Nucleic Acid Detection Systems for Enteroviruses · CLIN. MICROBIOL. REV. society for tens of...
13
CLINICAL MICROBIOLOGY REVIEWS, Apr. 1991, p. 156-168 Vol. 4, No. 2 0893-8512/91/020156-13$02.00/0 Copyright © 1991, American Society for Microbiology Nucleic Acid Detection Systems for Enteroviruses HARLEY A. ROTBART Departments of Pediatrics and Microbiologyllmmunology, University of Colorado School of Medicine, Denver, Color-ado 80262 INTRODUCTION .................................................... 156 CLINICAL SIGNIFICANCE .................................................... 156 Acute Infections .................................................... 156 Chronic Diseases .................................................... 157 DIAGNOSIS .................................................... 157 Need for a Rapid Diagnostic Test .................................................... 157 Current Diagnostic "Gold Standards" .................................................... 158 Antigen Detection .................................................... 158 Nucleic Acid Hybridization .................................................... 158 cDNA probes .................................................... 158 RNA probes .................................................... 160 Improvement of target retention prior to and during hybridization ............................................ 161 Amplification of target sequences prior to hybridization .................................................... 161 PATHOGENESIS .................................................... 162 In Vitro Studies .................................................... 162 Animal Models Using Animal Picornaviruses .................................................... 162 Animal Models Using Human EV Serotypes .................................................... 163 Studies of Human Tissues .................................................... 164 CONCLUSIONS .................................................... 165 ACKNOWLEDGMENTS .................................................... 165 REFERENCES .................................................... 165 INTRODUCTION The enteroviruses (EVs) are among the most common and most important viral pathogens of humans (22, 67). The paralytic potential of the polioviruses, prototypic EVs, was recognized as early as the 14th century B.C. in Egyptian art (61). Summer epidemics of poliomyelitis devastated the United States through the 1950s. Since the introduction of poliovirus vaccines in the late 1950s and early 1960s, much of the developed world is now essentially free of poliovirus infections. Developing countries, where vaccines are often either unavailable or ineffective, continue to struggle with these pathogens (6). It has been estimated by the World Health Organization that 4 of every 1,000 school-age chil- dren in developing countries contract paralytic disease due to poliovirus infections. Control of poliovirus infections in much of the world has focused attention on the nonpolio EVs, which include the coxsackieviruses, echoviruses, and newer numbered EVs (Table 1). In the United States alone, the nonpolio EVs are estimated to cause 5 to 10 million symptomatic infections annually (95). In temperate climates, these infections occur during the summer and fall months (70, 95); young children are the most common victims, as both the incidence and severity of nonpolio EV infections vary inversely with the patient's age (70, 71, 95). In addition to the actual diseases that EVs cause, the EV ability to mimic other pathogens is of great concern. Distinguishing EV infections from those due to common bacteria and herpes simplex viruses is often difficult on clinical grounds alone (22). Hence, unnecessary treatment for herpes simplex virus infections is frequently instituted during EV infections. The EVs have a special place in the history of modern virology. Polioviruses were the first viruses to be success- fully propagated in cell culture-a monumental accomplish- ment which led directly to the development of poliovirus vaccines (36). J. F. Enders and his colleagues were awarded the Nobel Prize for this work, which, in addition to its contribution to vaccine development, has to this day re- mained the "gold standard" method for all viral diagnosis. The availability of this cell culture technique rapidly led to the identification of new viruses, including the coxsackievi- ruses and echoviruses (33). Once again, within the past decade, polioviruses have played a significant role in ad- vancing the field of virology. The resolution of the atomic structure of poliovirus type 1 (44) and a similar achievement with rhinovirus 2 (78), a fellow member of the picornavirus family, have elucidated intricate details of virion surface structures, including host cell receptor-binding sites and potential antiviral drug-binding sites. What follows is a brief discussion of the clinical signifi- cance of the nonpolio EVs and a more comprehensive review of the current state of the art in diagnostic methods available for these pathogens. The emphasis of the latter will be on nucleic acid-based detection systems, since that is the area of my personal research endeavors. CLINICAL SIGNIFICANCE Acute Infections The EVs are responsible for a wide array of clinical diseases affecting all major body systems (Table 2). It is important to note that no disease is uniquely associated with any specific EV serotype and that no serotype is uniquely associated with any one disease (22, 67). This is true even of paralytic poliomyelitis, which has been associated with numerous nonpolio EV serotypes (40, 66, 104). For that 156 on July 10, 2019 by guest http://cmr.asm.org/ Downloaded from
Transcript of Nucleic Acid Detection Systems for Enteroviruses · CLIN. MICROBIOL. REV. society for tens of...
CLINICAL MICROBIOLOGY REVIEWS, Apr. 1991, p. 156-168 Vol. 4, No. 20893-8512/91/020156-13$02.00/0Copyright © 1991, American Society for Microbiology
Nucleic Acid Detection Systems for EnterovirusesHARLEY A. ROTBART
Departments of Pediatrics and Microbiologyllmmunology, University of Colorado School of Medicine,Denver, Color-ado 80262
INTRODUCTION .................................................... 156CLINICAL SIGNIFICANCE .................................................... 156
Acute Infections .................................................... 156Chronic Diseases .................................................... 157
DIAGNOSIS .................................................... 157Need for a Rapid Diagnostic Test .................................................... 157Current Diagnostic "Gold Standards".................................................... 158Antigen Detection .................................................... 158Nucleic Acid Hybridization.................................................... 158cDNA probes.................................................... 158RNA probes .................................................... 160Improvement of target retention prior to and during hybridization ............................................ 161Amplification of target sequences prior to hybridization .................................................... 161
PATHOGENESIS .................................................... 162In Vitro Studies .................................................... 162Animal Models Using Animal Picornaviruses .................................................... 162Animal Models Using Human EV Serotypes.................................................... 163Studies of Human Tissues .................................................... 164
CONCLUSIONS .................................................... 165ACKNOWLEDGMENTS .................................................... 165REFERENCES .................................................... 165
INTRODUCTION
The enteroviruses (EVs) are among the most common andmost important viral pathogens of humans (22, 67). Theparalytic potential of the polioviruses, prototypic EVs, wasrecognized as early as the 14th century B.C. in Egyptian art(61). Summer epidemics of poliomyelitis devastated theUnited States through the 1950s. Since the introduction ofpoliovirus vaccines in the late 1950s and early 1960s, muchof the developed world is now essentially free of poliovirusinfections. Developing countries, where vaccines are ofteneither unavailable or ineffective, continue to struggle withthese pathogens (6). It has been estimated by the WorldHealth Organization that 4 of every 1,000 school-age chil-dren in developing countries contract paralytic disease dueto poliovirus infections.
Control of poliovirus infections in much of the world hasfocused attention on the nonpolio EVs, which include thecoxsackieviruses, echoviruses, and newer numbered EVs(Table 1). In the United States alone, the nonpolio EVs areestimated to cause 5 to 10 million symptomatic infectionsannually (95). In temperate climates, these infections occurduring the summer and fall months (70, 95); young childrenare the most common victims, as both the incidence andseverity of nonpolio EV infections vary inversely with thepatient's age (70, 71, 95). In addition to the actual diseasesthat EVs cause, the EV ability to mimic other pathogens is ofgreat concern. Distinguishing EV infections from those dueto common bacteria and herpes simplex viruses is oftendifficult on clinical grounds alone (22). Hence, unnecessarytreatment for herpes simplex virus infections is frequentlyinstituted during EV infections.The EVs have a special place in the history of modern
virology. Polioviruses were the first viruses to be success-
fully propagated in cell culture-a monumental accomplish-ment which led directly to the development of poliovirusvaccines (36). J. F. Enders and his colleagues were awardedthe Nobel Prize for this work, which, in addition to itscontribution to vaccine development, has to this day re-mained the "gold standard" method for all viral diagnosis.The availability of this cell culture technique rapidly led tothe identification of new viruses, including the coxsackievi-ruses and echoviruses (33). Once again, within the pastdecade, polioviruses have played a significant role in ad-vancing the field of virology. The resolution of the atomicstructure of poliovirus type 1 (44) and a similar achievementwith rhinovirus 2 (78), a fellow member of the picornavirusfamily, have elucidated intricate details of virion surfacestructures, including host cell receptor-binding sites andpotential antiviral drug-binding sites.What follows is a brief discussion of the clinical signifi-
cance of the nonpolio EVs and a more comprehensivereview of the current state of the art in diagnostic methodsavailable for these pathogens. The emphasis of the latter willbe on nucleic acid-based detection systems, since that is thearea of my personal research endeavors.
CLINICAL SIGNIFICANCE
Acute InfectionsThe EVs are responsible for a wide array of clinical
diseases affecting all major body systems (Table 2). It isimportant to note that no disease is uniquely associated withany specific EV serotype and that no serotype is uniquelyassociated with any one disease (22, 67). This is true even ofparalytic poliomyelitis, which has been associated withnumerous nonpolio EV serotypes (40, 66, 104). For that
156
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from

NUCLEIC ACID DETECTION SYSTEMS FOR ENTEROVIRUSES
TABLE 1. EV serotypes
Subgroup Serotypes
Poliovirus.............1-3Coxsackieviruses A............. 1-22. 24"Coxsackieviruses B............. 1-6Echovirus............. 1-9, 11-27, 29-31"Numbered EVs ............. 68-72
" Coxsackievirus A23 and echoviruses 10 and 28 have been reclassified.
reason, it is sufficient to speak of diseases "that EVs cause"and to diagnose "an EV" in the laboratory without neces-sarily specifying or identifying the particular serotype. Cer-tain clinical syndromes are indeed more likely to be causedby one or a few serotypes (see below), but significant overlapexists among the serotypes and the diseases they cause.The most common clinical manifestation ofEV infection is
a nonspecific febrile illness, with or without a rash. Thisso-called viral syndrome is the most common cause of feveramong children. When accompanied, as it often is, by upperrespiratory symptoms, the "summer cold" is indistinguish-able from the same illness caused by rhinoviruses (fellowpicornaviruses) in the winter months. By far the most vexingclinical EV syndrome that the physician encounters is asep-tic meningitis (106). The EVs are the most common cause ofmeningitis in the United States. In young infants with thedisease, clinical criteria to distinguish EV meningitis fromthat due to bacteria and herpes simplex virus are unreliable.As a result, even though EV meningitis is generally benign inoutcome and no specific therapy is indicated (or available;
TABLE 2. Clinical syndromes caused by EVs
Organ system Disease
Neurologic .......... Aseptic meningitis"Encephalitis"Poliomyelitis"Transverse myelitisGuillain-Barre syndromeCerebellar ataxiaPeripheral neuritis
Respiratory .......... Common cold"Stomatitis, herpangina, hand-foot-mouthsyndrome"
Pharyngitis, tonsillitis, rhinitis"Pleurodynia (Bornholm disease)Croup, bronchitis, bronchiolitisPneumoniaParotitis
Gastrointestinal .......... GastroenteritisHepatitis'Mesenteric adenitisPeritonitisPancreatitis (?diabetes mellitus)Reye's syndrome
Cardiovascular .......... Mycocarditis"PericarditisEndocarditislike valve lesions?Myocardial infarction
Miscellaneous .......... Febrile, exanthematous illness"Neonatal sepsis"
see below), thousands of children are hospitalized andtreated with unnecessary antibiotics and antiherpes medica-tions annually because of the fear that a case of meningitis isnot due to an EV (24). Additional acute clinical EV syn-dromes of significance include encephalitis, poliomyelitis(particularly due to the polioviruses), myocarditis (particu-larly due to the coxsackievirus B group) (56), hemorrhagicconjunctivitis (particularly due to serotypes coxsackievirusA24 and EV70) (18, 68), hand-foot-mouth syndrome, Born-holm disease (pleurodynia), and overwhelming neonatalsepsis (particularly due to the echoviruses and coxsackievi-ruses B) (55, 69). The last syndrome is thought to be due toperinatal transmission, either transplacentally or duringbirth, from mother to infant. Despite the name, entericdisease is not a prominent manifestation of EV infection,although diarrhea and vomiting may be significant manifes-tations of certain outbreaks of "summer flu" due to the EVs.EV72 (hepatitis A) is unique in that it is the only EV serotypewhich almost exclusively causes hepatitis; more-commonEV syndromes have not been associated with EV72. Forpurposes of the ensuing discussion, EV72 will not be con-sidered with the other EVs, since substantial data suggestthat, genetically, EV72 is only minimally related to the otherEV serotypes (25); reclassification of hepatitis A as anon-EV picornavirus would probably be appropriate. Mildhepatitis, almost always in association with other moresignificant findings, is common during infection with manyEV serotypes.
Chronic Diseases
In addition to being the causes of well-recognized acutediseases, EVs have been implicated in several chronicillnesses including juvenile onset diabetes mellitus (8, 111),chronic fatigue syndrome (5), dermatomyositis and polymy-ositis (13, 77), congenital hydrocephalus (38), and amyotro-pic lateral sclerosis (37). Evidence for these associations hasbeen largely from serology or from nucleic acid hybridiza-tion studies (see below); definitive proof is lacking, andconfirmatory studies remain to be done.
Persistent EV infections occur in agammaglobulinemicpatients; manifestations almost always include meningoen-cephalitis (64). Half of all patients with persistent EV me-ningoencephalitis have concomitant dermatomyositis or poly-myositis. These observations confirm the important role ofantibody in EV clearance, an unusual phenomenon, becausemost other viruses are contained largely by cell-mediatedimmunity. Recently, a syndrome of late-onset muscularatrophy and pain has been reported in individuals whosuffered paralytic poliomyelitis 20 to 40 years previously (32,52); evidence for persistent or latent infection in theseindividuals has not been found.
DIAGNOSIS
Need for a Rapid Diagnostic Test
There are numerous compelling reasons for seeking arapid diagnostic assay for the EVs. The diverse spectra ofclinical manifestations frequently present the physician witha confusing and lengthy differential diagnosis. The infantwith high fever, rash, and/or meningitis cannot be assumedto have EV infection; empiric therapeutic maneuvers formultiple potential pathogens are almost always undertaken.This approach results in significant personal and financialhardships on the patient and family (24). The annual cost to
" Most common and/or most important manifestations.bDue to serotypes other than EV72 (hepatitis A).
VOL. 4, 1991 157
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from

CLIN. MICROBIOL. REV.
society for tens of thousands of unnecessary hospital daysand treatments is substantial. Furthermore, although mostEV illness is benign, certain diseases are severe enough towarrant specific antiviral therapy were such available. Prom-ising anti-EV compounds have been developed (53, 63, 65,74, 108) but remain untested in humans, at least in partbecause a diagnostic test to identify infected patients rapidlyis not now available. Finally, as noted above, numerousdiseases have been circumstantially linked to the EVs with-out definitive proof. A clear association for the EVs withthese and, potentially, other illnesses of unknown etiologywould facilitate our understanding and treatment of suchconditions.
Implied in this discussion has been the inadequacy ofcurrent diagnostic modalities. The following section reviewsthat issue.
Current Diagnostic "Gold Standards"
Since its inception more than 40 years ago, cell culturecontinues to be the mainstay of EV diagnosis, despitewell-recognized limitations. The technique is labor intensiveand requires a high level of expertise. As many as 25 to 35%of EV serotypes, particularly the coxsackievirus A group, donot grow at all in cell culture (24, 58, 105). The latter can beidentified by suckling mouse inoculation, a technique toocumbersome to be widely available. The serotypes that dogrow in cell culture may do so slowly. Reported mean
isolation times for EVs from cerebrospinal fluid (CSF) rangefrom 3.7 to 8.2 days (24, 50). Cultures from other sites may
become positive sooner, but meningitis and encephalitiscause the greatest clinical consternation because their pre-sentations are often indistinguishable from those of bacterialand herpes simplex virus central nervous system infections.The use of multiple cell lines may improve the yield or therapidity with which an EV is isolated (23, 31) at the cost ofincreasing the labor and resources required.
Serologic testing has had only a limited role in EVdiagnosis. The best-studied clinical application has beenwith coxsackievirus B immunoglobulin M assays, whichtake advantage of the shared antigen among the six coxsack-ievirus B serotypes and the early appearance of the immu-noglobulin M class of antibodies (9, 34, 62). Except for thethree poliovirus serotypes, other EVs do not appear to sharea single antigen which can be exploited for serologic studies.If the specific serotype of an infecting EV is known or
suspected, e.g., in community-wide outbreaks, confirmatoryimmunoglobulin G serology can be performed to document a
rise in antibody titer from the acute to the convalescentphase of infection, thus providing information useful forepidemiologic purposes but of little benefit to the individualpatient. In the usual scenario, when a patient presents withmeningitis or other acute manifestations of illness and an EVis suspected, serologic testing for non-coxsackievirus B,nonpoliovirus serotypes is not an option; in fact, not even
the coxsackievirus B immunoglobulin M method is widelyavailable outside of the research laboratory setting.
Antigen Detection
The absence of a widely shared antigen has hampered thedevelopment of immunoassays for the EVs much as it hasrestricted the use of serologic assays (42, 109, 110). Thegreatest success has been with assays limited to a particularsubgroup of EV serotypes, e.g., the coxsackievirus B sero-
types, which share a common antigen (109). Recent reports
of shared VP3-2C antigens among many EV serotypes (76)and of a monoclonal antibody that cross-reacts with the VP1capsid protein of multiple serotypes (113) are promising, butfurther testing is required to determine the clinical relevanceof those observations.
Nucleic Acid Hybridization
The earliest efforts at RNA-RNA hybridization for theEVs were designed to explore the genetic similarity amongseemingly distantly related serotypes (112). Although thepredicted homologies from those studies were somewhatinaccurate because of limitations in the available moleculartechnology, the conclusion that EVs share sequences acrossa broad range of serotypes has been borne out. Biologicalclues certainly supported that hypothesis: EVs share theirseasonality (70, 95), overlap in their clinical manifestations(22, 67), and are virtually identical by physicochemicalcriteria (91), a fact responsible for their classification as EVs.The EVs also have in common their fecal-oral route oftransmission (from which the name enteroviruses evolved)and their appearance by electron microscopy. Early andvery limited sequence comparisons confirmed genomic re-gions of great similarity among certain serotypes (43), as didheteroduplex mapping techniques using electron microscopy(30).The subsequent evolution of nucleic acid-based detection
systems for the EVs is a testimony to the ongoing emergenceof ever more advanced molecular technology and the avail-ability of this technology to the clinical microbiologist. Thelandmark technology that has facilitated the development oftoday's promising EV detection systems includes molecularcloning, transcription vectors, automated DNA synthesiz-ers, and the polymerase chain reaction (PCR).cDNA probes. Early hybridization studies using viral RNA
labeled during replication within cells (112) or cDNA labeleddirectly during reverse transcription (102) identified homol-ogies among a number of the EVs. With the advent ofmolecular cloning techniques, segments of several EVs weresuccessfully cloned into plasmid vectors, permitting thedevelopment of well-defined cDNA probes for the furtherstudy of genomic similarities among the serotypes. The firstsuch studies, utilizing cloned and well-characterized regionsof coxsackievirus B3 and poliovirus type 1 (48, 89), werereported in 1984. These investigations, and similar ones overthe ensuing 5 years (16, 21, 35, 47, 54, 73, 90, 100, 101, 114)(Table 3), provided valuable data regarding conserved se-quences well in advance of the actual sequencing of specificEV serotypes. Furthermore, this approach identified ge-nomic regions that were broadly shared across most, if notall, serotypes and could therefore become potential genericor pan-EV probes for clinical diagnosis. Probes derived fromthe 5' noncoding region of the EV genome and others whichincluded the proteinase- and polymerase-coding regions inthe 3' half of the genome appeared to be the most broadlycross-reactive (Table 3).Although promising in cross-hybridization studies with
target EVs grown in cell culture, the application of thesecDNA probes to the direct testing of clinical specimensproved to be problematic (Table 4). Initially, CSF recon-struction experiments were performed in which variousbiologic variables that occur in clinical specimens wereintroduced, along with virus, into normal CSF to determinethe impact of those variables on viral detection by hybrid-ization (90). The sensitivity of this assay, under conditionsoptimized for CSF, was between 102 and 105 50% tissue
158 ROTBART
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from

NUCLEIC ACID DETECTION SYSTEMS FOR ENTEROVIRUSES
ao orl=. CD U¢ CoD
U) CD Y
Uri
CD
r0
CDU)
~o0P+UCDP.
-
001-
cPz(D O
CO CD
-U)00
_Z
- 0CD
r+ 'mCD co
CD w
CD CD
*CD
U~~~~~~~F
°> a,>fDc
0
0 '0 'Is0 \.0 'I 'I \o 0£ 0 'I£ o 0 0 'I o0 C %O %O00 00 00 00 00 00 00 00 00 00 00 00 00 00 00 00 00 00'IO '0C 00 0~ 00 00 ~ c 11O 00 00 00 -4 -_.) UA LA P. .4- -
w -
ftI
Q1
Qz
Nrn
tTlC
_ 0w
CDlC
- 3
U US0 0.
CDU)CD
00 -00
CD
CD
C)
-i. 0C)
.4 o3
0.DCD
00xr _-to CD
0'0
0
'00 00D q
CDU- 3
CDCL
nTi nm
1--
L.A LA L.A
_il _
0I
'L0 'i
p D
5U)
-rA
F. U)10
O0. 0D 0
CD
0
cr 0
CD co
0..
w
PI
w P.
110
00 -eCD E "I
"O
.w
CD
n
C)
) C) C) C*zt t -0tw C)<
-1 k0T
C) ) ~C)w w t
aQ aQtT t-A
C) C) C)
Q % QAC W)-Jo.i
nIl C) C)\0g0%
nuit_nuln
LA (-A LA LA
m m m tTn il
. *'0*0 0~~r
CD CD CD 51 CD
P P.L 9
(.A- U)(A m
CD v
h co r00%
IC C
s1)
0 .
- 500_P)CD
qr E
FQ
W 0% W1 W k-
Q) Q C)Q-~~
oni
5 -5I
5 - 5O-C-i
oo~~~~~~0
tZw<~~~~~~~~~~~~0
0~ ~ ~-, DCCDC
CD~~~~~~~~~~C
o0
CD CD
CD) CD
VOL. 4, 1991
oo oo
D'D
CD
CD CD CD C
-sX co.~ -9
0o>
CDp
00n.0
CD
CD
0n
U
0
159
r
z(D
E_.U
0
CJQ
0
Z.
0.0.CD
0
:U
rQq
CDCDU
CDCD
U)00
U)a
C,,04gCDC)
CDtp m
I 51
0.CD0 CD
rIRD)
m3U)roCD
04
0CD
U0CD
(DCL
0.DUz
(AQ F)IoS. 0.
=io r0 0
0'0
0
VSS_cn
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
CLIN. MICROBIOL. REV.
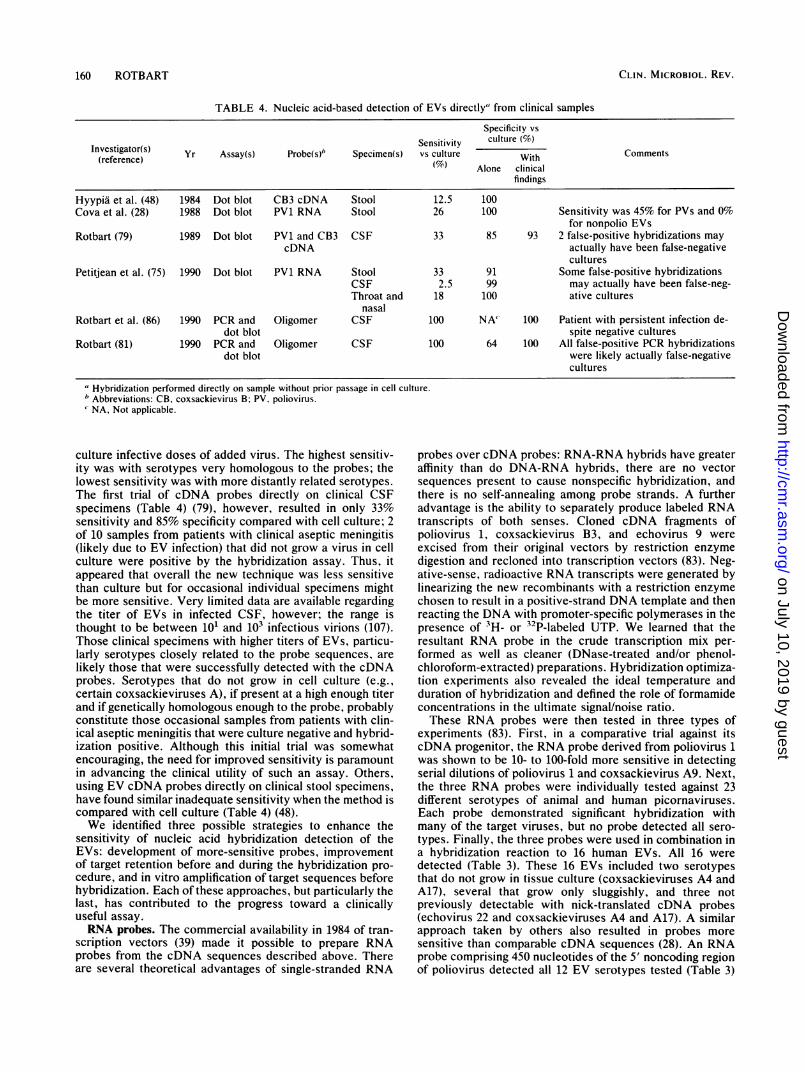
TABLE 4. Nucleic acid-based detection of EVs directly" from clinical samples
Specificity vs
Sensitivity culture (%)Investigator(s) Yr Assay(s) Probe(s)" Specimen(s) vs culture With Comments(reference)
Alone clinicalfindings
Hyypia et al. (48) 1984 Dot blot CB3 cDNA Stool 12.5 100Cova et al. (28) 1988 Dot blot PV1 RNA Stool 26 100 Sensitivity was 45% for PVs and 0%
for nonpolio EVsRotbart (79) 1989 Dot blot PV1 and CB3 CSF 33 85 93 2 false-positive hybridizations may
cDNA actually have been false-negativecultures
Petitjean et al. (75) 1990 Dot blot PV1 RNA Stool 33 91 Some false-positive hybridizationsCSF 2.5 99 may actually have been false-neg-Throat and 18 100 ative cultures
nasalRotbart et al. (86) 1990 PCR and Oligomer CSF 100 NA' 100 Patient with persistent infection de-
dot blot spite negative culturesRotbart (81) 1990 PCR and Oligomer CSF 100 64 100 All false-positive PCR hybridizations
dot blot were likely actually false-negativecultures
"Hybridization performed directly on sample without prior passage in cell culture.bAbbreviations: CB. coxsackievirus B; PV. poliovirus.NA, Not applicable.
culture infective doses of added virus. The highest sensitiv-ity was with serotypes very homologous to the probes; thelowest sensitivity was with more distantly related serotypes.The first trial of cDNA probes directly on clinical CSFspecimens (Table 4) (79), however, resulted in only 33%sensitivity and 85% specificity compared with cell culture; 2of 10 samples from patients with clinical aseptic meningitis(likely due to EV infection) that did not grow a virus in cellculture were positive by the hybridization assay. Thus, itappeared that overall the new technique was less sensitivethan culture but for occasional individual specimens mightbe more sensitive. Very limited data are available regardingthe titer of EVs in infected CSF, however; the range isthought to be between 10' and 103 infectious virions (107).Those clinical specimens with higher titers of EVs, particu-larly serotypes closely related to the probe sequences, arelikely those that were successfully detected with the cDNAprobes. Serotypes that do not grow in cell culture (e.g.,certain coxsackieviruses A), if present at a high enough titerand if genetically homologous enough to the probe, probablyconstitute those occasional samples from patients with clin-ical aseptic meningitis that were culture negative and hybrid-ization positive. Although this initial trial was somewhatencouraging, the need for improved sensitivity is paramountin advancing the clinical utility of such an assay. Others,using EV cDNA probes directly on clinical stool specimens,have found similar inadequate sensitivity when the method iscompared with cell culture (Table 4) (48).We identified three possible strategies to enhance the
sensitivity of nucleic acid hybridization detection of theEVs: development of more-sensitive probes, improvementof target retention before and during the hybridization pro-cedure, and in vitro amplification of target sequences beforehybridization. Each of these approaches, but particularly thelast, has contributed to the progress toward a clinicallyuseful assay.RNA probes. The commercial availability in 1984 of tran-
scription vectors (39) made it possible to prepare RNAprobes from the cDNA sequences described above. Thereare several theoretical advantages of single-stranded RNA
probes over cDNA probes: RNA-RNA hybrids have greateraffinity than do DNA-RNA hybrids, there are no vectorsequences present to cause nonspecific hybridization, andthere is no self-annealing among probe strands. A furtheradvantage is the ability to separately produce labeled RNAtranscripts of both senses. Cloned cDNA fragments ofpoliovirus 1, coxsackievirus B3, and echovirus 9 wereexcised from their original vectors by restriction enzymedigestion and recloned into transcription vectors (83). Neg-ative-sense, radioactive RNA transcripts were generated bylinearizing the new recombinants with a restriction enzymechosen to result in a positive-strand DNA template and thenreacting the DNA with promoter-specific polymerases in thepresence of 3H- or 32P-labeled UTP. We learned that theresultant RNA probe in the crude transcription mix per-formed as well as cleaner (DNase-treated and/or phenol-chloroform-extracted) preparations. Hybridization optimiza-tion experiments also revealed the ideal temperature andduration of hybridization and defined the role of formamideconcentrations in the ultimate signal/noise ratio.These RNA probes were then tested in three types of
experiments (83). First, in a comparative trial against itscDNA progenitor, the RNA probe derived from poliovirus 1was shown to be 10- to 100-fold more sensitive in detectingserial dilutions of poliovirus 1 and coxsackievirus A9. Next,the three RNA probes were individually tested against 23different serotypes of animal and human picornaviruses.Each probe demonstrated significant hybridization withmany of the target viruses, but no probe detected all sero-types. Finally, the three probes were used in combination ina hybridization reaction to 16 human EVs. All 16 weredetected (Table 3). These 16 EVs included two serotypesthat do not grow in tissue culture (coxsackieviruses A4 andA17), several that grow only sluggishly, and three notpreviously detectable with nick-translated cDNA probes(echovirus 22 and coxsackieviruses A4 and A17). A similarapproach taken by others also resulted in probes moresensitive than comparable cDNA sequences (28). An RNAprobe comprising 450 nucleotides of the 5' noncoding regionof poliovirus detected all 12 EV serotypes tested (Table 3)
160 ROTBART
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from

NUCLEIC ACID DETECTION SYSTEMS FOR ENTEROVIRUSES
(28), whereas an RNA probe derived from the coding regionfor the VP1 protein of poliovirus was poliovirus specific (28).To determine the analytic sensitivity of this assay, we
prepared and quantitated positive-sense RNA that was ab-solutely complementary to the coxsackievirus B3-derivednegative-sense RNA probe by using the same transcriptionvector construct but oppositely oriented primer and poly-merase. This positive-sense RNA was used as target to testthe probe. Under optimized solid-phase hybridization con-ditions, 10 pg of target RNA was shown to be the lower limitof sensitivity (88). The clinical sensitivity of hybridizationwith RNA probes, while slightly improved over the resultswith cDNA reagents, is still too low to be of practical use(Table 4) (28, 75). In one study, sensitivity (versus culture) ofan RNA probe derived from poliovirus was 2.5% for CSFspecimens, 18.1% for throat or nasal aspirates, and 33% forstool specimens (75).Improvement of target retention prior to and during hybrid-
ization. To determine the extent of loss of target EV RNAduring the course of our solid-phase hybridization assay, weseparately prepared 3H-labeled EV virions and 3H-labeledEV RNA. Added separately to CSF, target molecules couldbe monitored for retention through the hybridization proce-dure by scintillography (88). Free RNA added to CSF wassufficiently degraded by RNases within 15 s of contact withthe body fluid to result in loss of >90% of counts duringfiltration through all commercially available membranestested. Much of the remaining RNA was lost during subse-quent hybridization incubations and washes. RNase inhibi-tors were protective, but only if added to the CSF prior toaddition of the RNA. In contrast, radiolabeled virions sur-vived exposure to CSF and the hybridization and washprocedures, with >65% retention of counts on membranefilters. We determined that formaldehyde added to theCSF-virion specimen protects the RNA during the subse-quent heating step in which viral capsids are presumablyopened (allowing access of probes to target RNA duringhybridization).The lability of free RNA in CSF makes the preservation of
intact virions of utmost importance. Addition of formalde-hyde or another RNase inhibitor immediately after collectionof the specimen from the patient protects any RNA thatbecomes exposed by viral capsid opening during transport tothe laboratory as well as during the subsequent hybridizationprotocol. Unfortunately, free EV RNA or partially exposedRNA (e.g., defective particles) in the specimen collectedfrom the patient cannot be expected to remain viable forhybridization, regardless of technique. The preservation ofintact RNA within virions is also of paramount importancefor the enzymatic amplification approach discussed below.
Amplification of target sequences prior to hybridization.Despite optimization of hybridization methods, developmentof more-sensitive probes, and attempts at reducing targetloss during hybridization, clinical applicability was stillrestricted by the low titer of EVs in certain specimens. Inthis laboratory, we have employed two strategies for in-creasing the number of target RNA molecules available forhybridization with EV probes: biologic and enzymatic. Inthe biologic amplification approach, 102 50% tissue cultureinfective doses of EVs (below the level of sensitivity ofdirect hybridization) were inoculated onto LLC-MK2 tissueculture cells and allowed to incubate for various lengths oftime (87). Medium was decanted, and membrane filters wereapplied directly to the infected monolayer. The entire cellsheet was peeled off the culture dish onto the membrane,which was then fixed and hybridized with cDNA probes.
Although cytopathic effect was not noted until after 60 h ofincubation in cell culture, the same inoculum of virus wasdetected with this "monolayer blot" technique in 36 h byscintillography or in 42 h by autoradiography (87). Furtherenhancement of these methods may permit even brieferincubations in tissue culture before hybridization. We hadhoped that EV serotypes that do not produce cytopathiceffect in tissue culture might still replicate their RNA,allowing detection with monolayer blot hybridization. Ourattempts with several such coxsackievirus A serotypes,however, were unsuccessful, resulting in no detectable hy-bridization signals (unpublished data).The enzymatic amplification of single genes or short
sequences of DNA by repeated cycling of polymerase chainelongation reactions has recently been reported (72, 94).Critical to the success of this technique is the ability tospecifically bind (hybridize) short oligomeric sequences toregions of the target genome; these oligomers serve asprimers for the elongation of complementary strands and asprobes for detection of the amplified product. Our firstefforts in this area, therefore, were directed at demonstratingoligomeric hybridization to a variety of EV serotypes. Withthe availability of rapid synthetic methods for producing andcolor labeling oligomeric DNA sequences (92, 93), we de-signed EV oligomeric probes to test their spectrum ofreactivity and, in the hope that a nonisotopic system mightbe developed, to facilitate the ultimate adaptation to thediagnostic laboratory (85). Two 22-mer sequences werechosen on the basis of sequence information then availablefor the few EV serotypes that had been fully sequenced.These oligomers were labeled either with 32p in a standardkinase end-labeling reaction or with alkaline phosphataseadded during the synthetic process by means of a carbonchain linker arm chemically attached to one of the nucleo-tides. Cross-reactivity of the probes with multiple EV sero-types was observed (Table 3), confirming that short-se-quence probes with broad diagnostic potential can be chosenand that a colorimetric assay using this technology is feasible(85). Sensitivity of the nonisotopic probes, however, was10-fold lower than with the same oligomeric sequence la-beled with 32P and 100- to 1,000-fold lower than with RNAprobes. Much as cDNA (and therefore RNA) probes can bechosen to be either broadly cross-reactive or serotype spe-cific, serotype-specific oligomers with potential for use in acheckerboard-type analysis to determine the serotype of aparticular isolate can also be designed (Table 3) (4). It isunlikely, however, that the need to know the particularserotype of an infecting EV will arise often enough in clinicalpractice to require routine use of large panels of serotype-specific reagents. Thus, while the sensitivity of oligomericEV sequences used directly as probes is low, their potentialas primers for enzymatic amplification is great because of thebroad range of EV serotypes that do bind the oligomericmolecules.By using a computer-assisted analysis of the genomic
RNA sequences of the six EV serotypes that had been fullysequenced at the time (poliovirus types 1 to 3 and coxsack-ieviruses Bi, B3, and B4) (49, 51, 57, 99), we identified three20- to 25-base regions of absolute (100%) sequence conser-vation that define a 154-base segment within the 5' noncod-ing region of the viral genome (80, 82). The 5' end was
chosen because of its demonstrated conservation amongmany serotypes in the cDNA and RNA probe studies notedabove (Table 3). The two flanking sequences were chosen as
primers for PCR, and the middle sequence, which did notoverlap with either of the primers, was used as a probe.
VOL. 4, 1991 161
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from

CLIN. MICROBIOL. REV.
Since the selection of those oligomers, three additional EVshave been fully sequenced (coxsackieviruses A9 and A21and EV70) (19, 45, 98); all three are also 100% homologousto the primers and probe initially chosen. These threeoligomeric strands were synthesized as single-stranded DNAby using an automated synthesizer. The downstream primerand the probe were synthesized in the antisense orientationto genomic viral RNA, and the upstream primer was synthe-sized in the sense orientation to genomic RNA. Eleven EVserotypes were separately added to saline or CSF, and EVRNA was extracted and precipitated. A first strand of cDNAwas generated by reverse transcription with the downstreamprimer. PCR was then performed using both upstream anddownstream primers, with 25 repeated cycles of denatur-ation, annealing, and extension. Successful RNA amplifica-tion with the described primers was achieved for all 11 EVserotypes tested. Bands 154 bases long, a distance thatspanned both primers and the intervening sequence, wereseen after the first 25 PCR cycles for all EV serotypes exceptechoviruses 2 and 22, both of which were detectable follow-ing an additional 25 cycles. Hybridization with the 32p_labeled oligomeric probe confirmed the gel results. In con-trast, the same procedure with the same primers and probeapplied to herpes simplex virus, cytomegalovirus, and res-
piratory syncytial virus resulted neither in 154-base bands byelectrophoresis nor in positive hybridization (80, 82). Twoother laboratories have recently reported similar successusing different primer and probe combinations, also withinthe 5' noncoding region of the EV genome (20, 46). In one ofthose reports, a single pair of primers amplified the RNA ofeight of nine EV serotypes tested and six of six rhinovirusserotypes tested; discrimination between EVs and rhinovi-ruses was made in the subsequent hybridization step byusing genus-specific probes, although some cross-reactivityof the EV probe was seen with rhinovirus serotypes (46). Inthe second study, 40 of 41 EV serotypes were amplified byusing a single primer pair (46). Echovirus 22 is the only EVserotype thus far tested by PCR analysis that has consist-ently been difficult to amplify with primers that amplifymany other EV serotypes (20, 46, 82); this serotype is knownto be atypical of the EVs in many respects and, like EV72(hepatitis A), may require reclassification (26).The first two attempts at clinical application of this method
have been extremely promising (Table 4). EV RNA has beenshown to be persistently present in the CSF of a child withagammaglobulinemia, even during periods of virus culturenegativity (86). The patient, like others with agammaglobu-linemia and EV meningoencephalitis (64), had waxing andwaning symptoms of infection despite periods of virus cul-ture negativity. Negative cultures have been presumed to bedue to virus neutralization by aggressive gamma globulinreplacement therapy; however, this PCR application was thefirst definitive proof that virus does persist throughout bothculture-positive and culture-negative intervals. In a secondclinical application, and one most germane to the practicingphysician, CSF specimens collected from children undergo-ing lumbar puncture for suspected meningitis were studiedprospectively for EV infection by PCR (81). Of 12 patientswith the clinical diagnosis of aseptic meningitis, all were
positive for EV RNA by PCR; one child with the clinicaldiagnosis of viral encephalitis was also positive. Four chil-dren with bacterial meningitis and three with miscellaneousnoninfectious illnesses were all negative for EVs by PCR.That study found PCR to be more sensitive than and equallyspecific to concurrently performed cell cultures for thediagnosis of EV meningitis. Studies such as this will neces-
sitate calculation of true sensitivity and specificity on thebasis of a new "gold standard" that must include supple-mental data in addition to viral culture results (Table 4). Inthe absence of practical and reliable serologic tests orimmunoassays, clinical stigmata of EV infections may helpto corroborate PCR findings (81).
PATHOGENESIS
Much of what is assumed to be the pathogenesis of EVinfections has been derived from experiments done morethan 40 years ago involving poliovirus inoculations intononhuman primates (10, 11). The methodology at the timeincluded careful histologic observations and cell culture.Similar approaches as well as immunoassay techniques havemore recently been applied to the study of specific nonpolioEVs (56, 60). Nucleic acid probes used for in situ hybridiza-tion offer numerous advantages over immunoassay and cellculture for pathogenesis studies while preserving the tissuesfor concomitant histologic evaluation. In situ hybridizationallows detection of latent viral nucleic acid (where noreplication is occurring) and can localize viral genomeswithin cells (e.g., to nuclear versus cytoplasmic compart-ments). Furthermore, particularly in the case of the EVs,probes broadly reactive across many serotypes can detectviral infection in patients in whom the infecting serotype isunknown (in much the same way that such detection canoccur in body fluids, as noted above, by solid-phase hybrid-ization).
In Vitro Studies
The potential use of nucleic acid probes for EV in situhybridization has been demonstrated in a study of coxsack-ievirus B3 cell culture infection (84). Cytospin preparationsof infected and uninfected LLC-MK2 monkey kidney cellswere hybridized, using an in situ technique, with coxsack-ievirus B3-derived RNA probes for both sense and antisensetarget RNA. During productive infection, both RNA moi-eties were detected, in an approximate ratio of 40 sense EVRNA molecules to 1 antisense molecule, an observationconsistent with quantitation by nonhybridization methods(7). Uninfected cells demonstrated no hybridization witheither orientation of probe. The ability to detect viral RNAof both sense and antisense configurations may in itself haveimportant applications to the study of pathogenesis. There isevidence, for example, that the ability to generate theantisense molecule may influence the establishment of per-sistent infection by the EVs (see below) (17).
Animal Models Using Animal Picornaviruses
Nucleic acid-based studies of EV pathogenesis have beenperformed in animal model systems as well as on humantissue specimens. The earliest applications involved a modelof demyelinating central nervous system infection caused byTheiler's murine encephalomyelitis virus (TMEV), a natu-rally occurring murine picornavirus (59). This same patho-gen constituted an important early model of human paralyticpoliomyelitis, as the early phase of murine infection withTMEV results in an acute polioencephalomyelitis. It hassince been observed that mice that survive the early diseasedevelop a later-onset demyelinating encephalopathy thatresembles human multiple sclerosis (59). In situ hybridiza-tion experiments with cDNA probes in this model systemduring the early 1980s represent some of the earliest ad-
162 ROTBART
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from

NUCLEIC ACID DETECTION SYSTEMS FOR ENTEROVIRUSES
vances in the development of nucleic acid-based pathogen-esis research (14, 15, 96, 97). During the acute polioenceph-alomyelitis phase of infection, neurons distributed widely inthe brain were shown to be infected; white matter wasrelatively spared during this early phase (96). The clinicalsymptoms were demonstrated to be secondary to neuronallysis by virus rather than to hypoxia. Specific regions of thecentral nervous system were most affected, including thepyramidal layer of the hippocampus and the anterior horncells of the spinal cord. Other areas, such as the molecularlayer and dentate gyrus of the hippocampus and the entirecerebellum, were uninfected. In contrast, when survivinganimals were studied during the late demyelinating phase oftheir infection, viral RNA was consistently detected in glialcells of the white matter (15, 97). The investigators proposethat the pathogenesis of the late demyelinating phase of thisinfection involves persistent white-matter infection, thehost's inflammatory response, and the ability of circulatingantibodies to limit the further spread of virus. Most recently,RNA probes for antisense viral RNA have demonstratedthat a block at the level of synthesis of the viral antisenseRNA (a critical step in replication of EVs) may explain theability of TMEV to persist throughout the late (demyelinat-ing) phases of disease (17). Endothelial cells have also beenshown by in situ hybridization to be targets of TMEV centralnervous system infection, implying a possible additionalroute for EVs to cross the blood brain barrier (115).
Recently, in situ hybridization of TMEV has been used ina murine model of gestational EV infection (2). As notedabove, human infection with EVs during pregnancy has beenassociated with both teratogenesis and a syndrome of over-whelming neonatal sepsis, the former likely due to infectionearly in gestation and the latter due to infection near term orduring delivery. Pregnant mice were experimentally infectedwith TMEV in early, middle, and late gestation and sacri-ficed before delivery. Fetuses and placentas were culturedfor TMEV and studied by in situ hybridization using aTMEV-derived single-stranded RNA probe. Late-gestationinfections uniformly resulted in infection of the murineplacentas, but fetal infection never occurred (2). In situhybridization revealed a functional barrier to infection at thelevel of the spongiotrophoblast and labyrinth interface. Thelabyrinthal layer, that region of the placenta that lies closestto the fetus and in which maternal-fetal vascular exchangeoccurs, is entirely spared of TMEV RNA in late-gestationinfection. In contrast, early-gestation infection results inboth placental and fetal infection (3). In situ hybridization ofearly-gestation infection demonstrates dramatic virus infec-tion of the labyrinthal placenta and often massive fetalinfection. Tissue tropisms within the fetus could readily bedetermined and included heart, brain, liver, and lung, anal-ogous to the target tissues most affected in human gesta-tional EV infections. Serially timed sacrifices followingearly-gestation TMEV infection have revealed that giantcells near the lacunae containing maternal blood and sur-rounding the yolk cavity and embryo are the principal targetcells of infection (1). These giant cells are known to bephagocytic, and the hypothesis raised by this study is thatthe functional maturity of these cells determines whether theplacenta permits (early-gestation) or prevents (late-gesta-tion) TMEV infection of the fetus. Culture and in situhybridization of middle-gestation TMEV infection reveal anintermediate pattern of fetal infection and placental distribu-tion of viral RNA. A similar nucleic acid-based approach topathogenesis is currently being applied in the same model
system to study the effect of various exogenous factors onthe integrity of the placental-fetal barrier (unpublished data).
Using another murine picornavirus, encephalomyocarditisvirus (EMCV), investigators have developed a model ofchronic inflammatory myopathy (29). EMCV induces anacute infection in mice followed by resolution over severalweeks. Virus is culturable from muscle during the period ofhistologically documented inflammation; as the inflammationresolves, EMCV can no longer be recovered. In situ hybrid-ization localized the virus to the myocytes themselves,commonly in areas of inflammation. Occasionally EMCVRNA was detected where there was no inflammation, and,conversely, areas of inflammation existed where no viralRNA could be shown. EMCV could be detected by in situhybridization beyond the period of cultivability of virus andbeyond the time when extracted muscle tissue could beshown by dot blot hybridization to contain viral RNA.Similar viral persistence was observed in heart and brain,tissues known to be target organs for EMCV. Again, in situhybridization demonstrated viral RNA beyond the period ofviral cultivability.
Animal Models Using Human EV Serotypes
Several in situ hybridization model systems using humanEVs in animals have been reported. In the first, a cDNAprobe derived from coxsackievirus B3 was used to studymyocardial coxsackievirus infection in athymic mice (54).Virus was found to be distributed randomly and multifocallyin the hearts of infected animals, with evidence for cell-to-cell spread seen in the regions of histologic lesions; infectionwas transmural.
Coxsackievirus B3-induced myocarditis in mice was alsostudied by another group of investigators using in situ as wellas dot blot hybridization methods (114). By the formertechnique, viral RNA was detected with a biotin-labeledcDNA probe in muscle fibers but not in the lymphocytesparticipating in the inflammatory reaction. When coxsackie-virus Bi was used, murine skeletal-muscle myositis wasinduced and was also studied by the same two hybridizationtechniques (114). Once again, hybridization signal was con-fined to myocytes. In situ hybridization results were con-firmed by a dot blot assay on extracted RNA using ahybridization index method described below.
Coxsackievirus B3 has also been used to induce and studypancreatitis in a murine model (103). In situ hybridizationusing biotin or 32P-labeled cDNA probes derived fromcoxsackievirus B3 revealed viral RNA within necrotic acinarcells of the exocrine pancreas; cells within the islets ofLangerhans were never involved in the histologic inflamma-tion or shown to be infected by in situ hybridization. Theinitial inflammation and necrosis of the pancreas was fol-lowed by brief recovery and subsequent recrudescent in-flammation. This second phase of pancreatitis was notassociated with recovery of virus by cell culture or withdetectable RNA by in situ hybridization. Myocarditis alsodeveloped, according to histologic criteria, and coxsackievi-rus B3 could be recovered from heart tissue, but in situhybridization was not sensitive enough to detect viral RNAin those tissues (103).
Finally, in a primate animal model using a human EV,monkeys were intraspinally inoculated with virulent or at-tenuated strains of poliovirus type 1 (27). Virulent strainsproduced more-intense and more widely distributed inflam-matory lesions in the central nervous system than attenuatedstrains; in situ hybridization revealed poliovirus-killed neu-
VOL. 4, 1991 163
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from

164 ROTBART CLIN. MICROBIOL. REV.
rons. Small neural cells in the spinal cord were found tocontain viral RNA after infection with virulent strains butnot after infection with attenuated poliovirus infection.Quantitation of autoradiographic grains per cell, obtained byin situ hybridization, revealed no differences between strainsor between neurons from paralyzed versus clinically asymp-tomatic infected monkeys (27). These investigators reachedthe important conclusion that motor neuron death in polio-myelitis is the result of direct viral infection, multiplication,and lysis of neurons rather than of inflammation in responseto the infection as others had hypothesized.
Studies of Human Tissues
Nucleic acid hybridization techniques for the EVs havealso been applied to human tissues in an effort to makedisease associations and study pathogenesis (Table 5). Inone approach, RNA has been extracted from biopsy speci-mens of muscle tissues and studied by dot blot hybridizationusing a coxsackievirus B2-derived cDNA probe (5, 12, 13).Results were expressed as an index of virus-specific versuscellular-RNA-specific hybridization signal strengths, calcu-lated by densitometry quantitation of the autoradiogramsobtained separately with two probes, coxsackievirus B2 and,B-tubulin. The latter is said to be a marker for total cellularRNA, and therefore its use is a way to standardize theextraction procedure from specimen to specimen. Thesestudies associated EV infection with 9 of 17 patients withmyocarditis and dilated cardiomyopathy (12), 5 of 9 patientswith polymyositis or dermatomyositis (13), and 20 of 96patients with chronic fatigue syndrome (5). Unlike in situhybridization, this method cannot localize viral RNA to celltype or to compartments within cells (Table 5).EV detection by in situ hybridization in human tissues has
also been accomplished by a few investigators (Table 5). Thepaucity of these reports probably reflects the rarity ofobtaining human tissue specimens during acute infection, theunlikelihood of EV persistence in tissues beyond the acuteinfection, and/or the relative insensitivity of the techniquefor low levels of viral RNA, with the last factor probably aresult of both limitations in hybridization technology and thelability of free (nonencapsidated) intracellular RNA. A singlepatient with neurologic deterioration accompanying Staphy-lococcus aureus sepsis had a rise in antibody titer to cox-sackievirus B5 and in situ hybridization studies of brain atautopsy which were positive for EV RNA (41). The datawere presented in letter-to-the-editor format, so hybridiza-tion details were not provided except that the probe wasbiotin-labeled cDNA derived from coxsackievirus B4. Hy-bridization revealed signal in the meninges and perivascularareas; pictures demonstrating those findings were not pub-lished. Confounding the conclusion that the patient hadfulminant and fatal coxsackievirus B5 meningoencephalitisin addition to documented staphylococcal sepsis was theabsence of any abnormal CSF findings as well as negativeviral cultures and antibody tests on the CSF. The sameprobe was used to study autopsy heart specimens frompatients suspected, either because of serologic conversion oractual viral isolation, of having coxsackievirus infection atthe time of death (35). Six of 13 such patients had positivecardiac in situ hybridization assays, with probe distributed intwo different and seemingly mutually exclusive patterns,either perivascularly or within cardiac myocytes. In ourexperience, only a single patient (of approximately 10 stud-ied to date) with suspected EV myocarditis has been foundpositive by in situ hybridization using coxsackievirus-de-
r.0
-
40
a)0
*-o
40U,4)
-
0
U,
:30
.0
0000a)a)"0
-
0
[L
10
CO
.0
0z
..C
02
ut0
04z o =v-
00
la.00
Cl)
0
U.00
0.
0
0.
0.0
0.
6.
ay)
OC)
C001)
la)
0
O 00
o oo 001
-
0 0%- SO
r- t1 c u
0% '4 (A0 w
CZ, CZ C
a) a) a)
a) 00 O oa a)- 00 0' -
a)= a) a)a) ,00 0
z zz z
IIQ "Q Ql H
.0
co
a)0
+-,
co0
0
0.
Co
OD 4-. C6
Ct E
CX >= °=
0
0
.0 0 0 COCO00
.caO = =
Z00
z zzm
.0) O 0 c
00 0Oc
~~~~ b
e -
*3o~~~~~~~'.
c' 'Q O
0
0
N
10
0.5
a)m
c)
0
ea)
.0C
. .
.4-
.9._
D3
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from

NUCLEIC ACID DETECTION SYSTEMS FOR ENTEROVIRUSES
rived EV probes (unpublished data). In a third in situhybridization study of human tissues for EV infection,muscle biopsy specimens from 33 patients were blindlystudied for EV RNA (77). When an RNA probe derived fromTMEV was used, three of five specimens from patients withadult-onset dermatomyositis were positive; 15 patients withother types of inflammatory myopathy, 9 patients withnoninflammatory myopathy, and 4 patients with no muscledisease were all negative by in situ hybridization. Positivehybridization was mostly limited to macrophages within theinterstitial connective tissue of muscle bundles. Controlprobes, consisting of a combination of RNA probes derivedfrom poliovirus type 1 and coxsackievirus B3, producednegative results with all 33 specimens, leading the investiga-tors to suggest that a novel picornavirus, genomically moresimilar to TMEV than to human EV serotypes, may beetiologically responsible for some cases of dermatomyositis.The novelty of nucleic acid-based testing for tissue diag-
nosis of human EV infections necessarily engenders skepti-cism in interpreting results. This is true primarily becausethose cases in which these newer techniques are appliedusually involve patients in whom conventional virologictechniques have failed to establish EV causality. That failurecould be due to the timing of tissue sampling (perhapsbeyond the acute-infection stage, when viral isolation mighthave been expected), to infection by serotypes that do notreadily grow in cell culture, or to the inability of serology todefinitively prove causation of a particular syndrome by anagent (versus coincidental infection with the agent near thetime of disease onset). Controls are thus of utmost impor-tance in interpreting such studies. Table 5 summarizes thecontrols used in the hybridization studies of human tissuesdescribed above.
CONCLUSIONS
During the past 6 years, great strides have been madetoward the adaptation of nucleic acid-based detection sys-tems to clinical EV diseases. Inherent shortcomings inhybridization techniques, primarily due to inadequate sensi-tivity, make direct hybridization of clinical samples unfeasi-ble. Recently introduced nucleic acid amplification methodsappear to have the potential for overcoming the inadequaciesof direct hybridization. Critical to the preliminary success ofenzymatic amplification techniques for the EVs is substan-tial groundwork, including the demonstration of genomic-sequence conservation across a broad range of EV sero-types; determination of regions of greatest conservation;demonstration that oligomeric sequences could hybridize tomany EV serotypes as potential primers and probes; and,finally, the sequencing of enough EV serotypes from whichspecific primer and probe reagents could be constructed.
In situ hybridization studies using the same probe reagentsemployed for diagnostic testing promise to lend new insightsinto the pathogenesis of EV infections. Once again, partic-ularly with chronic or postinfectious diseases, sensitivitywill likely be the limiting variable. It is probably reasonableto assume that a PCR-based assay, or similar amplificationscheme, will someday soon be applied in situ, with the samedramatic impact on the field of viral pathogenesis that PCRhas had on the field of viral diagnostics.
ACKNOWLEDGMENTS
This work was supported by Public Health Service grantPO1AGNSO7347-03 from the National Institute on Aging and by the
Max Rotbart Memorial Fund at the University of Colorado HealthSciences Center.
REFERENCES1. Abzug, M. J., S. A. Magliato, H. A. Rotbart, and M. J. Levin.
1990. Program Abstr. 30th Intersci. Conf. Antimicrob. AgentsChemother., abstr. no. 1231.
2. Abzug, M. J., H. A. Rotbart, and M. J. Levin. 1989. Demon-stration of a barrier to transplacental passage of murine entero-viruses in late gestation. J. Infect. Dis. 159:761-765.
3. Abzug, M. J., H. A. Rotbart, S. A. Magliato, and M. J. Levin.1989. Program Abstr. 29th Intersci. Conf. Antimicrob. AgentsChemother., abstr. no. 910.
4. Alksnis, M., M. Lindberg, P. Stalhandske, and H. Hultberg.1989. Use of synthetic oligodeoxyribonucleotides for typespecific identification of coxsackie B viruses. Mol. Cell. Probes3:103-108.
5. Archard, L. C., N. E. Bowles, P. 0. Behan, E. J. Bell, and D.Doyle. 1988. Postviral fatigue syndrome: persistence of entero-virus RNA in muscle and elevated creatine kinase. J. R. Soc.Med. 81:326-331.
6. Assaad, F., and K. Ljungars-Esteves. 1984. World overview ofpoliomyelitis: regional patterns and trends. Rev. Infect. Dis.6:S302-S307.
7. Baltimore, D., and M. Girard. 1966. An intermediate in syn-thesis of poliovirus RNA. Proc. Natl. Acad. Sci. USA 56:741-748.
8. Barrett-Conner, E. 1985. Is insulin-dependent diabetes mellituscaused by coxsackievirus B infection? A review of the epide-miologic evidence. Rev. Infect. Dis. 7:207-215.
9. Bell, E. J., R. A. McCartney, D. Basquill, and A. K. R.Chaudhuri. 1986. ,u-Antibody capture ELISA for the rapiddiagnosis of enterovirus infections in patients with asepticmeningitis. 1986. J. Med. Virol. 19:213-217.
10. Bodian, D. 1954. Poliomyelitis: pathogenesis and histopathol-ogy, p. 479-518. In T. M. Rivers and F. L. Horsfall, Jr. (ed.),Viral and rickettsial infections of man, 3rd ed. Lippincott,Philadelphia.
11. Bodian, D. 1955. Emerging concept of poliomyelitis infection.Science 122:105-108.
12. Bowles, N. E., P. J. Richardson, E. G. J. Olsen, and L. C.Archard. 1986. Detection of coxsackievirus-B-virus-specificRNA sequences in myocardial biopsy samples from patientswith myocarditis and dilated cardiomyopathy. Lancet i:1120-1122.
13. Bowles, N. E., C. A. Sewry, V. Dubowitz, and L. C. Archard.1987. Dermatomyositis, polymyositis, and coxsackie-B virusinfection. Lancet i:1004-1007.
14. Brahic, M., A. T. Hasse, and E. Cash. 1984. Simultaneous insitu detection of viral RNA and antigens. Proc. Natl. Acad.Sci. USA 81:5445-5448.
15. Brahic, M., W. G. Stroop, and J. R. Baringer. 1981. Theiler'svirus persists in glial cells during demyelinating disease. Cell26:123-128.
16. Bruce, C., W. Al-Nakib, M. Forsyth, G. Stanway, and J. W.Almond. 1989. Detection of enteroviruses using cDNA andsynthetic oligonucleotide probes. J. Virol. Methods 25:233-240.
17. Cash, E., M. Chamorro, and M. Brahic. 1988. Minus-strandRNA synthesis in the spinal cords of mice persistently infectedwith Theiler's virus. J. Virol. 62:1824-1826.
18. Centers for Disease Control. 1987. Acute hemorrhagic conjunc-tivitis caused by coxsackievirus A24-Caribbean. Morbid. Mor-tal. Weekly Rep. 36:245-251.
19. Chang, K. H., P. Auvinen, T. Hyypiai, and G. Stanway. 1989.The nucleotide sequence of coxsackievirus A9: implicationsfor receptor binding and enterovirus classification. J. Gen.Virol. 70:3269-3280.
20. Chapman, N. M., S. Tracy, C. J. Gauntt, and U. Fortmueller.1990. Molecular detection and identification of enterovirusesusing enzymatic amplification and nucleic acid hybridization.J. Clin. Microbiol. 28:843-850.
21. Chatterjee, N. K., M. Kaehler, and R. Deibel. 1988. Detection
VOL. 4, 1991 165
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
CLIN. MICROBIOL. REV.
of enteroviruses using subgenomic probes of coxsackie virusB4 by hybridization. Diagn. Microbiol. Infect. Dis. 11:129-136.
22. Cherry, J. D. 1987. Enteroviruses: polioviruses (poliomyelitis),coxsackieviruses, echoviruses, and enteroviruses, p. 1729-1841. In R. D. Feigin and J. D. Cherry (ed.), Textbook ofpediatric infectious diseases, 2nd ed. The W. B. Saunders Co.,Philadelphia.
23. Chonmaitree, T., C. Ford, C. Sanders, and H. L. Lucia. 1988.Comparison of cell cultures for rapid isolation of enterovi-ruses. J. Clin. Microbiol. 26:2576-2580.
24. Chonmaitree, T., M. A. Menegus, and K. R. Powell. 1982. Theclinical relevance of CSF viral culture. A two-year experiencewith aseptic meningitis in Rochester, New York. J. Am. Med.Assoc. 247:1843-1847.
25. Cohen, J. I., J. R. Ticehurst, R. H. Purcell, A. Buckler-White,and B. M. Baroudy. 1987. Complete nucleotide sequence ofwild-type hepatitis A virus: comparison with different strainsof hepatitis A and other picornaviruses. J. Virol. 61:50-59.
26. Coller, B.-A. G., N. M. Chapman, M. A. Beck, M. A. Pal-lansch, C. J. Gauntt, and S. M. Tracy. 1990. Echovirus 22 is anatypical enterovirus. J. Virol. 64:2692-2701.
27. Couderc, T., C. Christodoulou, H. Kopecka, S. Marsden, L. F.Taffs, R. Crainic, and F. Horaud. 1989. Molecular pathogenesisof neural lesions induced by poliovirus type 1. J. Gen. Virol.70:2907-2918.
28. Cova, L., H. Kopecka, M. Aymard, and M. Girard. 1988. Useof cRNA probes for the detection of enteroviruses by molec-ular hybridization. J. Med. Virol. 24:11-18.
29. Cronin, M. E., L. A. Love, F. W. Miller, P. R. McClintock, andP. H. Plotz. 1988. The natural history of encephalomyocarditisvirus-induced myositis and myocarditis in mice: viral persist-ence demonstrated by in situ hybridization. J. Exp. Med.168:1639-1648.
30. Cumakov, I. M., G. Y. Lipskaya, and V. I. Agol. 1979.Comparative studies on the genomes of some picornaviruses:denaturation mapping of replicative form RNA and electronmicroscopy of heteroduplex RNA. Virology 92:259-270.
31. Dagan, R., and M. A. Menegus. 1986. A combination of fourcell types for rapid detection of enteroviruses in clinicalspecimens. J. Med. Virol. 19:219-228.
32. Dalakas, M. C., J. L. Sever, D. L. Madden, N. M. Papadopou-los, I. C. Shekarchi, P. Albrecht, and A. Krezlewicz. 1984. Latepostpoliomyelitis muscular atrophy: clinical, virologic, andimmunologic studies. Rev. Infect. Dis. 6:S562-S567.
33. Dalldorf, G., and G. M. Sickles. 1948. An unidentified, filtrableagent isolated from the feces of children with paralysis. Sci-ence 108:61-62.
34. Dorries, R., and V. Ter Meulen. 1983. Specificity of 1gMantibodies in acute human coxsackievirus B infections, ana-lysed by indirect solid phase enzyme immunoassay and immu-noblot technique. J. Gen. Virol. 64:159-167.
35. Easton, A. J., and R. P. Eglin. 1988. The detection of coxsack-ievirus RNA in cardiac tissue by in situ hybridization. J. Gen.Virol. 69:285-291.
36. Enders, J. F., T. H. Weller, and F. C. Robbins. 1949. Cultiva-tion of the Lansing strain of poliomyelitis virus in culture ofvarious human embryonic tissues. Science 109:85-99.
37. Fallis, R. J., and L. P. Weiner. 1982. Further studies in searchof a virus in amyotrophic lateral sclerosis, p. 355-360. In L. P.Rowland (ed.), Human motor neuron diseases. Raven Press,New York.
38. Gauntt, C. J., R. J. Gudvangen, Jr., Y. W. Brans, and A. E.Marlin. 1985. Coxsackie group B antibodies in the ventricularfluid of infants with severe anatomic defects in the centralnervous system. Pediatrics 76:68-78.
39. Green, M. R., T. Maniatis, and D. A. Melton. 1983. Human,B-globin pre-mRNA synthesized in vitro is accurately splicedin Xenopus oocyte nuclei. Cell 32:681-694.
40. Grist, N. R., and E. J. Bell. 1984. Paralytic poliomyelitis andnonpolio enteroviruses: studies in Scotland. Rev. Infect. Dis.6:S385-S386.
41. Hallam, N. F., R. P. Eglin, P. Holland, E. J. Bell, and M. V.Squier. 1986. Fatal coxsackie B meningoencephalitis diag-
nosed by serology and in-situ nucleic acid hybridisation. Lan-cet ii:1213-1214.
42. Herrmann, J. E., R. M. Hendry, and M. F. Collins. 1979.Factors involved in enzyme-linked immunoassay of virusesand evaluation of the method for identification of enterovi-ruses. J. Clin. Microbiol. 10:210-217.
43. Hewlett, M. J., and R. Z. Florkiewicz. 1980. Sequence ofpicornavirus RNAs containing a radioiodinated 5'-linked pep-tide reveals a conserved 5' sequence. Proc. Natl. Acad. Sci.USA 77:303-307.
44. Hogle, J. M., M. Chow, and D. J. Filman. 1985. Three-dimensional structure of poliovirus at 2.9 A resolution. Science229:1358-1365.
45. Hughes, P. J., C. North, P. D. Minor, and G. Stanway. 1989.The complete nucleotide sequence of coxsackievirus A21. J.Gen. Virol. 70:2943-2952.
46. Hyypia, T., P. Auvinen, and M. Maaronen. 1989. Polymerasechain reaction for human picornaviruses. J. Gen. Virol. 70:3261-3268.
47. Hyypia, T., M. Maaronen, P. Auvinen, P. Stalhandske, U.Pettersson, G. Stanway, P. Hughes, M. Ryan, J. Almond, M.Stenvik, and T. Hovi. 1987. Nucleic acid sequence relation-ships between enterovirus serotypes. Mol. Cell. Probes 1:169-176.
48. Hyypia, T., P. Stalhandske, R. Vainionpaa, and U. Pettersson.1984. Detection of enteroviruses by spot hybridization. J. Clin.Microbiol. 19:436-438.
49. lizuka, N., S. Kuge, and A. Nomoto. 1987. Complete nucleotidesequence of the genome of coxsackievirus Bi. Virology 156:64-73.
50. Jarvis, W. R., and G. Tucker. 1981. Echovirus type 7 menin-gitis in young children. Am. J. Dis. Child. 135:1009-1012.
51. Jenkins, O., J. D. Booth, P. D. Minor, and J. W. Almond. 1987.The complete nucleotide sequence of coxsackievirus B4 and itscomparison to other members of the picornaviridae. J. Gen.Virol. 68:1835-1848.
52. Johnson, R. T. 1984. Late progression of poliomyelitis paraly-sis: discussion of pathogenesis. Rev. Infect. Dis. 6:S568-S570.
53. Jubelt, B., A. K. Wilson, S. L. Ropka, P. L. Guidinger, andM. A. McKinlay. 1989. Clearance of a persistent human en-terovirus infection of the mouse central nervous system by theantiviral agent Disoxaril. J. Infect. Dis. 159:866-871.
54. Kandolf, R., D. Ameis, P. Kirschner, A. Canu, and P. H.Hofschneider. 1987. In situ detection of enteroviral genomes inmyocardial cells by nucleic acid hybridization: an approach tothe diagnosis of viral heart disease. Proc. Natl. Acad. Sci.USA 84:6272-6276.
55. Kaplan, M. H., S. W. Klein, J. McPhee, and R. G. Harper.1983. Group B coxsackievirus infections in infants youngerthan three months of age: a serious childhood illness. Rev.Infect. Dis. 5:1019-1032.
56. Leslie, K., R. Blay, C. Haisch, A. Lodge, A. Weller, and S.Huber. 1989. Clinical and experimental aspects of viral myo-carditis. Clin. Microbiol. Rev. 2:191-203.
57. Lindberg, A. M., P. 0. K. Stalhandski, and U. Pettersson. 1987.Genome of coxsackievirus B3. Virology 156:50-63.
58. Lipson, S. M., R. Walderman, P. Costello, and K. Szabo. 1988.Sensitivity of rhabdomyosarcoma and guinea pig embryo cellcultures to field isolates of difficult-to-cultivate group A cox-sackieviruses. J. Clin. Microbiol. 26:1298-1303.
59. Lipton, H. L. 1975. Theiler's virus infection in mice: anunusual biphasic disease process leading to demyelination.Infect. lmmun. 11:1147-1153.
60. Lipton, H. L., J. Kratochvil, P. Sethi, and M. C. Dal Canto.1984. Theiler's virus antigen detected in mouse spinal cord 21/2 years after infection. Neurology 34:1117.
61. Lyons, A. S., and R. J. Petracelli. 1978. Medicine: an illustratedhistory. Harry M. Abrams, Publisher, New York.
62. McCartney, R. A., J. E. Banatvala, and E. J. Bell. 1986.Routine use of ,u-antibody-capture ELISA for the serologicaldiagnosis of coxsackie B virus infections. J. Med. Virol.19:205-212.
63. McKinlay, M. A., J. A. Frank, Jr., D. P. Benziger, and B. A.
166 ROTBART
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from
NUCLEIC ACID DETECTION SYSTEMS FOR ENTEROVIRUSES
Steinberg. 1986. Use of WIN 51711 to prevent echovirus type9-induced paralysis in suckling mice. J. Infect. Dis. 154:676-681.
64. McKinney, R. E., S. L. Katz, and C. M. Wilfert. 1987. Chronicenteroviral meningoencephalitis in agammaglobulinemic pa-tients. Rev. Infect. Dis. 9:334-356.
65. McSharry, J. J., L. A. Caliguiri, and H. J. Eggers. 1979.Inhibition of uncoating of poliovirus by Arildone, a newantiviral drug. Virology 97:307-315.
66. Melnick, J. L. 1984. Enterovirus type 71 infections: a variedclinical pattern sometimes mimicking paralytic poliomyelitis.Rev. Infect. Dis. 6:S387-S390.
67. Melnick, J. L. 1990. Enteroviruses: polioviruses, coxsackievi-ruses, echoviruses, and newer enteroviruses, p. 549-605. InB. N. Fields and D. M. Knipe (ed.), Virology. Raven Press,New York.
68. Mirkovic, R. R., R. Kono, and M. Yin-Murphy. 1983. Entero-virus type 70: the etiologic agent of pandemic hemorrhagicconjunctivitis. Bull. W.H.O. 49:341-346.
69. Modlin, J. F. 1986. Perinatal echovirus infection: insights froma literature review of 61 cases of serious infection and 16outbreaks in nurseries. Rev. Infect. Dis. 8:918-926.
70. Moore, M. 1982. Enteroviral disease in the United States,1970-1979. J. Infect. Dis. 146:103-108.
71. Morens, D. M. 1978. Enteroviral disease in early infancy. J.Pediatr. 92:374-377.
72. Mullis, K. B., and F. A. Faloona. 1987. Specific synthesis ofDNA in vitro via a polymerase-catalyzed chain reaction.Methods Enzymol. 155:335-350.
73. Newman, C. L., J. Modlin, R. H. Yolken, and R. P. Viscidi.1989. Solution hybridization and enzyme immunoassay forbiotinylated DNA-RNA hybrids to detect enteroviral RNA incell culture. Mol. Cell. Probes 3:375-382.
74. Otto, M. J., M. P. Fox, M. J. Fancher, M. F. Kuhrt, G. D.Diana, and M. A. McKinlay. 1985. In vitro activity of WIN51711, a new broad-spectrum antipicornavirus drug. Antimi-crob. Agents Chemother. 27:883-886.
75. Petitjean, J., M. Quibriac, F. Freymuth, F. Fuchs, N. Laconche,M. Aymard, and H. Kopecka. 1990. Specific detection ofenteroviruses in clinical samples by molecular hybridizationusing poliovirus subgenomic riboprobes. J. Clin. Microbiol.28:307-311.
76. Romero, J., J. R. Putnak, and E. Wimmer. 1986. Abstr. no.967. Pediatr. Res. 20:319.
77. Rosenberg, N. L., H. A. Rotbart, M. J. Abzug, S. P. Ringel,and M. J. Levin. 1989. Evidence for a novel picornavirus inhuman dermatomyositis. Ann. Neurol. 26:204-209.
78. Rossmann, M. G., E. Arnold, J. W. Erickson, E. A. Franken-berger, J. P. Griffit, H.-J. Hecht, J. E. Johnson, G. Kamer, M.Luo, A. G. Mosser, R. R. Rueckert, B. Sherry, and G. Vriend.1985. Structure of a human common cold virus and functionalrelationship to other picornaviruses. Nature (London) 317:145-153.
79. Rotbart, H. A. 1989. Human enterovirus infections-molecularapproaches to diagnosis and pathogenesis, p. 243-264. In B. L.Semler and E. Ehrenfeld (ed.), Molecular aspects of picorna-virus infection and detection. American Society for Microbi-ology, Washington, D.C.
80. Rotbart, H. A. 1989. Abstr. no. 1119. Pediatr. Res. 25:189.81. Rotbart, H. A. 1990. Diagnosis of enteroviral meningitis with
the polymerase chain reaction. J. Pediatr. 117:85-89.82. Rotbart, H. A. 1990. Enzymatic RNA amplification of the
enteroviruses. J. Clin. Microbiol. 28:438-42.83. Rotbart, H. A., M. J. Abzug, and M. J. Levin. 1988. Develop-
ment and application of RNA probes for the study of picorna-viruses. Mol. Cell. Probes 2:65-73.
84. Rotbart, H. A., M. J. Abzug, R. S. Murray, N. L. Murphy, andM. J. Levin. 1988. Intracellular detection of sense and an-
tisense enteroviral RNA by in situ hybridization. J. Virol.Methods 22:295-301.
85. Rotbart, H. A., P. S. Eastman, J. L. Ruth, K. K. Hirata, andM. J. Levin. 1988. Nonisotopic oligomeric probes for thehuman enteroviruses. J. Clin. Microbiol. 26:2669-2671.
86. Rotbart, H. A., J. P. Kinsella, and R. L. Wasserman. 1990.Persistent enterovirus infection in culture-negative meningoen-cephalitis: demonstration by enzymatic RNA amplification. J.Infect. Dis. 161:787-791.
87. Rotbart, H. A., and M. J. Levin. 1989. Progress toward thedevelopment of a panenteroviral nucleic acid probe, p. 193-209. In F. C. Tenover (ed.), DNA probes for infectious dis-eases. CRC Press, Inc., Boca Raton, Fla.
88. Rotbart, H. A., M. J. Levin, N. L. Murphy, and M. J. Abzug.1987. RNA target loss during solid phase hybridization of bodyfluids-a quantitative study. Mol. Cell. Probes 1:347-358.
89. Rotbart, H. A., M. J. Levin, and L. P. Villarreal. 1984. Use ofsubgenomic poliovirus DNA hybridization probes to detect themajor subgroups of enteroviruses. J. Clin. Microbiol. 20:1105-1108.
90. Rotbart, H. A., M. J. Levin, L. P. Villarreal, S. Tracy, B. L.Semler, and E. Wimmer. 1985. Factors affecting the detectionof enteroviruses in cerebrospinal fluid with coxsackievirus B3and poliovirus type 1 cDNA probes. J. Clin. Microbiol. 22:220-224.
91. Rueckert, R. R. 1990. Picornaviruses and their replication, p.507-548. In B. N. Fields and D. M. Knipe (ed.), Virology.Raven Press, New York.
92. Ruth, J. L. 1984. Chemical synthesis of non-radioactively-labeled DNA hybridization probes. DNA 4:123-128.
93. Ruth, J. L., C. Morgan, and A. Pasko. 1985. Linker armnucleotide analogs useful in oligonucleotide synthesis. DNA4:93-97.
94. Saiki, R. K., S. Scharf, F. Faloona, K. B. Mullis, G. T. Horn,H. A. Erlich, and N. Arnheim. 1985. Enzymatic amplificationof 3-globin genomic sequences and restriction site analysis fordiagnosis of sickle cell anemia. Science 230:1350-1354.
95. Strikas, R. A., L. J. Anderson, and R. A. Parker. 1986.Temporal and geographic patterns of isolates of nonpolioenterovirus in the United States, 1970-1983. J. Infect. Dis.153:346-351.
96. Stroop, W. G., J. R. Baringer, and M. Brahic. 1981. Detectionof Theiler's virus RNA in mouse central nervous system by insitu hybridization. Lab. Invest. 45:504-509.
97. Stroop, W. G., M. Brahic, and J. R. Baringer. 1982. Detectionof tissue culture-adapted Theiler's virus RNA in spinal cordwhite matter cells throughout infection. Infect. Immun. 37:763-770.
98. Takeda, N. 1989. Complete nucleotide and amino acid se-
quences of enterovirus 70, p. 419-424. In K. Ishii, Y. Uchida,K. Miyamara, and S. Yamazaki (ed.), Acute hemorrhagicconjunctivitis etiology, epidemiology, and clinical manifesta-tions. University of Tokyo Press, Tokyo.
99. Toyoda, H., M. Kohara, Y. Kataoka, T. Suganuma, T. Omata,N. Imura, and A. Nomoto. 1984. Complete nucleotide se-
quences of all three poliovirus serotype genomes: implicationfor genetic relationship, gene function and antigenic determi-nants. J. Mol. Biol. 174:561-585.
100. Tracy, S. 1984. A comparison of the genomic homologiesamong the coxsackievirus B group: use of fragments of thecloned coxsackievirus B3 genome as probes. J. Gen. Virol.65:2167-2172.
101. Tracy, S. 1985. Comparison of genomic homologies in thecoxsackievirus B group by use of cDNA:RNA dot-blot hybrid-ization. J. Clin. Microbiol. 21:371-374.
102. Tracy, S., and R. A. Smith. 1981. A comparison of the genomesof polioviruses by cDNA:RNA hybridization. J. Gen. Virol.55:193-199.
103. Vuorinen, T., M. Kallajoki, T. Hyypia, and Vainionpiai. 1989.Coxsackievirus B3-induced acute pancreatitis: analysis of his-topathological and viral parameters in a mouse model. Br. J.Exp. Pathol. 70:395-403.
104. Wadia, N. H., S. M. Katrak, V. P. Misra, P. N. Wadia, K.Miyamura, K. Hashimoto, T. Ogino, T. Hikiju, and R. Kono.1983. Polio-like motor paralysis associated with acute hemor-rhagic conjunctivitis in an outbreak in 1981 in Bombay, India:clinical and serologic studies. J. Infect. Dis. 147:660-668.
105. Wildin, S., and T. Chonmaitree. 1987. The importance of the
VOL. 4, 1991 167
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from

CLIN. MICROBIOL. REV.
virology laboratory in the diagnosis and management of viralmeningitis. Am. J. Dis. Child. 141:454-457.
106. Wilfert, C. M., S. N. Lehrman, and S. L. Katz. 1983. Entero-viruses and meningitis. Pediatr. Infect. Dis. 2:333-341.
107. Wilfert, C. M., and J. Zeller. 1985. Enterovirus diagnosis, p.85-107. In L. de la Maza and E. M. Peterson (ed.), Medicalvirology IV: proceedings of the 1984 International Symposiumon Medical Virology. Lawrence Erlbaum Associates, London.
108. Woods, M. G., G. D. Diana, M. C. Rogge, M. J. Otto, F. J.Dutko, and M. A. McKinlay. 1989. In vitro and in vivo activi-ties of WIN 54954, a new broad-spectrum antipicornavirusdrug. Antimicrob. Agents Chemother. 33:2069-2074.
109. Yolken, R. H., and V. M. Torsch. 1980. Enzyme-linked im-munosorbent assay for detection and identification of cox-sackie B antigen in tissue cultures and clinical specimens. J.Med. Virol. 6:45-52.
110. Yolken, R. H., and V. M. Torsch. 1981. Enzyme-linked im-munosorbent assay for detection and identification of coxsack-ieviruses A. Infect. Immun. 31:742-750.
111. Yoon, J., M. Ausatin, T. Onodera, and A. L. Notkins. 1979.Virus-induced diabetes mellitus: isolation of a virus from thepancreas of a child with diabetic ketoacidosis. N. Engl. J. Med.300:1173-1179.
112. Young, N. A. 1973. Polioviruses, coxsackieviruses, and echo-viruses: comparison of the genomes by RNA hybridization. J.Virol. 11:832-839.
113. Yousef, G. E., I. N. Brown, and J. F. Mowbray. 1987. Deriva-tion and biochemical characterization of an enterovirus group-specific monoclonal antibody. Intervirology 28:163-170.
114. Zhang, H. Y., G. E. Yousef, N. E. Bowles, L. C. Archard, G. F.Mann, and J. F. Mowbray. 1988. Detection of enterovirusRNA in experimentally infected mice by molecular hybridisa-tion: specificity of subgenomic probes in quantitative slot blotand in situ hybridisation. J. Med. Virol. 26:375-386.
115. Zurbriggen, A., and R. S. Funjinami. 1988. Theiler's virusinfection in nude mice: viral RNA in vascular endothelial cells.J. Virol. 62:3589-3596.
168 ROTBART
on July 10, 2019 by guesthttp://cm
r.asm.org/
Dow
nloaded from