
Nuovi dati Colon -...
34
Nuovi dati Colon Roma, 7 Ottobre 2017 Alain Gelibter Policlinico Umberto I UOC Oncologia «B»
-
Upload
nguyendiep -
Category
Documents
-
view
217 -
download
0
Transcript of Nuovi dati Colon -...

Nuovi dati Colon
Roma, 7 Ottobre 2017
Alain Gelibter
Policlinico Umberto I
UOC Oncologia «B»
1
NEOADJUVANT FOLFOX 4 VERSUS FOLFOX 4 PLUS CETUXIMAB VERSUS IMMEDIATE SURGERY FOR HIGH-
RISK STAGE II AND III COLON CANCERS: A PHASE II MULTICENTRE RANDOMISED CONTROLLED TRIAL
(PRODIGE 22) KAROUI Mehdi, RULLIER Anne, MARIETTE Christophe, MAILLARD Emilie, BARDIER Armelle, POIZAT Flora, LUCIANI
Alain, SARRAN Anthony, LEGOUX Jean-Louis, DE CHAISEMARTIN Cécile, LECAILLE Cédric, BOUCHE Olivier, MAUVAIS François, BRUNETTI Francesco, PRUDHOMME Michel, SEITZ Jean-François, LEPAGE Côme, TAIEB Julien
esmo.org
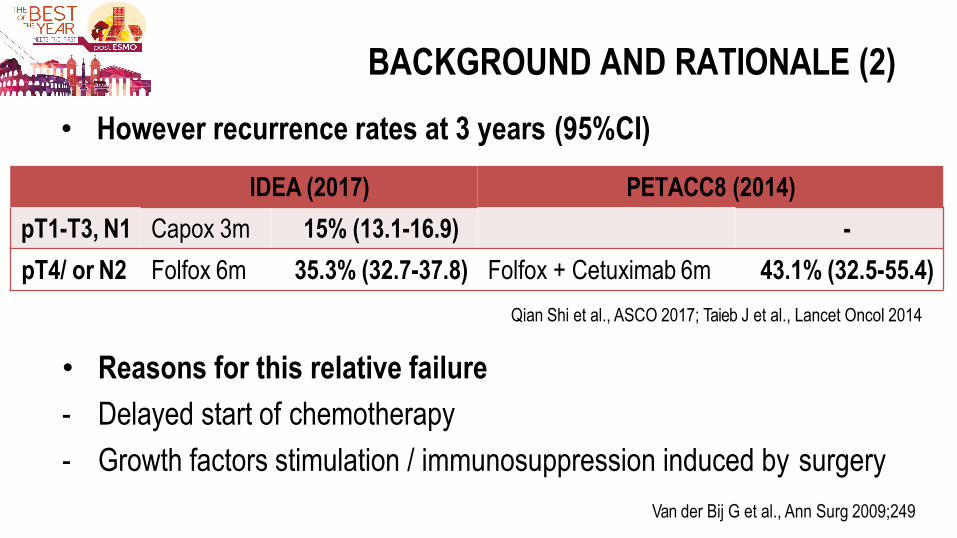
• However recurrence rates at 3 years (95%CI)
IDEA (2017) PETACC8 (2014)
pT1-T3, N1 Capox 3m 15% (13.1-16.9) -
pT4/ or N2 Folfox 6m 35.3% (32.7-37.8) Folfox + Cetuximab 6m 43.1% (32.5-55.4)
Qian Shi et al., ASCO 2017; Taieb J et al., Lancet Oncol 2014
BACKGROUND AND RATIONALE (2)
• Reasons for this relative failure
- Delayed start of chemotherapy
- Growth factors stimulation / immunosuppression induced by surgery
Van der Bij G et al., Ann Surg 2009;249
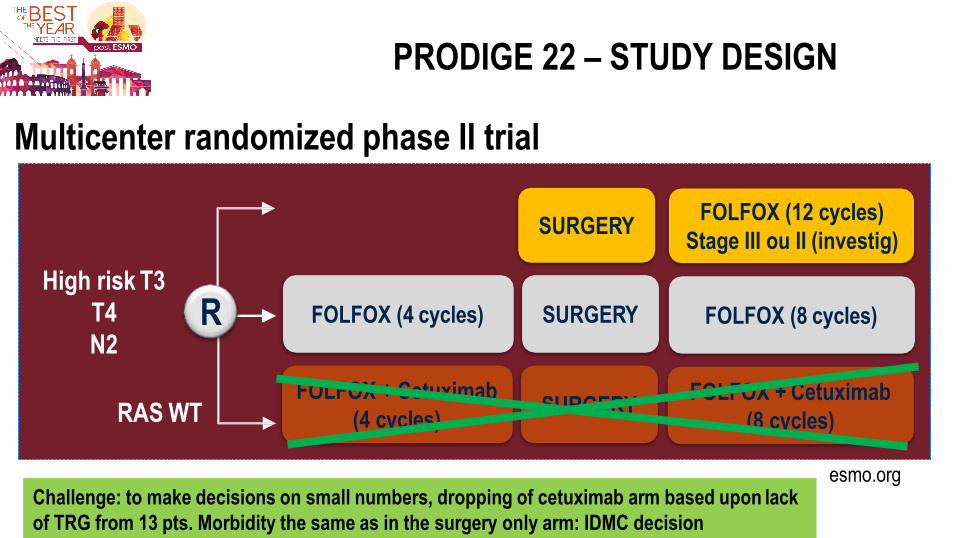
PRODIGE 22 – STUDY DESIGN
Multicenter randomized phase II trial
FOLFOX (4 cycles)
High risk T3
T4
N2
SURGERY
SURGERY
FOLFOX (12 cycles)
Stage III ou II (investig)
FOLFOX (8 cycles)
FOLFOX + Cetuximab
(4 cycles) SURGERY
FOLFOX + Cetuximab
(8 cycles)
R
RAS WT
esmo.org Challenge: to make decisions on small numbers, dropping of cetuximab arm based upon lack
of TRG from 13 pts. Morbidity the same as in the surgery only arm: IDMC decision
esmo.org
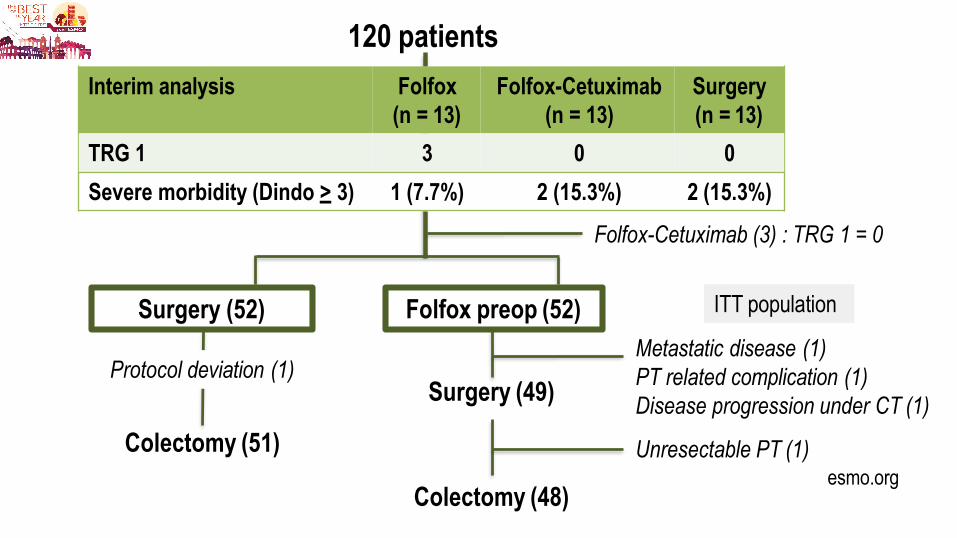
120 patients
Surgery (52) ITT population
Folfox-Cetuximab (3) : TRG 1 = 0
Folfox preop (52)
Interim analysis Folfox
(n = 13)
Folfox-Cetuximab
(n = 13)
Surgery
(n = 13)
TRG 1 3 0 0
Severe morbidity (Dindo > 3) 1 (7.7%) 2 (15.3%) 2 (15.3%)
Colectomy (51)
Protocol deviation (1) Metastatic disease (1)
PT related complication (1)
Disease progression under CT (1) Surgery (49)
Unresectable PT (1)
Colectomy (48)
esmo.org
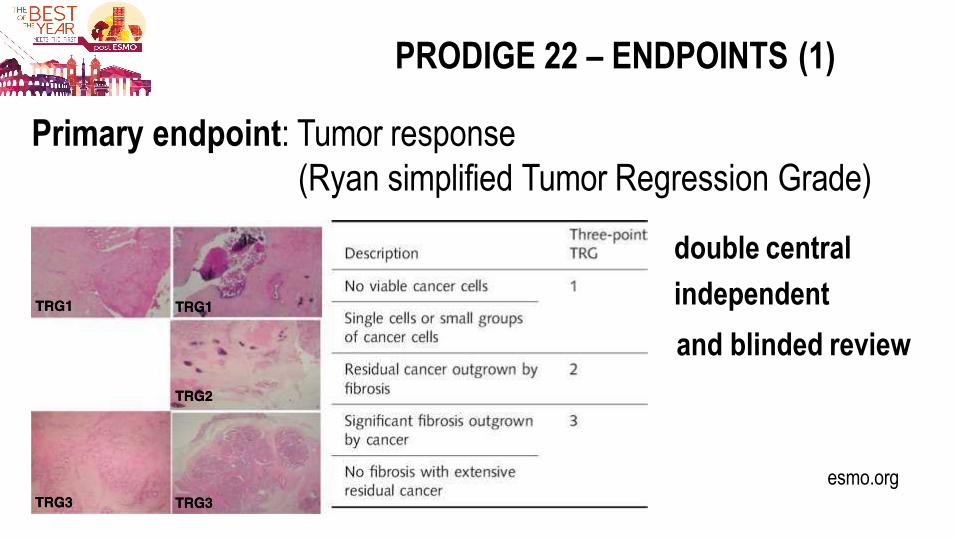
PRODIGE 22 – ENDPOINTS (1)
Primary endpoint: Tumor response
(Ryan simplified Tumor Regression Grade)
double central
independent
and blinded review
esmo.org
PRODIGE 22 – ENDPOINTS (2)
Secondary outcome measures
- Chemotherapy toxicity
- Primary tumor (PT) complications under chemotherapy
- Postoperative morbidity
- Quality of surgery
- Radiological staging
- 3 years DFS
- Quality of life
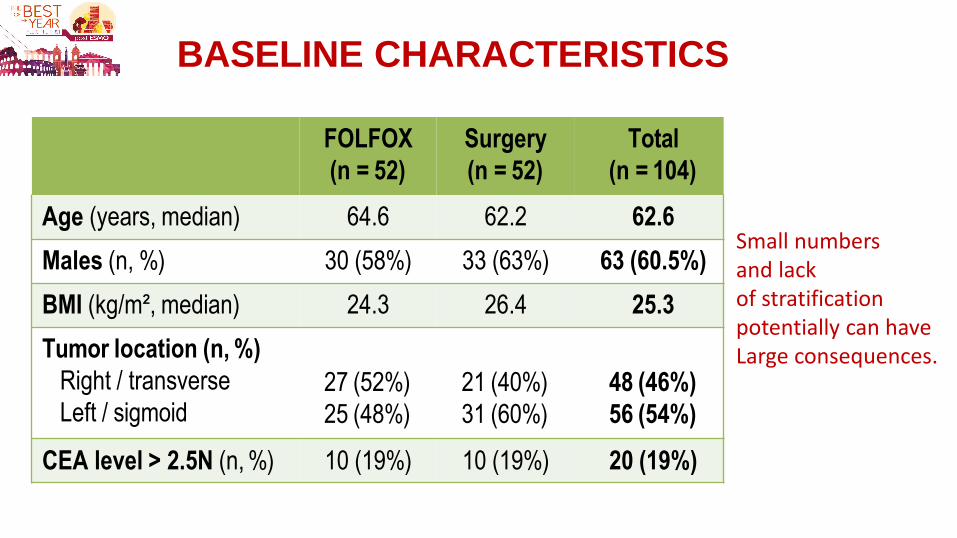
BASELINE CHARACTERISTICS
FOLFOX
(n = 52)
Surgery
(n = 52)
Total
(n = 104)
Age (years, median) 64.6 62.2 62.6
Males (n, %) 30 (58%) 33 (63%) 63 (60.5%)
BMI (kg/m², median) 24.3 26.4 25.3
Tumor location (n, %)
Right / transverse
Left / sigmoid
27 (52%)
25 (48%)
21 (40%)
31 (60%)
48 (46%)
56 (54%)
CEA level > 2.5N (n, %) 10 (19%) 10 (19%) 20 (19%)
Small numbers and lack of stratification potentially can have Large consequences.
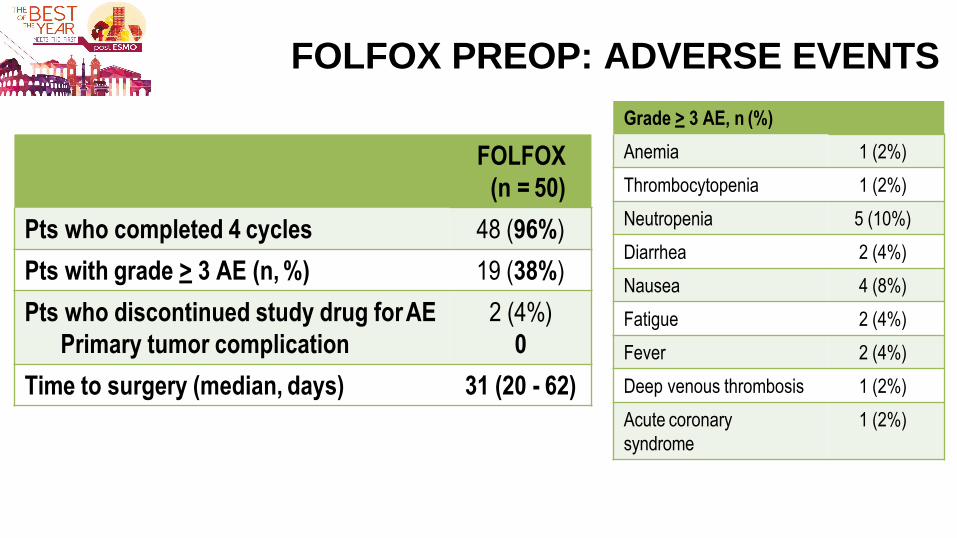
FOLFOX PREOP: ADVERSE EVENTS
FOLFOX
(n = 50)
Pts who completed 4 cycles 48 (96%)
Pts with grade > 3 AE (n, %) 19 (38%)
Pts who discontinued study drug for AE
Primary tumor complication
2 (4%)
0
Time to surgery (median, days) 31 (20 - 62)
Grade > 3 AE, n (%)
Anemia 1 (2%)
Thrombocytopenia 1 (2%)
Neutropenia 5 (10%)
Diarrhea 2 (4%)
Nausea 4 (8%)
Fatigue 2 (4%)
Fever 2 (4%)
Deep venous thrombosis 1 (2%)
Acute coronary
syndrome
1 (2%)
esmo.org
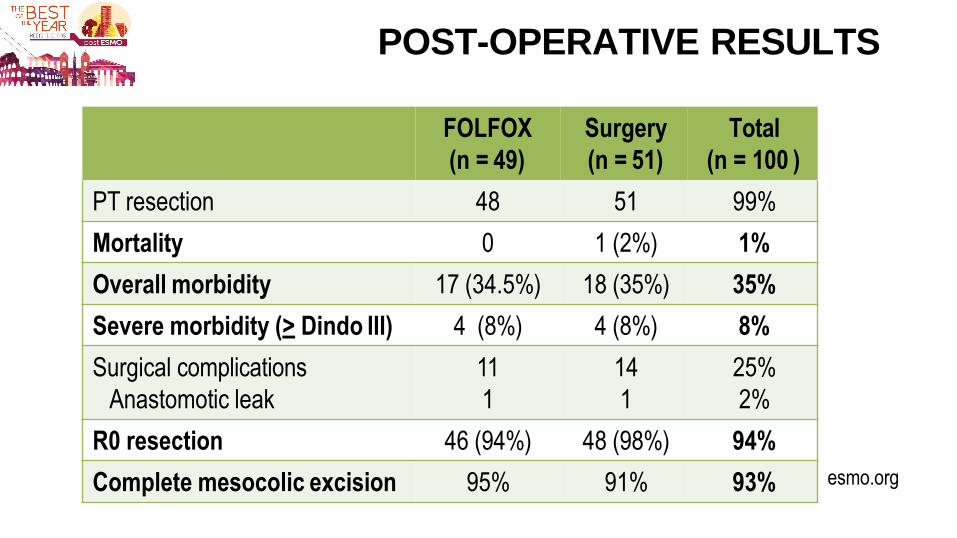
POST-OPERATIVE RESULTS
FOLFOX
(n = 49)
Surgery
(n = 51)
Total
(n = 100 )
PT resection 48 51 99%
Mortality 0 1 (2%) 1%
Overall morbidity 17 (34.5%) 18 (35%) 35%
Severe morbidity (> Dindo III) 4 (8%) 4 (8%) 8%
Surgical complications
Anastomotic leak
11
1
14
1
25%
2%
R0 resection 46 (94%) 48 (98%) 94%
Complete mesocolic excision 95% 91% 93%
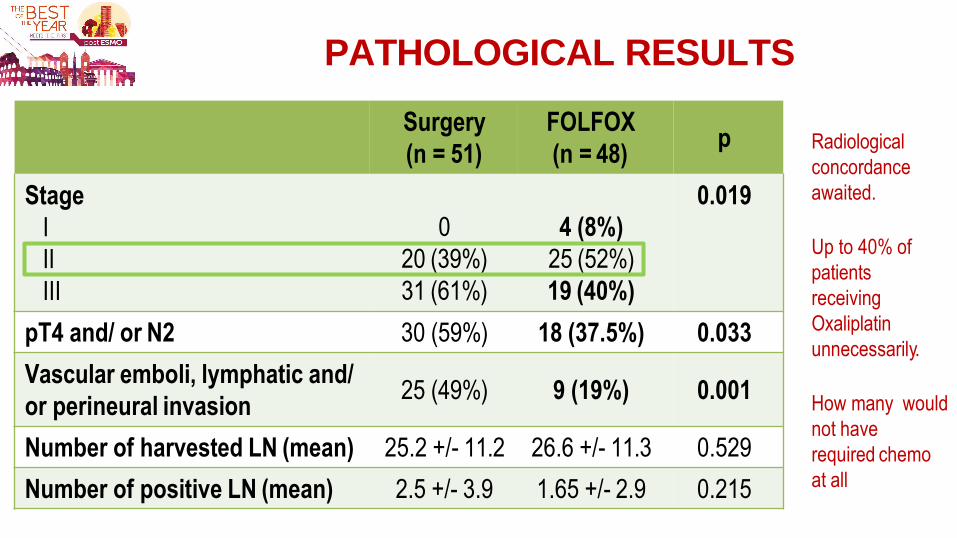
PATHOLOGICAL RESULTS
Surgery
(n = 51)
FOLFOX
(n = 48) p
Stage
I
II
III
0.019
0
20 (39%)
31 (61%)
4 (8%)
25 (52%)
19 (40%)
pT4 and/ or N2 30 (59%) 18 (37.5%) 0.033
Vascular emboli, lymphatic and/
or perineural invasion 25 (49%) 9 (19%) 0.001
Number of harvested LN (mean) 25.2 +/- 11.2 26.6 +/- 11.3 0.529
Number of positive LN (mean) 2.5 +/- 3.9 1.65 +/- 2.9 0.215
Radiological
concordance
awaited.
Up to 40% of
patients
receiving
Oxaliplatin
unnecessarily.
How many would
not have
required chemo
at all
esmo.org
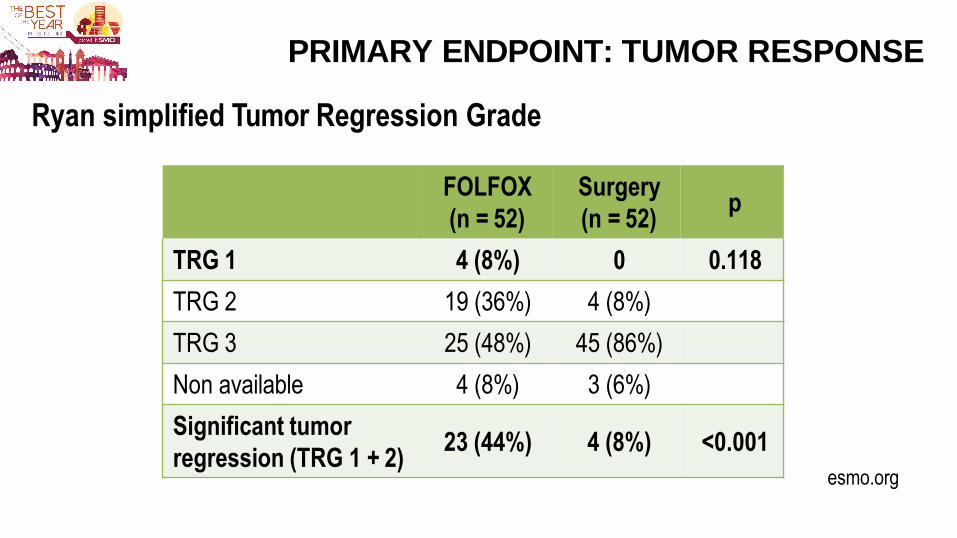
PRIMARY ENDPOINT: TUMOR RESPONSE
FOLFOX
(n = 52)
Surgery
(n = 52) p
TRG 1 4 (8%) 0 0.118
TRG 2 19 (36%) 4 (8%)
TRG 3 25 (48%) 45 (86%)
Non available 4 (8%) 3 (6%)
Significant tumor
regression (TRG 1 + 2) 23 (44%) 4 (8%) <0.001
Ryan simplified Tumor Regression Grade
esmo.org
PRODIGE 22 : CONCLUSION
• Neoadjuvant FOLFOX chemotherapy (4 cycles) in a perioperative
setting in patients with locally advanced colon cancer :
- is well tolerated
- does not increase surgical morbidity
- is not associated with major histological response (TRG1)
- is associated with significant tumor regression as compared
to upfront surgery (TRG 1+2 : 44% vs. 8% p<0.001)
- induces tumor downstaging
• Phase III studies testing this strategy to see if it significantly impacts 3y
DFS and 5y OS are now awaited
Failed to meet primary endpoint
VOLFI:
mFOLFOXIRI + PANITUMUMAB VERSUS FOLFOXIRI
esmo.org
Abstract 475O
AS FIRST-LINE TREATMENT IN PATIENTS WITH RAS WILD-TYPE
METASTATIC COLORECTAL CANCER (mCRC):
A RANDOMIZED PHASE II TRIAL OF THE AIO (AIO-KRK-0109)
M. Geissler (Esslingen, Germany), U. M. Martens (Heilbronn, Germany),
J. R. Knorrenschield (Marburg, Germany), J. Greeve (Paderborn, Germany),
A. Florschuetz (Dessau, Germany), A. Tannapfel (Bochum, Germany),
S. Wessendorf (Esslingen, Germany), P. Büchner-Steudel (Halle, Germany), T. J. Ettrich (Ulm, Germany), S. Kanzler (Schweinfurt, Germany), V. Heinemann (Munich, Germany),
S. Held (Leverkusen, Germany), A. Reinacher-Schick (Bochum, Germany)
Presented by Michael Geissler at the ESMO congress 2017.
Slides are property of the author. Permission required for reuse.
The study was sponsored by AIO-Studien-gGmbH (Berlin, Germany)
The study was financially supported by an unrestricted grant from Amgen. NCT01328171
EudraCT 2009-017731-17
RATIONALE
1
7
• FOLFOXIRI is an active and intensive chemotherapeutic regimen in mCRC
(Falcone et al. 2007)
• FOLFOXIRI+bevacizumab (TRIBE, STEAM, OLIVIA) and FOLFOXIRI + anti-
EGFR mAb (TRIP, MACBETH) resulted in high RR and long OS
• However, there is no randomized trial demonstrating superiority of FOLFOXIRI
plus an anti-EGFR or anti-VEGF mAb compared to FOLFOXIRI alone
• Therefore, the VOLFI trial compared the FOLFOXIRI Falcone protocol with
modified FOLFOXIRI + panitumumab
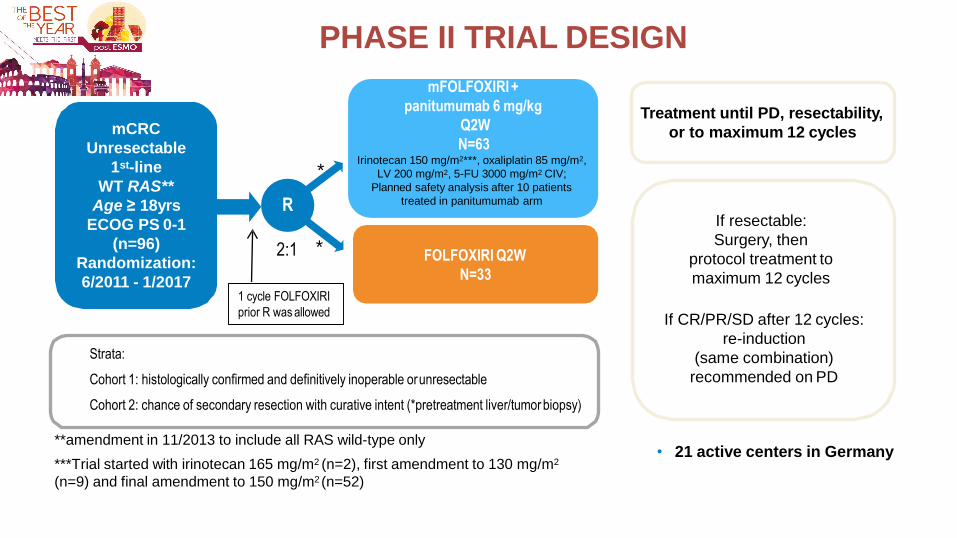
PHASE II TRIAL DESIGN
mCRC
Unresectable
1st-line
WT RAS**
Age ≥ 18yrs
ECOG PS 0-1
(n=96)
Randomization:
6/2011 - 1/2017
R
Treatment until PD, resectability,
or to maximum 12 cycles
mFOLFOXIRI +
panitumumab 6 mg/kg
Q2W
N=63 Irinotecan 150 mg/m2***, oxaliplatin 85 mg/m2,
LV 200 mg/m2, 5-FU 3000 mg/m2 CIV;
Planned safety analysis after 10 patients
treated in panitumumab arm
FOLFOXIRI Q2W
N=33
2:1
If resectable:
Surgery, then
protocol treatment to
maximum 12 cycles
If CR/PR/SD after 12 cycles:
re-induction
(same combination)
recommended on PD
Strata:
Cohort 1: histologically confirmed and definitively inoperable or unresectable
Cohort 2: chance of secondary resection with curative intent (*pretreatment liver/tumor biopsy)
*
*
• 21 active centers in Germany **amendment in 11/2013 to include all RAS wild-type only
***Trial started with irinotecan 165 mg/m2 (n=2), first amendment to 130 mg/m2
(n=9) and final amendment to 150 mg/m2 (n=52)
1 cycle FOLFOXIRI
prior R was allowed
1
8
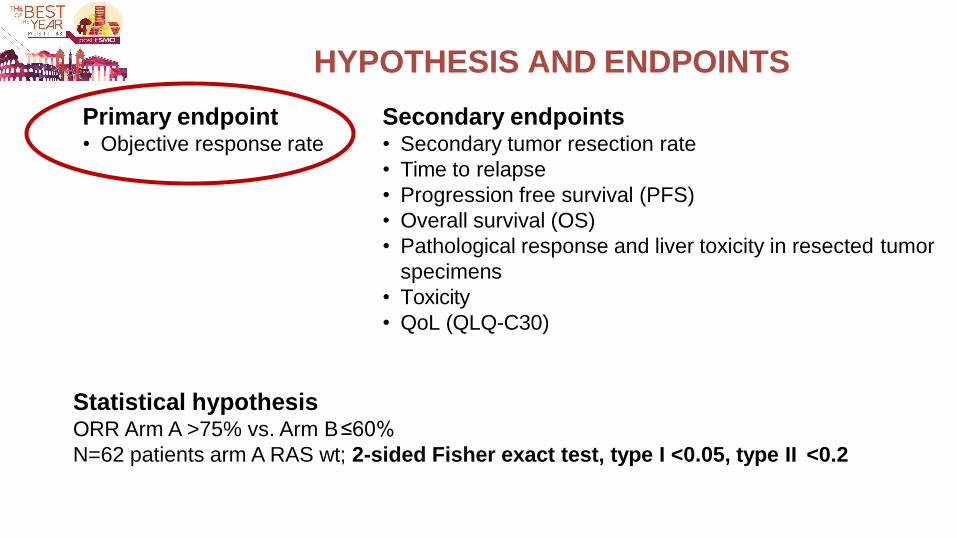
HYPOTHESIS AND ENDPOINTS
Secondary endpoints • Secondary tumor resection rate
• Time to relapse
• Progression free survival (PFS)
• Overall survival (OS)
• Pathological response and liver toxicity in resected tumor
specimens
• Toxicity
• QoL (QLQ-C30)
Statistical hypothesis ORR Arm A >75% vs. Arm B ≤60%
N=62 patients arm A RAS wt; 2-sided Fisher exact test, type I <0.05, type II <0.2
Primary endpoint • Objective response rate
RAS mutations
N = 4
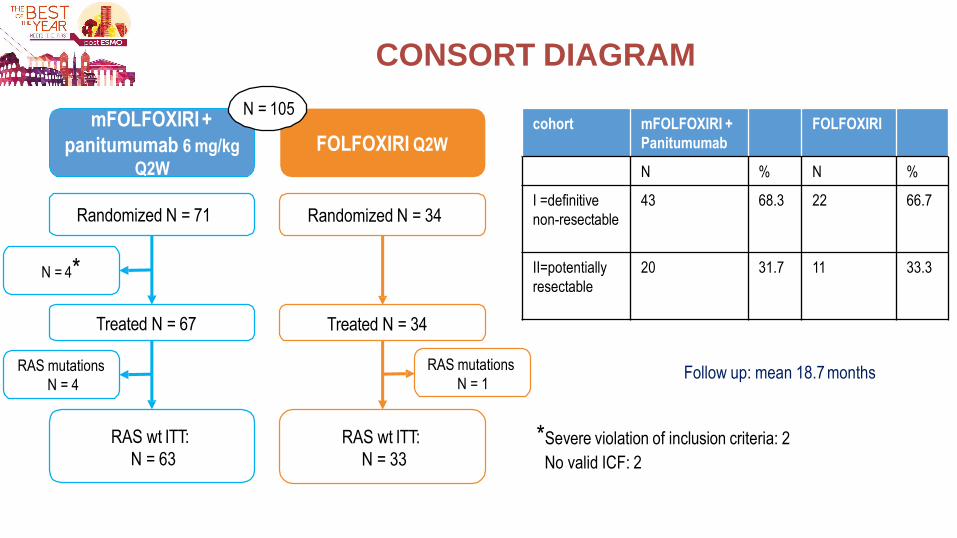
CONSORT DIAGRAM
FOLFOXIRI Q2W
Follow up: mean 18.7 months
*Severe violation of inclusion criteria: 2
No valid ICF: 2
Randomized N = 34
Treated N = 34
RAS wt ITT:
N = 33
mFOLFOXIRI +
panitumumab 6 mg/kg
Q2W
Randomized N = 71
Treated N = 67
RAS wt ITT:
N = 63
N = 105
RAS mutations
N = 1
N = 4*
20
cohort mFOLFOXIRI +
Panitumumab
FOLFOXIRI
N % N %
I =definitive
non-resectable
43 68.3 22 66.7
II=potentially
resectable
20 31.7 11 33.3
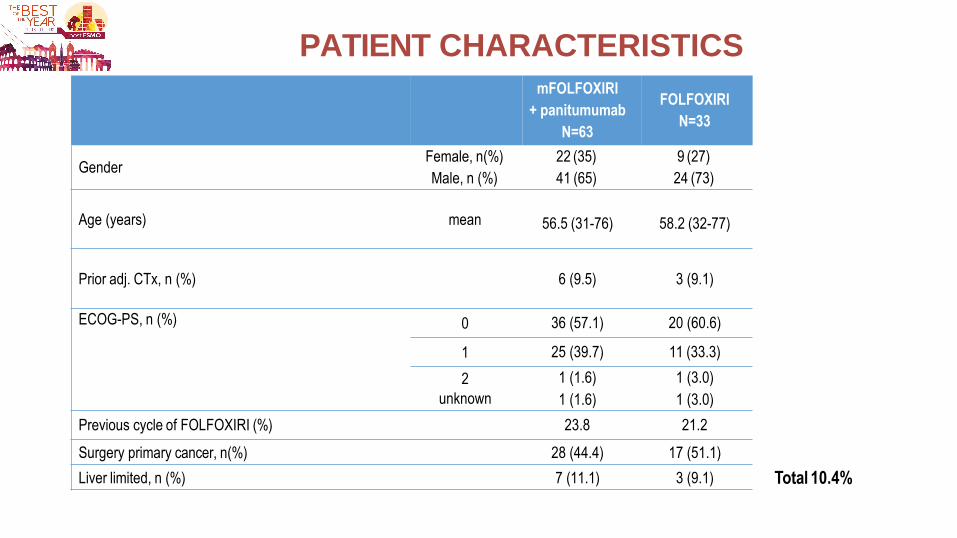
PATIENT CHARACTERISTICS
21
mFOLFOXIRI
+ panitumumab
N=63
FOLFOXIRI
N=33
Gender Female, n(%)
Male, n (%)
22 (35)
41 (65)
9 (27)
24 (73)
Age (years)
mean
56.5 (31-76)
58.2 (32-77)
Prior adj. CTx, n (%)
6 (9.5)
3 (9.1)
ECOG-PS, n (%) 0 36 (57.1) 20 (60.6)
1 25 (39.7) 11 (33.3)
2 1 (1.6) 1 (3.0)
unknown 1 (1.6) 1 (3.0)
Previous cycle of FOLFOXIRI (%) 23.8 21.2
Surgery primary cancer, n(%) 28 (44.4) 17 (51.1)
Liver limited, n (%) 7 (11.1) 3 (9.1) Total 10.4%
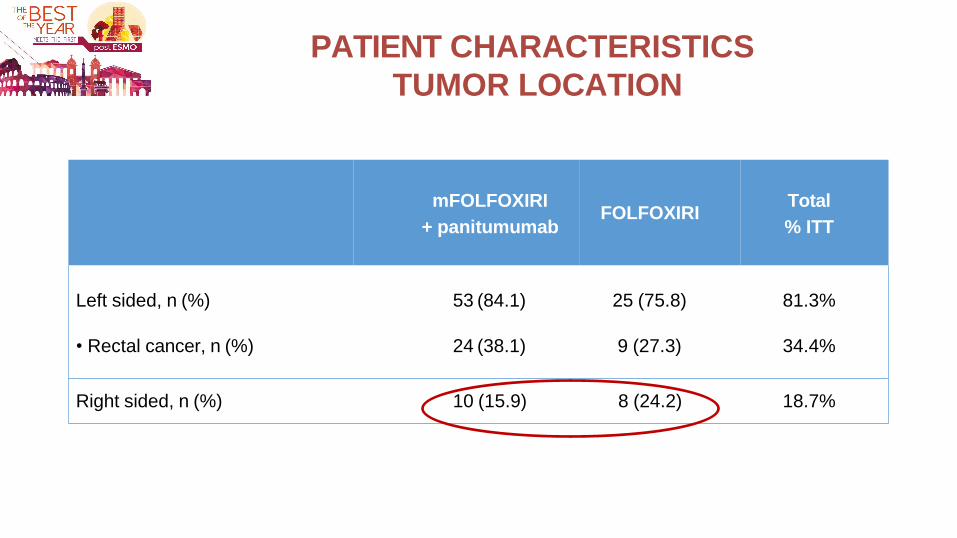
PATIENT CHARACTERISTICS
TUMOR LOCATION
22
mFOLFOXIRI
+ panitumumab
FOLFOXIRI
Total
% ITT
Left sided, n (%)
• Rectal cancer, n (%)
53 (84.1)
24 (38.1)
25 (75.8)
9 (27.3)
81.3%
34.4%
Right sided, n (%) 10 (15.9) 8 (24.2) 18.7%
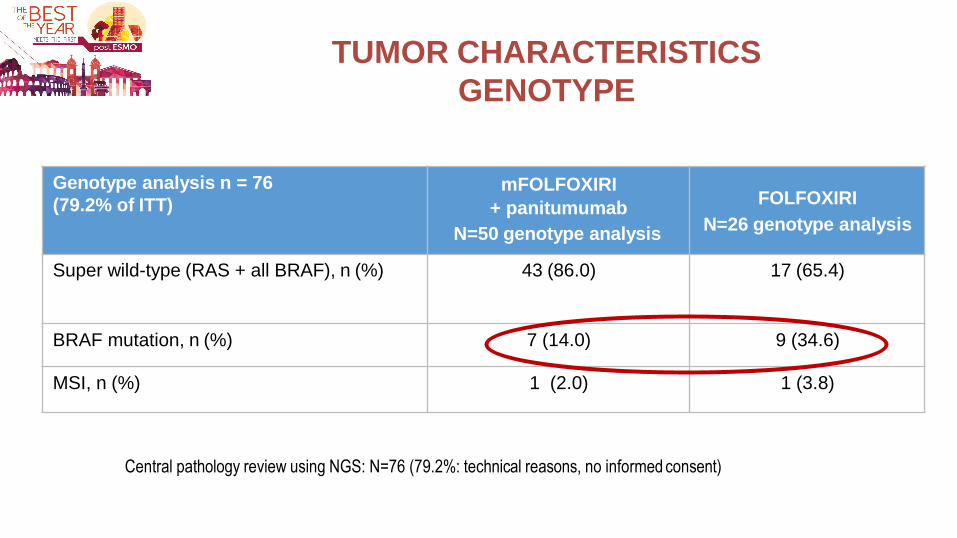
TUMOR CHARACTERISTICS
GENOTYPE
23
Central pathology review using NGS: N=76 (79.2%: technical reasons, no informed consent)
Genotype analysis n = 76
(79.2% of ITT) mFOLFOXIRI
+ panitumumab
N=50 genotype analysis
FOLFOXIRI
N=26 genotype analysis
Super wild-type (RAS + all BRAF), n (%) 43 (86.0) 17 (65.4)
BRAF mutation, n (%) 7 (14.0) 9 (34.6)
MSI, n (%) 1 (2.0) 1 (3.8)
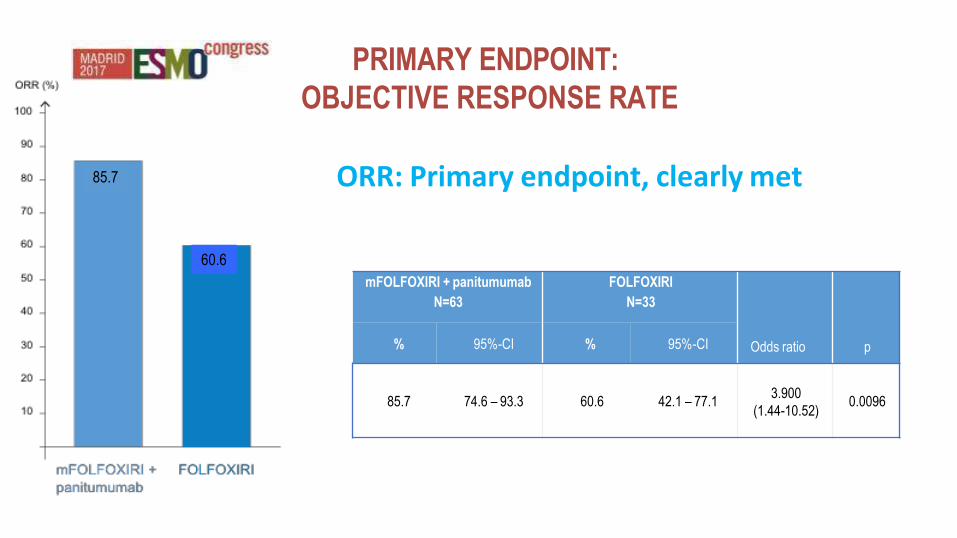
PRIMARY ENDPOINT:
OBJECTIVE RESPONSE RATE
mFOLFOXIRI + panitumumab
N=63
FOLFOXIRI
N=33
Odds ratio
p % 95%-CI % 95%-CI
85.7
74.6 – 93.3
60.6
42.1 – 77.1
3.900
(1.44-10.52)
0.0096
85.7
24
60.6
ORR: Primary endpoint, clearly met
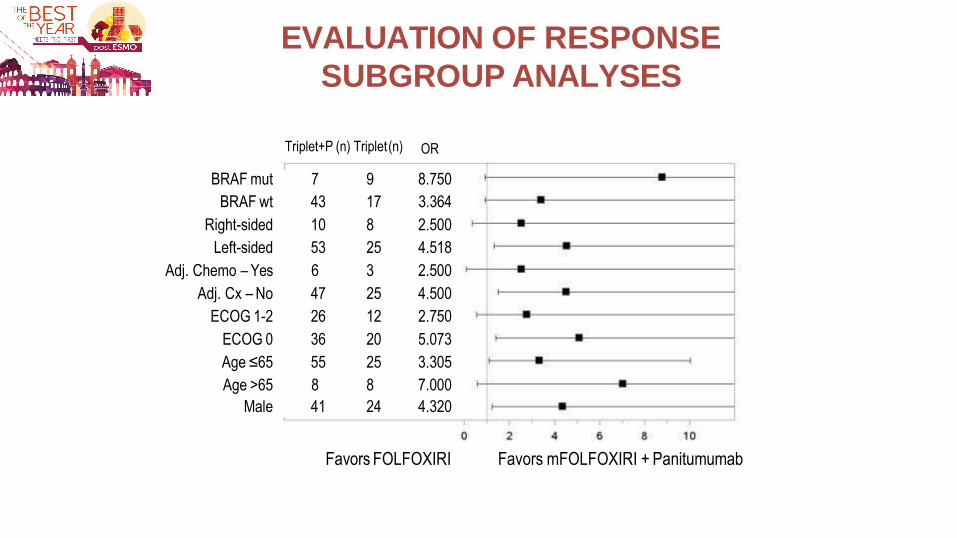
EVALUATION OF RESPONSE
SUBGROUP ANALYSES
OR Triplet+P (n) Triplet (n)
BRAF mut 7 9 8.750
BRAF wt 43 17 3.364
Right-sided 10 8 2.500
Left-sided 53 25 4.518
Adj. Chemo – Yes 6 3 2.500
Adj. Cx – No 47 25 4.500
ECOG 1-2 26 12 2.750
ECOG 0 36 20 5.073
Age ≤65 55 25 3.305
Age >65 8 8 7.000
Male 41 24 4.320
Favors FOLFOXIRI Favors mFOLFOXIRI + Panitumumab
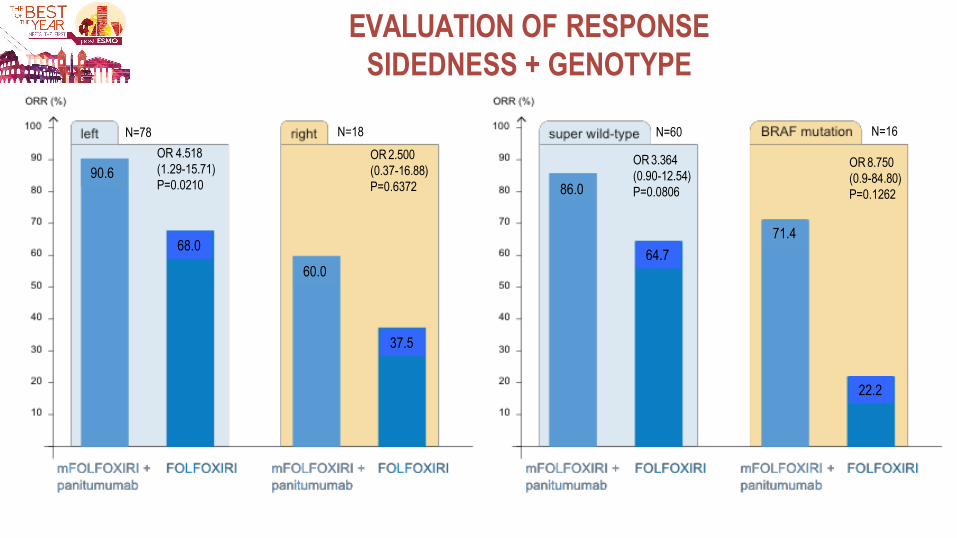
EVALUATION OF RESPONSE
SIDEDNESS + GENOTYPE
OR 4.518
(1.29-15.71)
P=0.0210
OR 2.500
(0.37-16.88)
P=0.6372
OR 8.750
(0.9-84.80)
P=0.1262
26
N=60
OR 3.364
(0.90-12.54)
P=0.0806
N=16 N=78 N=18
90.6
68.0
60.0
37.5
86.0
64.7
71.4
22.2
TRIBE
n=252
STEAM
n=93
MOMA
n=232*
CHARTA
n=125
VOLFI
=99 RAS WT
FOLFOXIRI/Bev vs FOLFIRI/Bev
FOLFOXIRI/Bev (seq’l vs conc’t) vs FOLFOX/Bev
FOLFOXIRI/Bev →
Bev ± metroCT
FOLFOX/Bev
± IRI
FOLFOXIRI +/- pan
RAS WT Regimen
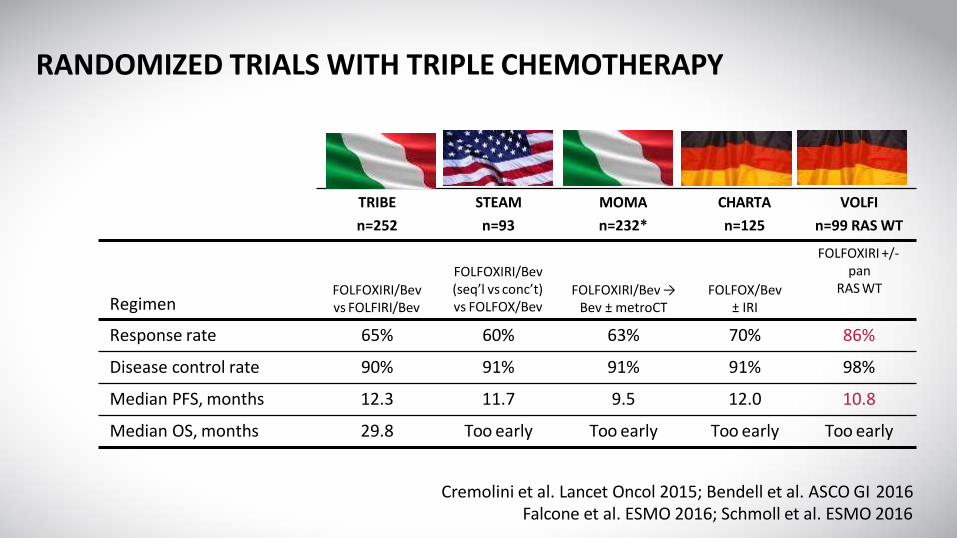
Response rate 65% 60% 63% 70% 86%
Disease control rate 90% 91% 91% 91% 98%
Median PFS, months 12.3 11.7 9.5 12.0 10.8
Median OS, months 29.8 Too early Too early Too early Too early
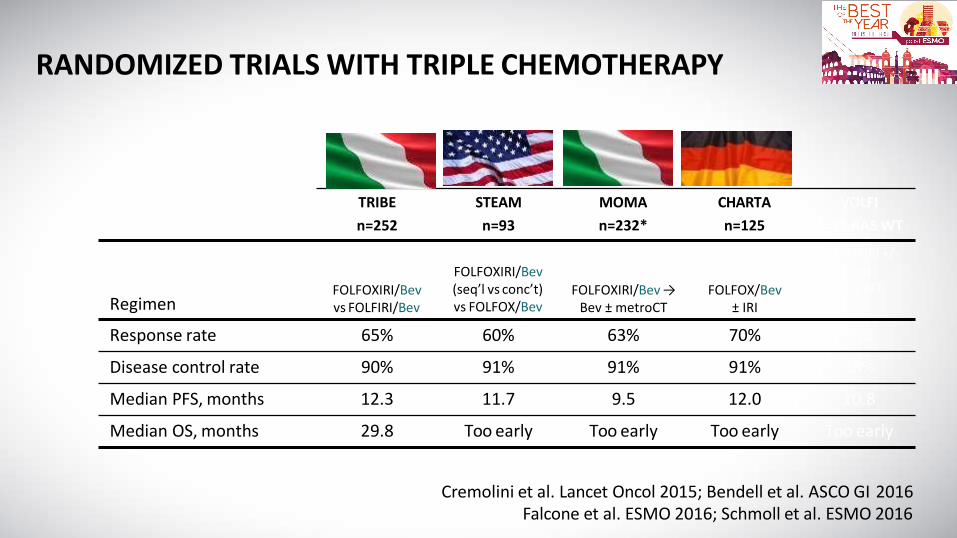
RANDOMIZED TRIALS WITH TRIPLE CHEMOTHERAPY
Cremolini et al. Lancet Oncol 2015; Bendell et al. ASCO GI 2016 Falcone et al. ESMO 2016; Schmoll et al. ESMO 2016
TRIBE
n=252
STEAM
n=93
MOMA
n=232*
CHARTA
n=125
VOLFI
n=99 RAS WT
FOLFOXIRI/Bev vs FOLFIRI/Bev
FOLFOXIRI/Bev (seq’l vs conc’t) vs FOLFOX/Bev
FOLFOXIRI/Bev →
Bev ± metroCT
FOLFOX/Bev
± IRI
FOLFOXIRI +/- pan
RAS WT Regimen
Response rate 65% 60% 63% 70% 86%
Disease control rate 90% 91% 91% 91% 98%
Median PFS, months 12.3 11.7 9.5 12.0 10.8
Median OS, months 29.8 Too early Too early Too early Too early
RANDOMIZED TRIALS WITH TRIPLE CHEMOTHERAPY
Cremolini et al. Lancet Oncol 2015; Bendell et al. ASCO GI 2016 Falcone et al. ESMO 2016; Schmoll et al. ESMO 2016
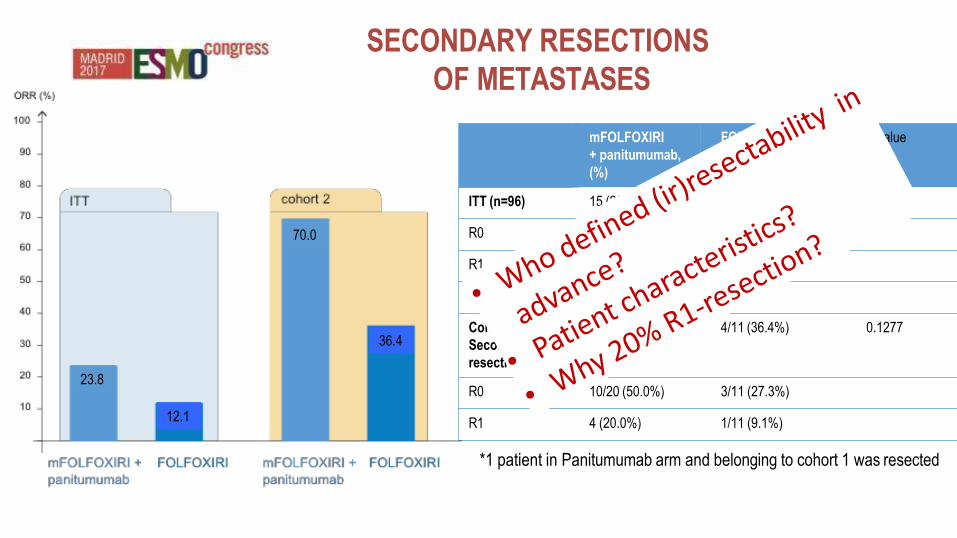
SECONDARY RESECTIONS
OF METASTASES
mFOLFOXIRI
+ panitumumab,
(%)
FOLFOXIRI
(%)
P value
ITT (n=96) 15 (23.8) 4 (12.1) 0.2802
R0 10 (15.9) 3 (9.1)
R1 4 (6.3) 1 (3.0)
Cohort 2 (n=31)
Secondary
resection
14/20 (70%)* 4/11 (36.4%) 0.1277
R0 10/20 (50.0%) 3/11 (27.3%)
R1 4 (20.0%) 1/11 (9.1%)
*1 patient in Panitumumab arm and belonging to cohort 1 was resected
23.8
12.1
70.0
36.4
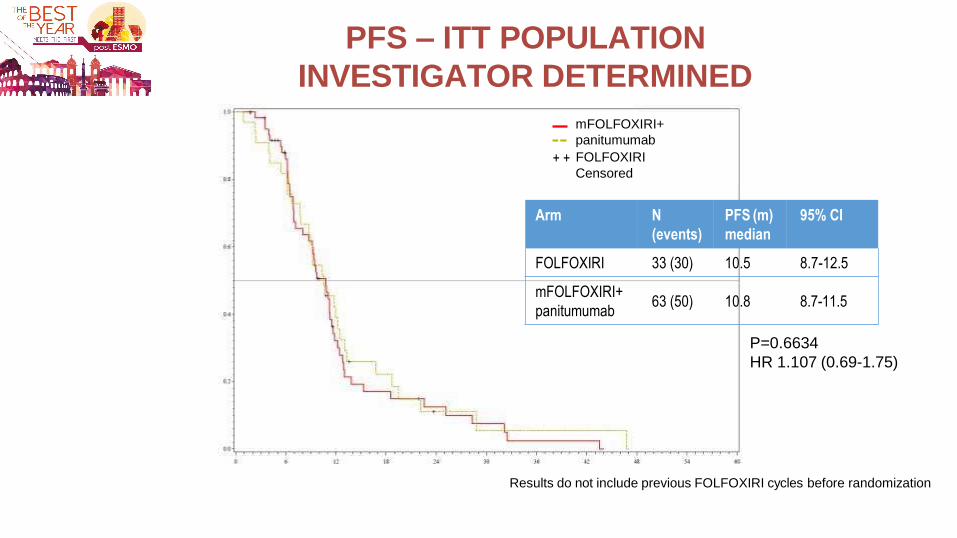
PFS – ITT POPULATION
INVESTIGATOR DETERMINED
mFOLFOXIRI+
panitumumab
+ + FOLFOXIRI
Censored
Results do not include previous FOLFOXIRI cycles before randomization
30
P=0.6634
HR 1.107 (0.69-1.75)
Arm N
(events)
PFS (m)
median
95% CI
FOLFOXIRI 33 (30) 10.5 8.7-12.5
mFOLFOXIRI+
panitumumab 63 (50) 10.8 8.7-11.5
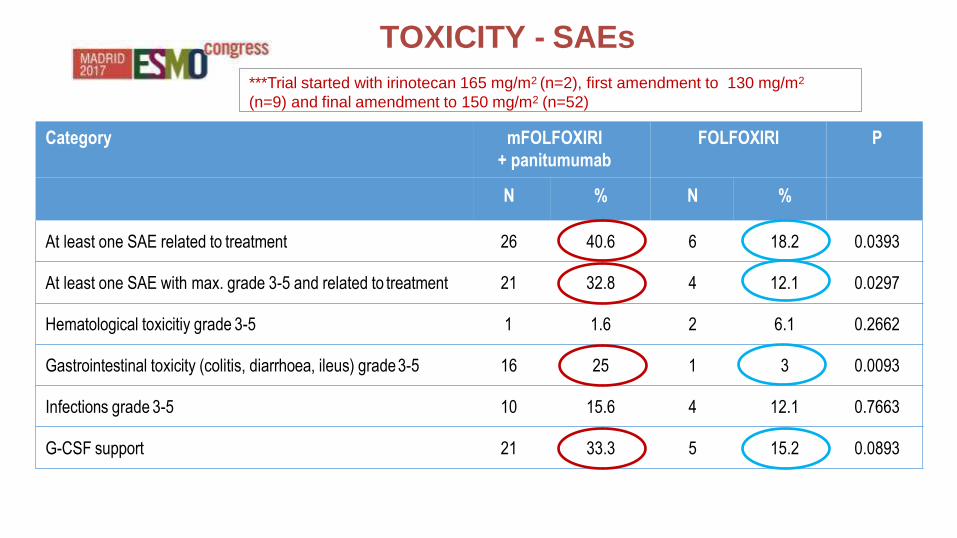
TOXICITY - SAEs
31
Category mFOLFOXIRI
+ panitumumab
FOLFOXIRI P
N % N %
At least one SAE related to treatment 26 40.6 6 18.2 0.0393
At least one SAE with max. grade 3-5 and related to treatment 21 32.8 4 12.1 0.0297
Hematological toxicitiy grade 3-5 1 1.6 2 6.1 0.2662
Gastrointestinal toxicity (colitis, diarrhoea, ileus) grade 3-5 16 25 1 3 0.0093
Infections grade 3-5 10 15.6 4 12.1 0.7663
G-CSF support 21 33.3 5 15.2 0.0893
***Trial started with irinotecan 165 mg/m2 (n=2), first amendment to 130 mg/m2
(n=9) and final amendment to 150 mg/m2 (n=52)
32
• Primary endpoint was positive: first line treatment with mFOLFOXIRI +
panitumumab resulted in significantly higher ORR compared to FOLFOXIRI.
• The addition of panitumumab to FOLFOXIRI resulted in high response rates in left
and right sided as well as BRAF mutated mCRC.
• PFS was in the expected range, however, there was no difference in PFS
between both arms. OS data are still immature.
Conclusions
• DpR, ETS analyses
• EORTC QLQ-C30
• PFS/OS/TTR in secondary resected patients
• OS ITT, RAS/BRAF, sidedness
• Toxicity / AEs
• Dose reductions, relative dosage, numbers of delivered cycles
• Pathological response and liver toxicity in resected tumor specimens
33
VOLFI (AIO-KRK-0109)
DATA PENDING
• EGFR moAb´s (here: panitumumab) add to improvement of ORR, even with triple chemotherapy
– and even in „unexpected“ subgroups (right-sided, BRAF mutant)
• The regimen seems to be tolerable – however, more toxicity and quality of life data needed
• Clinical role a bit unclear
R1 rates higher
PFS not improved
OS pending
34
Personal conclusions:
Damien Hirst: Drugs
SUMMARY (II)
36
• mFOLFOXIRI + panitumumab has relevant, but manageable hematological
and gastrointestinal toxicity and should be used in ECOG 0-1 patients only.
Compared to the GONO FOLFOXIRI protocol, the irinotecan dose should be
reduced to 150 mg/m2.
• The high response rates are of particular interest for symptomatic patients and
those with a chance of secondary resections of initially unresectable
metastatic sites in left/right as well as BRAF mutated mCRC.


















