
NOVEDADES EN SABCS EN CANCER DE MAMA HER2+ · PDF fileNOVEDADES EN SABCS EN CANCER DE MAMA...
72
NOVEDADES EN SABCS EN CANCER DE MAMA HER2+ Prof. Miguel Martín Servicio de Oncología Médica Hospital General Universitario Gregorio Marañón Universidad Complutense Madrid [email protected]
Transcript of NOVEDADES EN SABCS EN CANCER DE MAMA HER2+ · PDF fileNOVEDADES EN SABCS EN CANCER DE MAMA...

NOVEDADES EN SABCS EN
CANCER DE MAMA HER2+
Prof. Miguel Martín
Servicio de Oncología Médica
Hospital General Universitario Gregorio Marañón
Universidad Complutense
Madrid

Mukohara T. Cancer Sci 102:1, 2011

Mukohara T. Cancer Sci 102:1, 2011
– Impaired access of trastuzumab
to HER2:
– Overexpression of extracellular
domain-truncated HER2 (p95
HER2)
• Overexpression of MUC4

Mukohara T. Cancer Sci 102:1, 2011
– Activating mutations or
deletions of downstream
proteins
• PI3K
• AKT
• Aberrating downstream
signaling caused by PTEN
loss

Mucohara T. Cancer Sci 102:1, 2011
– Activation of
compensatory pathways
• Other TK receptors:
IGFR1, EGFR, HER3, MET
• ER signaling

Mucohara T. Cancer Sci 102:1, 2011
– Cell cycle related
• Downregulation of p27
• Cyclin E overexpression


Pertuzumab
Mechanism of action

There are four receptors in the HER family
HER2 HER1/EGFR HER4 HER3
Yarden & Sliwkowski. Nat Rev Mol Cell Biol 2001;2:127–137 EGFR = epidermal growth factor receptor

There are four receptors in the HER family
• Receptors are able to homo- and heterodimerise
HER2 HER1/EGFR HER4 HER3
Yarden & Sliwkowski. Nat Rev Mol Cell Biol 2001;2:127–137 EGFR = epidermal growth factor receptor

There are four receptors in the HER family
• Receptors are able to homo- and heterodimerise • HER2 does not appear to have a direct ligand and HER3 lacks kinase activity
HER2 HER3
Yarden & Sliwkowski. Nat Rev Mol Cell Biol 2001;2:127–137 EGFR = epidermal growth factor receptor

There are four receptors in the HER family
• Receptors are able to homo- and heterodimerise • HER2 does not appear to have a direct ligand and HER3 lacks kinase activity • However, HER2 and HER3 are highly complementary to each other
HER2 HER3
Yarden & Sliwkowski. Nat Rev Mol Cell Biol 2001;2:127–137 EGFR = epidermal growth factor receptor

Homodimers Heterodimers
HER2:HER3 dimers initiate the strongest mitogenic signalling
HER1:HER1 HER2:HER2
HER3:HER3 HER4:HER4
HER1:HER2 HER1:HER3 HER1:HER4
HER2:HER4 HER3:HER4
Tzahar et al. Mol Cell Biol 1996;16:5276–5287; Citri et al. Exp Cell Res 2003;284:54–65; Huang et al. Cancer Res 2010;70:1204–1214.
HER2:HER3

Homodimers Heterodimers
HER2:HER3 dimers initiate the strongest mitogenic signalling
HER1:HER1 HER2:HER2
HER3:HER3 HER4:HER4
HER1:HER2 HER1:HER3 HER1:HER4
HER2:HER4 HER3:HER4
Tzahar et al. Mol Cell Biol 1996;16:5276–5287; Citri et al. Exp Cell Res 2003;284:54–65; Huang et al. Cancer Res 2010;70:1204–1214.
Signalling activity
+ + + + + + + + + + + + + + + +
+
HER2:HER3

HER2 dimerises preferentially with HER3 to drive downstream signalling
Baselga, Swain. Nat Rev Cancer 2009;9:463–475; Yarden, Sliwkowski. Nat Rev Mol Cell Biol 2001;2:127–137; Graus-Porta et al. EMBO J 1997;1647–1655; Tzahar et al. Mol Cell Biol 1996;16:5276–5287;
Lee-Hoeflich et al. Cancer Res 2008;68:5878–5887.
HER2 HER3

HER2 dimerises preferentially with HER3 to drive downstream signalling
Ligand-activated HER2:HER3 dimer
Baselga, Swain. Nat Rev Cancer 2009;9:463–475; Yarden, Sliwkowski. Nat Rev Mol Cell Biol 2001;2:127–137; Graus-Porta et al. EMBO J 1997;1647–1655; Tzahar et al. Mol Cell Biol 1996;16:5276–5287;
Lee-Hoeflich et al. Cancer Res 2008;68:5878–5887.
HER2 HER3

HER2 dimerises preferentially with HER3 to drive downstream signalling
Ligand-activated HER2:HER3 dimer
Baselga, Swain. Nat Rev Cancer 2009;9:463–475; Yarden, Sliwkowski. Nat Rev Mol Cell Biol 2001;2:127–137; Graus-Porta et al. EMBO J 1997;1647–1655; Tzahar et al. Mol Cell Biol 1996;16:5276–5287;
Lee-Hoeflich et al. Cancer Res 2008;68:5878–5887.
HER2 HER3
Phosphorylation of the HER3 intracellular domain by HER2
initiates a signalling cascade
P P P P

Please refer to disclaimer on slide 2
Akt
Shc
HER2:HER3 dimerisation initiates multiple signalling pathways,
including increased tumour cell proliferation
Downstream PI3K/Akt signalling is mainly mediated
by HER3 after transphosphorylation by HER2
Yarden, Sliwokowski. Nat Rev Mol Cell Biol 2001;2:127–137; Olayioye et al. EMBO J 2000;19:3159–3167; Kim et al. J Biol Chem 1994;269:24747–24755; Soltoff et al. Mol Cell Biol 1994;14:3550–3558;
HER2 HER3
GRb2 Sos RAS
PI3K P P
P P PDK1
P P P
RAF
MEK
MAPK P
P
mTOR
Cyclin 01
GSK36
NF B
BAD
p27
Angiogenesis Proliferation
Cell cycle control
Apoptosis
Survival

Please refer to disclaimer on slide 2
Pertuzumab is the first in a new class of targeted anticancer
therapeutic agents called HER2 Dimerisation Inhibitors
By blocking HER2 dimerisation, pertuzumab inhibits key HER
signalling pathways that mediate cancer cell proliferation and survival1–
4
Pertuzumab prevents the formation of HER2:HER3 receptor pairs1,5
HER2
Dimerisation domain
1. Agus et al. Cancer Cell 2002;2:127–137; 2. Baselga. Cancer Cell 2002;2:93–95; 3. Citri et al. Exp Cell Res 2003;284:54–65. 4. Franklin et al. Cancer Cell 2004;5:317–328;
5. Hughes et al. Mol Cancer Ther 2009;8:1885–1892
HER3

Please refer to disclaimer on slide 2
Pertuzumab is the first in a new class of targeted anticancer
therapeutic agents called HER2 Dimerisation Inhibitors
By blocking HER2 dimerisation, pertuzumab inhibits key HER
signalling pathways that mediate cancer cell proliferation and survival1–
4
Pertuzumab prevents the formation of HER2:HER3 receptor pairs1,5
HER2
Dimerisation domain
1. Agus et al. Cancer Cell 2002;2:127–137; 2. Baselga. Cancer Cell 2002;2:93–95; 3. Citri et al. Exp Cell Res 2003;284:54–65. 4. Franklin et al. Cancer Cell 2004;5:317–328;
5. Hughes et al. Mol Cancer Ther 2009;8:1885–1892
Pertuzumab
HER3

Please refer to disclaimer on slide 2
Pertuzumab is the first in a new class of targeted anticancer
therapeutic agents called HER2 Dimerisation Inhibitors
By blocking HER2 dimerisation, pertuzumab inhibits key HER
signalling pathways that mediate cancer cell proliferation and survival1–
4
Pertuzumab prevents the formation of HER2:HER3 receptor pairs1,5
HER2
Dimerisation domain
1. Agus et al. Cancer Cell 2002;2:127–137; 2. Baselga. Cancer Cell 2002;2:93–95; 3. Citri et al. Exp Cell Res 2003;284:54–65. 4. Franklin et al. Cancer Cell 2004;5:317–328;
5. Hughes et al. Mol Cancer Ther 2009;8:1885–1892
Pertuzumab
HER3

Summary of pertuzumab combination trials in HER2-positive breast cancer
EBC (Neo-adjuvant)
First-line MBC Third-line MBC Second-line MBC
BO17929 cohorts 1+2 (n=66) P+T
BO17929 cohort 3 (n=29) P mono then P+T
NCI study (n=11) P+T
CLEOPATRA (n=800) D+T±P
PHEREXA (n=450)
Capecitabine+T±P
NEOSPHERE (n=400)
D+T vs D+T+P vs T+P vs D+P
TRYPHAENA (n=225)
D+FEC+T+P vs carboplatin+D+T+P
Enrolling Enrolment complete
Data on file. Genentech USA, Inc., CA, USA and F Hoffmann-La Roche Ltd., Basel, Switzerland
D = docetaxel; EBC = early-stage breast cancer; FEC = 5-fluorouracil, epirubicin, cyclophosphamide; MBC = metastatic breast cancer; P = pertuzumab; T = trastuzumab

San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6‒10, 2011
Copyrights for this presentation are held by the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
Neoadjuvant Pertuzumab and Trastuzumab Concurrent
or Sequential with an Anthracycline-Containing or
Concurrent with an Anthracycline-Free Standard
Regimen: A Randomized Phase II Study (TRYPHAENA)
A Schneeweiss,1 S Chia,2 T Hickish,3 V Harvey,4 A Eniu,5 R Hegg,6
C Tausch,7 J-H Seo,8 Y-F Tsai,9 A Ackrill,10 G Ross,10 J Cortés11
1National Center for Tumor Diseases, University Hospital, Heidelberg, Germany;
2British Columbia Cancer Agency – Vancouver Centre, University of British Columbia, Vancouver, Canada; 3Royal Bournemouth Hospital, Bournemouth University, Bournemouth, UK; 4Regional Cancer and Blood Centre, Auckland
City Hospital, Auckland, New Zealand; 5Cancer Institute “I Chiricuta”, Cluj-Napoca, Romania; 6Hospital Pérola Byington, São Paulo, Brazil; 7Breast Center, Zürich, Switzerland;
8Department of Internal Medicine, Korea University Guro Hospital, Korea; 9Taipei-Veterans General Hospital, Taipei, Taiwan;
10Roche Products Limited, Welwyn, United Kingdom; 11Vall d'Hebron University Hospital, Barcelona, Spain

Copyrights for this presentation are held by the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6‒10, 2011
24
Study design
AUC, area under the plasma concentration-time curve; EBC, early breast cancer; FEC, 5-fluorouracil, epirubicin, cyclophosphamide
HER2-positive
EBC
centrally confirmed
(n = 225)
FEC
Trastuzumab
to complete
1 year
S
u
r
g
e
r
y
• All 3 arms were experimental
• Study dosing q3w: − FEC: 500 mg/m2, 100 mg/m2, 600 mg/m2
− Carboplatin: AUC 6
− Trastuzumab: 8 mg/kg loading dose, 6 mg/kg maintenance
− Pertuzumab: 840 mg loading dose, 420 mg maintenance
− Docetaxel: 75 mg/m2 (escalating to 100 mg/m2 if tolerated, in Arms A and B only)
Docetaxel
Cycles 1‒3 4‒6
Pertuzumab + trastuzumab
Pertuzumab + trastuzumab
FEC Docetaxel
Carboplatin
Docetaxel
Pertuzumab + trastuzumab C
B
A

Copyrights for this presentation are held by the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6‒10, 2011
25
Study endpoints
• Primary endpoint:
– Cardiac safety
• Symptomatic LVSD (grade ≥3)
• LVEF declines (≥10 percentage points and below 50%)
• Secondary endpoints:
– Toxicity
– pCR (defined as the absence of invasive tumor residues in the breast at surgery; remaining in situ lesions allowed; ypT0/is)
• Study was not powered for formal comparison between arms
– Clinical response rate
– Rate of breast-conserving surgery
– Disease-free survival and overall survival
– Biomarker evaluation
LVEF, left ventricular ejection fraction; LVSD, left ventricular systolic dysfunction; pCR, pathologic complete response

Copyrights for this presentation are held by the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6‒10, 2011
26
Cardiac events during neoadjuvant treatment
FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; LVEF, left ventricular ejection fraction; LVSD, left ventricular systolic dysfunction;
P, pertuzumab; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
FEC+H+P x3
T+H+P x3
n = 72
FEC x3 T+H+P x3
n = 75
TCH+P x6
n = 76
Symptomatic LVSD (grade ≥3),
n (%) 0 (0.0) 2 (2.7) 0 (0.0)
LVSD (all grades), n (%) 4 (5.6) 3 (4.0) 2 (2.6)
LVEF decline ≥10% points and
below 50%, n (%) 3 (4.2) 4 (5.3) 3 (3.9)

Copyrights for this presentation are held by the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6‒10, 2011
27
Pathologic complete response
FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; P, pertuzumab; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
Pa
tho
log
ic c
om
ple
te r
es
po
ns
e (
%)
FEC+H+P x3
T+H+P x3
(n = 73)
FEC x3
T+H+P x3
(n = 75)
TCH+P x6
(n = 77)
50.7
45.3
51.9
ypT0/is ypT0 ypN0
61.6
66.2
57.3

Copyrights for this presentation are held by the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6‒10, 2011
28
Summary and conclusions
• Results from TRYPHAENA indicate a low incidence of symptomatic and asymptomatic LVSD across all arms
– Concurrent administration of pertuzumab plus trastuzumab with epirubicin resulted in similar cardiac tolerability compared with sequential administration or the anthracycline-free regimen
• Regardless of chemotherapy chosen, the combination of pertuzumab with trastuzumab in the neoadjuvant setting resulted in high pCR rates (57‒66%)
• TRYPHAENA supports the ongoing APHINITY study, a Phase III trial to evaluate pertuzumab and trastuzumab plus standard chemotherapy in the adjuvant setting (poster: OT1-02-04) (NCT01358877)

Original Article Pertuzumab plus Trastuzumab plus Docetaxel for
Metastatic Breast Cancer
José Baselga, M.D., Ph.D., Javier Cortés, M.D., Sung-Bae Kim, M.D., Seock-Ah Im, M.D., Roberto Hegg, M.D., Young-Hyuck Im, M.D., Laslo
Roman, M.D., José Luiz Pedrini, M.D., Tadeusz Pienkowski, M.D., Adam Knott, Ph.D., Emma Clark, M.Sc., Mark C. Benyunes, M.D., Graham
Ross, F.F.P.M., Sandra M. Swain, M.D., for the CLEOPATRA Study Group
N Engl J Med Volume 366(2):109-119
January 12, 2012

CLEOPATRA: Study design
MBC, metastatic breast cancer; PD, progressive disease
Patients with
HER2-positive MBC
centrally confirmed
(N = 808)
Placebo + trastuzumab n=406
• Randomization was stratified by geographic region and prior treatment
status (neo/adjuvant chemotherapy received or not)
• Study dosing q3w: − Pertuzumab/Placebo: 840 mg loading dose, 420 mg maintenance
− Trastuzumab: 8 mg/kg loading dose, 6 mg/kg maintenance
− Docetaxel: 75 mg/m2, escalating to 100 mg/m2 if tolerated
1:1
n=402
Docetaxel* ≥6 cycles recommended
PD
Pertuzumab + trastuzumab
Docetaxel* ≥6 cycles recommended
PD
* <6 cycles allowed for unacceptable toxicity or PD; >6 cycles allowed at investigator discretion

Study endpoints
• Primary endpoint
– Independently assessed progression-free survival (PFS)
• Secondary endpoints
– PFS by investigator assessment
– Objective response rate
– Overall survival
– Safety
– Duration of response
– Evaluation of biomarkers and correlation with clinical outcomes
– Time to symptom progression

Baseline characteristics (I)
Placebo
+ trastuzumab + docetaxel
(n = 406)
Pertuzumab
+ trastuzumab + docetaxel
(n = 402)
Median age, years
(range)
54.0
(27–89)
54.0
(22–82)
Region, n (%)
Asia
Europe
North America
South America
128 (31.5)
152 (37.4)
68 (16.7)
58 (14.3)
125 (31.1)
154 (38.3)
67 (16.7)
56 (13.9)
ECOG PS, n (%)
0
1
≥2
248 (61.1)
157 (38.7)
1 (0.2)
274 (68.2)
125 (31.1)
3 (0.7)
ECOG PS, Eastern Cooperative Oncology Group performance status

Primary endpoint: Independently assessed PFS n = 433 PFS events
D, docetaxel; PFS, progression-free survival; Pla, placebo; Ptz, pertuzumab; T, trastuzumab
0 5 10 15 20 25 30 35 40
0
10
20
30
40
50
60
70
80
90
100
n at risk
402 345 267 139 83 32 10 0 0 Ptz + T + D
406 311 209 93 42 17 7 0 0 Pla + T + D
Time (months)
Ptz + T + D: median 18.5 months
Pla + T + D: median 12.4 months
HR = 0.62
95% CI 0.51‒0.75
p<0.0001
∆ = 6.1 months
Pro
gre
ss
ion
-fre
e s
urv
ival
(%)
Stratified by prior treatment status and region

808 0.63 0.52‒0.76
432 0.63 0.49‒0.82 376 0.61 0.46‒0.81
306 0.72 0.53‒0.97 135 0.51 0.31‒0.84 114 0.46 0.27‒0.78 253 0.68 0.48‒0.95 681 0.65 0.53‒0.80 127 0.52 0.31‒0.86 789 0.64 0.53‒0.78 19 0.55 0.12‒2.54
480 0.62 0.49‒0.80 30 0.64 0.23‒1.79 261 0.68 0.49‒0.95 37 0.39 0.13‒1.18
630 0.55 0.45‒0.68 178 0.96 0.61‒1.52
388 0.72 0.55‒0.95 408 0.55 0.42‒0.72 12 ─
721 0.60 0.49‒0.74
767 0.64 0.53‒0.78
n HR 95% CI
All
No Yes
Europe North America South America
Asia
<65 years ≥65 years
<75 years ≥75 years
White Black Asian Other
Visceral disease Non-visceral disease
Positive Negative
Unknown
IHC 3+
FISH-positive
0 0.2
ER/PgR status
Disease type
Race
Age group
Region
HER2 status
Prior (neo)adjuvant chemotherapy
0.4 0.6 1 2
Independently assessed PFS in predefined subgroups
ER, estrogen receptor; IHC, immunohistochemistry; FISH, fluorescence in situ hybridization; PgR, progesterone receptor;
PFS, progression-free survival
Favors placebo
Favors pertuzumab
Unstratified analyses

Independently assessed PFS by prior trastuzumab
therapy in patients with (neo)adjuvant therapy
PFS, progression-free survival
Placebo
+ trastuzumab
+ docetaxel
Median PFS, months
Pertuzumab
+ trastuzumab
+ docetaxel
Median PFS, months
Hazard ratio
(CI)
Prior (neo)adjuvant
trastuzumab treatment
(n = 88)
10.4 16.9 0.62
(0.35‒1.07)
No prior (neo)adjuvant
trastuzumab treatment
(n = 288)
12.6 21.6 0.60
(0.43‒0.83)

Independently reviewed objective response In patients with measurable disease at baseline
Placebo
+ trastuzumab
+ docetaxel
(n = 336)
Pertuzumab
+ trastuzumab
+ docetaxel
(n = 343)
Objective response rate, n (%)
Complete response rate, n (%)
Partial response rate, n (%)
233 (69.3)
14 (4.2)
219 (65.2)
275 (80.2)
19 (5.5)
256 (74.6)
p = 0.0011*
Stable disease, n (%) 70 (20.8) 50 (14.6)
Progressive disease, n (%) 28 (8.3) 13 (3.8)
Unable to assess or no assessment,
n (%) 5 (1.5) 5 (1.5)
* The statistical test result is deemed exploratory

Overall survival: Predefined interim analysis Median follow-up: 19.3 months, n = 165 OS events
D, docetaxel; OS, overall survival; Pla, placebo; Ptz, pertuzumab; T, trastuzumab
0 5 10 15 20 25 30 35 40 45
0
10
20
30
40
50
60
70
80
90
100
n at risk
Pertuzumab + T + D 402 387 367 251 161 87 31 4 0 0
406 383 347 228 143 67 24 2 0 0 Placebo + T + D
Time (months)
Ptz + T + D: 69 events
Pla + T + D: 96 events
HR = 0.64*
95% CI 0.47‒0.88
p = 0.0053*
* The interim OS analysis did not cross the pre-specified O’Brien-Fleming stopping boundary (HR ≤0.603; p ≤0.0012)
Overa
ll s
urv
iva
l (%
)

Safety results

Cardiac tolerability
LVEF, left ventricular ejection fraction; LVSD, left ventricular systolic dysfunction
Placebo
+ trastuzumab + docetaxel
(n = 397)
Pertuzumab
+ trastuzumab + docetaxel
(n = 407)
Investigator-assessed
symptomatic LVSD* 1.8% 1.0%
Independently adjudicated
symptomatic LVSD* 1.0% 1.0%
Fall in LVEF to <50% and by
≥10 percentage points from
baseline
6.6% 3.8%
* LVSD was defined as NYHA class III/IV

Adverse events (all grades)
≥25% incidence or ≥5% difference between arms
Adverse event, n (%)
Placebo
+ trastuzumab + docetaxel
(n = 397)
Pertuzumab
+ trastuzumab + docetaxel
(n = 407)
Diarrhea 184 (46.3) 272 (66.8)
Alopecia 240 (60.5) 248 (60.9)
Neutropenia 197 (49.6) 215 (52.8)
Nausea 165 (41.6) 172 (42.3)
Fatigue 146 (36.8) 153 (37.6)
Rash 96 (24.2) 137 (33.7)
Decreased appetite 105 (26.4) 119 (29.2)
Mucosal inflammation 79 (19.9) 113 (27.8)
Asthenia 120 (30.2) 106 (26.0)
Peripheral edema 119 (30.0) 94 (23.1)
Constipation 99 (24.9) 61 (15.0)
Febrile neutropenia 30 (7.6) 56 (13.8)
Dry skin 17 (4.3) 43 (10.6)

Summary and conclusions
• CLEOPATRA met its primary endpoint and demonstrated a statistically
significant and clinically meaningful improvement in PFS (HR = 0.62) in
patients with HER2-positive MBC
– Median PFS increased by 6.1 months from 12.4 to 18.5 months
– The PFS improvement was consistent across subgroups and supported by
the secondary endpoints of ORR and OS (immature)
• The combination of pertuzumab and trastuzumab plus docetaxel increased rates
of diarrhea, rash, mucosal inflammation, febrile neutropenia, and dry skin
– These adverse events were primarily grades 1‒2, manageable, and occurred
during docetaxel therapy
– There was no increase in cardiac adverse events or LVSD
• This new regimen may be practice-changing in HER2-positive
first-line MBC

clinicaloptions.com/oncology
An Update on Metastatic Breast Cancer
Women with previously
untreated HER2-positive
locally recurrent/metastatic
breast cancer
(N = 424)
Trastuzumab 6 mg/kg† +
Docetaxel 100 mg/m2 +
Bevacizumab 15 mg/kg,
all given q3w
(n = 216)
Trastuzumab 6 mg/kg† +
Docetaxel 100 mg/m2,
both given q3w
(n = 208)
Treatment until disease progression
or unacceptable toxicity*
Stratified by previous (neo)adjuvant taxane,
adjuvant trastuzumab, hormone receptor status,
measurable disease
*Planned minimum of 6 docetaxel cycles administered. †Trastuzumab 8 mg/kg loading dose given.
Gianni L, et al. SABCS 2011. Abstract S4-8.
AVEREL: Study Design
Primary endpoint: PFS (investigator assessed)
Secondary endpoints: OS, ORR, duration of response, TTF, safety

clinicaloptions.com/oncology
An Update on Metastatic Breast Cancer
AVEREL: PFS, Interim OS Analysis, and
Response
ORR similar between T + Doc + Bev and T + Doc in investigator assessment (74.3% vs 69.9, respectively; P = .3492)
ORR significantly higher with addition of Bev in IRC assessment (76.5% vs 65.9, respectively; P = .0265)
Outcome, Mos T + Doc + Bev
(n = 216)
T + Doc
(n = 208)
HR (95% CI) P Value
Median PFS
(Investigator assessment) 16.5 13.7
0.82
(0.65-1.02) .0775
Median PFS
(IRC assessment) 16.8 13.9
0.72
(0.54-0.94) .0162
Median OS 38.5 38.3
1.01
(0.74-1.38)
(unstratified)
.9543
0.94
(0.68-1.30)
(stratified)
.7078
Gianni L, et al. SABCS 2011. Abstract S4-8.

clinicaloptions.com/oncology
An Update on Metastatic Breast Cancer
AVEREL: Conclusions
Addition of bevacizumab to first-line treatment with trastuzumab and docetaxel in patients with HER2-positive advanced breast cancer may prolong PFS
– Findings not significant according to investigator-assessed PFS (primary endpoint; P = .0775)
– Findings significant according to independent review of PFS (exploratory endpoint; P = .0162)
Bevacizumab-associated AEs led to higher incidence of discontinuation of any study drug
Gianni L, et al. SABCS 2011. Abstract S4-8.

45
A Phase 2, Randomized, Open-label Study of
Neratinib (HKI-272) Versus Lapatinib Plus
Capecitabine for 2nd/3rd-line Treatment of HER2+
Locally Advanced or Metastatic Breast Cancer
Miguel Martin,1 Jacques Bonneterre,2 Charles E. Geyer Jr,3 Yoshinori Ito,4 Jungsil Ro,5 Istvan Lang,6 Sung-Bae Kim,7
Caroline Germa,8,* Jennifer Vermette,9 Marie-Louise Vo Van,8 Kenneth Wang,9,* Kongming Wang,9 Ahmad Awada10
1Hospital Universitario Gregorio Marañón, Madrid, Spain; 2Centre Oscar Lambret, Lille, France; 3University of Texas Southwestern Medical Center, Dallas, TX, USA; 4The Cancer
Institute Hospital of JFCR, Tokyo, Japan; 5National Cancer Center, Goyang, Korea; 6National Institute of Oncology, Budapest, Hungary; 7Asan Medical Center, Seoul, Korea; 8Pfizer Global Research and Development, Paris, France; 9Pfizer Inc, Cambridge, MA, USA; 10Jules Bordet
Institute, Brussels, Belgium.
*This author was employed at Pfizer during the conduct of this study, but has since become employed at another company.
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

46
Phase 2, open-label
trial in HER2+
locally advanced or
metastatic BC
patients
Neratinib
240 mg/day
n = 117
L + C
L 1,250 mg/day + C 2,000 mg/m2 per day
n = 116
R
A
N
D
O
M
I
Z
E
Randomization is stratified based on geographical regions.
Study Design (cont)
● Patients were randomized 1:1 to neratinib or L + C
– Neratinib was administered orally at 240 mg/day continuously
– L 1,250 mg/day was administered orally continuously;
C 2,000 mg/m2 was administered orally on Days 1 to 14 of each
21-day cycle
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

47
1. Calculated from data published in Cameron D, et al. Breast Cancer Res Treat. 2008;112(3):533-543.
Phase 2 Sample Size Determination
● Non-inferiority design intended to show that neratinib monotherapy
was not inferior to L + C
● Assumption was for non-inferiority in terms of PFS, defined as a
non-inferiority margin of 15% equivalent to retaining 50% of the
benefit demonstrated for L + C over capecitabine monotherapy1
● A total of 163 PFS events were needed for analysis, given the
following assumptions for sample size calculations
– Median PFS of 27.5 weeks for the L + C arm and 33.9 weeks for
the neratinib arm (25% improvement in median PFS; true hazard
ratio = 0.80)
– Enrollment rate of approximately 3 patients per week
– Design based on a 1-sided log-rank test
• Alpha = 0.1; power = 85%; 1-year dropout rate = 20%
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

48
Baseline Characteristics: ITT Population
Characteristic
Neratinib
(n = 117)
L + C
(n = 116)
Median age (range), y 52 (28–79) 56 (30–79)
Ethnicity, %
White 66 55
Asian 27 40
Other 7 5
ECOG Performance Status, %a
0 60 60
1 37 34
2 3 4
Estrogen receptor–positive, %b 44 40
Progesterone receptor–positive, %c 27 28
No. of prior anti-cancer regimens, %
1 14 14
2 33 33
≥3 53 53
Prior trastuzumab therapy, %
Adjuvant/neoadjuvant settings 20 32
Metastatic setting 79 68 L, lapatinib; C, capecitabine; ECOG, Eastern Cooperative Oncology Group. aECOG information was missing for 1 patient (1%) in the neratinib arm and 3 (3%) patients in the L + C arm. bEstrogen receptor status was unknown for 1 (1%) patient in the neratinib arm and 2 (2%) patients in the L + C arm. cProgesterone receptor status was unknown for 31 (26%) patients in the neratinib arm and 32 (28%) patients in the L + C arm.
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

49
Incidences of Diarrhea and PPE:
Safety Population
0
20
40
60
80
100
Neratinib L + C
Pa
tie
nts
wit
h d
iarr
he
a (
%)
P = 0.002
85% all grades
28% grade 3/4
68% all grades
10% grade 3/4
n = 116 n = 115
Neratinib L + C
Grade 1/2 Grade 1/2
Grade 3/4 Grade 3/4
0
20
40
60
80
100
Neratinib L + C
Pa
tie
nts
wit
h P
PE
(%
)
P <0.001
5% all grades
0% grade 3/4
65% all grades
14% grade 3/4
n = 116 n = 115
PPE, palmar-plantar erythrodysesthesia syndrome; L, lapatinib; C, capecitabine.
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

50
Treatment Modifications, Discontinuations,
and Deaths Due to Adverse Events
Modification, %
Neratinib
(n = 116)
L + C
(n = 115)
Dose reduction 19 53
Dose delay 32 74
Treatment discontinuationsa 6 17
Diarrhea 2 4
Nausea 0 2
Stomatitis 0 2
PPE 0 4
Dizziness 0 2
Deaths 0 0
L, lapatinib; C, capecitabine; PPE, palmar-plantar erythrodysesthesia syndrome. aAdverse events leading to 2 discontinuations are listed in the table.
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

51
0 30 5 10 15 20 25
0
10
20
30
40
50
60
70
80
90
100
PFS: ITT Population
n Median PFS 95% CI P value
Neratinib 117 4.5 mo 3.1–5.7 mo 0.231
L + C 116 6.8 mo 5.9–8.2 mo
L, lapatinib; C, capecitabine; PFS, progression-free survival; CI, confidence interval.
Time since randomization (mo)
Pro
bab
ilit
y o
f P
FS
(%
) Neratinib
L + C
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

52
Analysis of Non-inferiority
ITT population PP populationa
Non-inferiority margin
1 1.15
HR (Ner/L + C)
1.19 0.89 1.60
Neratinib better
1
Non-inferiority margin
1.15
1.14
L + C better
0.84 1.55
HR (Ner/L + C)
● Non-inferiority of treatment with neratinib versus L + C
could not be demonstrated
Neratinib better
L + C better
ITT, intent-to-treat; PP, per protocol; HR, hazard ratio; L, lapatinib; C, capecitabine. aPP protocol population included patients who were randomized and received at least 1 week of study treatment, incurred no major
protocol violations, and had tumor assessments at screening and at least 1 valid post-baseline tumor assessment.
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

53
Best Overall Response: ITT Population
Modification, %
Neratinib
(n = 117)
L + C
(n = 116)
Complete response 2 4
Partial response 27 36
Stable disease ≥24 weeks 15 23
Stable disease <24 weeks 29 24
Progressive disease 17 7
Unknown/missing 9 5
L, lapatinib; C, capecitabine.
● The ORR was 29% in the neratinib arm compared with
40% in the L + C arm
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

54
Conclusions
● Neratinib did not demonstrate non-inferiority versus L + C in terms of PFS
● In addition, the antitumor activity of neratinib
monotherapy in heavily pretreated patients with
advanced or metastatic HER2+ BC was robust (ORR
of 29%)
● Diarrhea was the most frequently reported adverse
event, but was typically transient and manageable
● These findings support the continued development
of neratinib as monotherapy and in combination with
other agents for treatment of recurrent HER2+ BC
1. Burstein HJ, et al. J Clin Oncol. 2010;28(8):1301-1307.
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.




San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center
at UT Health Science Center – December 6-10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
Results of the TEACH Trial Lapatinib in Women With Early-Stage HER2-Overexpressing Breast Cancer
A Double-blind, Placebo-controlled, Phase III Trial
Paul Goss1, Ian Smith2, Joyce O’Shaughnessy3, Bent Ejlertsen4, Manfred Kaufmann5, Frances Boyle6, Aman Buzdar7, Pierre Fumoleau8, William Gradishar9, Miguel Martin10, Beverly Moy1, Martine Piccart-Gebhart11, Kathleen I. Pritchard12, Deborah Lindquist13,
Gursel Aktan14, Erica Rappold14, Lisa Williams14, Dianne Finkelstein1
1Massachusetts Gen Hosp, Boston MA; 2Royal Marsden Hosp, London, UK; 3Baylor Sammons Cancer Ctr and US Oncology, Dallas TX; 4Rigshospitalet, Copenhagen, Denmark; 5JW Goethe-Universität, Frankfurt, Germany; 6Mater Hosp, Sydney, Australia; 7UT MD Anderson Cancer Ctr, Houston TX; 8Centre GF Leclerc, Dijon, France; 9Northwestern Univ, Chicago IL; 10Hospital Universitario Gregorio Maranon, Madrid, Spain; 11Jules Bordet Inst, Brussels, Belgium; 12Sunnybrook Odette Cancer Ctr, Toronto, Ontario; 13Arizona Oncology and US Oncology, Sedona, AZ; 14GlaxoSmithKline, Collegeville PA and Uxbridge, UK.

San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center
at UT Health Science Center – December 6-10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
TEACH Trial
Placebo
qd × 1 yr
Lapatinib
1500 mg qd × 1 yr
Stratification
• Time from diagnosis ≤4 vs >4 yrs
• Lymph node +ve vs -ve
• ER+ and/or PgR+ vs ER–/PgR–
4 yr
Eligibility
• HER2+ Local IHC3+ or FISH +ve
•Resected Stage I-IIIc primary BRCA
•No prior trastuzumab
•Neo-/adjuvant chemotherapy (CMF,
anthracycline, or taxane)
•Appropriate endocrine therapy
1 yr
<1 yr only if unable or did
not receive trastuzumab N=3147
Aug 2006-May 2008
33 countries
R
A
N
D
O
M
I
Z
E
59
Diagnosis

San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center
at UT Health Science Center – December 6-10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
TEACH Trial Objectives Primary
• Disease-free survival (DFS): • local, regional, distant recurrence, contralateral BRCA
• other 2nd primary cancers
• death from any cause
Secondary • Recurrence-free survival
• Distant recurrence-free survival
• Overall survival (OS)
• Rate of CNS recurrences and recurrence-free survival
• DFS in key-defined subgroups, including all strata
• Health-related quality of life
• Compliance and treatment exposure
• Safety, including cardiac and liver abnormalities 60

San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center
at UT Health Science Center – December 6-10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
TEACH: ITT and Confirmed FISH+ Patient Population
61
0
25
50
75
100
N. America/Canada(n=473)
Latin America(n=344)
Europe(n=1235)
Asia Pacific
(n=863)
Central FISH+ 79% Confirmed
Confirmed FISH+
Ce
ntr
all
y C
on
firm
ed
FIS
H P
ati
en
t
Po
pu
lati
on
by
Re
gio
n (
%)

San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center
at UT Health Science Center – December 6-10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
0.0
TEACH Primary Endpoint: K-M Plot of DFS in ITT Population—Time From Randomization
62 ap value based on 2-sided stratified log-rank test
Lapatinib
Placebo HR 0.83 (0.70-1.00); p=0.053a
Median Follow up: 4 years
Number of patients at risk
Lapatinib 1500 mg 1571 1431 1349 1293 1233 1168 1001 661 299
Placebo 1576 1487 1412 1343 1295 1247 1048 706 327

San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center
at UT Health Science Center – December 6-10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
TEACH: K-M Plot of DFS in Confirmed FISH+ Population—Time From Randomization
0.0
63
Lapatinib
Placebo
HR 0.82 (0.67-1.00); p=0.04a
ap value based on 2-sided stratified log-rank test.
Number of patients at risk
Lapatinib 1500 mg 1230 1137 1069 1026 980 934 810 533 245
Placebo 1260 1186 1125 1075 1035 993 840 578 275

San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center
at UT Health Science Center – December 6-10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
TEACH Common AEs: Maximum NCI CTC Toxicity Grades
64 NCI=National Cancer Institute; CTC=Common Toxicity Criteria.

San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center
at UT Health Science Center – December 6-10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
TEACH Conclusions
• Although DFS did not reach statistical significance in the overall patient population enrolled over a broad time frame, in centrally confirmed FISH+ tumors, DFS improvement reached statistical significance
• In the overall patient population, DFS improvement was significant in key prespecified subgroups – ER/PgR-ve patients
– Patients ≤ 1 year from diagnosis
• Predominantly low grade diarrhea and skin rash affect compliance, but no new or unexpected serious safety concerns were found
65

T-DM1: A novel antibody−drug conjugate
T-DM1
Monoclonal antibody: trastuzumab
Target expression: HER2
Highly potent chemotherapy (DM1, a tubulin destabiliser)
Cytotoxic drug: DM1
Systemically stable
Linker

Please refer to disclaimer on slide 2
TDM4450g Phase II Study: T-DM1 vs Trastuzumab
+ Docetaxel in HER2-Positive MBC
Multicenter, randomized study
Primary end points
– PFS by INV
– Safety
Secondary end points
– Overall survival (OS), ORR, CBR, duration of response, duration of survival, pharmacokinetics, time-to-treatment failure (TTF)
• HER2-positive,
recurrent, LABC
or MBC (N=137)
• No prior therapy for
advanced breast cancer
or MBC
Trastuzumab (8-mg/kg loading dose,
then 6 mg/kg) + docetaxel
(75 or 100 mg/m2) q3w
T-DM1 3.6 mg/kg q3w until
PD/unnacceptable toxicity
or study termination
Cross-
over
to T-DM1 PD
1:1
PD, progressive disease.
Perez et al. UPDATE FROM ESMO 2010. Abstract/oral presentation LBA3.

68
Selected Patient Demographic and Baseline
Characteristics
Trastuzumab + docetaxel
(n=70)
T-DM1
(n=67)
Median age, y (range) 52.0 (33–75) 55.0 (27–82)
World region, %
US
Non-US 28.6
71.4
31.3
68.7
ECOG PS 0, %
ECOG PS 1, % 63.8a
36.2a
65.7
34.3
HER2-positive status by central lab, %b
85.2 85.2
ER+ and/or PR+, %
ER– and PR–, %
ER and PR unknown, %
54.3
41.1
4.3
49.3
47.8
3.0
Lung or liver involvement, %
Yes
No
Unknown
67.1
31.4
1.4
71.6
26.9
1.5
Disease-free interval, %
<24 months
>24 months 64.3
35.7
59.7
40.3
aECOG PS data were available for 69 patients in the trastuzumab + docetaxel arm. bCentral testing for HER2 status was performed for 61 patients in the trastuzumab + docetaxel arm and 61 patients in the
T-DM1 arm.
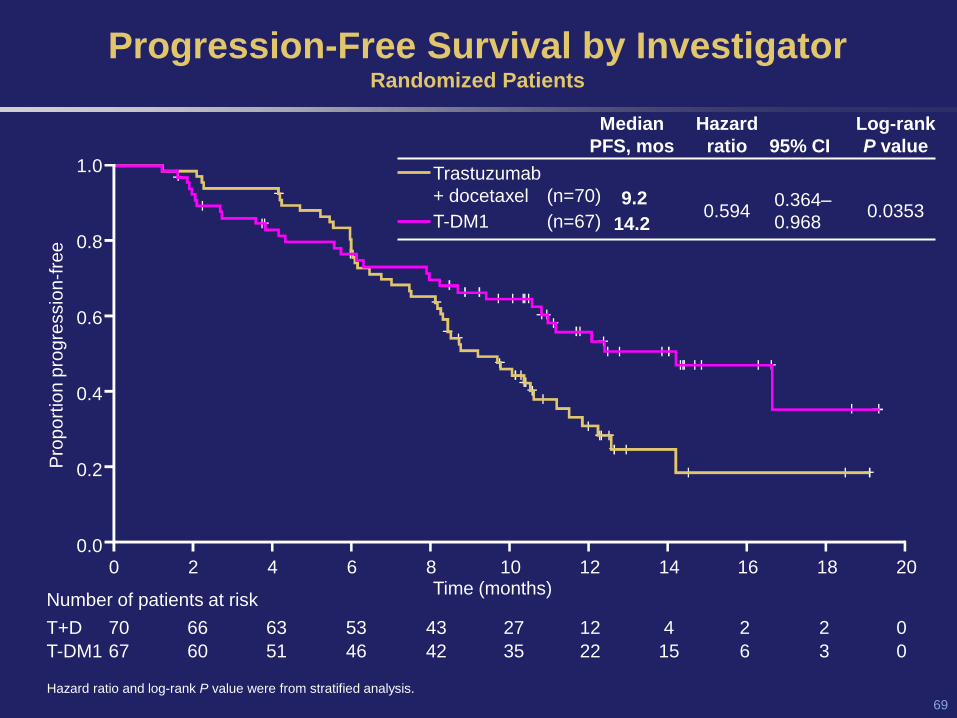
69
Time (months)
Progression-Free Survival by Investigator Randomized Patients
Pro
po
rtio
n p
rog
ressio
n-f
ree
1.0
0.8
0.6
0.4
0.2
0.0 0 2 4 6 8 10 12 14 16 18 20
Number of patients at risk
T+D 70 66 63 53 43 27 12 4 2 2 0
T-DM1 67 60 51 46 42 35 22 15 6 3 0
Hazard ratio and log-rank P value were from stratified analysis.
Trastuzumab
+ docetaxel (n=70)
T-DM1 (n=67)
Median
PFS, mos
Hazard
ratio
95% CI
Log-rank
P value
9.2
14.2
0.594
0.364–
0.968
0.0353

70
Cardiac Safety
• Cardiac function was assessed locally and centrally based on cardiac ECHO/MUGA
• Prior anthracycline in the adjuvant setting was 44.8% and 48.6% in the T-DM1 and trastuzumab + docetaxel arms, respectively
• Asymptomatic LV dysfunction
• There were no clinically significant cardiac events reported
LVEF assessment Trastuzumab +
docetaxel T-DM1
Local assessment
Patients assessed 65 67
Patients with post-baseline LVEF ≤40% 2a 0
Central assessment
Patients assessed 60 65
Patients with post-baseline LVEF ≤40% 1b 0
aBoth patients had prior anthracycline therapy in the adjuvant setting; 1 patient received prior trastuzumab therapy in the
adjuvant setting. bThis patient did not receive prior treatment with an anthracycline.

71
Summary and Conclusions
•This is the first randomized study to evaluate an antibody-drug
conjugate for HER2-positive MBC
•First-line treatment of HER2-positive MBC with T-DM1,
compared with trastuzumab + docetaxel was associated with:
–A significant improvement in PFS (14.2 vs 9.2 mos; HR=0.594; P
value=0.0353)
–A lower rate of grade ≥3 AEs (46.4% vs 89.4%)
•T-DM1 is being evaluated in phase III randomized clinical trials
for HER2-positive MBC

CONCLUSIONES
-Pertuzumab en asociación con trastuzumab incrementa
significativamente la actividad de éste sin apenas añadir
toxicidad
-TDM-1 posee una gran actividad antitumoral en tumores
HER2+
-El papel del lapatinib como adyuvancia tardía está
pendiente de definir
-El neratinib parece poseer una interesante actividad en
cáncer de mama HER2+
-El bloqueo dual del receptor de HER2 se traduce de
nuevo en un beneficio clínico


















