
Nurse-patient consultations in leg ulcer care do patients ... · PDF fileNurse-patient...
22
Health Services Research Unit HS RU Nurse-patient consultations in leg ulcer care – do patients disclose their concerns? Dr. Julie Green. PhD, M.Sc., B.Sc. (Hons), PGCert, RGN., B.Ed. Lecturer & Award lead for Community Nursing Practice (District Nursing). Keele University. [email protected]
Transcript of Nurse-patient consultations in leg ulcer care do patients ... · PDF fileNurse-patient...

Health Services Research Unit
HS RU
Nurse-patient consultations
in leg ulcer care – do patients
disclose their concerns?
Dr. Julie Green. PhD, M.Sc., B.Sc. (Hons), PGCert, RGN., B.Ed.
Lecturer & Award lead for Community
Nursing Practice (District Nursing).
Keele University.
Health Services Research Unit
HS RU
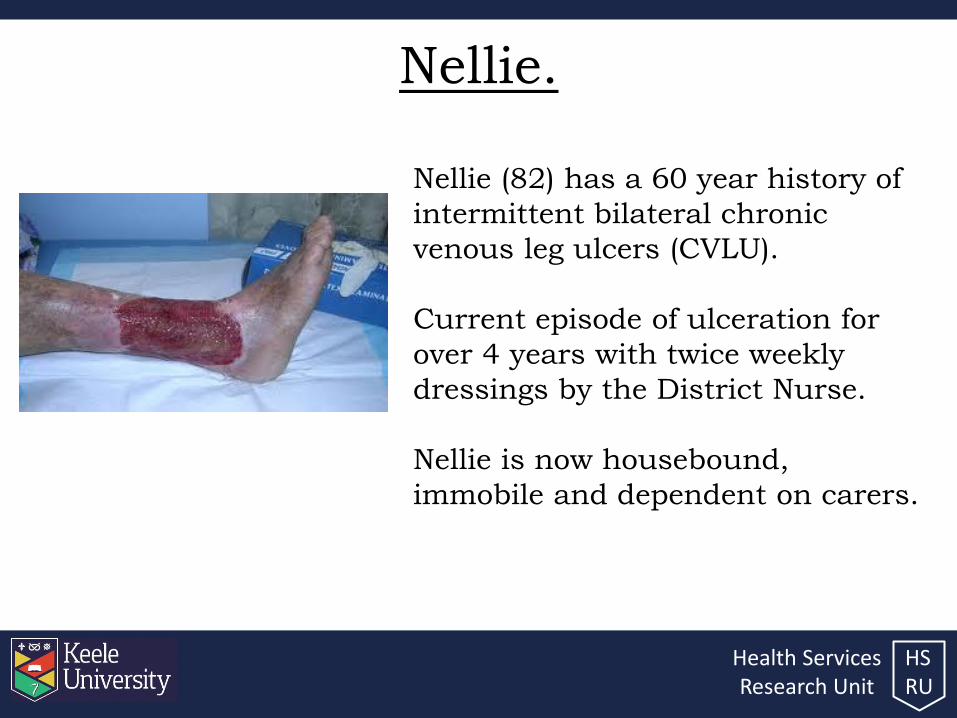
Nellie.
Nellie (82) has a 60 year history of
intermittent bilateral chronic
venous leg ulcers (CVLU).
Current episode of ulceration for
over 4 years with twice weekly
dressings by the District Nurse.
Nellie is now housebound,
immobile and dependent on carers.

Health Services Research Unit
HS RU
Aims & objectives.
• To outline patient centredness.
• To put the research question into context.
• To provide a synopsis of the research project as a whole.
• To provide a summary of phases 1 and 2 and an overview of the findings.

Health Services Research Unit
HS RU
Patient-centred care. • Patient centred care (PCC) is a relationship between the
patient and their health care practitioner which focusses on the well-being of the patient, where their experiences are central. Shared decision-making is key, with decisions made jointly between practitioner and patient (1-4).
• The key factors of patient-centredness identified by patients include (2,3,6-10): – The practitioner knowing about the patient’s progress.
– Responsiveness to patient needs.
– Encouraging patient participation in planning care.
– Providing information on condition and treatment plan.
– Treating the patient with respect.

Health Services Research Unit
HS RU
Patient-centred care (PCC).
• Despite these benefits, practitioners frequently fail to
elicit patient concerns or negotiate treatment options
during consultations. (6, 7)
– 54% of patient problems and 45% of patient concerns were
either not elicited by the doctor or disclosed by the patient. (8)
– The physician and patient failed to agree on the presenting
problem during 50% of consultations. (10)
– Nurses fail to communicate effectively and mainly approach
patients when undertaking administrative or functional
activities. (12)

Health Services Research Unit
HS RU
Chronic Venous Leg Ulcers. • Occur frequently.
– 1.5 - 3 per 1000 of the population suffer from venous ulceration. (18)
• Are expensive.
– Costs for care are estimated to be in excess of £200 million per year. (19)
• Recur.
– Annual recurrence rate of between 33-42% - a statistic that has remained unchanged for over 20 years. (20, 21)
• Impact on quality of life.
– Life is complicated by many issues and this negatively impacts on quality of life. (22, 23; 24)

Health Services Research Unit
HS RU
Phase 1 & 2 study aims.
1) To establish the factors that leg ulcer sufferers feel
have an impact on their day-to-day lives (Phase 1).
2) To determine the extent to which these factors are
addressed during patients’ current consultations with
their nursing team (Phase 2).

Health Services Research Unit
HS RU
Phase 1.
• Unstructured interviews
undertaken with patient
participants from two local
District Nursing Teams.
• CVLU for in excess of 6
weeks was required.
• Interviews patient-led,
audio recorded, transcribed
verbatim and continued
until saturation.
• Thematic analysis was
undertaken. (25)
• Four main themes – the
ulcer, symptoms, wound
management and effects
on daily life - each
containing a number of
subthemes.

Health Services Research Unit
HS RU
Phase 1 findings.
• Restrictions
• Mobility
• Hygiene
• Clothes and shoes
• Sleep
• Relationships
• The nurse.
• Location of treatment.
• The treatment applied and understanding.
• Concordance.
• Pain
• Exudate and odour
• Emotional effects of ulceration.
• Family history
• Comorbidities
• The cause, position and duration of ulceration.
The Ulcer Symptoms
Effects on daily life
Wound Management

Health Services Research Unit
HS RU
Phase 2.
• An observation checklist
was developed based on
phase 1 findings.
• Consultations for the
same participants were
observed.
• Each participant
underwent four
observations, providing
20 observation
opportunities in total.
• The checklist was completed
during each observation and
field notes promptly
recorded.
• Data analysis determined
the extent that phase 1
themes were raised and
addressed during patients’
consultations.

Health Services Research Unit
HS RU
Consultation
checklist.
• The checklist
contained 28
theme.
• Each theme
was rated
between 0 – 5.

Health Services Research Unit
HS RU
Phase 2 results. • The checklist was completed during each phase 2
consultation; providing 20 observations and a total of 560
item assessment opportunities.
• Analysis revealed the following ratings for checklist items
overall:
• Where study participants highlighted a theme as being of
significance during their phase 1 interview, these were
specifically monitored during their phase 2 consultations.
These statistics are presented in the following slides.
Score 0 Score 1 Score 2 Score 3 Score 4 Score 5
293 26 5 138 23 75
52% 5% 1% 25% 4% 13%

Health Services Research Unit
HS RU
The ulcer.
• Without exception, the participants were keen to describe
their ‘story’ which included their:
– family history;
– ‘all my mother’s sisters had it and me mother...runs in my family it does with us....’
(Mary, 72).
– co-morbidities and
– the cause, location and duration of ulceration.
– ‘God, they’ve been doing it....this Christmas it’ll be just over about 14 years...it’s just
been millimetres...millimetres all the time just going in…..very, very slow…..’(Steve, 39).
All patient talked of their experiences of ulceration which
provided an overview of their leg ulcer ‘journey’.

Health Services Research Unit
HS RU
Symptoms. • Pain was consistently reported and dominated the
interviews. – ‘.....it was getting more painful, it was like one time it was like burning pain, then it was
more like a stabbing pain, then.....now it’s like real sore....like someone is just rubbing,
rubbing, rubbing, all the time....Oh, the pain......it’s just unbearable.’ (Steve, 39).
• There was a reluctance to take analgesia and, when taken, it
was often deemed to be ineffective. – ‘I don’t take them unless I have to....I’d rather not take painkillers though....’ (Sam, 86).
• Where pain was raised as significant during the phase 1
interview, phase 2 observations revealed:
Score 0 Score 1 Score 2 Score 3 Score 4 Score 5
55 9 1 36 9 21
42% 7% 1% 27% 7% 16%

Health Services Research Unit
HS RU
Symptoms. • Exudate was described as a challenge to daily life.
• For many odour caused embarrassment and stress, this
often led to a restricting of contact with others. – ‘oh, and when you first have them......I wondered what the smell was....ohhhh, it’s
terrible the smell....it all comes out, a lot of rubbish........when you went anywhere.....you
didn’t get too close to people.....because I can smell it terrible.....and you can smell it in
your bed....you know...’ (Ellen, 80).
• Where exudate and odour were raised as significant
during the phase 1 interview, phase 2 observations
revealed:
Score 0 Score 1 Score 2 Score 3 Score 4 Score 5
9 1 1 5 1 11
32% 4% 4% 18% 4% 39%

Health Services Research Unit
HS RU
Symptoms. • Emotional effects due to ulceration included feeling
depressed, having a poor self-image and a range of fears. – ‘it’s just depressing really, if you think about it....I am on antidepressants ......I just have
to put up with it.....it’s either that or kill myself.....’ (Steve, 39).
– ‘I tell you......you have to shake yourself....you have to shake your feathers and when you
go out you have to put your outside face on......you know, you just have to.....’ (Margaret,
72).
• Where the emotional effects of ulceration were raised as
significant during the phase 1 interview, phase 2
observations revealed:
Score 0 Score 1 Score 2 Score 3 Score 4 Score 5
16 2 1 8 0 1
57% 7% 4% 29% 0% 4%

Health Services Research Unit
HS RU
Wound management. • Wound management included the role of the nurse, the
treatment regime, patient understanding and concordance
issues. – ‘..with the consistency of a team...much better. They did once send another from another
surgery out of........it wasn’t the same....when you’re seeing someone only once....it isn’t
the same....nothing wrong with her...did the job just the same....fine...but I wasn’t used to
her...’ (Tom, 76).
– ‘....but I’ve had loads of different dressings on before that....I’ve had a lot of different
things ....silver.......honey…..’ (Sam, 86).
• Where wound management themes were raised as
significant during the phase 1 interview, phase 2
observations revealed:
Score 0 Score 1 Score 2 Score 3 Score 4 Score 5
3 0 1 9 4 18
9% 0% 3% 28% 13% 47%

Health Services Research Unit
HS RU
Effects on daily life. • CVLUs impacted on every aspect of daily living: restricting
mobility; creating problems whilst working; difficulties
maintaining personal hygiene and restricted choices with
clothes and shoes; disturbed sleep and changing
relationships. – ‘Social life? ‘Errrr.....I haven’t got one........I just don’t bother cause I know I’ve got to get myself
better...but relationship wise.......no chance...I couldn’t...once these have healed then, obviously
yes...but it’s just, you know, with these on me legs all the time......there was one girl and I
tried...she said ‘what’s all that on your legs?’ and I tried make out that I’d been in a fire and I’d
burned myself but....with the smelling and that...it didn’t last...and I’ve just sort of put it off....’
(Steve, 39).
• Where the effects on daily life were raised as significant during
the phase 1 interview, phase 2 observations revealed:
Score 0 Score 1 Score 2 Score 3 Score 4 Score 5
32 8 1 33 3 7
38% 10% 1% 39% 4% 8%

Health Services Research Unit
HS RU
Conclusion. • Research exposes concerns for CVLU sufferers that go beyond
their actual wound care (26; 24) ; however, a review of consultations demonstrates that important themes are often not raised or are inadequately addressed during current consultations.
• Research demonstrates that communication in the consultation can be improved by either enhancing the ability of the practitioner to facilitate communication or by activating the patient to communicate their needs. (15)
• The development and pilot of a new patient-centred consultation template for people with leg ulcers, will encourage the exploration of important themes during consultations. The feasibility of this will be evaluated in phase 3.

Health Services Research Unit
HS RU
With thanks to my supervisory team for their support:
Professor Robert McKinley
Professor Rebecca Jester
Doctor Alison Pooler
I also gratefully acknowledge my funding from the
former West Midlands Strategic Health Authority.

Health Services Research Unit
HS RU
References. 1. Ballint, M. (1957). The doctor, his patient and the illness. London, Tavistock Publications.
2. Henbest, R. J. & Stewart, M. (1989). Patient-Centredness in the Consultation. 1: A Method for Measurement. Family Practice. 6, 4, 249 – 254.
3. Stewart, M. (2001). Towards a global definition of patient centred care. BMJ. 322, 444-445.
4. Stewart, M., Meredith, L., Brown, J.B. & Galajda, J. (2000). The influence of older patient-physician communication on health and health-related outcomes. Clinics in Geriatric Medicine. 16, 1, 25-36.
5. Poochikian-Sarkissian, S., Sidani, S., Ferguson-Pare, M. & Doran, D. (2010). Examining the relationship between patient-centred care and outcomes. Canadian Journal of Neuroscience Nursing. 32, 4, 14 – 21.
6. Irwin, P.S. & Richards, N.D. (2006). Patient-focused Care. Chest. 130, 73S-82S.
7. Michie, S., Miles, J. & Weinman, J. (2002). Patient-centredness in chronic illness: what is it and does it matter? Patient Education and Counselling. 51, 197-206.
8. Brown, D., McWilliam, C. & Ward-Griffin, C. (2006). Client-centred empowering partnering in nursing. Journal of Advanced Nursing. 53 (2), 160-168.
9. Mead, N. & Bower, P. (2000). Patient-centredness: a conceptual framework and review of empirical literature. Social Science and Medicine. 51, 1087-1110.
10. Lewin, S., Skea, Z., Entwistle, V.A., Zwarenstein, M. & Dick, J. (2009). Interventions for providers to promote a patient-centred approach to clinical consultations. The Cochrane Collaboration. Issue 1.
11. Ley, P., Whitworth, M.A., Skilbeck, C.E., Woodward, R., Pinsent, R.I,F,H., Pike, L.A., Clarkson, M.E. & Clark, P.B. (1976). Improving doctor-patient communication in general practice. Journal of the Royal College of General Practitioners. 26, 720-724.
12. Griffin, S. J., Kinmouth, A., Veltman, M., Gillard, S., Grant, S. & Stewart, M. (2004). Effect on Health-Related Outcomes of Interventions to Alter the Interaction between Patients & Practitioners: a systematic review of trials. Annals of Family Medicine. 2, 6, 595 – 608.
13. Stewart, M., McWhinney, I.R. & Buck, C. W. (1979) The doctor/patient relationship and its effect upon outcome. Journal of the Royal College of General Practitioners. 29, 77-82.
14. Tuckett, D., Boulton, M., Olson, C. & Williams, A. (1985). Meetings Between Experts: an approach to sharing ideas in medical consultations. London, Tavistock.

Health Services Research Unit
HS RU
References. 15. Stewart, M. (1995) Effective physician-patient communication and health outcomes: A Review. Canadian
Medical Association Journal. 152 (9) 1423-1433.
16. Campion, P., Foulkes, J., Neighbour, R. & Tate, P. (2002). Patient-centredness in the MRCGP video examination: analysis of large cohort. BMJ. 325, 691-692.
17. McCabe, C. (2004). Nurse-patient communication: an exploration of patients’ experiences. Journal of Clinical Nursing. 13, 41-49.
18. Graham, I., Harrison, M., Nelson, E., Lorimer, K. & Fisher, A. (2003). Prevalence of lower limb ulceration: a systematic review of prevalence studies. Advances in Skin and Wound Care. 16; 305-316.
19. Posnett, J. and Franks,P. (2007). The costs of skin breakdown and ulceration in the UK in Smith and Nephew Foundation (2007) Skin Breakdown – The silent epidemic. UK, snfoundation.
20. Heit, J., Rooke, T., Silverstein, M., Mohr, D., Lohse, C., Petterson, T., O’Fallon, M. and Melton, J. (2001) Trends in the incidence of venous stasis syndrome and venous ulcer: A 25-year population-based study. Journal of Vascular Surgery 33, 5, 1022-1027.
21. Ehrenberg, A. & Birgersson, C. (2003). Nursing documentation of leg ulcers: Adherence to clinical guidelines in a Swedish primary health care district. Scandinavian Journal of Caring Sciences. 17; 278-284.
22. Jones, J. and Nelson,E. (2005). Skin grafting for venous leg ulcers Cochrane Database Systematic Review. (1):CD001737.
23. Franks, P. and Moffatt, C. (2007) Leg Ulcers in Smith and Nephew Foundation (2007) Skin Breakdown – The silent epidemic. UK, snfoundation.
24. Palfreyman, S. (2008). Assessing the impact of venous ulceration on quality of life. Nursing Times. 104 (41), 34-37.
25. Braun, V. & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology. 3: 2, 77 — 101
26. Hopkins, A. (2004) Disrupted lives: investigating coping strategies for non-healing leg ulcers. British Journal of Nursing. 13, 9, 556–563.


















