NOTE: Should you have landed here as a result of a search ...File... · • Useof a bed for...
96
NOTE: Should you have landed here as a result of a search engine (or other) link, be advised that these files contain material that is copyrighted by the American Medical Association. You are forbidden to download the files unless you read, agree to, and abide by the provisions of the copyright statement. Read the copyright statement now and you will be linked back to here.
Transcript of NOTE: Should you have landed here as a result of a search ...File... · • Useof a bed for...
NOTE Should you have landed here as a result of a search engine (or other) link be advised that these files contain material that is copyrighted by the American Medical Association You are forbidden to download the files unless you read agree to and abide by the provisions of the copyright statement Read the copyright statement now and you will be linked back to here
Level of Care
Palmetto GBA
Inpatient or
Outpatient Observation
Provider Outreach and Education
Objective bull Provide billing and documentation guidance for Medicare Part A providers
bull Increase knowledge of Observation requirements
bull Improve understanding of the impact of medically reviewed claims
bull Assist in remaining compliant with Medicare Program
Agenda bull Observation = Outpatient Status
bull Inpatient Status
bull Observation versus Inpatient Status
bull Scenarios
bull National Paid Claims Error Rate
The information provided in this handout is current as of 11062012 Any changes or new information superseding this information will be provided in
articles and publication dates after 11062012 posted at wwwPalmettoGBAcom
OutpatientObservation
Observation Services Defined
bull Use of a bed for physician periodic monitoring and active monitoring by hospitals nursing or other ancillary staff bull For patient care which are reasonable and necessary to evaluate an outpatients condition or determine need for an inpatient admission
Observation Services bull Must be patient specific
bull Intended for short term
bull Generally does not exceed 24 hours
bull Greater than 48 hours would be seen rare and exceptional cases
bull Outpatient services
Observation Services
bull Observation only medically necessary when bull Patientrsquos current condition requires outpatient hospital services
OR
bull Therersquos a significant risk of deterioration in the immediate future
Observation Services
bull Medical Necessity and Proper Setting bull Considerations to determine appropriate setting for care based on patient needs bull Can treatment be provided on an outpatient basis or home health basis or at home
bull Are these alternatives more economical and effective than inpatient care
bull Does the patientrsquos physical condition and familysocial support system allow them access to care option
Observation Services bull Physicianrsquos order required and order must be part of medical record bull Order should clearly define what service is being requested
bull Clearly differentiate observation from an order for an inpatient admission bull Admit as inpatient or place in observation
bull Condition requires outpatient hospital services bull Observation services for convenience of patient or others are not medically necessary
Verbal Orders
bull Code of Federal Regulations (CFR) 48223 (c) (2) (i) Verbal Orders bull To be used infrequently
bull Used only to meet the care needs of patient when it is impossible or impractical for ordering physician to write an order
bull Not to be used for convenience of the ordering physician
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Level of Care
Palmetto GBA
Inpatient or
Outpatient Observation
Provider Outreach and Education
Objective bull Provide billing and documentation guidance for Medicare Part A providers
bull Increase knowledge of Observation requirements
bull Improve understanding of the impact of medically reviewed claims
bull Assist in remaining compliant with Medicare Program
Agenda bull Observation = Outpatient Status
bull Inpatient Status
bull Observation versus Inpatient Status
bull Scenarios
bull National Paid Claims Error Rate
The information provided in this handout is current as of 11062012 Any changes or new information superseding this information will be provided in
articles and publication dates after 11062012 posted at wwwPalmettoGBAcom
OutpatientObservation
Observation Services Defined
bull Use of a bed for physician periodic monitoring and active monitoring by hospitals nursing or other ancillary staff bull For patient care which are reasonable and necessary to evaluate an outpatients condition or determine need for an inpatient admission
Observation Services bull Must be patient specific
bull Intended for short term
bull Generally does not exceed 24 hours
bull Greater than 48 hours would be seen rare and exceptional cases
bull Outpatient services
Observation Services
bull Observation only medically necessary when bull Patientrsquos current condition requires outpatient hospital services
OR
bull Therersquos a significant risk of deterioration in the immediate future
Observation Services
bull Medical Necessity and Proper Setting bull Considerations to determine appropriate setting for care based on patient needs bull Can treatment be provided on an outpatient basis or home health basis or at home
bull Are these alternatives more economical and effective than inpatient care
bull Does the patientrsquos physical condition and familysocial support system allow them access to care option
Observation Services bull Physicianrsquos order required and order must be part of medical record bull Order should clearly define what service is being requested
bull Clearly differentiate observation from an order for an inpatient admission bull Admit as inpatient or place in observation
bull Condition requires outpatient hospital services bull Observation services for convenience of patient or others are not medically necessary
Verbal Orders
bull Code of Federal Regulations (CFR) 48223 (c) (2) (i) Verbal Orders bull To be used infrequently
bull Used only to meet the care needs of patient when it is impossible or impractical for ordering physician to write an order
bull Not to be used for convenience of the ordering physician
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Objective bull Provide billing and documentation guidance for Medicare Part A providers
bull Increase knowledge of Observation requirements
bull Improve understanding of the impact of medically reviewed claims
bull Assist in remaining compliant with Medicare Program
Agenda bull Observation = Outpatient Status
bull Inpatient Status
bull Observation versus Inpatient Status
bull Scenarios
bull National Paid Claims Error Rate
The information provided in this handout is current as of 11062012 Any changes or new information superseding this information will be provided in
articles and publication dates after 11062012 posted at wwwPalmettoGBAcom
OutpatientObservation
Observation Services Defined
bull Use of a bed for physician periodic monitoring and active monitoring by hospitals nursing or other ancillary staff bull For patient care which are reasonable and necessary to evaluate an outpatients condition or determine need for an inpatient admission
Observation Services bull Must be patient specific
bull Intended for short term
bull Generally does not exceed 24 hours
bull Greater than 48 hours would be seen rare and exceptional cases
bull Outpatient services
Observation Services
bull Observation only medically necessary when bull Patientrsquos current condition requires outpatient hospital services
OR
bull Therersquos a significant risk of deterioration in the immediate future
Observation Services
bull Medical Necessity and Proper Setting bull Considerations to determine appropriate setting for care based on patient needs bull Can treatment be provided on an outpatient basis or home health basis or at home
bull Are these alternatives more economical and effective than inpatient care
bull Does the patientrsquos physical condition and familysocial support system allow them access to care option
Observation Services bull Physicianrsquos order required and order must be part of medical record bull Order should clearly define what service is being requested
bull Clearly differentiate observation from an order for an inpatient admission bull Admit as inpatient or place in observation
bull Condition requires outpatient hospital services bull Observation services for convenience of patient or others are not medically necessary
Verbal Orders
bull Code of Federal Regulations (CFR) 48223 (c) (2) (i) Verbal Orders bull To be used infrequently
bull Used only to meet the care needs of patient when it is impossible or impractical for ordering physician to write an order
bull Not to be used for convenience of the ordering physician
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Agenda bull Observation = Outpatient Status
bull Inpatient Status
bull Observation versus Inpatient Status
bull Scenarios
bull National Paid Claims Error Rate
The information provided in this handout is current as of 11062012 Any changes or new information superseding this information will be provided in
articles and publication dates after 11062012 posted at wwwPalmettoGBAcom
OutpatientObservation
Observation Services Defined
bull Use of a bed for physician periodic monitoring and active monitoring by hospitals nursing or other ancillary staff bull For patient care which are reasonable and necessary to evaluate an outpatients condition or determine need for an inpatient admission
Observation Services bull Must be patient specific
bull Intended for short term
bull Generally does not exceed 24 hours
bull Greater than 48 hours would be seen rare and exceptional cases
bull Outpatient services
Observation Services
bull Observation only medically necessary when bull Patientrsquos current condition requires outpatient hospital services
OR
bull Therersquos a significant risk of deterioration in the immediate future
Observation Services
bull Medical Necessity and Proper Setting bull Considerations to determine appropriate setting for care based on patient needs bull Can treatment be provided on an outpatient basis or home health basis or at home
bull Are these alternatives more economical and effective than inpatient care
bull Does the patientrsquos physical condition and familysocial support system allow them access to care option
Observation Services bull Physicianrsquos order required and order must be part of medical record bull Order should clearly define what service is being requested
bull Clearly differentiate observation from an order for an inpatient admission bull Admit as inpatient or place in observation
bull Condition requires outpatient hospital services bull Observation services for convenience of patient or others are not medically necessary
Verbal Orders
bull Code of Federal Regulations (CFR) 48223 (c) (2) (i) Verbal Orders bull To be used infrequently
bull Used only to meet the care needs of patient when it is impossible or impractical for ordering physician to write an order
bull Not to be used for convenience of the ordering physician
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
OutpatientObservation
Observation Services Defined
bull Use of a bed for physician periodic monitoring and active monitoring by hospitals nursing or other ancillary staff bull For patient care which are reasonable and necessary to evaluate an outpatients condition or determine need for an inpatient admission
Observation Services bull Must be patient specific
bull Intended for short term
bull Generally does not exceed 24 hours
bull Greater than 48 hours would be seen rare and exceptional cases
bull Outpatient services
Observation Services
bull Observation only medically necessary when bull Patientrsquos current condition requires outpatient hospital services
OR
bull Therersquos a significant risk of deterioration in the immediate future
Observation Services
bull Medical Necessity and Proper Setting bull Considerations to determine appropriate setting for care based on patient needs bull Can treatment be provided on an outpatient basis or home health basis or at home
bull Are these alternatives more economical and effective than inpatient care
bull Does the patientrsquos physical condition and familysocial support system allow them access to care option
Observation Services bull Physicianrsquos order required and order must be part of medical record bull Order should clearly define what service is being requested
bull Clearly differentiate observation from an order for an inpatient admission bull Admit as inpatient or place in observation
bull Condition requires outpatient hospital services bull Observation services for convenience of patient or others are not medically necessary
Verbal Orders
bull Code of Federal Regulations (CFR) 48223 (c) (2) (i) Verbal Orders bull To be used infrequently
bull Used only to meet the care needs of patient when it is impossible or impractical for ordering physician to write an order
bull Not to be used for convenience of the ordering physician
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Observation Services Defined
bull Use of a bed for physician periodic monitoring and active monitoring by hospitals nursing or other ancillary staff bull For patient care which are reasonable and necessary to evaluate an outpatients condition or determine need for an inpatient admission
Observation Services bull Must be patient specific
bull Intended for short term
bull Generally does not exceed 24 hours
bull Greater than 48 hours would be seen rare and exceptional cases
bull Outpatient services
Observation Services
bull Observation only medically necessary when bull Patientrsquos current condition requires outpatient hospital services
OR
bull Therersquos a significant risk of deterioration in the immediate future
Observation Services
bull Medical Necessity and Proper Setting bull Considerations to determine appropriate setting for care based on patient needs bull Can treatment be provided on an outpatient basis or home health basis or at home
bull Are these alternatives more economical and effective than inpatient care
bull Does the patientrsquos physical condition and familysocial support system allow them access to care option
Observation Services bull Physicianrsquos order required and order must be part of medical record bull Order should clearly define what service is being requested
bull Clearly differentiate observation from an order for an inpatient admission bull Admit as inpatient or place in observation
bull Condition requires outpatient hospital services bull Observation services for convenience of patient or others are not medically necessary
Verbal Orders
bull Code of Federal Regulations (CFR) 48223 (c) (2) (i) Verbal Orders bull To be used infrequently
bull Used only to meet the care needs of patient when it is impossible or impractical for ordering physician to write an order
bull Not to be used for convenience of the ordering physician
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Observation Services bull Must be patient specific
bull Intended for short term
bull Generally does not exceed 24 hours
bull Greater than 48 hours would be seen rare and exceptional cases
bull Outpatient services
Observation Services
bull Observation only medically necessary when bull Patientrsquos current condition requires outpatient hospital services
OR
bull Therersquos a significant risk of deterioration in the immediate future
Observation Services
bull Medical Necessity and Proper Setting bull Considerations to determine appropriate setting for care based on patient needs bull Can treatment be provided on an outpatient basis or home health basis or at home
bull Are these alternatives more economical and effective than inpatient care
bull Does the patientrsquos physical condition and familysocial support system allow them access to care option
Observation Services bull Physicianrsquos order required and order must be part of medical record bull Order should clearly define what service is being requested
bull Clearly differentiate observation from an order for an inpatient admission bull Admit as inpatient or place in observation
bull Condition requires outpatient hospital services bull Observation services for convenience of patient or others are not medically necessary
Verbal Orders
bull Code of Federal Regulations (CFR) 48223 (c) (2) (i) Verbal Orders bull To be used infrequently
bull Used only to meet the care needs of patient when it is impossible or impractical for ordering physician to write an order
bull Not to be used for convenience of the ordering physician
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Observation Services
bull Observation only medically necessary when bull Patientrsquos current condition requires outpatient hospital services
OR
bull Therersquos a significant risk of deterioration in the immediate future
Observation Services
bull Medical Necessity and Proper Setting bull Considerations to determine appropriate setting for care based on patient needs bull Can treatment be provided on an outpatient basis or home health basis or at home
bull Are these alternatives more economical and effective than inpatient care
bull Does the patientrsquos physical condition and familysocial support system allow them access to care option
Observation Services bull Physicianrsquos order required and order must be part of medical record bull Order should clearly define what service is being requested
bull Clearly differentiate observation from an order for an inpatient admission bull Admit as inpatient or place in observation
bull Condition requires outpatient hospital services bull Observation services for convenience of patient or others are not medically necessary
Verbal Orders
bull Code of Federal Regulations (CFR) 48223 (c) (2) (i) Verbal Orders bull To be used infrequently
bull Used only to meet the care needs of patient when it is impossible or impractical for ordering physician to write an order
bull Not to be used for convenience of the ordering physician
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Observation Services
bull Medical Necessity and Proper Setting bull Considerations to determine appropriate setting for care based on patient needs bull Can treatment be provided on an outpatient basis or home health basis or at home
bull Are these alternatives more economical and effective than inpatient care
bull Does the patientrsquos physical condition and familysocial support system allow them access to care option
Observation Services bull Physicianrsquos order required and order must be part of medical record bull Order should clearly define what service is being requested
bull Clearly differentiate observation from an order for an inpatient admission bull Admit as inpatient or place in observation
bull Condition requires outpatient hospital services bull Observation services for convenience of patient or others are not medically necessary
Verbal Orders
bull Code of Federal Regulations (CFR) 48223 (c) (2) (i) Verbal Orders bull To be used infrequently
bull Used only to meet the care needs of patient when it is impossible or impractical for ordering physician to write an order
bull Not to be used for convenience of the ordering physician
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Observation Services bull Physicianrsquos order required and order must be part of medical record bull Order should clearly define what service is being requested
bull Clearly differentiate observation from an order for an inpatient admission bull Admit as inpatient or place in observation
bull Condition requires outpatient hospital services bull Observation services for convenience of patient or others are not medically necessary
Verbal Orders
bull Code of Federal Regulations (CFR) 48223 (c) (2) (i) Verbal Orders bull To be used infrequently
bull Used only to meet the care needs of patient when it is impossible or impractical for ordering physician to write an order
bull Not to be used for convenience of the ordering physician
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Verbal Orders
bull Code of Federal Regulations (CFR) 48223 (c) (2) (i) Verbal Orders bull To be used infrequently
bull Used only to meet the care needs of patient when it is impossible or impractical for ordering physician to write an order
bull Not to be used for convenience of the ordering physician
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Verbal Orders ndash Policy amp Procedures bull Hospitals are expected to develop appropriate policies and procedures bull Describe limitations or prohibitions on use
bull Provide a mechanism to ensure validityauthenticity of physician issuing a verbal order
bull List elements required for inclusion in the process
bull Describe situations that verbal orders may be used
bull Define types of personnel who may issue and receive verbal orders
bull Establish protocols for clear and effective communication and authentication of verbal orders
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Verbal Orders ndash Communication amp Documentation bull Clearly communicate
bull Immediately document medical record which is to be signed by individual receiving order
bull Verbal orders should be recorded directly onto order sheet or into electronic health record
bull A read‐back verification practice to be implemented for every verbal order
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Communication
bull An outpatient patient status for observation services will have an impact on beneficiaryrsquos benefits if transfer to another setting bull Such as a Skilled Nursing Facility (SNF)
bull Explain to beneficiary outpatient services were rendered and would not meet the technical requirement for a SNF inpatient admission
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Observation Services BillingRequirements bull Type of Bill 13X
bull Appropriateapplicable coding bull Ancillary revenue codes
bull Healthcare Common Procedural Code System (HCPCS)
bull Current Procedure Terminology (CPT) codes
bull Diagnosis codes
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Hospital Observation BillingRequirements bull When outpatient observation services span more than 1 calendar day bull All of the hours for entire period of observation must be included on a single line
bull Only one date of service is reported bull Report the date Observation care began
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Hospital Observation BillingRequirements
Revenue Code Description
0762 Observation
Only revenue code 0762 should be reported when billing observation services
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Hospital Observation Codes
bull G0378 ndashHospital Observation Services Per Hour
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Hospital Observation CodeG0379
bull G0379 ndashDirect (Referral) Admission of Patient for Hospital Observation Services bull Only report when applicable
bull When patient is referred directly to observation care after being seen by a physician in community bull Without an associated ER visit hospital outpatient clinic visit or critical care service on day of initiation of observation
bull Clock time begins when patient placed in observation bull This must be documented in the medical record
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Hospital Observation TimeRequirements bull Observation time must be documented in medical record
bull Begins at clock time documented coincides with time observation services are initiated in accordance to physicianrsquos order
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Hospital Observation TimeRequirements bull Nursersquos patient assessment prior to physician order is not counted towards observation time
bull Hospitals should round to nearest hour
bull Units of service billed must equal number of hours patient is in observation status
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Hospital Observation TimeRequirements continued bull Observation time ends when all clinical or medical interventions have been completed including follow up care furnished by hospital staff and
bull After a physician has ordered patient to be discharged or admitted as an inpatient bull Number of units reported with G0378 must equal or exceed 8 hours to receive separate payment
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Hospital Observation TimeRequirements continued
bull Observation less than 8 hours must be documented in medical record and are packaged into Ambulatory Payment Classification (APC) for Outpatient Prospective Payment System (OPPS) providers
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Timing for DiagnosticServices
bull Observation services should not be billed concurrently with diagnostic or therapeutic services for which active monitoring is a part of the procedure or service
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Rounding Observation TimeExample 1
bull No active monitoring carve out bull Order to place in Observation documented 1020 am
bull Order to discharge home at 945 pm
bull 11 hours 25 minutes in Observation
bull Total units to bill 11
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Rounding Observation TimeExample 2
bull Active monitoring carved out bull Order to place in Observation documented at 1220 am
bull Order to admit as inpatient at 1145 am bull 11 hrs 25 min in Observation
bull 1 hr 40 min at diagnostic test bull Time carved out of Observation units
bull 9 hrs 45 min total time spent in Observation
bull Total units to bill 10
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Observation Services BillingRequirements bull One of these services must be reported with same date of service or day before date reported for observation bull Type A or B emergency department visit CPT codes 99284 or 99285 or HCPCS code G0384 or
bull A clinic visit (CPT code 99205 or 99215) or
bull Critical care (CPT code 99291) or
bull Direct referral for observation care reported with G0379 must be reported on same date of service as the date reported for observation services
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient Status
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient Services Defined
bull An inpatient is a person who has been admitted to a hospital for bed occupancy for the purposes of receiving inpatient hospital services
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient Admission bull Term ldquoadmitrdquo
bull Observation or Inpatient
bull Inpatient admission are based on
bull Severity of illness bull Intensity of services
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Payment Window
bull Payment window includes all outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to the inpatient stay bull On date of inpatient admission or bull Three days immediately preceding the date of admission
bull Unless ldquothe hospital demonstrates that such services are not related to such admissionrdquo
bull Statute does not change billing of diagnostic services
Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom

Payment Window
bull Hospitals are able to bill correctly for admission‐related outpatient non‐diagnostic services without modifying dates on the inpatient claim bull Bundle services on inpatient hospital claim
bull ICD‐9‐CM procedure code dates for non‐diagnostic services will be allowed
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Payment Window CodingRequirement
bull Change Request (CR) 7142 Clarification of Payment Window for Outpatient Services Treated as Inpatient Services bull Effective June 25 2010 bull Implementation date April 4 2011
bull Outpatient Services unrelated to inpatient admission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient versusOutpatient
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient Changed toOutpatient Policy bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospital must ensure all UR requirements are fulfilled
bull UR committee consists of two or more physicians carries out UR function
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient Changed toOutpatient Policy
bull Determination that an admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of the patient either concurs with the determination or fails to present their view when afforded opportunity or
bull Two members of the UR committee in all other cases
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient Changed toOutpatient Policy
bull UR committee must consult with physician responsible for patientrsquos care and allow them to present their views before making the determination
bull If UR committee determines admission is not medically necessary bull Committee must give written notification no later than 2 days after determination to the hospital patient and practitioner responsible for the care of the patient
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Disagreement of the Changein Status
bull Attending physicians does not concur with UR decision bull If two physician members of UR determine patientrsquos stay is not medically necessary their decision becomes final
bull In no case may a non‐physician make a final determination that a patientrsquos stay is not medically necessary or appropriate
bull httpwwwcmsgovmanualsDownloadssom107ap _a_hospitalspdf
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient Changed toOutpatient Policy bull It is the hospital UR committee that changes the beneficiaryrsquos status from inpatient to outpatient bull Physician concurrence is required
bull Two physician members of UR committee in all other instances
bull Hospital may not change a patient status from inpatient to outpatient without UR committee involvement
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Use of Condition Code 44 Policy
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with Utilization Review (UR) committeersquos decision and
bull Physicianrsquos concurrence is documented in the patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient is still in treatment
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Utilization Review
bull Reporting Condition Code (CC) 44 should become rare
bull CC 44 is not a substitute for adequate staffing or continued education of hospital existing policies and admission protocols bull Review of medical necessity admissions and continued stays
bull Review of admissions may be performed before at or after hospital admission
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Frequently Asked Question
bull How should the hospital report Observation services when the patients status is changed from inpatient to outpatient using Condition Code 44
bull May the hospital report Observation services from the beginning of the hospital outpatient encounter
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Frequently Asked Question ‐Answer bull CMS Answer Identification 9973
bull httpsquestionscmshhsgovappanswersdetaila _id9973kwObservation
bull When Condition Code 44 is appropriately used bull Hospital reports on outpatient bill services that were orderedprovided to patient for entire patient encounter
bull Reporting of individual HCPCS codes on an outpatient claim must be consistent with all applicable instructions and CMS guidance
bull Observation cannot be ordered retroactively
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Medical Record bull Entries in the medical record cannot be expunged or deleted and must be retained in their original form
bull All orders and entries related to the inpatient admission must be retained in the record in their original form
bull If a patientrsquos status changes in accordance with requirements for use of Condition Code 44 ‐ change must be fully documented in medical record
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Medical Records bull Must be complete with orders
bull Who What When
bull Note when the change was made
bull Note the care that was furnished
bull Include the participants in making the decision to change the patientrsquos status
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Condition Code 44 Billing bull Entire episode of care should be treated as if inpatient admission never occurred
bull Medically necessary Part B services should be billed as an outpatient episode of care bull Type of Bill (TOB) 13x or 85x bull Condition Code 44 bull Report all other applicable data elements
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Condition Code 44 Billing bull Billing for services prior to observation order in Condition Code 44 situations bull Hospital encounter prior to physicianrsquos order for Observation
bull May not report HCPCS code G0378 bull Include charges on outpatient claim for cost of all hospital resources utilized in patientrsquos care during entire encounter
bull Revenue code 0762 without coding on outpatient claim
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Condition Code 44 Billing Example
bull Patient is admitted as inpatient and receives 12 hours of care bull Hospital Utilization Review (UR) changes status from inpatient to outpatient
bull Physician orders Observation services for additional 24 hours before patient is sent home
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
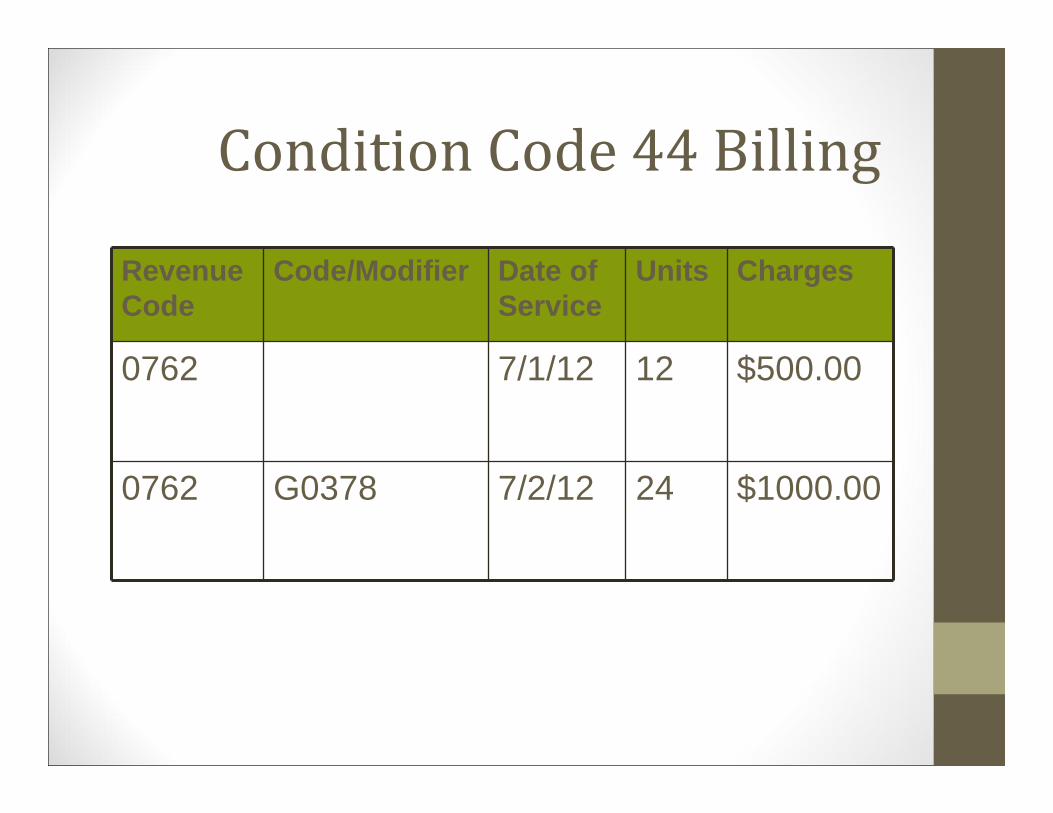
Condition Code 44 Billing
Revenue Code
CodeModifier Date of Service
Units Charges
0762 7112 12 $50000
0762 G0378 7212 24 $100000
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Physician Changes PatientStatus
bull Can a hospital change a patients status using Condition Code 44 when a physician changes patients status without Utilization Review (UR) committee involvement bull No the determination to change a patientrsquos status must be made by the UR committee with physician concurrence
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Condition Code Policy 44 NotMet bull Decision to change patient status from Inpatient admission to Outpatient status was after patient discharged
bull No beneficiary liability due to patient was not notified of financial liabilities prior to discharge
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Condition Code Policy 44 NotMet Billing
bull Submit a 11X Type of Bill (TOB) bull Or adjust 11X TOB making a 117 TOB
bull Then submit 12x TOB for covered Part B services furnished to the inpatient
bull Part A 11X TOB must process before 12X TOB
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Filing the Inpatient No PayClaim bull Report days as covered on claim page one
bull Report Occurrence Span Code 77
bull Dates must equal from and through date of no payment claim
bull Report charges as non‐covered on claim page 2
bull Add a brief clear and concise explanation for filing a no payment claim
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
References
bull CMS Change Request (CR) 3444
httpwwwcmsgovtransmittalsdownloads R299CPpdf
bull Medicare Learning Network Matters Article SE0622
httpwwwcmsgovMLNMattersArticlesdow nloadsSE0622pdf
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
References CMS IOM 100‐04 Medicare Claims Processing Manual
bull General Billing Instructions Chapter 1 Section 503 httpwwwcmsgovmanualsdownloadsclm104c01pdf
bull Inpatient Hospital Billing Chapter 3 Section 104 and Section 403
httpwwwcmsgovmanualsdownloadsclm104c03pdf
bull Financial Liability Protection Chapter 30 httpwwwcmsgovmanualsdownloadsclm104c30pdf
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
References Palmetto GBA Web Site Articles
bull Ancillary Services Hospital Part A httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~Hospitals~8 CKTNX5473openampnavmenu=7C7C
bull Not Medically Necessary Inpatient Admissions and Provider Liable Billing Requirements
httpwwwpalmettogbacompalmettoprovidersnsfDocsCat Providers~Jurisdiction20120Part20A~Articles~General~7R XNU91083openampnavmenu=7C7C
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Case Studies and Billing Scenarios
Inpatient or Outpatient
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Medicare Coverage Review
bull Two patient statuses at a hospital
bull Outpatient bull Observation is a service not a status
bull Inpatient bull ldquoAdmitrdquo refers to an inpatient admission
bull Communication between staff patients and patient advocates is expected
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Admission Considerations
bull Patientrsquos medical history bull Severity of signs and symptomsbull Current medical needs bull Intensity of services bull Facilities and services
available bull Severity of illness
bull Hospital by‐laws and bull Medical predictability
admission policies bull Need for diagnostic
bull Relative appropriateness studies
bull Availability of diagnostic procedures
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Coverage Considerations
Medicare Covered
bull Hospital services while waiting SNF placement
bull Care as a result of complications of a type ldquoTrdquo procedure bull Same day surgical procedure
Medicare Non‐Covered Services
bull Short stay inpatient admissions
bull Delayed discharge
bull Inconvenience to the patient or family member
Note Admissions are not covered or non-covered solely on length of time patient actually spends in the hospital
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient or Outpatient bull Any care must be medically necessary Social Security Act 1862 (a)(1)(a) bull Physician Order Dates and Signatures
bull Lack of inpatient admission medical necessity does not equate to outpatient observation bull Outpatient observation services must be medically necessary
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Definition References
bull Definition of Inpatient
bull CMS Publication 100‐02 Medicare Benefit Policy Manual Chapter 1 Section 10
bull Definition of Observation
bull CMS Publication 100‐2 Medicare Benefit Policy Manual Chapter 6 Section 206
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Screening ToolsGuidelines bull CMS does not require or endorse any particular brand of screening guidelines bull Payment is not based on ldquopassrdquo or ldquofailrdquo when screening tools are utilized bull ie Milliman InterQual
bull Reviewer must apply clinical review judgment in the determination of the medical necessity of an inpatient stay bull Based on the medical documentation submitted
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Hospital Billing Scenarios
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 1 Emergency Room (ER)
bull Day One ‐ Patient presents to ER and attending physician writes an inpatient admission order
bull Day Two ‐ Utilization Review (UR) determines that inpatient admission is not medically necessary and observation is more appropriate bull Attending physician is presented with UR committeersquos concerns and agrees
bull Attending physician writes an order for observation
How is time prior to Observation order captured on the claim
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Condition Code 44 Guidelines
bull Decision to change patient status is prior to discharge and while still a patient
bull No inpatient claim has been submitted
bull Physician concurs with UR committeersquos decision bull Physicianrsquos concurrence must be documented in patientrsquos medical record bull Physicians must be educated on importance of working with UR Committee while patient still in treatment
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Billing Prior to Order for Observationin CC 44 Situations bull Hospital encounter prior to physicianrsquos order for Observation bull May not report Healthcare Common Procedure Coding System (HCPCS) code G0378
bull Include charges on outpatient claim for cost of all hospital resources utilized in the care of the patient during the entire encounter bull Uncoded line with revenue code 0762 on outpatient claim
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
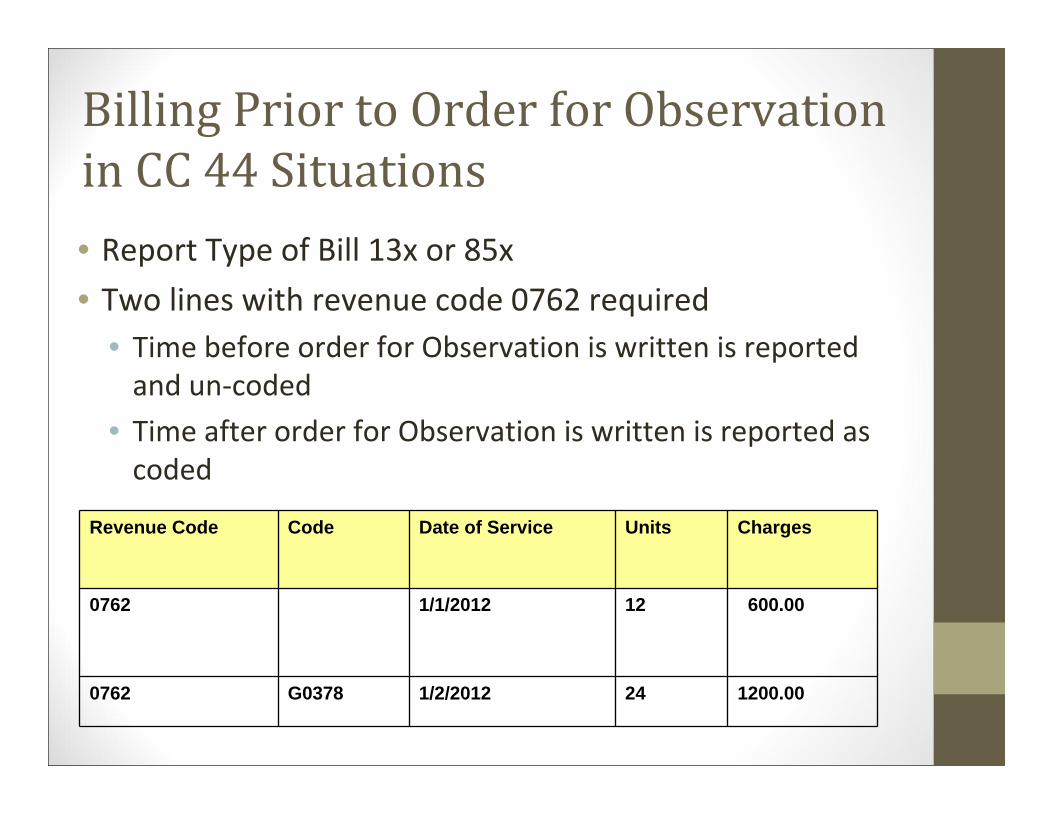
Billing Prior to Order for Observationin CC 44 Situations bull Report Type of Bill 13x or 85x
bull Two lines with revenue code 0762 required bull Time before order for Observation is written is reported and un‐coded
bull Time after order for Observation is written is reported as coded
Revenue Code Code Date of Service Units Charges
0762 112012 12 60000
0762 G0378 122012 24 120000
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 2 Admit ‐ Reverse to Outpatient ‐ Admit bull Day One ‐ patient presents to ER and is admitted as inpatient
bull Day Two ‐ UR reviews case and determines observation is more appropriate bull Attending physician is presented with UR committee concerns and agrees
bull Day Four ‐ patient is readmitted as an inpatient
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
3 or 1 Day Payment WindowOutpatient Services Treated as Inpatient bull All outpatient diagnostic services and non‐diagnostic services ldquorelatedrdquo to inpatient stay bull On the date of inpatient admission or bull 3 days immediately preceding the date of admission bull Statute does not change the billing of diagnosticservices
bull Outpatient Services unrelated to inpatientadmission bull Add Condition Code 51 attest unrelated outpatient non‐diagnostic service
bull Change Request (CR) 7142httpwwwcmsgovtransmittalsdownloadsR796OTNpdf
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Payment Window for OutpatientServices Treated as Inpatient Services
bull Publication 100‐04 Chapter 4 Section 1012 and Chapter 1 Section 5032 bull Updated from CR 7672 January 2012 bull Update of the Hospital OPPS
bull Clarification bull No Part A coverage for the inpatient stay bull Services prior to admission may be separately billed to Part B as outpatient services
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Payment Window and WhollyOwnedOperated Entities
bull CR 7502 Transmittal 2373 bull Services rendered on or after January 1 2012 bull For claims received on or after July 1 2012 bull Patient seen in a wholly owned or operated physician practice is admitted as inpatient within 3 days (1 day for non‐IPPS hospitals)
bull 3 day payment window will apply to diagnostic and non‐diagnostic services clinically related to admission regardless of diagnosis
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 2 Timing
bull July 26 ‐ Admitted inpatient order 830 pm
bull July 27 ‐ Reversed inpatient admission to outpatient 830 am bull Condition code 44 criteria met bull An observation order was written at 1000 am bull Patient remained in observation from July 27 at 1000 am until July 29 at 100 am
bull July 29 ‐ Admitted inpatient order 200 am
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 2 Admit Reverse toOutpatient Admit bull Does the Condition Code 44 Policy apply
bull What is the admission date bull Publication 100‐02 Chapter 3 Section 403 ldquohellipthe day on which the patient is formally admitted as an inpatient is counted as the first inpatient dayrdquo
bull Medicare does not permit retroactive orders or the inference of physician orders
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 3 PhysicianChanged Patient Status bull Patient presents to ER and attending physician decides to admit the patient as an inpatient
bull While patient is still in the ER attending physician changes patientrsquos status to outpatient and writes order for observation
bull Utilization Review (UR) committee is not consulted
Is this a situation when CC 44 can be billed
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 3 Inpatient Changed toOutpatient Policy
bull Hospital Conditions of Participation require hospitals to have a utilization review (UR) plan bull Hospitals must ensure all UR requirements fulfilled
bull UR committee consists of two or more physicians to carry out UR function
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 3 Inpatient Changed toOutpatient Policy
bull Determination that admission or continued stay is not medically necessary must be made by bull One member of UR committee if physician responsible for care of patient either concurs with determination or fails to present their view when afforded opportunity
OR bull Two members of the UR committee in all other cases
bull Condition Code 44 does not apply
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 3 Conclusion
bull Is this a situation when the Condition Code 44 can be billed
bull No ‐ Determination to change a patientrsquos status must be made by UR Committee with physician concurrence
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 3 Considerations
bull Inpatient‐Only services not paid under OPPS
bull Services identified as Status Indicator ldquoCrdquo
bull Refer to Addendum B for Status Indicator
bull Refer to Addendum E for inpatient‐only list
bull All other services ‐ If outpatient = not paid
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient‐Only Exception 1
bull Defined in CPT to be a separate procedure
bull Other services contain procedure that can be paid outpatient with Status Indicator ldquoTrdquo
bull Same date as inpatient‐only
bull Payment made for separate procedure and remaining payable outpatient services
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient‐Only Exception 2
bull Patient ceases to breath before admission or transfer to another hospital
bull Report procedure with modifier ndashCA
bull Only on one procedure
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Inpatient‐Only Impact toPayment Window
bull Inpatient‐only procedures rendered to anoutpatient on date of admission or duringpayment window are not paid bull Submit a no pay claim Type of Bill (TOB) 110
bull In relation to exceptions two claims required bull Covered servicesprocedures on TOB 11x (withexception of 110)
bull Non‐covered servicesprocedures on TOB 110 bull Both covered and non covered claims must have a matching Statement Covers Period
bull Effective 07‐01‐11
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 4 Admission with Outpatient Services
bull On Saturday (081312) patient presents to ER with a headache is evaluated and sent home with medication as needed
bull On Sunday (081412) patient returns to ER again with a headache but also has shortness of breath and chest pain bull Patient is placed in observation and diagnostic tests are ordered
bull On Monday (081512) patientrsquos condition worsens and is admitted as an inpatient
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 4 Admission with Outpatient Services
bull Would statement fromthrough dates begin with date services were rendered on Saturday
OR
bull Sunday when patient began observation services
OR
bull Monday when the patient was actually admitted
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 4 Admission with Outpatient Services
bull Is admit date reported as Saturday when patient presented to ER
OR
bull Sunday when observation services began
OR
bull Monday when patient was admitted as inpatient
Can an outpatient claim be submitted
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Special Edition (SE) 1117
Correct Provider Billing of Admission Date and Statement Covers Period
bull National Uniform Billing Committee (NUBC) definitions bull Admission date = Date patient admitted as inpatient
bull Statement covers period = Identifies span of service dates reported on claim bull Pub 100‐04 Chapter 1 Section 80322
bull Pub 100‐04 Chapter 25 Section 751
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 5 Patient On Dialysis
bull Patient presents to ER for an unrelated medical emergency and order is written to place in observation bull While in observation patient misses regularly scheduled dialysis treatment
bull Patient subsequently receives dialysis treatment concurrent to observation services
Is this carved out as active monitoring time
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 5 BillingUnscheduled Dialysis
bull End Stage Renal Dialysis (ESRD) requires active monitoring bull While in observation this time is carved out
bull Report HCPCS G0257 ‐ Unscheduled or emergency dialysis treatment for an ESRD patient in a hospital outpatient department that is not certified as an ESRD facility
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Scenario 5 Special Servicesfor Outpatient Billing bull Routine dialysis treatments not paid under OPPS
bull Payment for unscheduled dialysis is limited to bull Emergency Room and missed routine treatment
bull Emergency dialysis to avoid inpatient admission
bull Following or in connection with dialysis related procedures
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Rate Review National Paid Claim Error
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Outpatient Observation
bull National Paid Claim Error Rate indicates concern regarding one‐day inpatient admissions amp outpatient observation services bull Errors indicate observation would have sufficed
bull Nationally accounts for $15 billion in claims payment errors for the November 2011 report
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
National Paid Claim Error Rate bull National Claim Paid Error Rate
bull 78 = $241 Billion
bull Impacts all providers submitting Fee for Service claims bull Limited random claim sample bull Record requests must be received within 30 days from the initial CERT letter
bull Right to Appeal Yes
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
National Paid Claim Error Rate ndash Common Errors bull Insufficient Documentation
bull Documentation did not contain a valid physicianrsquos signature
bull Documentation did not support services billed
bull Documentation did not contain a valid physician order
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
National Paid Claim Error Rate ndash Common Errors
bull Medical Necessity bull Lab andor diagnostic services did not contain a physicianrsquos order or valid requisition form in the documentation
bull Physician signature was not legible
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
National Paid Claim Error Rate ndash Common Errors
bull Incorrect coding bull Lab services billed incorrectly
bull Incorrect number of unitsservices submitted on claim
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom
Thank You For more Self Paced
Learning go to Learning ampEducation on our website at wwwpalmettogbacom