November/December 2008, Vol 1, No 9
99
NOVEMBER/DECEMBER 2008 VOLUME 1, NUMBER 9 ©2008 Engage Healthcare Communications, LLC www.AHDBonline.com THE PEER-REVIEWED FORUM FOR EVIDENCE IN BENEFIT DESIGN ™ e-Prescribing: A Move Toward Appropriate Medication Use Jack E. Fincham, PhD, RPh Erythropoiesis-Stimulating Agents in a Meta-Stable State: Guidelines, Economics, and Policy in Flux Interview (Part 2) with Samuel M. Silver, MD, PhD Role for Automated Communication Strategies in Medication Adherence Management S. Michael Ross, MD, MHA An Overview of Cholesterol Management Robyn A. Burns Schaiff, PharmD, BCPS; Richard M. Moe, MD, PhD; Daniel W. Krichbaum, PharmD ◆ Generic Drug Trends ◆ FDA Watch ◆ Medical Tourism ◆ AHA Meeting Highlights ◆ AMCP Meeting Highlights REGULATORY CLINICAL BUSINESS EDITORIAL DEPARTMENTS ™
-
Upload
dalia-buffery -
Category
Documents
-
view
228 -
download
3
description
American Health & Drug Benefits
Transcript of November/December 2008, Vol 1, No 9

NOVEMBER/DECEMBER 2008 VOLUME 1, NUMBER 9
©2008 Engage Healthcare Communications, LLCwww.AHDBonline.com
THE PEER-REVIEWED FORUM FOR EVIDENCE IN BENEFIT DESIGN™
e-Prescribing: A Move Toward Appropriate Medication UseJack E. Fincham, PhD, RPh
Erythropoiesis-Stimulating Agents in a Meta-Stable State: Guidelines,Economics, and Policy in FluxInterview (Part 2) with Samuel M. Silver, MD, PhD
Role for Automated Communication Strategies in Medication Adherence ManagementS. Michael Ross, MD, MHA
An Overview of Cholesterol ManagementRobyn A. Burns Schaiff, PharmD, BCPS; Richard M. Moe, MD, PhD; Daniel W. Krichbaum, PharmD
◆ Generic Drug Trends ◆ FDA Watch ◆ Medical Tourism◆ AHA Meeting Highlights◆ AMCP Meeting Highlights
REGULATORY
CLINICAL
BUSINESS
EDITORIAL
DEPARTMENTS
™
Covers_NovDec.qxp:Cover 11/25/08 10:35 AM Page C1

Covers_NovDec.qxp:Cover 11/25/08 10:36 AM Page C2

TOC_Editorial_NovDec.qxp:Cover 11/25/08 10:37 AM Page 1

2 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
6 e-Prescribing: A Move Toward Appropriate Medication UseJack E. Fincham, PhD, RPh
14 Erythropoiesis-Stimulating Agents in a Meta-Stable State: Guidelines, Economics, and Policy in FluxInterview (Part 2) with Samuel M. Silver, MD, PhDStakeholder Perspective by F. Randy Vogenberg, RPh, PhD
20 Role for Automated Communication Strategies in Medication Adherence ManagementS. Michael Ross, MD, MHAStakeholder Perspective by Geoffrey P. Cole, MD, MBA
34 An Overview of Cholesterol ManagementRobyn A. Burns Schaiff, PharmD, BCPS; Richard M. Moe, MD, PhD; Daniel W. Krichbaum, PharmDStakeholder Perspective: JUPITER by Wayne KuznarStakeholder Perspective by Thomas McCarter, MD, FACP
NOVEMBER/DECEMBER 2008 VOLUME 1, NUMBER 9
CLINICAL
EDITORIAL
BUSINESS
™ ™
PublisherNicholas [email protected]
Associate PublisherMaurice [email protected]
National Account ManagerCristopher [email protected]
Editorial DirectorDalia [email protected]
Associate EditorLara J. Reiman732-992-1892
Senior Production ManagerRobyn Jacobs
Business ManagerBlanche Marchitto
PresidentBrian F. [email protected]
Editor-in-ChiefRobert E. [email protected]
American Health & Drug Benefits is founded onthe concept that health and drug benefitshave undergone a transformation: the econo-metric value of a drug is of equal importanceto clinical outcomes as it is to serving as thebasis for securing coverage in formularies anddrug benefit designs. Benefit designs are great-ly affected by numerous clinical, business, andpolicy conditions.
This publication provides benefit design deci-sion makers the integrated industry informa-tion they require to devise formularies anddrug benefit designs that stand up to today’sspecial healthcare delivery and business needs.
Contact Information:For reprints, subscription information, andeditorial queries, please contact:[email protected]
T: 732-992-1880F: 732-992-1881
Mission Statement
REGULATORY
Continued on page 4
American Health & Drug Benefits is included in the following indexing and database services:
Cumulative Index to Nursing and Allied Health Literature (CINAHL)
EBSCOhost research databases (EBSCO)
10 GENERIC DRUG TRENDSFocus on Lowest Net Cost Drug Reduces Costs for Patients, Plan SponsorsDana H. Felthouse, MBA
32 FDA WATCHThe Obama Administration and the FDAMark Senak, JD
DEPARTMENTS
TOC_Editorial_NovDec.qxp:Cover 11/25/08 10:37 AM Page 2

If it matters to patients, it matters to us. That’s why Eli Lilly and Company is
committed to providing the programs, services, and manpower that help you deliver
positive outcomes for the patients under your care. And while health care may be a
numbers game, we’re interested in the one number that matters most.
One focus. One promise. One patient at a time.
1120
145,827
more person with time to focus on her family
health care professionals dedicated to providing answers
lives touched by Lilly assistance programs
MG53855 COPYRIGHT © 2008 ELI LILLY AND COMPANY.All numbers current as of January 2008.
100668_014_AHDB_Mother_112008.indd 1 11/18/08 4:31:17 PM
TOC_Editorial_NovDec.qxp:Cover 11/25/08 10:37 AM Page 3

4 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
Clinical EditorThomas McCarter, MD, FACPChief Clinical OfficerExecutive Health [email protected]
Business/Government EditorKip Piper, MA, CHEPresident, Health Results [email protected]
ActuaryDavid Williams
Clinical ResearchNirav R. Shah, MD, MPHSamuel M. Silver, MD, MPHMichael A. Weber, MD
EmployersAlberto M. Colombi, MD, MPHArthur F. Shinn, PharmD, FASCPF. Randy Vogenberg, RPh, PhD
Health Information TechnologyJ.B. Jones, ABD, MBA
Healthcare OutcomesGary M. Owens, MD
Managed Care & Government AffairsSharad Mansukani, MD
Managed Markets MarketingJeffrey A. Bourret, MS, RPh, FASHPCharles E. Collins, Jr, MS, MBA
Outcomes ResearchGordon M. Cummins, MSTimothy S. Regan, BPharm, RPh
Patient AdvocacyWilliam E. Fassett, PhD, RPh, MBA
PharmacoeconomicsJeff Jianfei Guo, BPharm, MS, PhD
Pharmacy Benefit DesignJan E. Berger, MD, MJJoel V. Brill, MDPaul A. Polansky, BSPharm, MBAScott R. Taylor, RPh, MBA
Pharmacy & Specialty ProductsJames T. Kenney, RPh, MBA
Policy & Public HealthJoseph R. Antos, PhDAlex A. Hathaway, MD, MPH, FACPMJack E. Fincham, PhD, RPh
Reimbursement PolicyMichael Schaffer, PharmD, MBAGrant D. Lawless, MD, BSPharm, FACP
Research & DevelopmentMichael F. Murphy, MD, PhDWayne A. Rosenkrans, Jr, PhD
NOVEMBER/DECEMBER 2008 VOLUME 1, NUMBER 9
American Health & Drug Benefits, ISSN 1942-2962 (print); ISSN 1942-2970 (online), is published 9 times a year by Engage HealthcareCommunications, LLC, 241 Forsgate Drive, Suite 205B, Monroe Township, NJ 08831. Copyright © 2008 by Engage Healthcare Communications,LLC. All rights reserved. American Health & Drug Benefits and The Peer-Reviewed Forum for Evidence in Benefit Design are trademarks of EngageHealthcare Communications, LLC. No part of this publication may be reproduced or transmitted in any form or by any means now or here-after known, electronic or mechanical, including photocopy, recording, or any informational storage and retrieval system, without written per-mission from the Publisher. Printed in the United States of America. Address all editorial correspondence to: [email protected],Telephone: 732-992-1889. Fax: 732-992-1881. American Health & Drug Benefits, 241 Forsgate Drive, Suite 205A, Monroe Township, NJ 08831.
POSTMASTER: CORRESPONDENCE REGARDING SUBSCRIPTIONS OR CHANGE OF ADDRESS should be directed to CIRCU-LATION DIRECTOR, American Health & Drug Benefits, 241 Forsgate Drive, Suite 205A, Monroe Township, NJ 08831. Fax: 732-992-1881.YEARLY SUBSCRIPTION RATES: One year: $99.00 USD; Two years: $149.00 USD; Three years: $199.00 USD.
Permission requests to reprint all or part of any article published in this journal should be addressed to REPRINT PERMISSIONS DEPART-MENT, Engage Healthcare Communications, LLC, 241 Forsgate Drive, Suite 205A, Monroe Township, NJ 08831. The ideas and opinionsexpressed in American Health & Drug Benefits do not necessarily reflect those of the Editorial Board, the Editors, or the Publisher. Publicationof an advertisement or other product mentioned in American Health & Drug Benefits should not be construed as an endorsement of the prod-uct or the manufacturer’s claims. Readers are encouraged to contact the manufacturers about any features or limitations of products mentioned.Neither the Editors nor the Publisher assume any responsibility for any injury and/or damage to persons or property arising out of or related toany use of the material mentioned in this publication.
™ ™
37
WEB EXCLUSIVE www.AHDBonline.com
•2008 Annual Index •2008 List of Peer Reviewers •Payer Pulse: Use of Comparative Effectiveness Analysis in Managed Care•AMCP: Humana’s Tools Help Members Navigate Medicare Part D
CAPTION CONTEST
8
UNMANAGED MOMENT
DEPARTMENTS
Continued
34 AHA MEETING HIGHLIGHTSThe Antiplatelet Drug Pipeline: Some Promising CandidatesBy Wayne Kuznar
36 AMCP MEETING HIGHLIGHTS• Specialty Pipeline Dominated by Biologics
• Real-World Data Better than RCTs for Formulary DecisionsBy Alice Goodman
49 MEDICAL TOURISMPromotion of Medical Tourism in the Media Creates a Trend J. Warren Salmon, PhD
52 EXECUTIVE SUMMARIES
TOC_Editorial_NovDec.qxp:Cover 11/25/08 10:37 AM Page 4

The only complete line of strengths for dosing flexibility
Stock OXYCODONE HCI from ETHEX today and be ready for prescription requests!• Generically priced• Supported by an awareness campaign
to prescribers• Patient Sample Vouchers, redeemable at
the pharmacy, offer a free trial of 10 mg or20 mg tablets (with a valid prescription,void where prohibited by law)
For more information log on towww.ethex.com or call 1-888-567-9176.
NDC 58177-625-04 5 mg 100’sNDC 58177-625-11 5 mg 10x10 UD
NDC 58177-461-04 10 mg 100’s
NDC 58177-445-04 15 mg 100’s
NDC 58177-462-04 20 mg 100’s
NDC 58177-446-04 30 mg 100’s
TOC_Editorial_NovDec.qxp:Cover 11/25/08 10:38 AM Page 5

6 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
The way physicians order medicationsfor patients has not changed for morethan a century. New technologies,
including electronic prescribing (e-prescrib-ing), make the handwritten prescriptionseem like an archaic link to the past.
e-Prescribing has been defined as the useof computing devices to enter, modify,review, and output or communicate drugprescriptions.1 The earliest application of physiciansordering medications and other therapies by computerwas in hospitals in the 1970s; it became more promi-nent when the US Institute of Medicine endorsed itsuse as a way to reduce the 98,000 annual deaths frommedication errors among hospitalized patients.2
Now we see the promotion of e-prescribing fromvarying parties. Current physician use of e-prescribingis estimated to be between 3% and 18%, depending onthe definition used.
The need to change how drugs are ordered stemsfrom the tremendous duplication, waste, and ineffi-ciency in the current prescribing of medications. Oneof the earliest mentions of e-prescribing in the medicalliterature was in the early 1990s in a study conductedin Wales, which profiled the use of computers for refillprescription prescribing (ie, repeat prescribing).3 Asmall percentage (11%) of the Welsh physicians usedcomputers for this purpose.3 The authors concluded thearticle with an exhortation that, “Mechanisms toencourage greater and more sophisticated use of com-puters and information technology need to beexplored.”3 In the United States, e-prescribing wastouted in the mid-1990s as a means to more accuratelytransmit physicians’ orders.4 Others suggested that itwould lead to enhanced medication use in hospitalsand beyond.5 Medicare has begun a process of incen-tivizing physicians who successfully use e-prescribingover a 4-year period. These payments amount to a 2%
incentive in 2009 and 2010, 1% in 2011 and2012, and 0.5% in 2013.6
Alaska became the last of the 50 USstates to enable e-prescribing in mid-August2007. Varying estimates have suggested that21% of physicians have access to informa-tion technology with e-prescribing systemsin place.7 A recent survey showed thatalthough a vast majority of the physicians
surveyed (85%) think e-prescribing is a “good idea,”only 7% use the technology at present.8
Several observations are important. Small, inde-pendent pharmacies have been slow to upgrade theirpharmacy management systems to accept e-prescrip-tions because of large fees charged by software vendors.Large chain pharmacies embrace e-prescribing at thecorporate level, but local store support is low, and thereis inadequate training of pharmacy staff.9
The Limits of e-Prescribing A number of problems related to the prescribing,
dispensing, and drug-use process will not be influencedby e-prescribing. Some of these are drug-specific,patient-specific, or system-specific. Patient medicationnoncompliance and persistence, over the counter(OTC) drug misuse, adverse drug reactions, prescribingerrors, and/or dispensing errors are commonplace. Nosystems yet devised or planned can totally eliminatethese problems from negatively influencing appropriatedrug use in the US healthcare system.
There are fundamental flaws in the drug-use processin the United States. Medication compliance hoversaround 50%, and prescription drug misuse is rampant.OTC medications are misused. Adverse drug events(often preventable) occur because of inadequate infor-mation available. Antibiotic misuse and overuse hasled to many drug-resistant strains. Despite recentchanges to Medicare with the Part D program, manypatients remain uninsured for prescription medica-tions. e-Prescribing will not by itself affect these andother systemic medication-related error-producing sys-tem segments.
Despite elaborate and sophisticated health informa-tion technology (HIT)-enabled e-prescribing, errorswill continue to be made. Physicians have the potential
Dr Fincham is Professor of Pharmacy Practice andAdministration, University of Missouri School of Pharmacy,Kansas City, MO. His new book, e-Prescribing:The Electronic Transformation of Medicine, will be published in 2009. Some material from the book is presentedin this editorial.
e-Prescribing: A Move Toward AppropriateMedication UseJack E. Fincham, PhD, RPh
EDITORIAL
TOC_Editorial_NovDec.qxp:Cover 11/25/08 10:38 AM Page 6

7www.AHDBonline.comVOL. 1 NO. 9
to make errors in prescribing (wrong patient; rightpatient wrong drug; wrong dose and/or wrong durationof therapy). Pharmacists also commit errors in dispens-ing, labeling, misreading orders, and/or dispensing tothe wrong patient. Patients are also able to underdose,overdose, use the wrong drugs for the wrong length oftime, and/or use the right drug for the wrong period oftime.
A startling 15% of diagnoses are estimated to bemade in error.10 Groopman further suggests that 80% ofthese errors are predictable, based on the compressedand hurried fashion in which physicians now diagnosepatients’ maladies.10 e-Prescribing will not reverse thisrate of inaccuracy. If the right drug is prescribed for thewrong diagnosis, the patient will always suffer.
The Benefits of e-Prescribinge-Prescribing provides enhanced decision support
for the selection of prescription products, informationabout formularies, dosing and frequency of such formu-laries, checking for allergies to particular medications,drug interactions, avoidance of therapeutic duplica-tion, and maximum or minimum doses. Many havenoted that e-prescribing can provide computer-basedsupport for creation, transmission, dispensing, andmonitoring of drug therapies. Clinical decision supportand computerized physician order entry have madeimpacts on medication errors and have been promotedas providing a major opportunity to make huge inroadson medication errors.11
e-Prescribing has been suggested to reduce clinicalrisk management and provide operational efficiency aswell as access to electronic patient records. Enablingclinical risk management and enhanced communica-tion can reduce the incidence of adverse drug events. e-Prescribing can provide a more accurate detailing ofprescriptions and associated records.
Reduced Drug SpendingSpending on drugs as a percentage of the total US
healthcare spending increased slightly between 2006and 2007, from 10.07% to 10.14%.12 Drivers for the sig-nificant costs of medications include increased tech-nologies available, increasing numbers of patients andprescriptions per patient, and the number of seniorstaking advantage of the Medicare Part D drug benefit.
Generic drug use accounts for more than 63% ofprescriptions filled in the United States, but it remainsonly 20% of the total drug expenditures.13 One of thetangible benefits of e-prescribing in third-party pro-grams is the potential to reduce excess spending on
drugs that are not on plan formularies and to reducespending on drugs for which generic substitutes areavailable and for drugs prescribed inappropriately.Third-party plans include prescription drug plans,Medicare Advantage plans, and Medicaid plans thathave formulary and generic option warnings that indi-cate to the prescriber and/or to the dispenser that a cer-tain drug prescribed may not be appropriate. As morewidespread adoption of e-prescribing by physiciansoccurs, rates of formulary compliance and generic drugutilization undoubtedly will increase.
Improved Drug-Use Process It is difficult to predict what issues will be addressed
when in the new Congress. Attempts will undoubtedlybe made to streamline the drug-use process from manyangles and to reduce the rate of increase in drug expen-ditures. The compliance of prescribers and pharmacistswith formulary guidelines will be enhanced by e-pre-scribing, and incorporating e-prescribing as a part of agreater emphasis on HIT applications will no doubt befront and center of proposals seeking to enable moreefficient drug prescribing and therapeutic use.
Several segments of e-prescribing systems willenable drugs to be used more appropriately and thusless expensively. Physicians will have alerts about for-mulary acceptability or lack thereof when entering aspecific drug for patients; in addition, pharmacists willhave computer prompts that will serve as “gate keeper”warnings for nonformulary, expensive, and inappropri-ately prescribed drugs.
Practical Considerations• With hundreds of thousands of physicians’ offices
still to be electronically equipped to transfer pre-scriptions, there will be a major shift in how pre-scriptions are transmitted. Drug-use records willneed to be converted to digital access—how this willbe paid for is a concern. The Centers for Medicare& Medicaid Services has and will continue to offerincentives for e-prescribing to encourage use.
• Physicians have lagged behind other professions inutilizing electronic communication. Studies haveshown that only 17% of physicians communicatewith their patients via e-mail.14 This percentage willincrease once electronic medical records, HIT, andpolicy influences are better accepted by the medicalcommunity.
• As with any computer-associated programs, appro-priate care will need to be taken in the training ofphysicians on how to use the program. e-Prescribing
e-Prescribing
TOC_Editorial_NovDec.qxp:Cover 11/25/08 10:38 AM Page 7

8 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
EDITORIAL
in and of itself will not solve all drug-related errors.Some have suggested that e-prescribing willenhance patient compliance with medications. Datafrom European studies do not necessarily bear thisout.15 e-Prescribing has been in place elsewhere inthe world where we see national health insuranceschemes and programs. This new technology will beeffective only as far as it directly improves patientcare and patient outcomes and does so in an eco-nomically sound fashion.
• e-Prescribing has unlimited potential to enhancethe drug-use process from prescribing to the point ofpatient delivery of medications. Error reduction,precise dosing, help in choosing the appropriatedrug, and enhancement of quality of care are but afew of the potential and very real consequences of e-prescribing. As is often the case, the recognition ofthe many potential benefits and a thorough assess-ment of the issues that e-prescribing can and cannotaddress will bode well for all involved in the drug-use process. For optimal effect, e-prescribing must bepart of a comprehensive revamping of how informa-tion is gathered, stored, and shared in the healthcaredelivery system. ■
References1. Teich JM, Marchibroda JM. Electronic prescribing: toward maximumvalue and rapid adoption. A report of the Electronic PrescribingInitiative. Washington, DC: eHealth Initiative; April 14, 2004.http://ehr.medigent.com/assets/collaborate/2004/04/14/eHealth%20Initiative%20Electronic%20Prescribing%20Report%2004.14.04%20
Executive%20Summary.pdf. Accessed October 28, 2008.2. Institute of Medicine. To Err Is Human: Building a Safer Health System.November 1999. http://www.iom.edu/Object.File/Master/4/117/ToErr8pager.pdf. Accessed October 27, 2008.3. Goves JR, Davies T, Reilly T. Computerisation of primary care inWales. BMJ. 1991;303:93-94. 4. Siwicki B. Electronic prescriptions: just what the doctor ordered.Health Data Manag. 1995;3:62-68. 5. Schiff GD, Rucker TD. Computerized prescribing: building the electron -ic infrastructure for better medication usage. JAMA. 1998;280:516-517.6. US Department of Health & Human Services. HHS takes new steps to accelerate adoption of electronic prescribing. HHS.gov. July21, 2008. http://www.hhs.gov/news/facts/eprescribing. html. AccessedOctober 28, 2008.7. Grossman JM, Gerland A, Reed MC, Fahlman C. Physicians’ experi-ences using commercial e-prescribing systems. Health Aff (Millwood).2007;26:w393-w404. 8. Glendinning D. Pharmacy benefit managers push Medicare e-prescrib-ing. Am Med News. August 13, 2007. http://www.ama-assn.org/amednews/2007/08/13/gvsd0813.htm. Accessed August 17, 2007.9. Mohr R, Islam S, Proctor K, et al. Readers’ perspectives: pharmacybenefit plans and pharmacies are moving expeditiously to support elec-tronic prescriptions. Health Data Manag. 2005;13:88.10. Groopman J. How Doctors Think. New York, NY: Houghton Mifflin;2007:24.11. Teich JM, Osheroff JA, Pifer EA, et al. The CDS Expert ReviewPanel. Clinical decision support in electronic prescribing: recommenda-tions and an action plan. J Am Med Inform Assoc. 2005;12:365-376. 12. Poisal JA, Truffer C, Smith S, et al. Health spending projectionsthrough 2016: modest changes obscure Part D’s impact. Health Aff(Millwood). 2007;26:w242-w253.13. The Henry J. Kaiser Family Foundation. Prescription Drug Trends.May 2007. Fact Sheet (#3057-06). http://www.kff.org/rxdrugs/upload/3057_06.pdf. Accessed October 9, 2008.14. Brooks RG, Menachemi N. Physicians’ use of email with patients:factors influencing electronic communication and adherence to bestpractices. J Med Internet Res. 2006;8:e2.15. Chhanabhai PN, Holt A, Benwell G. Sustainable health systems: ad -dress ing three key areas. Stud Health Technol Inform. 2007;129:1139-1143.
CAPTION CONTEST
Submission deadline: January 5, 2009
Winners’ names posted: January 7, 2009
Submit your caption atwww.AHDBonline.com
Winners Receive $50
TOC_Editorial_NovDec.qxp:Cover 11/25/08 10:38 AM Page 8

Eisai Inc. has established theDVTeamCare™ Hospital Award torecognize hospitals that have made asignificant commitment to preventingDVT and dedicating the necessaryresources to achieve this goal. Theaward program will showcase thedetails of the winning hospital’sprotocol and implementation planto help other hospitals enhance theirefforts to prevent DVT and itspotentially fatal complications.
Eisai is proud to be joined in thisnew initiative by the NorthAmerican ThrombosisForum (NATF),*
a nonprofit organization that focuses on unmet needs andissues related to thrombosis and cardiovascular diseases.
The DVTeamCare Hospital Award is an extensionof the Eisai human health care (hhc)
mission, which regards patientsand their families as the mostimportant participants in the
health care process.To learn more about the
award and how tonominate your hospital, visit
www.DVTeamCareAward.comtoday.
*NATF has been engaged to independently developthe criteria for the award, and judge the award and does
not endorse or promote any product or service offered byEisai, Inc. or any award nominee or recipient.
©2008 Eisai Inc. EISDVT006MMG 612
Tell Us How You Fight
www.DVTeamCareAward.com
INTRODUCING THE
Share your strategyfor preventing
Deep Vein Thrombosis (DVT)and your hospital could be
recognized nationally.
TOC_Editorial_NovDec.qxp:Cover 11/25/08 10:38 AM Page 9

10 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
GENERIC DRUG TRENDSGENERIC DRUG TRENDS
The use of generic drugs isone of the key drivers ofvalue in the pharmacy ben-
efit today. Both drug benefit plansponsors and beneficiaries realizecost-savings by increasing the useof generic drugs when medicallyappropriate. On average, generic
drugs cost 30% to 80% less than their brand-namecounterparts.1 It is important for plan sponsors and planbeneficiaries to understand the safety and efficacy ofgeneric drugs, as well as the potential cost-savings.
Therapeutic Scope of Generics The increasing availability of generic drug therapies
is slowing the rate of growth in prescription drugexpenditures. For the first time since the mid-1980s,the growth in per-capita spending on prescription drugshas dropped below the percentage of growth in the UShealthcare expenditures.2
The average rate of increase for drug expenditures forUS employers in 2008 was 4.86%,3 according to findingsfrom the 2008 Pharmacy Benefit Management Institute(PBMI)’s annual drug benefit plan design survey of USemployers.3 This growth rate represents the lowest costincrease since PBMI began conducting its annual surveyin 1995. This new survey, conducted in May and June2008, was completed by 223 employers, representing15,137,168 members. The increasing use of generic drugscontributes to this single-digit growth in expenditures.
When purchasers and consultants discuss genericdrugs, they refer to 2 different rates or metrics—generic-dispensing rate and generic substitution rate (Table 1).Generic-dispensing rate is a clear metric for trackingprogress in the use of lower-cost prescription drugs. Inmost cases, the generic-dispensing rate is the most
actionable metric to monitor improvement in genericuse and the associated savings. PBMI’s 2008 study alsodocuments continued increases in average generic-dis-pensing rates for US employers in retail and in mail dis-pensing since 2002 (Table 2).3 Generic-dispensing rateswill continue to increase as more brand-name drugs usedby ambulatory populations become available as generics.
The creation of incentives for plan members to usegeneric drugs is essential for a high-performing drug ben-efit program. Generic incentives are of increasing im -portance in 2008 as more branded drugs come off patent.The result is a growing range of generic drug options totreat allergies, arthritis, asthma, depression, elevatedcholesterol levels, hypertension, and chronic pain.
Education Tools for Plan MembersDrug companies are spending billions of dollars to
encourage consumers to request high-cost, brand-namedrugs from their physicians. Consumers and drug bene-fit plan sponsors will realize reduced prescription drugcosts if consumers make the choice to purchase thelowest-cost drug that is medically appropriate for theirneeds. Empowering consumers to make that choice is a challenge.
Complex benefit designs make it difficult for con-sumers to keep track of their plans’ preferred drugs andbeneficiary cost-sharing, and discuss this informationwith their prescribing physicians. Consumers needaccess to up-to-the-minute information on their plans’copayments and prescription costs to make educated,cost-effective decisions.
RepetitionResearch has shown that people often need to see or
hear a message multiple times (as many as 7) before itmakes an impression. Repetition is good, as is using avariety of ways to communicate because people havedifferent learning styles. Organizations should leverageevery available opportunity to deliver messages thatincrease confidence in and encourage the use of gener-ics. Messaging opportunities include: • Direct mail targeted to high utilizers of prescription
drugs
Ms Felthouse is President, Pharmacy Benefit ManagementInstitute (PBMI), Scottsdale, AZ. She has been the lead author of PBMI’s annual Prescription Drug Benefit Cost and Plan Design Report and PBM Customer SatisfactionReport since 2001. She can be reached at [email protected]. The annual reports can be accessed at www.pbmi.com.
Focus on Lowest Net Cost Drug ReducesCosts for Patients, Plan SponsorsDana H. Felthouse, MBA
GenericDrugNovDec .qxp:Cover 11/25/08 10:42 AM Page 10

11www.AHDBonline.comVOL. 1 NO. 9
GENERIC DRUG TRENDS
• Employee meetings• Employee/retiree/member publications, both print
and electronic • Employee/member intranet• Online tools for comparing brand and generic
alternatives• Payroll envelopes and electronic funds transfer
notifications• Podcasts• Posters in break rooms and high-traffic areas• Retiree association events.
Consumer ResourcesThe following consumer-focused resources can sup-
plement plan benefits communication efforts:• Consumer Reports Best Buy Drugs is an independ-
ent, online resource that helps beneficiaries learnabout generic alternatives and empowers them todiscuss cost-effective options with their physicians.Beneficiaries can obtain free reports that comparethe safety, efficacy, and cost of brand-name andgeneric drug options for 16 different medical condi-tions (www.crbestbuydrugs.org).
• The Generic Pharmaceutical Association offersconsumer education on generics, including a fre-quently asked question-and-answer section anddownloadable brochures (www.gphaonline.org/AM/Template.cfm?Section=About_Generics).
• The US Food and Drug Administration (FDA)offers consumer education materials that can bedownloaded, ordered in quantities, or used asresources for developing employer-specific materials.Resources available in multiple languages includeprint brochures, posters, articles, PowerPoint presen-tations, audio presentations and handouts (www.fda.gov/cder/consumerinfo/generic_all_re sources.htm).Aligning your drug benefit plan to encourage the uti-
lization of the lowest net cost drug that is medically appro-priate for a patient will enhance the clinical and econom-ic returns of your investment in prescription drugs. ■
References 1. Generic Pharmaceutical Association. About generics: same medicine,same results, lower cost. http://www.gphaonline.org/AM/Template.cfm?Section=About_Generics. Accessed November 10, 2008.2. PricewaterhouseCoopers Health Research Institute. Behind the Num -bers: Healthcare Cost Trends for 2008. 2008. www.pwc.com/extweb/pwcpublications.nsf/docid/88FF5DC2E5E1143085257300006C68B1.Accessed November 10, 2008.3. Pharmacy Benefit Management Institute. Prescription Drug BenefitCost and Plan Design Report, 2008-2009 Edition. 2008. www.pbmi.com/2008_report/index.html. Accessed November 10, 2008.
Tracking Availability and Price of Generic DrugsUsing generic drugs to save money is a winning strategy for
every drug benefit program. The savings begin when a brand-name drug goes off patent. Here is a list of tools to help track theavailability and price of generic drugs.• Trends in Manufacturer Prices of Prescription Drugs Used by
Medicare Beneficiaries: The AARP’s Public Policy Institute’sannual report on changes in manufacturer list prices forbrand-name and generic drugs. Includes average annual per-cent change in manufacturer prices for the top 25 generic pre-scription drugs. Shows price changes by manufacturer andtherapeutic category for the most widely used generic drugs.www.aarp.org/research/health/drugs/rx_ watchdog.html.
• Drug Patent Watch: Information on drugs and their patent expi-rations. Subscribe to free bulletins on imminent patent expira-tions. www.drugpatentwatch.com/.
• Drugs@FDA: Monthly drug approval reports. Search abledatabase of FDA-approved drugs. Search by brand name oractive ingredient for availability of generic alternatives. www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm.
• FDA Electronic Orange Book: Searchable database of all FDA-approved prescription drugs—brand-name and generic drugs,with therapeutic equivalence evaluations. Daily updates fornew generic approvals. www.fda.gov/cder/ob/.
• FDA Generic Drug Approvals: Monthly reports on first-timegeneric drug approvals. www.fda.gov/cder/ogd/approvals/default.htm.
• Generic Pharmaceutical Association: Statistics and resources for consumers and researchers. Includes list of generic pre-scription medications recently approved by the FDA and guidelines for navigating the Drugs@FDA website.www.gphaonline.org/AM/Template.cfm?Section=Home.
Table 1 Must-Know Generic Terms
• Generic-Dispensing Rate: Percentage of total prescriptions filled with a generic drug
• Generic Substitution Rate: Percentage of total prescriptions that could be filled with a genericdrug that actually are filled with a generic
Source: Pharmacy Benefit Management Institute. The ABCs of Generic Drugs. White Paper Series. 2008.http://www.pbmi.com/pbm101white paperseries.asp.
Table 2 Trends in Average Generic-Dispensing Rates
Year Average retail Average mail generic-dispensing generic-dispensingrate, % rate, %
2002 42.0 32.02003 44.0 34.02004 47.0 38.02005-2006 51.0 39.02007 54.5 41.72008 60.4 49.3Source: Pharmacy Benefit Management Institute. Prescription Drug Benefit Cost and Plan Design Report, 2008-2009 Edition. 2008. www.pbmi.com/2008_report/index.html.
GenericDrugNovDec .qxp:Cover 11/25/08 10:42 AM Page 11

“We either do it right orwe don’t do it at all.”
©2008 Mylan Pharmaceuticals Inc.
GenericDrugNovDec .qxp:Cover 11/25/08 10:42 AM Page 12

In 1961, two U.S. Army buddies, Milan (Mike) Puskar and
Don Panoz, founded a pharmaceutical company with a handful
of employees in a small town in West Virginia. From the
beginning, the founders were determined to build a company
based on quality and integrity and to follow Mike’s philosophy—
“We either do it right or we don't do it at all.”
Over the past 47 years, that company, Mylan Pharmaceuticals,
has grown to become the largest U.S.-based manufacturer
of generic pharmaceuticals by total prescriptions*. . . and
Mike Puskar is still Chairman of the Board. His no-compromise
attitude continues to guide all aspects of company business,
from research and development, to manufacturing and
distribution.
Today, every employee in the Mylan family is always ready to
take the extra step necessary to ensure that Mylan Products
deliver the high quality that patients expect and deserve. This
unwavering commitment assures that products from Mylan will
always offer quality and affordability for the patients who need
them and peace of mind for the pharmacists who dispense them.
He’s kept his wordfor 47 Years.
MYNMKT276A
*IMS National Prescription Audit. Total Prescriptions: June 2007 - June 2008.
GenericDrugNovDec .qxp:Cover 11/25/08 10:42 AM Page 13

14 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
REGULATORY
F. Randy Vogenberg: There have been attempts to lookat large claim databases (eg, WellPoint’s) of patients receiv-ing erythropoiesis-stimulating agents (ESAs). News aboutthe cutback on ESA use was accompanied by reports aboutthe rise in the number of transfusions. At the same time,articles published in pharmacy and hospital journals wereadvocating the use of ESAs to avoid transfusions. So, themessage is mixed. What people are doing in an inventoryenvironment is not the same as what they are doing in aninstitutional inpatient environment. And hospitals may con-tinue to use ESAs to avoid the more costly transfusion, apurely cost consideration. Is this how you see it?
Samuel Silver: I think this may be true. But theissue of transfusion is beyond cost, especially in the out-patient setting today, where 85% of cancer patient careoccurs in the community and not in academic medicalcenters.
The first issue is that giving transfusions at centerssuch as the University of Michigan is relatively simple,and our facilities are well prepared to administer them.
We have a good blood bank on site and plenty of chairsfor transfusions, so we can get people set up, and wehave blood irradiators (see below). But in the commu-nity, physicians by and large don’t give transfusions intheir offices because of the administrative and proce-dural hassle. Rather, they send patients to their hospi-tal outpatient infusion area, which is usually very small,where they can run out of transfusion chairs relativelyrapidly, so that we now have a group of patients eitherrequiring admission for transfusion or experiencing asignificant delay waiting for an outpatient chair. Andthese are not patients with shortness of breath whorequire admission but rather it’s a quality-of-life (QOL)matter, because of the requirement of an inpatient stay.
The second issue is that the typical Medicare bene-ficiary has many comorbid conditions (eg, heart fail-ure) in addition to cancer. Thus, we are no longer talk-ing only about potential infectious complications oftransfusion but also about issues of fluid overload thatwould not occur when using an ESA.
The third concern is that many patients receivingchemotherapy, especially those with hematologicmalignancies, are immunosuppressed. They requireirradiated blood products to avoid transfusion-associat-ed graft-versus-host disease. Irradiating blood is veryeasy; any university blood bank will have a blood irra-
Erythropoiesis-Stimulating Agents in aMeta-Stable State: Guidelines,Economics, and Policy in FluxInterview (Part 2) with Samuel M. Silver, MD, PhD
Medicare coverage of erythropoiesis-stimulating agents is a complex issue with implicationsfor a variety of healthcare stakeholders. In the first part of the interview (see AHDB, May2008), Samuel M. Silver, MD, PhD, examined the evolution and clinical implications of theMedicare coverage decisions and the eventual shift in clinical practice away from theapproved indication to situations involving quality-of-life issues. In this second part, Dr Silverdiscusses with F. Randy Vogenberg, RPh, PhD, the clinical implications of the Medicare cov-erage decision regarding erythropoiesis-stimulating agents, pointing out the noneconomicreasons why transfusions can be risky to cancer patients, and how such policy decisions canhave profound implications for patients. Dr Silver calls for new studies to be initiated, which
would be funded by the 2 major manufacturers of these drugs, to investigate the concerns regarding tumor pro-gression and thromboembolic events that are potentially associated with these expensive and potentially toxicmedications. The discussion resumes where Dr Silver explains why it would be good to compare claims data ofcancer patients who are receiving these medications and their transfusion requirements. [ADHB. 2008;1(9):14-18.]
Dr Silver is Professor of Internal Medicine, Director, CancerCenter Network, Division of Hematology/Oncology, andAssistant Dean for Research, University of Michigan HealthSystems, Ann Arbor, MI.
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 14

15www.AHDBonline.comVOL. 1 NO. 9
ESAs in a Meta-Stable State
diator. It does not require much time, but it will addsome expense. Nonetheless, it is well worth it.However, if the patient is in a suburban or rural com-munity, that patient may not have immediate access toirradiated blood and will have to wait a day or two toget it. So, all of a sudden something that would be sim-ple for me at the University of Michigan becomes aprocess that takes several days for a patient thatreceives chemotherapy in a suburban or rural facility.These are some of the noneconomic, procedural issuesthat are involved in giving transfusions.
Vogenberg: The other side of this issue concerns youngerpopulations. The 50- to 60-year-old patient may still have acommercial insurance and not Medicare. Thus, there arealso direct economic costs to consider, such as absence fromwork, particularly when the patient may be tied up for a dayor two, as you said. There are many repercussions forMedicare, which is the focus for the Centers for Medicare &Medicaid Services (CMS), and for commercial insurers andemployers, who are paying the bills. This is not well under-stood; the tendency is to just look at the drug cost and thedrug companies, and this is more emotional than rational.
Silver: True. And the next thing we know, we aretalking about Medicare Part B, and we begin to reachout to Medicare Part A, when we start admitting peo-ple to the hospital. Apparently those involved inMedicare Part B decisions don’t see this, but we cer-tainly see this as citizens and on the private side. Andthe employers see this. So the US Food and DrugAdministration (FDA) has issued new warnings, whichessentially reflect the concerns about potential tumorprogression, venous thromboembolism, and keepingthe hemoglobin level at <12 g/dL (although this cut-offmeasure was dropped by the FDA from the most recentESA labeling).
The FDA reiterated this in its most recent state-ment. That is where we are from the point of view ofthe FDA and CMS. And the Senate passed a nonbind-ing resolution about it, since the Senate has a sensethat the National Coverage Decision (NCD) has noweight and should be changed.
Vogenberg: This NCD issue probably comes at a goodtime for CMS, because the current Congress is deadlockedon many issues. So nothing is going to happen. There are norepercussions against CMS’s decision about ESAs, and itcan come back and say it has saved a lot of money, whilepreventing further harm to their beneficiaries. It is reallyalmost a neutral situation from a public policy perspective.
Silver: In the meantime, Representatives PeterStark and Henry Waxman are saying they are protect-ing the patients from this “miracle grow for tumors.”And because we have no quality-of-life (QOL) data,there are no improvements in QOL issues. Now whatdo we do? We definitely require more data.
Vogenberg: How transparent is CMS regarding its data?
Silver: CMS is not transparent at all. When youread the NCD, their background materials have beentightened up a bit. But the intellectual basis to bridgebetween the final coverage decision background mate-rial and the rules is missing.
Vogenberg: This is very typical of what you would seein almost any insurance company. You get caught up in thisdynamic of economics and cost, and you are trying to pro-vide just enough access so that people are happy, but at thesame time less attention is paid to QOL than to the science,so it really is about economics. For CMS, it appears to beabout money. They had to stay within a budget, and they
KEY POINTS▲ Despite the high costs of the ESAs, the issue of transfusions
in cancer patients is beyond economics.▲ The noneconomic issues surrounding transfusions that trans-
late to unnecessary risks for patients are:1. Inadequate facilities that mean long waiting periods2. Many patients are Medicare beneficiaries and thus often
have multiple comorbidities3. These patients are often immunosuppressed, requiring
irradiated blood products, which could be a problem innonacademic centers.
▲ Although Medicare is not supposed to consider costs in itsdecisions, cost is an underlying context for Medicare cover-age for these very expensive medications, which, neverthe-less, may reduce hospitalization for transfusions.
The next thing we know, we are talking about Medicare Part B, and we begin to reach out to Medicare Part A, when we startadmitting people to the hospital.
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 15

16 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
REGULATORY
knew the ESA coverage was a budget buster and a high-expenditure category, as it is for any employer. This is theperfect moment to come up with a Solomon-like decision.CMS is not required to disclose as much as the FDA. Thismakes it easier for the commercial carriers to follow suit.
Silver: In addition, CMS will identify 10 more ques-tions that should be answered, as they did 1 year ago,even though many of these questions are unanswerable,because the data don’t exist, and CMS knows it; a trueCatch-22.
Vogenberg: This points to an interesting dichotomybetween what the Agency for Healthcare Research andQuality is doing and Medicare Part D initiatives and thegeneral Medicare initiatives about quality issues in hospi-tals, such as pay-for-performance. On one hand, CMS is saying it is going to pay for improved performance andoutcomes in the hospitals, which, based on the current lit-erature, suggests they would be using ESAs; these drugslead to better results and reduce complications and read-missions, which are the criteria for quality. But on theother hand, Medicare coverage decision, which was basedon an outpatient basis, prevents clinicians from using these drugs.
Silver: That brings up an interesting point. InCMS’s Physicians’ Quality Reporting Initiative, one ofthe early reporting initiatives dealt with the use ofESAs in myelodysplastic syndrome (MDS). It was nec-essary to make sure patients had sufficient iron stores,which was a quality point. Yet, the payment for MDSassociated with ESAs was denied at that time, as wediscussed in the first part of this interview (AHDB.May 2008;1[4]:46-50).
Vogenberg: And then it could be argued that the cost ofthese medications is too high?
Silver: Actually, Medicare is not supposed to talkabout costs or to consider it in its decisions, but ofcourse it is the underlying context.
Vogenberg: And what is the Veterans Administration(VA) doing with the coverage?
Silver: I do not have the answer to that. The VA hasan excellent electronic medical records system; howev-er, in the past few months the VA was unable to useany of their data for Health Services Research purpos-es because of confidentiality and HIPAA (HealthInsurance Portability and Accountability Act) issues.
Vogenberg: There must have been some kind of analy-ses done within the VA military review structure when allthis was transpiring, because they are so cost and qualityconscious. I wonder what the VA system is doing aboutTRICARE and the active military, which represents a largepopulation?
Silver: This is a very important issue. The FDA hasasked the American Society of Clinical Oncology(ASCO) and the American Society of Hematology(ASH) to determine what studies should be done inthe future. ASH has asked the American Associationof Cancer Research (AACR) to participate in this ini-tiative. We are trying to convene a meeting with rep-resentatives from the FDA, CMS, ASH, ASCO, andAACR to determine what trials are needed and whoshould be running them.
Vogenberg: Would they be doing a corresponding healtheconomics analysis with clinical studies parameters?
Silver: That would be an important thing to look atas well, but the executive committee of ASH believesthat the National Institutes of Health (NIH) shouldnot be paying for such studies to help determine thebest hemoglobin range for ESA use. The ExecutiveCommittee is concerned that this type of study costs alot of money. And diverting NIH money for this clini-cal question would leave less money for important basicscience research.
Vogenberg: That is a good point.
Silver: It would be important to engage bothJohnson & Johnson and Amgen to design an openstudy that would be funded by an unrestricted grantfrom both drug manufacturers to examine the patho-physiology of ESA-associated thromboembolism. Andmaybe we should involve the NIH and the NationalCancer Institute or the National Institute of Diabetesand Kidney Disease to address issues surrounding end-
Medicare is not supposed to talk about costs or to consider it in its decisions, but of course it is the underlying context.
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 16

17www.AHDBonline.comVOL. 1 NO. 9
ESAs in a Meta-Stable State
stage renal disease (ESRD). So we need to focus on 3aspects of the drugs—tumor promotion, the biology of venous thromboembolism, and the relationship toESRD, which can teach us a lot. And these 3 thingsshould happen in parallel, along with the economicissues that are related to these clinical considerations.
Vogenberg: Clinically speaking, where would you wantthe focus of these studies to remain?
Silver: Future studies should somehow focus on QOL in a meaningful way. Combining the efforts ofJohnson & Johnson and Amgen may be effective. Inthat way, individual marketing agendas could be put aside. For at least the moment, private payers havebeen using the ASH/ASCO guidelines as opposed toMedicare guidelines. This, of course, could changetomorrow. When I spoke with Dr Lee Newcomer of UnitedHealthcare a while back, he made no promis-es. He seemed to think it was very reasonable to use theASH/ASCO guidelines, using an initial hemoglobinlevel of <10 g/dL, and then maintaining patients athemoglobin levels between 10 g/dL and 12 g/dL. As Imentioned in the previous article in this journal (May2008), oncologists have come to view this issue withconcern; we are generally maintaining patients at orbelow hemoglobin levels of 12 g/dL.
Vogenberg: Are physicians still providing ESAs as freelyas they had before the new Medicare coverage ruling wasannounced?
Silver: No. In fact, the number of those using ESAshas declined significantly. This may have been associ-ated with the FDA issuing the black box warnings inMarch 2007. I think the bottom line is that most physi-cians want to use drugs in a reasonable way, and per-haps they overcompensate when they hear the cynicalperspective about perverse physician incentives. Sowhen the black box warning was issued, there was agreat deal of self-correction.
Vogenberg: Carriers will be more willing to take the softapproach UnitedHealthcare has taken, unlike that taken byMedicare. They will seek the benefit of the reduced expen-ditures by informing their provider networks and offeringthem the opportunity to avoid potential complications and tobe in compliance with the guidelines. This could be a win-win situation for everybody.
Silver: Possibly. But it is a complicated issue. Pa -
tients getting chemotherapy are receiving toxic agentswith therapeutic ratios that are some of the most diffi-cult in medicine. Many of the patients, especially thosein the Medicare population, have incurable cancers;they are receiving chemotherapy mainly for palliation.The goal is to give them as high a QOL as possible. Ifthey are receiving chemotherapy and spend the last 2months of their lives in the hospital, we are not doingthe right thing.
Debilitating patients for the majority of theirremaining time to shrink a tumor is not good care. APyrrhic victory in this scenario is no victory at all. Andusing a drug that potentially can cause thromboembol-ic events only complicates this picture.
I was called to an FDA meeting in which a patientrepresentative was anxiously going on about tumorgrowth associated with ESAs that patient was receiv-ing. This is a difficult thing to say, but having progres-sion of an incurable cancer is not always the worstthing that can happen. Chemotherapy is rarely provid-ed with curative intent in this population. Appropriatepalliation may include chemotherapy along withadjunctive therapies, such as ESAs, that may cause asmall risk of tumor growth.
Vogenberg: This is a valid point that many people for-get. Patients who are seriously ill often lose sight of realityor don’t want to face it.
Silver: Right. Sometimes we need to reach deeperinto the bag for more information.
As I have said, finding this would be tantamount tofinding the Holy Grail, and unfortunately, you cannotinfallibly predict outcomes. ■
Disclosure StatementDr Silver is a consultant to Bear Stearns, Lehman Brothers, and
the Gerson Lehrman Group, and receives grant/research supportfrom Blue Cross Blue Shield of MI.
We need to focus on 3 aspects of the drugs—tumor promotion, the biology ofvenous thromboembolism, and the relationship to ESRD, which can teach us a lot.
Stakeholder Perspective on page 18
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 17

18 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
REGULATORY
Stakeholder PerspectiveThe Clinical and Economic Complexity of Biologics
PAYERS/PATIENTS: The inability to predictoutcomes with erythropoiesis-stimulating agents(ESAs) or with other biologic agents is emerging asa key concern. Whether in rheumatoid arthritis,multiple sclerosis, or erythropoiesis, unintended orunknown effects from these new biologic medica-tion technologies are gradually better detected andbetter understood, helping to determine the mostappropriate uses. From the perspective of economic decision makers—patients, health plans, or employ-ers—the easy clinical decision to use biologic med-ications has become muddier, while these same(typically elderly) patients are rethinking their needfor a wider variety of end-of-life therapies that have focused more on quality-of-life issues than onchanging the lifespan.
ESAs provide an interesting insight into thecomplexity of clinical use of biologics and their eco-nomic impacts on all payers, as well as the types ofclinical service providers. Given that many patientswho are using biologics are covered under aMedicare drug plan but also have multiple comor-bidities, this further illustrates the dilemma of find-ing a technological advancement end point wherecosts become more predictable. As Dr Silver pointsout in the interview, several concerns involvingpatients who receive ESA therapy go beyond a sin-gle decision point.
Because of the paucity of data to clearly guide themultipoint clinical and coverage decisions, theCenters for Medicare & Medicaid Services (CMS)and private insurers are erring on the side of limitedcoverage, following the evidence-based medicine(EBM) model. Although in itself not siding withany coverage position, EBM can conveniently beused for any stakeholder’s position, whether eco-nomic or clinical. In the case of ESAs, there seemsto be a clinical and an economic dilemma forebod-
ing of the bigger and more expansive decisions oursociety faces through the lens of healthcare insur-ance coverage for the growing pipeline of biologic-based technologies.
The role of regulators (CMS, US Food and Drug Administration) and system researchers(Association for Healthcare Research and Quality,quality improvement organizations) should bedetermined by Congress to better align incentives,along with a clearer direction for the use of newtechnologies (diagnostic or therapeutic). Mixedmessages and misalignment of incentives has longbeen an albatross around the US healthcare systemthat has fed many debates and articles arguing themyriad of issues relevant to each of the stakeholders.This has been good for academics, consultants, andspecial interest lobbyists, but not for frontlinepatients and healthcare professionals, or those pay-ing the bills for care.
Based on reports from the recent presidentialcampaign and from groups such as the KaiserFoundation or the Wall Street Journal, neither partynor either of the candidates has had the single obvi-ous solution to our looming healthcare crisis in thenext decade. Perhaps our economic distress will aidpatients, as reflective of our society, in establishingnew parameters around life-and-death decisionsthat will help our healthcare system seek a new bal-ance in harnessing technologies for the most appro-priate use, which will then determine its hierarchi-cal cost in our economy.
F. Randy Vogenberg, RPh, PhDChief Strategy OfficerEmployer-based Pharmaceutical Strategies, LLCSenior Scholar, Department of Health PolicyThomas Jefferson University, Jefferson MedicalSchool
Subscribe to our e-Newsletter at www.AHDBonline.com
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 18

Early and intensive treatment can help patients reach their A1C goal Are your plan members not taking their type 2 diabetes medications?
Many patients are not reaching the ADA A1C target goal of <7%, and many are stopping their medications.1,2
Recent data show a drop in the use of oral antidiabetic medications3
The need for early treatmentBecause many patients already have chronic complications at the time of diagnosis, treatment plans must be aggressive from the start to optimally manage type 2 diabetes.4
Long-term benefits of diabetes medications can only be realized if patients adhere to their treatment regimen.2
“Early, intensive intervention has the potential to get patients to glycaemic goals more quickly and
be more effective at keeping them at goal...”5
2,000
2,100
2,200
2,300
2,400
2,500
3/16/2007 Days 6/6/2008
TRx
(000
s)
OAD TRx 4 week moving avg Trend (Pre-NEJM)
References: 1. Hoerger TJ, Segel JE, Gregg EW, Saaddine JB. Is glycemic control improving in U.S. adults? Diabetes Care. 2008;31:81-86. 2. Rodgers K. Ensuring compliance in patients with diabetes. In: Diabetes: Disease Management Guide. 4th ed. Montvale, NJ: Thomson PDR; 2004:501-505. 3. Data on file, Takeda Pharmaceuticals North America, Inc. 4. Cornell SA. Clinical case study: achieving long-term control of insulin resistance. J Manag Care Pharm. 2007;13(suppl B):S11-S15. 5. Goldstein BJ, Gomis R, Lee H-K, Leiter LA, on behalf of the Global Partnership for Effective Diabetes Management. Type 2 diabetes—treat early, treat intensively. Int J Clin Pract. 2007;61(suppl 157):16-21.
©2008 Takeda Pharmaceuticals North America, Inc. PIO-00658 6/08 Printed in U.S.A.
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 19

20 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
BUSINESS
Adherence to medications is essential forpatients with chronic disease for optimizingclinical outcomes. When used appropriately,
medication is a very cost-effective method for treat-ment and prevention of disease. Patients who fail totake their medications as prescribed do not get the fullbenefit from the drugs, and they may also end up withunnecessary hospitalizations, emergency departmentvisits, and nursing home admissions. Cost-effective,scalable interventions are essential to reduce nonad-herence. In this article, we examine the use of auto-mated phone-based patient communication to supportoutreach efforts, as well as the impact this type of inter-vention can have on clinical outcomes and costs.
In their 2005 study of medication-taking behaviors,Osterberg and Blaschke observed that, “Common bar-riers to adherence are under the patient’s control, soattention to them is a necessary and important step inimproving adherence.”1 In that study, the followingreasons were cited by patients for not adhering to their
medication regimens1:• Forgetfulness—30%• No reason—27%• Other priorities—16%• Decision to omit doses—11%• Lack of information—9%• Emotional factors—7%.
Lack of information and forgetfulness combinedcomprise 39% of the reasons cited in this study for poormedication ahderence.1 These 2 areas can be positivelyaffected by improved communications between thecare provider and the patient that, in turn, can improvemedication adherence.
One other common and well-documented reason forpoor adherence is side effects.2,3 Patients who experi-ence unpleasant or unexpected side effects may stoptaking their medications, often without informing theirphysicians or other care providers.2,3
In their study, Osterberg and Blaschke furtherobserve that there are 4 general methods to helpimprove patient adherence1:1. Patient education2. Revised dosing schedules
Role for Automated CommunicationStrategies in Medication AdherenceManagement S. Michael Ross, MD, MHA
Lack of medication adherence is a prevalent problem that causes a broad range of health-and health-economics–related issues. Adherence management is therefore an importantstrategy, but it also presents its own set of challenges. Interventional communication fromcare support teams at managed care organizations and disease management and wellnessprograms has proved effective at modifying patients’ medication adherence and reportingbehaviors. However, these communications do not work well from an economic standpoint.It is not economically feasible to scale call centers and the numbers of clinical and profes-sional staff to communicate with the increasing number of patients with chronic diseaseswho require ongoing medication use. Using communication automation to augment tradi-tional call center outreach can help to mediate patient medication-taking behaviors. Specific
design criteria for the automation of this interaction are discussed in this article, offering supporting data from arecent trial of 304 elderly patients with hypertension, and showing the benefits of using such a system for effec-tive blood pressure monitoring, at reduced costs. [AHDB. 2008;1(9):20-27.]
“Drugs don’t work in patients who don’t take them.” —C. Everett Koop, former US Surgeon General
Dr Ross is Vice President of Healthcare, Varolii Corporation,Seattle, WA.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 20

21www.AHDBonline.comVOL. 1 NO. 9
Automated Communication Strategies
3. Expanded hours when the clinic is open, includingevening hours
4. Shorter wait times and improved communicationbetween physicians and patients.
Although not all of these general methods are relevantto our topic, patient education and communicationbetween physicians and patients are 2 areas that can beaffected by effective communications.
Illustrative CaseTom’s blood pressure (BP) was elevated during his past
2 visits to his physician. At the most recent visit, his doc-tor suggests an antihypertensive regimen and prescribeslisinopril. Tom fills the prescription order for lisinopril atthe local pharmacy and takes it home. As part of his rou-tine care, Tom schedules a follow-up examination. Aftera period of time, we may expect a reduction in Tom’s BPlevel. But instead, at his follow-up visit, Tom’s BP is stillelevated. Was lisinopril ineffective in Tom’s case? Notnecessarily. In fact, the medication might well haveproved effective if Tom had remembered to take it. ButTom took the first day’s dosage, put the bottle in his med-icine chest, and then promptly forgot about it. He alsowas not reminded to take the medication.
The Challenge: Improving Care for 10 Million “Toms”Tom is not alone. Findings from Osterberg and
Blaschke’s study show that, “Of all medication-relatedhospital admissions in the United States, 33% to 69%are due to poor medication adherence, with a resultantcost of approximately $100 billion a year.”1 In addition,according to well-documented surveys, failure toadhere to treatment, also known as noncompliance, isa large-scale problem.4,5
The 2006 Case Management Adherence Guide -lines, issued by the Case Management Society ofAmerica, offer insight into the magnitude of the issue,noting that “the number one problem in treating ill-ness today is patients’ failure to take prescription med-ications correctly, regardless of patient age.”4
In a 2003 study, the World Health Organizationfound that approximately 50% of the 1.8 billion pre-scription medications dispensed annually in the UnitedStates are not taken correctly by patients.5 It is reason-able to assume that at least some of these nonadherentpatients are not receiving the full benefits of the pre-scribed medication. In 1998, nonadherence to heart dis-ease medication regimens alone was reported to be thecause of 125,000 preventable deaths each year in theUnited States.6 This places medication nonadherenceamong the major causes of health-related deaths in the
United States, after heart disease, cancer, stroke, andchronic lower respiratory diseases, according to the 2005National Vital Statistics Reports (Table).7 In reality, deathsfrom all medication nonadherence could be much largerthan the 125,000 deaths for heart disease only.
Patients who stop taking medication as a result offorgetfulness, lack of information, or side effects canoften be helped by effective outreach from their physi-cian or clinical care professionals to remind patients totake their medications, elicit information about sideeffects and their impact on noncompliance, offerencouragement, and even connect them with their
KEY POINTS▲ Medication nonadherence is a major cause of morbidity and
mortality, and is a large contributor to escalating health-related economic costs.
▲ Lack of information and forgetfulness are 2 main reasons fornonadherence that can be positively affected by improvedpatient–provider communication.
▲ With chronic diseases estimated to involve hundreds of millions of patients, the scale of disease management enroll-ment is too great to be cost-effective using traditional out-reach methods.
▲ The challenge is to scale outreach programs efficiently, with-out losing the personal touch necessary to help changebehavior.
▲ In a new study of automated telephony for blood pressuremonitoring, this technology reduced the cost of blood pres-sure reading by 95% compared with supportive care reading.
▲ The study results suggest that efficient, effective automatedcommunications with patients can produce positive clinicaloutcomes at reduced costs.
Table Medication Nonadherence Major Cause of Death in theUnited States
Condition Annual deaths, N 1. Heart disease 652,0912. Cancer 559,3123. Stroke 143,5794. Chronic lower respiratory diseases 130,9335. Medication nonadherence 125,000*
6. Diabetes 75,1197. Alzheimer’s disease 71,599
* This number refers to medication nonadherence deaths from heart diseasealone; the number for all deaths from medication nonadherence could there-fore be higher. Source: McCarthy R. The price you pay for the drug not taken.Bus Health. 1998;16:27-33.Source: Kung HC, Hoyert DL, Xu JQ, Murphy SL. Deaths: final data for 2005.Natl Vital Stat Rep. 2008;56:1-120.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 21

22 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
BUSINESS
clinical care team, if needed. This, in fact, is one of thekey premises around which managed care organizations(MCOs) and wellness programs are organized: by offer-ing regular, relevant “interventional” communicationsin a structured program, these organizations can posi-tively affect medication-taking behaviors of their pro-gram members.
Health Economics: The Costs of Noncompliance Adherence is critical to everyone involved in
healthcare: from patients and payers (insurance, gov-ernment, employers) to retail pharmacies and pharma-ceutical manufacturers. And it is the sheer number ofthese patients that forms the heart of the adherencechallenge. For patients, adherence is an important factor in improving clinical outcomes; this issue hasbeen well documented in the literature.1 Indeed, theCase Management Society of America observes,“Nonadherence to medications is a common factorthat prevents patients from achieving the full thera-peutic benefit of their therapies.”4
For organizations, improved patient adherencemeans the ability to deliver better care while reducingmedical expense ratios driven by unnecessary hospital-izations, emergency department visits, nursing homeadmissions, and excess consumption of interventionaltreatments.5
For manufacturers and retail pharmacies, whosenonadherent patients do not fill prescriptions as indi-cated, or who have poor medication possession ratios,improving patient adherence is not only important to
patient health but can also affect bottom-line revenues.Let’s return briefly to our hypertensive patient, Tom.
During the follow-up appointment, Tom’s doctor asks ifhe is taking his medication as prescribed. Tom sheep-ishly admits he has forgotten. Tom’s doctor remindshim of the importance of taking medications as pre-scribed, and provides information about hypertension,the associated health risks of stroke and heart attack,and strongly encourages him to “stick” with the med-ication regimen. Concerned about his health andencouraged by his healthcare provider, Tom signs up fora wellness program through his employer. A care repre-sentative from the wellness program contacts Tom,enrolls him in the program, and begins to provide himwith information, tips, and additional encouragement.The outcome? Tom’s BP is much better managed now,and he will likely have an improved clinical outcome as a result.
Of course, Tom is a hypothetical patient, but this isa common story for millions of real patients with hyper-tension. Illustrative of the scale of this particular condition, the 2005 National Ambulatory MedicalCare Survey revealed that there were 44 million visitsto office-based physicians with hypertension as a pri-mary diagnosis.8
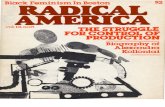
Further complicating the issue is the fact that manyof these patients may be older and may take more than1 medication regularly.4 We live in a society experi-encing a “graying” of its population, as the baby boomgeneration begins to mature past the age of 65 years.Many boomers, as well as millions of others, will be prescribed multiple medications (Figure 1) for chron-ic conditions, such as hypertension, high cholesterol,depression, and diabetes.8 The Centers for DiseaseControl and Prevention’s (CDC) Health, UnitedStates, 2007, survey shows that slightly more than 30% of all individuals between the ages of 45 and 64had taken 3 or more prescription medications in thepast month.9
Provider CommunicationIt is well-documented that clear, consistent provider
communication can have a positive impact on patientwell-being. In an article on literature searches forphysician–patient relations, Stewart notes that “Mostof the studies reviewed demonstrated a correlationbetween effective physician–patient communicationand improved patient health outcomes.”10
Thus, it is not surprising that regular, consistentcommunications from care support teams, such asthose in wellness organizations, can have the same
Prescriptions filled, %60
50
40
30
20
10
0
1823
30
10
23
42
57
32
24
1992 1996 2000Year
0 1-2 3-4 5+Chronic conditions (N), 2000
Yes NoRx coverage, 2000
Figure 1 Average Annual Prescriptions Filled by Noninstitutionalized Medicare Enrollees, ≥65 y
Source: Cherry DK, Woodwell DA, Rechtsteiner EA. National AmbulatoryMedical Care Survey: 2005 summary. Adv Data. 2007;(387):1-39.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 22

23www.AHDBonline.comVOL. 1 NO. 9
Automated Communication Strategies
effect. If it were just 1 doctor effectively communicat-ing to 1 patient the importance of consistently takingmedication as prescribed, it might be easier to resolvethe adherence problem. But, as we have noted, thereare tens of millions of “Toms” with a variety of chron-ic conditions who require this type of outreach. TheCDC notes in its Health, United States, 2007, that in2005, the percentage of adults with 3 or more chronicconditions increased with age from 7% of adults aged45 to 54 years to 37% of adults aged 75 years andolder.9 Although managing chronic conditions is aproblem of scale, the real challenge lies in scaling effi-ciently, without losing the personal touch necessary tohelp change behavior.
The Economics of Outreach: Scaling Clinical CallCenters Is Expensive
Clinical outreach centers typically employ a blend oftrained care professionals and clinical care professionals,such as registered nurses and pharmacists. The fullyloaded hourly wage of these individuals can exceed $50,which means the cost of even a relatively brief (15-20minute) phone call can approach $20. This figure isconservative, given that the industry-standard cost for acall for technical support centers ranges between $20and $40,11 using significantly less costly staff. This costdoes not decrease with increased call center staff or withlarger numbers of patients to call, so organizations’ abil-ities to scale outreach programs using care representa-tives are significantly limited.
Today, health plans and disease management pro-grams are evolving new strategies and solutions to helptheir patient populations adhere to treatment plans.We suggest that any strategy must meet 2 primary tests:1. Is it efficient? Efficient solutions scale well and offer a
low marginal cost of operation.2. Is it effective? Effective solutions deliver similar re -sponse rates and engagement rates as the current gold standard—human outreach by care support representatives.
What Needs to Be Done Today and TomorrowTraditionally, MCOs and disease management pro-
grams use a broad range of outreach methods, includingnurses or other specialty practitioners to contact par-ticipants, review program benefits, respond to ques-tions, and ultimately, enroll members. Once enrolled,these same specialists may contact members for surveys,health status updates, medication reminders, and othercommunications designed to foster compliance.
In principle, this form of operation should be effec-
tive (and often is with small populations). For theorganizations paying for these programs, cost benefitsare largely dependent on the ability to reach large num-bers of patients, enroll them, and provide ongoinghealth and wellness support. Considering that thenumber of individuals with chronic diseases is estimat-ed to be in the hundreds of millions, the scale of enroll-ment is too great to manage cost-effectively with tradi-tional outreach methods.
Communication Works, but Not Cost-EffectiveIn the Medicare Health Support phase 1 study, the
Centers for Medicare & Medicaid Services determinedthat the value delivered by these programs does notovercome program costs.12 It was simply not cost-effi-cient (nor economically feasible) for clinical staff orcare support specialists to communicate with evenmoderately large at-risk populations. And yet, the samestudy found that this type of interventional communi-cation had a clear beneficial impact on participants.“Participating beneficiaries tend to be a healthier andless-costly subset of the intervention group. Thus, highparticipation rates will likely be a factor in the abilityof the [Medicare Health Support organizations] toimpact their assigned intervention populations.”12
And although human communication is certainlythe benchmark for clinical results, automating commu-nication shows some positive results. Properly imple-mented, this form of communication may deliver simi-lar clinical results at a far lower marginal cost.
Communications Automation: Scalable Interactionfor Large Populations
As noted earlier, any type of automated communi-cation must be able to connect efficiently with largenumbers of patients or members. Automated commu-nication must also connect effectively, by delivering anexperience that resembles an actual clinician–patientinteraction. Modern communications systems can bemodeled against good examples of productive clinicalinteractions (eg, a system could emulate the voice and
For organizations, improved patient adherence means the ability to deliver bettercare while reducing medical expense ratiosdriven by unnecessary hospitalizations andexcess interventions.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 23

24 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
BUSINESS
persona of an experienced call center representative oran outreach nurse).
Effective interventional dialogue with patientsinvolves understanding the patient’s specific concernsand health beliefs, embracing that information, andthen using it to tailor interventions specific to theirneeds. When insights such as these are applied to thetreatment regimen, adherence improves dramatically.13
And as discussed before, improved adherence can pro-vide a positive boost to health outcomes, both proxi-mal and for the long-term.
Automated patient communication offers addition-al potential benefits. With the majority of contactsmanaged through an automated system, organizationscan optimize the use of live agent care supportresources by triaging those patients most in need,thereby responding more efficiently to critical patientcare questions (see below).
The ability to deliver automated patient communi-cation programs efficiently (at a low unit cost) andeffectively (with a positive result across the majority ofrespondents) may offer additional distinct advantages,including increased scope (the lowered unit costimproves the provider’s ability to reach out to morepatients or members) and improved health economics(improved individual outcomes across a broad segmentof the at-risk population that contributes to improve-ment in the aggregate outcome profile).
Key Criteria for Successful Automation of PatientOutreach Communications
Varolii Corporation’s healthcare division has beencommunicating with tens of millions of patients on amonthly basis on a variety of healthcare-related areas.Based on the experience of delivering these automatedcalls, and on Varolii’s general experience in deliveringbillions of automated notifications over the past sever-al years in a variety of industries, we believe that 5 keycriteria can determine whether automated communica-
tions will serve as a useful adjunct to patient outreach.These criteria revolve around the concepts of efficien-cy and effectiveness discussed earlier:1. Scalability. If you cannot reach large populations
cost-effectively, then any other enabling criteria will not matter.
2. Clarity. Most people, particularly older or at-riskindividuals, find artificial voices, varying intona-tions, pace, and variable volume levels not onlyannoying, but difficult to understand.14
3. Personalization and Interactivity. “Personaliza -tion,” or tailoring the message to specifically addressindividual concerns, enables automated communica-tions to more closely match the experience of con-versing with a clinician or specialty representative.Results of Datamonitor’s Patient Compliance Survey,2004, authored by Adele Schulz, “support the ideathat personalized communication with patients is animportant tool in compliance initiatives.”15
“Interactivity” is the ability to accept patientrespon ses either through keypad presses or voice re -sponse, and deliver the next question or informationbased on the previous response. Interactivity can helpensure regulatory compliance by enabling appropriateauthentication. As an example, HIPAA (HealthInsurance Portability and Accountability Act) com-pliance through authentication, sometimes known asright party contact, could be managed as follows:
• Before giving any personalized information, an auto-mated system could ask the individual to confirmthat he/she is the correct party
• If further authentication is required, the systemcould ask for appropriate credentials.
This type of interactivity can also be used to collect survey data and patient feedback throughsurvey questions.
4. Reporting Visibility. Reporting is important bothto understand aggregate behaviors and make usefulprogram changes, as well as to provide substantiated,auditable performance data. Automation offers sig-nifi cant advantages in data collection and speed ofanalysis. Reporting can help organizations measurethe results of their outreach efforts more effectively.Demonstration of results against required objectives,such as the Health Effectiveness Data and In for ma -tion Set and other programs from accrediting andregulatory bodies, may enable organizations to satis-fy these requirements more efficiently with a betteroutcome.
5. Analytics. Analytics underlies useful personaliza-tion. Applying a detailed scoring model helps the
The ability to deliver automated patient communication programs efficientlyand effectively may offer additional distinct advantages, including increased scopeand improved health economics.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 24

25www.AHDBonline.comVOL. 1 NO. 9
Automated Communication Strategies
evaluation of several key factors,such as which patients are mostlikely to take action, and whetherthey are being contacted too lit-tle, too much, or the right amountusing the best method. At a deep-er level, analytics also providesinsight on the best approach forcontacting patients, evaluatingsuch treatment strategies as thebest calling windows, media(voice, e-mail, text message, or acombination of these), persona,retry strategy, among near-infinitecombinations of these.
The impact of automated com-munication is further enhancedby tailoring interventional strate-gies on a per-patient basis, com-bining analysis of historicalpatient clinical data along withactual patient response data. Forexample, an analytics-enabledsolution may initially help deter-mine which patients should becontacted first, based on drug andtherapeutic categories, number ofmaintenance medications, com-plexity of medication regimen, orpatient demographics.By looking at the history of patient refill behaviors,
the system can determine whether, when, and how fre-quently to communicate with the individual patient.Over time, the system can become increasingly “intel-ligent” and better capable of determining the profile ofthe most receptive patients.
Results from automated systems capable of decision-making can support effective personalized communica-tions with many patients on an individualized basis. Thisprocess is sometimes referred to as “mass personalization.”
Automated Communication Improves BP Monitoringin Frail Elderly: New Study Results
The following study was developed to addressuncontrolled hypertension and the use of automatedcommunication in a patient cohort from the MedicareHealth Support (MHS) pilot program in Maryland andthe District of Columbia during a 2-month period(March 19, 2007-May 24, 2007).16
The Treat to Target (TTT) initiative approachesuncontrolled hypertension by the simple principle that
lower is better. The TTT also bases optimal targetranges on specific patient diagnoses, such as BP<140/90 mm Hg for patients with heart failure (HF)but BP <130/80 mm Hg for patients with diabetes.
For the present trial, a cohort of approximately 800patients was selected from the MHS pilot population,based on a primary diagnosis of HF or diabetes andrecently reported BP readings above the established tar-get range.16 Of these, 318 agreed to participate in a trialof an automated telephony system and home BP moni-toring. A matched cohort of 304 hypertensive benefici-aries continued to receive the usual nurse-based diseasemanagement services of the MHS program as a compar-ison group. The study examined whether frail, elderly(median age, 75 years) patients with hypertension werewilling and able to listen and respond to weekly auto-mated phone calls that provided support for therapeuticand medication regimens, while offering care supportpersonnel with weekly reporting on the results. Thestudy covered 2 areas—patient BP and patient adher-ence to specific antihypertensive regimens. The objec-
Auth
No
No Yes
Yes
Greeting callDynamic prompts
3rd party
Answering machine Message
retrieval with PIN
“Did you check your blood pressure?”
“What prevented you from
checking it?”“What were
the results?”Out oflimits
“Why not?”
My doctor discontinued Rx
I didn’t feel well
“Thank you”
I didn’t think it was working
I forgot
“Thank you”Immediate transfer to
care specialist
Within limits
“Did you take your medication?”
Figure 2 Survey Call Flow
Source: Montijo M, Ross M. Use of automated telephony to optimize blood pressure and medicationmanagement of hypertensive frail elderly patients. Presented at the Disease Management Associationof America 9th Annual Disease Management Leadership Forum and Integrated Case Summit;September 16, 2007; Las Vegas, NV.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 25

26 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
BUSINESS
tives were to improve quality of care and lower care sup-port personnel utilization.
The study posed a series of questions using branch-ing logic to generate targeted questioning of yes/no and multiple choice questions. Figure 2 depicts the for-mat of the survey, showing the nature of the logic, thelocation of the transfers to human clinical support, and
the types of questions asked. The main results of thissurvey were16:• 245 patients (87.5%) achieved systolic BP within
target or had marked improvement from baseline>160 mm Hg
• 302 patients (96.8%) achieved diastolic BP within target or significantly improved from baseline>100 mm Hg
• 66% of the contacts validated as a “live answer” (ie,the patient answered the call, or someone else in thehousehold handed the phone to the patient, afterwhich the patient validated)
• Of those responding, 581 (33%) completed theentire survey, and 33% were transferred to a caresupport specialist for additional assistance
• No difference was seen between the automatedtele-phony and nurse-contacted cohorts in percentachieving targeted systolic and diastolic BP or percentreceiving antihypertensive medication adjustment
• Cost of automated telephony for a BP reading was95% lower than using a care support representativeto retrieve the reading.Perhaps the most important outcome of this study
was that 174 patients (54% of the study group) hadtheir antihypertensive regimens altered based on surveyresponses.16 The clear inference is that frequent report-ing on patient BP and medication-taking behaviors,along with the ability to efficiently gather and analyzethat information, offers clinicians significant insightson ongoing titration of medication or other elements ofa therapeutic regimen.
Better Health and Health EconomicsResults of this study show how applying certain
forms of automated communication to treatmentadherence programs may potentially offer distinct
advantages to patients and organizations.16 In additionto the improvements in clinical outcomes delivered byregular communications, automating outreach pro-grams may enable MCOs and disease management/wellness programs to:• Reach out to more patients cost-effectively• Target and reach substantially more patients, and
enroll more patients overall into existing programsfor improved return on investment
• Consistently manage patient adherence across largepopulations
• Gain potential insights into patient medication-tak-ing and other relevant behaviors for further analysis
• Empower existing care support staff by drivinginbound, interested patients into the call center andby triaging the more acute or at-risk individuals.
ConclusionsIt is well understood that regular, consistent commu-
nications from care teams can mediate medication-tak-ing behaviors in many patients with chronic diseasesand, in many cases, the health outcomes are dependenton those behaviors. These communications comprise afocus area in healthcare that can be extended by usingmodern automated communications to augment otheroutreach strategies. Although all the data from the newstudy cited here are not in yet, automated communica-tions satisfying the criteria outlined in this article aredemonstrating some ability to connect with, and medi-ate behavior in, large populations of chronically illpatients. Our hope is that in the future, automated com-munications systems will enable organizations to pro-vide communications at a scale that will improve healthoutcomes, both proximal and longer-term, for the mil-lions of “Toms” with chronic conditions. ■
References1. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med.2005;353:487-497.2. Pharmaceutical Safety Institute. Pharmaceutical Safety Institute andHarris Interactive Consumer Drug Safety Perception Survey Results.http://www.psisafety.org/images/InstituteHarrisSurvey.pdf. AccessedSeptember 12, 2008.3. Sud A, Kline-Rogers E, Fang J, et al. Reasons for non-adherence tocardiac medications in patients discharged with acute coronary symp-toms. Presented at the American College of Cardiology AnnualScientific Session; March 7-10, 2004; New Orleans, LA.4. Case Management Society of America. Case Management AdherenceGuidelines, Version 2.0. http://www.cmsa.org/portals/0/pdf/CMAG2.pdf.Accessed June 7, 2008.5. Sabaté E, ed. Adherence to long-term therapies: evidence for action[monograph online]. World Health Organization; 2003. http://whqlibdoc.who.int/publications/2003/9241545992.pdf. Accessed June 9, 2008.6. McCarthy R. The price you pay for the drug not taken. Bus Health.1998;16:27-33. http://findarticles.com/p/articles/mi_m0903/is_n10_v16/ai_n27541886/pg_1?tag=artBody;col1. Accessed October 22, 2008.
Perhaps the most important outcome of this study was that 174 patients (54% of the study group) had their antihypertensiveregimens altered.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 26

27www.AHDBonline.comVOL. 1 NO. 9
Automated Communication Strategies
Stakeholder PerspectiveEfficient Automated Call System Improves Adherence, but What about Net Costs?
PAYERS/FINANCIAL OFFICERS: Managed careorganizations (MCOs) strive to deliver the highestlevel of value for each healthcare dollar that theorganization must spend. An MCO incurs anexpense to buy pharmaceuticals for its membersand, in turn, those medications should improve thehealth of the member/patient. The MCO, in return,wants its members to improve their health, main-tain their current health, or avoid catastrophichealth problems because of their member’s adher-ence to a prescribed medication regimen. Dr Rossdescribes an outgoing automated phone calling system that he reports improves adherence forpatients in following their prescribed antihyperten-sive medication regimen. He reports results of hisrecent study that follows 304 elderly patients withhypertension who are matched to another 304 con-trol patients.
An automated phone system makes outboundcalls to these patients. Dr Ross reports this automat-ed calling system as having variable costs that are lessexpensive than those calls initiated from the clinicaloutreach call centers of disease management compa-nies. It is appropriate to note that Dr Ross is VicePresident of Healthcare for Varolii Corporation,which provides such automated calling systems.
At MCOs, the chief medical officers, medicaldirectors, directors of pharmacy, directors of utiliza-
tion management, and directors of quality manage-ment are all interested in methods that improvepatient compliance, improve outcomes for patients,or improve the documentation of that compliance.
The chief financial officers of these organizations,however, want to know if these programs thatimprove medication adherence will also save theMCO money. The present article clearly addressesthe first issue by proposing a method where an MCOcan efficiently improve pharmacy compliance. Inthat, this article is useful for those involved in med-ication compliance.
The article, however, does not address the chieffinancial officer’s usual question, “How does effi-ciently increasing medication adherence save theMCO money in the long run?” That question isimportant and is worthy of further research, by DrRoss or by others. It could be reframed as, “Will thecash outflows spent to operate an automated callcenter yield a positive net present value when meas-ured against the future savings (ie, decreased cashoutflows) in medical expenses on those same target-ed patients?”
Geoffrey P. Cole, MD, MBAChief Medical OfficerHealth Plan SelectAthens, Georgia
7. Kung HC, Hoyert DL, Xu JQ, Murphy SL. Deaths: final data for 2005.Natl Vital Stat Rep. 2008;56:1-120. 8. Cherry DK, Woodwell DA, Rechtsteiner EA. National AmbulatoryMedical Care Survey: 2005 summary. Adv Data. 2007;387:1-39.9. Centers for Disease Control and Prevention. National Center forHealth Statistics. Health, United States, 2007. Hyattsville, MD: USDepartment of Health and Human Services; 2007. http://www.cdc.gov/nchs/data/hus/hus07.pdf. Accessed June 8, 2008. 10. Stewart MA. Effective physician-patient communication and healthoutcomes: a review. Can Med Assoc J [serial online]. 1995;152:1423-1433.http://www.cmaj.ca/cgi/content/abstract/152/9/1423. Accessed June 7, 2008.11. HDI Advisory Services. Advisory Services Q&A page. http://www.thinkhdi.com/library/deliverfile.aspx?filecontentid=350. AccessedJune 12, 2008.12. McCall N, Cromwell J, Bernard S. Evaluation of Phase I of MedicareHealth Support (Formerly Voluntary Chronic Care Improvement) PilotProgram Under Traditional Fee-for-Service Medicare. Baltimore, MD: RTI
International; June 2007. Project No: 0207960.002. Contract No: 500-00-0022. Sponsored by Centers for Medicare & Medicaid Services. 13. Friedman RH, Kazis LE, Jette A, et al. A telecommunications systemfor monitoring and counseling patients with hypertension: impact onmedication adherence and blood pressure control. Am J Hypertens.1996;9:285-292.14. Boehm E, for Forrester Research Inc. Designing interactions for anaging population. July 2007. http://www.forrester.com/Research/PDF/0,5110,42827,00.pdf. Accessed November 6, 2008.15. Non-compliance costs drug industry dear. September 6, 2004.http://www.in-pharmatechnologist.com/layout/set/print/content/view/print/183261. Accessed October 22, 2008. 16. Montijo M, Ross M. Use of automated telephony to optimize bloodpressure and medication management of hypertensive frail elderlypatients. Presented at the Disease Management Association of America9th Annual Disease Management Leadership Forum and IntegratedCase Summit; September 16, 2007; Las Vegas, NV.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 27

When Treating Your Patients:
• Evaluate for other treatable etiologies of anemia (iron, folate, or B12 defi ciency, hemolysis, or bleeding) to treat appropriately
• PROCRIT therapy should not be initiated at hemoglobin (Hb) levels 10 g/dL
• The dose of PROCRIT should be titrated for each patient to achieve and maintain the lowest Hb level suffi cient to avoid the need for red blood cell (RBC) transfusion
• The rate of Hb increase should not exceed 1 g/dL in any 2-week period
• Monitor Hb weekly until stable, and then regularly during therapy
For Anemic Cancer Patients With Metastatic, Non-myeloid Malignancies Receiving Chemotherapy…
CONTROLTHE RESPONSE
MANAGE HEMOGLOBIN AND REDUCE TRANSFUSIONS
43156ALT_Control Ad_V1 1-2 11/11/08 6:11:14 PM
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 28

PROCRIT Indication PROCRIT is indicated for the treatment of anemia due to the effect of concomitantly administered chemotherapy based on studies that have shown a reduction in the need for RBC transfusions in patients with metastatic, non-myeloid malignancies receiving chemotherapy for a minimum of 2 months. Studies to determine whether PROCRIT increases mortality or decreases progression-free/recurrence-free survival are ongoing. • PROCRIT is not indicated for use in patients receiving hormonal
agents, therapeutic biologic products, or radiotherapy unless receivingconcomitant myelosuppressive chemotherapy.
• PROCRIT is not indicated for patients receiving myelosuppressive therapy when the anticipated outcome is cure due to the absence of studies that adequately characterize the impact of PROCRIT on progression-free and overall survival (see WARNINGS: Increased Mortality and/or Increased Risk of Tumor Progression or Recurrence).
• PROCRIT is not indicated for the treatment of anemia in cancer patients due to other factors such as iron or folate deficiencies, hemolysis, or gastrointestinal bleeding (see PRECAUTIONS: Lack or Loss of Response).
• PROCRIT use has not been demonstrated in controlled clinical trials to improve symptoms of anemia, quality of life, fatigue, or patient well-being.
Important Safety Information
WARNINGS: INCREASED MORTALITY, SERIOUS CARDIOVASCULAR and THROMBOEMBOLIC EVENTS, and INCREASED RISK OF TUMOR PROGRESSION OR RECURRENCE
Renal failure: Patients experienced greater risks for death and serious cardiovascular events when administered erythropoiesis-stimulating agents (ESAs) to target higher versuslower hemoglobin levels (13.5 vs. 11.3 g/dL; 14 vs. 10 g/dL) in two clinical studies. Individualize dosing to achieve and maintain hemoglobin levels within the range of 10 to 12 g/dL.
Cancer: • ESAs shortened overall survival and/or increased the risk of
tumor progression or recurrence in some clinical studies in patients with breast, non-small cell lung, head and neck, lymphoid, and cervical cancers (see WARNINGS: Table 1).
• To decrease these risks, as well as the risk of serious cardio- and thrombovascular events, use the lowest dose needed to avoid red blood cell transfusion.
• Use ESAs only for treatment of anemia due to concomitant myelosuppressive chemotherapy.
• ESAs are not indicated for patients receiving myelosuppressivetherapy when the anticipated outcome is cure.
• Discontinue following the completion of a chemotherapy course.
Perisurgery: PROCRIT® (Epoetin alfa) increased the rate of deep venous thromboses in patients not receiving prophylactic anticoagulation. Consider deep venous thrombosis prophylaxis.
Contraindications• PROCRIT is contraindicated in patients with uncontrolled hypertension
or with known hypersensitivity to albumin (human) or mammalian cell-derived products.
Additional Important Safety Information• Patients with chronic renal failure experienced greater risks for death
and serious cardiovascular events (including myocardial infarction, stroke, congestive heart failure, and hemodialysis vascular access thrombosis) when administered ESAs to target higher versus lower hemoglobin levels (13.5 vs.11.3 g/dL; 14 vs. 10 g/dL) in two clinicalstudies; these risks also increased in controlled clinical trials of patients with cancer. A rate of hemoglobin rise of >1 g/dL over 2 weeks may contribute to these risks.
• PROCRIT therapy should not be initiated at hemoglobin levels 10 g/dL.
• The dose of PROCRIT should be titrated for each patient to achieve and maintain the lowest hemoglobin level suffi cient to avoid the need for blood transfusion.
• When the hemoglobin reaches a level needed to avoid transfusion or, increases by more than 1 g/dL in a 2-week period, the PROCRIT dose should be reduced by 25%. Withhold the dose of PROCRIT if the hemoglobin exceeds a level needed to avoid transfusion. Restart dose at 25% below the previous dose when the hemoglobin approaches a level where transfusions may be required. Discontinue if after 8 weeks of therapy there is no response as measured by hemoglobin levels or if transfusions are still required.
• Monitor hemoglobin regularly during therapy, weekly until hemoglobin becomes stable.
• Cases of pure red cell aplasia (PRCA) and of severe anemia, with or without other cytopenias, associated with neutralizing antibodies to erythropoietin have been reported in patients treated with PROCRIT; predominantly in patients with chronic renal failure receiving PROCRIT by subcutaneous administration. If any patient develops a sudden lossof response to PROCRIT, accompanied by severe anemia and low reticulocyte count, and anti-erythropoietin antibody-associated anemia is suspected, withhold PROCRIT and other erythropoietic proteins. Contact ORTHO BIOTECH (1-888-2ASKOBI or 1-888-227-5624) to perform assays for binding and neutralizing antibodies. If erythropoietin antibody-mediated anemia is confirmed, PROCRIT should be permanently discontinued and patients should not be switched to other erythropoietic proteins.
• The safety and effi cacy of PROCRIT therapy have not been established in patients with a known history of a seizure disorder or underlyinghematologic disease (e.g., sickle cell anemia, myelodysplastic syndromes, or hypercoagulable disorders).
• In some female patients, menses have resumed following PROCRIT therapy; the possibility of pregnancy should be discussed and the need for contraception evaluated.
• Prior to and regularly during PROCRIT therapy monitor iron status; transferrin saturation should be 20% and ferritin should be
100 ng/mL. During therapy absolute or functional iron deficiency may develop and all patients will eventually require supplemental iron to adequately support erythropoiesis stimulated by PROCRIT.
• Treatment of patients with grossly elevated serum erythropoietin levels (e.g., >200 mUnits/mL) is not recommended.
• During PROCRIT therapy, blood pressure should be monitored carefully and aggressively managed, particularly in patients with an underlying history of hypertension or cardiovascular disease.
• Seizures in PROCRIT-treated patients have been reported in the context of a signifi cant increase in hemoglobin from baseline; increasesin blood pressure were not always observed; and patients may have had other underlying central nervous system pathology.
• The most commonly reported side effects (>10%) for PROCRIT in clinical trials were pyrexia, diarrhea, nausea, vomiting, edema, asthenia, fatigue, shortness of breath, paresthesia, and upper respiratory infection.
Manufactured by: Amgen Inc., Thousand Oaks, California 91320-1789Distributed by: Ortho Biotech Products, L.P., Bridgewater, New Jersey 08807-0914 © Ortho Biotech Products, L.P. 2008 11/08 08PCTC2487 308470
Please see Brief Summary of Prescribing Information, including Boxed WARNINGS, on adjacent page.
43156ALT_Control Ad_V1 1-2 11/11/08 6:11:14 PM43156ALT_Control Ad_V1 1-2 11/11/08 6:11:14 PM
Business_FDA_NovDec .qxp:Cover 11/25/08 12:15 PM Page 29

BRIEF SUMMARY OF PROCRIT® PRESCRIBING INFORMATION FOR THE TREATMENT OF ANEMIA INCANCER PATIENTS ON CHEMOTHERAPY
PROCRIT®
(Epoetin alfa)
FOR INJECTION
FOR FULL PRESCRIBING INFORMATION FOR ALL INDICATIONS,REFER TO THE PHYSICIANS’ DESK REFERENCE®
INDICATIONS AND USAGE
PROCRIT® is indicated for the treatment of anemia due to the effect of concomitantly administeredchemotherapy based on studies that have shown a reduction in the need for RBC transfusions in patients withmetastatic, non-myeloid malignancies receiving chemotherapy for a minimum of 2 months. Studies to determinewhether PROCRIT® increases mortality or decreases progression-free/recurrence-free survival are ongoing.
• PROCRIT® is not indicated for use in patients receiving hormonal agents, therapeutic biologic products, orradiotherapy unless receiving concomitant myelosuppressive chemotherapy.
• PROCRIT® is not indicated for patients receiving myelosuppressive therapy when the anticipated outcomeis cure due to the absence of studies that adequately characterize the impact of PROCRIT® on progression-free and overall survival (see WARNINGS: Increased Mortality and/or Increased Risk of Tumor Progressionor Recurrence).
• PROCRIT ® is not indicated for the treatment of anemia in cancer patients due to other factors such as ironor folate deficiencies, hemolysis, or gastrointestinal bleeding (see PRECAUTIONS: Lack or Loss ofResponse).
• PROCRIT ® use has not been demonstrated in controlled clinical trials to improve symptoms of anemia,quality of life, fatigue, or patient well-being.
CONTRAINDICATIONSPROCRIT® is contraindicated in patients with: 1. Uncontrolled hypertension. 2. Known hypersensitivity tomammalian cell-derived products. 3. Known hypersensitivity to Albumin (Human).
WARNINGS
Pediatrics
Risk in Premature InfantsThe multidose preserved formulation contains benzyl alcohol. Benzyl alcohol has been reported to beassociated with an increased incidence of neurological and other complications in premature infants which aresometimes fatal.
Adults
Increased Mortality, Serious Cardiovascular and Thromboembolic EventsPatients with chronic renal failure experienced greater risks for death and serious cardiovascular events whenadministered erythropoiesis-stimulating agents (ESAs) to target higher versus lower hemoglobin levels (13.5vs. 11.3 g/dL; 14 vs. 10 g/dL) in two clinical studies. Patients with chronic renal failure and an insufficienthemoglobin response to ESA therapy may be at even greater risk for cardiovascular events and mortality thanother patients. PROCRIT® and other ESAs increased the risks for death and serious cardiovascular events incontrolled clinical trials of patients with cancer. These events included myocardial infarction, stroke, congestiveheart failure, and hemodialysis vascular access thrombosis. A rate of hemoglobin rise of > 1 g/dL over 2 weeksmay contribute to these risks.
In a randomized prospective trial, 1432 anemic chronic renal failure patients who were not undergoing dialysiswere assigned to Epoetin alfa (rHuEPO) treatment targeting a maintenance hemoglobin concentration of 13.5 g/dL or 11.3 g/dL. A major cardiovascular event (death, myocardial infarction, stroke, or hospitalization forcongestive heart failure) occurred among 125 (18%) of the 715 patients in the higher hemoglobin groupcompared to 97 (14%) among the 717 patients in the lower hemoglobin group (HR 1.3, 95% CI: 1.0, 1.7,p = 0.03).
Increased risk for serious cardiovascular events was also reported from a randomized, prospective trial of 1265hemodialysis patients with clinically evident cardiac disease (ischemic heart disease or congestive heartfailure). In this trial, patients were assigned to PROCRIT® treatment targeted to a maintenance hematocrit ofeither 42 ± 3% or 30 ± 3%. Increased mortality was observed in 634 patients randomized to a targethematocrit of 42% [221 deaths (35% mortality)] compared to 631 patients targeted to remain at a hematocritof 30% [185 deaths (29% mortality)]. The reason for the increased mortality observed in this study is unknown,however, the incidence of non-fatal myocardial infarctions (3.1% vs. 2.3%), vascular access thromboses (39%vs. 29%), and all other thrombotic events (22% vs. 18%) were also higher in the group randomized to achievea hematocrit of 42%. An increased incidence of thrombotic events has also been observed in patients withcancer treated with erythropoietic agents.
In a randomized controlled study (referred to as Cancer Study 1 - the ‘BEST’ study) with another ESA in 939women with metastatic breast cancer receiving chemotherapy, patients received either weekly Epoetin alfa orplacebo for up to a year. This study was designed to show that survival was superior when an ESA wasadministered to prevent anemia (maintain hemoglobin levels between 12 and 14 g/dL or hematocrit between36% and 42%). The study was terminated prematurely when interim results demonstrated that a highermortality at 4 months (8.7% vs. 3.4%) and a higher rate of fatal thrombotic events (1.1% vs. 0.2%) in the first4 months of the study were observed among patients treated with Epoetin alfa. Based on Kaplan-Meierestimates, at the time of study termination, the 12-month survival was lower in the Epoetin alfa group than inthe placebo group (70% vs. 76%; HR 1.37, 95% CI: 1.07, 1.75; p = 0.012).
A systematic review of 57 randomized controlled trials (including Cancer Studies 1 and 5 - the ‘BEST’ and‘ENHANCE’ studies) evaluating 9353 patients with cancer compared ESAs plus red blood cell transfusion withred blood cell transfusion alone for prophylaxis or treatment of anemia in cancer patients with or withoutconcurrent antineoplastic therapy. An increased relative risk of thromboembolic events (RR 1.67, 95% CI: 1.35,2.06; 35 trials and 6769 patients) was observed in ESA-treated patients. An overall survival hazard ratio of 1.08(95% CI: 0.99, 1.18; 42 trials and 8167 patients) was observed in ESA-treated patients.
An increased incidence of deep vein thrombosis (DVT) in patients receiving Epoetin alfa undergoing surgicalorthopedic procedures has been observed (see ADVERSE REACTIONS, Surgery Patients: Thrombotic/VascularEvents in full Prescribing Information). In a randomized controlled study (referred to as the ‘SPINE’ study), 681adult patients, not receiving prophylactic anticoagulation and undergoing spinal surgery, received either 4 doses of 600 U/kg Epoetin alfa (7, 14, and 21 days before surgery, and the day of surgery) and standard ofcare (SOC) treatment, or SOC treatment alone. Preliminary analysis showed a higher incidence of DVT,
determined by either Color Flow Duplex Imaging or by clinical symptoms, in the Epoetin alfa group [16 patients(4.7%)] compared to the SOC group [7 patients (2.1%)]. In addition, 12 patients in the Epoetin alfa group and 7 patients in the SOC group had other thrombotic vascular events. Deep venous thrombosis prophylaxis shouldbe strongly considered when ESAs are used for the reduction of allogeneic RBC transfusions in surgical patients(see BOXED WARNINGS and DOSAGE AND ADMINISTRATION in full Prescribing Information).
Increased mortality was also observed in a randomized placebo-controlled study of PROCRIT® in adult patientswho were undergoing coronary artery bypass surgery (7 deaths in 126 patients randomized to PROCRIT®
versus no deaths among 56 patients receiving placebo). Four of these deaths occurred during the period ofstudy drug administration and all four deaths were associated with thrombotic events. ESAs are not approvedfor reduction of allogeneic red blood cell transfusions in patients scheduled for cardiac surgery.
Increased Mortality and/or Increased Risk of Tumor Progression or Recurrence Erythropoiesis-stimulating agents resulted in decreased locoregional control/progression-free survival and/oroverall survival (see Table 1). These findings were observed in studies of patients with advanced head and neckcancer receiving radiation therapy (Cancer Studies 5 and 6), in patients receiving chemotherapy for metastaticbreast cancer (Cancer Study 1) or lymphoid malignancy (Cancer Study 2), and in patients with non-small cell lungcancer or various malignancies who were not receiving chemotherapy or radiotherapy (Cancer Studies 7 and 8).
Table 1: Randomized, Controlled Trials with Decreased Survival and/or Decreased Locoregional Control
Adverse Achieved Outcome for
Hemoglobin Hemoglobin Primary ESA-containingStudy / Tumor / (n) Target (Median Q1,Q3) Endpoint Arm
Chemotherapy
Cancer Study 1Metastatic breast 12-14 g/dL 12.9 g/dL 12-month overall Decreased 12-monthcancer (n=939) 12.2, 13.3 g/dL survival survival
Cancer Study 2Lymphoid 13-15 g/dL (M) 11.0 g/dL Proportion of Decreased overallmalignancy (n=344) 13-14 g/dL (F) 9.8, 12.1 g/dL patients achieving survival
a hemoglobinresponse
Cancer Study 3Early breast 12.5-13 g/dL 13.1 g/dL Relapse-free and Decreased 3 yr.cancer (n=733) 12.5, 13.7 g/dL overall survival relapse-free and
overall survival
Cancer Study 4Cervical Cancer 12-14 g/dL 12.7 g/dL Progression-free Decreased 3 yr.(n=114) 12.1, 13.3 g/dL and overall survival progression-free
and locoregional and overall survivalcontrol and locoregional
control
Radiotherapy Alone
Cancer Study 5Head and neck ≥15 g/dL (M) Not available Locoregional Decreased 5-yearcancer (n=351) ≥14 g/dL (F) progression-free locoregional
survival progression-free survival
Decreased overallsurvival
Cancer Study 6Head and neck 14-15.5 g/dL Not available Locoregional Decreasedcancer (n=522) disease control locoregional
disease control
No Chemotherapy or Radiotherapy
Cancer Study 7Non-small cell 12-14 g/dL Not available Quality of life Decreased overalllung cancer (n=70) survival
Cancer Study 8Non-myeloid 12-13 g/dL 10.6 g/dL RBC transfusions Decreased overallmalignancy (n=989) 9.4, 11.8 g/dL survival
Decreased overall survival:Cancer Study 1 (the ‘BEST’ study) was previously described (see WARNINGS: Increased Mortality, SeriousCardiovascular and Thromboembolic Events). Mortality at 4 months (8.7% vs. 3.4%) was significantly higher inthe Epoetin alfa arm. The most common investigator-attributed cause of death within the first 4 months wasdisease progression; 28 of 41 deaths in the Epoetin alfa arm and 13 of 16 deaths in the placebo arm wereattributed to disease progression. Investigator assessed time to tumor progression was not different betweenthe two groups. Survival at 12 months was significantly lower in the Epoetin alfa arm (70% vs. 76%, HR 1.37,95% CI: 1.07, 1.75; p = 0.012).
Cancer Study 2 was a Phase 3, double-blind, randomized (darbepoetin alfa vs. placebo) study conducted in 344anemic patients with lymphoid malignancy receiving chemotherapy. With a median follow-up of 29 months,overall mortality rates were significantly higher among patients randomized to darbepoetin alfa as comparedto placebo (HR 1.36, 95% CI: 1.02, 1.82).
Cancer Study 7 was a Phase 3, multicenter, randomized (Epoetin alfa vs. placebo), double-blind study, in whichpatients with advanced non-small cell lung cancer receiving only palliative radiotherapy or no active therapywere treated with Epoetin alfa to achieve and maintain hemoglobin levels between 12 and 14 g/dL. Followingan interim analysis of 70 of 300 patients planned, a significant difference in survival in favor of the patients onthe placebo arm of the trial was observed (median survival 63 vs. 129 days; HR 1.84; p = 0.04).
Cancer Study 8 was a Phase 3, double-blind, randomized (darbepoetin alfa vs. placebo), 16-week study in 989anemic patients with active malignant disease, neither receiving nor planning to receive chemotherapy orradiation therapy. There was no evidence of a statistically significant reduction in proportion of patientsreceiving RBC transfusions. The median survival was shorter in the darbepoetin alfa treatment group (8months) compared with the placebo group (10.8 months); HR 1.30, 95% CI: 1.07, 1.57.
Decreased progression-free survival and overall survival:Cancer Study 3 (the ‘PREPARE’ study) was a randomized controlled study in which darbepoetin alfa wasadministered to prevent anemia conducted in 733 women receiving neo-adjuvant breast cancer treatment.After a median follow-up of approximately 3 years, the survival rate (86% vs. 90%, HR 1.42, 95% CI: 0.93, 2.18)and relapse-free survival rate (72% vs. 78%, HR 1.33, 95% CI: 0.99, 1.79) were lower in the darbepoetin alfa-treated arm compared to the control arm.
Cancer Study 4 (protocol GOG 191) was a randomized controlled study that enrolled 114 of a planned 460cervical cancer patients receiving chemotherapy and radiotherapy. Patients were randomized to receiveEpoetin alfa to maintain hemoglobin between 12 and 14 g/dL or to transfusion support as needed. The studywas terminated prematurely due to an increase in thromboembolic events in Epoetin alfa-treated patientscompared to control (19% vs. 9%). Both local recurrence (21% vs. 20%) and distant recurrence (12% vs. 7%)were more frequent in Epoetin alfa-treated patients compared to control. Progression-free survival at 3 yearswas lower in the Epoetin alfa-treated group compared to control (59% vs. 62%, HR 1.06, 95% CI: 0.58, 1.91).Overall survival at 3 years was lower in the Epoetin alfa-treated group compared to control (61% vs. 71%, HR1.28, 95% CI: 0.68, 2.42).
Cancer Study 5 (the ‘ENHANCE’ study) was a randomized controlled study in 351 head and neck cancerpatients where Epoetin beta or placebo was administered to achieve target hemoglobin of 14 and 15 g/dL for women and men, respectively. Locoregional progression-free survival was significantly shorter inpatients receiving Epoetin beta (HR 1.62, 95% CI: 1.22, 2.14; p = 0.0008) with a median of 406 days Epoetinbeta vs. 745 days placebo. Overall survival was significantly shorter in patients receiving Epoetin beta (HR 1.39,95% CI: 1.05, 1.84; p = 0.02).
WARNINGS: INCREASED MORTALITY, SERIOUS CARDIOVASCULAR and THROMBOEMBOLIC EVENTS,and INCREASED RISK OF TUMOR PROGRESSION OR RECURRENCE
Renal failure: Patients experienced greater risks for death and serious cardiovascular events whenadministered erythropoiesis-stimulating agents (ESAs) to target higher versus lower hemoglobinlevels (13.5 vs. 11.3 g/dL; 14 vs. 10 g/dL) in two clinical studies. Individualize dosing to achieve andmaintain hemoglobin levels within the range of 10 to 12 g/dL.
Cancer:• ESAs shortened overall survival and/or increased the risk of tumor progression or recurrence in
some clinical studies in patients with breast, non-small cell lung, head and neck, lymphoid, andcervical cancers (see WARNINGS: Table 1).
• To decrease these risks, as well as the risk of serious cardio- and thrombovascular events, usethe lowest dose needed to avoid red blood cell transfusion.
• Use ESAs only for treatment of anemia due to concomitant myelosuppressive chemotherapy.
• ESAs are not indicated for patients receiving myelosuppressive therapy when the anticipatedoutcome is cure.
• Discontinue following the completion of a chemotherapy course.
Perisurgery: PROCRIT® increased the rate of deep venous thromboses in patients not receiving prophylactic anticoagulation. Consider deep venous thrombosis prophylaxis.
(See WARNINGS: Increased Mortality, Serious Cardiovascular and Thromboembolic Events,WARNINGS: Increased Mortality and/or Increased Risk of Tumor Progression or Recurrence,INDICATIONS AND USAGE, and DOSAGE AND ADMINISTRATION in full Prescribing Information.)
43156ALT_Control Ad_V1 3-4 11/11/08 6:12:25 PM
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 30

Decreased locoregional control:Cancer Study 6 (DAHANCA 10) was conducted in 522 patients with primary squamous cell carcinoma of thehead and neck receiving radiation therapy randomized to darbepoetin alfa with radiotherapy or radiotherapyalone. An interim analysis on 484 patients demonstrated that locoregional control at 5 years was significantlyshorter in patients receiving darbepoetin alfa (RR 1.44, 95% CI: 1.06, 1.96; p = 0.02). Overall survival was shorterin patients receiving darbepoetin alfa (RR 1.28, 95% CI: 0.98, 1.68; p = 0.08).
Pure Red Cell AplasiaCases of pure red cell aplasia (PRCA) and of severe anemia, with or without other cytopenias, associated withneutralizing antibodies to erythropoietin have been reported in patients treated with PROCRIT®. This has beenreported predominantly in patients with chronic renal failure (CRF) receiving PROCRIT® by subcutaneousadministration.Any patient who develops a sudden loss of response to PROCRIT®, accompanied by severe anemiaand low reticulocyte count, should be evaluated for the etiology of loss of effect, including the presence ofneutralizing antibodies to erythropoietin (see PRECAUTIONS: Lack or Loss of Response). If anti-erythropoietinantibody-associated anemia is suspected, withhold PROCRIT® and other erythropoietic proteins. Contact ORTHO BIOTECH at 1 888 2ASK OBI (1-888-227-5624) to perform assays for binding and neutralizing antibodies.PROCRIT® should be permanently discontinued in patients with antibody-mediated anemia. Patients should notbe switched to other erythropoietic proteins as antibodies may cross-react (see ADVERSE REACTIONS:Immunogenicity).
Albumin (Human)
PROCRIT® contains albumin, a derivative of human blood. Based on effective donor screening and productmanufacturing processes, it carries an extremely remote risk for transmission of viral diseases. A theoreticalrisk for transmission of Creutzfeldt-Jakob disease (CJD) also is considered extremely remote. No cases oftransmission of viral diseases or CJD have ever been identified for albumin.
PRECAUTIONSThe parenteral administration of any biologic product should be attended by appropriate precautions in caseallergic or other untoward reactions occur (see CONTRAINDICATIONS). In clinical trials, while transient rasheswere occasionally observed concurrently with PROCRIT® therapy, no serious allergic or anaphylactic reactionswere reported (see ADVERSE REACTIONS in full Prescribing Information for more information regarding allergicreactions).
The safety and efficacy of PROCRIT® therapy have not been established in patients with a known history of aseizure disorder or underlying hematologic disease (eg, sickle cell anemia, myelodysplastic syndromes, orhypercoagulable disorders).
In some female patients, menses have resumed following PROCRIT® therapy; the possibility of pregnancy shouldbe discussed and the need for contraception evaluated.
Hematology: Exacerbation of porphyria has been observed rarely in patients with CRF treated with PROCRIT®.However, PROCRIT® has not caused increased urinary excretion of porphyrin metabolites in normal volunteers,even in the presence of a rapid erythropoietic response. Nevertheless, PROCRIT® should be used with cautionin patients with known porphyria.
In preclinical studies in dogs and rats, but not in monkeys, PROCRIT® therapy was associated with subclinicalbone marrow fibrosis. Bone marrow fibrosis is a known complication of CRF in humans and may be related tosecondary hyperparathyroidism or unknown factors. The incidence of bone marrow fibrosis was not increasedin a study of adult patients on dialysis who were treated with PROCRIT® for 12 to 19 months, compared to theincidence of bone marrow fibrosis in a matched group of patients who had not been treated with PROCRIT®.
Cancer patients should have hemoglobin measured once a week until hemoglobin has been stabilized, andmeasured periodically thereafter.
Lack or Loss of Response: If the patient fails to respond or to maintain a response to doses within therecommended dosing range, the following etiologies should be considered and evaluated: 1. Iron deficiency:Virtually all patients will eventually require supplemental iron therapy (see IRON EVALUATION); 2. Underlyinginfectious, inflammatory, or malignant processes; 3. Occult blood loss; 4. Underlying hematologic diseases (ie, thalassemia, refractory anemia, or other myelodysplastic disorders); 5. Vitamin deficiencies: Folic acid orvitamin B12; 6. Hemolysis; 7. Aluminum intoxication; 8. Osteitis fibrosa cystica; 9. Pure Red Cell Aplasia (PRCA)or anti-erythropoietin antibody-associated anemia: In the absence of another etiology, the patient should beevaluated for evidence of PRCA and sera should be tested for the presence of antibodies to erythropoietin (seeWARNINGS: Pure Red Cell Aplasia).
Iron Evaluation: During PROCRIT® therapy, absolute or functional iron deficiency may develop. Functional irondeficiency, with normal ferritin levels but low transferrin saturation, is presumably due to the inability tomobilize iron stores rapidly enough to support increased erythropoiesis. Transferrin saturation should be atleast 20% and ferritin should be at least 100 ng/mL.
Prior to and during PROCRIT® therapy, the patient’s iron status, including transferrin saturation (serum irondivided by iron binding capacity) and serum ferritin, should be evaluated. Virtually all patients will eventuallyrequire supplemental iron to increase or maintain transferrin saturation to levels which will adequately supporterythropoiesis stimulated by PROCRIT®.
Drug Interaction: No evidence of interaction of PROCRIT® with other drugs was observed in the course ofclinical trials.
Carcinogenesis, Mutagenesis, and Impairment of Fertility: Carcinogenic potential of PROCRIT® has notbeen evaluated. PROCRIT® does not induce bacterial gene mutation (Ames Test), chromosomal aberrations inmammalian cells, micronuclei in mice, or gene mutation at the HGPRT locus. In female rats treated IV withPROCRIT®, there was a trend for slightly increased fetal wastage at doses of 100 and 500 Units/kg.
Pregnancy Category C: PROCRIT® has been shown to have adverse effects in rats when given in doses 5 times the human dose. There are no adequate and well-controlled studies in pregnant women. PROCRIT®
should be used during pregnancy only if potential benefit justifies the potential risk to the fetus.
In studies in female rats, there were decreases in body weight gain, delays in appearance of abdominal hair,delayed eyelid opening, delayed ossification, and decreases in the number of caudal vertebrae in the F1 fetusesof the 500 Units/kg group. In female rats treated IV, there was a trend for slightly increased fetal wastage atdoses of 100 and 500 Units/kg. PROCRIT® has not shown any adverse effect at doses as high as 500 Units/kgin pregnant rabbits (from day 6 to 18 of gestation).
Nursing Mothers: Postnatal observations of the live offspring (F1 generation) of female rats treated withPROCRIT® during gestation and lactation revealed no effect of PROCRIT® at doses of up to 500 Units/kg. Therewere, however, decreases in body weight gain, delays in appearance of abdominal hair, eyelid opening, anddecreases in the number of caudal vertebrae in the F1 fetuses of the 500 Units/kg group. There were noPROCRIT®-related effects on the F2 generation fetuses.
It is not known whether PROCRIT® is excreted in human milk. Because many drugs are excreted in human milk,caution should be exercised when PROCRIT® is administered to a nursing woman.
Pediatric Use: See WARNINGS: Pediatrics
Pediatric Cancer Patients on Chemotherapy: The safety and effectiveness of PROCRIT® were evaluated in arandomized, double-blind, placebo-controlled, multicenter study (see CLINICAL EXPERIENCE, Weekly (QW)Dosing, Pediatric Patients in full Prescribing Information).
Geriatric Use: Insufficient numbers of patients age 65 or older were enrolled in clinical studies of PROCRIT®
for the treatment of anemia associated with pre-dialysis chronic renal failure, cancer chemotherapy, andZidovudine-treatment of HIV infection to determine whether they respond differently from younger subjects.
Information for Patients
Patients should be informed of the increased risks of mortality, serious cardiovascular events, thromboembolicevents, and increased risk of tumor progression or recurrence (see WARNINGS). In those situations in which thephysician determines that a patient or their caregiver can safely and effectively administer PROCRIT® at home,
instruction as to the proper dosage and administration should be provided. Patients should be instructed to readthe PROCRIT® Medication Guide and Patient Instructions for Use and should be informed that the MedicationGuide is not a disclosure of all possible side effects. Patients should be informed of the possible side effects ofPROCRIT® and of the signs and symptoms of allergic drug reaction and advised of appropriate actions. If homeuse is prescribed for a patient, the patient should be thoroughly instructed in the importance of proper disposaland cautioned against the reuse of needles, syringes, or drug product. A puncture-resistant container should beavailable for the disposal of used syringes and needles, and guidance provided on disposal of the full container.
Hypertension: Hypertension, associated with a significant increase in hemoglobin, has been noted rarely inpatients treated with PROCRIT®. Nevertheless, blood pressure in patients treated with PROCRIT® should bemonitored carefully, particularly in patients with an underlying history of hypertension or cardiovasculardisease.
Seizures: In double-blind, placebo-controlled trials, 3.2% (n = 2/63) of patients treated with PROCRIT® TIWand 2.9% (n = 2/68) of placebo-treated patients had seizures. Seizures in 1.6% (n = 1/63) of patients treatedwith PROCRIT® TIW occurred in the context of a significant increase in blood pressure and hematocrit frombaseline values. However, both patients treated with PROCRIT® also had underlying CNS pathology which mayhave been related to seizure activity.
In a placebo-controlled, double-blind trial utilizing weekly dosing with PROCRIT®, 1.2% (n = 2/168) of safety-evaluable patients treated with PROCRIT® and 1% (n = 1/165) of placebo-treated patients had seizures.Seizures in the patients treated with weekly PROCRIT® occurred in the context of a significant increase inhemoglobin from baseline values however significant increases in blood pressure were not seen. Thesepatients may have had other CNS pathology.
Thrombotic Events: In double-blind, placebo-controlled trials, 3.2% (n = 2/63) of patients treated withPROCRIT® TIW and 11.8% (n = 8/68) of placebo-treated patients had thrombotic events (eg, pulmonaryembolism, cerebrovascular accident), (see WARNINGS: Increased Mortality, Serious Cardiovascular andThromboembolic Events).
In a placebo-controlled, double-blind trial utilizing weekly dosing with PROCRIT®, 6.0% (n = 10/168) of safety-evaluable patients treated with PROCRIT® and 3.6% (n = 6/165) (p = 0.444) of placebo-treated patients hadclinically significant thrombotic events (deep vein thrombosis requiring anticoagulant therapy, embolic eventincluding pulmonary embolism, myocardial infarction, cerebral ischemia, left ventricular failure and thromboticmicroangiopathy). A definitive relationship between the rate of hemoglobin increase and the occurrence ofclinically significant thrombotic events could not be evaluated due to the limited schedule of hemoglobinmeasurements in this study.
The safety and efficacy of PROCRIT® were evaluated in a randomized, double-blind, placebo-controlled,multicenter study that enrolled 222 anemic patients ages 5 to 18 receiving treatment for a variety of childhoodmalignancies. Due to the study design (small sample size and the heterogeneity of the underlying malignanciesand of anti-neoplastic treatments employed), a determination of the effect of PROCRIT® on the incidence ofthrombotic events could not be performed. In the PROCRIT® arm, the overall incidence of thrombotic events was10.8% and the incidence of serious or life-threatening events was 7.2%.
ADVERSE REACTIONS
Immunogenicity
As with all therapeutic proteins, there is the potential for immunogenicity. Neutralizing antibodies toerythropoietin, in association with PRCA or severe anemia (with or without other cytopenias), have been reportedin patients receiving PROCRIT® (see WARNINGS: Pure Red Cell Aplasia) during post-marketing experience.
There has been no systematic assessment of immune responses, i.e., the incidence of either binding orneutralizing antibodies to PROCRIT®, in controlled clinical trials.
Where reported, the incidence of antibody formation is highly dependent on the sensitivity and specificity of theassay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assaymay be influenced by several factors including assay methodology, sample handling, timing of samplecollection, concomitant medications, and underlying disease. For these reasons, comparison of the incidenceof antibodies across products within this class (erythropoietic proteins) may be misleading.
Adverse Experiences Reported in Clinical TrialsIn double-blind, placebo-controlled studies of up to 3 months duration involving 131 cancer patients, adverseevents with an incidence > 10% in either patients treated with PROCRIT® or placebo-treated patients were asindicated below:
Percent of Patients Reporting Event
Patients Treated Placebo-treatedWith PROCRIT® Patients
Event (n = 63) (n = 68)
Pyrexia 29% 19%
Diarrhea 21%* 7%
Nausea 17%* 32%
Vomiting 17% 15%
Edema 17%* 1%
Asthenia 13% 16%
Fatigue 13% 15%
Shortness of Breath 13% 9%
Parasthesia 11% 6%
Upper Respiratory Infection 11% 4%
Dizziness 5% 12%
Trunk Pain 3%* 16%
* Statistically significant
Although some statistically significant differences between patients being treated with PROCRIT® and placebo-treated patients were noted, the overall safety profile of PROCRIT® appeared to be consistent with the diseaseprocess of advanced cancer. During double-blind and subsequent open-label therapy in which patients (n = 72for total exposure to PROCRIT®) were treated for up to 32 weeks with doses as high as 927 Units/kg, theadverse experience profile of PROCRIT® was consistent with the progression of advanced cancer.
Three hundred thirty-three (333) cancer patients enrolled in a placebo-controlled double-blind trial utilizingWeekly dosing with PROCRIT® for up to 4 months were evaluable for adverse events. The incidence of adverseevents was similar in both the treatment and placebo arms.
OVERDOSAGE
The expected manifestations of PROCRIT® overdosage include signs and symptoms associated with anexcessive and/or rapid increase in hemoglobin concentration, including any of the cardiovascular eventsdescribed in WARNINGS and listed in ADVERSE REACTIONS in full Prescribing Information. Patients receiving anoverdosage of PROCRIT® should be monitored closely for cardiovascular events and hematologicabnormalities. Polycythemia should be managed acutely with phlebotomy, as clinically indicated. Followingresolution of the effects due to PROCRIT® overdosage, reintroduction of PROCRIT® therapy should beaccompanied by close monitoring for evidence of rapid increases in hemoglobin concentration (>1 gm/dL per14 days). In patients with an excessive hematopoietic response, reduce the PROCRIT® dose in accordance withthe recommendations described in DOSAGE AND ADMINISTRATION in full Prescribing Information.
PROCRIT® (Epoetin alfa) FOR INJECTION
43156ALT_Control Ad_V1 3-4 11/11/08 6:12:25 PM
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 31

DOSAGE AND ADMINISTRATION
IMPORTANT: See BOXED WARNINGS and WARNINGS: Increased Mortality, Serious Cardiovascular andThromboembolic Events.
Prior to initiating treatment with PROCRIT® a hemoglobin should be obtained to establish that it is >10 to≤ 13 g/dL. The recommended dose of PROCRIT® is 300 Units/kg/day subcutaneously for 10 days beforesurgery, on the day of surgery, and for 4 days after surgery.
An alternate dose schedule is 600 Units/kg PROCRIT® subcutaneously in once weekly doses (21, 14, and 7 days before surgery) plus a fourth dose on the day of surgery.
All patients should receive adequate iron supplementation. Iron supplementation should be initiated no laterthan the beginning of treatment with PROCRIT® and should continue throughout the course of therapy. Deep venous thrombosis prophylaxis should be strongly considered (see BOXED WARNINGS).
PREPARATION AND ADMINISTRATION OF PROCRIT®
1. Do not shake. It is not necessary to shake PROCRIT®. Prolonged vigorous shaking may denature anyglycoprotein, rendering it biologically inactive.
2. Protect the solution from light. Parenteral drug products should be inspected visually for particulate matterand discoloration prior to administration. Do not use any vials exhibiting particulate matter or discoloration.
3. Using aseptic techniques, attach a sterile needle to a sterile syringe. Remove the flip top from the vialcontaining PROCRIT®, and wipe the septum with a disinfectant. Insert the needle into the vial, andwithdraw into the syringe an appropriate volume of solution.
4. Single-dose: 1 mL vial contains no preservative. Use one dose per vial; do not re-enter the vial. Discardunused portions.
Multidose: 1 mL and 2 mL vials contain preservative. Store at 2° to 8°C after initial entry and betweendoses. Discard 21 days after initial entry.
5. Do not dilute or administer in conjunction with other drug solutions. However, at the time of SCadministration, preservative-free PROCRIT® from single-use vials may be admixed in a syringe withbacteriostatic 0.9% sodium chloride injection, USP, with benzyl alcohol 0.9% (bacteriostatic saline) at a1:1 ratio using aseptic technique. The benzyl alcohol in the bacteriostatic saline acts as a local anestheticwhich may ameliorate SC injection site discomfort. Admixing is not necessary when using the multidosevials of PROCRIT® containing benzyl alcohol.
Manufactured by:Amgen Inc.One Amgen Center DriveThousand Oaks, CA 91320-1799
Distributed by:Ortho Biotech Products, L.P.Raritan, New Jersey 08869-0670
Revised 08/2008© OBPLP 200010112802BC
PROCRIT® (Epoetin alfa) FOR INJECTION
43156ALT_Control Ad_V1 5 11/11/08 6:12:49 PM
Talk is swirling around Washington as to who mayreplace Dr Andrew C. von Eschenbach at thehelm of the US Food and Drug Administration
(FDA). One well-known blogger has even begun a vot-ing contest where readers can choose from several can-didates for FDA Commissioner and cast a vote. There islittle question that the policy environment is pregnantwith change, but in most cases, it is quite possibly lessimportant who is appointed rather than what thechanges may entail.
This was obviously true with the presidential elec-tion. Given that both the McCain and Obama positionsfavored the import of prescription drugs, the ability ofthe government to negotiate prices under Medicare PartD, and the increasing uptake of generic drugs before thecampaign, it is virtually certain that the outcome of thepresidential contest mattered less to the pharmaceuticaland biotechnology industries than the contests in Con -gress. Not only did the November 4 election decide thatDemocrats were to achieve solid majorities in bothchambers, it has also paved the way for new congres-sional committee assignments and chairs.
This is the one area where “who” may matter, althoughonly in a matter of degree. Consider the case of the chair-manship for the Committee on Energy and Commerce. A clash of the titans emerged between 2 powerful andprominent members of Congress—Congressman John D.Dingell, the current chair, and Congressman HenryWaxman, who emerged the winner. This committee iskey to the oversight of various aspects of the FDA and theregulation of pharmaceutical industry. The activity of thiscommittee for October 2008 includes the following inves-tigations, announcements, statements, and reports:• Dingell, Stupak to Investigate Melamine Contam -
ination in Chinese Milk Products (10/2)• Dingell, Stupak Question FDA’s No-Bid Contract
with a PR Firm (10/2)• Dingell, Stupak Question Whether FDA Knowingly
Allowed Dangerous Drugs to be Sold to U.S. Con -sumers (10/8)
• Dingell, Stupak Continue DTC Ad Investigation(10/14)
GENERIC DRUG TRENDSFDA WATCH
The ObamaAdministration and the FDAMark Senak, JD
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 32

33www.AHDBonline.comVOL. 1 NO. 9
FDA WATCH
• Dingell, Stupak Continue Investigation into FDA’sQuestionable Handling of Bisphenol A (10/14)
• Dingell, Stupak Request Interview with von Esch -enbach on Bisphenol A (10/15)
• GAO Report Finds FDA’s Foreign Drug InspectionProgram Needs Significant Improvement (10/22).Ironically, Congressman Dingell made the case
that he is the preferable chair, because he is friendlierto industry with this 1-month track record. Now that Congressman Waxman has prevailed overCongressman Dingell for the chairmanship, one canexpect a great deal more intensity in terms of thebreadth and depth regarding scrutiny of the FDA andthe pharmaceutical industry than was shown inOctober 2008.
However, for the balance of the change, “who” isnot as important as “what” in terms of what must beaccomplished.
There is also a great deal of unfinished business withrespect to the FDA itself. Once a gold standard agency,the FDA has suffered tremendously during the past 8years and will have a great deal to do to reclaim its posi-tion as a flagship agency overseeing one fourth of thenation’s economy.
The following qualities are the ones that President-Elect Obama may seek for the individual who will takeover the FDA. That person must:• Have a solid grasp of the pharmaceutical industry,
without being directly associated with it. There aremembers in the Senate, particularly SenatorKennedy, who may insist that the individual haveno ties to the pharmaceutical industry itself. Still,the designee must have a good understanding ofclinical research and public health.
• Be able to balance the policymakers hunger for safe-ty, while assuring that the pipeline produces to pro-vide access. Although the public appetite isextremely risk averse, our slant to caution may bringa slowdown in new drug approvals. Longer approvaltime in the end means potentially higher drugprices, as patented drugs will have less time on themarket to recoup research and development costs.
• Have the credibility and gravitas to tell policy -makers on the Hill to stop using the agency as apolitical means, to gently remind members ofCongress that it is a new administration, that thereis a 1-party rule, and that most of them are in thatvery same party.
• Possess solid visionary and have noteworthy com-munication skills. The agency is in trouble not onlyfrom a functional point of view, but it has also donevery little to proactively address the descent of itsimage and to communicate and assure the publicand policymakers that it has a vision. In fact, theagency does not seem to acknowledge much of aproblem, much less to have a plan for solving it. Thenew commissioner will need to understand this, acton it, and seize leadership.In addition to these qualities, the first order of pri-
ority should be to completely implement the Food andDrug Administration Amendment Act (FDAAA).Right now the pipeline is getting clogged with Com -plete Response Letters and shifting the PrescriptionDrug User Fee Act dates, as the FDA tries to under-stand and implement the FDAAA. The FDA has beencharged with implementing a fairly broad scope ofreforms, but the longer it takes to identify and follow a roadmap for doing so, the more in the dark drug sponsors are going to be, which again contributes to a sluggish pipeline.
And as the policy and the communications environ-ments undergo breathtaking changes, it is importantthat the agency enunciate some points of view aboutthe uses of digital and social media by pharmaceuticalcompanies in marketing. The potential uses for socialand digital media are extraordinary, from public serviceannouncements to patient education videos, to riskmanagement tools; however, because regulatory cul-tures of most pharmaceuticals are generally conserva-tive, most are waiting for the FDA to say somethingwith regard to the use of such media.
The FDA appears nowhere near doing this, eventhough other industries have begun to embrace andstrategically anticipate and respond to the migrationinto digital media. It is time for the FDA to be a leader,not continue to be a follower, and give companies someguidance. And that guidance should be the medium,not the message.
All this and more needs to be accomplished by anObama-appointed FDA Commissioner, and in no shortorder, for the sake of the agency, public health, and the economy. ■
Mr Senak is Senior Vice President at Fleishman-Hillardin Washington, DC, and writes the Eye on FDA blog,www.eyeonfda.com.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 33

34 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
AHA MEETING HIGHLIGHTS
Several antithrombotic drugs in late-stage develop-ment were featured at the 2008 Scientific Sessionsof the American Heart Association (AHA).
Prasugrel. A new analysis of the antiplatelet drugprasugrel, a direct-acting P2Y12 antagonist currentlyunder US Food and Drug Administration review, ques-tions this agent’s supposed superiority over the currentstandard in this class, clopidogrel (Plavix). Results ofthe pivotal phase 3 Trial to Assess Improvement inTherapeutic Outcomes by Optimizing PlateletInhibition with Prasugrel (TRITON), which comparedprasugrel and clopidogrel, were released in late 2007.Among patients being considered for coronary stents,prasugrel prevented more future cardiac events thanclopidogrel, but with excess bleeding. Despite thisexcess risk, the net benefit still favored prasugrel—23fewer myocardial infarctions (MIs) per 1000 patientstreated, at a cost of 6 extra bleeding events.
More recent analyses of TRITON have shown thatmuch of the benefit of prasugrel in preventing ischemicevents occurs early on, but the excess bleeding occursafter 30 days of use. New analyses have shown that pra-sugrel is better than clopidogrel at preventing stentthrombosis (blood clots forming in stents).
At the AHA, a team of investigators at Cedars-Sinai Medical Center in Los Angeles discussed its inde-pendent statistical analysis (using a Bayesian method),showing that the true superiority of prasugrel in TRITON was not as large. In their analysis, the proba-bility of a 10% or more benefit with prasugrel overclopidogrel is less than 80%, and the chance that pra-sugrel is 20% better than clopidogrel in preventing cardiac events is less than 5%. If bleeding events are considered, the probability of a net benefit with prasugrel is even smaller, they argued.
Because of the risk-benefit ratio, Sanjay Kaul, MD,MPH, Director of the Vascular Physiology andThrombosis Research Laboratory at the Burns andAllen Research Institute at Cedars-Sinai, and leadinvestigator of the reanalysis, proposed a strategy forusing prasugrel. “One potential approach to optimizing
the benefit-risk profile of prasugrel could involve giv-ing it during the first 30 days as acute ‘induction’ ther-apy, followed by maintenance ‘consolidation’ therapywith a less potent antiplatelet agent, such as clopido-grel, in patients who receive stents,” he said.
Rivaroxaban. This oral drug factor Xa inhibitor—anew class of anticlotting agents—is entering a phase 3trial (and will enroll 16,000 patients) after the releaseof phase 2 data at the AHA. The data showed thatrivaroxaban could reduce MI and stroke risk, with anacceptable bleeding risk at its 2 lowest doses.
That study enrolled 3491 stable patients with arecent MI who were taking aspirin and clopidogrel (ifnecessary). Patients were randomized to placebo or 1 of4 doses of rivaroxaban (2.5-10 mg twice daily) for 6months, and were followed for 1 month after stoppingtherapy. As expected, higher doses of rivaroxabanincreased the rate of clinically significant bleeding.
Rivaroxaban reduced the risk of ischemic events by21% relative to placebo, but this difference was notdefinitive, given the small number of patients enrolled,reported C. Michael Gibson, MD, Chief of ClinicalResearch, Beth Israel Deaconess Medical Center,Boston. “We have decided to go forward to phase 3with the 2 lower doses—2.5 mg and 5 mg twice daily,”he said. These doses reduced the risk of death, MI, andstroke by 46% compared with placebo (P = .08) andwere associated with a major bleeding rate of 1.2%.
There was no drug-induced liver injury with rivarox-aban. The development of an oral direct thrombininhibitor—ximelagatran—was derailed as a result ofliver toxicity.
Other late-phase antithrombotic/antiplatelet drugsinvestigated for various thrombotic indications werediscussed at the meeting, including: • Apixaban, another oral factor Xa inhibitor• Cangrelor, another direct-acting P2Y12 antagonist• Dabigatran, an oral direct thrombin inhibitor,
which was recently approved in Europe (brandname, Pradaxa)
• Idraparinux, a long-acting factor Xa inhibitor. ■
The Antiplatelet Drug Pipeline: Some Promising CandidatesBy Wayne Kuznar
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 34

Do you measure resource utilization and costs associatedwith depression?
Managing quality and cost is the foundation of today’s
managed care structure. Wyeth recognizes that balancing
quality and cost is a formidable challenge for managed health
care professionals. We also recognize that success, in part,
hinges on tools and resources that can aid in the evaluation
of care management and may lead to reinforcing solutions. As
part of our continuing efforts to improve the quality of care for
patients with depression, we are proud to sponsor this
comprehensive claims-based review to promote ongoing
clinical and financial assessments that improve care in this
patient population.
To learn more about this exclusive program,
please contact your Wyeth Pharmaceuticals
Account Manager today!
N e w E d i t i o n N o w A v a i l a b l eAward-winning
Depression Benchmarks!
Gold AwardAster Awards, May 2007
Merit Awards (2)Healthcare Advertising Awards,
April 2007
A comprehensive, claims-based analysis of more than 600,000
patient episodes of depression (1 episode = 1 year)
highlighting direct costs and utilization of
resources across 5 domains of care:
� Inpatient care
� Outpatient care
� Ancillary care (labs, tests, procedures)
� Emergency department
� Pharmaceuticals
“Depression Benchmarks” and “TRU Benchmarks” are trademarks owned by Managed Care Measures, LLC. Depression BenchmarksTM
publication cover design, photograph, and color scheme (except for Total Resource
UtilizationTM
blue banner): © 2008, Wyeth Pharmaceuticals Inc., Philadelphia, PA 19101. Total Resource UtilizationTM
blue banner: © 1999-2008 Managed Care Measures, LLC. The remainder of this advertisement:
© 2008, Wyeth Pharmaceuticals Inc., Philadelphia, PA 19101. 223008-01
DepressionBenchmarksTM
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 35

36 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
AMCP MEETING HIGHLIGHTS
Anumber of new specialty products are in latestages of development, said Deborah B. Cooper,PharmD, Clinical Advisor, Pipeline Series,
CVS/Caremark, at the 2008 educational conference ofthe Academy of Managed Care Pharmacy. Specialtyproducts comprise 49% of new chemical compoundscurrently in phase 3 and 55% of the phase 3 ambulato-ry care agents. The 53 new specialty drugs slated forlaunch in 2008-2009 are for these categories (severalproducts are included in more than 1 category):• Oncology—17• Rare or orphan diseases—11• Metabolic diseases—8• Immunology—6• Infectious diseases—5• Neurologic disorders—5• Cardiovascular disorders—3• Respiratory disorders—3• Dermatology—2• Gastrointestinal disorders—2.
Key trends for the specialty pipeline include (1)increased numbers of drugs for rare/orphan diseases, (2)emergence of more drugs with Risk Evaluation andMitigation Strategy (REMS) programs, (3) expansionof adjunctive/additive agents for multiple disease states,and (4) a shift from injectable to oral therapies.
Rheumatoid Arthritis Toxilizumab (Actemra), an anti-interleukin-6
receptor monoclonal antibody, is pending approval forrheumatoid arthritis (RA) and is expected to belaunched with a REMS program. It is administeredintravenously every 4 weeks. Adverse events reportedinclude infections, hypersensitivity reactions, head -ache, nasopharyngitis, and pleurisy.
Golimumab is a humanized anti-tumor necrosis factor drug pending approval for RA, psoriatic arthritis,and ankylosing spondylitis. It is administered as a sub-cutaneous injection every 4 weeks. An intravenous(IV) formulation is in phase 2, to be administered every12 weeks. Adverse events included headache andinjection-site and allergic reactions.
Multiple Sclerosis Fampridine SR is a twice-daily oral agent in phase 3,
for the symptomatic treatment of multiple sclerosis(MS), to be used in conjunction with other MS drugs.
It blocks potassium channels on axons of nerves and in -creases walking speed and/or muscle strength. Adverseevents reported include falls, insomnia, paresthesias,dizziness, urinary tract infections, and nausea. Seizureshave been reported with high doses of the drug.
Fingolimod is a once-daily oral immunosuppressantin phase 3, which, if approved, will be the first oral dis-ease-modifying agent for MS. It causes a dose-relatedreduction in the number of circulating lymphocytes,leading to a decrease in the number of activated T-cellsin the blood and central nervous system. Adverseevents include headache and dose-dependent upperrespiratory tract infection.
Psoriasis Ustekinumab (Stelara) is a fully humanized mono-
clonal antibody that targets interleukin-12 and -23,which are thought to be proinflammatory cytokines.Approval is pending for chronic moderate-to-severe pso-riasis. The drug is administered subcutaneously every 12weeks. Adverse reactions include headache, infections,injection-site reactions, and respiratory tract infections.
SLE Epratuzumab, a monoclonal antibody that targets the
CD22 antigen on the surface of B cells, is in phase 3 forthe treatment of moderate-to-severe systemic lupus ery-thematosus (SLE). The CD22 receptor is implicated ininflammation. Epratuzumab is administered as an IV infu-sion every other week. Adverse reactions in clinical trialsinclude arthralgia, hypotension, nausea, and palpitations.
Belimumab (LymphoStat-B), also in phase 3 forSLE, is a fully human monoclonal antibody that inhibitsthe biologic activity of B-lymphocyte stimulator, whichat high levels may contribute to the pathogenesis ofautoimmune diseases (eg, SLE, RA). It is administeredintravenously every 28 days. It has shown a significantreduction in SLE flares and disease activity.
Hepatitis C Two drugs in phase 3 trials for hepatitis C virus (HCV)
show very promising results for those who failed therapywith pegylated interferon alfa and ribavirin: Zadaxin (thy-malfasin), an immunomodulator that stimulates T-cellsand decreases viral replication; telaprevir, the first pro-tease inhibitor for HCV, to be used with current therapies.Approval and launch are expected in 2009 or 2010. ■
Specialty Pipeline Dominated by BiologicsBy Alice Goodman
AMCP_36_37NovDec .qxp:Cover 11/24/08 4:37 PM Page 36

37www.AHDBonline.comVOL. 1 NO. 9
AMCP MEETING HIGHLIGHTS
Real-world data on a new therapy and a user-friendly assessment tool to evaluate real-worldstudies facilitate formulary and reimbursement
decisions, said Diana Brixner, PhD, RPh, Professor andChair, Department of Pharmacotherapy, and ExecutiveDirector, Pharmacy Outcomes Research Center,University of Utah, at the 2008 educational conferenceof the Academy of Managed Care Pharmacy.
Payers need information beyond randomized con-trolled trials (RCTs) to make the best decisions abouthow to deploy limited budgets for large patient popula-tions. RCTs are conducted in a select patient popula-tion, according to strict protocols, and the results arenot generalizable to large patient populations.Supplemental observational open-label trials and post-marketing surveillance provide data on the effect ofnew treatments that are more relevant for managedcare organizations (MCOs), such as quality-adjustedlife-years, productivity, and absenteeism.
Dr Brixner summarized the proceedings of 2 roundta-bles that addressed issues surrounding use of real-worlddata in managed care. A roundtable in July 2007 includ-ed 4 MCO directors and 4 economists. The panel tack-led the quality of real-world evidence, the complexity ofreal-world research, the lack of consistency in qualityassurance and assessment in decision-making, and thetime delay between accrual of real-world data and prod-uct launch. Recommendations for further study include: • Analysis of tools for quality assessment of observa-
tional studies• Development of a consolidated instrument to meas-
ures the quality assurance of these data• Establishment of a process to support application of
a comprehensive quality assessment tool• Development of training for producers and users of
observational studies on the consolidated tool.“Our healthcare system is fragmented. A consolidat-
ed tool would reduce the impact of fragmentation,” saidDr Brixner.
Developing a new tool for quality assurance to eval-uate real-world studies is a daunting task, and is stillongoing, Dr Brixner explained. In analyzing existingchecklists, participants found that none of them ful-filled the criteria for a simple-to-use, comprehensive
checklist to evaluate published real-world studies.Existing checklists were either too long or too academ-ic to support decision-making.
A second roundtable, held in March 2008, discussedhow to act on the recommendations of the first round-table. Participants agreed on the need: • For quality and convenience in assessment of real-
world data• To recognize that the process of implementation of a
new tool is as important as the new tool itself• For peer validation of a new tool• To educate all constituents about the tool and its
implementation.A small survey of 4 MCOs found that although none
of them currently uses a checklist to evaluate real-world studies, they would use a tool if it was short andconcise, validated, and recommended by a nationalorganization, Dr Brixner said. ■
Real-World Data Better than RCTs forFormulary DecisionsBy Alice Goodman
Unmanaged Moment
“On the other hand, where would we be if not for our overmedicated society?”
AMCP_36_37NovDec .qxp:Cover 11/24/08 4:37 PM Page 37

March 4-6, 2009 • Pointe Hilton Tapatio Cliffs Resort • Phoenix, Arizona
Attend PBMI’s 14th Annual Drug Benefit Conference
Visit www.pbmi.com/conference.asp for Detailed Agenda and Faculty.
Register Now!© 2008, Pharmacy Benefit Management Institute, LP All Rights Reserved
AMCP_36_37NovDec .qxp:Cover 11/24/08 4:37 PM Page 38

39www.AHDBonline.comVOL. 1 NO. 9
CLINICAL
Cardiovascular (CV) disease (CVD) is the lead-ing cause of mortality and one of the leadingcauses of disability worldwide.1 In the United
States alone, more than 80 million adults have at leastone type of CVD, with hypertension, coronary heartdisease (CHD), stroke, and heart failure among themost common forms of the disease. Elevated levels ofcholesterol (hypercholesterolemia) and abnormal lipidprofiles (dyslipidemia) are important risk factors forCVD. The American Heart Association (AHA) esti-mates that more than 100 million Americans have ele-vated cholesterol levels (>200 mg/dL) and 34 millionhave cholesterol levels that necessitate treatment.2
Cholesterol is an essential component of cell mem-branes and steroid hormones. The body synthesizesmost of its required cholesterol with the remaindercoming from the diet. Since cholesterol is mostly insoluble in blood, it is packaged with proteins andphospholipids to form lipoprotein complexes that cir-culate in the bloodstream. The types of cholesterol-containing lipoproteins are high-density lipoproteins(HDL-C), low-density lipoproteins (LDL-C), very low-density lipoproteins (VLDL-C), and chylomicrons.
High levels of LDL-C are associated with increasedCV risk in epidemiologic studies. In addition, numer-ous clinical studies using a variety of therapies havedemonstrated decreased CV events and mortality withLDL reduction. Therefore, the first goal of therapy is
reduction of LDL-C levels for the most common formsof dyslipidemia. Conversely, high levels of HDL-C areassociated with decreased risk of CV events. However,clinical trials assessing the morbidity and mortalitybenefits of drug therapies that raise HDL-C levels havehad varied results. HDL-C–modifying trials with niacinhave demonstrated CV event reduction.3,4 Conversely,other treatments that raise HDL-C, including hormonereplacement therapy5 and torcetrapib,6 have notdecreased CV events. Because of this, in the absence oflarge clinical outcome trials, therapies that elevate HDLcannot be assumed to produce clinical event reduction.
Approach to Patient Assessment, Treatment The National Cholesterol Education Program
(NCEP) evaluates evidence and develops guidelines forlipid management. The approach to patient manage-ment provided here comes primarily from the guide-lines published in 2001 and updated in 2004.7,8
Since the primary goal of lipid management is todecrease the risk of CV events and death, the first stepin management is to assess the patient’s overall CVrisk. To make this assessment, a fasting lipoproteinanalysis should be obtained to determine the patient’sLDL-C. Optimal levels for LDL-C and total cholesterolare <100 mg/dL and <200 mg/dL, respectively. TheNCEP guidelines recommend that a fasting lipid panel be drawn at least every 5 years in all adults older than 20 years.7
In addition to LDL-C levels, the presence orabsence of CHD or CHD-equivalent conditions mustbe assessed. CHD-equivalent conditions listed by theNCEP include diabetes mellitus, peripheral vasculardisease, abdominal aortic aneurysm, symptomaticcarotid disease, and a 10-year CV risk of less than 20%
Cardiovascular disease is the leading cause of death worldwide. Elevated cholesterol (hyper-cholesterolemia) and abnormal lipid profiles (dyslipidemia) are important risk factors for thedevelopment of cardiovascular disease. This article discusses the role of cholesterol in thebody and the relationship between different cholesterol fractions and the risk of cardiovas-cular disease. The guidelines for assessment and treatment of dyslipidemia from the NationalCholesterol Education Program are outlined, and cholesterol targets and goals of therapy arediscussed. The mechanism of action, place in therapy (eg, first-line, second-line, or add-on),and common side effects are also discussed for each of the available classes of drugs usedin the treatment of dyslipidemia. [ADHB. 2008;1(9):39-48.]
Dr Burns Schaiff is Senior Director, Regional Medical &Research Specialist, Pfizer, Inc, New York, NY; Dr Moe isClinical Associate Professor, University of Missouri-KansasCity, Kansas City, MO; Dr Krichbaum is Senior DirectorTeam Leader, Regional Medical & Research Specialist,Pfizer, Inc, New York, NY.
An Overview of Cholesterol ManagementRobyn A. Burns Schaiff, PharmD, BCPS; Richard M. Moe, MD, PhD; Daniel W. Krichbaum, PharmD
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:54 AM Page 39

40 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
CLINICAL
calculated with the Framingham risk calculator.7
Although not addressed by the NCEP, the NationalKidney Foundation also considers chronic kidney dis-ease (glomerular filtration rate <60 mL/min) to be ahigh-risk state and recommends that this patient groupbe treated as having a CHD-equivalent disease.9
Likewise, the AHA and the American StrokeAssociation recommend the use of a statin with inten-sive lipid-lowering effects in patients with atheroscle-rotic stroke or transient ischemic attack, even in theabsence of known CHD.10
In the absence of CHD or CHD-equivalent condi-tions, CVD risk factors (Table 1) should be carefullyassessed using the Framingham risk score to determinethe patient’s 10-year risk of CV events (Table 2).7
Goals of TherapyFor patients with CHD or CHD-equivalent disease,
the NCEP recommends the LDL-C goal of ≤100mg/dL, with <70 mg/dL a therapeutic option forpatients considered at very high risk for CV events.8
For patients with 2 or more CV risk factors but with a10-year Framingham risk of less than 20%, the LDL-Cgoal is <130 mg/dL, with <100 mg/dL a therapeuticoption. Finally, for patients with 0 to 1 risk factors, theLDL-C target is <160 mg/dL.8
Therapeutic Lifestyle ChangesThe NCEP Adult Treatment Panel III guidelines
recommend that therapeutic lifestyle changes beimplemented for all patients at risk for CVD.7 Thesechanges include reducing intake of saturated fats andcholesterol while increasing soluble fiber intake andphysical activity. Optimization of weight, moderationof alcohol consumption, and cessation of smoking arealso encouraged. If drug therapy is needed, it should beused as an addition to, rather than a substitute for, ther-apeutic lifestyle changes.
Treatment InitiationSince the clinical evidence of benefit is greatest
with the statin drug class, the American College ofCardiology (ACC) recommends drug therapy beginwith a statin and that titration to goal or the maximal-ly tolerated dose of a statin be achieved before consid-eration of adding other agents.11 Regardless of the ini-tial treatment chosen, it is critical that the patient bereevaluated and therapy titrated or added until the goalLDL-C is attained.
For patients with 0 to 1 risk factors and no CHD, treatment is initiated with therapeutic lifestyle changeswith reassessment after 6 weeks. If goal LDL of <160mg/dL is not reached at 6 weeks, lifestyle changesshould be intensified and reinforced and a visit with a dietitian considered. If after 12 weeks of therapeuticlifestyle changes the patient is not at the LDL-C goal of <160 mg/dL, drug therapy, usually a statin, should be added.
For patients at moderate risk, with 2 or more risk fac-tors and a 10-year CV risk of less than 20%, treatmentbegins with therapeutic lifestyle changes. Drug therapy,usually a statin, can be initiated concurrently if theLDL is >100 mg/dL at baseline or if LDL-C remains>100 mg/dL after a 6-week trial of lifestyle changes.
For the highest risk patients with CHD or equivalentconditions, statin therapy and therapeutic lifestylechanges should be initiated simultaneously for all
KEY POINTS▲ Cholesterol is an essential component of cell membranes
and steroid hormones. ▲ Hypercholesterolemia and dyslipidemia are important risk
factors for cardiovascular disease, which affects more than 80 million Americans.
▲ Evidence shows that high levels of LDL-C are associatedwith increased cardiovascular risk; reducing LDL levels hasbeen associated with significant reduction in mortality.
▲ The first goal of therapy in hypercholesterolemia is reduc-tion of LDL-C levels.
▲ Statins are considered the most effective lipid-loweringagents available, both in lowering LDL levels and in the prevention of cardiovascular events.
Table 1 Major Risk Factors (Exclusive of LDL-C) that Modify LDL Goals*
Cigarette smokingHypertension (blood pressure ≥140/90 mm Hg or on antihypertensive medication)Low HDL-C (<40 mg/dL)†
Family history of premature CHD (CHD in male first-degreerelative <55 y, CHD in female first-degree relative <55 y)Age (men ≥45 y; women ≥55 y)*Diabetes is regarded a CHD risk equivalent.†HDL cholesterol ≥60 mg/dL counts as a negative risk factor; its presenceremoves 1 risk factor from the total count.LDL-C indicates low-density lipoprotein cholesterol; HDL-C, high-densitylipoprotein cholesterol; CHD, coronary heart disease.Reprinted with permission from Expert Panel on Detection, Evaluation, andTreatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 40

41www.AHDBonline.comVOL. 1 NO. 9
Cholesterol Management
HDL indicates high-density lipoprotein; BP, blood pressure. Reprinted with permission from Expert Panel on Detection Evaluation and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.
Table 2 An Overview of Cholesterol Management
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 41

42 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
CLINICAL
patients with LDL-C >100 mg/dL. Drug therapy mayalso be considered in very high-risk patients with LDL-C <100 mg/dL targeted to achieve the optional goal of<70 mg/dL.8
Pharmacotherapy OptionsA variety of lipid-lowering agents are available,
including 3-hydroxy-3-methylglutaryl coenzyme A(HMG-CoA) reductase inhibitors, bile acid seques-trants, cholesterol absorption inhibitors, fibrates, nico-tinic acid derivatives, and omega-3 fatty acids. Dosageranges, US Food and Drug Administration (FDA) indi-cations, evidence of clinical outcome benefit, and sideeffects are highlighted in Table 3.
HMG-CoA Reductase Inhibitors (Statins)HMG-CoA reductase inhibitors, or statins, are the
recommended first-line therapy for most patients.These are the most prescribed drugs in the world andare considered the most effective lipid-lowering agentsavailable, both in lowering LDL-C levels and in theprevention of CV events. Statins are similar in struc-ture to HMG-CoA, a precursor of cholesterol, and actas competitive inhibitors of HMG-CoA reductase, thelast regulated enzymatic step in cholesterol synthesis.Therefore, statins reduce the rate of synthesis of choles-terol. The liver responds by increasing the number ofLDL receptors, which increases hepatic uptake andcatabolism of circulating LDL-C. Statins reduce LDL-Cby 24% to 60% and decrease triglycerides (TGs) by 5%to 50% (percentages are based on the various packageinserts), depending on the agent selected and the base-line lipid profile. HDL-C levels are usually increased.The effects on HDL are a class effect and are small rel-ative to the effects on LDL-C and TGs. In addition,statins have a variety of anti-inflammatory effects thatare independent of the LDL-C lowering, which maycontribute to the clinical benefit in CVD, especiallyearly in therapy.12 However, a recent meta-analysis of 23lipid-lowering trials demonstrated that the majority(89%-98%) of the anti-inflammatory effects of lipid-lowering therapy is related to the degree of LDL reduc-tion,13 which suggests a limited influence of a non-LDL-
C–related anti-inflammatory mechanism.Adverse events, relatively uncommon with this
class, include gastrointestinal (GI) disturbances, mus-cle aches, and asymptomatic transaminasemia. Rareserious adverse events may include myopathy and rhab-domyolysis. FDA-approved labeling recommendsassessment of liver function at baseline, after 12 weeksof therapy, after dose escalation, and twice yearly there-after. However, the National Lipid Association has sug-gested that this practice does not increase the safety ofstatin therapy, but merely increases cost.14
Bile Acid SequestrantsBile acid sequestrants bind to bile acids in the intes-
tine, reducing absorption of cholesterol and other lipids.The resultant decrease in available cholesterol causesan increase in the number of LDL receptors on hepato-cytes, further promoting clearance of LDL-C from theblood. Bile acid sequestrants are recommended as sec-ond-line therapy for patients with elevated cholesterol,but not elevated TGs, as both VLDL-C and TG con-centrations may increase during therapy. Agents in thisclass lower LDL-C by 15% to 30% and increase HDL-Cby 3% to 5% on average.9 Patient adherence with theseagents is frequently poor due to the need for frequentdosing, poor palatability, and frequent GI side effects.Since these drugs remain in the GI tract, systemicadverse effects are minimal; however, these agents caninterfere with absorption of concomitantly adminis-tered drugs as well as fat-soluble vitamins.
Nicotinic Acid DerivativesNiacin reduces synthesis of VLDL-C in the liver and
therefore reduces LDL-C production. Pharmacologicdoses of niacin (1.5-2 g/day) lower LDL-C and TGs by15% to 20% and 30% to 40%, respectively, andincrease HDL-C by 15% to 25%. Niacin is used as sec-ond-line therapy in concert with other lipid-loweringagents. The most common adverse events includevasodilation with flushing and pruritis, which frequent-ly is dose-limiting. Other adverse events include dys-pepsia, gastric ulceration, hyperuricemia, palpitations,and, rarely, peripheral neuropathy.
Niacin-induced hyperglycemia may be problematicfor patients with diabetes mellitus or with impaired glu-cose tolerance, particularly in the first 6 months oftherapy, but long-term clinical benefits have beendemonstrated in these patients.15 The most serious sideeffect is hepatotoxicity; cases of fatal fulminant hepat-ic failure have been associated with niacin administra-tion, particularly with older formulations.16
These are the most prescribed drugs in theworld and are considered the most effectivelipid-lowering agents available.
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 42

43www.AHDBonline.comVOL. 1 NO. 9
Tabl
e 3
Phar
mac
othe
rapy
for L
ipid
Dis
orde
rs
Con
tinue
d
Pop
ulat
ions
w/
Cos
t,de
mon
stra
ted
Pri
mar
y ef
fect
Side
eff
ects
30-d
ayD
rug
Dos
age
rang
eA
vaila
ble
dose
sIn
dica
tion
sev
ent
redu
ctio
n†on
lipi
ds(m
ost
ofte
n re
port
ed)
supp
ly
Que
stra
n*8-
24 g
/d,
Que
stra
n Li
ght:
pac
kets
•A
djuc
t the
rapy
of
Men
wit
h pr
imar
yLD
L-C
↓A
bdom
inal
dis
com
fort
,$$
$$(c
hole
styr
amin
e)2
divi
ded
and
pow
der (
each
5 g
hy
perc
hole
ster
olem
iahy
perc
hole
ster
olem
ia10
%-3
0%co
nsti
pati
on, f
latu
lenc
e,
dose
sco
ntai
n 4
g an
hydr
ous
•Pru
riti
s due
to p
arti
al b
iliar
y(L
RC
-CT
TP1 )
naus
ea a
nd v
omit
ing,
ch
oles
tyra
min
e re
sin)
obst
ruct
ion
vita
min
A, D
def
icie
ncy
Que
stra
n: p
owde
r and
pa
cket
s (ea
ch 9
gco
ntai
n 4
g an
hydr
ous
chol
esty
ram
ine
resin
)
Wel
chol
3.
75 g
/d62
5-m
g ta
blet
s•A
djuc
t the
rapy
of h
yper
chol
este
role
mia
LDL-
C↓
Ast
heni
a, c
onst
ipat
ion,
$$$$
(col
esev
elam
)•A
djun
ct th
erap
y to
impr
ove
10%
-18%
indi
gest
ion,
pha
ryng
itis
,gl
ycem
ic c
ontr
ol in
type
2 D
Mm
yalg
ia
Col
esti
d*2-
16 g
/d1-
g ta
blet
sA
djun
ct th
erap
y fo
r pri
mar
yLD
L-C
↓A
bdom
inal
dis
tens
ion,
ab-
$$$
(col
esti
pol)
2 di
vide
d hy
perc
hole
ster
olem
ia10
%-2
0%do
min
al p
ain,
con
stip
atio
n,do
ses
mus
culo
skel
etal
pai
n, h
eada
che
Zeti
a10
mg/
d10
-mg
tabl
ets
•Pri
mar
y hy
perl
ipid
emia
LDL-
C↓
Hea
dach
e, d
iarr
hea,
$$
$(e
zeti
mib
e)•M
ixed
dys
lipid
emia
10%
-20%
abdo
min
al p
ain,
art
hral
gia,
•H
omoz
ygou
s fam
ilial
hyp
erch
oles
tero
lem
iaba
ckac
he, m
yalg
ia, s
inus
itis
•Hom
ozyg
ous s
itos
tero
lem
ia
Ant
ara*
43-1
30 m
g/d
43-,
130-
mg
caps
ules
•Hyp
ertr
igly
ceri
dem
iaT
G↓
Ras
h, d
iarr
hea,
flat
ulen
ce,
$$(f
enof
ibra
te)
•Pri
mar
y hy
perg
lyce
ride
mia
20%
-50%
naus
ea a
nd v
omit
ing,
•Mix
ed d
yslip
idem
iam
yalg
ia, r
hini
tis
Lipo
fen*
(fen
ofib
rate
)50
-150
mg/
d50
-, 15
0-m
g ca
psul
es
Lofib
ra*
(fen
ofib
rate
)54
-200
mg/
d54
-, 16
0-m
g ta
blet
s67
-,134
-, 20
0-m
g ca
psul
es
TriC
or*
(fen
ofib
rate
)48
-145
mg/
d48
-, 14
5-m
g ta
blet
s
Trig
lide
(fen
ofib
rate
)50
-160
mg/
d50
-, 16
0-m
g ta
blet
s
Lopi
d*(g
emfib
rozi
l)60
0-12
00 m
g/d,
600-
mg
tabl
ets
•Red
ucin
g C
HD
risk
in p
atie
nts w
/type
2b
•Men
w/p
rim
ary
TG
↓R
ash,
abd
omin
al p
ain,
$2
divi
ded
dose
sdy
slip
idem
ia a
nd in
adeq
uate
resp
onse
tody
slip
idem
ia (
Hel
sink
i25
%-4
5%di
arrh
ea, f
latu
lenc
e,
TLC
, oth
er d
rug
ther
apy,
who
hav
eH
eart
Stu
dy2 )
indi
gest
ion,
xer
osto
mia
, hi
gh L
DL,
low
HD
L, h
igh
TG
•Men
w/C
HD
and
low
mya
lgia
•Fam
ilial
type
IV o
r V h
yper
lipid
emia
HD
L-C
(V
A H
it3 )
Lipi
tor
10-8
0 m
g/d
10-,
20-,
40-,
80-m
g•P
rim
ary
prev
enti
on o
f MI,
stro
ke in
•Pat
ient
s w/h
yper
tens
ion
and
LDL-
C↓
Abd
omin
al p
ain,
$$
$(a
torv
asta
tin)
tabl
ets
pati
ents
w/t
ype
2 D
M a
nd o
ther
CH
D≥3
CH
D ri
sk fa
ctor
s (A
SCO
T4 )
39%
-60%
cons
tipa
tion
,ri
sk fa
ctor
s•P
atie
nts w
/typ
e 2
DM
and
no
flatu
lenc
e, in
dige
stio
n,•P
rim
ary
prev
enti
on o
f MI,
stro
ke,
hist
ory
of C
VD
(C
AR
DS5 )
incr
ease
d liv
er e
nzym
es,
reva
scul
ariz
atio
n, h
ospi
taliz
atio
n fo
r •P
atie
nts w
/stab
le C
HD
(T
NT,
6he
adac
he, m
yalg
iahe
art f
ailu
re a
nd a
ngin
a in
pat
ient
s ID
EAL,
7 A
LLIA
NC
E,8
and
w/c
linic
ally
evi
dent
CA
Dan
d A
VER
T9 )
•Pri
mar
y hy
perc
hole
ster
olem
ia o
r •P
atie
nts w
/ath
eros
cler
otic
mix
ed d
yslip
idem
ia
stro
ke o
r TIA
w/o
doc
umen
ted
•Hyp
ertr
igly
ceri
dem
iaC
HD
(SP
AR
CL10
) •P
rim
ary
dysb
etal
ipop
rote
inem
ia•P
atie
nts w
/AC
S (P
RO
VE-
IT,11
•Hom
ozyg
ous F
H in
ado
lesc
ents
MIR
AC
L12)
•Het
eroz
ygou
s FH
in a
dole
scen
ts
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 43

44 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
Tabl
e 3
Phar
mac
othe
rapy
for L
ipid
Dis
orde
rs C
ontin
ued
Pop
ulat
ions
w/
Side
eff
ects
Cos
t,de
mon
stra
ted
Pri
mar
y ef
fect
(mos
t of
ten
30-d
ayD
rug
Dos
age
rang
eA
vaila
ble
dose
sIn
dica
tion
sev
ent
redu
ctio
n†on
lipi
dsre
port
ed)
supp
ly
Lesc
ol (
fluva
stat
in)
20-8
0 m
g/d
20-,
40-m
g•R
educ
e co
rona
ry re
vasc
ular
izatio
n in
CH
DPa
tien
ts w
ith
CH
D w
ho h
adLD
L-C
↓A
bdom
inal
pai
n, d
iarr
hea,
$$$
caps
ules
•Red
uce
prog
ress
ion
of c
oron
ary
coro
nary
inte
rven
tion
(LI
PS13
)20
%-3
5%dy
spep
sia,
nau
sea,
hea
dach
e,at
hero
scle
rosi
s in
CH
Dm
yalg
ia•H
yper
chol
este
role
mia
•Het
eroz
ygou
s FH
in a
dole
scen
ts
Lesc
ol X
L80
-mg
mg/
d80
-mg
exte
nded
- $$
$$(f
luva
stat
in E
R)
rele
ase
tabl
ets
Mev
acor
*10
-80
mg/
d10
-, 20
-, 40
-mg
•Pri
mar
y pr
even
tion
of M
I, un
stab
le
Hig
h ri
sk (
elev
ated
LD
L-C
LDL-
C↓
Abd
omin
al p
ain,
con
stip
atio
n,$$
(lov
asta
tin)
tabl
ets
angi
na, c
oron
ary
reva
scul
ariz
atio
nw
/low
HD
L-C
) pa
tien
ts w
/o25
%-4
5%di
arrh
ea, n
ause
a, h
eada
che,
•To
slow
pro
gres
sion
of c
oron
ary
clin
ical
CH
D
mya
lgia
, inc
reas
ed h
epat
icat
hero
scle
rosi
s in
CH
D(A
FCA
PS-T
exC
aps14
)tr
ansa
min
ase
leve
ls•H
yper
chol
este
role
mia
•Het
eroz
ygou
s FH
in a
dole
scen
ts
Prav
acho
l*10
-80
mg/
d10
-, 20
-, 40
-, 80
-mg
•Pri
mar
y pr
even
tion
of M
I, re
vasc
ular
i-•M
en w
/o h
isto
ry o
f MI
LDL-
C↓
Dia
rrhe
a, fl
atul
ence
, hea
rt-
$$(p
rava
stat
in)
tabl
ets
zati
on, a
nd C
V m
orta
lity
w/e
leva
ted
LDL
(WO
SCO
PS15
)25
%-4
0%bu
rn, n
ause
a, v
omit
ing,
•R
educ
tion
in to
tal m
orta
lity
by•P
atie
nts w
/MI i
n pr
eced
ing
asth
enia
, hea
dach
e, m
yalg
iare
duci
ng c
oron
ary
deat
h, M
I, 3-
20 m
o (C
AR
E16)
reva
scul
ariz
atio
n, st
roke
, and
to sl
ow•P
atie
nts w
/MI o
r uns
tabl
e pr
ogre
ssio
n of
cor
onar
y at
hero
scle
rosi
s in
angi
na in
pre
viou
s 3-3
6 m
opa
tien
ts w
ith
CH
D(L
IPID
17)
•Hyp
erch
oles
tero
lem
ia•H
eter
ozyg
ous F
H in
ado
lesc
ents
Cre
stor
5-40
mg/
d5-
, 10-
, 20-
, 40-
mg
•Pri
mar
y hy
perl
ipid
emia
Men
≥55
and
wom
en ≥
65LD
L-C
↓A
bdom
inal
pai
n, c
onst
ipat
ion,
$$$$
(ros
uvas
tati
n)ta
blet
san
d m
ixed
dys
lipid
emia
w/L
DL
≤130
mg/
dL a
nd C
RP
45%
-60%
naus
ea, a
rthr
algi
a, a
sthe
nia,
•Pri
mar
y hy
pert
rigl
ycer
idem
ia≥2
mg/
L (J
UPI
TER
18)
head
ache
, mya
lgia
, inc
reas
ed
•Hom
ozyg
ous f
amili
al h
yper
chol
este
role
mia
hepa
tic
tran
sam
inas
e le
vels
•To
slow
the
prog
ress
ion
of a
ther
oscl
eros
is
Zoco
r*5-
80 m
g/d
5-, 1
0-, 2
0- 4
0-, 8
0-m
g•P
reve
ntio
n of
CH
D m
orta
lity
and
•Exi
stin
g C
HD
and
ele
vate
dLD
L-C
↓C
onst
ipat
ion,
GI
$$(s
imva
stat
in)
tabl
ets
CV
eve
nts i
n pa
tien
ts w
/exi
stin
g C
HD
,to
tal c
hole
ster
ol (
4S19
)35
%-5
0%ir
rita
tion
, hea
dach
e,hi
stor
y of
stro
ke, d
iabe
tes,
or p
erip
hera
l•P
atie
nts a
t hig
h ri
sk o
f CV
uppe
r res
pira
tory
ar
tery
dis
ease
even
ts fr
om e
xist
ing
CH
D,
infe
ctio
n, m
yalg
ia,
•Hyp
erch
oles
tero
lem
iahi
stor
y of
stro
ke, o
ther
cer
ebro
-in
crea
sed
hepa
tic
•Het
eroz
ygou
s FH
in a
dole
scen
tsva
scul
ar d
isea
se, p
erip
hera
ltr
ansa
min
ase
leve
lsar
tery
dis
ease
, or h
yper
tens
ion
in m
en ≥
65 y
r (H
PS20
)
Slo-
Nia
cin
CR
*0.
5-2
g/d
Nia
cin
CR
: 250
-, 50
0-,
•Pri
mar
y hy
perc
hole
ster
olem
ia o
r mix
edM
en w
/his
tory
of M
I (C
DP21
;LD
L↓C
onst
ipat
ion,
flus
hing
, $$
(con
trol
led-
rele
ase
750-
mg
tabl
ets
dysl
ipid
emia
(al
one
or w
ith
lova
stat
in)
imm
edia
te-r
elea
se d
osag
e fo
rm)
5%-1
5%pr
urit
is, G
I irr
itat
ion,
ni
acin
)•S
ever
e hy
pert
rigl
ycer
idem
iaT
G↓
naus
ea, v
omit
ing
•To
redu
ce ri
sk o
f rec
urre
nt M
I in
patie
nts
15%
-30%
w/h
yper
chol
este
role
mia
and
his
tory
of M
IH
DL↑
$$$$
$N
iasp
an0.
5-2
g/d
Nia
cin
ER: 5
00-,
750-
,•W
/bile
aci
d–bi
ndin
g re
sin
to sl
ow15
%-2
0%(n
iaci
n ER
)10
00-m
g ta
blet
spr
ogre
ssio
n or
indu
ce re
gres
sion
of c
oron
ary
athe
rosc
lero
sis in
pat
ient
s w/C
AD
and
hype
rcho
lest
erol
emia
•W
/bile
aci
d–bi
ndin
g re
sin:
pri
mar
y hy
perc
hole
ster
olem
iaIm
med
iate
-rel
ease
0.
25-6
g/d
, 350
0-m
g ta
blet
s$
niac
in*
divi
ded
dose
s
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 44

45www.AHDBonline.comVOL. 1 NO. 9
Pop
ulat
ions
w/
Cos
t,de
mon
stra
ted
Pri
mar
y ef
fect
Side
eff
ects
30-d
ayD
rug
Dos
age
rang
eA
vaila
ble
dose
sIn
dica
tion
sev
ent
redu
ctio
n†on
lipi
ds(m
ost
ofte
n re
port
ed)
supp
ly
Om
ega-
3 fa
tty
acid
*2-
4 g/
dV
ario
usH
yper
trig
lyce
ride
mia
(T
G ≥
500
mg/
dL)
•Hyp
erch
oles
tero
lem
ic Ja
pane
seT
G↓
Incr
ease
d bl
eedi
ng/b
ruis
ing,
$$(L
ovaz
a)pa
tient
s (ov
er st
atin
bac
kgro
und
25%
-45%
burp
ing,
indi
gest
ion,
ther
apy)
(JE
LIS22
) al
tere
d ta
ste
sens
e•P
atie
nts w
/rece
nt M
I (G
ISSI
-Pre
venz
ione
23)
Adv
icor
Nia
cin-
ERN
iaci
n-ER
–•H
yper
chol
este
role
mia
LDL↓
30%
-45%
See
unde
r$$
$$(n
iaci
n-ER
/50
0 m
g–lo
vasta
tinlo
vast
atin
•Mix
ed d
yslip
idem
iaH
DL↑
20%
-30%
com
pone
nts
lova
stat
in)
20 m
g/d to
niac
in-E
R50
0 m
g-20
mg
TG
↓ 3
0%-4
5%20
00 m
g–lo
vast
atin
750
mg-
20 m
g40
mg/
d10
00 m
g-20
mg
Sim
cor
Nia
cin-
ERN
iaci
n-ER
–•H
yper
chol
este
role
mia
LDL↓
10%
-15%
$$
$(n
iaci
n-ER
/50
0 m
g–si
mva
stat
in•M
ixed
dys
lipid
emia
HD
L↑ 2
0%-3
0%si
mva
stat
in)
sim
vast
atin
500
mg-
20 m
g•H
yper
trig
lyce
ride
mia
TG
↓15
%-4
0%20
mg/
d to
750
mg-
20 m
g(a
ll w
hen
mon
othe
rapy
(from
bas
eline
niac
in-E
R10
00 m
g-20
mg
inad
equa
te)
trea
tmen
t w/
2000
mg–
sim
vast
atin
sim
vast
atin
0-
20 m
g/d)
40 m
g/d
Vyt
orin
Ezet
imib
e 10
mg–
Ezet
imib
e–•P
rim
ary
hype
rlip
idem
iaLD
L↓$$
$$(e
zete
mib
e/si
mva
stat
insi
mva
stat
inor
mix
ed h
yper
lipid
emia
45%
-60%
sim
vast
atin
)10
mg/
d to
10 m
g-10
mg
•Hom
ozyg
ous F
Hez
etim
ibe
10 m
g–10
mg-
20 m
gsi
mva
stat
in10
mg-
40 m
g80
mg/
d10
mg-
80 m
g
*Gen
eric
ava
ilabl
e. †
Stud
ies l
iste
d in
this
col
umn
may
not
be
incl
uded
in F
DA
-app
rove
d in
dica
tion
s.LD
L-C
indi
cate
s low
-den
sity
lipop
rote
in c
hole
ster
ol; D
M, d
iabe
tes m
ellit
us; T
G, t
rigly
cerid
es; C
HD
, cor
onar
y he
art d
iseas
e; T
LC, t
hera
peut
ic li
fest
yle
chan
ges;
HD
L-C
, hig
h-de
nsity
lipo
prot
ein
chol
este
rol;
MI,
myo
card
ial i
nfar
ctio
n; C
AD
,co
rona
ry a
rter
y di
seas
e; F
H, f
amili
al h
yper
chol
este
role
mia
; CV
D, c
ardi
ovas
cula
r dise
ase;
TIA
, tra
nsie
nt is
chem
ic a
ttac
k; A
CS,
acu
te c
oron
ary
synd
rom
e; C
V, c
ardi
ovas
cula
r; G
I, ga
stro
inte
stin
al; C
R, c
ontr
olle
d re
leas
e; E
R, e
xten
ded
rele
ase.
1.Li
pid
Res
earc
h C
linic
s Pro
gram
: the
lipi
d re
sear
ch c
linic
s cor
onar
y pr
imar
y pr
even
tion
tria
l res
ults
. I. R
educ
tion
in in
cide
nce
of c
oron
ary
hear
t dis
ease
. JA
MA
. 198
4;25
1:35
1-36
4.2.
Hel
sink
i Hea
rt S
tudy
. Pri
mar
y pr
even
tion
tria
l wit
h ge
mfib
rozi
l in
mid
dle-
aged
men
wit
h dy
slip
idem
ia. N
Eng
l J M
ed. 1
987;
317:
1237
-124
5.3.
Rub
ins H
B, R
obin
s SJ,
Col
lins D
, et a
l. G
emfib
rozi
l for
the
seco
ndar
y pr
even
tion
of c
oron
ary
hear
t dis
ease
in m
en w
ith
low
leve
ls o
f hig
h-de
nsit
y lip
opro
tein
cho
lest
erol
. N E
ngl J
Med
.19
99;3
41:4
10-4
18.
4.Se
ver P
S, D
ahlö
f B, P
oulte
r NR
, et a
l. Pr
even
tion
of c
oron
ary
and
stro
keev
ents
wit
h at
orva
stat
in in
hyp
erte
nsiv
e pa
tien
ts w
ho h
ave
aver
age
or lo
wer
-tha
n-av
erag
e ch
oles
tero
l con
cent
rati
ons,
in th
e A
nglo
-Sca
n din
avia
n C
ardi
acO
utco
mes
Tri
al-L
ipid
Low
erin
g A
rm (
ASC
OT-
LLA
): a
mul
tice
ntre
rand
omis
ed c
ontr
olle
d tr
ial.
Lanc
et.
2003
;361
:114
9-11
58.
5.C
olho
un H
M, B
ette
ridg
e D
J, D
urri
ngto
n PN
, et a
l. Pr
imar
y pr
even
tion
of c
ardi
ovas
cula
r dis
ease
wit
h at
orva
stat
in in
type
2 d
iabe
tes i
n th
e C
olla
bora
tive
Ato
rvas
tati
n D
iabe
tes S
tudy
(C
AR
DS)
: mul
tice
ntre
rand
omis
ed p
lace
bo-
cont
rolle
d tr
ial.
Lanc
et. 2
004;
364:
685-
696.
6.La
Ros
a JC
, Gru
ndy
SM, W
ater
s DD
, et a
l. In
tens
ive
lipid
low
erin
g w
ith
ator
vast
atin
in p
atie
nts w
ith
stab
le c
oron
ary
dise
ase.
N E
ngl J
Med
. 200
5;35
2:14
25-1
435.
7.Pe
derse
n T
R, F
aerg
eman
O, K
aste
lein
JJ, e
t al.
Hig
h-do
se a
torv
asta
tin v
s usu
al-d
ose
simva
statin
for s
econ
dary
pre
vent
ion
afte
r myo
card
ial i
nfar
ctio
n: th
e ID
EAL
study
: a ra
ndom
ized
cont
rolle
d tri
al. J
AM
A. 2
005;
294:
2437
-244
5.8.
Kor
en M
J, H
unni
ngha
ke D
B; A
LLIA
NC
E In
vest
igat
ors.
Clin
ical
out
com
es in
man
aged
-car
e pa
tien
ts w
ith
coro
nary
hea
rt d
isea
se tr
eate
d ag
gres
sive
ly in
lipi
d-lo
wer
ing
dise
ase
man
agem
ent c
linic
s: th
e A
LLIA
NC
E st
udy.
J A
m C
oll
Car
diol
. 200
4;44
:177
2-17
79.
9.Pi
tt B
, Wat
ers D
, Bro
wn
WV,
et a
l. A
ggre
ssiv
e lip
id-l
ower
ing
ther
apy
com
pare
d w
ith
angi
opla
sty
in st
able
cor
onar
y ar
tery
dis
ease
. N E
ngl J
Med
. 199
9;34
1:70
-76.
10.S
chw
artz
GG
, Olss
on A
G, E
zeko
witz
MD
, et a
l. Ef
fect
s of a
torv
asta
tin o
n ea
rly re
curr
ent i
sche
mic
eve
nts i
n ac
ute
coro
nary
synd
rom
es: t
he M
IRA
CL
stud
y: a
rand
omize
d co
ntro
lled
tria
l. JA
MA
. 200
1;28
5:17
11-1
718.
11.C
anno
n C
P, B
raun
wal
d E,
McC
abe
CH
, et a
l. In
tens
ive
vers
us m
oder
ate
lipid
low
erin
g w
ith
stat
ins a
fter
acu
te c
oron
ary
synd
rom
es. N
Eng
l J M
ed. 2
004;
350:
1495
-150
4.12
.Am
aren
co P
, Bog
ouss
lavs
ky J,
Cal
laha
n A
3rd
, et a
l. H
igh-
dose
ato
rvas
tati
n af
ter s
trok
e or
tran
sien
t isc
hem
ic a
ttac
k. N
Eng
l J M
ed. 2
006;
355:
549-
559.
13.S
erru
ys P
W, D
e Fe
yter
PJ,
Ben
ghoz
i R, e
t al.
The
Les
col(
R)
Inte
rven
tion
Pre
vent
ion
Stud
y (L
IPS)
: a d
oubl
e-bl
ind,
pla
cebo
-con
trol
led,
rand
omiz
ed tr
ial o
f the
long
-ter
m e
ffect
s of f
luva
stat
in a
fter
succ
essf
ul tr
ansc
athe
ter t
hera
py in
pati
ents
wit
h co
rona
ry h
eart
dis
ease
. Int
J C
ardi
ovas
c In
terv
ent.
2001
;4:1
65-1
72.
14.D
owns
JR, C
lear
field
M, W
eis S
, et a
l. Pr
imar
y pr
even
tion
of a
cute
cor
onar
y ev
ents
wit
h lo
vast
atin
in m
en a
nd w
omen
wit
h av
erag
e ch
oles
tero
l lev
els:
resu
lts o
f AFC
APS
/Tex
CA
PS. A
ir F
orce
/Tex
as C
oron
ary
Ath
eros
cler
osis
Prev
enti
on S
tudy
. JA
MA
. 199
8;27
9:16
15-1
622.
15.S
heph
erd
J, C
obbe
SM
, For
d I,
et a
l. Pr
even
tion
of c
oron
ary
hear
t dis
ease
wit
h pr
avas
tati
n in
men
wit
h hy
perc
hole
ster
olem
ia. W
est o
f Sco
tlan
d C
oron
ary
Prev
enti
on S
tudy
Gro
up. N
Eng
l J M
ed. 1
995;
333:
1301
-130
7.16
.Sac
ks F
M, P
feffe
r MA
, Moy
e LA
, et a
l. T
he e
ffect
of p
rava
stat
in o
n co
rona
ry e
vent
s afte
r myo
card
ial i
nfar
ctio
n in
pat
ient
s with
ave
rage
cho
lest
erol
leve
ls. C
hole
ster
ol a
nd R
ecur
rent
Eve
nts T
rial i
nves
tigat
ors.
N E
ngl J
Med
. 199
6;33
5:10
01-1
009.
17.T
he L
ong-
Term
Inte
rven
tion
wit
h Pr
avas
tati
n in
Isch
aem
ic D
isea
se (
LIPI
D)
Stud
y G
roup
. Pre
vent
ion
of c
ardi
ovas
cula
r eve
nts a
nd d
eath
wit
h pr
avas
tati
n in
pat
ient
s wit
h co
rona
ry h
eart
dis
ease
and
a b
road
rang
e of
init
ial
chol
este
rol l
evel
s. N
Eng
l J M
ed. 1
998;
339:
1349
-135
7.18
.Rid
ker P
M, D
anie
lson
MIA
, Fon
seca
AH
, et a
l, fo
r the
JUPI
TER
Stu
dy G
roup
. Ros
uvas
tatin
to p
reve
nt v
ascu
lar e
vent
s in
men
and
wom
en w
ith e
leva
ted
C-r
eact
ive
prot
ein.
N E
ngl J
Med
. 200
8;35
9:21
95-2
207.
19.T
he S
cand
inav
ian
Sim
vast
atin
Sur
viva
l Stu
dy G
roup
. Ran
dom
ised
tria
l of c
hole
ster
ol lo
wer
ing
in 4
444
pati
ents
wit
h co
rona
ry h
eart
dis
ease
: the
Sca
ndin
avia
n Si
mva
stat
in S
urvi
val S
tudy
(4S
). L
ance
t. 19
94;3
44:1
383-
1389
.20
.Hea
rt P
rote
ctio
n St
udy
Col
labo
rativ
e G
roup
. MR
C/B
HF
Hea
rt P
rote
ctio
n St
udy
of c
hole
ster
ol lo
wer
ing
with
sim
vast
atin
in 2
0,53
6 hi
gh-r
isk in
divi
dual
s: a
rand
omise
d pl
aceb
o-co
ntro
lled
tria
l. La
ncet
. 200
2;36
0:7-
22.
21.C
anne
r PL,
Ber
ge K
G, W
enge
r NK
, et a
l. Fi
ftee
n ye
ar m
orta
lity
in C
oron
ary
Dru
g Pr
ojec
t pat
ient
s: lo
ng-t
erm
ben
efit
wit
h ni
acin
. J A
m C
oll C
ardi
ol. 1
986;
8:12
45-1
255.
22Yo
koya
ma
M, O
riga
sa H
, Mat
suza
ki M
, et a
l. Ef
fect
s of e
icos
apen
taen
oic
acid
on
maj
or c
oron
ary
even
ts in
hyp
erch
oles
tero
laem
ic p
atie
nts (
JELI
S): a
rand
omiz
ed, o
pen-
labe
l, bl
inde
d en
dpoi
nt a
naly
sis.
Lanc
et. 2
007;
369:
1090
-109
8.23
.Mar
chio
li R
, Sch
wei
ger C
, Tav
azzi
L, V
alag
ussa
F. E
ffica
cy o
f n-3
pol
yuns
atur
ated
fatt
y ac
ids a
fter
myo
card
ial i
nfar
ctio
n: re
sult
s of G
ISSI
-Pre
venz
ione
tria
l. G
rupp
o It
alia
no p
er lo
Stu
dio
della
Sop
ravv
iven
za n
ell’I
nfar
to M
ioca
rdic
o.Li
pids
. 200
1;36
(sup
pl):
S119
-S12
6.C
ost:
$ 0-
25, $
$ 26
-50,
$$$
51-
100,
$$$
$ 10
1-20
0, $
$$$$
>20
0 So
urce
s: C
linic
al d
ata
com
pile
d fr
om M
icro
med
ex w
ebsi
te. h
ttp:
//ww
w.th
omso
nhc.
com
. Acc
esse
d A
ugus
t 22,
200
8. C
ost i
nfor
mat
ion
from
ww
w.dr
ugst
ore.
com
. Acc
esse
d A
ugus
t 22,
200
8.
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 45

46 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
CLINICAL
FibratesFibric acid derivatives, or fibrates, such as gemfi-
brozil and fenofibrate, are agonists of the peroxisome-activated receptor-α in muscle, liver, and other tissues.Fibrates can lower TG levels by up to 50% and are therefore considered the first-line agents in patients with hypertriglyceridemia (TG >400 mg/dL).However, LDL-C reduction is variable (10%-15%),with some patients exhibiting increased levels of LDL-C. HDL-C levels may be increased up to 25% in patients with very high TG levels at baseline.17 Themost common adverse events are rash and dyspepsia for fenofibrate and GI disturbances for gemfibrozil. All fibrates may increase the risk of gallstones. In addi-tion, gemfibrozil has been shown to increase plasmaconcentration of statins, thereby increasing the risk ofmuscle toxicity.18
EzetimibeAs with bile acid sequestrants, ezetimibe inhibits the
absorption of cholesterol. However, since it does notinterfere with the absorption of other dietary fats, it isbetter tolerated. Ezetimibe localizes at the brush borderof the small intestine, where it binds to a critical medi-ator of cholesterol absorption, the Niemann-Pick C1-like 1 protein on the GI tract epithelial cells19 and livercells. Like the bile acid sequestrants, by reducing theavailability of LDL-C, ezetimibe also induces LDLreceptor upregulation leading to increased uptake ofLDL-C into cells, further lowering circulating LDL-Clevels. While ezetimibe effectively lowers LDL-C, stud-ies assessing clinical event reduction are lacking. In arecent study, no additional decrease in the carotid inti-ma-media thickness was demonstrated with ezetimibe-simvastatin combination therapy compared with sim-vastatin alone, despite significantly greater reductionin LDL-C in the combination group.20
In addition, in another study, an increased risk ofcancer death was observed in the simvastatin-ezetimibegroup compared with the placebo group,21 but an analy-sis of more than 20,000 patients in ongoing randomizedtrials revealed no increase in cancer risk in patientsreceiving ezetimibe compared with placebo.22 However,given the lack of documented outcome benefit withthis agent, the ACC recommends that it be reservedfor patients who cannot reach LDL-C goal with maxi-mal dose statins.11
Omega-3 Fatty AcidsEpidemiologic studies have demonstrated that peo-
ple who have diets rich in omega-3 fatty acids have a
lower risk of CV events compared with those with atypical Western diet. Studies of omega-3 fatty acidadministration have demonstrated reductions in TGsof up to 45% in patients with baseline TG levels >500mg/dL.23 Smaller reductions are expected in patientswith lower baseline levels. In addition to the reductionin TGs, HDL-C levels may be increased by as much as9%. The addition of omega-3 fatty acids to statin ther-apy produces further reductions in VLDL-C and TGsand further elevations in HDL-C. The putative mech-anisms for TG reduction with high-dose omega-3 fatsinclude increased beta oxidation. ■
ConclusionElevated cholesterol level is a major risk factor for
CVD, the leading cause of death worldwide. Reductionof LDL-C has been shown to decrease the risk of CVevents in a large number of clinical trials. Because theyare the best studied, have a favorable risk/benefit pro-file, and have been demonstrated to produce clinicalbenefits in many large trials, statins are the first-linetreatment for patients with hypercholesterolemia.
Disclosure StatementDr Moe is on the Speakers’ Bureau for Pfizer, BMS, Novartis,
Abbott, and GlaxoSmithKline. Drs Burns Schaiff and Krichbaum areemployees of Pfizer, Inc. Limited editorial support was provided byPaul Lane, PhD, at Envision Pharma, Ltd, and was funded byPfizer, Inc.
References1. Mensah GA, Brown DW. An overview of cardiovascular disease bur-den in the United States. Health Aff (Millwood). 2007;26:38-48.2. Rosamond W, Flegal K, Furie K, et al. Heart disease and stroke statis-tics—2008 update: a report from the American Heart AssociationStatistics Committee and Stroke Statistics Subcommittee. Circulation.2008;117:e25-146.3. The Lipid Research Clinics Coronary Primary Prevention TrialResults. I. Reduction in incidence of coronary heart disease. JAMA.1984;251:351-364.4. Brown G, Albers JJ, Fisher LD, et al. Regression of coronary artery dis-ease as a result of intensive lipid-lowering therapy in men with high lev-els of apolipoprotein B. N Engl J Med. 1990;323:1289-1298.5. Manson JE, Hsia J, Johnson KC, et al. Estrogen plus progestin and therisk of coronary heart disease. N Engl J Med. 2003;349:523-534.6. Barter PJ, Caulfield M, Eriksson M, et al. Effects of torcetrapib in pa -tients at high risk for coronary events. N Engl J Med. 2007;357:2109-2122.7. Expert Panel on Detection, Evaluation, and Treatment of High BloodCholesterol in Adults. Executive Summary of the Third Report of theNational Cholesterol Education Program (NCEP) Expert Panel onDetection, Evaluation, and Treatment of High Blood Cholesterol inAdults (Adult Treatment Panel III). JAMA. 2001;285:2486-2497.8. Grundy SM, Cleeman JI, Bailey Merz CN, et al. Implications ofrecent clinical trials for the National Cholesterol Education ProgramAdult Treatment Panel III guidelines. Circulation. 2004;110:227-239.9. National Kidney Foundation. K/DOQI Clinical practice guidelinesfor managing dyslipidemias in chronic kidney disease. Part 3: treatingdyslipidemias. Am J Kidney Dis. 2003;41(4 suppl 3):S39-S58.
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 46

47www.AHDBonline.comVOL. 1 NO. 9
Cholesterol Management
10. Adams RJ, Albers G, Alberts MJ, et al. Update to the AHA/ASArecommendations for the prevention of stroke in patients with strokeand transient ischemic attack. Stroke. 2008;39:1647-1652.11. American College of Cardiology. ACC Statement on ENHANCETrial. January 15, 2008. http://www.acc.org/enhance_statement.htm.Accessed October 10, 2008.12. Libby P. Current concepts of the pathogenesis of atherosclerosis.Circulation. 2001;104:365-372.13. Kinlay S. Low density lipoprotein-dependent and independenteffects of cholesterol lowering therapies on C-reactive protein: a meta-analysis. J Am Coll Cardiol. 2007;49:2003-2009.14. Cohen DE, Anania FA, Chalasani N; National Lipid AssociationStatin Safety Task Force Liver Expert Panel. An assessment of statinsafety by hepatologists. Am J Cardiol. 2006;97(8A):77C-81C.15. Canner PL, Furberg CD, Terrin ML, McGovern ME. Benefits ofniacin by glycemic status in patients with healed myocardial infarction(from the Coronary Drug Project). Am J Cardiol. 2005;95:254-257.16. Ferenchick G, Rovner D. Hepatitis and hematemesis complicatingnicotinic acid use. Am J Med Sci. 1989;298:191-193.
17. Guay DR. Micronized fenofibrate: a new fibric acid hypolipidemicagent. Ann Pharmacother. 1999;33:1083-1103.18. Noé J, Portmann R, Brun ME, Funk C. Substrate-dependent drug-drug interactions between gemfibrozil, fluvastatin and other organicanion-transporting peptide (OATP) substrates on OATP1B1,OATP2B1, and OATP1B3. Drug Metab Dispos. 2007;35:1308-1314.19. Garcia-Calvo M, Lisnock J, Bull HG, et al. The target of ezetimibeis Niemann-Pick C1-Like 1 (NPC1L1). Proc Natl Acad Sci. 2005;102:8132-8137.20. Kastelein JP, Akdim F, Stroes ES, et al. Simvastatin with or without eze-timibe in familial hypercholesterolemia. N Engl J Med. 2008;358: 1431-1443.21. Rossebo AB, Pedersen TR, Boman K, et al. Intensive lipid loweringwith simvastatin and ezetimibe in aortic stenosis. N Engl J Med. 2008;359:1343-1356.22. Peto R, Emberson J, Landray M, et al. Analysis of cancer data fromthree ezetimibe trials. N Engl J Med. 2008;359:1357-1366.23. Kris-Etherton PM, Harris WS, Appel LJ; American HeartAssociation. Nutrition Committee. Fish consumption, fish oil, omega-3fatty acids, and cardiovascular disease. Circulation. 2002;106:2747-2757.
Stakeholder PerspectivesExperts Debate Meaning of JUPITER for Clinical Practice
PHYSICIANS/PAYERS: Should the indications forstatins be expanded? This was the question that hadmany cardiovascular (CV) experts talking, but withlittle consensus, in light of the findings from theJUPITER (Justification for the Use of Statins inPrimary Prevention: An Intervention Trial EvaluatingRosuvastatin) study released in November 2008 at theAmerican Heart Association annual meeting andthen published in the New England Journal ofMedicine.1 The results have also created a buzz amongP & T Committee members: Should they change planbenefits for statins? Will physicians begin to prescribethe drugs to a new patient population even off-label?
JUPITER showed that apparently healthy indi-viduals with unremarkable levels of low-densitylipoprotein cholesterol (LDL-C) but with elevatedlevels of high-sensitivity C-reactive protein (hs-CRP)—2.0 mg/L or more—had a dramatic reduc-tion in the risk for CV events by taking rosuvastatin(Crestor) compared with placebo.
The large benefit of rosuvastatin—a 44% relativereduction in CV risk—surpassed the expectations ofthe lead investigator, Paul Ridker, MD, Director ofthe Center for Cardiovascular Disease Prevention atBrigham and Women’s Hospital, who has champi-oned the use of hs-CRP to estimate CV risk for quitesome time. “Getting CRP down appears to haveincremental benefit to lowering LDL cholesterol,”Dr Ridker said. “There was a large number in our
study who had an elevation of CRP without otherrisk factors, and this group had a benefit from rosu-vastatin as well.” Of those who fit the profile of thestudy population, 25 patients would need to be treat-ed to prevent 1 CV event, which is “smaller than weanticipated,” said Dr Ridker.
Steve Nissen, MD, Chairman of the Departmentof Cardiovascular Medicine at the Cleveland Clinic,is a believer in CRP testing and is already using it toguide treatment decisions. He noted that the reduc-tion in death and major CV events with rosuvastatinwas larger than in any other trial of a statin, and hewas impressed that it occurred after only an averageof 1.9 years of treatment (the study had beenplanned to last 5 years but was terminated earlybecause of the large benefit found).
According to Dr Nissen, applying the findingsfrom JUPITER to the US population could add 10million persons who could benefit from statins.
Critics point out that although the magnitude ofthe 44% relative reduction in risk was large, theabsolute risk reduction was rather small—only 0.9%(1.8% in the placebo group had an event comparedwith 0.9% in the rosuvastatin group). Of note, sub-jects enrolled in the trial were at low risk at baseline,and this low risk accounted for the small reductionin absolute risk. Only 157 of 8901 subjects takingplacebo had an event compared with 83 of 8901 ran-domized to rosuvastatin.
Continued
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 47

48 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
CLINICAL
Cholesterol Management: The Complexity of Multiple Effectives Treatments
PAYERS: High levels of serum cholesterol havelong been recognized as a significant risk factor forthe development and progression of atherosclerosis.Lowering cholesterol has been shown to effectivelyreduce mortality and morbidity associated with acutecoronary syndromes and stroke—2 of the top 3 caus-es of death in the United States. As our understand-ing of the role of cholesterol has evolved, we havecome to realize the individual effects that low-densi-ty lipoprotein (LDL) and high-density lipoproteincan have in risk assessment and modification.
As the authors of this article highlight, a largenumber of effective treatments are available. Theavailability of multiple agents adds to the complexi-ty of their use: Are all these agents equal in theirability to affect lipid levels? Are they equal in theirability to influence outcomes? For an individualpatient with a specific set of risk factors and a specif-ic lipid profile, which agents will best affect theirlipid panel and their overall risk of cardiovascular orcerebrovascular complications?
The availability of several effective treatmentsalso raises questions about thresholds for screeningand treatment. A number of organizations have pro-vided such guidance, including the American HeartAssociation, the National Cholesterol EducationProgram, the United States Preventive Services TaskForce (USPSTF), and the American Academy ofPediatrics. As is often the case for the clinicianattempting to determine the best recommendationfor a given patient, or for the patient attempting toparticipate in decision-making—the rapid develop-ment of new science and research and the conflict-ing guidance of expert panel recommendations cancompound the confusion. For example, the USPSTFcurrently recommends screening of patients olderthan 20 years, citing insufficient evidence for screen-ing younger populations. Meanwhile, a recommen-
dation issued in 2008 by the American Academy ofPediatrics is much more aggressive with regard toscreening, and even treatment, of children with cer-tain risk factors.1
This complexity is further increased with the pub-licity related to the early termination of theJUPITER trial (see previous page), which was pub-lished in November 2008.2 In JUPITER, patientswithout a history of cardiovascular disease, with LDLlevels <130 mg/dL but with high-sensitivity C-reac-tive protein levels of 2.0 mg/L or more, were ran-domized to receive rosuvastatin or placebo. The trialwas ended early because patients in the treatmentgroup showed very significant reductions in myocar-dial infarction, stroke, arterial revascularization, hos-pitalization for unstable angina, or death from car-diovascular causes. This study will raise questionsregarding the thresholds that must be met to initiatetherapy. It will also raise issues concerning the rela-tive effectiveness of various agents, depending ontheir ability to affect “inflammation” as a separaterisk factor for atherosclerosis.
Until the evidence becomes clearer, we mustempower clinicians facing these decisions with asmany options as possible. They must be able to per-sonalize therapy—the best agent for the individualpatient—without undue restrictions.
1. Daniels SR, Greer FR; Committee on Nutrition. Lipid screeningand cardiovascular health in childhood. Pediatrics. 2008;122:198-208.
2. Ridker PM, Danielson E, Fonseca FAH, et al, for the JUPITERStudy Group. Rosuvastatin to prevent vascular events in men andwomen with elevated C-reactive protein. N Engl J Med. 2008;359:2195-2207.
Thomas McCarter, MD, FACPChief Clinical OfficerExecutive Health Resources
Using Crestor to prevent 1 death in persons withelevated CRP levels has been estimated at $500,000,a cost that may be too high. Some suggest that pre-scribing Crestor to reduce CRP could add $8.9 bil-lion to the cost of treatment in this country. But thiscost would be reduced to about $25,000 to prevent 1death, using a generic statin, if generic statins are aseffective as the brand drug at reducing CRP levels.
Evidence indicates that all the statins reduce CRP,but to different degrees.
1. Ridker PM, Danielson E, Fonseca FAH, et al, for the JUPITER StudyGroup. Rosuvastatin to prevent vascular events in men and womenwith elevated C-reactive protein. N Engl J Med. 2008;359:2195-2207.
Wayne KuznarMedical Writer
Continued
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 48

49www.AHDBonline.comVOL. 1 NO. 9
MEDICAL TOURISM
Whether Americans are flocking overseas formedical care remains a question. One esti-mate put the number at 150,000 in 2006,1
jumping to 750,000 in 2007.2 Nevertheless, the popularpress continues to devote articles to this phenomenonthat may very well be creating the market.
The LureThe lure of medical tourism for patients is the ability
to obtain services for relatively cheap cost, which canhelp uninsured and underinsured Americans gain accessto care; allow richer patients to get services quicker; orenable private health plans to arrange “bargain care”elsewhere for their insured patients. This has fostered athriving industry in some countries, and the lay presshas found such outsourcing a source for attractive sto-ries—“recovering from a medical procedure while lyingon a palm-swept beach, relaxing by the hotel pool, orshopping for terrific bargains sounds good.”3
Just a few years ago, medical tourism was depicted ascare associated with an exotic vacation or with anattendant spa recovery postsurgery. Yet escalating med-ical costs began to make the travel portion seem rea-sonable for those who were denied access at home.Travel sections of newspapers featured pleased unin-sured working and poorer patients who received amuch-needed operation at a mere fraction of the UScost. Major publications (eg, New York Times, LosAngeles Times), generally in states bordering the PacificRim and Latin America, published stories accompaniedby advertisements for touring agencies, and thus beganthe fledgling middleman industry that generated atten-tion to medicine overseas.
The Los Angeles Times ran articles first examiningmedical tourism, later denoting its growth, and thenmarking it as a trend. Articles appeared in Arkansas,Tennessee, Washington, and other states removed fromthe nonstop airplane routes, as the public graduallybecame acquainted with travel for healthcare. Fox,CNN, and CBS’s “60 Minutes” ran segments on people
traveling for services. Forbes and the Wall Street Journalfocused on the business aspects of the phenomenon, asmiddlemen aggressively marketed it to consumers,employers, and insurers.
“Hot destinations” came into the spotlight—Singapore, India, Thailand, Mexico, Costa Rica, China,and more. And the base broadened. Europeans optingout of their national health systems, along with wealthyclientele from the Middle East and other regions, wereidentified as medical tourists. The Internet further facil-itated clever marketing campaigns by private providersseeking to service the burgeoning international market.
Cheaper care for dental services, cosmetic interven-tions, and specialty pharmacy began to be proffered in travel packages to lure patients to providers who arranged “customer care” in luxurious hotels, tout-ing huge savings for “quality care.” Inroads into “bargain surgery” in modern facilities with advancedequipment were made. Lower-cost facelifts, hormonetherapy, and the like now appeal to “aging cohorts” inthe developed world.
Many of the private hospitals across Asia haveEnglish-speaking and American-trained staff, who nowcan deliver organ and bone marrow transplants, ortho-pedic, oncology, cardiovascular, and more hi-tech andcomplex care. In 2007, Forbes’s article “Open-HeartSurgery—90% off!” highlighted the differences in costand quality of care between the United States andother countries.4
Thus, the media caught the fancy of comparativecosts as a way to promote access to affordable health-care for Americans, including small businesses. TheFinancial Times and San Francisco Chronicle covered the2008 Deloitte study, which found that almost 40% ofAmericans would travel abroad for care, provided thatquality appeared comparable with that in the UnitedStates.5 People with private insurance were more likelyto consider traveling.
In the medical literature, a discussion amongst pay-ers and providers has begun concerning medicaltourism. A 2006 New England Journal of Medicine arti-cle warned that “American physicians who are con-cerned about the growth of this phenomenon have two
Dr Salmon is Professor of Health Policy and Administration,School of Public Health, University of Illinois at Chicago, IL.
Promotion of Medical Tourism in theMedia Creates a TrendJ. Warren Salmon, PhD
MedTourismNovDec .qxp:Cover 11/25/08 11:16 AM Page 49

50 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
MEDICAL TOURISM
choices: they can denounce and attempt to restrict it,or they can lead and more actively support efforts byothers to speed the discovery and uptake of more effi-cient domestic healthcare delivery methods.”6
Policy Concerns Doubts about patient care quality abroad and poten-
tial safety issues emerged in the popular press before theprofessional literature. Can quality be assured? Whatabout complications when returning home? Will fol-low-up care at home be available? What is the legalrecourse in nations without malpractice laws or “a cul-ture” of suing doctors? A series of cautions is clearlyneeded for an unregulated medical tourism industry.
As the hubs for foreign care are investigated, assur-ances on such concerns are hard to come by. The US-based Joint Commission International accredits morethan 140 hospitals overseas, with a doubling of thatnumber projected in 2 years. But this is by no means acomplete safeguard to a botched surgery. Locationanalyses of provider destinations are necessary, alongwith specific reviews of providers, the host of entrepre-neurial middlemen making travel arrangements, andeven the motives and diligence of new US insurers andemployers who are looking for potential savings fromsending their insured members overseas.
AlterNet raises a concern that medical tourism maypose competition to the US healthcare system: “Theproblem with turning to medical tourism as an answerto healthcare problems goes beyond personal storiesand into the realm of hard policy. There are lots ofstakeholders that are eager to trump up medical tourismas a silver bullet for healthcare costs….[Some suggestthat ] since insurers and employers can pay less to coverprocedures, the US healthcare system will benefitgreatly from medical tourism.”7
It will be interesting to see how US payers respondto all this. And how the US government and others
react to this emerging phenomenon will be critical.Tourism is a trade that is under World TradeOrganization consideration. Siphoning off the wealthyto posh concierge care in private health systems over-seas and leaving a subpar public sector for the poorermasses pose ethical dilemmas. At a time of rising glob-al epidemics, for developing nations to neglect regula-tory directions to preserve and protect their publichealth is a concern.8
The lay press’ attention to medical tourism hashelped to create a new market, spurring entrepreneur-ial enterprises stateside to facilitate it, as well as settingup a host of private providers overseas to capitalize onthis nascent trend. This phenomenon has also pro-voked issues that force us to reflect on the impact ofglobalization at home and abroad. ■
References1. AMA press release. AMA provides first ever guidance on medicaltourism. June 16, 2008. http://www.ama-assn.org/ama/pub/category/18678.html. Accessed November 3, 2008.2. Madden CL. Medical tourism causes complications. October 27,2008. http://www.policyinnovations.org/ideas/briefings/data/000083.Accessed November 3, 2008.3. Kaderli B, Kaderli A. Medical vacations: the retiree health-care solution? MotleyFool.com. August 12, 2008. http://www.fool.com/personal-finance/retirement/2008/08/12/medical-vacations-the-retiree-health-care-solution. aspx. Accessed November 3, 2008.4. Forbes S. Open-heart surgery—90% off! Forbes. August 13, 2007.http://www.forbes.com/columnists/forbes/2007/0813/021.html. AccessedNovember 3, 2008.5. Deloitte. Medical tourism: consumers in search of value, 2008.http://www.deloitte.com/dtt/cda/doc/content/us_chs_MedicalTourismStudy(1).pdf. Accessed November 3, 2008.6. Milstein A, Smith M. America’s new refugees—seeking affordablesurgery offshore. N Engl J Med. 2006;355:1637-1640.7. Mahar M. Medical tourism is great—for those who can afford it.AlterNet. August 21, 2008. http://www.alternet.org/healthwellness/95827/medical_tourism_is_great_—_for_those_who_can_afford_it/.Accessed November 3, 2008.8. Salmon JW, Aruru M. Health tourism to India: challenges againstresource competition to sustaining a viable public health infrastructure forthe local populace. Presented at the Annual Expo and Meeting of theAmerican Public Health Association; San Diego, CA; October 27, 2008.
Signature (Required) ____________________________________ Date (Required) _________
Name ______________________________________________________________
Title ________________________________________________________________
Company ________________________________ Specialty ______________________
Address_____________________________________________________________
City/State/ZIP_________________________________________________________
E-mail _____________________________________ Phone ____________
FREE Subscription Request
Fax to (732) 992-1881
Request your FREE subscription to AMERICAN HEALTH & DRUG BENEFITS®
AHDB 11/08Incomplete cards will not be processed.
❑ YES! I would like to receive American Health & Drug Benefits ® as well as related educational supplements FREE!
❑ NO. Please discontinue my subscription.
MedTourismNovDec .qxp:Cover 11/25/08 11:16 AM Page 50

1 in 4 adults suffer from a diagnosable mental disorder
in any given year.1 Open access is especially important in the treatment of mental disorders because the response to therapy can vary greatly from individual to individual and from one medication to the next. Restrictions in the form of prior authorizations and preferred lists may have the unintended consequences of jeopardizing patient health while failing to reduce costs.
Open Access. Because different people
have different needs.Bristol-Myers Squibb supports open and unrestricted access to mental health medications. For people with mental illness, having access to newer and potentially more effective medications can be a crucial component of treatment.
N O T E V E R Y O N E I S C U T O U T F O R T H E S A M E T R E A T M E N T .
SUPPORT OPEN ACCESS AND GIVE PROVIDERS THE FREEDOM TO FIND THE MOST APPROPRIATE MEDICATION FOR EACH INDIVIDUAL.
1. National Institute of Mental Health. Available at: http://www.nimh.nih.gov/healthinformation/statisticsmenu.cfm. Accessed August 7, 2006.
D6-K0178DD October 2006 AA444681/10-06
D6K0178DD_8.125x10.875.indd 1 7/2/08 4:20:32 PM
Exec Sum_NovDecqxp.qxp:Cover 11/24/08 4:50 PM Page 51

VOL. 1 NO. 9
EXECUTIVE SUMMARIES
52 AMERICAN HEALTH & DRUG BENEFITS November/December 2008
Cardiovascular disease (CVD) remains the leadingcause of death worldwide. Hypercholesterolemia anddyslipidemia are significant risk factors for the develop-ment of CVD, which affects more than 80 millionAmericans. A team of 3 experts discusses the relation-ship between cholesterol levels and the risk of CVD,outlining the National Cholesterol Education Programguidelines for assessment and treatment of dyslipidemia,and summarizing current cholesterol targets. The firstgoal of therapy in hypercholesterolemia is reduction oflow-density lipoprotein (LDL) cholesterol levels.Evidence shows that statins are the most effective lipid-lowering agents available. Drs Schaiff, Moe, and
Krichbaum provide an extensive drug table that coversall lipid-lowering classes, their mechanisms of action,place in therapy, side effects, as well as costs. Finally,new evidence from the recently published JUPITERstudy has shown that in addition to lowering lipid lev-els, statins are important for preventing vascular eventsin patients with elevated C-reactive protein (CRP) lev-els, even in those with normal cholesterol levels. Adebate is currently raging among experts and decisionmakers whether persons with normal lipid levels butwith elevated CRP levels should be taking a statin on aregular basis. These results may have implications for allhealth benefit programs.
An Overview of Cholesterol ManagementBy Robyn A. Burns Schaiff, PharmD, BCPS; Richard M. Moe, MD, PhD; Daniel W. Krichbaum, PharmD
In this second interview, Dr Silver, director of theCancer Center Network at the Division ofHematology/Oncology at the University of MichiganHealth Systems, focuses on the impact of Medicare cov-erage decision for erythropoiesis-stimulating agents(ESAs), and why ESAs are so important for patients. Heemphasizes the risk of transfusions to cancer patientsand why policy decisions that restrict the use of ESAscan have profound implications for patients. Dr Silver,who is also Assistant Dean for Research at theUniversity of Michigan, calls for new studies, to be fund-ed by the manufacturers of the 2 major ESAs, to inves-
tigate the concerns for tumor progression and throm-boembolic events that are potentially associated withthese expensive medications. Such research could betterguide policy decisions by Medicare and improve patientcare. Despite the very high cost of the ESAs, the issue oftransfusions in cancer patients is beyond economics, DrSilver says, since they expose patients to unnecessaryrisks. And although Medicare is not supposed to consid-er costs in its decisions, cost is an underlying context forcoverage decisions, especially for as expensive medica-tions as ESAs, which nevertheless may reduce hospital-ization for transfusions, he says.
Erythropoiesis-Stimulating Agents in a Meta-Stable StateInterview (Part 2) with Samuel M. Silver, MD, PhD
Medication nonadherence is a major cause of mor-bidity and mortality in the United States. Non -adherence to drug therapy is also a major contributor toescalating costs of healthcare. Lack of information andforgetfulness are 2 main reasons cited by patients forlack of adherence. These 2 causes can be positivelyinfluenced by improved patient–provider communica-tion, Dr Ross explains. With chronic diseases estimatedto involve hundreds of millions of patients, the scale ofdisease management enrollment is too great to be cost-effective using traditional outreach methods. The chal-lenge is to scale outreach programs efficiently, without
losing the personal touch necessary to help changebehavior. Using communication automation to aug-ment traditional call center outreach can help to medi-ate patient medication-taking behaviors. Dr Rossreports results of his new study that involved an auto-mated telephony to 304 elderly patients with hyperten-sion. Using this automated system helped reduce costsand improve the blood pressure monitoring of patients.In addition to significant improvements in outcomes,174 patients had their antihypertensive regimen alteredbased on their responses to the survey part of the auto-mated system.
Role for Automated Communication Strategies in MedicationAdherence ManagementBy S. Michael Ross, MD, MHA
Exec Sum_NovDecqxp.qxp:Cover 11/24/08 4:50 PM Page 52

Brief Summary of Prescribing Information
USE IN PREGNANCYWhen used in pregnancy during the second and third trimesters, drugs that act directly on therenin-angiotensin system can cause injury and even death to the developing fetus. When pregnancy is detected, MICARDIS® tablets should be discontinued as soon as possible.See WARNINGS: Fetal/Neonatal Morbidity and Mortality
INDICATIONSMICARDIS is indicated for the treatment of hypertension. It may be used alone or in combination with otherantihypertensive agents.
CONTRAINDICATIONSMICARDIS (telmisartan) is contraindicated in patients who are hypersensitive to any component of this product.
WARNINGSFetal/Neonatal Morbidity and Mortality Drugs that act directly on the renin-angiotensin system can causefetal and neonatal morbidity and death when administered to pregnant women. Several dozen cases have beenreported in the world literature in patients who were taking angiotensin converting enzyme inhibitors. Whenpregnancy is detected, MICARDIS (telmisartan) tablets should be discontinued as soon as possible. The use ofdrugs that act directly on the renin-angiotensin system during the second and third trimesters of pregnancyhas been associated with fetal and neonatal injury, including hypotension, neonatal skull hypoplasia, anuria,reversible or irreversible renal failure, and death. Oligohydramnios has also been reported, presumablyresulting from decreased fetal renal function; oligohydramnios in this setting has been associated with fetallimb contractures, craniofacial deformation, and hypoplastic lung development. Prematurity, intrauterinegrowth retardation, and patent ductus arteriosus have also been reported, although it is not clear whetherthese occurrences were due to exposure to the drug. These adverse effects do not appear to have resultedfrom intrauterine drug exposure that has been limited to the first trimester. Mothers whose embryos andfetuses are exposed to an angiotensin II receptor antagonist only during the first trimester should be soinformed. Nonetheless, when patients become pregnant, physicians should have the patient discontinue theuse of MICARDIS tablets as soon as possible. Rarely (probably less often than once in every thousandpregnancies), no alternative to an angiotensin II receptor antagonist will be found. In these rare cases, the mothersshould be apprised of the potential hazards to their fetuses, and serial ultrasound examinations should beperformed to assess the intra-amniotic environment. If oligohydramnios is observed, MICARDIS tablets shouldbe discontinued unless they are considered life-saving for the mother. Contraction stress testing (CST), anon-stress test (NST), or biophysical profiling (BPP) may be appropriate, depending upon the week ofpregnancy. Patients and physicians should be aware, however, that oligohydramnios may not appear untilafter the fetus has sustained irreversible injury. Infants with histories of in utero exposure to an angiotensinII receptor antagonist should be closely observed for hypotension, oliguria, and hyperkalemia. If oliguriaoccurs, attention should be directed toward support of blood pressure and renal perfusion. Exchangetransfusion or dialysis may be required as a means of reversing hypotension and/or substituting fordisordered renal function. There is no clinical experience with the use of MICARDIS tablets in pregnantwomen. No teratogenic effects were observed when telmisartan was administered to pregnant rats at oraldoses of up to 50 mg/kg/day and to pregnant rabbits at oral doses up to 45 mg/kg/day. In rabbits,embryolethality associated with maternal toxicity (reduced body weight gain and food consumption) wasobserved at 45 mg/kg/day [about 12 times the maximum recommended human dose (MRHD) of 80 mg on amg/m2 basis]. In rats, maternally toxic (reduction in body weight gain and food consumption) telmisartandoses of 15 mg/kg/day (about 1.9 times the MRHD on a mg/m2 basis), administered during late gestation andlactation, were observed to produce adverse effects in neonates, including reduced viability, low birth weight,delayed maturation, and decreased weight gain. Telmisartan has been shown to be present in rat fetusesduring late gestation and in rat milk. The no observed effect doses for developmental toxicity in rats andrabbits, 5 and 15 mg/kg/day, respectively, are about 0.64 and 3.7 times, on a mg/m2 basis, the maximumrecommended human dose of telmisartan (80 mg/day). Hypotension in Volume-Depleted Patients Inpatients with an activated renin-angiotensin system, such as volume- and/or salt-depleted patients (e.g., those being treated with high doses of diuretics), symptomatic hypotension may occur after initiation oftherapy with MICARDIS® tablets. This condition should be corrected prior to administration of MICARDIS tablets,or treatment should start under close medical supervision with a reduced dose. If hypotension does occur, thepatient should be placed in the supine position and, if necessary, given an intravenous infusion of normalsaline. A transient hypotensive response is not a contraindication to further treatment, which usually can becontinued without difficulty once the blood pressure has stabilized.PRECAUTIONSGeneral. Impaired Hepatic Function: As the majority of telmisartan is eliminated by biliary excretion, patientswith biliary obstructive disorders or hepatic insufficiency can be expected to have reduced clearance. MICARDIS(telmisartan) tablets should be used with caution in these patients. Impaired Renal Function: As a consequenceof inhibiting the renin-angiotensin-aldosterone system, changes in renal function may be anticipated insusceptible individuals. In patients whose renal function may depend on the activity of the renin-angiotensin-aldosterone system (e.g., patients with severe congestive heart failure), treatment with angiotensin-converting enzyme inhibitors and angiotensin receptor antagonists has been associated with oliguria and/orprogressive azotemia and (rarely) with acute renal failure and/or death. Similar results may be anticipatedin patients treated with MICARDIS tablets. In studies of ACE inhibitors in patients with unilateral or bilateralrenal artery stenosis, increases in serum creatinine or blood urea nitrogen were observed. There has beenno long term use of MICARDIS tablets in patients with unilateral or bilateral renal artery stenosis but an effectsimilar to that seen with ACE inhibitors should be anticipated. Information for Patients. Pregnancy: Femalepatients of childbearing age should be told about the consequences of second- and third-trimester exposureto drugs that act on the renin-angiotensin system, and they should also be told that these consequences donot appear to have resulted from intrauterine drug exposure that has been limited to the first trimester. Thesepatients should be asked to report pregnancies to their physicians as soon as possible. Drug Interactions.Digoxin: When telmisartan was coadministered with digoxin, median increases in digoxin peak plasmaconcentration (49%) and in trough concentration (20%) were observed. It is, therefore, recommended thatdigoxin levels be monitored when initiating, adjusting, and discontinuing telmisartan to avoid possible over-or under-digitalization. Warfarin: Telmisartan administered for 10 days slightly decreased the mean warfarintrough plasma concentration; this decrease did not result in a change in International Normalized Ratio (INR).Other Drugs: Coadministration of telmisartan did not result in a clinically significant interaction withacetaminophen, amlodipine, glibenclamide, simvastatin, hydrochlorothiazide or ibuprofen. Telmisartan is notmetabolized by the cytochrome P450 system and had no effects in vitro on cytochrome P450 enzymes,except for some inhibition of CYP2C19. Telmisartan is not expected to interact with drugs that inhibitcytochrome P450 enzymes; it is also not expected to interact with drugs metabolized by cytochrome P450enzymes, except for possible inhibition of the metabolism of drugs metabolized by CYP2C19.Carcinogenesis, Mutagenesis, Impairment of Fertility There was no evidence of carcinogenicity whentelmisartan was administered in the diet to mice and rats for up to 2 years. The highest doses administered tomice (1000 mg/kg/day) and rats (100 mg/kg/day) are, on a mg/m2 basis, about 59 and 13 times, respectively,the maximum recommended human dose (MRHD) of telmisartan. These same doses have been shown toprovide average systemic exposures to telmisartan >100 times and >25 times, respectively, the systemicexposure in humans receiving the MRHD (80 mg/day). Genotoxicity assays did not reveal any telmisartan-related effects at either the gene or chromosome level. These assays included bacterial mutagenicity testswith Salmonella and E. coli (Ames), a gene mutation test with Chinese hamster V79 cells, a cytogenetic testwith human lymphocytes, and a mouse micronucleus test. No drug-related effects on the reproductiveperformance of male and female rats were noted at 100 mg/kg/day (the highest dose administered), about 13times, on a mg/m2 basis, the MRHD of telmisartan. This dose in the rat resulted in an average systemic exposure(telmisartan AUC as determined on day 6 of pregnancy) at least 50 times the average systemic exposure inhumans at the MRHD (80 mg/day). Pregnancy Pregnancy Categories C (first trimester) and D (second andthird trimesters). See WARNINGS, Fetal/Neonatal Morbidity and Mortality. Nursing Mothers It is notknown whether telmisartan is excreted in human milk, but telmisartan was shown to be present in the milk oflactating rats. Because of the potential for adverse effects on the nursing infant, a decision should be made whetherto discontinue nursing or discontinue the drug, taking into account the importance of the drug to the mother.Pediatric Use Safety and effectiveness in pediatric patients have not been established. Geriatric Use Of thetotal number of patients receiving MICARDIS in clinical studies, 551 (18.6%) were 65 to 74 years of age and 130(4.4%) were 75 years or older. No overall differences in effectiveness and safety were observed in these patientscompared to younger patients and other reported clinical experience has not identified differences in responsesbetween the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
ADVERSE REACTIONSMICARDIS (telmisartan) has been evaluated for safety in more than 3700 patients, including 1900 treated for
over six months and more than 1300 for over one year. Adverse experiences have generally been mild andtransient in nature and have only infrequently required discontinuation of therapy. In placebo-controlled trialsinvolving 1041 patients treated with various doses of telmisartan (20-160mg) monotherapy for up to 12 weeks,an overall incidence of adverse events similar to that of placebo was observed. Adverse events occurring at anincidence of 1% or more in patients treated with telmisartan and at a greater rate than in patients treated withplacebo, irrespective of their causal association, are presented as follows: The most common adverse eventsoccurring with MICARDIS Tablets monotherapy at a rate of ≥1% and greater than placebo, respectively, were:upper respiratory tract infection (URTI) (7%, 6%), back pain (3%, 1%), sinusitis (3%, 2%), diarrhea (3%, 2%), andpharyngitis (1%, 0%). In addition to the adverse events, the following events occurred at a rate of 1% but wereat least as frequent in the placebo group: influenza-like symptoms, dyspepsia, myalgia, urinary tract infection,abdominal pain, headache, dizziness, pain, fatigue, coughing, hypertension, chest pain, nausea and peripheraledema. Discontinuation of therapy due to adverse events was required in 2.8% of 1455 patients treated withMICARDIS tablets and 6.1% of 380 placebo patients in placebo-controlled clinical trials. The incidence of adverseevents was not dose-related and did not correlate with gender, age, or race of patients. The incidence of coughoccurring with telmisartan in six placebo-controlled trials was identical to that noted for placebo-treatedpatients (1.6%). In addition to those listed above, adverse events that occurred in more than 0.3% of 3500patients treated with MICARDIS monotherapy in controlled or open trials are listed below. It cannot bedetermined whether these events were causally related to MICARDIS tablets: Autonomic Nervous System:impotence, increased sweating, flushing; Body as a Whole: allergy, fever, leg pain, malaise; Cardiovascular:palpitation, dependent edema, angina pectoris, tachycardia, leg edema, abnormal ECG; CNS: insomnia,somnolence, migraine, vertigo, paresthesia, involuntary muscle contractions, hypoaesthesia; Gastrointestinal:flatulence, constipation, gastritis, vomiting, dry mouth, hemorrhoids, gastroenteritis, enteritis, gastroesophageal reflux,toothache, non-specific gastrointestinal disorders; Metabolic: gout, hypercholesterolemia, diabetes mellitus;Musculoskeletal: arthritis, arthralgia, leg cramps; Psychiatric: anxiety, depression, nervousness; ResistanceMechanism: infection, fungal infection, abscess, otitis media; Respiratory: asthma, bronchitis, rhinitis, dyspnea,epistaxis; Skin: dermatitis, rash, eczema, pruritus; Urinary: micturition frequency, cystitis; Vascular:cerebrovascular disorder; and Special Senses: abnormal vision, conjunctivitis, tinnitus, earache. During initialclinical studies, a single case of angioedema was reported (among a total of 3781 patients treated withtelmisartan). Clinical Laboratory Findings In placebo-controlled clinical trials, clinically relevant changes instandard laboratory test parameters were rarely associated with administration of MICARDIS tablets.Hemoglobin: A greater than 2 g/dL decrease in hemoglobin was observed in 0.8% telmisartan patientscompared with 0.3% placebo patients. No patients discontinued therapy due to anemia. Creatinine: A 0.5 mg/dLrise or greater in creatinine was observed in 0.4% telmisartan patients compared with 0.3% placebopatients. One telmisartan-treated patient discontinued therapy due to increases in creatinine and blood ureanitrogen. Liver Enzymes: Occasional elevations of liver chemistries occurred in patients treated withtelmisartan; all marked elevations occurred at a higher frequency with placebo. No telmisartan-treatedpatients discontinued therapy due to abnormal hepatic function. Post-Marketing Experience The followingadverse reactions have been identified during post-approval use of MICARDIS tablets. Because these reactionsare reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate theirfrequency or establish a causal relationship to drug exposure. Decisions to include these reactions in labelingare typically based on one or more of the following factors: (1) seriousness of the reaction, (2) frequency ofreporting, or (3) strength of causal connection to MICARDIS tablets. The most frequently spontaneously reportedevents include: headache, dizziness, asthenia, coughing, nausea, fatigue, weakness, edema, face edema, lowerlimb edema, angioneurotic edema, urticaria, hypersensitivity, sweating increased, erythema, chest pain, atrialfibrillation, congestive heart failure, myocardial infarction, blood pressure increased, hypertension aggravated,hypotension (including postural hypotension), hyperkalemia, syncope, dyspepsia, diarrhea, pain, urinary tractinfection, erectile dysfunction, back pain, abdominal pain, muscle cramps (including leg cramps), myalgia,bradycardia, eosinophilia, thrombocytopenia, uric acid increased, abnormal hepatic function/liver disorder, renalimpairment including acute renal failure, anemia, and increased CPK. Rare cases of rhabdomyolysis have beenreported in patients receiving angiotensin II receptor blockers, including MICARDIS.
OVERDOSAGELimited data are available with regard to overdosage in humans. The most likely manifestation of overdosagewith MICARDIS (telmisartan) tablets would be hypotension, dizziness and tachycardia; bradycardia couldoccur from parasympathetic (vagal) stimulation. If symptomatic hypotension should occur, supportive treatment should be instituted. Telmisartan is not removed by hemodialysis.
DOSAGE AND ADMINISTRATIONDosage must be individualized.The usual starting dose of MICARDIS (telmisartan) tablets is 40 mg once a day. Bloodpressure response is dose related over the range of 20-80 mg. Special Populations:Patients with depletion ofintravascular volume should have the condition corrected or MICARDIS tablets should be initiated underclose medical supervision (see WARNINGS, Hypotension in Volume-Depleted Patients). Patients withbiliary obstructive disorders or hepatic insufficiency should have treatment started under close medicalsupervision (see PRECAUTIONS, General, Impaired Hepatic Function, and Impaired Renal Function). Mostof the antihypertensive effect is apparent within two weeks and maximal reduction is generally attained afterfour weeks. When additional blood pressure reduction beyond that achieved with 80 mg MICARDIS isrequired, a diuretic may be added. No initial dosing adjustment is necessary for elderly patients or patientswith mild-to-moderate renal impairment, including those on hemodialysis. Patients on dialysis may developorthostatic hypotension; their blood pressure should be closely monitored. MICARDIS tablets may beadministered with other antihypertensive agents. MICARDIS tablets may be administered with or without food.
Rx only
MC-BS (03/07)
Copyright © 2007, Boehringer Ingelheim Pharmaceuticals, Inc. All rights reserved.
Printed in U.S.A. (10/07) MC48827
gCovers_NovDec.qxp:Cover 11/25/08 10:36 AM Page C3

MICARDIS is indicated for the treatment of hypertension. It may be used alone or in combination with other antihypertensive agents.
MICARDIS is contraindicated in patients who are hypersensitive to any component of this product. The most common adverse events occurring with
MICARDIS Tablets monotherapy at a rate of ≥1% and greater than placebo, respectively, were: upper respiratory tract infection (URTI) (7%, 6%), back pain
(3%, 1%), sinusitis (3%, 2%), diarrhea (3%, 2%), and pharyngitis (1%, 0%).
Please see Brief Summary of Product Information on adjacent page.
USE IN PREGNANCYWhen used in pregnancy during the second and third trimesters, drugs that act directly on the renin-angiotensin system can causeinjury and even death to the developing fetus. When pregnancy is detected, MICARDIS Tablets should be discontinued as soon as possible
(see WARNINGS, Fetal/Neonatal Morbidity and Mortality).
Copyright © 2007, Boehringer Ingelheim Pharmaceuticals, Inc. All rights reserved. Printed in U.S.A. (10/07) MC48828
Get patients with difficult-to-control hypertension to goal1
MICARDIS. More than POWER…
BP PROTECTION in the early morning2
References: 1. Weber MA,White WB, Giles TD, et al. An effectiveness study comparing algorithm-based antihypertensivetherapy with previous treatments using conventional and ambulatory blood pressure measurements. J Clin Hypertens.2006;8:241-250. 2. White WB, Giles T, Bakris GL, et al. Measuring the efficacy of antihypertensive therapy by ambulatoryblood pressure monitoring in the primary care setting. Am Heart J. 2006;151:176-184.
Please visit www. micardis.com for more information, including Prescribing Information.
Covers_NovDec.qxp:Cover 11/25/08 10:36 AM Page C4

10 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
GENERIC DRUG TRENDSGENERIC DRUG TRENDS
The use of generic drugs isone of the key drivers ofvalue in the pharmacy ben-
efit today. Both drug benefit plansponsors and beneficiaries realizecost-savings by increasing the useof generic drugs when medicallyappropriate. On average, generic
drugs cost 30% to 80% less than their brand-namecounterparts.1 It is important for plan sponsors and planbeneficiaries to understand the safety and efficacy ofgeneric drugs, as well as the potential cost-savings.
Therapeutic Scope of Generics The increasing availability of generic drug therapies
is slowing the rate of growth in prescription drugexpenditures. For the first time since the mid-1980s,the growth in per-capita spending on prescription drugshas dropped below the percentage of growth in the UShealthcare expenditures.2
The average rate of increase for drug expenditures forUS employers in 2008 was 4.86%,3 according to findingsfrom the 2008 Pharmacy Benefit Management Institute(PBMI)’s annual drug benefit plan design survey of USemployers.3 This growth rate represents the lowest costincrease since PBMI began conducting its annual surveyin 1995. This new survey, conducted in May and June2008, was completed by 223 employers, representing15,137,168 members. The increasing use of generic drugscontributes to this single-digit growth in expenditures.
When purchasers and consultants discuss genericdrugs, they refer to 2 different rates or metrics—generic-dispensing rate and generic substitution rate (Table 1).Generic-dispensing rate is a clear metric for trackingprogress in the use of lower-cost prescription drugs. Inmost cases, the generic-dispensing rate is the most
actionable metric to monitor improvement in genericuse and the associated savings. PBMI’s 2008 study alsodocuments continued increases in average generic-dis-pensing rates for US employers in retail and in mail dis-pensing since 2002 (Table 2).3 Generic-dispensing rateswill continue to increase as more brand-name drugs usedby ambulatory populations become available as generics.
The creation of incentives for plan members to usegeneric drugs is essential for a high-performing drug ben-efit program. Generic incentives are of increasing im -portance in 2008 as more branded drugs come off patent.The result is a growing range of generic drug options totreat allergies, arthritis, asthma, depression, elevatedcholesterol levels, hypertension, and chronic pain.
Education Tools for Plan MembersDrug companies are spending billions of dollars to
encourage consumers to request high-cost, brand-namedrugs from their physicians. Consumers and drug bene-fit plan sponsors will realize reduced prescription drugcosts if consumers make the choice to purchase thelowest-cost drug that is medically appropriate for theirneeds. Empowering consumers to make that choice is a challenge.
Complex benefit designs make it difficult for con-sumers to keep track of their plans’ preferred drugs andbeneficiary cost-sharing, and discuss this informationwith their prescribing physicians. Consumers needaccess to up-to-the-minute information on their plans’copayments and prescription costs to make educated,cost-effective decisions.
RepetitionResearch has shown that people often need to see or
hear a message multiple times (as many as 7) before itmakes an impression. Repetition is good, as is using avariety of ways to communicate because people havedifferent learning styles. Organizations should leverageevery available opportunity to deliver messages thatincrease confidence in and encourage the use of gener-ics. Messaging opportunities include: • Direct mail targeted to high utilizers of prescription
drugs
Ms Felthouse is President, Pharmacy Benefit ManagementInstitute (PBMI), Scottsdale, AZ. She has been the lead author of PBMI’s annual Prescription Drug Benefit Cost and Plan Design Report and PBM Customer SatisfactionReport since 2001. She can be reached at [email protected]. The annual reports can be accessed at www.pbmi.com.
Focus on Lowest Net Cost Drug ReducesCosts for Patients, Plan SponsorsDana H. Felthouse, MBA
GenericDrugNovDec .qxp:Cover 11/25/08 10:42 AM Page 10

11www.AHDBonline.comVOL. 1 NO. 9
GENERIC DRUG TRENDS
• Employee meetings• Employee/retiree/member publications, both print
and electronic • Employee/member intranet• Online tools for comparing brand and generic
alternatives• Payroll envelopes and electronic funds transfer
notifications• Podcasts• Posters in break rooms and high-traffic areas• Retiree association events.
Consumer ResourcesThe following consumer-focused resources can sup-
plement plan benefits communication efforts:• Consumer Reports Best Buy Drugs is an independ-
ent, online resource that helps beneficiaries learnabout generic alternatives and empowers them todiscuss cost-effective options with their physicians.Beneficiaries can obtain free reports that comparethe safety, efficacy, and cost of brand-name andgeneric drug options for 16 different medical condi-tions (www.crbestbuydrugs.org).
• The Generic Pharmaceutical Association offersconsumer education on generics, including a fre-quently asked question-and-answer section anddownloadable brochures (www.gphaonline.org/AM/Template.cfm?Section=About_Generics).
• The US Food and Drug Administration (FDA)offers consumer education materials that can bedownloaded, ordered in quantities, or used asresources for developing employer-specific materials.Resources available in multiple languages includeprint brochures, posters, articles, PowerPoint presen-tations, audio presentations and handouts (www.fda.gov/cder/consumerinfo/generic_all_re sources.htm).Aligning your drug benefit plan to encourage the uti-
lization of the lowest net cost drug that is medically appro-priate for a patient will enhance the clinical and econom-ic returns of your investment in prescription drugs. ■
References 1. Generic Pharmaceutical Association. About generics: same medicine,same results, lower cost. http://www.gphaonline.org/AM/Template.cfm?Section=About_Generics. Accessed November 10, 2008.2. PricewaterhouseCoopers Health Research Institute. Behind the Num -bers: Healthcare Cost Trends for 2008. 2008. www.pwc.com/extweb/pwcpublications.nsf/docid/88FF5DC2E5E1143085257300006C68B1.Accessed November 10, 2008.3. Pharmacy Benefit Management Institute. Prescription Drug BenefitCost and Plan Design Report, 2008-2009 Edition. 2008. www.pbmi.com/2008_report/index.html. Accessed November 10, 2008.
Tracking Availability and Price of Generic DrugsUsing generic drugs to save money is a winning strategy for
every drug benefit program. The savings begin when a brand-name drug goes off patent. Here is a list of tools to help track theavailability and price of generic drugs.• Trends in Manufacturer Prices of Prescription Drugs Used by
Medicare Beneficiaries: The AARP’s Public Policy Institute’sannual report on changes in manufacturer list prices forbrand-name and generic drugs. Includes average annual per-cent change in manufacturer prices for the top 25 generic pre-scription drugs. Shows price changes by manufacturer andtherapeutic category for the most widely used generic drugs.www.aarp.org/research/health/drugs/rx_ watchdog.html.
• Drug Patent Watch: Information on drugs and their patent expi-rations. Subscribe to free bulletins on imminent patent expira-tions. www.drugpatentwatch.com/.
• Drugs@FDA: Monthly drug approval reports. Search abledatabase of FDA-approved drugs. Search by brand name oractive ingredient for availability of generic alternatives. www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm.
• FDA Electronic Orange Book: Searchable database of all FDA-approved prescription drugs—brand-name and generic drugs,with therapeutic equivalence evaluations. Daily updates fornew generic approvals. www.fda.gov/cder/ob/.
• FDA Generic Drug Approvals: Monthly reports on first-timegeneric drug approvals. www.fda.gov/cder/ogd/approvals/default.htm.
• Generic Pharmaceutical Association: Statistics and resources for consumers and researchers. Includes list of generic pre-scription medications recently approved by the FDA and guidelines for navigating the Drugs@FDA website.www.gphaonline.org/AM/Template.cfm?Section=Home.
Table 1 Must-Know Generic Terms
• Generic-Dispensing Rate: Percentage of total prescriptions filled with a generic drug
• Generic Substitution Rate: Percentage of total prescriptions that could be filled with a genericdrug that actually are filled with a generic
Source: Pharmacy Benefit Management Institute. The ABCs of Generic Drugs. White Paper Series. 2008.http://www.pbmi.com/pbm101white paperseries.asp.
Table 2 Trends in Average Generic-Dispensing Rates
Year Average retail Average mail generic-dispensing generic-dispensingrate, % rate, %
2002 42.0 32.02003 44.0 34.02004 47.0 38.02005-2006 51.0 39.02007 54.5 41.72008 60.4 49.3Source: Pharmacy Benefit Management Institute. Prescription Drug Benefit Cost and Plan Design Report, 2008-2009 Edition. 2008. www.pbmi.com/2008_report/index.html.
GenericDrugNovDec .qxp:Cover 11/25/08 10:42 AM Page 11

“We either do it right orwe don’t do it at all.”
©2008 Mylan Pharmaceuticals Inc.
GenericDrugNovDec .qxp:Cover 11/25/08 10:42 AM Page 12

In 1961, two U.S. Army buddies, Milan (Mike) Puskar and
Don Panoz, founded a pharmaceutical company with a handful
of employees in a small town in West Virginia. From the
beginning, the founders were determined to build a company
based on quality and integrity and to follow Mike’s philosophy—
“We either do it right or we don't do it at all.”
Over the past 47 years, that company, Mylan Pharmaceuticals,
has grown to become the largest U.S.-based manufacturer
of generic pharmaceuticals by total prescriptions*. . . and
Mike Puskar is still Chairman of the Board. His no-compromise
attitude continues to guide all aspects of company business,
from research and development, to manufacturing and
distribution.
Today, every employee in the Mylan family is always ready to
take the extra step necessary to ensure that Mylan Products
deliver the high quality that patients expect and deserve. This
unwavering commitment assures that products from Mylan will
always offer quality and affordability for the patients who need
them and peace of mind for the pharmacists who dispense them.
He’s kept his wordfor 47 Years.
MYNMKT276A
*IMS National Prescription Audit. Total Prescriptions: June 2007 - June 2008.
GenericDrugNovDec .qxp:Cover 11/25/08 10:42 AM Page 13

14 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
REGULATORY
F. Randy Vogenberg: There have been attempts to lookat large claim databases (eg, WellPoint’s) of patients receiv-ing erythropoiesis-stimulating agents (ESAs). News aboutthe cutback on ESA use was accompanied by reports aboutthe rise in the number of transfusions. At the same time,articles published in pharmacy and hospital journals wereadvocating the use of ESAs to avoid transfusions. So, themessage is mixed. What people are doing in an inventoryenvironment is not the same as what they are doing in aninstitutional inpatient environment. And hospitals may con-tinue to use ESAs to avoid the more costly transfusion, apurely cost consideration. Is this how you see it?
Samuel Silver: I think this may be true. But theissue of transfusion is beyond cost, especially in the out-patient setting today, where 85% of cancer patient careoccurs in the community and not in academic medicalcenters.
The first issue is that giving transfusions at centerssuch as the University of Michigan is relatively simple,and our facilities are well prepared to administer them.
We have a good blood bank on site and plenty of chairsfor transfusions, so we can get people set up, and wehave blood irradiators (see below). But in the commu-nity, physicians by and large don’t give transfusions intheir offices because of the administrative and proce-dural hassle. Rather, they send patients to their hospi-tal outpatient infusion area, which is usually very small,where they can run out of transfusion chairs relativelyrapidly, so that we now have a group of patients eitherrequiring admission for transfusion or experiencing asignificant delay waiting for an outpatient chair. Andthese are not patients with shortness of breath whorequire admission but rather it’s a quality-of-life (QOL)matter, because of the requirement of an inpatient stay.
The second issue is that the typical Medicare bene-ficiary has many comorbid conditions (eg, heart fail-ure) in addition to cancer. Thus, we are no longer talk-ing only about potential infectious complications oftransfusion but also about issues of fluid overload thatwould not occur when using an ESA.
The third concern is that many patients receivingchemotherapy, especially those with hematologicmalignancies, are immunosuppressed. They requireirradiated blood products to avoid transfusion-associat-ed graft-versus-host disease. Irradiating blood is veryeasy; any university blood bank will have a blood irra-
Erythropoiesis-Stimulating Agents in aMeta-Stable State: Guidelines,Economics, and Policy in FluxInterview (Part 2) with Samuel M. Silver, MD, PhD
Medicare coverage of erythropoiesis-stimulating agents is a complex issue with implicationsfor a variety of healthcare stakeholders. In the first part of the interview (see AHDB, May2008), Samuel M. Silver, MD, PhD, examined the evolution and clinical implications of theMedicare coverage decisions and the eventual shift in clinical practice away from theapproved indication to situations involving quality-of-life issues. In this second part, Dr Silverdiscusses with F. Randy Vogenberg, RPh, PhD, the clinical implications of the Medicare cov-erage decision regarding erythropoiesis-stimulating agents, pointing out the noneconomicreasons why transfusions can be risky to cancer patients, and how such policy decisions canhave profound implications for patients. Dr Silver calls for new studies to be initiated, which
would be funded by the 2 major manufacturers of these drugs, to investigate the concerns regarding tumor pro-gression and thromboembolic events that are potentially associated with these expensive and potentially toxicmedications. The discussion resumes where Dr Silver explains why it would be good to compare claims data ofcancer patients who are receiving these medications and their transfusion requirements. [ADHB. 2008;1(9):14-18.]
Dr Silver is Professor of Internal Medicine, Director, CancerCenter Network, Division of Hematology/Oncology, andAssistant Dean for Research, University of Michigan HealthSystems, Ann Arbor, MI.
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 14

15www.AHDBonline.comVOL. 1 NO. 9
ESAs in a Meta-Stable State
diator. It does not require much time, but it will addsome expense. Nonetheless, it is well worth it.However, if the patient is in a suburban or rural com-munity, that patient may not have immediate access toirradiated blood and will have to wait a day or two toget it. So, all of a sudden something that would be sim-ple for me at the University of Michigan becomes aprocess that takes several days for a patient thatreceives chemotherapy in a suburban or rural facility.These are some of the noneconomic, procedural issuesthat are involved in giving transfusions.
Vogenberg: The other side of this issue concerns youngerpopulations. The 50- to 60-year-old patient may still have acommercial insurance and not Medicare. Thus, there arealso direct economic costs to consider, such as absence fromwork, particularly when the patient may be tied up for a dayor two, as you said. There are many repercussions forMedicare, which is the focus for the Centers for Medicare &Medicaid Services (CMS), and for commercial insurers andemployers, who are paying the bills. This is not well under-stood; the tendency is to just look at the drug cost and thedrug companies, and this is more emotional than rational.
Silver: True. And the next thing we know, we aretalking about Medicare Part B, and we begin to reachout to Medicare Part A, when we start admitting peo-ple to the hospital. Apparently those involved inMedicare Part B decisions don’t see this, but we cer-tainly see this as citizens and on the private side. Andthe employers see this. So the US Food and DrugAdministration (FDA) has issued new warnings, whichessentially reflect the concerns about potential tumorprogression, venous thromboembolism, and keepingthe hemoglobin level at <12 g/dL (although this cut-offmeasure was dropped by the FDA from the most recentESA labeling).
The FDA reiterated this in its most recent state-ment. That is where we are from the point of view ofthe FDA and CMS. And the Senate passed a nonbind-ing resolution about it, since the Senate has a sensethat the National Coverage Decision (NCD) has noweight and should be changed.
Vogenberg: This NCD issue probably comes at a goodtime for CMS, because the current Congress is deadlockedon many issues. So nothing is going to happen. There are norepercussions against CMS’s decision about ESAs, and itcan come back and say it has saved a lot of money, whilepreventing further harm to their beneficiaries. It is reallyalmost a neutral situation from a public policy perspective.
Silver: In the meantime, Representatives PeterStark and Henry Waxman are saying they are protect-ing the patients from this “miracle grow for tumors.”And because we have no quality-of-life (QOL) data,there are no improvements in QOL issues. Now whatdo we do? We definitely require more data.
Vogenberg: How transparent is CMS regarding its data?
Silver: CMS is not transparent at all. When youread the NCD, their background materials have beentightened up a bit. But the intellectual basis to bridgebetween the final coverage decision background mate-rial and the rules is missing.
Vogenberg: This is very typical of what you would seein almost any insurance company. You get caught up in thisdynamic of economics and cost, and you are trying to pro-vide just enough access so that people are happy, but at thesame time less attention is paid to QOL than to the science,so it really is about economics. For CMS, it appears to beabout money. They had to stay within a budget, and they
KEY POINTS▲ Despite the high costs of the ESAs, the issue of transfusions
in cancer patients is beyond economics.▲ The noneconomic issues surrounding transfusions that trans-
late to unnecessary risks for patients are:1. Inadequate facilities that mean long waiting periods2. Many patients are Medicare beneficiaries and thus often
have multiple comorbidities3. These patients are often immunosuppressed, requiring
irradiated blood products, which could be a problem innonacademic centers.
▲ Although Medicare is not supposed to consider costs in itsdecisions, cost is an underlying context for Medicare cover-age for these very expensive medications, which, neverthe-less, may reduce hospitalization for transfusions.
The next thing we know, we are talking about Medicare Part B, and we begin to reach out to Medicare Part A, when we startadmitting people to the hospital.
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 15

16 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
REGULATORY
knew the ESA coverage was a budget buster and a high-expenditure category, as it is for any employer. This is theperfect moment to come up with a Solomon-like decision.CMS is not required to disclose as much as the FDA. Thismakes it easier for the commercial carriers to follow suit.
Silver: In addition, CMS will identify 10 more ques-tions that should be answered, as they did 1 year ago,even though many of these questions are unanswerable,because the data don’t exist, and CMS knows it; a trueCatch-22.
Vogenberg: This points to an interesting dichotomybetween what the Agency for Healthcare Research andQuality is doing and Medicare Part D initiatives and thegeneral Medicare initiatives about quality issues in hospi-tals, such as pay-for-performance. On one hand, CMS is saying it is going to pay for improved performance andoutcomes in the hospitals, which, based on the current lit-erature, suggests they would be using ESAs; these drugslead to better results and reduce complications and read-missions, which are the criteria for quality. But on theother hand, Medicare coverage decision, which was basedon an outpatient basis, prevents clinicians from using these drugs.
Silver: That brings up an interesting point. InCMS’s Physicians’ Quality Reporting Initiative, one ofthe early reporting initiatives dealt with the use ofESAs in myelodysplastic syndrome (MDS). It was nec-essary to make sure patients had sufficient iron stores,which was a quality point. Yet, the payment for MDSassociated with ESAs was denied at that time, as wediscussed in the first part of this interview (AHDB.May 2008;1[4]:46-50).
Vogenberg: And then it could be argued that the cost ofthese medications is too high?
Silver: Actually, Medicare is not supposed to talkabout costs or to consider it in its decisions, but ofcourse it is the underlying context.
Vogenberg: And what is the Veterans Administration(VA) doing with the coverage?
Silver: I do not have the answer to that. The VA hasan excellent electronic medical records system; howev-er, in the past few months the VA was unable to useany of their data for Health Services Research purpos-es because of confidentiality and HIPAA (HealthInsurance Portability and Accountability Act) issues.
Vogenberg: There must have been some kind of analy-ses done within the VA military review structure when allthis was transpiring, because they are so cost and qualityconscious. I wonder what the VA system is doing aboutTRICARE and the active military, which represents a largepopulation?
Silver: This is a very important issue. The FDA hasasked the American Society of Clinical Oncology(ASCO) and the American Society of Hematology(ASH) to determine what studies should be done inthe future. ASH has asked the American Associationof Cancer Research (AACR) to participate in this ini-tiative. We are trying to convene a meeting with rep-resentatives from the FDA, CMS, ASH, ASCO, andAACR to determine what trials are needed and whoshould be running them.
Vogenberg: Would they be doing a corresponding healtheconomics analysis with clinical studies parameters?
Silver: That would be an important thing to look atas well, but the executive committee of ASH believesthat the National Institutes of Health (NIH) shouldnot be paying for such studies to help determine thebest hemoglobin range for ESA use. The ExecutiveCommittee is concerned that this type of study costs alot of money. And diverting NIH money for this clini-cal question would leave less money for important basicscience research.
Vogenberg: That is a good point.
Silver: It would be important to engage bothJohnson & Johnson and Amgen to design an openstudy that would be funded by an unrestricted grantfrom both drug manufacturers to examine the patho-physiology of ESA-associated thromboembolism. Andmaybe we should involve the NIH and the NationalCancer Institute or the National Institute of Diabetesand Kidney Disease to address issues surrounding end-
Medicare is not supposed to talk about costs or to consider it in its decisions, but of course it is the underlying context.
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 16

17www.AHDBonline.comVOL. 1 NO. 9
ESAs in a Meta-Stable State
stage renal disease (ESRD). So we need to focus on 3aspects of the drugs—tumor promotion, the biology of venous thromboembolism, and the relationship toESRD, which can teach us a lot. And these 3 thingsshould happen in parallel, along with the economicissues that are related to these clinical considerations.
Vogenberg: Clinically speaking, where would you wantthe focus of these studies to remain?
Silver: Future studies should somehow focus on QOL in a meaningful way. Combining the efforts ofJohnson & Johnson and Amgen may be effective. Inthat way, individual marketing agendas could be put aside. For at least the moment, private payers havebeen using the ASH/ASCO guidelines as opposed toMedicare guidelines. This, of course, could changetomorrow. When I spoke with Dr Lee Newcomer of UnitedHealthcare a while back, he made no promis-es. He seemed to think it was very reasonable to use theASH/ASCO guidelines, using an initial hemoglobinlevel of <10 g/dL, and then maintaining patients athemoglobin levels between 10 g/dL and 12 g/dL. As Imentioned in the previous article in this journal (May2008), oncologists have come to view this issue withconcern; we are generally maintaining patients at orbelow hemoglobin levels of 12 g/dL.
Vogenberg: Are physicians still providing ESAs as freelyas they had before the new Medicare coverage ruling wasannounced?
Silver: No. In fact, the number of those using ESAshas declined significantly. This may have been associ-ated with the FDA issuing the black box warnings inMarch 2007. I think the bottom line is that most physi-cians want to use drugs in a reasonable way, and per-haps they overcompensate when they hear the cynicalperspective about perverse physician incentives. Sowhen the black box warning was issued, there was agreat deal of self-correction.
Vogenberg: Carriers will be more willing to take the softapproach UnitedHealthcare has taken, unlike that taken byMedicare. They will seek the benefit of the reduced expen-ditures by informing their provider networks and offeringthem the opportunity to avoid potential complications and tobe in compliance with the guidelines. This could be a win-win situation for everybody.
Silver: Possibly. But it is a complicated issue. Pa -
tients getting chemotherapy are receiving toxic agentswith therapeutic ratios that are some of the most diffi-cult in medicine. Many of the patients, especially thosein the Medicare population, have incurable cancers;they are receiving chemotherapy mainly for palliation.The goal is to give them as high a QOL as possible. Ifthey are receiving chemotherapy and spend the last 2months of their lives in the hospital, we are not doingthe right thing.
Debilitating patients for the majority of theirremaining time to shrink a tumor is not good care. APyrrhic victory in this scenario is no victory at all. Andusing a drug that potentially can cause thromboembol-ic events only complicates this picture.
I was called to an FDA meeting in which a patientrepresentative was anxiously going on about tumorgrowth associated with ESAs that patient was receiv-ing. This is a difficult thing to say, but having progres-sion of an incurable cancer is not always the worstthing that can happen. Chemotherapy is rarely provid-ed with curative intent in this population. Appropriatepalliation may include chemotherapy along withadjunctive therapies, such as ESAs, that may cause asmall risk of tumor growth.
Vogenberg: This is a valid point that many people for-get. Patients who are seriously ill often lose sight of realityor don’t want to face it.
Silver: Right. Sometimes we need to reach deeperinto the bag for more information.
As I have said, finding this would be tantamount tofinding the Holy Grail, and unfortunately, you cannotinfallibly predict outcomes. ■
Disclosure StatementDr Silver is a consultant to Bear Stearns, Lehman Brothers, and
the Gerson Lehrman Group, and receives grant/research supportfrom Blue Cross Blue Shield of MI.
We need to focus on 3 aspects of the drugs—tumor promotion, the biology ofvenous thromboembolism, and the relationship to ESRD, which can teach us a lot.
Stakeholder Perspective on page 18
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 17

18 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
REGULATORY
Stakeholder PerspectiveThe Clinical and Economic Complexity of Biologics
PAYERS/PATIENTS: The inability to predictoutcomes with erythropoiesis-stimulating agents(ESAs) or with other biologic agents is emerging asa key concern. Whether in rheumatoid arthritis,multiple sclerosis, or erythropoiesis, unintended orunknown effects from these new biologic medica-tion technologies are gradually better detected andbetter understood, helping to determine the mostappropriate uses. From the perspective of economic decision makers—patients, health plans, or employ-ers—the easy clinical decision to use biologic med-ications has become muddier, while these same(typically elderly) patients are rethinking their needfor a wider variety of end-of-life therapies that have focused more on quality-of-life issues than onchanging the lifespan.
ESAs provide an interesting insight into thecomplexity of clinical use of biologics and their eco-nomic impacts on all payers, as well as the types ofclinical service providers. Given that many patientswho are using biologics are covered under aMedicare drug plan but also have multiple comor-bidities, this further illustrates the dilemma of find-ing a technological advancement end point wherecosts become more predictable. As Dr Silver pointsout in the interview, several concerns involvingpatients who receive ESA therapy go beyond a sin-gle decision point.
Because of the paucity of data to clearly guide themultipoint clinical and coverage decisions, theCenters for Medicare & Medicaid Services (CMS)and private insurers are erring on the side of limitedcoverage, following the evidence-based medicine(EBM) model. Although in itself not siding withany coverage position, EBM can conveniently beused for any stakeholder’s position, whether eco-nomic or clinical. In the case of ESAs, there seemsto be a clinical and an economic dilemma forebod-
ing of the bigger and more expansive decisions oursociety faces through the lens of healthcare insur-ance coverage for the growing pipeline of biologic-based technologies.
The role of regulators (CMS, US Food and Drug Administration) and system researchers(Association for Healthcare Research and Quality,quality improvement organizations) should bedetermined by Congress to better align incentives,along with a clearer direction for the use of newtechnologies (diagnostic or therapeutic). Mixedmessages and misalignment of incentives has longbeen an albatross around the US healthcare systemthat has fed many debates and articles arguing themyriad of issues relevant to each of the stakeholders.This has been good for academics, consultants, andspecial interest lobbyists, but not for frontlinepatients and healthcare professionals, or those pay-ing the bills for care.
Based on reports from the recent presidentialcampaign and from groups such as the KaiserFoundation or the Wall Street Journal, neither partynor either of the candidates has had the single obvi-ous solution to our looming healthcare crisis in thenext decade. Perhaps our economic distress will aidpatients, as reflective of our society, in establishingnew parameters around life-and-death decisionsthat will help our healthcare system seek a new bal-ance in harnessing technologies for the most appro-priate use, which will then determine its hierarchi-cal cost in our economy.
F. Randy Vogenberg, RPh, PhDChief Strategy OfficerEmployer-based Pharmaceutical Strategies, LLCSenior Scholar, Department of Health PolicyThomas Jefferson University, Jefferson MedicalSchool
Subscribe to our e-Newsletter at www.AHDBonline.com
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 18

Early and intensive treatment can help patients reach their A1C goal Are your plan members not taking their type 2 diabetes medications?
Many patients are not reaching the ADA A1C target goal of <7%, and many are stopping their medications.1,2
Recent data show a drop in the use of oral antidiabetic medications3
The need for early treatmentBecause many patients already have chronic complications at the time of diagnosis, treatment plans must be aggressive from the start to optimally manage type 2 diabetes.4
Long-term benefits of diabetes medications can only be realized if patients adhere to their treatment regimen.2
“Early, intensive intervention has the potential to get patients to glycaemic goals more quickly and
be more effective at keeping them at goal...”5
2,000
2,100
2,200
2,300
2,400
2,500
3/16/2007 Days 6/6/2008
TRx
(000
s)
OAD TRx 4 week moving avg Trend (Pre-NEJM)
References: 1. Hoerger TJ, Segel JE, Gregg EW, Saaddine JB. Is glycemic control improving in U.S. adults? Diabetes Care. 2008;31:81-86. 2. Rodgers K. Ensuring compliance in patients with diabetes. In: Diabetes: Disease Management Guide. 4th ed. Montvale, NJ: Thomson PDR; 2004:501-505. 3. Data on file, Takeda Pharmaceuticals North America, Inc. 4. Cornell SA. Clinical case study: achieving long-term control of insulin resistance. J Manag Care Pharm. 2007;13(suppl B):S11-S15. 5. Goldstein BJ, Gomis R, Lee H-K, Leiter LA, on behalf of the Global Partnership for Effective Diabetes Management. Type 2 diabetes—treat early, treat intensively. Int J Clin Pract. 2007;61(suppl 157):16-21.
©2008 Takeda Pharmaceuticals North America, Inc. PIO-00658 6/08 Printed in U.S.A.
RegulatorySilver_NovDec .qxp:Cover 11/24/08 4:28 PM Page 19

20 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
BUSINESS
Adherence to medications is essential forpatients with chronic disease for optimizingclinical outcomes. When used appropriately,
medication is a very cost-effective method for treat-ment and prevention of disease. Patients who fail totake their medications as prescribed do not get the fullbenefit from the drugs, and they may also end up withunnecessary hospitalizations, emergency departmentvisits, and nursing home admissions. Cost-effective,scalable interventions are essential to reduce nonad-herence. In this article, we examine the use of auto-mated phone-based patient communication to supportoutreach efforts, as well as the impact this type of inter-vention can have on clinical outcomes and costs.
In their 2005 study of medication-taking behaviors,Osterberg and Blaschke observed that, “Common bar-riers to adherence are under the patient’s control, soattention to them is a necessary and important step inimproving adherence.”1 In that study, the followingreasons were cited by patients for not adhering to their
medication regimens1:• Forgetfulness—30%• No reason—27%• Other priorities—16%• Decision to omit doses—11%• Lack of information—9%• Emotional factors—7%.
Lack of information and forgetfulness combinedcomprise 39% of the reasons cited in this study for poormedication ahderence.1 These 2 areas can be positivelyaffected by improved communications between thecare provider and the patient that, in turn, can improvemedication adherence.
One other common and well-documented reason forpoor adherence is side effects.2,3 Patients who experi-ence unpleasant or unexpected side effects may stoptaking their medications, often without informing theirphysicians or other care providers.2,3
In their study, Osterberg and Blaschke furtherobserve that there are 4 general methods to helpimprove patient adherence1:1. Patient education2. Revised dosing schedules
Role for Automated CommunicationStrategies in Medication AdherenceManagement S. Michael Ross, MD, MHA
Lack of medication adherence is a prevalent problem that causes a broad range of health-and health-economics–related issues. Adherence management is therefore an importantstrategy, but it also presents its own set of challenges. Interventional communication fromcare support teams at managed care organizations and disease management and wellnessprograms has proved effective at modifying patients’ medication adherence and reportingbehaviors. However, these communications do not work well from an economic standpoint.It is not economically feasible to scale call centers and the numbers of clinical and profes-sional staff to communicate with the increasing number of patients with chronic diseaseswho require ongoing medication use. Using communication automation to augment tradi-tional call center outreach can help to mediate patient medication-taking behaviors. Specific
design criteria for the automation of this interaction are discussed in this article, offering supporting data from arecent trial of 304 elderly patients with hypertension, and showing the benefits of using such a system for effec-tive blood pressure monitoring, at reduced costs. [AHDB. 2008;1(9):20-27.]
“Drugs don’t work in patients who don’t take them.” —C. Everett Koop, former US Surgeon General
Dr Ross is Vice President of Healthcare, Varolii Corporation,Seattle, WA.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 20

21www.AHDBonline.comVOL. 1 NO. 9
Automated Communication Strategies
3. Expanded hours when the clinic is open, includingevening hours
4. Shorter wait times and improved communicationbetween physicians and patients.
Although not all of these general methods are relevantto our topic, patient education and communicationbetween physicians and patients are 2 areas that can beaffected by effective communications.
Illustrative CaseTom’s blood pressure (BP) was elevated during his past
2 visits to his physician. At the most recent visit, his doc-tor suggests an antihypertensive regimen and prescribeslisinopril. Tom fills the prescription order for lisinopril atthe local pharmacy and takes it home. As part of his rou-tine care, Tom schedules a follow-up examination. Aftera period of time, we may expect a reduction in Tom’s BPlevel. But instead, at his follow-up visit, Tom’s BP is stillelevated. Was lisinopril ineffective in Tom’s case? Notnecessarily. In fact, the medication might well haveproved effective if Tom had remembered to take it. ButTom took the first day’s dosage, put the bottle in his med-icine chest, and then promptly forgot about it. He alsowas not reminded to take the medication.
The Challenge: Improving Care for 10 Million “Toms”Tom is not alone. Findings from Osterberg and
Blaschke’s study show that, “Of all medication-relatedhospital admissions in the United States, 33% to 69%are due to poor medication adherence, with a resultantcost of approximately $100 billion a year.”1 In addition,according to well-documented surveys, failure toadhere to treatment, also known as noncompliance, isa large-scale problem.4,5
The 2006 Case Management Adherence Guide -lines, issued by the Case Management Society ofAmerica, offer insight into the magnitude of the issue,noting that “the number one problem in treating ill-ness today is patients’ failure to take prescription med-ications correctly, regardless of patient age.”4
In a 2003 study, the World Health Organizationfound that approximately 50% of the 1.8 billion pre-scription medications dispensed annually in the UnitedStates are not taken correctly by patients.5 It is reason-able to assume that at least some of these nonadherentpatients are not receiving the full benefits of the pre-scribed medication. In 1998, nonadherence to heart dis-ease medication regimens alone was reported to be thecause of 125,000 preventable deaths each year in theUnited States.6 This places medication nonadherenceamong the major causes of health-related deaths in the
United States, after heart disease, cancer, stroke, andchronic lower respiratory diseases, according to the 2005National Vital Statistics Reports (Table).7 In reality, deathsfrom all medication nonadherence could be much largerthan the 125,000 deaths for heart disease only.
Patients who stop taking medication as a result offorgetfulness, lack of information, or side effects canoften be helped by effective outreach from their physi-cian or clinical care professionals to remind patients totake their medications, elicit information about sideeffects and their impact on noncompliance, offerencouragement, and even connect them with their
KEY POINTS▲ Medication nonadherence is a major cause of morbidity and
mortality, and is a large contributor to escalating health-related economic costs.
▲ Lack of information and forgetfulness are 2 main reasons fornonadherence that can be positively affected by improvedpatient–provider communication.
▲ With chronic diseases estimated to involve hundreds of millions of patients, the scale of disease management enroll-ment is too great to be cost-effective using traditional out-reach methods.
▲ The challenge is to scale outreach programs efficiently, with-out losing the personal touch necessary to help changebehavior.
▲ In a new study of automated telephony for blood pressuremonitoring, this technology reduced the cost of blood pres-sure reading by 95% compared with supportive care reading.
▲ The study results suggest that efficient, effective automatedcommunications with patients can produce positive clinicaloutcomes at reduced costs.
Table Medication Nonadherence Major Cause of Death in theUnited States
Condition Annual deaths, N 1. Heart disease 652,0912. Cancer 559,3123. Stroke 143,5794. Chronic lower respiratory diseases 130,9335. Medication nonadherence 125,000*
6. Diabetes 75,1197. Alzheimer’s disease 71,599
* This number refers to medication nonadherence deaths from heart diseasealone; the number for all deaths from medication nonadherence could there-fore be higher. Source: McCarthy R. The price you pay for the drug not taken.Bus Health. 1998;16:27-33.Source: Kung HC, Hoyert DL, Xu JQ, Murphy SL. Deaths: final data for 2005.Natl Vital Stat Rep. 2008;56:1-120.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 21

22 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
BUSINESS
clinical care team, if needed. This, in fact, is one of thekey premises around which managed care organizations(MCOs) and wellness programs are organized: by offer-ing regular, relevant “interventional” communicationsin a structured program, these organizations can posi-tively affect medication-taking behaviors of their pro-gram members.
Health Economics: The Costs of Noncompliance Adherence is critical to everyone involved in
healthcare: from patients and payers (insurance, gov-ernment, employers) to retail pharmacies and pharma-ceutical manufacturers. And it is the sheer number ofthese patients that forms the heart of the adherencechallenge. For patients, adherence is an important factor in improving clinical outcomes; this issue hasbeen well documented in the literature.1 Indeed, theCase Management Society of America observes,“Nonadherence to medications is a common factorthat prevents patients from achieving the full thera-peutic benefit of their therapies.”4
For organizations, improved patient adherencemeans the ability to deliver better care while reducingmedical expense ratios driven by unnecessary hospital-izations, emergency department visits, nursing homeadmissions, and excess consumption of interventionaltreatments.5
For manufacturers and retail pharmacies, whosenonadherent patients do not fill prescriptions as indi-cated, or who have poor medication possession ratios,improving patient adherence is not only important to
patient health but can also affect bottom-line revenues.Let’s return briefly to our hypertensive patient, Tom.
During the follow-up appointment, Tom’s doctor asks ifhe is taking his medication as prescribed. Tom sheep-ishly admits he has forgotten. Tom’s doctor remindshim of the importance of taking medications as pre-scribed, and provides information about hypertension,the associated health risks of stroke and heart attack,and strongly encourages him to “stick” with the med-ication regimen. Concerned about his health andencouraged by his healthcare provider, Tom signs up fora wellness program through his employer. A care repre-sentative from the wellness program contacts Tom,enrolls him in the program, and begins to provide himwith information, tips, and additional encouragement.The outcome? Tom’s BP is much better managed now,and he will likely have an improved clinical outcome as a result.
Of course, Tom is a hypothetical patient, but this isa common story for millions of real patients with hyper-tension. Illustrative of the scale of this particular condition, the 2005 National Ambulatory MedicalCare Survey revealed that there were 44 million visitsto office-based physicians with hypertension as a pri-mary diagnosis.8
Further complicating the issue is the fact that manyof these patients may be older and may take more than1 medication regularly.4 We live in a society experi-encing a “graying” of its population, as the baby boomgeneration begins to mature past the age of 65 years.Many boomers, as well as millions of others, will be prescribed multiple medications (Figure 1) for chron-ic conditions, such as hypertension, high cholesterol,depression, and diabetes.8 The Centers for DiseaseControl and Prevention’s (CDC) Health, UnitedStates, 2007, survey shows that slightly more than 30% of all individuals between the ages of 45 and 64had taken 3 or more prescription medications in thepast month.9
Provider CommunicationIt is well-documented that clear, consistent provider
communication can have a positive impact on patientwell-being. In an article on literature searches forphysician–patient relations, Stewart notes that “Mostof the studies reviewed demonstrated a correlationbetween effective physician–patient communicationand improved patient health outcomes.”10
Thus, it is not surprising that regular, consistentcommunications from care support teams, such asthose in wellness organizations, can have the same
Prescriptions filled, %60
50
40
30
20
10
0
1823
30
10
23
42
57
32
24
1992 1996 2000Year
0 1-2 3-4 5+Chronic conditions (N), 2000
Yes NoRx coverage, 2000
Figure 1 Average Annual Prescriptions Filled by Noninstitutionalized Medicare Enrollees, ≥65 y
Source: Cherry DK, Woodwell DA, Rechtsteiner EA. National AmbulatoryMedical Care Survey: 2005 summary. Adv Data. 2007;(387):1-39.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 22

23www.AHDBonline.comVOL. 1 NO. 9
Automated Communication Strategies
effect. If it were just 1 doctor effectively communicat-ing to 1 patient the importance of consistently takingmedication as prescribed, it might be easier to resolvethe adherence problem. But, as we have noted, thereare tens of millions of “Toms” with a variety of chron-ic conditions who require this type of outreach. TheCDC notes in its Health, United States, 2007, that in2005, the percentage of adults with 3 or more chronicconditions increased with age from 7% of adults aged45 to 54 years to 37% of adults aged 75 years andolder.9 Although managing chronic conditions is aproblem of scale, the real challenge lies in scaling effi-ciently, without losing the personal touch necessary tohelp change behavior.
The Economics of Outreach: Scaling Clinical CallCenters Is Expensive
Clinical outreach centers typically employ a blend oftrained care professionals and clinical care professionals,such as registered nurses and pharmacists. The fullyloaded hourly wage of these individuals can exceed $50,which means the cost of even a relatively brief (15-20minute) phone call can approach $20. This figure isconservative, given that the industry-standard cost for acall for technical support centers ranges between $20and $40,11 using significantly less costly staff. This costdoes not decrease with increased call center staff or withlarger numbers of patients to call, so organizations’ abil-ities to scale outreach programs using care representa-tives are significantly limited.
Today, health plans and disease management pro-grams are evolving new strategies and solutions to helptheir patient populations adhere to treatment plans.We suggest that any strategy must meet 2 primary tests:1. Is it efficient? Efficient solutions scale well and offer a
low marginal cost of operation.2. Is it effective? Effective solutions deliver similar re -sponse rates and engagement rates as the current gold standard—human outreach by care support representatives.
What Needs to Be Done Today and TomorrowTraditionally, MCOs and disease management pro-
grams use a broad range of outreach methods, includingnurses or other specialty practitioners to contact par-ticipants, review program benefits, respond to ques-tions, and ultimately, enroll members. Once enrolled,these same specialists may contact members for surveys,health status updates, medication reminders, and othercommunications designed to foster compliance.
In principle, this form of operation should be effec-
tive (and often is with small populations). For theorganizations paying for these programs, cost benefitsare largely dependent on the ability to reach large num-bers of patients, enroll them, and provide ongoinghealth and wellness support. Considering that thenumber of individuals with chronic diseases is estimat-ed to be in the hundreds of millions, the scale of enroll-ment is too great to manage cost-effectively with tradi-tional outreach methods.
Communication Works, but Not Cost-EffectiveIn the Medicare Health Support phase 1 study, the
Centers for Medicare & Medicaid Services determinedthat the value delivered by these programs does notovercome program costs.12 It was simply not cost-effi-cient (nor economically feasible) for clinical staff orcare support specialists to communicate with evenmoderately large at-risk populations. And yet, the samestudy found that this type of interventional communi-cation had a clear beneficial impact on participants.“Participating beneficiaries tend to be a healthier andless-costly subset of the intervention group. Thus, highparticipation rates will likely be a factor in the abilityof the [Medicare Health Support organizations] toimpact their assigned intervention populations.”12
And although human communication is certainlythe benchmark for clinical results, automating commu-nication shows some positive results. Properly imple-mented, this form of communication may deliver simi-lar clinical results at a far lower marginal cost.
Communications Automation: Scalable Interactionfor Large Populations
As noted earlier, any type of automated communi-cation must be able to connect efficiently with largenumbers of patients or members. Automated commu-nication must also connect effectively, by delivering anexperience that resembles an actual clinician–patientinteraction. Modern communications systems can bemodeled against good examples of productive clinicalinteractions (eg, a system could emulate the voice and
For organizations, improved patient adherence means the ability to deliver bettercare while reducing medical expense ratiosdriven by unnecessary hospitalizations andexcess interventions.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 23

24 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
BUSINESS
persona of an experienced call center representative oran outreach nurse).
Effective interventional dialogue with patientsinvolves understanding the patient’s specific concernsand health beliefs, embracing that information, andthen using it to tailor interventions specific to theirneeds. When insights such as these are applied to thetreatment regimen, adherence improves dramatically.13
And as discussed before, improved adherence can pro-vide a positive boost to health outcomes, both proxi-mal and for the long-term.
Automated patient communication offers addition-al potential benefits. With the majority of contactsmanaged through an automated system, organizationscan optimize the use of live agent care supportresources by triaging those patients most in need,thereby responding more efficiently to critical patientcare questions (see below).
The ability to deliver automated patient communi-cation programs efficiently (at a low unit cost) andeffectively (with a positive result across the majority ofrespondents) may offer additional distinct advantages,including increased scope (the lowered unit costimproves the provider’s ability to reach out to morepatients or members) and improved health economics(improved individual outcomes across a broad segmentof the at-risk population that contributes to improve-ment in the aggregate outcome profile).
Key Criteria for Successful Automation of PatientOutreach Communications
Varolii Corporation’s healthcare division has beencommunicating with tens of millions of patients on amonthly basis on a variety of healthcare-related areas.Based on the experience of delivering these automatedcalls, and on Varolii’s general experience in deliveringbillions of automated notifications over the past sever-al years in a variety of industries, we believe that 5 keycriteria can determine whether automated communica-
tions will serve as a useful adjunct to patient outreach.These criteria revolve around the concepts of efficien-cy and effectiveness discussed earlier:1. Scalability. If you cannot reach large populations
cost-effectively, then any other enabling criteria will not matter.
2. Clarity. Most people, particularly older or at-riskindividuals, find artificial voices, varying intona-tions, pace, and variable volume levels not onlyannoying, but difficult to understand.14
3. Personalization and Interactivity. “Personaliza -tion,” or tailoring the message to specifically addressindividual concerns, enables automated communica-tions to more closely match the experience of con-versing with a clinician or specialty representative.Results of Datamonitor’s Patient Compliance Survey,2004, authored by Adele Schulz, “support the ideathat personalized communication with patients is animportant tool in compliance initiatives.”15
“Interactivity” is the ability to accept patientrespon ses either through keypad presses or voice re -sponse, and deliver the next question or informationbased on the previous response. Interactivity can helpensure regulatory compliance by enabling appropriateauthentication. As an example, HIPAA (HealthInsurance Portability and Accountability Act) com-pliance through authentication, sometimes known asright party contact, could be managed as follows:
• Before giving any personalized information, an auto-mated system could ask the individual to confirmthat he/she is the correct party
• If further authentication is required, the systemcould ask for appropriate credentials.
This type of interactivity can also be used to collect survey data and patient feedback throughsurvey questions.
4. Reporting Visibility. Reporting is important bothto understand aggregate behaviors and make usefulprogram changes, as well as to provide substantiated,auditable performance data. Automation offers sig-nifi cant advantages in data collection and speed ofanalysis. Reporting can help organizations measurethe results of their outreach efforts more effectively.Demonstration of results against required objectives,such as the Health Effectiveness Data and In for ma -tion Set and other programs from accrediting andregulatory bodies, may enable organizations to satis-fy these requirements more efficiently with a betteroutcome.
5. Analytics. Analytics underlies useful personaliza-tion. Applying a detailed scoring model helps the
The ability to deliver automated patient communication programs efficientlyand effectively may offer additional distinct advantages, including increased scopeand improved health economics.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 24

25www.AHDBonline.comVOL. 1 NO. 9
Automated Communication Strategies
evaluation of several key factors,such as which patients are mostlikely to take action, and whetherthey are being contacted too lit-tle, too much, or the right amountusing the best method. At a deep-er level, analytics also providesinsight on the best approach forcontacting patients, evaluatingsuch treatment strategies as thebest calling windows, media(voice, e-mail, text message, or acombination of these), persona,retry strategy, among near-infinitecombinations of these.
The impact of automated com-munication is further enhancedby tailoring interventional strate-gies on a per-patient basis, com-bining analysis of historicalpatient clinical data along withactual patient response data. Forexample, an analytics-enabledsolution may initially help deter-mine which patients should becontacted first, based on drug andtherapeutic categories, number ofmaintenance medications, com-plexity of medication regimen, orpatient demographics.By looking at the history of patient refill behaviors,
the system can determine whether, when, and how fre-quently to communicate with the individual patient.Over time, the system can become increasingly “intel-ligent” and better capable of determining the profile ofthe most receptive patients.
Results from automated systems capable of decision-making can support effective personalized communica-tions with many patients on an individualized basis. Thisprocess is sometimes referred to as “mass personalization.”
Automated Communication Improves BP Monitoringin Frail Elderly: New Study Results
The following study was developed to addressuncontrolled hypertension and the use of automatedcommunication in a patient cohort from the MedicareHealth Support (MHS) pilot program in Maryland andthe District of Columbia during a 2-month period(March 19, 2007-May 24, 2007).16
The Treat to Target (TTT) initiative approachesuncontrolled hypertension by the simple principle that
lower is better. The TTT also bases optimal targetranges on specific patient diagnoses, such as BP<140/90 mm Hg for patients with heart failure (HF)but BP <130/80 mm Hg for patients with diabetes.
For the present trial, a cohort of approximately 800patients was selected from the MHS pilot population,based on a primary diagnosis of HF or diabetes andrecently reported BP readings above the established tar-get range.16 Of these, 318 agreed to participate in a trialof an automated telephony system and home BP moni-toring. A matched cohort of 304 hypertensive benefici-aries continued to receive the usual nurse-based diseasemanagement services of the MHS program as a compar-ison group. The study examined whether frail, elderly(median age, 75 years) patients with hypertension werewilling and able to listen and respond to weekly auto-mated phone calls that provided support for therapeuticand medication regimens, while offering care supportpersonnel with weekly reporting on the results. Thestudy covered 2 areas—patient BP and patient adher-ence to specific antihypertensive regimens. The objec-
Auth
No
No Yes
Yes
Greeting callDynamic prompts
3rd party
Answering machine Message
retrieval with PIN
“Did you check your blood pressure?”
“What prevented you from
checking it?”“What were
the results?”Out oflimits
“Why not?”
My doctor discontinued Rx
I didn’t feel well
“Thank you”
I didn’t think it was working
I forgot
“Thank you”Immediate transfer to
care specialist
Within limits
“Did you take your medication?”
Figure 2 Survey Call Flow
Source: Montijo M, Ross M. Use of automated telephony to optimize blood pressure and medicationmanagement of hypertensive frail elderly patients. Presented at the Disease Management Associationof America 9th Annual Disease Management Leadership Forum and Integrated Case Summit;September 16, 2007; Las Vegas, NV.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 25

26 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
BUSINESS
tives were to improve quality of care and lower care sup-port personnel utilization.
The study posed a series of questions using branch-ing logic to generate targeted questioning of yes/no and multiple choice questions. Figure 2 depicts the for-mat of the survey, showing the nature of the logic, thelocation of the transfers to human clinical support, and
the types of questions asked. The main results of thissurvey were16:• 245 patients (87.5%) achieved systolic BP within
target or had marked improvement from baseline>160 mm Hg
• 302 patients (96.8%) achieved diastolic BP within target or significantly improved from baseline>100 mm Hg
• 66% of the contacts validated as a “live answer” (ie,the patient answered the call, or someone else in thehousehold handed the phone to the patient, afterwhich the patient validated)
• Of those responding, 581 (33%) completed theentire survey, and 33% were transferred to a caresupport specialist for additional assistance
• No difference was seen between the automatedtele-phony and nurse-contacted cohorts in percentachieving targeted systolic and diastolic BP or percentreceiving antihypertensive medication adjustment
• Cost of automated telephony for a BP reading was95% lower than using a care support representativeto retrieve the reading.Perhaps the most important outcome of this study
was that 174 patients (54% of the study group) hadtheir antihypertensive regimens altered based on surveyresponses.16 The clear inference is that frequent report-ing on patient BP and medication-taking behaviors,along with the ability to efficiently gather and analyzethat information, offers clinicians significant insightson ongoing titration of medication or other elements ofa therapeutic regimen.
Better Health and Health EconomicsResults of this study show how applying certain
forms of automated communication to treatmentadherence programs may potentially offer distinct
advantages to patients and organizations.16 In additionto the improvements in clinical outcomes delivered byregular communications, automating outreach pro-grams may enable MCOs and disease management/wellness programs to:• Reach out to more patients cost-effectively• Target and reach substantially more patients, and
enroll more patients overall into existing programsfor improved return on investment
• Consistently manage patient adherence across largepopulations
• Gain potential insights into patient medication-tak-ing and other relevant behaviors for further analysis
• Empower existing care support staff by drivinginbound, interested patients into the call center andby triaging the more acute or at-risk individuals.
ConclusionsIt is well understood that regular, consistent commu-
nications from care teams can mediate medication-tak-ing behaviors in many patients with chronic diseasesand, in many cases, the health outcomes are dependenton those behaviors. These communications comprise afocus area in healthcare that can be extended by usingmodern automated communications to augment otheroutreach strategies. Although all the data from the newstudy cited here are not in yet, automated communica-tions satisfying the criteria outlined in this article aredemonstrating some ability to connect with, and medi-ate behavior in, large populations of chronically illpatients. Our hope is that in the future, automated com-munications systems will enable organizations to pro-vide communications at a scale that will improve healthoutcomes, both proximal and longer-term, for the mil-lions of “Toms” with chronic conditions. ■
References1. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med.2005;353:487-497.2. Pharmaceutical Safety Institute. Pharmaceutical Safety Institute andHarris Interactive Consumer Drug Safety Perception Survey Results.http://www.psisafety.org/images/InstituteHarrisSurvey.pdf. AccessedSeptember 12, 2008.3. Sud A, Kline-Rogers E, Fang J, et al. Reasons for non-adherence tocardiac medications in patients discharged with acute coronary symp-toms. Presented at the American College of Cardiology AnnualScientific Session; March 7-10, 2004; New Orleans, LA.4. Case Management Society of America. Case Management AdherenceGuidelines, Version 2.0. http://www.cmsa.org/portals/0/pdf/CMAG2.pdf.Accessed June 7, 2008.5. Sabaté E, ed. Adherence to long-term therapies: evidence for action[monograph online]. World Health Organization; 2003. http://whqlibdoc.who.int/publications/2003/9241545992.pdf. Accessed June 9, 2008.6. McCarthy R. The price you pay for the drug not taken. Bus Health.1998;16:27-33. http://findarticles.com/p/articles/mi_m0903/is_n10_v16/ai_n27541886/pg_1?tag=artBody;col1. Accessed October 22, 2008.
Perhaps the most important outcome of this study was that 174 patients (54% of the study group) had their antihypertensiveregimens altered.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 26

27www.AHDBonline.comVOL. 1 NO. 9
Automated Communication Strategies
Stakeholder PerspectiveEfficient Automated Call System Improves Adherence, but What about Net Costs?
PAYERS/FINANCIAL OFFICERS: Managed careorganizations (MCOs) strive to deliver the highestlevel of value for each healthcare dollar that theorganization must spend. An MCO incurs anexpense to buy pharmaceuticals for its membersand, in turn, those medications should improve thehealth of the member/patient. The MCO, in return,wants its members to improve their health, main-tain their current health, or avoid catastrophichealth problems because of their member’s adher-ence to a prescribed medication regimen. Dr Rossdescribes an outgoing automated phone calling system that he reports improves adherence forpatients in following their prescribed antihyperten-sive medication regimen. He reports results of hisrecent study that follows 304 elderly patients withhypertension who are matched to another 304 con-trol patients.
An automated phone system makes outboundcalls to these patients. Dr Ross reports this automat-ed calling system as having variable costs that are lessexpensive than those calls initiated from the clinicaloutreach call centers of disease management compa-nies. It is appropriate to note that Dr Ross is VicePresident of Healthcare for Varolii Corporation,which provides such automated calling systems.
At MCOs, the chief medical officers, medicaldirectors, directors of pharmacy, directors of utiliza-
tion management, and directors of quality manage-ment are all interested in methods that improvepatient compliance, improve outcomes for patients,or improve the documentation of that compliance.
The chief financial officers of these organizations,however, want to know if these programs thatimprove medication adherence will also save theMCO money. The present article clearly addressesthe first issue by proposing a method where an MCOcan efficiently improve pharmacy compliance. Inthat, this article is useful for those involved in med-ication compliance.
The article, however, does not address the chieffinancial officer’s usual question, “How does effi-ciently increasing medication adherence save theMCO money in the long run?” That question isimportant and is worthy of further research, by DrRoss or by others. It could be reframed as, “Will thecash outflows spent to operate an automated callcenter yield a positive net present value when meas-ured against the future savings (ie, decreased cashoutflows) in medical expenses on those same target-ed patients?”
Geoffrey P. Cole, MD, MBAChief Medical OfficerHealth Plan SelectAthens, Georgia
7. Kung HC, Hoyert DL, Xu JQ, Murphy SL. Deaths: final data for 2005.Natl Vital Stat Rep. 2008;56:1-120. 8. Cherry DK, Woodwell DA, Rechtsteiner EA. National AmbulatoryMedical Care Survey: 2005 summary. Adv Data. 2007;387:1-39.9. Centers for Disease Control and Prevention. National Center forHealth Statistics. Health, United States, 2007. Hyattsville, MD: USDepartment of Health and Human Services; 2007. http://www.cdc.gov/nchs/data/hus/hus07.pdf. Accessed June 8, 2008. 10. Stewart MA. Effective physician-patient communication and healthoutcomes: a review. Can Med Assoc J [serial online]. 1995;152:1423-1433.http://www.cmaj.ca/cgi/content/abstract/152/9/1423. Accessed June 7, 2008.11. HDI Advisory Services. Advisory Services Q&A page. http://www.thinkhdi.com/library/deliverfile.aspx?filecontentid=350. AccessedJune 12, 2008.12. McCall N, Cromwell J, Bernard S. Evaluation of Phase I of MedicareHealth Support (Formerly Voluntary Chronic Care Improvement) PilotProgram Under Traditional Fee-for-Service Medicare. Baltimore, MD: RTI
International; June 2007. Project No: 0207960.002. Contract No: 500-00-0022. Sponsored by Centers for Medicare & Medicaid Services. 13. Friedman RH, Kazis LE, Jette A, et al. A telecommunications systemfor monitoring and counseling patients with hypertension: impact onmedication adherence and blood pressure control. Am J Hypertens.1996;9:285-292.14. Boehm E, for Forrester Research Inc. Designing interactions for anaging population. July 2007. http://www.forrester.com/Research/PDF/0,5110,42827,00.pdf. Accessed November 6, 2008.15. Non-compliance costs drug industry dear. September 6, 2004.http://www.in-pharmatechnologist.com/layout/set/print/content/view/print/183261. Accessed October 22, 2008. 16. Montijo M, Ross M. Use of automated telephony to optimize bloodpressure and medication management of hypertensive frail elderlypatients. Presented at the Disease Management Association of America9th Annual Disease Management Leadership Forum and IntegratedCase Summit; September 16, 2007; Las Vegas, NV.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:47 AM Page 27

When Treating Your Patients:
• Evaluate for other treatable etiologies of anemia (iron, folate, or B12 defi ciency, hemolysis, or bleeding) to treat appropriately
• PROCRIT therapy should not be initiated at hemoglobin (Hb) levels 10 g/dL
• The dose of PROCRIT should be titrated for each patient to achieve and maintain the lowest Hb level suffi cient to avoid the need for red blood cell (RBC) transfusion
• The rate of Hb increase should not exceed 1 g/dL in any 2-week period
• Monitor Hb weekly until stable, and then regularly during therapy
For Anemic Cancer Patients With Metastatic, Non-myeloid Malignancies Receiving Chemotherapy…
CONTROLTHE RESPONSE
MANAGE HEMOGLOBIN AND REDUCE TRANSFUSIONS
43156ALT_Control Ad_V1 1-2 11/11/08 6:11:14 PM
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 28

PROCRIT Indication PROCRIT is indicated for the treatment of anemia due to the effect of concomitantly administered chemotherapy based on studies that have shown a reduction in the need for RBC transfusions in patients with metastatic, non-myeloid malignancies receiving chemotherapy for a minimum of 2 months. Studies to determine whether PROCRIT increases mortality or decreases progression-free/recurrence-free survival are ongoing.
• PROCRIT is not indicated for use in patients receiving hormonal agents, therapeutic biologic products, or radiotherapy unless receivingconcomitant myelosuppressive chemotherapy.
• PROCRIT is not indicated for patients receiving myelosuppressive therapy when the anticipated outcome is cure due to the absence of studies that adequately characterize the impact of PROCRIT on progression-free and overall survival (see WARNINGS: Increased Mortality and/or Increased Risk of Tumor Progression or Recurrence).
• PROCRIT is not indicated for the treatment of anemia in cancer patients due to other factors such as iron or folate deficiencies, hemolysis, or gastrointestinal bleeding (see PRECAUTIONS: Lack or Loss of Response).
• PROCRIT use has not been demonstrated in controlled clinical trials to improve symptoms of anemia, quality of life, fatigue, or patient well-being.
Important Safety Information
WARNINGS: INCREASED MORTALITY, SERIOUS CARDIOVASCULAR and THROMBOEMBOLIC EVENTS, and INCREASED RISK OF TUMOR PROGRESSION OR RECURRENCE
Renal failure: Patients experienced greater risks for death and serious cardiovascular events when administered erythropoiesis-stimulating agents (ESAs) to target higher versuslower hemoglobin levels (13.5 vs. 11.3 g/dL; 14 vs. 10 g/dL) in two clinical studies. Individualize dosing to achieve and maintain hemoglobin levels within the range of 10 to 12 g/dL.
Cancer: • ESAs shortened overall survival and/or increased the risk of
tumor progression or recurrence in some clinical studies in patients with breast, non-small cell lung, head and neck, lymphoid, and cervical cancers (see WARNINGS: Table 1).
• To decrease these risks, as well as the risk of serious cardio- and thrombovascular events, use the lowest dose needed to avoid red blood cell transfusion.
• Use ESAs only for treatment of anemia due to concomitant myelosuppressive chemotherapy.
• ESAs are not indicated for patients receiving myelosuppressivetherapy when the anticipated outcome is cure.
• Discontinue following the completion of a chemotherapy course.
Perisurgery: PROCRIT® (Epoetin alfa) increased the rate of deep venous thromboses in patients not receiving prophylactic anticoagulation. Consider deep venous thrombosis prophylaxis.
Contraindications• PROCRIT is contraindicated in patients with uncontrolled hypertension
or with known hypersensitivity to albumin (human) or mammalian cell-derived products.
Additional Important Safety Information
• Patients with chronic renal failure experienced greater risks for death and serious cardiovascular events (including myocardial infarction, stroke, congestive heart failure, and hemodialysis vascular access thrombosis) when administered ESAs to target higher versus lower hemoglobin levels (13.5 vs.11.3 g/dL; 14 vs. 10 g/dL) in two clinicalstudies; these risks also increased in controlled clinical trials of patients with cancer. A rate of hemoglobin rise of >1 g/dL over 2 weeks may contribute to these risks.
• PROCRIT therapy should not be initiated at hemoglobin levels 10 g/dL.
• The dose of PROCRIT should be titrated for each patient to achieve and maintain the lowest hemoglobin level suffi cient to avoid the need for blood transfusion.
• When the hemoglobin reaches a level needed to avoid transfusion or, increases by more than 1 g/dL in a 2-week period, the PROCRIT dose should be reduced by 25%. Withhold the dose of PROCRIT if the hemoglobin exceeds a level needed to avoid transfusion. Restart dose at 25% below the previous dose when the hemoglobin approaches a level where transfusions may be required. Discontinue if after 8 weeks of therapy there is no response as measured by hemoglobin levels or if transfusions are still required.
• Monitor hemoglobin regularly during therapy, weekly until hemoglobin becomes stable.
• Cases of pure red cell aplasia (PRCA) and of severe anemia, with or without other cytopenias, associated with neutralizing antibodies to erythropoietin have been reported in patients treated with PROCRIT; predominantly in patients with chronic renal failure receiving PROCRIT by subcutaneous administration. If any patient develops a sudden lossof response to PROCRIT, accompanied by severe anemia and low reticulocyte count, and anti-erythropoietin antibody-associated anemia is suspected, withhold PROCRIT and other erythropoietic proteins. Contact ORTHO BIOTECH (1-888-2ASKOBI or 1-888-227-5624) to perform assays for binding and neutralizing antibodies. If erythropoietin antibody-mediated anemia is confirmed, PROCRIT should be permanently discontinued and patients should not be switched to other erythropoietic proteins.
• The safety and effi cacy of PROCRIT therapy have not been established in patients with a known history of a seizure disorder or underlyinghematologic disease (e.g., sickle cell anemia, myelodysplastic syndromes, or hypercoagulable disorders).
• In some female patients, menses have resumed following PROCRIT therapy; the possibility of pregnancy should be discussed and the need for contraception evaluated.
• Prior to and regularly during PROCRIT therapy monitor iron status; transferrin saturation should be 20% and ferritin should be
100 ng/mL. During therapy absolute or functional iron deficiency may develop and all patients will eventually require supplemental iron to adequately support erythropoiesis stimulated by PROCRIT.
• Treatment of patients with grossly elevated serum erythropoietin levels (e.g., >200 mUnits/mL) is not recommended.
• During PROCRIT therapy, blood pressure should be monitored carefully and aggressively managed, particularly in patients with an underlying history of hypertension or cardiovascular disease.
• Seizures in PROCRIT-treated patients have been reported in the context of a signifi cant increase in hemoglobin from baseline; increasesin blood pressure were not always observed; and patients may have had other underlying central nervous system pathology.
• The most commonly reported side effects (>10%) for PROCRIT in clinical trials were pyrexia, diarrhea, nausea, vomiting, edema, asthenia, fatigue, shortness of breath, paresthesia, and upper respiratory infection.
Manufactured by: Amgen Inc., Thousand Oaks, California 91320-1789Distributed by: Ortho Biotech Products, L.P., Bridgewater, New Jersey 08807-0914 © Ortho Biotech Products, L.P. 2008 11/08 08PCTC2487 308470
Please see Brief Summary of Prescribing Information, including Boxed WARNINGS, on adjacent page.
43156ALT_Control Ad_V1 1-2 11/11/08 6:11:14 PM
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 29

BRIEF SUMMARY OF PROCRIT® PRESCRIBING INFORMATION FOR THE TREATMENT OF ANEMIA INCANCER PATIENTS ON CHEMOTHERAPY
PROCRIT®
(Epoetin alfa)
FOR INJECTION
FOR FULL PRESCRIBING INFORMATION FOR ALL INDICATIONS,REFER TO THE PHYSICIANS’ DESK REFERENCE®
INDICATIONS AND USAGE
PROCRIT® is indicated for the treatment of anemia due to the effect of concomitantly administeredchemotherapy based on studies that have shown a reduction in the need for RBC transfusions in patients withmetastatic, non-myeloid malignancies receiving chemotherapy for a minimum of 2 months. Studies to determinewhether PROCRIT® increases mortality or decreases progression-free/recurrence-free survival are ongoing.
• PROCRIT® is not indicated for use in patients receiving hormonal agents, therapeutic biologic products, orradiotherapy unless receiving concomitant myelosuppressive chemotherapy.
• PROCRIT® is not indicated for patients receiving myelosuppressive therapy when the anticipated outcomeis cure due to the absence of studies that adequately characterize the impact of PROCRIT® on progression-free and overall survival (see WARNINGS: Increased Mortality and/or Increased Risk of Tumor Progressionor Recurrence).
• PROCRIT ® is not indicated for the treatment of anemia in cancer patients due to other factors such as ironor folate deficiencies, hemolysis, or gastrointestinal bleeding (see PRECAUTIONS: Lack or Loss ofResponse).
• PROCRIT ® use has not been demonstrated in controlled clinical trials to improve symptoms of anemia,quality of life, fatigue, or patient well-being.
CONTRAINDICATIONSPROCRIT® is contraindicated in patients with: 1. Uncontrolled hypertension. 2. Known hypersensitivity tomammalian cell-derived products. 3. Known hypersensitivity to Albumin (Human).
WARNINGS
Pediatrics
Risk in Premature InfantsThe multidose preserved formulation contains benzyl alcohol. Benzyl alcohol has been reported to beassociated with an increased incidence of neurological and other complications in premature infants which aresometimes fatal.
Adults
Increased Mortality, Serious Cardiovascular and Thromboembolic EventsPatients with chronic renal failure experienced greater risks for death and serious cardiovascular events whenadministered erythropoiesis-stimulating agents (ESAs) to target higher versus lower hemoglobin levels (13.5vs. 11.3 g/dL; 14 vs. 10 g/dL) in two clinical studies. Patients with chronic renal failure and an insufficienthemoglobin response to ESA therapy may be at even greater risk for cardiovascular events and mortality thanother patients. PROCRIT® and other ESAs increased the risks for death and serious cardiovascular events incontrolled clinical trials of patients with cancer. These events included myocardial infarction, stroke, congestiveheart failure, and hemodialysis vascular access thrombosis. A rate of hemoglobin rise of > 1 g/dL over 2 weeksmay contribute to these risks.
In a randomized prospective trial, 1432 anemic chronic renal failure patients who were not undergoing dialysiswere assigned to Epoetin alfa (rHuEPO) treatment targeting a maintenance hemoglobin concentration of 13.5 g/dL or 11.3 g/dL. A major cardiovascular event (death, myocardial infarction, stroke, or hospitalization forcongestive heart failure) occurred among 125 (18%) of the 715 patients in the higher hemoglobin groupcompared to 97 (14%) among the 717 patients in the lower hemoglobin group (HR 1.3, 95% CI: 1.0, 1.7,p = 0.03).
Increased risk for serious cardiovascular events was also reported from a randomized, prospective trial of 1265hemodialysis patients with clinically evident cardiac disease (ischemic heart disease or congestive heartfailure). In this trial, patients were assigned to PROCRIT® treatment targeted to a maintenance hematocrit ofeither 42 ± 3% or 30 ± 3%. Increased mortality was observed in 634 patients randomized to a targethematocrit of 42% [221 deaths (35% mortality)] compared to 631 patients targeted to remain at a hematocritof 30% [185 deaths (29% mortality)]. The reason for the increased mortality observed in this study is unknown,however, the incidence of non-fatal myocardial infarctions (3.1% vs. 2.3%), vascular access thromboses (39%vs. 29%), and all other thrombotic events (22% vs. 18%) were also higher in the group randomized to achievea hematocrit of 42%. An increased incidence of thrombotic events has also been observed in patients withcancer treated with erythropoietic agents.
In a randomized controlled study (referred to as Cancer Study 1 - the ‘BEST’ study) with another ESA in 939women with metastatic breast cancer receiving chemotherapy, patients received either weekly Epoetin alfa orplacebo for up to a year. This study was designed to show that survival was superior when an ESA wasadministered to prevent anemia (maintain hemoglobin levels between 12 and 14 g/dL or hematocrit between36% and 42%). The study was terminated prematurely when interim results demonstrated that a highermortality at 4 months (8.7% vs. 3.4%) and a higher rate of fatal thrombotic events (1.1% vs. 0.2%) in the first4 months of the study were observed among patients treated with Epoetin alfa. Based on Kaplan-Meierestimates, at the time of study termination, the 12-month survival was lower in the Epoetin alfa group than inthe placebo group (70% vs. 76%; HR 1.37, 95% CI: 1.07, 1.75; p = 0.012).
A systematic review of 57 randomized controlled trials (including Cancer Studies 1 and 5 - the ‘BEST’ and‘ENHANCE’ studies) evaluating 9353 patients with cancer compared ESAs plus red blood cell transfusion withred blood cell transfusion alone for prophylaxis or treatment of anemia in cancer patients with or withoutconcurrent antineoplastic therapy. An increased relative risk of thromboembolic events (RR 1.67, 95% CI: 1.35,2.06; 35 trials and 6769 patients) was observed in ESA-treated patients. An overall survival hazard ratio of 1.08(95% CI: 0.99, 1.18; 42 trials and 8167 patients) was observed in ESA-treated patients.
An increased incidence of deep vein thrombosis (DVT) in patients receiving Epoetin alfa undergoing surgicalorthopedic procedures has been observed (see ADVERSE REACTIONS, Surgery Patients: Thrombotic/VascularEvents in full Prescribing Information). In a randomized controlled study (referred to as the ‘SPINE’ study), 681adult patients, not receiving prophylactic anticoagulation and undergoing spinal surgery, received either 4 doses of 600 U/kg Epoetin alfa (7, 14, and 21 days before surgery, and the day of surgery) and standard ofcare (SOC) treatment, or SOC treatment alone. Preliminary analysis showed a higher incidence of DVT,
determined by either Color Flow Duplex Imaging or by clinical symptoms, in the Epoetin alfa group [16 patients(4.7%)] compared to the SOC group [7 patients (2.1%)]. In addition, 12 patients in the Epoetin alfa group and 7 patients in the SOC group had other thrombotic vascular events. Deep venous thrombosis prophylaxis shouldbe strongly considered when ESAs are used for the reduction of allogeneic RBC transfusions in surgical patients(see BOXED WARNINGS and DOSAGE AND ADMINISTRATION in full Prescribing Information).
Increased mortality was also observed in a randomized placebo-controlled study of PROCRIT® in adult patientswho were undergoing coronary artery bypass surgery (7 deaths in 126 patients randomized to PROCRIT®
versus no deaths among 56 patients receiving placebo). Four of these deaths occurred during the period ofstudy drug administration and all four deaths were associated with thrombotic events. ESAs are not approvedfor reduction of allogeneic red blood cell transfusions in patients scheduled for cardiac surgery.
Increased Mortality and/or Increased Risk of Tumor Progression or Recurrence Erythropoiesis-stimulating agents resulted in decreased locoregional control/progression-free survival and/oroverall survival (see Table 1). These findings were observed in studies of patients with advanced head and neckcancer receiving radiation therapy (Cancer Studies 5 and 6), in patients receiving chemotherapy for metastaticbreast cancer (Cancer Study 1) or lymphoid malignancy (Cancer Study 2), and in patients with non-small cell lungcancer or various malignancies who were not receiving chemotherapy or radiotherapy (Cancer Studies 7 and 8).
Table 1: Randomized, Controlled Trials with Decreased Survival and/or Decreased Locoregional Control
Adverse Achieved Outcome for
Hemoglobin Hemoglobin Primary ESA-containingStudy / Tumor / (n) Target (Median Q1,Q3) Endpoint Arm
Chemotherapy
Cancer Study 1Metastatic breast 12-14 g/dL 12.9 g/dL 12-month overall Decreased 12-monthcancer (n=939) 12.2, 13.3 g/dL survival survival
Cancer Study 2Lymphoid 13-15 g/dL (M) 11.0 g/dL Proportion of Decreased overallmalignancy (n=344) 13-14 g/dL (F) 9.8, 12.1 g/dL patients achieving survival
a hemoglobinresponse
Cancer Study 3Early breast 12.5-13 g/dL 13.1 g/dL Relapse-free and Decreased 3 yr.cancer (n=733) 12.5, 13.7 g/dL overall survival relapse-free and
overall survival
Cancer Study 4Cervical Cancer 12-14 g/dL 12.7 g/dL Progression-free Decreased 3 yr.(n=114) 12.1, 13.3 g/dL and overall survival progression-free
and locoregional and overall survivalcontrol and locoregional
control
Radiotherapy Alone
Cancer Study 5Head and neck ≥15 g/dL (M) Not available Locoregional Decreased 5-yearcancer (n=351) ≥14 g/dL (F) progression-free locoregional
survival progression-free survival
Decreased overallsurvival
Cancer Study 6Head and neck 14-15.5 g/dL Not available Locoregional Decreasedcancer (n=522) disease control locoregional
disease control
No Chemotherapy or Radiotherapy
Cancer Study 7Non-small cell 12-14 g/dL Not available Quality of life Decreased overalllung cancer (n=70) survival
Cancer Study 8Non-myeloid 12-13 g/dL 10.6 g/dL RBC transfusions Decreased overallmalignancy (n=989) 9.4, 11.8 g/dL survival
Decreased overall survival:Cancer Study 1 (the ‘BEST’ study) was previously described (see WARNINGS: Increased Mortality, SeriousCardiovascular and Thromboembolic Events). Mortality at 4 months (8.7% vs. 3.4%) was significantly higher inthe Epoetin alfa arm. The most common investigator-attributed cause of death within the first 4 months wasdisease progression; 28 of 41 deaths in the Epoetin alfa arm and 13 of 16 deaths in the placebo arm wereattributed to disease progression. Investigator assessed time to tumor progression was not different betweenthe two groups. Survival at 12 months was significantly lower in the Epoetin alfa arm (70% vs. 76%, HR 1.37,95% CI: 1.07, 1.75; p = 0.012).
Cancer Study 2 was a Phase 3, double-blind, randomized (darbepoetin alfa vs. placebo) study conducted in 344anemic patients with lymphoid malignancy receiving chemotherapy. With a median follow-up of 29 months,overall mortality rates were significantly higher among patients randomized to darbepoetin alfa as comparedto placebo (HR 1.36, 95% CI: 1.02, 1.82).
Cancer Study 7 was a Phase 3, multicenter, randomized (Epoetin alfa vs. placebo), double-blind study, in whichpatients with advanced non-small cell lung cancer receiving only palliative radiotherapy or no active therapywere treated with Epoetin alfa to achieve and maintain hemoglobin levels between 12 and 14 g/dL. Followingan interim analysis of 70 of 300 patients planned, a significant difference in survival in favor of the patients onthe placebo arm of the trial was observed (median survival 63 vs. 129 days; HR 1.84; p = 0.04).
Cancer Study 8 was a Phase 3, double-blind, randomized (darbepoetin alfa vs. placebo), 16-week study in 989anemic patients with active malignant disease, neither receiving nor planning to receive chemotherapy orradiation therapy. There was no evidence of a statistically significant reduction in proportion of patientsreceiving RBC transfusions. The median survival was shorter in the darbepoetin alfa treatment group (8months) compared with the placebo group (10.8 months); HR 1.30, 95% CI: 1.07, 1.57.
Decreased progression-free survival and overall survival:Cancer Study 3 (the ‘PREPARE’ study) was a randomized controlled study in which darbepoetin alfa wasadministered to prevent anemia conducted in 733 women receiving neo-adjuvant breast cancer treatment.After a median follow-up of approximately 3 years, the survival rate (86% vs. 90%, HR 1.42, 95% CI: 0.93, 2.18)and relapse-free survival rate (72% vs. 78%, HR 1.33, 95% CI: 0.99, 1.79) were lower in the darbepoetin alfa-treated arm compared to the control arm.
Cancer Study 4 (protocol GOG 191) was a randomized controlled study that enrolled 114 of a planned 460cervical cancer patients receiving chemotherapy and radiotherapy. Patients were randomized to receiveEpoetin alfa to maintain hemoglobin between 12 and 14 g/dL or to transfusion support as needed. The studywas terminated prematurely due to an increase in thromboembolic events in Epoetin alfa-treated patientscompared to control (19% vs. 9%). Both local recurrence (21% vs. 20%) and distant recurrence (12% vs. 7%)were more frequent in Epoetin alfa-treated patients compared to control. Progression-free survival at 3 yearswas lower in the Epoetin alfa-treated group compared to control (59% vs. 62%, HR 1.06, 95% CI: 0.58, 1.91).Overall survival at 3 years was lower in the Epoetin alfa-treated group compared to control (61% vs. 71%, HR1.28, 95% CI: 0.68, 2.42).
Cancer Study 5 (the ‘ENHANCE’ study) was a randomized controlled study in 351 head and neck cancerpatients where Epoetin beta or placebo was administered to achieve target hemoglobin of 14 and 15 g/dL for women and men, respectively. Locoregional progression-free survival was significantly shorter inpatients receiving Epoetin beta (HR 1.62, 95% CI: 1.22, 2.14; p = 0.0008) with a median of 406 days Epoetinbeta vs. 745 days placebo. Overall survival was significantly shorter in patients receiving Epoetin beta (HR 1.39,95% CI: 1.05, 1.84; p = 0.02).
WARNINGS: INCREASED MORTALITY, SERIOUS CARDIOVASCULAR and THROMBOEMBOLIC EVENTS,and INCREASED RISK OF TUMOR PROGRESSION OR RECURRENCE
Renal failure: Patients experienced greater risks for death and serious cardiovascular events whenadministered erythropoiesis-stimulating agents (ESAs) to target higher versus lower hemoglobinlevels (13.5 vs. 11.3 g/dL; 14 vs. 10 g/dL) in two clinical studies. Individualize dosing to achieve andmaintain hemoglobin levels within the range of 10 to 12 g/dL.
Cancer:• ESAs shortened overall survival and/or increased the risk of tumor progression or recurrence in
some clinical studies in patients with breast, non-small cell lung, head and neck, lymphoid, andcervical cancers (see WARNINGS: Table 1).
• To decrease these risks, as well as the risk of serious cardio- and thrombovascular events, usethe lowest dose needed to avoid red blood cell transfusion.
• Use ESAs only for treatment of anemia due to concomitant myelosuppressive chemotherapy.
• ESAs are not indicated for patients receiving myelosuppressive therapy when the anticipatedoutcome is cure.
• Discontinue following the completion of a chemotherapy course.
Perisurgery: PROCRIT® increased the rate of deep venous thromboses in patients not receiving prophylactic anticoagulation. Consider deep venous thrombosis prophylaxis.
(See WARNINGS: Increased Mortality, Serious Cardiovascular and Thromboembolic Events,WARNINGS: Increased Mortality and/or Increased Risk of Tumor Progression or Recurrence,INDICATIONS AND USAGE, and DOSAGE AND ADMINISTRATION in full Prescribing Information.)
43156ALT_Control Ad_V1 3-4 11/11/08 6:12:25 PM
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 30

Decreased locoregional control:Cancer Study 6 (DAHANCA 10) was conducted in 522 patients with primary squamous cell carcinoma of thehead and neck receiving radiation therapy randomized to darbepoetin alfa with radiotherapy or radiotherapyalone. An interim analysis on 484 patients demonstrated that locoregional control at 5 years was significantlyshorter in patients receiving darbepoetin alfa (RR 1.44, 95% CI: 1.06, 1.96; p = 0.02). Overall survival was shorterin patients receiving darbepoetin alfa (RR 1.28, 95% CI: 0.98, 1.68; p = 0.08).
Pure Red Cell AplasiaCases of pure red cell aplasia (PRCA) and of severe anemia, with or without other cytopenias, associated withneutralizing antibodies to erythropoietin have been reported in patients treated with PROCRIT®. This has beenreported predominantly in patients with chronic renal failure (CRF) receiving PROCRIT® by subcutaneousadministration.Any patient who develops a sudden loss of response to PROCRIT®, accompanied by severe anemiaand low reticulocyte count, should be evaluated for the etiology of loss of effect, including the presence ofneutralizing antibodies to erythropoietin (see PRECAUTIONS: Lack or Loss of Response). If anti-erythropoietinantibody-associated anemia is suspected, withhold PROCRIT® and other erythropoietic proteins. Contact ORTHO BIOTECH at 1 888 2ASK OBI (1-888-227-5624) to perform assays for binding and neutralizing antibodies.PROCRIT® should be permanently discontinued in patients with antibody-mediated anemia. Patients should notbe switched to other erythropoietic proteins as antibodies may cross-react (see ADVERSE REACTIONS:Immunogenicity).
Albumin (Human)
PROCRIT® contains albumin, a derivative of human blood. Based on effective donor screening and productmanufacturing processes, it carries an extremely remote risk for transmission of viral diseases. A theoreticalrisk for transmission of Creutzfeldt-Jakob disease (CJD) also is considered extremely remote. No cases oftransmission of viral diseases or CJD have ever been identified for albumin.
PRECAUTIONSThe parenteral administration of any biologic product should be attended by appropriate precautions in caseallergic or other untoward reactions occur (see CONTRAINDICATIONS). In clinical trials, while transient rasheswere occasionally observed concurrently with PROCRIT® therapy, no serious allergic or anaphylactic reactionswere reported (see ADVERSE REACTIONS in full Prescribing Information for more information regarding allergicreactions).
The safety and efficacy of PROCRIT® therapy have not been established in patients with a known history of aseizure disorder or underlying hematologic disease (eg, sickle cell anemia, myelodysplastic syndromes, orhypercoagulable disorders).
In some female patients, menses have resumed following PROCRIT® therapy; the possibility of pregnancy shouldbe discussed and the need for contraception evaluated.
Hematology: Exacerbation of porphyria has been observed rarely in patients with CRF treated with PROCRIT®.However, PROCRIT® has not caused increased urinary excretion of porphyrin metabolites in normal volunteers,even in the presence of a rapid erythropoietic response. Nevertheless, PROCRIT® should be used with cautionin patients with known porphyria.
In preclinical studies in dogs and rats, but not in monkeys, PROCRIT® therapy was associated with subclinicalbone marrow fibrosis. Bone marrow fibrosis is a known complication of CRF in humans and may be related tosecondary hyperparathyroidism or unknown factors. The incidence of bone marrow fibrosis was not increasedin a study of adult patients on dialysis who were treated with PROCRIT® for 12 to 19 months, compared to theincidence of bone marrow fibrosis in a matched group of patients who had not been treated with PROCRIT®.
Cancer patients should have hemoglobin measured once a week until hemoglobin has been stabilized, andmeasured periodically thereafter.
Lack or Loss of Response: If the patient fails to respond or to maintain a response to doses within therecommended dosing range, the following etiologies should be considered and evaluated: 1. Iron deficiency:Virtually all patients will eventually require supplemental iron therapy (see IRON EVALUATION); 2. Underlyinginfectious, inflammatory, or malignant processes; 3. Occult blood loss; 4. Underlying hematologic diseases (ie, thalassemia, refractory anemia, or other myelodysplastic disorders); 5. Vitamin deficiencies: Folic acid orvitamin B12; 6. Hemolysis; 7. Aluminum intoxication; 8. Osteitis fibrosa cystica; 9. Pure Red Cell Aplasia (PRCA)or anti-erythropoietin antibody-associated anemia: In the absence of another etiology, the patient should beevaluated for evidence of PRCA and sera should be tested for the presence of antibodies to erythropoietin (seeWARNINGS: Pure Red Cell Aplasia).
Iron Evaluation: During PROCRIT® therapy, absolute or functional iron deficiency may develop. Functional irondeficiency, with normal ferritin levels but low transferrin saturation, is presumably due to the inability tomobilize iron stores rapidly enough to support increased erythropoiesis. Transferrin saturation should be atleast 20% and ferritin should be at least 100 ng/mL.
Prior to and during PROCRIT® therapy, the patient’s iron status, including transferrin saturation (serum irondivided by iron binding capacity) and serum ferritin, should be evaluated. Virtually all patients will eventuallyrequire supplemental iron to increase or maintain transferrin saturation to levels which will adequately supporterythropoiesis stimulated by PROCRIT®.
Drug Interaction: No evidence of interaction of PROCRIT® with other drugs was observed in the course ofclinical trials.
Carcinogenesis, Mutagenesis, and Impairment of Fertility: Carcinogenic potential of PROCRIT® has notbeen evaluated. PROCRIT® does not induce bacterial gene mutation (Ames Test), chromosomal aberrations inmammalian cells, micronuclei in mice, or gene mutation at the HGPRT locus. In female rats treated IV withPROCRIT®, there was a trend for slightly increased fetal wastage at doses of 100 and 500 Units/kg.
Pregnancy Category C: PROCRIT® has been shown to have adverse effects in rats when given in doses 5 times the human dose. There are no adequate and well-controlled studies in pregnant women. PROCRIT®
should be used during pregnancy only if potential benefit justifies the potential risk to the fetus.
In studies in female rats, there were decreases in body weight gain, delays in appearance of abdominal hair,delayed eyelid opening, delayed ossification, and decreases in the number of caudal vertebrae in the F1 fetusesof the 500 Units/kg group. In female rats treated IV, there was a trend for slightly increased fetal wastage atdoses of 100 and 500 Units/kg. PROCRIT® has not shown any adverse effect at doses as high as 500 Units/kgin pregnant rabbits (from day 6 to 18 of gestation).
Nursing Mothers: Postnatal observations of the live offspring (F1 generation) of female rats treated withPROCRIT® during gestation and lactation revealed no effect of PROCRIT® at doses of up to 500 Units/kg. Therewere, however, decreases in body weight gain, delays in appearance of abdominal hair, eyelid opening, anddecreases in the number of caudal vertebrae in the F1 fetuses of the 500 Units/kg group. There were noPROCRIT®-related effects on the F2 generation fetuses.
It is not known whether PROCRIT® is excreted in human milk. Because many drugs are excreted in human milk,caution should be exercised when PROCRIT® is administered to a nursing woman.
Pediatric Use: See WARNINGS: Pediatrics
Pediatric Cancer Patients on Chemotherapy: The safety and effectiveness of PROCRIT® were evaluated in arandomized, double-blind, placebo-controlled, multicenter study (see CLINICAL EXPERIENCE, Weekly (QW)Dosing, Pediatric Patients in full Prescribing Information).
Geriatric Use: Insufficient numbers of patients age 65 or older were enrolled in clinical studies of PROCRIT®
for the treatment of anemia associated with pre-dialysis chronic renal failure, cancer chemotherapy, andZidovudine-treatment of HIV infection to determine whether they respond differently from younger subjects.
Information for Patients
Patients should be informed of the increased risks of mortality, serious cardiovascular events, thromboembolicevents, and increased risk of tumor progression or recurrence (see WARNINGS). In those situations in which thephysician determines that a patient or their caregiver can safely and effectively administer PROCRIT® at home,
instruction as to the proper dosage and administration should be provided. Patients should be instructed to readthe PROCRIT® Medication Guide and Patient Instructions for Use and should be informed that the MedicationGuide is not a disclosure of all possible side effects. Patients should be informed of the possible side effects ofPROCRIT® and of the signs and symptoms of allergic drug reaction and advised of appropriate actions. If homeuse is prescribed for a patient, the patient should be thoroughly instructed in the importance of proper disposaland cautioned against the reuse of needles, syringes, or drug product. A puncture-resistant container should beavailable for the disposal of used syringes and needles, and guidance provided on disposal of the full container.
Hypertension: Hypertension, associated with a significant increase in hemoglobin, has been noted rarely inpatients treated with PROCRIT®. Nevertheless, blood pressure in patients treated with PROCRIT® should bemonitored carefully, particularly in patients with an underlying history of hypertension or cardiovasculardisease.
Seizures: In double-blind, placebo-controlled trials, 3.2% (n = 2/63) of patients treated with PROCRIT® TIWand 2.9% (n = 2/68) of placebo-treated patients had seizures. Seizures in 1.6% (n = 1/63) of patients treatedwith PROCRIT® TIW occurred in the context of a significant increase in blood pressure and hematocrit frombaseline values. However, both patients treated with PROCRIT® also had underlying CNS pathology which mayhave been related to seizure activity.
In a placebo-controlled, double-blind trial utilizing weekly dosing with PROCRIT®, 1.2% (n = 2/168) of safety-evaluable patients treated with PROCRIT® and 1% (n = 1/165) of placebo-treated patients had seizures.Seizures in the patients treated with weekly PROCRIT® occurred in the context of a significant increase inhemoglobin from baseline values however significant increases in blood pressure were not seen. Thesepatients may have had other CNS pathology.
Thrombotic Events: In double-blind, placebo-controlled trials, 3.2% (n = 2/63) of patients treated withPROCRIT® TIW and 11.8% (n = 8/68) of placebo-treated patients had thrombotic events (eg, pulmonaryembolism, cerebrovascular accident), (see WARNINGS: Increased Mortality, Serious Cardiovascular andThromboembolic Events).
In a placebo-controlled, double-blind trial utilizing weekly dosing with PROCRIT®, 6.0% (n = 10/168) of safety-evaluable patients treated with PROCRIT® and 3.6% (n = 6/165) (p = 0.444) of placebo-treated patients hadclinically significant thrombotic events (deep vein thrombosis requiring anticoagulant therapy, embolic eventincluding pulmonary embolism, myocardial infarction, cerebral ischemia, left ventricular failure and thromboticmicroangiopathy). A definitive relationship between the rate of hemoglobin increase and the occurrence ofclinically significant thrombotic events could not be evaluated due to the limited schedule of hemoglobinmeasurements in this study.
The safety and efficacy of PROCRIT® were evaluated in a randomized, double-blind, placebo-controlled,multicenter study that enrolled 222 anemic patients ages 5 to 18 receiving treatment for a variety of childhoodmalignancies. Due to the study design (small sample size and the heterogeneity of the underlying malignanciesand of anti-neoplastic treatments employed), a determination of the effect of PROCRIT® on the incidence ofthrombotic events could not be performed. In the PROCRIT® arm, the overall incidence of thrombotic events was10.8% and the incidence of serious or life-threatening events was 7.2%.
ADVERSE REACTIONS
Immunogenicity
As with all therapeutic proteins, there is the potential for immunogenicity. Neutralizing antibodies toerythropoietin, in association with PRCA or severe anemia (with or without other cytopenias), have been reportedin patients receiving PROCRIT® (see WARNINGS: Pure Red Cell Aplasia) during post-marketing experience.
There has been no systematic assessment of immune responses, i.e., the incidence of either binding orneutralizing antibodies to PROCRIT®, in controlled clinical trials.
Where reported, the incidence of antibody formation is highly dependent on the sensitivity and specificity of theassay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assaymay be influenced by several factors including assay methodology, sample handling, timing of samplecollection, concomitant medications, and underlying disease. For these reasons, comparison of the incidenceof antibodies across products within this class (erythropoietic proteins) may be misleading.
Adverse Experiences Reported in Clinical TrialsIn double-blind, placebo-controlled studies of up to 3 months duration involving 131 cancer patients, adverseevents with an incidence > 10% in either patients treated with PROCRIT® or placebo-treated patients were asindicated below:
Percent of Patients Reporting Event
Patients Treated Placebo-treatedWith PROCRIT® Patients
Event (n = 63) (n = 68)
Pyrexia 29% 19%
Diarrhea 21%* 7%
Nausea 17%* 32%
Vomiting 17% 15%
Edema 17%* 1%
Asthenia 13% 16%
Fatigue 13% 15%
Shortness of Breath 13% 9%
Parasthesia 11% 6%
Upper Respiratory Infection 11% 4%
Dizziness 5% 12%
Trunk Pain 3%* 16%
* Statistically significant
Although some statistically significant differences between patients being treated with PROCRIT® and placebo-treated patients were noted, the overall safety profile of PROCRIT® appeared to be consistent with the diseaseprocess of advanced cancer. During double-blind and subsequent open-label therapy in which patients (n = 72for total exposure to PROCRIT®) were treated for up to 32 weeks with doses as high as 927 Units/kg, theadverse experience profile of PROCRIT® was consistent with the progression of advanced cancer.
Three hundred thirty-three (333) cancer patients enrolled in a placebo-controlled double-blind trial utilizingWeekly dosing with PROCRIT® for up to 4 months were evaluable for adverse events. The incidence of adverseevents was similar in both the treatment and placebo arms.
OVERDOSAGE
The expected manifestations of PROCRIT® overdosage include signs and symptoms associated with anexcessive and/or rapid increase in hemoglobin concentration, including any of the cardiovascular eventsdescribed in WARNINGS and listed in ADVERSE REACTIONS in full Prescribing Information. Patients receiving anoverdosage of PROCRIT® should be monitored closely for cardiovascular events and hematologicabnormalities. Polycythemia should be managed acutely with phlebotomy, as clinically indicated. Followingresolution of the effects due to PROCRIT® overdosage, reintroduction of PROCRIT® therapy should beaccompanied by close monitoring for evidence of rapid increases in hemoglobin concentration (>1 gm/dL per14 days). In patients with an excessive hematopoietic response, reduce the PROCRIT® dose in accordance withthe recommendations described in DOSAGE AND ADMINISTRATION in full Prescribing Information.
PROCRIT® (Epoetin alfa) FOR INJECTION
43156ALT_Control Ad_V1 3-4 11/11/08 6:12:25 PM
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 31

DOSAGE AND ADMINISTRATION
IMPORTANT: See BOXED WARNINGS and WARNINGS: Increased Mortality, Serious Cardiovascular andThromboembolic Events.
Prior to initiating treatment with PROCRIT® a hemoglobin should be obtained to establish that it is >10 to≤ 13 g/dL. The recommended dose of PROCRIT® is 300 Units/kg/day subcutaneously for 10 days beforesurgery, on the day of surgery, and for 4 days after surgery.
An alternate dose schedule is 600 Units/kg PROCRIT® subcutaneously in once weekly doses (21, 14, and 7 days before surgery) plus a fourth dose on the day of surgery.
All patients should receive adequate iron supplementation. Iron supplementation should be initiated no laterthan the beginning of treatment with PROCRIT® and should continue throughout the course of therapy. Deep venous thrombosis prophylaxis should be strongly considered (see BOXED WARNINGS).
PREPARATION AND ADMINISTRATION OF PROCRIT®
1. Do not shake. It is not necessary to shake PROCRIT®. Prolonged vigorous shaking may denature anyglycoprotein, rendering it biologically inactive.
2. Protect the solution from light. Parenteral drug products should be inspected visually for particulate matterand discoloration prior to administration. Do not use any vials exhibiting particulate matter or discoloration.
3. Using aseptic techniques, attach a sterile needle to a sterile syringe. Remove the flip top from the vialcontaining PROCRIT®, and wipe the septum with a disinfectant. Insert the needle into the vial, andwithdraw into the syringe an appropriate volume of solution.
4. Single-dose: 1 mL vial contains no preservative. Use one dose per vial; do not re-enter the vial. Discardunused portions.
Multidose: 1 mL and 2 mL vials contain preservative. Store at 2° to 8°C after initial entry and betweendoses. Discard 21 days after initial entry.
5. Do not dilute or administer in conjunction with other drug solutions. However, at the time of SCadministration, preservative-free PROCRIT® from single-use vials may be admixed in a syringe withbacteriostatic 0.9% sodium chloride injection, USP, with benzyl alcohol 0.9% (bacteriostatic saline) at a1:1 ratio using aseptic technique. The benzyl alcohol in the bacteriostatic saline acts as a local anestheticwhich may ameliorate SC injection site discomfort. Admixing is not necessary when using the multidosevials of PROCRIT® containing benzyl alcohol.
Manufactured by:Amgen Inc.One Amgen Center DriveThousand Oaks, CA 91320-1799
Distributed by:Ortho Biotech Products, L.P.Raritan, New Jersey 08869-0670
Revised 08/2008© OBPLP 200010112802BC
PROCRIT® (Epoetin alfa) FOR INJECTION
43156ALT_Control Ad_V1 5 11/11/08 6:12:49 PM
Talk is swirling around Washington as to who mayreplace Dr Andrew C. von Eschenbach at thehelm of the US Food and Drug Administration
(FDA). One well-known blogger has even begun a vot-ing contest where readers can choose from several can-didates for FDA Commissioner and cast a vote. There islittle question that the policy environment is pregnantwith change, but in most cases, it is quite possibly lessimportant who is appointed rather than what thechanges may entail.
This was obviously true with the presidential elec-tion. Given that both the McCain and Obama positionsfavored the import of prescription drugs, the ability ofthe government to negotiate prices under Medicare PartD, and the increasing uptake of generic drugs before thecampaign, it is virtually certain that the outcome of thepresidential contest mattered less to the pharmaceuticaland biotechnology industries than the contests in Con -gress. Not only did the November 4 election decide thatDemocrats were to achieve solid majorities in bothchambers, it has also paved the way for new congres-sional committee assignments and chairs.
This is the one area where “who” may matter, althoughonly in a matter of degree. Consider the case of the chair-manship for the Committee on Energy and Commerce. A clash of the titans emerged between 2 powerful andprominent members of Congress—Congressman John D.Dingell, the current chair, and Congressman HenryWaxman, who emerged the winner. This committee iskey to the oversight of various aspects of the FDA and theregulation of pharmaceutical industry. The activity of thiscommittee for October 2008 includes the following inves-tigations, announcements, statements, and reports:• Dingell, Stupak to Investigate Melamine Contam -
ination in Chinese Milk Products (10/2)• Dingell, Stupak Question FDA’s No-Bid Contract
with a PR Firm (10/2)• Dingell, Stupak Question Whether FDA Knowingly
Allowed Dangerous Drugs to be Sold to U.S. Con -sumers (10/8)
• Dingell, Stupak Continue DTC Ad Investigation(10/14)
GENERIC DRUG TRENDSFDA WATCH
The ObamaAdministration and the FDAMark Senak, JD
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 32

33www.AHDBonline.comVOL. 1 NO. 9
FDA WATCH
• Dingell, Stupak Continue Investigation into FDA’sQuestionable Handling of Bisphenol A (10/14)
• Dingell, Stupak Request Interview with von Esch -enbach on Bisphenol A (10/15)
• GAO Report Finds FDA’s Foreign Drug InspectionProgram Needs Significant Improvement (10/22).Ironically, Congressman Dingell made the case
that he is the preferable chair, because he is friendlierto industry with this 1-month track record. Now that Congressman Waxman has prevailed overCongressman Dingell for the chairmanship, one canexpect a great deal more intensity in terms of thebreadth and depth regarding scrutiny of the FDA andthe pharmaceutical industry than was shown inOctober 2008.
However, for the balance of the change, “who” isnot as important as “what” in terms of what must beaccomplished.
There is also a great deal of unfinished business withrespect to the FDA itself. Once a gold standard agency,the FDA has suffered tremendously during the past 8years and will have a great deal to do to reclaim its posi-tion as a flagship agency overseeing one fourth of thenation’s economy.
The following qualities are the ones that President-Elect Obama may seek for the individual who will takeover the FDA. That person must:• Have a solid grasp of the pharmaceutical industry,
without being directly associated with it. There aremembers in the Senate, particularly SenatorKennedy, who may insist that the individual haveno ties to the pharmaceutical industry itself. Still,the designee must have a good understanding ofclinical research and public health.
• Be able to balance the policymakers hunger for safe-ty, while assuring that the pipeline produces to pro-vide access. Although the public appetite isextremely risk averse, our slant to caution may bringa slowdown in new drug approvals. Longer approvaltime in the end means potentially higher drugprices, as patented drugs will have less time on themarket to recoup research and development costs.
• Have the credibility and gravitas to tell policy -makers on the Hill to stop using the agency as apolitical means, to gently remind members ofCongress that it is a new administration, that thereis a 1-party rule, and that most of them are in thatvery same party.
• Possess solid visionary and have noteworthy com-munication skills. The agency is in trouble not onlyfrom a functional point of view, but it has also donevery little to proactively address the descent of itsimage and to communicate and assure the publicand policymakers that it has a vision. In fact, theagency does not seem to acknowledge much of aproblem, much less to have a plan for solving it. Thenew commissioner will need to understand this, acton it, and seize leadership.In addition to these qualities, the first order of pri-
ority should be to completely implement the Food andDrug Administration Amendment Act (FDAAA).Right now the pipeline is getting clogged with Com -plete Response Letters and shifting the PrescriptionDrug User Fee Act dates, as the FDA tries to under-stand and implement the FDAAA. The FDA has beencharged with implementing a fairly broad scope ofreforms, but the longer it takes to identify and follow a roadmap for doing so, the more in the dark drug sponsors are going to be, which again contributes to a sluggish pipeline.
And as the policy and the communications environ-ments undergo breathtaking changes, it is importantthat the agency enunciate some points of view aboutthe uses of digital and social media by pharmaceuticalcompanies in marketing. The potential uses for socialand digital media are extraordinary, from public serviceannouncements to patient education videos, to riskmanagement tools; however, because regulatory cul-tures of most pharmaceuticals are generally conserva-tive, most are waiting for the FDA to say somethingwith regard to the use of such media.
The FDA appears nowhere near doing this, eventhough other industries have begun to embrace andstrategically anticipate and respond to the migrationinto digital media. It is time for the FDA to be a leader,not continue to be a follower, and give companies someguidance. And that guidance should be the medium,not the message.
All this and more needs to be accomplished by anObama-appointed FDA Commissioner, and in no shortorder, for the sake of the agency, public health, and the economy. ■
Mr Senak is Senior Vice President at Fleishman-Hillardin Washington, DC, and writes the Eye on FDA blog,www.eyeonfda.com.
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 33

34 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
AHA MEETING HIGHLIGHTS
Several antithrombotic drugs in late-stage develop-ment were featured at the 2008 Scientific Sessionsof the American Heart Association (AHA).
Prasugrel. A new analysis of the antiplatelet drugprasugrel, a direct-acting P2Y12 antagonist currentlyunder US Food and Drug Administration review, ques-tions this agent’s supposed superiority over the currentstandard in this class, clopidogrel (Plavix). Results ofthe pivotal phase 3 Trial to Assess Improvement inTherapeutic Outcomes by Optimizing PlateletInhibition with Prasugrel (TRITON), which comparedprasugrel and clopidogrel, were released in late 2007.Among patients being considered for coronary stents,prasugrel prevented more future cardiac events thanclopidogrel, but with excess bleeding. Despite thisexcess risk, the net benefit still favored prasugrel—23fewer myocardial infarctions (MIs) per 1000 patientstreated, at a cost of 6 extra bleeding events.
More recent analyses of TRITON have shown thatmuch of the benefit of prasugrel in preventing ischemicevents occurs early on, but the excess bleeding occursafter 30 days of use. New analyses have shown that pra-sugrel is better than clopidogrel at preventing stentthrombosis (blood clots forming in stents).
At the AHA, a team of investigators at Cedars-Sinai Medical Center in Los Angeles discussed its inde-pendent statistical analysis (using a Bayesian method),showing that the true superiority of prasugrel in TRITON was not as large. In their analysis, the proba-bility of a 10% or more benefit with prasugrel overclopidogrel is less than 80%, and the chance that pra-sugrel is 20% better than clopidogrel in preventing cardiac events is less than 5%. If bleeding events are considered, the probability of a net benefit with prasugrel is even smaller, they argued.
Because of the risk-benefit ratio, Sanjay Kaul, MD,MPH, Director of the Vascular Physiology andThrombosis Research Laboratory at the Burns andAllen Research Institute at Cedars-Sinai, and leadinvestigator of the reanalysis, proposed a strategy forusing prasugrel. “One potential approach to optimizing
the benefit-risk profile of prasugrel could involve giv-ing it during the first 30 days as acute ‘induction’ ther-apy, followed by maintenance ‘consolidation’ therapywith a less potent antiplatelet agent, such as clopido-grel, in patients who receive stents,” he said.
Rivaroxaban. This oral drug factor Xa inhibitor—anew class of anticlotting agents—is entering a phase 3trial (and will enroll 16,000 patients) after the releaseof phase 2 data at the AHA. The data showed thatrivaroxaban could reduce MI and stroke risk, with anacceptable bleeding risk at its 2 lowest doses.
That study enrolled 3491 stable patients with arecent MI who were taking aspirin and clopidogrel (ifnecessary). Patients were randomized to placebo or 1 of4 doses of rivaroxaban (2.5-10 mg twice daily) for 6months, and were followed for 1 month after stoppingtherapy. As expected, higher doses of rivaroxabanincreased the rate of clinically significant bleeding.
Rivaroxaban reduced the risk of ischemic events by21% relative to placebo, but this difference was notdefinitive, given the small number of patients enrolled,reported C. Michael Gibson, MD, Chief of ClinicalResearch, Beth Israel Deaconess Medical Center,Boston. “We have decided to go forward to phase 3with the 2 lower doses—2.5 mg and 5 mg twice daily,”he said. These doses reduced the risk of death, MI, andstroke by 46% compared with placebo (P = .08) andwere associated with a major bleeding rate of 1.2%.
There was no drug-induced liver injury with rivarox-aban. The development of an oral direct thrombininhibitor—ximelagatran—was derailed as a result ofliver toxicity.
Other late-phase antithrombotic/antiplatelet drugsinvestigated for various thrombotic indications werediscussed at the meeting, including: • Apixaban, another oral factor Xa inhibitor• Cangrelor, another direct-acting P2Y12 antagonist• Dabigatran, an oral direct thrombin inhibitor,
which was recently approved in Europe (brandname, Pradaxa)
• Idraparinux, a long-acting factor Xa inhibitor. ■
The Antiplatelet Drug Pipeline: Some Promising CandidatesBy Wayne Kuznar
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 34

Do you measure resource utilization and costs associatedwith depression?
Managing quality and cost is the foundation of today’s
managed care structure. Wyeth recognizes that balancing
quality and cost is a formidable challenge for managed health
care professionals. We also recognize that success, in part,
hinges on tools and resources that can aid in the evaluation
of care management and may lead to reinforcing solutions. As
part of our continuing efforts to improve the quality of care for
patients with depression, we are proud to sponsor this
comprehensive claims-based review to promote ongoing
clinical and financial assessments that improve care in this
patient population.
To learn more about this exclusive program,
please contact your Wyeth Pharmaceuticals
Account Manager today!
N e w E d i t i o n N o w A v a i l a b l eAward-winning
Depression Benchmarks!
Gold AwardAster Awards, May 2007
Merit Awards (2)Healthcare Advertising Awards,
April 2007
A comprehensive, claims-based analysis of more than 600,000
patient episodes of depression (1 episode = 1 year)
highlighting direct costs and utilization of
resources across 5 domains of care:
� Inpatient care
� Outpatient care
� Ancillary care (labs, tests, procedures)
� Emergency department
� Pharmaceuticals
“Depression Benchmarks” and “TRU Benchmarks” are trademarks owned by Managed Care Measures, LLC. Depression BenchmarksTM
publication cover design, photograph, and color scheme (except for Total Resource
UtilizationTM
blue banner): © 2008, Wyeth Pharmaceuticals Inc., Philadelphia, PA 19101. Total Resource UtilizationTM
blue banner: © 1999-2008 Managed Care Measures, LLC. The remainder of this advertisement:
© 2008, Wyeth Pharmaceuticals Inc., Philadelphia, PA 19101. 223008-01
DepressionBenchmarksTM
Business_FDA_NovDec .qxp:Cover 11/25/08 10:48 AM Page 35

36 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
AMCP MEETING HIGHLIGHTS
Anumber of new specialty products are in latestages of development, said Deborah B. Cooper,PharmD, Clinical Advisor, Pipeline Series,
CVS/Caremark, at the 2008 educational conference ofthe Academy of Managed Care Pharmacy. Specialtyproducts comprise 49% of new chemical compoundscurrently in phase 3 and 55% of the phase 3 ambulato-ry care agents. The 53 new specialty drugs slated forlaunch in 2008-2009 are for these categories (severalproducts are included in more than 1 category):• Oncology—17• Rare or orphan diseases—11• Metabolic diseases—8• Immunology—6• Infectious diseases—5• Neurologic disorders—5• Cardiovascular disorders—3• Respiratory disorders—3• Dermatology—2• Gastrointestinal disorders—2.
Key trends for the specialty pipeline include (1)increased numbers of drugs for rare/orphan diseases, (2)emergence of more drugs with Risk Evaluation andMitigation Strategy (REMS) programs, (3) expansionof adjunctive/additive agents for multiple disease states,and (4) a shift from injectable to oral therapies.
Rheumatoid Arthritis Toxilizumab (Actemra), an anti-interleukin-6
receptor monoclonal antibody, is pending approval forrheumatoid arthritis (RA) and is expected to belaunched with a REMS program. It is administeredintravenously every 4 weeks. Adverse events reportedinclude infections, hypersensitivity reactions, head -ache, nasopharyngitis, and pleurisy.
Golimumab is a humanized anti-tumor necrosis factor drug pending approval for RA, psoriatic arthritis,and ankylosing spondylitis. It is administered as a sub-cutaneous injection every 4 weeks. An intravenous(IV) formulation is in phase 2, to be administered every12 weeks. Adverse events included headache andinjection-site and allergic reactions.
Multiple Sclerosis Fampridine SR is a twice-daily oral agent in phase 3,
for the symptomatic treatment of multiple sclerosis(MS), to be used in conjunction with other MS drugs.
It blocks potassium channels on axons of nerves and in -creases walking speed and/or muscle strength. Adverseevents reported include falls, insomnia, paresthesias,dizziness, urinary tract infections, and nausea. Seizureshave been reported with high doses of the drug.
Fingolimod is a once-daily oral immunosuppressantin phase 3, which, if approved, will be the first oral dis-ease-modifying agent for MS. It causes a dose-relatedreduction in the number of circulating lymphocytes,leading to a decrease in the number of activated T-cellsin the blood and central nervous system. Adverseevents include headache and dose-dependent upperrespiratory tract infection.
Psoriasis Ustekinumab (Stelara) is a fully humanized mono-
clonal antibody that targets interleukin-12 and -23,which are thought to be proinflammatory cytokines.Approval is pending for chronic moderate-to-severe pso-riasis. The drug is administered subcutaneously every 12weeks. Adverse reactions include headache, infections,injection-site reactions, and respiratory tract infections.
SLE Epratuzumab, a monoclonal antibody that targets the
CD22 antigen on the surface of B cells, is in phase 3 forthe treatment of moderate-to-severe systemic lupus ery-thematosus (SLE). The CD22 receptor is implicated ininflammation. Epratuzumab is administered as an IV infu-sion every other week. Adverse reactions in clinical trialsinclude arthralgia, hypotension, nausea, and palpitations.
Belimumab (LymphoStat-B), also in phase 3 forSLE, is a fully human monoclonal antibody that inhibitsthe biologic activity of B-lymphocyte stimulator, whichat high levels may contribute to the pathogenesis ofautoimmune diseases (eg, SLE, RA). It is administeredintravenously every 28 days. It has shown a significantreduction in SLE flares and disease activity.
Hepatitis C Two drugs in phase 3 trials for hepatitis C virus (HCV)
show very promising results for those who failed therapywith pegylated interferon alfa and ribavirin: Zadaxin (thy-malfasin), an immunomodulator that stimulates T-cellsand decreases viral replication; telaprevir, the first pro-tease inhibitor for HCV, to be used with current therapies.Approval and launch are expected in 2009 or 2010. ■
Specialty Pipeline Dominated by BiologicsBy Alice Goodman
AMCP_36_37NovDec .qxp:Cover 11/24/08 4:37 PM Page 36

37www.AHDBonline.comVOL. 1 NO. 9
AMCP MEETING HIGHLIGHTS
Real-world data on a new therapy and a user-friendly assessment tool to evaluate real-worldstudies facilitate formulary and reimbursement
decisions, said Diana Brixner, PhD, RPh, Professor andChair, Department of Pharmacotherapy, and ExecutiveDirector, Pharmacy Outcomes Research Center,University of Utah, at the 2008 educational conferenceof the Academy of Managed Care Pharmacy.
Payers need information beyond randomized con-trolled trials (RCTs) to make the best decisions abouthow to deploy limited budgets for large patient popula-tions. RCTs are conducted in a select patient popula-tion, according to strict protocols, and the results arenot generalizable to large patient populations.Supplemental observational open-label trials and post-marketing surveillance provide data on the effect ofnew treatments that are more relevant for managedcare organizations (MCOs), such as quality-adjustedlife-years, productivity, and absenteeism.
Dr Brixner summarized the proceedings of 2 roundta-bles that addressed issues surrounding use of real-worlddata in managed care. A roundtable in July 2007 includ-ed 4 MCO directors and 4 economists. The panel tack-led the quality of real-world evidence, the complexity ofreal-world research, the lack of consistency in qualityassurance and assessment in decision-making, and thetime delay between accrual of real-world data and prod-uct launch. Recommendations for further study include: • Analysis of tools for quality assessment of observa-
tional studies• Development of a consolidated instrument to meas-
ures the quality assurance of these data• Establishment of a process to support application of
a comprehensive quality assessment tool• Development of training for producers and users of
observational studies on the consolidated tool.“Our healthcare system is fragmented. A consolidat-
ed tool would reduce the impact of fragmentation,” saidDr Brixner.
Developing a new tool for quality assurance to eval-uate real-world studies is a daunting task, and is stillongoing, Dr Brixner explained. In analyzing existingchecklists, participants found that none of them ful-filled the criteria for a simple-to-use, comprehensive
checklist to evaluate published real-world studies.Existing checklists were either too long or too academ-ic to support decision-making.
A second roundtable, held in March 2008, discussedhow to act on the recommendations of the first round-table. Participants agreed on the need: • For quality and convenience in assessment of real-
world data• To recognize that the process of implementation of a
new tool is as important as the new tool itself• For peer validation of a new tool• To educate all constituents about the tool and its
implementation.A small survey of 4 MCOs found that although none
of them currently uses a checklist to evaluate real-world studies, they would use a tool if it was short andconcise, validated, and recommended by a nationalorganization, Dr Brixner said. ■
Real-World Data Better than RCTs forFormulary DecisionsBy Alice Goodman
Unmanaged Moment
“On the other hand, where would we be if not for our overmedicated society?”
AMCP_36_37NovDec .qxp:Cover 11/24/08 4:37 PM Page 37

March 4-6, 2009 • Pointe Hilton Tapatio Cliffs Resort • Phoenix, Arizona
Attend PBMI’s 14th Annual Drug Benefit Conference
Visit www.pbmi.com/conference.asp for Detailed Agenda and Faculty.
Register Now!© 2008, Pharmacy Benefit Management Institute, LP All Rights Reserved
AMCP_36_37NovDec .qxp:Cover 11/24/08 4:37 PM Page 38

39www.AHDBonline.comVOL. 1 NO. 9
CLINICAL
Cardiovascular (CV) disease (CVD) is the lead-ing cause of mortality and one of the leadingcauses of disability worldwide.1 In the United
States alone, more than 80 million adults have at leastone type of CVD, with hypertension, coronary heartdisease (CHD), stroke, and heart failure among themost common forms of the disease. Elevated levels ofcholesterol (hypercholesterolemia) and abnormal lipidprofiles (dyslipidemia) are important risk factors forCVD. The American Heart Association (AHA) esti-mates that more than 100 million Americans have ele-vated cholesterol levels (>200 mg/dL) and 34 millionhave cholesterol levels that necessitate treatment.2
Cholesterol is an essential component of cell mem-branes and steroid hormones. The body synthesizesmost of its required cholesterol with the remaindercoming from the diet. Since cholesterol is mostly insoluble in blood, it is packaged with proteins andphospholipids to form lipoprotein complexes that cir-culate in the bloodstream. The types of cholesterol-containing lipoproteins are high-density lipoproteins(HDL-C), low-density lipoproteins (LDL-C), very low-density lipoproteins (VLDL-C), and chylomicrons.
High levels of LDL-C are associated with increasedCV risk in epidemiologic studies. In addition, numer-ous clinical studies using a variety of therapies havedemonstrated decreased CV events and mortality withLDL reduction. Therefore, the first goal of therapy is
reduction of LDL-C levels for the most common formsof dyslipidemia. Conversely, high levels of HDL-C areassociated with decreased risk of CV events. However,clinical trials assessing the morbidity and mortalitybenefits of drug therapies that raise HDL-C levels havehad varied results. HDL-C–modifying trials with niacinhave demonstrated CV event reduction.3,4 Conversely,other treatments that raise HDL-C, including hormonereplacement therapy5 and torcetrapib,6 have notdecreased CV events. Because of this, in the absence oflarge clinical outcome trials, therapies that elevate HDLcannot be assumed to produce clinical event reduction.
Approach to Patient Assessment, Treatment The National Cholesterol Education Program
(NCEP) evaluates evidence and develops guidelines forlipid management. The approach to patient manage-ment provided here comes primarily from the guide-lines published in 2001 and updated in 2004.7,8
Since the primary goal of lipid management is todecrease the risk of CV events and death, the first stepin management is to assess the patient’s overall CVrisk. To make this assessment, a fasting lipoproteinanalysis should be obtained to determine the patient’sLDL-C. Optimal levels for LDL-C and total cholesterolare <100 mg/dL and <200 mg/dL, respectively. TheNCEP guidelines recommend that a fasting lipid panel be drawn at least every 5 years in all adults older than 20 years.7
In addition to LDL-C levels, the presence orabsence of CHD or CHD-equivalent conditions mustbe assessed. CHD-equivalent conditions listed by theNCEP include diabetes mellitus, peripheral vasculardisease, abdominal aortic aneurysm, symptomaticcarotid disease, and a 10-year CV risk of less than 20%
Cardiovascular disease is the leading cause of death worldwide. Elevated cholesterol (hyper-cholesterolemia) and abnormal lipid profiles (dyslipidemia) are important risk factors for thedevelopment of cardiovascular disease. This article discusses the role of cholesterol in thebody and the relationship between different cholesterol fractions and the risk of cardiovas-cular disease. The guidelines for assessment and treatment of dyslipidemia from the NationalCholesterol Education Program are outlined, and cholesterol targets and goals of therapy arediscussed. The mechanism of action, place in therapy (eg, first-line, second-line, or add-on),and common side effects are also discussed for each of the available classes of drugs usedin the treatment of dyslipidemia. [ADHB. 2008;1(9):39-48.]
Dr Burns Schaiff is Senior Director, Regional Medical &Research Specialist, Pfizer, Inc, New York, NY; Dr Moe isClinical Associate Professor, University of Missouri-KansasCity, Kansas City, MO; Dr Krichbaum is Senior DirectorTeam Leader, Regional Medical & Research Specialist,Pfizer, Inc, New York, NY.
An Overview of Cholesterol ManagementRobyn A. Burns Schaiff, PharmD, BCPS; Richard M. Moe, MD, PhD; Daniel W. Krichbaum, PharmD
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:54 AM Page 39

40 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
CLINICAL
calculated with the Framingham risk calculator.7
Although not addressed by the NCEP, the NationalKidney Foundation also considers chronic kidney dis-ease (glomerular filtration rate <60 mL/min) to be ahigh-risk state and recommends that this patient groupbe treated as having a CHD-equivalent disease.9
Likewise, the AHA and the American StrokeAssociation recommend the use of a statin with inten-sive lipid-lowering effects in patients with atheroscle-rotic stroke or transient ischemic attack, even in theabsence of known CHD.10
In the absence of CHD or CHD-equivalent condi-tions, CVD risk factors (Table 1) should be carefullyassessed using the Framingham risk score to determinethe patient’s 10-year risk of CV events (Table 2).7
Goals of TherapyFor patients with CHD or CHD-equivalent disease,
the NCEP recommends the LDL-C goal of ≤100mg/dL, with <70 mg/dL a therapeutic option forpatients considered at very high risk for CV events.8
For patients with 2 or more CV risk factors but with a10-year Framingham risk of less than 20%, the LDL-Cgoal is <130 mg/dL, with <100 mg/dL a therapeuticoption. Finally, for patients with 0 to 1 risk factors, theLDL-C target is <160 mg/dL.8
Therapeutic Lifestyle ChangesThe NCEP Adult Treatment Panel III guidelines
recommend that therapeutic lifestyle changes beimplemented for all patients at risk for CVD.7 Thesechanges include reducing intake of saturated fats andcholesterol while increasing soluble fiber intake andphysical activity. Optimization of weight, moderationof alcohol consumption, and cessation of smoking arealso encouraged. If drug therapy is needed, it should beused as an addition to, rather than a substitute for, ther-apeutic lifestyle changes.
Treatment InitiationSince the clinical evidence of benefit is greatest
with the statin drug class, the American College ofCardiology (ACC) recommends drug therapy beginwith a statin and that titration to goal or the maximal-ly tolerated dose of a statin be achieved before consid-eration of adding other agents.11 Regardless of the ini-tial treatment chosen, it is critical that the patient bereevaluated and therapy titrated or added until the goalLDL-C is attained.
For patients with 0 to 1 risk factors and no CHD, treatment is initiated with therapeutic lifestyle changeswith reassessment after 6 weeks. If goal LDL of <160mg/dL is not reached at 6 weeks, lifestyle changesshould be intensified and reinforced and a visit with a dietitian considered. If after 12 weeks of therapeuticlifestyle changes the patient is not at the LDL-C goal of <160 mg/dL, drug therapy, usually a statin, should be added.
For patients at moderate risk, with 2 or more risk fac-tors and a 10-year CV risk of less than 20%, treatmentbegins with therapeutic lifestyle changes. Drug therapy,usually a statin, can be initiated concurrently if theLDL is >100 mg/dL at baseline or if LDL-C remains>100 mg/dL after a 6-week trial of lifestyle changes.
For the highest risk patients with CHD or equivalentconditions, statin therapy and therapeutic lifestylechanges should be initiated simultaneously for all
KEY POINTS▲ Cholesterol is an essential component of cell membranes
and steroid hormones. ▲ Hypercholesterolemia and dyslipidemia are important risk
factors for cardiovascular disease, which affects more than 80 million Americans.
▲ Evidence shows that high levels of LDL-C are associatedwith increased cardiovascular risk; reducing LDL levels hasbeen associated with significant reduction in mortality.
▲ The first goal of therapy in hypercholesterolemia is reduc-tion of LDL-C levels.
▲ Statins are considered the most effective lipid-loweringagents available, both in lowering LDL levels and in the prevention of cardiovascular events.
Table 1 Major Risk Factors (Exclusive of LDL-C) that Modify LDL Goals*
Cigarette smokingHypertension (blood pressure ≥140/90 mm Hg or on antihypertensive medication)Low HDL-C (<40 mg/dL)†
Family history of premature CHD (CHD in male first-degreerelative <55 y, CHD in female first-degree relative <55 y)Age (men ≥45 y; women ≥55 y)*Diabetes is regarded a CHD risk equivalent.†HDL cholesterol ≥60 mg/dL counts as a negative risk factor; its presenceremoves 1 risk factor from the total count.LDL-C indicates low-density lipoprotein cholesterol; HDL-C, high-densitylipoprotein cholesterol; CHD, coronary heart disease.Reprinted with permission from Expert Panel on Detection, Evaluation, andTreatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 40

41www.AHDBonline.comVOL. 1 NO. 9
Cholesterol Management
HDL indicates high-density lipoprotein; BP, blood pressure. Reprinted with permission from Expert Panel on Detection Evaluation and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.
Table 2 An Overview of Cholesterol Management
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 41

42 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
CLINICAL
patients with LDL-C >100 mg/dL. Drug therapy mayalso be considered in very high-risk patients with LDL-C <100 mg/dL targeted to achieve the optional goal of<70 mg/dL.8
Pharmacotherapy OptionsA variety of lipid-lowering agents are available,
including 3-hydroxy-3-methylglutaryl coenzyme A(HMG-CoA) reductase inhibitors, bile acid seques-trants, cholesterol absorption inhibitors, fibrates, nico-tinic acid derivatives, and omega-3 fatty acids. Dosageranges, US Food and Drug Administration (FDA) indi-cations, evidence of clinical outcome benefit, and sideeffects are highlighted in Table 3.
HMG-CoA Reductase Inhibitors (Statins)HMG-CoA reductase inhibitors, or statins, are the
recommended first-line therapy for most patients.These are the most prescribed drugs in the world andare considered the most effective lipid-lowering agentsavailable, both in lowering LDL-C levels and in theprevention of CV events. Statins are similar in struc-ture to HMG-CoA, a precursor of cholesterol, and actas competitive inhibitors of HMG-CoA reductase, thelast regulated enzymatic step in cholesterol synthesis.Therefore, statins reduce the rate of synthesis of choles-terol. The liver responds by increasing the number ofLDL receptors, which increases hepatic uptake andcatabolism of circulating LDL-C. Statins reduce LDL-Cby 24% to 60% and decrease triglycerides (TGs) by 5%to 50% (percentages are based on the various packageinserts), depending on the agent selected and the base-line lipid profile. HDL-C levels are usually increased.The effects on HDL are a class effect and are small rel-ative to the effects on LDL-C and TGs. In addition,statins have a variety of anti-inflammatory effects thatare independent of the LDL-C lowering, which maycontribute to the clinical benefit in CVD, especiallyearly in therapy.12 However, a recent meta-analysis of 23lipid-lowering trials demonstrated that the majority(89%-98%) of the anti-inflammatory effects of lipid-lowering therapy is related to the degree of LDL reduc-tion,13 which suggests a limited influence of a non-LDL-
C–related anti-inflammatory mechanism.Adverse events, relatively uncommon with this
class, include gastrointestinal (GI) disturbances, mus-cle aches, and asymptomatic transaminasemia. Rareserious adverse events may include myopathy and rhab-domyolysis. FDA-approved labeling recommendsassessment of liver function at baseline, after 12 weeksof therapy, after dose escalation, and twice yearly there-after. However, the National Lipid Association has sug-gested that this practice does not increase the safety ofstatin therapy, but merely increases cost.14
Bile Acid SequestrantsBile acid sequestrants bind to bile acids in the intes-
tine, reducing absorption of cholesterol and other lipids.The resultant decrease in available cholesterol causesan increase in the number of LDL receptors on hepato-cytes, further promoting clearance of LDL-C from theblood. Bile acid sequestrants are recommended as sec-ond-line therapy for patients with elevated cholesterol,but not elevated TGs, as both VLDL-C and TG con-centrations may increase during therapy. Agents in thisclass lower LDL-C by 15% to 30% and increase HDL-Cby 3% to 5% on average.9 Patient adherence with theseagents is frequently poor due to the need for frequentdosing, poor palatability, and frequent GI side effects.Since these drugs remain in the GI tract, systemicadverse effects are minimal; however, these agents caninterfere with absorption of concomitantly adminis-tered drugs as well as fat-soluble vitamins.
Nicotinic Acid DerivativesNiacin reduces synthesis of VLDL-C in the liver and
therefore reduces LDL-C production. Pharmacologicdoses of niacin (1.5-2 g/day) lower LDL-C and TGs by15% to 20% and 30% to 40%, respectively, andincrease HDL-C by 15% to 25%. Niacin is used as sec-ond-line therapy in concert with other lipid-loweringagents. The most common adverse events includevasodilation with flushing and pruritis, which frequent-ly is dose-limiting. Other adverse events include dys-pepsia, gastric ulceration, hyperuricemia, palpitations,and, rarely, peripheral neuropathy.
Niacin-induced hyperglycemia may be problematicfor patients with diabetes mellitus or with impaired glu-cose tolerance, particularly in the first 6 months oftherapy, but long-term clinical benefits have beendemonstrated in these patients.15 The most serious sideeffect is hepatotoxicity; cases of fatal fulminant hepat-ic failure have been associated with niacin administra-tion, particularly with older formulations.16
These are the most prescribed drugs in theworld and are considered the most effectivelipid-lowering agents available.
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 42

43www.AHDBonline.comVOL. 1 NO. 9
Tabl
e 3
Phar
mac
othe
rapy
for L
ipid
Dis
orde
rs
Con
tinue
d
Pop
ulat
ions
w/
Cos
t,de
mon
stra
ted
Pri
mar
y ef
fect
Side
eff
ects
30-d
ayD
rug
Dos
age
rang
eA
vaila
ble
dose
sIn
dica
tion
sev
ent
redu
ctio
n†on
lipi
ds(m
ost
ofte
n re
port
ed)
supp
ly
Que
stra
n*8-
24 g
/d,
Que
stra
n Li
ght:
pac
kets
•A
djuc
t the
rapy
of
Men
wit
h pr
imar
yLD
L-C
↓A
bdom
inal
dis
com
fort
,$$
$$(c
hole
styr
amin
e)2
divi
ded
and
pow
der (
each
5 g
hy
perc
hole
ster
olem
iahy
perc
hole
ster
olem
ia10
%-3
0%co
nsti
pati
on, f
latu
lenc
e,
dose
sco
ntai
n 4
g an
hydr
ous
•Pru
riti
s due
to p
arti
al b
iliar
y(L
RC
-CT
TP1 )
naus
ea a
nd v
omit
ing,
ch
oles
tyra
min
e re
sin)
obst
ruct
ion
vita
min
A, D
def
icie
ncy
Que
stra
n: p
owde
r and
pa
cket
s (ea
ch 9
gco
ntai
n 4
g an
hydr
ous
chol
esty
ram
ine
resin
)
Wel
chol
3.
75 g
/d62
5-m
g ta
blet
s•A
djuc
t the
rapy
of h
yper
chol
este
role
mia
LDL-
C↓
Ast
heni
a, c
onst
ipat
ion,
$$$$
(col
esev
elam
)•A
djun
ct th
erap
y to
impr
ove
10%
-18%
indi
gest
ion,
pha
ryng
itis
,gl
ycem
ic c
ontr
ol in
type
2 D
Mm
yalg
ia
Col
esti
d*2-
16 g
/d1-
g ta
blet
sA
djun
ct th
erap
y fo
r pri
mar
yLD
L-C
↓A
bdom
inal
dis
tens
ion,
ab-
$$$
(col
esti
pol)
2 di
vide
d hy
perc
hole
ster
olem
ia10
%-2
0%do
min
al p
ain,
con
stip
atio
n,do
ses
mus
culo
skel
etal
pai
n, h
eada
che
Zeti
a10
mg/
d10
-mg
tabl
ets
•Pri
mar
y hy
perl
ipid
emia
LDL-
C↓
Hea
dach
e, d
iarr
hea,
$$
$(e
zeti
mib
e)•M
ixed
dys
lipid
emia
10%
-20%
abdo
min
al p
ain,
art
hral
gia,
•H
omoz
ygou
s fam
ilial
hyp
erch
oles
tero
lem
iaba
ckac
he, m
yalg
ia, s
inus
itis
•Hom
ozyg
ous s
itos
tero
lem
ia
Ant
ara*
43-1
30 m
g/d
43-,
130-
mg
caps
ules
•Hyp
ertr
igly
ceri
dem
iaT
G↓
Ras
h, d
iarr
hea,
flat
ulen
ce,
$$(f
enof
ibra
te)
•Pri
mar
y hy
perg
lyce
ride
mia
20%
-50%
naus
ea a
nd v
omit
ing,
•Mix
ed d
yslip
idem
iam
yalg
ia, r
hini
tis
Lipo
fen*
(fen
ofib
rate
)50
-150
mg/
d50
-, 15
0-m
g ca
psul
es
Lofib
ra*
(fen
ofib
rate
)54
-200
mg/
d54
-, 16
0-m
g ta
blet
s67
-,134
-, 20
0-m
g ca
psul
es
TriC
or*
(fen
ofib
rate
)48
-145
mg/
d48
-, 14
5-m
g ta
blet
s
Trig
lide
(fen
ofib
rate
)50
-160
mg/
d50
-, 16
0-m
g ta
blet
s
Lopi
d*(g
emfib
rozi
l)60
0-12
00 m
g/d,
600-
mg
tabl
ets
•Red
ucin
g C
HD
risk
in p
atie
nts w
/type
2b
•Men
w/p
rim
ary
TG
↓R
ash,
abd
omin
al p
ain,
$2
divi
ded
dose
sdy
slip
idem
ia a
nd in
adeq
uate
resp
onse
tody
slip
idem
ia (
Hel
sink
i25
%-4
5%di
arrh
ea, f
latu
lenc
e,
TLC
, oth
er d
rug
ther
apy,
who
hav
eH
eart
Stu
dy2 )
indi
gest
ion,
xer
osto
mia
, hi
gh L
DL,
low
HD
L, h
igh
TG
•Men
w/C
HD
and
low
mya
lgia
•Fam
ilial
type
IV o
r V h
yper
lipid
emia
HD
L-C
(V
A H
it3 )
Lipi
tor
10-8
0 m
g/d
10-,
20-,
40-,
80-m
g•P
rim
ary
prev
enti
on o
f MI,
stro
ke in
•Pat
ient
s w/h
yper
tens
ion
and
LDL-
C↓
Abd
omin
al p
ain,
$$
$(a
torv
asta
tin)
tabl
ets
pati
ents
w/t
ype
2 D
M a
nd o
ther
CH
D≥3
CH
D ri
sk fa
ctor
s (A
SCO
T4 )
39%
-60%
cons
tipa
tion
,ri
sk fa
ctor
s•P
atie
nts w
/typ
e 2
DM
and
no
flatu
lenc
e, in
dige
stio
n,•P
rim
ary
prev
enti
on o
f MI,
stro
ke,
hist
ory
of C
VD
(C
AR
DS5 )
incr
ease
d liv
er e
nzym
es,
reva
scul
ariz
atio
n, h
ospi
taliz
atio
n fo
r •P
atie
nts w
/stab
le C
HD
(T
NT,
6he
adac
he, m
yalg
iahe
art f
ailu
re a
nd a
ngin
a in
pat
ient
s ID
EAL,
7 A
LLIA
NC
E,8
and
w/c
linic
ally
evi
dent
CA
Dan
d A
VER
T9 )
•Pri
mar
y hy
perc
hole
ster
olem
ia o
r •P
atie
nts w
/ath
eros
cler
otic
mix
ed d
yslip
idem
ia
stro
ke o
r TIA
w/o
doc
umen
ted
•Hyp
ertr
igly
ceri
dem
iaC
HD
(SP
AR
CL10
) •P
rim
ary
dysb
etal
ipop
rote
inem
ia•P
atie
nts w
/AC
S (P
RO
VE-
IT,11
•Hom
ozyg
ous F
H in
ado
lesc
ents
MIR
AC
L12)
•Het
eroz
ygou
s FH
in a
dole
scen
ts
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 43

44 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
Tabl
e 3
Phar
mac
othe
rapy
for L
ipid
Dis
orde
rs C
ontin
ued
Pop
ulat
ions
w/
Side
eff
ects
Cos
t,de
mon
stra
ted
Pri
mar
y ef
fect
(mos
t of
ten
30-d
ayD
rug
Dos
age
rang
eA
vaila
ble
dose
sIn
dica
tion
sev
ent
redu
ctio
n†on
lipi
dsre
port
ed)
supp
ly
Lesc
ol (
fluva
stat
in)
20-8
0 m
g/d
20-,
40-m
g•R
educ
e co
rona
ry re
vasc
ular
izatio
n in
CH
DPa
tien
ts w
ith
CH
D w
ho h
adLD
L-C
↓A
bdom
inal
pai
n, d
iarr
hea,
$$$
caps
ules
•Red
uce
prog
ress
ion
of c
oron
ary
coro
nary
inte
rven
tion
(LI
PS13
)20
%-3
5%dy
spep
sia,
nau
sea,
hea
dach
e,at
hero
scle
rosi
s in
CH
Dm
yalg
ia•H
yper
chol
este
role
mia
•Het
eroz
ygou
s FH
in a
dole
scen
ts
Lesc
ol X
L80
-mg
mg/
d80
-mg
exte
nded
- $$
$$(f
luva
stat
in E
R)
rele
ase
tabl
ets
Mev
acor
*10
-80
mg/
d10
-, 20
-, 40
-mg
•Pri
mar
y pr
even
tion
of M
I, un
stab
le
Hig
h ri
sk (
elev
ated
LD
L-C
LDL-
C↓
Abd
omin
al p
ain,
con
stip
atio
n,$$
(lov
asta
tin)
tabl
ets
angi
na, c
oron
ary
reva
scul
ariz
atio
nw
/low
HD
L-C
) pa
tien
ts w
/o25
%-4
5%di
arrh
ea, n
ause
a, h
eada
che,
•To
slow
pro
gres
sion
of c
oron
ary
clin
ical
CH
D
mya
lgia
, inc
reas
ed h
epat
icat
hero
scle
rosi
s in
CH
D(A
FCA
PS-T
exC
aps14
)tr
ansa
min
ase
leve
ls•H
yper
chol
este
role
mia
•Het
eroz
ygou
s FH
in a
dole
scen
ts
Prav
acho
l*10
-80
mg/
d10
-, 20
-, 40
-, 80
-mg
•Pri
mar
y pr
even
tion
of M
I, re
vasc
ular
i-•M
en w
/o h
isto
ry o
f MI
LDL-
C↓
Dia
rrhe
a, fl
atul
ence
, hea
rt-
$$(p
rava
stat
in)
tabl
ets
zati
on, a
nd C
V m
orta
lity
w/e
leva
ted
LDL
(WO
SCO
PS15
)25
%-4
0%bu
rn, n
ause
a, v
omit
ing,
•R
educ
tion
in to
tal m
orta
lity
by•P
atie
nts w
/MI i
n pr
eced
ing
asth
enia
, hea
dach
e, m
yalg
iare
duci
ng c
oron
ary
deat
h, M
I, 3-
20 m
o (C
AR
E16)
reva
scul
ariz
atio
n, st
roke
, and
to sl
ow•P
atie
nts w
/MI o
r uns
tabl
e pr
ogre
ssio
n of
cor
onar
y at
hero
scle
rosi
s in
angi
na in
pre
viou
s 3-3
6 m
opa
tien
ts w
ith
CH
D(L
IPID
17)
•Hyp
erch
oles
tero
lem
ia•H
eter
ozyg
ous F
H in
ado
lesc
ents
Cre
stor
5-40
mg/
d5-
, 10-
, 20-
, 40-
mg
•Pri
mar
y hy
perl
ipid
emia
Men
≥55
and
wom
en ≥
65LD
L-C
↓A
bdom
inal
pai
n, c
onst
ipat
ion,
$$$$
(ros
uvas
tati
n)ta
blet
san
d m
ixed
dys
lipid
emia
w/L
DL
≤130
mg/
dL a
nd C
RP
45%
-60%
naus
ea, a
rthr
algi
a, a
sthe
nia,
•Pri
mar
y hy
pert
rigl
ycer
idem
ia≥2
mg/
L (J
UPI
TER
18)
head
ache
, mya
lgia
, inc
reas
ed
•Hom
ozyg
ous f
amili
al h
yper
chol
este
role
mia
hepa
tic
tran
sam
inas
e le
vels
•To
slow
the
prog
ress
ion
of a
ther
oscl
eros
is
Zoco
r*5-
80 m
g/d
5-, 1
0-, 2
0- 4
0-, 8
0-m
g•P
reve
ntio
n of
CH
D m
orta
lity
and
•Exi
stin
g C
HD
and
ele
vate
dLD
L-C
↓C
onst
ipat
ion,
GI
$$(s
imva
stat
in)
tabl
ets
CV
eve
nts i
n pa
tien
ts w
/exi
stin
g C
HD
,to
tal c
hole
ster
ol (
4S19
)35
%-5
0%ir
rita
tion
, hea
dach
e,hi
stor
y of
stro
ke, d
iabe
tes,
or p
erip
hera
l•P
atie
nts a
t hig
h ri
sk o
f CV
uppe
r res
pira
tory
ar
tery
dis
ease
even
ts fr
om e
xist
ing
CH
D,
infe
ctio
n, m
yalg
ia,
•Hyp
erch
oles
tero
lem
iahi
stor
y of
stro
ke, o
ther
cer
ebro
-in
crea
sed
hepa
tic
•Het
eroz
ygou
s FH
in a
dole
scen
tsva
scul
ar d
isea
se, p
erip
hera
ltr
ansa
min
ase
leve
lsar
tery
dis
ease
, or h
yper
tens
ion
in m
en ≥
65 y
r (H
PS20
)
Slo-
Nia
cin
CR
*0.
5-2
g/d
Nia
cin
CR
: 250
-, 50
0-,
•Pri
mar
y hy
perc
hole
ster
olem
ia o
r mix
edM
en w
/his
tory
of M
I (C
DP21
;LD
L↓C
onst
ipat
ion,
flus
hing
, $$
(con
trol
led-
rele
ase
750-
mg
tabl
ets
dysl
ipid
emia
(al
one
or w
ith
lova
stat
in)
imm
edia
te-r
elea
se d
osag
e fo
rm)
5%-1
5%pr
urit
is, G
I irr
itat
ion,
ni
acin
)•S
ever
e hy
pert
rigl
ycer
idem
iaT
G↓
naus
ea, v
omit
ing
•To
redu
ce ri
sk o
f rec
urre
nt M
I in
patie
nts
15%
-30%
w/h
yper
chol
este
role
mia
and
his
tory
of M
IH
DL↑
$$$$
$N
iasp
an0.
5-2
g/d
Nia
cin
ER: 5
00-,
750-
,•W
/bile
aci
d–bi
ndin
g re
sin
to sl
ow15
%-2
0%(n
iaci
n ER
)10
00-m
g ta
blet
spr
ogre
ssio
n or
indu
ce re
gres
sion
of c
oron
ary
athe
rosc
lero
sis in
pat
ient
s w/C
AD
and
hype
rcho
lest
erol
emia
•W
/bile
aci
d–bi
ndin
g re
sin:
pri
mar
y hy
perc
hole
ster
olem
iaIm
med
iate
-rel
ease
0.
25-6
g/d
, 350
0-m
g ta
blet
s$
niac
in*
divi
ded
dose
s
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 44

45www.AHDBonline.comVOL. 1 NO. 9
Pop
ulat
ions
w/
Cos
t,de
mon
stra
ted
Pri
mar
y ef
fect
Side
eff
ects
30-d
ayD
rug
Dos
age
rang
eA
vaila
ble
dose
sIn
dica
tion
sev
ent
redu
ctio
n†on
lipi
ds(m
ost
ofte
n re
port
ed)
supp
ly
Om
ega-
3 fa
tty
acid
*2-
4 g/
dV
ario
usH
yper
trig
lyce
ride
mia
(T
G ≥
500
mg/
dL)
•Hyp
erch
oles
tero
lem
ic Ja
pane
seT
G↓
Incr
ease
d bl
eedi
ng/b
ruis
ing,
$$(L
ovaz
a)pa
tient
s (ov
er st
atin
bac
kgro
und
25%
-45%
burp
ing,
indi
gest
ion,
ther
apy)
(JE
LIS22
) al
tere
d ta
ste
sens
e•P
atie
nts w
/rece
nt M
I (G
ISSI
-Pre
venz
ione
23)
Adv
icor
Nia
cin-
ERN
iaci
n-ER
–•H
yper
chol
este
role
mia
LDL↓
30%
-45%
See
unde
r$$
$$(n
iaci
n-ER
/50
0 m
g–lo
vasta
tinlo
vast
atin
•Mix
ed d
yslip
idem
iaH
DL↑
20%
-30%
com
pone
nts
lova
stat
in)
20 m
g/d to
niac
in-E
R50
0 m
g-20
mg
TG
↓ 3
0%-4
5%20
00 m
g–lo
vast
atin
750
mg-
20 m
g40
mg/
d10
00 m
g-20
mg
Sim
cor
Nia
cin-
ERN
iaci
n-ER
–•H
yper
chol
este
role
mia
LDL↓
10%
-15%
$$
$(n
iaci
n-ER
/50
0 m
g–si
mva
stat
in•M
ixed
dys
lipid
emia
HD
L↑ 2
0%-3
0%si
mva
stat
in)
sim
vast
atin
500
mg-
20 m
g•H
yper
trig
lyce
ride
mia
TG
↓15
%-4
0%20
mg/
d to
750
mg-
20 m
g(a
ll w
hen
mon
othe
rapy
(from
bas
eline
niac
in-E
R10
00 m
g-20
mg
inad
equa
te)
trea
tmen
t w/
2000
mg–
sim
vast
atin
sim
vast
atin
0-
20 m
g/d)
40 m
g/d
Vyt
orin
Ezet
imib
e 10
mg–
Ezet
imib
e–•P
rim
ary
hype
rlip
idem
iaLD
L↓$$
$$(e
zete
mib
e/si
mva
stat
insi
mva
stat
inor
mix
ed h
yper
lipid
emia
45%
-60%
sim
vast
atin
)10
mg/
d to
10 m
g-10
mg
•Hom
ozyg
ous F
Hez
etim
ibe
10 m
g–10
mg-
20 m
gsi
mva
stat
in10
mg-
40 m
g80
mg/
d10
mg-
80 m
g
*Gen
eric
ava
ilabl
e. †
Stud
ies l
iste
d in
this
col
umn
may
not
be
incl
uded
in F
DA
-app
rove
d in
dica
tion
s.LD
L-C
indi
cate
s low
-den
sity
lipop
rote
in c
hole
ster
ol; D
M, d
iabe
tes m
ellit
us; T
G, t
rigly
cerid
es; C
HD
, cor
onar
y he
art d
iseas
e; T
LC, t
hera
peut
ic li
fest
yle
chan
ges;
HD
L-C
, hig
h-de
nsity
lipo
prot
ein
chol
este
rol;
MI,
myo
card
ial i
nfar
ctio
n; C
AD
,co
rona
ry a
rter
y di
seas
e; F
H, f
amili
al h
yper
chol
este
role
mia
; CV
D, c
ardi
ovas
cula
r dise
ase;
TIA
, tra
nsie
nt is
chem
ic a
ttac
k; A
CS,
acu
te c
oron
ary
synd
rom
e; C
V, c
ardi
ovas
cula
r; G
I, ga
stro
inte
stin
al; C
R, c
ontr
olle
d re
leas
e; E
R, e
xten
ded
rele
ase.
1.Li
pid
Res
earc
h C
linic
s Pro
gram
: the
lipi
d re
sear
ch c
linic
s cor
onar
y pr
imar
y pr
even
tion
tria
l res
ults
. I. R
educ
tion
in in
cide
nce
of c
oron
ary
hear
t dis
ease
. JA
MA
. 198
4;25
1:35
1-36
4.2.
Hel
sink
i Hea
rt S
tudy
. Pri
mar
y pr
even
tion
tria
l wit
h ge
mfib
rozi
l in
mid
dle-
aged
men
wit
h dy
slip
idem
ia. N
Eng
l J M
ed. 1
987;
317:
1237
-124
5.3.
Rub
ins H
B, R
obin
s SJ,
Col
lins D
, et a
l. G
emfib
rozi
l for
the
seco
ndar
y pr
even
tion
of c
oron
ary
hear
t dis
ease
in m
en w
ith
low
leve
ls o
f hig
h-de
nsit
y lip
opro
tein
cho
lest
erol
. N E
ngl J
Med
.19
99;3
41:4
10-4
18.
4.Se
ver P
S, D
ahlö
f B, P
oulte
r NR
, et a
l. Pr
even
tion
of c
oron
ary
and
stro
keev
ents
wit
h at
orva
stat
in in
hyp
erte
nsiv
e pa
tien
ts w
ho h
ave
aver
age
or lo
wer
-tha
n-av
erag
e ch
oles
tero
l con
cent
rati
ons,
in th
e A
nglo
-Sca
n din
avia
n C
ardi
acO
utco
mes
Tri
al-L
ipid
Low
erin
g A
rm (
ASC
OT-
LLA
): a
mul
tice
ntre
rand
omis
ed c
ontr
olle
d tr
ial.
Lanc
et.
2003
;361
:114
9-11
58.
5.C
olho
un H
M, B
ette
ridg
e D
J, D
urri
ngto
n PN
, et a
l. Pr
imar
y pr
even
tion
of c
ardi
ovas
cula
r dis
ease
wit
h at
orva
stat
in in
type
2 d
iabe
tes i
n th
e C
olla
bora
tive
Ato
rvas
tati
n D
iabe
tes S
tudy
(C
AR
DS)
: mul
tice
ntre
rand
omis
ed p
lace
bo-
cont
rolle
d tr
ial.
Lanc
et. 2
004;
364:
685-
696.
6.La
Ros
a JC
, Gru
ndy
SM, W
ater
s DD
, et a
l. In
tens
ive
lipid
low
erin
g w
ith
ator
vast
atin
in p
atie
nts w
ith
stab
le c
oron
ary
dise
ase.
N E
ngl J
Med
. 200
5;35
2:14
25-1
435.
7.Pe
derse
n T
R, F
aerg
eman
O, K
aste
lein
JJ, e
t al.
Hig
h-do
se a
torv
asta
tin v
s usu
al-d
ose
simva
statin
for s
econ
dary
pre
vent
ion
afte
r myo
card
ial i
nfar
ctio
n: th
e ID
EAL
study
: a ra
ndom
ized
cont
rolle
d tri
al. J
AM
A. 2
005;
294:
2437
-244
5.8.
Kor
en M
J, H
unni
ngha
ke D
B; A
LLIA
NC
E In
vest
igat
ors.
Clin
ical
out
com
es in
man
aged
-car
e pa
tien
ts w
ith
coro
nary
hea
rt d
isea
se tr
eate
d ag
gres
sive
ly in
lipi
d-lo
wer
ing
dise
ase
man
agem
ent c
linic
s: th
e A
LLIA
NC
E st
udy.
J A
m C
oll
Car
diol
. 200
4;44
:177
2-17
79.
9.Pi
tt B
, Wat
ers D
, Bro
wn
WV,
et a
l. A
ggre
ssiv
e lip
id-l
ower
ing
ther
apy
com
pare
d w
ith
angi
opla
sty
in st
able
cor
onar
y ar
tery
dis
ease
. N E
ngl J
Med
. 199
9;34
1:70
-76.
10.S
chw
artz
GG
, Olss
on A
G, E
zeko
witz
MD
, et a
l. Ef
fect
s of a
torv
asta
tin o
n ea
rly re
curr
ent i
sche
mic
eve
nts i
n ac
ute
coro
nary
synd
rom
es: t
he M
IRA
CL
stud
y: a
rand
omize
d co
ntro
lled
tria
l. JA
MA
. 200
1;28
5:17
11-1
718.
11.C
anno
n C
P, B
raun
wal
d E,
McC
abe
CH
, et a
l. In
tens
ive
vers
us m
oder
ate
lipid
low
erin
g w
ith
stat
ins a
fter
acu
te c
oron
ary
synd
rom
es. N
Eng
l J M
ed. 2
004;
350:
1495
-150
4.12
.Am
aren
co P
, Bog
ouss
lavs
ky J,
Cal
laha
n A
3rd
, et a
l. H
igh-
dose
ato
rvas
tati
n af
ter s
trok
e or
tran
sien
t isc
hem
ic a
ttac
k. N
Eng
l J M
ed. 2
006;
355:
549-
559.
13.S
erru
ys P
W, D
e Fe
yter
PJ,
Ben
ghoz
i R, e
t al.
The
Les
col(
R)
Inte
rven
tion
Pre
vent
ion
Stud
y (L
IPS)
: a d
oubl
e-bl
ind,
pla
cebo
-con
trol
led,
rand
omiz
ed tr
ial o
f the
long
-ter
m e
ffect
s of f
luva
stat
in a
fter
succ
essf
ul tr
ansc
athe
ter t
hera
py in
pati
ents
wit
h co
rona
ry h
eart
dis
ease
. Int
J C
ardi
ovas
c In
terv
ent.
2001
;4:1
65-1
72.
14.D
owns
JR, C
lear
field
M, W
eis S
, et a
l. Pr
imar
y pr
even
tion
of a
cute
cor
onar
y ev
ents
wit
h lo
vast
atin
in m
en a
nd w
omen
wit
h av
erag
e ch
oles
tero
l lev
els:
resu
lts o
f AFC
APS
/Tex
CA
PS. A
ir F
orce
/Tex
as C
oron
ary
Ath
eros
cler
osis
Prev
enti
on S
tudy
. JA
MA
. 199
8;27
9:16
15-1
622.
15.S
heph
erd
J, C
obbe
SM
, For
d I,
et a
l. Pr
even
tion
of c
oron
ary
hear
t dis
ease
wit
h pr
avas
tati
n in
men
wit
h hy
perc
hole
ster
olem
ia. W
est o
f Sco
tlan
d C
oron
ary
Prev
enti
on S
tudy
Gro
up. N
Eng
l J M
ed. 1
995;
333:
1301
-130
7.16
.Sac
ks F
M, P
feffe
r MA
, Moy
e LA
, et a
l. T
he e
ffect
of p
rava
stat
in o
n co
rona
ry e
vent
s afte
r myo
card
ial i
nfar
ctio
n in
pat
ient
s with
ave
rage
cho
lest
erol
leve
ls. C
hole
ster
ol a
nd R
ecur
rent
Eve
nts T
rial i
nves
tigat
ors.
N E
ngl J
Med
. 199
6;33
5:10
01-1
009.
17.T
he L
ong-
Term
Inte
rven
tion
wit
h Pr
avas
tati
n in
Isch
aem
ic D
isea
se (
LIPI
D)
Stud
y G
roup
. Pre
vent
ion
of c
ardi
ovas
cula
r eve
nts a
nd d
eath
wit
h pr
avas
tati
n in
pat
ient
s wit
h co
rona
ry h
eart
dis
ease
and
a b
road
rang
e of
init
ial
chol
este
rol l
evel
s. N
Eng
l J M
ed. 1
998;
339:
1349
-135
7.18
.Rid
ker P
M, D
anie
lson
MIA
, Fon
seca
AH
, et a
l, fo
r the
JUPI
TER
Stu
dy G
roup
. Ros
uvas
tatin
to p
reve
nt v
ascu
lar e
vent
s in
men
and
wom
en w
ith e
leva
ted
C-r
eact
ive
prot
ein.
N E
ngl J
Med
. 200
8;35
9:21
95-2
207.
19.T
he S
cand
inav
ian
Sim
vast
atin
Sur
viva
l Stu
dy G
roup
. Ran
dom
ised
tria
l of c
hole
ster
ol lo
wer
ing
in 4
444
pati
ents
wit
h co
rona
ry h
eart
dis
ease
: the
Sca
ndin
avia
n Si
mva
stat
in S
urvi
val S
tudy
(4S
). L
ance
t. 19
94;3
44:1
383-
1389
.20
.Hea
rt P
rote
ctio
n St
udy
Col
labo
rativ
e G
roup
. MR
C/B
HF
Hea
rt P
rote
ctio
n St
udy
of c
hole
ster
ol lo
wer
ing
with
sim
vast
atin
in 2
0,53
6 hi
gh-r
isk in
divi
dual
s: a
rand
omise
d pl
aceb
o-co
ntro
lled
tria
l. La
ncet
. 200
2;36
0:7-
22.
21.C
anne
r PL,
Ber
ge K
G, W
enge
r NK
, et a
l. Fi
ftee
n ye
ar m
orta
lity
in C
oron
ary
Dru
g Pr
ojec
t pat
ient
s: lo
ng-t
erm
ben
efit
wit
h ni
acin
. J A
m C
oll C
ardi
ol. 1
986;
8:12
45-1
255.
22Yo
koya
ma
M, O
riga
sa H
, Mat
suza
ki M
, et a
l. Ef
fect
s of e
icos
apen
taen
oic
acid
on
maj
or c
oron
ary
even
ts in
hyp
erch
oles
tero
laem
ic p
atie
nts (
JELI
S): a
rand
omiz
ed, o
pen-
labe
l, bl
inde
d en
dpoi
nt a
naly
sis.
Lanc
et. 2
007;
369:
1090
-109
8.23
.Mar
chio
li R
, Sch
wei
ger C
, Tav
azzi
L, V
alag
ussa
F. E
ffica
cy o
f n-3
pol
yuns
atur
ated
fatt
y ac
ids a
fter
myo
card
ial i
nfar
ctio
n: re
sult
s of G
ISSI
-Pre
venz
ione
tria
l. G
rupp
o It
alia
no p
er lo
Stu
dio
della
Sop
ravv
iven
za n
ell’I
nfar
to M
ioca
rdic
o.Li
pids
. 200
1;36
(sup
pl):
S119
-S12
6.C
ost:
$ 0-
25, $
$ 26
-50,
$$$
51-
100,
$$$
$ 10
1-20
0, $
$$$$
>20
0 So
urce
s: C
linic
al d
ata
com
pile
d fr
om M
icro
med
ex w
ebsi
te. h
ttp:
//ww
w.th
omso
nhc.
com
. Acc
esse
d A
ugus
t 22,
200
8. C
ost i
nfor
mat
ion
from
ww
w.dr
ugst
ore.
com
. Acc
esse
d A
ugus
t 22,
200
8.
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 45

46 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
CLINICAL
FibratesFibric acid derivatives, or fibrates, such as gemfi-
brozil and fenofibrate, are agonists of the peroxisome-activated receptor-α in muscle, liver, and other tissues.Fibrates can lower TG levels by up to 50% and are therefore considered the first-line agents in patients with hypertriglyceridemia (TG >400 mg/dL).However, LDL-C reduction is variable (10%-15%),with some patients exhibiting increased levels of LDL-C. HDL-C levels may be increased up to 25% in patients with very high TG levels at baseline.17 Themost common adverse events are rash and dyspepsia for fenofibrate and GI disturbances for gemfibrozil. All fibrates may increase the risk of gallstones. In addi-tion, gemfibrozil has been shown to increase plasmaconcentration of statins, thereby increasing the risk ofmuscle toxicity.18
EzetimibeAs with bile acid sequestrants, ezetimibe inhibits the
absorption of cholesterol. However, since it does notinterfere with the absorption of other dietary fats, it isbetter tolerated. Ezetimibe localizes at the brush borderof the small intestine, where it binds to a critical medi-ator of cholesterol absorption, the Niemann-Pick C1-like 1 protein on the GI tract epithelial cells19 and livercells. Like the bile acid sequestrants, by reducing theavailability of LDL-C, ezetimibe also induces LDLreceptor upregulation leading to increased uptake ofLDL-C into cells, further lowering circulating LDL-Clevels. While ezetimibe effectively lowers LDL-C, stud-ies assessing clinical event reduction are lacking. In arecent study, no additional decrease in the carotid inti-ma-media thickness was demonstrated with ezetimibe-simvastatin combination therapy compared with sim-vastatin alone, despite significantly greater reductionin LDL-C in the combination group.20
In addition, in another study, an increased risk ofcancer death was observed in the simvastatin-ezetimibegroup compared with the placebo group,21 but an analy-sis of more than 20,000 patients in ongoing randomizedtrials revealed no increase in cancer risk in patientsreceiving ezetimibe compared with placebo.22 However,given the lack of documented outcome benefit withthis agent, the ACC recommends that it be reservedfor patients who cannot reach LDL-C goal with maxi-mal dose statins.11
Omega-3 Fatty AcidsEpidemiologic studies have demonstrated that peo-
ple who have diets rich in omega-3 fatty acids have a
lower risk of CV events compared with those with atypical Western diet. Studies of omega-3 fatty acidadministration have demonstrated reductions in TGsof up to 45% in patients with baseline TG levels >500mg/dL.23 Smaller reductions are expected in patientswith lower baseline levels. In addition to the reductionin TGs, HDL-C levels may be increased by as much as9%. The addition of omega-3 fatty acids to statin ther-apy produces further reductions in VLDL-C and TGsand further elevations in HDL-C. The putative mech-anisms for TG reduction with high-dose omega-3 fatsinclude increased beta oxidation. ■
ConclusionElevated cholesterol level is a major risk factor for
CVD, the leading cause of death worldwide. Reductionof LDL-C has been shown to decrease the risk of CVevents in a large number of clinical trials. Because theyare the best studied, have a favorable risk/benefit pro-file, and have been demonstrated to produce clinicalbenefits in many large trials, statins are the first-linetreatment for patients with hypercholesterolemia.
Disclosure StatementDr Moe is on the Speakers’ Bureau for Pfizer, BMS, Novartis,
Abbott, and GlaxoSmithKline. Drs Burns Schaiff and Krichbaum areemployees of Pfizer, Inc. Limited editorial support was provided byPaul Lane, PhD, at Envision Pharma, Ltd, and was funded byPfizer, Inc.
References1. Mensah GA, Brown DW. An overview of cardiovascular disease bur-den in the United States. Health Aff (Millwood). 2007;26:38-48.2. Rosamond W, Flegal K, Furie K, et al. Heart disease and stroke statis-tics—2008 update: a report from the American Heart AssociationStatistics Committee and Stroke Statistics Subcommittee. Circulation.2008;117:e25-146.3. The Lipid Research Clinics Coronary Primary Prevention TrialResults. I. Reduction in incidence of coronary heart disease. JAMA.1984;251:351-364.4. Brown G, Albers JJ, Fisher LD, et al. Regression of coronary artery dis-ease as a result of intensive lipid-lowering therapy in men with high lev-els of apolipoprotein B. N Engl J Med. 1990;323:1289-1298.5. Manson JE, Hsia J, Johnson KC, et al. Estrogen plus progestin and therisk of coronary heart disease. N Engl J Med. 2003;349:523-534.6. Barter PJ, Caulfield M, Eriksson M, et al. Effects of torcetrapib in pa -tients at high risk for coronary events. N Engl J Med. 2007;357:2109-2122.7. Expert Panel on Detection, Evaluation, and Treatment of High BloodCholesterol in Adults. Executive Summary of the Third Report of theNational Cholesterol Education Program (NCEP) Expert Panel onDetection, Evaluation, and Treatment of High Blood Cholesterol inAdults (Adult Treatment Panel III). JAMA. 2001;285:2486-2497.8. Grundy SM, Cleeman JI, Bailey Merz CN, et al. Implications ofrecent clinical trials for the National Cholesterol Education ProgramAdult Treatment Panel III guidelines. Circulation. 2004;110:227-239.9. National Kidney Foundation. K/DOQI Clinical practice guidelinesfor managing dyslipidemias in chronic kidney disease. Part 3: treatingdyslipidemias. Am J Kidney Dis. 2003;41(4 suppl 3):S39-S58.
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 46

47www.AHDBonline.comVOL. 1 NO. 9
Cholesterol Management
10. Adams RJ, Albers G, Alberts MJ, et al. Update to the AHA/ASArecommendations for the prevention of stroke in patients with strokeand transient ischemic attack. Stroke. 2008;39:1647-1652.11. American College of Cardiology. ACC Statement on ENHANCETrial. January 15, 2008. http://www.acc.org/enhance_statement.htm.Accessed October 10, 2008.12. Libby P. Current concepts of the pathogenesis of atherosclerosis.Circulation. 2001;104:365-372.13. Kinlay S. Low density lipoprotein-dependent and independenteffects of cholesterol lowering therapies on C-reactive protein: a meta-analysis. J Am Coll Cardiol. 2007;49:2003-2009.14. Cohen DE, Anania FA, Chalasani N; National Lipid AssociationStatin Safety Task Force Liver Expert Panel. An assessment of statinsafety by hepatologists. Am J Cardiol. 2006;97(8A):77C-81C.15. Canner PL, Furberg CD, Terrin ML, McGovern ME. Benefits ofniacin by glycemic status in patients with healed myocardial infarction(from the Coronary Drug Project). Am J Cardiol. 2005;95:254-257.16. Ferenchick G, Rovner D. Hepatitis and hematemesis complicatingnicotinic acid use. Am J Med Sci. 1989;298:191-193.
17. Guay DR. Micronized fenofibrate: a new fibric acid hypolipidemicagent. Ann Pharmacother. 1999;33:1083-1103.18. Noé J, Portmann R, Brun ME, Funk C. Substrate-dependent drug-drug interactions between gemfibrozil, fluvastatin and other organicanion-transporting peptide (OATP) substrates on OATP1B1,OATP2B1, and OATP1B3. Drug Metab Dispos. 2007;35:1308-1314.19. Garcia-Calvo M, Lisnock J, Bull HG, et al. The target of ezetimibeis Niemann-Pick C1-Like 1 (NPC1L1). Proc Natl Acad Sci. 2005;102:8132-8137.20. Kastelein JP, Akdim F, Stroes ES, et al. Simvastatin with or without eze-timibe in familial hypercholesterolemia. N Engl J Med. 2008;358: 1431-1443.21. Rossebo AB, Pedersen TR, Boman K, et al. Intensive lipid loweringwith simvastatin and ezetimibe in aortic stenosis. N Engl J Med. 2008;359:1343-1356.22. Peto R, Emberson J, Landray M, et al. Analysis of cancer data fromthree ezetimibe trials. N Engl J Med. 2008;359:1357-1366.23. Kris-Etherton PM, Harris WS, Appel LJ; American HeartAssociation. Nutrition Committee. Fish consumption, fish oil, omega-3fatty acids, and cardiovascular disease. Circulation. 2002;106:2747-2757.
Stakeholder PerspectivesExperts Debate Meaning of JUPITER for Clinical Practice
PHYSICIANS/PAYERS: Should the indications forstatins be expanded? This was the question that hadmany cardiovascular (CV) experts talking, but withlittle consensus, in light of the findings from theJUPITER (Justification for the Use of Statins inPrimary Prevention: An Intervention Trial EvaluatingRosuvastatin) study released in November 2008 at theAmerican Heart Association annual meeting andthen published in the New England Journal ofMedicine.1 The results have also created a buzz amongP & T Committee members: Should they change planbenefits for statins? Will physicians begin to prescribethe drugs to a new patient population even off-label?
JUPITER showed that apparently healthy indi-viduals with unremarkable levels of low-densitylipoprotein cholesterol (LDL-C) but with elevatedlevels of high-sensitivity C-reactive protein (hs-CRP)—2.0 mg/L or more—had a dramatic reduc-tion in the risk for CV events by taking rosuvastatin(Crestor) compared with placebo.
The large benefit of rosuvastatin—a 44% relativereduction in CV risk—surpassed the expectations ofthe lead investigator, Paul Ridker, MD, Director ofthe Center for Cardiovascular Disease Prevention atBrigham and Women’s Hospital, who has champi-oned the use of hs-CRP to estimate CV risk for quitesome time. “Getting CRP down appears to haveincremental benefit to lowering LDL cholesterol,”Dr Ridker said. “There was a large number in our
study who had an elevation of CRP without otherrisk factors, and this group had a benefit from rosu-vastatin as well.” Of those who fit the profile of thestudy population, 25 patients would need to be treat-ed to prevent 1 CV event, which is “smaller than weanticipated,” said Dr Ridker.
Steve Nissen, MD, Chairman of the Departmentof Cardiovascular Medicine at the Cleveland Clinic,is a believer in CRP testing and is already using it toguide treatment decisions. He noted that the reduc-tion in death and major CV events with rosuvastatinwas larger than in any other trial of a statin, and hewas impressed that it occurred after only an averageof 1.9 years of treatment (the study had beenplanned to last 5 years but was terminated earlybecause of the large benefit found).
According to Dr Nissen, applying the findingsfrom JUPITER to the US population could add 10million persons who could benefit from statins.
Critics point out that although the magnitude ofthe 44% relative reduction in risk was large, theabsolute risk reduction was rather small—only 0.9%(1.8% in the placebo group had an event comparedwith 0.9% in the rosuvastatin group). Of note, sub-jects enrolled in the trial were at low risk at baseline,and this low risk accounted for the small reductionin absolute risk. Only 157 of 8901 subjects takingplacebo had an event compared with 83 of 8901 ran-domized to rosuvastatin.
Continued
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 47

48 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
CLINICAL
Cholesterol Management: The Complexity of Multiple Effectives Treatments
PAYERS: High levels of serum cholesterol havelong been recognized as a significant risk factor forthe development and progression of atherosclerosis.Lowering cholesterol has been shown to effectivelyreduce mortality and morbidity associated with acutecoronary syndromes and stroke—2 of the top 3 caus-es of death in the United States. As our understand-ing of the role of cholesterol has evolved, we havecome to realize the individual effects that low-densi-ty lipoprotein (LDL) and high-density lipoproteincan have in risk assessment and modification.
As the authors of this article highlight, a largenumber of effective treatments are available. Theavailability of multiple agents adds to the complexi-ty of their use: Are all these agents equal in theirability to affect lipid levels? Are they equal in theirability to influence outcomes? For an individualpatient with a specific set of risk factors and a specif-ic lipid profile, which agents will best affect theirlipid panel and their overall risk of cardiovascular orcerebrovascular complications?
The availability of several effective treatmentsalso raises questions about thresholds for screeningand treatment. A number of organizations have pro-vided such guidance, including the American HeartAssociation, the National Cholesterol EducationProgram, the United States Preventive Services TaskForce (USPSTF), and the American Academy ofPediatrics. As is often the case for the clinicianattempting to determine the best recommendationfor a given patient, or for the patient attempting toparticipate in decision-making—the rapid develop-ment of new science and research and the conflict-ing guidance of expert panel recommendations cancompound the confusion. For example, the USPSTFcurrently recommends screening of patients olderthan 20 years, citing insufficient evidence for screen-ing younger populations. Meanwhile, a recommen-
dation issued in 2008 by the American Academy ofPediatrics is much more aggressive with regard toscreening, and even treatment, of children with cer-tain risk factors.1
This complexity is further increased with the pub-licity related to the early termination of theJUPITER trial (see previous page), which was pub-lished in November 2008.2 In JUPITER, patientswithout a history of cardiovascular disease, with LDLlevels <130 mg/dL but with high-sensitivity C-reac-tive protein levels of 2.0 mg/L or more, were ran-domized to receive rosuvastatin or placebo. The trialwas ended early because patients in the treatmentgroup showed very significant reductions in myocar-dial infarction, stroke, arterial revascularization, hos-pitalization for unstable angina, or death from car-diovascular causes. This study will raise questionsregarding the thresholds that must be met to initiatetherapy. It will also raise issues concerning the rela-tive effectiveness of various agents, depending ontheir ability to affect “inflammation” as a separaterisk factor for atherosclerosis.
Until the evidence becomes clearer, we mustempower clinicians facing these decisions with asmany options as possible. They must be able to per-sonalize therapy—the best agent for the individualpatient—without undue restrictions.
1. Daniels SR, Greer FR; Committee on Nutrition. Lipid screeningand cardiovascular health in childhood. Pediatrics. 2008;122:198-208.
2. Ridker PM, Danielson E, Fonseca FAH, et al, for the JUPITERStudy Group. Rosuvastatin to prevent vascular events in men andwomen with elevated C-reactive protein. N Engl J Med. 2008;359:2195-2207.
Thomas McCarter, MD, FACPChief Clinical OfficerExecutive Health Resources
Using Crestor to prevent 1 death in persons withelevated CRP levels has been estimated at $500,000,a cost that may be too high. Some suggest that pre-scribing Crestor to reduce CRP could add $8.9 bil-lion to the cost of treatment in this country. But thiscost would be reduced to about $25,000 to prevent 1death, using a generic statin, if generic statins are aseffective as the brand drug at reducing CRP levels.
Evidence indicates that all the statins reduce CRP,but to different degrees.
1. Ridker PM, Danielson E, Fonseca FAH, et al, for the JUPITER StudyGroup. Rosuvastatin to prevent vascular events in men and womenwith elevated C-reactive protein. N Engl J Med. 2008;359:2195-2207.
Wayne KuznarMedical Writer
Continued
ClinicalSchaiiff_NovDec .qxp:Cover 11/25/08 10:55 AM Page 48

49www.AHDBonline.comVOL. 1 NO. 9
MEDICAL TOURISM
Whether Americans are flocking overseas formedical care remains a question. One esti-mate put the number at 150,000 in 2006,1
jumping to 750,000 in 2007.2 Nevertheless, the popularpress continues to devote articles to this phenomenonthat may very well be creating the market.
The LureThe lure of medical tourism for patients is the ability
to obtain services for relatively cheap cost, which canhelp uninsured and underinsured Americans gain accessto care; allow richer patients to get services quicker; orenable private health plans to arrange “bargain care”elsewhere for their insured patients. This has fostered athriving industry in some countries, and the lay presshas found such outsourcing a source for attractive sto-ries—“recovering from a medical procedure while lyingon a palm-swept beach, relaxing by the hotel pool, orshopping for terrific bargains sounds good.”3
Just a few years ago, medical tourism was depicted ascare associated with an exotic vacation or with anattendant spa recovery postsurgery. Yet escalating med-ical costs began to make the travel portion seem rea-sonable for those who were denied access at home.Travel sections of newspapers featured pleased unin-sured working and poorer patients who received amuch-needed operation at a mere fraction of the UScost. Major publications (eg, New York Times, LosAngeles Times), generally in states bordering the PacificRim and Latin America, published stories accompaniedby advertisements for touring agencies, and thus beganthe fledgling middleman industry that generated atten-tion to medicine overseas.
The Los Angeles Times ran articles first examiningmedical tourism, later denoting its growth, and thenmarking it as a trend. Articles appeared in Arkansas,Tennessee, Washington, and other states removed fromthe nonstop airplane routes, as the public graduallybecame acquainted with travel for healthcare. Fox,CNN, and CBS’s “60 Minutes” ran segments on people
traveling for services. Forbes and the Wall Street Journalfocused on the business aspects of the phenomenon, asmiddlemen aggressively marketed it to consumers,employers, and insurers.
“Hot destinations” came into the spotlight—Singapore, India, Thailand, Mexico, Costa Rica, China,and more. And the base broadened. Europeans optingout of their national health systems, along with wealthyclientele from the Middle East and other regions, wereidentified as medical tourists. The Internet further facil-itated clever marketing campaigns by private providersseeking to service the burgeoning international market.
Cheaper care for dental services, cosmetic interven-tions, and specialty pharmacy began to be proffered in travel packages to lure patients to providers who arranged “customer care” in luxurious hotels, tout-ing huge savings for “quality care.” Inroads into “bargain surgery” in modern facilities with advancedequipment were made. Lower-cost facelifts, hormonetherapy, and the like now appeal to “aging cohorts” inthe developed world.
Many of the private hospitals across Asia haveEnglish-speaking and American-trained staff, who nowcan deliver organ and bone marrow transplants, ortho-pedic, oncology, cardiovascular, and more hi-tech andcomplex care. In 2007, Forbes’s article “Open-HeartSurgery—90% off!” highlighted the differences in costand quality of care between the United States andother countries.4
Thus, the media caught the fancy of comparativecosts as a way to promote access to affordable health-care for Americans, including small businesses. TheFinancial Times and San Francisco Chronicle covered the2008 Deloitte study, which found that almost 40% ofAmericans would travel abroad for care, provided thatquality appeared comparable with that in the UnitedStates.5 People with private insurance were more likelyto consider traveling.
In the medical literature, a discussion amongst pay-ers and providers has begun concerning medicaltourism. A 2006 New England Journal of Medicine arti-cle warned that “American physicians who are con-cerned about the growth of this phenomenon have two
Dr Salmon is Professor of Health Policy and Administration,School of Public Health, University of Illinois at Chicago, IL.
Promotion of Medical Tourism in theMedia Creates a TrendJ. Warren Salmon, PhD
MedTourismNovDec .qxp:Cover 11/25/08 11:16 AM Page 49

50 AMERICAN HEALTH & DRUG BENEFITS November/December 2008 VOL. 1 NO. 9
MEDICAL TOURISM
choices: they can denounce and attempt to restrict it,or they can lead and more actively support efforts byothers to speed the discovery and uptake of more effi-cient domestic healthcare delivery methods.”6
Policy Concerns Doubts about patient care quality abroad and poten-
tial safety issues emerged in the popular press before theprofessional literature. Can quality be assured? Whatabout complications when returning home? Will fol-low-up care at home be available? What is the legalrecourse in nations without malpractice laws or “a cul-ture” of suing doctors? A series of cautions is clearlyneeded for an unregulated medical tourism industry.
As the hubs for foreign care are investigated, assur-ances on such concerns are hard to come by. The US-based Joint Commission International accredits morethan 140 hospitals overseas, with a doubling of thatnumber projected in 2 years. But this is by no means acomplete safeguard to a botched surgery. Locationanalyses of provider destinations are necessary, alongwith specific reviews of providers, the host of entrepre-neurial middlemen making travel arrangements, andeven the motives and diligence of new US insurers andemployers who are looking for potential savings fromsending their insured members overseas.
AlterNet raises a concern that medical tourism maypose competition to the US healthcare system: “Theproblem with turning to medical tourism as an answerto healthcare problems goes beyond personal storiesand into the realm of hard policy. There are lots ofstakeholders that are eager to trump up medical tourismas a silver bullet for healthcare costs….[Some suggestthat ] since insurers and employers can pay less to coverprocedures, the US healthcare system will benefitgreatly from medical tourism.”7
It will be interesting to see how US payers respondto all this. And how the US government and others
react to this emerging phenomenon will be critical.Tourism is a trade that is under World TradeOrganization consideration. Siphoning off the wealthyto posh concierge care in private health systems over-seas and leaving a subpar public sector for the poorermasses pose ethical dilemmas. At a time of rising glob-al epidemics, for developing nations to neglect regula-tory directions to preserve and protect their publichealth is a concern.8
The lay press’ attention to medical tourism hashelped to create a new market, spurring entrepreneur-ial enterprises stateside to facilitate it, as well as settingup a host of private providers overseas to capitalize onthis nascent trend. This phenomenon has also pro-voked issues that force us to reflect on the impact ofglobalization at home and abroad. ■
References1. AMA press release. AMA provides first ever guidance on medicaltourism. June 16, 2008. http://www.ama-assn.org/ama/pub/category/18678.html. Accessed November 3, 2008.2. Madden CL. Medical tourism causes complications. October 27,2008. http://www.policyinnovations.org/ideas/briefings/data/000083.Accessed November 3, 2008.3. Kaderli B, Kaderli A. Medical vacations: the retiree health-care solution? MotleyFool.com. August 12, 2008. http://www.fool.com/personal-finance/retirement/2008/08/12/medical-vacations-the-retiree-health-care-solution. aspx. Accessed November 3, 2008.4. Forbes S. Open-heart surgery—90% off! Forbes. August 13, 2007.http://www.forbes.com/columnists/forbes/2007/0813/021.html. AccessedNovember 3, 2008.5. Deloitte. Medical tourism: consumers in search of value, 2008.http://www.deloitte.com/dtt/cda/doc/content/us_chs_MedicalTourismStudy(1).pdf. Accessed November 3, 2008.6. Milstein A, Smith M. America’s new refugees—seeking affordablesurgery offshore. N Engl J Med. 2006;355:1637-1640.7. Mahar M. Medical tourism is great—for those who can afford it.AlterNet. August 21, 2008. http://www.alternet.org/healthwellness/95827/medical_tourism_is_great_—_for_those_who_can_afford_it/.Accessed November 3, 2008.8. Salmon JW, Aruru M. Health tourism to India: challenges againstresource competition to sustaining a viable public health infrastructure forthe local populace. Presented at the Annual Expo and Meeting of theAmerican Public Health Association; San Diego, CA; October 27, 2008.
Signature (Required) ____________________________________ Date (Required) _________
Name ______________________________________________________________
Title ________________________________________________________________
Company ________________________________ Specialty ______________________
Address_____________________________________________________________
City/State/ZIP_________________________________________________________
E-mail _____________________________________ Phone ____________
FREE Subscription Request
Fax to (732) 992-1881
Request your FREE subscription to AMERICAN HEALTH & DRUG BENEFITS®
AHDB 11/08Incomplete cards will not be processed.
❑ YES! I would like to receive American Health & Drug Benefits ® as well as related educational supplements FREE!
❑ NO. Please discontinue my subscription.
MedTourismNovDec .qxp:Cover 11/25/08 11:16 AM Page 50

1 in 4 adults suffer from a diagnosable mental disorder
in any given year.1 Open access is especially important in the treatment of mental disorders because the response to therapy can vary greatly from individual to individual and from one medication to the next. Restrictions in the form of prior authorizations and preferred lists may have the unintended consequences of jeopardizing patient health while failing to reduce costs.
Open Access. Because different people
have different needs.Bristol-Myers Squibb supports open and unrestricted access to mental health medications. For people with mental illness, having access to newer and potentially more effective medications can be a crucial component of treatment.
N O T E V E R Y O N E I S C U T O U T F O R T H E S A M E T R E A T M E N T .
SUPPORT OPEN ACCESS AND GIVE PROVIDERS THE FREEDOM TO FIND THE MOST APPROPRIATE MEDICATION FOR EACH INDIVIDUAL.
1. National Institute of Mental Health. Available at: http://www.nimh.nih.gov/healthinformation/statisticsmenu.cfm. Accessed August 7, 2006.
D6-K0178DD October 2006 AA444681/10-06
D6K0178DD_8.125x10.875.indd 1 7/2/08 4:20:32 PM
Exec Sum_NovDecqxp.qxp:Cover 11/24/08 4:50 PM Page 51

VOL. 1 NO. 9
EXECUTIVE SUMMARIES
52 AMERICAN HEALTH & DRUG BENEFITS November/December 2008
Cardiovascular disease (CVD) remains the leadingcause of death worldwide. Hypercholesterolemia anddyslipidemia are significant risk factors for the develop-ment of CVD, which affects more than 80 millionAmericans. A team of 3 experts discusses the relation-ship between cholesterol levels and the risk of CVD,outlining the National Cholesterol Education Programguidelines for assessment and treatment of dyslipidemia,and summarizing current cholesterol targets. The firstgoal of therapy in hypercholesterolemia is reduction oflow-density lipoprotein (LDL) cholesterol levels.Evidence shows that statins are the most effective lipid-lowering agents available. Drs Schaiff, Moe, and
Krichbaum provide an extensive drug table that coversall lipid-lowering classes, their mechanisms of action,place in therapy, side effects, as well as costs. Finally,new evidence from the recently published JUPITERstudy has shown that in addition to lowering lipid lev-els, statins are important for preventing vascular eventsin patients with elevated C-reactive protein (CRP) lev-els, even in those with normal cholesterol levels. Adebate is currently raging among experts and decisionmakers whether persons with normal lipid levels butwith elevated CRP levels should be taking a statin on aregular basis. These results may have implications for allhealth benefit programs.
An Overview of Cholesterol ManagementBy Robyn A. Burns Schaiff, PharmD, BCPS; Richard M. Moe, MD, PhD; Daniel W. Krichbaum, PharmD
In this second interview, Dr Silver, director of theCancer Center Network at the Division ofHematology/Oncology at the University of MichiganHealth Systems, focuses on the impact of Medicare cov-erage decision for erythropoiesis-stimulating agents(ESAs), and why ESAs are so important for patients. Heemphasizes the risk of transfusions to cancer patientsand why policy decisions that restrict the use of ESAscan have profound implications for patients. Dr Silver,who is also Assistant Dean for Research at theUniversity of Michigan, calls for new studies, to be fund-ed by the manufacturers of the 2 major ESAs, to inves-
tigate the concerns for tumor progression and throm-boembolic events that are potentially associated withthese expensive medications. Such research could betterguide policy decisions by Medicare and improve patientcare. Despite the very high cost of the ESAs, the issue oftransfusions in cancer patients is beyond economics, DrSilver says, since they expose patients to unnecessaryrisks. And although Medicare is not supposed to consid-er costs in its decisions, cost is an underlying context forcoverage decisions, especially for as expensive medica-tions as ESAs, which nevertheless may reduce hospital-ization for transfusions, he says.
Erythropoiesis-Stimulating Agents in a Meta-Stable StateInterview (Part 2) with Samuel M. Silver, MD, PhD
Medication nonadherence is a major cause of mor-bidity and mortality in the United States. Non -adherence to drug therapy is also a major contributor toescalating costs of healthcare. Lack of information andforgetfulness are 2 main reasons cited by patients forlack of adherence. These 2 causes can be positivelyinfluenced by improved patient–provider communica-tion, Dr Ross explains. With chronic diseases estimatedto involve hundreds of millions of patients, the scale ofdisease management enrollment is too great to be cost-effective using traditional outreach methods. The chal-lenge is to scale outreach programs efficiently, without
losing the personal touch necessary to help changebehavior. Using communication automation to aug-ment traditional call center outreach can help to medi-ate patient medication-taking behaviors. Dr Rossreports results of his new study that involved an auto-mated telephony to 304 elderly patients with hyperten-sion. Using this automated system helped reduce costsand improve the blood pressure monitoring of patients.In addition to significant improvements in outcomes,174 patients had their antihypertensive regimen alteredbased on their responses to the survey part of the auto-mated system.
Role for Automated Communication Strategies in MedicationAdherence ManagementBy S. Michael Ross, MD, MHA
Exec Sum_NovDecqxp.qxp:Cover 11/24/08 4:50 PM Page 52