Chest Tubes by Charlotte Cooper RN, MSN, CNS modified by Kelle Howard RN, MSN.
Upload
dustin-leonardCategory
view
215download
4
NURS 207: Promoting Pediatric Wellness in the Family & Community
Elizabeth Hartman, MSN, RNCAllan J. V. Cresencia, MSN, RN
Christine Limann, BSN, RN
West Coast University - Los Angeles

Health Promotion of the School-Age Child and Family
Chapter 17
Promoting Optimum Growth and Development
• “School age” generally defined as 6 to 12 years
• Physiologically begins with shedding of first deciduous teeth and ends at puberty with acquisition of final permanent teeth
• Gradual growth and development
• Progress with physical and emotional maturity

Shedding Deciduous Teeth
Maturation of Systems
• Bladder capacity increases
• Heart smaller in relation to the rest of body
• Immune system increasingly effective
• Bones increase in ossification
• Physical maturity not necessarily correlated with emotional and social maturity

Prepubescence
• Defined as 2 years preceding puberty
• Typically occurs during preadolescence
• Varying ages from 9 to 12 (girls about 2 years earlier than boys)
• Average age of puberty is 12 in girls and 14 in boys

Psychosocial Development
• Relationships center around same-sex peers
• Freud described it as “latency” period of psychosexual development

Erikson:Developing a Sense of Industry
• Eager to develop skills and participate in meaningful and socially useful work
• Acquire sense of personal and interpersonal competence
• Growing sense of independence
• Peer approval is strong motivator
School-Age Children Are Motivated to Complete Tasks

Erikson: Inferiority
• Feelings may derive from self or social environment
• May occur if incapable or unprepared to assume the responsibilities associated with developing a sense of accomplishment
• All children feel some degree of inferiority regarding skill(s) they cannot master

Piaget: Cognitive Development
• Concrete operations• Use thought processes to experience events and
actions• Develop understanding of relationships between
things and ideas• Able to make judgments based on reason
(“conceptual thinking”)• CONSERVATION

School-Age Children Are Often Avid Collectors

Kohlberg: Moral Development
• Development of conscience and moral standards
• Age 6 to 7: reward and punishment guide choices
• Older school age: able to judge an act by the intentions that prompted it
• Rules and judgments become more founded on needs and desires of others

Spiritual Development
• Children think in very concrete terms
• Children expect punishment for misbehavior
• May view illness or injury as punishment for a real or imagined misdeed

Children Are Comforted by Prayer

Language Development
• Efficient language skills
• Important linguistic accomplishments
• Correct syntax, improved grammar, word usage
• “Metalinguistic awareness”

Social Development
• Importance of the peer group
• Identification with peers is a strong influence in child gaining independence from parents
• Sex roles strongly influenced by peer relationships
Engaging in Activities with a “Best Friend”
9-Year-Olds’ Club Rules
Relationships with Families
• Parents are primary influence in shaping child’s personality, behavior, and value system
• Increasing independence from parents is primary goal of middle childhood
• Children not ready to abandon parental control

Developing a Self-Concept
• Definition: a conscious awareness of a variety of self-perceptions (abilities, values, appearance, etc.)
• Importance of significant adults in shaping child’s self-concept
• Positive self-concept leads to feelings of self-respect, self-confidence, and happiness

Developing a Body Image
• Generally children like their physical selves less as they grow older
• Body image is influenced by significant others
• Increased awareness of “differences” may influence feelings of inferiority

Development of Sexuality
• Normal curiosity of childhood
• Attitudes toward sex
• Use of terminology
Sex Education
• Sex play as part of normal curiosity during preadolescence
• Middle childhood is ideal time for formal sex education• Life span approach• Information on sexual maturity and process of
reproduction• Effective communication with parents
Nurse’s Role in Sex Education
• Treat sex as normal part of growth and development
• Questions and answers
• Differentiate between “sex” and “sexuality”
• Values, problem-solving skills
• Open for communication with parents
Play
• Involves physical skill, intellectual ability, and fantasy
• Children form groups, cliques, clubs, secret societies
• Rules and rituals
• See need for rules in games they play

Activities Vary by Interest and Opportunity

Play (cont.)
• Team play
• Quiet games and activities
• Ego mastery

Selecting a Book with an Adult
Pride in Learning New Skills

Coping with Concerns Related to Normal Growth and
Development• School experience
• Second only to the family as socializing agent• Transmission of values of the society• Peer relationships become increasingly
important
Coping with Concerns Related to Normal Growth and Development (cont.)
• Teachers
• Parents
• Limit setting and discipline
• Dishonest behavior
• Stress and fear

Teachers’ Influence on Children

Latch-key Children
Promoting Optimum Health During the School Years
• Nutrition• Importance of balanced diet to promote growth• Quality of diet related to family’s pattern of
eating• Fast-food concerns

Sleep and Rest
• Average 9½ hours/night during school age but highly individualized
• Ages 8 to 11 may resist going to bed
• 12 years and up generally less resistant to bedtimes
Physical Activity
• Exercise essential for development and function
• Importance of physical fitness for children

Exercise and Activity
• Sports• Controversy regarding early participation in
competitive sports• Concerns with physical and emotional maturity in
competitive environment
• Acquisition of skills
• Generally like competition
Music Is a Favorite Form of Expression

Performing Household Tasks

Dental Health
• Permanent teeth eruption
• Good dental hygiene
• Prevention of dental caries
• Malocclusion
• Dental injury
• Dental evulsion—replacement or reattachment

School Health
• Responsibilities of parents, schools, and health departments
• Ongoing assessment, screening, and referrals
• Routine services, emergency care, and safety and infection control instruction
• Increase knowledge of health and health habits

Injury Prevention
• Most common cause of severe injury and death in school-age children is motor vehicle crashes—pedestrian and passenger
• Bicycle injuries—benefits of bike helmets
• Appropriate safety equipment for all sports

Bicycle Safety

Anticipatory Guidance—Care of Families
• Parents adjust to child’s increasing independence
• Parents provide support as unobtrusively as possible
• Child moves from narrow family relationships to broader world of relationships
Health Problems of Middle Childhood
Chapter 18

DISORDERS AFFECTING THE SKIN

Purposes of the Skin
• Protection
• Impermeability
• Heat regulation
• Sensation
Origin of Skin Lesions
• Contact with injurious agents
• Hereditary factors
• External factor that produces a reaction in the skin
• Systemic disease in which lesions are a manifestation
Examples of Age-Related Skin Manifestations
• Infants: birthmarks
• Early childhood: atopic dermatitis
• School-age children: ringworm
• Adolescents: acne

Dermatitis
• Pathophysiology
• Diagnostic evaluation
• History and symptoms: pruritus, sensation
• Objective findings: lesion

Types of Lesions• Papule• Macule• Vesicle/bulla• Pustule• Cyst• Patch• Plaque• Wheal• Striae
• Scale
• Crust
• Keloid
• Fissure
• Ulcer
• Petechiae
• Purpura
• Ecchymosis
Nursing Considerations
• Prevent spread of bacterial infection
• Prevent complications
Viral Skin Infections
• Most communicable diseases of childhood have characteristic rash
• Examples: verruca, herpes simplex types 1 and 2, varicella zoster, molluscum contagiosum
Fungal Skin Infections
• Superficial infections that live on the skin
• Also called dermatophytoses, tinea
• Transmission: person to person or infected animal to human
• Examples: tinea capitis, tinea corporis, tinea pedis, candidiasis

Scabies
• Inflammation occurs 30 to 60 days after exposure
• Topical treatment: scabicides such as permethrin 5% or lindane
• Oral treatment: ivermectin if body weight is greater than 15 kg
Scabies (cont.)
• Caused by scabies mite as female burrows into the epidermis to deposit eggs and feces
• Inflamed, intense pruritus, excoriation
• Therapeutic management with scabicide (permethrin 5% preferred) for 30 to 60 days
• Treat all contacts
• Nursing considerations

Pediculosis Capitis (Head Lice)
• Very common, especially in school age
• Adult louse lives only 48 hours without human host; female louse has life span of 30 days
• Females lay eggs (nits) at base of hair shaft
• Nits hatch in 7 to 10 days
• Treatment: pediculicides and nit removal
• Preventing spread and recurrence
Systemic Mycotic (Fungal) Infections
• Invade viscera as well as the skin
• Wide spectrum of disease
• May appear as granulomatous ulcers, plaques, nodules, and abscesses

Rickettsial Infections
• Intracellular parasites generally transmitted by infected fleas, ticks, and mites
• Infections widely varied from benign and self-limiting to fatal
Lyme Disease
• Most common tick-borne disorder in United States
• Clinical stages
• Diagnosis and therapeutic management
• Vaccine against Lyme disease
• Focus on prevention
Cat Scratch Disease (CSD)
• Most common cause of regional lymphadenitis in pediatric population
• Usually follows the scratch or bite of an animal (90% cats)
• Usually benign, self-limiting course lasting 2 to 4 months
• Treatment: supportive

Contact Dermatitis
• Inflammatory reaction of skin to chemical
• Initial reaction in the exposed region
• Characteristic sharp delineation between inflamed and normal skin
• Primary irritant
• Sensitizing agent
• Examples: diaper dermatitis, reaction to wool, reaction to specific chemical

Poison Ivy, Oak, and Sumac
• Produce localized lesions
• Caused by urushiol from the plant’s leaves and stems
• Sensitivity may develop after one or two exposures and may change over time
• Therapeutic management
Poison Ivy

Foreign Bodies
• Wood splinters
• Cactus spines
• May require medical treatment if difficult to see or remove

Sunburn
• Ultraviolet A waves
• Ultraviolet B waves
• Importance of protection: sunscreen

Cold Injury: Chilblain
• Redness/swelling especially of hands
• Vasodilation, edema, bluish patches, itching
and burning; symptoms continue after
rewarming
• Usually resolve in a few days
• Tissue damage due to ice crystals in tissues
• Blisters appear 24 to 48 hours after rewarming
• Treatment of blisters similar to burn treatment
Cold Injury: Frostbite

Hypothermia
• Definition: less than 35° C
• Effect of decrease in core temperature
• Therapeutic management
• Nursing considerations
• Prevention
Drug Reactions
• Adverse drug reactions are most often seen in skin (rashes most common reaction)
• May be immediate or delayed following administration of the drug
• Treatment: discontinue the drug; give antihistamines, corticosteroid therapy if severe
Erythema Multiforme Exudativum
(Stevens-Johnson Syndrome)• Onset with flulike symptoms
• Balanitis, conjunctivitis, stomatitis
• Erythematous, papular rash
• Lesions on all surfaces (even palms and soles of feet) except scalp
• Prognosis
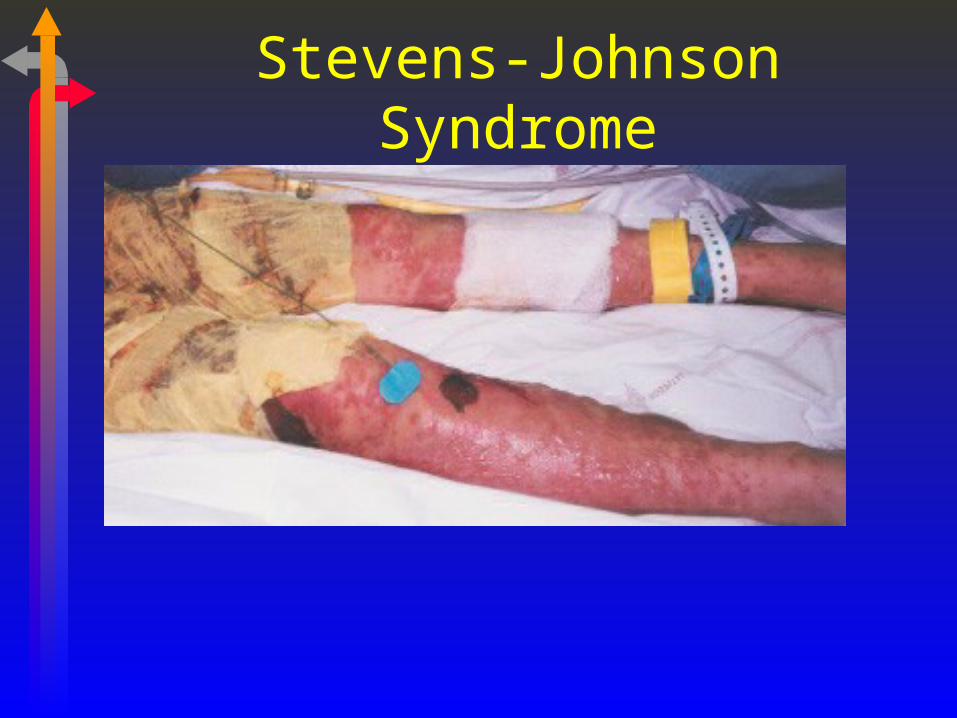
Stevens-Johnson Syndrome
Toxic Epidermal Necrolysis (TEN)
• Also called Lyell disease
• Clinical appearance is same as for staphylococcal scalded skin syndrome (SSSS)
• Protracted illness
• 25% to 50% mortality
• Precipitating factors: antiseizure medications, sulfa, penicillin
Neurofibromatosis-1
• Also called von Recklinghausen disease
• Autosomal dominant
• Initial presentation: café-au-lait spots, pigmented nevi, axillary/inguinal freckling
• Elephantiasis may occur
• Nursing considerations

BITES AND STINGS

Arthropod Bites and Stings
• May cause mild to moderate discomfort
• Manage with symptomatic measures and prevention of secondary infection
• Bees: stinger penetrates the skin• Remove stinger ASAP• Sensitization to bee stings may result in
anaphylaxis

Arachnid Bites
• Most in United States are relatively harmless
• Scorpions, brown recluse spider, and black widow spider inject venom: potentially deadly

Ticks
• Partially embed in skin as they feed
• Remove by grasping tick close to point of attachment (with forceps)
• Preventive measures
Mammal Bites
• Common pediatric problem especially in children younger than 5 years old
• Wound care
• Prophylactic antibiotics for some types of bites
• Rabies concern
Snakebites
• Manifestations and morbidity are highly variable, based on species, size of snake, size of child, location of bite
• Maintain a calm response to the victim
• Apply loose tourniquet proximal to the bite: DO NOT OCCLUDE SYSTEMIC CIRCULATION
• Suction in appropriate cases

Human Bites
• Lacerations from teeth of other humans
• Risk of infection
• Wound care

DENTAL DISORDERS

Dental Caries
• Overall incidence decreased since introduction of fluoridation
• Continues to be principal oral problem in pediatric population
• Greatest vulnerability • Ages 4 to 8• Ages 12 to 18

Pathophysiology of Dental Caries
• Multifactorial• Host• Microorganisms• Substrate• Time
Pathophysiology of Dental Caries (cont.)
• Diagnostic evaluation
• Therapeutic management• Plasticized sealant• Removal of carious portions• Restoration of involved teeth
• Nursing considerations• Oral hygiene• Dietary influences

Periodontal Disease
• Inflammatory and degenerative condition involving the gums and supporting tissues
• Gingivitis
• Periodontitis
• Acute necrotizing ulcerative gingivitis (“trench mouth”)
• Nursing considerations
Malocclusion
• Heredity
• Habits• Thumb sucking• Tongue thrusting
• Orthodontic treatment
• Nursing considerations
Dental Trauma
• Tooth evulsion• Cold milk = osmolality to maintain evulsed tooth
• Reimplantation of teeth
• Emotional response

DISORDERS OF CONTINENCE

Enuresis
• “Bed wetting”
• More common in boys
• Usually ceases between 6 and 8 years of age
• Diagnosis • Developmental age of more than 5 years• Two times per week or more for 3 months• May have urgency, frequency

Enuresis (cont.)
• Organic causes• Structural defects• UTI, impaired kidney function, chronic renal
failure• Neurologic deficits, endocrine disorders
(diabetes)• Sickle cell disease
• Bladder volume of 300 to 350 ml is sufficient to hold a night’s urine
Psychologic Factors
• “Sleep more soundly than other children”
• Emotional factors
• Familial tendency
Treatment for Enuresis
• Drugs• Tofranil• Oxybutynin• DDAVP
• Bladder training
• Fluid restriction in evenings
• Interruption of sleep to void
• Conditioned reflex response device

Encopresis• Repeated voluntary or involuntary passage of feces
of normal or near normal consistency into places not appropriate for that purpose
• Not caused by any physiologic effect (e.g., laxative) or medical problem
• Primary encopresis = fecal incontinence after age 4 years
• Secondary encopresis = fecal incontinence in a child older than 4 years after period of prior established fecal continence
Encopresis (cont.)
• More common in males
• May follow psychological stress
• May be secondary to constipation or impaction
• Therapeutic management• Determine cause• Dietary intervention, management of constipation• Psychotherapeutic interventions

DISORDERS WITH BEHAVIORAL COMPONENTS
Attention Deficit Hyperactivity Disorder (ADHD)
• Etiology unknown; probably multifactorial
• Inattention, impulsiveness, and hyperactivity
• Typical onset before age 7
• Diagnostic criteria for ADHD
Therapeutic Management of ADHD
• Classroom
• Family education and counseling
• Behavioral therapy and/or psychotherapy for child
• Environmental manipulation
• Medication

Medications for ADHD
• Not all children benefit from pharmacologic therapy
• Stimulants• Dexedrine, Adderall• Ritalin
• Side effects: insomnia, anorexia and weight loss, hypertension; long-term use may suppress growth
Learning Disability (LD)
• Learning disability: a heterogeneous group of disorders with difficulties in acquisition and use of listening, speaking, reading, writing, reasoning, math and/or social skills
• Includes dyslexia, dysgraphia, dyscalculia, right/left confusion, and short attention span

Battery of Tests for LD and ADHD
• IQ
• Hand-eye coordination
• Visual and auditory perception
• Comprehension
• Memory

Therapeutic Management of LD• Primarily educational interventions
• Wide variation of diagnostic severity

Tic Disorders
• Definition: tic is an involuntary, recurrent, random, rapid, highly stereotyped movement or vocalization
• Increases with stress, decreases markedly with sleep
• Most are self-limiting, less than 1 year, usually resolve by late childhood or adolescence
Tourette Syndrome (TS)
• Severe, complex form of tic disorder
• Onset ages 2 to 16; persists throughout life
• Etiology uncertain
• Diagnostic criteria
• Associated problems include ADHD, disruptive behavior, learning disabilities
Therapeutic Management of TS
• Symptomatic treatment
• Family support
• Pharmacologic interventions
• Nursing considerations
Posttraumatic Stress Disorder (PTSD)
• Development of characteristic symptoms following exposure to extremely traumatic experience or catastrophic event
• May function adequately but have foreboding regarding the future
PTSD: Response to the Event
• Initial response• Intense arousal; lasts 1 to 2 hours• “Fight or flight” response
• Second phase• Lasts approximately 2 weeks• Denial, period of quiescence
• Third phase• Appears to get worse; lasts 2 to 3 months
PTSD Symptoms
• Depression, anxiety, conversion reactions
• Phobic symptoms, repetitive actions
• Flashbacks are common
• Inquiry about what has happened
• Nursing considerations
School Phobia
• Defined as extreme reluctance to attend school for a sustained period as a result of severe anxiety or fear of school-related experiences
• Also called “school refusal” and “school avoidance”
• Most common in children older than 10 years
School Phobia (cont.)
• Physical symptoms
• Symptoms subside after staying at home
• No symptoms on weekends, holidays, etc.
• Nursing considerations
Recurrent Abdominal Pain (RAP)
• May have psychogenic origin
• May have real pain
• Psychological aspects
• Nursing considerations
Conversion Reactions
• Also called hysteria, hysterical conversion reaction, and childhood hysteria
• Sudden onset, traced to a precipitating event
• Symptoms: abdominal pain, fainting, pseudoseizures, paralysis, headaches, visual field restriction
• Rule out true seizures with EEG

Childhood Depression
• Temporary: acute depression precipitated by a traumatic event
• Chronic depression• May accompany chronic illness or disability• Familial circumstances
• Nursing considerations
Childhood Schizophrenia
• Severe deviation in ego functioning
• Psychotic disorder that appears after ages 4 to 5
• Characterized by gradual onset of neurotic symptoms
• Lack of contact with reality; “A world of his own”
• Nursing considerations
Health Promotion of the Adolescent and Family
Chapter 19
Promoting Optimum Growth and Development
• Complex interplay of biologic, cognitive, psychologic, and social change, perhaps more so than at any other time of life
• Change on multiple levels• Biologic maturation• Cognitive development• Psychologic development

Adolescence
• Early: ages 11 to 14
• Middle: ages 15 to 17
• Late: ages 18 to 20
Biologic Development
• Neuroendocrine events of puberty

Hormonal Interaction Between Hypothalamus, Pituitary, and
Gonads
Changes in Reproductive Hormones
• Females• Menarche• Ovulation
• Males

Pubertal Sexual Maturation
• Tanner stages 1 through 5
COGNITIVE DEVELOPMENT
Piaget: Emergence of Formal Operational Thought
• Formal operational thinking: ages 11 to 14
• Abstract terms, possibilities, and hypotheses
• Decision-making abilities increase
• May not use formal operational thought and reasoned decision making all the time— “choices”
• ADAPTATION
Adolescent Conceptions of Self
• Adolescent egocentrism
• Self-absorption
• Health-related beliefs:• Imaginary audience (everyone is watching)• Personal fable (won’t happen to me)

Changes in Social Cognition
• Understanding of others’ thoughts and feelings
• Mutual role taking
• Effect on health-related choices

Development of Value Autonomy
• Struggle to clarify values
• Development of a personal value system
• Gradual process in late adolescence

Moral Development
• Parallels advances in reasoning and social cognition
• Conventional level of moral reasoning
• Principled moral reasoning
Spiritual Development
• Religious beliefs may become more abstract during adolescence
• Late adolescents may reexamine and reevaluate beliefs and values of their childhood

PSYCHOSOCIAL DEVELOPMENT
Identity Development
• Social forces shape sense of self
• Identity achievement
• “Moratorium”
• “Foreclosure”
• “Identity diffusion”
Development of Autonomy
• Emotional autonomy
• Behavioral autonomy
• Value autonomy
Achievement
• Development of motives, capabilities, interests, and behaviors
• Progress toward occupational achievement
• Relationship between social class and educational and occupational achievement

Sexuality
• Hormonal, physical, cognitive, and social changes affect sexual development
• Body image
• Sexual identity
• Sexual orientation

Romantic Relationships Are Important During Adolescence
Intimacy
• Intimate relationship begins to emerge in adolescence
• Developmental course of intimacy• Self-focused• Role focused• Individual connected

Social Environments
• Ecological model
• Microsystems
• Mesosystems
• Exosystems
• Macrosystems

Families
• Changes in family structure and parent employment
• Parenting styles
• Socioeconomic influences

Peer Groups
• Significance in socialization
• Significance in development
• Value placed on peer relationships

The Peer Group Influences Adolescent Development

Schools
• Play increasingly important role in preparation for adulthood
• Parental involvement in schools
• Effect of academic success or failure on self-esteem

Work
• Workplace as fourth microsystem
• Positive or negative
• May encourage development of intellectual and social skills, autonomy
• May result in decreased interest in school, fewer extracurricular activities, and poorer grades
Community and Society
• Media influences
• Community’s economic resources play role in health and well-being of young people
• Resources for health promotion
Promoting Optimum Health During Adolescence
• Empowering individuals, families, and communities
• Power, authority, and opportunities to make healthy choices
• Risk reduction in areas of mental health, substance use, sexual behavior, violence, unintentional injury, nutrition, physical activity and fitness, and oral health
Adolescents’ Perspectives on Health
• Factors promoting adolescent health and well-being
• Contexts for adolescent health promotion
• School-based and school-linked health services
• Adolescent health screening• “Safe times”: method for screening interviews
with teens
Health Concerns of Adolescence
• Parenting and family adjustment
• Psychosocial adjustment
• Intentional and unintentional injury
• Dietary habits, eating disorders, and obesity
• Physical fitness

Snacking on Empty Calories Is Common Among Adolescents

Adolescent Physical Fitness

Health Concerns of Adolescence (cont.)
• Sexual behavior, STDs, and unintended pregnancy
• Use of tobacco, alcohol, and other substances
• Depression and suicide
• Physical, sexual, and emotional abuse

Coping with Stress

Health Concerns of Adolescence(cont.)
• School and learning problems
• Hypertension
• Hyperlipidemia
• Infectious diseases/immunizations

Health Promotion Among Special Groups of Adolescents
• Adolescents of color
• Gay, lesbian, and bisexual adolescents
• Rural adolescents

Physical Health Problems of Adolescence
Chapter 20

Acne
• More than 50% of adolescents affected
• Etiology• Familial aspect• Hormonal influence• Other influences
• Psychosocial ramifications• Self-esteem issues

Acne (cont.)
• Pathophysiology• Involves hair follicle and sebaceous glands• Comedogenesis
• Therapeutic management• General measures/overall health• Medications• Nursing considerations

Vision Changes
• Refractory errors peak in adolescence due to growth spurts
• Vision screening
• Myopia most common
Male Reproductive Health Problems
• Penile problems• Uncorrected congenital problems• HPV• Trauma

Testicular Tumors
• Usually malignant
• Testicular CA is most common solid tumor in males ages 15 to 34
• Testicular self-examination (TSE)

Varicocele
• Usually asymptomatic scrotal mass or aching sensation
• Occurs in about 15% of males
• Varicocelectomy controversial in adolescence

Epididymitis
• Causes• Infection (bacterial or viral)• Chemical irritant• Local trauma
• Presentation: pain, redness, swelling
• Treatment: analgesics, antibiotics, supportive care

Testicular Torsion
• Partial or complete venous occlusion with rotation of testicle
• Occurrence: 1 in 4000 males
• Peak onset: age 13
• Surgical emergency to prevent necrosis
• Nursing considerations

Gynecomastia
• Normal if transient (less than 1 year’s duration) and during puberty
• Prepubescent or Tanner stage 5: need evaluation for adrenal or gonadal tumors, liver disease, or Klinefelter syndrome
• Drug induced: Ca++ channel blockers, H2 blockers, ketoconazoles, possibly marijuana
Female Reproductive Health Problems
• Gynecologic examination indicated• Menstrual disorders• Undiagnosed abdominal pain or pelvic mass• Sexually active and/or request contraception• Rape• Virginal, 18 years old• Requested by patient

Menstrual Disorders
• Primary amenorrhea: no menses by age 17
• Secondary amenorrhea: no menses for
6 months in previously menstruating female
• Irregular menses common in adolescence

Causes of Primary Amenorrhea
• Structural abnormality: septum, hymen, female circumcision
• Unresponsive to hormonal stimulation• Hypothalamic, pituitary, ovarian, uterine origin
• Systemic disorders• Thyroid dysfunction, prolonged or severe
infections, adrenal hyperplasia, DM, obesity, malnutrition
Causes of Secondary Amenorrhea
• Most common cause: pregnancy
• Stress, chronic illness, polycystic ovarian disease, anorexia, ovarian disturbance, phenothiazines, heroin

Menstrual Irregularities in the Female Athlete
• Delayed menarche
• Anovulation with dysfunctional bleeding
• Oligomenorrhea or amenorrhea with hypoestrogenic states
• Treatment options: trial of decreased exercise, oral contraceptives

Dysmenorrhea
• Primary dysmenorrhea
• Secondary dysmenorrhea
• Therapeutic management• NSAIDs• Estrogen therapy• Oral contraceptives• Dietary changes• Exercises, comfort measures

Endometriosis
• Definition: presence of endometrial glands and stroma outside of the normal intrauterine endometrial cavity
• Etiology unclear
• Treatment: medical, surgical, pharmacologic suppression
• Nursing considerations

Premenstrual Syndrome (PMS)
• Symptoms
• Diagnosis
• Therapeutics • SSRIs• Nutrition/nutritional supplements• Supportive care

Dysfunctional Uterine Bleeding (DUB)
• Occurs in absence of pregnancy, infection, neoplasms, and known pathology
• Usually with anovulation
• Hormonal therapy treatments
• Surgical treatment (D&C)
• Nursing considerations

Vaginitis and Vulvitis
• Causes may be physical, chemical, or infectious
• Diagnosis confirmed by vaginal exam, microscopic evaluation of vaginal secretions
• Health teaching

Infections
• Candidiasis
• Trichomoniasis
• Bacterial vaginosis (BV)
Health Problems Related to Sexuality
• Sexual activity among adolescents
• Sexual risk-taking behaviors
• Family influences
• Peer influences
Adolescent Pregnancy
• Rates of teen pregnancy in United States
• Physiologic aspects
• Pregnancy risks associated with teen pregnancy
• Nutritional needs
Infants of Adolescent Mothers
• Higher risk of prematurity
• Higher incidence of low birth weight
• Potential for developmental delay
• Cumulative risk factors for infant

Social and Economic Effects of Teen Pregnancy
• School/education disruption
• Social relationship deprivation
• Statistical risk of poverty
• Emotional effect on infant and parents
Adolescent Fathers
• Changing social expectations
• Legal rights
• Emotional effect
• Parenting skill development
• Economic effect
Adolescent Abortion
• Roe v. Wade 1973
• Counseling
• Associated risks

Contraception
• Methods• Prescription and nonprescription
• Use of contraception
• Conflict about sexual activity
• Desire for pregnancy
• Nursing considerations

Rape
• SANE—sexual assault nurse examiners
• Diagnostic evaluation• Obtain account of incident• Sensitivity to victim’s emotional status• Physical evidence
• Vaginal secretions for evidence of sperm, blood, DNA
• GC culture to rule out preexisting condition
• HIV testing, other STD testing initially and at appropriate intervals
STDs
• Major cause of morbidity during adolescence and young adulthood
• Strong relationship between STDs and infertility
• Transmission and follow-up of contacts

Gonorrhea
• Cause: Neisseria gonorrhoeae
• Clinical manifestations
• Diagnosis
• Therapeutic management
• Prevention

Chlamydia
• Cause: bacterium Chlamydia trachomatis
• Clinical manifestations
• Diagnosis
• Therapeutic management
• Prevention
Human Papillomavirus
• Anogenital warts
• Strong link to cervical carcinoma
• Clinical manifestations
• Diagnosis
• Therapeutic management
• Prevention

Pelvic Inflammatory Disease (PID)
• Infection of upper genital tract• Tubo-ovarian abcess• Salpingitis• Long-term effects: infertility due to tubal
scarring• Symptoms• Therapeutics• Nursing considerations
HIV and AIDS
• Time lag between infection with HIV and development of clinical AIDS
• Transmission
• Follow-up of sexual contacts
• Adolescent perception of risk of AIDS

Hepatitis B Virus (HBV)
• Transmission via body fluids
• Effects on liver
• Maternal-infant transmission
• Immunization• Series begun at birth• Series of three IM injections• Goal to target children before onset of high-risk
behaviors

Behavioral Health Problems of Adolescence
Chapter 21
Obesity
• Defined as increase in body weight due to accumulation of excessive body fat relative to lean body mass
• Obese: generally considered when weight more than 95th percentile for age, gender, and height
• Overweight: generally considered when more than 90th percentile
• 25% to 30% of children are obese

Complex Relationships in
Adolescent Obesity

Effect of Childhood Obesity
• Increase in type 2 diabetes
• Risk of adult obesity
• Hypertension, hyperlipidemia, cardiovascular disease
• Social isolation, low self-esteem, depression
Causes of Childhood Obesity
• 5% due to underlying disease (hypothyroidism, other metabolic disease, CNS disorders)
• Role of heredity
• Inactivity
• Patterns of eating behaviors
Diagnostic Evaluation
• Skinfold measurements
• Body mass index (BMI) calculations
• Body fat measurements
• Diagnostics to rule out metabolic and endocrine disorders
Nursing Considerations
• Assessment, planning, implementation
• Diet, exercise, behavioral and group therapy
• Prevention, evaluation
• Medical therapies• Pharmacologic: generally not recommended in
children• Surgical: hazardous in children

Anorexia Nervosa (AN)
• Eating disorder: refusal to maintain normal body weight
• Primarily in adolescent and young adult females
• Mean age of onset 13.75 years, ranging from 10 to 25 years or more
• LIFE THREATENING!
Etiology/Pathophysiology of AN
• Etiology unclear• Distinct psychological component• Diagnosis based on psychological and
behavioral criteria• Relentless pursuit of thinness• Distorted body image• Media influence• Concept of “control”
Clinical Manifestations of AN
• Severe weight loss
• Altered metabolic activity• Amenorrhea• Bradycardia, decreased BP• Hypothermia, cold intolerance• Dry skin, brittle hair and nails• Appearance of lanugo

Therapeutic Management of AN
• Treat life-threatening malnutrition• IV, tube feedings• Monitor CV status
• Behavior modification
• Long-term (lifelong?) treatment and management
Bulimia
• Eating disorder characterized by binge eating
• May be followed by purging behaviors • Laxative abuse• Self-induced vomiting• Diuretic abuse• Rigorous exercise regimens
• Up to eight or more cycles per day
Bulimia (cont.)
• Weight may be normal or slightly above
• Weight may be low: bulimarexia
• Tooth erosion, esophageal damage, other GI concerns
• Psychologic issues• Self-deprecating thoughts, depressed mood• History of unsuccessful dieting, overweight in
childhood• Low impulse control
Therapeutic Management
• Similar to anorexia management
• Hospitalization to treat potassium depletion, esophageal damage
• Cardiac monitoring indicated
• Behavioral management

“Fear of Fat” Syndrome
• Differs from AN
• Worry that being overweight will make them physically unattractive, jeopardize their health, and shorten life span
• Diets lacking in iron, calcium, zinc
• May stop growing and have delayed puberty
Substance Abuse
• Drug abuse, misuse, and addiction• Voluntary behaviors• Culturally defined• Use of drugs for other than acceptable medical
purpose
• Drug tolerance and physical dependence• Involuntary physical responses
Types of Drugs Abused
• Tobacco
• Alcohol
• Cocaine
• Narcotics
• CNS depressants
• CNS stimulants
• Hallucinogens
• Inhalants

Nursing Considerations
• Acute care
• Long-term management
• Family needs/family support
• Prevention
Suicide
• Third leading cause of death in teens
• Suicide
• Suicidal ideation
• Suicide attempt/parasuicide

Suicide (cont.)
• Etiology
• Methods
• Motivation
• Diagnostic evaluation/therapeutic management
• Nursing considerations