

North East Leading Improvement for Health and Wellbeing Programme Masterclass 19 April 2012
date post
19-Dec-2015Category
view
213download
0
North East Leading Improvement for Health and Well-being Programme
Improvement Methods Workshop 1

Jean PennyAll working life in NHSDiagnostic Radiographer and teacherImprovement roles since 1994
BPR Leicester Royal Infirmary 1994 - 1999National Patients ‘Access Team 1999 - 2002NHS Modernisation Agency 2002 – 2005NHS Institute for Innovation and Improvement 2005 -2008
Awarded OBE for services to NHS 2003Visiting professor University of Derby 2008

Introductions
Who are you?
Where are you from?
Which of the 10 work streams are you working on

Leadership and improvement

Leadership framework for improvement
6
1. Set Direction: Mission, Vision and Strategy
Make the status quo uncomfortable
Make the future attractive
3. Build Will• Plan for improvement• Set aims/allocate resources• Measure system
performance• Provide encouragement• Make financial linkages• Learn subject matter
5. Execute Change• Use Model for Improvement for
design and redesign• Review and guide key initiatives• Spread ideas• Communicate results• Sustain improved levels of performance
4. Generate Ideas• Understand organisation as a
system• Read and scan widely, learning
from other industries and disciplines
• Benchmark to find ideas• Listen to patients• Invest in research and
development• Manage knowledge
2. Establish the Foundation• Prepare personally• Choose and align the senior
team
• Build relationships• Develop future leaders
• Reframe operating values• Build improvement capability
Source: Robert LloydExecutive Director Performance Improvement
Institute for Healthcare Improvement January 16, 2007

Basics of improvement

Deming
8
Knowledge of Systems
Theory of knowledge
Knowledge about Variation
Knowledge of Psychology
W Edwards Deming (1994) The New Economics
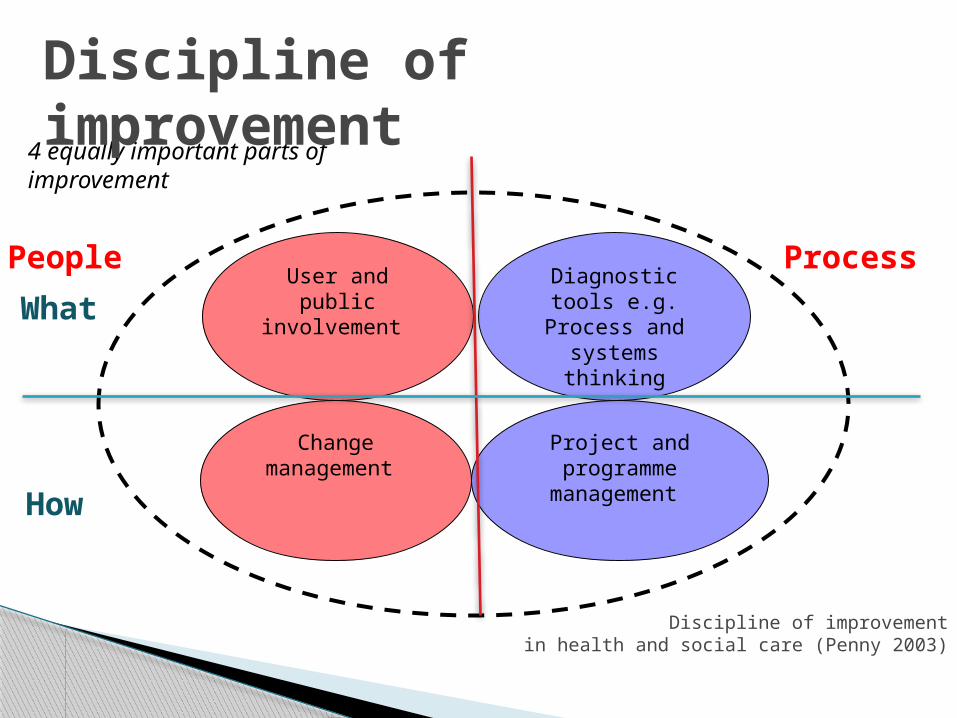
4 equally important parts of improvement
Diagnostic tools e.g. Process and systems
thinking
Project and programme
management
User and public involvement
Change management
Discipline of improvement
Discipline of improvement in health and social care (Penny 2003)
People Process
What
How

Diagnostic tools e.g. Process and systems
thinking
Project and programme
management
User and public involvement
Change management
‘Every single person is enabled, encouraged and capable to work with others to improve their part of the service.’
Discipline of improvement in health and social care (Penny 2003)
People Process
What
How

What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
Act Plan
Study Do
Understanding the problem. Knowing what you’re trying to do - clear and desirable aims and objectives
Measuring processes and outcomes
What have others done? What hunches do we have? What can we learn as we go along?Langley G, Moen R, Nolan K, Nolan
T, Norman C, Provost L, (2009), The improvement guide: a practical approach to enhancing organisational performance 2nd ed, Jossey Bass Publishers, San Francisco

Linking strategic goals and frontline improvement

Defining status and position
Tools to find out the current status and position of an organisation or individual in relation to their environment and current role.
Use as a basis for future planning and strategic management.
Prioritisation – ‘something considered to be more important than other things’ (PMMI, 2006)

PESTLE Political – what are the key political drivers of
relevance? Economic – what are the important economic
factors? Social – what are the main social and cultural
aspects? Technological - what are current technology
imperatives, changes and innovations? Legal - what current and impending legislation
factors? Environmental - What are the environmental
considerations, locally and further afield?

Discussion 1: Using PESTLE take stock of the position of
your improvement topicthen
Use PESTLE to map the things that will influence the way your service is delivered

Tools and techniques: PESTLE & SWOT

Understand the Complexity of Your Project
Macro
Meso
Micro
©Profound Knowledge Products, Inc. 2008 All Rights Reserved

Ask yourself
• What are the problems that cause the bigger problem?
• What are you trying to achieve? (aim for each driver)
• How will you know a change is an improvement ? (outcome measures for each driver )
Drivers
Which in turn contribute directly to the ‘bigger’ aim
AimThe ‘big’ dots
Ask yourself
• What is the big (possibly strategic) problem you are addressing?
• What are you trying to achieve? (aim)
• How will you know a change is an improvement ? (outcome measures)
Ask yourself
What changes can you make that will result in the improvement you seek?
• What are the change ideas / interventions/ solutions to test with PDSA cycles before implementing?
• How will you know a change is an improvement? (process measures for each intervention)
Intervention 1
Intervention 2
Intervention 3
Intervention 1
Intervention 2
Intervention 3
Intervention 1
Intervention 2
Intervention 3
Interventions The ‘small’ frontline dots
Contribute directly to the drivers

Intervention 1
Intervention 2
Intervention 3
Intervention 1
Intervention 2
Intervention 3
Intervention 1
Intervention 2
Intervention 3
The interventions / change ideas that contribute directly to secondary drivers
Secondary Drivers:Contribute directly to
primary drivers
Intervention 1
Intervention 2
Intervention 3
Intervention 1
Intervention 2
Intervention 3
?
Primary Drivers:Contribute
directly to the strategic aim
The strategic aim (and
big problem)

Reducing harm in perioperative
care
Reduce surgical site infections
Improve team work and
communications
Appropriate use of prophylactic antibodies
Maintain normothermia
Maintain glycaemic control in known diabetes
Use recommended hair removal methods
Use of the WHOSurgical safety checklist
Primary Drivers Secondary Drivers
Ref. Patients Safety First

Developing measures to support an objective
To provide accessible rented housing
Make effective use of existing public housing
Work with registered social landlords to develop public housing
Manage housing benefit effectively
• Percentage dwellings empty• Relet intervals for all public housing• Percentage housing stock in good repair
• Total number of dwellings available
• Speed of processing claims• Accuracy of processing claims

Discussion 2: Consider the position of your improvement
topic in a driver diagram
Is it a primary or secondary driver?
What would your driver diagram look like?

The Model For Improvement

Measurement: Big dots and little dots The Model for Improvement breaks things
down into small steps and works of the ‘little dots’ – at the frontline
These small steps should be part of the answer to the question of how to move the big dots
Align all improvement projects to strategy

26
Define The Problem
An example Process Map:
Process Mapping The patient journey
◦ Who does what to the patient?◦ Define which group of patients◦ Define the scope (beginning
and end)◦ Identify everyone involved◦ Together, write it down or draw
it Other (sub-) processes
◦ Transport◦ Communication

Analysing a process map
How many steps? How many hand-offs? What is the approx. time of or between each
step? Where are possible delays and why? Where are the problems for users, carers and
staff? How many steps do not “add value”?
WASTE!
Ask why 5 times!!

Why is Lean Relevant?
“Lean thinking is not a manufacturing tactic or a cost reduction programme, but a management strategy that is applicable to all organisations because it has to do with improving processes. All organisations – including health care organisations – are composed of a series of processes, or sets of actions, intended to create value for those who use or depend on them (customer/patients)”
IHI: Going Lean in Health Care 2005
Eliminating Non Value Add has a major impact on
Quality, Cost and Service Delivery

Defects – “stuff” that is not right and
needs fixing e.g a leaky tap
Inventory – “stuff” waiting to be
worked on e.g patients
on a waiting list Overproduction – too much “stuff”
e.g. requesting unnecessary tests and X-rays
Motion – unnecessary movement e.g having to walk up and down
the ward to obtain appropriate supplies
Transportation – moving “stuff” e.g
moving patients from ward to ward
Waiting – people
waiting for “stuff” to arrive
e.g waiting for a ward
round
Injuries – damage to people e.g stress
Processing waste – “stuff” we have to do that doesn’t add value.
E.g continuing to care for patients in hospital when they could be discharged
What is Waste?Lean Principles
Mark Rahman NHS Scotland

Analysis of a process map
For each step ask ‘does it add value?’. If not ask: ◦ Can it be eliminated?◦ Can it be done in some other way?◦ Can it be done in a different order?◦ Can it be done somewhere else?◦ Can it be done in parallel?◦ Can any “Bottlenecks” be removed?◦ Is it being done by the most appropriate person?

31
What are the problems for users, carers and staff and what are the causes of the problem?Ishikawa (Fishbone) Diagrams
PPPP
People Place
Procedures Policies

33
Use Pareto Principle to identify cause(s) of problem to work on first
‘The 80-20 Rule’ ‘The Law of the Vital Few’ For many phenomena,
80% of the consequences stem from20% of the causes
Observation that 80% of income went to 20% of the population
Vilfredo Pareto, 1906

What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
Act Plan
Study Do
Understanding the problem. Knowing what you’re trying to do - clear and desirable aims and objectives
Measuring processes and outcomes
What have others done? What hunches do we have? What can we learn as we go along?Langley G, Moen R, Nolan K, Nolan
T, Norman C, Provost L, (2009), The improvement guide: a practical approach to enhancing organisational performance 2nd ed, Jossey Bass Publishers, San Francisco
• The more specific the aim, the more likely the improvement
• Repeated clarification - without it aims drift
• Meet needs of external customers

35
Discussion 3:
Have you defined the problem and agreed the aim for your improvement topic? Can you verbalise it in order to
communicate?
Use a fishbone diagram to start to identify the causes of the problem

Lunch

Valuing the differences

4 equally important parts of improvement
Diagnostic tools e.g. Process and systems
thinking
Project and programme
management
User and public involvement
Change management
Discipline of improvement
Discipline of improvement in health and social care (Penny 2003)

Managing The Human Dimensions Of Change
Ways of helping others to change: Building trust and relationships Creating rapport Managing conflict Negotiation Effective communication

Value (and learn about) the differences
No rights or wrongs just differences!

Analytical• formal• measured + systematic• seek accuracy / precision• dislike unpredictability and surprises
Driver• business like• fast + decisive• seek control• dislike inefficiency and indecision
Amiable• conforming• less rushed + easy going • seek appreciation• dislike insensitivity and impatience
Expressive• flamboyant• fast + spontaneous• seek recognition• dislike routine and boredom
Personal styles Controlsemotions
Ask Tell
Showsemotions
Merrill D, Reid R (1991) Personal Styles and Effective Performance, CRC Press, London
What are your fears about change?How do you behave under stress?

Analytical• formal• measured + systematic• seek accuracy / precision• dislike unpredictability and surprises
Driver• business like• fast + decisive• seek control• dislike inefficiency and indecision
Amiable• conforming• less rushed + easy going • seek appreciation• dislike insensitivity and impatience
Expressive• flamboyant• fast + spontaneous• seek recognition• dislike routine and boredom
Personal styles Controlsemotions
Ask Tell
Showsemotions
Merrill D, Reid R (1991) Personal Styles and Effective Performance, CRC Press, London
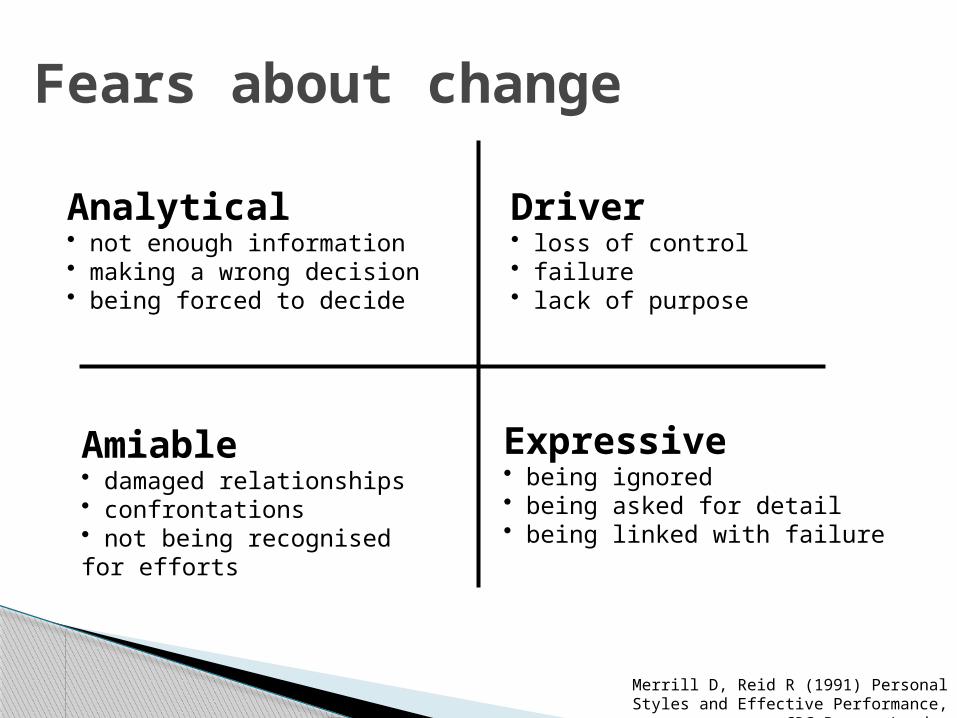
Fears about change
Analytical• not enough information• making a wrong decision• being forced to decide
Driver• loss of control• failure• lack of purpose
Amiable• damaged relationships• confrontations• not being recognised for efforts
Expressive• being ignored• being asked for detail• being linked with failure
Merrill D, Reid R (1991) Personal Styles and Effective Performance, CRC Press,
London

Under stress
Analytical• will withdraw
Driver• will become
autocratic
Amiable• will submit
Expressive• will become
offensive/sarcastic
Merrill D, Reid R (1991) Personal Styles and Effective Performance, CRC Press, London

Personal styles
Ask Tell
Driver• Objective focused• Know what they want and how to get
there• Sometimes tactless and brusque• Hardworking, high energy. Does not shy
from conflict
Controlsemotions
Showsemotions
Merrill D, Reid R (1991) Personal Styles and Effective Performance, CRC Press, London
• Natural sales people and story tellers• Warm and enthusiastic but can be
competitive • Good motivators and communicators• Can exaggerate, leave out facts and details
• Highly detail orientated• Can have difficulty making decisions
without all the facts• Tend to be highly critical• Very perceptive
• Kind hearted people who avoid conflict
• Can blend into any situation• Can appear wishy-washy and have
difficulty with firm decisions• Can be quiet and soft spoken
Expressive Amiable
Analytical

How to recognise personal styles
The Driver: Command Specialist
Perceived positively as: Perceived negatively as:
Decisive PushyIndependent One man/woman showPractical ToughDetermined DemandingEfficient DominatingAssertive An AgitatorA risk taker Cuts cornersDirect InsensitiveA problem solver
Merrill D, Reid R (1991) Personal Styles and Effective Performance, CRC Press, London
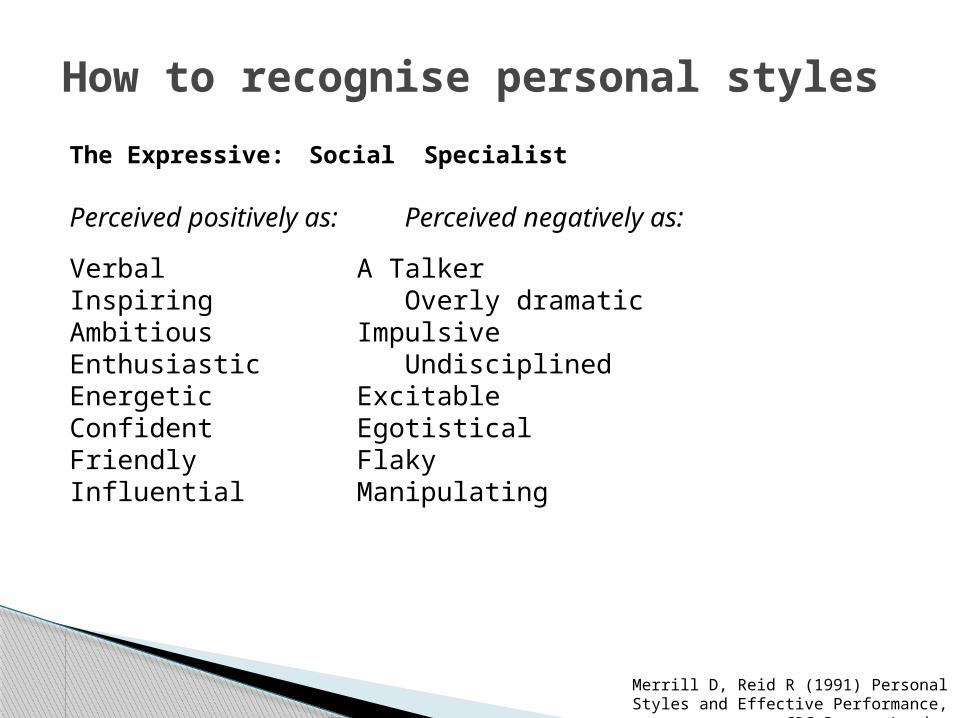
How to recognise personal styles
The Expressive: Social Specialist
Perceived positively as: Perceived negatively as:
Verbal A TalkerInspiring Overly dramaticAmbitious ImpulsiveEnthusiastic UndisciplinedEnergetic ExcitableConfident EgotisticalFriendly FlakyInfluential Manipulating
Merrill D, Reid R (1991) Personal Styles and Effective Performance, CRC Press, London

How to recognise personal styles
The Amiable: Relationship Specialist
Perceived positively as: Perceived negatively as:
Patient HesitantRespectful Wishy WashyWilling PliantAgreeable ConformingDependable DependentConcerned UnsureRelaxed Laid BackOrganizedMatureEmpathetic
Merrill D, Reid R (1991) Personal Styles and Effective Performance, CRC Press, London

How to recognise personal style
The Analytical: Technical Specialist
Perceived positively as: Perceived negatively as:
Accurate CriticalExacting PickyConscientious MoralisticSerious StuffyPersistent StubbornOrganized IndecisiveDeliberateCautious
Merrill D, Reid R (1991) Personal Styles and Effective Performance, CRC Press, London
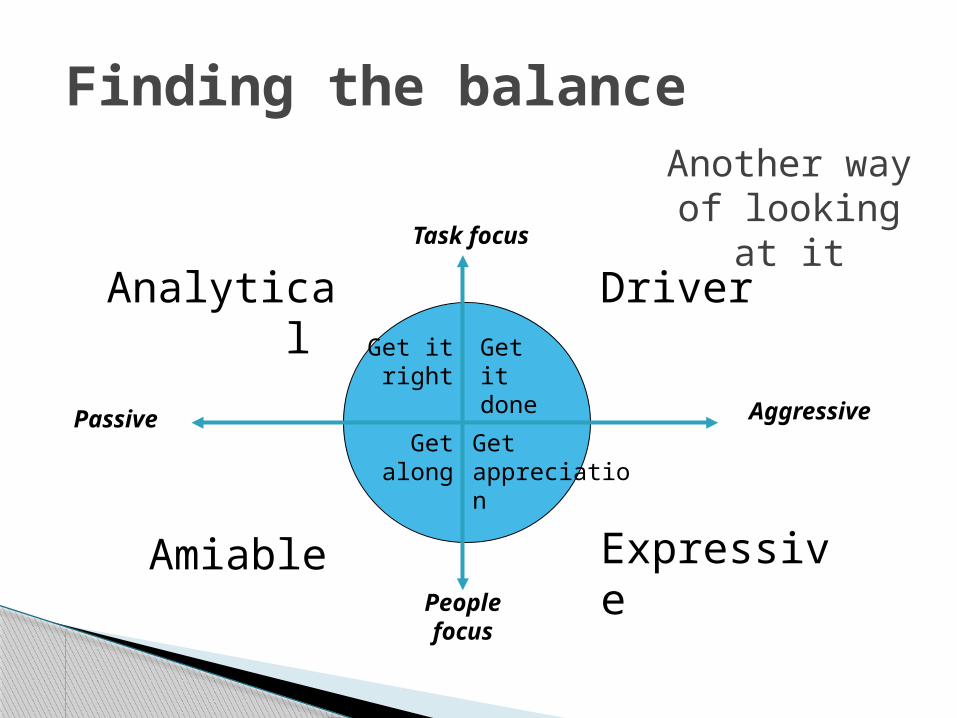
Task focus
People focus
Passive Aggressive
Get it right
Get it done
Get along
Get appreciation
Finding the balance
Driver
ExpressiveAmiable
Analytical
Another way of looking at it

Discussion 4: The Importance of Personal Styles
Indicate◦ A person’s interests &
priorities◦ Behaviour and actions◦ Strengths and
weaknesses
Use this insight to◦ Choose effective ways to
communicate ideas◦ Know how to work better
with that person
51
Think about • Your team strength• How the team can
be more effective• The style of the
individual who may cause most difficulty

Trust: Caring & Competency
Affection Trust
Distrust Respect
Extent to which I believe
you care about me
Extent to which I believe you are competent and capable
LOW
HIGH
HIGH
Adapted from P Scholtes (1998) The Leaders’ Handbook; McGraw Hill

Measuring for improvement (not judgement)
What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
Act Plan
Study Do
Understanding the problem. Knowing what you’re trying to do - clear and desirable aims and objectives
Measuring processes and outcomes
What have others done? What hunches do we have? What can we learn as we go along?Langley G, Moen R, Nolan K, Nolan
T, Norman C, Provost L, (2009), The improvement guide: a practical approach to enhancing organisational performance 2nd ed, Jossey Bass Publishers, San Francisco

The Three Faces of Performance MeasurementAspect Improvement Accountability Research
Aim Improvement of care Comparison, choice, reassurance, spur for
change
New knowledge
Methods:• Test Observability
Tests are observable No test; merely evaluate current performance
Test blinded or controlled tests
• Bias Accept consistent bias Measure and adjust to reduce bias
Design to eliminate bias
• Sample Size “Just enough” data, small sequential samples
Obtain 100% of available, relevant data
“Just in case” data
• Flexibility of
Hypothesis
Hypothesis flexible, changes as learning takes
place
No hypothesis Fixed hypothesis
• Testing Strategy Sequential tests No tests One large test
• Determining if a Change is an Improvement
Run charts or control charts
No change focus Hypothesis, statistical tests (t-test, F-test, chi
square), p-vlaues
• Confidentiality of the Data
Data used only by those involved with improvement
Data available for public consumption and review
Research subjects’ identities protected
Robert Lloyd Executive Director IHI adapted from Solberg L, Mosser G, Mcdonald S (1997) Three faces of performance
measurement: Improvement, accountability and research Journal of Quality Improvement Vol. 3 No 3

56
Charts vs. Tables

540
550
560
570
580
590
600
610
2007 2008
What does this tell us?

300
350
400
450
500
550
600
650
Jan-07
Feb-07
Mar-07
Apr-07 May-07
Jun-07
Jul-07 Aug-07
Sep-07
Oct-07 Nov-07
Dec-07
Jan-08
Feb-08
Mar-08
Apr-08 May-08
Jun-08
Jul-08 Aug-08
Sep-08
Oct-08 Nov-08
Dec-08
What does this tell us?

Somethingvery important!
Lastmonth
Thismonth
What actionis appropriate?
Given two different numbers, one will always be bigger than the other!

21.6 23.9 23.3 22.6 28.8 22.7 23.822.8 28.7 22.9 24.2 23.3 28.6 22.8 23.9 23.2 23.7 28.5 23.2 23.5 23.1 27.7
What does this data tell us?

Mean = 24.4
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
Wee
kly
pro
du
ctio
n v
olu
me
July Aug OctSeptWeek
What does this data tell us?

Run charts
0102030405060708090
Day
1 4 7 10 13 16 19
Seco
nds
to
answ
er p
hone
Average based on first 10 days
Seven one side
Seven down (or up)
DO
Look for a run of seven points all above or all below the centre line, or all increasing or all decreasing

How often you measure can also have an effect on how you look at
the results
Mike DavidgeNHS Institute for Innovation and Improvement
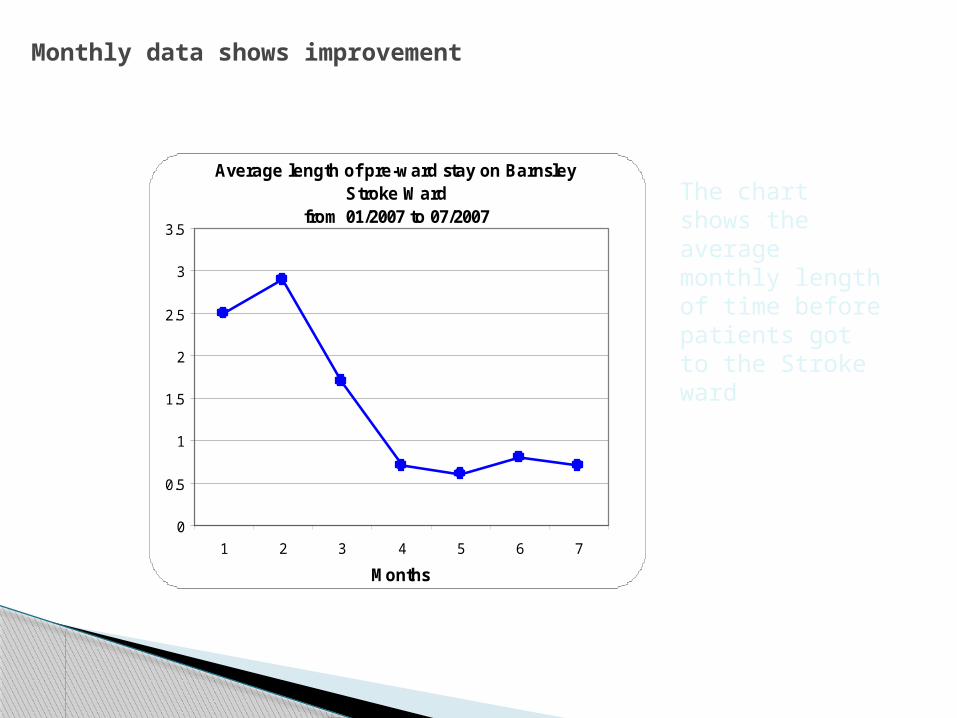
Monthly data shows improvement
Average length of pre-ward stay on Barnsley Stroke Ward
from 01/2007 to 07/2007
0
0.5
1
1.5
2
2.5
3
3.5
1 2 3 4 5 6 7
Months
The chart shows the average monthly length of time before patients got to the Stroke ward

Weekly data tells a slightly different story
Average length of pre-ward stay on Barnsley Stroke Ward
from 01/2007 to 07/2007
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31Weeks

Patient level data adds another level of understanding
Patient length of pre-ward stay on Barnsley Stroke Ward
from 01/2007 to 07/2007
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
Patients

Ask yourself
• What are the problems that cause the bigger problem?
• What are you trying to achieve? (aim for each driver)
• How will you know a change is an improvement ? (outcome measures for each driver )
Drivers
Which in turn contribute directly to the ‘bigger’ aim
AimThe ‘big’ dots
Ask yourself
• What is the big (possibly strategic) problem you are addressing?
• What are you trying to achieve? (aim)
• How will you know a change is an improvement ? (outcome measures)
Ask yourself
What changes can you make that will result in the improvement you seek?
• What are the change ideas / interventions/ solutions to test with PDSA cycles before implementing?
• How will you know a change is an improvement? (process measures for each intervention)
Intervention 1
Intervention 2
Intervention 3
Intervention 1
Intervention 2
Intervention 3
Intervention 1
Intervention 2
Intervention 3
Interventions The ‘small’ frontline dots
Contribute directly to the drivers

68
Discussion 5: Measuring for Improvement
Think about Question 1 of The Improvement Model and the primary and secondary drivers of your improvement work What ARE you trying to achieve? How will you KNOW that a change is an improvement?
How can you display measures for improvement on run charts to share with others – the big dots and the little dots?
Link improvement measures to strategic measures

What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
Act Plan
Study Do
Understanding the problem. Knowing what you’re trying to do - clear and desirable aims and objectives
Measuring processes and outcomes
What have others done? What hunches do we have? What can we learn as we go along?Langley G, Moen R, Nolan K, Nolan
T, Norman C, Provost L, (2009), The improvement guide: a practical approach to enhancing organisational performance 2nd ed, Jossey Bass Publishers, San Francisco
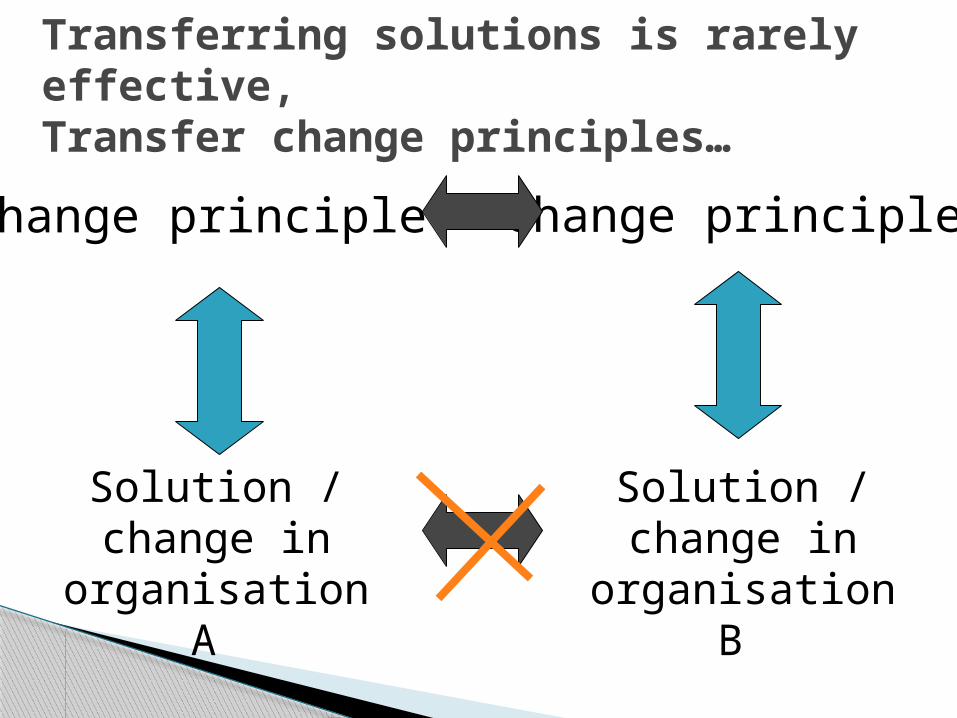
Transferring solutions is rarely effective,Transfer change principles…
Solution / change in
organisation A
Change principle Change principle
Solution / change in
organisation B

Speaking in PDSA Language
We planned to….. ( state the basic plan) In order to ….. (tie it back to the Aim)
What we did was….. (brief description of actions)
Looking at what happened, what we learned from this was….. ( lessons learned)
What we plan to do next is …. (state next plan)
© Paul Plsek
P
D
S
A

72
The Learning Cycle
Having an experience
Reviewing the experience
Concluding from the
experience
Planning the next steps
Honey & Mumford, 1992

Discussion 6: Developing change ideas Where will the
change ideas come from?
How will you gather them?
How will you test them?
Go back to your driver diagram
Ideas for change: Yours and othersExperienceBrainstormingEvidenceSteal ideas shamelessly

What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
Act Plan
Study Do
Understanding the problem. Knowing what you’re trying to do - clear and desirable aims and objectives
Measuring processes and outcomes
What have others done? What hunches do we have? What can we learn as we go along?Langley G, Moen R, Nolan K, Nolan
T, Norman C, Provost L, (2009), The improvement guide: a practical approach to enhancing organisational performance 2nd ed, Jossey Bass Publishers, San Francisco

Understand the Complexity of Your Project
Macro
Meso
Micro
©Profound Knowledge Products, Inc. 2008 All Rights Reserved

Leadership framework for improvement
76
1. Set Direction: Mission, Vision and Strategy
Make the status quo uncomfortable
Make the future attractive
3. Build Will• Plan for improvement• Set aims/allocate resources• Measure system
performance• Provide encouragement• Make financial linkages• Learn subject matter
5. Execute Change• Use Model for Improvement for
design and redesign• Review and guide key initiatives• Spread ideas• Communicate results• Sustain improved levels of performance
4. Generate Ideas• Understand organisation as a
system• Read and scan widely, learning
from other industries and disciplines
• Benchmark to find ideas• Listen to patients• Invest in research and
development• Manage knowledge
2. Establish the Foundation• Prepare personally• Choose and align the senior
team
• Build relationships• Develop future leaders
• Reframe operating values• Build improvement capability
Source: Robert LloydExecutive Director Performance Improvement
Institute for Healthcare Improvement January 16, 2007

4 equally important parts of improvement
Diagnostic tools e.g. Process and systems
thinking
Project and programme
management
User and public involvement
Change management
Discipline of improvement
Discipline of improvement in health and social care (Penny 2003)
Two sides of improvementHelps ‘what’ and ‘how’
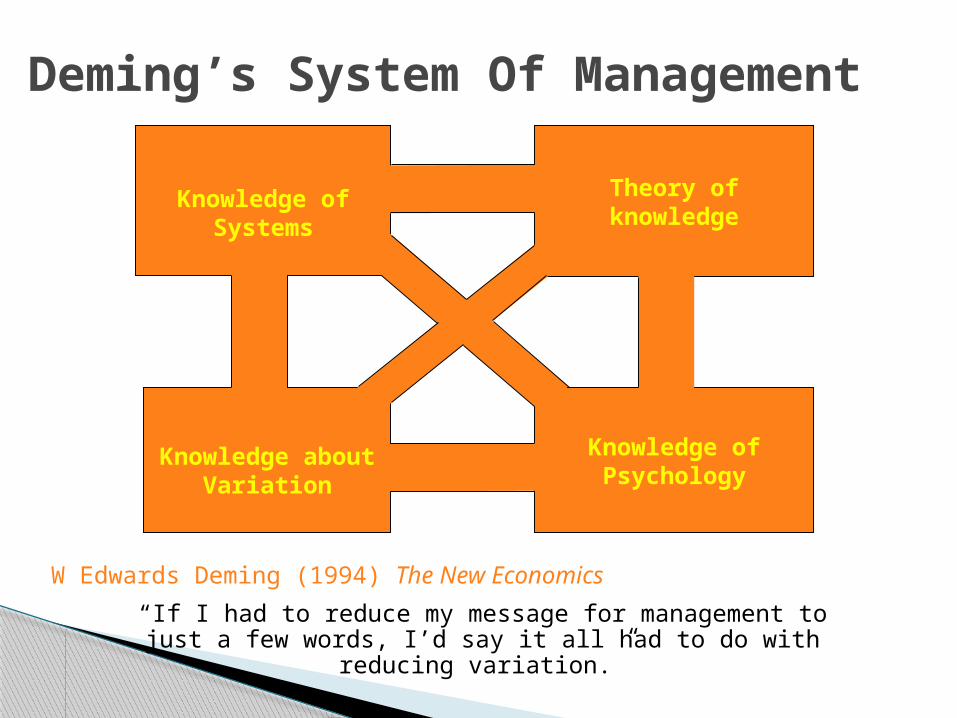
Deming’s System Of Management
Knowledge of Systems
Theory of knowledge
Knowledge about Variation
Knowledge of Psychology
W Edwards Deming (1994) The New Economics
“If I had to reduce my message for management to just a few words, I’d say it all had to do with reducing variation.”
79
Discussion 7: So what?????? Do you / your organisation currently use
improvement tools and techniques?
What are you going to do next?
One thing you will do as a result of today
One thing you have learnt / Ah-ah moment

Use resources Boaden, Harvey, Moxham Proudlove (2008) Quality
Improvement: theory and practice in healthcare NHS Institute for Innovation and Improvement
Improvement Leaders’ Guides
NHS Evidence specialist collection on innovation and improvement www.library.nhs.uk/IMPROVEMENT
General Improvement
Skills
Process and systems thinking
Personal and organisational development

Improvement workshop 2 Please complete your feedback forms for us
At Improvement workshop 2 Be prepared to share
◦ What you have done ◦ What you wish you had done differently◦ What you have learned about improvement
Next time◦ Managing transitions◦ Variation◦ Engaging others◦ Sustainability and spread


















