Nuclear Medical Imaging — Techniques and Challenges Nuclear ...
Upload
ravi-sarviCategory
view
1.663download
0description

USE OF NUCLEAR USE OF NUCLEAR IMAGING IN KIDNEY IMAGING IN KIDNEY
DISEASES : DISEASES : INDICATIONS AND INDICATIONS AND INTERPRETATIONSINTERPRETATIONS
20-5-1320-5-13

IsotopesIsotopes
Any given element may have many isotopesAny given element may have many isotopes All isotopes of a given element have the same All isotopes of a given element have the same
no of protons and differ only in the no of no of protons and differ only in the no of neutronsneutrons
Some of these isotopes have unstable nuclear Some of these isotopes have unstable nuclear configuration and seek greater stability by configuration and seek greater stability by decay/disintegration to a more stable formdecay/disintegration to a more stable form
Isotopes attempting to reach stability by Isotopes attempting to reach stability by emitting radiation are called emitting radiation are called radionuclides/radioisotopesradionuclides/radioisotopes

RadionuclidesRadionuclides
Photon Emitting(imaging) – TcPhoton Emitting(imaging) – Tc99m99m; ; MoMo9999;I;I123123;Ga;Ga6767;In;In113113;Kr;Kr8181;Th;Th201201
Positron Emitting(imaging) Positron Emitting(imaging) CC1111;N;N1313;O;O1515;F;F1818;Rb;Rb8282
Used for therapy- Used for therapy- PP3232;Sr;Sr8989;Y;Y9090;I;I131131;Sm;Sm153153

Radionuclides for Radionuclides for ImagingImaging
Desirable characteristics Desirable characteristics
Minimum particulate emissionMinimum particulate emission
Primary photon energy between 50-500 keVPrimary photon energy between 50-500 keV
Physical T1/2 > time reqd to prepare Physical T1/2 > time reqd to prepare materialmaterial
Effective T1/2 longer than examination timeEffective T1/2 longer than examination time
Low toxicityLow toxicity
Stability or near stability of the productStability or near stability of the product

TechnetiumTechnetium99m99m
Fulfills many criteria of ideal Fulfills many criteria of ideal radionuclideradionuclide
No particulate emissionNo particulate emission 6 hour half life6 hour half life A predominant (98%) 148KeV A predominant (98%) 148KeV
photon conversionphoton conversion Used in > 70% of nuclear imaging Used in > 70% of nuclear imaging
procedures in United Statesprocedures in United States

Nuclear medicineNuclear medicine is a branch of is a branch of medicinemedicine and and imagingimaging that uses that uses radionuclides and relies on the radionuclides and relies on the process of process of radioactive decayradioactive decay in the in the diagnosis and treatment of disease.diagnosis and treatment of disease.
Used in Nephro-Urology since Used in Nephro-Urology since 1960s1960s

Functional and anatomic informationFunctional and anatomic information
More organ / tissue specific c/t whole More organ / tissue specific c/t whole body scansbody scans
RADIOPHARMACEUTICALS = RADIOPHARMACEUTICALS = RADIONUCLIDES + PHARMACEUTICALRADIONUCLIDES + PHARMACEUTICAL

NUCLEAR NUCLEAR SCINTIGRAPHYSCINTIGRAPHY
TECHNIQUESTECHNIQUES 2D2D Scintigraphy - use of internal radionuclides - use of internal radionuclides
to create two-dimensionalto create two-dimensional images.images.
3D3D SPECT - tomographic technique using - tomographic technique using gamma camera data from many projections gamma camera data from many projections and reconstructed in different planesand reconstructed in different planes
HYBRID SCAN HYBRID SCAN - SPECT/CT and PET/CT- SPECT/CT and PET/CT

TOPICSTOPICS Renal ScintigraphyRenal Scintigraphy
ACEI renal scanACEI renal scan
Renal Transplant Scintigraphy
Radionuclide cystogramRadionuclide cystogram

Renal scintigraphy Renal scintigraphy
INDICATIONSINDICATIONS Renal perfusion and functionRenal perfusion and function Urinary Tract Obstruction (Furosemide renal Urinary Tract Obstruction (Furosemide renal
scan)scan) Reno-vascular HTN (Captopril renal scan)Reno-vascular HTN (Captopril renal scan) Infection (renal morphology Infection (renal morphology
scan)scan) Pre-surgical quantitation (nephrectomy) Pre-surgical quantitation (nephrectomy) Renal transplantationRenal transplantation Congenital anomalies/masses(renal morphology Congenital anomalies/masses(renal morphology
scan)scan)

Radiopharmaceutical Radiopharmaceutical AgentsAgents
Grouped into three categories: Grouped into three categories:
1.1. Those excreted by glomerular Those excreted by glomerular filtration,filtration,
1.1. Those excreted by tubular secretion, Those excreted by tubular secretion, andand
2.2. Those retained in the renal tubules for Those retained in the renal tubules for long periods long periods

Radiopharmaceutical Radiopharmaceutical AgentsAgents
Glomerular AgentsGlomerular Agents
Tc 99m DTPATc 99m DTPA
5151Cr-EDTACr-EDTA
I 125 IothalamateI 125 Iothalamate

Glomerular Filtrating AgentsGlomerular Filtrating AgentsTc-99m DTPA Tc-99m DTPA
(Diethylenetriamine pentaacetic (Diethylenetriamine pentaacetic acid)acid) COOH COOH N
N
N COOH
COOH
HOOC

Tc 99m DTPATc 99m DTPA
• Inulin clearance remains the gold Inulin clearance remains the gold standard to measure GFR, but it is standard to measure GFR, but it is expensive, time consuming, and requires a expensive, time consuming, and requires a steady-state plasma concentration and steady-state plasma concentration and accurate and timed urine collectionaccurate and timed urine collection
• 99m99mTc-DTPA is recommended agent is for Tc-DTPA is recommended agent is for GFR measurement.GFR measurement.
• 5- 10% plasma protein binding, so it tends 5- 10% plasma protein binding, so it tends to underestimate the GFR(insignificant)to underestimate the GFR(insignificant)

• Peak renal activity after 3 – 4 min.Peak renal activity after 3 – 4 min.• 90 % filtered within 4 hours.90 % filtered within 4 hours.• The extraction fraction of The extraction fraction of 99m99mTc-DTPA is Tc-DTPA is
approximately 20 per cent; for this approximately 20 per cent; for this reason, not useful for imaging , in reason, not useful for imaging , in patients with patients with impaired renal functionimpaired renal function..
• In such cases, agents with higher In such cases, agents with higher extraction efficiencies such as extraction efficiencies such as 99m99mTc-Tc-MAG3 more appropriate.MAG3 more appropriate.

5151Cr-EDTA, which may provide more Cr-EDTA, which may provide more accurate values for GFR, but accurate values for GFR, but cannot cannot be used for imaging.be used for imaging.

Tubular secreting agents:Tubular secreting agents:
I131/I123 OIHI131/I123 OIH Tc99m MAG3Tc99m MAG3 Tc99m ECTc99m EC
Proximal convoluted tubules

p-Aminohippuric acid (PAH) is the p-Aminohippuric acid (PAH) is the gold standard for the measurement gold standard for the measurement of ERPF. of ERPF.
However, it is not well suited for However, it is not well suited for routine studies.routine studies.

I-131/I-123 I-131/I-123 OrthoiodohippurateOrthoiodohippurate
-C-NH-CH2-COOH
O
I
Chemical structure similar to the Paraaminohippuric acid

I-131 OIHI-131 OIH
Secreted by tubules – 80% & Secreted by tubules – 80% & glomerular filtration - 20%glomerular filtration - 20%
Chemically & pharmacokinetically Chemically & pharmacokinetically similar to PAHsimilar to PAH
Plasma protein binding – 70%Plasma protein binding – 70%
Cortical peak time = 3-5 minCortical peak time = 3-5 min
Radiation absorbed dose to Radiation absorbed dose to bladder= 0.74 rad/mCibladder= 0.74 rad/mCi

The main disadvantages of The main disadvantages of 131131I-OIH I-OIH are the suboptimal imaging are the suboptimal imaging characteristics of characteristics of 131131I.I.
123123I-OIH has better imaging qualities, I-OIH has better imaging qualities, but but 123123I is more expensive and less I is more expensive and less available.available.

TcTc99m99m MAG3 MAG3(Mercaptoacetyl triglycine)(Mercaptoacetyl triglycine)
S O N
Tc
N N
O
O
CH2-COO

TcTc99m99m MAG3 MAG3
70 – 90 % PROTEIN BINDING70 – 90 % PROTEIN BINDING 89% TUBULAR SECRETION89% TUBULAR SECRETION 11% 11% GLOMERULARGLOMERULAR FILTRATION FILTRATION Extraction fraction of 40-50%.Extraction fraction of 40-50%. Provides a high target-to-background Provides a high target-to-background
ratio, good image quality, and more ratio, good image quality, and more accurate numerical values, particularly accurate numerical values, particularly when the kidney function is low or when the kidney function is low or immature immature
5 TO 10 mCi i.v. ( ADULTS) 5 TO 10 mCi i.v. ( ADULTS)

TcTc99m99m L,L-EC L,L-EC(Ethylene dicysteine)(Ethylene dicysteine)
N NN N
-ooc coo--ooc coo-
TcTc
S SS S
Exists in 4 different forms D,D-EC; L,L-EC; D,L-EC & L,D-EC

EC:EC:
Metabolite of the L,L-ECD(ethylene Metabolite of the L,L-ECD(ethylene cystine dimer) with cortical uptakecystine dimer) with cortical uptake
Secretion in proximal convoluted Secretion in proximal convoluted tubulestubules
Plasma protein binding is 50%Plasma protein binding is 50% Exact excretion mechanism is not Exact excretion mechanism is not
knownknown Clearance is 69-85% of OIHClearance is 69-85% of OIH

Cortical Binding Agents:Cortical Binding Agents:
Tc99m DMSATc99m DMSA
Tc99m GHATc99m GHA

Tc-99m DMSA Tc-99m DMSA (Dimercaptosuccinic Acid)(Dimercaptosuccinic Acid)
H
HS COOH
HS COOH
H

Cortical agentsCortical agents TcTc99m99m DMSA- DMSA-PYELONEPHRITIS, INFARCTS, SCARS, PYELONEPHRITIS, INFARCTS, SCARS,
ANOMALIESANOMALIES 75% protien binding in 6 hrs75% protien binding in 6 hrs 5- 20 % excretion 2 hrs5- 20 % excretion 2 hrs 37% excretion in 24 hrs37% excretion in 24 hrs 40-50% cortical localisation40-50% cortical localisation Maximum activity at 3-6 hrs Maximum activity at 3-6 hrs 2 TO 5 mCi i.v.2 TO 5 mCi i.v. Images at 2 – 4 hrsImages at 2 – 4 hrs

Importantly, acute infection can Importantly, acute infection can produce abnormalities in the scan; produce abnormalities in the scan; and if the test is being performed to and if the test is being performed to evaluate for cortical scarring, it evaluate for cortical scarring, it should be done at least 3 months should be done at least 3 months after an acute infection ( Rosenberg after an acute infection ( Rosenberg et al, 1992 ). et al, 1992 ).

Tc 99m GHATc 99m GHA(Glucoheptonate)(Glucoheptonate)
O O O
C Tc C
CH CH O O (CHOH)4
CH2OH CH2OH
(CHOH)4
OO

CONTD..CONTD..
Tc 99m GHTc 99m GH It is both filtered by the glomerulus and It is both filtered by the glomerulus and
bound by the tubules.bound by the tubules. Glomerular filtration 80-90%Glomerular filtration 80-90% Tubular secretion 10-20%Tubular secretion 10-20% 25-40% in 1 hr & 70% in 24 hrs in urine25-40% in 1 hr & 70% in 24 hrs in urine 15% bound to PCT15% bound to PCT EARLY DYNAMIC FUNCTIONAL imagingEARLY DYNAMIC FUNCTIONAL imaging
DELAYED CORTICAL imagingDELAYED CORTICAL imaging 10-15 mCi10-15 mCi


Choosing Renal Choosing Renal RadiotracersRadiotracers
PerfusionPerfusion MAG3, DTPA, GHAMAG3, DTPA, GHA
MorphologyMorphology DMSA, GHA DMSA, GHA
Obstruction Obstruction MAG3, DTPA, OIHMAG3, DTPA, OIH
GFR quantitationGFR quantitation I-125 I-125 iothalamate, iothalamate,
Cr-51 EDTA, DTPACr-51 EDTA, DTPA
ERPF quantitationERPF quantitation MAG3, OIH MAG3, OIH
Clin. Question Agent

Basic Renal ScanBasic Renal Scan
ProcedureProcedure

Basic Renal ScintigraphyBasic Renal Scintigraphy
PatientPatient PreparationPreparation
Patient must be well hydratedPatient must be well hydrated Give 5-10 ml/kg water (2-4 cups) Give 5-10 ml/kg water (2-4 cups)
30-60 min. pre-injection30-60 min. pre-injection Can measure U - specific gravity Can measure U - specific gravity
(<1.015)(<1.015) Void before injectionVoid before injection Void @ end of studyVoid @ end of study
Int’l Consens. Comm.Int’l Consens. Comm.Semin NM ‘99:146-159Semin NM ‘99:146-159

Basic Renal ScintigraphyBasic Renal Scintigraphy AcquisitionAcquisition
Supine position preferredSupine position preferred Flow (angiogram) : 2-3 sec / fr x 1 Flow (angiogram) : 2-3 sec / fr x 1
minmin Dynamic: 15-30 sec / frame x 20-Dynamic: 15-30 sec / frame x 20-
30 min30 min (display @ 1-3 (display @ 1-3
min/frame)min/frame)

Basic Renal ScintigraphyBasic Renal Scintigraphy Acquisition Acquisition (cont’d)(cont’d)
Obtain a 30-60 sec. image over injection Obtain a 30-60 sec. image over injection site @ end of study site @ end of study if infiltration >0.5% dose if infiltration >0.5% dose do not report do not report
clearanceclearance
Obtain post-void supine image of kidneys Obtain post-void supine image of kidneys @ end of study@ end of study
Taylor, SeminNM 4/99:102-127

International Consensus Committee International Consensus Committee Recommendations for Basic Recommendations for Basic
RenogramRenogram
Tracer: MAG3, (DTPA)Tracer: MAG3, (DTPA) Dose: 2 - 5 mCi adult, minimum 0.5 mCi pedsDose: 2 - 5 mCi adult, minimum 0.5 mCi peds
Pt. position: supine (motion, depth issues)Pt. position: supine (motion, depth issues) Include bladder, heartInclude bladder, heart
Collimator: LEAPCollimator: LEAP Image over injection siteImage over injection site
Int’l Consens. Comm.Int’l Consens. Comm.Semin NM ‘99:146-159Semin NM ‘99:146-159

Radionuclide Renal Radionuclide Renal EvaluationEvaluation
Functional Imaging(visual Functional Imaging(visual assessment of perfusion and assessment of perfusion and function)function)
Renography (time activity curve Renography (time activity curve representative of renal function)representative of renal function)
Quantification of renal function(GFR Quantification of renal function(GFR & ERPF)& ERPF)
Anatomic imaging( cortical imaging)Anatomic imaging( cortical imaging)

Functional ImagingFunctional Imaging Perfusion imaging Perfusion imaging –– Evaluation of renal blood flow and Evaluation of renal blood flow and
function of native kidneys – posterior function of native kidneys – posterior projection ; transplanted kidneys – projection ; transplanted kidneys – anterior projectionanterior projection
10-20mCi of radiopharmaceutical injected 10-20mCi of radiopharmaceutical injected iv in antecubital vein.iv in antecubital vein.
Imaging renal perfusion is usually begun Imaging renal perfusion is usually begun as soon as bolus is seen in abd. Aortaas soon as bolus is seen in abd. Aorta
Subsequent images are taken every 1-5 Subsequent images are taken every 1-5 secssecs

In normal renal blood flowIn normal renal blood flow
By 3 sec aorta is fully visualized.By 3 sec aorta is fully visualized.
By 5-6 sec, both kidneys are seen.By 5-6 sec, both kidneys are seen.
Maximal kidney activity is reached Maximal kidney activity is reached in 30-60 sec.in 30-60 sec.

DTPA normalDTPA normal

Renal functional imagingRenal functional imaging
At the end of perfusion sequence , At the end of perfusion sequence , imaging for function begins.imaging for function begins.
Dynamic or sequential static; 3-5 Dynamic or sequential static; 3-5 min Tcmin Tc99m 99m DTPA or MAG3 are then DTPA or MAG3 are then obtained over 20-30 mins.obtained over 20-30 mins.
Evaluation is similar to an IVP with – Evaluation is similar to an IVP with – anatomy, position, symmetry and anatomy, position, symmetry and adequacy of function & collecting adequacy of function & collecting system patency. system patency.

With TcWith Tc99m99m MAG3 maximal MAG3 maximal parenchymal activity is seen at 3-5 parenchymal activity is seen at 3-5 min min
Activity in collecting system and Activity in collecting system and bladder by 4-8 mins.bladder by 4-8 mins.

DTPA normalDTPA normal

RenographyRenography
A Time Activity CurveA Time Activity Curve
Graphic representation of uptake Graphic representation of uptake and excretion of and excretion of radiopharmaceuticalradiopharmaceutical
Information is displayed from time of Information is displayed from time of injection to abt 20-30 mins injection to abt 20-30 mins

Renogram PhasesRenogram Phases FLOW / VASCULAR FLOW / VASCULAR
PHASE PHASE
(RADIONUCLETIDE (RADIONUCLETIDE
ANGIOGRAM)ANGIOGRAM)
• Last for 30-60 sec.Last for 30-60 sec.
• Max activity 4-6 Max activity 4-6
secs after peak secs after peak
aortic activityaortic activity
FUNCTIONAL PHASE FUNCTIONAL PHASE
( 30 MIN )( 30 MIN )
II.II. Parenchymal Parenchymal
phase(uptakephase(uptake))
• Max activity 3to 5 minMax activity 3to 5 min
• UPTAKE AT 2 TO 3 MIN UPTAKE AT 2 TO 3 MIN
FOR SPLIT FUNCTIONFOR SPLIT FUNCTION
III.III. Washout (excretory) phaseWashout (excretory) phase
no activity after 30 minno activity after 30 min

RENOGRAM PHASES

Data obtained from Data obtained from renogramrenogram
Time to peak cortical activity- 3-5Time to peak cortical activity- 3-5 min min
Half-time excretion- time for half of Half-time excretion- time for half of peak activity to be cleared from kidney. peak activity to be cleared from kidney. N – 8-12 minsN – 8-12 mins
Cortical activity at 20 min/ peak Cortical activity at 20 min/ peak activity : activity :
< 0.30 on MAG3 renogram. < 0.30 on MAG3 renogram.

RELATIVE/SPLIT RELATIVE/SPLIT FUNCTIONFUNCTION
Contribution of each kidney to the Contribution of each kidney to the total functiontotal function
net cts in Lt ROInet cts in Lt ROI % Lt kid% Lt kid = --------------------------------------- x 100% = --------------------------------------- x 100%
net cts Lt + net cts Rt ROInet cts Lt + net cts Rt ROI
ROI: Region of interestROI: Region of interestNormalNormal 50/50 - 56/44 50/50 - 56/44
BorderlineBorderline 57/43 - 59/4157/43 - 59/41
AbnormalAbnormal > 60/40> 60/40 Taylor, SeminNM Apr 99

Relative (split) functionRelative (split) functionROI’sROI’s



Quantitation of Renal Quantitation of Renal Function Function
GFR & ERPF measurementGFR & ERPF measurement Two methods :Two methods : Plasma sample based clearances Plasma sample based clearances : : The amt of activity remaining in blood at The amt of activity remaining in blood at
prefixed times is a measurement of activity not prefixed times is a measurement of activity not yet cleared – indirect measure of activity yet cleared – indirect measure of activity already cleared.already cleared.
More accurate ,but requires determination of More accurate ,but requires determination of pharmaceuticals levels in plasma and some pharmaceuticals levels in plasma and some times in urine.times in urine.

Camera based clearances Camera based clearances : : Counts are obtained from syringe Counts are obtained from syringe
before inj. & subsequently over before inj. & subsequently over kidneys after injection.kidneys after injection.
No blood and urine collection.No blood and urine collection. Sufficiently reliable method.Sufficiently reliable method.

Anatomic(Cortical) ImagingAnatomic(Cortical) Imaging(Tc99m DMSA or GH )(Tc99m DMSA or GH )
Images obtained after 2 to 4 hrs of injectionImages obtained after 2 to 4 hrs of injection Posterior/ right post. Oblique/ left post. Posterior/ right post. Oblique/ left post.
ObliqueOblique
NORMAL FINDINGSNORMAL FINDINGS Smooth contour with Homogeneous Smooth contour with Homogeneous
activityactivity Less uptake in medullaLess uptake in medulla No activity in PCS No activity in PCS

Diuretic (Furosemide) Renal Diuretic (Furosemide) Renal ScanScan
Obstructive uropathyObstructive uropathy (hydronephrosis, (hydronephrosis, hydroureter) may lead to hydroureter) may lead to obstructive obstructive nephropathynephropathy (loss of renal function) (loss of renal function)Indications:Indications:
Evaluate functional significance of hydronephrosisEvaluate functional significance of hydronephrosis Determine need for surgeryDetermine need for surgery
obstructive hydronephrosis - surgical Rxobstructive hydronephrosis - surgical Rx non-obstructive hydronephrosis - medical Rx/ non-obstructive hydronephrosis - medical Rx/
follow upfollow up Monitor effect of therapyMonitor effect of therapy

PRINCIPLEPRINCIPLE
Hydronephrosis - tracer pooling in Hydronephrosis - tracer pooling in dilated renal pelvisdilated renal pelvis
Furesemide induces increased urine flowFuresemide induces increased urine flow If obstructed >>> will not wash outIf obstructed >>> will not wash out If dilated, non-obstructed >>> will wash If dilated, non-obstructed >>> will wash
out out Can quantitate rate of washout (Can quantitate rate of washout (TT1/21/2))

PROTOCOLPROTOCOL
Oral hydration prior to studyOral hydration prior to study NS @ 15ml/kg over 30 min 15 min prior to NS @ 15ml/kg over 30 min 15 min prior to
injection & continued in study @ 200ml/kg/24 injection & continued in study @ 200ml/kg/24 hrhr
Bladder catheterization is required in childrenBladder catheterization is required in children Tc 99m MAG3 – agent of choice in children Tc 99m MAG3 – agent of choice in children
with limited functionwith limited function high target-to-background ratio, good image high target-to-background ratio, good image
quality, and more accurate numerical valuesquality, and more accurate numerical values

PROTOCOLPROTOCOL Pre requisite – residual function to Pre requisite – residual function to
respondrespond Diuretic given Diuretic given ( infants- 1mg/kg, ( infants- 1mg/kg,
children 0.5 mg/kg, 40 mg adults ) children 0.5 mg/kg, 40 mg adults ) 20-30 min 20-30 min after radiotracer injectionafter radiotracer injection
Imaging for 20 – 30 minutes, post Imaging for 20 – 30 minutes, post micturition imagemicturition image
Functional images, renogram Functional images, renogram time/activity curve( before & after ), time/activity curve( before & after ), wash out half time calculated wash out half time calculated
symmetric uptake and good washout symmetric uptake and good washout is by definition not obstructedis by definition not obstructed

Diuretic Renal ScanDiuretic Renal Scan WashoutWashout
(diuretic response)(diuretic response)
TT1/21/2
time required for 50% tracer to leave time required for 50% tracer to leave the dilated unit the dilated unit
i.e. time required for activity to fall i.e. time required for activity to fall
to 50% of peakto 50% of peak

TT1/21/2
Normal Normal < 10 min< 10 min Obstructed Obstructed > 20 min> 20 min Indeterminate Indeterminate 10 - 20 min10 - 20 min
Best to obtain own normals for each Best to obtain own normals for each institution, depending on protocol usedinstitution, depending on protocol used

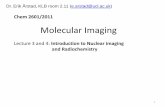
Showing non-obstructive hydronephrosis of the left kidney, The arrow indicating a brisk response to intravenous diuretic.
Scintigraphic evaluation of Hydronephrosis

Scintigraphic evaluation of Hydronephrosis
Showing obstructive hydronephrosis of the right kidney, The arrow indicating a no response to intravenous diuretic.

““F minus 15” F minus 15” Diuretic Diuretic RenogramRenogram
Furosemide (Lasix) injected 15 min Furosemide (Lasix) injected 15 min before before radiopharmaceuticalradiopharmaceutical
Rationale: kidney in maximal diuresis,Rationale: kidney in maximal diuresis,under maximal stressunder maximal stress
Some equivocals will become clearly Some equivocals will become clearly positive, some clearly negativepositive, some clearly negative
English, Br JUrol 1987:10-14Upsdell, Br JUrol 1992:126-132

Captopril Renal ScanCaptopril Renal Scan (ACEI Renography) (ACEI Renography)
Evaluation of Evaluation of Renovascular Renovascular HypertensionHypertension

Captopril Renal ScanCaptopril Renal Scan (ACEI Renography) (ACEI Renography)
Renovascular Disease Renovascular Disease
Renal artery stenosis (RAS)Renal artery stenosis (RAS)
Ischemic nephropathyIschemic nephropathy
Renovascular hypertension (RVH)Renovascular hypertension (RVH)
RAS RAS RVH RVH

Renin-Angiotensin Renin-Angiotensin SystemSystem
RAS
CaptoprilCaptopril
Angiotensinogen
Angiotensin I
Angiotensin II
Aldosterone Vasoconstriction
HTN
Renin
ACE

Effect of RAS on GFREffect of RAS on GFR

Renovascular Renovascular HypertensionHypertension
PrevalencePrevalence <1% unselected population with HTN<1% unselected population with HTN
Clinical featuresClinical features Abrupt onset HTN in child, adult < 30 or > Abrupt onset HTN in child, adult < 30 or >
60y60y Severe HTN resistant to medical RxSevere HTN resistant to medical Rx Unexplained or post-ACEI impairment in Unexplained or post-ACEI impairment in
ren fctren fct HTN + abdominal bruitsHTN + abdominal bruits
If these present - moderate risk of RVH (20-If these present - moderate risk of RVH (20-30%)30%)

Diagnosis of RASDiagnosis of RAS
Gold standard: angiographyGold standard: angiography Initial non-invasive tests:Initial non-invasive tests:
ACEI renographyACEI renography Duplex sonographyDuplex sonography
Other tests: Other tests: MRA - insensitive for distal / segmental MRA - insensitive for distal / segmental
RASRAS Renal vein renin levelsRenal vein renin levels

Captopril Renal ScanMAG 3Captopril Renal ScanMAG 3
Tc 99m MAG 3 = gold standardTc 99m MAG 3 = gold standard
Stop ACE inhibitors 48 hrs prior and no Stop ACE inhibitors 48 hrs prior and no solid food before 4 hrssolid food before 4 hrs
Before procedure, orally fluid – 10 ml/kgBefore procedure, orally fluid – 10 ml/kg
Hydration continued i.v. 4ml/ minHydration continued i.v. 4ml/ min
Baseline BP & PR recorded→ captopril 50 Baseline BP & PR recorded→ captopril 50 mgmg

Protocol: Protocol: 1 day 1 day vsvs. 2 day test. 2 day test 1 day test: 1 day test: baseline scan (1-2 mCi) baseline scan (1-2 mCi)
followed by followed by post-Capto post-Capto scan (8-10 mCi)scan (8-10 mCi)
2 day test: 2 day test: post-Capto scan, post-Capto scan, only if abnormal >> only if abnormal >>
baseline baseline

Abnormal captopril Abnormal captopril RenographyRenography
Delayed time to maximal activity >11 Delayed time to maximal activity >11 minutes(normal -5min)minutes(normal -5min)
Significant asymmetry of peak activity of Significant asymmetry of peak activity of each kidneyeach kidney
Marked cortical retention of radionuclide Marked cortical retention of radionuclide A marked decrease in the GFR of the A marked decrease in the GFR of the
ipsilateral kidney. ipsilateral kidney. 20-minute counts /peak counts [N <0.3 ], 20-minute counts /peak counts [N <0.3 ],
0.15 change is considered significant.0.15 change is considered significant.

Captopril Renal Captopril Renal ScanMAG 3ScanMAG 3
MAG3 RENOGRAMMAG3 RENOGRAMCAPTOPRIL RENOGRAM CAPTOPRIL RENOGRAM TIME/ACTIVITY CURVETIME/ACTIVITY CURVE

AFTER 48 HOURSAFTER 48 HOURS
MAG3 RENOGRAMMAG3 RENOGRAM CAPTOPRIL RENOGRAM CAPTOPRIL RENOGRAM TIME/ACTIVITY CURVETIME/ACTIVITY CURVE

AORTOGRAMAORTOGRAM

ACEI RenographyACEI Renography
In normal renal function - sens/spec ~ 90%In normal renal function - sens/spec ~ 90% In poor renal function / ischemic nephropathy, In poor renal function / ischemic nephropathy,
ACEI renography often indeterminate ACEI renography often indeterminate >>> do MRA, Duplex US, angiogram>>> do MRA, Duplex US, angiogram

Renal Cortical ScintigraphyRenal Cortical Scintigraphy
Indications Indications
Determine involvement of upper tractDetermine involvement of upper tract
(kidney) in acute UTI (acute (kidney) in acute UTI (acute
pyelonephritis)pyelonephritis)
Detect cortical scarring (chronic Detect cortical scarring (chronic
pyelonephr.)pyelonephr.)
Follow-up post RxFollow-up post Rx

CONTD..CONTD..
gold standard gold standard 99m99mTc DMSATc DMSA The radiotracer is taken up only by The radiotracer is taken up only by
functioning PCT mass functioning PCT mass Pyelonephritis impairs tubular uptake Pyelonephritis impairs tubular uptake
of radiotracer, these areas appear as of radiotracer, these areas appear as unexposed or underexposed unexposed or underexposed
Persisting areas on follow up indicates Persisting areas on follow up indicates irreversible renal damage or scarring.irreversible renal damage or scarring.

Renal Cortical ScintigraphyRenal Cortical Scintigraphy
Cold Defect Cold Defect Acute or chronic PNAcute or chronic PN CystCyst TumorsTumors InfarctInfarct Trauma (contusion, laceration,hematoma)Trauma (contusion, laceration,hematoma)
Cortical defects are not always d/t Cortical defects are not always d/t infection & allinfection & all
DMSA defects are not necessarily scars.DMSA defects are not necessarily scars.

—2-year-old girl with fever.
Lim R AJR 2009;192:1197-1208
©2009 by American Roentgen Ray Society


Renal Cortical ScintigraphyRenal Cortical Scintigraphy
Congenital Anomalies Congenital Anomalies AgenesisAgenesis EctopyEctopy Fusion Fusion (horseshoe, crossed fused ectopia)(horseshoe, crossed fused ectopia) Polycystic kidneyPolycystic kidney Multicystic dysplastic kidneyMulticystic dysplastic kidney Pseudotumors Pseudotumors (fetal lobulation, (fetal lobulation,
hypertrophic column of Bertin , lobar hypertrophic column of Bertin , lobar nephronia)nephronia)

NORMAL DMSA SCANNORMAL DMSA SCAN

HORSE SHOE KIDNEYHORSE SHOE KIDNEY

Horseshoe kidney with normal function

RENAL AGENESISRENAL AGENESIS

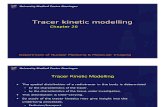
Patient with Recurrent UTI
Tc99m-DMSA renal SPECT scintigraphy Ectopic left kidney with multiple scars

Renal Transplant Evaluation:
Anterior images are obtained.Anterior images are obtained. Normal perfusion study: radioactive Normal perfusion study: radioactive
bolus reaches the renal transplant bolus reaches the renal transplant simultaneously with iliac vessels. simultaneously with iliac vessels.
Max parenchymal phase :3-5 minMax parenchymal phase :3-5 min Bladder activity appears : 4-8 minBladder activity appears : 4-8 min Up to 2 weeks after Tx, prominent Up to 2 weeks after Tx, prominent
visualisation of ureter due to edema visualisation of ureter due to edema at UV anastomotic site.at UV anastomotic site.

Renal Transplant Scintigraphy
Transplant kidney is showing good perfusion, uptake and drainage of radiotracer- Normal Study
Tc99m-DTPA renal dynamic scintigraphy

POST OP 1 WEEKPOST OP 1 WEEK POST OP 2 WEEKSPOST OP 2 WEEKS

Acute Tubular Necrosis: Acute Tubular Necrosis: Preserved or mildly reduced renal perfusion but Preserved or mildly reduced renal perfusion but
diminished renal function and progressive diminished renal function and progressive cortical retention of tubular agents.cortical retention of tubular agents.
Acute Rejection :Acute Rejection :
Poor perfusion than function in early stagePoor perfusion than function in early stage
Renogram demonstrates a diminished nephrogram phase and delayed Renogram demonstrates a diminished nephrogram phase and delayed appearance of bladder activity.appearance of bladder activity.

Renal Transplant Scintigraphy
Tc99m-DTPA renal dynamic scintigraphy
Acute Rejection Acute Tubular Necrosis

Transplant kidney is showing poor perfusion, uptake and drainage of radiotracer- Chronic Rejection
Renal Transplant Scintigraphy
Tc99m-DTPA renal dynamic scintigraphy

Cyclosporin nephrotoxicity :Cyclosporin nephrotoxicity : Scintigraphic appearance similar to Scintigraphic appearance similar to
ATN, with relative good transplant ATN, with relative good transplant perfusion and poor tubular function.perfusion and poor tubular function.
Compared to ATN ,it occurs several Compared to ATN ,it occurs several weeks after transplatation.weeks after transplatation.

Renal transplants scintigraphy Renal transplants scintigraphy Surgical complicationsSurgical complications
Urinary leak-Urinary leak-Initial photopenic defect with Initial photopenic defect with progressive accumulation of radiotracer progressive accumulation of radiotracer
Hematoma/ Abscess-Hematoma/ Abscess- Initial photopenic Initial photopenic defect not changing with time.defect not changing with time.
Lymphocele-Lymphocele- Initial photopenic defect- equal Initial photopenic defect- equal to background activity in delayed images.to background activity in delayed images.
Ureteral obstructionUreteral obstruction
Arterial stenosis and hypertensionArterial stenosis and hypertension

Renal Transplant Scintigraphy
10th Post operative day of renal transplant decreased urine output and pelvic collection
Urinary leak

Renal Transplant Scintigraphy
2nd Post operative day of renal transplant Hematoma / abscess

Renal Transplant Scintigraphy
7th Post operative day of renal transplant c/o Increased serum creatinine and pelvic collection
Lymphocele

Radionuclide CystogramRadionuclide Cystogram
INDICATIONSINDICATIONS Assess effect of Assess effect of
therapy / surgerytherapy / surgery Screening of Screening of
siblings of reflux siblings of reflux ptspts
Evaluation of Evaluation of children with children with recurrent UTIrecurrent UTI(30-50% have VUR)(30-50% have VUR)
PROsPROs More sensitiveMore sensitive 100 times less 100 times less
radiationradiationCONsCONs Inferior anatomic Inferior anatomic
deleniationdeleniation

Radionuclide CystogramRadionuclide Cystogram

RefrencesRefrences
Oxford text book of clnilcal Oxford text book of clnilcal nephrology-3nephrology-3rdrd ed. ed.
Essentials of Nuclear Medicine Essentials of Nuclear Medicine Imaging – Mettler & GuiberteauImaging – Mettler & Guiberteau
Brenner and Rector’s The kidney– 9Brenner and Rector’s The kidney– 9thth ed.ed.
www.google.comwww.google.com