Nurse Practitioners: Breaking Down Barriers to · PDF fileNurse Practitioners: Breaking Down...
27
August 20, 2013 Nurse Practitioners: Breaking Down Barriers to Practice Joanne T. Clavelle DNP, RN, NEA-BC, FACHE Vice President, Patient Care Services Chief Nursing Officer August 23, 2013 Nurse Practitioners of Idaho 2013 Annual Fall Conference
Transcript of Nurse Practitioners: Breaking Down Barriers to · PDF fileNurse Practitioners: Breaking Down...

August 20, 2013
Nurse Practitioners: Breaking Down
Barriers to Practice
Joanne T. Clavelle DNP, RN, NEA-BC, FACHE
Vice President, Patient Care Services
Chief Nursing Officer
August 23, 2013
Nurse Practitioners of Idaho 2013
Annual Fall Conference

Objectives
• Understand context for Nurse Practitioner (NP) practice:
IOM Future of Nursing Report
Elements of the Accountable Care Act (ACA)
Regional trends increasing demand
• Cite common barriers to NPs practicing to their full scope of
practice
• Review St. Luke’s case study:
Apply a collaborative organizational change model to
promote expanded privileges across the care continuum
Foster collaborative relationships with medical staff in
designing new models of care
• Examine service/academic partnerships and impact upon NP
supply
• Identify resources to lead through assessment and change
• Questions
2

Context for Practice
• IOM Future of Nursing Report
Blueprint to transform nursing practice, patient
care & education
Nurse leaders participate in redesign and
improvement in full partnership with physicians
Ensure that nurses can practice to full extent of
their education and training
Improve data collection for workforce planning
and policy-making

IOM Future of Nursing Report
• Messages
Nurses should be able to practice to full extent
of their education and training
Nurses should be full partners with physicians
and others in redesigning U.S. health care
• Recommendations
Remove scope-of-practice barriers
Expand opportunities for nurses to lead and
diffuse collaborative improvement efforts

CNO Context for Practice
• Challenges of healthcare reform:
Assure safe, high quality, effective patient-
centered care
Position nurses as integral to design and
delivery
Design new nursing roles and care models
across care continuum
Value-based purchasing
Align with the Triple Aim
Workforce shortages

Positioning for Accountable Care
• Group of physicians, hospitals and providers that come
together to deliver coordinated, high-quality care to Medicare
beneficiaries
• St. Luke’s ACO was created to participate in the Medicare
Shared Savings Program (MSSP)
• Goals
Improve quality
Improve patient experience
Coordinate care
Improve patient safety
Improve health/manage populations
• Full Risk Medicare Advantage Programs
• Preparing for state health insurance exchange and expansion
of Medicaid
6

Positioning for Accountable Care
• SelectHealth & Clinical Integration
Payer partnership
Employed and independent providers aligned across the
continuum
Best practices, clinical guidelines, standard order sets and
contracts with SNIFs, LTACHs, Rehab and Behavioral
Health
Care management & coordination
Managing care transitions
Medical homes & care of patients at risk (CoPar)
• Integrated electronic medical record (EMR)
• Healthy U
7
Primary Care Medical Home
Accountable Care Organization

Why ACA Provisions Will Move Forward
• Republicans and Democrats
Agree >80%
• Lower cost
• Improved quality
• Greater access
• Focus on prevention and
wellness
• Patient Centered Medical
Home / ACO
• Can’t afford not to

What to Expect
Nationally ~
• ACA is here to stay
• Integration and coordination of care
• Cost reduction
• Quality of care NOT quantity of care
• More focus on health and less on health care
• Greater focus on primary care
• Greater focus on collaborative care
McGowan Peak, Sawtooth National Recreation Area, Central Idaho
State-wide/regionally ~
• Health insurance
Exchanges
• State/Regional Co-Ops
• Medicaid expansion
• Local primary care
• Community health
• Improved models of
collaborative care
• SHIP grant – assists
Medicare beneficiaries
understand benefits/plans

Idaho Workforce Rankings
Physicians per
Capita 49th
Primary Care
Physicians per
Capita
47th
Nurses per Capita 50th
Nurse Practitioners
per Capita 45th
Physician
Assistants per
Capita
Tied
14th
Idaho Department of Labor, Idaho Primary Care Physicians Workforce Overview, Winter 2012-2013; Idaho Department of Labor, Idaho Nursing
Overview, January 2011; Idaho Department of Labor, Idaho Physician Assistants Workforce Overview, Fall 2012

Idaho Workforce Projections
Today 2018
Physicians 1,393 1,580
Primary Care
Physicians
777
862
Nurses 13,430 17,050
Nurse
Practitioners 441 560
Physician
Assistants 539 763
Idaho Department of Labor, Idaho Primary Care Physicians Workforce Overview, Winter 2012-2013; Idaho Department of Labor, Idaho Nursing
Overview, January 2011; Idaho Department of Labor, Idaho Physician Assistants Workforce Overview, Fall 2012
Idaho Department of Labor, Idaho Primary Care Physicians Workforce Overview, Winter 2012-2013; Idaho Department of Labor, Idaho
Nursing Overview, January 2011; Idaho Department of Labor, Idaho Physician Assistants Workforce Overview, Fall 2012

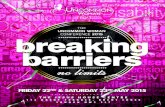
Primary Care HPSAs
Health Professional Shortage Areas
- (county or service area)
(demographic – low income population)

St. Luke’s Treasure Valley
• Founded as a 6-bed frontier hospital in 1902
• Two hospitals (548 beds)
• 100 provider-based clinics
• Five regional cancer centers
• Home care & hospice services
• Three ambulatory surgery centers
• 2200 RNs/100 Nurse Practitioners
• 39th organization to receive Magnet®, 3rd 2011 designation

Professional Practice Model
14

Eight Steps to Creating Change*
• Establish a Sense of Urgency
• Create the Guiding Coalition
• Develop a Vision and Strategy
• Communicate the Change vision
• Empower Broad-based Action
• Generate Short-Term Wins
• Consolidate the Gains/Produce More Change
• Anchor New Approaches in Culture
*Adapted from: Kotter, J. Leading Change. Boston, MA: Harvard Business School Press; 1996

Establishing a Sense of Urgency
• Traditional medical staff philosophy of supervision
and restriction
Prohibited from admitting and discharging,
writing orders, H & Ps, rounding, diagnosing
• Clinic expansion, managing populations,
primary care provider shortages
• Expanding APRN privileges priority for both
physician and nursing leadership

August 20, 2013

Outdated Terms: Talking Points*
• Limited licensure providers
Unique, no “limit” outside of scope of practice as regulated by
Idaho Board of Nursing
• Dependent care providers
In Idaho, APRNs are independent; physician involvement not
required for practice. We support collaborative practice.
• Mid-level practitioner
Unique body of knowledge/scope, all practicing at highest level
under privileges granted from organization
• Physician extender
Professional nurses practice rooted in nursing body of
knowledge, physician provides medical care
One profession cannot “extend” another
Physician assistants are physician extenders as they practice
under the physician’s license and are regulated by the BOM
Adapted from J. Clavelle. SBAR on Nursing Practitioner Privileges. Boise, ID. 2010

Creating the Guiding Coalition
• CNO catalyst for change
• Validate vision: CEO, CMO and MEC Chair
agreeing to lead task force
• SBAR document for situational briefing
• Individual meetings with more than 20 physicians
• Selection of a professional facilitator
• CNO as nursing practice expert; no NPs

Developing the Vision and Strategy
• Nurse Practitioner privileges need to be revised in
order to:
Align with physician expectations regarding how
they collaborate to care for patients across the
care continuum
Reflect current IBN scope of practice
Place St. Luke’s in a better position for
accountable care and achieving vision of
partnering with providers to achieve patient-
centered, quality, integrated care
• Nursing strategic plan - Goal

Communicating the Change Vision
• SBAR to convey vision and educate on outdated
terms
• Supervision of practice not aligned with scope
• MDs and NPs have separate, but related body of
knowledge
• CNO as highest level authority and practice expert
– DNP
• APRNs and physicians work in partnership to care
for their patients

Empowering Broad-Based Action
• Core privileges
• Admission, discharge, H & P, consults, writing
orders, prescriptive authority
• Specialty privileges at department level
• Expedited process and approvals
• Significant dialogue on differentiating NPs and PAs
• Assessment of privileges in other organizations, review
of literature
• BON role and rules, nursing practice guidelines, peer
review
• Sponsoring vs. supervising for shared patients

Generating Short-term Wins
• One year process to achieve core privileges
• Immediate impact
- Nursing strategic goal achieved and celebrated
- Addressed IOM report recommendation
- Aligned with Magnet® model component of
exemplary professional practice
- Created new NP Forum
- Align with Schools of Nursing plans to expand APRN
and DNP programs
- Improve physician satisfaction and integration, e.g.
hospitalists, across clinics/hospitals

Consolidating the Gains
• CNO leadership ~ next steps
Continue to engage key stakeholders
Create operational framework to support practice,
e.g. NP peer review
Modify and approve of medical staff bylaws, medical
records policies, job descriptions, FPPE and OPPEs
Educate staff, leaders, physicians, community
Align with Regional Action Coalition
Develop service/academic partnerships
Emphasize role clarity and consistency of care and
practice across settings
Goal is long-term change in health and health care.

Recommendations
• CNOs must rise to challenge to lead and transform their organizations, influencing organizational policy to create change
• Partnering with physician colleagues integral to achieving outcomes
• Task force model effective at removing barriers to nurses practicing at their full scope of practice, improving clarity and meeting physician and nursing expectations
• Continue to develop new roles, structures and processes to achieve best outcomes for our patients and community
• Access organizational support: AARP, Idaho Regional Action Coalition, Robert Wood Johnson’s Campaign for Action, National Council of State Legislators Scope of Practice Tracking web site

References
1. The future of nursing: the institute of medicine (IOM) issues report. The future of nursing: leading change,
advancing health. Nursing News. 2011;35(1):1p.
2. IOM. The Future of Nursing: Leading Change, Advancing Health. 2010; www.iom.edu/Reports/2010/The-
Future-of-Nursing-Leading-Change-Advancing-Health. Accessed July 16, 2011.
3. Bleich MR. IOM report. The future of nursing: leading change, advancing health: milestones and challenges
in expanding nursing science. Research in Nursing & Health. 2011;34(3):169-170.
4. IOM future of nursing report recommendations are in: now what? Implications for nursing. New Jersey
Nurse. 2011;41(3):10-10.
5. Berwick DM, Nolan TW, Whittington J. The triple aim: care, health, and cost. Health Affairs. 2008;27(3):759-
769.
6. Tolman DR. Breaking away: the ethical case for nurse practitioner independence. American Journal for
Nurse Practitioners. 2011;15(7-8):38.
7. ACNP testifies before IOM hearings on the future of nursing. Journal for Nurse Practitioners. 2010;6(3):229-
229.
8. Bleich MR. "The Research Imperative and the IOM Future of Nursing: Strengthening Nursing's
Contributions to Leading Change and Advancing Health". Communicating Nursing Research. 2011;44:1 -
11.
9. Kuntz K. "Deadly Spin on Nurse Practitioner Practice". Journal of the American Academy of Nurse
Practitioners. 2011;23:573 - 576.
10. Kotter J. Leading Change. Boston: Harvard Business School Press; 1996.
11. Idaho Rules of the Board of Nursing 2012, http://adminrules.idaho.gov/rules/current/23/0101.pdf
12. Leonard M, Graham S, Bonacum D. The human factor: the critical importance of effective teamwork and
communication in providing safe care. Quality & Safety in Health Care. 2004;13:i85-90.
13. ANA. Nursing Administration: Scope and Standards of Practice. Silver Spring: Nursesbooks.org; 2009.
14. ANCC, ed Application Manual: Magnet Recognition Program. Silver Spring: American Nurse's
Credentialing Center; 2008.

Questions?