NSW Stroke Reperfusion Program Evaluation Report€¦ · Health Economics and Evaluation Team –...
89
Collaboration. Innovation. Better Healthcare. REPORT NSW Stroke Reperfusion Program Evaluation Report Health Economics and Evaluation Team
Transcript of NSW Stroke Reperfusion Program Evaluation Report€¦ · Health Economics and Evaluation Team –...

Collaboration. Innovation. Better Healthcare.
REPORT
NSW Stroke Reperfusion ProgramEvaluation Report
Health Economics and Evaluation Team

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 2
AGENCY FOR CLINICAL INNOVATION
Level 4, Sage Building
67 Albert Avenue
Chatswood NSW 2067
PO Box 699 Chatswood NSW 2057
T +61 2 9464 4666 | F +61 2 9464 4728
E [email protected] | www.aci.health.nsw.gov.au
Produced by ACI Health Economics and Evaluation Team
SHPN (ACI) 150420
ISBN 978-1-76000-244-2
Further copies of this publication can be obtained from
the Agency for Clinical Innovation website at www.aci.health.nsw.gov.au
Disclaimer: Content within this publication was accurate at the time of publication. This work is copyright. It may be reproduced
in whole or part for study or training purposes subject to the inclusion of an acknowledgment of the source. It may not be
reproduced for commercial usage or sale. Reproduction for purposes other than those indicated above, requires written
permission from the Agency for Clinical Innovation.
Version: V1
Date Amended: 29/05/2015
© Agency for Clinical Innovation 2015
The Agency for Clinical Innovation (ACI) works with clinicians, consumers and managers to design and promote better healthcare for NSW. It does this by:
• service redesign and evaluation – applying redesign methodology to assist healthcare providers and
consumers to review and improve the quality, effectiveness and efficiency of services.
• specialist advice on healthcare innovation – advising on the development, evaluation and adoption of
healthcare innovations from optimal use through to disinvestment.
• initiatives including guidelines and models of care – developing a range of evidence-based healthcare
improvement initiatives to benefit the NSW health system.
• implementation support – working with ACI Networks, consumers and healthcare providers to assist
delivery of healthcare innovations into practice across metropolitan and rural NSW.
• knowledge sharing – partnering with healthcare providers to support collaboration, learning capability
and knowledge sharing on healthcare innovation and improvement.
• continuous capability building – working with healthcare providers to build capability in redesign, project
management and change management through the Centre for Healthcare Redesign.
ACI Clinical Networks, Taskforces and Institutes provide a unique forum for people to collaborate across clinical
specialties and regional and service boundaries to develop successful healthcare innovations.
A priority for the ACI is identifying unwarranted variation in clinical practice and working in partnership with
healthcare providers to develop mechanisms to improve clinical practice and patient care.
www.aci.health.nsw.gov.au

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 3
Contents
Abbreviatons 6
Evaluation snapshot 7
Executive summary 8
Background 8
Methods 8
Key findings 8
Recommendations 9
Section 1 Introduction 11
1.1 Stroke 11
1.2 Intravenous thrombolysis for stroke 11
Section 2 Background 12
2.1 NSW Stroke Reperfusion Program 12
Section 3 Evaluation of the program 15
3.1 Purpose 15
3.2 Evaluation 16
3.3 Limitations of the evaluation 17
Section 4 Methods 18
Section 5 Stroke in NSW 21
Section 6 Key findings from site visits and interviews 25
6.1 Access to information 25
6.2 Coherent planning 27
6.3 People and engagement 28
6.4 Business processes 28
6.5 Leadership 30
6.6 Culture and values 30
Section 7 Key findings from SRAT review 32
7.1 Stroke Reperfusion Assessment Tool 32
Section 8 Discussion 41
8.1 Program fidelity 41
8.2 Barriers to program implementation and delivery 41
8.3 Factors facilitating success of the program 42
Section 9 Conclusion and preliminary recommendations 43
Section 10 Next steps 45
Section 11 References 46
Appendix I 47
Appendix II 55
Appendix III 89

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 4
Figures
Figure 1: NSW SRP Pathway 14
Figure 2: SRP site visits by participants and position 20
Figure 3: Code groupings and emerging themes 20
Figure 4: Average NWAU for SRP sites 21
Figure 5: NSW ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 23
Figure 6: SRP ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 23
Figure 7: Non-SRP sites ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 24
Figure 8: Gosford Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 56
Figure 9: Nepean Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 58
Figure 10: Campbelltown Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 60
Figure 11: Orange Health Service ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 62
Figure 12: Bathurst Base Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 64
Figure 13: St Vincent’s Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 66
Figure 14: Royal Prince Alfred Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 68
Figure 15: Prince of Wales Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 70
Figure 16: Bankstown-Lidcombe Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 72
Figure 17: Westmead Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 74
Figure 18: Liverpool Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 76
Figure 19: Royal North Shore Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 78
Figure 20: St George Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 80
Figure 21: Wagga Wagga Base Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 82
Figure 22: Hornsby and Ku-Ring-Gai Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 84
Figure 23: Blacktown Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 86
Figure 24: Concord Hospital ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 88

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 5
Tables
Table 1: Key evaluation questions 16
Table 2: Summary activity by SRP site 2012-13 22
Table 3: Emerging themes 25
Table 4: Stroke Reperfusion Assessment Tool summary 47
Table 5: Gosford Hospital selected stroke DRGs 2007-08 to 2012-13 55
Table 6: Nepean Hospital selected stroke DRGs 2007-08 to 2012-13 57
Table 7: Campbelltown Hospital selected stroke DRGs 2007-08 to 2012-13 59
Table 8: Orange Health Service selected stroke DRGs 2007-08 to 2012-13 61
Table 9: Bathurst Base Hospital selected stroke DRGs 2007-08 to 2012-13 63
Table 10: St Vincent’s Hospital selected stroke DRGs 2007-08 to 2012-13 65
Table 11: Royal Prince Alfred Hospital selected stroke DRGs 2007-08 to 2012-13 67
Table 12: Prince of Wales Hospital selected stroke DRGs 2007-08 to 2012-13 69
Table 13: Bankstown-Lidcombe Hospital selected stroke DRGs 2007-08 to 2012-13 71
Table 14: Westmead Hospital selected stroke DRGs 2007-08 to 2012-13 73
Table 15: Liverpool Hospital selected stroke DRGs 2007-08 to 2012-13 75
Table 16: Royal North Shore Hospital selected stroke DRGs 2007-08 to 2012-13 77
Table 17: St George Hospital selected stroke DRGs 2007-08 to 2012-13 79
Table 18: Wagga Wagga Base Hospital selected stroke DRGs 2007-08 to 2012-13 81
Table 19: Hornsby and Ku-Ring-Gai Hospital selected stroke DRGs 2007-08 to 2012-13 83
Table 20: Blacktown Hospital selected stroke DRGs 2007-08 to 2012-13 85
Table 21: Concord Hospital selected stroke DRGs 2007-08 to 2012-13 87

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 6
Abbreviatons
ABF Activity-based funding
ABS Australian Bureau of Statistics
ACI Agency for Clinical Innovation
AH After hours
AIHW Australian Institute of Health and Welfare
ALOS Average length of stay
AR Australian-refined
ASNSW Ambulance Service New South Wales
ASC Australian Stroke Coalition
ASU Acute stroke unit
ATC Acute Thrombolytic Centre
AuSCR Australian Stroke Clinical Registry
AuSDaT Australian Stroke Data Tool
BH Business hours
BHI Bureau of Health Information
CE Chief Executive
CPDI Clinical program design and
implementation
CT Computed tomography
CTP Computed tomographic perfusion
DRG Diagnosis-related group
DTN Door-to-needle
ECI Emergency Care Institute
ED Emergency department
FAST+ Face, arm, speech, time – positive
GP General practitioner
HDU High dependency unit
HNE Hunter New England
ICD International Classification of Disease
ICU Intensive care unit
HOD Head of Department
KPI Key performance indicator
LHD Local health district
MD Multidisciplinary
MDT Multidisciplinary team
MoH Ministry of Health
M&M Mortality and morbidity
NIHSS National Institute of Health Stroke Scale
NSF National Stroke Foundation
NSW New South Wales
NWAU National weighted activity unit
PET Patient and Staff Experience Tracker
rtPA Recombinant tissue plasminogen activator
SITS Safe implementation of treatment
in strokes
SRAT Stroke reperfusion assessment tool
SRP Stroke Reperfusion Program
SSA Stroke Society of Australasia
TIA Transient ischaemic attack
TIPS Thrombolysis ImPlementation in Stroke
TGA Therapeutic Goods Administration
USA United States of America
VMO Visiting Medical Officer

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 7
Key evaluation questions Key findings
Was the program design effective in delivering the SRP program?
Yes, the design is supported by a clear evidence base with reperfusion being provided at all 20 of the sites prior to the official launch of the SRP. A more thorough analysis of effectiveness will be undertaken in the next stage of the evaluation.
What processes did ACI use to implement the program across sites and is it consistent with the ACI Implementation Framework?
Yes. The processes used are consistent with the ACI Implementation Framework. Implementation comprised identifiying leaders, corresponding with Chief Executives and developing tools to aid consistent implementation.
Were the processes consistent at each site? Yes. A standardised format was used by ACI accompanied by the development of a generic model of care, implementation toolkit and checklist.
Were the processes used for each component of implementation effective?
Yes. All processes were standardised and comprised site visits to review each component and documented standards for each as contained in the toolkit.
What inhibited implementation? There was a lack of access to information in terms of baseline and ongoing data collection, reporting and sharing systems to enable monitoring and evaluation, benchmarking and program improvements.
What facilitated implementation success? Leadership and champions at each site facilitated implementation success along with a team approach across SRP units (ASNSW, ED, ATC/ASU). Where several SRP sites are located within a District, a District approach to stroke care was identified as facilitaingr successful implementation.
What strategies can be used to improve the program design and implementation process?
Identification, agreement and establishment of program objectives and associated data collection methods prior to implementation to enable comprehensive monitoring, evaluation and benchmarking across sites.
Have the minimum requirements for stroke reperfusion been implemented and sustained?
Yes. Minimum standards for stroke reperfusion (pre-notification, 24/7 service, acute stroke teams) have been implemented and sustained. However, analysis is required in the next stage of the evaluation to determine if all components of the program operate within the designated time frames.
Are implementation processes in place (stroke team meetings, reviews, MD thrombolysis committee, training and education)?
Somewhat. This varies across sites with most sites using a locally-adapted, hybridised model for governance, review and training.
Are standards of care upheld (guidelines, pathways, protocols)?
Yes. All sites have appropriate guidelines, protocols and pathways in place, and regularly review and update them.
Are data collection systems in place and implemented? No. Although most sites use a local database, there is no overarching data collection method, data dictionary or agreed database for the systematic collection and use of program and outcomes data.
Evaluation snapshot

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 8
Executive summary
Background
The New South Wales Stroke Reperfusion Program
The NSW Stroke Reperfusion Program (SRP) was formally
launched by the NSW Health Minister in January 2013.
Stroke reperfusion is a clinical intervention that involves
injection of a clot-busting medication – recombinant tissue
plasminogen activator (rtPA), which can greatly improve
patient outcomes if administered in a brief time period
after the onset of an ischaemic stroke. In this report,
stroke reperfusion is referred to as thrombolysis or
thrombolytic intervention.
Central to the SRP was the establishment, within existing stroke units, of 20 Acute Thrombolytic Centres (ATCs) within
metropolitan and rural NSW. The 20 ATCs comprise specialist services to care for patients including 24/7 access to
Medical Imaging Departments, 24/7 Emergency Departments (EDs) where staff are trained in the administration of
intravenous thrombolysis and a 24/7 multidisciplinary (MD) stroke team that is based within a stroke unit with
collocated beds for monitoring.
Program objective
The objective of the NSW Stroke Reperfusion Program is to reduce the time from symptom onset to thrombolytic
intervention (onset-to-needle and door-to-needle [DTN] times) for people experiencing an ischaemic stroke. The program
is consistent with the Stroke Foundation’s Clinical Guidelines for Stroke Management 2010 (NSF, 2010) that stipulates
streamlining ambulance and hospital services to treat people experiencing the signs and symptoms of stroke, increasing
the use of thrombolysis for eligible patients from an estimated 7% in 2010 to 20%, and reducing the composite primary
end point of death or disability.
This report provides an overview of Stage one of the evaluation of the SRP. The evaluation is in three stages to enable the
identification and collection of relevant data throughout the project. Stage one is predominantly a descriptive analysis of
the program focusing on implementation processes and program fidelity.
Methods
This stage of the evaluation is based on visits to each of the SRP sites, with the exception of Tamworth and John Hunter
Hospitals, both of which respectfully declined to take part in the evaluation and are advanced in practice compared with
other sites in NSW.
The site visits comprised assessing program components to test the fidelity of implementation and additional interviews
as part of the formative evaluation process designed to identify barriers and success factors for program delivery.
Key findings
• Compared with the treatment of all strokes, stroke units where SRP is provided (over 50% of all strokes) had:
° a higher complexity of patients with an average National Weighted Activity Units (NWAU) of 1.9 compared with
the NSW average of 1.5 in 2012-13
° an average length of stay of 6.9 days in 2012-13, which is only slightly higher than the NSW average of 6 days
° experienced an increased volume of 14% over the period 2007-08 to 2012-13. compared with a 3% increase for
NSW in total for the same period.
Stroke units significantly improve
health outcomes of stroke patients. Between
2007 and 2011, the number of stroke units in
public hospitals {nationally} increased from 54
to 74 and the proportion of patients receiving
stroke care increased from 50% to 60%.
“ “
AIHW, 2013

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 9
• The fastest DTN times self-reported for the past year were at Royal Prince Alfred and St George Hospitals at
17 and 18 minutes, respectively. However, there is no consistent statistical method used across sites to
analyse and compare data. Further work is required to determine median times during business hours (BH)
and after hours (AH) for each site to provide a more comprehensive understanding. This will occur at the
next stage of evaluation.
• There was fidelity in the way SRP was implemented across the sites, resulting from a consistent model of care,
the implementation approach, input from the ACI Implementation Team, implementation toolkit and
checklists. However, delivery of the SRP at sites differed, particularly between metro and rural areas.
• The need for a comprehensive data collection, reporting and knowledge exchange system in place prior to
implementing any program was raised as a major theme in the evaluation. The lack of a consistent system
resulted in barriers for local monitoring and planning, evaluation and benchmarking.
• Access to medical imaging was found to be the program component most associated with delayed treatment
times. Although most sites are actively working towards addressing this, a consistent approach to scan types
and AH access was viewed as a requirement to hasten treatment times. This was also viewed as a substantial
contributor to differences in service provision during BH and AH. A total of seven sites reported that imaging
was not pre-notified for FAST+ patients.
• Pre-notification of FAST+ patients is occurring from ambulance to EDs at all sites. However, three of the SRP sites
do not pre-notify the acute stroke team until after the patient has arrived and diagnosis is confirmed. Although
it was noted that acute stroke teams can be mobilised quickly, this has potential to slow times to treatment.
• Rural services indicated a need for flexibility in service design to enable localisation consistent with resources,
staffing and throughput. Local leaders and champions were indicated in successful program delivery,
particularly in rural sites to ensure program visibility.
• The establishment of executive sponsors and clinical champions at all sites provided leadership of the program,
effectively raising awareness of stroke pathways and emphasising the time-critical treatments.
• Where there were several SRP sites located within a District, a District-wide collaborative approach to stroke
care facilitated program success with shared medical teams, pathways, protocols and an established
knowledge-sharing environment. Similarly, a collaborative working relationship with ambulance services being
acknowledged as part of the patients’ treatment journey was seen as facilitating program success at those sites
where it occurred.
• Although most SRP sites have been thrombolysing patients prior to the official ‘‘go live’1’ date of the SRP,
anecdotal evidence suggests that improvements in pre-hospital notification and faster transfer to SRP sites has
increased rates of thrombolysis from 7% of eligible patients in 2010 (NSF, 2010) to triple that at some sites. This
will be investigated in Stage two of the evaluation when the relevant data is available.
Recommendations
The following recommendations have been made as a starting point in overall program improvement. It is anticipated
that further recommendations will be made as data is gathered and analysed at each stage of evaluation.
1 ‘Go live’ refers to the date that the NSW Health Matrix was released requiring ASNSW to transfer potential FAST+ patients to the nearest SRP site. This occurred in January 2013 and is sometimes referred to as the ‘official launch of the SRP’.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 10
Access to information
1. Consistent data collection methods to be determined for SRP, development of a data dictionary and guidelines for
collection, access and reporting.
2. Data provided across all components of the program to SRP stakeholders (sites, Ambulance Service New South
Wales (ASNSW) and ACI), including, at a minimum, data on ASNSW FAST+ patients by site, DTS time,
scan-to-needle time, transfer times and destinations, and patient outcomes. This data will be used for monitoring,
evaluation and benchmarking.
3. ACI to continue work with the Activity-based Funding (ABF) taskforce to undertake a costing and counting study of
stroke thrombolysis treatment with a view to standardising the identification of activities and costs associated with
the provision of stroke thrombolysis services within administrative and ABF data.
4. Consider including formalised feedback loops that will provide patient outcomes to ASNSW within an agreed time
frame from patient delivery to the site to keep ASNSW staff informed.
5. ASNSW to provide weekly data of FAST+ patients taken to each site.
Coherent planning
6. Within the mandate of ACI, consideration to be given to how ACI can best support program delivery and
sustainability beyond implementation. Formalised discussions with key local health district (LHD) stakeholders
regarding their needs is suggested.
7. All models of care are to include baseline data and data collection systems prior to implementation.
8. Further discussion to occur with relevant sites about establishing adequate governance structures to oversee the SRP.
People and engagement
9. A public awareness campaign is suggested comprising stroke and time-critical aspects of treatment with a specific
focus on rural areas and cohorts with the highest stroke prevalence – Aboriginal and Torres Strait Islander people and
people from low socio-economic backgrounds. Although noted in the SRP, public awareness campaigns are outside
the remit of ACI. Therefore, it is suggested that the Stroke Network discusses potential recommendations and
forward them to the relevant bodies for consideration.
Business processes
10. The Stroke Network to convene an expert group to discuss and determine guidelines for SRP sites regarding the
relevant scan types required to ascertain eligibility for stroke thrombolysis treatment and subsequent decision-making
(remote, telehealth) and access to imaging (via ED or directly from ambulance).
11. Matrix to be reviewed in terms of providing statewide coverage and allocation of workload within catchment areas.
12. The Stroke Network to convene a forum of SRP and relevant sites to discuss issues of repatriation with the purpose of
resolution. These discussions are to include commencing rehabilitation, services and capacity at outlying sites and
assessing options for patients.
Leadership
13. ACI and Emergency care institute (ECI) to continue to discuss options for affirming thrombolysis treatment for stroke
as standard practice in stroke care.
Culture and values
14. Promote SRP as an integrated program across ASNSW and LHDs.
15. Define and promote a person-/patient-centred care focus for stroke care in NSW.
16. Further explore the areas of interest as contained in the attached Patient Experience Trackers Report at Appendix III.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 11
Section 1 Introduction
1.1 Stroke
Stroke is the second biggest killer in Australia, after heart disease (ABS, 2009), and in 2008-09, had an estimated
financial cost of $606 billion (ICD-10 codes 160-164) (AIHW, 2013).
There are two predominant types of stroke – ischaemic and haemorrhagic. Ischaemic strokes account for up to 80
per cent of strokes in Australia and occur when a clot blocks blood flow to the brain. A haemorrhagic stroke is due
to bleeding in the brain.
During the period from July 2009 to June 2012, more than 14,200 people were hospitalised in NSW with a principal
diagnosis of ischaemic stroke and almost 5700 people admitted with a principle diagnosis of haemorrhagic stroke
(BHI, 2013). Thirteen percent of people experiencing ischaemic stroke died within 30 days. Two percent of these
deaths occurred on the first day of hospitalisation, 51% within seven days of hospitalisation and 31% occurred after
discharge (BHI, 2013).
Ischaemic strokes are amenable to intravenous thrombolytic intervention, and as documented in a Cochrane
meta-analysis of this treatment, if administered within a few hours of stroke onset, can reduce death and disability
by up to 44% (Wardlaw et al, 2009).
Ischaemic stroke is identified using a brain scan. Ischaemic and haemorrhagic strokes, and transient ischaemic
attacks (TIAs), all present as stroke, and although thrombolytic intervention is not appropriate for haemorrhagic
strokes and TIAs , patients experiencing these conditions may benefit from the intensive care received through a
dedicated stroke unit.
In providing timely thrombolytic treatment to eligible stroke patients, Lovett et al have shown that the provision of
dedicated stroke units comprising multidisciplinary teams (MDTs) and acute stroke pathways have indicated a 30%
improvement in mortality of ischaemic stroke patients in metropolitan NSW compared with stroke patients
receiving care in general wards (Lovett et al, 2003).
The National Stroke Foundation (NSF) has developed guidelines for the management of stroke patients in acute
stroke units. The guidelines comprise coordinated care by MDTs and define the need for 24/7 access to medical
imaging, EDs where staff are trained in thrombolysis for stroke and MD stroke teams within a stroke unit.
1.2 Intravenous thrombolysis for stroke
Intravenous thrombolysis is the injection of a clot-busting medication, rtPA. Administration of thrombolytic therapy
is subject to adhering to a strict criterion for administering up to 4.5 hours after stroke onset (this comprises
90-minute transfer and 3-hour hospital targets) depending upon the patients’ medical history. The earlier rtPA is
administered, the sooner blood flow to the brain is restored, resulting in more benefits being conferred in terms of
ameliorating stroke-related disability, because every 20-minute delay from stroke onset to thrombolysis
significantly reduces the benefits of this treatment. Accordingly, DTN time is a major indicator when evaluating the
clinical outcomes of intravenous thrombolysis (Wardlaw JM, 2009). The administration of rtPA in this paper is
referred to as thrombolytic intervention or thrombolysis.
Thrombolytic intervention administered within 3 hours of the onset of stroke symptoms was licenced for use by the
Therapeutics Goods Administration (TGA) in Australia in 2003. The TGA has since reviewed the evidence and has
licenced its use up to 4.5 hours after symptom onset based on more recent evidence. From 2007 to 2010, patients
admitted for ischaemic stroke who received thrombolysis increased from 461 per year to 1,170 in Australia (AIHW,
2013). This increase is indicative of the increase in stroke units offering the treatment. However, the use of
thrombolysis intervention for stroke is still relatively low in Australia, with the treatment being used for an
estimated 7% of patients presenting with ischaemic stroke nationally (Hoffman T, 2013).

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 12
Section 2 Background
In 1998, the Helsinki University Central Hospital began thrombolysing patients for ischaemic
stroke using a specific protocol to ensure that the treatment could be administered safely in a
time-critical manner.
The protocol encompassed the key components of:
• ambulance pre-notification
• the transfer of patients directly from triage to radiology for scans; and, if eligible
• administering of thrombolysis in radiology (Lindsberg et al, 2006).
The key components of the Helsinki model have been successful in reducing DTN time to approximately 20 minutes.
It has since been implemented in several other countries including European nations, the United States of America
(USA), Canada and Australia.
The model has been adapted and implemented on a large scale in the states of North Carolina and New York in the
USA (Asimos et, 2014; Goldstein, 2010; Jaunch et al, 2013), in two centralised metropolitan areas in the United
Kingdom – Greater Manchester and London (Morris, 2014), and in Ontario, Canada (Merino et al, 2014).
In Australia, increasing access to thrombolysis forms part of the Victorian statewide and Western Australian Stroke
Care Plans (WA Gov, 2012; Vic Gov, 2013).
In Victoria, the model has been successfully operating at the Royal Melbourne Hospital, achieving a median
20-minute door-to-needle time (Meretoja et al, 2013). Hunter New England (HNE) was the first place in NSW to
adopt the key components of the model in the early 2000s.
Using the formal definition of program innovation as defined by Wyatt Knowlton and Phillips, innovation occurs
as a result of programs designed from hypotheses derived from research synthesis, whereas benchmark
programs are those based on the evidence of existing and similar programs (Wyatt Knowlton et al, 2013). Thus,
although the NSW SRP is not an innovation, it is based on sound evidence, with its foundations in well-
researched and successful programs.
2.1 NSW Stroke Reperfusion Program
The NSW Stroke Reperfusion Program was formally launched in January 2013 by the NSW Health Minister along
with the formal establishment of 20 ATCs within metropolitan and rural NSW. The ACI Stroke Network Manager,
Clinical Program Design and Implementation (CPDI) Team within ACI and a project officer from ASNSW have
worked collaboratively with LHDs to establish the program across NSW. Throughout this report, ATCs and SRP sites
are used interchangeably.
ATCs are located within existing stroke units and include several key components, as detailed below.
• They have specialist services to care for patients including 24/7 access to medical imaging departments, EDs
where staff are trained in the administration of intravenous thrombolysis and a MD stroke team within a stroke
unit with collocated beds for monitoring. The stroke team members are expertly trained in the management of
people experiencing stroke.
• They are required to undertake a robust process to demonstrate ability to safely and competently deliver 24/7
intravenous thrombolysis and provide the hyper-acute care needed for these patients.
• They have collocated monitored beds and staff facilitate timely transfer of care (ACI, 2013). Each ATC
underwent a pre-implementation process, which included ongoing monitoring and governance processes. An
important element of the program is a well-defined process of transfer to appropriate post-thrombolysis and
post-acute care.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 13
The objective of the NSW SRP is to reduce the time from symptom onset to thrombolytic intervention (onset-to-
needle and DTN times) for patients with an ischaemic stroke. The program is consistent with the National Stroke
Foundation’s Clinical Guidelines for Stroke Management 2010 (NSF, 2010) that stipulates streamlining ambulance
and hospital services to treat people experiencing the signs and symptoms of stroke, increasing the use of
thrombolysis for eligible patients and reducing the primary composite end point of death or disability.
Through the program, all paramedics in NSW have received training in the nationally recognised and validated
FAST+ tool. Paramedics use this tool and their clinical skills to:
• rapidly assess and identify patients with the signs and symptoms of stroke
• transport these patients with onset under 3 hours to the nearest ATC (within a 90-minute drive time), pre-notifying
en route to mobilise the stroke team on pre-arrival through what is often called a stroke code or ‘bat call’.
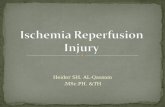
Figure 1 shows the pathway for the NSW SRP. Through the pre-hospital-led redesign, the NSW Health Matrix (the
Matrix) was reviewed with an additional category of Stroke FAST+ positive created by the NSW Ministry of Health
(MoH). This helps ensure paramedics take patients who meet the criteria to one of the 16 metropolitan ATCs for
definitive treatment.
The program includes protocols on the repatriation and transfer of care for people experiencing stroke back to
their local hospital, as appropriate. Rural hospitals (and Wollongong Hospital) do not operate under the Matrix
system. However, hospitals are still pre-notified of FAST+ patients irrespective of whether an ATC is present.
Patients arriving at a hospital with an ATC by transport other than ambulance are assessed using relevant
assessment tools and if identified as experiencing stroke, the stroke team is notified and mobilised immediately.
The stroke team provides intensive and timely assessment and monitoring to patients while determining eligibility
for thrombolytic intervention (the type of stroke is identified through scans). Once eligibility is confirmed, these
patients are treated, and those not considered eligible are transferred to the relevant units for treatment, i.e.
intensive care, high dependency or stroke units.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 14
Source: ACI Stroke Reperfusion Program evaluation plan, 2014
NSW Ambulance - use FAST+ to
identify people experiencing stroke
NSW Ambulance-determine time of
onset (or last seen well) of stroke
FAST positive patients
Stroke FAST positive, patient trans
ported to nearest Acute Thrombolysis
Centre if within 3 hour clinical time
Eligible patients receive
thrombolytic intervention
Patients arriving to
Emergency Department by
non-Ambulance transport
Non-eligible patients are transferred
to ward (ICU, HOU, stroke care beds)
Pre-notification of FAST positive
patient to Acute Thrombolysis Centre
or hospital if no ATC
Patients transferred to ICU, HDU,
acute stroke care beds with in 3 hours
Staff identify patients
experiencing stroke
Discharge (including rehab, local
hospital, home, aged care facility)
Stroke team mobilised (24-hour service)
Bedside patient assessment with completion of IV
thrombolysis and acute clinical management checklist
Eligibility for thrombolysis determined by checklist, general
assessment and brain scan
3 hours
4.5 Hours
CUMULATIVE TIMELINE
Stroke onset
Figure 1: NSW SRP Pathway

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 15
Section 3 Evaluation of the program
3.1 Purpose
The overall purpose of the evaluation of the SRP is to:
• examine whether the aims of the program have been achieved at a system, staff and patient level
(a process-outcome evaluation)
• determine if the implementation approach has been effective, well-designed and appropriate.
As the SRP has several components, and given the lack of inclusion of stroke reperfusion in administrative
datasets, the evaluation will be undertaken in three stages as follows:
3.1.1 Stage one
Stage one will comprise a review of the program design and components implemented across the SRP sites and
within ASNSW. The aim is to identify what aspects of the program have been implemented and delivered and
what inhibits or facilitates program success.
This stage will examine the fidelity of the implementation approach by examining the intent and design of the
program and how this relates to the implementation processes and subsequent program delivery. This
descriptive study will examine various design elements and link to specific implementation strategies and
program delivery to determine success factors that can be adopted at a generic program design level and those
that are specific to the SRP. The results of this part of the study will be used to inform ACI of areas that can be
improved in future design and implementation activities.
The first stage will use a variety of methods and instruments including surveys, interviews and audits – including
the Stroke Reperfusion Assessment Tool (SRAT) and the collection of a minimum dataset around stroke
thrombolysis process – and observation. The SRAT tool and datasets are to be routinely used in the governance
of the program.
3.1.2 Stage two
Stage two of the evaluation will examine outputs and subsequent outcomes of the program at SRP sites compared
with non-SRP sites being assessed before and after inception of the program. Where data are available, this will
comprise DTN time, whether the patient received thrombolytic intervention, and death and disability rates. Stage
two will investigate reasons why eligible patients experiencing ischaemic stroke did not receive thrombolytic
intervention, and why ineligible patients receive intervention and their clinical outcomes in all participating SRP
sites. Examination of changes in clinical outcomes for patients experiencing non-ischaemic stroke and receiving the
intensive assessment, monitoring and care provided by the stroke teams until eligibility is determined will occur.
Stage two will comprise audits of data systems, and linked administrative ambulance, inpatient and death data.
Patient and Staff Experience Trackers (PETs) will be used to examine changes in the experience of staff and
patients. The PET analysis will be undertaken in Stage one of the evaluation to establish a baseline of the staff and
patient journey, and continue at intervals throughout the evaluation. It is anticipated that the PETs will provide
qualitative assessment linked from ambulance to ED (commencing at ED for those patients not arriving by
ambulance), SRP site, transfer destination and at discharge.
3.1.3 Stage three
A third stage of evaluation of the program will occur at a later date once the program is considered settled and
there is adequate data available to examine long-term clinical outcomes. This stage will also comprise a system-
wide analysis and economic appraisal.
Currently funding contained in ABF datasets is based on costs that reflect the more “traditional” treatments for stroke.
This means that the prices paid for the treatment of stroke with thrombolytic intervention may not capture the costs

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 16
associated with determining whether a patient is a suitable candidate for thrombolytic intervention and for undertaking
the intervention. Additional separate work is underway to establish realistic costings and ABF pricing for stroke
intervention and care. The development of the ABF platform is considered to be the preliminary phase of the economic
component of the evaluation. Full scoping of this stage will occur once comprehensive ABF stroke reperfusion data are
available to inform the analysis.
In the interim, ABF data concerning the treatment of ischaemic stroke will provide an indicative guide to potential costs of
the program.
This report documents the findings of the first stage of the evaluation only. As subsequent stages are completed,
additional chapters will be added to this document. The information gathered at each stage of the evaluation will be
triangulated to form a comprehensive assessment of the impact of the program.
3.2 Evaluation
This first stage of the evaluation is primarily a descriptive, qualitative study that will assess implementation, function and
fidelity of the program at the participating sites. This is aimed at identifying what aspects of the program have been
implemented and delivered and what inhibits or facilitates program success.
This stage examines the fidelity of the implementation approach by examining the intent and design of the program and
how this relates to the implementation processes and subsequent program delivery. This includes assessment of various
design elements and links to specific implementation strategies and program delivery to determine success factors that
can be adopted at a generic program design level and those that are specific to the SRP. The results of this part of the
study will be used to inform ACI of areas that can be improved in future design and implementation activities.
This first stage has used a variety of methods and instruments including surveys, interviews and audits – including the
SRAT – to collect data. As discussed further in the limitations section, it is not known what data are collected at sites,
therefore it was unknown prior to Stage one what data was available for further investigation. This includes whether data
concerning time of stroke onset, rates of thrombolysis intervention and protocol compliance or violation is available. A
component of the first stage has been to identify data that is collected at each site required for output (key indicators)
and outcome measures that will be used in the proceeding stages of the evaluation.
The key evaluation questions for Stage one comprise:
Table 1: Key evaluation questions
Fidelity Process, quality and quantity
Was the program design effective in delivering the SRP program?
Have the minimum requirements for stroke reperfusion been implemented and sustained (staffing / protocols)?
What processes did ACI use for program implementation across sites and is it consistent with the ACI Implementation Framework?
Are implementation processes in place (stroke team meetings, reviews, MD thrombolysis committee, training and education)?
Were the processes consistent at each site? Are standards of care upheld (guidelines, pathways, protocols)?
Were the processes used for each component of implementation effective?
Are data collection systems in place and implemented?
What inhibited implementation?
What facilitated implementation success?
What strategies can be used to improve the program design and implementation process?

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 17
3.3 Limitations of the evaluation
1. There are several gaps in data that limit knowledge in several areas of stroke care and thrombolysis treatment
for stroke. A major limitation of the SRP evaluation was the unknown nature of data collection systems and
availability at sites. To address this, the evaluation of the SRP has been staged and part of this first stage was an
investigation of the local data sources to inform analysis at Stage two.
2. There is no defined coding system used consistently for thrombolytic treatment for stroke. This means that
treatment cannot be identified and analysed at each site through administrative data. To address this, stroke
episodes have been used to provide a general overview of trends and provided in this report, with further
analysis to occur in subsequent evaluation stages. This has prompted additional work with the ABF Unit in the
NSW MoH to define costs associated with thrombolytic intervention and potential identification through
improved coding.
3. Sites visited were asked to include staff from ED, stroke units, imaging and stroke committees in the interview
process, as well as executive sponsors, clinical leaders and project officers. Participation varied across sites and
this may have impacted on the information gathered and subsequently reported in this document. The reader
should therefore be mindful of interview participation when reading findings.
4. Several sites raised issues of program resourcing in the course of interviews. Although ACI acknowledges that
there may be local issues with regards to program funding, stroke reperfusion is considered the standard
practice of stroke treatment rather than an additional program, and therefore, local resourcing is not within
the scope of this evaluation.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 18
Section 4 Methods
The Stage one evaluation of the SRP is a descriptive, qualitative study based on assessment of the SRAT and a series
of interviews. All 20 sites delivering the SRP were invited to participate in the evaluation, with all but two accepting.
The HNE LHD respectfully declined the invitation for the John Hunter and Tamworth Hospitals to participate.
Descriptive statistics for stroke separations in NSW (for patients 18 years and older) have been included in this
report (in Attachment II) to contribute to the overview of stroke activity across the state and within the SRP sites.
Site-specific stroke and thrombolysis data will not be available for analysis until Stage two of the evaluation where
the patient journey will be fully investigated. The descriptive statistics in this report are to be viewed as an
indicative overview of stroke care but do not specify thrombolysis treatment specifically. The statistics are derived
from the NSW Admitted Patient Data Collection using the following International Classification of Disease (ICD)-10
codes for stroke where the ICD code occurs as the primary diagnosis:
• I63 Cerebral infarction (I63.0, I63.1, I63.2, I63.3, I63.4, I63.5, I63.6, I63.8, I63.9)
• I64 Stroke, not specified as haemorrhage or infarction
• I61 Intracerebral haemorrhage (I61.0-I61.9)
• I62 Other non-traumatic intracerebral haemorrhage (I62.0, I62.1, I62.9)
• G45 TIA (all G45 codes).
These codes were agreed by the SRP Evaluation Advisory Committee. An acute flag and further filtering by acute
care type was used to ensure only acute episodes were captured.
Further analysis then occurred at diagnosis-related group (DRG) level using AR-DRG version 6. DRGs were selected
on the basis of volume, with stroke patients being grouped into four main DRGs comprising:
• B02 Cranial procedures
• B04 Extracranial vascular procedures
• B69 TIA and precerebral occlusion
• B70 Stroke and other cerebrovascular disorders.
The use of AR-DRG codes in extracting the patient data has enabled analysis of the NWAUs as a proxy of complexity
and cost. The slight difference between DRG and ICD numbers may be accounted for by type change in ICD codes,
whereas DRGs are based on primary diagnosis at separation along with the elimination of some DRGs for further
analysis given lack of volume or materiality. This results in a slightly higher number of episodes grouped within the
ICD codes, but this does not change the average NWAU as this calculation is based on the primary DRGs.
Site visits
The ACI Evaluation Manager visited the 18 participating sites between 14 May and 14 August 2014 as follows:
• Gosford Hospital
• Nepean Hospital
• Campbelltown Hospital
• Orange Hospital
• Bathurst Hospital
• St Vincent’s Hospital
• Royal Prince Alfred Hospital

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 19
• Prince of Wales Hospital
• Bankstown-Lidcombe Hospital
• Westmead Hospital
• Liverpool Hospital
• Royal North Shore Hospital
• Sydney Adventist Hospital
• St George Hospital
• Wagga Wagga Base Hospital
• Hornsby Ku-Ring-Gai Hospital
• Blacktown Hospital
• Concord Hospital.
A semi-structured group interview format was employed at each site, guided by the SRAT, to map the components
of the program and local translation. The interviews included discussion about the ACI implementation processes,
barriers and support factors of program delivery. Each interview took between 1 and 1.5 hours. A site visit pack was
developed and distributed to each site prior to the visits.
Six of the 18 sites plus ASNSW were invited to participate in a more in-depth semi-structured group interview
focusing on:
• assessment of the implemented program at each site and within ASNSW
• identification of factors that facilitate or impede implementation and, where relevant, an audit of
implementation processes, such as sighting of MD stroke team meeting minutes, local pathways, patient
assessment sheets and other relevant documents in place such as local guidelines and policies.
The intention of the interviews was to gather more detailed information than that provided by the SRAT. Site
selection for these interviews was based on 2012-13 quantum of separations for ischaemic stroke and included a mix
of metropolitan and rural sites. The interviews were conducted by the ACI Evaluation Manager and comprised the
following sites:
• Gosford Hospital
• Royal Prince Alfred Hospital
• Bankstown-Lidcombe Hospital
• St George Hospital
• Blacktown Hospital
• Wagga Wagga Hospital.
An interview guide was developed for sites and for ASNSW. A simple audit tool was developed to guide the
sighting of relevant documents and this was included in the site visit pack.
In total, 90 people attended the interviews comprising ED medical officers (n=6) and nursing (n=16), stroke and
neurology medical officers (n=23) and nursing (n=28), data managers (n=2), pharmacy (n=1) and administration and
executive directors (n=14) as depicted in Figure 2.
All interviews were recorded and transcribed. A data reduction matrix was developed and used to code themes and
sub-themes. This was based in part on the Success Factors for Strategic Change Initiatives (Kash et al, 2014). This
informed the development of a data display grid quantifying emerging themes. An emerging theme is classified as
any topic that has been raised by three or more sites. Other issues are raised in the key findings section where

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 20
considered important for discussion and improvement. To assist the reader in determining if it is emerging as a
theme, the number of sites relating to the points is noted in the narrative. Emerging themes are summarised in
the Key findings section from the site visits and interviews section in this report.
Figure 3 shows the code groupings for emerging themes.
Number of attendees
Posi
tio
ns
0
Pharmacy
Data Manager
Stroke Nurse
Administration / Medical Director
Neurology / Directors
ED Nurse
ED Medical Officers / Directors
2010 305 2515
Site visit meetings
Figure 2: SRP site visits by participants and position
Data, benchmarking, reports Access to information
Planning, implementation, sustainability Coherent planning
Training, engagement, public awareness People and engagement
Patient flows, governance, resources Business processes
Leadership, champions Leadership
Collaboration, patient-centred care Cultures and values
Code groupings Emerging themes
Figure 3: Code groupings and emerging themes
Further semi-structured interviews were undertaken with ACI staff to ascertain the implementation process
used to support the sites with SRP, barriers and enablers. This comprised face-to-face interviews with the ACI
Stroke Network Manager and the ACI Implementation Manager, and assessment of a written submission
provided by the ACI Implementation Officer involved with the SRP. The data has been coded into themes and
incorporated in the narrative in the Key findings from the site visits section and interviews section.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 21
Section 5 Stroke in NSW
Compared with the treatment of all strokes, stroke units where SRP is provided (over 50% of
all strokes) had a higher complexity of patients, an only slightly longer length of stay than
the NSW average and had experienced increased volume over the period 2007-08 to 2012-
13.
As the growth in volume started to occur before the formal implementation of the SRP, care
needs to be taken in terms of attribution. A number of factors may have influenced this
including the establishment of stroke units prior to the SRP, differences in access to post-
acute care, consolidation of stroke patients in formalised stroke units and transfer patterns
at non-stroke unit hospitals. Detailed work around attribution will occur in the next
evaluation stages.
Across NSW in the 2012-13 year, there were a total of 14,991 acute episodes of stroke with almost 51% presenting to
SRP sites. It needs to be noted that SRP services are part of formal stroke units and the data in this section reflects
all strokes as defined by the ICD list in Section 5. As noted, it is not possible, at this stage, to determine how many
of these strokes received thrombolysis.
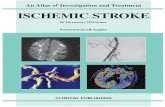
Using the average NWAU associated with the specified AR-DRGs as a proxy for complexity (with 1 being standard),
SRP sites combined are indicated to have patients with higher complexity than non-SRP sites at 1.9 and 1.2
respectively. The Royal Prince Alfred Hospital has the highest complexity of patients in this cohort as indicated by
the average NWAU at 2.5, followed by St George Hospital at 2.4 and Liverpool Hospital at 2.3.
Figure 4 shows the average NWAU per SRP site compared to the average NWAU for NSW in total, SRP sites in total
and non-SRP sites in total.
Figure 4: Average NWAU for SRP sites
Average NWAU for selected stroke DRGs by SRP sites 2012-13
SRP sites
0.0
0.5
1.0
1.5
2.0
2.5
Ave
rag
e N
WA
U
Concord
Hosp
ital
Blackt
own H
ospita
l
Wag
ga Wag
ga Bas
e Hosp
ital
Royal N
orth Sh
ore H
ospita
l
Wes
tmea
d Hosp
ital
Prin
ce o
f Wale
s Hosp
ital
St V
ince
nt’s H
ospita
l
Orange H
ealth
Serv
ice
Nepea
n Hosp
ital
John H
unter H
ospita
l
Hornsb
y Ku-R
ing-G
ai Hosp
ital
St G
eorg
e Hosp
ital
Liver
pool Hosp
ital
Banks
tow
n Hosp
ital
Royal P
rince
Alfr
ed H
ospita
l
Bathurst
Hosp
ital
Campbell
tow
n Hosp
ital
Gosford
Hosp
ital
Tam
worth B
ase H
ospita
l
Average NWAU by site NSW SRP Non-SRP

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 22
SRP sites had a slightly higher average length of stay compared to the NSW average and had a higher average
NWAU. This indicates that although the complexity of patients presenting at SRP sites was higher than the NSW
and non-SRP site averages, the length of stay was only minimally increased. This may be due to the timeliness of
stroke care provided at SRP sites indicating a more effective mode of service provision. This preliminary finding
is to be explored further in subsequent stages of the evaluation. The average length of stay varies across sites
with the NSW average at 6 days, SRP sites at 6.9 days and non-SRP sites at 5.2 days in 2012-13. The sites with the
highest average length of stay within SRP sites are generally those with higher complexity than the state and
combined SRP averages.
Royal North Shore Hospital had the highest volume of patients experiencing stroke in the 2012-13 year with 645
episodes (acute ICD codes) and accounting for 4.3% of all episodes for NSW and 8.4% of all episodes at SRP sites.
This is followed by St George Hospital, which had 626 acute episodes, accounting for 8.1% of all episodes
presenting to SRP sites, and Gosford Hospital, with 607 episodes and 7.9% of the SRP patient load for this cohort.
The intensity summary in Table 2 is shaded from white to dark crimson to emphasise the lowest to highest
scores in each column with white as the lowest score. Although all episodes of stroke presenting to NSW
hospitals have risen by 3%, from 14,229 in 2007-08 to 14,700 in 2012-13, stroke presentations to SRP sites have
risen by 14% in the same period, indicating that prior to the ‘‘go live’’ date (January 2013) of the SRP, diversion
to these sites was well underway.
Table 2: Summary activity by SRP site 2012-13
2012-13ACUTE
AR-DRGACUTE
ICD% NSW
ACUTE ICD% SRP
ACUTE ICDAVERAGE
NWAU ALOS
NSW combined 2012-13 14700 14991 100.0 1.5 7.5
Acute episodes SRP sites 2012-13 7516 7699 51.4 100.0 1.9 6.7
Acute episodes non-SRP sites 2012-13
7184 7292 48.6 0.0 1.2 5.2
Concord Hospital 354 359 2.4 4.7 2.0 8.3
Blacktown Hospital 403 405 2.7 5.3 1.6 6.4
Hornsby Ku-Ring-Gai Hospital 229 235 1.6 3.1 1.3 6.2
Wagga Wagga Base Hospital 255 263 1.8 3.4 1.4 5.0
St George Hospital 592 626 4.2 8.1 1.9 7.5
Royal North Shore Hospital 628 645 4.3 8.4 2.1 6.8
Liverpool Hospital 571 594 4.0 7.7 2.3 8.1
Westmead Hospital 552 564 3.8 7.3 2.0 6.3
Bankstown-Lidcombe Hospital 339 350 2.3 4.5 1.8 8.0
Prince of Wales Hospital 399 417 2.8 5.4 2.4 8.0
Royal Prince Alfred Hospital 433 443 3.0 5.8 2.5 7.8
St Vincent's Hospital 360 365 2.4 4.7 1.5 6.1
Bathurst Hospital 132 132 0.9 1.7 1.1 4.7
Orange Health Service 197 197 1.3 2.6 1.1 4.0
Campbelltown Hospital 297 298 2.0 3.9 1.4 6.8
Nepean Hospital 443 451 3.0 5.9 2.1 6.4
Gosford Hospital 594 607 4.0 7.9 1.3 5.7
John Hunter Hospital 549 554 3.7 7.2 2.1 7.3
Tamworth Base Hospital 189 194 1.3 2.5 1.5 6.5

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 23
From 2007-08 to 2012-13, the acute episodes for stroke by selected DRG had the highest volume in stroke and other
cerebrovascular disorders at 56,357 episodes for this period.
The ICD within these DRGs have remained relatively stable as shown in Figure 5 with cerebral infarction having the
highest volume as shown in the first graph. The second graph depicts the average length of stay for all acute
episodes within the selected codes showing a decline across NSW from 7.8 days in 2007-08 to 6 days in 2012-13.
It must be noted that although the first graph in Figure 5 shows the episodes by selected ICD-10 codes as all are
relevant to the presentation of stroke and subsequent assessment for thrombolysis, once condition is determined,
only cerebral infarction and stroke, not specified will be potentially amenable to thrombolysis.
The second graph in Figure 5 shows the length of stay for all selected ICD-10 codes to provide the broad context of
stroke care in NSW; however, subsequent analysis of length of stay by SRP site includes only those conditions
relevant to SRP – contained in Attachment II.
Figure 5: NSW ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13
Figure 6: SRP ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13
Similar to the NSW rates, cerebral infarction had the highest volume at SRP sites in total with 43,442 acute episodes
from 2007-08 to 2012-13. Consistent with the total NSW trend, in 2007-08, the average length of stay for these sites
was 8.8 days, which has declined steadily for all stroke types to 6.9 days in 2012-13. Figure 6 shows the episodes and
average length of stay for selected ICDs.
Deriving from these DRGs, the following tables shows the episodesand average length of stay by the specified ICD codes These have remained relatively stable from 2007/08 to 2012/13 with a total increase of 3.8 percent over this time period. The largest volume was for cerebral infarction with 5455 episodes in 2012/13.The average lengtyh of stay hase steadily decreased over this time period for all specified ICD with an overall average of 7.4 days in 2012/13.
07/08 to 2012/13 in NSW public hospitals.
me of episodes each year being for Stroke and other cerebral vascular disorders followed by TIA and cerebral occlusion.
0
1000
2000
3000
4000
5000
6000
2007/08 2008/09 2009/10 2010/11 2011/12 2012/13
Epis
od
es
Year
Stroke by ICD-10 NSW 2007/08 to 2012/13 Episodes and average length of stay
Other non-traumatic intracerebral haemorrhage
Stroke not specified
Intracerebral haemorrhage
Cerebral infarction.
Transient ischaemic attack
0
2
4
6
8
10
12
2007/08 2008/09 2009/10 2010/11 2011/12 2012/13
Days
Year
0
2000
4000
6000
8000
10000
12000
2007/08 2008/09 2009/10 2010/11 2011/12 2012/13
Episides
Year
Stroke by DRG NSW 2007/08 to 2012/13 Acute episodes
Cranial procedures
Extracranial vascular procedures
TIA and precerebral occlusion
Stroke and other cerebovascular disorders
0
500
1000
1500
2000
2500
3000
3500
4000
2007/08 2008/09 2009/10 2010/11 2011/12 2012/13
Epis
od
es
Year
Stroke by ICD-10 SRP sites 2007/08 to 2012/13 Acute episodes and average length of stay
Intracerebral haemorrhage Other non-traumatic intracerebral haemorrhage
Cerebral infarction Stroke not specified
Transient ischaemic attack
0
2
4
6
8
10
12
2007/08 2008/09 2009/10 2010/11 2011/12 2012/13
Days
Year

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 24
Non-SRP sites had a total of 44,503 acute episodes in selected ICD codes from 2007-08 to 2012-13 as depicted in
Figure 7, the highest volume being for TIA at 2,668 episodes in 2012-13. The average length of stay has steadily
declined from 6.9 days in 2007-08 to 5.2 days in 2012-13, with the biggest decline being for cerebral infarction from
10.4 days to 7.7 days over the same time period.
Figure 7: Non-SRP sites ICD-10 stroke episodes and average length of stay 2007-08 to 2012-13 2012/13
Cranial procedures
Extracranial vascular procedures
TIA and precerebral occlusion
Stroke and other cerebovascular disorders 0
500
1000
1500
2000
2500
3000
2007/08 2008/09 2009/10 2010/11 2011/12 2012/13
Epis
od
es
Year
Stroke by ICD-10 non SRP sites 2007/08 to 2012/13 Acute episodes and average length of stay
Other non-traumatic intracerebral haemorrhage
Stroke not specified
Intracerebral haemorrhage
Cerebral infarction
Transient ischaemic attack
0
2
4
6
8
10
12
2007/08 2008/09 2009/10 2010/11 2011/12 2012/13
Day
s
Year
0
500
1000
1500
2000
2500
3000
3500
4000
2007/08 2008/09 2009/10 2010/11 2011/12 2012/13
Epis
od
es
Year
Stroke by ICD-10 SRP sites 2007/08 to 2012/13 Acute episodes and average length of stay
Other non-traumatic intracerebral haemorrhage
Stroke not specified
Intracerebral haemorrhage
Cerebral infarction
Transient ischaemic attack

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 25
Section 6 Key findings from site visits and interviews
Table 3 shows a summary of the emergent themes emanating from site visits, interviews with
selected sites and interviews with ASNSW. The proceeding narrative provides an outline of the
key findings from these data and includes interviews with ACI Implementation Officers. The
results reflect the perspectives of the interview participants and until completion of Stage two
evaluation comprising quantitative analysis, provide a descriptive case study only forming part of
the baseline.
Table 3: Emerging themes
Emerging themes Issues raised Number of responses
Access to information Statewide consistency neededAbility to benchmark and share knowledge transferData collection system mandatedProvision of ASNSW FAST+ dataData collection established prior to program commencement Lack of ability to identify thrombolysis patients in administrative datasets
18 5 4 4 3 4
Coherent planning Limited impact of implementationPre-notification improved timeliness of treatmentSupport for program delivery and sustainability required
8 4 4
People and engagement Need for a public awareness and training campaign about stroke systems and time-critical treatment
3
Business processes Models of care to comprise key performance indicators (KPIs) rather than processes to enable flexibility Difficulty in timely transfer to ward
3 4
Leadership Perceived leadership of an evidence-based program (HNE)Local champions and leadersDistrict-wide leadership and coordinationACI and ECI leadership in promoting thrombolysis as standard care for stroke
5 3 3 4
Culture and values Positive relationships with ASNSWAdopting a patient-centred approach to stroke care
3 3
6.1 Access to information
Data has emerged as the major theme discussed by 17 of the 18 sites visited and by ASNSW. All of these discussions
included the need for a consistent and statewide data collection approach at a minimum with other emerging
themes around data concerning:
• the need for projects to have data collection systems in place prior to launching, with participating sites
mandated to use this as part of the program
• the provision of FAST+ patient data by ASNSW by site
• transparency of consistent data enabling sites to benchmark and share knowledge.
6.1.1 Research
Several sites noted a preference for using either existing national or worldwide datasets. Sites also referred to the
large number of data collections occurring for stroke including:

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 26
• Australian Stroke Clinical Registry (AuSCR) hosted through a partnership between the National Stroke
Foundation, George Institute for Global Health, Stroke Society of Australasia and the National Stroke Research
Institute (NSF website). The collection is aimed at monitoring quality improvements for stroke.
• Safe Implementation of Treatments in Stroke (SITS). This database is used by an international network of stroke
centres as part of a prospective, international, multicentre controlled study to determine the benefits and
safety of thrombolectomy and intravenous thrombolysis for stroke (SITS website).
• INSPIRE, an international stroke perfusion imaging registry providing a web-based data collection of imaging and
clinical stroke data to validate the use of CTP to refine the selection of patients for thrombolysis (SSA website).
• Thrombolysis ImPlementation in Stroke (TIPS) is hosted by the National Stroke Foundation aimed at evaluating
the effectiveness of thrombolysis for the treatment of stroke (SSA website).
In addition to these databases, the Australian Stroke Coalition (ASC) data and quality working group is working on
the development of the Australian Stroke Data Tool (AuSDaT) that will combine the AuSCR, INSPIRE, SITS and TIPS
as well as various telemedicine projects. The AusDat tool was released and is being rolled out to participating
hospitals throughout 2015.
These datasets have been established for research purposes and have an important function in collecting
information to enable national and international monitoring and evaluation of stroke care. SRP sites will continue
to be involved in and contribute to selected collections at the discretion of the participating site.
6.1.2 NSW administrative data requirements
Most sites have local data collections in place and several provide data to the research-orientated collections noted
above. It was noted by four sites that ACI should not develop a new database and suggested that ACI mandate use
of one of the existing databases to monitor the program. Five sites noted the importance of having consistent data
collection and reporting systems and retrieval to provide sites with the ability to benchmark against other sites and
to facilitate knowledge transfer of lessons learned. Three sites strongly stated that the official launch of the program
should not have occurred until a data collection system was in place to monitor and evaluate progress, and one site
noted that consistent data collections are essential for moving towards an accredited system for stroke services.
Due to the considerable onus that the establishment of another data collection system will place on sites, it is more
feasible to collect the relevant data required to enable collection and extraction of patient activity within the
existing statewide administrative datasets. Collection of this data will support identification of the patient cohort.
6.1.3 Patient outcome data
Four sites noted that ASNSW data showing FAST+ patients arriving by ambulance is needed for sites to monitor the
pre-notification system, the quantum of bypasses, accuracy of FAST+ diagnosis, and subsequent thrombolysis rates
and patient outcomes. ASNSW noted the need for sites to provide data to enable identification of any issues, with
the aim of resolving these issues quickly.
Thrombolysis treatment for stroke is not assigned with a dedicated DRG. This was raised by four sites as a potential
disincentive to thrombolysis as a standard of care for stroke patients. In response, ACI is working with the ABF
Taskforce to identify the resource requirements for stroke thrombolysis and to potentially establish a way to
identify the patient cohort in administrative datasets to address this. This may be adequately addressed through
the refinement of coding systems rather than establishing a dedicated DRG. Several options are being canvassed
and it is anticipated that this work will continue throughout Stage two of the evaluation.
In March 2014, the Australian Commission on Safety
and Quality released a consultation draft: Clinical
Care Standard for Stroke. The paper comprises seven
quality standards incorporating stroke assessment,
thrombolysis, acute stroke care, initiation of
rehabilitation, stroke prevention, carer training and
EDs and people who are seeing acute
patients don’t like to collect data for data’s sake
unless it’s going to drive their processes.“ “

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 27
support and individualised care plans. At a minimum, these standards, once endorsed, should form the basis of
KPIs for SRP sites in NSW and guide data collection requirements. The consultation draft can be accessed at
http://www.safetyandquality.gov.au/wp-content/uploads/2014/03/Full-version-Consultation-Draft-Clinical-Care-
Standard-for-Stroke.pdf.
Other issues raised with regard to data included the limited ability of the FirstNet system to track stroke patients
adequately, as it does not include time of onset data, and the need for sites to collect the National Institute of
Health Stroke Scale (NIHSS) information for all patients to enable assessment of patient outcomes. One site noted
that it is overly prescriptive for ACI to request data from sites at this stage of the program.
6.2 Coherent planning
The SRP initiative commenced in the MoH in 2010 and was handed over to ACI in 2012. The then DDG was the
executive sponsor of the program and ECI was involved in the design of the model through engagement on the
SRP Steering Committee. It was initially based on a successful program operating in the then HNE Area Health
Service that was achieving thrombolysis rates and times comparative to international best practice standards.
The ACI process involved the exploration of what was working well (the HNE model) to apply to the rest of NSW to
improve stroke care and address clinical variation and to design elements that were considered more relevant to
NSW as a whole (e.g. using FAST+ rather than the identification model used by HNE). At the time, it was estimated
that only 7% of stroke patients were receiving thrombolysis (NSF, 2010).
The MoH provided funding to ASNSW for FAST+ training for paramedics and for ACI to document the NSW SRP model.
Development of the program involved:
• establishment of a bypass system so that smaller sites that do not provide thrombolysis can be bypassed and
patients transported directly to SRP sites
• training paramedics in advanced stroke recognition to identify these patients (FAST+)
• development of a pre-notification system to enable acute stroke teams to be mobilised at the receiving sites
and imaging ready to complete required scans to determine eligibility for treatment.
The ACI adopted a redesign process and designed a model of care for the SRP based on aspects of the HNE
model and using the NSF Clinical Guidelines for Stroke Management 2010. Chief Executives of each District were
asked to identify services in place that would satisfy the requirements set out in the model of care followed by a
validation process of those sites identified. This comprised audits, site visits, discussions with clinicians and a
‘walk-through’ of the patient journey to assess each component of the model. To facilitate this process, an
implementation toolkit and self-assessment checklist were developed and disseminated to sites to assist in
service review and quality improvement.
Once endorsed for inclusion as an official SRP site, each CE was requested to nominate an executive sponsor, a
clinical champion and a project officer to support the program. Sites were tasked with establishing local
governance committees to facilitate the implementation and delivery process.
To support the process, the ASNSW undertook workload modelling to project patient flows to SRP sites once
the bypass system was in place to enable planning by sites. At the time, it was reported that discussion occurred
around measuring for effectiveness and quality improvement; however, agreement was not reached on what
systems should be used, resulting in the program launched without clear data collection requirements.
A 12-month time-limited community of practice was established comprising SRP sites and hosted by ACI
(through a regularly scheduled teleconference) to provide a forum for discussion of lessons learned, knowledge
exchange, processes and issues arising. Attendees at this forum changed over time.
It was reported by ACI staff that major factors facilitating success of the implementation process included:

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 28
• support for the program by all levels of the LHDs from clinicians to executive members
• establishment of local governance arrangements
• the collaborative approach adopted by the ACI Implementation Team, Stroke Network Manager, ASNSW and
ACI Stroke Network in developing the specific SRP model of care and visiting sites to support local
implementation.
In relation to the ACI involvement in implementation, there were several key issues, as outlined below.
• A large number of sites considered the ‘‘go live’’ date in January 2013 to comprise the ASNSW pre-notification
system only. Accordingly, eight sites noted that the implementation processes employed by ACI had little or no
impact on their existing services although four sites said that the pre-notification system was instrumental in
improving patient transport times from onset to hospital.
• Two sites noted that the ACI implementation process assisted in gaining executive support for SRP at the local
level and in reviewing current service delivery.
• Four sites perceived the support provided by ACI to be relatively minimal and would have preferred an ongoing
structure to support delivery and sustainability of the program.
• One site noted that the ACI process assisted in overcoming the resistance to thrombolysis held by ED physicians
through the provision of leadership of thrombolysis as standard stroke care, while another site noted the
importance of ACI involvement in the adoption of a standardised tool (FAST+).
Separate from the implementation process, many sites mentioned the ongoing support provided by the ACI Stroke
Network Manager and the ASNSW Program Manager as a positive contribution to the program.
It must be noted that interview participants at sites consisted primarily of clinicians from stroke units, neurology
and emergency departments, and therefore may not be reflective of the perceptions held by administrators. In
addressing this potential bias, it is suggested that a small number of group interviews with LHD administrators
occurs at Stage two of the evaluation to expand the dataset surrounding the implementation process.
6.3 People and engagement
The need for ongoing public awareness campaigns was
raised by all of the rural services visited. It was perceived
that the information about stroke incorporates acute
symptoms only and the message about how time-critical
it is to seek treatment is not portrayed. As a result, rural
sites spoke of situations where patients did not
recognise symptoms and consequently, help was sought
too late for patients to be eligible for thrombolysis.
6.4 Business processes
Several themes specific to rural sites emerged throughout the site visit processes. These included the need for
flexible models of care that can be locally translated to each site and specifically to the needs of rural sites. This
would involve the establishment of shared principles around specific programs and development of a succinct set of
key performance indicators rather than prescriptive processes. As noted by all of the rural sites visited, flexibility for
LHDs to determine service structures will increase access to services for rural people and buy-in for local clinicians.
Vast distances in rural areas affect the time that patients arrive at designated SRP sites, as raised by two sites. Both
of these sites discussed concerns that there are other sites that provide thrombolysis treatment for stroke that may
be closer to the patient’s home but as they are not specifically identified as part of the SRP, predominantly due to
operating in business hours only, they are bypassed, resulting in longer transport times. This prompted further
discussion around the need for flexibility in models of care, as discussed above, and a review of the ambulance
bypass system.
The bigger hospitals, they have the
formal meetings. The smaller hospitals, they
have a cup of coffee and know what’s
happening in ward 5.
“ “

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 29
6.4.1 NSW Health Matrix
The principle relating to the Matrix system is that each ED will accept emergency patients from ambulance
consistent with clinical specialities offered on site and from within the respective hospital catchments.
There were no emerging themes relating to the Matrix system in relation to stroke, however it was raised by several
sites and ASNSW. The most prominent issue was raised by two sites concerning the lack of Matrix coverage in rural
areas. Discussion ensued around the need for the Matrix to include stroke on a statewide basis and concern was
raised with regards to limited awareness of the SRP in rural, non-SRP sites. It was perceived that this may delay
treatment for some patients as they may not be transferred to ATC and acute stroke unit (ASU) sites. It was also
noted that there are inherent difficulties in implementing a statewide protocol (pre-notification) because of the
diversity of sites with differing operational systems, pathways and awareness.
ASNSW discussed the benefits of establishing helicopter transport in rural sites for time-critical emergencies, such as
stroke. The use of helicopters for acute stroke patient transport has been used in the HNE District and is currently
under review.
One metropolitan site raised concerns about the apparent opaqueness of the Matrix and suggested that several
patients incorrectly classified as FAST+ are regularly transported to an ED outside of their district. However, without
access to FAST+ and local site data, this has not been quantified. This will be pursued further in Stage two when
data is provided. It was noted that the Matrix substantially increased the throughput of stroke patients to
participating sites, but limited data availability has resulted in the site not having the evidence to support an
increase in ASU beds.
Two metropolitan sites advocated for a review of the Matrix to enable an equitable work distribution among sites
in the catchment areas. The Matrix is reviewed every two years and required amendments are made at these times.
6.4.2 Repatriation
Repatriation of patients back to their local hospitals (where appropriate in relation to their respective care
requirements) is a component of the SRP model. Although issues of repatriation were not raised as emerging
themes, concerns are important for further discussion. Two sites, one metropolitan and one rural, discussed the
difficulties of transferring patients back to their local area, and in the case of the metropolitan site, back to the
patient’s LHD. This was noted to be due to bed shortages, minimum neurological support in smaller outlying areas
and the wishes of patients to remain in place and not start care at a new service.
An important issue was raised by one site in terms of repatriation and rehabilitation. There is substantial evidence
to support early rehabilitation for stroke patients (see, for example, AIHW, 2013). However, if a patient is to be
repatriated back to their local facility, it was noted that rehabilitation plans are not started at the first site, and
instead, are developed at the local facility. This delay in rehabilitative support is considered potentially detrimental
for the patient.
6.4.3 Treatment
There were three emergent themes regarding treatment for stroke patients. The first is the inequity of care
between BH and AH and the second the timely transfer of patients from ED to ward – both are discussed in the
section on Key findings from SRAT review in the next chapter. The third theme raised by three sites is a call for ACI
and ECI to provide leadership in promoting thrombolysis as standard care for eligible stroke patients. Other sites
identified some scepticism of the treatment, particularly amongst ED physicians, however did not feel that this
delayed or hindered the treatment as it was now accepted as standard care.
Two sites discussed the perceived accuracy of the FAST+ tool, noting that this was difficult to determine without
analysing the data. It was suggested that once accuracy is defined, this could be compared against that of the tool
used in the HNE LHD, with a view to adopting the most effective tool. However, sound evidence is required prior to
changing tools. In general, most sites were satisfied with the FAST+ assessments and several noted that accuracy has
improved as paramedic training has progressed.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 30
Issues raised in terms of resourcing comprised the ability of sites to recruit and maintain staff with specific stroke
care skills and the subsequent, substantial workload of neurologists. This is particularly pertinent to rural sites that
do not have the throughput of patients to keep staff skills current.
6.5 Leadership
There were several emergent themes with regard to what sites considered enablers for the success of SRP. Due to
the lack of program data availability, these factors have not been analysed against progress indicators at this stage
of the evaluation.
The leadership provided by the HNE LHD in the development and delivery of the program was raised by five sites as
a success factor in the acceptance of thrombolysis as standard practice in treating stroke, alongside confidence
derived from the ongoing research and improvement. It was stated that ongoing research has ensured that the
program has been supported by a sound evidence base from its inception to its current iteration.
Local champions and leaders were seen to be pivotal in the success of the program in raising its profile and
acceptance. Three sites noted that District-wide leadership and service coordination has contributed substantially
towards the success of the program. This included the:
• support provided to the Sydney Adventist Hospital from Royal North Shore Hospital in installing the program
• shared protocols, pathways, coordination and medical staff across Liverpool, Bankstown-Lidcombe and
Campbelltown Hospitals
• delivery of a hub-and-spoke model of stroke care from Orange Hospital to the outlying facilities
• coordinated stroke care by Concord and Royal Prince Alfred Hospitals across the District including an outreach
stroke care team comprising allied health staff streamlining the patient journey across the continuum of care.
Two sites noted that there is a lack of coordination within their respective Districts resulting in difficulties for
consultants who work across the sites. Work was progressing in one site to develop a coordinated approach to SRP.
The three sites raising ACI and ECI leadership in this area stated that cultural changes will occur if thrombolysis is
promoted by lead agencies as a standard care for stroke. This is considered important for raising awareness about
stroke care outside of SRPs to ensure that contracted staff provide suitable care while working in SRP sites.
6.6 Culture and values
A positive relationship between sites and ASNSW was an emergent theme and considered a good indicator of
program success by several sites. At these same sites it was noted that ASNSW is involved in local site committees,
feedback is provided and sought by paramedics and regular contact with the ASNSW Program Manager is
maintained. Similarly, ASNSW discussed the importance of feedback loops and providing paramedics with patient
outcomes in a timely manner. Feedback loops informing paramedics of patient outcomes (for those arriving by
ambulance) are provided by the site within 48 hours in a formalised process in the HNE model. It is unclear why this
was not translated into the SRP model, and it has been suggested that its inclusion be reviewed and considered.
Taking a patient-centred approach to stroke care emerged as a strong theme throughout the site visits and is seen
as a success factor for SRP. However, although raised as a success factor, no site reported that patient-centred care
was an ongoing and formalised component of SRP delivery at their site. Patient-centred care was described as all
staff and units taking ownership and responsibility for patient stroke care from ambulance to ED staff, radiology,
stroke units and rehabilitation. Several sites noted that responsibility for stroke care is seen as a function of
neurology, rather than a shared responsibility, and suggested that clear mapping of the patient journey at each site
and identification of what each staff or unit contributes to that would be a good starting point for dialogue and
ensuing cultural shifts.
This is consistent with the ASNSW view that paramedics are part of the patient healthcare journey, not just the
transport. It was suggested by one site that ACI take a coordinating role in facilitating this process by bringing
people who contribute to the patient stroke care journey together to progress discussion. This was considered a

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 31
larger membership than that currently involved in the Stroke Network. However, if people don’t currently consider
their roles to be core to stroke care, they are unlikely to attend such a meeting. It may be a more viable option to
consider establishing a small, key team of people comprising representatives from ACI Stroke Network, ASNSW, ACI
and ECI, and Allied Health to map out the change management process for cultural shifts in patient care
responsibility prior to broadening the dialogue to sites.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 32
Section 7 Key findings from SRAT review
7.1 Stroke Reperfusion Assessment Tool
The implementation of the SRP was based on a consistent service redesign approach indicating fidelity of
implementation processes as noted in the section above. However, as documented in the summary SRAT table (at
Appendix 1), there is a diversity of approaches adopted at sites and differences across metropolitan and rural areas
signifying infidelity in program delivery. This chapter provides an overview of each site that has participated in the
SRP evaluation Stage one.
Inpatient descriptive statistics (episodes of care and length of stay) are contained in Appendix II. Although most
sites stated that thrombolysis has been occurring prior to the formal implementation of SRP, improved rates of
thrombolysis (anecdotal) have been associated with improved pre-hospital identification and faster transfer of
patients to dedicated SRP sites. A full assessment of this requires consistent data. Further information, particularly
concerning site-specific patient data, will be assessed and reported in Stage two.
7.1.1 Gosford Hospital
Gosford Hospital has had an acute stroke team and has been thrombolysing people for several years prior to the
‘‘go live’’ date of the SRP. Pre-notification by ASNSW has been in place prior to the SRP and this comprises pre-
notification directly to the Acute Stroke Team rather than to ED. Gosford Hospital reported a close working
relationship with ASNSW, which was viewed as having positive benefits for the program.
Barriers identified in the SRP Pathway included blockages to radiology for imaging, for example, imaging is not
pre-notified of the imminent arrival of FAST+ and stroke patients.
There is no stroke reperfusion or general stroke governance committee in place at Gosford Hospital. It was
acknowledged that the establishment of such a body would provide value through the oversight of all components
of the patient journey, and ensure clear and consistent guidelines and criteria for each stage, monitoring and
addressing issues arising. This includes the ability to address potential blockages in imaging and the inclusion of EDs
as partners in the SRP to foster increased connection with the program. It was reported that the site is considering
the establishment of an SRP governance committee in the near future. The inclusion of a local governance structure
is a required component of formal SRP recognition. Patients are discussed at standard ED Mortality and Morbidity
(M&M) meetings, as required.
7.1.2 Nepean Hospital
Nepean Hospital reported that thrombolysis treatment had been occurring for several years prior to the official ‘‘go
live’’ of the SRP, and pathways and systems are consequently well established. Pre-notification of incoming FAST+
patients occurs from ambulance to ED and ED notifies the Stroke Team once diagnosis is verified by ED.
The patient pathways are the same after hours although processes differ by way of treatment lead. Within hours,
the Stroke Team leads the process once notified by ED. After hours, the process is led by ED. Stroke patients are
prioritised for scanning. However, access to scans is seen as the program component with the largest delay.
Regular in-services and training are provided to nurses and through the orientation of medical staff. At the
commencement of the SRP involving ASNSW, a stroke steering committee was established. However, this
committee has not met for almost 12 months.
Barriers reported included access to neurologists AH and difficulties encountered with limited and changing
staffing. On-call neurologists resided at a distance from the hospital, and consequently, delays were often
experienced in their arrival to assess patients. As a result, there has been an occasion when thrombolysis treatment
was administered by ED prior to neurology assessment. To address this issue, the hospital has now installed
telehealth facilities into the ED, and although a recent action, it is reported as a successful strategy in accessing
neurologists in a timely manner.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 33
Nepean Hospital has had difficulty in attracting and maintaining neurologists over the past year. This transpired as
a major barrier in having no constant clinical champions or leadership for the SRP. The hospital is in the process of
engaging a team of neurologists and this is considered a major step to future program improvements through the
establishment of champions and leadership, reconvening the Stroke Committee (with the inclusion of ASNSW) to
provide governance, monitoring and facilitating broader awareness, education of best practice and importance of
time for thrombolysis treatment for stroke. The former Stroke Committee has been convened only once since the
‘‘go live’’ SRP date. Patients are discussed at regular ED and Neurology M&M meetings, as required.
7.1.3 Campbelltown Hospital
A 24/7 acute stroke service was in place at Campbelltown Hospital prior to SRP implementation in January 2013.
The official launch of the SRP assisted in providing validity to the program across all units involved in the patients’
journey. The current DTN time is reported at an average of 70 minutes.
A comprehensive training program occurs with the training of medical registrars in stroke and thrombolysis
treatment as part of the St Vincent’s – Wollongong Network orientation. A theory-based in-service accompanied
by an exam is held for nurses using a ‘train the trainer’ model, as well as training for ICU staff to enable
thrombolysis within the ICU.
Issues for ASNSW in the bypass system were reported stating that patients identified as FAST+ in the
Wingecarribee area bypass Bowral Hospital and go to Campbelltown or Liverpool. This potentially puts pressure
on the only two ambulances located in that area when transporting patients the considerable distance to the SRP
sites. Discussion ensued regarding possible assessment of patients at Bowral to confirm eligibility for thrombolysis
prior to transporting as a way to alleviate this problem. However, this would require access to a computed
tomography (CT) scanner. It was agreed that further discussion is needed to address this and similar issues at a
statewide level.
Another barrier identified concerned the lack of pathways and policies for patients in which thrombolysis doesn’t
work, i.e. for those requiring intra-arterial thrombolysis or thrombolectomy. This was suggested as the next phase
of the SRP development.
Campbelltown Hospital is part of a District-wide stroke service providing 24/7 thrombolysis, along with Liverpool
and Bankstown-Lidcombe Hospitals. This is reported as a SRP success due to District-wide knowledge sharing and
collaboration, localised flow charts reflecting different processes of care in each hospital underpinned by District-
wide policies, data collection, education packages and governance. The District is now aiming towards
standardised thrombolysis protocols across the District to complement the program. Medical teams are also shared
across the District enabling seamless patient transfers, where required, and shared agreement on tests, treatments
and approaches. This teamwork is reported as a major facilitator of the success of the SRP, with the ASNSW seen as
a major part of the team.
The Stroke Committee is District-wide and meets regularly as the governance body for the SRP. Patients are also
discussed at regular M&M meetings and the ED Neurology meetings, as required.
7.1.4 Orange Health Service
Orange Hospital has been operating a 24/7 stroke and thrombolysis service for several years. The internal pathways
for stroke care have remained relatively stable over that time. However, the official launch of the SRP enabled
Orange Hospital to develop external pathways for peripheral hospitals. This has established a hub-and-spoke model
resulting in more timely transfer and effective stroke care.
The Orange Hospital SRP is based in Cardiology. Neurologists working in the area are primarily room-based,
providing consultancy to the hospital and not available for on-call services. This has highlighted barriers to the AH
SRP that relies on on-call medical staff and Cardiology without leadership from Neurology. It was reported that this
limitation in staffing has resulted in several physicians being involved in thrombolysis, and due to the small
throughput, it is difficult to maintain practical skills, and therefore to sustain the program effectively.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 34
Internal education is provided to medical registrars and Cardiology on a regular basis. In-services for nurses occur
regularly and through the orientation program.
Education of the peripheral hospitals has been identified as a success factor in the SRP at Orange Hospital. Sites
and general practitioners (GPs) are becoming increasingly aware of the time-critical nature of thrombolysis
treatment and transfer times are reported to be decreasing. A local evaluation of this is in progress and will be
used to guide service improvements across the sites.
Regular feedback to peripheral hospitals and GPs is suggested as a successful strategy to increase engagement and
education through the benchmarking of diagnosis, transfer times and outcomes across the spokes.
Stroke Committee and Patient Safety Meetings occur on a monthly basis and act as the local governance structure
for SRP. Patients are also discussed at regular M&M meetings, as required.
7.1.5 Bathurst Base Hospital
Similar to the Orange Health Service, Bathurst Base Hospital works on a hub-and-spoke model with peripheral
sites. The peripheral feeder hospitals include Rylstone, Blayney and Oberon. Although Lithgow is out of the LHD,
an increase in presentations from there has occurred due to the SRP FAST+ protocol being implemented.
Bathurst Base Hospital does not have a neurology service and relies significantly on locum, fly in/fly out staff,
particularly in ED. The need for stroke care and thrombolysis treatment to be standardised is therefore paramount
to ensure all attending staff are aware of practices and time-critical processes. Standardised care is seen as
essential in ensuring that staff at any hospital follow best practice in stroke care, inclusive of thrombolysis
treatment, not just those at designated sites.
Access to scans was reported as the program component where delays are most likely to occur. However, it was
noted that delays are shorter AH.
Internal education is provided to ED nurses and registrars at regular sessions. However, the nature of the rural
workforce and locum staff means that not all staff are adequately trained and aware of stroke care or thrombolysis.
Ongoing education was considered the biggest barrier to the effective delivery of SRP, particularly education
provided to peripheral sites and GPs. It was noted that the importance of timely transfer and GP referral requires
ongoing dialogue.
Similar to Orange Hospital, the Bathurst Base Hospital has monthly Stroke Committee and Patient Safely
Committee meetings that act as the governance structure for SRP. Patients are also discussed at regular M&M
meetings, where required.
7.1.6 St Vincent’s Hospital
St Vincent’s Hospital was the site of the official launch of SRP and commenced thrombolysis in 2003. It has a
well-established system for stroke care consistent with the requirements outlined in the SRP.
A comprehensive training program is in place at St Vincent’s Hospital comprising regular in-services for ED nurses
and registrars and orientation at triage. The Hospital has a simulation centre and provides six-monthly training for
ED consultants, registrars and nurses, and provides a six-monthly didactic lecture.
Collecting patient history was reported as a barrier to timeliness of the SRP. It was stated that this may take
considerable time once a patient arrives at ED, potentially resulting in treatment delays. It was considered more
successful when patient history is collected in transit and provided to ED along with the patient. However, it is
acknowledged that this is not always possible.
The SRP governance structure at St Vincent’s Hospital comprises a monthly governance, quality and variation
meeting where all aspects of the program are discussed. Patients are also discussed at regular M&M meetings,
where required.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 35
7.1.7 Royal Prince Alfred Hospital
Royal Prince Alfred Hospital has been thrombolysing for stroke since 2000 and has well-established stroke care services, policies and pathways in place.
Training occurs every two months for all ED staff, on grand rounds for RMOs and during orientation for all hospital staff.
Stroke patients have priority for scanning. However, delays in scans have been identified as a potential barrier. It was reported that the journey for the patient works well from ambulance to ED and although radiology is pre-notified of potential stroke patients, ordering of scans is digital and cannot occur until registration, as registration and medical record numbers are required to generate the order. Discussions to find a viable solution are ongoing.
Previous delays in scans were identified resulting from neurology requests for labour-intensive diffusion/perfusion contrast studies. Consequent discussions resulted in agreement that non-contrast brain scans would be the standard and any decision about the need for more esoteric scanning would be made on a case-by-case basis. This reportedly decreased times significantly.
The success of the program was reported to include use of data for continuous improvement. Any DTN time beyond 60 minutes is interrogated to identify delays and remedied accordingly (average DTN currently 55 minutes).
The collaborative relationships across ambulance, ED, radiology and neurology was stated as a major facilitator of success and this is considered to be strengthened by other work involving partnerships between ED and neurology for several clinical trials.
The Royal Prince Alfred Hospital holds quarterly meetings as the governance structure for the SRP and provides reports about the program to the Executive and the Clinical Council. Attendants at quarterly meetings include ASNSW, ED Nursing, ED Medical Staff, Radiology, ICU Staff, Stroke Ward NUM, Rehabilitation Staff, Neurologists and Allied Health.
Patients are also discussed at regular M&M meetings.
7.1.8 Prince of Wales Hospital
The Prince of Wales Hospital commenced stroke thrombolysis in 2006. The ED is pre-notified of incoming FAST+ stroke patients, however the stroke team is not pre-notified. ED assesses patients to confirm diagnosis prior to notifying the stroke team. This notification includes medical imaging.
The SRP has clear policies and procedures in place and undertakes regular monitoring of KPIs through quality, morbidity and mortality meetings. Training and orientation is provided in ED to new nursing graduates and in-services.
Brain scans that contribute to the determination of a patient’s eligibility for thrombolysis vary in type requested across staff and a need for consistency was raised to facilitate accurate, but timely treatment.
Some feedback is provided to ASNSW, primarily concerning missed FAST+ patients and those incorrectly diagnosed. However, this is not a formalised process. Similarly, there is no formal feedback mechanism from the stroke unit to ED concerning patient outcomes.
After-hours access to scanning was reported as a barrier to timely administration of treatment and it was noted that staff education and cultural change is required to provide a seamless service across all aspects of the patient journey. The ACI has worked with Prince of Wales Hospital to review the SRP in depth resulting in a series of recommendations to improve the program.
The governance structure for SRP at Prince of Wales Hospital comprises regular meetings for stroke with membership from Neurology, ED and Imaging.
7.1.9 Bankstown-Lidcombe Hospital
Bankstown/Lidcombe Hospital has been offering stroke thrombolysis in BH since 2008. This expanded into a 24/7 service in 2011 and is part of the District-wide stroke care. The SRP at Bankstown/Lidcombe Hospital now has revised processes enabling neurologists to provide remote consent for thrombolysis treatment rather than having to attend the hospital. This has reportedly streamlined the SRP considerably.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 36
Education is embedded into ED orientation and junior medical officer teaching and nurse orientation training.
Thrombolysis training is undertaken by nurses to enable administering of thrombolysis. The current mean door-to-
needle time is reported as approximately 50 minutes.
Success factors of the SRP at Bankstown-Lidcombe are reported as the collaborative working relationships across
the different components of the program. Radiology is considered an asset in prioritising stroke patients and clear
policies that are in place facilitate the smooth operation from arrival to discharge.
The SRP governance committee for Bankstown-Lidcombe Hospital meets bi-monthly and includes membership from ED,
Neurology, the Stroke Team, and the District Stroke Liaison Officer. Patients are also discussed at regular M&M meetings.
7.1.10 Westmead Hospital
Westmead has been thrombolysing people for stroke for several years and in the 2013/14 year, had a median DTN
time (in BH) of 52 minutes for the 39 patients thrombolysed, with the fastest at 17 minutes. The median door-to-
imaging time for the same period was 12 minutes. The Hospital is increasing the number of FAST+ patients taken
directly from ambulance to radiology for scans, although this has not yet been formalised.
Westmead Hospital provides ongoing ED training in stroke care and thrombolysis and an annual formal induction
for registrars on the stroke roster. In BH, stroke is led by the stroke registrar; AH, there is an age split, with patients
aged 70 years and over having treatment led by the on-call geriatrician, and those under 70 years, by the on-call
neurologist.
A barrier identified was the differential in consultants’ diagnostic preferences for scans, and another is access to the
drug for thrombolysis treatment. Being expensive, it is located in a locked cupboard and there are protocols that
must be followed for access, which may reportedly delay treatment. Westmead Hospital also identified difficulties
in patient transfer from ED to the stroke unit due to bed blockages.
Westmead Hospital does not have a specific governance structure for SRP in place. Patients are discussed at regular
M&M meetings.
7.1.11 Liverpool Hospital
Liverpool Hospital started thrombolysing in 2004 as a 9-to-5 service, gradually expanding to a 24/7 program.
Average DTN time is reportedly 40–50 minutes within BH, and similar to many other SRP sites, longer AH with an
estimated average of 100 minutes. The reasons noted for this inequity between in and out of hours include travel
time for stroke consultants and registrars to arrive at the hospital and the ED decision to not pre-notify AH until a
patient is assessed and diagnosis confirmed. The stroke consultant can read a scan remotely, but still undertakes an
on-site stroke medical assessment.
Access to radiology was reported as good, although can be tightened to improve time. The need for radiographers
to respond to AH pages and faster pathology were discussed as requirements for streamlining the service.
Training and orientation occurs regularly for ED nursing, junior medical officers and registrars. Nursing uses a
train-the-trainer model enabling the ongoing orientation of staff. Additionally, ED nurses have been trained in
administering thrombolysis treatment, which has resulted in improved DTN time. It was reported that further
internal education would raise awareness about the SRP, and consequently, involvement of the Acute Stroke Team
in internal strokes.
Cohesion across the District was raised as the success of the program effectively facilitated a “learn and share”
model, an avenue for solving any issues and development of shared protocols.
The committee established as the governance structure for SRP at Liverpool Hospital has convened only twice since
the ‘‘go live’’ date in January 2013. However, quarterly District-wide stroke meetings do occur and act as an
overarching governance structure for the program. Meetings are attended by ASNSW, Administration, Neurology,
Medical and Nursing, ED and Allied Health. Patients are also discussed at M&M meetings as required.
7.1.12 Royal North Shore Hospital

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 37
Royal North Shore Hospital commenced thrombolysing patients for stroke approximately 10 years ago. In the 2013 calendar year, the service reportedly thrombolysed 51 patients, or 20% of patients presenting with ischaemic stroke.
Royal North Shore Hospital provides orientation and education through in-services to ED nursing, registrars, ED medical and stroke unit staff. All training occurred on a six-weekly rotating roster. However, it now occurs as needed as staff are aware of the processes. Registrars receive three-monthly training to ensure coverage with staff changes.
The site undertakes advanced imaging which adds an estimated 20 minutes to treatment time. To address this, treatment for eligible patients starts in radiology or ED. Once treatment starts, patients are not moved until completion to minimise treatment error potentially caused by perfusion pump vial sizes. The pumps take only 50mg syringes. Whilst most patients require 60mg of medication, so a further syringe is required, and if the patient is transferred, there is potential for receiving staff to assume that the completion of the first syringe is all that is required.
The cost of the thrombolysis medication was identified as a barrier to its use, because the medication is required to be stored in a locked cabinet requiring dual identification for access. In addressing this, medication is now placed in a thrombolysis bag that accompanies the patient to radiology, effectively streamlining the process.
The Stroke Team meets regularly, forming the governance structure for SRP at Royal North Shore Hospital. As staff share the same physical office location, they also meet informally, as required, and patients are discussed at regular M&M meetings. The Stroke Team meetings comprise the Director of Stroke Network, Clinical Nurse Consultants (CNCs), Stroke Fellow, Data Manager and the Area Coordinator.
7.1.13 Sydney Adventist Hospital
The Sydney Adventist Hospital commenced acute stroke services in 2005 and established protocols and pathways to
guide service provision. A major review of stroke services was completed in 2012 resulting in changes to AH imaging
to streamline the process. This comprised formal agreement for scanners to operate 24/7 without requiring the
on-call radiologist to be contacted. Neurologists review scans AH, which are then formally reported by the
radiologist during BH. It was reported that an estimated 12% of FAST+ patients are thrombolysed.
The Sydney Adventist Hospital does not have an AH Acute Stroke Team registrar. After-hours services for acute
stroke are led by the senior doctor in ED with direct consultation from an on-call neurologist. The hospital does
treat public patients for stroke. Once stabilised, these patients are transferred to a suitable facility, such as Hornsby
Ku-Ring-Gai Hospital.
Orientation to stroke care and thrombolysis occurs for new staff through stroke workshops, and refreshers are held
as needed.
Sydney Adventist Hospital is working towards installation of a full location tracking system of patients and chores.
This consists of radio monitoring systems located throughout the hospital and has the potential to accurately track
the journey and treatment of stroke patients.
The committee that forms the governance structure for the SRP at Sydney Adventist Hospital convenes six-monthly
and includes Emergency Staff, Medical Officers, Neurology, Neuroscience Nurse Unit Manager (NUM) and other
invitees, as required. Patients are also discussed on a regular basis at Neurology Section meetings.
Sydney Adventist Hospital is a private hospital. Therefore, ACI does not have direct access to admitted inpatient
data for the site, but the hospital is providing data to the ACI from 1 October 2014 and this will be used for Stage
two of the evaluation.
7.1.14 St George Hospital
St George Hospital has had a stroke unit for many years and commenced thrombolysing for stroke in 2007. It is the
southernmost thrombolysis service in the metropolitan area and receives patients from Wollongong, Canterbury
and Sutherland.
St George Hospital reportedly thrombolyses an estimated 10–15% of patients arriving with stroke calls with the best
DTN time in the past year recorded at 18 minutes.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 38
Training is provided on stroke care and thrombolysis through regular in-services to ED staff and at orientation
as new registrars commence at the hospital.
A major barrier for the service has been identified as the limitations to repatriating patients back to their local
area due to bed capacity issues. There are also issues regarding limited rehabilitation services in the patients’
local area, further impacting on repatriation.
The St George Hospital SRP is a busy service and the strict rules enforced on admission to the stroke unit have
been identified as a success factor. All admissions must be reviewed and approved by the neurologists.
The bi-monthly St George Hospital Stroke meetings acts as the governance structure for the SRP. Additionally,
each department has separate meetings and interdepartmental meetings occur, as required. Patients are
discussed at regular M&M meetings.
7.1.15 Wagga Wagga Base Hospital
The Wagga Wagga Base Hospital commenced thrombolysing for stroke in 2008. The service was regarded as
well-established by the time the SRP was officially launched in 2013.
The hospital shares registrars with Campbelltown and St Vincent’s Hospital and each year the stroke consultant
travels to Sydney to meet with those that will be going to Wagga Wagga. The meeting comprises a full day of
stroke and thrombolysis management orientation.
Additional training occurs regularly with ED junior medical staff, as well as orientation and training for nursing
staff in administering thrombolysis. Emergency department nurses have completed NET SMART online training
– a series of modules for stroke management associated with the TIPS trial.
Thrombolysis treatment occurs in ED prior to the patient being transferred to the high-dependency unit (HDU)
or acute stroke ward. The DTN time was reported to be on average 60 minutes with the door-to-scan time an
average of 24 minutes. Thrombolysis rates were noted as increasing from 3.7% of patients presenting with
ischaemic stroke in 2012 to 8.9% in 2013.
Radiology prioritises stroke patients, enabling streamlining of the service. This was enhanced in early 2014 with
the commencement of an advanced stroke trainee, effectively enabling this position to assess the patient on
site, while the neurologist can read scans remotely.
Similar to other sites, Wagga Wagga Base Hospital reported that there was an initial barrier to the SRP in ED
with the acronym FAST. In ED, FAST refers to a Focussed Abdominal Sonographic Trauma Exam and it has taken
some time to differentiate between this and stroke FAST+.
Delays in transfers from outlying hospitals were noted as a barrier to timely treatment. It was reported that
several patients were transported to the closest hospital rather than bypassed to the ASU. Wagga Wagga Base
Hospital has a large catchment area covering Griffith, Leeton, West Wyalong, Young, Lockhart, Nanandera and
Loxton. Thus, timely transfer to the appropriate service is crucial for treatment.
Community awareness of stroke FAST was raised as a major concern with an internal evaluation indicating that
of 132 patients experiencing ischaemic stroke, only 8% were aware of the FAST symptoms.
The governance structure for SRP at Wagga Wagga Base Hospital is the Executive Stroke meeting that occurs
bi-monthly. This comprises participation by the Stroke Consultant, Stroke Unit NUM, an Executive
representative, Allied Health and a Consumer representative. Patients are discussed at regular M&M meetings,
as necessary.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 39
7.1.16 Hornsby and Ku-Ring-Gai Hospital
The Hornsby and Ku-Ring-Gai Hospital has been operating an acute stroke and thrombolysis service for several
years. The site reportedly thrombolyses approximately 10 to 12 patients per annum for stroke. The current
average DTN time was reported to be approximately 60 minutes.
Regular orientation and education occurs via in-services for ED staff and any changes to the pathways are
discussed with all staff. There is a stroke website that is consistently updated with information.
A recent LHD initiative has embedded e-copies of useful thrombolysis tools in the local Firstnet (in ‘ad-hoc
charting’) i.e. NIHSS, a version of inclusion and exclusion criteria and a decision-assist tool for treatment of
ischaemic stroke, including management of blood pressure etc.
Door-to-needle time can be improved.
• A CPI project is underway to facilitate improved rates of neurology-alert from the triage desk i.e. to include
FAST+ as an emergency-call alert (via the ‘33’ call to ‘Switch’).
• Order of initial CT: to address a particular delay in CT image availability, staff are now required to order CTs
and CT angiograms separately. If ordered together, the images can take up to 30 minutes longer to process.
• Strategies to prioritise and expedite pathology (‘bloods’) for stroke patients are being reviewed.
A small, local stroke meeting is used as the governance structure for the SRP. This meets quarterly. The meetings
include Stroke Unit NUM and ED staff. The neurologist at Hornsby and Ku-Ring-Gai Hospital is a Visiting Medical
Officer (VMO) and attends and chairs the meetings.
Eligible and thrombolysed patients are mini-case-studied monthly, and as necessary. Patients are discussed, as
needed, at M&M meetings and informal discussions occur about patient care, as required.
7.1.17 Blacktown Hospital
Blacktown Hospital has had an ASU offering thrombolysis in place for several years. Similar to Westmead, this
operates on a split service with the neurology unit treating patients up to 69 years old, while the geriatric
service treats those aged 70 years and older. The average DTN time is reported at 69 minutes.
Orientation and education is provided through in-services to ED nursing and medical staff. However, this is on
an “as needed” basis rather than scheduled for regular sessions.
After hours is serviced by an on-call neurologist who has remote access to scans, pathology and ED presentation
data. This system is considered ideal by the neurology staff because patients’ access to treatment may be more
timely, if seen by specialists in the field in the first instance. A barrier reported is the reluctance of ED staff to
call AH to access this process.
Inserting a bolus as soon as practical to streamline treatment was noted as a success in improving treatment
time. Attempts have been made to divert patients directly to imaging from the ambulance. However, unless a
patient is formally registered, scans cannot be generated.
A collaborative working relationship between the SRP units and support for the program from the executive
was reported as facilitating the success of the program.
The SRP governance structure for Blacktown Hospital meets regularly and comprises neurologists, Stroke CNC,
ED CNC, ED managers, Stroke Unit staff, geriatricians and ED senior physicians. Patients are discussed at M&M
meetings as required.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 40
7.1.18 Concord Hospital
The Concord Hospital had the first stroke unit in NSW, commencing in 1994. The hospital has been thrombolysing
people for stroke for approximately 5 years. The DTN time was reported to be on average between 45 and 50
minutes. However, a recent extension of time has been attributed to new ED medical staff who are unaware of the
protocols. This is in the process of being addressed.
The Concord Hospital provides training and orientation to staff on an “as needed” basis and schedules formal
meetings to discuss stroke care and thrombolysis treatment when a new group of registrars commence.
Concord Hospital works on a District level regarding stroke care. Regular meetings occur with Royal Prince Alfred
Hospital to discuss shared knowledge, learnings, protocols and issues arising. A stroke outreach team (allied health)
is shared across the District. The governance committee for the SRP meets quarterly and includes representatives
from ASNSW, ED, Radiology and the Stroke Team. Additionally, patients are discussed at regular M&M meetings.
Ambulances pre-notify Concord Hospital ED of incoming FAST+ patients. However, ED does not notify the Stroke
Team or Radiology until the patient is assessed in ED to verify the diagnosis.
It was reported that the system works effectively within BH, however, AH can pose potential issues when new and/
or locum positions are rostered in ED and unaware of the protocol. When this occurs, a formal meeting is arranged
to discuss protocols with staff.
Radiology was identified as the program component with the most delays AH as the scanner must be started using
specific protocols and reviewed prior to commencing scans.
The presence of strong advocates in ED for thrombolysis treatment for stroke was considered a success factor of the
program and in raising awareness about the importance of time in treatment.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 41
Section 8 Discussion
The context of Stage one of the evaluation is based on the perceptions of the program by
key stakeholders. Although this requires quantitative data analysis to fully consider the
implications, an analysis of the data gathered thus far indicates several areas for
consideration and further improvement.
8.1 Program fidelity
In terms of implementation fidelity, delivery as well as the implementation approach need to be considered. This is
consistent with the themes of ongoing support for delivery and sustainability of programs. ACI needs to consider
strategies to address this while being mindful of the role of ACI; to develop, implement and evaluate models of care,
but not necessarily provide ongoing program support. A balance between the requirements of LHDs and the role of
ACI is needed to enable adequate support and program sustainability.
Discussions with the ACI Implementation Team involved in this project and sighting of relevant documentation
confirmed fidelity of the implementation approach. However, SRP delivery has limited fidelity for all components of
the program. There is considerable variation across sites with the biggest differences, and potential for slowing the
treatment process, located within the scanning components of the program. A total of seven sites reported that
Imaging was not pre-notified for FAST+ patients.
Practices around pre-notification of FAST+ patients vary across sites, with all sites receiving pre-notification from
ambulance to ED, although Nepean, Prince of Wales and Concord Hospitals do not pre-notify the Acute Stroke Team
until ED assesses and verifies a patient’s diagnosis. Some sites reported that the Stroke Team can be contacted and
mobilised quickly once a diagnosis is confirmed; however, this has potential to slow times to treatment.
The redesign methods adopted by ACI and the benchmarking with a tested and successful program (the HNE model)
resulted in an evidence-based program design that is considered effective in delivering the SRP. Although sites
reported the usefulness of the design and implementation tools, many noted that some ongoing support to sites
would assist in program sustainability.
8.2 Barriers to program implementation and delivery
The issues raised pertaining to data are substantial and require an agreed approach not only in establishing systems to
collect data about the program now, but also in the establishment of methods of data collection prior to the
implementing programs in general, to enable adequate monitoring, benchmarking and evaluation.
Recognition of the SRP as a whole-of-system program incorporating all key components as part of the patients’ care is
required to foster a shared understanding and responsibility for patient needs and consequently, a patient-centred
model of care. This includes everything from ASNSW being recognised as part of the patient journey through to
adequate rehabilitation support. To achieve this, clearly articulated and detailed mapping of the program and
transparent systems (including the provision of data and timely feedback) is required at each stage of the SRP.
Within the program, medical imaging has shown the greatest diversity across sites and is potentially a major barrier to
timely thrombolysis intervention. Further investigation is required to ascertain the most effective processes for timely
imaging and establishment of guidelines for types of scans required, acceptable modes of neurology input (remote
monitoring, telehealth, face-to-face consultation) and SRP pathways to imaging (direct from ED or from ASNSW), and
subsequent processes to facilitate these processes. These decisions fall within the remit of the stroke discipline and
dialogue should commence in the near future to ensure any potential elements of clinical variation are addressed.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 42
Local governance structures for the oversight of the SRP are a major component of the program and were an
element required for ACI to officially recognise sites as SRP sites. Although identification of existing structures or
establishment of specific structures were part of the SRP implementation, 6 out of the 18 sites interviewed stated
that there was not a formal governance structure in place that met at least quarterly. One of the sites noted a
structure that met six monthly, another was a local structure that met as required and another did not meet locally,
but had the benefit of District-wide governance meetings. Of the three remaining sites without governance
structures in place, all noted consideration to reconvene these structures, but no formal commitment was stated.
This is a concern worthy of further discussion with the sites. Formal governance of SRP is considered good practice
for the consistency and sustainability of the program.
8.3 Factors facilitating success of the program
The factors that promoted success of the program in implementation, delivery and sustainability comprised local
leadership, particularly in terms of executive sponsors and clinical champions. These roles were reported to be
instrumental in ensuring that the SRP remained a priority and worked with clinicians at each unit in the patient
journey to raise awareness of the SRP and stroke care and provided regular review reports and feedback to relevant
staff and governance bodies.
A District-wide collaborative approach across SRP sites within a District was reported as a positive influence on the
program. Shared knowledge, protocols, pathways and sometimes, medical teams, provided a cohesive service and
learning environment.
It was noted that positive relationships with ASNSW facilitated program success. This aligned with the point raised
in discussions from some sites and from ASNSW that ambulance officers are a key part of the patient journey and
consequently, should be regarded as an important part of the Acute Stroke Team. Similarly, adopting a patient-
centred approach to stroke care was seen as essential to program success and this comprised each unit delivering
care along the patient journey to take responsibility and accountability for that care.
To further expand on this concept, community awareness in stroke prevention, symptoms and time-critical
treatment will contribute to increasing patient and community literacy about stroke care. A comprehensive patient-
centred approach would include training and information to families and carers, individualised care plans for
patients and timely access to rehabilitation services.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 43
Section 9 Conclusion and preliminary recommendations
The following recommendations are included in this document as a starting point to address
areas for improvement in the SRP. It is acknowledged that further analysis will occur in the next
stages of the evaluation as is required to make more fully considered changes. The following
provide areas for consideration in terms of formative assessment.
9.1 Recommendations
Access to information
1. Consistent data collection methods to be determined for the SRP, development of a data dictionary and
guidelines for collection, access and reporting.
2. Data provided across all components of the program to SRP stakeholders (sites, ASNSW and ACI) at a minimum
of ASNSW FAST+ patients by site, door-to-scan time, scan-to-needle time, transfer times and destinations, and
patient outcomes. This will be used for monitoring, evaluation and benchmarking.
3. ACI to continue work with the ABF taskforce to undertake a costing and counting study of stroke thrombolysis
treatment with the view of standardising identification of activity and costs associated with the provision of
stroke thrombolysis services within administrative and ABF data.
4. Consider the inclusion of formalised feedback loops that will provide patient outcomes to ASNSW within an
agreed time frame from patient delivery to the site to keep ASNSW staff informed.
5. ASNSW to provide weekly data of FAST+ patients taken to each site.
Coherent planning
6. Within the mandate of ACI, consideration to be given in how to ACI can best support delivery and
sustainability of programs beyond implementation. Formalised discussions with key LHD stakeholders
concerning needs is suggested.
7. All models of care are to include baseline data and data collection systems prior to implementation.
8. Further discussion to occur with relevant sites about the need to establish adequate governance structures to
oversee the SRP.
People and engagement
9. A public awareness campaign is suggested comprising stroke and time-critical aspects of treatment with a
specific focus on rural areas and cohorts with highest stroke prevalence – Aboriginal and Torres Strait Islander
people and people from low socio-economic backgrounds. Although noted as an SRP, public awareness
campaigns are outside the remit of ACI suggesting that the Stroke Network discuss options for these
recommendations and forward to the relevant bodies for consideration.
Business processes
10. Stroke Network to convene an expert group to discuss and determine guidelines for SRP sites concerning
relevant scan types required for ascertaining eligibility for stroke thrombolysis treatment and subsequent
decision making (remote, telehealth) and access to imaging (via ED or directly from ambulance).
11. Matrix to be reviewed in terms of providing statewide coverage and allocation of workload within catchment areas.
12. Stroke Network to convene a forum of SRP and other relevant sites to discuss issues of repatriation with the
purpose of resolution. To include commencement of rehabilitation services and capacity at outlying sites and
assessment of options for patients.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 44
Leadership
13. ACI and ECI to continue the discussion of options for affirming thrombolysis treatment for stroke as standard
practice in stroke care.
Culture and values
14. Promote the SRP as an integrated program across ASNSW and LHDs.
15. Define and promote a person/patient-centred focus for stroke care in NSW.
16. Further explore the areas of interest as contained in the attached Patient Experience Trackers Report at
Appendix III.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 45
Section 10 Next steps
The next stage of the evaluation will comprise analysis of data from ASNSW and sites to assess
KPIs for the SRP and provide more in-depth context for Stage one.
Stage two will also incorporate the work discussed with the ABF Taskforce to investigate potential coding solutions
for stroke thrombolysis treatment. The time frame for Stage two will be reliant on access to site data (may be
subject to various ethics approvals) and will be confirmed once Stage one is complete.

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 46
Section 11 References
1. ABS Causes of death (cat no 3303.0), Canberra, Australia; 2009.
2. ACI Stroke Program: Early Access to Stroke Thrombolysis - Implementation Toolkit.
3. ACI What is the NSW Stroke Reperfusion Service and why do we need it?; 2013.
4. AIHW Stroke and its management in Australia: an update. Canberra; 2013.
5. Asimos, A., Ward, S., Brice, J., Enright, D., Rosamond, W., Goldstein, L., Studnek, J. A geographical information system analysis of the impact of a statewide acute stroke emergency medical services routing protocol on community hospital bypass, Journal of Stroke and Cerebralvascular Disease, Nov-Dec 2014, vol 23, issue 10; 2014.
6. Australian Commission on Safety and Quality in Health Care. Consultation draft: Clinical care standards for stroke 2014. [Online] Available at: http://www.safetyandquality.gov.au/wp-content/uploads/2014/03/Full-version-Consultation-Draft-Clinical-Care-Standard-for-Stroke.pdf
7. BHI The Insight Series: 30 day mortality following hospitalisation, five clinical conditions, NSW, July 2009 - June 2012. Chatswood: BHI; 2013.
8. Department of Health Model of Stroke Care. Perth: Health Networks Branch, Department of Health, Western Australia; 2010.
9. Department of Health Framework for Regional Acute Stroke Services in Victoria, State Government; October 2013.
10. Golstein, L. Statewide Hospital-Based Stroke Services in North Carolina: Changes Over 10 Years. Stroke: Journal of the American Heart Association, vol 41; February 2010.
11. Hoffman T, L. R. Stroke care in Australia: why is it still the poor cousin of health care? Medical Journal Australia, 5; 2013.
12. Jaunch, S., Adams, H., del Zoppo, G., Alberts, M., Bhatt, D., Brass, L., Furlan, A., Grubb, R., Higashida, R., Kidwell, C., Lyden, P., Morgenstern, L., Oureshi, A., Rosenwasser, R., Scott, P., Wijdicks, E. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke: Journal of the American Heart Association, published on PubMed; March 2013.
13. Kash, B., Spaulding, A., Johnson, C., Gamm, L. Success factors for strategic change initiatives: a qualitative study of healthcare administrators perspectives, Journal of Healthcare Management, 59:1; January-February 2014.
Lindsberg, P., Happola, O., Kallela, M., Valanne, L.,
Kuisma, M., Kaste, M. Door to thrombolysis: ER
reorganization and reduced delays to stroke treatment,
Neurology, vol 67 no 2; July 2006.
14. Lovett, J., Sandercock, P., Bamford, J., Warlow, C.,
Rothwell, P. Very early risk of stroke after a fgirst transient
ischaemic attack, Stroke v34; 2003.
15. Mansour, O. Thrombolysis for ishaemic stroke: Where we
are (time is brain). The Internet Journal of Interventional
Medicine, vol 2 #1; 2013.
Meretoja, A., Weir, L., Ugalde, M., Yassi, N., Yan, B., Hand,
P., Truesdale, M., Davis, S., Campbell, B. Helsinki model cut
stroke thrombolysis delays to 25 minutes in Melbourne in
only 4 months, Neurology, vol 81 no 12; Sept 17 2013.
16. Merino, J., Silver, B., Wong, E., Foell, B., Demaerschalk, B.,
Tamayo, A., Poncha, F., Hachinski, V. Extending Tissue
Plasminogen Activator Use to Community and Rural
Stroke Patients. Stroke: Journal of the American Heart
Association, vol 33; 2002.
17. Morris, S. Impact of centralising acute stroke services in
English metropolitan areas on mortality and length of
hospital stay: difference-in-differences analysis, British
Medical Journal; August 2014.
18. National Stroke Foundation website. [Online] Available at:
http://strokefoundation.com.au/health-professionals/
auscr-partnership
19. National Stroke Foundation. Clinical guidelines for
stroke management. Canberra: National Stroke
Foundation; 2010.
20. Stroke Society of Australia website. [Online] Available at:
http://www.strokesociety.com.au/index.php?option=com_
content&view=article&id=367:inspire-international-
stroke-perfusion-imaging-registry&catid=40:astn&Item
id=162
Wardlaw JM, M. V., Berge E, del Zoppo GJ. Thrombolysis
for acute ischaemic stroke (Review). Cochrane
Collaboration(4); 2009.
21. Wyatt Knowlton. L., Phillips. C. The logic model
guidebook: better strategies for great results, 2nd Ed.
Sage Publications Inc., Thousand Oaks, California; 2013.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 4
7
App
endi
x I
Go
sfo
rd
Ho
spit
alN
epea
n
Ho
spit
alC
amp
bel
ltow
n
Ho
spit
alO
ran
ge
Ho
spit
alB
ath
urs
t H
osp
ital
St
Vin
cen
t’s
Ho
spit
al
Roy
al
Prin
ce
Alf
red
H
osp
ital
Prin
ce o
f W
ales
H
osp
ital
Co
nco
rd
Ho
spit
al
Do
yo
u r
ecei
ve s
tro
ke F
AST
+ p
atie
nts
?Ye
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
s
Are
th
ere
syst
ems
in p
lace
fo
r ac
tiva
tin
g a
st
roke
pag
e al
ert?
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Is E
D p
re-n
oti
fied
of
FAST
+ p
atie
nts
?N
o (
Acu
te
Stro
ke T
eam
n
oti
fied
)
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Is M
edic
al Im
agin
g p
re-n
oti
fied
of
stro
ke
FAST
+ p
atie
nts
?N
oN
oYe
sYe
sYe
sYe
sYe
sN
oN
o
Is A
cute
Str
oke
Tea
m p
re-n
oti
fied
of
stro
ke
FAST
+ p
atie
nts
?Ye
sN
oYe
sYe
sYe
s Ye
sYe
sN
oN
o
Are
pat
ien
ts t
riag
ed a
s C
ateg
ory
2?
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Are
AH
Neu
rolo
gy,
Rad
iolo
gy,
Str
oke
Un
it
and
Pat
ien
t Fl
ow s
taff
aw
are
of
pro
cess
es
AH
fo
r FA
ST+
pat
ien
ts?
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Is t
he
pro
cess
fo
r FA
ST+
the
sam
e 24
/7?
If
no
t w
hat
are
th
e d
iffe
ren
ces?
Yes
No
, ED
-led
A
H, S
tro
ke
Team
- led
in
BH
No
ED
-led
AH
, St
roke
Tea
m-l
ed
in B
H
No
, AH
ra
dio
log
y re
adin
g
serv
ice,
m
edic
al
on
-cal
l AH
No
, AH
ra
dio
log
y re
adin
g
serv
ice
No
, ED
-led
A
H, S
tro
ke
Team
-led
in
BH
Yes
Yes
No
, ED
-led
A
H, S
tro
ke
Team
led
in
BH
Are
str
oke
pat
ien
ts t
hat
arr
ive
by
amb
ula
nce
, bu
t n
ot
iden
tifi
ed a
s FA
ST+
ap
pro
pri
atel
y as
sess
ed a
nd
tri
aged
? W
hat
m
easu
res
are
use
d t
o a
sses
s th
is?
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
FAST
+R
oss
ier
FAST
+FA
ST+
14.1
Str
oke
Rep
erfu
sio
n A
sses
smen
t To
ol
Tab
le 4
: Str
oke
Rep
erfu
sio
n A
sses
smen
t To
ol s
um
mar
y

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 4
8
Go
sfo
rd
Ho
spit
alN
epea
n
Ho
spit
alC
amp
bel
ltow
n
Ho
spit
alO
ran
ge
Ho
spit
alB
ath
urs
t H
osp
ital
St
Vin
cen
t’s
Ho
spit
al
Roy
al
Prin
ce
Alf
red
H
osp
ital
Prin
ce o
f W
ales
H
osp
ital
Co
nco
rd
Ho
spit
al
Are
FA
ST+
pat
ien
ts w
ho
arr
ive
by n
on
-am
bu
lan
ce m
ean
s ap
pro
pri
atel
y id
enti
fied
an
d a
sses
sed?
Wh
at m
easu
res
are
use
d t
o
asse
ss t
his
?
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
FAST
+R
oss
ier
FAST
+FA
ST+
Pati
ents
rec
eive
tre
atm
ent
wit
h
intr
aven
ou
s th
rom
bo
lysi
s as
per
pro
toco
l <
60 m
ins
No
t al
lYe
sN
oYe
sN
oN
oYe
sU
sual
lyN
o
Pati
ents
are
tra
nsf
erre
d t
o A
SU/I
CU
/HD
U
do
or
to a
dm
issi
on
<3
ho
urs
No
No
t al
way
s Ye
sYe
sN
oN
oN
oN
o –
bed
av
aila
bili
ty
an is
sue
Yes
Hav
e p
athw
ays
chan
ged
sin
ce ‘‘
go
live
’’ d
ate
in J
anu
ary
2013
? H
ow?
No
, pat
hw
ay
imp
lem
ente
d
pri
or
to t
he
SRP
No
, alr
ead
y in
pla
ceYe
s, u
pd
ated
to
re
flec
t p
re-
no
tifi
cati
on
Yes,
ad
ded
es
cala
tio
n
pro
cess
fr
om
su
rro
un
din
g
site
s
Yes,
ad
ded
es
cala
tio
n
pro
cess
fr
om
su
rro
un
din
g
site
s
No
, pat
hw
ay
imp
lem
ente
d
pri
or
to t
he
SRP
No
, pat
hw
ay
imp
lem
ente
d
pri
or
to t
he
SRP
No
, alr
ead
y in
pla
ceN
o, a
lrea
dy
in p
lace
Has
pro
po
sed
loca
l pat
hway
bee
n
succ
essf
ully
imp
lem
ente
d? I
f n
ot
wh
at a
re
the
bar
rier
s?
See
abo
veSe
e ab
ove
Yes
Yes
Yes
See
abo
veSe
e ab
ove
Yes
See
abo
ve
All
staf
f ar
e aw
are
of
the
chan
ges
to
g
uid
elin
es a
nd
po
licie
sN
o –
no
ch
ang
e in
p
ract
ice
No
– s
ee
abo
veYe
sYe
sYe
sYe
sYe
sYe
sYe
s
Ori
enta
tio
n a
nd
tra
inin
g o
n t
he
SRP
is
sch
edu
led
on
a r
egu
lar
bas
is f
or
all s
taff
in
volv
ed a
cro
ss t
he
ho
spit
al
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
Are
th
rom
bo
lyse
d p
atie
nts
/th
ose
ass
esse
d
for
thro
mb
oly
sis
reco
rded
in a
dat
abas
e o
r cl
inic
al lo
g?
Yes
– lo
cal
dat
abas
e,
INSP
IRE
Yes
– lo
cal
dat
abas
e,
INSP
IRE
Yes
– D
istr
ict
dat
abas
e, T
IPS
Yes,
TIP
S,
INSP
IRE
Yes
– lo
cal
dat
abas
eYe
s –
SITS
Yes
– lo
cal
dat
abas
e,
Au
SCR
Yes,
loca
l d
atab
ase
Yes,
loca
l d
atab
ase

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 4
9
Go
sfo
rd
Ho
spit
alN
epea
n
Ho
spit
alC
amp
bel
ltow
n
Ho
spit
alO
ran
ge
Ho
spit
alB
ath
urs
t H
osp
ital
St
Vin
cen
t’s
Ho
spit
al
Roy
al
Prin
ce
Alf
red
H
osp
ital
Prin
ce o
f W
ales
H
osp
ital
Co
nco
rd
Ho
spit
al
The
SRP
com
mit
tee
mee
ts a
t le
ast
qu
arte
rly
No
No
Yes
– D
istr
ict
mee
tin
g, n
ot
SRP-
spec
ific
Yes
– M
on
thly
St
roke
C
om
mit
tee
and
Pat
ien
t Sa
fety
m
eeti
ng
s
Yes
– M
on
thly
St
roke
C
om
mit
tee
and
Pat
ien
t Sa
fety
m
eeti
ng
s
Yes
–
Mo
nth
ly
go
vern
ance
qu
alit
y an
d
vari
atio
n
man
agem
ent
mee
tin
gs
Yes
– Q
uar
terl
y m
eeti
ng
s an
d f
eed
b
ack
to
Exec
uti
ve
and
Clin
ical
C
ou
nci
l
Yes
– st
roke
u
nit
tea
m,
no
t-SR
P sp
ecifi
c
Yes
– Q
uar
terl
y
Wh
o r
egu
larl
y at
ten
ds
the
SRP
mee
tin
gs?
n/a
n/a
Stro
ke D
irec
tor,
st
roke
tea
ms
and
oth
ers
as
invi
ted
GM
, DO
N,
DM
S, D
DO
N,
Qu
alit
y
Man
ager
,
Infe
ctio
n
Co
ntr
ol,
Car
dio
log
y
CN
Cs
, Str
oke
Car
e
Co
ord
inat
or,
Hea
lth
Co
un
cil r
ep,
GP
rep
,
NU
MS
See
Ora
ng
e H
osp
ital
fo
r d
etai
ls
ED C
NC
, D
irec
tor
Med
Tr
ain
ing
, D
irec
tor
Stro
ke U
nit
, C
NC
Str
oke
U
nit
ASN
SW, E
D
nu
rse
and
med
ical
sta
ff,
rad
iolo
gy,
ICU
,
NU
M s
tro
ke
war
d,
Reh
abili
atio
n,
Neu
rolo
gy,
Alli
ed h
ealt
h
Neu
rolo
gy,
ED
, Im
agin
gA
SNSW
, ED
, R
adio
log
y,
Stro
ke T
eam
Wh
at d
ata
is r
ou
tin
ely
colle
cted
to
mo
nit
or
the
clin
ical
an
d o
per
atio
nal
asp
ects
of
this
se
rvic
e an
d w
ho
has
acc
ess
to t
his
in
form
atio
n? D
escr
ibe
the
feed
bac
k p
roce
sses
fo
r p
arti
cip
atin
g s
ervi
ces
DTN
, tim
es,
trea
tmen
t,
len
gth
of
stay
(LO
S)
– re
gu
larl
y re
view
ed
rele
van
t st
aff
No
ne
at
pre
sen
tTr
iag
e, a
rriv
al,
CT,
DTN
, NH
ISS,
is
sues
# FA
ST+
/
thro
mb
oly
sed
/
reas
on
no
t/
on
set
to
nee
dle
, DTN
,
bar
rier
s
See
Ora
ng
e H
osp
ital
fo
r d
etai
ls
All
SITS
dat
a (o
nse
t to
n
eed
le,
DTN
, o
utc
om
es)
On
set,
as
sess
men
t,
trea
tmen
t,
DTN
Yes
– re
po
rted
to
st
roke
un
it
mee
tin
gs,
q
ual
ity
and
M
&M
m
eeti
ng
s
DTN
, d
oo
r-to
-CT,
o
nse
t to
st
roke
te
am,
ou
tco
mes
(m
od
ified
R
anki
n)

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 5
0
Go
sfo
rd
Ho
spit
alN
epea
n
Ho
spit
alC
amp
bel
ltow
n
Ho
spit
alO
ran
ge
Ho
spit
alB
ath
urs
t H
osp
ital
St
Vin
cen
t’s
Ho
spit
al
Roy
al
Prin
ce
Alf
red
H
osp
ital
Prin
ce o
f W
ales
H
osp
ital
Co
nco
rd
Ho
spit
al
How
are
issu
es r
epo
rted
an
d r
eso
lved
?M
on
ito
red
th
rou
gh
d
atab
ase,
o
n s
tro
ke
war
d
IMS
Neu
rolo
gy
M&
MD
iscu
ssed
at
mo
nth
ly
mee
tin
gs
Iden
tifi
ed
and
d
iscu
ssed
at
mo
nth
ly
mee
tin
gs,
cl
inic
ian
in
terv
iew
s
Stro
ke U
nit
Thro
mb
oly
sis
and
Go
vern
ance
M&
M
Thro
ug
h
mee
tin
gs
as
no
ted
ab
ove
Thro
ug
h
abo
ve
pro
cess
es
– IM
S
Info
rmal
ly,
un
less
IMS
req
uir
ed
The
team
has
cle
ar r
ole
s an
d
resp
on
sib
iliti
esYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
s
Pati
ents
are
dis
cuss
ed a
t M
&M
mee
tin
gs
Stan
dar
d E
D
M&
MED
M&
M,
Neu
rolo
gy
M&
M
Yes
– ED
, N
euro
log
yYe
s Ye
sYe
s –
see
abo
veYe
sYe
sYe
s
Wh
at is
th
e p
roce
ss t
o a
sses
s an
d im
pro
ve
the
SRP
pat
hway
an
d s
ervi
ces
in p
lace
to
m
on
ito
r an
d r
esp
on
d t
o a
dve
rse
even
ts in
cl
inic
al o
utc
om
es?
No
–
gen
eral
sy
stem
m
on
ito
rin
g
on
ly
Mo
nit
or
exis
tin
g
syst
ems
– IM
S
Mo
nit
ori
ng
of
issu
es a
risi
ng
, IM
S
IMS
IMS
Dis
cuss
ion
th
rou
gh
va
rio
us
com
mit
tees
, m
on
ito
rin
g
Ever
y
trea
tmen
t
ove
r 60
min
ute
s
inte
rro
gat
ed
to id
enti
fy
po
ten
tial
del
ays
and
reso
lve
Stro
ke
mee
tin
gs
Info
rmal
m
eeti
ng
s,
Dis
tric
t St
roke
m
eeti
ng
s,
Stro
ke
mee
tin
gs
Wh
at is
th
e p
roce
ss t
o m
axim
ise
use
of
clin
ical
bes
t p
ract
ice
and
use
th
e SR
P to
im
pro
ve p
atie
nt
safe
ty a
nd
ou
tco
mes
?
Reg
ula
r re
view
ag
ain
st
gu
idel
ines
Reg
ula
r m
on
ito
rin
gM
on
ito
rin
gN
etw
ork
ing
st
atew
ide
Net
wo
rkin
g
stat
ewid
eR
egu
lar
revi
ew
Rev
iew
com
plic
atio
ns,
feed
bac
k,
ben
chm
arki
ng
/
KPI
s, r
egu
lar
revi
ew
Rev
iew
an
d
mo
nit
or

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 5
1
Ban
ksto
wn
H
osp
ital
Wes
tmea
d
Ho
spit
alLi
verp
oo
l H
osp
ital
Roy
al
No
rth
Sh
ore
H
osp
ital
Syd
ney
A
dve
nti
st
Ho
spit
alSt
Geo
rge
Ho
spit
al
Wag
ga
Wag
ga
Ho
spit
al
Ho
rnsb
y K
uri
ng
-Gai
H
osp
ital
Bla
ckto
wn
H
osp
ital
Do
yo
u r
ecei
ve s
tro
ke F
AST
+ p
atie
nts
?Ye
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
s
Are
th
ere
syst
ems
in p
lace
fo
r ac
tiva
tin
g a
st
roke
pag
e al
ert?
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Is E
D p
re-n
oti
fied
of
FAST
+ p
atie
nts
?Ye
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
s
Is M
edic
al Im
agin
g p
re-n
oti
fied
of
stro
ke
FAST
+ p
atie
nts
?N
oYe
sYe
sYe
sYe
sYe
sN
oN
oYe
s
Is A
cute
Str
oke
Tea
m p
re-n
oti
fied
of
stro
ke
FAST
+ p
atie
nts
?Ye
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
s
Are
pat
ien
ts t
riag
ed a
s C
ateg
ory
2?
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Are
AH
Neu
rolo
gy,
Rad
iolo
gy,
Str
oke
Un
it
and
Pat
ien
t Fl
ow s
taff
aw
are
of
pro
cess
es
AH
fo
r FA
ST+
pat
ien
ts?
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Is t
he
pro
cess
fo
r FA
ST+
the
sam
e 24
/7?
If
no
t w
hat
are
th
e d
iffe
ren
ces?
No
, ED
-led
A
H, S
tro
ke
Team
in B
H
Yes
No
, ED
cal
ls
on
-cal
l n
euro
log
ist
on
ce p
atie
nt
asse
ssed
No
, led
by
stro
ke
fello
w in
B
H, o
n-c
all
reg
istr
ar A
H
Yes,
n
euro
log
y re
gis
trar
in
BH
, on
-cal
l n
euro
log
ist
AH
Yes
Yes
No
, on
-cal
l n
euro
AH
Yes
Are
str
oke
pat
ien
ts t
hat
arr
ive
by a
mb
ula
nce
, b
ut
no
t id
enti
fied
as
FAST
+ ap
pro
pri
atel
y as
sess
ed a
nd
tri
aged
? W
hat
mea
sure
s ar
e u
sed
to
ass
ess
this
?
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes,
Ro
ssie
rN
IHSS
Ro
ssie
r an
d
NIH
SSN
IHSS
Cat
ego
ry
3/4
as p
er
nat
ion
al
gu
idel
ines

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 5
2
Ban
ksto
wn
H
osp
ital
Wes
tmea
d
Ho
spit
alLi
verp
oo
l H
osp
ital
Roy
al
No
rth
Sh
ore
H
osp
ital
Syd
ney
A
dve
nti
st
Ho
spit
alSt
Geo
rge
Ho
spit
al
Wag
ga
Wag
ga
Ho
spit
al
Ho
rnsb
y K
uri
ng
-Gai
H
osp
ital
Bla
ckto
wn
H
osp
ital
Are
FA
ST+
pat
ien
ts w
ho
arr
ive
by n
on
-am
bu
lan
ce m
ean
s ap
pro
pri
atel
y id
enti
fied
an
d a
sses
sed?
Wh
at m
easu
res
are
use
d t
o
asse
ss t
his
?
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ro
ssie
rN
IHSS
Ro
ssie
r an
d
NIH
SSN
IHSS
Pati
ents
rec
eive
tre
atm
ent
wit
h in
trav
eno
us
thro
mb
oly
sis
as p
er p
roto
col <
60 m
ins
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
Pati
ents
are
tra
nsf
erre
d t
o A
SU/I
CU
/HD
U
do
or–
to-a
dm
issi
on
<3
ho
urs
Yes
No
Yes
Yes
No
No
No
Yes
No
Hav
e p
athw
ays
chan
ged
sin
ce ‘g
o li
ve’ d
ate
in J
an 2
013?
How
?Ye
s, w
ent
24/7
Yes,
in
crea
sed
am
bu
lan
ce
dir
ect
to C
T
Yes,
re
view
ed
exis
tin
g
pat
hw
ays
No
, exi
stin
g
serv
ice
No
, exi
stin
g
serv
ice
No
, exi
stin
g
serv
ice
No
, exi
stin
g
serv
ice
No
, exi
stin
g
serv
ice
Yes
,
com
mu
nic
atio
n
chan
ged
,
imp
rove
d E
D
tim
ing
Has
pro
po
sed
loca
l pat
hway
bee
n
succ
essf
ully
imp
lem
ente
d?If
no
t, w
hat
are
th
e b
arri
ers?
Yes
Yes
Yes
See
abo
veSe
e ab
ove
See
abo
veSe
e ab
ove
See
abo
veYe
s
All
staf
f ar
e aw
are
of
the
chan
ges
to
g
uid
elin
es a
nd
po
licie
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
s
Ori
enta
tio
n a
nd
tra
inin
g o
n t
he
SRP
is
sch
edu
led
on
a r
egu
lar
bas
is f
or
all s
taff
in
volv
ed a
cro
ss t
he
ho
spit
al
Yes
Yes
Yes
Yes
Yes
Yes
Yes
No
No
Are
th
rom
bo
lyse
d p
atie
nts
/th
ose
ass
esse
d
for
thro
mb
oly
sis
reco
rded
in a
dat
abas
e o
r cl
inic
al lo
g?
Yes
– lo
cal
dat
abas
e,
SITS
Yes
– lo
cal
dat
abas
eYe
s –
loca
l d
atab
ase
Yes
– lo
cal
dat
abas
e,
TIPS
Yes
– lo
cal
dat
abas
e,
TIPS
Yes
– lo
cal
dat
abas
eYe
s –
loca
l d
atab
ase,
TI
PS, S
ITS
Yes
– lo
cal
dat
abas
eYe
s ––
loca
l d
atab
ase,
TI
PS

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 5
3
Ban
ksto
wn
H
osp
ital
Wes
tmea
d
Ho
spit
alLi
verp
oo
l H
osp
ital
Roy
al
No
rth
Sh
ore
H
osp
ital
Syd
ney
A
dve
nti
st
Ho
spit
alSt
Geo
rge
Ho
spit
al
Wag
ga
Wag
ga
Ho
spit
al
Ho
rnsb
y K
uri
ng
-Gai
H
osp
ital
Bla
ckto
wn
H
osp
ital
The
SRP
com
mit
tee
mee
ts a
t le
ast
qu
arte
rly
Yes
– b
i-m
on
thly
No
No
– m
et
twic
e si
nce
Ja
nu
ary
2013
. Q
uar
terl
y D
istr
ict
stro
ke
mee
tin
gs
occ
ur
Yes
– St
roke
te
am,
info
rmal
No
–
6-m
on
thly
Yes
– St
roke
m
eeti
ng
b
i-m
on
thly
Yes
– St
roke
Ex
ecu
tive
, b
i-m
on
thly
No
– S
mal
l lo
cal
mee
tin
g
Yes
Wh
o r
egu
larl
y at
ten
ds
the
SRP
mee
tin
gs?
ED,
Neu
rolo
gy,
St
roke
Te
am,
Stro
ke
Liai
son
O
ffice
r
n/a
Ad
min
, M
edic
al,
Nu
rsin
g, E
D,
Alli
ed
hea
lth
, A
SNSW
Dir
ecto
r o
f St
roke
N
etw
ork
, C
NC
s, S
tro
ke
fello
w, D
ata
man
ager
, A
rea
coo
rdin
ato
r
EC, A
MO
s,
Neu
rolo
gy
reg
istr
ar,
Neu
rosc
ien
ces
NU
M
– in
vite
es a
s
nee
ded
Each
d
epar
tmen
t h
as s
epar
ate
mee
tin
gs.
In
form
al
dis
cuss
ion
s in
tra-
dep
artm
ent
Stro
ke
con
sult
ant,
Stro
ke IU
it
NU
M, E
xecu
tive
rep
rese
nta
tive
,
Alli
ed h
ealt
h,
con
sum
er
NU
M, s
tro
ke
un
it, E
D
– n
o
neu
rolo
gy
as V
MO
Neu
rolo
gy,
Stro
ke C
NC
,
ED C
NC
, ED
man
ager
s,
Stro
ke U
nit
,
ger
iatr
icia
ns,
ED s
enio
r
ph
ysic
ian
s
Wh
at d
ata
is r
ou
tin
ely
colle
cted
to
mo
nit
or
the
clin
ical
an
d o
per
atio
nal
asp
ects
of
this
se
rvic
e an
d w
ho
has
acc
ess
to t
his
in
form
atio
n? -
des
crib
e th
e fe
edb
ack
pro
cess
es f
or
par
tici
pat
ing
ser
vice
s
SITS
req
uir
emen
t,
i.e. o
nse
t to
nee
dle
, DTN
,
ou
tco
mes
Stro
ke c
alls
,
ou
tco
mes
dat
a, D
TN,
ble
edin
g
com
plic
atio
ns
Stro
ke
cod
es, D
TN,
do
or-
to-
scan
, re
spo
nse
ti
me,
o
utc
om
es
DTN
, d
oo
r-to
-sc
an,
trea
tmen
t,
ou
tco
mes
FAST
dat
a,
thro
mb
oly
sis
All
pat
ien
t
dat
a fr
om
adm
issi
on
to
dis
char
ge
has
bee
n k
ept
for
all
thro
mb
oly
sed
pat
ien
ts s
ince
2007
DTN
, d
oo
r-to
-sc
an,
trea
tmen
t,
ou
tco
mes
DTN
, d
oo
r-to
-sc
an,
trea
tmen
t,
ou
tco
mes
Tim
ing
, im
ages
, N
IHSS
, ad
vers
e re
acti
on
s,
del
ays,
o
utc
om
es

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 5
4
Ban
ksto
wn
H
osp
ital
Wes
tmea
d
Ho
spit
alLi
verp
oo
l H
osp
ital
Roy
al
No
rth
Sh
ore
H
osp
ital
Syd
ney
A
dve
nti
st
Ho
spit
alSt
Geo
rge
Ho
spit
al
Wag
ga
Wag
ga
Ho
spit
al
Ho
rnsb
y K
uri
ng
-Gai
H
osp
ital
Bla
ckto
wn
H
osp
ital
How
are
issu
es r
epo
rted
an
d r
eso
lved
?IM
S, lo
cal
rep
ort
ing
to
ol
To C
linic
al
Lead
or
rele
van
t H
OD
/NU
M
Dis
cuss
ion
, fo
rmal
is
sues
re
gis
ter,
w
eekl
y st
roke
m
eeti
ng
s,
IMS
M&
M
mee
tin
gs,
IM
S, R
CA
Dat
a re
view
ed b
y St
roke
C
om
mit
tee
M&
Ms,
re
gu
lar
mee
tin
gs,
as
aris
e
Ro
uti
ne
serv
ice
revi
ew
IMS,
reg
ula
r re
view
IMS,
M&
M
mee
tin
gs
The
team
has
cle
ar r
ole
s an
d r
esp
on
sib
iliti
esYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
sYe
s
Pati
ents
are
dis
cuss
ed a
t M
&M
mee
tin
gs
Yes
Yes
Yes
Yes
Neu
rolo
gy
sect
ion
m
eeti
ng
s
Yes
Dis
cuss
ed,
as n
eed
edYe
sYe
s
Wh
at is
th
e p
roce
ss t
o a
sses
s an
d im
pro
ve
the
SRP
pat
hway
an
d s
ervi
ces
in p
lace
to
m
on
ito
r an
d r
esp
on
d t
o a
dve
rse
even
ts in
cl
inic
al o
utc
om
es?
Dis
cuss
ion
at
reg
ula
r m
eeti
ng
s,
revi
ew o
f d
ata
Dis
sem
inat
ion
of
dat
a,
dis
cuss
ion
reg
ard
ing
dat
a w
ith
ED
Rev
iew
of
dat
aD
iscu
ssio
n
at r
egu
lar
mee
tin
gs,
d
ata
revi
ew
Feed
bac
k,
M&
Ms,
St
roke
C
om
mit
tee
Dis
cuss
ion
at
reg
ula
r m
eeti
ng
s,
revi
ew o
f d
ata
Reg
ula
r re
view
s o
ccu
r,
inte
rnal
an
d
exte
rnal
au
dit
s
Inte
rro
gat
ion
of
dat
a,
reg
ula
r
dis
cuss
ion
Reg
ula
r re
view
of
po
licy
and
p
roce
du
res

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 5
5
App
endi
x II
15.1
SR
P si
tes
– in
pat
ient
uti
lisat
ion
dat
a
15.1
.1 G
osf
ord
Ho
spit
al
Go
sfo
rd H
osp
ital
rec
eive
d 7
.9%
of
the
tota
l pat
ien
t lo
ad t
hat
pre
sen
ted
at
SRP
site
s in
201
2-13
. Fro
m 2
007-
08 t
o 2
012-
13, 3
552
acu
te s
tro
ke e
pis
od
es b
y se
lect
ed D
RGs
are
sho
wn
in T
able
5. T
he
hig
hes
t vo
lum
e D
RG w
as s
tro
ke a
nd
oth
er c
ereb
rova
scu
lar
dis
ord
ers.
Tab
le 5
: Go
sfo
rd H
osp
ital
sel
ecte
d s
tro
ke D
RG
s 20
07-0
8 to
201
2-13 A
cute
ep
iso
des
AR
-DR
G G
osf
ord
Ho
spit
al
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
08
138
398
2008
-09
05
119
470
2009
-10
07
145
491
2010
-11
07
176
393
2011
-12
18
181
411
2012
-13
08
176
410
Wit
hin
th
ese
DRG
s, t
her
e w
ere
a to
tal o
f 36
30 a
cute
ep
iso
des
fro
m 2
007-
08 t
o 2
012-
13 b
y se
lect
ed IC
D a
s sh
ow
n in
Fig
ure
8. T
he
hig
hes
t vo
lum
e w
as f
or
cere
bra
l
infa
rcti
on
wit
h 2
80 e
pis
od
es in
201
2-13
.
The
aver
age
len
gth
of
stay
ste
adily
dec
lined
fro
m 9
day
s in
200
7-08
to
5.8
day
s 20
12-1
3. In
201
2-13
, th
e av
erag
e N
WA
U w
as 1
.3 in
dic
atin
g a
slig
htl
y hi
gh
er c
om
ple
xity
leve
l
than
no
n-S
RP
site
s, a
lth
ou
gh
thi
s w
as lo
wer
th
an N
SW in
to
tal.
The
firs
t g
rap
h in
Fig
ure
8 s
ho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s at
pat
ien
t p
rese
nta
tio
n a
nd
are
sh
ow
n h
ere
to p
rovi
de
an in
dic
atio
n o
f th
e vo
lum
e o
f ep
iso
des
. Th
e se
con
d g
rap
h s
ho
ws
the
len
gth
of
stay
, in
day
s, f
or
on
ly t
he
ICD
-10
epis
od
es t
hat
wer
e am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 5
6
Fig
ure
8: G
osf
ord
Ho
spit
al IC
D-1
0 st
roke
ep
iso
des
an
d a
vera
ge
len
gth
of
stay
200
7-08
to
201
2-13
0 50
100
150
200
250
300
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Go
sfo
rd H
osp
ital
St
roke
by
sele
cted
ICD
-10
2007
/08
to 2
012/
13 e
pis
od
es a
nd
ALO
S
Oth
er n
on
-tra
um
atic
intr
acer
ebra
l hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
14
16
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 5
7
15.1
.2 N
epea
n H
osp
ital
Nep
ean
Ho
spit
al h
ad a
to
tal o
f 24
84 a
cute
ep
iso
des
fo
r se
lect
ed D
RGs
fro
m 2
007-
08 t
o 2
012-
13 a
s sh
ow
n in
Tab
le 6
. Th
e hi
gh
est
volu
me
was
fo
r st
roke
an
d o
ther
cere
bro
vasc
ula
r d
iso
rder
s at
286
ep
iso
des
in 2
012-
13.
Tab
le 6
: Nep
ean
Ho
spit
al s
elec
ted
str
oke
DR
Gs
2007
-08
to 2
012-
13 Acu
te e
pis
od
es A
R-D
RG
Nep
ean
Ho
spit
al
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
313
125
228
2008
-09
254
131
257
2009
-10
131
130
251
2010
-11
285
123
240
2011
-12
416
132
267
2012
-13
323
122
286
Wit
hin
th
ese
DRG
s, t
her
e w
ere
2549
ep
iso
des
in s
elec
ted
ICD
s fo
r th
e p
erio
d 2
007-
08 t
o 2
012-
13, a
s d
epic
ted
in F
igu
re 9
. Th
e hi
gh
est
volu
me
was
fo
r ce
reb
ral i
nfar
ctio
n a
t
174
epis
od
es in
201
2-13
.
The
aver
age
len
gth
of
stay
fo
r in
trac
ereb
ral h
aem
orr
hag
e in
crea
sed
fro
m 9
.6 d
ays
in 2
007-
08 t
o 1
2.3
day
s in
201
2-13
. TIA
has
rem
ain
ed s
tab
le a
t th
is t
ime
wit
h 3
.2 d
ays
whi
le o
ther
str
oke
ep
iso
des
hav
e st
ead
ily d
ecre
ased
. Th
e sp
ike
sho
wn
in t
he
aver
age
len
gth
of
stay
fo
r o
ther
no
n-t
rau
mat
ic in
trac
ereb
ral h
aem
orr
hag
e m
ay in
dic
ate
a
cod
ing
issu
e o
r in
clu
sio
n o
f o
utl
ier
bed
day
s. O
vera
ll, t
he
aver
age
len
gth
of
stay
dec
reas
ed f
rom
7.7
day
s in
200
7-08
to
6.4
day
s in
201
2-13
.
The
aver
age
NW
AU
fo
r N
epea
n H
osp
ital
in 2
012-
13 w
as 2
.1 in
dic
atin
g a
hig
her
co
mp
lexi
ty t
han
SR
P si
tes
in t
ota
l.
The
firs
t g
rap
h in
Fig
ure
9 s
ho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s at
pat
ien
t p
rese
nta
tio
n a
nd
are
sh
ow
n h
ere
to p
rovi
de
an in
dic
atio
n o
f th
e vo
lum
e o
f ep
iso
des
.
The
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0 ep
iso
des
th
at a
re a
men
able
to
th
rom
bo
lysi
s to
pro
vid
e an
ind
icat
ive
pic
ture
of
any
tren
ds
that
may
be
emer
gin
g in
inp
atie
nt
care
fo
r th
is c
oh
ort
.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 5
8
Fig
ure
9: N
epea
n H
osp
ital
ICD
-10
stro
ke e
pis
od
es a
nd
ave
rag
e le
ng
th o
f st
ay 2
007-
08 t
o 2
012-
13
0 20
40
60
80
100
120
140
160
180
200
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Nep
ean
Ho
spit
al
Stro
ke b
y se
lect
ed IC
D-1
0 20
07/0
8 to
201
2/13
. Acu
te e
pis
od
es a
nd
ALO
S
Oth
er n
on
-tra
um
atic
intr
acer
ebra
l hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 5
9
15.1
.3 C
amp
bel
ltow
n H
osp
ital
Cam
pb
ellt
ow
n H
osp
ital
had
a t
ota
l of
1726
acu
te e
pis
od
es f
or
sele
cted
DRG
s fr
om
200
7-08
to
201
2-13
as
sho
wn
in T
able
7. T
he
hig
hes
t vo
lum
e w
as f
or
stro
ke a
nd
oth
er
cere
bro
vasc
ula
r d
iso
rder
s at
179
ep
iso
des
in 2
012-
13.
Tab
le 7
: Cam
pb
ellt
own
Ho
spit
al s
elec
ted
str
oke
DR
Gs
2007
-08
to 2
012-
13
Acu
te e
pis
od
es A
R-D
RG
Cam
pb
ellt
own
Ho
spit
al
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
00
100
177
2008
-09
00
102
178
2009
-10
00
118
183
2010
-11
00
106
187
2011
-12
00
100
178
2012
-13
00
118
179
Acu
te e
pis
od
es b
y se
lect
ed IC
D c
od
es t
ota
lled
173
7 fo
r th
e 20
07-0
8 to
201
2-13
per
iod
. Th
e hi
gh
est
volu
me
was
fo
r ce
reb
ral i
nfar
ctio
n w
ith
131
ep
iso
des
in 2
012-
13. T
he
aver
age
len
gth
of
stay
dec
lined
fro
m 7
.1 d
ays
in 2
007-
08 t
o 6
.8 d
ays
in 2
012-
13. H
ow
ever
, as
sho
wn
in F
igu
re 1
0, t
her
e w
as a
n in
crea
se in
oth
er n
on
-tra
um
atic
intr
acer
ebra
l
hae
mo
rrh
age
fro
m 1
.5 d
ays
in 2
007-
08 t
o 4
.5 d
ays
in 2
012-
13 a
nd
str
oke
no
t sp
ecifi
ed f
rom
5.8
day
s to
17.
2 fo
r th
e sa
me
per
iod
. Th
ere
wer
e re
lati
vely
sm
all n
um
ber
s o
f
pat
ien
ts in
th
ese
coh
ort
s so
incr
ease
s m
ay r
epre
sen
t o
utl
iers
in b
ed d
ays.
The
aver
age
NW
AU
fo
r C
amp
bel
lto
wn
Ho
spit
al in
201
2-13
was
1.4
. Thi
s in
dic
ates
a lo
wer
co
mp
lexi
ty c
om
par
ed t
o S
RP
site
s in
to
tal a
nd
th
e N
SW a
vera
ge,
alt
ho
ug
h a
hig
her
co
mp
lexi
ty t
han
th
at f
or
no
n-S
RP
site
s.
The
firs
t g
rap
h in
Fig
ure
10
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 6
0
Fig
ure
10:
Cam
pb
ellt
own
Ho
spit
al IC
D-1
0 st
roke
ep
iso
des
an
d a
vera
ge
len
gth
of
stay
200
7-08
to
201
2-13
0 20
40
60
80
100
120
140
160
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Cam
pb
ellt
ow
n H
osp
ital
St
roke
by
sele
cted
ICD
-10
2007
/08
to 2
012/
13. A
cute
ep
iso
des
an
d A
LOS
Oth
er n
on
-tra
um
atic
intr
acer
ebra
l hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 5 10
15
20
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 6
1
15.1
.4 O
ran
ge
Hea
lth
Ser
vice
Ove
r th
e p
erio
d 2
007-
08 t
o 2
012-
13, t
he
Ora
ng
e H
ealt
h S
ervi
ce h
ad a
to
tal o
f 10
16 a
cute
ep
iso
des
fo
r se
lect
ed D
RGs.
Th
e se
rvic
e d
id n
ot
hav
e an
y ep
iso
des
fo
r cr
ania
l or
extr
acra
nial
vas
cula
r p
roce
du
res
and
th
e hi
gh
est
volu
me
for
stro
ke a
nd
oth
er c
ereb
rova
scu
lar
dis
ord
ers.
Tab
le 8
: Ora
ng
e H
ealt
h S
ervi
ce s
elec
ted
str
oke
DR
Gs
2007
-08
to 2
012-
13
Acu
te e
pis
od
es A
R-D
RG
Ora
ng
e H
ealt
h S
ervi
ce
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
00
3511
0
2008
-09
00
6411
4
2009
-10
00
6096
2010
-11
00
4710
0
2011
-12
00
5014
3
2012
-13
00
5813
9
Ther
e w
ere
1032
acu
te e
pis
od
es f
or
sele
cted
ICD
co
des
acc
ou
nti
ng
fo
r 2.
6% o
f th
e SR
P p
atie
nt
load
. Lik
e m
ost
sit
es, c
ereb
ral i
nfar
ctio
n h
as t
he
hig
hes
t q
uan
tum
of
pre
sen
tati
on
s co
nsi
sten
tly
over
thi
s ti
me
wit
h 7
6 ep
iso
des
in 2
012-
13 d
eclin
ing
fro
m 9
0 ep
iso
des
th
e p
revi
ou
s ye
ar.
The
aver
age
len
gth
of
stay
is s
tead
ily d
eclin
ing
fro
m 5
.5 d
ays
in 2
007-
08 f
or
all e
pis
od
es t
o 4
day
s in
201
2-13
.
The
aver
age
NW
AU
is 1
.1 in
dic
atin
g a
low
er c
om
ple
xity
th
an m
ost
oth
er s
ites
.
The
firs
t g
rap
h in
Fig
ure
11
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay, i
n d
ays
for
on
ly t
he
ICD
-10
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 6
2
Fig
ure
11:
Ora
ng
e H
ealt
h S
ervi
ce IC
D-1
0 st
roke
ep
iso
des
an
d a
vera
ge
len
gth
of
stay
200
7-08
to
201
2-13
0 10
20
30
40
50
60
70
80
90
100
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Ora
ng
e H
ealt
h S
ervi
ce
Stro
ke b
y se
lect
ed IC
D-1
0 20
07/0
8 t
o 2
012/
13. A
cute
ep
iso
des
an
d A
LOS
Oth
er n
on-t
rau
mat
ic in
trac
ereb
ral h
aem
orr
hag
e
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 1 2 3 4 5 6 7 8 9 10
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 6
3
15.1
.5 B
athu
rst
Bas
e H
osp
ital
Fro
m 2
007-
08 t
o 2
012-
13, t
he
Bat
hu
rst
Bas
e H
osp
ital
had
707
to
tal a
cute
ep
iso
des
fo
r se
lect
ed D
RGs.
Sim
ilar
to t
he
Ora
ng
e H
ealt
h S
ervi
ce, t
her
e w
ere
no
cra
nial
or
extr
acra
nial
vas
cula
r p
roce
du
res
wit
h t
he
hig
hes
t q
uan
tum
of
epis
od
es b
ein
g f
or
stro
ke a
nd
oth
er c
ereb
rova
scu
lar
dis
ord
ers
as s
ho
wn
in T
able
9.
Tab
le 9
: Bat
hu
rst
Bas
e H
osp
ital
sel
ecte
d s
tro
ke D
RG
s 20
07-0
8 to
201
2-13
Acu
te e
pis
od
es A
R-D
RG
Bat
hu
rst
Bas
e H
osp
ital
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
00
3851
2008
-09
00
5482
2009
-10
00
4365
2010
-11
00
5263
2011
-12
00
5869
2012
-13
00
4389
Wit
hin
th
ese
DRG
s, t
her
e w
ere
715
acu
te e
pis
od
es in
sel
ecte
d IC
D c
od
es w
ith
th
e hi
gh
est
volu
me
for
cere
bra
l inf
arct
ion
at
46 e
pis
od
es in
201
2-13
clo
sely
fo
llow
ed b
y TI
A
wit
h 4
3 ep
iso
des
fo
r th
e sa
me
per
iod
.
Ther
e h
as b
een
a s
har
p d
eclin
e in
th
e av
erag
e le
ng
th o
f st
ay f
rom
11
day
s in
200
7-08
to
4.7
day
s in
201
2-13
ind
icat
ive
of
the
hig
h le
vel o
f TI
A e
pis
od
es.
The
Bat
hu
rst
Bas
e H
osp
ital
had
an
ave
rag
e N
WA
U f
or
the
sele
cted
DRG
s co
mb
ined
in 2
012-
13 o
f 1.
1. T
his
ind
icat
es a
low
er c
om
ple
xity
fo
r st
roke
th
an m
ost
oth
er s
ites
.
The
firs
t g
rap
h in
Fig
ure
12
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 6
4
Fig
ure
12:
Bat
hu
rst
Bas
e H
osp
ital
ICD
-10
stro
ke e
pis
od
es a
nd
ave
rag
e le
ng
th o
f st
ay 2
007-
08 t
o 2
012-
13
0 10
20
30
40
50
60
70
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Bat
hu
rst
Bas
e H
osp
ital
St
roke
by
sele
cted
ICD
-10
2007
/08
to 2
012/
13. A
cute
ep
iso
des
an
d A
LOS
Oth
er n
on-t
rau
mat
ic in
trac
ereb
ral h
aem
orr
hag
e
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 5 10
15
20
25
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 6
5
15.1
.6 S
t V
ince
nt’s
Ho
spit
al
St V
ince
nt’
s H
osp
ital
has
had
a t
ota
l of
2119
acu
te e
pis
od
es f
or
sele
cted
DRG
s fo
r th
e p
erio
d 2
007-
08 t
o 2
012-
13.
The
hig
hes
t vo
lum
e o
f ep
iso
des
, as
sho
wn
in T
able
10,
was
fo
r st
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s w
ith
222
acu
te e
pis
od
es in
201
2-13
.
Tab
le 1
0: S
t V
ince
nt’
s H
osp
ital
sel
ecte
d s
tro
ke D
RG
s 20
07-0
8 to
201
2-13
Acu
te e
pis
od
es A
R-D
RG
St
Vin
cen
t’s
Ho
spit
al
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
155
138
227
2008
-09
184
120
228
2009
-10
126
105
211
2010
-11
232
109
188
2011
-12
179
124
198
2012
-13
156
117
222
Ther
e w
ere
2146
acu
te e
pis
od
es f
or
sele
cted
ICD
co
des
wit
h t
he
hig
hes
t vo
lum
e b
ein
g f
or
cere
bra
l inf
arct
ion
wit
h 1
36 e
pis
od
es in
201
2-13
an
d 1
20 e
pis
od
es f
or
TIA
fo
r th
e
sam
e p
erio
d.
The
aver
age
len
gth
of
stay
is s
tead
ily d
eclin
ing
fo
r al
l ep
iso
des
wit
h t
he
tota
l dec
reas
ing
fro
m 8
.1 d
ays
in 2
007-
08 t
o 6
.1 d
ays
in 2
012-
13.
The
aver
age
NW
AU
is c
on
sist
ent
wit
h t
he
NSW
ave
rag
e at
1.5
. Thi
s is
low
er t
han
th
e to
tal a
vera
ge
for
SRP
site
s an
d h
igh
er t
han
th
at f
or
no
n-S
RP
site
s.
The
firs
t g
rap
h in
Fig
ure
13
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 6
6
Fig
ure
13:
St
Vin
cen
t’s
Ho
spit
al IC
D-1
0 st
roke
ep
iso
des
an
d a
vera
ge
len
gth
of
stay
200
7-08
to
201
2-13
0 20
40
60
80
100
120
140
160
180
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
St V
ince
nt'
s H
osp
ital
St
roke
by
sele
cted
ICD
-10
2007
/08
to 2
012/
13. A
cute
ep
iso
des
an
d A
LOS
Oth
er n
on-t
rau
mat
ic in
trac
ereb
ral h
aem
orr
hag
e
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 6
7
15.1
.7 R
oyal
Pri
nce
Alf
red
Ho
spit
al
Fro
m 2
007-
08 t
o 2
012-
13, R
oyal
Pri
nce
Alf
red
Ho
spit
al h
ad a
to
tal o
f 22
83 a
cute
ep
iso
des
fo
r se
lect
ed D
RGs
wit
h t
he
hig
hes
t vo
lum
e b
ein
g f
or
stro
ke a
nd
oth
er
cere
bro
vasc
ula
r d
iso
rder
s w
ith
288
ep
iso
des
in 2
012-
13. T
able
11
sho
ws
the
epis
od
es b
y D
RG.
Tab
le 1
1: R
oyal
Pri
nce
Alf
red
Ho
spit
al s
elec
ted
str
oke
DR
Gs
2007
-08
to 2
012-
13
Acu
te e
pis
od
es A
R-D
RG
Roy
al P
rin
ce A
lfre
d H
osp
ital
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
4321
6923
6
2008
-09
3817
6623
9
2009
-10
4016
9022
2
2010
-11
4416
7122
6
2011
-12
4820
7325
5
2012
-13
4821
7628
8
The
Roya
l Pri
nce
Alf
red
Ho
spit
al r
ecei
ved
5.8
% o
f th
e to
tal p
atie
nt
load
pre
sen
tin
g a
t SR
P si
tes
in 2
012-
13. D
uri
ng
th
e p
erio
d 2
007-
08 t
o 2
012-
13, i
t h
ad 2
328
acu
te
epis
od
es b
y se
lect
ed IC
D c
od
es w
ith
th
e hi
gh
est
volu
me
for
cere
bra
l inf
arct
ion
wit
h 1
99 e
pis
od
es in
201
2-13
.
The
aver
age
len
gth
of
stay
has
dec
lined
ste
adily
in t
ota
l fro
m 8
.1 d
ays
in 2
007-
08 t
o 7
.8 d
ays
in 2
012-
13.
The
aver
age
NW
AU
fo
r th
e se
lect
ed D
RGs
for
Roya
l Pri
nce
Alf
red
Ho
spit
al w
as 2
.5 in
201
2-13
. Thi
s is
th
e hi
gh
est
wei
gh
tin
g f
or
all S
RP
site
s an
d in
dic
ates
th
at t
he
site
has
the
hig
hes
t p
atie
nt
com
ple
xity
load
.
The
firs
t g
rap
h in
Fig
ure
14
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 6
8
Fig
ure
14:
Roy
al P
rin
ce A
lfre
d H
osp
ital
ICD
-10
stro
ke e
pis
od
es a
nd
ave
rag
e le
ng
th o
f st
ay 2
007-
08 t
o 2
012-
13
0 50
100
150
200
250
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Ro
yal P
rin
ce A
lfre
d H
osp
ital
St
roke
by
sele
cted
ICD
-10
2007
/08
to 2
012/
13. A
cute
ep
iso
des
an
d A
LOS
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
Days
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Year
Oth
er n
on-t
rau
mat
ic in
trac
ereb
ral h
aem
orr
hag
e
Stro
ke n
ot
spec
ified

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 6
9
15.1
.8 P
rin
ce o
f W
ales
Ho
spit
al
The
Prin
ce o
f W
ales
Ho
spit
al h
ad a
to
tal o
f 22
88 a
cute
ep
iso
des
by
sele
cted
DRG
fo
r th
e p
erio
d 2
007-
08 t
o 2
012-
13, a
s sh
ow
n in
Tab
le 1
2. T
he
hig
hes
t vo
lum
e w
as f
or
stro
ke a
nd
oth
er v
ascu
lar
dis
ord
ers
at 2
57 e
pis
od
es in
201
2-13
fo
llow
ed b
y TI
A a
nd
cer
ebra
l occ
lusi
on
at
90 e
pis
od
es f
or
the
sam
e ti
me.
Tab
le 1
2: P
rin
ce o
f W
ales
Ho
spit
al s
elec
ted
str
oke
DR
Gs
2007
-08
to 2
012-
13
Acu
te e
pis
od
es A
R-D
RG
Pri
nce
of
Wal
es H
osp
ital
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
3611
127
252
2008
-09
226
9526
6
2009
-10
364
103
238
2010
-11
267
7223
2
2011
-12
286
7724
5
2012
-13
3913
9025
7
The
Prin
ce o
f W
ales
Ho
spit
al h
ad a
to
tal o
f 23
58 a
cute
ep
iso
des
fo
r th
e se
lect
ed IC
D c
od
es a
s sh
ow
n in
Fig
ure
15.
Thi
s re
pre
sen
ts 5
.4%
of
the
tota
l SR
P p
atie
nt
load
an
d
sim
ilar
to m
ost
oth
er s
ites
, th
e hi
gh
est
volu
me
was
fo
r ce
reb
ral i
nfar
ctio
n w
ith
a t
ota
l of
200
epis
od
es in
201
2-13
.
The
aver
age
len
gth
of
stay
is d
eclin
ing
fo
r al
l ep
iso
des
wit
h a
to
tal d
ecre
ase
fro
m 9
.7 d
ays
in 2
007-
08 t
o 8
day
s in
201
2-13
.
The
aver
age
NW
AU
fo
r th
e se
lect
ed s
tro
ke D
RGs
was
2.4
in 2
012-
13 in
dic
atin
g a
hig
h le
vel o
f p
atie
nt
com
ple
xity
an
d t
he
seco
nd
hig
hes
t am
on
gst
SR
P si
tes.
The
firs
t g
rap
h in
Fig
ure
15
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 7
0
Fig
ure
15:
Pri
nce
of
Wal
es H
osp
ital
ICD
-10
stro
ke e
pis
od
es a
nd
ave
rag
e le
ng
th o
f st
ay 2
007-
08 t
o 2
012-
13
0 50
100
150
200
250
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Prin
ce o
f W
ales
Ho
spit
al
Stro
ke b
y se
lect
ed IC
D-1
0 20
07/0
8 to
201
2/13
. Acu
te e
pis
od
es a
nd
ALO
S
Oth
er n
on
-tra
um
atic
intr
acer
ebra
l
hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
14
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 7
1
15.1
.9 B
anks
tow
n-L
idco
mb
e H
osp
ital
The
Ban
ksto
wn
-Lid
com
be
Ho
spit
al h
ad a
to
tal o
f 21
63 a
cute
ep
iso
des
fo
r se
lect
ed D
RGs
fro
m 2
007-
08 t
o 2
012-
13, a
s sh
ow
n in
Tab
le 1
3. T
he
hig
hes
t vo
lum
es a
re f
or
stro
ke
and
oth
er c
ereb
rova
scu
lar
dis
ord
ers
and
TIA
an
d p
rece
reb
ral o
cclu
sio
n.
Tab
le 1
3: B
anks
tow
n-L
idco
mb
e H
osp
ital
sel
ecte
d s
tro
ke D
RG
s 20
07-0
8 to
201
2-13
Acu
te e
pis
od
es A
R-D
RG
Ban
ksto
wn
-Lid
com
be
Ho
spit
al
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
07
104
282
2008
-09
05
106
257
2009
-10
03
101
243
2010
-11
04
103
260
2011
-12
04
8925
6
2012
-13
14
105
229
By
sele
cted
ICD
co
des
, Ban
ksto
wn
-Lid
com
be
Ho
spit
al h
ad a
to
tal o
f 22
24 e
pis
od
es f
or
the
per
iod
200
7-08
to
201
2-13
. Thi
s h
as r
emai
ned
rel
ativ
ely
stab
le o
ver
the
tim
e
per
iod
. In
201
2-13
, thi
s re
pre
sen
ted
4.5
% o
f th
e to
tal p
atie
nt
load
pre
sen
tin
g a
t SR
P si
tes.
The
aver
age
len
gth
of
stay
is d
eclin
ing
in t
ota
l fro
m 1
2.4
day
s in
200
7-08
to
8 d
ays
in 2
012-
13. F
igu
re 1
6 sh
ow
s th
e av
erag
e le
ng
th o
f st
ay f
or
sele
cted
ICD
co
des
.
In 2
012-
13, B
anks
tow
n-L
idco
mb
e H
osp
ital
had
an
ave
rag
e N
WA
U f
or
sele
cted
DRG
s o
f 1.
8. T
his
is h
igh
er t
han
th
e N
SW a
nd
no
n-S
RP
site
to
tal a
vera
ges
an
d o
nly
slig
htl
y
low
er t
han
th
e to
tal S
RP
site
ave
rag
e o
f 1.
9.
The
firs
t g
rap
h in
Fig
ure
16
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 7
2
Fig
ure
16:
Ban
ksto
wn
-Lid
com
be
Ho
spit
al IC
D-1
0 st
roke
ep
iso
des
an
d a
vera
ge
len
gth
of
stay
200
7-08
to
201
2-13
0 20
40
60
80
100
120
140
160
180
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Ban
ksto
wn-L
idcomb
e H
osp
ital
St
roke
by
sele
cted
ICD
-10
2007
/08
to 2
012/
13. A
cute
ep
iso
des
an
d A
LOS
Oth
er n
on-t
rau
mat
ic in
trac
ereb
ral
hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
14
16
18
20
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 7
3
15.1
.10
Wes
tmea
d H
osp
ital
Fro
m 2
007-
08 t
o 2
012-
13, W
estm
ead
Ho
spit
al h
ad a
to
tal o
f 30
95 a
cute
str
oke
ep
iso
des
by
sele
cted
DRG
wit
h t
he
hig
hes
t vo
lum
e fo
r st
roke
an
d o
ther
cer
ebro
vasc
ula
r
dis
ord
ers
at 3
29 in
201
2-13
.
Tab
le 1
4 sh
ow
s al
l ep
iso
des
by
sele
cted
DRG
fo
r fr
om
200
7-08
to
201
2-13
.
Tab
le 1
4: W
estm
ead
Ho
spit
al s
elec
ted
str
oke
DR
Gs
2007
-08
to 2
012-
13
Acu
te e
pis
od
es A
R-D
RG
Wes
tmea
d H
osp
ital
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
4211
111
302
2008
-09
495
137
363
2009
-10
5810
116
307
2010
-11
466
126
329
2011
-12
459
121
350
2012
-13
3915
127
371
Ther
e w
ere
3148
acu
te e
pis
od
es b
y se
lect
ed IC
D c
od
es f
or
the
2007
-08
to 2
012-
13 t
ime
per
iod
wit
h t
he
hig
hes
t vo
lum
e fo
r ce
reb
ral i
nfar
ctio
n w
ith
228
ep
iso
des
in 2
012-
13.
This
has
rem
ain
ed r
elat
ivel
y st
able
ove
r th
e ti
me
per
iod
.
The
aver
age
len
gth
of
stay
has
dec
lined
by
all s
elec
ted
ICD
co
des
wit
h a
to
tal d
ecre
ase
fro
m 9
.1 d
ays
in 2
007-
08 t
o 6
.3 d
ays
in 2
012-
13.
The
aver
age
NW
AU
fo
r se
lect
ed D
RGs
for
2012
-13
was
2. T
his
is h
igh
er t
han
th
e SR
P si
te a
vera
ge
of
1.9
and
rep
rese
nts
a h
igh
pat
ien
t co
mp
lexi
ty.
The
firs
t g
rap
h in
Fig
ure
17
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 7
4
Fig
ure
17:
Wes
tmea
d H
osp
ital
ICD
-10
stro
ke e
pis
od
es a
nd
ave
rag
e le
ng
th o
f st
ay 2
007-
08 t
o 2
012-
13
0 50
100
150
200
250
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Wes
tmea
d H
osp
ital
St
roke
by
sele
cted
ICD
-10.
Acu
te e
pis
od
es a
nd
ALO
S
Oth
er n
on-t
rau
mat
ic in
trac
ereb
ral
hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 7
5
15.1
.11
Live
rpo
ol H
osp
ital
Ove
r th
e p
erio
d 2
007-
08 t
o 2
012-
13, L
iver
po
ol H
osp
ital
had
a t
ota
l of
3420
acu
te e
pis
od
es o
f st
roke
by
sele
cted
DRG
. In
201
2-13
, th
e hi
gh
est
volu
me
was
fo
r st
roke
an
d
oth
er c
ereb
rova
scu
lar
dis
ord
ers
wit
h 3
46 e
pis
od
es, a
s sh
ow
n in
Tab
le 1
5.
Tab
le 1
5: L
iver
po
ol H
osp
ital
sel
ecte
d s
tro
ke D
RG
s 20
07-0
8 to
201
2-13
Acu
te e
pis
od
es A
R-D
RG
Liv
erp
oo
l Ho
spit
al
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
6415
145
294
2008
-09
5515
148
352
2009
-10
6613
152
343
2010
-11
6520
152
351
2011
-12
4919
189
342
2012
-13
5314
158
346
Live
rpo
ol H
osp
ital
had
a t
ota
l of
3508
acu
te e
pis
od
es b
y se
lect
ed IC
D c
od
es f
or
the
per
iod
200
7-08
to
201
2-13
rep
rese
nti
ng
7.7
% o
f th
e to
tal p
atie
nt
load
pre
sen
tin
g t
o
SRP
site
s in
201
2-13
. Ep
iso
de
volu
mes
rem
ain
ed s
tab
le f
rom
200
7-08
to
201
2-13
wit
h t
he
hig
hes
t vo
lum
e b
ein
g f
or
cere
bra
l inf
arct
ion
wit
h 2
50 e
pis
od
es in
201
2-13
.
Ther
e w
as a
dec
line
in t
he
aver
age
len
gth
of
stay
fo
r al
l sel
ecte
d IC
D c
od
es w
ith
th
e ex
cep
tio
n o
f st
roke
, no
t sp
ecifi
ed w
hich
rem
ain
ed s
tead
y at
12.
8 d
ays
in 2
007-
08 a
nd
12.7
day
s in
201
2-13
. In
to
tal,
the
aver
age
len
gth
of
stay
dec
reas
ed f
rom
12.
4 d
ays
in 2
007-
08 t
o 8
day
s in
201
2-13
.
The
aver
age
NW
AU
fo
r se
lect
ed D
RGs
for
Live
rpo
ol H
osp
ital
in 2
012-
13 w
as 2
.3. T
his
is t
he
thir
d h
igh
est
for
SRP
site
s in
dic
atin
g a
hig
h p
atie
nt
com
ple
xity
.
The
firs
t g
rap
h in
Fig
ure
18
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
-pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 7
6
Fig
ure
18:
Liv
erp
oo
l Ho
spit
al IC
D-1
0 st
roke
ep
iso
des
an
d a
vera
ge
len
gth
of
stay
200
7-08
to
201
2-13
0 50
100
150
200
250
300
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Live
rpo
ol H
osp
ital
St
roke
by
sele
cted
ICD
-10.
Acu
te e
pis
od
es a
nd
ALO
S
Oth
er n
on-t
rau
mat
ic in
trac
ereb
ral
hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Year
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
14
16
18
20
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 7
7
15.1
.12
Roya
l Nor
th S
hore
Ho
spit
al
The
Roya
l No
rth
Sh
ore
Ho
spit
al h
ad a
to
tal o
f 34
20 a
cute
str
oke
ep
iso
des
by
sele
cted
DRG
s in
th
e p
erio
d 2
007-
08 t
o 2
012-
13. T
he
hig
hes
t vo
lum
e, a
s sh
ow
n in
Tab
le 1
6,
was
fo
r st
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s w
ith
415
ep
iso
des
in 2
012-
13.
Tab
le 1
6: R
oyal
No
rth
Sh
ore
Ho
spit
al s
elec
ted
str
oke
DR
Gs
2007
-08
to 2
012-
13
Acu
te e
pis
od
es A
R-D
RG
Roy
al N
ort
h S
ho
re H
osp
ital
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
4910
9932
6
2008
-09
5711
116
353
2009
-10
7225
143
353
2010
-11
6528
121
353
2011
-12
7218
116
405
2012
-13
659
139
415
Ther
e w
ere
3506
acu
te s
tro
ke e
pis
od
es f
or
sele
cted
ICD
co
des
fo
r th
e p
erio
d 2
007-
08 t
o 2
012-
13 r
epre
sen
tin
g t
he
hig
hes
t p
atie
nt
load
pre
sen
tin
g t
o S
RP
site
s at
8.4
% o
f
the
tota
l qu
anti
ty.
Cer
ebra
l inf
arct
ion
is t
he
hig
hes
t vo
lum
e an
d a
cco
un
ted
fo
r 25
6 ac
ute
ep
iso
des
in 2
012-
13. T
he
aver
age
len
gth
of
stay
has
dec
reas
ed f
or
all s
elec
ted
ICD
s fo
r th
e p
erio
d
2007
-08
to 2
012-
13 w
ith
th
e ex
cep
tio
n o
f o
ther
no
n-t
rau
mat
ic in
trac
ereb
ral h
aem
orr
hag
e, w
hich
sta
yed
sta
ble
at
7.7
day
s in
200
7-08
an
d 7
.6 d
ays
in 2
012-
13. I
n t
ota
l, th
e
aver
age
len
gth
of
stay
dec
reas
ed f
rom
9 d
ays
to 6
.8 d
ays
resp
ecti
vely
fo
r th
e sa
me
tim
e p
erio
d.
The
aver
age
NW
AU
fo
r se
lect
ed D
RGs
was
2.1
in 2
012-
13 s
igni
fyin
g h
igh
er c
om
ple
xity
th
an t
he
aver
age
for
NSW
in t
ota
l an
d S
RP
site
s co
mb
ined
.
The
firs
t g
rap
h in
Fig
ure
19
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 7
8
Fig
ure
19:
Roy
al N
ort
h S
ho
re H
osp
ital
ICD
-10
stro
ke e
pis
od
es a
nd
ave
rag
e le
ng
th o
f st
ay 2
007-
08 t
o 2
012-
13
0 50
100
150
200
250
300
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Ro
yal N
ort
h S
ho
re H
osp
ital
St
roke
by
sele
cted
ICD
-10
2007
/08
to 2
012/
13. A
cute
ep
iso
des
an
d A
LOS
Oth
er n
on-t
rau
mat
ic in
trac
ereb
ral
hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 7
9
15.1
.13
Sydn
ey A
dven
tist
Ho
spit
al
Syd
ney
Ad
ven
tist
Ho
spit
al is
a p
riva
te h
osp
ital
; th
eref
ore
AC
I do
es n
ot
hav
e ac
cess
to
ad
mit
ted
inp
atie
nt
dat
a fo
r th
e si
te. I
t is
an
tici
pat
ed t
hat
SR
P-sp
ecifi
c d
ata
will
be
colle
cted
fo
r St
age
two
of
this
eva
luat
ion
.
15.1
.14
St G
eorg
e H
osp
ital
St G
eorg
e H
osp
ital
had
a t
ota
l of
3407
acu
te s
tro
ke e
pis
od
es b
y se
lect
ed D
RG o
ver
the
per
iod
200
7-08
to
201
2-13
. As
sho
wn
in T
able
17,
th
e hi
gh
est
volu
me
was
fo
r st
roke
and
oth
er c
ereb
rova
scu
lar
dis
ord
ers
wit
h 4
19 e
pis
od
es f
or
2012
-13.
Tab
le 1
7: S
t G
eorg
e H
osp
ital
sel
ecte
d s
tro
ke D
RG
s 20
07-0
8 to
201
2-13
Acu
te e
pis
od
es A
R-D
RG
St
Geo
rge
Ho
spit
al
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
274
131
359
2008
-09
411
151
371
2009
-10
313
156
377
2010
-11
296
137
387
2011
-12
404
145
415
2012
-13
264
143
419
Wit
hin
th
ese
DRG
s, t
her
e w
ere
a to
tal o
f 35
62 a
cute
ep
iso
des
by
sele
cted
ICD
co
des
fro
m 2
007-
08 t
o 2
012-
13 a
cco
un
tin
g f
or
8.1%
of
the
tota
l pat
ien
t lo
ad p
rese
nti
ng
at
SRP
site
s in
201
2-13
. Thi
s is
th
e se
con
d h
igh
est
pat
ien
t lo
ad a
fter
Roy
al N
ort
h S
ho
re H
osp
ital
. As
sho
wn
in F
igu
re 2
1, t
he
hig
hes
t vo
lum
e w
as f
or
cere
bra
l inf
arct
ion
whi
ch
had
a 2
0% in
crea
se f
rom
238
ep
iso
des
in 2
007-
08 t
o 2
86 e
pis
od
es in
201
2-13
.
The
aver
age
len
gth
of
stay
dec
reas
ed f
or
all s
elec
ted
ICD
exc
ept
for
cere
bra
l inf
arct
ion
an
d s
tro
ke, n
ot
spec
ified
, whi
ch b
oth
rem
ain
ed s
tead
y at
aro
un
d 1
0 d
ays
and
5.5
day
s re
spec
tive
ly. I
n t
ota
l, th
e av
erag
e le
ng
th o
f st
ay d
ecre
ased
fro
m 8
.4 d
ays
in 2
007-
08 t
o 7
.6 d
ays
in 2
012-
13.
The
aver
age
NW
AU
fo
r 20
12-1
3 fo
r se
lect
ed D
RGs
was
1.9
. Thi
s is
co
nsi
sten
t w
ith
th
e SR
P av
erag
e.
The
firs
t g
rap
h in
Fig
ure
20
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 8
0
Fig
ure
20:
St
Geo
rge
Ho
spit
al IC
D-1
0 st
roke
ep
iso
des
an
d a
vera
ge
len
gth
of
stay
200
7-08
to
201
2-13
0 50
100
150
200
250
300
350
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
St G
eorg
e H
osp
ital
St
roke
by
sele
cted
ICD
-10
2007
/08
to 2
012/
13. A
cute
ep
iso
des
an
d A
LOS
Oth
er n
on-t
rau
mat
ic in
trac
ereb
ral
hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 8
1
15.1
.15
Wag
ga W
agga
Bas
e H
osp
ital
For
the
per
iod
200
7-08
to
201
2-13
, Wag
ga
Wag
ga
Bas
e H
osp
ital
had
a t
ota
l of
1380
acu
te s
tro
ke e
pis
od
es b
y se
lect
ed D
RGs.
Th
ere
wer
e n
o e
pis
od
es f
or
cran
ial p
roce
du
res
and
th
e hi
gh
est
nu
mb
er o
f ep
iso
des
bei
ng
fo
r st
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s w
ith
179
ep
iso
des
in 2
012-
13.
Tab
le 1
8: W
agg
a W
agg
a B
ase
Ho
spit
al s
elec
ted
str
oke
DR
Gs
2007
-08
to 2
012-
13
Acu
te e
pis
od
es A
R-D
RG
Wag
ga
Wag
ga
Bas
e H
osp
ital
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
03
5710
8
2008
-09
03
7118
3
2009
-10
01
7516
8
2010
-11
02
6813
8
2011
-12
01
6917
8
2012
-13
08
6817
9
Ther
e w
ere
1411
acu
te s
tro
ke e
pis
od
es b
y se
lect
ed IC
D c
od
es w
ith
a 9
4% in
crea
se in
th
e n
um
ber
of
cere
bra
l inf
arct
ion
ep
iso
des
fro
m 7
3 in
200
7-08
to
142
in 2
012-
13.
The
aver
age
len
gth
of
stay
is d
ecre
asin
g f
or
all I
CD
s w
ith
a t
ota
l co
mb
ined
dec
reas
e fr
om
6.2
day
s in
200
7-08
to
5 d
ays
in 2
012-
13.
Wag
ga
Wag
ga
Bas
e H
osp
ital
had
an
ave
rag
e N
WA
U f
or
sele
cted
DRG
s o
f 1.
4 w
hich
is s
ligh
tly
low
er t
han
th
e N
SW a
vera
ge
and
hig
her
th
an t
he
aver
age
for
SRP
site
s
com
bin
ed.
The
firs
t g
rap
h in
Fig
ure
21
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 8
2
Fig
ure
21:
Wag
ga
Wag
ga
Bas
e H
osp
ital
ICD
-10
stro
ke e
pis
od
es a
nd
ave
rag
e le
ng
th o
f st
ay 2
007-
08 t
o 2
012-
13
0 20
40
60
80
100
120
140
160
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Wag
ga
Wag
ga
Bas
e H
osp
ital
St
roke
by
sele
cted
ICD
-10
2007
/08
to 2
012/
13. A
cute
ep
iso
des
an
d A
LOS
Oth
er n
on
-tra
um
atic
intr
acer
ebra
l
hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 1 2 3 4 5 6 7 8 9
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 8
3
15.1
.16
Hor
nsb
y an
d K
u-R
ing
-Gai
Ho
spit
al
The
Ho
rnsb
y an
d K
u-R
ing
-Gai
Ho
spit
al h
ad a
to
tal o
f 11
7 ac
ute
str
oke
DRG
s fr
om
200
7-08
to
201
2-13
. Th
ere
wer
e n
o e
pis
od
es f
or
cran
ial p
roce
du
res
in t
his
tim
e an
d t
he
hig
hes
t vo
lum
e w
as f
or
stro
ke a
nd
oth
er c
ereb
rova
scu
lar
dis
ord
ers
wit
h 1
55 e
pis
od
es in
201
2-13
, as
sho
wn
in T
able
19.
Tab
le 1
9: H
orn
sby
and
Ku
-Rin
g-G
ai H
osp
ital
sel
ecte
d s
tro
ke D
RG
s 20
07-0
8 to
201
2-13
Acu
te e
pis
od
es A
R-D
RG
Ho
rnsb
y an
d K
u-R
ing
-Gai
Ho
spit
al
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
00
5112
1
2008
-09
02
4614
5
2009
-10
00
3916
3
2010
-11
02
5612
1
2011
-12
01
4814
9
2012
-13
01
7315
5
Wit
hin
th
ese
DRG
s, t
her
e w
ere
a to
tal o
f 12
04 a
cute
ep
iso
des
in t
he
sele
cted
ICD
co
des
, wit
h s
tead
y in
crea
ses
for
cere
bra
l inf
arct
ion
an
d T
IA, w
hile
th
e o
ther
s re
mai
ned
stab
le, a
s d
epic
ted
in F
igu
re 2
2 b
elo
w.
The
aver
age
len
gth
of
stay
dec
reas
ed s
tead
ily f
rom
7.1
day
s in
200
7-08
to
6.2
day
s in
201
2-13
.
The
aver
age
NW
AU
fo
r th
e se
lect
ed D
RGs
in 2
012-
13 w
as 1
.3. T
his
rep
rese
nts
a h
igh
er c
om
ple
xity
th
an t
hat
exp
erie
nce
d b
y n
on
-SR
P si
tes,
alt
ho
ug
h lo
wer
th
an t
he
NSW
aver
age
in t
ota
l.
The
firs
t g
rap
h in
Fig
ure
22
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 8
4
Fig
ure
22:
Ho
rnsb
y an
d K
u-R
ing
-Gai
Ho
spit
al IC
D-1
0 st
roke
ep
iso
des
an
d a
vera
ge
len
gth
of
stay
200
7-08
to
201
2-13
0 20
40
60
80
100
120
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Ho
rnsb
y an
d K
u-R
ing
-Gai
Ho
spit
al
Stro
ke b
y se
lect
ed IC
D-1
0 20
07/0
8 to
201
2/13
. Acu
te e
pis
od
es a
nd
ALO
S
Oth
er n
on-t
rau
mat
ic in
trac
ereb
ral h
aem
orr
hag
e
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 8
5
15.1
.17
Bla
ckto
wn
Ho
spit
al
Fro
m 2
007-
08 t
o 2
012-
13, t
ota
l of
stro
ke e
pis
od
es b
y se
lect
ed D
RGs
for
Blac
kto
wn
Ho
spit
al a
re s
ho
wn
in T
able
20.
Th
e hi
gh
est
volu
me
was
fo
r st
roke
an
d o
ther
cere
bro
vasc
ula
r d
iso
rder
s at
268
ep
iso
des
in 2
012-
13. T
her
e w
ere
no
cra
nial
pro
ced
ure
s d
uri
ng
thi
s ti
me.
Tab
le 2
0: B
lack
tow
n H
osp
ital
sel
ecte
d s
tro
ke D
RG
s 20
07-0
8 to
201
2-13
Acu
te e
pis
od
es A
R-D
RG
Bla
ckto
wn
Ho
spit
al
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
00
5623
0
2008
-09
00
9022
5
2009
-10
00
108
228
2010
-11
00
7923
6
2011
-12
04
111
242
2012
-13
00
135
268
Fro
m 2
007-
08 t
o 2
012-
13, t
her
e w
ere
a to
tal o
f 20
27 e
pis
od
es f
or
sele
cted
ICD
co
des
rep
rese
nti
ng
5.3
% o
f th
e to
tal p
atie
nt
load
pre
sen
tin
g t
o S
RP
site
s in
201
2-13
. Th
ere
wer
e in
crea
ses
in c
ereb
ral i
nfar
ctio
n f
rom
159
ep
iso
des
in 2
007-
08 t
o 1
97 in
201
2-13
an
d s
tro
ke, n
ot
spec
ified
fro
m 2
0 to
45
epis
od
es f
or
the
sam
e ti
me
per
iod
s.
The
aver
age
len
gth
of
stay
dec
reas
ed in
to
tal f
rom
7.2
day
s in
200
7-08
to
6.4
day
s in
201
2-13
. As
can
be
seen
in F
igu
re 2
3, t
her
e w
ere
incr
ease
s in
th
e av
erag
e le
ng
th o
f
stay
fo
r al
l IC
Ds
fro
m 2
009-
10 t
o 2
011-
12, b
efo
re t
his
aver
age
dec
reas
ed a
gai
n.
The
aver
age
NW
AU
fo
r th
e se
lect
ed D
RGs
is 1
.6 in
dic
atin
g h
igh
er p
atie
nt
com
ple
xity
th
an t
hat
fo
r N
SW in
to
tal a
nd
low
er t
han
th
e SR
P co
mb
ined
ave
rag
e o
f 1.
9.
The
firs
t g
rap
h in
Fig
ure
23
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 8
6
Fig
ure
23:
Bla
ckto
wn
Ho
spit
al IC
D-1
0 st
roke
ep
iso
des
an
d a
vera
ge
len
gth
of
stay
200
7-08
to
201
2-13
0 50
100
150
200
250
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Bla
ckto
wn
Ho
spit
al
Stro
ke b
y se
lect
ed IC
D-1
0 20
07/0
8 to
201
2/13
. Acu
te e
pis
od
es a
nd
ALO
S
Oth
er n
on
-tra
um
atic
intr
acer
ebra
l hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 8
7
15.1
.18
Co
nco
rd H
osp
ital
Co
nco
rd H
osp
ital
had
a t
ota
l of
1919
acu
te s
tro
ke e
pis
od
es f
or
sele
cted
DRG
s fr
om
200
7-08
to
201
2-13
. Th
e hi
gh
est
volu
me,
as
sho
wn
in T
able
21,
was
fo
r st
roke
an
d o
ther
cere
bro
vasc
ula
r d
iso
rder
s w
ith
256
ep
iso
des
in 2
012-
13.
Tab
le 2
1: C
on
cord
Ho
spit
al s
elec
ted
str
oke
DR
Gs
2007
-08
to 2
012-
13
Acu
te e
pis
od
es A
R-D
RG
Co
nco
rd H
osp
ital
C
ran
ial p
roce
du
res
Extr
acra
nia
l vas
cula
r p
roce
du
res
TIA
an
d p
rece
reb
ral o
cclu
sio
nSt
roke
an
d o
ther
cer
ebro
vasc
ula
r d
iso
rder
s
2007
-08
155
6422
4
2008
-09
213
5919
3
2009
-10
137
7121
3
2010
-11
184
8024
6
2011
-12
333
6023
3
2012
-13
96
8325
6
Wit
hin
th
ese
DRG
s th
ere
wer
e a
tota
l of
1947
ep
iso
des
fo
r se
lect
ed IC
D c
od
es f
or
the
per
iod
200
7-08
to
201
2-13
. Th
e hi
gh
est
volu
me
of
epis
od
es w
as f
or
cere
bra
l
infa
rcti
on
wit
h 1
71 e
pis
od
es in
201
2-13
rep
rese
nti
ng
a 2
5% in
crea
se f
rom
136
ep
iso
des
in 2
007-
08.
The
aver
age
len
gth
of
stay
dec
reas
ed in
to
tal f
rom
9.8
day
s in
200
7-08
to
8.3
day
s in
201
2-13
.
The
aver
age
NW
AU
fo
r th
e se
lect
ed D
RGs
was
2 in
201
2-13
sig
nify
ing
a s
ligh
tly
hig
her
pat
ien
t co
mp
lexi
ty t
han
SR
P si
tes
com
bin
ed a
vera
ge.
The
firs
t g
rap
h in
Fig
ure
24
sho
ws
the
epis
od
es o
f ca
re b
y se
lect
ed IC
D-1
0 co
des
. Th
ese
are
con
sist
ent
wit
h t
he
con
dit
ion
s th
at a
re a
sses
sed
fo
r el
igib
ility
fo
r th
rom
bo
lysi
s
at p
atie
nt
pre
sen
tati
on
an
d a
re s
ho
wn
her
e to
pro
vid
e an
ind
icat
ion
of
the
volu
me
of
epis
od
es. T
he
seco
nd
gra
ph
sh
ow
s th
e le
ng
th o
f st
ay in
day
s fo
r o
nly
th
e IC
D-1
0
epis
od
es t
hat
are
am
enab
le t
o t
hro
mb
oly
sis
to p
rovi
de
an in
dic
ativ
e p
ictu
re o
f an
y tr
end
s th
at m
ay b
e em
erg
ing
in in
pat
ien
t ca
re f
or
this
co
ho
rt.

Hea
lth
Econ
omic
s an
d Ev
alua
tion
Tea
m –
NSW
Str
oke
Rep
erfu
sion
Pro
gram
Eva
luat
ion
repo
rtPa
ge 8
8
Fig
ure
24:
Co
nco
rd H
osp
ital
ICD
-10
stro
ke e
pis
od
es a
nd
ave
rag
e le
ng
th o
f st
ay 2
007-
08 t
o 2
012-
13
0 20
40
60
80
100
120
140
160
180
200
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Episodes
Year
Co
nco
rd H
osp
ital
St
roke
by
sele
cted
ICD
-10
2007
/08
to 2
012/
13. A
cute
ep
iso
des
an
d A
LOS
Oth
er n
on
-tra
um
atic
intr
acer
ebra
l hae
mo
rrh
age
Stro
ke n
ot
spec
ified
Intr
acer
ebra
l hae
mo
rrh
age
Cer
ebra
l in
farc
tio
n
Tran
sien
t is
chae
mic
att
ack
0 2 4 6 8 10
12
14
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
Days
Year

Health Economics and Evaluation Team – NSW Stroke Reperfusion Program Evaluation Report Page 89
Appendix III