
Nursing Through the Lifespan I Exam 3(1)
19
Nursing Through the Lifespan I Exam 3 1 The Human Eye: The 3 Layers of the Eye: 1.) Sclera & Cornea (outer layer) 2.) Uveal Tract (iris, choroid, ciliary body) (middle layer) 3.) Retina (inner layer) Structures & Functions of the Eye: Sclera o White of the eye o Helps protect the intraocular structures Cornea o Transparent & avascular o Allows light to enter the eye o Refracts (bends) incoming light rays to help focus them on the retina o Has no vascular system
-
Upload
jessfriend -
Category
Documents
-
view
234 -
download
3
description
Study Guide, Nursing 201, Shelton State
Transcript of Nursing Through the Lifespan I Exam 3(1)

Nursing Through the Lifespan I Exam 3
1
The Human Eye:
The 3 Layers of the Eye: 1.) Sclera & Cornea (outer layer) 2.) Uveal Tract (iris, choroid, ciliary body) (middle layer) 3.) Retina (inner layer) Structures & Functions of the Eye:
-‐ Sclera o White of the eye o Helps protect the intraocular structures
-‐ Cornea o Transparent & avascular o Allows light to enter the eye o Refracts (bends) incoming light rays to help focus them on the retina o Has no vascular system

Nursing Through the Lifespan I Exam 3
2
-‐ Ciliary Body o Changes the shape of the lens and secretes aqueous humor o The aqueous humor bathes and nourishes the lens & cornea o Excess production or decreased outflow of aqueous humor can elevate intraocular
pressure above the normal 10-‐21 mm Hg. -‐ Lens
o Bends light rays to fall on the retina -‐ Choroid
o Highly vascular structure that nourishes the ciliary body, the iris, & the outermost portion of the retina
-‐ Retina o Forms the optic nerve o Cannot regenerate as it is composed primarily of neurons o Converts images the brain can understand as vision o Photoreceptor cells: rods and cones o Rods stimulated in dim light o Cones receptive to color in bright light o Fovea centralis provides sharpest vision o Macula surrounds the fovea
-‐ External Structures: (Eyebrows, Eyelids, Eyelashes) o Serve as a physical barrier primarily for protection of the eyeball or globe
-‐ Conjunctiva: o Secrete mucus and tears
Assessment of Visual System:
-‐ Subjective Data o Past health history o Ocular information such as visual tests, family history, and head or eye trauma o Nonocular health problems such as systemic, cardiac, or pulmonary diseases o Medications including OTC, eye drops, herbal therapies, or dietary supplements o Surgery or other procedures, including brain surgery or laser treatments o Patient’s perception of the problem o Safety o Allergies o Hereditary diseases and visual problems o Nutritional-‐metabolic pattern (Vitamins A, D, E & Beta-carotene) o Elimination pattern
-‐ Objective Data o Physical Examination (May be as brief as measuring visual acuity or in-‐depth and
require special training. Always based on what is appropriate and necessary for the specific patient)
o Snellen Eye Chart (chart with the big E at top) o Jaegar Eye Chart (hand-‐held vision screener with varying print sizes) o Ishihara Color Test (color vision)
Nursing Through the Lifespan I Exam 3
3
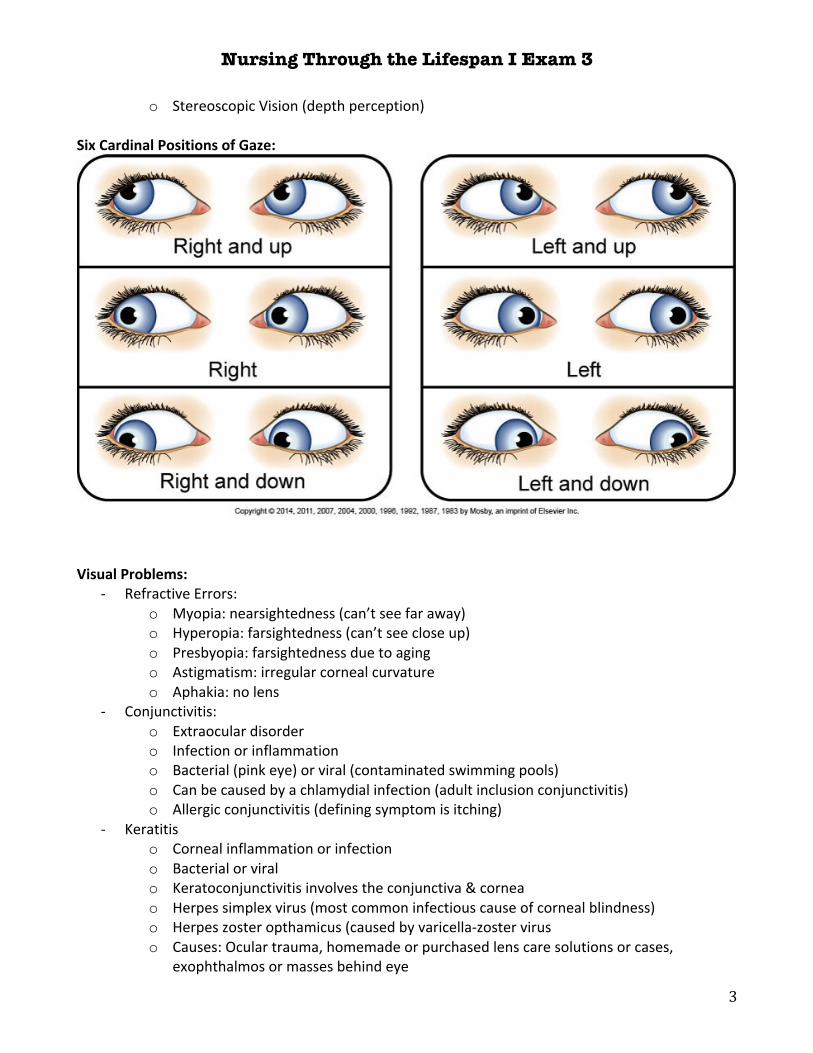
o Stereoscopic Vision (depth perception) Six Cardinal Positions of Gaze:
Visual Problems:
-‐ Refractive Errors: o Myopia: nearsightedness (can’t see far away) o Hyperopia: farsightedness (can’t see close up) o Presbyopia: farsightedness due to aging o Astigmatism: irregular corneal curvature o Aphakia: no lens
-‐ Conjunctivitis: o Extraocular disorder o Infection or inflammation o Bacterial (pink eye) or viral (contaminated swimming pools) o Can be caused by a chlamydial infection (adult inclusion conjunctivitis) o Allergic conjunctivitis (defining symptom is itching)
-‐ Keratitis o Corneal inflammation or infection o Bacterial or viral o Keratoconjunctivitis involves the conjunctiva & cornea o Herpes simplex virus (most common infectious cause of corneal blindness) o Herpes zoster opthamicus (caused by varicella-‐zoster virus o Causes: Ocular trauma, homemade or purchased lens care solutions or cases,
exophthalmos or masses behind eye

Nursing Through the Lifespan I Exam 3
4
-‐ Corneal Ulcer o Tissue loss caused by infection of the cornea o Aggressive treatment necessary to avoid permanent vision loss
-‐ Dry Eye Disorders o Keratoconjunctivitis sicca (dry eyes)
-‐ Strabismus o The PT cannot consistently focus 2 eyes simultaneously on the same object (crosseyed) o Esotropia (eye deviates in) o Exotropia (eye deviates out) o Hypertropia (eye deviates up) o Hypotropia (eye deviates down) o Primary complaint is double vision
-‐ Retinopathy o Slow or rapid process of microvascular damage to the retina o Common complication in uncontrolled, long-‐standing diabetes (diabetic retinopathy) o Hypertension can create vascular blockages in retinal blood vessels (hypertensive
retinopathy) o Retinopathy is irreversible
-‐ Retinal Detachment o Almost all patients become blind in effected eye if untreated o Symptoms: light flashes, floaters, or rings in vision are painless o Surgical intervention is indicated
-‐ Age-‐Related Macular Degeneration o Is most common cause of central vision loss in older adults o Nonexudative is slower to progress & more common (dry) o Exudative is more severe & rapid (wet)
-‐ Cataract o An opacity (cloudiness) within the lens o Leading cause of blindness o Most common surgical procedure for those aged over 65 o Factors: Age, blunt trauma, congenital, UV light exposure, long-‐term corticosteroid
use, ocular inflammation o Senile cataract (most common type; age related) o S/S: decrease in vision, abnormal color perception (color not as bright or sharp),
glaring of vision o No nonsurgical cure o Surgical therapy: antianxiety medication before local anesthesia; cataract extracted &
sutured; corticosteroid & ABT ointment applied with protective shield o Visual acuity improves immediately after surgery o There should be no pain after surgery (notify MD immediately if PT reports pain)
-‐ Glaucoma o A group of disorders characterized by: increased IOP & consequences of elevated
pressure, optic nerve atrophy, peripheral visual field loss o 2nd leading cause of blindness
Nursing Through the Lifespan I Exam 3
5
o leading cause of blindness in African Americans o Primary open-‐angle glaucoma (POAG): most common, outflow of aqueous humor is
decreased in trabecular meshwork; develops slowly, no symptoms, IOP is 22-‐32 mm Hg
o Primary angle-‐closure glaucoma (PACG): angle closure decreases the flow of aqueous humor, caused by age & pupil dilation, possibly drug induced
o Acute angle-‐closure glaucoma: sudden onset, excruciating pain in or around eyes, N/V, seeing colored halos around lights, blurred vision, ocular redness, IOP is >50 mm Hg
o Peripheral vision does not come back -‐ Intraocular Pressure (IOP):
o Elevated in glaucoma o Normal IOP 10-‐21 mm Hg
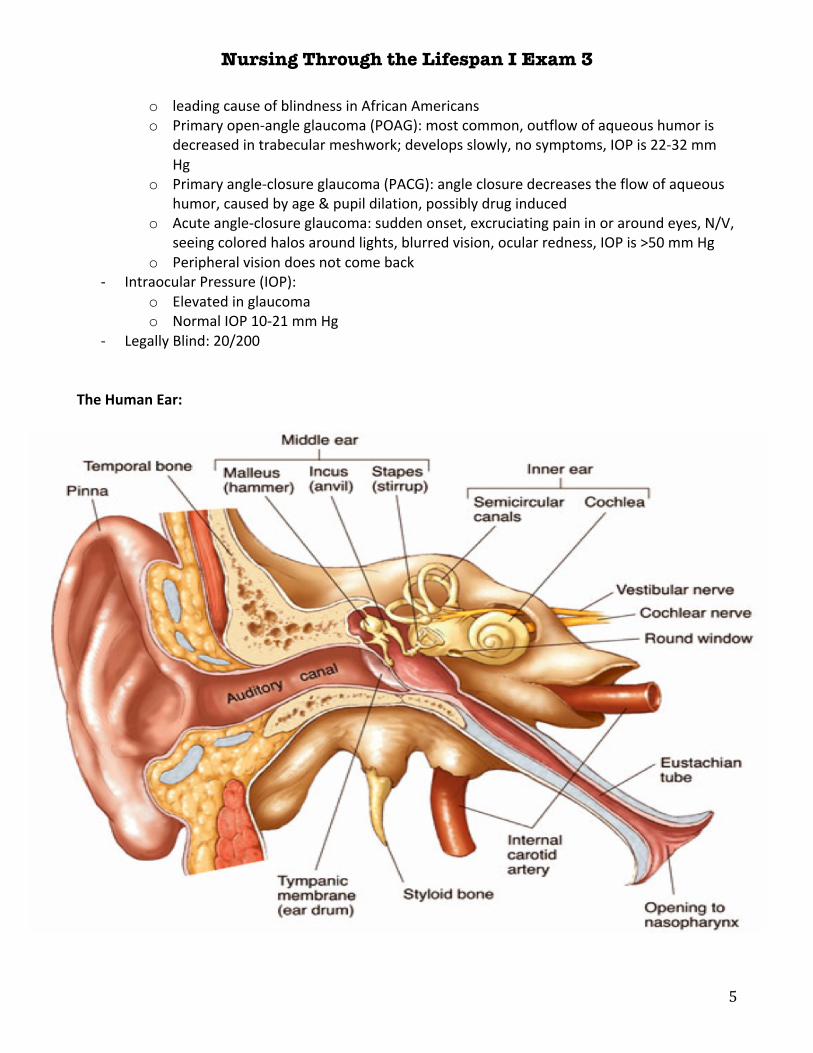
-‐ Legally Blind: 20/200 The Human Ear:

Nursing Through the Lifespan I Exam 3
6
External Ear: -‐ Auricle (pinna), external auditory canal, tympanic membrane (TM) -‐ Collect & transmit sound waves to the tympanic membrane (eardrum)
Middle Ear:
-‐ Eustachian (auditory) tube, malleus, incus, stapes (ossicles) -‐ Transmits sound waves from the TM to the liquid medium of the inner ear
Inner Ear:
-‐ Contains the functional organs for hearing & balance -‐ Cochlea, semicircular canals, vestibule -‐ Cochlea is the main organ for translating
Transmission of Sound:
-‐ Air Conduction: Conduction and amplification of sound waves from the environment -‐ Bone Conduction: the bones of the skull transmit sound directly to the inner ear (tuning fork)
Subjective Data:
-‐ Past medical history (measles & mumps can affect hearing) -‐ Medications (ototoxic meds: PCN, ASA, Lasix) -‐ Surgery or other treatments -‐ Auditory & vestibular problems may be hard to differentiate:
o Vertigo: a sense that the person or objects around the person are moving or spinning & is usually stimulated by movement of the head
o Dizziness: a sensation of being off balance that occurs when standing or walking o Nystagmus: an abnormal eye movement that may e observed as a twitching of the
eyeball or described by the patient as a blurring of vision with head or eye movement Objective Data:
-‐ Physical examination o Ears symmetric in location & shape o Auricles & tragus nontender, without lesions o Canal clear, tympanic membrane intact, landmarks & light reflex intact o Able to hear low whisper at 30 cm. Weber test results, no lateralization. Rinne test
results AC>BC. -‐ Tuning Fork Test
o Aid in differentiating between conductive & sensorineural hearing loss o Weber Test The examiner places an activated tuning fork on the midline of the skull or
the forehead. Ask the patient to indicate where the sound is heard best. In normal auditory function, the patient perceives a midline tone and the sound is heard equally in both ears. If a patient has conductive hearing loss in one ear, the sound will be heard louder (lateralizes) in that ear. If sensorineural loss is present, the sound is louder (lateralizes) in the unaffected ear. Normal results: no lateralization

Nursing Through the Lifespan I Exam 3
7
o Rinne Test The examiner holds the base of a tuning fork against the mastoid bone (BC—bone conduction of sound) and notes the time. When the sound is no longer perceived behind the ear (BC), the time is noted once again and the still vibrating fork is moved 0.5 to 2 inches in front of the ear canal (AC—air conduction of sound). Have the patient report when the sound next to the ear canal (AC) is no longer heard and note the time. Normally, the sound is heard twice as long in front of the ear as it is on the bone. The Rinne test is positive when the patient reports that air conduction (AC) is heard longer than bone conduction (BC). This can indicate a sensorineural hearing loss. If the patient hears the tuning fork better by bone conduction, the Rinne test is negative, which suggests a conductive hearing loss.
-‐ Whisper Test: o Stand 12-‐24 in to the side of the patient & after exhaling, speak in a low whisper o Test each ear separately o The ear not being tested is covered by the patient
-‐ Audiometry o The audiometer produces pure tones at varying intensities to which the patient can
respond. o Hertz (Hz) is the unit of measurement used to classify the frequency of a tone o Decibels (dB) measures the intensity or strength of a sound wave
Auditory Problems:
-‐ Presbycupsis: o Hearing loss as a result of aging o Factors: noise exposure, systemic diseases, poor nutrition, ototoxic drugs, pollution
exposure over the lifespan o Is greater for high pitched sounds
-‐ Tinnitus: o Ringing in the ears o Prevalence expected to rise as life span increases
-‐ Trauma o Blows to the ear can cause conductive hearing loss o Head trauma that injures the temporal lobe of the cerebral cortex can impair the
ability to understand the meaning of sounds -‐ External Otitis
o Involves inflammation or infection of the epithelium of the auricle & ear canal o Swimmer’s Ear o Ear pain (otalgia) is one of the first signs of external otitis o Muffled hearing, drainage & fever (occurs when the infection spreads to surrounding
tissues) o Moist heat, mild analgesics & topical anesthetic drops usually control the pain
-‐ Otitis Media o Infection of the middle ear o S/S: pain, fever, malaise & reduced hearing o Acute Otitis Media: common in children

Nursing Through the Lifespan I Exam 3
8
o Otitis media with effusion: is an inflammation of the middle ear with a collection of fluid in the middle ear space
-‐ Otosclerosis o Is a hereditary autosomal dominant disease o Results in conductive hearing loss o Examination may reveal a reddish blush of the tympanum (Schwartz’s Sign)
-‐ Ménière’s Disease o Is characterized by symptoms caused by inner ear disease, including episodic vertigo,
tinnitus, fluctuating sensorineural hearing loss, & aural fullness. o Symptoms usually begin between 30-‐60 years of age o The cause is unknown o Attacks may last hours or days & may occur several times a year
-‐ Benign Paroxysmal Positional Vertigo o BPPV is a common cause of vertigo o Free floating debris in the semicircular canal causes vertigo with specific head
movements o Treatment: Epley maneuver (ear debris is moved from one area to another)
-‐ Acoustic Neuroma o Is a unilateral benign tumor that occurs where the vestibulocochlear nerve enters the
internal auditory canal. o Symptoms begin between 40-‐60 years of age o Removal of small tumors preserve hearing o Removal of large tumors can cause permanent hearing loss
-‐ Conductive Hearing Loss o Occurs when conditions in the outer or middle ear impair the transmission of sound
through air to the inner ear o Causes: Otitis media with effusion, impacted cerumen, perforation of the TM
-‐ Sensorineural Hearing Loss o Is caused by impairment of function of the inner ear or the vestibulocochlear nerve. o Causes: congenital, hereditary, noise trauma over time, aging, Ménière’s Disease,
ototoxicity, Paget’s disease, DM, bacterial meningitis o The main problems are the ability to hear sound but not to understand speech
-‐ Central Hearing Loss o Involves an inability to interpret sound, including speech, because of a problem in the
brain (CNS). -‐ Functional hearing Loss
o May be caused by an emotional or psychologic factor -‐ Classification of Hearing Loss
o Normal hearing: 0-‐15 dB o Profound Deafness: >90 (congenitally deaf)

Nursing Through the Lifespan I Exam 3
9
Endocrine System: Pituitary Gland
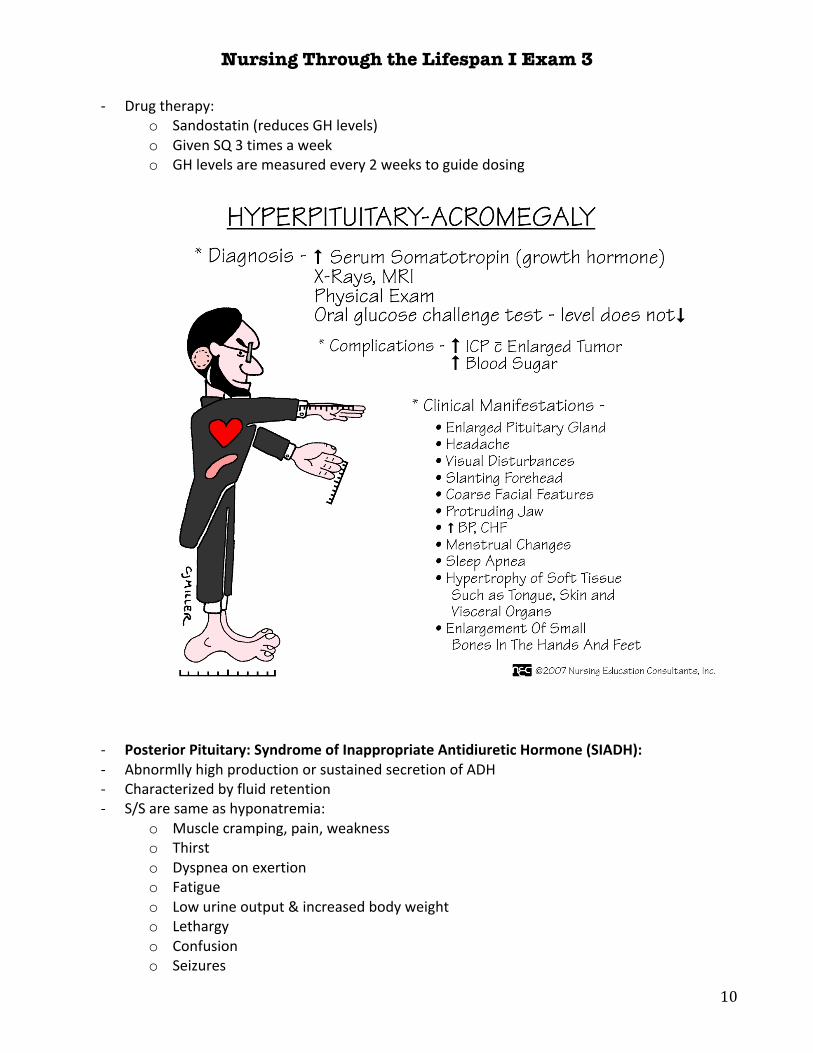
Anterior Pituitary: Growth Hormone: -‐ Target tissue: long bones & soft tissue -‐ Overproduction of GH in adulthood: Acromegaly -‐ Overproduction of GH in childhood: Gigantism -‐ Often occurs as a result of a benign pituitary tumor (adenoma) -‐ S/S: enlargement of hands, feet & face -‐ Diagnostic Studies:
o Oral glucose tolerance test -‐ Surgical therapy:
o Hypophysectomy: removal of pituitary gland o Treatment of choice o Permanent loss of all pituitary hormones o Hormone therapy continues throughout life
-‐ Post-‐op Care: o Elevate head of bed 30° o Perform mouth care every 4 hrs o Avoid tooth brushing for 10 days o Avoid vigorous coughing, sneezing, straining at stool to prevent CSF leakage
Nursing Through the Lifespan I Exam 3
10
-‐ Drug therapy: o Sandostatin (reduces GH levels) o Given SQ 3 times a week o GH levels are measured every 2 weeks to guide dosing
-‐ Posterior Pituitary: Syndrome of Inappropriate Antidiuretic Hormone (SIADH): -‐ Abnormlly high production or sustained secretion of ADH -‐ Characterized by fluid retention -‐ S/S are same as hyponatremia:
o Muscle cramping, pain, weakness o Thirst o Dyspnea on exertion o Fatigue o Low urine output & increased body weight o Lethargy o Confusion o Seizures

Nursing Through the Lifespan I Exam 3
11
-‐ Diagnostic: o Simultaneous measurements of urine & serum osmolarity o Dilutional hyponatremia: serum sodium less than 134 mEq/L o Normal sodium levels: 135-‐145
-‐ Treatment: o Fluid restriction o Position head of bed flat or elevated no more than 10° to enhance venous return o IV hypertonic saline solution (3-‐5%) may be slowly administered (monitor B/P) o Loop Diuretic (Lasix) o Declomycin: blocks the effect of ADH
Posterior Pituitary: Diabetes Insipidus:
-‐ Deficiency of production or secretion of ADH -‐ The decrease in ADH results in fluid & electrolyte imbalances -‐ Causes increased urine output & increased plasma osmolality -‐ Characterized by polydipsia (excessive thirst) & polyuria (excessive urination)
o Urine output of 2-‐20 liters/day o Very low specific gravity <1.005 o Hypernatremia caused by pure water loss (irritability & mental dullness) o Fatigued from nocturia (excessive urination during the night) o Generalized weakness
-‐ If oral fluid intake cannot keep up with urinary losses, severe dehydration results o Poor skin turgor o Hypotension o Tachycardia o Hypovolemic shock
-‐ Diagnostic Studies: Water Deprivation Test o Before the test, body weight, urine osmolarity, volume & specific gravity are measured o Patient is deprived of water for 8-‐12 hours o Patient is given desmopressin (increases ADH) SQ or nasally o Patients with DI exhibit a drastic increase in urine osmolarity & significant decrease in
urine volume o Nurse will want to stop test immediately if dehydration symptoms occur
-‐ Treatment: o Increase fluids o Hypotonic IV solutions (D5W) o Monitor blood sugar, B/P, heart rate, urine output, S/S of dehydration o Monitor intake & output o Monitor daily weights to determine fluid volume status o Low-‐Sodium diet (3g/day) o Desmopressin (DDAVP): ADH hormone replacement (SQ or nasal spray)
Anterior Pituitary: Hyperthyroidism:
-‐ A sustained increase in synthesis & release of thyroid hormones by thyroid gland

Nursing Through the Lifespan I Exam 3
12
-‐ Most common form is Graves’ Disease o Autoimmune disease of unknown etiology o Characterized by thyroid enlargement & excessive thyroid hormone secretion o Remissions & exacerbations o Hyperthyroidism & thyrotoxicosis occur together
-‐ Thyrotoxicosis (Thyrotoxic Crisis or Thyroid Storm) o Physiologic effect/clinical syndrome of hypermetabolism o Is the result of increased circulating levels of T3 & T4 o All the symptoms of hyperthyroidism are prominent & severe o Severe tachycardia, heart failure, shock, hyperthermia (up to 105.3°F) o Avoid palpation of thyroid (causes more T3 & T4 to be released)
-‐ Diagnostic Studies: o Decreased TSH levels & elevated free T4 o Total T3 & T4 levels may be assessed, but they are not as definitive
-‐ Drug Therapy: o Pylthiouracil (PTU) & Mehimazole (Tapazole) o Inhibit the synthesis of thyroid hormones o Improvement begins 1-‐2 weeks after start of therapy o Abrupt discontinuation can result in a return of hyperthyroidism
-‐ Radioactive Iodine Therapy: (RAI) o Treatment in nonpregnant adults o Damages or destroys thyroid tissue

Nursing Through the Lifespan I Exam 3
13
o Has a delayed response, maximum effect may not be seen for up to 3 months o Administered on an outpatient basis o Pregnancy test is done before initiation of therapy o May cause dryness & irritation of the mouth & throat o Iodine is mixed with water or juice, sipped through a straw & administered after meals
-‐ Home precautions for RAI: o Flush 2-‐3 times after toilet use o Separately laundering towels, bed linens, & clothes daily o Do not prepare food for others that require prolonged handling with bare hands o Avoid being close to pregnant women or children for 7 days after therapy
-‐ Nutritional Therapy: o A high caloric diet (4,000-‐5,000/day) o Six full meals a day & snacks high in protein & carbs o Avoid highly seasoned & high-‐fiber foods (stimulate the GI tract) o Avoid caffeine containing liquids (increase restlessness & sleep disturbances)
-‐ Thyroidectomy: o Removal of the thyroid gland o Patient is given antithyroid drugs, iodine & beta blockers to achieve a euthyroid state o Oxygen, suction equipment, & a tracheostomy tray should be readily available in the
patient’s room o Pre-‐op Teaching:
! Importance of performing leg exercises ! How to support the head while turning in bed ! Range of motion exercises of the neck ! Talking is likely to be difficult a short time after the surgery ! Routine post op care such as IV infusions
o Post-‐op Complications: ! Hypothyroidism ! Damage or accidental removal of parathyroid glands ! Hemorrhage ! Injury to laryngeal nerve (vocal cord paralysis) (both cords=spastic airway
obstruction) ! Laryngeal Stridor (harsh, vibatory sound during inspiration & expieration) ! Thyrotoxic crisis ! Infection
o Post-‐op Care: ! Assess Q2hrs for signs of hemorrhage or tracheal compression (irregular
breathing, neck swelling, frequent swallowing, sensations of fullness at the incision site, choking, blood on the anterior or posterior dressings)
! Place the pt in semi-‐Fowler’s position & support head with pillows. ! Avoid flexion of the neck & any tension on the suture line ! Monitor vital signs & calcium levels ! Check for tetany (Trousseau’s & Chvostek Signs) ! Control post-‐op pain by giving medications
Nursing Through the Lifespan I Exam 3
14
! Patient ambulates within hours after surgery ! Eats a soft diet the day after surgery ! Permitted to take fluid as soon as tolerated
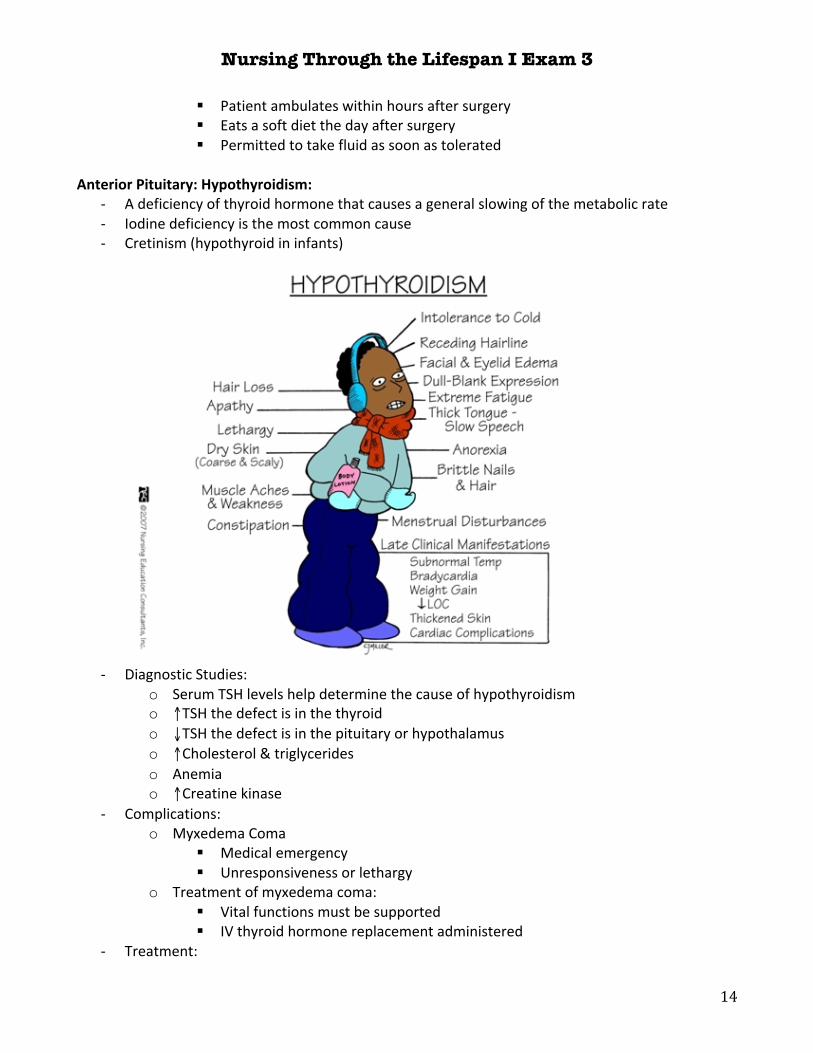
Anterior Pituitary: Hypothyroidism:
-‐ A deficiency of thyroid hormone that causes a general slowing of the metabolic rate -‐ Iodine deficiency is the most common cause -‐ Cretinism (hypothyroid in infants)
-‐ Diagnostic Studies: o Serum TSH levels help determine the cause of hypothyroidism o ↑TSH the defect is in the thyroid o ↓TSH the defect is in the pituitary or hypothalamus o ↑Cholesterol & triglycerides o Anemia o ↑Creatine kinase
-‐ Complications: o Myxedema Coma
! Medical emergency ! Unresponsiveness or lethargy
o Treatment of myxedema coma: ! Vital functions must be supported ! IV thyroid hormone replacement administered
-‐ Treatment:
Nursing Through the Lifespan I Exam 3
15
o Hormone replacement therapy o Levothyroxine (synthroid)
! The drug of choice ! Initial doses are low
o Carefully monitor patients with cardiovascular disease o Monitor heart rate & report pulse >100 beats/min or an irregular heartbeat o Promptly report chest pain, weight loss, nervousness, tremors &/or insomnia
-‐ Patient Teaching: o Discuss the importance of thyroid hormone therapy o Caution patient not to switch brands of the hormone o Emphasize the need for a comfortable warm environment o Teach measures to prevent skin breakdown o Caution the patient to avoid sedatives o Discuss with the patient measures to minimize constipation o Tell patient to avoid using enemas because they produce vagal stimulation
Anterior Pituitary: Hyperparathyroidism:
-‐ An increased secretion of parathyroid hormone (PTH) -‐ PTH helps regulate serum calcium -‐ ↑serum calcium levels -‐ Excessive levels of PTH usually lead to hypercalcemia & hypophosphatemia -‐ Clinical Manifestations:
o Muscle weakness o Loss of appetite o Constipation o Fatigue o Osteoporosis o Fractures o Kidney stones
-‐ Complications: o Renal Failure o Pancreatitis o Cardiac changes o Long bone, rib & vertebral fractures
-‐ Diagnostic Studies: o ↑PTH levels o ↑Serum calcium levels >10mg/dL
-‐ Surgical Therapy o Criteria for surgery:
! ↑Serum calcium levels ! Hypercalciuria ! Markedly reduced bone mineral density ! Those under age 50
o Autotransplantation:
Nursing Through the Lifespan I Exam 3
16
! Normal parathyroid tissue is placed in the forearm -‐ Nonsurgical Therapy:
o High fluid & moderate calcium intake o Several drugs help lower calcium levels but do not treat the underlying cause
Anterior Pituitary: Hypoparathyroidism:
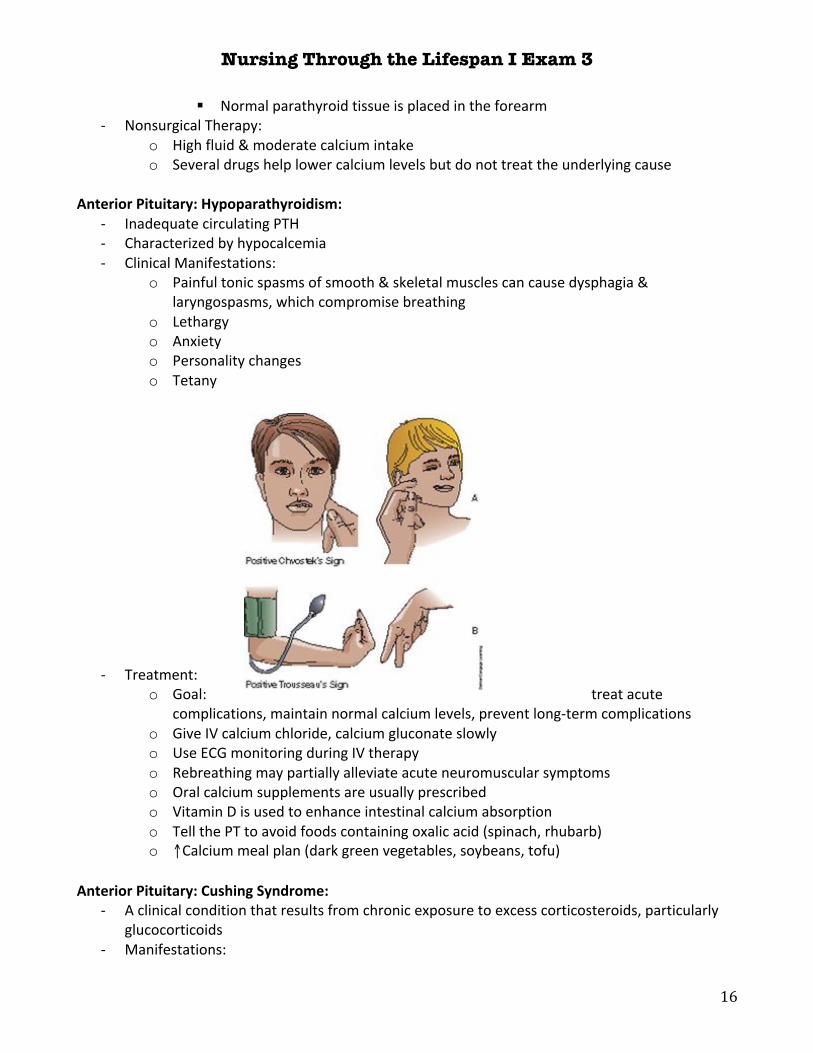
-‐ Inadequate circulating PTH -‐ Characterized by hypocalcemia -‐ Clinical Manifestations:
o Painful tonic spasms of smooth & skeletal muscles can cause dysphagia & laryngospasms, which compromise breathing
o Lethargy o Anxiety o Personality changes o Tetany
-‐ Treatment: o Goal: treat acute
complications, maintain normal calcium levels, prevent long-‐term complications o Give IV calcium chloride, calcium gluconate slowly o Use ECG monitoring during IV therapy o Rebreathing may partially alleviate acute neuromuscular symptoms o Oral calcium supplements are usually prescribed o Vitamin D is used to enhance intestinal calcium absorption o Tell the PT to avoid foods containing oxalic acid (spinach, rhubarb) o ↑Calcium meal plan (dark green vegetables, soybeans, tofu)
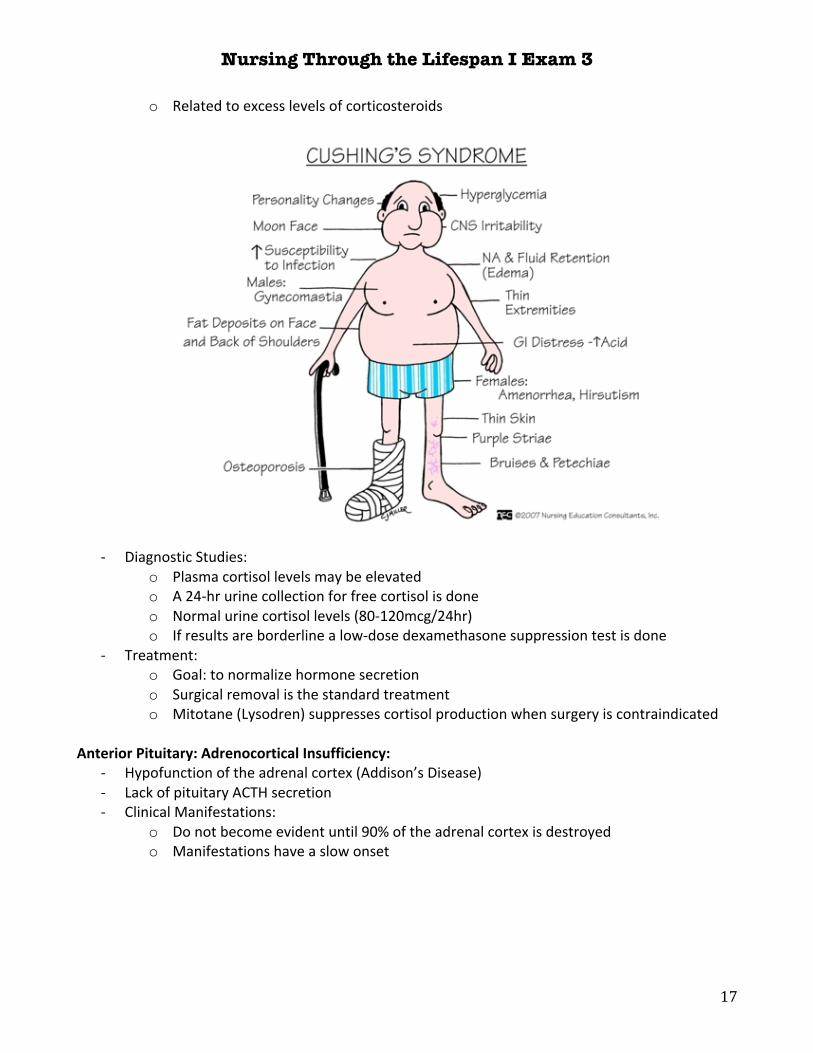
Anterior Pituitary: Cushing Syndrome:
-‐ A clinical condition that results from chronic exposure to excess corticosteroids, particularly glucocorticoids
-‐ Manifestations:
Nursing Through the Lifespan I Exam 3
17
o Related to excess levels of corticosteroids
-‐ Diagnostic Studies: o Plasma cortisol levels may be elevated o A 24-‐hr urine collection for free cortisol is done o Normal urine cortisol levels (80-‐120mcg/24hr) o If results are borderline a low-‐dose dexamethasone suppression test is done
-‐ Treatment: o Goal: to normalize hormone secretion o Surgical removal is the standard treatment o Mitotane (Lysodren) suppresses cortisol production when surgery is contraindicated
Anterior Pituitary: Adrenocortical Insufficiency:
-‐ Hypofunction of the adrenal cortex (Addison’s Disease) -‐ Lack of pituitary ACTH secretion -‐ Clinical Manifestations:
o Do not become evident until 90% of the adrenal cortex is destroyed o Manifestations have a slow onset

Nursing Through the Lifespan I Exam 3
18
-‐ Complications: Addisonian Crisis (acute adrenal insufficiency)
o Life-‐threatening emergency o Insufficient adrenocortical hormones o Triggered by:
! Stress ! Sudden withdrawal of corticosteroid hormone therapy ! Adrenal surgery ! Sudden pituitary gland destruction
o Symptoms: ! Postural hypotension ! Tachycardia ! Dehydration ! Hyponatremia ! Hyperkalemia ! Hypoglycemia ! Fever ! Weakness ! Confusion ! Severe vomiting ! Diarrhea ! Abdominal Pain
-‐ Diagnostic Studies: o Depressed serum & urinary cortisol levels
Nursing Through the Lifespan I Exam 3
19
-‐ Treatment: o Hormone therapy o Hydrocortisone (mineralcorticoid & glucocorticoid properties) o Fludrocortisone (Florinef) mineralcorticoid o Increase salt intake in diet
-‐ Patient Teaching: o The PT should carry an emergency kit at all times
! 100mg IM hydrocortisone ! Syringes ! Instructions for use
Pheochromocytoma:
-‐ Tumor in the adrenal medulla -‐ Excess production of catecholamines (epinephrine & norepinephrine) -‐ Manifestations:
o Severe hypetension o Severe pounding headache o Tachycardia with palpitations o Profuse sweating o Unexplained abdominal or chest pain o Attacks may last from a few minutes to several hours
-‐ Diagnostic Studies: o Measurement of urinary fractionated metanephrines (catecholamine metabolites) o Usually done as a 24-‐hr urine collection
-‐ Treatment: o Surgical removal of tumor o Beta blockers are required pre-‐op to control B/P & to prevent an intraoperative
hypertensive crisis


















