
NSAIDs.ppt
34
Dr Khulood Alsaraf Dr Khulood Alsaraf
-
Upload
alikhasaki -
Category
Documents
-
view
115 -
download
2
description
فارما
Transcript of NSAIDs.ppt
Dr Khulood AlsarafDr Khulood AlsarafDr Khulood AlsarafDr Khulood Alsaraf

Inflammation
-The classical signs of inflammation are redness, swelling, heat, pain & loss of function. -The actual expression of these processes depend on the site of inflammation for e.g skin abscess may result in the appearance of all of these features. -In contrast, pneumonia, bec. of inaccessibility of the lung to examination, may manifest only as loss of function [ shortness of breath & hypoxia ].-Inflammation is characterized by the occurrence of several processes.-Initiation of the event by a foreign subs. or physical injury, recruitment & chemoattraction of inflammatory mediators capable of damaging or killing an invading microbe or tumor.-Inflammation can also result from an auto-immune Inflammation can also result from an auto-immune response to the host’s own tissue, as occurs in rheumatoid response to the host’s own tissue, as occurs in rheumatoid arthritis.arthritis.
The inflammatory process:The inflammatory process:Inflammation begins when a stimulus, such as Inflammation begins when a stimulus, such as infection, Physical stress, or chemical stress, infection, Physical stress, or chemical stress, produces cellular damage. This damage initiates produces cellular damage. This damage initiates the activation of transcription factors that the activation of transcription factors that control the expression of many inflammatory control the expression of many inflammatory mediators.mediators. Among the more important inflammatory Among the more important inflammatory mediators are: eicosanoids, biological oxidants, mediators are: eicosanoids, biological oxidants, cytokines, adhesion factors, and digestive cytokines, adhesion factors, and digestive enzyme (proteases, hyaluronidase, collagenase, enzyme (proteases, hyaluronidase, collagenase, and elastase)and elastase)

The inflammatory response changes with time & can be divided into phases :-
The rapid phase occurs with in seconds to min. & consist of :- -Vasodilation -Increased blood flow -Edema -Pain The acute phase is charac. by induction of inflammatory genes by NF-kB & other transcription factors, during this phase, moderate amounts of inflammatory mediators are produced
The chronic phase occurs over months to years & is marked by dramatically increased production of inflammatory mediators. The secondary chronic phase occurs after years of oxidative damage has degraded blood vessels & tissues Such chronic inflammation appear to play a role in many disease state, such as arteriosclerosis & cancer.

Treatment of inflammation
1-Relief the pain which is the main symptoms.
2-Slow or arresting of the tissue – damaging process.
So Antiinflammatory drugs are divided into :-
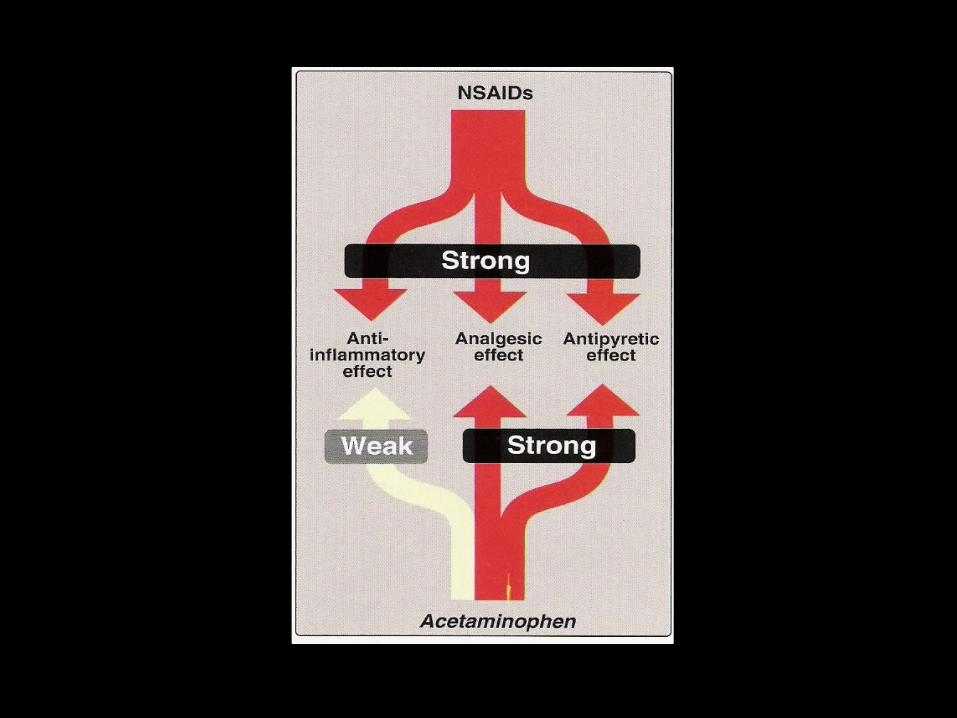
1- NSAIDs which have an antiinflammatory, analgesic & antipyretic effects & useful for treatment of both acute & chronic inflammation.
2- Steroids which have a powerful antiinflammatory effect but long or chronic use of steroid associated with many side effects or toxic effects.
3- Disease – modifying anti Rheumatic drugsThey slow the bone damage associated with the Rhumatoid arithritis & they are more toxic than NSAIDS.

NSAIDs
-Have a variety of clinical uses as antipyretic, analgesic, & antiinflammatory effect.-They reduce body Temp. in febrile states & thus are effective as antipyretics.-They are useful as analgesic, relieving mild to moderate pain such as myalgia, dental pain, dysmenorrhea & headache. -They are also used to treat the chronic pain & inflammation Rhumatoid arithritis, osteoartritis & ankylosing spondylitis.


Mechanism of action
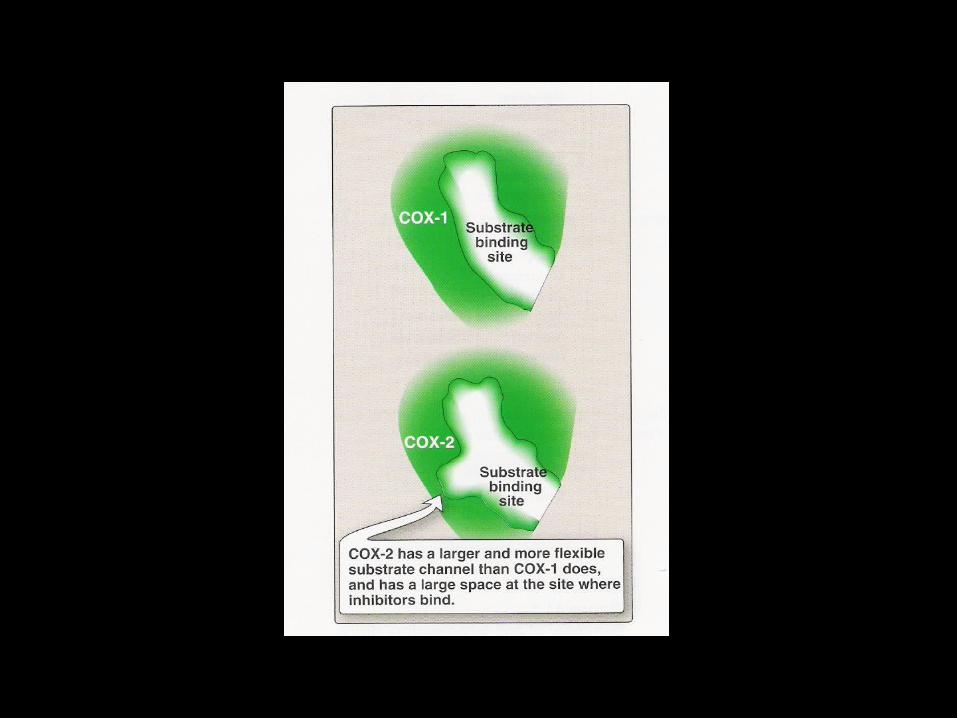
-The antiinflammatory actions of the NSAIDs are most likely explained by their inhibition of PG syn. By COX2 .-The COX2 isoform is the predominant COX involved in production of PGs during inflammatory processes .-PGs of the E & F series evoke some of the local & systemic manifestation of inflammation, such as vasodilation, increased vascular permeability, swelling, pain, & increased leukocyte migration. -They intensify the effect of inflammatory mediators such as histamine, bradykinin, & 5HT-All NSAIDs [except the COX2 – selective agents] inhibit both Cox isoform & the degree of inhibition of COX1 varies from drug to drug.
Home workHome workProstaglandins Prostaglandins What is ------prostaglandinsWhat is ------prostaglandinsRole of PGs as local mediatorsRole of PGs as local mediatorsSynthesis of PGsSynthesis of PGsTypes of PGsTypes of PGsActions of PGsActions of PGsTherapeutic uses of PGsTherapeutic uses of PGs

Adverse effects
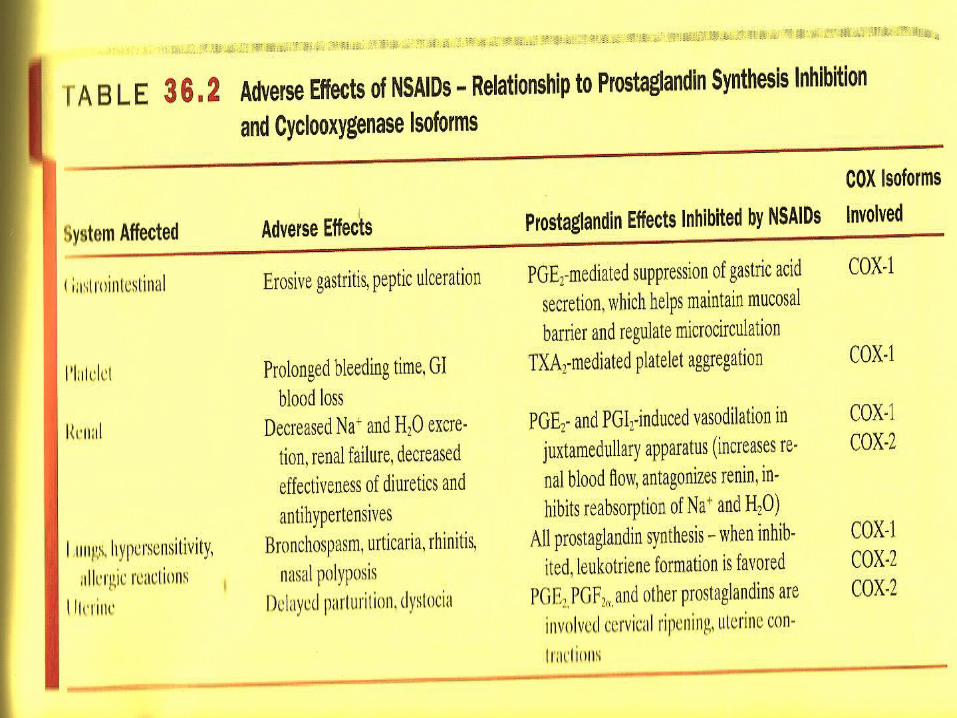
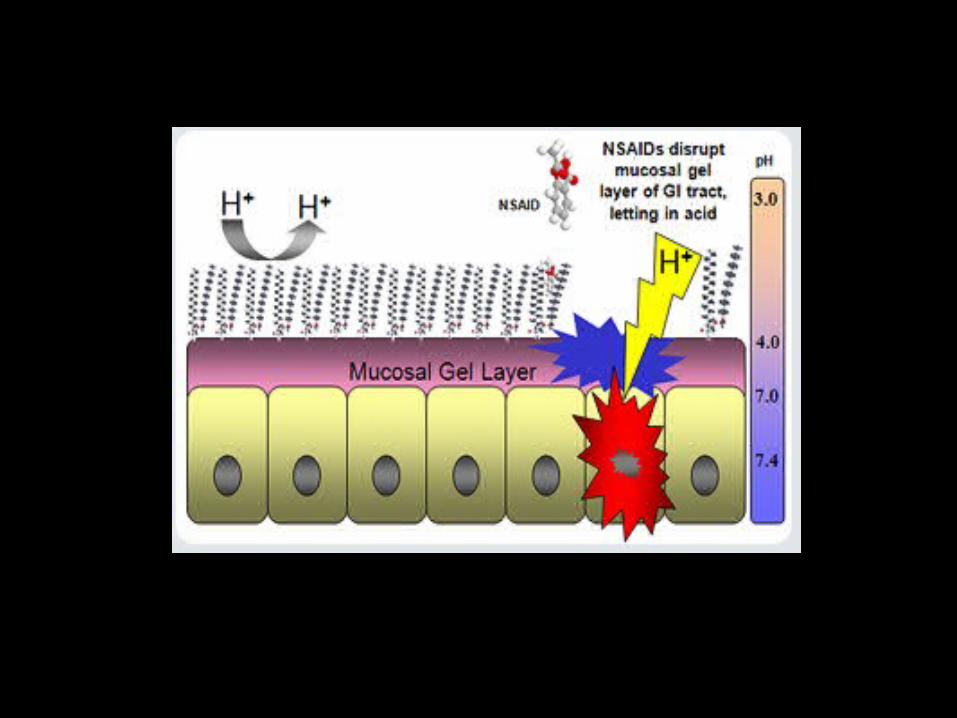
-The ability of NSAIDs to increase gastric acid secretion & inhibit blood clotting can lead to GI toxicity -They can impair renal function, cause fluid retention & provoke hypersensitivity reactions, including :-Bronchospasm, aggravation of asthma, urticaria, nasal polyps & rarely anaphylactic reactions. -Developed drugs selectivity inhibit COX2 & there for do not elicit the GI & antiplatelet side effects common to drug that inhibit COX1. -Other side effects not related to PG syn. :--Hepatic necrosis, Cholestatic jaundice, Photosensitivities, Headache, Dizziness, Tinnitus, Confusion & Nervousness
CI -In patient with history of ulcer disease -In patient with renal impairment, heart failure, hypertension, & edema [ used with caution] -Hypersensitivity to salicylate or any other NSAIDs (like (like asthmatic patients)asthmatic patients)
A significant number of drug interactions are common to A significant number of drug interactions are common to most of the NSAIDs.most of the NSAIDs.GI toxicity increased by concomitant treatment with GI toxicity increased by concomitant treatment with corticosteroids.corticosteroids.Certain NSAIDs can also compete for protein binding sites Certain NSAIDs can also compete for protein binding sites with warfarin.with warfarin.NSAIDs can decrease the clearance of methotrexate, NSAIDs can decrease the clearance of methotrexate, resulting in severe hematological and GI toxicity.resulting in severe hematological and GI toxicity.Because NSAIDs, decrease PG synthesis in the kidney, these Because NSAIDs, decrease PG synthesis in the kidney, these drug can increase the nephrotoxicity of agents such as drug can increase the nephrotoxicity of agents such as aminoglycosides, amphotericin B, cisplatin, ganciclovir and aminoglycosides, amphotericin B, cisplatin, ganciclovir and vancomycin.vancomycin.

Classification of NSAIDs
NSAIDs are classified according to their selectivity to COX1 or COX2 into :-
1- Less selective for COX1 :- Ibuprofen & Paracetamol
2- Equipotent on both enzymes :- Naproxen & Diclofenac
3- Relative selective for COX1 :- Aspirin & Indomethacin
4- More selective for COX2 :- Meloxicam, Celecoxib

Specific NSAIDsAspirin and other salicylic acid
derivatives
Salicylates -Is a weak organic acid that is unique among the NSAIDs, in irreversibly acetylating & [ thus inactivating ] cyclooxygenase. -It decreases inflammation & pain by inhibiting COX2, however when COX1 decreased, the stomach lining is not protected, thus stomach ulcer & bleeding may occur. -The anti-inflammatory and antipyretic effects of salicylates are due to blockade of PG synthesis in the thermoregulatory centers in the hypothalamus and at peripheral target sites.-Salicylates prevents the senistization of pain receptors to both mechanical and chemical stimuli.
Pharmacological effects of aspirin
1- Antiinflammatory effectIn addition to reducing the syn. of PG, aspirin also interferes with the chemical mediators of Kallikren system as a result :- A- inhibit granulocyte to damaged vasculature.B- stabilizes lysosomes.C- inhibits the migration of polymorphonuclear leukocyte & macrophages into the site of inflammation.
2- Analgesic effectIts effective in reducing mild to moderate pain of somatic type but not useful in visceral pain . It alleviates pain of muscular, vascular & dental origin & arthritis. aspirin acts peripherally through it is effect on inflammation but also inhibits pain stimuli at subcortical site
3- Antipyretic effect
-Aspirin reduces the elevated body Temp. by impeding PGE2 synthesis and release & also related to increase heat loss by vasodilation of superficial blood vessels & increased sweating.
4- Effect on platelets [ effect on homeostasis ]
-Single low doses of aspirin [ about 80 mg ] produce a slight increase in the bleeding time & this occur due to inhibition of platelets aggregation secondary to inhibition of thromboxane syn.

Clinical uses Analgesic and antipyreticAnalgesic and antipyreticExternal application: External application: salicylic acid used topically to treat salicylic acid used topically to treat corns and epidermaphytosis (eruption caused by fungi).corns and epidermaphytosis (eruption caused by fungi).Cardiovascular application: Cardiovascular application: due to inhibition of platelet due to inhibition of platelet aggregation and low doses of Aspirin used prophylactically aggregation and low doses of Aspirin used prophylactically to decrease the incidence of transient Ischemic attack, to decrease the incidence of transient Ischemic attack, unstable angina and coronary artery thrombosis.unstable angina and coronary artery thrombosis.

Side effects 1- gastric & intestinal mucosal damage2- prolongation of bleeding time3- skin allergy [ rashes ] & other allergic reaction 4- Raye’s syndrom5- nephrotoxicity
C.I C.I -In asthmatic patients In asthmatic patients -In children under 12 yearsIn children under 12 years-In bleeding disorder In bleeding disorder -In gouty patients In gouty patients
Mild to sever toxicity occur with Aspirin if administered in Mild to sever toxicity occur with Aspirin if administered in high doses.high doses. Mild one (also called salicylism) characterized by:Mild one (also called salicylism) characterized by:Nausea and vomiting, Hyperventilation, Mental confusion, Nausea and vomiting, Hyperventilation, Mental confusion, Headache, Dizziness, Tinnitus (ringing in the ear)Headache, Dizziness, Tinnitus (ringing in the ear) Sever toxicity occur when large doses of Aspirin are Sever toxicity occur when large doses of Aspirin are administered and characterize by:administered and characterize by:Restlessness, Delirium , Hallucination, Convulsion, ComaRestlessness, Delirium , Hallucination, Convulsion, ComaRespiratory and metabolic acidosis and death from Respiratory and metabolic acidosis and death from respiratory failure.respiratory failure.
TreatmentTreatmentIn mild cases, symptomatic treatment are sufficient and In mild cases, symptomatic treatment are sufficient and sometime increasing urinary PH enhances the elimination of sometime increasing urinary PH enhances the elimination of salicylate.salicylate.In serious cases, fluid I-V administration, dialysis and In serious cases, fluid I-V administration, dialysis and correction of acid-base and electrolyte balanced.correction of acid-base and electrolyte balanced.


Other NSAIDs
A- propionic acid derivatives Ibuprofen, Fenoprofen, Flurbiprofen, Ketoprofen, Naproxen
- Equal selectivity for COX1 &COX2
-Well absorbed orally, totally bound to serum albumin & inactivated by metabolism.
-All of these drugs posses antiinflammatory, analgesic, & antipyretic activity Useful in treatment of chronic rheumatoid & osteoarthritis & preferable on aspirin bec. GI effects less intense than aspirin.
-The common S.E of this groups are:1-GI disorder ranging from dyspepsia to bleeding 2-CNS S.E like headache, tinnitus & dizziness.
B-Acetic-acid derivativesIndomethacin, Sulindac, Tolmetin
Indomethacin moderate selective for COX1, more potent than aspirin as an antiinflammatory agent & used in the following condition: 1-More selective in relieving inflammation with acute gouty arthritis, ankylosing spondylitis & osteoarthritis of the hip.
2-Effective in treating patent ductus arteriosus
Side effects-GIT,nausea, vomiting, diarrhea, & abdominal pain -Frontal headache, dizziness, & vertigo -Hypersensitivity like rash, urticaria, itching & acute attack of asthma. Sulindac prodrug, metabolized to an active sulfide metabolite
Not highly concentrated at gastric mucosa, so that the incidence of GI S.E is lower than for Indomethacin

C-Fenamates derivativesMefenamic acid & Meclofenamate
Mefenamic acid indicated for analgesic & primary dysmenorrhea when therapy will not exceed 1 week.
Meclofenamate sodium for rheumatoid arthritis& osteoarthritis
D-Oxicam derivativesPiroxicam, Meloxicam Meloxicam & Piroxicam long half-life allows for once-daily dosing Piroxicam indicated for rheumatoid arthritis & osteoarthritis Meloxicam also indicated for rheumatoid arthritis& osteoarthritis & certain acute condition More selective to COX-2 frequency of GI S.E is lower than Piroxicam and other NSAIDs
E-Heteroaryl acetic derivatives
Diclofenac rheumatoid arthritis, osteoarthritis, ankylosing spondylitis, dysmenorrhea & topically for the treatment of ocular inflammation & actinic keratosis
F-Selective COX-2 inhibitors (sulfonyl phenyl derivatives)
Celecoxib -Highly COX-2 inhibitors less erosion of the GI mucosa & cause less inhibition of platelet aggregation than do the nonselective COX inhibitors -Indicated for the treatment of rheumatoid arthritis, osteoarthritis, and acute to moderate pain.-Headache, dyspepsia, diarrhea, and abdominal pain are the most common adverse effects


Paracetamol (Acetaminophen)
-Inhibit PG synthesis in CNS explain their antipyretic & analgesic properties.-Less effects on peripheral COX weak antiinflammatory activity -No effect on platelet function
Clinical uses 1-Analgesic & antipyretic, specially for those whose suffer from gastric irritation 2-Drug of choice as analgesic & antipyretic for children with viral infection3-Drug of choice for gouty patients bec. it dose not antagonize the uricosuric agents like probenecid.
Side effects With normal therapeutic doses paracetamol is free of significant S.E Skin rash, minor allergic reaction, minor alteration in leukocyte count may be occur. Prolonged & large dose therapy 1- hepatic necrosis 2- renal tubular necrosis

Disease modifying antirhaumatic drugs
Rhaumatic diseasesA chronic inflammatory disease with frequent acute attacks.The immune system is involved in attacking the joints and surrounding structure such as muscle tendons and most other connective tissue. There is inflammation of the synovial membrane.
-DMARDs are chemically diverse class of agents, all of which have varying capacity to slow the progression of disease -Their action manifest over the course of week to months; they are usually employed in combination with NSAIDs some time other DMARDs
Disease modifying antirhaumatic drugs
1-Cytotoxics : Azothioprine and Methotrexate 2-Gold peparations : Auranofin3-Biological response modifiers : Etanercept, Rituximab & Infliximab4-Other DMARDs : Cyclosporine, Hydroxychloroquine, Penicillamine and Sulfasalazine

Drugs employed in the treatment of GoutGout Hereditary metabolic disease that is a form of acute arthritis and is marked by inflammation of joints.Gout associated with increased body stored of uric acid.Acute attacks involve joint inflammation caused by precipitation of uric acid crystals.hyperuricemia urate crystal in joints inflammatory responseMost therapeutic strategies for Gout involve lowering the uric acid level below the saturation point (below 6mg/dl), thus preventing the deposition of urate crystals.This can accomplished by:
1- interfering with uric acid synthesis with Allopurinol2- increasing uric acid excretion with Probenecid3- inhibiting leukocyte entry into affected joint with Colchicine4- administration of NSAIDs



















