8±483.7, 53.6 3.9±4.1, 3.2 2.6 234.0±349.8, 51.1 5.6±4.4, 2.6 12.031.9±25.0, 22.6 15.7±18.5, 9.9 4.1 38.8±25.1, 29.8 11.9±5.9, 12.0 18.929.1±25.6, 17.8 8.1±8.6, 5.7 3.6 34.6±27.7, 22.3 6.0±3.3, 5.0 9.237.2±32.1, 32.3 7.7±8.1, 4.5 9.8 35.5±19.8, 34.3 5.0±3.4, 5.3 28.69.4±10.6, 6.2 2.7±4.0, 1.8 0.6 6.1±5.0, 3.8 1.6±0.7, 1.7 1.019.4±20.1, 13.2 47.4±63.7, 23.0 2.2 85.4±152.9, 21.2 44.2±30.7, 34.5 0.738.3±32.7, 31.2 24.3±22.2, 17.6 0.2 37.5±21.9, 27.3 19.4±11.2, 20.5 0.828.1±25.7, 18.0 16.0±16.1, 7.5 3.9 35.3±30.2, 19.8 12.0±7.1, 14.1 12.926.1±24.6, 15.4 23.4±21.2, 13.5 5.2 37.9±38.8, 25.2 20.0±11.5, 24.1 6.925.6±24.3, 15.9 2.8±4.5, 1.3 4.1 39.3±50.4, 25.7 1.5±1.1, 1.4 5.724.8±22.0, 14.8 16.8±13.4, 12.7 5.2 39.1±37.3, 25.1 14.4±6.9, 13.9 5.527.4±54.5, 8.6 0.8±1.2, 0.5 0.5 34.7±29.9, 44.3 1.3±1.1, 1.1 5.218.0±19.9, 8.2 5.9±13.5, 12.7 3.6 26.8±31.1, 17.2 2.2±1.8, 2.2 5.129.9±29.8, 17.3 6.0±5.7, 4.3 6.9 38.6±34.7, 22.1 5.4±2.7, 4.3 6.622.9±20.9, 13.6 11.6±9.2, 7.8 3.9 32.2±28.8, 22.7 10.3±5.2, 10.9 4.422.2±23.3, 10.7 9.2±13.5, 4.3 4.4 36.5±41.3, 21.4 5.6±2.7, 5.2 10.523.9±20.8, 12.9 18.4±23.1, 7.8 4.5 34.9±29.7, 26.4 11.3±6.2, 10.1 7.08.4±8.7, 12.9 3.4±5.0, 1.0 0.3 91.0±249.7, 10.6 2.5±3.4, 1.4 0.77.7±9.0, 2.8 10.0±11.1, 4.4 0.3 108.4±299.5, 9.6 8.7±8.9, 5.6 0.913.2±15.8, 10.0 8.0±15.9, 2.8 0.7 33.4±66.3, 15.7 4.5±3.8, 5.1 12.115.8±17.1, 8.0 11.4±23.4, 3.5 1.8 45.8±68.6, 8.6 6.0±4.8, 4.1 6.2
CVVHD clearance of amino acids measured on Day 2 and Day 5 N=15

0
10
20
30
40
50
60
K ml/min/1.73m2
Thr Glu Gln Pro Gly Ala Val Met Phe Lys His Arg
Amino Acids
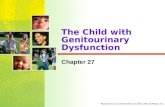
Combined results of clearance of essential amino acids by CRRT. Zappitelli et al (submitted) and Maxvold et al, Critical Care, 2000 (n=6).
Several studies, adult and child: ~ 10-20% intake “lost” through hemofilter.
Both studies: Highest losses with Glutamine/Glutamic acid

Amino acid, trace metal and folate clearance by continuous renal replacement therapy in critically ill children. Zappitelli et al, submitted
Amino Acid2 CVVHD initiation % low/normal/high3 Day 2 % low/high/normal Day 5 % low/normal/high
TauAspThrSerAsnGluGlnProGlyAlaCitValCysMetIleLeuTyrPheOrnLysHisArg
43±96, 16 0/ 93.3/6.7 40±102, 14 6.7/ 86.7/ 6.7 18±14, 13 11.1/ 88.9/ 0 4±3, 3 0/ 100.0/ 0 5±5, 3 6.7/ 93.3/ 0 13±16, 8 11.1/ 66.7/ 22.2100±81, 66 20.0/60.0/20.0 99±54, 109 13.3/ 80.0/ 6.7 105±67, 95 0/ 88.9/ 11.153±26, 51 60.0/ 40.0/ 0 65±30, 56 53.3/ 46.7/ 0 66±34, 58 44.4/ 55.6/ 0 37±21, 30 0/ 100.0/ 0 42±23, 43 0/ 93.3/ 6.7 42±27, 41 11.1/ 77.8/ 11.157±89, 23 0/ 86.7/ 13.3 55±55, 37 0/ 80.0/ 20.0 119±146, 82 11.1/ 44.4/ 44.4315±146, 295 46.7/ 53.3/ 0 372±167, 364 0/ 33.3/ 66.7 382±261, 336 33.3/ 55.6/ 11.1124±66, 111 6.7/ 93.3/ 0 142±69, 127 0/ 100.0/ 0 182±113, 132 0/ 88.9/ 11.1200±135, 167 26.7/ 66.7/ 6.7 186±89, 177 20.0/ 66.7/ 13.3 190±100, 165 11.1/ 77.8/ 11.1195±133, 157 13.3/ 80.0/ 6.7 259±149, 210 13.3/ 80.0/ 6.7 283±192, 236 11.1/ 77.8/ 11.112±7, 10 13.3/ 86.7/ 0 12±8, 11 20.0/ 80.0/ 0 12±7, 12 22.2/ 77.8/ 0148±58, 151 20.0/ 80.0/ 0 144±43, 142 6.7/ 93.3/ 0 140±57, 148 11.1/ 88.9/ 027±25, 21 20.0/ 60.0/ 20.0 17±24, 10 33.3/ 60.0/ 6.7 24±35, 12 33.3/ 55.6/ 11.132±52, 16 6.7/ 80.0/ 13.3 37±39, 25 6.7/ 53.3/ 40.0 25±16, 26 0/ 88.9/ 11.131±19, 24 13.3/ 86.7/ 0 43±22, 42 6.7/ 93.3/ 0 45±23, 41 0/ 88.9/ 11.178±34, 70 0/ 93.3/ 6.7 97±28, 95 0/ 100.0/ 0 101±41, 100 11.1/ 77.8/ 11.157±38, 42 6.7/ 73.3/ 20.0 51±27, 45 6.7/ 86.7/ 6.7 46±27, 45 22.2/ 77.8/ 092±59, 71 0/ 73.3/ 26.7 98±63, 79 0/ 46.7/ 53.3 83±45, 87 0/ 44.4/ 55.647±37, 38 0/ 86.7/ 13.3 56±41, 51 0/ 86.7/ 13.3 67±84, 52 11.1/ 77.8/ 11.1152±65, 136 0/ 86.7/ 13.3 173±84, 153 0/ 66.7/ 33.3 153±90, 127 11.1/ 66.7/ 22.276±32, 71 6.7/ 80.0/ 13.3 75±38, 65 6.7/ 80.0/ 13.3 65±36, 57 11.1/ 77.8/ 11.143±26, 39 20.0/ 80.0/ 0 74±56, 55 0/ 93.3/ 6.7 56±31, 50 11.1/ 88.9/ 0
Amino Acid serum levels measured on Days 1, 2 and 5

Amino acid, trace metal and folate clearance by continuous renal replacement therapy in critically ill children. Zappitelli et al, submitted
CVVHD initiation (N=15) Day 2 (N=15) Day 5 (N=9)Mean±SD, Median Mean±SD, Median Mean±SD, Median
Protein intake (g/kg/d)N balance (g/kg/d)Caloric intake (kcal/kg/d)Caloric balance (kcal/kg/day)
1.98±1.24, 1.75 2.04±1.02, 2.09 1.85±0.60, 2.08
NA -0.88±1.60, -0.22 -0.23±0.19, -0.24
32.6±27.6, 23.8 40.3±22.3, 33.6 43.2±18.4, 42.7
-0.4±25.4, -8.0 +7.7±21.7, +1.5 +10.6±17.7, +10.8
Protein and energy intake and output at CVVHD1 initiation, Day 2 and Day 5.
Maxvold et al, Crit Care Med, 2000
Protein intake was 1.5 g/kg/day – Negative nitrogen balance
It’s not easy to achieve a positive nitrogen balance.
Logic: bigger filter, higher Qd or Quf = increased clearance

Does increasing protein intake help?Does increasing protein intake help?
Scheinkestel et al.Scheinkestel et al.1. 1. Nutrition, 2003Nutrition, 2003 In 11 critically ill adults on CRRT, protein intake 2.5 In 11 critically ill adults on CRRT, protein intake 2.5
g/kg/day led to a) normal amino acid levels and b) g/kg/day led to a) normal amino acid levels and b) positive nitrogen balance. positive nitrogen balance.
2. 2. Nutrition, 2003Nutrition, 2003 50 critically ill adults on CRRT: 1.5 vs 2.0 vs 2.5 50 critically ill adults on CRRT: 1.5 vs 2.0 vs 2.5
g/kg/day.g/kg/day. NB related to protein intake.NB related to protein intake. NB related to hospital stayNB related to hospital stay Protein intake 2.5 g/kg/d: improved survival!Protein intake 2.5 g/kg/d: improved survival!

What are we doing?What are we doing?Protein and calorie prescription for children and young adults receiving CRRT: a report from the Prospective Pediatric Continuous Renal Replacement Therapy Registry group. Zappitelli et al, submitted.
Age (years)
CRRT duration (days)
Diagnostic category Sepsis/Infection Renal Respiratory Cardiac Hematology Oncology Gastrointestinal/Hepatic Other
CRRT indication Electrolyte imbalance Fluid overload only Fluid overload and electrolytes
CRRT modality CVVHD CVVH CVVHDF
8.8 ± 6.8 (8.1, 12.8)
10.2±10.7 (7.0, 11.0) days N (%) 74 (38.1) 29 (15.0) 12 (6.2) 21 (10.8) 35 (18.0) 15 (7.7) 9 (4.6)
31 (15.9) 66 (33.9) 98 (50.3)
94 (48.2) 52 (26.7) 49 (25.1)

Protein and calorie prescription for children and young adults receiving CRRT: a report from the Prospective Pediatric Continuous Renal Replacement Therapy Registry group. Zappitelli et al, submitted.
01
23
45
1 2 3 4 5 6 7 8 9 10excludes outside values
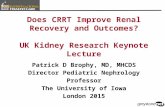
Protein intake(g/kg/day)
Day of CRRT
Daily change in protein prescription during treatment with CRRT.

Protein and calorie prescription for children and young adults receiving CRRT: a report from the Prospective Pediatric Continuous Renal Replacement Therapy Registry group. Zappitelli et al, submitted.
025
5075
100
125
150
1 2 3 4 5 6 7 8 9 10excludes outside values
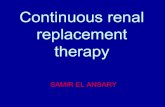
Caloric Intake(kcal/kg/day)
Day of CRRT
Daily change in caloric prescription during treatment with CRRT.

Protein and calorie prescription for children and young adults receiving CRRT: a report from the Prospective Pediatric Continuous Renal Replacement Therapy Registry group. Zappitelli et al, submitted.
Characteristics (N) Protein intake (g/kg/day) Initial Maximal
Gender Males (111) Females (84) p-value1
Age Group≤ 1 year (35)1 to ≤13 years (95)>13 years (65)p-value
MODS (155)No MODS (40)p-valueSurvival Survivors (117) Non-survivors (78) p-valueCRRT indication Electrolytes (31) Fluid overload (66) Electrolytes and fluid overload (98) p-value
1.4, 1.0[1.4] 2.0, 1.6[1.6]1.3, 1.0[1.2] 1.9, 1.8[1.5] 0.7 0.9
1.5, 1.8[1.5] 2.5, 2.4[2.3] 1.3, 1.0[1.2] 2.0, 1.9[1.5] 1.4, 1.0[1.0] 1.6, 1.3[1.1] 0.09 0.009*
1.3, 1.0[1.2] 1.9, 1.8[1.5]1.5, 1.0[0.8] 2.0, 1.3[1.7] 0.1 0.2
1.4, 1.0[1.2] 2.0, 1.6[1.5]1.3, 1.0[1.3] 1.8, 1.8[1.7] 0.6 0.9
1.2, 1.0[0.9] 1.6, 1.4[1.1]1.6, 1.2[1.2] 2.1, 1.8[1.8]1.2, 1.0[1.3] 2.0, 1.8[1.6] 0.07 0.2
All groups:-Maximal protein>initial
Multivariate predictors ofmaximal protein intake
- Younger age- Higher initial protein Rx- #CRRT days
Protein Rx >2g/kg/day in 40%

Critical Illness & AKI - LipidsCritical Illness & AKI - Lipids
LDL and VLDLLDL and VLDL Cholesterol and HDL-CholesterolCholesterol and HDL-Cholesterol
Impaired LipolysisImpaired Lipolysis Lipase Activity ~50%Lipase Activity ~50% Lipoprotein LipaseLipoprotein Lipase Hepatic Triglyceride LipaseHepatic Triglyceride Lipase

Critical Illness - VitaminsCritical Illness - Vitamins
Water SolubleWater SolubleVit BVit B1 1 Def Altered Energy Metabolism, Def Altered Energy Metabolism,
Lactic Acid, Tubular damageLactic Acid, Tubular damageVit BVit B66 Def Altered Amino acid and lipid Def Altered Amino acid and lipid
metabolism metabolism Folate Def Anemia Folate Def Anemia Vit C Def Limit 200 mg/d as precursor to Vit C Def Limit 200 mg/d as precursor to
Oxalic acidOxalic acidPotential for losses during CRRT.Potential for losses during CRRT.

Critical Illness - VitaminsCritical Illness - Vitamins
Fat SolubleFat Soluble
Vit D Def HypocalcemiaVit D Def HypocalcemiaVit A Excess Vit A Excess renal catabolism of renal catabolism of
retinol binding proteinretinol binding proteinVit E Def Vit E Def >50% plasma and RBC >50% plasma and RBC

CRRT-VitaminsCRRT-Vitamins
02468
10121416
Serum folate level (ng/ml)
Pre CRRT Day 2 Day 5
Day of CRRT
Amino acid, trace metal and folate clearance by continuous renal replacement therapy in critically ill children. Zappitelli et al, submitted
**

Critical Illness – trace metalsCritical Illness – trace metals
Deficiencies linked to:Deficiencies linked to:- Lymphocyte dysfunctionLymphocyte dysfunction- Cardiovascular dysfunctionCardiovascular dysfunction- Platelet activityPlatelet activity- Antioxidant functionAntioxidant function- Wound healingWound healing

Amino acid, trace metal and folate clearance by continuous renal replacement therapy in critically ill children. Zappitelli et al, submitted
K1 Day 2 K Day 5 Serum concentrations _____________________ (ml/min/1.73m2) (ml/min/1.73m2) Initiation Day 2 Day 5 Reference range2
SeleniumCopperChromiumZincManganeseFolate
10.1±7.2, 9.5 8.6±3.9, 7.2 55±19, 49 61±24, 59 64±23, 63 23 to 190 (µg/l) 0.4±0.3, 0.3 0.54±0.46, 0.44 88±21, 87 L3 110±27, 106 104±27, 103 90 to 190 (µg/dl)24.0±10.6, 25.4 24.7±7.1, 26.0 2±1, 2 2±1, 2 2±0.4, 2 0 to 2.1 (µg/l)4.2±4.1, 3.2 4.0±2.4, 2.9 66±44, 53 L 68±28, 61 76±38, 68 60 to 120 (µg/dl)9.0±12.9, 4.6 38.2±121.4, 5.1 9±16, 4 H3 8±15, 3 H 8±15, 3 H 0 to 2 (µg/l)29.4±54.9, 16.2 15.6±3.2, 16.3 16±12, 12 10±4, 9 8±2, 7 5.4 to 40 (ng/l)
Churchwell et al, NDT, 2007
Critically ill adults receiving CVVHD and CVVHDFTransmembrane clearancesMuch lower clearance of selenium and chromiumOverall, trace metal clearance negligible.

SynthesisSynthesisNutritional parameter
Nutrition modality
Energy
Protein
Vitamins
Trace elements
Monitoring
Consider
- Early enteral feeding, will often require parenteral nutrition
- Approximately 25% above basal metabolic needs as measured by metabolic cart or estimated with equations.-20 to 25% as carbohydrates (insulin as needed) 30 to 40% lipid formulations (20% lipid emulsions) 40 to 50% protein- 2 to 3 g/kg/day with AKI- Increase intake if on CRRT (by 20%)
- Daily recommended intake - Monitor serum folate, water soluble vitamin levels ± replacement
- Daily recommended intake
-Resting energy expenditure, nitrogen balance, electrolytes, vitamins, trace elements
- Glutamine

AcknolwedgementsAcknolwedgements
Timothy E. BunchmanTimothy E. Bunchman
Norma J. MaxvoldNorma J. Maxvold
Stuart L. GoldsteinStuart L. Goldstein