
…Nurses’ Role… - MSICmsic.org.my/filedownloader.asp?filename=asmic2015_MageswaryLapc… · AM...
38
…Nurses’ Role… L.Mageswary Dietitian Hospital Selayang 14 -15 Aug ASMIC 2015
Transcript of …Nurses’ Role… - MSICmsic.org.my/filedownloader.asp?filename=asmic2015_MageswaryLapc… · AM...

…Nurses’ Role…
L.Mageswary Dietitian
Hospital Selayang
14 -15 Aug ASMIC 2015

Doctor
Dietitian
Pharmacist
Nurse Physiotherapist
Occupational therapist
Patient
Patient Centered Care • Patients’ needs & preferences • Good communication between healthcare professionals & patients • To promote & provide education • To develop common protocols and guidelines

Discussion Today…
• Safe EN Orders
• EN Label
• Storage & Administration
• Safe EN Preparation
• Selection and Maintenance of Enteral Access
• EN Complication & Management

Nutrition Screening & Assessment
• Patient Risk for Malnutrition
• Any critically – ill patient who is anticipated to remain unable to take oral nutrition for ≥ 5 days with significant comorbid disease.
• Any patient who has or had oral intake that is inadequate to meet current nutritional needs. (i.e < 50% of estimated required calories for > 5 days)
Weight Height Knee
height Intake/ Output
Appetite
Ability to
swallow and eat

Formula Orders
Orders of EN should be written completely and specifically for each patient:
• Pt demographics (Name, Age, MRN and Bed No.)
• Formula trade name
• Enteral route (gastric or postpyloric) and access (nasogastric NG or nasoduodenal)
• Administration method (pump-assisted or bolus)
• Rate of administration

Label: EN formula administration
• Pt name
• Formula type
• Enteral access
• Administration method
• Name/ initial of those preparing & hanging products
• Date & time of formula preparation and hung
• Expiration date & time
• Not for I.V Use
All feeding bottles, bags
and syringes in feeding pumps
should have label
Always confirm that the correct formula is being given to the patient by comparing the label to the order.

Storage and administration
Check date of expiry
Store unopened formula in a designated dark, dry, cool place, according to institutional protocol and
manufacturer recommendations
Reconstituted formula that’s not used should be immediately refrigerated and discarded within 24 hours
Liquid EN formulas should be used in preference to powdered
• reconstituted formulas has higher risk of contamination
• Blenderised Diet NOT RECOMMENDED
Enteral administration set with a drip chamber is preferable to one with no drip chamber to prevent retrograde bacterial contamination
of the formula during administration.
Preparation of EN
EN formulas be prepared in a clean environment by specially trained personnel using sterile technique.
wearing a disposable mask, gown, gloves, and head cover may reduce the spread of airborne bacteria.
Hand hygiene
• before preparing and administering EN
• When accessing the enteral tube hub, clean each tubing connection with an alcohol swab.
• Between glove changes and when moving from a dirty procedure, such as gastric residual aspiration, to a clean procedure, such as handling the EN formula
Don’t let any part of the delivery system come into contact with non-disinfected hands, skin, clothing, or other surfaces.

Water
• Type of water in EN – Purified Water
• sterile, solute-free, non pyrogenic water • used for preparing or reconstituting commercial products, • rinsing equipment and utensils • required to produce steril water for irrigation and sterile
water for injection.
– Distilled Water • water that has been vaporized and recondensed but is not
necessarily free of dis-solved or suspended matter; therefore should not be used for the preparation or administration of medications.
– Tap Water • municipal or locally-available potable water that meets the
Drinking Water regulations and is consistent with World Health Organization (WHO) guidelines for water safety.

Selection & Maintenance of Enteral access
Type of enteral access is depending on
• Patient’s disease state
• GI anatomy
• GI function
• Estimated length of therapy
• Capacity of patient or caregiver
Devices inserted via the nose or mouth are intended for short-term use, usually no longer than 6 weeks.
An X-ray is the gold standard for confirming the correct position
Bedside checks for placement can be done by testing the pH of the aspirate.
• Fluid from the stomach is typically clear and colorless or grassy green and has a pH of 5 or less
• However, gastric aspirate may not be reliable if a patient is taking a medication to suppress gastric acid, such as famotidine or pantoprazole
• If the tube could possibly have migrated into the lungs, fluid looks pale yellow and has a pH of 7 or higher
The auscultatory method isn’t reliable.
1
2
3
4
5
Selection & Maintenance of Enteral access
• Percutaneous endoscopic gastrostomy (PEG),
• percutaneous endoscopic jejunostomy, and
• Percutaneous endoscopic gastrojejunostomy
Long term feeding devices (> 4 weeks)
• DO NOT USE Urinary drainage catheters or GI drainage – they don’t have external anchoring devices and can migrate, causing
obstruction or aspiration
• Feedings Initiation: within 2 hours of the placement of a PEG tube in adult. – without waiting for flatus or a bowel movement.

EN Formula Hang Time
ASPEN Enteral Nutrition Practice Recommendations 2009
Hang time is defined as the time an EN formula is considered safe for delivery to the patient, beginning from the time when the formula was reconstituted, warmed, or decanted, or from the time when the original package seal was broken.
Administration sets for open systems should be changed at least every 24 hours

Tube Occlusion
• Poor flushing technique
• Interaction between multiple medications and protein-rich formula
• Inappropriate administration of medication
• Mixing of tube feeding formula with gastric fluid during gastric residual
checks
• small-diameter tubes
Loosening and rotating a gastrostomy tube may prevent blockage through mucosal overgrowth and may reduce peristomal infections (grade C).
Do
• Use liquid form drugs when available
• Dilute thick liquid medications to
reduce osmolality
• Consider timing of medication –
empty or full stomach
– Phenytoin
– Warfarin
– Antibiotics (Tetracyclines, Quinolone)
• Flush feeding tube with 15 – 30 ml
water frequently
– Before and after checking residuals
– Before and after feeding
– between medication doses
– Every 4 hourly if continuous feeding
• Choose feeding tube with
appropriate size
Do not
• Use acidic flush fluids
Cranberry juice, carbonated
cola
Water is the best flush fluid
Tube Occlusion
use sterile water in immuno-compromised or critically ill
& Post-pyloric feeding

Enteral Tube Misconnections • Multiple medical committees have convened since 1972 to address
the safety requirements for enteral feeding set connectors and adaptors.
– Color-coding and/or labeling should always be used (doesn’t entirely eliminate the risk)
– Be knowledgeable about • the use of the devices,
• trace all lines back to their origin, and
• ensure that they’re secure.
– Use only oral syringes, not luer-lock syringes, labeled “for oral use only,” to draw up and administer medications into the feeding tube
Golden Standard: Develop and use enteral equipment that is designed to be completely incompatible with all existing I.V. connections

GRV AND ASPIRATION RISK
When should I get worried ?

Gastric Residual Volumes:
Controversial?
• ADA Guidelines 2008 > 250 cc
• Canadian C.P.G. > 250 cc
• ESPEN Guidelines 2006 not addressed
• ASPEN / SCCM > 500 cc
• New Canadian CPG Guidelines late 2009 over
400 cc
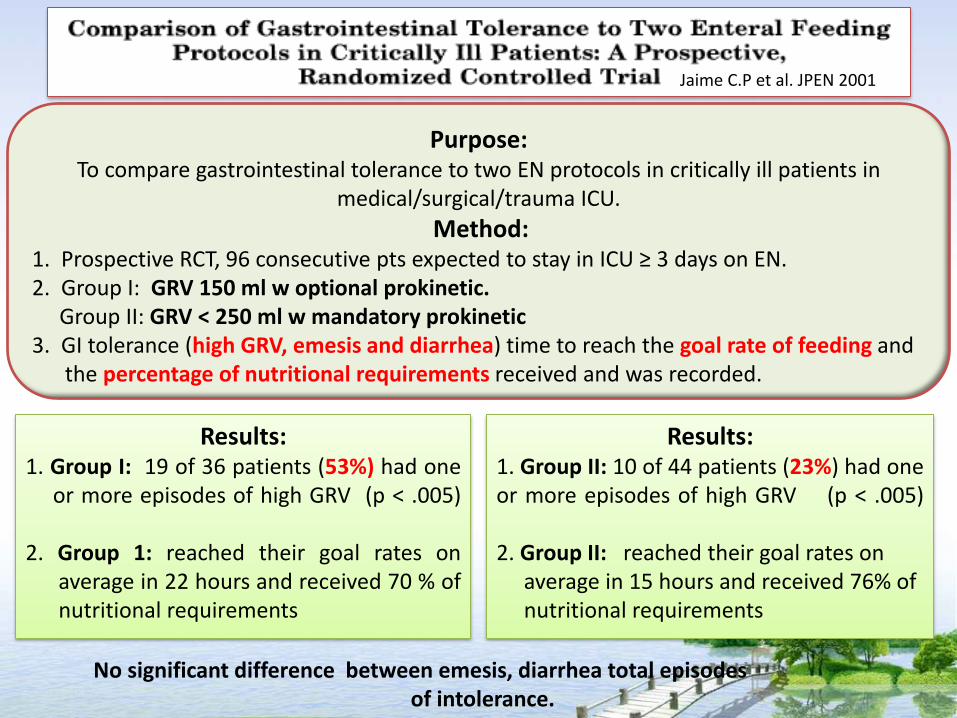
Jaime C.P et al. JPEN 2001
Purpose: To compare gastrointestinal tolerance to two EN protocols in critically ill patients in
medical/surgical/trauma ICU.
Method: 1. Prospective RCT, 96 consecutive pts expected to stay in ICU ≥ 3 days on EN. 2. Group I: GRV 150 ml w optional prokinetic. Group II: GRV < 250 ml w mandatory prokinetic 3. GI tolerance (high GRV, emesis and diarrhea) time to reach the goal rate of feeding and the percentage of nutritional requirements received and was recorded.
Results: 1. Group I: 19 of 36 patients (53%) had one or more episodes of high GRV (p < .005) 2. Group 1: reached their goal rates on average in 22 hours and received 70 % of nutritional requirements
Results: 1. Group II: 10 of 44 patients (23%) had one or more episodes of high GRV (p < .005) 2. Group II: reached their goal rates on average in 15 hours and received 76% of nutritional requirements
No significant difference between emesis, diarrhea total episodes of intolerance.
Jaime C.P et al. JPEN 2001
Conclusion: The incidence of EN intolerance was reduced by using a GRV of 250 mL along
with the mandatory use of prokinetics.
The study showed a trend of improved enteral nutrition provision and reduced the time to reach the goal rate in group II.
These improvements support the adoption of the proposed feeding protocol
for critically ill patients.
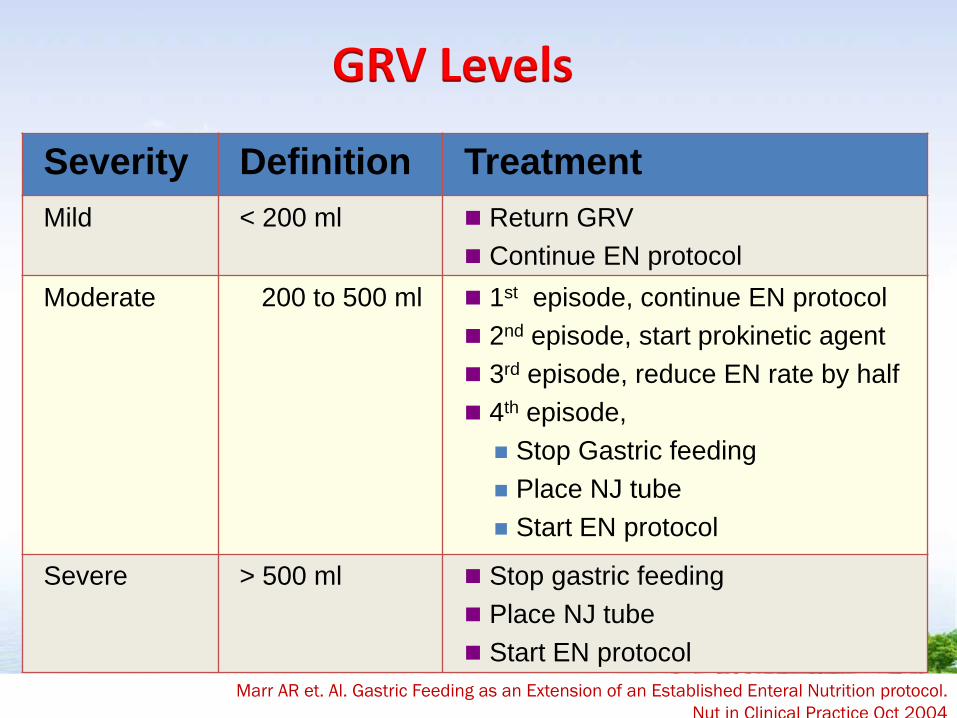
Severity Definition Treatment
Mild < 200 ml Return GRV
Continue EN protocol
Moderate 200 to 500 ml 1st episode, continue EN protocol
2nd episode, start prokinetic agent
3rd episode, reduce EN rate by half
4th episode,
Stop Gastric feeding
Place NJ tube
Start EN protocol
Severe > 500 ml Stop gastric feeding
Place NJ tube
Start EN protocol
Marr AR et. Al. Gastric Feeding as an Extension of an Established Enteral Nutrition protocol.
Nut in Clinical Practice Oct 2004
GRV Levels


Recommendation: To reintroduce gastric content to improve GRV management without
increasing the risk for potential complications

Recommendation Evidence
Level
EN patients should be assessed for aspiration risk E
Elevate head of the bed 30 - 45º in all patients C
Switch to continuous infusion if intolerant D
Initiate agents to promote motility where feasible Prokinetic drugs (metoclopramide and erythromycin) Narcotic antagonists (naloxone and alvimopan)
C
Divert level of feeding by post-pyloric placement C
Use of chlorhexidine mouthwash twice daily to reduce risk of ventilator-associated pneumonia.
C
Reduce Risk of Aspiration

Both gastric enteral feeding and feeding in supine position vs. semi recumbent position, are
independent risk factors for nosocomial pneumonia in ventilated patients
Drakulovic MB, 1999. Lancet 354:1851–58
Prop-up patient at 30 – 45 ° during and after feeding
Head Up Position
To minimise aspiration, patients should be fed propped up by 30° or more and should be kept propped up for 30 minutes after feeding.
Continuous feed should not be given overnight in patients who are
at risk (grade C).
Small bowel fed patients have improved energy delivery in
some studies
Improved tolerance of enteral nutrition and concomitant faster achievement of desired calories
Kortbeek JB J. Trauma 46:992–96
Long term rehabilitation patients should transit to gastric feeding
AM Cook et al. Nutrition Consideration in Traumatic Brain Injury, NCP Dec 2008
Postpyloric tube suggested for high-risk patients in ICU • High gastric residual volume
• Sedation
• Supine position Canadian Clinical Practice Guidelines, JPEN 2003
Small Bowel Feeding

• Quantify stool volume – Is it really diarrhea?
• Review medication list – Switch from IV to enteral route
– Antibiotic prescription
– Sodium and potassium phosphate
– Lactulose
• Check for C. difficile or other infectious causes
• Check hypoalbuminemia
• Try fiber (soluble fiber)
• Check feeding method
• Anti-diarrheal agents once infectious causes are rule out
• Continue to feed
Not Always the Formula
Diarrhea
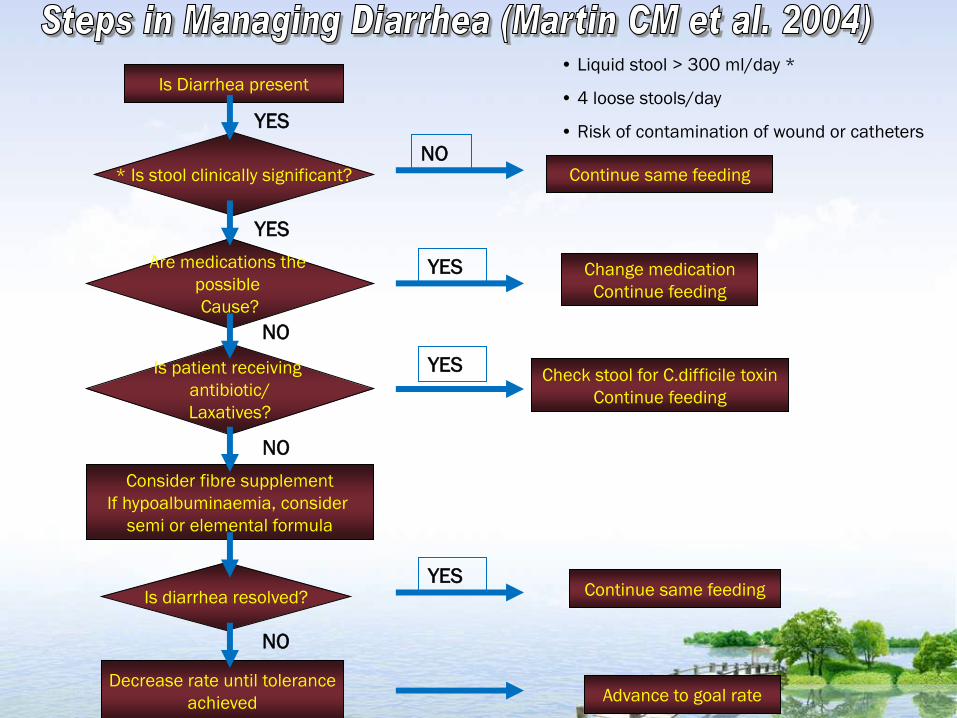
Is Diarrhea present
Continue same feeding
Change medication
Continue feeding
Check stool for C.difficile toxin
Continue feeding
Advance to goal rate
Continue same feeding
Decrease rate until tolerance
achieved
Consider fibre supplement
If hypoalbuminaemia, consider
semi or elemental formula
* Is stool clinically significant?
Are medications the
possible
Cause?
Is patient receiving
antibiotic/
Laxatives?
Is diarrhea resolved?
YES
YES
YES
YES
YES
NO
NO
NO
NO
• Liquid stool > 300 ml/day *
• 4 loose stools/day
• Risk of contamination of wound or catheters
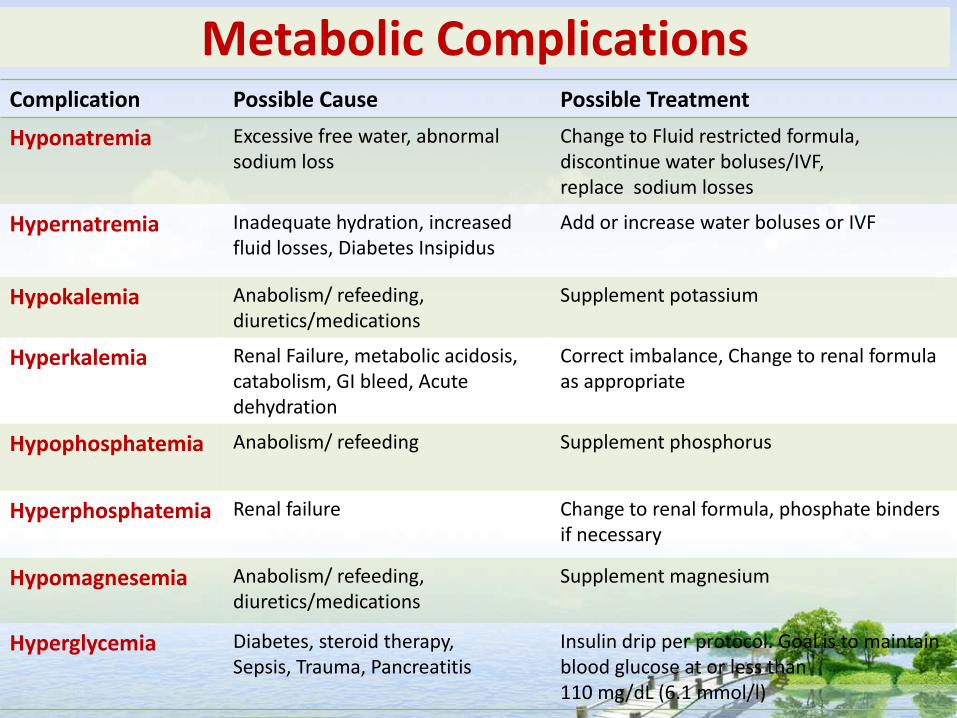
Metabolic Complications Complication Possible Cause Possible Treatment
Hyponatremia Excessive free water, abnormal sodium loss
Change to Fluid restricted formula, discontinue water boluses/IVF, replace sodium losses
Hypernatremia Inadequate hydration, increased fluid losses, Diabetes Insipidus
Add or increase water boluses or IVF
Hypokalemia Anabolism/ refeeding, diuretics/medications
Supplement potassium
Hyperkalemia Renal Failure, metabolic acidosis, catabolism, GI bleed, Acute dehydration
Correct imbalance, Change to renal formula as appropriate
Hypophosphatemia
Anabolism/ refeeding
Supplement phosphorus
Hyperphosphatemia
Renal failure
Change to renal formula, phosphate binders if necessary
Hypomagnesemia Anabolism/ refeeding, diuretics/medications
Supplement magnesium
Hyperglycemia Diabetes, steroid therapy, Sepsis, Trauma, Pancreatitis
Insulin drip per protocol. Goal is to maintain blood glucose at or less than 110 mg/dL (6.1 mmol/l)
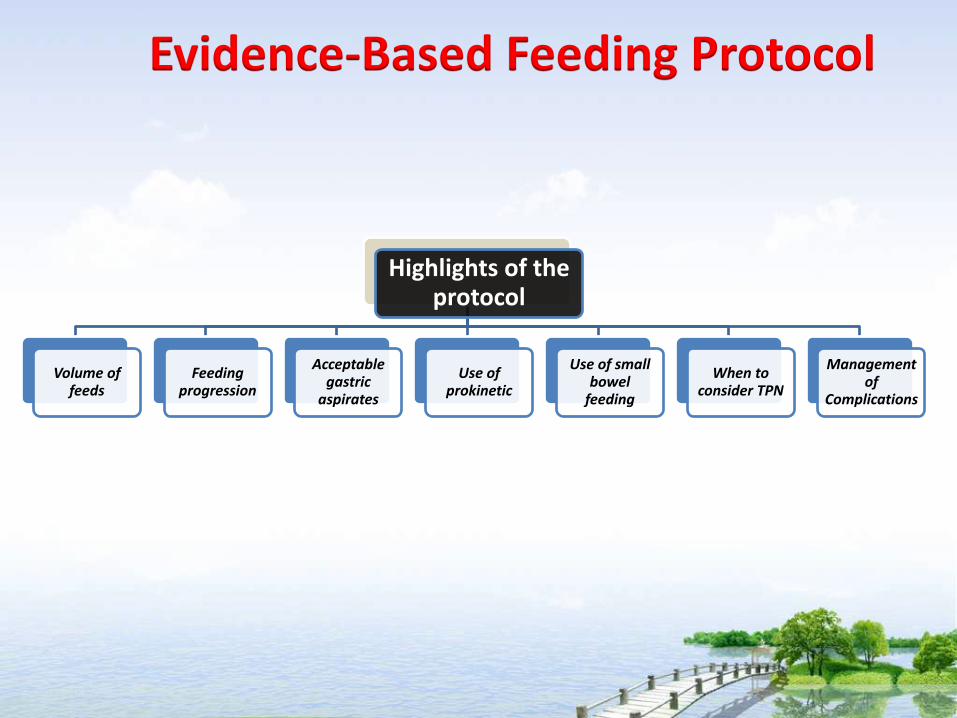
Highlights of the protocol
Volume of feeds
Feeding progression
Acceptable gastric
aspirates
Use of prokinetic
Use of small bowel
feeding
When to consider TPN
Management of
Complications
Evidence-Based Feeding Protocol

Intermittent Feeding Bolus Feeding

At all ward
Hospital Selayang
Storage Preparation
Delivery Cleanliness of utensil

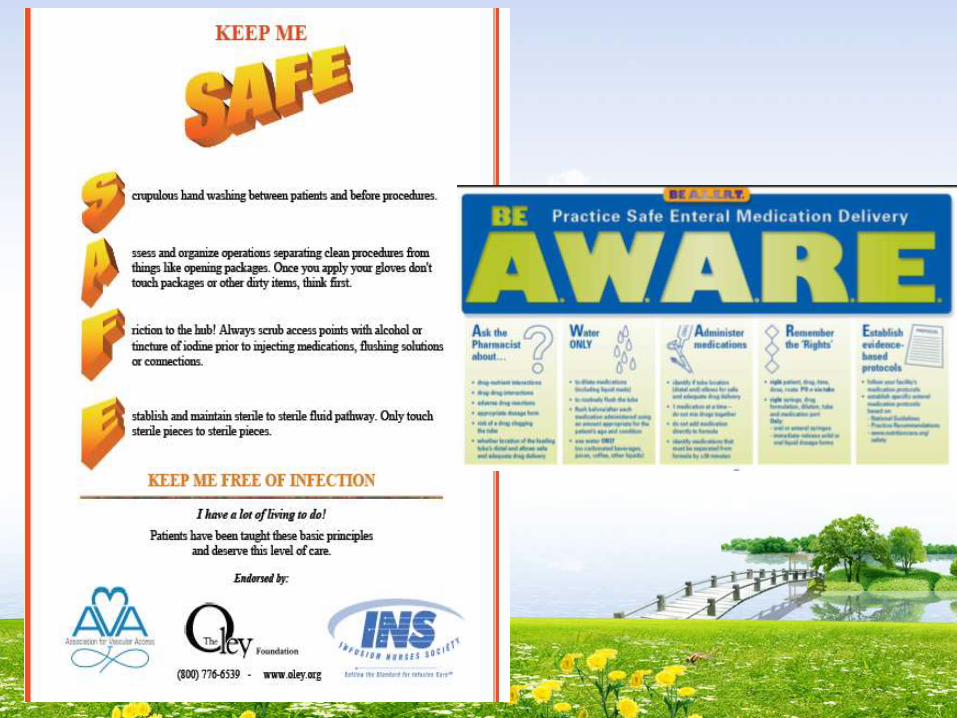

Stay current to keep patient safe
1. Practice hand hygiene and sterile technique
2. Proper patient positioning 3. Appropriate medication administration
technique 4. Good & Safe Nutrition Support Practices 5. Detailed documentation

Continuous Nurses Education in GICU
Feeding Pump Training

Kursus Nutrition Support for Nurses

…Safe Delivery of Nutrition Support Involves Multidisciplinary Approach…
THE MOST IMPORTANT MEMBER ARE
***NURSES***


















