
North%20 Perth%20 Bus%20 Plan %20 Sept%2006 Pdf
67
Coulson and Associates, Health Services Consultants 9/5/06 North Perth Family Health Team Business and Operational Plan September 5, 2006
description
Transcript of North%20 Perth%20 Bus%20 Plan %20 Sept%2006 Pdf

C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
North Perth Family Health Team
Business and Operational Plan
September 5, 2006

North Perth Family Health TeamBusiness and Operational Plan 2
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
North Perth Family Health Team
Business Plan
I – Executive Summary...............................................................................................................3II – Business Plan .......................................................................................................................5Governance and Accountability ..................................................................................................5Vision, Mission, Values and Strategic Objectives .......................................................................8Population Characteristics and Health Status.............................................................................10Health Status.............................................................................................................................11Utilization of Health Services ...................................................................................................12General Information and List of Programs and Services............................................................13Core/Comprehensive Services...................................................................................................15Summary of Program Staffing Requirements ............................................................................18Implementation Timelines.........................................................................................................19Location of Services and Programs ...........................................................................................22Physical Facility Needs.............................................................................................................22Location of After-Hours Services..............................................................................................23Current and projected patient enrolment....................................................................................23Five-Year Financial Forecast ....................................................................................................24III- Operational Plan .................................................................................................................25Strategic Planning Objectives....................................................................................................25Enrollment of Patients...............................................................................................................26Core Primary Care Services ......................................................................................................27Chronic Disease Management...................................................................................................29Primary Mental Health Services................................................................................................30Substance Abuse (Adolescents and Young Adults) ...................................................................33Health Promotion and Disease Prevention.................................................................................34Case Management and System Navigation................................................................................37Rehab Services .........................................................................................................................38Summary of Staffing Requirements ..........................................................................................40Linkages and Partnerships.........................................................................................................40Human Resources .....................................................................................................................41Collaborative Team Practice .....................................................................................................42Extended Hours ........................................................................................................................44Other Programs.........................................................................................................................44Evaluation Mechanisms ............................................................................................................45Consolidated Timelines for Implementation..............................................................................46Physical Facilities .....................................................................................................................46Information Technology............................................................................................................47Annual Budget..........................................................................................................................49

North Perth Family Health TeamBusiness and Operational Plan 3
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
I – Executive SummaryThe North Perth Family Health Team (NPFHT) has been approved by the Ministry of Health toprovide primary health care services to the community of North Perth and portions of thesurrounding townships of Howick, Huron East, Minto, Mapleton, Wellesley and Woolwich.
At present, the nine family physicians who work at the Listowel Medical Clinic as well as thenursing and support staff who work within this clinic provide most primary care services. After-hours and on weekends, the family physicians staff the Emergency Department of the ListowelMemorial Hospital and provide both true emergency and non-urgent primary care from thislocation.
For many years, the Listowel Medical Clinic has operated as an independent health facilityfunded by the family physicians who own this facility. Several years ago the family physiciansformed the Listowel Family Health Network and moved to a new, blended payment method ofpayment. All of the family physicians in Listowel are members of the Family Health Network(FHN). The physicians have enrolled approximately 15,000 patients to date.
This Business and Operational Plan has been prepared in accordance with Ministry of Healthguidelines for Family Health Teams. The Plan requests funding from the Ministry of Health forthe recruitment of 16 FTE allied health professionals as well as 4.5 FTE administrative staff forthe NPFHT as follows:
Health Professionals ProposedComplement
Family Physicians 12Nurse practitioners 2Registered Nurses 3.5Registered Practical Nurses 3Social workers 2Youth Counselor 1Case Managers 1Dietician 1Occupational therapist 0.5Pharmacist 1Health educator 1FHT Administrator 1Clerical staff 2Clinical Coordinator 1Data Analyst 0.5

North Perth Family Health TeamBusiness and Operational Plan 4
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Based on the guidelines provided by the Ministry of Health, it is estimated that the NPFHTwill require $1,134,365 for the first year (7 months) of its operation. This amount will increasein future years. In addition, the NPFHT is requesting one-time start-up costs of $174,200 for thepurchase of supplies and equipment to implement the FHT.
The NPFHT has developed a governance structure that requires the formation of a new, non-profit corporation that will be managed by a Board of Directors comprised of family physiciansand representatives of the Listowel Memorial Hospital, the Huron Perth CCAC, the Perth PublicHealth Unit and other members of the community. Representatives of other allied healthprofessionals will also be selected to become members of the Board of Directors. A CommunityAdvisory Committee will be formed to assist the NPFHT in the ongoing development ofprograms and services. This Committee will be comprised of a number of organizationsincluding:
• The Listowel Memorial Hospital
• Hospital Foundation
• Perth CCAC (or its successor)
• Perth District Health Unit
• Community mental health services
• Municipality of North Perth
• Representative of the long-term care sector
• Seniors services representatives
• VON
• Other community representatives as appropriate.
An implementation plan has been developed that sets out the numerous activities that must becompleted in order to ensure that the NPFHT is developed in a logical, effective, efficient andtimely manner.
The Steering Committee for the NPFHT is confident that this Business and Operational Plan willresult in the successful development of a Family Health Team that will meet the primary healthcare needs of the citizens of North Perth and surrounding communities for many years. TheSteering Committee looks forward to the opportunity of meeting with the Ministry of Health todiscuss this Plan.

North Perth Family Health TeamBusiness and Operational Plan 5
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
II – Business PlanThis Business Plan has been prepared in accordance with guidelines provided by the Ministry ofHealth for the development of Family Health Teams.
Governance and AccountabilityThe North Perth Family Health Team (NPFHT) will be a mixed Family Health Team and will begoverned by a Board of Directors comprised of representatives of the Listowel Family HealthNetwork and other representatives of the community. A new non-profit corporation will beformed with a separate Board to manage the affairs of the NPFHT. At the present time, there arenine full-time family physicians in Listowel who are members of a non-incorporated professionalAssociation, called the Listowel Family Health Network. The Listowel FHN receives fundingfrom the Ministry of Health and Long Term Care under the terms of the FHN capitated paymentmechanism.
The Listowel Family Health Network is comprised of all physicians in Listowel and has beenin operation for several years. The Listowel family physicians are all in a single clinic across thestreet from the Hospital. There is a governance structure in place to manage the business affairsof the Listowel Medical Clinic as well as a governance structure to manage the affairs of theFHN. Historically, there has always been a close working relationship between the Listowel
Memorial Hospital and the Listowel family physicians. The formation of the NPFHT will build
on this successful working relationship.
In developing this Business and Operational Plan, a NPFHT Steering Committee was createdcomprised of representatives of the Listowel FHN as well as the CCAC, Public Health, theHospital and the Municipality of North Perth. The Steering Committee has met on a monthlybasis over the past several months to prepare this Business Plan.
The Board of the FHT will be comprised of members of the FHN and representatives of the
Listowel Memorial Hospital, the Municipality of North Perth, the CCAC and the Public Health
Unit. The proposed governing Board for the NPFHT is shown in the chart below.

North Perth Family Health TeamBusiness and Operational Plan 6
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
As the NPFHT develops in the future, there may be a need to expand the Board of directors
to include other representatives of primary care organizations in the community. The NPFHT
Board of governors would select representatives from the following:
• Representatives of the Listowel FHN.
• Representatives from the Patient Care Council
• Representatives from a Community Advisory Committee comprised of the Hospital,
CCAC, mental health, public health, the Municipality of North Perth and other members
of the community.
Patient Care Council
It will be important to provide an opportunity for all allied health members of the FHT to
participate in the ongoing development of the FHT. In particular, it will be important for the
FHT to focus on the best way to meet the needs of patients who require primary care services.
To assist in the development of a collaborative practice model that focuses on the needs of
patients, a Patient Care Council would be formed comprised of representatives of the following
regulated health professional groups:
• Family physicians
• Nurse practitioners
• Family practice nurses
• Social workers
• Mental health workers
North PerthFamily Health Team10 to 12 Board members
Listowel FHN Patient Care CouncilNP, RN, RPG, SW, PT, OT,Pharm, Diet.
CommunityAdvisoryCommitteeHospital, CCAC,Public Health,Municipality ofNorth Perth
3 members
3 - 5 members
3 - 5members

North Perth Family Health TeamBusiness and Operational Plan 7
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
• Pharmacists
• Dieticians
• Physiotherapists.
As other primary health care professionals are added to the Family Health Team, they should be
represented on the Patient Care Council. It may also be appropriate to have members of the
Community Advisory Committee as ex-officio members of this Council. The responsibilities of
the Patient Care Council would include the following:
• Develop an approach to patient care that focuses on the needs of patients and their
families
• Develop a collaborative practice model for the NPFHT that recognizes the standards of
clinical practice of each of the allied health professional groups
• Provide advice on the NPFHT clinical human resource plan
• Advise the Board on all matters pertaining to professional, clinical, and technical services
• Review the effectiveness of the program delivery model used by the NPFHT and to
identify any problems, challenges and barriers to the delivery of care
• Develop a dispute resolution process for resolving any conflicts among the allied health
professionals
• Ensure that all patient/client programs are meeting their goals and objectives
• Propose any new and expanded programs that should be developed by the FHT
• Ensure that continuing education programs that focus on the development of a multi-
disciplinary collaborative team are developed for the professional staff of the FHT
• Participate in the ongoing assessment of the health care needs of the community and
assess the FHTs role in meeting the needs of the Community
• Assist in the development of an information system that links family physicians and
allied health professionals
• Advise the NPFHT Board of any clinical practice issues.
Community Advisory Committee
The Community Advisory Committee will be comprised of a number of organizations including:• The Listowel Memorial Hospital
• Hospital Foundation
• Perth CCAC (or its successor)
• Perth District Health Unit
• Community mental health services

North Perth Family Health TeamBusiness and Operational Plan 8
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
• Municipality of North Perth
• Representative of the long-term care sector
• Seniors services representatives
• VON
• Other community representatives as appropriate.
The responsibilities of this Community Advisory Committee CAC) will include the following:
• Elect representatives to the Board of the NPFHT to represent the members of the CAC
• Ensure that the member of all primary care health organizations have the opportunity to
participate in the development of the strategic plan for the FHT
• Ensure that all primary care stakeholders are aware of the activities of the NPFHT
• Provide a form for discussion of issues of concern to the members
• Participate in the ongoing development of programs and services for the NPFHT
• Participate in the strategic planning process of the NPFHT
• Receive reports from the NPFHT on its activities and future plans.
A Transitional NPFHT Board
The governing structure described above represents a long-term vision of the future structure of
the NPFHT. In the short-term, a smaller governing Board will be formed to function as a
transitional Board for the NPFHT. As the NPFHT develops in the future, additional members
Vision, Mission, Values and Strategic ObjectivesThe following vision and mission statements have been developed by the Steering Committee forthe NPFHT to guide the work of the North Perth Family Health Team:
• VISION: North Perth: A healthy rural community• MISSION: To provide high quality, comprehensive primary care services in a timely
manner to the residents of North Perth.
Values
The development of the NPFHT will require considerable commitment from all health careproviders within the FHT to work together in a collaborative and mutually respectful manner.To guide all members of the FHT, it is important that the team develop a common set of valuesthat will be respected by all team members. The following guidelines have been developed bythe Steering Committee for consideration by the FHT:
• We value and are committed to delivering Patient-Centred Health Care
North Perth Family Health TeamBusiness and Operational Plan 9
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
• We are committed to ensuring Quality Care for all patients• We will strive to provide patients with Timely Access to care• We value Collaboration amongst all stakeholders within the Family Health Team• We are committed to ensuring a Balanced Work/Lifestyle for all FHT members• We are committed to individual and organizational Accountability• We will maintain and uphold Ethical practices.
Patient-Centered Practice Model
In serving the catchment area of North Perth, the Family Health Team is proposing to implementa patient-centered service delivery model. Within this approach, all services will be planned,coordinated and delivered based on the needs of patients and their families. Patients will haveinput into the scope and range of services to be provided by the NPFHT and service delivery willbe flexible to respond to the changing needs of the patient population. The ongoing needs ofpatients will be managed within the FHT and the FHT will provide comprehensive care topatients at all times.
Strategic Objectives
To assist in the ongoing development of the NPFHT, the Steering Committee has set out anumber of Strategic Objectives that will provide a framework to guide the future delivery ofprimary health care services by the North Perth Family Health Team. The Team will enhanceand strengthen the high quality primary care services currently provided by the family physiciansand the staff of the Listowel Medical Clinic. These enhancements will include: more effectivemanagement of chronic disease, greater focus on prevention of illness and injury, and reducinginappropriate hospital admissions.
• Strategic Objective #1: To develop an integrated and patient-centred primary health careteam
• Strategic Objective #2: To provide patients with timely access to primary care servicesand effective coordination of those services
• Strategic Objective #3: To provide quality health promotion and prevention services toreduce injury and disease (primary prevention)
• Strategic Objective #4: To provide enhanced screening and early identification ofdisease (secondary prevention)
• Strategic Objective #5: To effectively manage chronic disease in the catchmentpopulation served by the North Perth FHT

North Perth Family Health TeamBusiness and Operational Plan 10
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
• Strategic Objective #6: To transform the existing electronic medical record currentlyshared by the hospital and medical clinic into a common electronic health record which isshared by all regulated health care professionals in North Perth.
Population Characteristics and Health StatusThe NPFHT will service a geographic area that is very similar to the catchment population of theListowel Memorial Hospital. This catchment population will include the municipality of NorthPerth plus portions of the following surrounding municipalities:
• Howick Township, Huron County• Huron East, Huron County• Minto, Wellington County• Mapleton Township, Wellington County• Wellesley township, Regional Municipality of Waterloo• Woolwich Township, Regional Municipality of Waterloo.
In 2001, the population of North Perth was 12,055 and the estimated population of theadjacent communities was estimated at 26,000. Further detailed demographic information aboutthe catchment population to be served by the NPFHT is included in Appendix 1.
Demographics
Review of the socio-demographic characteristics of North Perth indicate a number of keyfeatures that will affect the future need for primary care services in the area.
The median age of the 2001 population in North Perth was 36.6 years slightly below theprovincial average of 37.2 years (Appendix 2). According to the Canadian Institute of HealthInformation, North Perth is located in a rural health region that has one of the oldest age profilesin Canada. According to CIHI, the Grey Bruce Huron Perth region ranks 1st in Ontario and 5th
highest in the country in terms of the proportion of seniors over the age of 65 yrs.
Average earnings for all working persons (both full-time and part-time) are $27,141, whichis lower than the provincial average of $35,185 (Appendix 2). Median family income wasreported as $57,442, which is again lower than the provincial average of $61,024. Thepercentage of the local population who has less than a high school graduation certificate is higherthan the provincial average across all age groups (Appendix 2).

North Perth Family Health TeamBusiness and Operational Plan 11
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
The proportion of the labour force employed in agriculture and other resource-basedindustries is 18% compared to the provincial average of 3% (Appendix 2).
North Perth is home to a large Anabaptist community, specifically seven distinct Amishand Mennonite cultural groups (Appendix 3). As of 2002, there were approximately 540families for a total Anabaptist population of over 3,000 individuals. Because of their religiousbeliefs, these individuals represent a significant challenge in terms of delivering primary healthservices.
Health StatusOne of the standard indicators for a population’s overall health status is a mortality rate. InAppendix 4, age-standardized mortality rates and the standard measure of premature death(PYLL – potential years of life lost) are shown for the Grey Bruce Huron Perth planning area(i.e. the northern and central parts of the Southwest LHIN planning region) compared to theprovincial average and the Thames Valley planning area (i.e. the southern part of the SouthwestLHIN). On both of these mortality indicators, the rates for the residents of the Grey BruceHuron Perth area are significantly higher than the provincial average and higher than the ThamesValley area.
Another important source of information about a community’s health status is the resultsfrom the Canadian Community Health Survey. The results are based on a random survey ofresidents in each public health unit district. In terms of possible gaps in service, 8.8% of Perthresidents reported that they had unmet health care needs which is less than the provincial averageof 12.1%. In terms of lifestyle choices and health behaviours, the proportion of overweightmales in Perth is higher than the provincial average but obesity levels are slightly less than theprovincial average. These higher BMI scores may be attributable to levels of fitness and activity;and Perth residents are generally less physically active than the provincial average (Appendix 5).
Hospital discharges summaries are another source of information about the health status of acommunity. Data from the Listowel Memorial Hospital is provided in Appendix 6. This dataindicates that maternal and child-care account for the greatest number of inpatient hospitaladmissions. This data also indicates that chronic conditions such as cardiac conditions (heartfailure, heart attack, chest pain), gastrointestinal problems, stroke and diabetes all account for asignificant number of inpatient hospital admissions.

North Perth Family Health TeamBusiness and Operational Plan 12
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
The Anabaptist communities have some specific health status issues that require specialmention. These include but are not limited to:
• Poor dental health (especially the low German speaking Mennonites from Mexico)• Lack of prenatal care• Lack of knowledge of preventive health care• Higher incidence of certain genetic disorders• Tendency to use alternate health practitioners before seeking medical attention.
Because of their religious beliefs, some of these Amish/Mennonite groups do not have anOntario health card, preferring to pay cash for their medical care. This means that health careaccess can be limited by a family’s financial situation.
Utilization of Health ServicesOver the past three years, the Listowel Memorial hospital has seen a dramatic increase inambulatory visits through its Emergency Department (Appendix 7). Between 2003-04 and 2005-06, Emergency visits increased by over 40%. Many of these ambulatory cases are non-urgentand could be classified as primary care. Based on interviews with Hospital and medical staff,these significant increases in emergency volumes can be attributed to:
• The shortage of family physicians leading to increasing numbers of ‘orphan’ patients andgrowing wait lists at the medical clinic
• A greater in-migration from surrounding rural communities and townships.
In the future, many of these patients will be cared for by the Family Health Team and thiswill allow the Listowel Memorial Hospital to better manage demands on its EmergencyDepartment.
Community Care Access Centre
Caseloads for the CCAC are also increasing. In the three-year period from 2003-04 to 2005-06,the CCAC caseload from North Perth went from 452 clients to 556 clients, an increase of over20%. This is not simply a result of population aging since half of the CCAC clients are less than65 years old (Appendix 8). The mix of CCAC clientele is also changing over time with adeclining proportion of acute care cases and increasing numbers of long term care and rehabclients. The lack of rehab resources in North Perth is well documented (Appendix 9).

North Perth Family Health TeamBusiness and Operational Plan 13
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Environmental Factors
North Perth is a largely rural area centered around the town of Listowel. The health differentialsbetween urban and rural populations have been well documented as well as the geographicchallenges of ensuring equitable access to health services for rural residents.1 The Romanowreport in 2002 highlighted that geography is indeed a ‘determinant of health’ and described theoverall problem in terms of an Inverse Care Law:
• “People in rural communities have poorer health status and (therefore) have greaterneeds for primary care, yet they are not as well served and have more difficulty accessinghealth care services than people in urban centres”2
Community Resources
There are a number of primary care providers and community resources who provide servicesthat will complement the services offered by the North Perth Family Health Team. Theseinclude:
• Canadian Mental Health Association, Huron-Perth Branch• Chiropractors• Community Care Access Centre for Perth• Dentists• Fordwich Nursing Home, Royal Terrance (Palmerston) and Caressant Care (Listowel)• Listowel Memorial Hospital• Optometrists• Perth District Health Unit• Registered Massage Therapists• Victorian Order of Nurses, Huron-Perth Branch.
General Information and List of Programs and ServicesCurrently, the nine Listowel family physicians receive funding from a number different sourcesincluding capitation payments through the FHN contract, alternative funding arrangements(AFA) for Emergency Department work, fee-for-service for hospital care, non-rostered patients,etc, hospital on call coverage for OB, anesthesia and third party billing. The chart below
1 Romanow Commission, Building on Values: The Future of Health Care in Canada, 2002 and the MinisterialAdvisory Committee on Rural Health, Rural Health in Rural Hands, 2002; Small Hospitals Provincial Advisory Group ofthe Ontario Hospital Association, “Ensuring Access to Care in Rural, Remote and Northern Communities”, August 20032 Romanow report, p. 162
North Perth Family Health TeamBusiness and Operational Plan 14
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
indicates the current status of each physician in terms of their FTE status and the services thatthey provide (e.g. FP = family practice, IN = inpatient, NH = nursing home, OB = obstetrics):
• Dr. Annis: 1.0 FTE, FP, IN, ER, OB, NH• Dr. Connors: 0.5 FTE, ER, anesthesia only• Dr. Edmonds (currently on maternity leave): 1.0 FTE , FP, IN, ER, NH, anaesthesia,• Dr. Klassen: 0.5 FTE, FP, IN, NH, and 2 public health sexual health clinics• Dr. Latuskie: 1.0 FTE, FP, IN, ER, OB, NH• Dr. Matthews: 1.0 FTE, FP, IN, ER, OB, NH• Dr. Qureshi: 1.0 FTE, FP, IN, ER, OB, NH and is a coroner• Dr. Rutherford: 0.5 FTE, FP, IN, ER, NH, anesthesia,• Dr. Suggit: 1.0 FTE, FP, IN, ER, OB, NH• Dr. Warren: 1.0 FTE, FP, IN, ER, NH, anesthesia• Dr. Westen: 0.5 FTE, FP, IN, OB, NH
All current staff at the Listowel Medical Clinic are paid for by the Listowel Family HealthNetwork. The existing staffing complement includes:
• 4.0 FTE Registered Practical Nurses• 3.5 FTE Registered Nurses• 3 FTE Receptionists• 5 FTE Office/Filing Staff.
The nursing staff play an important role in the provision of patient care. As additionalnursing staff are recruited, one of the RNs will play a role in assisting cancer patients byliasoning with the Ontario Breast Screening Program, helping patients navigate the system,arranging cancer check-ups, arranging a call-back system and answering patients questionsrelated to their disease or their treatment. This nurse will also participate in patient careconferences that are held with the patient’s surgeon and pathologist.
Population to be Served
The catchment population for the North Perth FHT is estimated at 26,000. There are 15,000individuals currently rostered with the Listowel Family Health Network. As the NPFHT isdeveloped, it is expected that the physicians and nurse practitioners will enroll approximately8,000 additional patients.
Until the successful implementation of this Operational Plan and the recruitment ofadditional family physicians and nurse practitioners, there will continue to be orphans patients

North Perth Family Health TeamBusiness and Operational Plan 15
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
who obtain their primary care either through the Hospital Emergency Department or who willhave to travel greater distances to larger centres which are further away (i.e. Stratford,Kitchener).
Core/Comprehensive ServicesThe North Perth Family Health Team will provide the following comprehensive range ofprimary care programs and services:
• Access to Prenatal, Obstetrical, Post-Natal and In-Hospital Newborn Care including theprovision of maternity services including antenatal care to term, labour and delivery, andmaternal and newborn care.
• Arrangements for 24/7 Coverage including extended office hours and Telephone HealthAdvisory Services.
• Coordination and Provision of Rehabilitative Services including referral to mostappropriate rehab service provider, participation in planning and follow up, and care mapdevelopment.
• Chronic Disease Management including screening, diagnosis, treatment, management,and care coordination.
• Diagnosis and Treatment of Episodic Illness and Injury including full range of acuteprimary illnesses and injuries.
• Education and Support for Self Care including health education, telephone advice anddirection, with a special emphasis on patients managing a chronic illness
• Health Assessment including history taking, physical exams, laboratory/diagnosticevaluation.
• Health Promotion including lifestyle counseling;• Illness Prevention including periodic exams, primary, secondary and tertiary prevention,
screening patients at risk, early detection initiatives, risk reduction counseling,immunization programs and an electronic call back system.
• Primary Reproductive Care including birth control counseling, pregnancy diagnosis,counseling re birth control and family planning, screening and treatment for sexuallytransmitted diseases;
• Primary Mental Health Care including diagnosis and treatment of emotional andpsychiatric problems/illness, monitoring, referral, and case management;
• Primary Palliative Care including home visits, individual and family support, painmanagement, monitoring and case management.

North Perth Family Health TeamBusiness and Operational Plan 16
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
• Support for Hospital, Home and Long-Term Care Programs including participation indischarge planning for FHT patients, rehabilitation services, outpatient follow up, andhome care services.
• System Navigation and Case Management including service coordination, monitoringand referral to other health care providers including specialists, rehabilitation services,home care and hospice programs, and diagnostic services.
To-date, approximately 15,000 patients have rostered with the Listowel Family HealthNetwork. Based on the current complement of 9.0 FTE physicians, this represents a ratio of1,667 patients per full-time doctor. With the introduction of new FHT allied health professionalssupporting and complementing existing physician practices, this ratio can be modestly increased.It is estimated that the total number of rostered patients could be increased to approximately17,000 with existing family doctors. To increase roster size further will require new familyphysicians and nurse practitioners.
As a result of physician shortages in North Perth and surrounding municipalities, there are anincreasing number of ‘orphan’ patients who are receiving their primary care through the HospitalEmergency Department. Over the last three years, the number of ambulatory visits to theEmergency Department has increased by 40%. Many of these ambulatory visits are non-urgentand could be handled by primary care health professionals in a clinic setting.
The NPFHT is requesting funding for three new family physicians (3.0 FTE); two NursePractitioners (2.0 FTE); one Registered Nurse (1.0 FTE); one Registered Practical Nurse (1.0FTE and a part-time Pharmacist (0.5 FTE) to expand these service to care for more patients. It isestimated that each Nurse Practitioner could care for 800 additional patients and each familyphysician could care for an additional 1,700 patients.
Chronic Disease Management
Like many rural populations, North Perth has a high incidence of chronic diseases such as heartand stroke disease, diabetes, and COPD. Much of this disease burden is a result of unhealthylifestyle choices including poor diet, smoking, alcohol abuse and lack of exercise. Bettermanagement of these chronic diseases will be a significant programmatic emphasis for the FHT,where allied health professionals will work collaboratively with patients and their families oncustomized care plans. In terms of program priorities, the FHT’s chronic disease managementprogram will start with Diabetes because it has the potential to lead to other diseases if notproperly managed and controlled.

North Perth Family Health TeamBusiness and Operational Plan 17
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
The NPFHT are requesting funding for the following positions Registered Nurse (1.0 FTE);Registered Practical Nurse (1.0 FTE); Dietician (1.0 FTE); Case Manager (0.5 FTE - contracted);Pharmacist (0.5 FTE) to expand this program. Medical specialists such as paeditrician and ageriatrician will also assist in this program.
Primary Mental Health Services
For many years, the Ministry of Health’s reform of the mental health system has focused ontreating and supporting the seriously mentally ill. As a result, for large numbers of patients whoare suffering mild to moderate mental health problems, the only choices are private therapists orfamily physicians offering psychotherapy. For rural family physicians with large and busypractices, it is very difficult to find the time to provide the proper care and support to thesechallenging patients. Because of the large and increasing rural elderly population, health careproviders in North Perth are dealing with a growing number of older patients with dementia.Funding for a part-time geriatrician has been requested to assist in this program.
Substance Abuse (Adolescent/Young Adult)
Choices for Change already provides a youth worker for North Perth (1 day per week) but thislevel of staffing has proven inadequate to deal with the significant number of substance abuseproblems among teenage youth (both alcohol and drugs, such as crystal meth). The NPFHT isrequesting funding for a Youth Addictions Counselor (1.0 FTE) to develop this program and forsessional fees for a child psychiatrist to assist in the provision of services.
Health Promotion/Disease Prevention
Two of the key strategic objectives of the NPFHT focus on the development of primaryprevention (promotion of healthy lifestyles) and secondary prevention (enhanced screening andearly identification of disease) programs and services. The NPFHT will develop a partnershipwith the Perth District Health Unit in planning for and delivering these programs. The NPFHT isrequesting funding for a Registered Nurse (1.0 FTE) and a Health Educator (1.0 FTE) to providethese programs. Funding for a paediatrician has also been requested to assist in this program.
Case Management/System Navigation
One of the key strategic objectives of the NPFHT is to improve the coordination of services forpatients both within the FHT and between the FHT and other service providers. Part of thiscoordination takes place at the point of triage where individuals may need help with
North Perth Family Health TeamBusiness and Operational Plan 18
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
referrals/linkages with other service providers; and part of this coordination takes place in themanagement of customized care plans where a case manager works with patients and families tomake sure that clinical goals are achieved (e.g. chronic disease management). These casemanagement/system navigation strategies will be accomplished in partnership with the PerthCommunity Care Access Centre who currently employ case managers. The NPFHT isrequesting funding for a Registered Practical Nurse (1.0 FTE) and a Case Manager (0.5 FTE) toprovide this expanded case management service.
Rehab Services
To assist in the identification of the need for rehabilitation services in North Perth, a specialrehab sub-committee of the FHT steering committee was formed. This committee has identifieda number of gaps in local rehabilitation services (Appendix 9). The NPFHT is requestingfunding for a part-time occupational therapist as the first stage in the development of a morecomprehensive program that will be implemented in the second year of operation of the NPFHT.
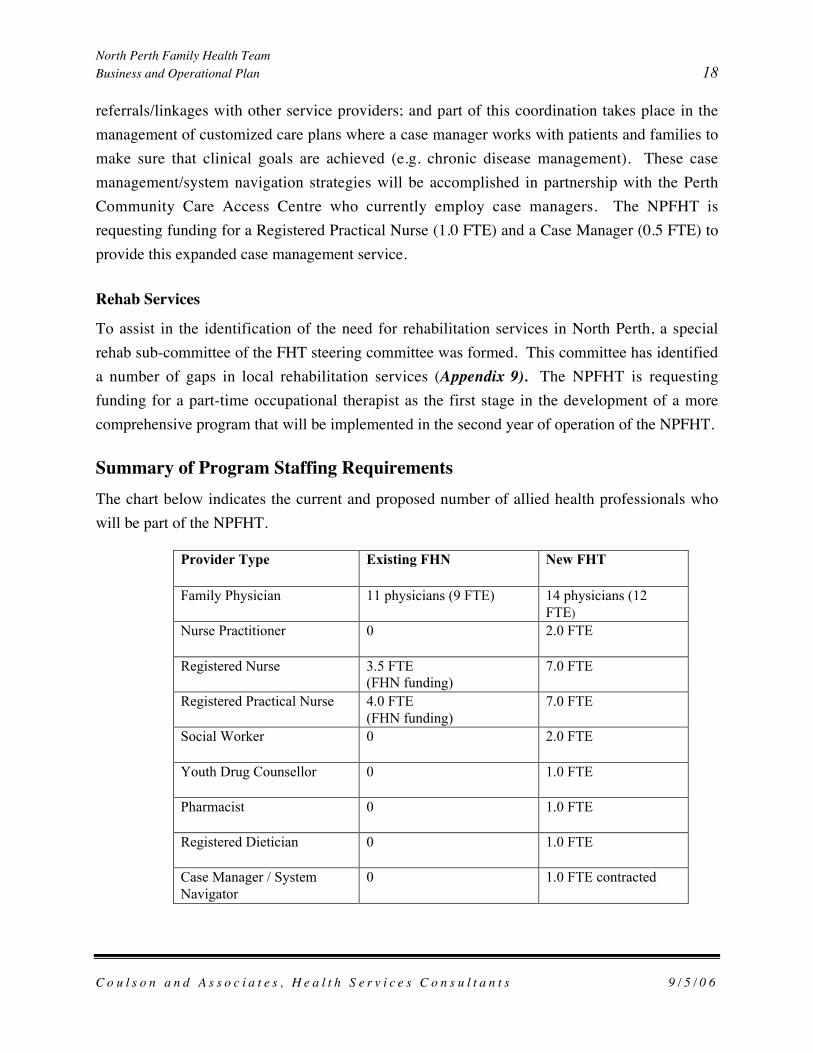
Summary of Program Staffing RequirementsThe chart below indicates the current and proposed number of allied health professionals whowill be part of the NPFHT.
Provider Type Existing FHN New FHT
Family Physician 11 physicians (9 FTE) 14 physicians (12FTE)
Nurse Practitioner 0 2.0 FTE
Registered Nurse 3.5 FTE(FHN funding)
7.0 FTE
Registered Practical Nurse 4.0 FTE(FHN funding)
7.0 FTE
Social Worker 0 2.0 FTE
Youth Drug Counsellor 0 1.0 FTE
Pharmacist 0 1.0 FTE
Registered Dietician 0 1.0 FTE
Case Manager / SystemNavigator
0 1.0 FTE contracted

North Perth Family Health TeamBusiness and Operational Plan 19
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Health Educator 0 1.0 FTE contracted
Occupational Therapist 0 0.5 FTE contracted
Specialist Consults:
Paediatrician (Amishgenetic)
Visits/consults 1 – contract / sessional
Child psychiatrist Visits/consults 1 – contract / sessional
Geriatrician Visits/consults 1 – contract / sessional
Administrative Staff
In addition to the clinical staff that will be required for the operation of the NPFHT, there are anumber of administrative support staff who will be required to ensure that the FHT isimplemented and managed in an efficient and effective manner. The chart below summarizesthese requirements.
AdministrativeSupportRequirements
Existing Staffing Proposed FHT
Administrator 0 1.0 FTE
Receptionist 4.0 FTE 4.0 FTE
Clerical staff 3.0 FTE 5.0 FTE
IT programmer 0 1.0 FTE
Implementation TimelinesThe development of the NPFHT will take time and a phased implementation plan has beencreated to ensure that staff are recruited and programs are developed in a systematic and logicalmanner. To accomplish the objectives that have been established for the NPFHT, a three-yearImplementation Plan has been developed as set out in the chart below.
YEAR ONE ACTVITIESSubmit Business and Operational Plan to the MinistryObtain approval from Ministry to proceed

North Perth Family Health TeamBusiness and Operational Plan 20
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Create an Interim NPFHT Governance Board and a managementstructurePrepare documents for the incorporation of the FHTSelect a FHT Administrator to manage the ongoing development of theFHTDevelop a detailed Implementation PlanDevelop a detailed Strategic Plan for the NPFHTConfirm the Vision, Mission and Strategic Objectives for the FHTConfirm the key program priorities for the NPFHTDevelop partnerships and linkages with community partners inaccordance with the program priorities set by the FHT BoardContinue to develop an Interdisciplinary Team modelRecruit first group of FHT staff (e.g. NPs, RNs, Mental health workers)Develop detailed operating policies and procedures for each programand service including job descriptions and equipment requirementsDevelop detailed plan for the redevelopment of the Medical Clinicbased on discussions with the Ministry of Health regarding the fundingthat will be available for this projectRecruit additional family physicians for the FHTDevelop and implement education programs for family physicians andother health care providers and stakeholders about the future plans forthe FHTDevelop a detailed plan for enrollment of additional patients andimplement the planDevelop second year Business and Operational PlanDevelop a detailed plan for providing access to the FHT informationtechnology system for the allied health professionalsDevelop a community communication plan for residents and healthprovidersConduct audit of first year of operation and submit to Ministry ofHealthHold annual meeting for the FHTDevelop a detailed plan for the evaluation of the progress of theNPFHT and select an independent team of researchers to conduct theevaluation

North Perth Family Health TeamBusiness and Operational Plan 21
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
evaluationYEAR TWO Develop a detailed plan for the redevelopment of the Medical Clinic
based on approved Business PlanDevelop program priorities for new and expanded programsEvaluate enrollment progress to date and adjust enrollmentimplementation plan as necessaryDevelop plans for satellite clinicsHire additional FHT staffRecruit additional family physiciansImplement the communications plan developed in first yearExpand scope of programs and servicesEvaluate progress to dateProvide educational programs for staff regarding the interdisciplinaryteam modelPrepare Business and Operational Plan for next yearEvaluate progress to date on the implementation of the FHTConduct audit of FHT and submit to the MinistryHold annual meeting for the FHTConsider the feasibility of developing shared programs and serviceswith other FHTs in the region
YEAR THREE Expand NPFHT BoardReview the strategic plan of the NPFHT and make any adjustments asappropriateReview the facilities plan to ensure that it meets the long range needs ofthe NPFHTConduct evaluation of programs and services in meeting theirobjectives and implement appropriate changes based on the evaluationRecruit additional physiciansHire additional FHT staffConduct audit of FHTSubmit next year Business and Operational PlanEvaluate communications plan for FHTEvaluate structure of the BoardEvaluate management structure

North Perth Family Health TeamBusiness and Operational Plan 22
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Revise strategic objectivesHold annual meeting of FHT
This preliminary Implementation plan provides a starting point for setting out the numeroustasks and activities that will be required to ensure that the NPFHT is developed in an effectiveand efficient manner. When the Ministry of Health has approved this Business and OperationalPlan, this Implementation Plan will be revised to reflect any changes that are proposed by theMinistry.
Location of Services and ProgramsInitially, all NPFHT services and programs will be offered in Listowel at the Medical Clinic orother facilities within the Listowel. As part of its longer range strategic plan, the NPFHT willexplore the feasibility of offering services in other communities in the rural townships. TheNPFHT will explore the potential of offering selected services in other communities in order toensure that patients who do not have access to transportation are able to access primary careservices. Several other rural FHTs are currently operating satellite clinics in smallercommunities and the NPFHT will review the experiences of these other FHTs as part of theplanning for expanding services to other locations.
Physical Facility NeedsThe Listowel Medical Clinic is out of date and requires expansion and upgrading to meet theneeds of current family physicians. With plans to recruit additional family physicians and to adda number of other allied health professionals to the primary care team, there is a need forexpanded facilities to accommodate these additional staff.
A Facilities Design sub-committee of the FHT steering committee has been established toassess a number of options for the redevelopment of the Medical Clinic. The options that arebeing considered include the following:
• Option 1 – Renovate the existing medical clinic, with an addition to the clinic eitherhorizontally or as a second floor or both.
• Option 2 – Demolish the current clinic and construct a new building on a new site.• Option 3- Renovate both the clinic and the Hospital outpatient building to meet the needs
of the NPFHT.

North Perth Family Health TeamBusiness and Operational Plan 23
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
The services of an architect and facilities planner have been engaged to review these optionsand to prepare cost estimates. In addition, the committee is considering how such a projectmight be funded and governed and the role that the Municipality, the Hospital, the familyphysicians and others may play in the redevelopment of these facilities. A business plan is beingprepared that will set out both the capital cost requirements as well as the funding andgovernance factors that must be considered as part of this project. When the business plan iscomplete, it will be submitted to the Ministry of Health for consideration.
The Ministry of Health has indicated that it is prepared to assist in the funding of capitalprojects related to the creation of FHTs. The NPFHT will present a plan to the Ministry for itsconsideration.
Location of After-Hours ServicesAt the present time, the Listowel FHN provides after-hours coverage for enrolled patientsthrough the Hospital Emergency Department. It is expected that this arrangement will continuefor some time until additional family physicians and nurse practitioners are recruited to the FHT.Physicians are remunerated for these services through an Alternative Payment Plan.
When the North Perth Family Health Team is at fully staffed as set out in this Business Plan,the need for and the feasibility of establishing an after-hours primary care clinic will be assessed.There is the potential that such a clinic could be staffed by Nurse Practitioners and primary carenurses in collaboration with the family physicians.
Current and projected patient enrolmentThere are 15,000 individuals rostered with the Listowel Family Health Network. Enrolment ofadditional patients is dependent on the successful recruitment of additional family physicians andnurse practitioners. Based on the projected recruitment of two new NPs, social workers andthree new family physicians, it is estimated that patient enrolment could be increased by some8,000 additional patients to over 23,000 patients by the end of 2009. The chart below indicates atime line for the enrollment of these additional patients based on the recruitment plans of theNPFHT.

North Perth Family Health TeamBusiness and Operational Plan 24
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
North Perth FHT Patient Enrolment Timelines
0
5,000
10,000
15,000
20,000
25,000
2006-Q4
2007-Q1
2007-Q2
2007-Q3
2007-Q4
2008-Q1
2008-Q2
2008-Q3
2008-Q4
2009-Q1
2009-Q2
2009-Q3
2009-Q4
Target Dates
No. o
f Pati
ents
Five-Year Financial ForecastIn accordance with Ministry of Health guidelines for the development of the Business andOperational Plan, a detailed operating budget has been prepared for the NPFHT for the next fiveyears. This detailed budget is presented in Appendix 11. Some of the key features of thisoperating plan include the following:
• In year one (7 months), the NPFHT will have an operating budget of $1,134,365 based on16 FTE allied health professionals and 4.5 FTE support staff.
• In year two, the NPFHT will have a projected operating budget of $1,568,426• In year three, the NPFHT will have a projected budget of $1,646,847• In year four, the NPFHT will have a projected budget of $1,726,061• In year five, the NPFHT will have a projected budget of $1,812,364.

North Perth Family Health TeamBusiness and Operational Plan 25
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
III- Operational PlanIn this section, the Operational Plan for the North Perth FHT is described as required by the
Ministry of Health and Long Term Care.
Strategic Planning ObjectivesThe specific objectives that have been developed for the NPFHT include the following:
• Strategic Objective #1: To develop an integrated and patient-centered primary healthcare team.
• Strategic Objective #2: To provide patients with timely access to primary care servicesand effective coordination of those services.
• Strategic Objective #3: To provide quality health promotion and prevention services toreduce injury and disease (primary prevention).
• Strategic Objective #4: To provide enhanced screening and early identification ofdisease (secondary prevention).
• Strategic Objective #5: To effectively manage chronic disease in the catchmentpopulation served by the North Perth FHT.
• Strategic Objective #6: To transform the existing electronic medical record currentlyshared by the hospital and medical clinic into a common electronic health record which isshared by all regulated health care professionals in North Perth.
One of the key activities that the NPFHT will undertake as soon as the Ministry of Healthapproves this Business and Operational Plan is to develop a detailed strategic plan that will setout how the FHT will move from its current operation to an expanded operation. As part of thisstrategic planning process, the NPFHT will give consideration to a number of key activities thatmust be completed to ensure that this Business Plan is achieved. These activities include:
• Development of an interim governance structure for the NPFHT that will integratefamily physicians, allied health professionals and other providers of primary care servicesin the community.
• Development of detailed program and services plans.• Development of strategic alliances and partnerships with the Listowel Memorial
Hospital, the Public Health Unit and the CCAC to provide specific services to the FHT.• The recruitment of a team of allied health professionals that will provide services to
target patient populations, especially those without family physicians.
North Perth Family Health TeamBusiness and Operational Plan 26
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
• Development of a management structure to assist in the ongoing development of theFHT.
• Development of management and operational guidelines for the Board and themanagement team to guide the ongoing development of the FHT.
• Creation of a patient care philosophy and a collaborative practice model that willensure that all allied health professionals are working together to best meet the needs ofpatients.
• Development of a business plan for the redevelopment of the Listowel Medical Clinic.
The completion of these tasks will be critical next steps for the NPFHT. The new NPFHTBoard and the management team must ensure that these tasks are undertaken in a timely fashion.
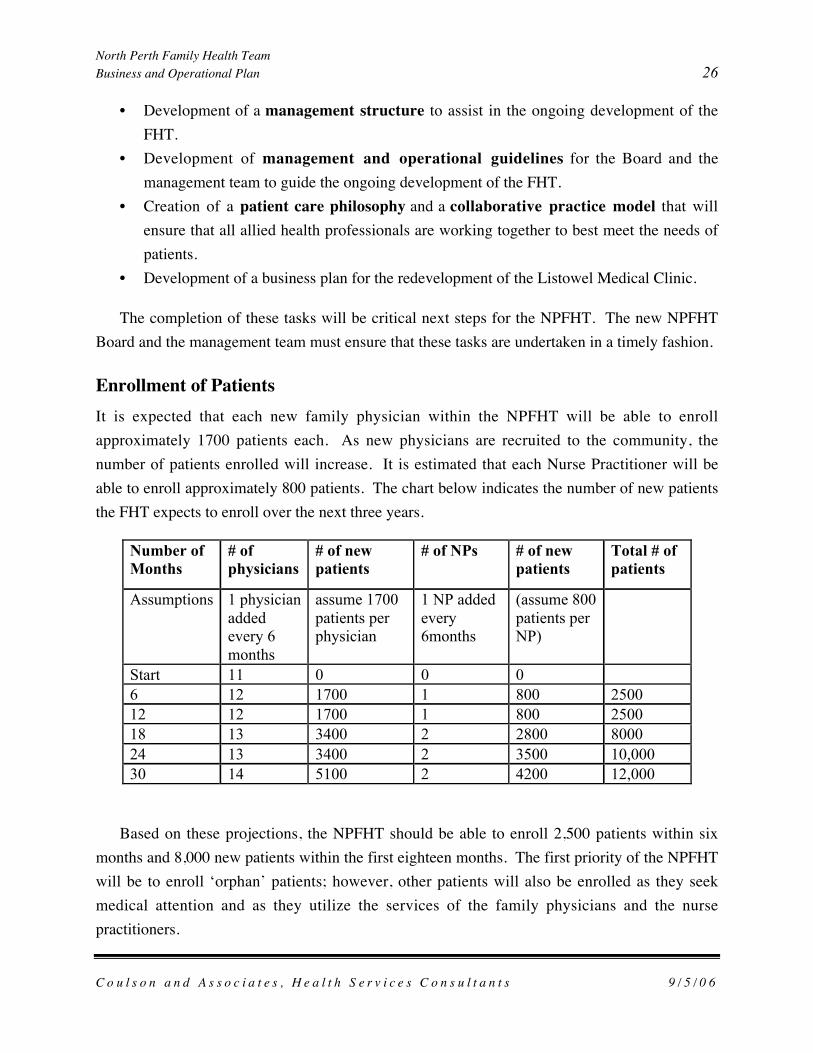
Enrollment of PatientsIt is expected that each new family physician within the NPFHT will be able to enrollapproximately 1700 patients each. As new physicians are recruited to the community, thenumber of patients enrolled will increase. It is estimated that each Nurse Practitioner will beable to enroll approximately 800 patients. The chart below indicates the number of new patientsthe FHT expects to enroll over the next three years.
Number ofMonths
# ofphysicians
# of newpatients
# of NPs # of newpatients
Total # ofpatients
Assumptions 1 physicianaddedevery 6months
assume 1700patients perphysician
1 NP addedevery6months
(assume 800patients perNP)
Start 11 0 0 06 12 1700 1 800 250012 12 1700 1 800 250018 13 3400 2 2800 800024 13 3400 2 3500 10,00030 14 5100 2 4200 12,000
Based on these projections, the NPFHT should be able to enroll 2,500 patients within sixmonths and 8,000 new patients within the first eighteen months. The first priority of the NPFHTwill be to enroll ‘orphan’ patients; however, other patients will also be enrolled as they seekmedical attention and as they utilize the services of the family physicians and the nursepractitioners.

North Perth Family Health TeamBusiness and Operational Plan 27
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
To assist in the enrollment process, the NPFHT will develop a communication strategy thatwill inform local residents of the implementation of the NPFHT and will encourage theseresidents to enroll with the family physicians and the nurse practitioners. Community enrollmentdays will be organized to promote the enrollment of patients. As the Team evolves and matures,it is expected that it will achieve further clinical efficiencies and that by Year Three, existingfamily doctors will be able to carry somewhat higher caseloads.
Core Primary Care ServicesIn this section of the Operational Plan, the programs and services that will be provided by theNPFHT are described in detail.
Comprehensive Care Services
The North Perth Family Health Team will improve access to primary health care through thecreation of an interdisciplinary health team that will offer a broad range of integrated programsand services. The core programs that will be offered by the North Perth Family Health Teameither directly or in partnership with other community service providers are described below.Comprehensive care requires that the ongoing needs of patients be considered within the contextof patients’ family and social needs. None of the identified core or special programs willfunction independently. The North Perth Family Health Team will provide all of the identifiedmandatory comprehensive care services, in addition to a range of optional and special services,targeted at the prevention and early identification of disease. The comprehensive care providedby the Family Health Team will include the following services:
• Health Assessment including history documentation, physical examinations anddiagnostic evaluation.
• Diagnosis and Treatment of Episodic Illness and Injury including acute minor andcomplex illness, acute minor and complex injury.
• Diagnosis and Treatment of Chronic Illness and injury, initial diagnosis and treatment,treatment adjustments, and monitoring.
• Primary Reproductive Care including birth control counseling, pregnancy diagnosis,counseling re birth control and family planning, screening and treatment for sexuallytransmitted diseases.
• Access to Prenatal, Obstetrical, Post-Natal and In-Hospital Newborn Care includingthe provision of maternity services including antenatal care to term, labour and delivery,and maternal and newborn care.

North Perth Family Health TeamBusiness and Operational Plan 28
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
• Illness Prevention including periodic exams, primary, secondary and tertiary prevention,screening patients at risk, early detection initiatives, risk reduction counseling,immunization, assessments.
• Health Promotion including Lifestyle counseling re determinants of health.• Education and Support for Self Care including health education, telephone advice and
direction.• Primary Mental Health Care including diagnosis and treatment of emotional and
psychiatric problems/illness, treatment adjustment, monitoring, referral, and casemanagement.
• Primary Palliative Care including home visits, individual and family support, initialtreatment, treatment adjustment, monitoring, referral, and case management.
• Support for Hospital, Home and Long-Term Care Programs including assisting withdischarge planning, rehabilitation services, outpatient follow up, and home care services.
• System Navigation and Case Management including service coordination, monitoringand referral to other health care providers including specialists, rehabilitation andphysiotherapy services, home care and hospice programs, and diagnostic services.Collaborate on medical treatment and monitor status.
• Coordination and Provision of Rehabilitative Services including referral to rehabservices, participate in planning and follow up, education and advocacy, and care mapdevelopment.
• Chronic Disease Management including screening, diagnosis, treatment, management,and care coordination.
• Arrangements for 24/7 Response including combining regular office hours withextended office hours and Telephone Health Advisory Services.
Patients without Family Physicians
There are an increasing number of orphan patients in the North Perth catchment area and manyof these patients are currently being cared for in the Hospital Emergency Department. In thefuture, it is expected that the NPFHT will care for an increasing number of these patients. Someof the patients will be referred to the NPFHT following their discharge from the Hospital andothers will be referred to the NPFHT following treatment in the Emergency Department. Otherswill be referred to the NPFHT as the community becomes more aware of the types of programsand services offered by the FHT. All family physicians in Listowel currently provide inpatienthospital care for their patients.

North Perth Family Health TeamBusiness and Operational Plan 29
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Chronic Disease ManagementThe Province of Ontario is pursuing and supporting a number of chronic disease managementinitiatives in areas such as diabetes, heart disease, stroke, cancer, osteoporosis, asthma, arthritis,Alzheimer Disease and others dementias and mental health that are aimed at enhancing patient’shealth and quality of life while reducing costs to the health care system. Over 80% of Ontariansover age 45, or 3.7 million people, are living with a chronic disease (Statistics Canada, 2003).Almost 70% of those individuals are living with two or more chronic conditions. In Ontario,diabetes is responsible for 25 – 33% of heart attacks, 34% of cases of heart failure, 30% ofstrokes, 64% of amputations, and 51% of new referrals for dialysis.
As of the 2001 census, there were 1,700 residents aged 65 years and older in North Perth.The 2006 census results will confirm that Perth’s senior’s population has grown significantly andis forecast to increase even more rapidly. The aging population means that there will be anincreasing challenge in meeting the needs of people with chronic diseases. Illnesses such ascardiovascular disease, diabetes and arthritis are becoming more prevalent and demands for careare rising.
Consultation with providers in North Perth has identified the need for improved coordinationand management of a variety of chronic diseases, specifically: arthritis, cancer, congestive heartfailure, diabetes, hypertension, respiratory diseases (such as chronic obstructive lung diseasesand asthma), osteoporosis and chronic renal failure.
Program Description
Chronic disease management is a proactive, population-based approach that addresses chronicdiseases early in the disease cycle to prevent disease progression and reduce potential healthcomplications. Multiple strategies are used to improve the health of all patients diagnosed withspecific conditions and, as such, the team concept inherent in Family Health Teams isadvantageous. This approach reduces the subsequent need for acute interventions in the futureand allows people to maintain their independence and remain healthy for as long as possible.The Family Health Team will develop chronic disease management programs that:
• Are evidence-based• Use multiple strategies and interventions• Are patient-centered• Empower individuals to increase control over and improve their health

North Perth Family Health TeamBusiness and Operational Plan 30
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
• Promote collaboration among providers, organizations, individuals, families, andcommunity groups
• Include an evaluation component to ensure that programs are achieving their objectives.
The Family Health Team steering committee recognizes the importance of effectivelymanaging all these chronic diseases and recommends a phased-in approach, with an initialprogram emphasis on Diabetic patients.
Staffing for this program will consist of a Registered Nurse (1.0 FTE); Registered PracticalNurse (1.0 FTE); Dietician (1.0 FTE); Case Manager (0.5 FTE - contracted) and a Pharmacist(0.5 FTE).
Primary Mental Health ServicesThe reform of Ontario’s mental health system has been in process for decades. The most recentstep in this long-standing reform process was the establishment of Regional Mental HealthImplementation Task Forces by the previous Conservative government. These Task Forcesmade extensive recommendations to enhance the capacity of local non-institutional services toprovide more community-based care. These initiatives support the need to ensure that allOntarians have access to a range of mental health services that embrace the following integralcomponents of a comprehensive mental health system: community focus, comprehensive,individualized and flexible, an integrated system, and geographically and culturally relevant.The spectrum of functions that comprise a complete mental health system include:
• Identification• Treatment and Crisis Support• Consultation• Coordination• Residential Support• Case Management• Social Support• Vocational Support• Self-Help/Peer Support• Family Support• Advocacy.
Broad-based prevalence studies suggest that over 2% of the total population in Ontario havesome form of severe mental illness (SMI). Further, it is estimated that only about half of the

North Perth Family Health TeamBusiness and Operational Plan 31
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
SMI group actually access the health system. Considerably more individuals suffer from chronicand less severe mental health problems, often categorized as “mild to moderate mental illness”.The most recent Ontario Health Survey indicates that 18% to 20% of the total population in theprovince reports either a substance abuse or mental health problem. This translates into over5,000 individuals in the North Perth area who would benefit from mental health services andsupports.
Historically, physicians have served as a first point of contact for patients with mental healthneeds but for rural family doctors with large practices, it has been difficult to provide thesepatients with the time and support they require. Accordingly, the North Perth Family HealthTeam will develop a comprehensive primary mental health program in partnership with existingmental health service providers in Perth County.
Mental Health Services in North Perth
There are two Ministry of Health-funded mental health agencies serving North Perth:• Huron-Perth branch of the Canadian Mental Health Association (CMHA); and• Outreach/Outpatient services of the Huron Perth Healthcare Alliance.
The CMHA has one community support worker working with SMI clients in North Perth toensure that there are appropriate resources in place (e.g. income, housing etc.) so that theseindividuals can be integrated into the community. This support worker has established strongworking relationships with the Amish and Mennonite communities. The CMHA also manages asupportive housing unit in Listowel that has three apartments.
The Huron Perth Healthcare Alliance (based at the Stratford hospital) currently provides thefollowing services to all residents of Perth County:
• Inpatient psychiatric unit at the Stratford hospital• Seniors mental health program• Sexual assault program• Psychiatric day/evening program (for individuals that can travel to their Stratford clinic).
The Huron Perth Healthcare Alliance (Stratford hospital) has also been providing outreachmental services to the Listowel area for many years. These services are provided in theoutpatient building across from the Listowel hospital. Currently, there are 2.5 FTE clinicians(social workers) that provide individual, group and family counseling; crisis case managementand community outreach and education. Some of their practice is office-based and for some

North Perth Family Health TeamBusiness and Operational Plan 32
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
clients, they travel to the home to provide services and supports. One of the clinicians worksspecifically with Mennonite and Amish families in which an individual has been diagnosed witha serious mental illness. Outreach services to North Perth also include visits from a Stratfordpsychiatrist (1 day per week) and a psycho geriatrician (1 day per week).
There are a number of unmet mental health needs in North Perth that require priorityconsideration and additional resources:
• Services for patients with primary/secondary prevention of mental health problems (i.e.without timely intervention, mild to moderate mental health problems can become SMIoften requiring hospitalization)
• Services for elderly patients who have mental health problems• Services for victims of sexual abuse (both male and female victims).
Program Description
The North Perth Family Health Team will work in partnership with Outpatient Mental HealthServices and the Huron-Perth Branch of the Canadian Mental Health Association to meet theneeds of the community and to ensure that there is no duplication of current services. NorthPerth Family Health Team’s primary mental health program will employ the same screeningmethods and direct services to individuals who suffer from mild to moderate mental illness,thereby addressing a significant unmet need in the community. Together with the primary carephysicians, the FHT’s new mental health professionals will work towards reducing the negativeimpact of mental illness and improving the health functioning of persons who experience a widerange of mental health disorders. The NPFHT will provide the following mental health services:
• Early identification, assessment and screening• Conduct bio-psycho-social assessments• Prepare a recommended plan of intervention and treatment• Share the assessment and plan with the primary care physician for review and
modification.• Implement agreed upon recommendations• Ongoing review of medications and adjustments as required• Provide case coordination and linkages with other services• Primary and secondary prevention, and public education.
To provide these services the NPFHT requires two Social Workers (1.0 FTE –psychogeriatrics; 1.0 FTE – adults with moderate mental illness) a part-time Registered Nurse

North Perth Family Health TeamBusiness and Operational Plan 33
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
(0.5 FTE) and psychiatric and psycho-geriatric consultation services provided by medicalspecialists.
Linkages/Partnerships
Both the CMHA and the Huron Perth Healthcare Alliance have indicated their strong support forpartnering with the North Perth Family Health Team to provide the services described above.
Substance Abuse (Adolescents and Young Adults)The only Ministry of Health-funded addictions treatment agency serving Perth County is Choicesfor Change. This organization provides assessment, referral and community counselling forindividuals impacted by their own or someone else’s substance use/abuse and problem gamblingfor persons age 12 and over. Their head office is in Stratford but they do have satellite officespace in Listowel.
According to statistics provided by Choices for Change, substance abuse among teenagersand young adults continues to escalate, in part because of the now well-documented crystal meth.problem.3 "Crystal Meth" (methamphetamine) is a designer amphetamine that simulatesdopamine and norepinephrine. Patients are at risk for hyperthermia, hypertensive emergencies,dysrhythmias, myocardial ischemia, and hyperkalemia associated with rhabdomyolysis. Patientsbecome paranoid, hyperalert, agitated and exhibit very bizarre delusional and/or violentbehavior. According to Choices for Change, crystal meth now accounts for approximately 20%of agency admissions.
Top five 2005-06 admissions to the Choices for Change program from North Perth are listedbelow for adults and youth (up to age 18):
Substance Abuse Problem Adults Youth
Alcohol 64 22
Cannabis 28 28
Methamphetamine 27 12
3 Starting in 2005, Perth County was identified as “Ontario’s Crystal Meth Capital” following busts of 11 separatedrug labs in the area (Source: Society for Rural Physicians of Canada, The Rural News, Vol. #7, Issue #23, October28, 2005).
North Perth Family Health TeamBusiness and Operational Plan 34
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Cocaine 24 6
Crack 9 -
Ecstasy - 7
There are several resources available to deal with this growing list of substance abuseproblems. Choices for Change has one youth worker who visits the local high school one dayper week. There is also an addictions counselor who provides services to adult clients three daysper week. This level of service is inadequate to deal with the prevalence of substance abuseproblems in the North Perth area.
Program Description
The North Perth Family Health Team will partner with Choices for Change to provide anenhanced addictions treatment service for adolescents and young adults with substance abuseproblems. The FHT program will consist of two key components:
• Assessment: A process of mutual investigation or exploration that provides the clinicianwith more detailed information for the purpose of determining specific client needs,goals, characteristics, problems and/or stage of change. Based on the informationgathered, a treatment plan is developed.
• Community Counseling. Includes brief intervention, lifestyle and personal counsellingto assist the client to develop skills to manage substance abuse problems, and/or maintainand enhance treatment goals.! A variety of modalities will be utilized such as CognitiveBehaviour Counselling, Social Learning, Narrative Therapy etc. !
The NPDFHT is requesting funding for a Youth Addictions Counselor (1.0 FTE) to developthis program.
Linkages/Partnerships
Choices for Change has indicated that it will partner with the North Perth Family Health Team toprovide the services described above.
Health Promotion and Disease PreventionThe health and wellness of individuals is determined by a number of factors including biologyand genetic endowment, the physical environment, living and working conditions, personalhealth practices and coping skills, and health services. Many of these determinants of health are

North Perth Family Health TeamBusiness and Operational Plan 35
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
beyond the control of the North Perth Family Health Team and it would not be reasonable toexpect the Family Health Team to be able to make an impact in all of these areas. However, it isreasonable to expect the Family Health Team to partner with its patients and staff of the PerthDistrict Health Unit to assume responsibility for addressing the broad determinants of healththrough advocacy, coalition building, and a broad range of protection, promotion and preventionactivities.
Programs to promote health, prevent illness and to assist the general population to makehealthy lifestyle choices are needed in every service sector. Too often, these types of preventiveinitiatives take a back seat to direct care and treatment. The Family Health Team’s holistic,wellness-oriented program spectrum will be able to make a significant contribution to thisimportant need.
The Perth District Health Unit has a satellite office in Listowel with 6.5 FTE health unit staffserving the North Perth area providing the following range of services. One of the staff membersis allocated specifically to work with the Amish/Mennonite families in the area.
PromotingHealthy LifestyleChoices
Preventing Injuryand Disease
Protecting Indivdualsand Families
Health Eating Alcohol and SubstanceAbuse Prevention
Communicable DiseaseInvestigation andOutbreak Control
Parenting Cancer PreventionFood Safety
Physical Activity Child SafetyPublic HealthEmergency Response
Pregnancy Support Immunization Rabies Investigation
Stop SmokingSupport
West Nile VirusMonitoring
Safe Drinking WaterMeasures
WorkplaceWellness Program
School-based Programs
Smoke-free PublicPlaces

North Perth Family Health TeamBusiness and Operational Plan 36
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Program Description
The North Perth Family Health Team will design and deliver wellness-oriented, healthpromotion and prevention services as part of all program/services offered through the FamilyHealth Team. These initiatives will be undertaken in partnership with existing public healthprograms to ensure ready access to a broad range of prevention/promotion strategies that willinclude:
• Individualized risk assessment and counseling, re: reproductive, maternal, child andfamily health
• Well-baby visits and childhood immunization• A broad range of screening initiatives i.e. breast, cancer etc.• Prevention of communicable diseases, e.g. flu shots• Chronic disease prevention (therapeutic counseling addressing specific diseases and
illnesses i.e. diabetes, heart disease, obesity)• Smoking Cessation• Programs for at-risk individuals and groups• Alcohol and drug abuse• Sexually transmitted diseases• Skills development education sessions to small groups, and group support programs in
response to local needs (e.g. postpartum depression)• Stress reduction.
It is expected that the FHT will complement outreach programs services offered by thePDHU through mandatory programs and Early Child Development initiatives.
Through this wellness program, the NPFHT will also develop special prevention andpromotion strategies for the Anabaptist communities, which have special service deliverychallenges. This will require the skills of a Health Educator with broad-based communityexperience since some services will need to be provided through home visits and remoteoutreach sites but still integrated with existing programs.
Because the Anabaptist communities have higher rates of congenital anomalies, there is apressing need for better genetic screening and counseling. In addition to the nursing servicesoffered through the FHT’s ‘Health Promotion and Disease Prevention’ program, the FHT willalso require regular consultations from paediatricians in Stratford. Because of the special healthneeds of the Amish and Mennonite communities, there is an opportunity for the North Perth FHT

North Perth Family Health TeamBusiness and Operational Plan 37
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
to collaborate with the Stratford and Perth Family Health Teams through a strong workingrelationship with the Perth District Health Unit.
Staffing requirements for this program include a Registered Nurse (1.0 FTE); HealthEducator (1.0 FTE - contracted) and paediatric consultations for Amish/Mennonite families.
Linkages/Partnerships
The Perth District Health Unit has indicated strong support for partnering with the North PerthFamily Health Team to provide the services described above.
Case Management and System NavigationWith the increasing number of health programs planned for North Perth and the increasingcomplexity of the health care system, there is a need for enhanced system navigation and casemanagement services to assist patients and their families to access current and new services.Patients with complex, chronic health problems will require linkages and referrals to multipleagencies and services to ensure that their care is coordinated and monitored on an ongoing basis.The Ministry of Health and Long-Term Care has identified “system navigation” as a top prioritywithin the program structure of the fourteen new Community Care Access Centres acrossOntario. Case management services are required both at the individual discipline level andacross the entire health service system. Most current programs provide a measure of casemanagement within their specific discipline. Broader system navigation services have beenembraced by Perth Community Care Access Centre where workers have developed casemanagement skills that cut across all disciplines, given their broad range of responsibilities andpartnerships with multiple providers throughout the community. The range of services providedby the Perth County CCAC includes:
• Personal Support• Nursing care• Occupational Therapy• Physiotherapy• Social services• Speech Therapy• Nutritional counseling• Case Management• Placement Coordination.

North Perth Family Health TeamBusiness and Operational Plan 38
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Program Description
The North Perth Family Health Team will contract with Community Care Access Centre toprovide in-house case management/system navigation services, recognizing the need to have anexperienced case management worker at the Family Health Team well linked to all communitypartners. The Community Care Access Centre through its ongoing referral program hasdeveloped strong working relationships with all existing components of the service spectrum.The CCAC is knowledgeable of changes in the system, has an ongoing inventory of information,and a standing relationship with the community partners that will be serving the Family HealthTeam members. In addition, CCAC will develop a comprehensive database, enabling them toprovide the Family Health Team with specific information about clients and their progressthrough the system. Generally, case managers or “system navigators” have a degree in aregulated health profession, often a nurse or therapist. The case manager with the Family HealthTeam may, subject to workload, be able to perform home visits for the purpose of establishingthe initial needs, with other professionals from the CCAC following up.
Staffing required for this program will include a Registered Practical Nurse (1.0 FTE) and aCase Manager (0.5 FTE) who will be contracted from the CCAC.
Linkages/Partnerships
The Perth CCAC has indicated strong support for partnering with the North Perth Family HealthTeam to provide the services described above.
Rehab ServicesWith the announcement of a Family Health Team for North Perth, rehab professionals in the areaapproached the FHT steering committee to ask if they could strike a time-limited sub-committee,which could provide input about local rehab needs. With the support of the steering committee,the rehab sub-committee met on several occasions in May and June 2006 (Appendix 9) in orderto accomplish the following:
• Prepare an up to date inventory of local rehab services• Compile rehab services statistics from different providers• Identify local gaps in rehab services• Identify opportunities for greater collaboration and integration.
Like many rural areas, North Perth suffers from a shortage of rehab professionals. Withrespect to physiotherapy, there are long waiting lists at the Hospital for outpatient physio for both

North Perth Family Health TeamBusiness and Operational Plan 39
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
adults and children. Priority is given to more acute cases so chronic patients have to wait longer.There is a private physiotherapy provider in North Perth (New Horizons Rehab) but many localresidents do not have private insurance coverage and so depend on publicly funded services.There are an increasing number of patients (e.g. stroke patients, patients with joint replacementsetc.) whose successful recovery depends on accessible rehab services.
In terms of occupational therapy, the situation is even more critical because of the lack oflocal therapists. There is notable service gap between what the CCAC can offer and what isneeded. Pediatric coverage is poor and only allows for one treatment every six weeks. School-age children and mild cases have almost no coverage for occupational therapy and autisticchildren do not receive services.
It is estimated that 10% of the preschool population have speech problems. Inpatients havepriority in terms of service. School-aged children often have to wait and often the number ofvisits is limited. There are two distinct groups of childhood cases: (1) children with languagedelays; (2) children with motor-related speech problems and both are underserviced, especiallycompared to what they receive through the pre-school speech initiative (Small Talk).
While there are unmet local needs in all three therapies, the Rehab Subcommitteerecommends that, if additional rehab can be offered through the Family Health Team,occupational therapy services should be enhanced as a first priority.
Program Description
In terms of geriatric FHT clients, the enhanced OT program offered through the FHT will beable to offer to patients following hospital discharge, services such as: hand-splinting, strokerecovery and education. The enhanced staffing will also allow the FHT to explore thedevelopment of a new vascular health clinic. Finally, the FHT may also be able to collaboratewith the CCAC to provide additional home follow-up to help with “activities of daily living”.
The NPFHT is requesting a part-time occupational therapist (0.5 FTE) with the expectationthat this position would commence in Year 2.
Linkages/Partnerships
The creation of the time-limited rehab sub-committee has already spawned a number of newopportunities for multi-disciplinary collaboration and integration, which the FHT will continue to

North Perth Family Health TeamBusiness and Operational Plan 40
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
explore and support as it becomes operational. In terms of possible ‘early wins’, the followinginitiatives are already under discussion:
• Implement the current electronic medical record system (developed by the physicians) tolocal rehab professionals so that rehab services are better linked to other hospital andmedical services
• Increase the use of local chiropractors in the assessment, diagnosis (incl. x-rays) andtreatment of FHT patients with arthritis and related conditions
• Work with local industry to develop strategies to address the large number of workplaceinjuries, which produce high costs for both the private sector and the health care industry.
Summary of Staffing RequirementsIn the previous section of this Business Plan, each program has been described and the humanresource requirements for each program have been set out. The chart below summarizes thehuman resource requirements of each program and indicates the total number of allied healthprofessionals required by the NPFHT. The FHT is requesting funding for 16 FTE allied healthprofessionals.
Program NP RN RPN SocialWorker
YouthCounselor
Dietician Pharmacist HealthEducator
CaseManager
OT
Primary Care –Orphan Patients
2 1 1 0.5
Chronic DiseaseManagement
1.5 2 1 0.5 0.5
Primary MentalHealth Service
2
Youth SubstanceAbuse
1
Health Promotion 0.5 1CaseManagement
0.5 0.5
Rehab Services 0.5Total Number of
allied healthprofessionals
2.0 3.5 3.0 2.0 1.0 1.0 1.0 1.0 1.0 0.5
Linkages and PartnershipsThe North Perth Family Health Team has developed a strategy that will build on existinglinkages and partnerships with current providers of primary care services in the community. Insome cases, the NPFHT will contract with these agencies to provide primary care services. TheFHT practitioners will carry out their primary health care function in partnership with a numberof successful programs that are currently operating. These programs are accessible to the entire

North Perth Family Health TeamBusiness and Operational Plan 41
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
community and the Family Health Team’s entry into these areas will be of a supplementary andcomplementary nature.
Human ResourcesThe roles and qualifications of allied health professionals referred to in this Business Plan are setout in the preliminary job descriptions e included in Appendix 12 . These job descriptions arebased on those currently used by the Listowel Memorial Hospital and job descriptions that havebeen developed by other Family Health Teams.
Recruitment Plan
The Listowel Memorial Hospital will provide human resource management assistance to theNPFHT on a contract basis. The Human Resource Department of the Hospital will assist theFHT management team in the following activities:
• Development of advertisements for these positions• Assisting in the finalization of job descriptions• Confirming salary and benefit arrangements• Confirming employment arrangements• Receiving and screening job applications• Short-listing qualified candidates• Developing selection criteria and interview questions• Assisting senior management in interviewing preferred candidates• Production of letters of offer to selected candidates• Arranging for orientation for new employees• Documentation of new employees for compensation, employee benefits, pension, etc.
The Hospital Human Resource Department currently provides these services for all Hospitalemployees and is familiar with industry requirements for the recruitment of employees.
Compensation of Allied Health Professionals
Allied health professionals will be compensated on a salary basis using the guidelines providedby the Ministry of Health. In some cases, it may be necessary to use hospital industry salarylevels that have been negotiated with the union which represent various health care professionals.Benefits for these professionals will be based on 20% of salary.

North Perth Family Health TeamBusiness and Operational Plan 42
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Compensation of Physicians
All of the family physicians in Listowel are currently members of the Listowel FHN and theywill continue to be compensated on a blended payment mechanism as members of the FHT.Some specialist physicians will be compensated on sessional basis.
Collaborative Team PracticeThe North Perth FHT is in the process of developing a collaborative practice model that will beused to guide the ongoing development of the FHT as physicians and allied health professionalswork together to meet the needs of their patients. A Patient Care Council will be created toprovide a forum for the ongoing identification and resolution of issues and problems related todevelopment of the collaborative practice model. Each member of the FHT will be representedon the Patient Care Council, which will meet monthly. Minutes of meetings will be circulated toall members of the FHT. To assist in the coordination, communication and resolution ofprofessional practice issues, a Collaborative Practice Leader will be appointed to assist in theongoing development of the Collaborative Practice Model employed by the NPFHT.
The collaborative practice model that will be adopted by the NPFHT will be based on thehealth care literature and models that have been developed in other teams. Some of the keyprinciples that will be considered in developing the patient care model will include:
• Respect for the scope of practice as defined by each of the regulated health professionalsgoverning bodies.
• A commitment to work together with mutual respect for the qualifications of eachmember and to clarify areas of conflict or disagreement in a mutually agreeable manner.
• Open communication will be critical to the ongoing success of the FHT and each memberof the team will ensure that issues are identified and referred to the Professional PracticeCouncil for discussion and resolution.
• Standards of practice for each health professional group will be circulated to all membersof the team.
• Protocols will be developed for all patient care programs and services that set out theagreed treatment practices for the care of patients and the role of each health discipline.
• Job descriptions setting out the roles and responsibilities of each health professionalgroup will be developed and circulated to each member of the allied health team.
• Education programs will be developed that focus on collaborative practice issues andthese sessions will be held on a quarterly basis for all members of the FHT.

North Perth Family Health TeamBusiness and Operational Plan 43
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
• Each health professional will be responsible for reporting any differences of opinion orconflicts that may arise regarding issues of collaborative practice to the CollaborativePractice Leader.
• Each member of the FHT will be expected to consult with other members of the FHTincluding the patients family physician regarding any issues that are beyond the scope ofpractice of his/her regulated profession.
• Monthly case conferences will be held with appropriate members of the FHT to reviewthe progress of patients.
• Guidelines for collaboration will be developed for each patient care program and theseguidelines will be reviewed and revised on an annual basis.
• All members of the FHT will participate in quarterly education sessions that focus on theongoing development of a collaborative practice model and the clarification of any issuesthat may arise and problems that may occur.
• All members of the allied health team will be expected to participate in collaborativepractice education sessions offered by their professional association and other educationalinstitutions.
• Guidelines will be developed that set out the procedures for requesting consultations fromother allied health professionals, the circumstance when consultations must be requested,diseases and disorders that must be referred to another allied health professional,documentation of the request for consultation and documentation of the results of theconsultation.
• Patient communication programs will be developed for all patient programs and servicesthat ensure that patients clearly understand the roles and responsibilities of the membersof their treatment team.
• An ongoing quality assurance program will be developed to include annualenvironmental scans, data collection, patient surveys, chart audits, team member programreviews and team member peer reviews.
The Role of the Nurse Practitioner in the Family Health Team
Family practitioners and the nurse practitioners can work autonomously as the first point of entryfor the Family Health Team, performing triage and delivering a broad range of primary careservices. However, the expectation of the North Perth Family Health Team is that new NursePractitioners will initially work closely with the family doctors so that strong clinicalrelationships can be built. Nurse practitioners, while providing primary care and responding to

North Perth Family Health TeamBusiness and Operational Plan 44
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
acute care needs, will also provide illness prevention and health promotion services. Nursepractitioners will provide a wide range of patient care services including:
• Administering/monitoring therapeutic interventions and regimens• Assessment of health indicators/needs, self-care empowerment, education and support• Management of client health/illness status• Identifying acute/chronic disease• Recommending diagnostic/therapeutic interventions• Reassessment and management of client’s needs• Providing emotional/informational support to clients and families• Ongoing assessment, monitoring and management of client care• Providing follow-up care to monitor patient progress.
Collaboration and consultation are critical themes that characterize all elements of nursepractitioner care.
Educational Programs
To ensure that this collaborative practice model is successfully implemented, it will be importantto provide continuing education programs and services for the FHT staff on an ongoing basis.Funding has been requested to provide ongoing education programs for all FHT to ensure thatinterdisciplinary team care is provided in the most effective and efficient manner.
Extended HoursFamily physicians in the Listowel Family Health Network currently provide emergency coveragefor the Hospital and are exempt from providing after-hours services in their offices. Whenadditional family physicians and nurse practitioners are recruited as part of the family healthteam, there is the potential that a plan for providing after-hours coverage for patients duringevenings and on weekends at the medical clinic may be considered.
Other ProgramsIn this section, a number of other programs that will be available to FHT patients are described.
Laboratory and Radiology Services
The Listowel Memorial Hospital provides a full range of laboratory and diagnostic imagingservices for patients on both an inpatient and outpatient basis. These services will be available to

North Perth Family Health TeamBusiness and Operational Plan 45
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
all patients enrolled in the NPFHT. A private specimen collection station is also located withinthe Medical clinic and this would be available for a FHT patients.
Pulmonary Function Testing
The Listowel Memorial Hospital provides pulmonary function testing, EKG and other diagnosticservices for both inpatients and outpatients. All of these services will be available forpatients enrolled with the NPFHT.
Day Surgery Services
The Listowel Memorial Hospital provides a full range of day surgery services for ambulatorycare patients. These services will be available to all members of the NPFHT.
Medical Specialists
The Listowel Memorial Hospital has access to a full range of medical and surgical specialists.Family physicians within the NPFHT will continue to refer patients to these medical and surgicalspecialists when appropriate. To assist in selected programs, the NPFHT has requested fundingfor stipends and travel expenses for a paediatrician, geriatrician and a child psychiatrist to workwith the family physicians and other allied health team members.
Evaluation MechanismsEvaluation of the effectiveness and efficiency of the programs and services that will be providedby the NPFHT will be critical to ensure that the FHT meets its objectives. The NPFHT willdevelop an evaluation framework for measuring the effectiveness and efficiency of programs andservices provided by the FHT. The evaluation framework will include:
• Patient satisfaction surveys• Provider satisfaction surveys• Level of collaboration• Management of health conditions• Changes in access to care• Achievement of program objectives• External evaluation of governance and management structure.
A detailed Workplan for the evaluation process will be developed as part of the programimplementation process, after new FHT professionals are hired. Data will be collected regardingeach program in order to measure the success of the various programs and services in meeting
North Perth Family Health TeamBusiness and Operational Plan 46
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
their objectives. Because the Listowel FHN already has an electronic medical record system, acomputer programmer will work with Team members to develop customized reports for eachFHT program which will include:
• Number of patients seen• Disease incidence/prevalence estimates• Services used• Wait times• Clinical outcomes.
Based on the primary care programs and services that are proposed for the NPFHT, a numberof expected patient outcomes have been identified but will need to be refined as the Ministrydevelops its reporting templates. The NPFHT will monitor these patient outcomes during thedevelopment of the FHT and will report to the Ministry on these outcomes.
Consolidated Timelines for ImplementationDuring the first eighteen months of operation, the NPFHT will focus on the recruitment of alliedhealth professionals, the recruitment of family physicians, the enrollment of patients and theestablishment of expanded programs. A detailed implementation plan will be developed settingout the activities and timing for each activity when the Ministry of Health has approved thisBusiness Plan.
The first year of operation will also focus on the creation of a new, non-profit Board togovern the FHT and the development of a management structure to provide daily management ofthe FHT as new staff are hired and new programs are prepared. Within six months ofcommencing operation, the FHT will also begin the planning process for the preparation of adetailed operating budget for the second year of operation of the FHT. With a new FHT Boardin place, a new Community Advisory Committee and new staff, the preparation of the OperatingPlan for the second year of operation of the FHT will be more complex and more timeconsuming.
Physical FacilitiesThe Listowel Medical Clinic is out of date and requires expansion and upgrading to meet theneeds of current family physicians. With plans to recruit additional family physicians and to adda number of other allied health professionals to the primary care team, there is a need forexpanded facilities to accommodate these additional staff.

North Perth Family Health TeamBusiness and Operational Plan 47
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
A Facilities Design sub-committee of the FHT steering committee has been established toassess a number of options for the redevelopment of the Medical Clinic. The options that arebeing considered include the following:
• Option 1 – Renovate the existing medical clinic, with an addition to the clinic eitherhorizontally or as a second floor or both.
• Option 2 – Demolish the current clinic and construct a new building on a new site.• Option 3- Renovate both the clinic and the Hospital outpatient building to meet the needs
of the NPFHT.
The services of an architect and facilities planner have been engaged to review these optionsand to prepare cost estimates. In addition, the committee is considering how such a projectmight be funded and governed and the role that the Municipality, the Hospital, the familyphysicians and others may play in the redevelopment of these facilities. A business plan is beingprepared that will set out both the capital cost requirements as well as the funding andgovernance factors that must be considered as part of this project. When the business plan iscomplete, it will be submitted to the Ministry of Health for consideration.
The Ministry of Health has indicated that it is prepared to assist in the funding of capitalprojects related to the creation of FHTs. The NPFHT will present a plan to the Ministry for itsconsideration.
Information TechnologyUnlike most other Family Health Teams, the Listowel FHN has already implemented a sharedelectronic medical record with the Listowel Memorial Hospital. The Listowel FHN physicianshave developed and refined their electronic medical record (EMR) system over many years usingthe resources of Purkinje systems. Recently, OntarioMD has provided funding to the FHN forthe ongoing operation of this system and the expansion of this system to include all familyphysicians.
The next stage of development of this EMR system has two components:• Allow other allied health professionals in North Perth to access the system (referred to as
the ‘community roll-out’)• Allow new members of the FHT to access the system.
The NPFHT believes that the ‘roll-out’ of the EMR to other allied health professionals wouldbe an enormous improvement in patient care. In particular, access to an updated patient profile,

North Perth Family Health TeamBusiness and Operational Plan 48
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
medication list, and test results would benefit all allied health professionals. It is recognized thateach caregiver may have different needs; for example, local chiropractors would find access to amedication list useful as well as access to x-ray reports. Nursing homes would appreciate accessto Emergency reports and discharge summaries when their residents are treated at the Hospital.The FHT steering committee created a time-limited focus group to discuss the EMR ‘communityroll-out’ and there was widespread support among local health care professionals (Appendix 10).
Expanding access to the current EMR will require modifications to the current systemsoftware to ensure that there is adequate confidentiality within the system and there areappropriate IT interfaces with computer networks used by other health care professionals. Acomputer programmer is required to make these IT changes. This individual will work with theresources of OntarioMD and there would not be a duplication of effort in undertaking this task.The Listowel Hospital currently has an IT resource person but additional staffing resources willbe required in conjunction with the Hospital IT staff to perform this work. Additionalprogramming work will also be required to develop customized EMR reports that monitor theutilization and outcomes of the programs and services offered by the NPFHT (discussed in moredetail under ‘Evaluation Mechanisms’).
In addition, access to secure e-mail for all North Perth health professionals and caregivershas been identified as a key communication tool that will improve the coordination of patientcare. Patients of the NPFHT would be the first to benefit from this system, but as more patientsare enrolled and as more health professionals and community health agencies participate in thesystem, it is envisioned that the entire North Perth community would eventually be includedwithin the system. Ultimately, the goal is to create a community health record for all North Perthresidents that links all caregivers and health care organizations.
In addition to the computer programming requirements, the FHT steering committee hasidentified privacy of patient records as a key EMR implementation issue. Even though writtenconsent may not be necessary from a strict interpretation of current federal and provincial healthinformation/privacy legislation, the steering committee believes that expanded use of the EMRsystem will require some type of overt consent to ensure that patients are comfortable with anexpanded use of a shared health record. Initial Family Health Team education at inception of theteam about appropriate levels of access to the EMR plus some patient education at the time ofenrollment are both seen as necessary steps to address these privacy issues. Even though healthcare professionals already use several different patient consent forms which allows them to sharepatient information, a new consent mechanism may need to be developed for patients who have

North Perth Family Health TeamBusiness and Operational Plan 49
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
information placed in the system that they want to keep confidential from other caregivers (e.g.visit to a sexual health clinic).
To address this issue, the FHT will establish a Privacy Committee to examine the potentialproblems and solutions related to these privacy concerns. The implementation of an expandedsystem will be undertaken on a phased basis so that these issues can be dealt with in a timelymanner. For example, the provision of secure e-mail would be immediately beneficial to manyhealth professionals and would be part of a first phase of implementation. Also, the roll-out ofthe EMR to solo health care professionals (e.g. chiropractors, dentists, optometrists etc.) isscheduled as part of Phase 1 implementation (Appendix 10) since designing the interfacebetween these solo practices and the current EMR system will be more straightforward thanconnecting to larger health care organizations (e.g. CCAC) that already have more complex ITsystems in place.
Annual BudgetIn Appendix 11, a detailed operating budget has been prepared in accordance with Ministryguidelines using Schedules 1, 2, 3, 4 and 5. Operating costs for the first seven months of theyear are estimated as follows:
• Human Resource costs are estimated at $960,532• Operating expenses are estimated at $173,833• One-time start-up costs are estimated at $174,200.
We look forward to meeting with the Ministry of Health to answer any questions regardingthis Business and Operational Plan for the North Perth Family Health Team.
––––––––––––––––––––––––––––––––––––––––––––

North Perth Family Health TeamBusiness and Operational Plan 50
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
APPENDIX 1
Current and Projected Catchment Area Population forListowel Memorial Hospital
AgeGroup 2003 2008
%Change2003-2008 2013
%Change2008-2013 2017
%Change2013-2017
0-14 5,474 4,866 -11.1% 4,634 -4.8% 4,866 5.0%15-19 2,232 2,100 -5.9% 1,909 -9.1% 1,449 -24.1%20-44 9,125 9,243 1.3% 9,542 3.2% 9,907 3.8%45-65 5,941 6,636 11.7% 6,807 2.6% 6,709 -1.4%65-74 1,841 1,937 5.2% 2,193 13.2% 2,407 9.8%75-84 1,233 1,254 1.7% 1,309 4.4% 1,344 2.7%85+ 494 575 16.4% 601 4.5% 653 8.7%Total 26,340 26,611 1.0% 26,995 1.4% 27,335 1.3%
Source: Master Plan, Listowel Memorial Hospital, 2003
Municipal Populations Contributing to Catchment Area Populationfor North Perth Family Health Team
NorthPerth
Howick HuronEast
Mapleton Minto Wellesley Woolwich
Population in 2001 12,055 3,779 9,680 9,303 8,164 9,365 18,201
Population in 1996 11,808 3,685 9,937 8,827 7,854 8,664 17,325
1996-2001 pop. change (**) 2.1% 2.6% -2.6% 5.4% 3.9% 8.1% 5.1%
Pop. density per square km. 24.4 13.1 14.5 17.4 27.2 33.7 55.8
Land area (square km) 493.2 287.4 669.2 534.7 300.4 277.9 326.0
Source: Statistics Canada, www.statscan.ca
**Average population growth (1996-2001) across 7 municipalities = 3.6%

North Perth Family Health TeamBusiness and Operational Plan 51
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
APPENDIX 2
Population and Dwelling Counts North PerthTotal
OntarioTotal
Population in 2001 12,055 11,410,046Population in 1996 11,808 10,753,5731996 to 2001 population change (%) 2.1 6.1Total private dwellings 4,529 4,556,240Population density per square km. 24.4 12.6
Land area (square km) 493.18 907,655.5
North Perth OntarioAge Characteristics Total Male Female Total Male FemaleTotal - All persons 12,055 5,925 6,130 11,410,050 5,577,055 5,832,990Age 0-4 730 385 350 671,250 343,340 327,905Age 5-14 1,815 915 900 1,561,500 801,355 760,145Age 15-19 1,035 535 495 769,420 394,915 374,500Age 20-24 825 395 430 718,420 359,645 358,775Age 25-44 3,205 1,605 1,600 3,518,010 1,724,535 1,794,480Age 45-54 1,545 790 760 1,635,280 801,540 833,740
Age 55-64 1,100 550 550 1,064,000 520,565 543,430Age 65-74 945 440 510 818,165 383,625 434,545Age 75-84 655 260 400 503,930 202,265 301,665Age 85 and over 190 50 140 150,075 45,260 104,810Median age of thepopulation 36.6 35.4 37.5 37.2 36.4 38.0% of the populationages 15 and over 78.9 78.1 79.6 80.4 79.5 81.3
North Perth OntarioEarnings in 2000 Total Male Female Total Male FemaleAll persons with earnings(counts) 6,970 3,710 3,260 6,319,535 3,311,105 3,008,425Average earnings (all personswith earnings ($)) 27,141 33,300 20,127 35,185 42,719 26,894Worked full year; full time(counts) 4,155 2,535 1,620 3,527,045 2,061,355 1,465,690Average earnings (worked fullyear; full time ($)) 35,047 40,377 26,700 47,299 53,937 37,962Median family income ($)- allcensus families 57,442 61,024Median family income ($)-couple families 60,611 66,476

North Perth Family Health TeamBusiness and Operational Plan 52
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Median family income ($) –lone-parent families 34,642 33,724
North Perth OntarioHighest Level of Schooling Total Male Female Total Male Female% of population aged 20-34 withless than a high schoolgraduation certificate 20.0 19.9 20.0 13.2 14.9 11.0% of population aged 35-44 withless than a high schoolgraduation certificate 23.9 27.6 20.5 17.3 18.8 16.0% of population aged 45-64 withless than a high schoolgraduation certificate 39.1 42.3 35.1 27.5 26.5 28.0
North Perth OntarioOccupation Total Male Female Total Male FemaleTotal labour force 6,730 5,992,765Agriculture and other resource-based industries 1,190 191,020Manufacturing and constructionindustries 1,910 1,316,580Wholesale and retail trade 1,125 950,730Finance and real estate 290 401,445Health and education 775 902,990Business services 705 1,145,910
Income in 2000North Perth
TotalOntario
TotalPersons 15 years of age and over with income 9,140 8,598,560Median total income of persons 15 years of age and over ($) 22,688 24,816Composition of total income (100%) 100.0 100.0
Earnings - % of income 75.7 78.7
Government transfers - % of income 12.1 9.8
Other money - % of income 12.2 11.5

North Perth Family Health TeamBusiness and Operational Plan 53
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
APPENDIX 3
Amish and Mennonite Communities in North Perth and East Perth
CulturalCommunity
Population Families Location(townships)
HealthInsurance?
Sources ofHealth Care
Old Order Amish 931 150 Mornington,Elma, NortheastHope
Most havehealth card
Chiropractors,Osteopaths,Homeopaths,Naturopaths,Midwives,MassageTherapists,Physicians
Old Order Mennonite 350 64 Mornington,Perth East
Do not useOHIP
Chiropractors first,then Physicians;Use of Midwivesfor hospital births
Amish Mennonite 338 58 Mornington,Elma, Ellice
75% havehealth card
Primarily usePhysicians withsome use ofChiropractors,MassageTherapists,Midwives
Conservative/MarkhamMennonite
870 145 Mornington,Wallace
Conservative –80% havehealth card;Markham –50%
Physicians,Chiropractors
Church of God in ChristMennonite
250 50 Mornington,Wallace,Blanshard,Fullarton
100% havehealth card
Primarily usePhysicians, withsome use ofChiropractors,Midwives
David Martin Mennonite 150 25 Mornington,Wellesley (nearLinwood)
100% havehealth card
Physicians,Chiropractors,Midwives
Low German SpeakingMennonites fromMexico
300 50 Mornington (buta more transientgroup)
Most havehealth card(once theyreceive landedimmigrantstatus)
Physicians,Chiropractors,Midwives
Totals: 3,189 542
Source: “A Descriptive Profile of Amish and Mennonite Communities in Perth County”, Perth District Health Unit,October 2002

North Perth Family Health TeamBusiness and Operational Plan 54
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
APPENDIX 4Age standardized mortality rates4 for total mortality (all causes of death) are listed below for theGrey Bruce Huron Perth district compared to the Thames Valley district and the Province ofOntario. The key finding is that age standardized mortality rates for residents of Grey BruceHuron Perth counties are significantly higher5 than Ontario and also higher than the ThamesValley planning area (including London). Within the 4-county district, Perth County has thelowest age standardized rate for total mortality.
Potential Years of Life Lost (PYLL)The potential years of life lost (PYLL) is a calculation of the years of life “lost” when a persondies from any cause before the age of 75 years6. In other words, PYLL represents the amount ofpremature death in any given population before age 75 years. The amount of premature deathamong residents of the Grey Bruce Huron Perth area is significantly higher than the ThamesValley planning area and the Province of Ontario.
Age Standardized Potential Years of Life Lost (PYLL) /100,000 Population Aged 0-74
Years, All Causes, GBHP, Thames Valley and Ontario, 1995-97
5,502.5
5,179.4
5,090.2
4,7004,8004,9005,0005,1005,2005,3005,4005,5005,6005,7005,8005,900
All Causes of Death
PY
LL
/100
,000
Po
pu
lati
on
GBHP
TV
Ontario
Source: Statistics Canada, Vital Statistics, Death Database and Demography Division(population estimates), 2003
4 Age standardized rates involve a set of mathematical techniques used to remove, as much as possible, the effects ofdifferences in age and other confounding variables when comparing two or more populations.5 To determine whether differences are of statistical significance (i.e. the difference is not due solely to randomerror), 95% confidence intervals were examined for overlap.6 PYLL – The age of 75 years was used since it is closest to the current life expectancy at birth as well as being theaccepted standard method for calculating this indicator

North Perth Family Health TeamBusiness and Operational Plan 55
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
APPENDIX 5
Results of Canadian Community Health Survey for Perth County
Leisure-time physical activity, by sex, household population aged 12 and over, Canada,provinces, territories, health regions and peer groups, 2000/01
Total Physically activeModerately
activePhysically inactive
Physical activity,not statedLeisure-time
physical activityNumber Number % Number % Number % Number %
Perth Health Unit(Peer group G)
62,847 8,688 13.8 12,522 19.9 38,229 60.8 3,407 5.4
Males 31,075 4,238 13.6 6,318 20.3 17,926 57.7 2,594 8.3
Females 31,771 4,451 14.0 6,204 19.5 20,303 63.9 na na
Ontario 9,877,292 2,101,583 21.3 2,104,850 21.3 4,918,534 49.8 752,324 7.6
Males 4,846,436 1,163,856 24.0 1,018,854 21.0 2,172,826 44.8 490,900 10.1
Females 5,030,856 937,728 18.6 1,085,996 21.6 2,745,708 54.6 261,424 5.2

North Perth Family Health TeamBusiness and Operational Plan 56
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
APPENDIX 6
Most Common Admissions to the Listowel Memorial Hospital, 2003-04 (> 20 cases)
CMG Title Cases Weighted Cases648 Normal newborn delivery 126 27.7611 Vaginal delivery 123 88.7294 Gastrointestinal/digestive disease 45 31.5143 Simple pneumonia 39 46.7847 Other specified aftercare 39 93.6851 Other factors causing hospitalization 34 34.5222 Heart failure 33 42.6841 Rehabilitation 32 91.8646 Low birth weight with caesarean 30 11.5290 GI obstruction 27 43.9242 Chest pain 26 11.9647 Newborn with minor problem 24 9.313 Cerebrovascular disorder 22 52.3237 Arrhythmia 22 16.9329 Biliary tract disease 22 26.2438 Diabetes 22 32.5208 AMI w/o specific cardiac condition 21 17.8609 Vaginal delivery with complications 21 18.4
Total Cases 1243 1295.4% of Total = 57%

North Perth Family Health TeamBusiness and Operational Plan 57
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
APPENDIX 7
Listowel Memorial Hospital Ambulatory Care Statistics (2003-04 to 2005-06)(cases >100 in 2005-06)
CAC# Clinical Category 2003-04 2004-05 2005-06 % Increase
310 General ENT Management 861 942 1261 46.457607453 Skin Procedures 740 771 724 -2.1621622
915 Skin and Subcutaneous 413 641 691 67.3123487420 General Respiratory Management 353 431 466 32.0113314835 Other Musculosketetal Management 266 350 465 74.8120301320 Otitis Media 345 376 431 24.9275362
2124 Sprains 256 330 403 57.4218752050 Follow-up or Convalescence 81 264 345 325.9259262130 Contusion 182 257 321 76.37362642010 Prophylactic Vaccination 67 187 318 374.626866
630 General GI Management 196 229 300 53.0612245910 Skin and Subcutaneous 142 243 296 108.450704
1165 Other Genitourological Management 191 213 282 47.64397912112 Fractures and Dislocations 204 238 246 20.58823532005 Management General Symptoms 135 211 245 81.48148152166 Other Major Injuries 187 227 239 27.8074866
620 General GI Management 108 171 226 109.259259640 General GI Management 122 192 222 81.9672131
2118 Open Wounds w-o Complications 225 148 214 -4.8888889510 General Circulatory Management 129 146 188 45.7364341210 Opthalmology Management 103 118 176 70.8737864
1810 Systemic Infection Management 106 155 163 53.7735849410 General Respiratory Minor Investigation 99 119 156 57.5757576
2163 Other Moderate Injuries 119 149 148 24.36974791992 Personality and Mood Disorders 98 114 145 47.9591837
430 General Respiratory Management 76 90 138 81.5789474120 Migraine Headache 76 80 131 72.3684211
6 Eye - Grade 1 80 95 129 61.252015 Therapeutic Counselling 68 138 129 89.7058824
340 Dental and Oral Disorders 95 101 126 32.6315789520 Vascular Problems 35 89 125 257.142857
2115 Head Injury 80 111 122 52.5610 General Gastro Minor Investigation 76 106 110 44.7368421500 General Circulatory Minor Investigation 75 78 109 45.3333333175 Management Vertigo 68 88 107 57.3529412
sub-totals: 6457 8198 9897% of total cases 75% 76% 80.00%
Total Cases 8,651 10,649 12,355 42.8158594

North Perth Family Health TeamBusiness and Operational Plan 58
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
APPENDIX 8
CCAC Caseload for North Perth clients
Age Group 2003-04 2004-05 2005-06< 20 years 100 132 14620-59 years 75 71 9260-85 years 179 188 217>85 years 98 86 101
Total cases: 452 477 556
Type of Care% acute care 30% 23% 21%% long term care 25% 27% 28%% rehab 19% 30% 44%% other 26% 20% 7%
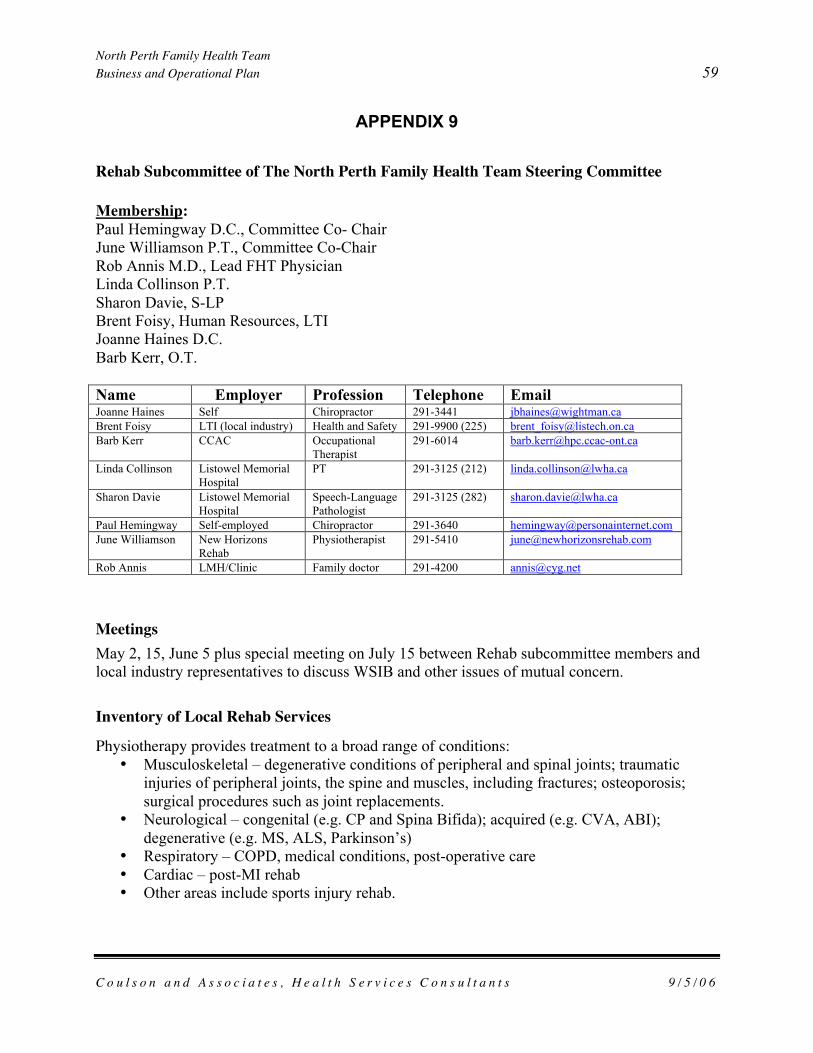
North Perth Family Health TeamBusiness and Operational Plan 59
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
APPENDIX 9
Rehab Subcommittee of The North Perth Family Health Team Steering Committee
Membership:Paul Hemingway D.C., Committee Co- ChairJune Williamson P.T., Committee Co-ChairRob Annis M.D., Lead FHT PhysicianLinda Collinson P.T.Sharon Davie, S-LPBrent Foisy, Human Resources, LTIJoanne Haines D.C.Barb Kerr, O.T.
Name Employer Profession Telephone EmailJoanne Haines Self Chiropractor 291-3441 [email protected] Foisy LTI (local industry) Health and Safety 291-9900 (225) [email protected] Kerr CCAC Occupational
Therapist291-6014 [email protected]
Linda Collinson Listowel MemorialHospital
PT 291-3125 (212) [email protected]
Sharon Davie Listowel MemorialHospital
Speech-LanguagePathologist
291-3125 (282) [email protected]
Paul Hemingway Self-employed Chiropractor 291-3640 [email protected] Williamson New Horizons
RehabPhysiotherapist 291-5410 [email protected]
Rob Annis LMH/Clinic Family doctor 291-4200 [email protected]
MeetingsMay 2, 15, June 5 plus special meeting on July 15 between Rehab subcommittee members andlocal industry representatives to discuss WSIB and other issues of mutual concern.
Inventory of Local Rehab Services
Physiotherapy provides treatment to a broad range of conditions:• Musculoskeletal – degenerative conditions of peripheral and spinal joints; traumatic
injuries of peripheral joints, the spine and muscles, including fractures; osteoporosis;surgical procedures such as joint replacements.
• Neurological – congenital (e.g. CP and Spina Bifida); acquired (e.g. CVA, ABI);degenerative (e.g. MS, ALS, Parkinson’s)
• Respiratory – COPD, medical conditions, post-operative care• Cardiac – post-MI rehab• Other areas include sports injury rehab.

North Perth Family Health TeamBusiness and Operational Plan 60
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
Physiotherapy services in North Perth are provided through the Listowel Memorial Hospital (in-patient and out-patient services), Perth CCAC, and to children through regional services such asThames Valley Children’s Centre in London. Private physiotherapy is provided through NewHorizons Rehabilitation Services Inc.Occupational TherapyThere are 1.4 FTEs serving North Perth (1 full-time OT for adults and 1 paediatric OT doing 2days per week). For School Services paeds, there is an OT working 2 days per week to coverListowel, Elma, Wallace, Christian, and St. Mary’s RC. The schools in Milverton/Morningtonand Mitchell and Howick area have an OT the equivalent of one day per week. According to theCCAC Case Manager for those schools, there are approximately 230 children on their caseloadand while not all are OT clients, that is the majority and the largest growing sector of the newreferrals.ChiropracticChiropractors diagnose and treat musculoskeletal conditions which include arthritis and relatedconditions (ARC). ARC are a varied group of problems affecting the musculoskeletal system andone of the most common conditions affecting Ontarians.7 In 2000-01, arthritis and back problemswere ranked second and third behind non-food related allergies. Prevalence increases with agebut 3 in 5 affected are of working age. The crude prevalence of ARC in the Grey Bruce HuronPerth planning district is about 20% of those surveyed which is similar to the provincial average.The associated costs related to the management of ARC are second only to cardiovasculardisease. The majority of costs are related to the indirect costs of disability and its consequenteffect on work productivity. Improving the coordination and continuity of care in patientssuffering from ARC would reduce the societal costs by reducing pain and suffering thathopefully would more than offset increases in health care expenditures.8
There are 3 chiropractors serving the Municipality of North Perth which represents a ratio of 1chiropractor per 4,522 residents. This level of service availability is worse than the average forall of Perth County (1:3537) and only slightly better than the provincial average (1:5063). Theutilization rate of chiropractors can be affected by regional variations in the prevalence andseverity of musculoskeletal conditions, the number of chiropractors, the availability of otherrehab professionals, and the availability of insurance coverage now that chiropractors have beende-listed from OHIP coverage.
Service Gaps and Other Key Issues:At the hospital, the waiting list for Physiotherapy is currently 8 months. Priority is given toacute injuries, post op., and fractures while chronic patients fall through the gaps. Pediatrics isanother gap in service. Current service is limited to infrequent visits (e.g. once every six weeks).The waiting list causes a lot of pressure and care can be affected (i.e. quality and time given getsrushed).
7 ICES Practice Atlas for Arthritis, Sept. 20048 Bradley et al, Arthritis and related conditions in Ontario

North Perth Family Health TeamBusiness and Operational Plan 61
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
The number of new patients who were started on out-patient physiotherapy at LMH for theperiod April 1/05 – March 30/06 was 394; for the same period the number of new patients startedon physiotherapy at New Horizons Rehabilitation Services Inc was 307 (243 – extended healthcare; 29 – WSIB). Consequently a total of 701 patients were started on physiotherapy treatmentin that period. In addition, 183 in-patients were provided with care at LMH.
There is an ongoing need for publicly funded physiotherapy to maintain mobility and functionalhealth in the populations identified above. For example, stroke patients benefit significantly byaccess to physiotherapy care to optimize, then maintain motor recovery, and consequentlyfunction with respect to transfers, ambulation and activities of daily living, allowing thatindividual to live independently for a longer period of time. Individuals who undergo jointreplacement, have degenerative joint and spine conditions require access in a timely fashion totreatment to optimize their recovery and maintain independence. Though some of North Perthresidents have private insurance to access private care, a significant part of the population doesnot have this benefit and consequently rely on the public system to provide care. In additionsome conditions require ongoing treatment (ex: congenital paediatric conditions and strokes)which can not be fully covered by private insurance.
In summary, there is need for additional physiotherapy services in North Perth.
Occupational Therapy
This is a significant issue locally as a result of OT shortages and poor funding provided for OT’sprovincially. There is notable service gap between what the CCAC can offers and what isneeded. Pediatric coverage is poor (it allows for only 1 treatment every 6 weeks). School agechildren and mild cases have almost no coverage for OT’s and autistic children ‘fall through thecracks’.
Geriatric OT clients are mostly things like hand-splinting, stroke recovery and education. Thereis a vascular health clinic that has had a hard time getting started. With respect to stroke patients,needs differ between age groups (i.e. 50 vs. 80 year old stroke patient). The follow-up afterdischarge is lacking. Additional funding might be able to help provide home follow up to helpwith things like ADL’s (activities of daily living). A lot of times patients are reliant on caregiversupport just to get to rehab (the CCAC does it at home but it is much less intensive care than atthe hospital). In summary, there is need for additional occupational therapy services in NorthPerth.
Speech Language PathologyPre-school children get service within three weeks (Small Talk). Ten percent of the preschoolpopulation have speech problems. Inpatients have priority. School-aged children often have towait (this is the gap) and often the number of visits is limited. There are two distinct groups ofchildhood cases: (1) children with language delays; (2) children with motor-related speechproblems and both are underserviced, especially compared to what they receive through the pre-school speech initiative.

North Perth Family Health TeamBusiness and Operational Plan 62
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
A formal system is in place to transition preschool children into the school based system butadequate amount of service may be challenge. The Board of Education also has problems withSLP staffing, which means that often not enough is done in the school. Adult outpatients arefewer in number and access the service without significant wait times. In summary, there is needfor additional speech language pathology services in North Perth.
Use Of Chiropractic ServicesChiropractic services have been recently de-listed by the provincial government, even withstrong evidence to the contrary (esp. lower back pain, WSIB stats). Chiropractors are one of the5 regulated health professions that have the ability to diagnose (i.e. neuromusculoskeletalconditions -NMS) and to take and read x-rays. With the introduction of the FHT, localchiropractors believe there is an opportunity to work more closely with physicians and otherprofessionals to order proper examinations (i.e. x-ray, Doppler) for patients with ARC so thatthey can be more quickly diagnosed and begin treatment sooner. This would have the positiveeffect of reducing wait times to see physicians. Chiropractors can also help reduce system costsin their treatment of ARC patients.
Partnering With Local Businesses To Reduce Negative Impacts Of Workplace InjuriesWorker injuries are a huge cost to the health system and a significant drain on businessproductivity. In terms of provincial statistics, the average lost-time injury in 2006 cost $98,000(up 66% from 2002). This includes both direct and indirect costs. Direct (WSIB) costs are 20%($19,560). From 1996-2004, WSIB approved more than 382,000 MSD claims which led to 27million days off and a direct cost to business of $3.3 billion. Indirect costs are 4 times greaterestimated at $12 billion and include: overtime, lost productivity, equipment modifications,administration, retraining and compliance costs.
Local industry in North Perth has huge costs related to WSIB. A lot of their employees comefrom out of town and local employers would like to refer to local practitioners to cut down onlost work time (e.g. having to miss a whole day of work for 1 treatment) and to keep the businesslocal. Local employers are anxious to provide safe and suitable ‘return to work’ (RTW) forinjured workers. There is a possibility of financial support from local industry especially if it canmake sense to their bottom line (i.e. cut WSIB costs, reduce indirect costs etc.).
Important statistics from local industry are as follows related to musculoskeletal disorders(MSD):
• they cause the majority of injuries in North Perth• 42% of all lost-time claim costs• 50% of all lost-time days
SYSTEM WEAKNESSES- Lack of OT (for stroke, splints, etc.)- Inadequate speech therapy (done through Board of Ed. and CCAC presently)- Lack of physio access; plus some physio is covered publicly and some is not

North Perth Family Health TeamBusiness and Operational Plan 63
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
- Patient’s aren’t sure where to access the system/who to see- Industry doesn’t always access the system appropriately (i.e. frequently to ER)- Communication between providers- Inability of chiropractors to order x-rays
POTENTIAL OPPORTUNITIES- Involve other “partners”, e.g. exercise facilities, Arthritis society, Fibromyalgia Group
etc.- Pain management post rehab care (chronic pain management)- Work with industry to offer multidisciplinary rehab appropriate care where funding is
costs-shared (WSIB, industry, OHIP, and the FHT)- Move “OT” care (for stroke, for example) close to home- Improve system navigation for patient- EMR roll out so rehab professionals are linked to a common patient medical record

North Perth Family Health TeamBusiness and Operational Plan 64
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
APPENDIX 10
Focus Group on EMR Community Implementation
Membership:Dr. Peter Trainor, dentistDr. Betty Fretz, optometristKathy Scanlon, CCACJason Shaw, pharmacistDr. Joanne Haines, chiropractorCathy Healy, Caressant Care NHJune Williamson, physiotherapistBrent Boschart, LMH Information TechnologyMike Lapaine, LMH acting CEOStephen Lafferty, PurkinjeDr. Russell Latuskie, Listowel FHNDr. Rob Annis, Listowel FHN
Meetings: March-April 2006 plus stakeholder survey (see below)Phased Implementation of EMR Community Roll-out:
Phase 1 (September – December 2006)Listowel community health professionals who have indicated their support for the Family HealthTeam project and are prepared to be part of ‘Phase 1’9 community roll-out of the ListowelElectronic Medical Record (EMR):
• Dr. Fretz (optometrist)• Tony Gangl (chiropractor) (519-291-1566)• Joanne Haines (chiropractor) (519-291-3441)• Dr. Paul Hemingway (chiropractor) (519-291-3640)• Dr. Rod MacKenzie (optometrist) (519-291-1511)• Dr. Peter Trainor (dentist) (519-291-3811)• June Williamson (physiotherapist)
Phase 2 (2007) ‘Phase 2’ of community roll-out of the Listowel EMR will focus on larger health careorganization who have expressed interest in working with the Listowel Family Health Team andaccessing the EMR but the computer interface and/or patient confidentiality issues are morecomplex and will require additional time and resources to resolve:
• Canadian Mental Health Association (Perth-Huron branch)
9 ‘Phase 1’ of EMR community roll-out will focus on solo health care professionals in Listowel that meet thefollowing criteria:
(1) written support for the FHT project and interest in using selected data elements from the EMR (basedon April 2006 questionnaire);
(2) already established policies to protect confidentiality of patient records/charts

North Perth Family Health TeamBusiness and Operational Plan 65
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
• Community Care Access Centre for Perth County• Fordwich Village Nursing Home• Perth District Health Unit• Victorian Order of Nurses (Perth-Huron branch)
Summary of Responses to EMR Roll-Out Survey (April 2006):-Dr. Fretz (optometry), Joanne Haines (chiropractor), Tony Gangl (chiropractor), R. Mackenzie,Dennis Nuhn (dentist), Peter Trainor (dentist), June Williamson (physiotherapist)
1. What data elements in the current Listowel EMR would you most like to have access toin terms of the patient care you provide?
a. Diagnostic imaging resultsb. Access to lab resultsc. Current medications plus allergiesd. Pertinent general health historye. Communicable diseasesf. Intelligent data searches for relevant topics (e.g. headaches, back pain etc.)g. Messaging system
2. What patient information do you collect now that could potentially be added as new dataelements to the EMR?
a. Patient record would be more comprehensive if visits to allied healthprofessionals are documented (incl. chief complaint, frequency of visits, treatmentparameters, outcomes) – true community record would create greater efficacy andimproved patient safety
b. Pertinent ocular historyc. Patients bring in copies of reports/x-rays from other centers or insurance
information (WSIB) and these reports could be scanned into recordd. Could contribute digital radiographs electronically – this could be beneficial for
panographic radiographs (sinus and full TMJ areas)3. Do you have a signed patient consent form which deals with sharing of patient
information?a. Yes (5)b. No (2)
4. What are your main concerns about participating in the community roll-out of theListowel EMR?
a. Uncharted waters?b. Patient understanding of community health record is key to successc. What will the sharing of information look like in the end?d. Assuring patients that their privacy is securee. The privacy issue is very significant – I feel that each participant must be
prepared to educate the patient on the purpose and process of the EMR in order togenerate patient comfort and ‘buy-in’ with the system

North Perth Family Health TeamBusiness and Operational Plan 66
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
5. Will you be able to contribute to the ‘start-up’ and/or ongoing costs of an expandedListowel EMR?
a. Yes, but need more information on costs and benefits.b. I have not thought much about this. Anything that is beneficial to our community
is something that I would be prepared to support financially. However, havingsaid that, I feel that the providers of health services should not be looked at forongoing financial support. I believe the users of the system and the community atlarge is where funding must come from.
c. Costs and benefits to patients and individual practitioners are linked – all partiesshould benefit from the sharing of information; dollars need to be known anddiscussed
d. What extent of cost-sharing is involved? It will be necessary to a cost-benefitanalysis in order to make prudent decisions.
6. Other comments?a. This initiative is of major clinical safety and importance to me at this time since
the delisting of chiropractic services by the government in Dec.2004….chiropractors must use appropriate means of determining treatmentefficacy based on a multitude of clinical and diagnostic tests – the x-ray being ofparamount importance to those who deal with the musculoskeletal system. Theintegration of the EMR may provide an avenue for us to send an x-ray request tothe patient’s physician to be reviewed and signed off to streamline this process.This has the potential to increase patient safety and I can give various instanceswhere unstable fractures and osseous tumours were located by chiropractors andthen treated with the appropriate allopathic medical intervention.
Health Organizations Responding-Fordwich Village Nursing Home, VON, CCAC_______________________________________________________________________
7. What data elements in the current Listowel EMR would you most like to have access toin terms of the patient care you provide?
a. Diagnostic imaging resultsb. Lab resultsc. Current medsd. History/discharge summariese. Basic health informationf. Treatment orders pertaining to nursingg. Specialist reports
8. Please list the other key regulated health professionals in your organization that wouldbenefit from some type of access to the Listowel EMR?
a. Physicians, dentists, dieticians, occupational therapists, physiotherapists

North Perth Family Health TeamBusiness and Operational Plan 67
C o u l s o n a n d A s s o c i a t e s , H e a l t h S e r v i c e s C o n s u l t a n t s 9 / 5 / 0 6
b. Nursing, community support services (especially adult day programs)
9. What patient information do you collect now that could potentially be added as new dataelements to the EMR?
a. Residents advance care directiveb. Community support services access to basic health information
10. Do you have a signed patient consent form which deals with sharing of patientinformation?
a. Yes (3)
11. What are your main concerns about participating in the community roll-out of theListowel EMR?
a. Main concern is to ensure the security of resident/patient records
12. Will you be able to contribute to the ‘start-up’ and/or ongoing costs of an expandedListowel EMR?
a. Would depend on the costs involvedb. Need to know more specifics


















