
Nurses are involved in interprofessional collaborative ...
27
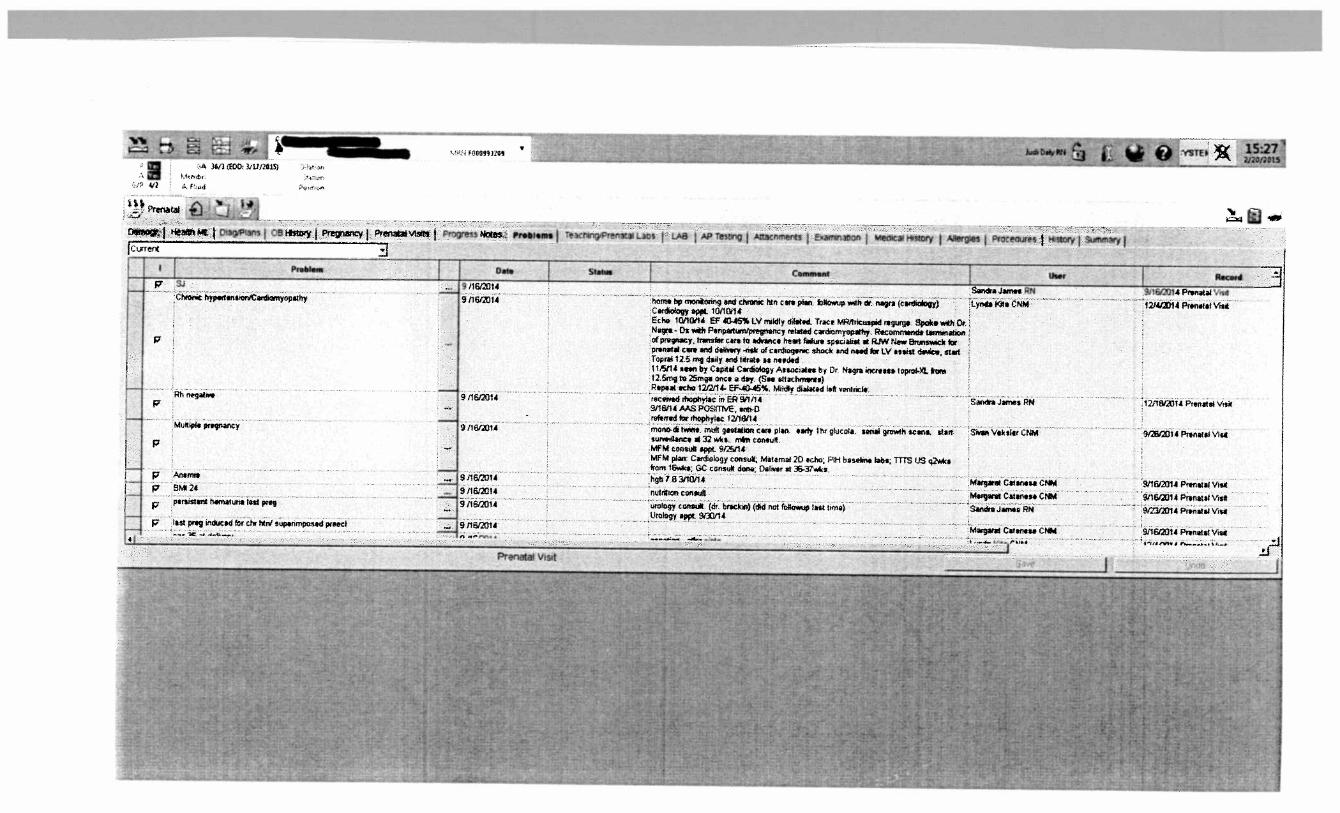
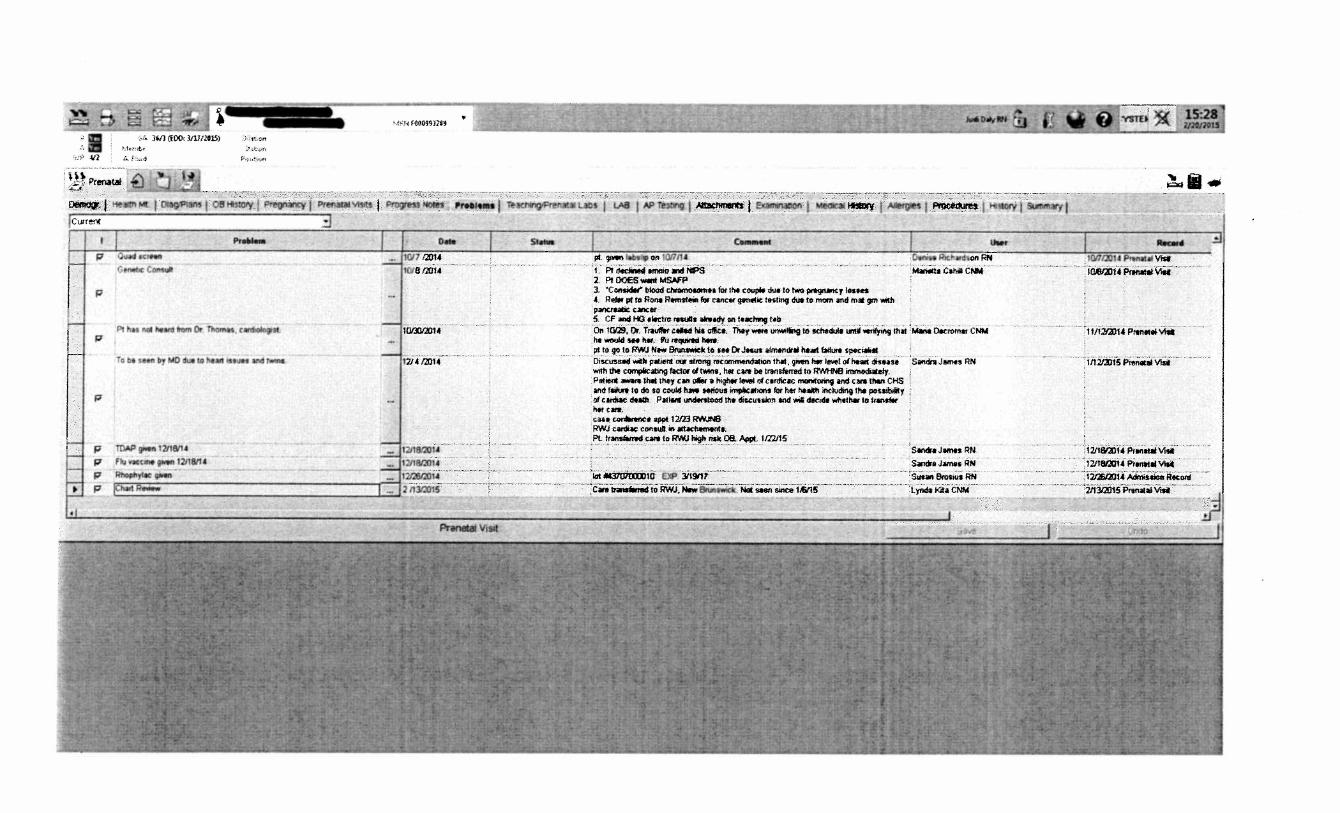
Exemplary Professional Practice Source of Evidence - EP5 Nurses are involved in interprofessional collaborative practice within the care delivery system to ensure care coordination and continuity of care. EP5: Provide two examples, with supporting evidence, of nurses’ involvement in interprofessional collaborative practice that ensures care coordination and continuity of patient care. Example a: High risk obstetrical multidisciplinary case conference Care coordination of services for high risk obstetric (OB) patients is a forum in place for providing continuous, coordinated, and integrated comprehensive services to meet the needs of the patient throughout their pregnancy and post partum period. The OB case conference (CC) is a multidisciplinary approach to meeting these needs and occurs every other Wednesday morning on a regular basis. There are participants from various departments and from various disciplines. These include: • Maternal Fetal Medicine Perinatologists, RNs, Ultrasonographers, and Genetic counselors • Prenatal Clinic Obstetricians, Certified Nurse Midwives, and RN/Case Managers Discussion and facilitation of the individual needs of the patient ensues and specific risk factors that had been identified by the prenatal clinic RN on intake and through follow up testing are addressed. In an effort to coordinate the plan of care, a care management plan is initiated identifying obstetrical issues and co-morbidities (Attachment 1). The attachment is a sample of a Case Conference list with the patient names blocked for reasons of confidentiality. Issues such as significant clinical history, medical needs, substance abuse concerns and other issues are addressed by the team. Prenatal clinic RNs review and update the patient records prior to each scheduled CC. Each CC has an accompanying list of patients for review (Attachment 2). Cases are presented to the multidisciplinary group by the RN, including current status, compliance, psychosocial issues and barriers to care. After group discussion, recommendations are made for referrals and the plan is updated. Attachment 2 shows a specific patient’s documentation following the discussion at CC. Sign in sheets are maintained and the updated electronic plan of care serves as documentation (Attachment 3). The highlighted names are those of nurses who attended the Case Conference in December, 2014. Example b: Pediatric simulation The literature supports that healthcare and academic organizations adopt simulation as a training tool to improve individual and team performance. Simulation is known to reduce human error, assess systems and resources, increase skill development, allow
Transcript of Nurses are involved in interprofessional collaborative ...
Exemplary Professional Practice Source of Evidence - EP5
Nurses are involved in interprofessional collaborative practice within the care delivery system to ensure care coordination and continuity of care.
EP5: Provide two examples, with supporting evidence, of nurses’ involvement in interprofessional collaborative practice that ensures care coordination and continuity of patient care.
Example a: High risk obstetrical multidisciplinary case conference Care coordination of services for high risk obstetric (OB) patients is a forum in place for providing continuous, coordinated, and integrated comprehensive services to meet the needs of the patient throughout their pregnancy and post partum period. The OB case conference (CC) is a multidisciplinary approach to meeting these needs and occurs every other Wednesday morning on a regular basis. There are participants from various departments and from various disciplines. These include:
• Maternal Fetal Medicine Perinatologists, RNs, Ultrasonographers, and Geneticcounselors
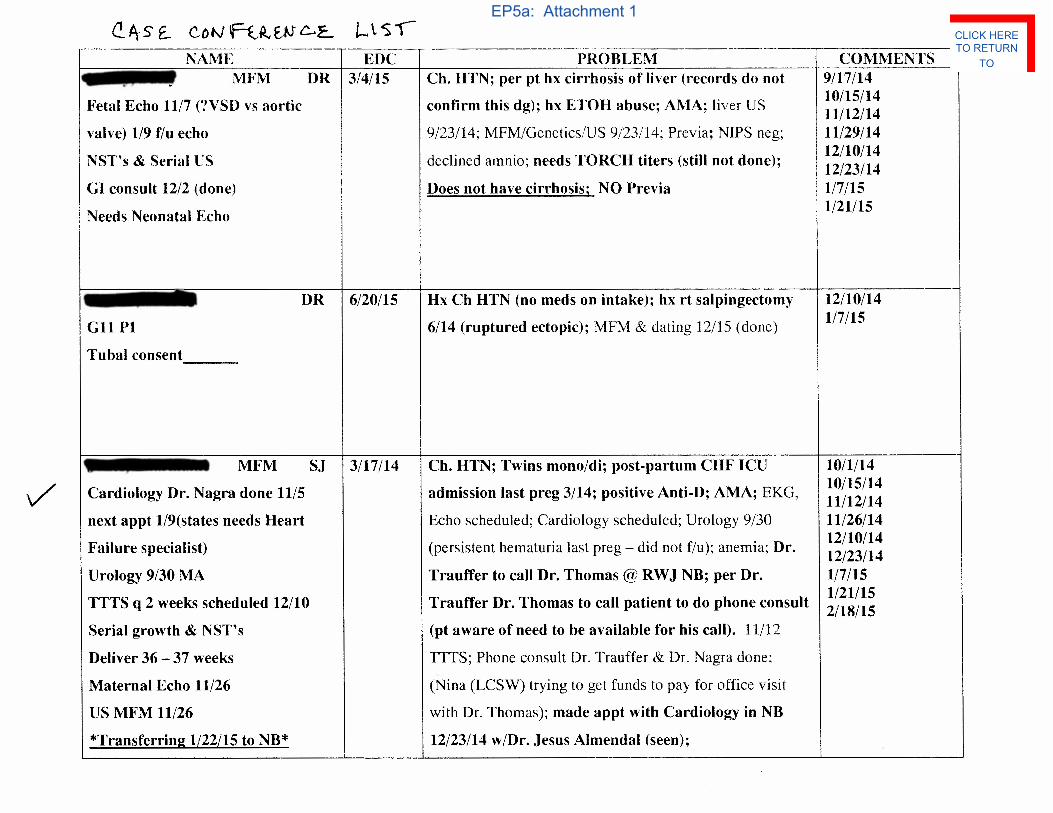
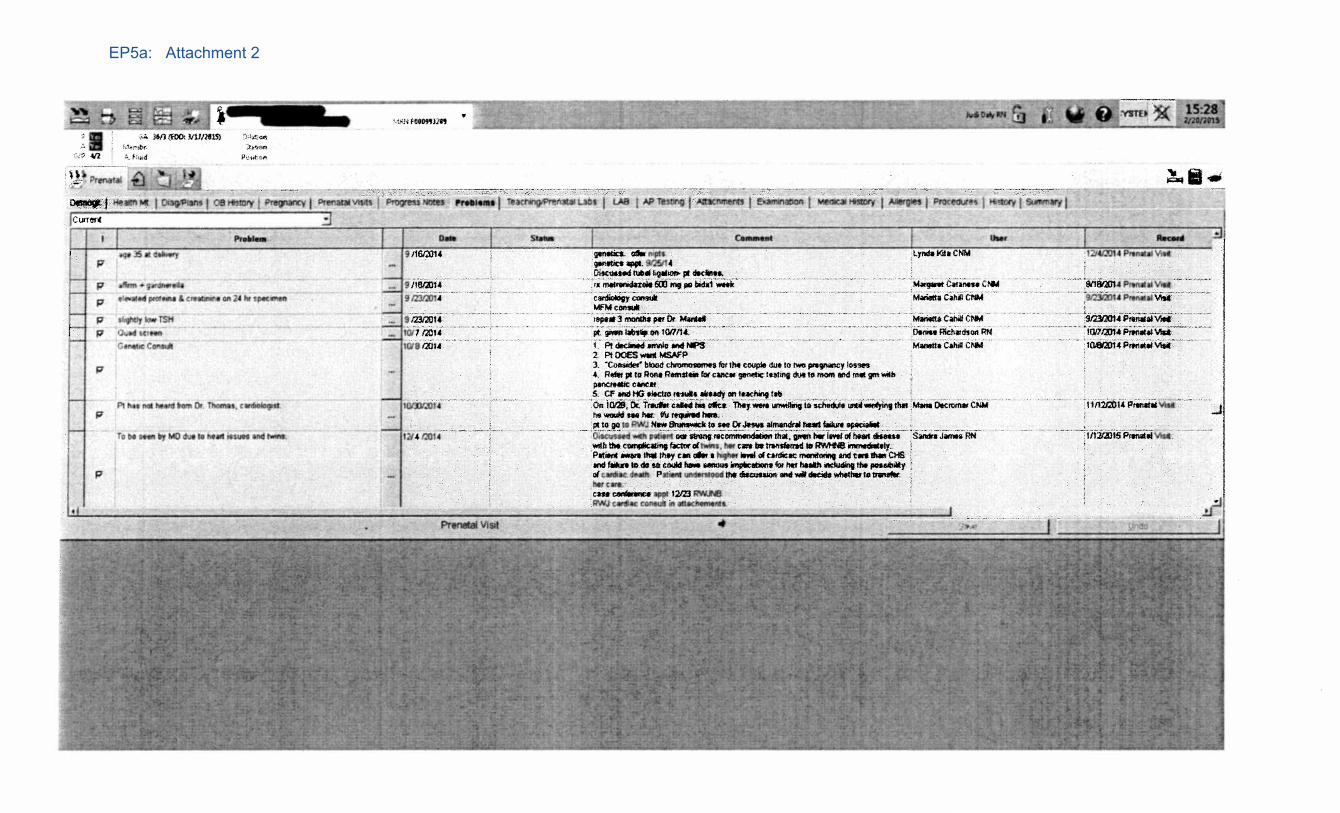
• Prenatal Clinic Obstetricians, Certified Nurse Midwives, and RN/Case ManagersDiscussion and facilitation of the individual needs of the patient ensues and specific risk factors that had been identified by the prenatal clinic RN on intake and through follow up testing are addressed. In an effort to coordinate the plan of care, a care management plan is initiated identifying obstetrical issues and co-morbidities (Attachment 1). The attachment is a sample of a Case Conference list with the patient names blocked for reasons of confidentiality. Issues such as significant clinical history, medical needs, substance abuse concerns and other issues are addressed by the team. Prenatal clinic RNs review and update the patient records prior to each scheduled CC. Each CC has an accompanying list of patients for review (Attachment 2). Cases are presented to the multidisciplinary group by the RN, including current status, compliance, psychosocial issues and barriers to care. After group discussion, recommendations are made for referrals and the plan is updated. Attachment 2 shows a specific patient’s documentation following the discussion at CC. Sign in sheets are maintained and the updated electronic plan of care serves as documentation (Attachment 3). The highlighted names are those of nurses who attended the Case Conference in December, 2014.
Example b: Pediatric simulation The literature supports that healthcare and academic organizations adopt simulation as a training tool to improve individual and team performance. Simulation is known to reduce human error, assess systems and resources, increase skill development, allow
practice in a controlled environment, and provide real life events to gain experience and to meet regulatory requirements. Simulation training assists in developing the health professionals’ knowledge, skills, and attitudes while protecting patients from unnecessary risk as they learn.
In 2010, Pediatric Services (Peds) conducted a research study which was a nurse driven model of pediatric resuscitation: A to D: Resuscitate Me. The model identified roles and responsibilities of the pediatric nurse during a resuscitation. Also, in 2012, proceeds from a hospital sponsored fund raising event were dedicated to Peds. This money was used to purchase a Simulation Junior mannequin (Sim) and its accompanying technology. Subsequently, five RN’s and two medical directors participated in a 2-day training session with the Laerdal representative. This education included: learning the features and capabilities of the Sim, use of the technology (personal computer and attached technology that provides the vital signs and systems e.g. adventitious breath sounds), and building of patient case scenarios that are savedin the system.
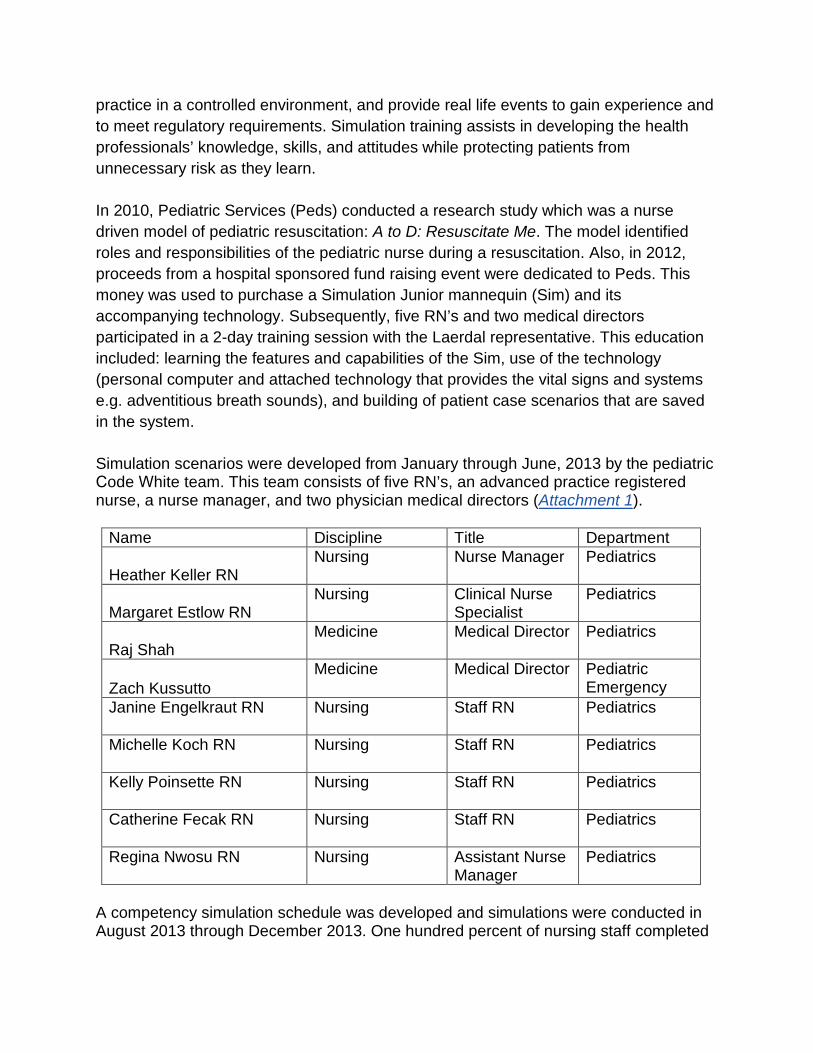
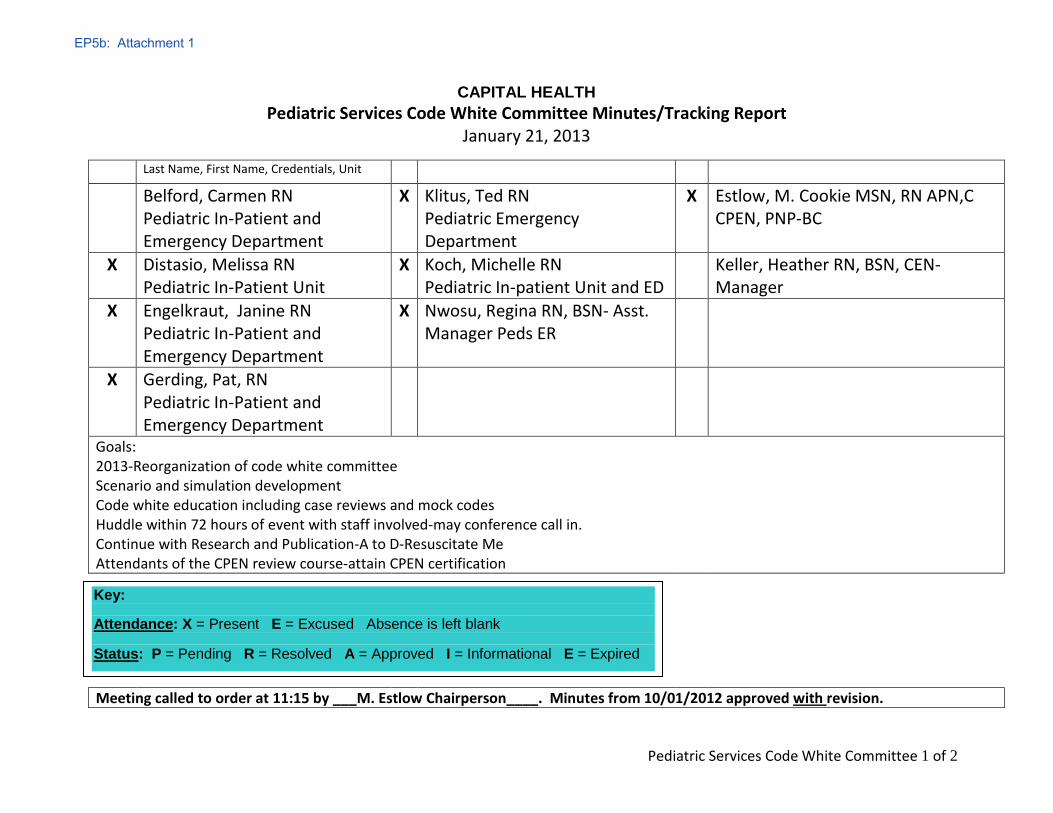
Simulation scenarios were developed from January through June, 2013 by the pediatric Code White team. This team consists of five RN’s, an advanced practice registered nurse, a nurse manager, and two physician medical directors (Attachment 1).
Name Discipline Title Department
Heather Keller RN Nursing Nurse Manager Pediatrics
Margaret Estlow RN Nursing Clinical Nurse
Specialist Pediatrics
Raj Shah Medicine Medical Director Pediatrics
Zach Kussutto Medicine Medical Director Pediatric
Emergency Janine Engelkraut RN Nursing Staff RN Pediatrics
Michelle Koch RN Nursing Staff RN Pediatrics
Kelly Poinsette RN Nursing Staff RN Pediatrics
Catherine Fecak RN Nursing Staff RN Pediatrics
Regina Nwosu RN Nursing Assistant Nurse Manager
Pediatrics
A competency simulation schedule was developed and simulations were conducted in August 2013 through December 2013. One hundred percent of nursing staff completed

the simulations including, upon their return, any nurses that had been on a leave of absence (Attachment 2).
In an effort to maintain competent and proficient pediatric nurses, the simulations incorporated code roles and have become an annual competency. In addition, there is an observation simulation for pediatric emergency education, Code White. These include:
• Airway, breathing, circulation• Emergent blood administration• Sedation• High risk medication administration• Chest tube set up and assistance with
insertion• Central line placement• Intraosseous placement• Troubleshooting equipment• Blood Administration
Competency assessment is by direct observation of the nurse by the Code White committee staff. The nurse is responsible for demonstrating and providing rationale that includes anatomy, physiology, and standards of care. A simulation competency checklist was created based on the various scenarios (Attachment 3).
The nurses have provided feedback that these simulations are beneficial and supportive to their practice. In March 2013, a lecture, Using Simulation to Examine Competence, was included in the Capital Health Annual Joseph Kline Pediatric Symposium (Attachment 4).
References Motolo, I., Devine, L. A., Chung, H. S., et al. (2013). Medical Teacher, Simulation in
Healthcare Education: A best evidence practical guide. AMEE Guide 82, 5(10). Web Paper Abstract.
Cook, D. A., Brydges, R., Zendejas, B., et. Al (2013). Academic Medicine: Mastery Learning for Health Professionals Using Technology-Enhanced Simulation: A Systematic Review and Meta-Analysis, 88(8), 1178-1186.
Billings, D. M., & Halstead, J. A. (2012). Teaching in nursing: A guide for faculty, clinical simulations: An experiential student centered pedagological approach. Fourth ed., Elsevier Publishing.

Exemplary Professional
Practice Exhibits for SOE - EP5
EP5a: Attachment 1
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE
EP5a: Attachment 2
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE
EP5a: Attachment 3
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE
Pediatric Services Code White Committee 1 of 2
CAPITAL HEALTH Pediatric Services Code White Committee Minutes/Tracking Report
January 21, 2013
Last Name, First Name, Credentials, Unit
Belford, Carmen RN Pediatric In-Patient and Emergency Department
X Klitus, Ted RN Pediatric Emergency Department
X Estlow, M. Cookie MSN, RN APN,C CPEN, PNP-BC
X Distasio, Melissa RN Pediatric In-Patient Unit
X Koch, Michelle RN Pediatric In-patient Unit and ED
Keller, Heather RN, BSN, CEN- Manager
X Engelkraut, Janine RN Pediatric In-Patient and Emergency Department
X Nwosu, Regina RN, BSN- Asst. Manager Peds ER
X Gerding, Pat, RN Pediatric In-Patient and Emergency Department
Goals: 2013-Reorganization of code white committee Scenario and simulation development Code white education including case reviews and mock codes Huddle within 72 hours of event with staff involved-may conference call in. Continue with Research and Publication-A to D-Resuscitate Me Attendants of the CPEN review course-attain CPEN certification
Meeting called to order at 11:15 by ___M. Estlow Chairperson____. Minutes from 10/01/2012 approved with revision.
Key:
Attendance: X = Present E = Excused Absence is left blank
Status: P = Pending R = Resolved A = Approved I = Informational E = Expired
EP5b: Attachment 1
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE
Pediatric Services Code White Committee 2 of 2
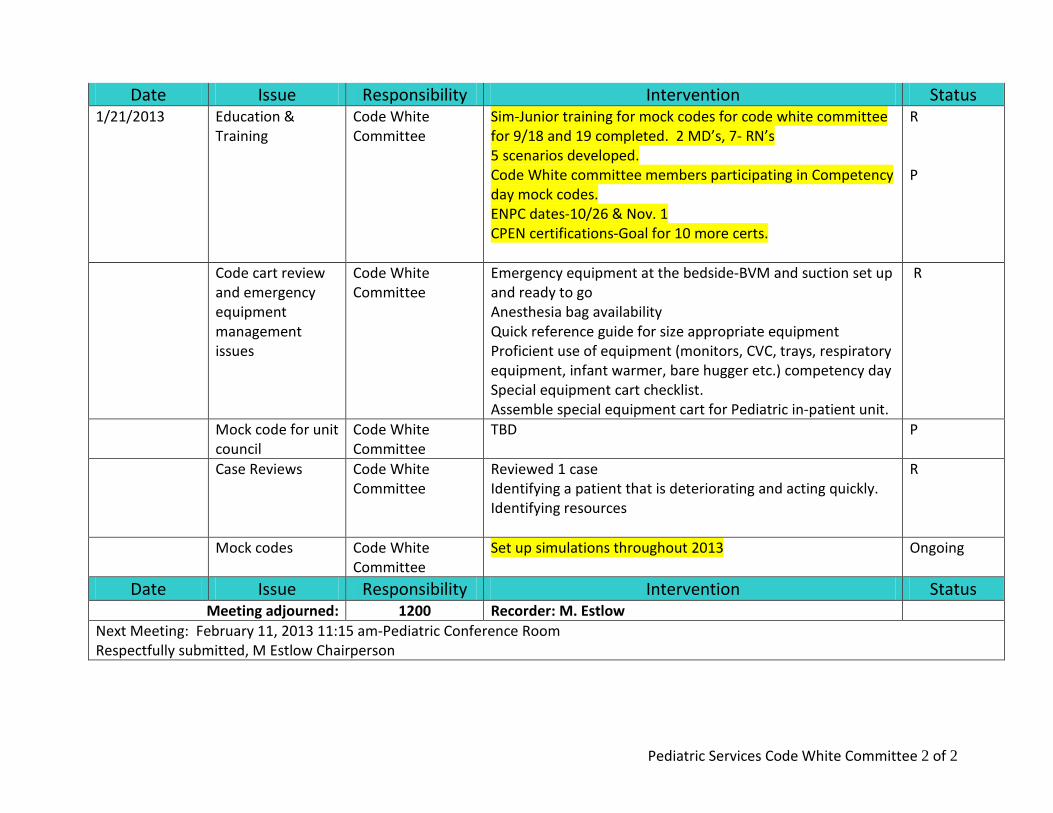
Date Issue Responsibility Intervention Status 1/21/2013 Education &
Training Code White Committee
Sim-Junior training for mock codes for code white committee for 9/18 and 19 completed. 2 MD’s, 7- RN’s 5 scenarios developed. Code White committee members participating in Competency day mock codes. ENPC dates-10/26 & Nov. 1 CPEN certifications-Goal for 10 more certs.
R P
Code cart review and emergency equipment management issues
Code White Committee
Emergency equipment at the bedside-BVM and suction set up and ready to go Anesthesia bag availability Quick reference guide for size appropriate equipment Proficient use of equipment (monitors, CVC, trays, respiratory equipment, infant warmer, bare hugger etc.) competency day Special equipment cart checklist. Assemble special equipment cart for Pediatric in-patient unit.
R
Mock code for unit council
Code White Committee
TBD P
Case Reviews Code White Committee
Reviewed 1 case Identifying a patient that is deteriorating and acting quickly. Identifying resources
R
Mock codes Code White Committee
Set up simulations throughout 2013 Ongoing
Date Issue Responsibility Intervention Status Meeting adjourned: 1200 Recorder: M. Estlow
Next Meeting: February 11, 2013 11:15 am-Pediatric Conference Room Respectfully submitted, M Estlow Chairperson

Pediatric Services Advanced Education Sessions
Critical Thinking Simulation: The nurse should have basic knowledge of Anatomy & Physiology and the most common Pediatric Pathophysiology.
Discuss and Demonstrate assessment and skills that include Advanced Anatomy & Physiology-Airway Management, Respiratory Physiology, Circulatory Physiology. Blood Administration Process Medication administration, Sedation and Pre-medication Practice & Process Assisting with and management of Chest Tube Insertion and Central Line Insertion
Station: 1. Airway- Intubation Equipment/Glidescope/Ventilator/LMA’s/ ETT Stylets/NGT2. Breathing-Ventilation-Ventilator3. Circulation-Access-I/O, Central Lines4. Disability-LOC/ Dextrose (glucometer)5. Code White:
a. Simulation on Sim Juniorb. Code Rolesc. Monitors-Capabilities-ETCO2, Temp monitoring, SAO2, ECG, RRd. Defibrillator-Use ofe. Blood Administration-Access, Set-up and Policyf. Chest Tubes and Central Line Equipment
Wednesday 9/11/2013 9am-11am CR A
Monday 9/16/13 8am-10am Peds ED
Thursday 10/10/13 7am-9am Peds ED
Monday 10/21/13 5pm-7pm Peds ED
11/12/13 and 11/21/13 7am-9am 12pm-2pm 5pm-7pm
TBD
EP5b: Attachment 2
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE

g. Warmer Bed set up h. Medication Calculations-Insulin Infusion, propofol i. DKA Pathophysiology
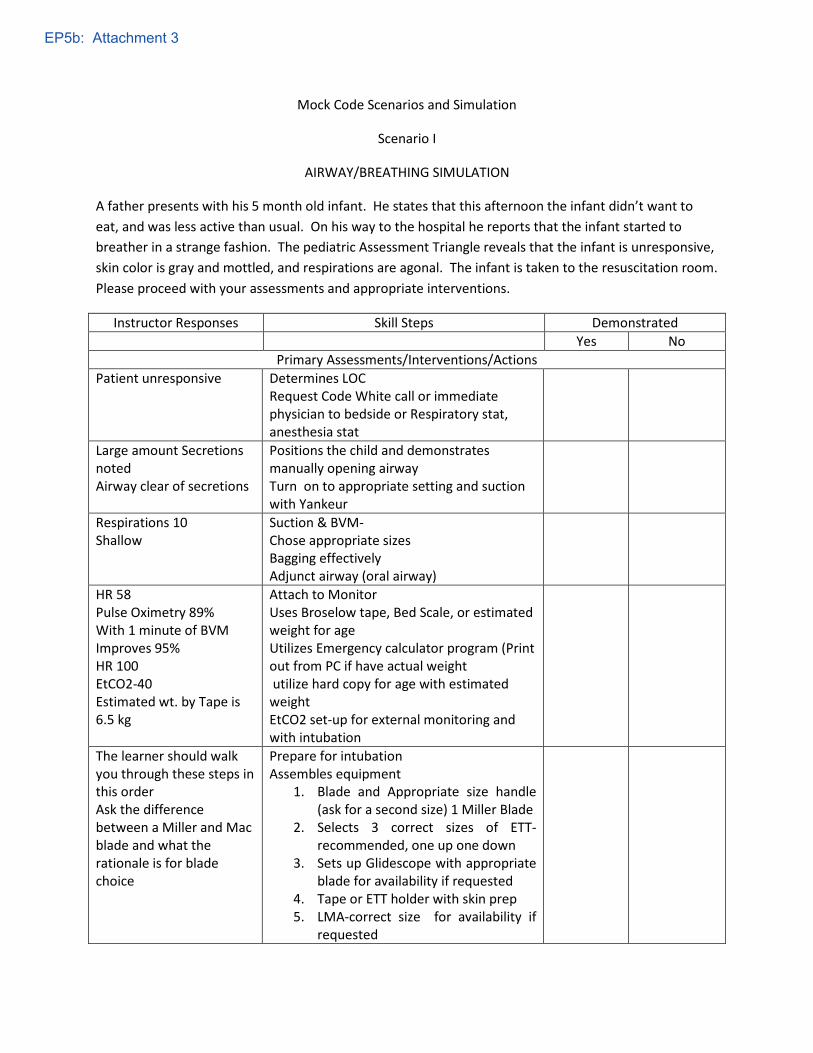
Mock Code Scenarios and Simulation
Scenario I
AIRWAY/BREATHING SIMULATION
A father presents with his 5 month old infant. He states that this afternoon the infant didn’t want to eat, and was less active than usual. On his way to the hospital he reports that the infant started to breather in a strange fashion. The pediatric Assessment Triangle reveals that the infant is unresponsive, skin color is gray and mottled, and respirations are agonal. The infant is taken to the resuscitation room. Please proceed with your assessments and appropriate interventions.
Instructor Responses Skill Steps Demonstrated Yes No
Primary Assessments/Interventions/Actions Patient unresponsive Determines LOC
Request Code White call or immediate physician to bedside or Respiratory stat, anesthesia stat
Large amount Secretions noted Airway clear of secretions
Positions the child and demonstrates manually opening airway Turn on to appropriate setting and suction with Yankeur
Respirations 10 Shallow
Suction & BVM- Chose appropriate sizes Bagging effectively Adjunct airway (oral airway)
HR 58 Pulse Oximetry 89% With 1 minute of BVM Improves 95% HR 100 EtCO2-40 Estimated wt. by Tape is 6.5 kg
Attach to Monitor Uses Broselow tape, Bed Scale, or estimated weight for age Utilizes Emergency calculator program (Print out from PC if have actual weight utilize hard copy for age with estimated weight EtCO2 set-up for external monitoring and with intubation
The learner should walk you through these steps in this order Ask the difference between a Miller and Mac blade and what the rationale is for blade choice
Prepare for intubation Assembles equipment
1. Blade and Appropriate size handle(ask for a second size) 1 Miller Blade
2. Selects 3 correct sizes of ETT-recommended, one up one down
3. Sets up Glidescope with appropriateblade for availability if requested
4. Tape or ETT holder with skin prep5. LMA-correct size for availability if
requested
EP5b: Attachment 3
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE
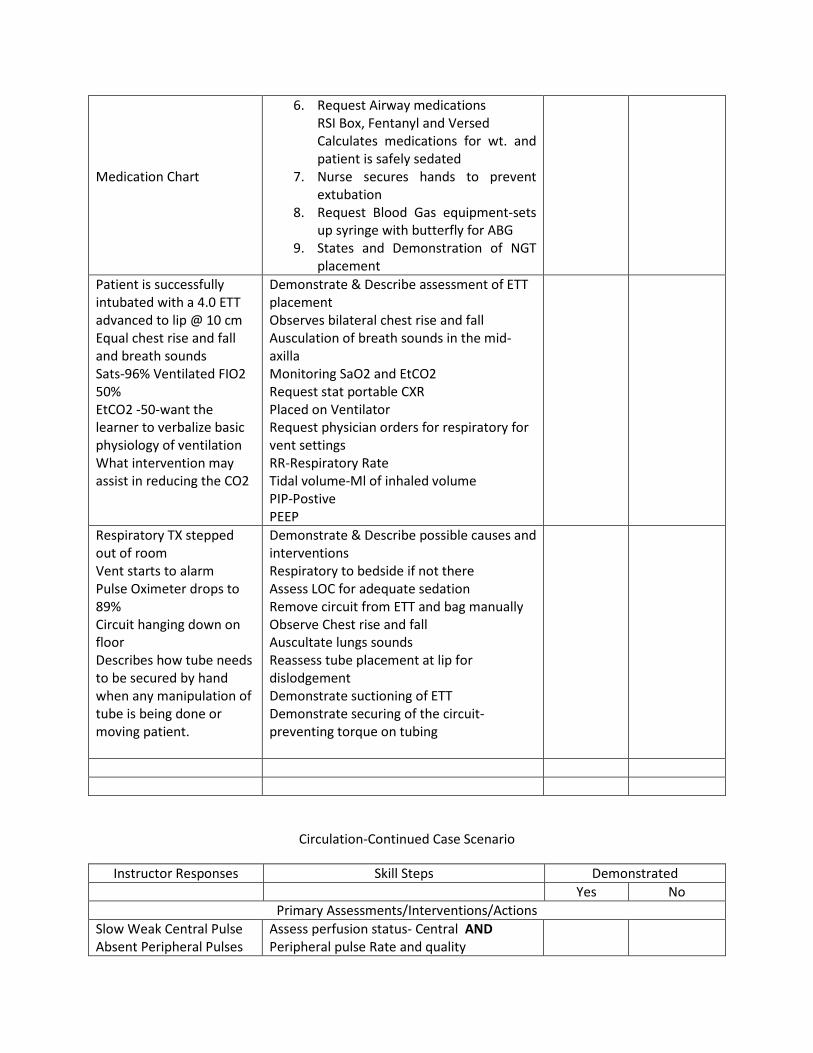
Medication Chart
6. Request Airway medications RSI Box, Fentanyl and Versed Calculates medications for wt. and patient is safely sedated
7. Nurse secures hands to prevent extubation
8. Request Blood Gas equipment-sets up syringe with butterfly for ABG
9. States and Demonstration of NGT placement
Patient is successfully intubated with a 4.0 ETT advanced to lip @ 10 cm Equal chest rise and fall and breath sounds Sats-96% Ventilated FIO2 50% EtCO2 -50-want the learner to verbalize basic physiology of ventilation What intervention may assist in reducing the CO2
Demonstrate & Describe assessment of ETT placement Observes bilateral chest rise and fall Ausculation of breath sounds in the mid- axilla Monitoring SaO2 and EtCO2 Request stat portable CXR Placed on Ventilator Request physician orders for respiratory for vent settings RR-Respiratory Rate Tidal volume-Ml of inhaled volume PIP-Postive PEEP
Respiratory TX stepped out of room Vent starts to alarm Pulse Oximeter drops to 89% Circuit hanging down on floor Describes how tube needs to be secured by hand when any manipulation of tube is being done or moving patient.
Demonstrate & Describe possible causes and interventions Respiratory to bedside if not there Assess LOC for adequate sedation Remove circuit from ETT and bag manually Observe Chest rise and fall Auscultate lungs sounds Reassess tube placement at lip for dislodgement Demonstrate suctioning of ETT Demonstrate securing of the circuit-preventing torque on tubing
Circulation-Continued Case Scenario
Instructor Responses Skill Steps Demonstrated Yes No
Primary Assessments/Interventions/Actions Slow Weak Central Pulse Absent Peripheral Pulses
Assess perfusion status- Central AND Peripheral pulse Rate and quality
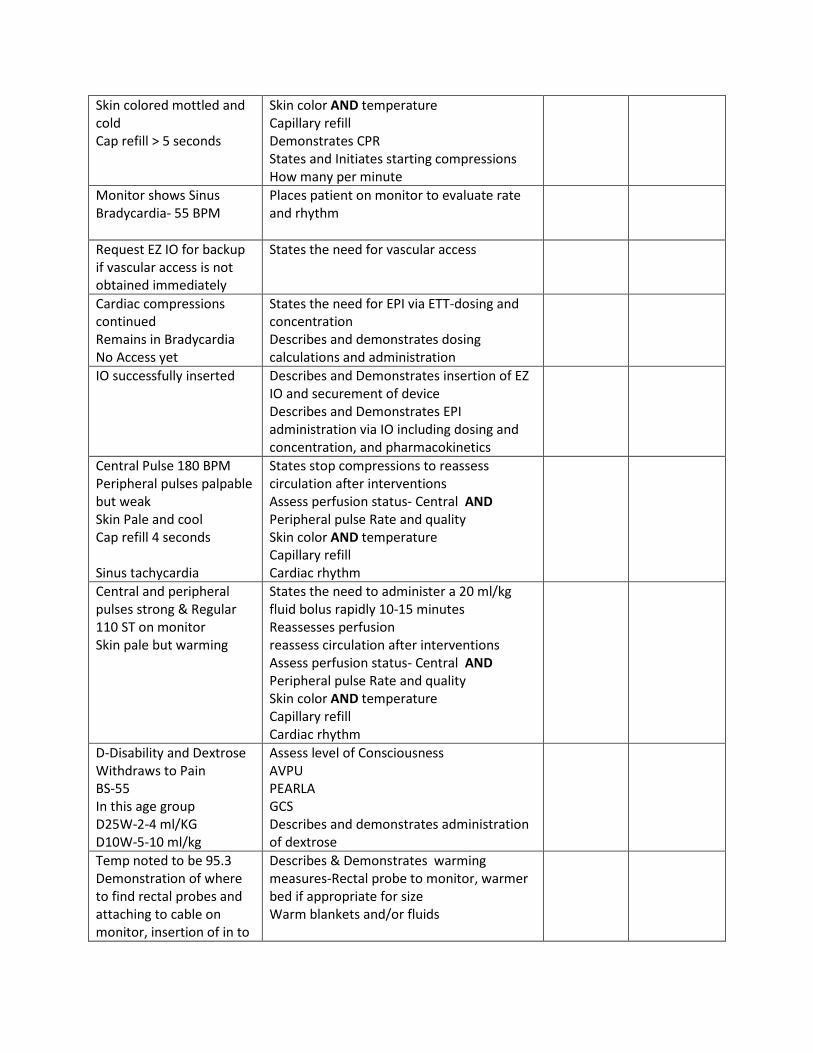
Skin colored mottled and cold Cap refill > 5 seconds
Skin color AND temperature Capillary refill Demonstrates CPR States and Initiates starting compressions How many per minute
Monitor shows Sinus Bradycardia- 55 BPM
Places patient on monitor to evaluate rate and rhythm
Request EZ IO for backup if vascular access is not obtained immediately
States the need for vascular access
Cardiac compressions continued Remains in Bradycardia No Access yet
States the need for EPI via ETT-dosing and concentration Describes and demonstrates dosing calculations and administration
IO successfully inserted Describes and Demonstrates insertion of EZ IO and securement of device Describes and Demonstrates EPI administration via IO including dosing and concentration, and pharmacokinetics
Central Pulse 180 BPM Peripheral pulses palpable but weak Skin Pale and cool Cap refill 4 seconds Sinus tachycardia
States stop compressions to reassess circulation after interventions Assess perfusion status- Central AND Peripheral pulse Rate and quality Skin color AND temperature Capillary refill Cardiac rhythm
Central and peripheral pulses strong & Regular 110 ST on monitor Skin pale but warming
States the need to administer a 20 ml/kg fluid bolus rapidly 10-15 minutes Reassesses perfusion reassess circulation after interventions Assess perfusion status- Central AND Peripheral pulse Rate and quality Skin color AND temperature Capillary refill Cardiac rhythm
D-Disability and Dextrose Withdraws to Pain BS-55 In this age group D25W-2-4 ml/KG D10W-5-10 ml/kg
Assess level of Consciousness AVPU PEARLA GCS Describes and demonstrates administration of dextrose
Temp noted to be 95.3 Demonstration of where to find rectal probes and attaching to cable on monitor, insertion of in to
Describes & Demonstrates warming measures-Rectal probe to monitor, warmer bed if appropriate for size Warm blankets and/or fluids
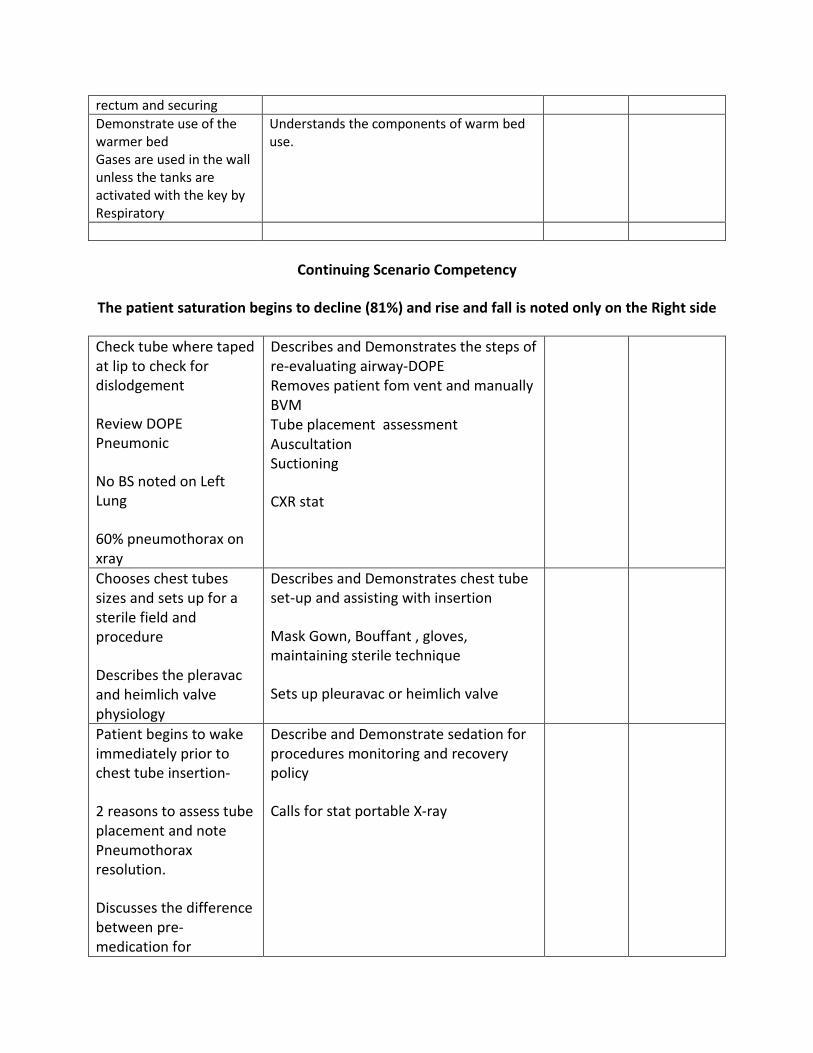
rectum and securing Demonstrate use of the warmer bed Gases are used in the wall unless the tanks are activated with the key by Respiratory
Understands the components of warm bed use.
Continuing Scenario Competency
The patient saturation begins to decline (81%) and rise and fall is noted only on the Right side
Check tube where taped at lip to check for dislodgement
Review DOPE Pneumonic
No BS noted on Left Lung
60% pneumothorax on xray
Describes and Demonstrates the steps of re-evaluating airway-DOPE Removes patient fom vent and manually BVM Tube placement assessment Auscultation Suctioning
CXR stat
Chooses chest tubes sizes and sets up for a sterile field and procedure
Describes the pleravac and heimlich valve physiology
Describes and Demonstrates chest tube set-up and assisting with insertion
Mask Gown, Bouffant , gloves, maintaining sterile technique
Sets up pleuravac or heimlich valve
Patient begins to wake immediately prior to chest tube insertion-
2 reasons to assess tube placement and note Pneumothorax resolution.
Discusses the difference between pre-medication for
Describe and Demonstrate sedation for procedures monitoring and recovery policy
Calls for stat portable X-ray
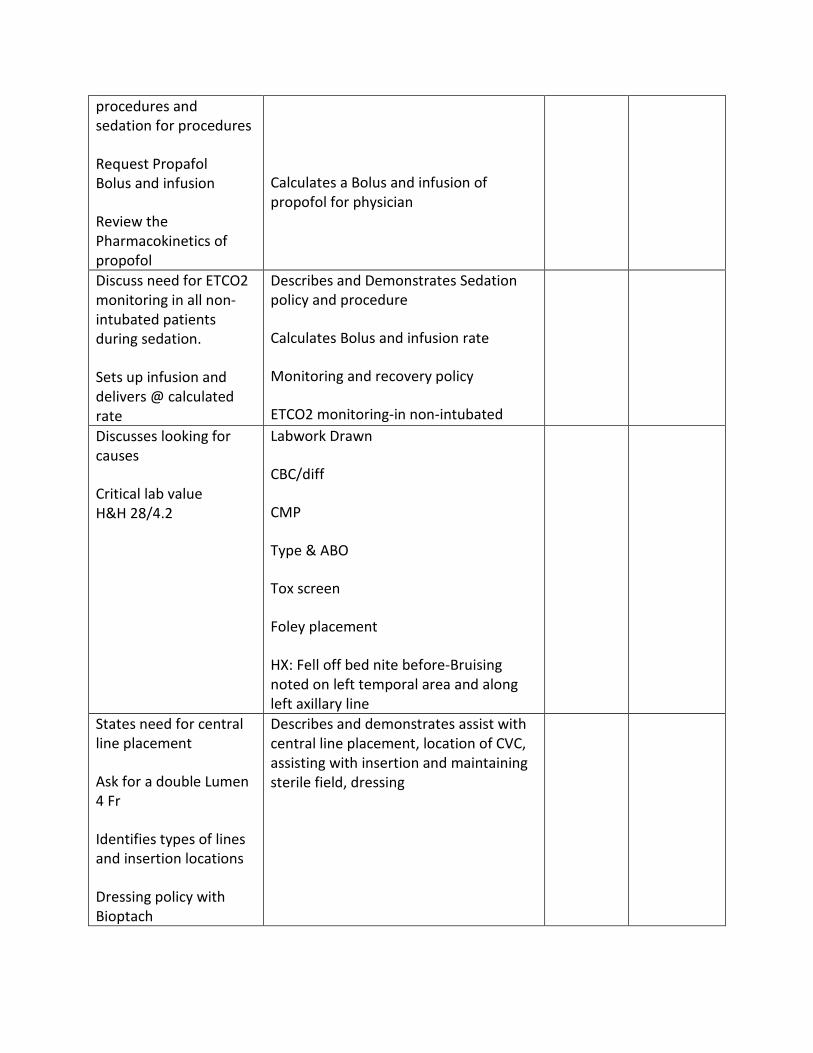
procedures and sedation for procedures
Request Propafol Bolus and infusion
Review the Pharmacokinetics of propofol
Calculates a Bolus and infusion of propofol for physician
Discuss need for ETCO2 monitoring in all non-intubated patients during sedation.
Sets up infusion and delivers @ calculated rate
Describes and Demonstrates Sedation policy and procedure
Calculates Bolus and infusion rate
Monitoring and recovery policy
ETCO2 monitoring-in non-intubated
Discusses looking for causes
Critical lab value H&H 28/4.2
Labwork Drawn
CBC/diff
CMP
Type & ABO
Tox screen
Foley placement
HX: Fell off bed nite before-Bruising noted on left temporal area and along left axillary line
States need for central line placement
Ask for a double Lumen 4 Fr
Identifies types of lines and insertion locations
Dressing policy with Bioptach
Describes and demonstrates assist with central line placement, location of CVC, assisting with insertion and maintaining sterile field, dressing
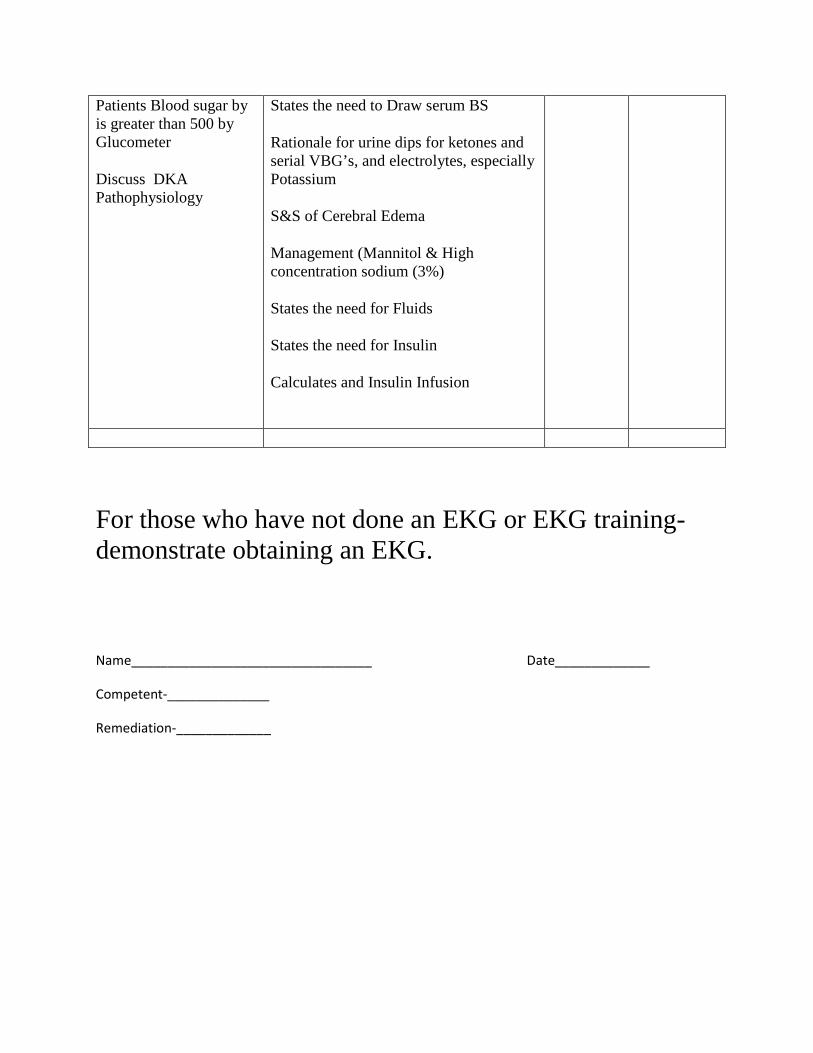
Patients Blood sugar by is greater than 500 by Glucometer
Discuss DKA Pathophysiology
States the need to Draw serum BS
Rationale for urine dips for ketones and serial VBG’s, and electrolytes, especially Potassium
S&S of Cerebral Edema
Management (Mannitol & High concentration sodium (3%)
States the need for Fluids
States the need for Insulin
Calculates and Insulin Infusion
For those who have not done an EKG or EKG training-demonstrate obtaining an EKG.
Name_________________________________ Date_____________
Competent-______________
Remediation-_____________
Attachments:
Respiratory Physiology
Positive end-expiratory pressure (PEEP) is the pressure in the lungs (alveolar pressure) above atmospheric pressure (the pressure outside of the body) that exists at the end of expiration.[1] The two types of PEEP are extrinsic PEEP (PEEP applied by a ventilator) and intrinsic PEEP (PEEP caused by a non-complete exhalation). Pressure that is applied or increased during an inspiration is termed pressure support.
Peak Inspired Pressure (PIP)- Peak inspiratory pressure (PIP) is the highest level of pressure applied to the lungs during inhalation.[1] In mechanical ventilation the number reflects a positive pressure in centimeters of water pressure (cmH2O). In normal breathing, it may sometimes be referred to as the maximal inspiratory pressure (MIPO), which is a negative value.[2]
A chest tube (chest drain, thoracic catheter, tube thoracostomy, or intercostal drain) is a flexible plastic tube that is inserted through the chest wall and into the pleural space or mediastinum. It is used to remove air (pneumothorax[2]) or fluid (pleural effusion, blood, chyle), or pus (empyema) from the intrathoracic space. Chest tubes are commonly made from clear plastics like PVC and soft silicone. Chest tubes are made in a range of sizes measured by their external diameter from 6 Fr to 40 Fr. Chest tubes, like most catheters, a measured in French catheter scale. For adults, 20 Fr to 40 Fr (5 to 11mm internal diameter) are commonly used, and 6 Fr to 26 Fr for children. Conventional chest tubes feature multiple drainage fenestrations in the section of the tube which resides inside the patient, as well as distance markers along the length of the tube, and a radiopaque stripe which outlines the first drainage hole.[6] Chest tubes are also provided in right angle, trocar, flared, and tapered configurations for different drainage needs. As well, some chest tubes are coated with heparin to help prevent thrombus formation, though the effect of this is disputed.[7]
Central Lines-Central venous access, a catheter is inserted into a subclavian, internal jugular, or (less commonly) a femoral vein and advanced toward the heart until it reaches the superior vena cava or right atrium.
Weight in Kg’s Age in Years Size
< 5 kg’s 0-0.5 3 Fr or 4 Fr
> 5 Kg’s 0.5 -1.5 5 Fr to 7 Fr
>15 Kg’s 5-Adult 7 Fr-11 Fr
MEDICATIONS/Pharmacokinetics
In 1948, adrenergic receptors were subdivided into alpha and beta by Ahlquist (a graduate of the University of Washington). The distinction was based on sensitivities of different organs to catecholamines of closely related structure. Regulation of the functions of different organs depends to a greater or lesser extent on alpha or beta receptors. Pharmacological differentiation of alpha and beta receptors, and application of this technology to the treatment of disease, is an outstanding biomedical achievement. Alpha receptors are located postsynaptically at sympathetic neuroeffector junctions of many organs. In general, alpha receptors mediate excitation or increased activity of the effector cells. Vascular smooth muscle is an important site of alpha receptors. SNS activity maintains vascular tone, and thus blood pressure, by maintaining a tone of neurotransmitter on vascular alpha receptors. Beta receptors are also located postsynaptically at sympathetic neuroeffector junctions of many organs. In general, beta receptors mediate relaxation or decreased activity of the effector cells. Thus, blood vessels dilate and uterine smooth muscle relaxes in response to activation of beta receptors. Heart muscle is an important exception to this rule. Activation of beta adrenoceptors in heart increases the automaticity and contractility of all parts of the heart. α-adrenergic receptors, alpha-adrenergic receptors that respond to norepinephrine and to such blocking agents as phenoxybenzamine. They are subdivided into two types: α1, found in smooth muscle, heart, and liver, with effects including vasoconstriction, intestinal relaxation, uterine contraction and pupillary dilation, and α2, found in platelets, vascular smooth muscle, nerve termini, and pancreatic islets, with effects including platelet aggregation, vasoconstriction, and inhibition of norepinephrine release and of insulin secretion. adrenergic receptors receptors for epinephrine or norepinephrine, such as those on effector organs innervated by postganglionic adrenergic fibers of the sympathetic nervous system. β-adrenergic receptors , beta-adrenergic receptor that respond particularly to epinephrine and to such blocking agents as propranolol. They are subdivided into two basic types: β1, in myocardium and causing lipolysis and cardiac stimulation, and β2, in smooth and skeletal muscle and liver and causing bronchodilation and vasodilation. Adrenaline/EPI is used as a drug to treat cardiac arrest and other cardiac dysrhythmias resulting in diminished or absent cardiac output. Its actions are to increase peripheral resistance via α1receptor-dependent vasoconstriction and to increase cardiac output via its binding to β1 receptors.
Epinephrine-is a hormone and neurotransmitter, epinephrine acts on nearly all body tissues. Its actions vary by tissue type and tissue expression of adrenergic receptors. For example, high levels of epinephrine causes smooth muscle relaxation in the airways but causes contraction of the smooth muscle that lines most arterioles.
Epinephrine acts by binding to a variety of adrenergic receptors. Epinephrine is a nonselective agonist of all adrenergic receptors, including the major subtypes α1, α2, β1, β2, and β3.[15] Epinephrine's binding to these receptors triggers a number of metabolic changes. Binding to α-adrenergic receptors inhibits insulin secretion by the pancreas, stimulates glycogenolysis in the liver and muscle, and stimulates glycolysis in muscle.[20] β-Adrenergic receptor binding triggers glucagon secretion in the pancreas, increased adrenocorticotropic hormone (ACTH) secretion by the pituitary gland, and increased lipolysis by adipose tissue. Together, these effects lead to increased blood glucose and fatty acids, providing substrates for energy production within cells throughout the body.[20]
Physiologic responses to epinephrine by organ Organ Effects
Heart Increases heart rate Lungs Increases respiratory rate Systemic Vasoconstriction or vasodilation Liver Stimulates glycogenolysis Systemic Triggers lipolysis Systemic Muscle contraction
Propofol (INN, marketed as Diprivan by AstraZeneca) is a short-acting, intravenously administered hypnotic/amnestic agent. Its uses include the induction and maintenance of general anesthesia, sedation for mechanically ventilated adults, and procedural sedation. Propofol is also commonly used in veterinary medicine. Propofol is not considered an analgesic, so opioids such as fentanyl may be combined with propofol to alleviate pain.[1] Propofol has been referred to as "milk of amnesia" (a play on words of milk of magnesia), because of the milk-like appearance of its intravenous preparation.[2]
Insulin is a peptide hormone, produced by beta cells of the pancreas, and is central to regulating carbohydrate and fat metabolism in the body. Insulin causes cells in the liver, skeletal muscles, and fat tissue to absorb glucose from the blood. In the liver and skeletal muscles, glucose is stored as glycogen, and in fat cells (adipocytes) it is stored as triglycerides.
Insulin stops the use of fat as an energy source by inhibiting the release of glucagon. With the exception of the metabolic disorder diabetes mellitus and metabolic syndrome, insulin is provided within the body in a constant proportion to remove excess glucose from the blood, which otherwise would be toxic. When blood glucose levels fall below a certain level, the body begins to use stored sugar as an energy source through glycogenolysis, which breaks down the

glycogen stored in the liver and muscles into glucose, which can then be utilized as an energy source. As a central metabolic control mechanism, its status is also used as a control signal to other body systems (such as amino acid uptake by body cells). In addition, it has several other anabolic effects throughout the body.
When control of insulin levels fails, diabetes mellitus can result. As a consequence, insulin is used medically to treat some forms of diabetes mellitus. Patients with type 1 diabetes depend on external insulin (most commonly injected subcutaneously) for their survival because the hormone is no longer produced internally.[2] Patients with type 2 diabetes are often insulin resistant and, because of such resistance, may suffer from a "relative" insulin deficiency. Some patients with type 2 diabetes may eventually require insulin if other medications fail to control blood glucose levels adequately. Over 40% of those with Type 2 diabetes require insulin as part of their diabetes management plan.
Pathophysiology of DKA
Diagnosis of DKA was made by using American Diabetes Association (ADA) criteria including serum glucose ≥ 250 mg/dL, serum anion gap > 10 mEq/L, bicarbonate ≤ 18 mEq/L, serum pH ≤ 7.30, and presence of ketosis.
Diagnosing diabetic ketoacidosis (DKA) has traditionally required a venous blood gas (VBG) to obtain serum pH and a serum chemistry panel to obtain electrolyte values.
The patient experiencing DKA presents significantly different from one who is hypoglycemic. This is due to the variation in the pathology of the condition. Like hypoglycemia, by understanding the basic pathophysiology of DKA, there is no need to memorize signs and symptoms in order to recognize and differentiate between hypoglycemia and DKA. Unlike hypoglycemia, where the insulin level is in excess and the blood glucose level is extremely low, DKA is associated with a relative or absolute insulin deficiency and a severely elevated blood glucose level, typically greater than 300 mg/dL. Due to the lack of insulin, tissue such as muscle, fat and the liver are unable to take up glucose. Even though the blood has an extremely elevated amount of circulating glucose, the cells are basically starving. Because the blood brain barrier does not require insulin for glucose to diffuse across, the brain cells are receiving more than an adequate amount of glucose. Basically, the general body tissue is starving while the brain has more than an adequate supply of glucose. Thus, the patient does not experience the sudden onset of signs and symptoms associated with hypoglycemia.
There are three major pathophysiologic syndromes associated with an excessively elevated blood glucose level in DKA: metabolic acidosis, osmotic diuresis and an electrolyte disturbance.
Due to the lack of insulin, cells are not receiving an adequate fuel source to produce energy. Even though the blood is loaded with glucose, the cells go into a starvation mode. This triggers the release of glucagon and other counter-regulatory hormones that promote the breakdown of triglycerides into free fatty acids and initiate gluconeogenesis to produce more glucose for the starving cells. This further elevates the blood glucose level as the body begins to metabolize protein and fat to produce a source of energy. Due to the insulin deficiency and release of large amounts of glucagon, free fatty acids circulate in abundance in the blood and are metabolized into acetoacetic acid and B-hydroxybutric acid — both of which are strong organic acids and are referred to as ketones. As acetoacetic acid is metabolized it produces acetone, which begins to accumulate in the blood. Small amounts of acetone are released in respiration and produce the characteristic “fruity breath” odor. In normal metabolism, ketones would be used as fuel in the peripheral tissue; however, due to the starvation state of the cells, the ketones are not used. An increase in ketone production and a decrease in peripheral cell use lead to metabolic acidosis – also called ketoacidosis. This is reflected in a decreasing pH value typically less than 7.40. The patient will also begin to eliminate large amounts of ketones through excretion in the urine. Typically, when the blood glucose level reaches approximately 225 mg/dL a significant amount of glucose spills over into the urine. A glucose molecule produces an osmotic effect by drawing water across a semipermeable membrane. As an excessive amount of glucose enters the renal tubules, it draws a large amount of water that ends up producing a significant amount of urine. This is known as osmotic diuresis and leads to volume depletion and dehydration in the patient. Large amounts of ketones also collect in the urine. Because ketones are strong organic acids, they must be buffered in order to be excreted. Sodium is typically used as the buffer. As we have been instructed, where sodium goes, water follows. Thus, the sodium used to buffer the ketones also draws a large amount of water into the renal tubules, which produces excessive urine and leads to further volume depletion and dehydration. The loss of large amounts of fluid also leads to the excretion of other electrolytes, such as potassium, calcium, magnesium and phosphorous. This produces electrolyte imbalance and disturbances.

AccreditAtionCapital Health System is accredited by the Medical Society of New Jersey to provide continuing medical education for physicians. Capital Health designates this educational activity for a maximum of (pending) AMA PRA Category I Credit(s). Physicians should only claim credit commensurate with the extent of their participation in the activity.
Capital Health System is an approved provider of continuing nursing education by the New Jersey State Nurses Association, an accredited approver by the American Nurses Credentialing Center’s COA. Provider Number P122-3/10-13.
HistoryDr. Joseph Kline practiced pediatric medicinefor 37 years at his hospital“home,” Mercer Medical Center. He cared for children, as an intern, active physician, chair of the pediatric department, and friend. In 1992, for his 80th birthday, his family and friends established the Dr. Joseph Kline Pediatric Lecture Fund. Since 2001, it along with Capital Health has been providing an annual symposium to further the education of pediatric care for professionals caring for children in the region.
PurPoseThis program is designed to enhance the participants’ knowledge regarding advances in cutting edge pediatric care in a community medical center. Target audience: Pediatricians, APN’s, Pediatric RN’s, ED RN’s, Case Management, Respiratory Therapist, Residents, Students (Medical school, PA’s, APN,s, Nursing).
PlAnning committeeKaren Adamczyck, BSN, RNCMargaret M Estlow, MSN, CPEN, PNP-BCPamela Graziadei, MSN, RNZach Kassutto, MDHeather Keller, BSN, CENJill Mahony, MSN, APN, CRajeev Shah, MD
cutting edge cAre for PediAtric PAtients
March 22, 2013
7:30 a.m. - 4 p.m.
Capital Health Medical Center - HopewellOne Capital Way | Pennington, NJ
capitalhealth.org
The 10Th AnnuAl DR. Joseph Kline peDiATRic syMposiuM
One
Cap
ital W
ayPe
nnin
gto
n, N
J 08
534
cu
ttin
g e
dg
e c
Ar
e f
or
P
ed
iAtr
ic P
Ati
en
ts
Mar
ch 2
2, 2
013
7:30
a.m
. - 4
p.m
.
Cap
ital H
ealth
Med
ical
Cen
ter
- H
op
ewel
lO
ne C
apita
l Way
| Pe
nnin
gto
n, N
J
The
10Th
An
nu
Al
DR
. Jo
seph
Kli
ne
pe
DiA
TRic
sy
Mpo
siu
M
feAtured sPeAkersRichard Drachtman, MDProfessor of Pediatrics, Robert Wood Johnson Medical School/UMDNJInterim Chief, Pediatric Hematology/Oncology Division at the Pediatric Hematology Oncology Cancer Institute of New JerseyRobert Wood Johnson-University HospitalNew Brunswick, NJ
Judi Galter, Msn, cRnpNeonatal Nurse PractitionerSt. Christopher’s Hospital for ChildrenHahnemann University Hospital, Philadelphia, PA
Zach Kassutto, MD, FAApMedical Director, Pediatric Emergency MedicineCapital HealthAssistant Professor of Pediatrics and Emergency Medicine, Drexel University College of Medicine
Achintya Moulick, MD, Ms, Mch, MBAChief, Department of Cardiac SurgeryCo-Director of the Heart CenterSt. Christopher’s Hospital for Children
nadine schwartz, MDAssistant Professor of PsychiatryDrexel University College of MedicineDirector of the Child & Adolescent Psychiatry Service, St. Christopher’s Hospital for Children Philadelphia, PA
linda Wilson, Rn, phD, cpAn, cApA, Bc, cne, chseAssistant Dean for Special Projects,Simulation and CNE AccreditationDrexel University, College of Nursing and Health Professions, Philadelphia, PA
If minimum registration numbers are not achieved Capital Health reserves the right to cancel program.
EP5b: Attachment 4
ndoolan
Text Box
CLICK HERE TO RETURN TO NARRATIVE
leArning objectives• Describe treatment options for the pediatric
patient with mild to moderate head injury
• Name clinical criteria that are associated with clinically important head injuries in children
• List current criteria and risks for imaging pediatric patients with mild to moderate head injury
• Describe the difficult balance of managing parental expectations/demands vs. evidence based guidelines
• Identify congenital heart patients in the Emergency Department (ED)
• Illustrate the appropriate tests for identifying the congenital heart defects
• Discuss the management of patients in the ED with single versus two ventricle pathology
• Discuss strategies to optimize management of patients with autism spectrum disorders in the pediatric ED and inpatient medical settings
• List the psychotropic medications currently approved for children with autism and typical indications for their utilization
• Classify the variable response children with autism may exhibit to commonly used psychotropic medications
• Review recent developments in the management of sickle cell disease
• Compare and contrast clinical criteria in the sickle cell patient for admission to the hospital and for transfer to a higher level of care
• Identify infants at increased risk for hypoglycemia and at increased risk for hypothermia
• Evaluate the degree of respiratory distress in neonates
• State presentation, causes, and initial treatment of hypovolemic, cardiogenic, and septic shock
• Demonstrate simulation techniques for establishing competency, using the Human Patient Simulator in both standardized and hybrid scenarios
cut
her
e
#
PAyment
Please make checks payable to: capital Health foundation
Forward registration & payment to:department of clinical education
capital Health one capital Way | Pennington, nj 08534
609.394.4027
Fax form to 609.815.7231 or register online atcapitalhealth.org/events to reserve your space
Payment must be obtained prior to presentation to attend.
Full refund for cancellations received up to 5 working days before program date. 50% cancellation policy after that date.
For more information, please contact: margaret estlow 609.303.4373 or kathy bayrasli 609.303.4513
Name
Profession
Organization
Home Address
City State Zip
Phone (H) (W)
Cell
(PLEASE PRINT)
registrAtion form
Registration is required. Registration deadline: MARCH 15, 2013
(Seating is limited)
registrAtion fee: (Fees include all handouts)
Capital Health Employees $20/person
Non-Employees $30/person
(Please copy this registration form as needed)
scHedule7:45-8:25a.m. Registration
(Continental breakfast)
8:25a.m. Welcome
morning session
8:30 -9:25a.m. The Emergent Management of Mild to Moderate Head Injury Zach Kassuto, MD, FAAP
9:30-10:25a.m. Emergency Management of a Pediatric Congenital Heart Patient in the ED Achintya Moulick, MD, MS, MCh, MBA
10:25-10:30a.m. Break
10:30-11:15a.m. Approach to Management of Children with Autism in the ED and In-Patient Unit Floor Nadine Schwartz, MD
11:15-11:55a.m. Sickle Cell Disease: An Update Richard Drachtman, MD
11:55-12p.m. Question, AnswerMorning session evaluations (CME/CH)
12:00-12:45p.m. Lunch provided
Afternoon session (Nurses, Respiratory Therapist, Students)
12:45-1:45p.m. Management of the Neonate in the Emergency Department Judi Galter, MSN, CRNP
1:45-1:55p.m. Break
1:55- 3:10p.m. Using Simulation to Examine Competence Linda Wilson, PhD, RN, CPAN, CAPA, BC, CNE, CHSE
3:10-3:55p.m. CE Evaluations
cutting edge cAre for PediAtric PAtients


















