Nutrition in Cancer Prevention and Treatment
36
Nutrition @ DEAKIN Nutrition in Cancer Prevention and Treatment 1 Associate Professor Tim Crowe School of Exercise and Nutrition Sciences Deakin University [email protected] @CroweTim www.thinkingnutrition.com .au
-
Upload
tim-crowe -
Category
Health & Medicine
-
view
594 -
download
0
description
This presentation will help you to understand the influence that dietary and lifestyle factors play in the prevention and causation of cancer. It outlines the important nutritional considerations for patients undergoing treatment for cancer and reviews procedures to improve patient safety by knowing the risks and benefits of antioxidant supplementation during cancer treatment
Transcript of Nutrition in Cancer Prevention and Treatment

Nutrition @ DEAKIN
Nutrition in Cancer Prevention and Treatment
1
Associate Professor Tim CroweSchool of Exercise and Nutrition Sciences
Deakin University
[email protected]@CroweTimwww.thinkingnutrition.com.au

Nutrition @ DEAKIN
Learning Objectives1. To understand the influence that dietary and
lifestyle factors play in the prevention and causation of cancer
2. To be aware of the important nutritional considerations for patients undergoing treatment for cancer
3. Review procedures to improve patient safety by knowing the risks and benefits of antioxidant supplementation during cancer treatment
2

Nutrition @ DEAKIN
Cancer in Australia
Summary• Cancer accounts for ~30% of all deaths• 108,368 new cancers diagnosed in 2007
(excluding non-melanocyte skin cancers)• 39,884 deaths in 2007 from cancer
In order of incidence: Prostate, colorectal,breast, melanoma and lung (61% of all cases)
3

Nutrition @ DEAKIN
Cancer in Australia: 2007
4
Cancer in Australia 2010: an overview. Cancer Series no. 60 AIHW. www.aihw.gov.au/publication-detail/?id=6442472454

Nutrition @ DEAKIN
Trends in Incidence and Mortality
In Australia between 1982-2007
• 27% ↑ incidence (age standardised)• Rise in incidence of most cancers
• 16% ↓ mortality (age standardised)• Falls in mortality for most cancers except liver,
melanoma, and lung cancer (in women)
5
Cancer in Australia 2010: an overview. Cancer Series no. 60 AIHW. www.aihw.gov.au/publication-detail/?id=6442472454

Nutrition @ DEAKIN
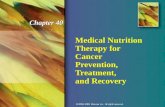
Lifestyle Factors Contributing to Cancer Risk
6
Fraction of cancer attributable to lifestyle and environmental factors in the UK in 2010
Parkin DM and Walker LC. Br J Cancer 2011;105:577-581

Nutrition @ DEAKIN
Lifestyle Factors Associated with Reduced Cancer Risk
Dietary Factor Cancer
Fibre Colorectal*, oesophagus,
Fruits and Vegetables Oral cavity, oesophagus, lung, stomach, colorectal
Physical Activity Colorectal*, breast, oesophagus, pancreas, liver, endometrial
Lactation Breast*
Calcium Colorectal
Dairy foods Colorectal
Fish Colorectal
Garlic Colorectal
Selenium Lung, colorectal, prostate
Folate Oesophagus, pancreas, colorectal
7
*Cancers bolded are where evidence is the strongestThe Second Expert Report, Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective www.dietandcancerreport.org

Nutrition @ DEAKIN
Lifestyle Factors Associated with Increased Cancer Risk
Dietary Factor Cancer
Overweight and obesity Oesophagus, pancreas, colorectal, breast (post-menopausal), endometrial, kidney
Alcohol Oral cavity, oesophagus, liver, colorectal, breast
Salted foods Stomach, nasopharynx
Red meat Colorectal
Aflatoxin Liver
Grilled/BBQ foods Colorectal, stomach
Very hot foods and drinks Oral cavity, oesophagus
8
*Cancers bolded are where evidence is the strongestThe Second Expert Report, Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective www.dietandcancerreport.org

Nutrition @ DEAKIN
Obesity and Cancer• Cancers most likely: breast,
colorectal, kidney, endometrium,oesophagus and pancreas
• True incidence likelyunderestimated due to effectof smoking and self-reportedheight and weight in some studies(↑BMI = ↑under-reporting)
Mechanism?• ↑ Insulin, insulin growth factor-1 and/or sex steroids• Reflux (for oesophageal cancer)• Chronic inflammation (↑ oxidative stress)
9

Nutrition @ DEAKIN
Breast Cancer• Life-time risk in the
western world is 10% and associated with a western lifestyle
• Risk increases with age• Genetics (family history)
explain 10% of cases• Hormonal and
dietary/lifestyle factors play the biggest role
10
www.sogc.org/media/guidelines-oc_e.asp

Nutrition @ DEAKIN
Dietary Modification of BC Risk• Increased dietary fibre ↓ estrogen• Levels of estrogen are lower in
vegetarians• Dietary restriction shown to lower
IGF-1, increase SHBG, lower insulin• Weight loss• Alcohol: ↑ estrogen concentration, ↓ folate, direct effects on
breast tissue• Omega-3s may be protective: ?anti-proliferative effect• Reduced fat diets shown to ↓ circulating estrogen• ? Phytoestrogens (soy products) protective
11

Nutrition @ DEAKIN
Dietary Fibre and Colorectal Cancer• Dietary fibre (and resistant starch), especially from
cereal and pulses, is likely protective• Unclear if it is the fibre or other nutrients in the food• Range of physiological actions:
– pH– Bulking effect– Butyric acid (anti-proliferative)– Transit time (also affected by exercise)
12

Nutrition @ DEAKIN
Does Red Meat Cause Cancer?
• ↑ risk estimates in the range of 20 to 50% for highest vs lowest intakes of red meat in prospective studies
• Not clear if it’s the intake of red meat (?excess Fe), form of meat (esp. processed), or the way meat is cooked
• Nitrosamines (endogenous and from nitrate preservatives)
• Cooking (charring) of meat produces two types of carcinogens– Polycyclic aromatic hydrocarbons (PAHs)– Heterocyclic amines (HCAs)
• World Cancer Research Fund 2007 report* ratesthe evidence as ‘Convincing’
13
*The Second Expert Report, Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective www.dietandcancerreport.org

Nutrition @ DEAKIN
Antioxidants and Cancer Prevention
• Free radicals can damage DNA• Antioxidants can neutralise the free radicals, preventing
the cancer initiation process• Additional benefits may lie in inhibiting proliferation and
angiogenesis• Observational epidemiological studies and case-control
studies strongly supported the theory
What do RCTs tell us?
14

Nutrition @ DEAKIN
ATBC StudyPremise: high fruit and vegetable intake protective against
lung cancer and smokers have lower serum retinol concentrations
• 29,133 male smokers in Finland, 50-69 y.o.• Given either Vit E (50 mg), beta-carotene (20 mg), both,
or placebo daily for 5-8 years
Results: 18% more lung cancers and 8% higher mortality with beta-carotene (effect only seen in drinkers)
32% decrease in incidence of prostate cancer in group taking vitamin E
15ATBC. New Engl J Med 1994:330:1029-35

Nutrition @ DEAKIN
CARET Study
• 14,000 smokers and ex-smokers 50-69 y.o.
• Beta-carotene (30 mg) and retinol (25,000 IU) for 4 yrs
28% more cancer and 17% greater mortality
16
CARET. New Eng J Med 1996;334:1150-5

Nutrition @ DEAKIN
ATBC and CARET Follow Up
8 yrs after the end of ATBC• Intervention effect of beta-carotene disappeared
and no ‘late’ preventative effects seen• Effect of vitamin E on prostate cancer reduced
5 yrs after the end of CARET• Elevated risk post-trial seen in females
17
ATBC Follow-up JAMA 2003;290:476-85
CARET Follow-up J Nat Cancer Inst 2004;96:1743-50

Nutrition @ DEAKIN
Beta-Carotene and Non-smokers?
• Physicians’ Health Study (22,000 males, 11% smokers)– Beta-carotene not harmful after 12 yrs
• 44% lower risk of adenoma recurrence in non-smokers and drinkers, but double the risk in smokers and drinkers
18Baron et al. J Nat Cancer Inst 2003;95:717-22

Nutrition @ DEAKIN
Mechanisms?
1. Beta-carotene: pro-oxidant activity at high O2 pressure in lungs
2. Smoking increases production of oxidised beta-carotene metabolites
3. High beta-carotene concentrations may decrease tissue retinoic acid
4. Vitamin E: displacement of other fat soluble vitamins
5. Synergistic effect important
19

Nutrition @ DEAKIN
HOPE-TOO, WHS and WACSHOPE-TOO: 5,900 patients randomised to 400 IU Vit E/day for
7.1 yrs• No differences in cancer incidence and deaths or major
CVD events (↑ in HF)WHS: 40,000 women (> 45 y.o.), RCT of 600 IU Vit E/day or
placebo for 10 yrs• No reduction in cancer or CVD events
WACS: 8,100 women, 600 IU Vit E, 500 mg Vit C, 50 mg beta-carotene or placebo for 9.4 yrs• No reduction in cancer morbidity of mortality• Indication of ↑ pancreatic and lung cancer with Vit C
20
HOPE-TOO JAMA 2005;293:1338-47 WACS J Nat Cancer Inst 2009;101:14-23
WHS JAMA 2005;294:56-65

Nutrition @ DEAKIN
Se, Vitamin E and Prostate CancerSecondary results from earlier studies showed ↓ prostate
cancer with Se and vitamin E supplements. Larger dedicated RCTs now done
SELECT: RCT (double blind) of 35,500 men > 50 yrs allocated to Se (200 μg/d), vitamin E (400 IU/d), Se + E, or placebo on prostate cancer occurrence Lippman et al. JAMA 2009;301:39-51
• Median follow up of 5.5 yrs: no reduction in prostate cancer or any other major cancers
• Trial stoped early because of evidence of harm (non-significant ↑ T2DM with Se and ↑ prostate cancer with vitamin E)
• Further follow up confirmed 17% ↑ prostate cancerwith vitamin E Klein et al. JAMA 2011;306:1549-1556
21

Nutrition @ DEAKIN
Physicians Health Study II• 14,600 male US physicians randomised to vitamin E
(400 IU/2d), vitamin C (500 mg/d), E + C, or placebo
• Mean follow up of 8 yrs: no reduction in prostate cancer or any other major cancers with any combination of supplements
22PHSII JAMA 2009;301:52-62
Se, Vitamin C and Prostate Cancer

Nutrition @ DEAKIN
SU.VI.MAX Study• RCT with 7 yr follow up using low-dose
supplements• 13,017 French adults (35-60 y.o.)• Single daily capsule:
• 120 mg vitamin C• 30 mg vitamin E• 6 mg beta-carotene• 100 µg Se• 20 mg Zn
23Hercberg S et al. Arch Int Med 2004;164:2335-42

Nutrition @ DEAKIN
SU.VI.MAX Results
• No change in total cancer or CVD incidence vs placebo• No change in all-cause mortality
• In men: 31% lower incidence of cancer and 37% reduction in all-cause mortality
• ? Benefit because of lower baseline antioxidant status (vitamin C and beta-carotene) in men
24

Nutrition @ DEAKIN
Effect of Antioxidant Supplements versus Placebo or no Intervention on Cancer Incidence in 22 RCTs
25Myung S et al. Ann Oncol 2010;21:166-179

Nutrition @ DEAKIN
Diet: Treatment and Recovery• Studies on diet post treatment few in number and
almost all observational• Some evidence that ‘prudent’ diet high in F&V,
wholegrains, legumes, fish and low in fat lowers breast and colorectal Ca recurrence and mortality*
• Due to improved survival rates, healthy diet important because patients may die from other diseases related to diet
26
*Robein K et al. J Am Diet Assoc 2011;111:368-375

Nutrition @ DEAKIN
Anticancer Therapies• RTx → ROS (reactive oxygen
species) production
• CTx → several modes of action– Many rely on ROS production:
• Anthracyclines (e.g. doxorubicin)• Alkylating agent (e.g. cyclophosphamide, ifosfamide)• Platinum complexes (e.g. cisplatin, carboplatin)• Cytotoxic antibiotics (e.g. bleomycin, mitomycin-C)
27

Nutrition @ DEAKIN
Antioxidants during TreatmentEstimates of 13-87% of Ca patients use antioxidant supplements
For• May protect normal cells from ROS damage, allowing better
tolerance of treatment and higher dosage• Enhance cytotoxic CTx by blocking ROS (which can slow rapid
cell proliferation by prolonging G1 phase)Against• Quenching ROS reduces efficacy• May repair damage to cancer cells caused by ROS damage
from treatment and inhibit apoptosis
28

Nutrition @ DEAKIN
Antioxidants during TreatmentFolate, methotrexate and 5-FU• Patients with higher folate intake may experience less
treatment-related side effects• Folate proposed to be protective against Ca
development (DNA mutation and replication repair), but cell-growth promoting once Ca developed
• Concern that may interfere with methotrexate therapy efficacy and promote tumour growth*
• Vitamin C shows reduced cytotoxic effect in vitro
29
*Robien K. Nutr Clin Prac 2005;20:411-22

Nutrition @ DEAKIN
Antioxidants and RTx: a RCT• 540 patients, stage I or II H&N Ca• RCT (double blind) with vitamin E (400 IU/day)
and beta-carotene (30 mg/day) on first day of RTx and then for 3 yrs post
• Beta-carotene ceased after first 156 patients enrolled
What happened?
30
Bairati I et al. J Clin Oncol 2005;23:5805-13

Nutrition @ DEAKIN
Follow-up: Adverse Events
After median follow-up of 52 months:• Those in supplement arm tended to have less
side-effects (OR=0.72; CI=0.52-1.02)• When combined with beta-carotene, ↓ side
effects seen (OR=0.38; CI=0.20-0.74)• QOL not improved• Local recurrence tended to be higher
(HR=1.37; CI=0.93-2.02)
31
Bairati I et al. J Clin Oncol 2005;23:5805-13

Nutrition @ DEAKIN
Follow-up: Cancer RecurrenceAfter median follow-up of 52 months:• Higher rate of second primary cancer incidence in
supplement group (HR=2.88; CI=1.56-5.31)• Higher rate of recurrence or second primary cancer in
supplement group (HR=1.86; CI=1.27-2.72)• Higher all-cause mortality (HR=1.38; CI=1.03-1.85)• Lower rate of recurrence or second primary cancers
after supplementation finished, though not statistically significant
32
Bairati I et al. J Clin Oncol 2005;23:5805-13

Nutrition @ DEAKIN
Commentary on Antioxidants
Review of 9 studies for RTx (3 RCTs, 2 meta-analyses) and 16 RCTs for CTx*
“On the basis of our review of the published randomized clinical trials, we conclude that the use of supplemental antioxidants during chemotherapy and radiation therapy should be discouraged because of the possibility of
tumor protection and reduced survival.”
"Despite some intriguing studies that have suggested the benefit of adjunctive antioxidant treatments in cancer patients, the totality of the available
evidence is equivocal at best and leaves us with seriousconcerns about the potential for harm.”
33
*Lawenda B et al. J Natl Cancer Inst 2008;100:773-783

Nutrition @ DEAKIN
Indications for Supplements in Ca Treatment
• During and after treatment, probable benefit to taking multivitamin at 100% of RDI
Also when:• Biochemically demonstrated deficiency• Chronic poor nutrient intake• To meet public health recommendations• Known health problems related to Ca
treatment
34

Nutrition @ DEAKIN
Recommendations for Cancer Prevention
1. Be as lean as possible within the normal range of body weight2. Be physically active as part of everyday life3. Limit consumption of energy-dense foods. Avoid sugary drinks4. Eat mostly foods of plant origin5. Limit intake of red meat and avoid processed meat6. Limit alcoholic drinks7. Limit consumption of salt. Avoid mouldy grains or legumes8. Aim to meet nutritional needs through diet alone rather than
supplements9. Mothers to breastfeed; children to be breastfed10. For cancer survivors: follow the recommendations for
cancer prevention35
The Second Expert Report, Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective www.dietandcancerreport.org

Nutrition @ DEAKIN
Nutrition and Physical Activity Recommendations
American Cancer Society Guidelines on nutrition and physical activity for cancer prevention: reducing the risk of cancer
with healthy food choices and physical activityCA: A Cancer Journal for Clinicians 2006;56:254-81
Nutrition and physical activity during and after cancer treatment: An American Cancer Society guide for informed
choicesCA: A Cancer Journal for Clinicians 2006;56:323-53
Available free online from:http://caonline.amcancersoc.org
36