NORMALIZATION AND FAMILY FUNCTIONING IN FAMILIES WITH …
289
NORMALIZATION AND FAMILY FUNCTIONING IN FAMILIES WITH A CHILD WHO IS TECHNOLOGY DEPENDENT by VALERIE A. BOEBEL TOLY Submitted in partial fulfillment of the requirements For the degree of Doctor of Philosophy Dissertation Advisor: Dr. Carol M. Musil Frances Payne Bolton School of Nursing CASE WESTERN RESERVE UNIVERSITY May, 2009
Transcript of NORMALIZATION AND FAMILY FUNCTIONING IN FAMILIES WITH …

NORMALIZATION AND FAMILY FUNCTIONING IN
FAMILIES WITH A CHILD WHO IS TECHNOLOGY DEPENDENT
by
VALERIE A. BOEBEL TOLY
Submitted in partial fulfillment of the requirements
For the degree of Doctor of Philosophy
Dissertation Advisor: Dr. Carol M. Musil
Frances Payne Bolton School of Nursing
CASE WESTERN RESERVE UNIVERSITY
May, 2009

ii
CASE WESTERN RESERVE UNIVERSITY
SCHOOL OF GRADUATE STUDIES We hereby approve the thesis/dissertation of Valerie A. Boebel Toly candidate for the Doctor of Philosophy degree * (signed) Carol M. Musil
(chair of the committee) John C. Carl Donna A. Dowling Susan Tullai-McGuinness (date) March 12, 2009 *We also certify that written approval has been obtained for any proprietary material contained therein.

iii
DEDICATION
This dissertation is dedicated in loving memory to my paternal grandmother,
Hedwig Matthias Boebel, whose compassionate care for others, keen perceptiveness and
ability to truly listen left an indelible impression on me and to my father, Carl Paul Boebel,
a true scientist who continually serves as a pattern and inspiration for my life. Also, this
work is dedicated to my husband Louis Toly and sons Joshua and Jason for their
unwavering love and support throughout life’s journey. You are my past, present and
future!

iv
TABLE OF CONTENTS
LIST OF TABLES……………………………………………………………………..…viii LIST OF FIGURES……………………………………………………………………..…ix ACKNOWLEDGEMENTS……………………………………………………………...…x ABSTRACT…………………………………………………………………….…...….....xii CHAPTER ONE ....................................................................................................................1
Background and Significance ............................................................................................1 Statement of the Problem...................................................................................................3 Purpose of the Study ..........................................................................................................8
Research Questions ........................................................................................................9 Significance of the Study to Nursing ...............................................................................11 Theoretical Framework ....................................................................................................12
Severity of Illness.........................................................................................................22 Depressive Symptoms..................................................................................................24 Normalization...............................................................................................................25 Family Functioning ......................................................................................................28
Definition of Terms..........................................................................................................32 Assumptions.....................................................................................................................34 Relationship of this Problem to the Nursing MetaParadigm ...........................................35 Summary ..........................................................................................................................37
CHAPTER TWO – REVIEW OF LITERATURE ..............................................................39 Introduction......................................................................................................................39 Chronic Illness Within A Family Context .......................................................................40
Necessary Adjustments ................................................................................................40 Positive Gains ..............................................................................................................41 Critical Times...............................................................................................................42 Father’s Perspective .....................................................................................................42 Family Response to Chronic Illness.............................................................................43 Needs of Parents...........................................................................................................44 Unpredictability of Symptoms .....................................................................................46 Theoretical Foundations for Chronic Illness Research ................................................47 Summary of Chronic Illness Within a Family Context................................................49
Psychological Effects of Caring for a Child with Chronic Illness ...................................49 Depressive Symptoms..................................................................................................49 Depressive Symptoms in Parents of Children who are Technology Dependent .........50 Correlates of Depression..............................................................................................51 Depressive Symptoms and Severity of Illness .............................................................52 Summary of Psychological Effects on Parents of a Child with Chronic Illness..........60
The Child Who is Technology Dependent.......................................................................61 Long-Term Home Care ................................................................................................62 Coping..........................................................................................................................62 Cost ..............................................................................................................................62

v
“Mothering” Role.........................................................................................................74 Process of Care.............................................................................................................76 Effective Management Factors ....................................................................................84 Social Support ..............................................................................................................86 Home Health Care Nursing Support ............................................................................88 Lack of Discharge Preparation.....................................................................................91 Positive Gains ..............................................................................................................92 Summary ......................................................................................................................93
Normalization as a Management Strategy .......................................................................94 Definition and Attributes .............................................................................................94 Normalization Management Behaviors........................................................................96 Family Management Style Framework........................................................................98 Goals of Normalization..............................................................................................100 Effects of Normalization on Families ........................................................................101 Threats to Normalization ...........................................................................................101 Strategies to Promote Normalization .........................................................................103 Child’s Psychosocial Adjustment ..............................................................................105 Normalization and the Child who is Technology Dependent ....................................107 Summary ....................................................................................................................108
Family Functioning ........................................................................................................109 History of the Concept ...............................................................................................109 McMaster Model of Family Functioning...................................................................109 Feetham Model of Family Functioning .....................................................................110 Wright and Leahey Model of Family Functioning ....................................................111 Structure and Process of Family Functioning ............................................................112 Cultural Context of Family Functioning....................................................................113 Family Development and Family Functioning ..........................................................114 Comprehensive Definition of Family Functioning ....................................................114 Preterm Infants and Family Functioning ...................................................................115 Maternal Mental Health and Family Functioning......................................................115 Severity of Illness and Family Functioning ...............................................................117 Unpredictability of Illness and Family Functioning ..................................................117 Factors that Promote Family Functioning..................................................................117 Normalization and Family Functioning .....................................................................118 Family Functioning and Psychosocial Adjustment of the Child................................119 Summary of Family Functioning ...............................................................................120
Theoretical and Empirical Linkages ..............................................................................120 Child’s Severity of Illness and Maternal Depressive Symptoms...............................120 Severity of Illness and Normalization........................................................................122 Severity of Illness and Family Functioning ...............................................................125 Family Functioning and Maternal Depressive Symptoms.........................................127 Family Functioning and Normalization .....................................................................128 Maternal Depressive Symptoms and Family Functioning.........................................129 Maternal Depressive Symptoms and Normalization..................................................130 Summary of Conceptual Linkages .............................................................................131
CHAPTER THREE - METHODS.....................................................................................132

vi
Introduction....................................................................................................................132 Study Design ..................................................................................................................133 Sampling ........................................................................................................................134
Criteria for Selection..................................................................................................134 Recruitment of Subjects .............................................................................................135 Sample Size................................................................................................................136
Procedure for Data Collection........................................................................................138 Instruments.....................................................................................................................138
Functional Status........................................................................................................140 Level of Technology Dependency .............................................................................142 Level of Depressive Symptoms .................................................................................144 Normalization.............................................................................................................146 Family Functioning ....................................................................................................149 Demographic Characteristics .....................................................................................150
Data Management ..........................................................................................................153 Data Analysis .................................................................................................................154
Independent Variables/Covariables: ..........................................................................155 Dependent Variable:...................................................................................................155
Research Questions ........................................................................................................156 Protection of Human Rights...........................................................................................164
CHAPTER FOUR - RESULTS .........................................................................................167 Description of Participants.............................................................................................167 Children of Participants..................................................................................................171 Description of Study Variables ......................................................................................175 Description of Measurement Results for Independent/Dependent Variables ................176 Description of Caregiving Variables..............................................................................179 Preliminary Data Analysis .............................................................................................180 Testing Assumptions for Multiple Regression...............................................................181
Secondary Regression Assumptions: .........................................................................183 Research Questions and Hypothesis Testing .................................................................184
Regression Analysis – Family Functioning ...............................................................189 Testing Assumptions for Analysis of Variance (ANOVA) ...........................................191
Mediation Testing ......................................................................................................195 Multiple Regression Analysis - Normalization..........................................................203
CHAPTER FIVE - DISCUSSION.....................................................................................207 Introduction....................................................................................................................207 Summary ........................................................................................................................207 Findings..........................................................................................................................210
Characteristics of Participants....................................................................................210 Characteristics of Participant’s Children ...................................................................211 Caregiving Variables..................................................................................................212 Depressive Symptoms................................................................................................213 Normalization.............................................................................................................217 Family Functioning ....................................................................................................226 Mediator Testing ........................................................................................................228
Instruments.....................................................................................................................229

vii
Study Limitations ...........................................................................................................231 Study Implications .........................................................................................................233
Clinical Implications ..................................................................................................233 Theory Implications ...................................................................................................236 Policy Implications.....................................................................................................237
Recommendations for Future Research .........................................................................239 Conclusions....................................................................................................................241
APPENDICES ...................................................................................................................244
Appendix A Functional Status II (Revised)....................................................................244 Appendix B Level of Technology Dependency Questionnaire......................................246 Appendix C Normalization Scale ...................................................................................247 Appendix D Center for Epidemiological Studies- Depression (CES-D)........................249 Appendix E Feetham Family Functioning Survey (FFFS) ............................................250 Appendix F Demographic Questionnaire ......................................................................254 Appendix G Introductory Letter .....................................................................................257 Appendix H Telephone Script for Recruitment..............................................................258 Appendix I Resources for Mental Health......................................................................259 Appendix J Consent Form.............................................................................................260 Appendix K HIPPA Release Form .................................................................................263 REFERENCES…………………………………………………………………………...265

viii
LIST OF TABLES
Table 3.1. Empirical Indicators and Reliability Coefficient .............................................139 Table 4.1. Location of Participant Recruitment (N=103) .................................................168 Table 4.2. Descriptive Statistics – Individual Characteristics of Mothers (N=103) .........170 Table 4.3. Descriptive Statistics – Individual Characteristics of Children (N=103) ........172 Table 4.4. Number of Technologies Used ........................................................................174 Table 4.5. Descriptive Statistics – Type of Technology Used (N=103) ...........................174 Table 4.6. Means, Standard Deviations, Ranges and Skew for Major Study Variable
(N=103)......................................................................................................175 Table 4.7. Functional Status II - Revised (N=103) ...........................................................176 Table 4.8. Depressive Symptoms. Center for Epidemiological Studies – Depression Scale
(CES-D) (N=103).......................................................................................177 Table 4.9. Normalization Scale. “Actual Effect of Chronic Physical Disorder on the
Family” Subscale (N=103).........................................................................178 Table 4.10. Feetham Family Functioning Survey (N=103) ..............................................179 Table 4.11. Descriptive Statistics – Caregiving Variables (N=103).................................180 Table 4.12. Correlations Among Study Variables (N=103) .............................................184 Table 4.13. Summary of Regression Analysis for Family Functioning (N=99)...............190 Table 4.14. Means, Standard Deviations and One-Way Analysis of Variance (ANOVA)
for Three Levels of Technology Dependence and Three Dependent Variables ....................................................................................................194
Table 4.15. Mediating Effect of Depressive Symptoms between Functional Status and Normalization (N=103)..............................................................................196
Table 4.16. Mediating Effect of Depressive Symptoms between Functional Status and Family Functioning (N=101) .....................................................................198
Table 4.17. Mediating Effect of Normalization between Functional Status and Family Functioning (N=101)..................................................................................200
Table 4.18. Mediating Effect of Normalization between Depressive Symptoms and Family Functioning (N=101)..................................................................................201
Table 4.19. Summary of Regression Analysis for Normalization (N=99) .......................204

ix
LIST OF FIGURES
Figure 1.1. Family Management Style Framework ............................................................14 Figure 1.2. A conceptual model of family functioning in families with a child who is
technology dependent. .................................................................................16 Figure 1.3. Theoretical Substruction...................................................................................21 Figure 4.1. Mediating effects of depressive symptoms between functional status and
normalization .............................................................................................197 Figure 4.2. Mediating effects of depressive symptoms between functional status and
family functioning......................................................................................199 Figure 4.3. Mediating effect of normalization between functional status and family
functioning .................................................................................................200 Figure 4.4. Mediating effect of Normalization between depressive symptoms and family
functioning .................................................................................................202 Figure 5.1. Study Model for Normalization and Family Functioning in Families with a
Child who is Technology Dependent.........................................................216

x
ACKNOWLEDGEMENTS
I will be forever grateful for the guidance, encouragement and support from the
members of my dissertation committee. Each member played a significant role in helping
to build the bridge between today and tomorrow for this population of children and their
families. Dr. Carol M. Musil, the chair of my committee, served as a wise counsel
throughout the process of completing my dissertation and encouraged me to strive for
nothing less than excellence. Our thoughtful discussions regarding the conceptual pieces of
this work will not soon be forgotten. Dr. John C. Carl who has long been a real champion
for this population of children and their families was a true collaborator and helped to
demonstrate the strength that can result from interdisciplinary research. I greatly appreciate
his expertise and insight as well as his willingness to take the time out of his already busy
schedule to assist with recruitment efforts for the study. Dr. Donna A. Dowling was
instrumental in encouraging me to pursue doctoral studies and provided valuable expertise
as a pediatric nurse who had worked with this population. Dr. Susan Tullai-McGuinness
was the voice of public policy for the committee and helped to direct attention towards
potential policy changes based on the study results. Also, a thank you to Dr. Gail McCain
who provided much needed thoughtful council at the beginning of proposal development.
I would also like to acknowledge the sources of funding for this study: Alpha Mu
Chapter of Sigma Theta Tau, Frances Payne Bolton School of Nursing Alumni
Association, Society of Pediatric Nurses and the Research ShowCASE Grand Prize Award.
Each of these funding sources was instrumental in being able to conduct this study. The

xi
Dahms Clinical Research Unit (Grant UL 1RR024989) provided much needed support by
making space available for some of the participant interviews.
My deepest appreciation to the staff from the many clinics and departments at
Rainbow Babies and Children’s Hospital who enthusiastically supported this study and
assisted with identifying potential participants: Technology Dependency Clinic,
Pulmonology, Gastroenterology, Otolaryngology, Surgery, Preterm Infant Follow-up, the
Family Learning Center and the Leroy W. Matthews Cystic Fibrosis Center.
A special thank you to all of the mothers who generously gave of their time to
share their stories thereby giving a window into their world. My deepest admiration for all
of the work that they do. These special mothers are truly profiles of courage.
Finally, I would like to acknowledge and thank all of my family, friends and
colleagues who steadfastly provided encouragement and emotional support to continue
forging ahead on this adventure. I greatly appreciate the flexibility of my colleagues Linda
Boseman, Kathleen Montgomery and Dr. Sister Rita McNulty who willing switched
assignments at crucial times during the completion of my dissertation. I am deeply
indebted to my husband, Louis Toly, my mother Marilyn Boebel and my mother-in-law
and father-in-law Elisabeth and Michael Toly who many times willingly cared for my
children and other family responsibilities so that I could devote time to my studies.
Without their continued support, the completion of this goal would not have been possible.
xii
Normalization and Family Functioning in
Families with a Child who is Technology Dependent
Abstract
by
VALERIE A. BOEBEL TOLY
The purpose of this study was to examine the relationship between child/maternal
factors (child’s functional status, level of technology dependence, mother’s depressive
symptoms, length of caregiving duration, amount of home health care nursing hours, race,
family income and age of the child) and (a) family functioning, as well as (b)
normalization in families with a child who is technology dependent. Additionally, this
study examined whether there are differences in family functioning, normalization and
mother’s depressive symptoms based upon the child’s level of technology dependence
(mechanical ventilation, intravenous nutrition/medication, respiratory/nutritional support).
A descriptive, correlational design was used in this cross-sectional study. Data were
collected using the Functional Status II-Revised, Center for Epidemiological Studies-
Depression, Feetham Family Functioning Survey and a subscale of the Normalization
Scale in face-to-face interviews. Mothers of 103 children who are technology dependent
and living at home comprised the sample. The sample of mothers aged 21-66 years were
73% Caucasian and 27% women of color, who cared for their technology dependent child
aged 7 months-16 years; 73% received solely respiratory/nutritional support. Pearson

xiii
correlations revealed that greater depressive symptoms and less use of normalization were
significantly associated with poorer family functioning. In the hierarchical regression
analysis, 35% of the variance in family functioning was explained, primarily by level of
depressive symptoms. Conversely, several independent variables/covariates were found to
be significant predictors and explained 34% of the variance in normalization. Better child’s
functional status, less depressive symptoms, fewer hours of nursing care, older child and
Non-Caucasian race or Hispanic ethnicity were related to greater normalization efforts.
Statistical analyses for mediation reveal that a mother’s depressive symptoms are a
mediator between the child’s functional status and normalization. ANOVA analysis
showed no statistically significant differences in outcomes based upon the child’s level of
technology dependence. Mothers of children who are technology dependent are at high risk
for psychological distress that can affect overall family functioning. This work will be
pivotal in designing interventions to assist families in the home management of this
vulnerable and growing population of children.

1
CHAPTER ONE
Background and Significance
Technological and scientific advances over the past 20 years have increased the
survival of infants and children, particularly those born prematurely. However, the
survival of these children has resulted in a dependency on technology and home care for
continued survival (Guyer, Mac Dorman, Martin, Peters, & Strobino, 1998; Jackson Allen,
2004; Madigan, Youngblut, & Haruzivishe, 1999). Technology assists patients to resume
a more “normal” life yet paradoxically constrains them in their daily lives (Sandelowski,
1993) and results in adverse consequences for the child and family related to social-
emotional, economic and care burdens (Kuster, Badr, Chang, Wuerker, & Benjamin, 2004;
Wang & Barnard, 2004). Additionally, the technology dependency and the chronic
illnesses of these children have a profound impact on the educational and health care
systems (Newacheck & Halfon, 1998).
The Office of Technology Assessment (1987) estimated that 11,000 to 68,000
children, dependent on technology such as mechanical ventilation, intravenous total
parenteral nutrition, respiratory or nutritional support and apnea monitors were receiving
home care in the United States. Subsequent to that report, between 1988 and 1996, there
was an eight-fold growth in home health care due not only to the aged population, but to
technological improvement which saved the lives of infants and children (Madigan, et al.,
1999). Therefore, the number of children dependent on technology and receiving home
care has exponentially increased over the last 20 years.

2
There are no current estimates of the number of children who are technology
dependent in the United States today. One survey conducted in 2002 and 2003, randomly
sampled 478 children who were participating in the State of Ohio Home Care/Transitions
Waiver Program. This survey provided projections of children under the age 18 years who
were dependent on technology such as mechanical ventilation, intravenous total parenteral
nutrition and respiratory or nutritional support. Findings include that approximately 38%
of these children or 910 of the 2,395 children participating in the State of Ohio Home
Care/Transitions, were classified as dependent on the aforementioned technology (Personal
communication, J. Nickel, Ohio Department of Jobs and Family Services, December 2,
2004). In another survey, a total of 1,914 children (0.22%) receiving Medicaid in North
Carolina were classified as medically fragile, technology dependent (Buescher, Whitmire,
Brunssen, & Kluttz-Hile, 2006). These surveys, when compared to the OTA estimate from
1987, support the notion that the population of children who are technology dependent has
increased exponentially over the last 20 years.
Equally compelling as the increase in number of children who are technology
dependent is the fact that a disproportionate amount of health care dollars are being
relegated to the care of children with special health care needs. Children who are
technology dependent comprise the high cost segment of children with special health care
needs due to the expenses related to their technological equipment, treatment, therapies and
home health care and hospitalization. Although children with special health care needs
comprise only 15.6% of all children under the age of 18 years, they accounted for 42.1% of
the medical expenditures (excluding dental) in 2000 (Newacheck & Kim, 2005). Children
with special health care needs had statistically significant more physician visits and non-

3
physician visits, medications, and out of pocket costs than other children (p=<.01)
(Newacheck & Kim, 2005). For example, one study found that medically fragile,
technology dependent children receiving Medicaid had medical expenditures of $69,906
per child as compared with $3,181 for a healthy, typically developing child receiving well
child care (Buescher et al., 2006).
Statement of the Problem
Families experience a tremendous cost burden related to at-home care for a child
who is technology dependent. This cost burden includes lost time, social isolation,
increased monetary expenditures, and a toll on psychological health. Furthermore, families
who bring their child who is technology dependent home following hospitalization
undergo major lifestyle changes that can effect family functioning.
Cost Burdens of Caring for a Child who is Technology Dependent at Home
Time
One major factor in the cost burden, is the tremendous amount of time parents often
need to spend providing technical care and administering a variety of treatments, unless the
child has 24-hour home nursing care. Time required for the care and the multitude of
treatments necessary to sustain the child who is technology dependent is daunting
(Heyman et al., 2004; Kirk & Glendinning2004; Wilson, Morse, & Penrod, 1998), and
requires considerably more time than given to healthy children or children who are
chronically ill but not technology dependent. Beyond the time required for technical
treatments, much time is required to manage practical issues related to having a child who
is dependent on technology such as dealing with insurance companies, ordering supplies
and the increased time required to pack necessary supplies for an outing (Torok, 2001).The

4
time factor also includes lost time for family, work, leisure and social activities (Kuster et
al., 2004; Neuss, 2004; Miller Rice, DeVoe, & Fos, 1998; O’Brien, 2001; Torok, 2001).
Social Isolation
Social isolation is another great cost burden related to caring for a child who is
technology dependent at home (Boland & Sims, 1996; Carnevale, Alexander, Daves,
Rennick, & Troini, 2006; Kirk, 2004; Neuss, 2004; O’Brien, 2001; Wang & Barnard,
2004). Frequently, the life of the caregiver, who is in most cases the mother, revolves
around the technology and the necessary care routines. Friends are noted to withdraw;
there is less contact with work colleagues and extended family and fewer social outings
(Boland & Sims, 1996; Kirk & Glendinning, 2004; Tommet, 2003). Often mothers of
children who are technology dependent, experience loneliness and a sense that their lives
are on hold (Neuss, 2004). Many report a lack of available respite care (Carnevale et al.,
2006; Heaton Noyes, Sloper, & Shah, 2005; Kirk, 2004).
Not only do families of children who are technology dependent encounter social
isolation as a cost burden, most families also face exorbitant expenses due to the fact that
not all of the medical bills for medicines, supplies, physician visits, and home health care
are covered by insurance (Newacheck & Kim, 2005). Additional expenditures that
families incur are due to increased use of electricity, heat, telephone, insurance, and
laundry, as well as travel (Kirk & Glendinning, 2004; Glendinning, Kirk, Guiffrida, &
Lawton, 2001). Economic costs also include lost income; often times in a dual income
family, one of the parents, typically the mother, is compelled to quit their job in order to
manage the demands of coordinating all of the visits to physicians, and therapists, and to

5
provide the technical care for the child (Case-Smith, 2004; Miller et al., 1998). Frequently,
there are other siblings as well as other household demands, in addition to the child who is
technology dependent, that make it a necessity for one parent to be a stay-at-home parent.
Often, to make up for the lost income, the working parent must take on a second job or
work overtime (Cavanagh, 1999; Miller et al., 1998; Case-Smith, 2004). Therefore,
economic hardships that the majority of families of children who are technology dependent
face, place increased hardship, worry and strain on families that can potentially effect
family functioning.
Psychological Distress
Psychological distress, another cost burden, is prevalent in parents of children who
are technology dependent. In as many as 75% of families, one or both parents experienced
distress symptoms, suggesting a possible need for psychological intervention (Leonard,
Brust, & Nelson, 1993). Cavanagh (1999) found that about half of caregivers of children
who are technology dependent experienced depressive symptoms that required either
counseling or antidepressant medication. In a longitudinal study of 67 mothers of preterm
infants who were technology dependent, Miles, Holditch-Davis, Burchinal, and Nelson
(1999) found that 45% at discharge and 36% at 12 months had Center for Epidemiological
Studies- Depression (CES-D) scores above 16, indicating risk for depression. Therefore,
research indicates that a large percentage of parents of children who are technology
dependent have significant depressive symptoms and are at risk for clinical depression.
While research indicates that a high percentage of parents of children who are
technology dependent are at risk for depression, it is also important to note the correlates
of depression. Extensive research conducted regarding depression in parents of children

6
with chronic illness, found overwhelming evidence that a key correlate of depression is
functional limitations in the chronically ill child (Silver, Westbrook, & Stein, 1998; Silver,
Bauman, & Ireys, 1995; Frankel & Wambolt, 1998; Lustig, Ireys, Sills, & Walsh, 1996;
Weiss & Chen, 2002). Children who are technology dependent have a variety of
functional limitations that require increased care and monitoring thus contributing to the
findings related to increased incidence of depression in these parents. Other correlates of
depression in these parents, according to the research, are decreased resources (Silver, et
al., 1995), decreased family income (Drotar, Agle, Eckl, & Thompson, 1997; Canning,
Harris, & Kelleher, 1996; Shore, Austin, Huster, & Dunn, 2002), increased number of
health care visits (Ireys & Silver, 1996), unpredictability of symptoms and need to watch
for sudden changes in condition (Ireys & Silver, 1996), and mother unemployed outside
the home (Thyen, Kuhlthau, & Perrin, 1999). Each of these correlates of depression,
described in past research, is present in the lives of parents of children who are technology
dependent. Thus, it is not surprising that such a large percentage of these parents have or
are at risk for significant depression.
In addition to the toll that caring for a child who is technology dependent takes on
psychological health, mothers also face major lifestyle changes that can effect family
functioning. Living with a child is technology dependent also means living with
uncertainty and unpredictability in their lives—described as “living in a house of cards”
(O’Brien, 2001). Loss of privacy, another lifestyle change, is frequently an issue for
families whose child receives pediatric home health care as numerous health care providers
enter and leave the family home at all times of the day disrupting the typical family routine
and dynamics (Cohen, 1999; Koblen, Beier, & Danzer, 2000; Lee, 1996; Murphy, 1997;

7
O’Brien & Wegner, 2002; Torok, 2001; Wang & Barnard, 2004). Additional problems
encountered by parents with a child who is technology dependent are housing adaptations
that must be made in order to accommodate the necessary care equipment (permanent
modifications such as an of addition to house or making a first floor room a mini-ICU)
(Kirk, Glendinning & Callery, 2005). Other modifications include changes in family goals
and activities, modified school experiences and strained family relationships (Kiernan,
1995; Neuss, 2004; Torok, 2001; O’Brien, 2001; Kirk & Glendinning, 2004; Allen,
Simone, & Wingenback, 1994).
There is a dearth of quantitative research studies that have examined the impact of
technology dependency on children living at home, on their families and on society. The
majority of studies have used qualitative methodology. Home care for children who are
technology dependent is encouraged as the result of anticipated cost savings by managed
care in the United States and universal health care plans in the United Kingdom and
Australia (OTA, 1987; Wang & Barnard, 2004). However, the lack of research provides
little evidence for guiding home health care or for establishing effective and efficient
social, fiscal and health care policies. Additionally, there is a lack of evidence regarding
how to improve the lives of children who are technology dependent and their families once
they are discharged home. This information is vitally important for maintaining the mental
health of caregivers as well as positive family functioning.
The Principal Investigator became interested in how families of children who are
technology dependent manage once they are discharged home while working as a pediatric
home health care nurse. This experience led to observations that families who were most
successful providing home care for their child easily integrated the child into family life,

8
normalizing their day to day experience despite all the challenges of the technology and
increased medical care needs, whereas other families struggled with the identical
challenges. The role of families in a child’s adjustment to illness is of paramount
importance. The entire family, as well as individual family members are impacted by the
presence of a child who is technology dependent (Knafl, Breitmayer, Gallo, & Zoeller,
1996). Children who are chronically ill as well as technology dependent create unique,
special challenges for families because they require considerable amounts of time and care.
Nurses are best suited to assist these families by enabling and empowering families to
function optimally in the management of the child who is technology dependent by
identifying and augmenting family strengths.
Purpose of the Study
The purpose of this study was to explore how mothers respond to and manage the
special challenges of children who are technology dependent after they are discharged
from the hospital to home. This descriptive, correlational study explored the relationship
between child/maternal factors (child’s functional status, level of technology dependence,
mother’s depressive symptoms, length of caregiving duration, amount of home health care
nursing hours, race, family income and age of the child) and (a) family functioning as well
as (b) normalization (how a family manages both family life and the child’s complex
medical needs/treatments) in families with a child who is technology dependent.
Additionally, this study examined whether there are differences in family functioning,
normalization and mother’s depressive symptoms based upon the child’s level of
technology dependence (Group 1 mechanical ventilation, Group 2 intravenous

9
nutrition/medication, Group 3 respiratory/nutritional support) using the Office of
Technology Assessment (1987) rubric.
No quantitative research could be located that examined efforts at normalization
and family functioning as reported by mothers with children who are technology
dependent. More research is needed to examine the relationships among child’s severity of
illness, mother’s depressive symptoms, normalization and the resultant impact on family
functioning in mothers of children who are technology dependent after adjusting for
caregiving duration, amount of home health care nursing hours, income, race and age of
the child who is technology dependent. This research is an essential foundation for the
design of effective interventions to assist families in the home management of this
vulnerable and growing population of children.
The long term goals of this study are threefold; to provide evidence to guide
pediatric home health care nursing practice, to provide evidence for intervention
development that would promote healthy outcomes for the family and ill child alike and, to
provide evidence to guide policy development for the child who is technology dependent
in the United States.
Research Questions
Five research questions will be addressed in this study:
1a. What are the relationships of mother’s depressive symptoms, child’s
severity of illness (functional severity and level of technology dependence)
and normalization efforts, with family functioning in families with a child
who is technology dependent? 1b. Do these relationships hold after
adjusting for length of caregiving duration, amount of home health care

10
nursing hours, race, family income and age of the child who is dependent on
technology? (Correlation Matrix, Multiple Regression)- F statistic
2. Are there differences in a) family functioning and b) normalization efforts
and c) mother’s level of depressive symptoms based on the child’s level of
technology dependence (3 levels)? (MANOVA)-F statistic
3. Do a mother’s depressive symptoms have a mediating effect on the
relationship between the child’s severity of illness (functional status) and
(a) normalization and (b) family functioning in mothers with a child who is
technology dependent? (Correlation Matrix, Mediation using
Hierarchical Multiple Regression)-F statistic
4. Does normalization have a mediating effect on the relationship between (a)
child’s severity of illness (functional status) and family functioning, (b)
depressive symptoms and family functioning in mothers with a child who is
technology dependent? (Correlation Matrix, Mediation using
Hierarchical Multiple Regression)-F statistic
5 a. What are the relationships among mother’s depressive symptoms, child’s
severity of illness (functional status, level of technology dependence),
family functioning on normalization efforts in families with a child who is
technology dependent? 5b. Do these relationships hold after adjusting for
length of caregiving duration, amount of home health care nursing hours,
race, family income and age of the child who is dependent on technology?
(Correlation Matrix, Multiple Regression)- F statistic

11
Significance of the Study to Nursing
Children who become dependent on technology are a significant concern for
nursing and society in general. According to Newacheck and Halfon (1998), a medical
disability profoundly impacts the child, the educational system, and the health care system.
This phenomenon is of particular significance to nursing not only due to its impact on the
child who is technology dependent but on the family as a whole. In 1994, registered
nurses were responsible for 73.2% of the pediatric home health care visits (Madigan et al.,
1999). As such, nurses interface in the home with families of children with complex health
care needs. Furthermore, children requiring home health care are often technology
dependent and cared for by their families who are then at significant risk for psychological
distress (Leonard et al., 1993). For example, preterm infants who are technology
dependent, particularly those with depressed mothers, are at risk for altered parent-child
interaction with possible deleterious effects on cognitive development (Miles et al., 1999).
Families often require assistance in the day to day management of the child’s
chronic condition. Nurses, therefore, are well situated to assist these families in the
management process once the child who is technology dependent is discharged from the
hospital to home. One way that nurses can best help these families is by enabling and
empowering families to function optimally in the management of the child who is
technology dependent by identifying and augmenting family strengths.
To date, the preponderance of studies regarding parents of children who are
technology dependent have used qualitative methodology. Few studies, using quantitative
methodology, have addressed how the family responds to and manages the special
challenges of a chronically ill child who is dependent on technology. Furthermore, no

12
studies have been located that have addressed the use of normalization within the Family
Management Style Framework (Knafl & Deatrick, 2003) as a means to assess which
families with a child who is technology dependent, are at greatest risk for dysfunction.
Additionally, no studies have simultaneously examined both depressive symptoms and
normalization as they relate to mothers of children who are technology dependent. The
study proposed here will address these gaps by systematically assessing the response of
mothers to the experience of caring for a child who is technology dependent.
Theoretical Framework
The orienting framework guiding this study is the Family Management Style
Framework developed by Knafl and Deatrick (2003) (Figure 1.1). The Family
Management Style Framework “describes how a family manages both family life and a
child’s serious health problems” (Deatrick et al., 2006, p. 20), in essence, how the “family
incorporates the demands of childhood illness into family life” (Knafl & Deatrick, 2003, p.
234) and how the family as a unit consistently responds to a child’s chronic illness
(Deatrick et al., 2006). The framework considers patterns of family management in a
systematic manner and allows for the planning of individualized care for families based on
their type of family management style. This study explored how the severity of a child’s
chronic illness (functional severity and level of technology dependence), mother’s
depressive symptoms, and efforts at normalization impact family functioning. The family
management styles reflect varying degrees of normalization used by families and are
impacted by a combination of the family’s definition of the situation, management
behaviors, and perceived consequences as well as relate to such outcomes as individual

13
functioning (depressive symptoms) and family functioning (Deatrick et al., 2006), some of
the concepts that are included in this study.
Most families who have children with serious illnesses eventually view their
children and their lives as normal and manage the illness-related demands successfully
(Deatrick et al., 2006). However, not all families see their lives as normal, and those who
do reach this point often use a variety of strategies over time as they undergo a continual
process of adjustment. The Family Management Style Framework describes ways families
define and manage illness-related demands and the resultant consequences for family life
(Deatrick et al., 2006). “Within the Family Management Style Framework, the general
issues/dimensions common to all families compose the major interacting dimensions of the
model. These dimensions or components include how family members define and manage
their situation, as well as what consequences they perceive for family life” (Deatrick et al.,
2006, p. 20).
The Family Management Style Framework is comprised of three components that
include the following (Figure 1.1): 1) definition of the situation, or the identification of
significant events and the subjective meaning family members attribute to the child’s
identity (normal and capable versus tragic and vulnerable), illness view (life goes on versus
serious/hateful), parent mutuality (shared versus different views of the illness and illness
management) and management mindset (ease or difficulty with treatment regimens); 2)
management behaviors or the behavioral accommodations made by family members to
manage on a daily basis such as the parenting philosophy (parent’s goals, priorities, and
values that guide the approach and strategies for illness management), and management
approach (parent’s assessment of development of a routine and strategies for managing the

14
illness and incorporating the illness into family life) and 3) perceived consequences or
whether the illness is in the foreground or background in family life such as the family
focus (balance between illness management and other aspects of family life) and future
expectations (parental assessment of illness implications for child’s/family’s future) (Knafl
& Deatrick, 2003; Deatrick et al., 2006). All three components of the Family Management
Style Framework; definition of the situation, management behaviors and perceived
consequences comprise a pattern of family response (Family Management Style) to a
child’s chronic illness and explicates how families incorporate the illness into family life
(Knafl & Deatrick, 2003).
Figure 1.1. Family Management Style Framework
The Family Management Style Framework also includes socio-cultural context.
The socio-cultural context are family members’ perceptions of contextual factors that
influence how the family defines and manages the illness, as well as any consequences the

15
family perceives the illness has; in other words, perceived influences on the family’s
management of the chronically ill child (Deatrick et al., 2006). Examples of contextual
factors include cultural practices and beliefs, as well as finances, personal/individual
factors, the health care provider’s level of support or the supportiveness of the health care
system (Deatrick et al., 2006). Therefore, The Family Management Style Framework takes
a holistic view of how the family manages family life as well as the child’s chronic illness
including the family’s definition of the situation, management behaviors, perceived
consequences and the socio-cultural context.
The Family Management Style Framework has guided a number of previous
studies of children with chronic conditions such as cancer, diabetes, asthma, cystic fibrosis,
juvenile rheumatoid arthritis, gastrointestinal and renal conditions and ventilator
dependence (Knafl & Deatrick, 2003) however all used qualitative methodology with the
exception of Murphy (1994) and Fleming et al. (1994). There is currently no tool available
to measure family management styles nor is there any model that depicts this study’s
identified concepts as well as their relationships; therefore, it was necessary for the purpose
of this study to develop a new conceptual framework (Figure 1.2). This conceptual
framework is based on a synthesis of the theoretical and empirical literature and
specifically incorporates theoretical underpinnings from several sources; the Family
Management Style Framework (Knafl & Deatrick, 2003), the Normalization Scale
(Murphy, 1994) and Feetham’s conceptualization of family functioning (Roberts &
Feetham, 1982).
The Family Management Style Framework (Knafl & Deatrick, 2006) (Figure 1.1)
was used as an orienting framework because it provides perspective on the idea of


17
These goals help to direct the efforts that will be used to manage the child’s illness
and ultimately affects their use of normalization and thus the Family Management Style
employed (Murphy, 1994). These management behaviors are another major component of
the Family Management Style Framework.
Therefore, a parent’s response to a chronically ill child who is technology
dependent is shaped in large part by their definition of the situation. A mother’s depressive
symptoms and the child’s severity of illness (functional severity, level of technology
dependence) (Figure 1.2) affect their definition of the situation and perceived
consequences and thus management behaviors, ultimately affecting normalization efforts.
Finally, as depicted in the Family Management Style Framework (Figure 1.1)
normalization efforts affect family functioning, an outcome.
In summary, parents who showed high emotional distress such as an increased
number of depressive symptoms have reported that the child’s illness is disruptive and had
a major impact on family life (Frankel & Wamboldt, 1998). Depressive symptoms,
therefore, can affect a mother’s definition of the situation, one of the major components of
the Family Management Style Framework that helps determine normalization efforts in a
Family Management Style and ultimately affects family functioning. Additionally,
according to the proposed theoretical framework, the severity of a child’s illness also
affects a mother’s definition of the situation, influence normalization efforts (Murphy,
1994) and ultimately impact family functioning (Frankel & Wamboldt, 1998).
The Normalization Scale (Murphy & Gottlieb, 1992) also influenced the conceptual
framework and was chosen for this study as it is currently the only instrument available to
quantitatively measure normalization. This instrument was primarily derived from

18
attributes of normalization as conceptualized by Knafl and Deatrick (1990). Items for this
scale were developed based on the original conceptualizations of Knafl and Deatrick that
includes four domains of normalization: 1) acknowledgement of the existence of the
impairment; 2) definition of family life as normal i. e. parents define and perceive their
child/family as similar to families without a chronically ill child, the child’s health
treatments are integrated into family life, the child with a chronic illness and their health
treatments are not the central focus of the family; 3) family minimizes the social
consequences of their situation i. e. parents perceive that others define their child and
family as basically normal, others treat the family and chronically ill child as normal; 4)
family engages in behaviors that demonstrate the family’s normality i. e. the family carries
out activities to demonstrate to others that their family behaves and acts like other families
who do not have a chronically ill child.
The conceptual model guiding Murphy’s (1994) study included the Family
Management Style Framework. Questions from the Normalization Scale reflect the major
components (definition of the situation, perceived consequences, management behaviors)
of the Family Management Style Framework. Therefore, the Normalization Scale (Murphy
& Gottlieb, 1992) is guided by the conceptualizations of normalization and the Family
Management Style Framework by Knafl and Deatrick (1990) and is congruent with the
concept of normalization that will be examined in this study.
The conceptual framework for this study also draws from Feetham’s
conceptualization of family functioning (Roberts & Feetham, 1982). Until the Feetham
Family Functioning Survey (FFFS) was developed, measures of family functioning only
addressed the relationship between individual members of the family such as the

19
parent/child or husband/wife. However, family functioning is greater than the
relationships between the immediate family members. Feetham identified and measured
two additional relationship aspects of family functions: the relationship between the family
and subsystems (relatives, friends and neighbors) and the relationship between the family
and the broader community (schools and place of employment) (Roberts & Feetham,
1982). Thus, the FFFS assesses intra-family relationships, relationships between the family
and external social units and the functional task-oriented subsystems of the family.
Feetham’s work drew from the family ecological framework (Bronfenbrenner,
1993) that identifies the family as the basic unit and includes the nested parts that make up
the system, the family’s relationships, the environment and the tasks performed by the
family resulting from the relationships of the parts. Central to Bronfenbrener’s ecological
framework is a view of development as an evolving process of development as an evolving
process of organism-environment interaction. The family system is thus dynamic and
continually in a state of change and adaptation whereby change in one layer ripples
throughout and affects the other layers i.e. subsystems and the broader community
(Paquette & Ryan, 2001). Therefore, Feetham’s conceptualization of family functioning
influenced the view of family functioning for this conceptual framework, particularly her
belief that the family system is dynamic, in a continual state of change and adaptation and
can be affected by all the subsystems with which the family interacts.
Based on a synthesis of the theoretical and empirical literature, the Family
Management Style Framework (Figure 1.1), the Normalization Scale (Murphy, 1994) and
Feetham’s conceptualizations of family functioning, this study proposed (Figure 1.2) that
the child’s severity of illness, mother’s depressive symptoms and the efforts at

20
normalization all directly affect family functioning. It is also proposed that there is a direct
correlation between child’s severity of illness (functional status and level of technology
dependence), in particular functional status, and mother’s depressive symptoms (Canning,
Harris, & Keller, 1996; Lustig et al., 1996; Silver et al., 1995; Silver et al., 1998; Frankel
& Wamboldt, 1998; Weiss & Chen, 2002). The child’s severity of illness, which includes
the child’s functional status and level of technology dependence, affects the mother’s level
of depressive symptoms, and is hypothesized to have direct effects on normalization efforts
and family functioning. Mother’s depressive symptoms are conceptualized as a mediator
between child’s severity of illness and family functioning as well as a mediator between
child’s severity of illness and normalization.
Normalization is proposed to mediate the relationship between child’s severity of
illness and family functioning as well as mother’s depressive symptoms and family
functioning. It is hypothesized that greater severity of the child’s illness, greater depressive
symptoms in mothers will result in lower levels of normalization. Lower levels of
normalization are hypothesized to result in poorer family functioning. Knafl and Deatrick
(2003) conjecture that normalization effort is antecedent to family functioning outcomes as
depicted in Figure 1.1. Normalization differs from family functioning conceptually
because it does not include the inter-relationship between the family and the subsystems
(relatives, friends and neighbors) or community (Figure 1.3). Additionally, normalization
differs from family functioning because it presupposes that there is an alteration in health.
Figure 1.3 provides a theoretical substruction of constructs, concepts, variables in the
theoretical system as well as the empirical indicators and scores/values for the operational
system in this study.

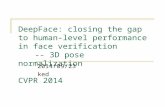
Theoretical
System Constructs Child’s Health Mother’s Mental
Health Family Management
Concepts
Severity of Illness
Depressive Symptoms
Normalization Family
Functioning
Variables
Technology Functional Dependence Severity
Level of Depressive Symptoms
Level of Satisfaction Normalization with Relationships
Operational System
Empirical Indicators
Level of Functional Technology Status II (R) Dependence OTA Groups (1987)
CES-D
Normalization Feetham Family Scale Functioning Survey
Scores/ Values
Nominal Interval
Interval
Interval Interval
Figure 1.3. Theoretical Substruction
21

22
Severity of Illness
While the main model guiding this study is the Family Management Style
Framework, the underpinnings of the theoretical framework come from a variety of
sources. The first concept in this study, the child’s severity of illness, is based on work
by Stein et al. (1987). The concept of severity of illness is challenging to quantify,
according to Stein et al. (1987), because clinical manifestations of an alteration in health
are an interaction between biological, genetic and environmental components. Illness
severity includes physiological severity, functional severity, technology dependence, and
burden of illness however, in this study, only two will be examined; functional severity
and technology dependence.
Functional Severity
Functional severity, which reflects the direct effect of an alteration in health on a
person, is the effect of a chronic health condition on the child’s ability to perform age-
appropriate daily life activities (Stein et al., 1987). Functional severity is manifestations
of a chronic health condition that interfere with a child’s performance of the full range of
age-appropriate behaviors such as communication, mobility, energy, play, sleep, eating
and toileting pattern (Stein et al., 1987). It is hypothesized that functional severity will
affect mother’s depression, normalization, and family functioning. Few studies
examining the impact of caring for a child who is technology dependent on parents have
used a standardized instrument to measure functional severity (Kuster et al., 2004;
Heyman et al., 2004). Most studies have used unstandardized measures with no reported
reliability, or those developed for adults (Leonard et al., 1993; Patterson, Leonard &
Titus, 1992; Teague et al., 1993; Miles et al., 1999). The Functional Status II-Revised

23
(FSII-R) was used in this study because it was specifically developed to assess the health
status of children with chronic illness. This revised instrument was developed using
children with significant chronic illness, as well as children with and without ongoing
health conditions. Therefore, use of a standardized instrument to measure functional
severity will strengthen the findings regarding relationships found between the variables.
Technology Dependence
Technology dependence is defined as the “short-or long-term reliance on devices
and techniques to evaluate or to satisfy or resolve health-related needs or problems”
(Sandelowski, 1993, p. 37). The Office of Technology Assessment (1987) provides
further detail in its definition of technology dependence. Their definition includes the
need of “substantial and ongoing nursing care to avert death or further disability. This
definition is independent of the setting of care or the particular credentials of the
caregiver” (p. 3) and may be provided by either a professional nurse, a trained parent or
trained lay caregiver (OTA, 1987). Children, who are technology dependent, have one or
more chronic illnesses and frequently have functional limitations that can be considered a
disability. The term, children who are technology dependent, encompasses those children
who are chronically ill, technology dependent and possibly disabled.
Technology dependence is hypothesized in this study to affect mother’s
depression, normalization, and family functioning. Few quantitative studies have closely
examined these variables together. One study by Fleming et al. (1994), found that
depression did not vary significantly among the four groups of technology dependence as
delineated by the Office of Technology Assessment (OTA, 1987). A study by Leonard
and colleagues (1993), concur with these findings that there were no statistically

24
significant differences in parental scores for psychological distress among the four groups
of technology dependence (OTA, 1987). Miles et al. (1999) did not find any difference
in the correlation between level of technology dependence and maternal depressive
symptoms, however a newly developed tool to measure technology dependence was
used.
Most studies used the OTA (1987) rubric to define four groups of technology
dependence based on the types of technological equipment used (Fleming et al., 1994;
Leonard et al., 1993). However, Miles et al. (1999) developed a tool that examined not
only the level of technology dependence but the acuity of the child as well as the burden
of caregiving. This scale is published only as part of a grant report; the psychometric
properties are not published in the literature. This scale used the OTA (1987) rubric for
technology as a guide and added technologies as well as 10 categories of medications.
Depressive Symptoms
An important factor related to the impact of a child’s illness on the family may be
the general emotional health and stability of the parents, especially the mother. Mothers’
functioning seems to impact the general functioning of other members of the family
(Frankel & Wamboldt, 1998). How sick the child actually is and how much a family’s
lifestyle is limited by the disease affects a parent’s perception of the illness’ and therefore
impacts family functioning (Frankel & Wamboldt, 1998). Parents who showed high
emotional distress reported that the child’s illness is disruptive and had a major impact on
family life (Frankel & Wamboldt, 1998). Therefore, emotional distress in the form of
depressive symptoms and severity of illness, more specifically, functional severity and

25
technology dependence, play an important role in perception of impact of illness on
family functioning.
As alluded to above, a mother’s depressive symptoms are hypothesized to directly
effect normalization and family functioning. The concept of depression is an alteration in
mental health that results from ineffective responses by the person to changes in the
environment (Foreman, 1997). Depression refers to a range of symptoms from a
subclinical “blue mood” state and general feelings of hopelessness to a major depressive
disorder (Foreman, 1997). The depressive symptoms then represent dimensions of the
concept of depression, and include depressed mood, feelings of guilt and worthlessness,
helplessness and hopelessness, psychomotor retardation, loss of appetite and sleep
disturbance (Radloff, 1977). Many studies examining the level of depressive symptoms
among parents of children who are technology dependent used the Center for
Epidemiological Studies- Depression Scale (CES-D) (Fleming et al., 1994; Miles et al.,
1999; Teague et al., 1993; Heyman et al., 2004; Kuster, 2002). Miles et al. (1999) found
that mothers with decreased satisfaction with family (family functioning) using the
Family Apgar Scale had higher levels of depressive symptoms (p=<.05) on the CES-D.
The CES-D will be used in this study because it was specifically designed to measure
depressive symptoms in the general population, it is quick and easy to administer and
therefore well suited for use with mothers who have children who are technology
dependent.
Normalization
Normalization is a concept that was developed and refined by Knafl, Deatrick and
colleagues since the 1980s (Deatrick, Knafl, & Murphy-Moore, 1999; Knafl & Deatrick,

26
1986; Knafl & Deatrick 2003) and is the foundational concept of the Family Management
Style Framework (Deatrick et al., 2006). Normalization includes cognitive and
behavioral dimensions and is defined as a pattern of family response to a child with a
chronic illness, an ongoing process of accommodating to the child’s evolving social,
emotional and physical needs (Deatrick, Knafl & Walsh, 1988; Morse, Wilson & Penrod,
2000). This includes “adjusting the environment to provide normal life experiences that
will meet the child’s evolving social, physical, intellectual and emotional needs”
(Murphy, 1994, p. 10) while at the same time managing family life and activities so that
they can lead as close to “normal” family life as possible (Murphy, 1994). Attributes of
normalization include that a family “(a) acknowledges the condition and its potential to
threaten their lifestyle, (b) adopts a ‘normalcy lens’ for defining the child and family, (c)
engages in parenting behaviors and family routines that are consistent with ‘normalcy
lens’, (d) develops a treatment regimen that is consistent with a ‘normalcy lens’, and (e)
interacts with others based on a view of child and family as normal” (Deatrick et al.,
1999, p. 211).
Therefore, based on the above attributes of normalization, a family’s definition of
“normal” is guided by a philosophical approach and not necessarily the reality of the
situation, primarily because parents choose to attend to what is “normal” and disregard
what is abnormal about their situation (Murphy, 1994). Families, therefore, modify and
redefine “normal” over time to fit their current circumstances and ongoing uncertainty
(Rehm & Franck, 2000). Consequently, the child with a chronic illness, or in the case of
this study, the child who is technology dependent, is treated as “normal”, living as close a
life like others in the outside world without illness so as not to be seen as deviant from
societal expectations; thus enabling them to “fit in” (Morse et al., 2000; Young, 1995).

27
Therefore, reality is reconstructed (“normalcy lens”) to emphasize those aspects of life
that remain unchanged despite the chronic illness. In conclusion, normalization is used to
manage the disparity between the preferred views of their family life as “normal” and the
problems and challenges they face in their everyday life (Rehm & Franck, 2000).
Qualitative studies of families with children who have a chronic illness, have
found that “families often come to view their child and their lives as normal. They
manage illness-related demands using family management styles that sustain usual
patterns of family and child functioning” (Deatrick et al., 2006, p. 19). Therefore,
families’ efforts at normalization have much to do with family functioning. In a
triangulated study of families of children with chronic conditions, Knafl and Zoeller
(2000) found an association among family management styles and family functioning
using the Feetham Family Functioning Survey. Families who used the Floundering
Family Management Style, the lowest level of normalization, had significantly less
satisfaction with family life (poorer family functioning) than families using the other
styles with higher levels of normalization (Knafl & Zoeller, 2000).
Paterson’s “Shifting Perspectives Model of Chronic Illness” (2001) also guided
this study’s conceptualization regarding the presence of a chronic illness in a family
member and their subsequent efforts at normalization. This model is also reflected in the
Family Management Style Framework particularly in one of the major components,
perceived consequences. Paterson’s Model (2001) posits that living with a chronic illness
is an ongoing, continually shifting process that includes an individual’s or family’s ever
changing perspectives about the disease including elements of wellness and illness.
Living life with chronic illness is an ongoing, continually shifting process whereby
illness or wellness-in-the foreground perspectives have specific functions. This model

28
helps explain variations in attention to symptoms over time. Furthermore, in this model,
perception of reality is how the individual with chronic illness and family members
interpret and respond to illness.
An illness-in-the-foreground perspective of chronic illness focuses on sickness,
loss, burden and suffering. The chronic illness is viewed as destructive to self and others
and individuals are absorbed by the illness experience. In a wellness-in-the-foreground
perspective, chronic illness is viewed as an opportunity for a change in relationship with
the environment and others. The fact that some describe their health as good or excellent
despite impaired physical functioning is not distortion of reality, but rather, revisioning of
what is possible and “normal” (Paterson, 2001). This model also fits well with views
held in the Family Management Style Framework regarding perspective in one of the
dimensions “definition of the situation” and helps to explain how families develop the
“normalcy lens” as described in the attributes of normalization.
Family Functioning
The final component of this model is the outcome variable of family functioning.
In this study, it is hypothesized that a child’s severity of illness, mother’s depressive
symptoms and efforts at normalization will effect family functioning. Clawson (1996)
examined children with chronic illness following discharge from the hospital. These
children are cared for by their families at home, placing increased demands on the family
due to the numerous treatments, health care appointments and disruptions in the every
day routine. This disruption requires a substantive change in the structure and
functioning of the family frequently requiring a redistribution of responsibilities and roles
(Clawson, 1996) ultimately affecting family functioning.

29
The concept of family functioning was greatly influenced by Roberts and
Feetham’s (1982) work. When initially developed in the 1950s, the concept of family
functioning and the ensuing McMaster Model of Family Functioning had structural-
functional theory as its base. It placed emphasis on the family meeting member’s
physical and psychological needs of food, clothing and socialization. It also emphasized
family structure, relationships, and organization as well as transactional patterns
(Goldenberg & Goldenberg, 1991).
Suzanne Feetham extended the work on the concept of family functioning in the
1970’s and developed The Feetham Family Functioning Survey (FFFS). According to
Feetham, family functioning refers to “those activities and relationships among and
between persons and the environment which in combination enable the family to
maintain itself as an open system” (Roberts & Feetham, 1982, p. 231). Her contributions
to the concept of family functioning was the inclusion of the family ecological
framework (Bronfenbrenner, 1979), general systems theory and Duvall’s model of family
development.
The family ecological framework identifies the family as the basic unit, and
includes the nested parts that make up the system, the family’s relationships, the
environment, and the tasks performed by the family resulting from the relationships of
the parts. The focus of the ecological framework is the interdependence of family
members with the environment and with one another. According to the ecological
framework, the family system is dynamic and continually in a state of change and
adaptation. Change in one layer ripples throughout the other layers. Layers or subsystems
of the ecological framework include microsystems (family, child care environment,
school), the relations between the individual and his or her immediate setting,

30
mesosystems (connects structures such as parents and teachers), the relations among
various settings in which the individual is involved, exosystem (larger social system that
is an extension of the mesosystem such as the mass media, government agencies,
educational or employment systems that influence microsystems) and macrosystem
(cultural, economic, social, political philosophy that influence other layers)
(Bronfenbrenner, 1993; Paquette & Ryan, 2001).
There is some overlap in the theories used for the concept of family functioning in
the FFFS. The structural-functional theory, family ecological framework and general
systems theory all use systems theory as its base. Duvall’s family development model
intersects with systems theory due to the fact that each family is a system where “the
whole is greater than the sum of its parts” (von Bertlannfy, 1968). In summary, the FFFS
is based on the McMaster Model of Family Functioning and includes components of
structural-functional theory, general systems theory, the family ecological framework and
Duvall’s model of family development.
Until the FFFS was developed, measures of family functioning only addressed the
relationship between individual members of the family such as the parent/child or
husband/wife. Feetham’s work influenced the view of family functioning for this study
because family functioning is greater than the relationships between the immediate
family members. Feetham identified and measured two additional relationship aspects of
family functions: the relationship between the family and subsystems (relatives, friends
and neighbors) and the relationship between the family and the broader community
(schools and place of employment).
The FFFS will be used in this study because it measures the parent’s perception
and level of satisfaction with relationships between individuals in the family, the family

31
and subsystems and between the family and the community. While this instrument was
designed to be administered to either parent, the mother was chosen to be the participant
because she is most often the primary caregiver and also typically accompanies the child
to clinic visits and would therefore be more accessible for recruitment purposes. This
measure is optimal because it uses the Porter Format (Roberts & Feetham, 1982) that
allows for a measurement of a discrepancy score between achieved and expected levels
of family functioning. The discrepancy score is the critical measure of overall family
functioning (Hock-Long, 1997) and will be used to conduct statistical analysis in this
study. The Porter format also decreases the risk of social desirability and controls for
cultural and ethnic diversity since each item is valued by the participant. An importance
score is also obtained along with the discrepancy score, and can be used to gain insight as
to the importance of particular aspects of family functioning (Roberts & Feetham, 1982).
The FFFS is also the optimal measure to use because it was developed for and
first tested on parents who had a child with myelomeningocele, a chronic condition that
involves long term, complex care. Children with myelomeningocele require a variety of
treatments that is somewhat similar to, but not as complex, in most cases, as children who
are technology dependent and generally not life-threatening. The FFFS was used in a
prior study of mothers with children who were dependent on mechanical ventilation
(Hock-Long, 1997).
Theoretically, family functioning can be viewed as a process that can be measured
at a particular point in time. Bauman (2000) described family functioning as a
phenomenon related to the reciprocity between the family and illness/wellness that is
linked with family structure and process. A description of activities related to family
functioning suggests that family functioning is a process. The process-based view of

32
family functioning includes a broad range of behaviors and implies an inter-relationship
between the individual and the family and the individual and the environment. These
behaviors have been described as those activities that are essential to family survival such
as socialization, protection, procreation, education and economic concerns (Roberts &
Feetham, 1982).
Definition of Terms
The conceptual and operational definitions for the study variables are as follows:
Functional Severity
Conceptual definition: the effect of a chronic health condition on the child’s
ability to perform age-appropriate behaviors, daily life activities and is applicable where
multiple conditions coexist (Stein et al., 1987).
Operational definition: behavioral manifestations of illness that interfere with a
child’s performance of the full range of age appropriate activities such as communication,
mood, energy, play, sleep, and eating patterns as measured by the Functional Status II-
Revised (Stein & Jessop, 1990).
Technology Dependence
Conceptual definition: “short-or long-term reliance on devices and techniques to
evaluate or to satisfy or resolve health-related needs or problems” (Sandelowski, 1993, p.
37) and includes the need of “substantial and ongoing nursing care to avert death or
further disability...independent of the setting of care or particular credentials of the
caregiver” (OTA, 1987, p. 3) and may be provided by either a professional nurse, a
trained parent or trained lay caregiver (OTA, 1987).

33
Operational definition: The level of technology necessary to satisfy or resolve
health-related needs or problems as categorized by the Office of Technology Assessment
(OTA, 1987): Group 1: children dependent at least part of the day on mechanical
ventilation; Group 2: children requiring prolonged intravenous administration of
nutritional substance or medications; Group 3: children requiring daily device-based
respiratory or nutritional support. Group 4: children with prolonged dependence on other
medical devices such as apnea monitors, urinary catheters. Groups are designed to be
mutually exclusive, however, if the child requires technology from more than one group,
he/she is considered as part of the applicable group with the lowest number (OTA, 1987).
Level of Depressive Symptoms
Conceptual definition: an alteration in mental health state that results from
ineffective responses to change in the environment based on negative appraisal of
internal/external stimuli. Symptoms can range in magnitude from a mild subclinical
“blue mood” state and general feelings of hopelessness to a major depressive disorder
(Foreman, 1997; Clark, Beck, & Alford, 1999).
Operational definition: current level of depressive symptomatology, including
depressed mood, feelings of guilt and worthlessness, helplessness and hopelessness,
psychomotor retardation, loss of appetite and sleep disturbance with emphasis on the
affective component as measured by the Center for Epidemiologic Studies Depression
Scale (CES-D) (Radloff, 1977).
Level of Normalization
Conceptual definition: a way that families respond to and manage a child with a
chronic condition. It is a process that families use over time that redefines what “normal”

34
is to fit their current circumstances (Rehm & Franck, 2000). Normalization includes
cognitive and behavioral dimensions and “adjusting the environment to provide normal
life experiences that will meet the child’s evolving social, physical, intellectual and
emotional needs” (Murphy, 1994, p. 10).
Operational definition: the adjustment families make over time when they have a
child who is technology dependent to manage family life and activities so that they can
lead as close to “normal” of a family life as possible as measured by the “Actual Effect of
the Chronic Physical Condition on the Family” subscale of the Normalization Scale
(Murphy & Gottlieb, 1992).
Family Functioning
Conceptual definition: an ongoing, dynamic process that changes with
developmental stages and crisis events and is comprised of inter-relationships and inter-
dependent parts, is influenced by cultural context, member’s expectations and perceptions
and has the goal of balancing equilibrium and disequilibrium such that individual and
family growth can occur and health is promoted (Toly, 2003).
Operational definition: parent’s perception and level of satisfaction with
relationships between the family and individuals, the family and subsystems and between
the family and the community as measured by the Feetham Family Functioning Survey
(Roberts & Feetham, 1982).
Assumptions
An assumption of this proposed study is that the child who is technology
dependent will stimulate the normalization process to begin and that the mother will find
the long term care of her child to be a chronic strain.

35
Relationship of this Problem to the Nursing MetaParadigm
The nursing metaparadigm is concerned with person, health, nursing and
environment. In this study, the concept of person is represented by the family. The role of
families in a child’s adjustment to a chronic illness is of paramount importance. The
entire family, not just individual family members are impacted by the presence of a child
who is technology dependent (Knafl, Breitmayer, Gallo, & Zoeller, 1996). Children who
are chronically ill as well as technology dependent create unique, special challenges for
families because they require considerable amounts of time and care. Technology assists
patients to resume a more “normal” life, yet, paradoxically constrains them in their daily
lives (Sandelowski, 1993) and results in increased physical, social-emotional, economic
and care burdens for the child and their families (Kuster et al., 2004; Wang & Barnard,
2004).
Bringing the child who is technology dependent home changes family functioning
due to the increased care demands placed on families. The discharge of a child who is
technology dependent may result in individual and family growth or to system
dysfunction, lack of homeostasis and possible physical and mental demise of the
members (Clawson, 1996; Miles et al., 1999).
Closely associated with family functioning is the concept of normalization.
Normalization is defined as how the family as a unit consistently responds to a child’s
chronic condition, taking into account the configuration of responses of individual
members. Normalization is comprised of definition of the situation, management
behaviors, and perceived consequences (Knafl & Deatrick, 2003). It differs conceptually
from family functioning in that it does not include the interrelationships of the family
with the other layers of the environment such as the school, community, society and

36
culture. Additionally, normalization differs from family functioning because it
presupposes that there is an alteration in health.
Research indicates that the home environment is better than an institutional
environment because of the positive effects on a child’s emotional, developmental and
social growth as well as improved health (Kuster, 2002; Murphy, 1994; O’ Brien, 2001;
Wang & Barnard, 2004). Benefits of bringing the child home for the family include less
disruption and expense related to travel to the hospital, missed work, absences from the
typically developing siblings and costs incurred with hospitalization (Miller et al., 1998).
Families however, who bring the child who is technology dependent home must
often modify the family home in order to accommodate the extra equipment and supplies
and to allow home health care providers a more convenient access to the child who is
technology dependent as well as to allow the family to monitor the child’s condition
throughout the day. Modifications may be as simple as turning a first floor room into the
child’s room—a mini ICU or may require more extensive modifications in the form of
home additions, wheel chair ramps and more. Bringing the child who is technology
dependent home also means changes for the family’s home environment, most notably
the loss of privacy that typically comes with visits by home health care providers. Some
children who are technology dependent may require up to 24 hours of skilled nursing care
in the home which changes family dynamics. In addition to home health care providers,
extended family members and friends may be more frequent visitors to the family home
to assist with instrumental tasks thereby changing the typical dynamics of the home.
Although this is frequently seen as welcomed help, it comes at a cost of family privacy
and a disruption to inter-personal relationships among family members.

37
Therefore, the identified research problem directly relates to the nursing
metaparadigm. Children who are chronically ill as well as technology dependent create
unique, special challenges for families because they require considerable amounts of time
and care. While the home environment is optimal in terms of a child’s emotional,
developmental and social growth as well as improved health, families frequently incur
high cost burdens. Nurses are best suited to assist these families when they are discharged
home by enabling and empowering families to function optimally in the management of
the child who is technology dependent by identifying and augmenting family strengths.
Summary
In summary, the purpose of this study was to explore how parents respond to and
manage the special challenges of a child who is technology dependent following
discharge from the hospital to home. This descriptive, correlational study explored the
relationship between child/maternal factors (child’s functional status, level of technology
dependence, mother’s depressive symptoms, length of caregiving duration, amount of
home health care nursing hours, race, family income and age of the child) and (a) family
functioning as well as (b) normalization in families with a child who is technology
dependent. The following study questions were addressed:
1a. What are the relationships of mother’s depressive symptoms, child’s
severity of illness (functional severity and level of technology
dependence) and normalization efforts, with family functioning in families
with a child who is technology dependent? 1b. Do these relationships hold
after adjusting for length of caregiving duration, amount of home health
care nursing hours, race, family income and age of the child who is

38
dependent on technology? (Correlation Matrix, Multiple Regression)-
F statistic
2. Are there differences in a) family functioning and b) normalization efforts
and c) mother’s level of depressive symptoms based on the child’s level of
technology dependence (3 levels)? (MANOVA)-F statistic
3. Do a mother’s depressive symptoms have a mediating effect on the
relationship between the child’s severity of illness (functional status) and
(a) normalization and (b) family functioning in mothers with a child who
is technology dependent? (Correlation Matrix, Mediation using
Hierarchical Multiple Regression)-F statistic
4. Does normalization have a mediating effect on the relationship between
(a) child’s severity of illness (functional status) and family functioning, (b)
depressive symptoms and family functioning in mothers with a child who
is technology dependent? (Correlation Matrix, Mediation using
Hierarchical Multiple Regression)-F statistic
5 a. What are the relationships among mother’s depressive symptoms, child’s
severity of illness (functional status, level of technology dependence),
family functioning on normalization efforts in families with a child who is
technology dependent? 5b. Do these relationships hold after adjusting for
length of caregiving duration, amount of home health care nursing hours,
race, family income and age of the child who is dependent on technology?
(Correlation Matrix, Multiple Regression)- F statistic

39
CHAPTER TWO – REVIEW OF LITERATURE
Introduction
Children with a chronic illness and their parents, particularly mothers, have been
examined extensively in the literature. Within the last 10 years, more focus has been
devoted in the literature to a segment of this population known as children with special
health care needs. Although children with special health needs comprise only 15.6% of
children under the age of 18 years, they accounted for 42.1% of the medical expenditures
(excluding dental) in 2000 (Newacheck & Kim, 2005). A large portion of these children
with special health care needs are technology dependent due to the technologic and
scientific advances over the past 20 years (Guyer et al., 1998; Jackson Allen, 2004;
Newacheck & Kim, 2005). Although technology assists patients to lead a more “normal”
life it also paradoxically constrains them in their daily lives (Sandelowski, 1993) and
results in adverse consequences for the child and family related to physical, social-
emotional, economic and care burdens (Kuster et al., 2004; Wang & Barnard, 2004).
As the trend toward the use of pediatric home care is increasing (Madigan et al.,
1999) there has been a corresponding increase in the number of studies regarding the
family impact of caring for a chronically ill child at home. Concomitantly, there has been
an increase in literature written over the last 10 years regarding children who are
technology dependent and their families. The following review includes studies of
parents of children with chronic conditions, particularly children who are technology
dependent. Studies in this review of the literature report the psychosocial effects on
parents as well as their needs and concerns. The review of literature is presented in four

40
sections: (a) chronic illness within a family context; (b) psychological effects of caring
for a child who is technology dependent on parents; (c) normalization as a management
strategy for families; and (d) family functioning.
Chronic Illness Within A Family Context
Stein (1992) defined chronic conditions in children as conditions that will produce
long-term sequelae such as dependency on medications or a specialized diet for normal
functioning or control of a chronic condition, disfigurement, limitation of functions more
than those expected for the child’s age and development, dependence on medical
technology for body functions, need for medical care/services more than usual for the
child’s age or special ongoing treatment at home or school. Much research has been
conducted regarding children with chronic illness. Some studies examined the effects of
chronic illness on parents, children or both. Researchers studied children with specific
chronic illnesses while others used a non-categorical approach and included
children/parents with various chronic illnesses. Studies regarding chronic illness in
children have been influenced by research on chronic illness in adults.
Necessary Adjustments
Changes and adjustments that take place in the lives of families when a child is
diagnosed with a chronic illness are numerous and have been studied extensively in the
literature. These numerous changes may include a change in career to allow more time
for caregiving (Case-Smith, 2004) or in some cases, the need to quit work altogether
(Case-Smith, 2004; Thyen, Terres, Yazdgerdi, & Perrrin, 1998), the need to take on
second or even third jobs by the working parent to help make ends meet (Case-Smith,
2004), an increase in the time needed for planning activities outside the home (Case-

41
Smith, 2004), cancellation of activities due to unpredictable symptoms (Dodgson et al,
2000) or feeling a need to always be there with the child (Case-Smith, 2004). Parents also
experience a change in their social lives as they frequently find maintaining a social life a
challenge due to the fact that friends and relatives don’t understand limitations placed on
them related to the child’s illness care needs (Case-Smith, 2004). Additionally, parents
may experience trouble building friendships because of a loss of experience with
socialization (Case-Smith, 2004). Adaptation responses range across a continuum from
optimal to ineffective (Clawson, 1996). Adaptive tasks including instrumental, emotional
components and growth responses are used to manage chronic illness with the goal of
satisfaction, approval and success with later tasks (Clawson, 1996). Therefore, many
parents of children with chronic illness experience a multitude of changes and
adjustments in their work and social life in order to care for their child.
Positive Gains
Positive gains experienced by parents are also noted in the literature. Due to their
experience with chronic illness in their child, parents frequently become an advocate for
the child/others (Case-Smith, 2004; Paterson, 2001), and experience personal growth
(Clawson, 1996; Chernoff, List, DeVet, & Ireys, 2001), increased family cohesion (Case-
Smith, 2004), decreased family conflict (Knafl & Gillis, 2002), greater appreciation of
life (Paterson, 2001; Case-Smith, 2004), and acquire a sensitivity and tolerance of
individual differences (Paterson, 2001; Case-Smith, 2004).
One study exemplifies the positive gains that parents of children with chronic
illness experience. In a study of 190 mothers of children 7-11 years with a chronic illness,
Chernoff and colleagues (2001), found that 88% felt better about themselves because

42
they learned to manage their child’s chronic illness, 70% thought their family was
stronger and 80% felt the family benefited in some way from having a child with a
chronic illness. Those mothers with an educational level of High School graduate or less
were more likely to report feeling better about the management of a child with a chronic
illness than those who finished college (p=<.05). Therefore, research has shown that for
some parents, particularly those with less education, effectively managing the care of a
chronically ill child has led to positive gains such as a sense of personal pride and
growth. Additionally, parents of children with chronic illness have reported that there
family is stronger and have benefited in a positive way from having a child with a chronic
illness.
Critical Times
Critical times in the chronic illness trajectory were also noted in the literature.
Times of particular disequilibrium include the time of diagnosis, or when the child
experiences increased physical symptoms, has an increase in physical care needs,
ominous physical health changes or rehospitalization (Clements, Copeland, & Loftus,
1990). Furthermore, new developmental needs in the child create a trigger point for
increased uncertainty for parents (Dodgson et al., 2000).
Father’s Perspective
While most studies of children with chronic illness have included mothers, a few
have included fathers as the major focus of study. In one such study conducted in Israel,
Katz and Krulik (1999) compared 80 fathers of children with chronic illness age 6
months-7 years who were receiving some type of daily treatment to 80 fathers of age
matched healthy children. Findings include that fathers of chronically ill children

43
experience a greater number of stressful life events (personal events p=<.05; stressful
family/social events p=<.001) and were more likely to have feelings of lower self-esteem
(p=<.005) than fathers of healthy children. The researchers found a positive correlation
between self-esteem and social support in fathers of chronically ill children. Both groups
however, had decreased marital satisfaction with increased life events (p=<.001). No
differences were found between fathers of chronically ill children and those with healthy
children on marital satisfaction and involvement in the care of the child. Important
findings in this study are that fathers with a greater number of stressful life events or less
satisfaction with social support were identified as a high risk group.
Family Response to Chronic Illness
Other literature focused on the family’s response to a member’s chronic illness. In
a meta-analysis and synthesis of current research regarding families and chronic illness,
Knafl and Gillis (2002), focused on the family’s response to a member’s chronic illness
as well as the contribution of the family to a member’s response to chronic illness. A total
of 66% of the articles were descriptive studies (48 articles reporting on 38 studies) of
family life in the context of a chronic illness. Findings from this synthesis of descriptive
studies include that the process of family adaptation to illness includes rising to the
challenge and gaining positive meaning and incorporating illness management into every
day routine so that every day life assumes a taken-for-granted quality. Furthermore,
families construct their own subjective illness meanings and develop strategies for
managing the chronic illness, as well as learn to master treatment and incorporate illness
management into everyday family life. Mastery and routine were found to be important
aspects of family life (Knafl & Gillis, 2002). The remaining 34% of studies were

44
explanatory (25 articles; 24 studies). Stress was most frequently studied in these
explanatory articles. Major findings from these articles include that few stressors are
consistently associated with better functioning. Gaps include the need to look at the
family’s response related to chronic illness, the role of health care professionals in
shaping the family illness response, and the development of nursing interventions to
address family strengths and weaknesses. Another crucial research gap according to
Knafl and Gillis (2002) was the identification of variables that are linked with levels of
individual/family functioning. Finally, another research gap was identification of
different patterns of response to illness so that interventions can be developed and tested
(Knafl & Gillis, 2002).
Needs of Parents
Literature related to chronic illness in children also identified needs of parents in
caring for these children. Specific needs identified by parents of children with chronic
illness include the need for professional support. Pelletier, Godin, Lepage, and Dussault
(1994) found that parents have a need to share personal feelings and worries about their
child as well a need to be encouraged and praised for their ability to care for their child.
Other needs of parents of chronically ill children addressed in the literature include the
combination of personal guidance and good quality information in the form of booklets
or concise directories using plain and simple terms that are accurate, up to date, and easy
to read (Mitchell & Sloper, 2002). Parents reported that information would be most
helpful at key times such as diagnosis, the start of school and at puberty.
Literature regarding families of children with chronic illness also examined unmet
needs. One study examined the unmet needs identified by 83 caregivers of chronically

45
children ages .2-17.4 years many of whom were preterm and had more than one diagnosis
(Farmer, Marien, Clark, Sherman, & Selva 2004). The researchers found that the
caregivers wanted more information about services and the best way to promote their
child’s health and development, as well as caregiver supports, community services and
help with family relationships and financial concerns. A total of 87% were happy with
the health care services their child received but were concerned with the lack of mental
health services for themselves. Another, 52% wanted help with care coordination.
Interestingly, there was a significant difference (p=<.03) in the number of unmet needs
related to ethnicity, with Caucasians reporting fewer unmet needs when compared to
families of other races/ethnicity. Social support and appraisal of family burden were
significant predictors of unmet needs. Additionally, the number of unmet needs also
varied somewhat by complexity of the child’s illness. The researchers concluded that
with adequate professional and informal community support, families are able to access
more resources, and as a consequence functioned more effectively, thereby promoting
health in the child while at the same time decreasing overall family needs (Farmer et al.,
2004). Additional findings were that a mother’s increased personal strain and burden
interferes with a mother’s ability to access necessary services and supports that
subsequently has a negative effect on child and family outcomes. Appraisals of the
impact of the child on the family were thought to be associated with the mother’s
depression. In conclusion, the researchers proposed that caregivers may benefit from
psychosocial interventions in primary care to increase social support and positive
appraisals of the impact of the child on the family. Additionally, an intervention that
would include dissemination of information regarding how the condition affects growth

46
and development, how to support learning and social integration, self care for caregivers
and how to support siblings would be greatly beneficial (Farmer et al., 2004).
Unpredictability of Symptoms
Parents of children with chronic illness not only identified unmet needs as
troublesome but often find the unpredictability of the child’s symptoms very challenging
as well. In a study of 173 mothers and 150 fathers of young children 12-30 months
diagnosed with a chronic physical health impairment within the past year, Dodgson et al.,
(2000) examined the effect of predictability of symptoms and the degree of certainty in
life expectancy on the level of family distress. A majority of those studied lived in two
parent homes, had an average family size of four and were Caucasian. Instruments used
in the study were the Impact on Family Scale, Characteristics of Chronic Condition
Questionnaire, and the Function Status II-Revised (FS II-R). Dodgson et al. (2000) found
that parents of children who had intermittently unpredictable symptoms experienced
significantly more family distress than those with more predictable symptoms. On the
other hand, there was no difference between mothers and fathers as to uncertain life
expectancy and family distress. For mothers and fathers, unpredictable symptoms was
significantly associated with increased family and social disruption, (p=.001) and
(p=.002) respectively. Unpredictable symptoms were also associated with emotional
strain (p=.001) and financial burden (p=>.008) for mothers (Dodgson et al., 2000). The
researchers concluded that parents of children with unpredictable symptoms are at
increased risk for negative outcomes.

47
Theoretical Foundations for Chronic Illness Research
Research regarding chronic illness in children has also drawn from foundations of
research regarding chronic illness in adults. Twenty years of research regarding chronic
illness in adults was examined by Thorne and Paterson (2000). The researchers found
commonalities and variations in chronic illness experiences but found little research that
included culturally/ethnically diverse groups. Thorne et al. (2002) found that most studies
used white, educated, middle class females. Gaps in the research include lack of diversity
in age, gender, socio-economic status, and ethnicity, outlook on life or geographical
location. In conclusion, gaps and therefore the limitations of prior research are that it has
mostly been studied in isolation from sociocultural and psychological factors that may
impact the chronic illness experience (Thorne et al., 2002).
Thorne and Paterson (2000) examined the sociocultural and psychological factors
associated with the experience of chronic illness in adults. They proposed that chronic
illness is often experienced in an uneven trajectory. At times, the disease is put in the
background of consciousness and other times it is overwhelmingly significant and
dominates daily life. Shifts in perspective are due therefore to personal and sociocultural
factors (Thorne & Paterson, 2000). Paterson's (2001) model, “Shifting Perspectives
Model of Chronic Illness” proposes that living life with chronic illness is an ongoing,
continually shifting process whereby illness or wellness-in-the-foreground perspectives
have specific functions for the chronically ill child/family. This model helps explain
variations in attention to symptoms over time and was derived from a metastudy of 292
qualitative research articles related to chronic physical illness published from 1980-1996.
Previously, researchers proposed that individuals with chronic illness follow a predictable
trajectory and implied that an end goal exists. The Shifting Perspectives Model posits that

48
living with a chronic illness is an ongoing, continually shifting process that includes the
individual’s ever-changing perspectives about their disease including elements of both
illness and wellness. As the illness experience, as well as personal and social context
changes, a corresponding shift occurs in the degree that illness shifts to the foreground or
background of their “world”. Perception of reality is how individuals with chronic illness
and family members interpret and respond to their illness (Paterson, 2001).
In an illness-in-the-foreground-perspective of chronic illness, the individual
focuses on sickness, loss, burden and suffering (Paterson, 2001). The chronic illness is
viewed as destructive to self/others and individuals are absorbed by the illness
experience. In a wellness-in-the-foreground perspective, chronic illness is appraised as an
opportunity for a change in their relationship with the environment and others. There is
congruence between self-identity, identity created by the disease, construction of illness
by other individuals/family members and life events. The fact that some individuals
describe their health as good or excellent despite impaired physical function is not a
distortion of reality, but rather, re-visioning of what is possible and normal (Paterson,
2001).
Shifts in perspective related to health for individuals with chronic illness may
occur for various reasons. A major factor in shifts from wellness to illness-in-the-
foreground is threats to the individual’s control. Threats may include signs of disease
progression, lack of skill in disease management, and interactions with health care
providers that emphasize hopelessness and dependence. On the other hand, a shift from
illness to wellness-in-the-foreground includes the ability of the individual to “bounce
back” with renewed hope and optimism when the individual identifies the need to return
to wellness or chooses to focus attention away from illness (Paterson, 2001).

49
Summary of Chronic Illness Within a Family Context
In summary, literature related to chronic illness within a family context has
addressed changes and adjustments in the lives of caregiver and families, positive gains
experienced by parents of these children, critical time periods in the illness trajectory,
needs/unmet needs of parents who are caring for chronically ill children and
predictability of the child’s symptoms and its relationship with family distress. The
Shifting Perspectives Model by Paterson (2001) was originally developed to help
elucidate the life of an adult with chronic illness but is apropos for children with chronic
illness and their families. This model proposes that chronic illness is experienced as an
uneven trajectory regarding the emphasis placed of the chronic illness in daily life. At
times the disease shifts from the background to the foreground of consciousness and vice
versa depending on a variety of factors such as disease progression or exacerbation and
disease management. Gaps related to research of chronic illness in children within a
family context include a lack of culturally/ethnically diverse participants in research
studies as well as a dearth of studies regarding the sociocultural/psychological factors
related to chronic illness, family response to chronic illness, the role of health care
professionals in shaping family illness response, variables linked with individual and
family functioning and development of nursing interventions to address family strengths
and weaknesses.
Psychological Effects of Caring for a Child with Chronic Illness
Depressive Symptoms
The literature regarding chronic illness in children has described the existence of
depressive symptoms in mothers of children with chronic illness and its relationship with

50
other variables. Many researchers studied the concept of depressive symptoms in parents
of preterm infants. Thompson, Oehler, Catlett, and Johndrow (1993) studied 90 mothers
of very low birthweight infants and found that rates of significant maternal psychological
distress varied over time from 48% at birth, 33% at 3 to 6 weeks postpartum, and up to
41% at 6 months corrected age as measured by the Symptom Checklist-90-Revised. This
instrument has excellent reliability and includes symptoms related to anxiety and
depression. Over time, mothers perceived less stress related to the infant but more stress
related to daily hassles, less family support and more conflict. Miles et al. (1999) in a
longitudinal study of 67 mothers of medically fragile, technology dependent, preterm
infants found that 45% at discharge and 36% at 12 months had Center for
Epidemiological Studies- Depression Scale (CES-D) scores above 16, indicating risk for
depression. Variables significantly related to an increase in depressive symptoms were
lower educational level, lower mastery, higher satisfaction with family, and more worry
about the child’s health (Miles et al., 1999). Therefore, studies of mothers of preterm,
medically fragile infants have found significant levels of psychological distress indicating
a risk for depression.
Depressive Symptoms in Parents of Children who are Technology Dependent
Research has also been conducted regarding depressive symptoms in parents of
children who are technology dependent. Significant findings include that in 75% of
families, one or both parents experienced distress symptoms indicating need for
psychological intervention (Leonard et al., 1993). Cavanagh (1999) found that six of 13
primary caregivers of children who are technology dependent had experienced depressive
symptoms that required either counseling or antidepressant medication. Fleming et al.

51
(1994) found that depression did not vary significantly among the four groups of
technology dependence established by the Office of Technology Assessment (OTA,
1987). Teague et al (1993) found that higher CES-D scores correlated with higher means
of the Family Inventory of Life Events and Changes (FILE) family stress subscales of
intra-family strains and marital stress. Therefore, studies of parents with children who are
technology dependent found significant levels of depressive symptoms in a large
percentage of participants that indicated a need for psychological intervention regardless
of the type of technology that the children were dependent on.
Correlates of Depression
Many studies have been conducted to investigate the correlates of depression in
the parents of children with chronic illnesses. Correlates of depression include functional
limitations in the chronically ill child (Silver et al., 1995; Silver et al., 1998; Frankel &
Wamboldt, 1998; Lustig et al., 1996; Weiss & Chen, 2002), decreased resources (Silver,
et al., 1995), decreased self esteem (Silver et al., 1995), low maternal self-efficacy (Silver
et al., 1995), decreased family income (Drotar et al., 1997; Canning et al., 1996; Shore et
al., 2002), decreased satisfaction with family relationships (Shore et al., 2002; Weiss &
Chen, 2002), increased child behavior problems (Shore et al., 2002), mother’s negative
perception of chronically ill child’s impact on the family(Ireys & Silver, 1996), increased
number of health care visits (Ireys & Silver, 1996), unpredictability of symptoms and
need to watch for sudden changes in condition (Ireys & Silver, 1996), increased anxiety
in the chronically ill child (Frankel & Wamboldt, 1998), maternal role restriction (Silver,
Bauman, & Weiss, 1999), lack of family support (Thyen et al., 1998), low social support
appraisal (Thyen et al., 1998), mother unemployed outside the home (Thyen et al., 1999),

52
young age of caregiver (Canning et al., 1996), perception of increased burden by
caregiver (Canning et al., 1996), unresponsiveness of the chronically ill child (Weiss &
Chen, 2002), increased life stress (Weiss & Chen, 2002), decreased perceived emotional
support (Weiss & Chen, 2002), decreased family cohesion (Weiss & Chen, 2002), and
the lack of a partner in the home (Weiss & Chen, 2002).
Many of the studies related to psychological distress included large sample sizes
with a variety of chronic illnesses. Although many of the studies used the term mental
distress, most were specific at some point in the article to mention depression. A majority
of the studies used mostly Caucasian subjects with the exception of Silver et al. (1995),
Ireys and Silver (1996), and Weiss and Chen (2002). Therefore, a major gap in research
regarding the correlates of depression in parents of children with chronic illness is that
the samples lacked racial diversity thus affecting generalizability of the studies.
Depressive Symptoms and Severity of Illness
Some studies examined the relationship between maternal depression and the
child’s severity of illness (Affleck, 1987; Affleck, Tennen, Rowe, & Higgins, 1990;
Miles, et al., 1999; Thompson, et al., 1993). Miles et al. (1999) found no significant
relationship between CES-D scores and severity of illness as measured by level of
technology dependence and multisystem diagnosis at discharge and 12 months after birth.
However, no reliability and validity data were reported for the tool that measured the
child’s disease acuity. Thompson et al. (1993) had similar findings but used birth weight,
gestational age and the Neurobiologic Risk Score to measure severity of illness. The
instrument was reported to be strongly predictive of developmental outcome however no
reliability was reported. Affleck et al. (1987) also found no significant relationship with

53
depression however rough estimates of severity of illness were used such as length of
hospital stay, gestational age at birth and perinatal complications. Affleck and colleagues
(1990), in a study of 94 mothers of preterm infants, also found no relationship between
severity of illness and depression as measured by the Profile of Mood States at discharge
and 6 months later. The literature therefore reports no significant relationship between the
mother’s level of depression and severity of illness in the chronically ill child. However,
a variety of instruments were used that were either un-standardized or had poor reliability
ratings.
Functional limitations were implicated as the major contributor to psychological
distress in parents and were for the most part measured via the Function Status II-Revised
(FS II-R) developed by Stein and Jessop (1990). Since the FS II-R is an instrument that
requires the parent to answer questions regarding the chronically ill child’s health, Dadds,
Stein and Silver (1995) conducted a study of 365 mothers of children 5-9 years old with a
chronic condition to examine whether a mother’s own mental health effected her
perceptions of the child’s health and general behavioral adjustment. The researchers
concluded that the FS II-R is not influenced by the mother’s psychological adjustment.
Researchers explored the correlates of psychological distress to ascertain if the
strongest relationship was severity of illness or, more specifically, functional status
limitations. Canning et al. (1996) in a study of 116 children age 9-18 years found that
when family income, gender, caregiver age were controlled, the child’s functional
limitation predicted increased caregiver distress while reported severity of illness did not.
Additionally, Canning et al. (1996) found that caregiver burden was a significant
predictor of a caregiver’s mental distress (p=<.01) using the Brief Symptom Inventory
For Caregivers. Theyen et al. (1998) proposed that functional disability is a greater factor

54
in family management of the chronic condition more than disease severity because it
describes the child’s ability to perform activities of daily living and participate in family
life, play, and school.
Lustig and colleagues (1996) conversely, found that both biological and
functional limitations accounted for nearly half of the variance of maternal mental health.
In this study, a total of 53% of mothers scored in the high range of depressive symptoms
using the Psychiatric Symptom Index (PSI). The child’s functional status was found to
have both direct and mediated associations with maternal mental health. It is thought the
mothers have increased responsibility for the ill child and may consequently experience
increased distress when the child’s functional status declines. Furthermore, it is proposed
that greater maternal demands increases the burden on emotional and financial resources
needed to meet other family task and may lead to mental health problems (Lustig et al.,
1996). The researchers also found that maternal appraisal of impact of child’s illness on
the family partially mediated effects of the child’s functional status on maternal mental
health (Lustig et al., 1996). It is important to note however that although the findings are
different than that of all other research, it was conducted on only 53 mothers from a
pediatric rheumatology clinic.
Further studies regarding the correlates of psychological distress in parents of
children with chronic illness also examined the amount of family resources and the
presence of role restriction. Silver et al. (1995) studied 365 low income, urban dwelling
mothers of children 5-9 years of age with diverse chronic illnesses to examine the extent
of maternal mental distress using the Psychiatric Symptom Index (PSI). Using multiple
regression to control for sociodemographics, the researchers found that functional
limitations in the chronically ill child as measured by the FS II-R and decreased family

55
resources were associated with increased psychiatric symptoms. In a later article
regarding the same study, Silver et al. (1999) examined role restriction (role strain such
as inability to pursue other interests or social activity due to parental demands) using the
Parenting Stress Index Form. Findings include that in a multiple regression model,
functional limitations predicted maternal depression. Furthermore, adding role restriction
to this model significantly increased explained variance in maternal depression scores
indicating that role restriction is directly related to a mother’s distress symptoms even
when other sociodemographic variables were controlled. High role restriction was related
to lower level of education, no other adult in the home, decreased social support,
mother’s own health, work status, receipt of welfare, and number of children in the home.
The conclusion of this study was that functional limitations and increased role restriction
were independently related to maternal depression (Silver et al., 1999).
In a subsequent study to further investigate parental mental health issues, Silver et
al. (1998) used random digit dialing to conduct a telephone survey of parent’s self-
reported distress related to their child’s chronic illness in 380 inner city parents and 398
parents from a population based national sample. The researchers administered the PSI
instrument to parents whose child had a chronic illness longer than one year to examine
the intensity of 29 common psychiatric symptoms in the parents and frequency over the
previous two weeks. The highest mean PSI scores were found in a sub-group of parents
whose child had functional limitations particularly for the national sample. A post-hoc
analysis of the data showed that the pattern continued even when parent gender, child age
and family income were controlled using analysis of covariance (ANCOVA). Increased
parental distress was equal in both mothers and fathers of children with functional
limitations. Interestingly, post-hoc analysis of the inner-city sample showed that having

56
any chronic health condition not just functional limitation was related to parental distress
(Silver et al., 1998). Therefore, functional limitations particularly for those living in inner
city areas were significantly related to increased parental psychiatric symptoms.
Ireys and Silver (1996) conducted a longitudinal study at 3 data points over 18
months to examine correlates of mental health in 169 mothers of children 5-8 years of
age with a chronic illness. The sample was demographically quite diverse with 46%
Hispanic, 32% Caucasian, 49% on welfare and 50% in two parent households. Findings
include that there is a mediating role of perception processes on mental health. A
mother’s perception of impact of the illness attenuated the relationship between the
number of hospitalizations and the mother’s mental health. Demographics, type of illness
and service use were found to be unrelated to a mother’s mental health and modestly
related to mother’s perception of illness impact on the family at one year. The researchers
concluded that how a mother perceives events such as hospitalization plays a role in how
she functions psychologically. Additionally, the authors proposed that uncertainty or
unpredictability of symptoms effects appraisal by reducing perceived control over the
condition course and outcome. Furthermore, they proposed that the reason increased
service use was linked to increased mental health symptoms was that visits can be
disruptive and may be a marker for mothers who have more difficulty responding to
challenges inherent with caring for a chronically ill child (Ireys & Silver, 1996).
In another study examining the correlates of depression, Thyen et al. (1998)
studied 65 mothers of children who were technology dependent and a control group of 54
mothers of children who were hospitalized for acute illness 6 months following
discharge. Instruments used in this study included the SF-36 to assess physical and
mental health concepts, the CES-D for depression, the FS II-R to examine the functional

57
status of the children, Family Environment Scale (FES) and a social support scale. The
purpose of the study was to examine the health outcomes of mothers of children
dependent on technology and associations with severity of illness and family/social
support. Mothers of children who were technology dependent had impaired health related
to pain, vitality, social function, mental health and greater depressive symptoms than
controls (p=<.001). Almost half the mothers of children who were technology dependent
had scores suggestive of clinical depression. Also, these mothers had lower family
income, were less likely to be employed and had higher out of pocket medical expenses
than controls. Additionally, increased scores on the CES-D, indicative of risk for
depression were significantly related to increased functional limitations in the chronically
ill child and increased out-of-pocket medical care expenses. Noteworthy is the fact that
the FS II-R, a measure of functional status, explained 34% of the variance in maternal
mental health status. The researchers found that mothers of children who were
technology dependent reported higher levels of depressive symptoms, poorer physical
health, less family support and fewer recreational and cultural activities. Other important
findings were that even 6 months after diagnosis or major hospitalization, functional
status was highly associated with mother’s emotional well being. Family support and
social support appraisal had moderate independent positive effects on mother’s emotional
well-being. In conclusion, a greater number of mothers of children who were technology
dependent reported significantly higher levels of depressive symptoms than controls
particularly those whose children had a lower functional status.
In a subsequent article published regarding the same study, Thyen et al. (1999)
examined how children who are technology dependent are cared for at home and how
having a child who is technology dependent affects maternal employment and child care.

58
Additionally, the study examined the way care at home and how the decision to leave
employment affects maternal mental health. Important findings include that the primary
effect of caring for a child assisted by technology on mental health was significant
(p<.001) and employment was a protective factor for mental health in the study group.
Moreover, there was significant interaction with maternal mental health, employment and
group membership (p=<.01) (Thyen et al. 1999).
Frankel and Wamboldt (1998) conducted an ambitious study to examine how
family functioning, coping, and child anxiety are related to parental psychological
distress in 70 chronically ill children and their parents using the Impact on Family Scale
(IOF) Scale, Psychiatric Symptom Index, Coping Health Inventory for Parents (CHIP),
Family Assessment Device (FAD), and Functional Disability Inventory. Findings include
that those parents with increased psychological distress and low perceived support report
that the child’s illness is disruptive and has a major impact on the family (Frankel &
Wamboldt, 1998). The researchers proposed that how a child’s illness interferes with and
impacts a family is determined by the psychological health of the main caretaking parent.
The psychological health of the parent is in turn affected by the age and gender of the
child, number of adults in the household, family functioning, and the functional
limitations, and level of anxiety of the child. The Psychiatric Symptom Index (PSI)
predicted the Impact on Family Scale, a measure of family functioning, accounting for
39% of the variance in this variable. Additionally, having a child who has functional
limitations as well as high anxiety was associated with higher PSI scores. Based on these
findings, the researchers propose that the major mediating factor between aspects of the
child/family and family functioning and the management of the chronic illness is the
caregiving parent’s psychological adaptation (Frankel & Wamboldt, 1998). Kuster et al.

59
(2002) concur with these findings and state that the Impact on Family Scale was
positively related to level of depression in mothers of ventilator dependent children.
Therefore, when the primary caretaker is psychologically distressed, the family is unable
to effectively manage the illness and the quality of life for the entire family is decreased.
In particular, mothers’ distress seems to impact the general function of all the other
family members. In conclusion, a mother’s mental distress (depressive symptoms)
impacts general family functioning and may contribute to how much the family is
impacted by the child’s chronic illness (Frankel & Wamboldt, 1998).
Another contribution to a parent’s mental health is the responsiveness of the child
to the caregiver. In a longitudinal study of 125 low birth weight infants and mothers
recruited within the first 2 weeks after birth, Weiss and Chen (2002) examined family
functioning during the first 3 months and collected data on maternal functioning and
infant health at 6, 9 and 12 months using Family Coping Strategies (F-COPES), DSM-IV,
Nursing Child Assessment Satellite Training (NCAST) feeding scale, Family
Adaptability and Cohesion Scales (FACES) to measure adaptation and cohesion of the
family and Emotional Support and Life Stress. The researchers found that infants who
were more responsive and interacted more with caregivers had mothers with better
mental health and families who were more cohesive and adaptable. It was proposed that
when the infant is less responsive there is less mutually satisfying interactions. Other
significant findings were that perceived emotional support was positively correlated with
degree of family cohesion (p=<.0001).
Another correlate of depression in parents of chronically ill children is the
presence of behavior problems. Shore et al. (2002) found that child behavior problems
were the strongest predictor of maternal depressive symptoms (p=<.0001) in a sample of

60
115 mother-child dyads. Other factors that helped to explain 32% of variance in maternal
depressive symptoms were income (p=.004) and low satisfaction with family
relationships (p=<.008).
Other researchers examined the magnitude of depression and mental distress in
caregivers of children with chronic illness and more specifically children who are
dependent on technology. Miles et al. (1999) found that at discharge, 45% of mothers
with children who are technology dependent had CES-D scores above the cutoff of 16
indicating risk for depression and 36% had scores above the cutoff at 12 months after
discharge. Kuster (2002) found that 45% of female caregivers of ventilator dependent
children were experiencing depressive mood symptoms. Interestingly, social support
(emotional, informational, and instrumental) was the only significant predictor of
depression (Kuster,2002).
Summary of Psychological Effects on Parents of a Child with Chronic Illness
In summary, many factors have been found to be associated with depression in
parents of children with chronic illness. Most notably, impaired functional status,
unpredictability of the child’s symptoms, decreased family income, decreased satisfaction
with family relationships and decreased family cohesion, increased number of health care
visits, maternal role restriction, maternal unemployment outside of the home, perception
of increased burden by the caregiver, child’s lack of responsiveness, child’s behavior
problems, increased anxiety in the child, residence in an urban area and perceived lack of
support contribute to increased depressive symptoms in the primary caregiver,
particularly mothers. Functional limitations were implicated as the major contributor to
psychological distress in parents of chronically ill children. Increased psychological

61
distress in caregivers, especially mothers, was also noted to have a negative effect on
family functioning as well. Noteworthy is the fact that large percentages of parents of
children who are dependent on technology, up to 45%, have depressive symptoms that
are indicative of the need for psychological intervention (Miles et al, 1999; Kuster, 2002).
The Child Who is Technology Dependent
Relatively few research studies have been conducted regarding the child who is
technology dependent or their families even though these children have been increasingly
cared for at home over the past 20 years. Some researchers have examined the level of
depression experienced by parents, impact on the family with regard to the four groups of
technology assistance (OTA, 1987), and severity of the child’s illness and more recently
the health promotion activities of mothers. Others have studied the issues and the cost in
terms of time, physical health of parents, careers, relationships, loss of sleep, loss of
privacy, recreational activities, as well as financial costs of providing home care. Still
others have researched the dual role of nurse and parent that is often assumed while
providing home care to the child who is technology dependent as well as the experience
of mothering these children. Another area of research regarding the child who is
technology dependent and their families is the process that parents journey through while
learning to manage the child at home. Last, researchers have examined the positive gains
experienced by parents managing the child who is technology dependent at home as well
as the expressed needs of parents. Parents reported that the following would be most
helpful to them: a true trusting partnership with health care professionals, social support,
and assistance with accessing resources and help. The majority of sample sizes for
quantitative studies were large with mean age of the child being 4-7 years. Use of

62
functional status instruments for the child who is technology dependent that were not
psychometrically tested was problematic. A majority of the studies done with children
who are technology dependent and their families, particularly those done recently, have
been qualitative.
Long-Term Home Care
Family experiences of long-term home care of the child who is technology
dependent (age 3-12 years) was examined in a qualitative study of 15 families (O’Brien,
2001). Parents identified uncertainty and unpredictability in their lives, describing “living
in a house of cards”. Parents attempted to increase the stability in their lives by using
advocacy, reframing and vigilance. Balance was required to manage daily life with
technology, maintain a functioning family and make sense of life (O’Brien, 2001).
Coping
Coping was also explored with of families with children who are technology
dependent. Youngblut, Brennan, and Swegart (1994) found that mobilizing family and
acquiring social support were the coping strategies used most often in a triangulated
study of 10 families. Stephenson (1999) found that higher levels of coping were
associated with lower levels of distress within families.
Cost
Cost- Time
Many studies noted the costs associated with caring for a child who is technology
dependent at home. One such cost associated with the care of these children is time. The

63
time required for the care and multitude of treatments necessary to sustain the child who
is technology dependent is daunting (Kirk & Glendinning, 2004; Wilson et al., 1998) and
is considerably more than the time required for children who are chronically ill. Heyman
et al. (2004) interviewed a group of maternal caregivers of 101 children who had a
chronic illness with (n=50) and without (n=51) a gastrostomy tube (GT) three times; at
three month intervals. Findings include that children with gastrostomy tubes required two
times the total care time from the primary caregiver as children without a gastrostomy
tube (484.5 versus 197.8 minutes (p=<.0001) particularly for technical care.
Beyond the time required for technical treatment, much time is required to deal
with practical issues related to the child who is technology dependent such as dealing
with insurance companies, ordering supplies, and packing up the necessary equipment
and supplies for outings (Torok, 2001). In a qualitative study of 36 families of children
who are technology dependent, Heaton and colleagues (2005) examined the care routines
of children who were technology dependent to study what was involved with this care
and how it affects family members. The researchers discovered that there is an
incompatibility between technology time frames and other social and institutional time
frames that contributes to social exclusion of families with children who are technology
dependent from many aspects of social life. Time demands related to care routines and
lack of compatibility with other social and institutional time frames were found to limit
the family’s participation in school, employment and social activities. School days were
particularly difficult because there was less time to deal with medical devices and
administration of various treatments prior to school therefore the child had to get up
extraordinarily early (Heaton et al., 2005). Therefore, the time required to care for the
child who is technology dependent is considerably more than the typically developing

64
child and the incorporation of the technology time frames can lead families to alienation
from participation in school, employment and social activities.
Cost- Physical Health
Another cost examined related to caregivers of the child who is technology
dependent is that of physical health. Ostwald et al. (1993) found that 19.2% of parents
caring for a child who is technology dependent reported that their physical health was fair
or poor. In a study of 89 infants who were technology dependent, Miller and colleagues
(1998) found that a total of 21.6% of their caregivers had physical problems that
interfered with daily activity that were directly related to caring for the child. Many
caregivers of children who are technology dependent experience physical exhaustion
(Kirk & Glendinning, 2004), fatigue (Neuss, 2004; Torok, 2001; Wilson et al., 1998) and
burnout (Wang & Barnard, 2004) mostly due to sleep disruption and deprivation because
of the constant vigilance necessary to monitor the alarms, perform treatments and oversee
the technology at night (Heaton et al, 2005; Kuster, et al., 2004; Neuss, 2004; Wang &
Barnard, 2004). Kuster et al. (2004) found that in 38 mothers with children who were
ventilator dependent, 60.5% never or only occasionally were able to get adequate sleep.
Along with sleep deprivation, mothers experience irritability, slowing of cognition and
altered memory (Neuss, 2004). Therefore, the costs associated with caring for a child
who is technology dependent on the caregiver’s physical health are high and sleep
deprivation, fatigue and burnout can consequently lead to difficulty with performing care
tasks.
Time constraints, due to care required by the child who is technology dependent,
can lead mothers to neglect health promotion activities such as recreation (Kuster et al.,

65
2004; Neuss, 2004; Miller et al., 1998; Torok, 2001), adequate nutrition, exercise,
relaxation, and general health promotion (Kuster et al., 2004) that will ultimately affect
their physical and mental health. In a study of 89 mothers of infants who were technology
dependent, Miller et al. (1998) found that 75.7% decreased the amount of recreational
activity they participated in beyond those associated with caring for a typical infant.
Furthermore, in a study of 38 maternal caregivers of children who were ventilator
dependent, Kuster et al. (2004), found that the functional status of the child and maternal
coping were positively related to perceived general health and health promotion activities
of the mother but the impact of the child on the family (IOF) was inversely related to
health promotion activities. Interestingly, 82% of the mothers never or only occasionally
planned exercise and 73.7% never or only occasionally get together with friends. Mothers
scored low on nutrition, exercise, relaxation and general health promotion subscales of
the Personal Lifestyle Questionnaire (Kuster et al, 2004). More specifically, the two
largest contributors to the 25% of the variance in the mother’s participation in health
promotion activities were functional status and impact on family. Decreased functional
status, out of pocket money paid for the child’s medical expenses and number of home
health care nursing hours was related to increased physical and psychological morbidity
(depression) for these mothers (Kuster et al., 2004). Additionally, the researchers
proposed that if the mother perceives that she is unable to meet all the needs of her child
and family an alteration in sense of mastery, self esteem, and psychological dysfunction
(depression) may occur (Kuster, 2002).
Therefore, factors that are proposed to impact a mother’s physical and
psychological well being include the child’s severity of illness, frequency of
hospitalization or exacerbations, amount of time to provide treatment and care, functional

66
and developmental status of the child, the level of care that the child requires and
available resources such as finances and number of home health care nursing hours as
these all directly effect the amount of time mothers must devote to caregiving (Kuster,
2002).
Cost- Alteration in Relationships
An alteration in relationships previously enjoyed was another cost associated with
caring for the child who is technology dependent. In a qualitative study of 12 mothers of
children who were technology dependent conducted by Neuss (2004), 10 said that their
life revolved around the child’s care at home and that they were no longer “dating” their
husbands. Some said this inability to spend time as a couple put a strain on the marital
relationship and some eventually divorced due to the stress of caring for a child who is
technology dependent (Kirk & Glendinning, 2004; Neuss, 2004; O’Brien, 2001). Others
parents reported marital discord due to the uneven work load that mothers perceived
(Wang & Barnard, 2004). Mothers also felt that friendships were now chosen by
convenience i.e. neighbors and home health care nurses and not necessarily by
compatibility. They felt a divide between themselves and others their own age because of
the difference in life views and the change in responsibilities. They could no longer relate
to others’ carefree attitude and mothers felt unable to leave for social events (Neuss,
2004). Furthermore, Allen and colleagues (1994), noted that according to the Impact on
Family (IOF) scale, illness of the child who is technology dependent had a negative effect
and was related to disruption of social relationships. In summary, alterations in
relationships with spouses, friends and other social contacts was a cost associated with
caring for the child who is technology dependent.

67
Cost- Alteration in Family Dynamics
An additional cost of caring for the child who is technology dependent is a change
in family dynamics. Mothers noted changes in family dynamics and were concerned they
were not spending adequate time with other family members (Torok, 2001). Finding time
together as a family was difficult and frustrating (O’Brien, 2001). Having a child who is
technology dependent influenced some parent’s decision regarding having more children
(O’Brien, 2001). Some voiced concern regarding the other siblings in the family
receiving less attention due to the time spent delivering required care to the child who is
technology dependent (Kirk, 2004; Allen et al., 1994). All 12 mothers in a study by
Neuss (2004) said that the relationship with the healthy child suffered. Parents noted
behavior changes in siblings (Wang & Barnard, 2004) and were concerned about the
healthy sibling’s mental health due to the unpredictable life at home (Heaton et al., 2005).
Some of the siblings were given more domestic responsibilities and/or had to look after
other siblings. A particularly difficult time for siblings was when the child who is
technology dependent was ill especially when they had to try and study for exams
(Heaton et al., 2005). Therefore, parent’s time with healthy siblings is reduced when
caring for a child who is technology dependent and causes parental concern regarding not
only their relationship with the child but the healthy sibling’s mental health as well.
Cost- Social Isolation
Many parents expressed feelings of social isolation, a cost associated with caring
for the child who is technology dependent (Boland & Sims, 1996; Carnevale et al., 2006;
Kirk & Glendinning, 2004; Neuss, 2004; O’Brien, 2001; Wang & Barnard, 2004). Their
lives revolve around the technology and the necessary care routines. Friends are noted to

68
withdraw; there is less contact with work colleagues and extended family and less social
outings according to parents (Boland & Sims, 1996; Kirk, 2004; Tommet, 2003). Often
women experience not only social isolation but also loneliness and a sense that their lives
are on hold (Neuss, 2004). There is a lack of spontaneity due to the need to coordinate
outings with availability of a home health care nurse. Many reported the lack of available
respite care (Carnevale et al., 2006; Heaton et al., 2005; Kirk, 2004) or did not share the
care with others if they perceived they were not skilled enough to care for the child due to
worry that the care would suffer (Boland & Sims, 1996). In conclusion, parents,
particularly mothers, experience social isolation, and loneliness often due to the care
required by the child who is technology dependent. Furthermore, parents report lack of
respite and others whom they believe could adequately care for their child.
Cost- Alteration in Employment Opportunities
A change in career or leaving employment (quitting job) was frequently
mentioned by parents as a cost of caring for the child who is technology dependent
(Neuss, 2004; Torok, 2001; Miller et al. 1998; Kirk & Glendinning, 2004). Other parents
decreased their hours of employment to meet the care needs of their child (Cohen, 1999;
Glendinning et al., 2001). Miller et al. (1998) found that 73% of 89 primary caregivers
were employed before the child who is technology dependent was born and of these, 63%
quit due to illness and/or care required by the baby. Neuss (2004) found that 6 of 12
mothers in her qualitative study were employed prior to having the child who is
technology dependent however 5 of 12 gave up work not by choice but due to care needs
of the child. The one mother who still worked full time said there was no opportunity for

69
upward mobility due to the need for a flexible schedule. Cavanagh and colleagues (1999)
found that only 4 of 13 primary caregivers worked outside the home mostly due to
problems with flexibility of the job if the child got sick, a home care nurse called off or
frequent medical appointments. Others said they missed career opportunities (Cohen,
1999; Torok, 2001) or were unable to return to school and further their education (Lee,
1996; Miller et al., 1998) unless they had a large number of home health care nursing
hours (Lee, 1996). Therefore, a major cost for mothers related to caring for a child who is
technology dependent at home was changing careers or leaving gainful employment
outside the home due to the child’s frequent illnesses, lack of dependable home health
care nursing coverage and frequent medical appointments.
A mother’s change in employment status as a cost of caring for the child who is
technology dependent held true over and above those mothers who had healthy, typically
developing children. Thyen et al. (1999) examined how children who are technology
dependent and cared for at home affect maternal employment and child care compared to
a control group of mothers with children hospitalized for acute illness, matched for age
and gender, 6 months post discharge. Findings for the study group of mothers were that
46% worked fewer hours following discharge and 23% took a different job in order to be
able to care for the child, 46% earned less because they cared for the child and 42% were
unable to change jobs due to potential loss of insurance. A total of 92% took time off to
care for the child who was technology dependent compared to 35% of controls, 35.7% of
study families had family incomes <$30,000 compared to 19% of controls 6 months
following discharge (p=<.05) and study families had greater out of pocket medical
expenses than controls; $5062 versus $265 respectively. The researchers do not report if
family income at discharge is significantly different however, mothers who left

70
employment had larger families, were single parents and had less child care assistance.
Using logistic regression, controls were three times more likely to work than the study
group. Mothers with college education were 2.5 times more likely to work. A total of
35.7% of the children who were technology dependent received home health care
nursing. Therefore, the cost of caring for child who is technology dependent in terms of
change in career and cessation of gainful employment held true even when these mothers
were compared to matched controls.
Cost- Alteration in Family Finances
Often, due to a mother’s cessation of employment outside the home in order to
care for the child who is technology dependent, total family income plummets. In a
qualitative study of children who are technology dependent, Cavanagh (1999) found the
continuous financial struggle that these families faced was a dominant theme. This
financial concern was present despite the money received from government programs and
family (Lee, 1996). Neuss (2004) found that 10 of 12 mothers reported a change in
financial status after the child who is technology dependent was discharged home. A
number of families were severely impacted financially from lost income when one of the
parents quit work in order to stay home and care for the child who is technology
dependent. Also, there were additional expenditures for the family due to increased use of
electricity, heat, phone, insurance, laundry as well as travel (Kirk & Glendinning, 2004;
Glendinning et al., 2001). In order to deal with this financial crunch, some parents used
savings to pay for the extra expenses (Miller et al., 1998) or even “spent down” all of
their savings so they would be eligible for state money (Cohen, 1999) while other parents
borrowed money (Miller et al., 1998). Miller et al. (1998) found that 40.5% of parents

71
who were employed (typically the father) worked overtime while 16.2% took on a second
job to meet expenses. Cavanagh (1999) found that some secondary caregivers (fathers)
worked 50-100% overtime and depend on the grandparents for supplies or used their 401
K to make ends meet. Some parents reported getting behind on house payments,
experienced foreclosure and had to use a food bank to get by (Cavanagh, 1999).
Therefore, after a child who is technology dependent is discharged home, many families
experience decreased family income with a concomitant rise in expenses related to the
child’s care that necessitates accessing additional financial resources in the form of
overtime work for the secondary caregiver, tapping savings and retirement monies and
borrowing from relatives.
The financial pressures that parents of children who are technology dependent
spoke of in a number of qualitative studies are very real. In a study of data from the 2000
Medical Expenditure Panel Survey (MEPS) for children, Newacheck and Kim (2005)
found that 949 of the 6965 children (15.6%) in the sample were identified as children
with special health care needs (CSHCN) of whom children who are technology
dependent are a part. It was found that CSHCN had 3 times higher health care
expenditures than healthy children ($2099 vs. $628; p=<.01). Families of CSHCN had
the best coverage for in-patient services. Families of CSHCN with out-of-pocket
expenses over 5% of family income were about 11 times more likely to have incomes
below 200% of the federal poverty level than families at or above 400% of federal
poverty level. The total cost and out-of-pocket cost for CSHCN was noted to be skewed,
therefore, the median total expense for health care was $558 but the upper decile of
CSHCN was $4304. Home health care and hospital costs were major cost items for upper
decile kids. Prescription medications and home health care comprise 1/3 of health care

72
expenses for CSHCN but only 1/20 for other children in the sample (Newacheck & Kim,
2005). Therefore, based on this survey of randomly selected children, those who are
technology dependent were more likely to come from families who were below 200% of
the federal poverty level and have a significantly greater amount of out of pocket medical
expenses that contribute to an already financially strained family.
Cost- Privacy
Parents of children who are technology dependent said that receiving home health
care nursing hours was extremely beneficial in many regards; however, many said that
this was at the cost of their privacy (Cohen, 1999; Lee, 1996; K. Murphy, 1997; O’Brien,
2002; Torok, 2001; Wang & Barnard, 2004). Cohen (1999) on the contrary, stated that
families who were socially marginalized (meaning that they were from low income,
minority families) did not experience this but, rather, enjoyed the extra company and
contact with someone from outside their social circle.
For some families, receiving home health care nursing changed the meaning of
home (Wang & Barnard, 2004). Kirk and colleagues (2005) found that the meaning of
home for many parents included thoughts of privacy, safety, intimacy, control and liberty.
The home was thought to embody the personal identity of the family and space and daily
routines have personal meaning. Technology transforms the home then so it is
consequently “medicalized” by equipment and is constantly being invaded by home
health care professionals. Additionally, the home is invaded and dominated by all the
equipment and supplies required to care for the child who is technology dependent (Kirk
et al., 2005). Often one of the rooms on the first floor is transformed into a mini-intensive
care unit (ICU). The home is now a public space and the family’s life is lived in front of

73
strangers. All family interactions are subject to inspection and judgment therefore many
families expressed fear of showing affection or having arguments. Many felt awkward
entertaining because it had to be conducted in the presence of the home health care
professionals (Kirk et al., 2005). Parents had conflicts regarding home care nurse
involvement in discipline (O’Brien & Wegner, 2002). Mothers often assumed the
leadership position with the home care nurses, identifying roles, protecting the privacy of
the other children, setting up family boundaries and a good working environment for the
nurses (Cavanagh, 1999). Therefore, having home health care nurses help in caring for
the child who is technology dependent comes at a cost; the loss of privacy and a
transformation of the meaning of “home” as well as a transformation of the physical
environment into that of a “mini-ICU”.
Cost- Alteration in Parenting Role
Another cost associated with caring for the child who is technology dependent is a
change related to the typical parenting role. Many qualitative studies describe the
discomfort parents experience when they need to assume the dual role of nurse and parent
while caring for their child who is technology dependent (Kirk & Glendinning, 2004;
Kirk et al., 2005; Wang & Barnard, 2004). They experience conflict regarding
performing procedures that may inflict pain on their child due to the fact that the main
role of the parent is typically that of protector (Wilson et al., 1998; Kirk et al., 2005).
Parents prefer to see themselves as primarily the parent and do not want the relationship
with their child to be defined by the nursing activities performed and resent how the
nursing role often dominates their parenting experience. In other words, parents are
seeking to have primarily a parent-child relationship (Kirk et al., 2005).

74
Not only do parents of children who are technology dependent assume the dual
role of nurse and parent but many times assume multiple additional roles as well. Parents
often manage the child’s condition, organize and advocate for services, access funds and
deal with nurses, equipment vendors, and insurance companies as well as perform a
multitude of procedures all the while monitoring the child’s progress in terms of health,
growth and development (Kirk, 2004; Allen et al., 1994). Additionally, parents frequently
have to make complex judgments regarding the dosing of medications depending on the
status of the signs and symptoms related to the condition (Kirk, 2004). Due to this
heightened responsibility, parents express worry that they will overlook problems and
that the child will suffer. Consequently, parents often look to home health care
professionals for reassurance that they are doing a good job (Torok, 2001). All 12
mothers in a study by Neuss (2004) had recurrent, intrusive anxiety regarding the child’s
death. Studies by Carnevale et al. (2006) and Lee (1996) concur with this finding.
Therefore, the multiple roles and the great responsibility that parents of children who are
technology dependent assume is daunting and can lead to worry and intrusive anxiety
regarding the child’s health and safety while they are caring for the child at home so look
for reassurance from home health care professionals that they are doing a good job.
“Mothering” Role
Mothers described their challenges in the role of “mothering” a child who is
technology dependent. Despite all the difficult and challenging work related to caring for
a child who is technology dependent, 11 of 12 mothers in a study by Neuss (2004) had
strong feelings of attachment to the child. Mothers frequently defined themselves
through their child. Though the mothers thought that they lost pieces of their prior self, it

75
was replaced by who they became; one who experienced positive growth and a greater
sense of self esteem due to competency they developed in mastering the techniques
required to care for the child who is technology dependent (Neuss, 2004; Lee, 1996). In a
qualitative study of two, single, African American mothers of infants who were
technology dependent, Lee (1996) found that their experience of mothering was no
different in KIND but different in DEGREE. Being able to show off their child helped
reinforce their identity as mother. Positive feelings regarding themselves as mother
increased as the baby became more responsive. The mother’s daily schedule was dictated
by the baby and was monotonous, fast paced, socially isolating leaving little personal
time for the mother. It was labor intensive to perform the care, go on multiple trips to the
doctor and get all equipment ready to leave the house. The first month was the scariest,
then the mothers felt much better about caring for the child who is technology dependent
as they developed increased confidence with the routine particularly when they were able
to handle novel situations in the first months after discharge. Rehospitalization decreased
a mother’s confidence as they second guessed if they could have prevented the illness.
The mothers felt like they were under house arrest and could not “pick up and go”
however they felt guilty if they did leave. Taking the baby out for car trips helped them
feel more normal. The two mothers got very little help mostly due to fear of relatives and
friends that something might happen that they would not know how to handle.
Previously, they could go out and socialize but now the telephone was the primary tool
for socializing (Lee, 1996).
The mothers in the study had a need to normalize the situation so they would not
be excluded from the experience of motherhood. The mother’s ability to do similar things
for the baby that all mothers do and have the infant respond was reassuring that the child

76
who is technology dependent is a baby first and foremost. Therefore, parents did things
so that they could display the normal aspects of the child such as hide the trach and
remove the oxygen temporarily. The mothers tried to show how care of the child who is
technology dependent was experienced as normal and everyday using phrases such as
“easy as changing a diaper”(Lee, 1996). In summary, “mothering” a child who is
technology dependent is labor intensive and often socially isolating yet affords an
opportunity for increased confidence, personal growth and satisfaction particularly when
the mothers found ways to normalize the child’s experience; viewing them as a child first
and foremost.
Process of Care
Process of Care- Goals
In addition to the costs of caring for the child who is technology dependent and
the plethora of changes in roles experienced by parents, research studies also examined
the process of care as experienced by the parent, most frequently, the mother. Some
researchers studied the process in terms of stages of adaptation while others looked at
themes. Still others looked at goals of managing the child who is technology dependent.
O’Brien (2001) described the goals for families of children who are technology
dependent as managing daily life with technology; maintaining a functioning family by
achieving some sense of stability while attending to multiple, complex issues, prioritizing
and making compromises that would not jeopardize health. Additional goals were to
make sense of life as well as to continually restructure family life. This restructuring is
due to the constantly changing needs of the child who is technology dependent and is
based on the child’s health, schedule, and routine as well as other family roles and

77
responsibilities (O’Brien, 2001). Therefore, important goals for families of children who
are technology dependent are managing the balance of daily life with technology to keep
the child stable and healthy while concomitantly maintaining a functioning family.
The process of caring for the child who is dependent on technology has also been
described as “phases of protective care” (Judson, 2004). In a study of 19 mothers of
children dependent on parenteral nutrition, Judson (2004) elucidated three phases that
mothers pass through in the journey of caring for their child who is technology
dependent. The first phase was gaining control that included committing to care by
preparing to go home, organizing chaos and establishing a routine. The next phase, taking
control, included watching over the child and developing expertise and vigilance in care,
challenging the system and promoting normalcy by being flexible, accepting uncertainty
and fostering acceptance. The last phase, maintaining control, includes putting life in
perspective, finding respite and support and celebrating the positive (Judson, 2004). The
researcher noted that in the process of care, the key to normalization for the child was for
parents to have clear expectations for behavior and discipline.
Bull (1992) identified the process of care as “phases of mastery” in the care of the
child who is technology dependent. Phases included the following: identify problems,
take action, modify the environment, change roles, and establish routines. In the
identification of problem phase, the worry parents experience is a symptom of underlying
problems such as new skill they had to learn, role changes or changes in family
functioning. In the take action phase, families sought information, practice new skills,
solve problems and access resources. This phase requires persistence, organization,
willingness to try new things and to get help from home care professionals. Parents must
also modify the environment in order to function and change roles; many times having to

78
give up former activities and take on new functions. Last, by two months after discharge,
parents establish routines and move to mastery where new routines are established and
the family is in control. Barriers to mastery include low income, lack of awareness of
resources, few network and informal supports and gaps in community services (Bull,
1992). Therefore, Bull (1992) found that within the process of care there are phases of
mastery that eventually led to a goal of establishing a routine and control of family
functioning by two months following discharge.
Process of Care- Organization
Organization was noted to be an important component in the process of care for
the technology dependent child. Torok (2001) found that within the first 4 weeks at home
some mothers of infants who were technology dependent had become experts while
others were floundering but with time and experience all progressed to managing
effectively. However, all 8 mothers included in this qualitative study were Caucasian,
with a mean age of 30 years, and all but one was married with a college education so it is
hardly representative of the population of mothers of children who are technology
dependent. Important findings from this study were that mothers moved from learning
care to making judgments regarding the infant’s health and getting to know the infants
likes/dislikes as well as health related behaviors. Mothers recognized changes in family
dynamics and met family needs by adjusting roles, responsibilities and lifestyles. Also, a
big part of caring for these infants was changing priorities so they no longer did things
that were previously important. Mothers learned to manage the increased work and time
required for infant care and navigated the ever changing emotions and concerns to

79
achieve near normalcy in the family. Mothers also noted that while they recognized the
differences, they also saw similarities to other infants. They also realized that they need
to be vigilant in care of the infant. Therefore, the main point related to effectively
managing the child who is technology dependent is to BE ORGANIZED AND HAVE A
SCHEDULE and also achieve a balance for family functioning that includes changing
priorities to maintain the child’s health while at the same time meeting family needs by
adjusting roles and responsibilities (Torok, 2001).
Mothers reported improvements in the infant and family since the infant came
home (Boland & Sims, 1996; Torok, 2001). In a qualitative study of 17 families (5
families with a child who is technology dependent and 12 families with a spouse or
parent who was technology dependent), Boland and Sims (1996) described caregiving as
a solitary journey. All families interviewed valued home as a healing place that provided
meaning and reason for participation in caregiving. Moderating the sense of burden was
their commitment to care and the view that home was a healing place. Families felt their
loved ones would recover faster and that home was a more “normalizing” environment.
Families said they had no one else to help and had continuous responsibility with no
respite. The constant stress included financial concerns, lack of support, burden of 24
hour care, fatigue, fear of the unknown and the need to balance other family demands.
Therefore, while home was viewed as a healing place for an ill family member,
caregivers often paid the price in terms of a 24 hour burden of care with no respite while
at the same time balancing other family demands.
Murphy (1997) identified stages of adaptation families of children who are
technology dependent experience to achieve “normalcy”. The first month was described
as “awful” due to the anxiety- no matter how well they were educated prior to discharge.

80
The next five months were critical but tolerable- things could “heat up” at any moment.
Parents felt it took 4-6 months to leave the house and resume other family and work
activities without major anxiety, and if they were unable to leave the house regularly
during this time they became socially isolated. The next 12-18 months were relatively
calm but families experienced increased difficulty with the home care nurses. The two
year point in home care was a critical point that included increased discord in the
marriage and/or with the home care nurses, possibly due to realizing that the situation
was permanent. At this time there were explosive firings of nurses or home care agencies.
Finally, the family reached the point of resolution and reorganized themselves to “get on
with life”. Families made a conscious effort to do normal everyday activities with the
child and came to accept that family life had changed but they did not need to be
consumed by it (Murphy, 1997). The researcher concluded that the adaptation process to
reach normalcy in family life occurs over time and can take over 2 years for many
families (Murphy, 1997).
Tommet (2003) also found that families of children who are technology
dependent undergo a process over time whereby they achieve an “order out of chaos”. In
a qualitative study of 5 couples (mother-father pairs) with a child who was technology
dependent ages 5-7 years, Tommet (2003) found that 2 patterns emerged over time-living
in uncertainty and order in chaos. Parents live in uncertainty with a period of intense
disruption and disorganization that was the dominant pattern for the first 2 ½ to 3 years
after their child was born. During this time, the family struggled to survive and gain
control of an uncontrollable situation. The time was characterized by intense medical,
caregiving and personal crisis. Families experienced an evolving relationship with home
care providers and isolation from family and friends. Order in chaos lasted from 3 to 5-6

81
years where they enjoyed relative medical stability. This period was characterized by
personal growth, greater family cohesion, a letting go of the past life and living in the
present and development of advocacy skills. Old friends often did not have the same
common interests so they developed a new network of support that included health and
educational providers (Tommet, 2003).
Process of Care- Ensure a Childhood
In another qualitative study of 23 caregivers of children age 1 to 13 years from 13
families, Cavanagh (1999) discovered 5 core processes that were similar across all
diagnoses, ages, and types of technology the children required. These processes were
accepting, learning, taking back the child, reshifting the everyday, and seeking validation.
Accepting meant coming to terms with the situation. Learning was more than
knowledge that can be gleaned from a textbook and was an essential element that allowed
the parent to regain authority and become an expert of their child’s condition. Taking
back the child gave meaning to life and required commitment and involvement of the
family to bring the child home. “Reshifting the everyday”, required family lifestyle
changes to fine tune the household in order to meet the physical and social needs of the
family. Seeking validation was the long term work of caregivers to show others why
caregiving is valuable and that the price they pay increases the quality of life for the child
who is technology dependent.
Parents strove to have their child recognized as a valued member of society and
worthy of a childhood. The process that families underwent sought to merge everyday
family routines and care for the child who is technology dependent to ensure a childhood

82
and normal family life. The motivating factor for caring for the child who is technology
dependent at home was to reconnect and bring them a childhood.
Perseverance was seen as important family attribute. The primary concern for all
of the families was to continue to preserve the family. Daily life was different from the
other families but became more predictable as time went on because the child care
became routine and the medical procedure became second nature to them (Cavanagh,
1999). This qualitative research study confirms that families of children who are
technology dependent undergo a process over time to merge the care of the child with
everyday family routines in order to ensure a childhood for the ill child while at the same
time preserving a normal family life. The normalizing of the child’s care and medical
procedures occurs as care becomes routine and second nature to parents.
Wilson and colleagues (1998) concur with these finding reporting that to gain a
sense of control and to stabilize family life the mother had to work with home health care
nurses to set role expectations. The mother’s attention to detail when caring for the child
was to ensure the standard of care. Goals for these mothers were to facilitate day-to-day
family life while giving care to the child who is technology dependent.
In a study of 38 family members of 12 children who were ventilator dependent,
Carnevale and colleagues (2006) found that the main goal families strive for is
STABILITY. This stability however can be undermined by limits in finances, cohesion
and the unpredictability of the child’s chronic illness. When families had things under
control, daily activities became routine. In other families who were unstable or on the
verge of unraveling, every new incident would unbalance the family organization and
every day life was chaos. Carnevale et al. (2006) found that all unstable families in her
study were those with single parents. Additionally, finances were found to be the sole

83
factor that differentiated between those families who had things under control and those
who were on the verge of unraveling. Families in both groups however reported living
daily with distress and enrichment.
Process of Care- Summary
In summary, qualitative research that explored the lives of families of children
who were technology dependent found that a family’s primary goal was managing the
balance of daily life with technology to keep the child stable and healthy while
concomitantly maintaining a functioning family (O’Brien, 2001). Additional goals for
these families as described in the literature include stability (Carnevale et al., 2006;
O’Brien, 2001), ensuring a childhood (Cavanagh, 1999), and promoting “normalcy” for
the child who is technology dependent as well as the family (Boland & Sims, 1996;
Cavanagh, 1999; Judson, 2004; Murphy, 1997; Torok, 2001). Many of the researchers
also described the process of caring for the child who is technology dependent in terms of
stages of adaptation. Bull (1992) found that the process of establishing routines took
approximately two months. Other researchers found that the process took much longer;
about 2-3 years (Murphy, 1997; Tommet, 2003).
The process of care, more specifically family management of the child who is
technology dependent, was described in qualitative studies as requiring a variety of skills
such as prioritizing (O’Brien, 2001; Torok, 2001), flexibility (O’Brien, 2001; Judson,
2004), organization (Judson, 2004; Bull, 1992; Torok, 2001; Murphy, 1997), and
establishing a routine/schedule (O’Brien, 2001; Judson, 2004; Bull, 1992; Torok, 2001;
Cavanagh, 1999; Carnevale et al., 2006). The process of managing the child’s care also
required a restructuring of family life to meet the needs of the child who is technology

84
dependent as well as the needs of other family members by shifting family roles and
responsibilities (O’Brien, 2001; Bull, 1992; Torok, 2001; Cavanagh, 1999). Gaining
control of the child’s care process by becoming an expert and mastering their child’s care
to the point that care became second nature to them was also noted as an important
feature of effectively managing the care of the child who is technology dependent
(Judson, 2004; Bull, 1992; Tommet, 2003; Cavanagh, 1999; Carnevale et al., 2006).
The final stage in the process of caring for the child who is technology dependent,
typically after approximately 2-3 years, was described as one where families were able to
put life in perspective and celebrate the positive (Judson, 2004). At this stage, many
families felt they had achieved personal growth (Tommet, 2003; Miles et al., 1999) and
increased family cohesion (Tommet, 2003). While they realized and accepted the fact that
their family life had changed, they were not consumed by it (Murphy, 1997). Researchers
in qualitative studies noted that the following were factors associated with difficulties in
managing the care of the child who is technology dependent: lower family income, lack
of community resources, low social support, single parent family, decreased family
cohesion and increased unpredictability of the child’s illness (Bull, 1992; Carnevale et
al., 2006).
Effective Management Factors
Effective Management Factors- Stability
While some qualitative researchers described a process of care related to the child
who is technology dependent, others described factors related to effective care
management. Managing the care of these children requires skill, organization and
creativity (O’Brien, 2001). Care includes frequent and unexpected changes, limited and

85
unpredictable parental control as well as fragility and instability. Families often hang
together by a thread and report that it doesn’t take much for it to crumble. Some families
described the experience as like “living in a house of cards” (O’Brien, 2001). O’Brien
(2001) proposed ways to increase stability: vigilance, advocacy, reframing, and humor.
Vigilance includes the close monitoring of health status, treatments and close oversight of
all parts of care. Reframing includes focusing on achievable outcomes, looking for the
positive in people and maintaining hope (O’Brien, 2001). Time management was also an
important component in managing the care of the child who is technology dependent.
Families over time became more organized and planned ahead. It was important to have a
routine and time schedule but the inflexibility and lack of spontaneity was frustrating.
Families frequently had disruptions in child/family routines and needed to continuously
make choices as to priorities (O’Brien, 2001).
Effective Management Strategies- Perspective
Wilson and colleagues (1998) identified four categories of success or lack thereof
in management of care that ranged from mothers who met the self-determined standard of
caregiving to mothers who were unable to recognize success. Mothers who met the self-
determined standard of caregiving were able to manage family needs, had a large social
network and knew they were successful so consequently felt confident, positive and
trusted professionals with the child’s care. Mothers who felt they did not meet a self-
determined standard managed the day to day needs of the family but were always looking
for ways to improve. They knew their limits but did not use process skills or strategies.
Mothers who were not successful in managing day to day life of the family but successful
caregivers were reclusive and dedicated themselves to the care of the child who is

86
technology dependent so consequently had little social life. The last group of mothers
was unable to recognize their success to the detriment of the family and saw themselves
as failures, distrusted others, felt they could never do enough, worried, felt lonely and
isolated with little social life (Wilson et al., 1998). This research points out that a
mother’s perspective regarding how successful she is related to her caregiving role and
family management has long range consequences for the mother’s, child’s, and family’s
well being. Of particular importance is the effect of the mother’s perspective of how she
is managing the child and family on mental health.
Social Support
Social Support- Family, Friends and Clergy
Another factor that greatly assists in care management is social support.
Maintaining connections with extended family and friends is important, however,
parental friendships often change over time as the family must devote greater time and
energy to family needs (O’Brien, 2001). Neuss (2004) found however that 11 of 12
mothers had difficulty making friends and maintaining friendships due to lack of energy,
time and inability to leave the child to enjoy social activities. Ostwald et al., 1993 found
that less than 30% of families with a child who is technology dependent receive
assistance from anyone except family and only 15.2% received emotional support from
clergy. Spiritual beliefs comforted the mothers however most felt they received
inadequate spiritual support. Furthermore, 4 out of 12 mothers had a negative experience
with a member of the clergy being unwilling to give spiritual help due to their discomfort

87
with disabilities and children who are technology dependent (Neuss, 2004). A few
mothers said that the nurse was their closest non-related relationship (Neuss, 2004).
Most extended family members were uncomfortable providing care to the child
who is technology dependent and mothers reported that fear and misunderstanding of the
disability were reasons that extended family was not more involved (Lee, 1996; Neuss,
2004). On the contrary, half of the mothers had help with the healthy sibling. Neuss
(2004) reported that not one of the 12 grandmothers of the child who is technology
dependent offered consistent emotional care or support. The telephone was found to be an
important tool in maintaining friendships and receiving social support (Lee, 1996).
Furthermore, Cavanagh (1999) found that community involvement was marginal.
Therefore, while social support was viewed by mothers as a tremendous help in their
being able to manage the care of the child who is technology dependent, most did not
receive this social, emotional or spiritual support from friends, relatives, members of the
clergy or their communities. Frequently this lack of involvement by others was due to
fear and discomfort with technology and disabilities.
Alternative Social Support
Going beyond the typical venues of social support, the literature described other
sources of support that were helpful to the mother in the management of care for a child
who is technology dependent. Mothers found that having computer access and on-line
support was very beneficial. Neuss (2004) found that 5 of 12 mothers found computers
helped them feel connected and was a helpful source of information. Computer support
groups would help parents of children who are technology dependent have a sense of
belonging, companionship and feeling of community (Neuss, 2004). Wilson and Morse

88
(1998) suggested a discharge hotline as a resource to help families of children who are
technology dependent who may still have management questions after they leave the
hospital.
The hospice model of service that includes family involvement and spiritual care
was suggested by Neuss (2004). Lee (1996) suggested that having other parents who can
relate to their experience as a peer support would help to decrease the isolation and give
them hope that things will get better. Mothers also reported that it was a tremendous help
when nurses set aside a block of time to sit down with them to discuss feelings and
concerns (Kirk et al., 2005; Lee, 1996). In summary, the literature described a variety of
alternative methods of supporting these families. Included in these supports are on-line
support groups that would assist with the challenge of leaving the child for extended
periods of time. Other supports include a hospital discharge hotline, hospice model of
support and one on one time with a nurse. These suggestions offer promise for future
research.
Home Health Care Nursing Support
Another area examined by researchers of families of children who are technology
dependent was the partnership that developed between families and health care
professionals, particularly home health care nurses. Few mothers had a smooth alliance
with nurses and often fought over control of their child (Judson, 2004; Murphy, 1997;
Wang & Barnard, 2004). It was difficult for many mothers to give up the care of their
child to others (Judson, 2004). Mothers reported having difficulty with TRUSTING the
nurses to care for their child as they would (Wang & Barnard, 2004; Kirk & Glendinning,
2004; Neuss, 2004; Wilson & Morse, 1998). Neuss (2004) found that 10 of 12 mothers in

89
her study lacked trust in other’s ability to care for their child. They reluctantly let others
care for their child but only for short periods of time and when the mother could monitor
what was happening however, this was often done with much trepidation and worry.
Mothers did not readily accept offers of help to care for the child who is technology
dependent (Neuss, 2004). Therefore, although mothers needed respite due to the long,
exhausting hours of care on a daily basis, researchers discovered an attitude of
ambivalence often due to lack of trust that others would care for the child as they would.
Relinquishing part of the child’s care also meant potential struggles with other caregivers
for control.
In interviews with mothers, Neuss (2004) identified factors that helped with care
management. Home nursing was a valued resource for many however, due to the recent
nursing shortage, shifts cannot be covered. Amazingly, these mothers continue to manage
the care of the child who is technology dependent despite the uncertainty related to the
child’s medical instability. Furthermore, these mothers help their children survive life-
threatening medical complications. Many of the children have an unpredictable life span
so although they prepare themselves for what might happen they make the effort to stop
death (Neuss, 2004).
Findings from research studies include mother’s reports of desirable attributes of
the ideal home health care nurse. What mothers wanted most was a knowledgeable,
medically competent nurse that CARED and would talk to, sing or read to the child as
well as be affectionate towards the child (Judson, 2004; Kirk et al., 2005; Neuss, 2004).
Kirk et al., (2004) found that many mothers felt that nurses only did the technical parts of
care and neglected the emotional care. Mothers felt that the lack of emotional connection
between the nurse and child influenced how they delivered care (Kirk et al., 2005).

90
Mothers wanted nurses who came to the home to be honest about limitations in their
knowledge (Kirk et al., 2004). With a competent nurse the mother felt relaxed at home or
able to leave the house (Neuss, 2004). Cavanagh (1999) discovered that mothers wanted
the nurse to be part of “family life” but did not want the nurse to be possessive of the
child who is technology dependent which required the nurse to walk a fine line. In other
words, they wanted the nurse to be there but not be there (Cavanagh, 1999). Therefore,
attributes of the ideal home care nurse were that the nurse would be caring,
knowledgeable, able to incorporate developmentally appropriate activities and sensitive
to family boundaries.
Mothers frequently were the liaison with home health care nurses. A mother’s
role included monitoring family boundaries, communicating and negotiating child rearing
expectations, ensuring that confidence was not betrayed and that the nurse was not over-
protective of the child (Cavanagh, 1999; O’Brien et al., 2002). Nurses in the home were
seen as supportive yet disruptive (Wang & Barnard, 2004) as their presence affected
privacy and family dynamics (O’Brien et al., 2002) such as marital, sibling and parental
relationships (Murphy, 1997). At times, judgments were made by nurses regarding family
lifestyle (Murphy, 1997). Parents also felt that health care professionals did not value
their experiential knowledge. Experiential knowledge with medical knowledge helped
them provide individual care so that they could detect minute changes that signaled that
their child was ill (Glendinning & Kirk, 2000; Kirk et al., 2005). Some health care
professionals however were threatened by the expertise of the parents (Glendinning &
Kirk, 2000).
Conversely, nurses were also seen in a positive light. There were sometimes
viewed as a member of the family therefore provided families with much needed social

91
support (Kuster, 2002) and decreased the sense of isolation particularly in socially
marginalized families (Cohen, 1999). Nurses helped mothers to develop increasing self
confidence and satisfaction by giving positive feedback on their skills and strategies used
to care for the child who is technology dependent (Lee, 1996; Wilson et al., 1998).
Having a primary nurse was highly valued from a continuity stand point (Kirk &
Glendinning, 2004) as was high quality and consistent nursing care (Tommet, 2003).
Lack of this consistent, high quality nursing care contributed to family disorganization
(Tommet, 2003). Therefore, while there were issues at times with home health care
nurses over control of the child, family boundaries, and privacy, nurses were also seen as
a valuable asset to families particularly related to social support and positive feedback
that helped to boost the mother’s self confidence.
Lack of Discharge Preparation
Studies of families with children who were technology dependent consistently
found that parents felt they lacked adequate preparation for the experience prior to
discharge. Parents felt there was a lack of preparation for the technical care they would
have to provide (Wang & Barnard, 2004) as well as the emotional strain they would
experience (Judson, 2004). Some had only preparation for the care of the child and not
the “rest” of what home care entails such as working with the nursing agency or the
weight of responsibility for managing home care (Allen et al., 1994; Carnevale et al.,
2006; Murphy, 1997; Torok, 2001).
Neuss (2004) found that all 12 mothers in her study reported that no amount of
training would have prepared them for the care that was required at home. Some mothers
suggested that hospital staff increase the family’s responsibility for the infant’s care and

92
equipment prior to discharge so that they can ease into the role (Kirk & Glendinning,
2004; Torok, 2001). Other suggestions were that families have multiple support people
trained for respite and that hospital staff should check up on families 6-12 months after
discharge to assess how they are adjusting to home care (Torok, 2001). Another
suggestion was to tell parents there are demands and hardships but also deep enrichments
and rewarding experiences (Carnevale et al., 2006).
Thyen et al. (1998) proposed that discharge planning and support needs to not
only focus on the child but also the prevention of secondary social and psychological
morbidity of caregivers. Therefore, findings from the literature suggest that increased
preparation and training prior to discharge should include not only technical care but
information on how to manage the many demands related to caring for a technology
dependent child. Furthermore, facilitating access to psychosocial supports would greatly
assist with prevention of social and psychological morbidity.
Positive Gains
Despite all of the challenges and hardships involved in caring for a child who is
technology dependent at home, parents also spoke of the positives. Many reported
satisfaction seeing the emotional, developmental and social growth and improved health
of their child following discharge from the hospital (Kuster, 2002; O’Brien, 2001; Wang
& Barnard, 2004) as well as improvement in the family situation (Torok, 2001). Many
mothers felt they were better able to assess their child’s day to day needs than any
professional (Neuss, 2004). Families, particularly those who are socially marginalized
experienced increased self esteem by learning skills necessary to care for the child who is
technology dependent (Lee, 1996; Neuss, 2004; Cohen, 1999). Mothers felt competent

93
and proud of what they had accomplished. These families also had the experience of a
close relationship with a health care professional who could serve as a positive role
model as well as decreased their social isolation (Cohen, 1999).
In a study of 14 families with children who were ventilator dependent, Allen et al.
(1994) found that 93% liked the decreased travel to the hospital, 71% reported improved
emotional condition, 50% thought the situation between siblings had improved, 43% felt
they had greater control, and 36% said that the medical condition of the child who is
technology dependent had improved. Some mothers reported that they had acquired
positive personality traits such as more patience and increased spirituality as a result of
caring for the child who is technology dependent (Neuss, 2004). Others felt that caring
for the child who is technology dependent had brought the family closer together. Still
others wanted to help others in similar situation. Furthermore, almost half of mothers in a
study by Neuss (2004) were thinking of a future career in a medical environment. Parents
living in uncertainty experienced growth when they were able to let go of trying to
achieve predictability and control and learned to live in the present (Tommet, 2003).
Finally, mothers received pleasure from interaction with the infant and their role as a
mother (Lee, 1996). Therefore, despite all the hardship and challenge related to caring for
a child who is technology dependent, mothers reported positive growth for themselves,
their families, and their child.
Summary
This review of the literature regarding the child who is technology dependent and
their families revealed many research gaps. Standardized instruments measuring severity
of illness would be helpful with this population. Other gaps are the absence of

94
longitudinal, quantitative studies that address how a culturally diverse sample of families
manage the child who is technology dependent who receives home care, particularly
related to normalization. Another gap in the research is the prospective account of the
first few months following discharge. There is also the need to examine the positive
aspects of mothering the child who is technology dependent in a longitudinal study over
the year following discharge matched with healthy controls. Furthermore, an additional
gap in the research literature is a study that would examine the personal characteristics of
parents, characteristics of child who is technology dependent and illness and their
relationship to distress. This would greatly assist with development of an intervention to
assist families, particularly mothers in the management of the child who is technology
dependent. Last, it is important to study which families are at greatest risk for family
dysfunction and distress so interventions can be developed that can assist with family
functioning.
Normalization as a Management Strategy
Definition and Attributes
Normalization is a concept that includes cognitive and behavioral dimensions and
is defined as a pattern of family response to a child with a chronic condition, an ongoing
process of accommodating the child’s evolving social, emotional and physical needs
(Deatrick et al., 1988; Morse et al., 2000). This includes “adjusting the environment to
provide normal life experiences that will meet the child’s evolving social, physical,
intellectual and emotional needs” (Murphy, 1994, p. 10) and at the same time manage
family life and activities so that they can lead as close to “normal” of a family life as
possible (Murphy, 1994). Attributes of normalization include that a family “(a)

95
acknowledges the condition and its potential to threaten their lifestyle, (b) adopts a
‘normalcy lens’ for defining child and family, (c) engages in parenting behaviors and
family routines that are consistent with ‘normalcy lens’, (d) develops a treatment regimen
that is consistent with a ‘normalcy lens’, and (e) interacts with others based on a view of
child and family as normal” (Deatrick et al., 1999, p. 211).
As one can surmise from the above attributes, a family’s definition of “normal” is
guided by a philosophical approach and not necessarily the reality of the situation,
primarily because parents choose to attend to what is “normal” and disregard what is
abnormal about their situation (Murphy, 1994). Families therefore, modify and redefine
“normal” over time to fit their current circumstances and ongoing uncertainty (Rehm &
Franck, 2000). Consequently, the child with a chronic illness is treated as “normal” living
a life like others in the outside world without illness so as not to be seen as deviant from
societal expectations; thus enabling them to “fit in” (Morse et al., 2000; Young, 1995).
Therefore, reality is reconstructed to emphasize those aspects of life that remain
unchanged despite the chronic illness. Normalization is used to manage the disparity
between the preferred views of their family life as “normal” and the problems and
challenges they face in their everyday life (Rehm & Franck, 2000).
Normalization is now seen as a clinical standard in judging family management
effectiveness and health care professionals encourage families who have a child with a
chronic condition to live their lives as close to normal as possible and continue
interactions with others (Deatrick et al., 1999). Other researchers have questioned this
standard and ideology of normalization, viewing it instead as a Western ideology that is
shaped by socio-political, economic and historical factors and not necessarily embraced
by Chinese immigrants to Canada (Elfert, Anderson, & Lai, 1989). Young (1995)

96
however, developed a theoretical framework to study the strengths and management
strategies African American families’ use when a member has a chronic illness.
Management strategies for these families included normalization due to the pressures
from society and the hazards of being considered “different” such as the stigma
associated with it (Young, 1995). Therefore, while many families use normalization in
response to a child’s chronic illness this is not always the case with families that are from
non-Western countries.
Some researchers emphasized exploring the childhood chronic illness experience
through the perspective of social stigma (Chisholm, 2000). Joachim and Acorn (2000)
however, encouraged researchers to examine chronic illness through the normalization
lens and the stigma lens. They argue that “in order to capture and understand the dynamic
and evolving experience of people with chronic condition, researchers should consider
the interdependence of the two perspectives and avoid assumptions that derive from
stigma or normalization alone” (p. 37). The authors posit that to study the chronic illness
perspective from a stigma lens overlooks the energy available in the process of
normalization, however, using only the normalization lens “may underestimate the power
of social context” (Joachim & Acorn, 2000, p. 45).
Normalization Management Behaviors
Many have researched management behaviors associated with normalization.
Management behaviors, also called strategies, are “discrete behavioral accommodations
that family members use to manage the illness on a daily basis” (Knafl et al., 1996, p.
316). Clarke-Steffen (1997) developed a model regarding the process of adaptation to the
diagnosis of cancer in a child that included use of management strategies to construct

97
reality as well as to construct a new normal. Cohen (1993) found that families dealing
with childhood cancer manage uncertainty by developing strategies to create certainty
and in the process create a “New Normal”. Gravelle (1997) described how parents
manage their child’s illness on a daily basis by “facing adversity” based on a changing
definition of adversity.
Other authors described management strategies within the process of defining the
ill family member as normal (Robinson, 1993), and in relation to parenting (Scharer &
Dixon, 1989). In a qualitative study of parents and children living with HIV, Rehm and
Franck (2000) identified long term goals for normalization and management strategies to
meet the goals. The goal of staying healthy meant making lifestyle decisions and actively
participating in treatment. Facilitating participation in school and social activities meant
managing the stigma and being selective regarding disclosure. Enhancing the social and
emotional health of family members was a goal that was managed by enlisting extended
family members to help (Rehm & Franck, 2000).
Sullivan-Bolyai, Knafl, Sadler, and Gilliss (2004) presented a list of management
responsibilities and activities for parents caring for a chronically ill child. The list was
developed to help address day-to-day management activities and responsibilities. The
four major categories include managing the illness; identifying accessing and
coordinating resources; maintaining the family unit; and maintaining their own
emotional, physical and spiritual health.
Jerrett (1994) and May (1997) in their research of children with Juvenile
Rheumatoid Arthritis and low birth weight infants, respectively, found that normalization
and management strategies were accomplished through learning care required by their

98
child. Jarrett (1994) found development of a routine and schedule assisted with
normalization and fostered integration of necessary caregiving into family life.
Gallo and Knafl (1998) in a secondary analysis of 58 families identified three
approaches to illness management: strict adherence; flexible adherence; and selective
adherence. No differences were found in management approaches across disease
conditions. Knafl and Deatrick (2002) found that families who choose to focus on
normalcy use a flexible approach regarding treatment regimens and incorporated the
treatment in the day-to-day routines of the family. Hatton, Canam, Thorne, and Hughes
(1995) concur with these findings that increased confidence in parents of diabetic infants
and toddlers led to more flexibility in the management of routines. Additionally, Thorne,
Radford and McCormick (1997), in a qualitative study of children with long term
gastrostomy tubes found that families adapted by manipulating feeding schedules and
treatments to suit the quality of life for the child and family. Therefore, family
management behaviors to accommodate a child’s chronic condition that incorporated
flexibility in adherence to medical regimen, assisted families in the normalization process
and led to a more desirable quality of life.
Family Management Style Framework
Knafl et al. (1996) comprehensively explored the use of family management
strategies to accomplish normalization. In a 1-year qualitative study of 63 families that
included both parents, the ill child and the siblings, the authors delineated five different
types of family response to childhood chronic illness Family Management Style (FMS)
that reflect the degree of normalization. Normalcy is the overriding theme in the Thriving
FMS and the dominant theme in the Accommodative FMS. The Enduring, Struggling and

99
Floundering FMS use consecutively lower degrees of normalization. The FMS
framework developed by Knafl and Deatrick (1990) guided design of this study. No
relationship was found between FMS and disease, ethnicity, or socioeconomic status.
Additionally, 37% of families in the study experienced long term difficulty managing the
child’s illness.
The FMS framework was developed by Knafl and Deatrick and has continued to
be refined since the 1980’s guided by further research by their team as well as others
(Knafl & Deatrick, 1990; Knafl et al., 1996; Knafl & Deatrick, 2006; Deatrick et al.,
2006). Knafl and Deatrick are also responsible for concept development related to
normalization (Deatrick et al., 1999; Knafl & Deatrick, 1986; Knafl & Deatrick, 2002).
FMS is directly related to normalization in that FMS is defined as a pattern of approach
regarding how a family manages both family life and the child’s serious health care needs
(Knafl & Deatrick, 2006).
FMS is comprised of components that include the following: definition of the
situation which is the identification of significant events and the subjective meaning for
the individual; management behaviors which are behavioral accommodations made by
family members to manage on a daily basis; and perceived consequences which includes
whether the illness is in the foreground or background in family life (Deatrick et al.,
2006). Definition of the situation includes whether the parent views the child “normal”
and focus on capabilities or tragic and focus on vulnerabilities; the illness view whether
seen as serious and disruptive or if seriousness is downplayed; mutuality of parent views
regarding child, illness and approach to illness management; and management mindset
regarding the ease or difficulty of the treatment regimen (Deatrick et al., 2006).

100
The management behaviors include a parent’s overall approach such as the ability
to develop a routine related to illness management and more specifically the parenting
philosophy regarding goals to ensure a normal life for the child; and the management
approach which is the development of routines and strategies to manage the illness as
well as incorporate the care into family life (Deatrick et al., 2006). Perceived
consequences includes the family focus which is parental assessment of balance between
aspects of family life and illness management ranging from family focus in those who are
using normalization to an illness focus in families who are floundering with illness
management; and future expectations according to both parents whether positive or
negative outlook. The socio-cultural context is those contextual factors that influence
how the family defines and manages the illness and the consequences of the illness they
perceive. These factors include cultural practices and beliefs, financial,
personal/individual and support received from the health care provider/health system
(Deatrick et al., 2006). The FMS Framework is currently in the process of being
translated into a qualitative instrument called the FMS Survey. Field testing is being
completed to test the instrument’s psychometric properties (Knafl & Deatrick, 2006).
Goals of Normalization
In a grounded study of parents of children with perinatally acquired HIV,
Santacroce, Deatrick and Ledlie (2002) found an evolution of Family Management Style
(FMS). Different management strategies were employed to adjust to the change in the
child’s medical condition and the stigma placed on the child from society. Other goals of
normalization described in the literature include that the child with a chronic illness be
integrated into the family without being the central focus. Additional goals are that the

101
child’s competencies are maximized; the child develops independence, is well-adjusted
and develops into a functioning member of the family and society (Murphy, 1994).
Effects of Normalization on Families
Findings from research regarding normalization include the impact of the child’s
chronic illness on the family. Dashiff (1993) found an increase in family cohesion,
emotional stress, and parental role function with a concomitant decrease in spousal role in
families of adolescent female diabetics. Hatton et al. (1995) found that half of the
mothers of diabetic infants and toddlers quit gainful employment after the child was
diagnosed. Additionally, parents had to change their lifestyle in order to accommodate
the child’s diabetes and experienced marital strain and miscommunication.
Other studies using qualitative techniques described the experience of parenting a
child with a chronic condition as “parent straddling” (Johnson, 2000), a “balancing act”
(Morse et al., 2000). Both discussed the struggle a parent experiences in living with the
view of their child as “normal” when realizing they are disabled. The parents felt caught
between assisting their child in the “disabled as normal world” and the outside “everyday
as normal world”.
Threats to Normalization
Threats to achieving normalization noted in the literature include:
chronic/sustained uncertainty (Cohen, 1993; Haase & Rostad, 1994); parental conflict;
developmental transition of adolescents; poor illness control (Dashiff, 1993); and the
“problem-saturated perspective” of health care providers (Robinson, 1993). Knafl and
Deatrick (2006) stated that barriers to normalization also include increased treatment
complexity, need for stigma management and a parental focus on ways the child is

102
different from peers. Additional factors that can affect the use of normalization are age of
the child (greater difficulty with adolescents), time since diagnosis (decreased
normalization if less than one year since diagnosis), lack of knowledge, visibility of
condition, and cultural issues (Asian populations have greater difficulty with
normalization) (Murphy, 1994).
Knafl and Deatrick (2002) also examined barriers to normalization in a
qualitative, longitudinal study they had conducted with 63 families of children with
chronic conditions. In families who, according to their qualitative grid, had never
experienced normalization, life was viewed as a series of multiple, ongoing difficulties.
Illness was the focus of family life and the treatment regimen was viewed as a significant
burden with behaviors that made the family different from other families. Their parenting
style and view of the child had changed as a result of the illness and conflicts with the
child were mainly regarding adherence to the treatment regimen. The child was viewed as
a tragic figure and parents were consequently protective and indulgent. Parents perceived
that the child’s illness had negative consequences for family life and had contributed to a
decreased quality of life. Illness management was seen as a source of conflict and a
burden. Spousal conflict occurred when parents did not hold a shared view of treatment
management (Knafl & Deatrick, 2002).
Knafl and Deatrick (2002) found that in families who had experienced
normalization earlier in the study but had changed in the later data collection phases did
so due to a change in the disease process. Once there was better control of the illness,
families shifted again to use of normalization. Illness management was part of the family
routine if the illness was in remission or well controlled. Once the illness flared up again
the illness was brought to the foreground. Knafl and Deatrick (2002) also stated that the

103
MAJOR BARRIER to normalization is parental conflict and not illness management
because the continual tension keeps the illness a focus of family life.
Strategies to Promote Normalization
Strategies parents use to help promote normalization were discussed in the
literature. Murphy (1994) found that families who use normalization ignore the abnormal
situation and expect others to do the same and prefer to attend to the “normal” aspects of
the child. Everyday life is carried on as usual despite the difficulty and parents reframe
the focus or perspective. Parents engage in usual parenting activities and participate in
normal activities by maintaining a routine. They are willing to allow the child to
experience “normal” developmentally appropriate activities without the parent’s
protection. Parents desensitize others or get people “used to” visible differences. The
child is integrated into the family and is not the central focus so there is less of a feeling
of vulnerability or stigma of being different. Parents foster the child’s independence and
positive self-perception and see their child as less affected than others. These families
tend not to be involved in groups for children with disabilities (Murphy, 1994). Knafl and
Deatrick (2002) found that families recognized the seriousness of the illness but hold the
view that the child and family are unchanged in important ways (normalcy lens). Having
a view that the child and family are “normal” sets the stage for managing the illness and
allows the family to sustain the usual pattern of family and child functioning (Knafl &
Deatrick, 2002).
Morse et al. (2000) studied 17 school age children who were ventilator dependent
and their parents at a day camp to determine “what is normal” from the perspective of the
child. Participant observation of the children in the day camp and interviews of the

104
parents were performed. Findings include that these children identified two distinct social
reference groups: the disabled world of disabled as normal and outside world of everyday
as normal. Mothers in the study were able to identify with both groups according to the
child’s ability, needs and risk. The child with a disability who was able to normalize
compared their ability to identify with both worlds according to need. The researchers
propose that normalization includes a process of identification with both the cultural
dominant group that is perceived as “normal” cognitively and the disabled children whom
they could identify with both physically and cognitively (Morse et al., 2000). Strategies
used by these children to fit in with the culturally dominant group was to use talents or
abilities to “fit in” with each world, seek commonalities to be “like them”, develop their
own capabilities and stretch the limits of their disability. Mothers introduced aspects of
the everyday as normal to their children by involving them in activities to heighten their
awareness of what was similar and different from others. The researchers propose that
this process of comparison was a foundation for normalization and gave the children an
opportunity to become independent (Morse et al., 2000). Factors that influenced
identification with both worlds were the age of the child, degree of social isolation,
degree of disability and the family.
Three qualitative studies described factors that promote normalization in families
of children who are technology dependent. Judson (2004) examined the process of
mothering a child who is dependent on parenteral nutrition in a qualitative study of 19
mothers. The researcher developed a theory of protective care comprised of 3 phases:
gaining control, taking control and maintaining control. Judson (2004) found that
normalization was related to the mother’s use of flexibility. Additionally, discipline came
up in interviews as a way to promote normalization. Promoting normalization, however,

105
began with efforts at fostering acceptance of the child. Key factors to acceptance were
related to behavior and discipline; the child’s appearance; and the child’s ability to
participate in age-related social activities.
In a study of two African American single mothers of children who are
technology dependent, Lee (1996) found that both mothers did things to make the infant
seem normal or tried to make the experience seem normal. The mothers used strategies
such as camouflaging the tracheostomy or removing the oxygen and moving about the
house so the infant could be seen as normal (Lee, 1996). Carnevale et al. (2006) concur
with these findings. In a qualitative study of 38 family members of 12 children who were
ventilator dependent, the researchers found participants promoted normalization by
normalizing the home. Medical devices and equipment were hidden or camouflaged so
that it would not dominate the home environment. Other strategies included that the
ventilator was covered with a cloth or towel and the oxygen was hidden under a table.
Also, hospital beds were covered with colorful covers so that the controls and special
mattress were not visible.
Child’s Psychosocial Adjustment
Only one study quantitatively addressed the use of normalization by parents. In a
study of 76 mothers and their children with chronic physical disorders (CPD) age 8-12
years, Murphy (1994) found that a families’ use of normalization was related to the
child’s psychosocial adjustment. The researcher specifically developed the Normalization
Scale (Murphy & Gottlieb, 1992) for the study guided by the concept of normalization
and the FMS framework (Deatrick & Knafl, 1990). Two hypotheses were tested in this
study: 1) Families who use high levels of normalization will have CPD children with high

106
personal and social adjustment and role skills and 2) Families who use high levels of
normalization will have CPD children with a high sense of self-competence. Specific
findings include that the mother’s perception that the family and other people perceived
the CPD family as normal was strongly related to overall high personal adjustment, good
peer relations and productivity in the child as well as low anxiety, depression, dependent
and hostility.
In this study, normalization was not related to a child’s perception of self
competence. The researcher proposed that this is because normalization is a philosophical
approach and a mother’s perception and appraisal of the situation is important to the
psychological adjustment of her child. To test the study’s first hypothesis, the researcher
found that the total score for the Personal Adjustment and Role Skills Scale and
specifically the anxiety/depression, withdrawal, and productivity subscales were
positively correlated with the “Actual Effect of the CPD on the Family” subscale of the
Normalization Scale (Murphy, 1994). Using regression analysis, it was found that the
best predictor of anxiety, depression, dependency, hostility and productivity was the
Normalization subscale of “Perception of Child and Family by Self and Others as
Normal”. Withdrawal was best predicted by the Normalization subscale “Actual Effect of
the CPD on the Family”. Using regression, mothers who perceived their child to be less
anxious and depressed as well as more productive also reported that their family and
others perceived the family and CPD child to be normal (Murphy, 1994).
The researcher did report a potential problem of wording on the Normalization
Scale. Mothers were asked to compare their family to both normal and CPD families and
a second set of items asked mothers about how others compared their family to these
same two groups. Factor solution showed that the mothers however, did not make the

107
distinction. The mothers instead distinguished between normal and CPD family rather
than distinguishing between who was judging the family. The researcher proposed that
this might also be due to the fact that they may not identify themselves as a CPD family
(Murphy, 1994).
Normalization and the Child who is Technology Dependent
One qualitative study examined the use of normalization in families of children
who are technology dependent. Rehm and Bradley (2005) analyzed the applicability of
normalization attributes for families raising a child who is technology dependent. The
study included 30 families of children who were technology dependent and
developmentally delayed of either Caucasian or Hispanic ethnicity; 28% had household
incomes <$10,000. The researchers found that developmental delays compounded the
effects of the chronic condition thereby affecting how families were able to organize and
manage daily life. They concluded that families of children who are technology
dependent do not fit the published attributes of normalization developed by Deatrick and
Knafl.
Rehm and Bradley (2005) reported that denial was not possible, therefore,
families incorporated differences into what they considered normal. Families reframed
changes in lifestyle related to the chronic illness as positives but did not consider them
typical or desirable. They considered family life as “crazy normal” due the need for
frequent intervention and continued vigilance. Families attempted to create a family
routine but with many limitations due to the illness however this did not necessarily
decrease the quality of family life. School helped to normalize family routines and
provide respite; allowing children to participate in a “normal” childhood activity. Due to

108
the fragility of the child’s condition, parents were not able to modify the treatment
regimen very much nor were they able to count on a predictable routine. Parents did not
view the child or family as normal; they realized the special needs and differences and
felt conspicuous in public due to the child’s equipment, appearance and behavior at
times. Many were upset regarding how their child was treated by others; their child was
often left out. The researchers concluded that a normalcy lens was impossible because
families needed to constantly attend to the care of the child and could not place the
condition in the background for long. Parents of children who are technology dependent,
the researchers proposed, did not relate to others as if their life was normal but strove
instead to reach a stable, positive state for all family members but not necessarily one the
was “normal”. Therefore one qualitative researcher, concluded that normalization can not
be achieved in families of children who are technology dependent and developmentally
delayed.
Summary
Noteworthy is the dearth of quantitative research regarding normalization,
particularly the relationship between the parent’s use of normalization and their own
psychological well-being. Additional gaps in the research regarding normalization
include the use of small sample sizes of mostly school age chronically ill children.
Sociocultural context and developmental transitions and their effect on family response
and management of chronic childhood conditions are largely unexplored. In particular,
the use of normalization by families of technology dependent children was explored in
only one qualitative study (Rehm & Bradley, 2005). Few studies examined normalization

109
from the viewpoint of both parents. Many of the studies did not describe the ethnicity of
the sample and in those that did, the majority was Caucasian.
Family Functioning
Following discharge from the hospital, children who are technology dependent
are cared for by their families at home placing increased demands on the family due to
the numerous treatments, health care appointments and disruptions in the everyday
routine. This disruption requires a substantive change in the structure and functioning of
the family often requiring a redistribution of responsibilities and roles (Clawson, 1996).
History of the Concept
Historically, the concept of family functioning was first discussed in the 1950’s
by a group of psychologists from McGill University and later McMaster University who
were researching ways to classify and assess families, particularly in relation to family
therapy needs. The ensuing model, The McMaster Model of Family Functioning, has
structural-functional theory as its base. Structural-functional theory views the family as a
social system but places greater emphasis on family functions such as meeting member’s
physical and psychological needs of food, clothing and socialization. In addition, this
theory emphasizes family relationships between the family, individual members, family
structure and the ability of the family to perform family functions.
McMaster Model of Family Functioning
The McMaster Model emphasizes family structure and organization as well as
transactional patterns. The focus is on three dimensions that have the greatest impact on
the emotional and physical well-being of the members: basic task area such as food and

110
shelter; developmental task area that occurs as a result of change over time in
development of the family such as birth of first child; and the hazardous task area such as
the way the family handles an illness crisis (Goldenberg & Goldenberg, 1992; Neabel,
Fotherfill-Bourbonnais & Dunning, 2000). Dimensions of family functioning related to
the three task areas include family communication, family problem solving, family roles,
affective responsiveness, affective involvement, and behavior control (Goldenberg &
Goldenberg, 1991).
Feetham Model of Family Functioning
Suzanne Feetham used the McMaster Model as a foundation and began her work
with the concept of family functioning, developing The Feetham Family Functioning
Survey (FFFS) in the 1970’s. According to Feetham, family functioning is “those
activities and relationships among and between persons and the environment which in
combination enable the family to maintain itself as an open system” (Roberts & Feetham,
1982, p. 231). The FFFS has as its base the family ecological framework, general systems
theory and Duvall’s theory of the stages of family development. The family ecological
framework identifies the family as the basic unit which involves examining the nested
parts that make up the system, the family’s relationships, the environment, and the tasks
performed by the family resulting from the relationships of the parts. The focus of the
ecological theory is the interdependence of family members with the environment and
with one another. According to the ecological framework, the family system is dynamic
and continually in a state of change and adaptation. General systems theory views the
family as a whole rather than separate parts and in addition as part of a larger supra-
system such as the community (Roberts & Feetham, 1982).

111
Up until the FFFS was developed, instruments only addressed the relationship
between the family and each individual such as the parent/child or husband/wife.
Feetham identified and measured two additional major areas of family functions as
relationships: the relationship between the family and subsystems (relatives, friends and
neighbors) and the relationship between the family and the broader community (schools
and place of employment).
Wright and Leahey Model of Family Functioning
Other researchers have explored and developed instruments to measure the
concept of family functioning. Wright and Leahey (1994) developed the Calgary Family
Assessment Model based on general systems theory, cybernetics, communication theory
and change theory. The model includes three assessment categories: structural,
developmental and functional. Structural assessment includes who is in the family, the
connections among the members and the family’s context. The developmental assessment
of families includes examining the stage of family development as delineated by Duvall
and fulfillment of the developmental tasks associated with that stage. The family
functional assessment includes “how individuals actually behave in relation to one
another” (Wright & Leahey, 1994, p. 80).
Two basic aspects of family functioning, instrumental and expressive functioning
were identified by Wright and Leahey (1994). Instrumental functioning refers to routine
activities of daily living such as eating, sleeping, changing dressings, and giving
medications. This area of functioning takes on greater significance for parents with a
child who is technology dependent as they would have to alter the manner in which they
take care of instrumental tasks. Expressive functioning includes nine subcategories:

112
emotional communication; verbal communication; non-verbal communication; circular
communication; problem-solving; roles; influence; beliefs; alliances/coalitions.
Therefore, while the Calgary Assessment Model takes into account instrumental and
expressive functioning it does not assess family functioning relative to relationships
outside the immediate family.
Structure and Process of Family Functioning
The literature not only describes family functioning in terms of instrumental and
expressive functioning but in terms of structure and process as well. Bauman (2000), in a
review of concepts germane to family nursing, described family function as a
phenomenon that is related to the reciprocity between the family and illness/wellness that
is then linked with family structure and process. A frequent question therefore, related to
family functioning is “what does it (family) do?” meaning the actual activities which
implies a process. The process-based view of family functioning includes a broad range
of behaviors and implies an inter-relationship between the individual and the family and
the individual and the environment. These behaviors have been described as those
activities that are essential to family survival such as socialization, protection,
procreation, education and economic concerns (Roberts & Feetham, 1982).
Lasky et al. (1985) delineate a structural view of family functioning which
includes aspects such as boundary maintenance, authority and dominance. In addition,
they identified eight bipolar dimensions that characterize family relationships using the
structural view of family functioning; individuation vs. enmeshment; mutuality vs.
isolation; flexibility vs. rigidity; stability vs. disorganization; clear communication vs.
distorted communication; role compatibility vs. role conflict; clear vs. unclear or

113
distorted perception; clear vs. diffuse or breached generational boundaries (Lasky et al.,
1985). Family functioning can also be viewed as an outcome based on a systems model.
Outcomes related to family functioning could include the care of dependent family
members, satisfaction with relationships, maintenance of family possessions, regulation
of family members’ behaviors and the transmission of family patterns across generations.
An analysis of the literature reveals a wide variety of definitions of family
functioning. Theoretical foundations for the definitions, models, and descriptions of this
concept include general systems theory, structural-functional theory, ecological theory,
change theory, communication theory, cybernetics and the theory of family
developmental stages. Donabedian’s model of structure, process, and outcome is also
implied in many of the definitions and the instruments developed to date that measure the
concept of family functioning.
Cultural Context of Family Functioning
Cultural contexts that influence the conceptual meaning, definition and
consequently the measurement of family functioning are of paramount importance. Each
culture and each family defines what is considered “family” and furthermore prescribes
norms and values on family functioning such as roles, tasks, communication and division
of labor assignments. A family’s definition of family functioning is influenced by the
broader systems in which they are nested such as the country, region, and neighborhood
and by demographic variables such as ethnicity, race, social class, and religion (Wright &
Leahey, 1994). Therefore, what is expected as far as the performance of various functions
and by whom they are to be performed is culturally influenced. In addition, perception is
an integral component of family functioning and is influenced not only by the cultural

114
context but by the individual members’ belief system regarding how a family should
function. The individual’s perception and expectations in turn influence the family
member’s level of satisfaction with family functioning. The ultimate goal of these
functions is to keep the family unit in a state of homeostasis thereby allowing growth of
the individual and family as a unit. Furthermore, by maintaining a state of homeostasis,
the health of all the members is promoted.
Family Development and Family Functioning
Differences in the meaning of family functioning also occur related to the stage of
family development as delineated by Duvall. Duvall’s model delineates the
developmental tasks of the family and is based on the premise that family growth occurs
in predictable stages. Instrumental and expressive functioning differs over time related to
the particular stage that the family is experiencing such that roles and division of labor
assignments may go through changes depending on the instrumental functioning demands
(Dickstein, 2002). In addition, historical context has brought about changes in the
meaning of the concept family functioning. Roles for family members related to
instrumental functioning have changed in many families over the past 25 years with more
male partners performing household and child care duties and an increased rate of women
working outside the home.
Comprehensive Definition of Family Functioning
A comprehensive definition of family functioning is an ongoing, dynamic process
that changes with developmental stages and crisis events and is comprised of inter-
relationships and inter-dependent parts. It is influenced by cultural context, members’
expectations and perceptions and has the goal of balancing equilibrium and

115
disequilibrium so that individual growth can occur and health is promoted (Toly, 2003).
Additionally, according to Roberts and Feetham (1982), family functioning is the
parent’s perception and level of satisfaction with the relationship between the family and
individual members, the subsystems and the community.
Preterm Infants and Family Functioning
Some studies reviewed examined the relationship between preterm infants and
family functioning. Thompson et al. (1993) looked at processes related to maternal
distress using the Family Environment Scale. At 3-6 weeks and 6 months after discharge,
family supportiveness decreased while conflict increased. McCain (1990) also used the
Family Apgar Scale and the Family Dynamics measure to determine if risk factors related
to preterm birth were associated with family functioning when the preterm child was 2-4
years old. Using multiple regression analysis, the researcher found that longer neonatal
hospitalizations but not child’s developmental status, length of hospital stay, adequacy of
family finances, parental age and marital status continued to be associated with poorer
family functioning related to role reciprocity and conflict for mothers (McCain, 1990).
Maternal Mental Health and Family Functioning
Weiss and Chen (2002) studied the factors influencing maternal mental health and
family functioning in 125 low birth weight infants and their mothers during the infant’s
first year of life. Specific aims of the study were to determine the effect of infant’s
medical vulnerability and psychosocial context of caregiving on the mother’s mental
health during the infant’s first year of life. Additionally, the researchers examined the
effect of the infant’s vulnerability on family functioning during the first 3 months of life.
The sample was diverse with 28% Hispanic, 19% African-American and 7% Asian or

116
Native American with a mean gestational age of 32 weeks. A total of 81% lived with
their partner but not necessarily a spouse; 54% were living below the poverty level; 61%
were employed at least part time. Family functioning was measured with The Family
Adaptability and Cohesion Scales, The Family Satisfaction Scale and the Family Crisis
Oriented Personal Evaluation Scales. Maternal mental health was measured using the
DSM-IV and Brief Symptom Inventory. Measures for infant physical health problems
were unstandardized and measured the infant’s symptoms.
Findings include that the infant responsiveness and severity of the child’s health
problems were associated with a mother’s overall mental health functioning (p<.005).
Family functioning aspects (adaptability and cohesion) had the strongest and most
consistent correlations with maternal mental health as well as perceived emotional
support. Interestingly, family cohesion explained 22% of the variance in severity of
maternal mental health symptoms. Severity of the infant’s illness was correlated with
only one aspect of family functioning-family use of internal coping strategies. Infant
responsiveness was significantly related to family cohesion and adaptability (p<.01)
while clarity of cues were less related to family cohesion and adaptability (p<.05) (Weiss
& Chen, 2002). Therefore, severity of the preterm infant’s illness and the infant’s
responsiveness were significantly related to a mother’s mental health status. Furthermore,
family functioning, particularly family cohesion explained a large percentage of the
variance of the mothers mental health symptoms. Interestingly, the infant’s
responsiveness was significantly related to the family cohesion and adaptability, aspects
of family functioning.

117
Severity of Illness and Family Functioning
In the research literature, an increased severity of illness has been associated with
poorer family functioning. Ostwald et al. (1993) studied 151 caregivers of frail elderly
and medically fragile children. Findings include that the ability of the caregivers to
continue managing the care of the child was related to the degree of physical impairment.
Those caregivers with children with severe neurological and respiratory problems had the
most difficulty. A total of 25% of the caregivers felt that they could not manage much
longer with the current arrangement (Ostwald et al., 1993).
Unpredictability of Illness and Family Functioning
Dodgson et al., (2000), in a study of 173 mothers and 150 fathers of children 12-
30 months diagnosed with a chronic physical illness within the last year, examined the
relationship between unpredictability of a child’s illness and family functioning using the
Impact on Family Scale. The researchers found that for mothers, unpredictability of
symptoms was significantly related to greater family/social disruption (p=.001),
emotional strain (p=.001) and financial burden. Fathers had similar findings-
unpredictability of symptoms was related to greater family/social disruption (p=.002).
Therefore, unpredictability of a child’s illness significantly correlated with family and
social disruption and was the source of greater emotional strain than for those with
symptoms that were more predictable.
Factors that Promote Family Functioning
Several factors have been found to promote family functioning. Findings from
past research indicate that a decreased severity of illness, greater predictability of the
child’s symptoms, availability of intimate and peer support, greater proficiency in illness

118
management, gender of the child (female), and a trusting relationship with a home health
care nurse were related to better family functioning (Dodgson et al., 2000; Kiernan, 1995;
Drotar, 1997; Kohlen et al., 2000; Ostwald et al., 1993).
Burke, Harrison, Kauffmann, and Wong (2001) examined the effect of a family-
focused intervention on family functioning in a longitudinal study. A sample of 115
children ages 1-15 with complex chronic illnesses were randomly assigned to Stress-
Point Intervention by Nurses (SPIN) or usual care. The researchers were examining
whether the SPIN families would have more satisfaction with family functioning and
better parent coping after hospitalization. The Feetham Family Functioning Survey and
Coping Health Inventory of Parents were completed by parents and results revealed that
SPIN parents were significantly more satisfied with family functioning and had better
coping than parents receiving usual care. Only 4% of SPIN parents reported poorer
family functioning versus 38% in usual care group while 31% of SPIN families had better
family functioning compared to only 19% of the usual care group (p<.0001) (Burke, et
al., 2001). Thus, interventions for families of children with chronic conditions related to
family functioning have shown that families were statistically more satisfied with family
functioning following the intervention than those receiving usual care.
Normalization and Family Functioning
In a longitudinal, triangulated study, Knafl and Zoeller (2000) found an
association among family management styles and family functioning using the Feetham
Family Functioning Survey. Families who used the floundering family management style,
the lowest level of normalization, had significantly less satisfaction with family life
(poorer family functioning) than families using the other styles with higher levels of

119
normalization (Knafl & Zoeller, 2000). Therefore, research has shown that family
functioning has been associated with normalization.
Family Functioning and Psychosocial Adjustment of the Child
Family functioning was also noted to be associated with psychosocial outcomes in
the chronically ill child. Murphy (1994) found that poor family functioning was related to
poor psychosocial adjustment in the child with a chronic physical disorder (Murphy,
1994). Stanton (1999) concurs with this finding and found in a meta-analysis of literature
related to families of children with traumatic brain injury that family functioning
influences behavioral adjustment and adaptive function after a traumatic brain injury in
children. Most studies found that family functioning accounted for 20% of variance in
outcome of the head injury (Stanton, 1999). Therefore, family functioning has been
associated with psychosocial adjustment in children with chronic conditions.
Drotar et al. (1997) looked specifically at family cohesion, an aspect of family
functioning, in families of children with chronic conditions. According to a meta-analysis
of 57 published studies, supportive family relationships (cohesion) predicted fewer
behavioral symptoms and greater self esteem in children with chronic conditions. In all
but 4 studies, family/parental functioning was significantly related to the child’s
psychological condition. On the contrary, measures of family conflict generally predicted
higher levels of behavioral symptoms and less competent psychological adjustment. Also,
a greater frequency of maternal psychological distress was reported among those who had
children who were considered psychologically maladjusted Drotar et al.,
(1997).Therefore, family cohesion, an important aspect of family functioning was found

120
to be significantly related to the chronically ill child’s behavior, self esteem, and
psychological adjustment.
Summary of Family Functioning
In summary, little research has been conducted related to family functioning in
families who have a child who is technology dependent. Family functioning has been
examined extensively in families with children who have chronic illnesses. Main findings
of these studies are that family functioning has a direct effect on the child’s psychological
functioning. Since family functioning is of paramount importance to the management of
the child who is technology dependent this is an area that requires further study.
Furthermore, no quantitative studies have examined the relationship between
normalization and family functioning as described in the Family Management Style
Framework by Knafl and Deatrick (2003; 2006). Research that can examine the
relationships between maternal depressive symptoms, child’s functional status and level
of technology dependence, normalization efforts on family functioning will help nurses to
identify families who are most at risk for family functioning distress so that interventions
can be implemented and the health of all members of the family can be maintained and
growth of all the family members promoted.
Theoretical and Empirical Linkages
Child’s Severity of Illness and Maternal Depressive Symptoms
The concepts in this study are theoretically and empirically linked (Figure 1.2).
The severity of a child’s illness, and in particular, functional status, has been linked to a
parent’s depressive symptoms (Canning, et al., 1996; Lustig et al., 1996; Silver et al.,

121
1995; Silver et al., 1998; Frankel & Wamboldt, 1998; Weiss & Chen, 2002). According
to Radloff (1977), there is a relationship between chronic strain and depressive
symptoms: the more negative the event, the higher the depressive symptoms. According
to the cognitive theory of depression, “affect (or emotion) is a subjective state resulting
from the appraisal or evaluation of internal/external stimuli…the emotional experience
occurs within the context of a dynamic interaction between the person and the
environment” (Clark et al., 1999, p. 76). Caring for a chronically ill, technology
dependent child at home could be assessed by some parents as chronic strain and could
therefore lead to elevated levels of depressive symptoms.
Caregiving strain is viewed as an “array of challenges experienced by families as
a consequence of someone’s illness” (Sales, Greeno, Shear, & Anderson, 2004, p. 212).
Biegel, Sales and Schulz (1991), developed a model that posits that caregiving strain is a
mediating variable that is affected by the severity of the ill family member’s care needs
and thus affects the mental health of the caregiver. In sum, this model portrays that the
relationship between the child’s illness severity and the caregiver’s mental health is
mediated by the caregiving strain experienced (Sales et al, 2004).
Many researchers of caregiver strain have examined and found associations
among a child’s behavioral problems, caregiver strain and maternal depression (Sales et
al., 2004). Few, however, have viewed caregiver strain as the link between the child’s
severity of illness and a mother’s depressive symptoms as most have viewed caregiver
strain as an outcome variable rather than a mediator affecting maternal depression (Sales
et al., 2004). In a study of 222 mothers of children with behavioral problems, mothers
with more severely affected children experienced more caregiving strain. Additionally,
the authors noted a significant relationship between caregiving strain and increased

122
depression using the Beck Depression Inventory, and the SF-36 Mental Health subscales
(Sales et al., 2004). In conclusion, Sales et al. (2004) found that caregiver strain was the
strongest predictor of maternal depression and the strongest predictor of caregiver strain
was perceived severity of the child’s problems.
Leonard and colleagues (1993) found that 59% of mothers and 67% of fathers
with children who were technology dependent had psychological distress symptoms at a
level indicating a need for intervention. Gennaro, Brooten, Roncoli, and Kumar (1993)
found a significant relationship between preterm infant morbidity and maternal level of
depression postpartum. Therefore, previous studies have found that severity of a child’s
illness is related to a higher level of parents’ depressive symptoms.
Severity of Illness and Normalization
Increased severity of illness has also been linked to decreased normalization
efforts. Components of the illness that have been found to interfere with efforts toward
normalization include illness control, uncertainty or unpredictability of the illness and
visibility of the condition to others. Dashiff (1993) found that poor illness control of
diabetic adolescents hindered efforts at normalization. Chronic uncertainty of the illness
and unpredictability of symptoms of an illness (Cohen, 1993; Haase & Rostad, 1994;
O’Brien, 2001) and visibility of the condition (Murphy, 1994) have also has been found
to hinder normalization efforts.
Severity of illness was also noted to be a major factor related to change in
normalization efforts in a longitudinal study conducted with families of children with
chronic conditions (Knafl & Deatrick, 2002). In families who experienced this change,
the level of difficulty in incorporating the illness into family life was linked to a change

123
in the disease process. With exacerbations and flare-ups of the disease, there was
dissolution of normalization even in parents who described themselves as competent and
confident caregivers and managers of the illness (Knafl & Deatrick, 2002). The illness
exacerbation made the illness management burdensome and the focus of family life; as in
Paterson’s Model of Shifting Perspectives, brought the disease to the foreground.
Conversely, as the illness improved or became better controlled, parents shifted to
normalization in their family life and increased their normalization efforts. While the
illness was in remission or was well controlled, the illness management was taken for
granted and became part of the family routine thus normalizing efforts were increased
(Knafl & Deatrick, 2002).
Morse and colleagues (2000) also linked severity of illness to normalization
efforts however they conceptualized normalization as including the process of
identification to fit into a desired reference group. The extent to which the child was able
to normalize and function in these two reference groups; “everyday as normal” and
“disabled as normal” is related to various factors including the degree of disability
(Morse et al., 2000).
Researchers who studied families with children who were technology dependent
also noted a link between increased severity of illness and difficulty with normalization
efforts. In a study of 12 families of ventilator dependent children, Carnevale and
colleagues (2006) found that normalization efforts were undermined by the
unpredictability of the child’s condition that was complicated and at times overwhelming.
All of these families however devoted significant effort toward normalizing the
experience; creating routines so that their lives would resemble that of “normal” families.
Lee (1996) found that mothers reported increased normalization efforts with decreased

124
dependency on technology i.e. less dependent on oxygen because the infant was seen as
less sick and more normal. Therefore, the literature describes an inverse relationship
between severity of illness and normalization efforts.
Rehm and Bradley (2005) examined normalization in 26 families with children
who were technology dependent and concur with the findings of an inverse relationship
with severity of illness and normalization efforts. Furthermore, the researchers found that
the child’s developmental delays compounded the effects of the child’s physical chronic
condition thus affecting how the family organized and managed their daily lives. The
researchers conducted a comparison of these families with the attributes of normalization
and concluded that these families did not fit the established attributes of normalization.
Families reported that it was possible to have a good life but that it was not “normal” by
the usual standard. Most notable was the finding that the “normalcy lens” was
impossible. Because the child’s condition required constant vigilance and frequent skilled
intervention, parents felt that they needed to continuously prioritize the care of the child
and not place the child’s condition in the background. Due to the child’s fragile
condition, families reported that they were unable to modify the treatments or develop a
predictable routine. Families arranged their daily life around the care of the child and
strove for stability for all family members but did not see life as “normal”. Due to the
visibility of the equipment and appearance of the child, parents felt conspicuous in public
and frequently experienced distress due to discrimination. The researchers concluded that
feeling and acting normal is not an all or nothing phenomenon but rather emphasized
aspects of typical family life like activities and traditions that all family members could
enjoy together (Rehm & Bradley, 2005).

125
Families of children who are technology dependent experienced many limits in
their routines and activities related to the child’s chronic condition. The equipment, time
required for treatments and care, the need for trained caregivers all affected efforts
normalization and the child’s ability to participate in normal childhood and family
experiences and socialization with peers (O’Brien & Wegner, 2002). The reliance on
technology also affected daily activities due to the time and planning required even for a
simple outing.
Severity of Illness and Family Functioning
The severity of a child’s illness can also be linked to family functioning. Ostwald
et al. (1993) in a study of 151 caregivers of frail elderly and medically fragile children
found that the ability to continuing to managing the care of the child was related to the
degree of the child’s physical impairment. A total of 25% of the caregivers said they felt
they could not continue to manage with the current arrangement. Those families that had
the most difficulty with family functioning were those families of children with severe
respiratory and neurological problems (Ostwald et al., 1993). Thus, the degree of the
child’s physical impairment is linked to family functioning.
Kiernan (1995) found that severity of diagnosis was inversely related to family
functioning using the Family APGAR in families of children dependent on intravenous
infusions receiving home health care. The researcher hypothesized that a there was a
stronger sense of family functioning with the perception that the diagnosis was less
severe.
The predictability of symptoms of an illness adds to the perceived severity of
illness that can thus affect family functioning. O’Brien (2001) found that families with

126
children who are technology dependent and receiving long term home health care
identified uncertainty and unpredictability in their lives as “living in a house of cards”.
Balance was therefore required in order to manage daily life with technology while at the
same time maintaining a functioning family. Donnelly (1994), Dodgson et al (2000), Kirk
(1998), Torok (2001), Case-Smith (2004) and Cavanagh (1999) concur with these
findings that the unpredictable nature of chronic disease and the demanding treatment
protocols are variables that negatively affect family functioning. In fact, families learn to
anticipate the unanticipated. Dodgson et al. (2000) found that mothers of children with
intermittently unpredictable symptoms reported significantly more disruption in family
functioning (p=.001). Therefore, severity of the child’s illness, particularly the
unpredictable nature of the illness, had a negative effect on family functioning.
Establishing family routines is one of the components of family functioning that is
affected by a child’s severity of illness. O’Brien (2001) found that families established
the environment and routines for themselves that incorporated and accommodated the
complex aspects of life with a child who was technology dependent. Managing the family
life with technology requires skill, organization and creativity. There were frequent
disruptions in the child and family routines due to the child’s care demands, however,
families incorporated the demands into family life and were not subsumed by them
(O’Brien, 2001). Incorporating illness care into family routines, therefore, promoted
family functioning.
Another component of family functioning that can be affected by the child’s
severity of illness was related to group activities for the family and relationships with
family and friends. O’Brien (2001) found that families of children dependent on
technology were able to meet the physical and health needs of the family however

127
enjoying activities together as a group was difficult and frustrating. Families also found
maintaining relationships with family and friends difficult (Allen et al., 1994; Case-
Smith, 2004; Cavanagh, 1999; Neuss, 2004).
The child’s severity of illness can also affect the relationship between the parents
of the child who is technology dependent; an important relationship in family
functioning. Marital strain has been noted due to the high care demands of these children
and the resultant lifestyle change (Hatton et al., 1995). The literature reports conflicting
information regarding marital breakups related to care of the child who is technology
dependent. O’Brien (2001) reports that 3 of 15 couples included in her study divorced
due to care of the child who was technology dependent however Neuss (2004) reported
no break up in marriages. Neuss (2004) hypothesized that this was due to their
compatibility in definitions of parenting roles and shared goals for the child.
Family Functioning and Maternal Depressive Symptoms
Family functioning is linked with a mother’s depressive symptoms. When the
major caregiver, typically the mother, is emotionally distressed, general family
functioning is affected and poor family functioning has been shown to affect the mother’s
psychological functioning (Kuster et al., 2002; Ireys & Silver, 1996; Hock-Long, 1997;
Weiss & Chen, 2002). How the child’s illness impacts the family is determined by the
emotional health of the main caregiver parent but the emotional health of the parent is
affected by family functioning and the child’s severity of illness (Frankel & Wamboldt,
1998).
Severity of the child’s illness and increased depressive symptoms of the mother
affected family functioning (Weiss & Chen, 2002). Ireys and Silver (1996) found that the

128
mother’s perception of family functioning due to the child’s illness was related to the
mother’s mental health even after controlling for other variables. Additionally, family
functioning accounted for a large percentage of variance on mental health measure
(p=<.001) (Ireys & Silver, 1996). Hock-Long (1997) found that family functioning was
significantly related to psychological functioning (p=<.001). Caregivers with high
discrepancy scores on the Feetham Family Functioning Scale had higher levels of anger,
confusion, depression, fatigue and low vigor levels on the Profile of Mood Scale (Hock-
Long, 1997). Therefore, the literature supports a relationship between depression and
family functioning.
Family Functioning and Normalization
Family functioning is also noted to be linked with normalization. Knafl and
Zoeller (2000) found that parents who matched on themes related to normalization, thus
sharing the same viewpoint related to normalization, had better family functioning. This
shared view of the illness, illness management and its impact on family life appeared to
downplay the impact of the child’s illness on the family. The researcher hypothesized that
when the shared view is positive regarding normalization efforts; families identify illness
management strategies that help with family functioning.
Family functioning is also linked with normalization related to flexibility of
treatment approaches. Normalization includes a flexible approach to carrying out
treatments so that illness care is incorporated into family routines (Gallo & Knafl, 1998;
Knafl & Deatrick, 2002; Knafl & Gilliss, 2002; Thorne et al., 1997; Wilson et al., 1998).
Additionally, care for the child who is technology dependent, if fit around other family

129
activities will facilitate family functioning. Families learned “tricks of the trade” to
facilitate this process of flexibility (Gallo & Knafl, 1998) and routinization of the
treatment regimen (Knafl & Gilliss, 2002). Rules were thus broken to deliver safe care
but would “normalize” childhood by giving experiences similar to other children while at
the same time maintaining family functioning (Wilson & Morse, 1998). Those who did
not normalize were noted to have difficulties related to strictly adhering to the treatment
regimen, saw the treatment regimen as the focus of family life and a burden that made
their family different from other families (Knafl & Deatrick, 2002). Therefore, family
management behaviors to accommodate a child’s chronic condition that incorporated
flexibility in adherence to medical regimen, assisted families in normalization efforts and
consequently led to improved family functioning.
Maternal Depressive Symptoms and Family Functioning
A mother’s depressive symptoms can then be linked to family functioning.
According to Clark et al. (1999), depression, and even sub-clinical depressive symptoms,
is associated with significant impairment in psychosocial and physical functioning and
well being, which could therefore affect family functioning. To date, this have not been
specifically addressed in the literature. Knafl and Zoeller (2000) did measure both family
functioning using the Feetham Family Functioning Survey (FFFS) and psychological
functioning using the Profile of Mood States in a triangulated study of parents of children
with chronic conditions. However, the researchers were reporting on the comparison
between mothers’ and fathers’ experiences and did not report the correlation between
family functioning and psychological functioning. Additionally, there was no significant
difference between scores for mothers and fathers on their overall discrepant or subscale

130
scores on the FFFS. Other findings include that the FFFS scores were similar to other
studies of family functioning in families with health care challenges (Knafl & Zoeller,
2000). Futhermore, mood disturbance was similar or lower than the population used to
develop the Profile of Mood States instrument. Mothers had more mood disturbance on
the confusion and fatigue subscales. The researchers attributed the findings to the
emotional costs incurred by mothers who are the parent primarily responsible for
managing the care and treatment of the child (Knafl & Zoeller, 2000).
Maternal Depressive Symptoms and Normalization
Research regarding caregivers found situational depression to be one of the most
frequent reactions to long term caregiving for adults who were technology dependent
(Smith, 1999). Some of the depressive symptoms such as sleep disturbances or inability
to concentrate can affect performance of complex technological procedures (Smith,
1999). Furthermore, definition of the situation, one of the major components of
normalization, can be influenced by the level of depression (Knafl & Deatrick, 2003).
Definition of the situation according to the Family Management Style Model is the
subjective meaning family members attribute to the child’s identity (normal versus
vulnerable), illness view (life goes on versus serious/hateful), parent mutuality (shared
versus different views of the illness and illness management), management mindset (ease
or difficulty with treatment regimens) (Deatrick et al., 2006). According to Frankel and
Wamboldt (1998), families are unable to effectively manage the illness and the quality of
life for families is diminished when the primary caretaker is emotionally distressed.

131
Summary of Conceptual Linkages
In conclusion, according to the theoretical and empirical literature reviewed, the
proposed study variables are linked. The purpose of this study is to explore how mothers
respond to and manage the special challenges of children who are technology dependent
after they are discharged from the hospital to home. This descriptive, correlational study
will explore the relationships of child’s severity of illness (functional status, technology
dependence), mother’s depressive symptoms (level of depressive symptoms), efforts at
normalization and family functioning of families with children who are technology
dependent. No quantitative research has been done examining efforts at normalization
and level of family functioning as reported by mothers with children who are technology
dependent. More research is needed to examine the relationships among child’s severity
of illness, mother’s depressive symptoms, normalization and the resultant impact on
family functioning in mothers of children who are technology dependent after adjusting
for caregiving duration, amount of home health care nursing hours, race, family income,
and age of the child who is technology dependent.

132
CHAPTER THREE - METHODS
Introduction
The purpose of this study was to explore how parents respond to and manage the
special challenges of a child who is technology dependent after they are discharged from
the hospital to home. This descriptive, correlational study explored the relationship
between child/maternal factors (child’s functional status, level of technology dependence,
mother’s depressive symptoms, length of caregiving duration, amount of home health
care nursing hours, race, family income and age of the child) and (a) family functioning
as well as (b) normalization in families with a child who is technology dependent.
Covariates for this study include length of caregiving duration, amount of home health
care nursing hours, race, family income and age of the child.
This study also examined whether there are differences in family functioning,
normalization and depressive symptoms based upon the child’s level of technology
dependence (Group 1 mechanical ventilation, Group 2 intravenous nutrition/medication,
Group 3 respiratory/nutritional support) using the Office of Technology Assessment
(1987) rubric. Additionally, mediating effects of normalization on family functioning as
well as mediating effects of mother’s depressive symptoms on normalization and family
functioning will be examined.
The Family Management Style Framework (Knafl & Deatrick, 2003) and the
Shifting Perspectives Model of Chronic Illness (Paterson, 2001) was the orienting
framework providing the theoretical foundation for this study. This chapter will describe
the methodology used in this study including the study design, sampling methods,

133
procedure for data collection, instruments, data management, data analysis, research
questions, limitations and protection of human rights.
Study Design
A descriptive, correlational study design is proposed. Data were collected a
minimum of two months after the child who is technology dependent was discharged
from the hospital and cared for at home. Data were be collected related to the family
demographics, child’s severity of illness, mother’s depressive symptoms, caregiving
duration, number of hours of assistance the child receives from home health care nurses,
age of the child who is dependent on technology, type of technology, normalization and
family functioning using quantitative instruments. By two months after discharge,
families will have had time to settle into a routine and experiment with ways to manage
the chronically ill, technology dependent child and develop management behaviors (Bull,
1992; Clements et al., 1990).
Few research studies have been conducted regarding the child who is technology
dependent and family functioning (Miles et al., 1999; Hock-Long, 1997). Researchers
looked at the level of depressive symptoms experienced by parents (Fleming et al., 1994;
Miles et al., 1999; Teague et al., 1993; Heyman et al., 2004; Kuster, 2002), impact on the
family with regard to the four groups of technology assistance (Office of Technology
Assessment, 1987) (Fleming et al., 1994; Leonard et al., 1993) and severity of the child’s
illness (Silver et al., 1995; Silver et al., 1998; Frankel & Wambolt, 1998; Lustig et al.,
1996; Weiss & Chen, 2002). Most studies used functional status instruments that were
not psychometrically tested or those developed for adults to measure a child’s health
status (Leonard et al., 1993; Patterson et al., 1992; Teague et al., 1993; Miles et al.,

134
1999). Two studies examining the impact of caring for a child who is technology
dependent on parents have used a standardized instrument to measure functional severity
(Kuster et al., 2004; Heyman et al., 2004). The vast majority of studies of families of
children who are technology dependent, however, used qualitative designs (Allen et al.,
1994; Carnevale et al., 2006; Cavanaugh, 1999; Cohen, 1999; Heaton et al., 2005;
Judson, 2004; Kirk, 1999; Kirk & Glendinning, 2004; Kirk et al., 2005; Lee, 1996;
Murphy, 1997; Neuss, 2004; O’Brien, 2001; O’Brien & Wegner, 2002; Rehm & Bradley,
2005; Torok, 2001; Wilson et al., 1998). Furthermore, no quantitative research has been
done examining the use of normalization and level of family functioning as reported by
mothers with children who are technology dependent. This study will use quantitative
methodology to address this gap.
Sampling
Criteria for Selection
The subjects for this study will be mothers who are caring for a child who is
dependent on technology at home. Inclusion criteria are mothers who are: 1) 18 years of
age and older; 2) caring for a child who is technology dependent (OTA, 1987 Groups 1-
3), with a stable course of illness, 16 years of age or younger; 3) caring for the child who
is technology dependent at home for a minimum of 2 months prior to participation in the
study; and 4) able to speak and understand English. Exclusion criteria include mothers
whose child has the diagnosis of cancer or is in the terminal stage of illness.

135
Recruitment of Subjects
The convenience sample of mothers with a child who is technology dependent
was obtained from Rainbow Babies and Children’s Hospital Pediatric Out-patient
Departments (Pulmonlogy, Gastroenterology, Otolaryngology, Surgery) as well as the
Preterm Infant Follow-up Program and the Family Learning Center. Convenience
sampling was chosen because it is time efficient, inexpensive, and more readily
accessible than random sampling.
The investigator will contact the Rainbow Babies and Children’s Hospital
Nursing Administration and the Chief Attending Physicians for the Pediatric
Pulmonology, Gastroenterology, Surgery and Otolaryngology Outpatient Departments as
well as the Preterm Infant Follow-up Program to explain the purpose of the study,
information related to the inclusion and exclusion criteria as well as telephone numbers to
contact the researcher. Approval for conducting this study will be obtained from the
Institutional Review Boards (IRB) of University Hospitals of Cleveland/Case Medical
Center.
Potential participants will be contacted in one of two ways. First, the Outpatient
Clinic Physician will ask if the mother would agree to be contacted regarding
participation in a research study of mothers of children with special technology needs.
Upon agreement from the mother, the Physician will notify the researcher. The researcher
will then approach the parents to give an overview of the study, assess for eligibility and
obtain informed consent. The second method of contact, as approved by the IRB, is to
have attending physicians identify potential participants so that a letter could be sent to
the mother introducing the study and inviting her to participate (Appendix G). The letter
will give a telephone number to contact the researcher. If the mother does not contact the

136
researcher within 2 weeks the researcher will call the mother (Appendix H) to ask if she
is willing to volunteer; assuring her that her child’s care will not be affected in any way
by her decision to participate. The researcher will assess for eligibility and set up a
mutually agreeable time and a place for the interview. Following both methods of
recruitment participants will be assigned an identification number.
The amount of time for each interview will be noted and the range reported in the
dissertation. It is estimated that the total amount of time to answer all questions is 45-50
minutes. The time for each participant to complete the packet of instruments will be
recorded and noted. Statistics for response rate such as number of potential participants
approached, number who agreed or refused as well as reasons for refusal will be noted.
Sample Size
Statistical power analysis was conducted to determine sample size using the other
factors involved in statistical inference: significance criterion (alpha), population effect
size (estimated size of the relationship of the independent variables to the dependent
variables), and statistical power (Cohen, 1992). The number of variables and type of
statistical tests to be conducted were considered in the sample size calculations as well.
Power analysis minimizes the risk of Type II error.
The significance criterion (alpha) indicates the risk of committing a Type I error
or the rejection of the null hypothesis when in fact it is true (Burns & Grove, 1997;
Cohen, 1992). The alpha was set at .05 in this study because it is most commonly used in
the behavioral sciences as a minimum value at which to reject a null hypothesis (Cohen,
1992).

137
The effect size is “the degree to which the phenomenon is present in the
population or to which the null hypothesis is false” (Burns & Grove, 1997, p. 780).
Phenomenon exists in a matter of degree, thus, the effect size can be estimated as small,
medium, or large. Cohen has established numerical values for the various estimated effect
sizes based on specific statistical procedures (1992). Effect size, estimates the size of the
relationship of the independent variables to the dependent variables and can be based on
previous research. If no such research has been conducted, a conservative value such as a
medium effect size can be used (Cohen, 1988). For this study, a medium effect size is
proposed because there has been no similar research conducted. A medium effect size of
.25 on the F test for MANOVA and .15 on the F test for Multiple Regression will be used
for this study (Cohen, 1992). According to the guidelines for power analysis set forth by
Cohen (1992), a sufficient sample size for this study was calculated to be 112. The
calculations used by Cohen (1988) to develop the table for sample size are: N=
[L/ ]+k+1. Convenience sampling techniques will be used to draw a sample of 112
mothers to achieve a power of .80 with 9 predictors (4 independent variables, 5
covariables), alpha ( ) of .05 and an effect size of .15 on the F test for Multiple
Regression (Cohen, 1992).
In order to compensate for any missing data, an additional 3% was added to the
total number of subjects to be recruited. A total of 115 participants will be needed to
examine 9 predictors including independent variables child’s severity of illness
(functional severity, level of technology dependence), mother’s depressive symptoms
(level of depressive symptoms), normalization efforts and covariables (amount of home
health care nursing hours, caregiving duration, race, family income and age of the child
who is dependent on technology) with the dependent variable, family functioning

138
(satisfaction with relationships) of families with children who are technology dependent
using a 5% risk of a Type I error and 20% risk of a Type II error. Normalization efforts
and family functioning will alternate between independent/dependent variable depending
on the research question being analyzed.
Procedure for Data Collection
Following approval from the Institutional Review Boards at University Hospitals
of Cleveland, participants were identified and given an overview of the study including
study purpose, data collection procedures, provisions for confidentiality and their ability
to drop out of the study at any time. All information will be given to participants in both
verbal and written form. After it has been ascertained that potential participants have met
the inclusion criteria, the researcher will provide and explain the informed consent and
HIPPA forms (Appendix J & K). After the informed consent form has been signed, the
investigator will administer the questionnaires during a face-to-face interview and answer
any questions. Face to face interviews decrease the chances of missing data. Interviews
will take place in a quiet setting that is agreeable with both participant and researcher
such as the participant’s home, clinic conference room or public library.
Instruments
Five instruments and a set of demographic questions will be organized into a
packet with special attention to order of sequence; less intrusive questions will be
administered first. Data will be collected by the researcher or research assistant using a
face-to-face structured interview technique. The first measure in the packet is the
Functional Status II-R (FS II-R) (Stein & Jessop, 1990) (Appendix A) that assesses the
functional health status of children with chronic physical disorders over time. Next, the

139
Level of Technology Dependency Questionnaire will measure the number and type(s) of
technology used by the child (Appendix B) followed by the Center for Epidemiological
Studies Depression Scale (CES-D) (Radloff, 1977) (Appendix C) to measure the
mother’s depressive symptoms. Normalization efforts will be measured using the “Actual
Effect of a Chronic Physical Disorder on Family” subscale of the Normalization Scale
(Murphy & Gottlieb, 1992) (Appendix D) followed by the outcome measurement of
family functioning using the Feetham Family Functioning Survey (Roberts & Feetham,
1982) (Appendix E). Table 3.1 displays the reliability coefficients for each of the
instruments for the current and previous studies. Last, the Demographic Questionnaire
(Appendix F) that includes number of home health care nursing hours, caregiving
duration, race, family income and age of the child who is dependent on technology will
be administered. A chart will then be completed to ascertain the child’s medical
diagnoses.
Table 3.1. Empirical Indicators and Reliability Coefficient Variable Instruments Cronbach’s alpha
Current Study Cronbach’s alpha Previous studies
Functional Status Functional Status II – Revised
.76 .84 – .86
Depressive Symptoms
Center for Epidemiological Studies – Depression (CES – D)
.92 .85 – .90
Normalization Normalization Scale
“Actual Effect of Chronic Physical Disorder on Family” Subscale
.83 .84
Family Functioning
Feetham Family Functioning Survey
.87 .85 – .88

140
Functional Status
The child’s functional status will be measured using the Functional Status II-R
(FS II-R) instrument that assesses the functional health status of children with chronic
physical disorders (Stein & Jessop, 1990). The 14-item instrument uses common items
across all ages (newborn to 16 years) and requires a parent’s report regarding their child.
The FS II-R can be used with children ages newborn to 16 years of age and is comprised
of two parts to assess for dysfunction due to illness. Part 1 asks questions related to
performance of the activity or behavior over the past two weeks. Examples of questions
included on this instrument are as follows: “thinking about (child’s name), during the last
two weeks did (he/she) (a) eat well, (b) sleep well, (c) seem lively and energetic”. A
response card is given to the mother and the response may be “never or rarely” (coded as
0), “some of the time” (coded as 1), or “almost always” (coded as 2). Part 2 is
administered after the completion of all items in Part 1 and probes those items that
received a starred response on the instrument, indicating poor functioning, to determine
whether this was due “fully”(coded as 2), “partly” (coded as 1), or “not at all”(coded as
0) to a health problem (Stein & Jessop, 1990). This procedure is performed to minimize a
response set. Any items that are probed in Part 2, that the parent indicates are “not at all”
related to illness, should be recoded to the closest non-starred response on Part 1 (Stein &
Jessop, 1990). Items that require recoding so that a high score indicates “good” function
include items FS4, FS6, FS9, FS12 and FS14 such that (0=2) and (2=0).
The FS II-R assesses behavioral manifestations of illness that interfere with the
child’s performance of age-appropriate activities (Stein & Jessop, 1990). According to
the developers of this tool, behavior includes age appropriate physical, psychological,
intellectual and social behaviors. The items on this tool cuts across diseases and lists

141
observable behaviors that reflect disturbances in the child’s function (Stein & Jessop,
1990).
The FS II-R score, an interval measure, is summed and converted to a percent of
the total 28 points possible with higher scores indicating higher function. This revised
instrument was tested with 456 children with a chronic illness and 276 well children for a
total of 732 children, ages 2 weeks to 16 years, with socioeconomic and racial diversity.
The psychometric data indicates that 12.9% of children with a chronic illness would score
below one standard deviation of the mean indicating severe dysfunction. The mean
percent of the total possible score for all ages was 86.8% SD+/- 15.7 for chronically ill
children and 96.1% SD+/-8.2 for well children (Stein & Jessop, 1990). The instrument
showed more variation in children with chronic illness and displayed discriminate
validity in that the mean for well children was higher than that of children with chronic
conditions. Included in the sample were children with significant chronic illness, as well
as children with and without ongoing health conditions. The Cronbach alpha, the measure
of internal consistency or reliability, for the short 14-item form in all ages was.86 for
children with chronic conditions and .87 for well children. The concurrent validity was
established using assessments made by physicians and measures of morbidity such as
school days missed and number of hospital days.
Few studies examining the impact of caring for a child who is technology
dependent on parents have used the FS II-R, a standardized instrument, to measure
functional severity (Kuster et al., 2004; Heyman et al., 2004). The Cronbach alpha for the
FS II-R in a study of ventilator dependent children conducted by Kuster et al. (2004) was
.84 for all ages. Heyman et al. (2004) did not report the Cronbach alpha for the FS II-R
for their study. Most studies have used unstandardized measures with no reported

142
reliability, or those developed for adults (Leonard et al., 1993; Patterson et al., 1992;
Teague et al., 1993; Miles et al., 1999). The Functional Status II-Revised (FSII-R) will
be used in this study because it was specifically developed to assess the functional health
status of children with chronic illness. Therefore, use of a standardized instrument to
measure functional severity will strengthen the findings regarding relationships found
between functional status, depression, normalization and family functioning.
Level of Technology Dependency
The level of technology dependency will be measured by asking parents to list all
medically necessary assistive equipment that the child currently uses. Types of
technology necessary for the care of the child who is technology dependent will be
assessed to determine group assignment for level of technology dependence according to
the Office of Technology Assessment (OTA) (1987). Most quantitative studies of
children who are dependent on technology used the OTA (1987) rubric to define four
groups of technology dependence based on the types of technological equipment used
(Fleming et al., 1994; Leonard et al., 1993). Miles et al. (1999) however, developed a tool
to measure the acuity level for children who are dependent on technology to expand the
rubric for groups established by the Office of Technology Assessment (1987). The tool
developed by Miles et al. (1999) however, does not include any information regarding
reliability and validity and has as its goal determination of acuity rather than the level of
technology dependency so will not be used in this study.
Technology will be dummy coded and includes a) nasogastric tube feeding 0=no
and 1=yes, b) gastrostomy tube feeding 0=no and 1=yes, c) intermittent intravenous
infusion 0=no and 1=yes, d) continuous intravenous infusion 0=no and 1=yes, e)

143
intravenous infusion of total parenteral nutrition 0=no and 1=yes, f) oxygen via nasal
cannula 0=no and 1=yes, g) oxygen via trach collar 0=no and 1=yes, h) oxygen via
continuous positive airway pressure (CPAP) 0=no and 1=yes, i) continuous positive
airway pressure (CPAP) without oxygen 0=no and 1=yes, j) tracheostomy tube 0=no and
1= yes, k) mechanical ventilator 0=no and 1=yes. Data will be collected regarding
technology for description purposes and to look at correlations and multiple analysis of
variance of the level of technology with depression, normalization and family
functioning.
Level of Technology Dependency will be categorized according to the groups
established by the Office of Technology Assistance (OTA, 1987) Group 1 as mechanical
ventilators (coded as 1), Group 2 intravenous total parenteral nutrition (coded as 2),
Group 3 respiratory or nutritional support equipment that could include such devices as
oxygen by nasal cannula or continuous positive airway pressure (CPAP), or CPAP
without oxygen, tracheostomy tubes, or gastrostomy tubes (coded as 3). For purposes of
the Multiple Regression analysis, level of technology dependency (Groups 1-3) will be
dummy coded as follows: variable x1) 1=Group 1 and 0=not Group 1, variable x2) 1=
Group 2 0=not Group 2. Group 3 then would be coded as zero for both variables.
Reliability will be based on accurate account of parents completing the questionnaire
regarding the types of technology the child uses. After completing the questionnaire
regarding the types of technology in use, parents will be asked if there are any other types
of technology that their child currently uses. Validity was based on review of the list by
the Pediatric Pulmonology Attending Physician who works with this population of
patients in the Technology Dependent Care Clinic.

144
Level of Depressive Symptoms
The mother’s level of depressive symptoms will be measured by The Center for
Epidemiologic Studies Depression Scale (CES-D) that was designed for use in general
population surveys to examine relationships between depressive symptomatology and
other variables across population subgroups. The CES-D is sensitive to possible
depressive reactions in response to life events and discriminated significantly between
clinical psychiatric inpatients and general populations (Radloff, 1977). This 20-item self-
report scale asks how often during the past week a depressive symptom was experienced.
Scores on this scale range from 0 to 60 with higher scores indicating a greater level of
depressive symptoms as an indicator of mental health.
Depressive symptoms are an indicator of mental well-being and tap one indicator
that is inversely related to positive mental health. Examples of some of the questions on
this instrument include: “during the past week (a) I was bothered by things that usually
don’t bother me, (b) I did not feel like eating; my appetite was poor, (c) I had trouble
keeping my mind on what I was doing. Items are rated on a 4-point likert scale ranging
from a score of 0 (rarely or none of the time; less than 1 day), 1(some or a little of the
time; 1-2 days), 2 (occasionally or a moderate amount of time; 3-4 days), to 3 (most or all
of the time; 5-7 days). CES-D items 4, 8, 12 and 16 are phrased in a positive way to
eliminate the possibility of a response set, therefore, reverse coding must be conducted on
those items such that a score of 0=3, 1=2, 2=1, 3=0. A cutoff point of 16 is commonly
used to indicate a clinically significant level of depressive symptoms as a means to
identify high-risk groups however is not intended for use as diagnostic tool for depression
(Radloff, 1977). The CES-D was able to discriminate between populations with a total of
70% of the inpatients but only 21% of the general population scored at or above 16 on

145
this instrument. The scale has been found to have high internal consistency with a
coefficient alpha of .85 in the general population and .90 with a population of adults
admitted to an inpatient psychiatric facility (Radloff, 1977). Validity was established by
conducting correlations with clinical depression ratings conducted by clinicians
(concurrent validity) and other self-report measures (Radloff, 1977). The scale was tested
on a probability sample of over 2,500 people with a wide range of demographic
characteristics (Radloff, 1977).
The CES-D has been used as a measure of depression symptoms in past studies of
caregivers who have children who are technology dependent. Heyman et al. (2004) found
that there was no significant difference in CES-D scores between caregivers of children
with a gastrostomy tube and those with a chronic illness without a gastrostomy tube.
Mean CES-D scores were 13.6 with SEM of 1.25 and 14.3 with SEM of 1.28 for
caregivers of children with and without gastrostomy tubes, respectively. Both groups,
however, had higher scores on the CES-D than those with healthy children (13.9 versus
10.0). The Cronbach alpha of the CES-D for the study was .90 (Heyman et al., 2004).
Miles et al. (1999) also used the CES-D to measure the level of depressive
symptoms in mothers of infants who were medically fragile and technology dependent.
The Cronbach alpha for this study was .90 at hospital discharge and .88 at 12 months.
The mean CES-D score was 15.4 (SD=12, range 0-52) at hospital discharge and 13.6
(SD=10, range 0-41) at 12 months (Miles et al., 1999).
Smith (1999) also examined level of depressive symptoms using the CES-D in
adult caregivers of adults who were technology dependent. The mean score on the CES-D
was 16.12 with a range of 14-33. The Cronbach alpha for this instrument was .86 for this
study (Smith, 1999).

146
In conclusion, the CES-D has been widely used in studies of caregivers of family
members who are technology dependent and has been found to have Cronbach alpha
levels ranging from .85 to .90. This instrument has been shown to be a valid and reliable
instrument to measure the level of depressive symptoms in caregivers of family members
who are technology dependent.
Normalization
Normalization efforts will be measured using the “Actual Effect of a Chronic
Physical Disorder on Family” subscale of the Normalization Scale (Murphy & Gottlieb,
1992). The 25 items of the Normalization Scale were derived from work by Knafl and
Deatrick on normalization attributes and the Family Management Style Framework. The
“Actual Effect of a Chronic Physical Disorder on Family” subscale consists of 10 items
that is the portion of the instrument that deals with the effect of having a chronic physical
disorder on the family. Items included questions regarding impact of the chronic physical
disorder on family, couple’s and sibling’s activities, differences for family and child if
child did not have a chronic physical disorder, hassles related to the chronic physical
disorder, other’s inclusion of the family in activities, and degree that others treated family
like other families (Murphy, 1994). Examples of questions from this subscale are as
follows: (a) If your child did not have this chronic condition, how different would your
family be compared to what it is like now? (b) How much of your family’s daily
activities have to be planned around your child’s needs? (c) How much of a hassle does
your child’s medical treatment create for your family’s routine?
The Normalization Scale uses a visual analog scale. This format was used for this
instrument because it has been found to be very sensitive, found to reduce bias and has

147
been shown to be helpful in measuring subjective experiences (Murphy, 1994).
Participants are asked to mark a slash on a 100 mm line between two extremes-a lot and a
little; with a right angle stop at either end. The slash’s distance is measured in
centimeters along the line and equals the score given with a theoretical range from 0-10.
Distances are rounded to the nearest millimeter with higher scores indicating greater
normalization efforts.
Content validity was established using three mothers of children with chronic
physical disorders and 10 expert nurses with clinical and research experience. The
Normalization Scale was then pilot tested with 10 mothers of diabetic children. Construct
validity of the scale was assessed using principal components analysis with varimax
rotation to identify scale’s statistical structure. Factors were accepted if they had an
eigenvalue greater than 1.0 with at least two items that loaded >.60 on it and were
clinically meaningful. The factor “Actual Effect of the Chronic Physical Disorder on the
Family”, the subscale that will be used in this study, had an Eigenvalue of 7.0, the highest
of all the factors. Factor loadings for this subscale ranged from 0.48 to .86. Internal
consistency was tested using Cronbach’s alpha on each of the subscales with the
following results: “Actual Effect of the Chronic Physical Disorder on the Family” (10
items) .84; “Perception by the Family and Others of the Chronic Physical Disorder Child
and Family” (7 items) .91; “Comparison of Chronic Physical Disorder Child and Family
to Other Chronic Physical Disorder Children and Families” (4 items) .33;
“Encouragement of Normal Activities” (4 items) .65. The “Actual Effect of the Chronic
Physical Disorder on the Family” subscale to be used in the proposed study had a range
of scores from 14-100 for 76 mothers with a mean of 71 and a SD of 22. The rationale for
using this subscale instead of the entire Normalization Scale is that this scale was

148
originally developed for families with children who are eight to twelve years old so many
of the items on the other subscales do not apply to preschool age children. This scale was
originally developed by Murphy and Gottlieb (1992) for use in a thesis. No further use of
this instrument has been documented in the literature.
Research thus far regarding normalization of chronic illness in childhood has used
qualitative methodology with the exception of Murphy (1994). However, there is
currently a federally funded research grant being conducted to translate the Family
Management Style Framework into a quantitative instrument, The Family Management
Style Survey (Knafl & Deatrick, 2006), that can be used to measure level of
normalization. This instrument will translate the major components and dimensions of the
Family Management Style Framework into a questionnaire that will assess a family’s
response to a child’s chronic illness and indicate the Family Management Style the
family is currently using. Efforts are underway to field test the instrument with a diverse
sample of 600-700 parents of children with chronic illnesses to assess the psychometric
properties. No target date was reported by the authors for completion of this tool for use
in research (Knafl & Deatrick, 2006).
Normalization is the major concept underlying The Family Management Style
Framework. In a qualitative study using the Family Management Style Framework, Knafl
et al. (1996) delineated five different family management styles to reflect the degree of
normalization used by families: Normalcy was the overriding theme in the Thriving
Family Management Style and the dominant theme in the Accommodative Family
Management Style. The Enduring, Struggling and Floundering Family Management
Styles use consecutively lower degrees of normalization (Knafl et al., 1996). Therefore,

149
The Family Management Style Survey, though not in completed form at this time, will be
a measure of a family’s efforts at normalization.
Family Functioning
Family functioning will be assessed using the Feetham Family Functioning
Survey (FFFS) (Roberts & Feetham, 1982). The FFFS measures the parent’s perception
and level of satisfaction with relationships between the family and individuals, the family
and subsystems and between the family and the community. The instrument has 25 items
on a 7-point likert scale ranging from 1 “little” to 7 “much” that ask participants to rate
(a) how much is there now? (b) how much should there be? (c) how important is this to
you? The Porter format that is used in this instrument allows for a measurement of a
discrepancy score between achieved (a) and expected (b) levels of functioning. The
higher the sum of the discrepant scores the greater the dissatisfaction with family
functioning. This format decreases the risk of social desirability and controls for cultural
and ethnic diversity since each item is valued by the participant. When the importance
scores (c) are used along with the discrepancy score, one can gain insight as to
importance of particular aspects of functioning (Roberts & Feetham, 1982). Only
discrepancy scores on this instrument will be used for analysis in this study. Examples of
questions on this instrument are as follows: (a) the amount of discussion with your
friends regarding your concerns and problems, (b) the amount of time you spend in
leisure/recreational activities, (c) the amount of time your work routine is disrupted
(including housework).
The FFFS is well established and has been used in numerous nursing research
studies, primarily in families with young children. The Cronbach’s alpha for the scale is

150
.85 with a test-retest reliability of .85 and a .72 correlation between husbands and wives
scores. Concurrent validity is supported by a -.54 correlation with the Family Functioning
Index (Roberts & Feetham, 1982). The FFFS is appropriate for single-parent families that
do not have someone assuming a spousal role (Feetham, 1991). The respondent scores
the spouse-related items as if there was a person taking the spousal role such that when
asked questions related to the spouse (a. how much is there) is scored low and (b. how
much should there be) is also scored low. The result is a low or zero discrepant score for
the spouse-related items (Feetham, 1991).
In a study examining the response of parents to their child’s chronic illness, Knafl
and Zoeller (2000) found the Cronbach alpha for the FFFS was .75 for fathers and .88 for
mothers. The mean score for the FFFS in this study was 23.44 with SD of 16.51 for
mothers and 26.23 with SD 11.81 for fathers. Hock-Long (1997) also used the FFFS in a
dissertation study of mothers caring for ventilator dependent children. No Cronbach alpha
was reported for this study.
In conclusion, the FFFS has been shown to be a reliable and valid tool to measure
family functioning in families who have children with chronic illness. This study will
examine the use of a family functioning tool related to satisfaction with various
relationships of a family who has a child who is technology dependent.
Demographic Characteristics
Study Covariates
The age of the child who is technology dependent will be assessed and measured
as age in months, rounded to the nearest month. This data was collected for descriptive

151
purposes and to examine the relationships between the child’s age as a covariable and
depressive symptoms, normalization and family functioning.
Duration of caregiving at home for the child who is technology dependent will be
measured in months and defined as the amount of time that the child has been cared for at
home with the special technology.
Amount of home health care nursing hours will be documented as a) number of
RN hours and b) number of LPN hours of care the child receives per week then added to
determine the total number of home health care nursing hours received in one week.
Both duration of caregiving and number of home health care nursing hours will be used
as covariables in three of the research questions; in particular related to family
functioning and normalization.
Race/ethnicity will be categorized and coded as 1=Caucasian, Latino or Hispanic,
2=African-American, 3=Caucasian, Non-Hispanic, 4=Asian, 5=Native American or
6=Bi-racial for descriptive purposes. These categories will be further collapsed to
1=Caucasian, Non-Hispanic and 0=all other races/ethnicity for the analysis of
normalization and family functioning.
Family income will be measured by asking the caregiver to select from the
following categories of total family income before taxes and coded as 0= equal or less
than $20,000, 1=$20,001-40,000, 2=$40,001-60,000, 3=$60,001-80,000, or 4=>$80,001.
Family income will be used as a covariate in the analysis of family functioning and
normalization.

152
Other Demographic Information
Other demographic information that will be collected for descriptive purposes
only include mother’s relationship to the child, mother’s marital status and level of
education, number living in the household, child’s gender and mother’s employment data.
Mother’s relationship to the child will be coded as 1=biological mother,
2=adoptive mother, 3=foster mother, 4=step mother, 5=grandmother. These will be
collapsed into categories of biological mother (coded as 1) and all others (coded as 0), to
examine the relationship of mother’s relationship with the child and depressive
symptoms, normalization and family functioning.
Marital status will be assessed using self-report coded as 1=single, never married,
2=single, living with partner, 3=married, 4=separated, 5=widowed, or 6=divorced. In the
analysis, these will be coded as married and living with spouse (coded as 1) and
everything else (coded as 0) to examine the relationships between marital status and
depressive symptoms, normalization and family functioning.
Education will be categorized and coded as 1=less than 7th grade, 2=completed 8th
grade, 3=partial high school, 4=high school graduate, 5=technical/vocational program
graduate 6=partial college, 7=associate’s college degree, 8=baccalaureate degree,
9=partial graduate school and 10=master’s degree, 11=doctoral degree, 12=other. These
will be further collapsed into three categories of high school graduate or less, some
college and up to a baccalaureate degree and the final category, graduate school and
beyond. In the analysis, educational categories will be used to examine the relationship of
education with depressive symptoms, normalization and family functioning.
Total number in household will be measured by asking for a) number of adults
and b) number of children living in the household.

153
Employment status will be coded as 0=not employed outside the home,
1=employed outside the home. Number of hours employed will be coded as number of
hours per week.
Data Management
Data integrity for this study will be maintained in the following ways. Instrument
pages will be labeled with the subject identification number only. The researcher will be
responsible for filling in missing codes, assigning codes to fill-in-the-blank items on the
Demographic and Level of Technology Dependency Questionnaire instruments,
measuring the Normalization Visual Analog Scale (VAS) as well as scoring the FS II-R
(after reverse coding), CES-D (after reverse coding), and the FFFS. A codebook will be
developed to give each variable in the study an abbreviated name up to 8 characters, as
well as a descriptive variable label, and a range of possible numerical values of every
variable entered in a computer file. Computer column numbers will be included on each
instrument form to aid data entry. Data entry will be conducted in a room free of
distractions with breaks at least every 2 hours to minimize the potential for errors in
computer entry. A research assistant will perform second-level coding of the instruments
to check for accuracy. Data from all the instruments will be double entered into the SPSS
15.0 software package. Accurate data entry will be ensured by printing out and
comparing the two versions of the data file. All data will be stored in locked file cabinets
and password secured computers. Back up files will be made at each step of the process
on the hard drive, school server and a jump drive that will be locked up in secure file
cabinet.

154
The researcher will use SPSS 15.0 to conduct a statistical analysis of the data.
Frequencies will be examined on all variables to determine outliers. After outliers are
identified, they will be compared with information recorded on the instruments to verify
accuracy.
Data Analysis
The data analysis will include descriptive statistical analysis, preliminary data
analysis, Pearson product-moment correlation, correlation matrix, hierarchical multiple
regression and multiple analysis of variance (MANOVA). The descriptive statistical
analysis will be conducted for each variable to examine the shape of distribution (normal,
skewness, kurtosis), central tendency (mean, median, mode) and dispersion of scores
(range, variance, standard deviation). Preliminary analysis will include data cleaning and
testing to ascertain that assumptions for each statistical test are met by examining
residuals. The steps to test the assumptions for regression analysis will include an
assessment for: 1) a zero mean for residuals by examining SPSS output; 2) residual
normality by plotting residuals on a histogram, examining a P-P plot to compare observed
to expected residuals and casewise diagnostics; 3) independence by examining that one
residual is not influenced by other residuals and that the data is not nested by ascertaining
that the Durbin Watson statistic is approximately 2.0. If the Durbin Watson statistic is
>2.5 or <1.5 there is a problem with independence; 4) homoscedasticity by plotting the
standard residuals against the standard predicted value and ascertaining that residuals are
in an even, random scatter around the zero line. Other assumptions to be examined are: 1)
fixed independent variables; 2) absence of measurement error; 3) absence of
multicollinearity by examining if correlation is >.80 between any of the independent

155
variables, tolerance is not equal to or <.20 and that the Variance Inflation Factor (VIF) is
not equal to or >10; 4) influential data points by determining that the Cook’s D is not
>1.0.
Number of independent variables for the multiple regression power analysis: 9 (4
independent variables and 5 covariables)
Independent Variables/Covariables:
Mother’s Mental Health:
Depressive Symptoms
Child Health:
Severity of Illness
Child's technology dependence
Child's functional severity
Normalization (May also function as a dependent variable depending on the
research question)
Level of normalization
Covariables: Length of caregiving duration, amount of home health care nursing, race,
family income and age of the child who is dependent on technology.
Dependent Variable:
Family Functioning (May function as an independent variable depending on the research
question).

156
According to Cohen's (1992) article on "A Power Primer" assuming a medium effect size,
alpha .05, Power.80 a sample of 115 would be needed given 3% additional participants to
account for any missing data.
Research Questions
Five research questions are identified for this study. Data analysis methods
include descriptive statistics, Pearson r product-moment correlation, correlation matrix,
hierarchical multiple regression, and multiple analysis of variance. The following study
questions will be addressed:
1a. What are the relationships of mother’s depressive symptoms, child’s
severity of illness (functional severity and level of technology
dependence) and normalization efforts, with family functioning in families
with a child who is technology dependent? 1b. Do these relationships hold
after adjusting for length of caregiving duration, amount of home health
care nursing hours, race, family income and age of the child who is
dependent on technology? (Correlation Matrix, Multiple Regression)-
F statistic
After the assumptions for multiple regression have been met, Pearson r product-
moment correlation will be performed to examine the relationships between 1) mother’s
depressive symptoms and family functioning; 2) child’s severity of illness and family
functioning; 3) efforts at normalization and family functioning. All variables and
covariables will then be entered into a correlation matrix to examine their relationships.
Statistical significance will be set at alpha .05.

157
It is hypothesized that greater level of mother’s depressive symptoms, greater
severity of the child’s illness and less normalization effort will be related to poorer family
functioning. A hierarchical multiple regression analysis will be conducted entering
mother’s depressive symptoms (level of depressive symptoms), child’s severity of illness
(functional severity and level of technology dependence), efforts at normalization (level
of normalization) in the first step of the model. For the first step of the analysis, the R2
(percent of explained variance) for the dependent variable (family functioning) accounted
for by the independent variables (mother’s depressive symptoms, child’s severity of
illness, efforts at normalization) will be determined. Next, the significance of the
equation (F test- alpha .05) as well as relative contribution of the independent variables
(Standardized Beta) will be determined. If the F test is not significant then none of the
independent variables were significant to explain the dependent variable therefore fail to
reject the null hypothesis. Additionally, the independent variable’s partial regression
coefficients (b’s) for significance will be examined via the t-test statistic. If the R2 is
significant and none of the partial correlations are significant then there is likely a very
high correlation between the independent variables (multicollinearity).
The covariables, length of caregiving duration, amount of home health care
nursing hours, race , family income and age of the child dependent on technology would
then be entered in the second step of this hierarchical multiple regression model to
determine if the relationships of mother’s depressive symptoms (level of depressive
symptoms), child’s severity of illness (functional severity and level of technology
dependence), efforts at normalization (level of normalization) still held. This would be
determined by using the above procedures of examining the amount of explained

158
variance, significance on the F test (alpha .05), and assessing the partial regression
coefficients for significance on the t-test statistic.
2. Are there differences in a) family functioning and b) normalization efforts
and c) mothers’ level of depressive symptoms based on the child’s level of
technology dependence (3 levels)? (MANOVA, Univaritate ANOVA)-F
statistic
The assumptions for the multiple analysis of variance (MANOVA) will be tested
as follows: 1) instruments for the dependent variables, family functioning, efforts at
normalization, and mother’s depressive symptoms are continuous, interval level
measurements and the independent variable must be categorical with at least two groups;
2) normal distribution of the variable’s residuals will be determined by plotting residuals
on a histogram, examining a P-P plot to compare observed to expected residuals and
casewise diagnostics; 3) independent variable groups (level of technology dependence)
will be mutually exclusive as determined by the Office of Technology Assessment (1987)
rubric; and 4) equality of variances (homogeneity of variance) will be ascertained by
examining the descriptive statistics and by examining the Levene statistic for a non-
significant result; 5) sample size in each cell will be examined to see that it is
approximately equal however the test is robust enough if there is about 20 in the smallest
cell (Tabachnick & Fidell, 2001), 6) ascertain that there is no measurement error 7) a
correlation matrix will be performed and examined to determine if the dependent
variables are correlated (MANOVA works best with highly negatively correlated
dependent variables and acceptably well if they are moderately correlated in either
direction of .60) (Tabachnick & Fidell, 2001), 8) linearity as determined by scatterplots

159
and 9) absence of outliers will be determined by examining the Mahalanobis distance
with an alpha not to exceed .001.
If the dependent variables are correlated at .3 or more MANOVA and univariate
analysis may proceed, otherwise, only the Analysis of Variance (ANOVA) can be
performed.Following the input of the variables into the MANOVA model, the Eta
squared will be examined to determine the explained variance (sum of squares between
the groups divided by the total sum of squares ie. the sum of the squared deviations of
each score in all groups from the grand mean for all).
To test for significance of the MANOVA, the Omnibus F test will be examined. If
the between group differences are greater than the within group differences there will be
a higher F statistic score (using either the Wilks’lambda, Hoetelling’s trace criterion,
Pillai’s criterion and Roy’s gcr criterion). The significance of the F distribution indicates
whether to reject the null hypothesis and conclude that one of the group means is
different from the others. Finally, post-hoc tests will be performed using the simultaneous
test procedures to determine which dependent variable(s) has the most influence in the
MANOVA model and the Scheffe test will be used for the ANOVA analyses.
3. Do a mother’s depressive symptoms have a mediating effect on the
relationship between the child’s severity of illness (functional status) and
(a) normalization and (b) family functioning in mothers with a child who
is technology dependent? (Correlation Matrix, Mediation using
Hierarchical Multiple Regression)-F statistic
After the assumptions for multiple regression have been met, Pearson product-
moment correlations will be performed to examine the relationships between the
independent variable in part (a), child’s severity of illness (functional status) and the

160
dependent variable, normalization, as well as the independent variable in part (b), child’s
severity of illness (functional status) and the dependent variable, family functioning.
Three assumptions should be met prior to proceeding with a test for mediation
effects. The first assumption is that there should be a significant direct effect of the
independent variable on the dependent variable in both part (a) and part (b). Another
assumption that should also be met is that the dependent variable does not predict the
mediator variable. The final assumption is that there is no measurement error in the
mediator (Baron & Kenney, 1986; Bennett, 2000). An independent variable functions as
a mediator when variation in the independent variable account for variations in the
proposed mediator (path a), variations in the mediator account for significant variations
in the dependent variable (path b) and finally when the previous paths (paths a and b) are
controlled, there is no longer a significant relationship between the independent variable
and the dependent variable (path c). The strongest evidence of mediation is when this
path (path c) is zero (Baron & Kenny, 1986).
Three multiple regression equations are needed to test the mediation hypotheses
in part (a) and (b) of this research question. In the first equation (path a), the independent
variable for part (a) and (b), child’s severity of illness (functional status) will first be
entered followed by the mediator (mother’s depressive symptoms). The independent
variable, child’s severity of illness (functional severity) should be a significant predictor
of the mediator (mother’s depressive symptoms) as indicated by a significant F test
(alpha .05). In the second equation (path b), the independent variable, child’s severity of
illness (functional status) would be entered first followed by the dependent variables,
normalization in part (a) and family functioning in part (b). The independent variables
should be significant predictors of the dependent variables as indicated by a significant F

161
test (alpha .05). In the final equation (path c), when the other paths (path a & b) are
controlled, the previously significant relationship between the independent variable and
the dependent variable will be less or no longer significant if mediation is present. It is
known as a complete mediation if the third equation (path c) becomes zero after the
independent variable and the mediator are added together in the same equation (Baron &
Kenney, 1986; Bennett, 2000).
4. Does normalization have a mediating effect on the relationship between
(a) child’s severity of illness (functional status) and family functioning, (b)
depressive symptoms and family functioning in mothers with a child who
is technology dependent? (Correlation Matrix, Mediation using
Hierarchical Multiple Regression)-F statistic
After the assumptions for multiple regression have been met, Pearson product-
moment correlations will be performed to examine the relationships between the
independent variable in part (a), child’s severity of illness (functional status) and the
dependent variable, family functioning, as well as the independent variable in part (b),
mother’s depressive symptoms and the dependent variable, family functioning. Three
assumptions should be met prior to proceeding with a test for mediation effects. The first
assumption is that there should be a significant direct effect of the independent variable
on the dependent variable in either part (a) and/or part (b). Another assumption that
should also be met is that the dependent variable does not predict the mediator variable.
The final assumption is that there is no measurement error in the mediator (Baron &
Kenney, 1986; Bennett, 2000).
An independent variable functions as a mediator when variation in the
independent variable account for variations in the proposed mediator (path a), variations

162
in the mediator account for significant variations in the dependent variable (path b) and
finally when the previous paths (paths a and b) are controlled, there is no longer a
significant relationship between the independent variable and the dependent variable
(path c). The strongest evidence of mediation is when this path (path c) is zero (Baron &
Kenny, 1986).
Three multiple regression equations are needed to test the mediation hypothesis in
part (a) and (b) of this research question. In the first equation (path a), the independent
variable for part (a) child’s severity of illness (functional status) and part (b) mother’s
depressive symptoms will first be entered followed by the mediator, normalization. The
independent variable should be a significant predictor of the mediator for both part (a)
and part (b) as indicated by a significant F test (alpha .05). In the second equation (path
b), the independent variable, child’s severity of illness (functional status) for part (a) and
mother’s depressive symptoms in part (b) would be entered first followed by the
dependent variable, family functioning (satisfaction with relationships). The independent
variables should be significant predictors of the dependent variables as indicated by a
significant F test (alpha .05). In the final equation (path c), when the other paths (path a &
b) are controlled, the previously significant relationship between the independent variable
and the dependent variable will be less or no longer significant if mediation is present. It
is known as a complete mediation if the third equation (path c) becomes zero after the
independent variable and the mediator are added together in the same equation (Baron &
Kenney, 1986; Bennett, 2000).
5 a. What are the relationships among mother’s depressive symptoms, child’s
severity of illness (functional status, level of technology dependence),
family functioning on normalization efforts in families with a child who is

163
technology dependent? 5b. Do these relationships hold after adjusting for
length of caregiving duration, amount of home health care nursing hours,
race, family income and age of the child who is dependent on technology?
(Correlation Matrix, Multiple Regression)- F statistic
After the assumptions for multiple regression have been met, Pearson product-
moment correlation will be performed to examine the relationships all variables and
covariables. All variables and covariables will then be entered into a correlation matrix to
examine their relationships. Statistical significance will be set at alpha .05. Less
depressive symptoms and severity of illness, Caucasian (non-Hispanic race), longer
caregiving duration, greater amount of home health care nursing hours and a younger
child are hypothesized to be significantly related to greater efforts at normalization while
controlling for length of caregiving duration, amount of home health care nursing hours,
race, family income and age of the child who is dependent on technology.
A multiple regression analysis will be conducted entering mother’s depressive
symptoms, child’s severity of illness (functional status, level of technology dependence),
and family functioning simultaneously. First, the R2 (percent of explained variance) for
the dependent variable (normalization) accounted for by the independent variables
(mother’s depressive symptoms, child’s functional status, level of technology
dependence, family functioning) will be determined. Next, the significance of the
equation (F test- alpha .05) as well as relative contribution of the independent variables
(Standardized Beta) will be determined. If the F test is not significant then none of the
independent variables were significant to explain the dependent variable therefore, fail to
reject the null hypothesis. Finally, the independent variable’s partial regression
coefficients (b’s) will be examined for significance via the t-test statistic. If the R2 is

164
significant and none of the partial correlations are significant then there is likely a very
high correlation between the independent variables (multicollinearity).
The covariables, length of caregiving duration, amount of home health care
nursing hours, race , family income and age of the child dependent on technology would
then be entered in the second step of this hierarchical multiple regression model to
determine if the relationships of mother’s depressive symptoms , child’s severity of
illness (functional severity and level of technology dependence), family functioning still
held. This would be determined by using the above procedures of examining the amount
of explained variance, significance on the F test (alpha .05), and assessing the partial
regression coefficients for significance on the t-test statistic.
Protection of Human Rights
Approval from the Institutional Review Boards at University Hospitals/Case
Medical Center to conduct the study will be obtained. The researcher will contact
potential participants after being notified by the outpatient clinic physician as discussed
previously. The researcher will give an overview of the study and obtain informed
consent from participants on the IRB approved form that contains a written description of
background information, procedures, risks and benefits, confidentiality. The voluntary
nature of the study will be described which includes the option to withdraw at any time
without affecting care of their child in any way. Parents will be told that they may choose
not to answer a question or discontinue the interview at any time.
Confidentiality will be maintained by using participant identification numbers on
all data collection sheets. Identifying data (participant names and code numbers) and
consent forms will be separated from the study data and maintained in a locked file

165
cabinet. The instruments will be coded and maintained along with the codebook in a
locked file cabinet. The data and codes will be kept for a period of five years following
completion of the study to allow for secondary analysis and will then be destroyed by the
researcher. Only the researcher and the dissertation chair will have access to the data and
codes.
Minimal risk is involved with participation in this study. Physical discomforts
might involve fatigue as the total time for the interview will be 45-50 minutes. Mothers
will be told that they may choose to take a break at any point during the interview. The
amount of time required for participation in the study may also be viewed as an
inconvenience. A potential emotional risk during the interview is that recalling
information regarding their child’s course of illness and potential home management
difficulties may make some mothers uncomfortable. The researcher will be vigilant to
assess the participant’s discomfort. Participants experiencing considerable discomfort
will be asked if they wish to stop the interview and will be given supportive assistance by
the interviewer. The parent will then be given the telephone number of an on call mental
health professional at a 24 Hour Crisis Center (Appendix I). Additionally, if any
participant is noted to have a level of depressive symptoms above the recognized cutoff
of 16 on the CES-D measure she will be told of the findings and given a mental health
information sheet as above (Appendix I). Any participant noted to have a score of 23 or
above on the CES-D will be assessed for imminent risk of suicide by asking if they have
had any thoughts of harming themselves in any way or perhaps killing themselves. If the
answer to any portion of the question is “yes” the participant will be told of a concern for
their safety and the necessity for the interviewer to contact the Mobile Crisis Team. The
risks and inconveniences involved are reasonable because the risks are temporary and can

166
be minimized by the above procedures. In addition, the discomfort is no more that what
the participant might experience in her daily life.
There is no direct benefit from participation in this research study. Participants
will however have the opportunity to learn more about the research process and to receive
results from the study which may be of benefit to their family. Participants may also
benefit from the interaction and the opportunity to discuss their thoughts and feelings
related to caring for the child who is technology dependent. Other families of children
who are technology dependent will benefit from the study findings related to factors that
assist with family management.

167
CHAPTER FOUR - RESULTS
The purpose of this study was to explore how families respond to and manage the
special challenges of children who are technology dependent after they are discharged
from the hospital to home. The study examined the relationships of the child’s severity of
illness (functional status, level of technology dependence), mother’s depressive
symptoms, and efforts at normalization with family functioning in families with children
who are technology dependent. Study covariates included age of the child, duration of
caregiving, amount of home health care nursing, family income and race. Additionally,
mediating effects of normalization on family functioning as well as mediating effects of
mother’s depressive symptoms on normalization and family functioning were examined.
A convenience sample of 103 mothers of children who are technology dependent were
recruited primarily from Rainbow Babies and Children’s (RB&C) Hospital in Cleveland,
Ohio to examine these questions. This chapter provides a summary of the results and an
interpretation of the findings.
Description of Participants
Mothers who were the participants in this study lived primarily in Northeastern
Ohio but due to the large service area of a tertiary children’s hospital some lived as far
away as Northwestern Pennsylvania and Southwestern New York. Participants were
identified and recruited from a number of specialty clinics at RB&C (Table 4.1). The
pulmonology department identified the majority of participants (n=56, 54.4%) to be
approached by the investigator and included the Technology Dependency Clinic (n=30),
Pulmonology Clinic/Service (n=20), and the Cystic Fibrosis Center (n=6). Other

168
departments that collaborated in identifying participants included the Gastroenterology
(n=18, 17.5%), Otolaryngology (n=4, 3.9%) and Pediatric Surgery (n=11, 10.7%)
Departments as well as the Preterm Infant Follow-up Clinic (n=5, 4.9%). Nine other
participants were also identified by the RB&C Family Learning Center (n=2, 1.9%), a
friend or recruitment flyer (n=5, 4.9%) and a primary care physician of children who are
technology dependent (n=2, 1.9%).
Table 4.1. Location of Participant Recruitment (N=103) LOCATION n % Pulmonology Department 56 54.4 Gastroenterology Department 18 17.5 Otolaryngology Department 4 3.9 Preterm Infant Follow-up 5 4.9 Pediatric Surgery Department 11 10.7 Other 9 8.7
There were a total of 21 additional potential participants who were invited to
participant but did not enroll in the study: 14 did not respond following an introductory
letter, follow-up phone calls and messages; 5 stated they were too busy and overwhelmed
with other responsibilities; 2 stated they were not interested. Therefore, there were a total
of 124 mothers approached with a response rate of 88.7% (110/124) and a participation
rate of 93.6% (103/110). Additionally, there were 2 Spanish-speaking mothers who were
ineligible to participate because they could not speak or read English and 2 mothers who
lived over 75 miles from Cleveland stated that they were no longer coming to Ohio and
RB&C for their health care.

169
Face-to-face interviews were conducted with mothers in outpatient clinics (n=38,
36.9%) or in another private place of the mother’s choosing such as their home (n=41,
39.8%), Dahm’s Clinical Research Unit at RB&C (n=9, 8.7%), United Cerebral Palsy
Center (n=4, 3.9%), Rehabilitation Services at RB&C (n=5, 4.9%), a public library (n=2,
1.9%) or other places such as their place of employment or their child’s school (n=4,
3.9%). Interviews ranged from 45 minutes up to 90 minutes with an average time of 55
minutes. The length of the interview depended on a number of factors such as
interruptions from the clinic staff, care required by the child who is technology dependent
or their siblings and issues that the mothers wanted to discuss triggered by the content of
the questionnaires. Whenever possible, further discussion regarding issues and concerns
was conducted following completion of the questionnaires. Mothers were directed to
contact their health care providers with any questions or concerns regarding their child’s
health care or service needs.
Table 4.2 provides a description of the 103 mothers who participated in this study.
Mothers in this study ranged in age from 21-66 years (M=37.87, SD=9.35); a majority
were between 31-40 years old (n=46, 44.6%). The race of participants was predominately
Caucasian (n=82, 79.6%) including those of Hispanic ethnicity (n=6) however the
percentage of participants from other races such as African American (n=17, 16.5%),
Asian (n=2, 1.9%) and Biracial (n=1, 1%) models the demographics of the greater
Northeastern Ohio population. One participant chose not to answer this question.
Mothers possessed a wide variation of educational backgrounds; 31.1% (n=32)
were technical/vocational, high school graduates or less, 38.8% (n=40) had a partial
college education or an associate’s degree and 29.1% (n=30) held a baccalaureate degree,
some graduate school, master’s degree or more. One mother chose not to answer this

170
question. A majority of the participants (n=88%, 85.4%) were the biological mother of
the child but there were also adoptive (n=8, 7.8%) and foster (n=5, 4.9%) mothers as well
as grandmothers (n=2, 1.9%) who had the primary caretaking responsibility. Most
participants were married (n=73, 70.9%) however others were single, never married (n=8,
7.8%) or never married and living with a partner (n=5, 4.9%), separated (n=3, 2.9%),
widowed (n=2, 1.9%) or divorced (n=12, 11.6%). Almost half of participants were not
Table 4.2. Descriptive Statistics – Individual Characteristics of Mothers (N=103) Variable n % Race of Mother African American 17 16.5 Caucasian 82 79.6 Asian 2 1.9 Bi-racial 1 1.0 Unknown 1 1.0 Age of Mother 21 – 30 24 23.3 31 – 40 46 44.6 41 – 50 22 21.4 51 10 9.7 unknown 1 1.0 Family Income (U.S. Dollars) $20,000 12 11.6 $20,001 to $40,000 25 24.3 $40,001 to $60,000 15 14.6 $60,001 to $80,000 29 28.2 $80,001 20 19.4 unknown 2 1.9 Education Junior High Graduate 2 1.9 Some High School 5 4.9 High School Graduate 12 11.7 Technical/Vocational Graduate 13 12.6 Partial College 31 30.1 College (Associate Degree) Graduate 9 8.7 College Graduate (4 years) 20 19.4 Partial Graduate School or more 10 9.7 unknown 1 1.0

171
Table 4.2 (Continued) Descriptive Statistics – Individual Characteristics of Mothers (N=103) Variable n % Mother’s relationship to child Biological mother 88 85.4 Adoptive mother 8 7.8 Foster mother 5 4.9 Grandmother 2 1.9 Marital Status Single, never married 8 7.8 Never married, living with partner 5 4.9 Married 73 70.9 Separated 3 2.9 Widowed 2 1.9 Divorced 12 11.6 Employment Status (hours worked / week) Not employed 47 45.6 10 – 24 hours per week 17 16.5 25 – 39 hours per week 11 10.7 40 hours per week 28 27.2
employed outside the home (n=47, 45.6%) while others worked 39 hours or less per week
(n=28, 27.2%) or full-time 40 hours or more per week (n=28, 27.2%). Yearly total family
income varied; about half of families earned $60,000 or less (n=52, 50.5%), 28.2%
(n=29) earned $60,001-$80,000 and 19.4% (n=20) earned $80,001 or more. Two
participants chose not to answer this question.
Children of Participants
Table 4.3 provides a description of the children who are technology dependent
whose mothers were participants in the study. About half of the children were age 5 years
or less (n=49, 47.6%) with 20.4% (n=21) age 23 months or less, 27.2% (n=28) 2-5 years
old, 31.1% (n=32) 6-10 years old and 21.3% (n=22) 11-16 years old. The gender of the

172
children was evenly divided; male (n=51, 49.5%) and female (n=52, 50.5%). About half
of the children (n=51, 49.5%) had a primary diagnosis that was due to a genetic disorder
and 27.1% (n=28) were born preterm at 36 weeks or less.
Table 4.3. Descriptive Statistics – Individual Characteristics of Children (N=103) Variable n % Age of Child 23 months 21 20.4 2 – 5 years 28 27.2 6 – 10 years 32 31.1 11 – 16 years 22 21.3 Gender of Child Male 51 49.5 Female 52 50.5 Primary Diagnosis Neuromuscular Dysfunction 45 43.7 Respiratory Dysfunction 23 22.3 Digestive Dysfunction 17 16.5 Circulatory Dysfunction 6 5.8 Cystic Fibrosis 6 5.8 Metabolic Dysfunction 4 3.9 Renal Dysfunction 2 1.9 Born Preterm (36 weeks or less) Yes 28 27.1 No 72 70.0 Unknown 3 2.9 Main Diagnosis Related to Genetic Disorder Yes 51 49.5 No 49 47.6 Unknown 3 2.9 Level of Technical Dependence OTA (1987) Group Group 1 18 17.5 Group 2 9 8.7 Group 3 76 73.8
A chart review was done to determine the primary diagnosis of the children. The
primary diagnosis was defined as the diagnosis that led to the cascade of events that
necessitated the child’s dependence on technology. The largest number of children in this

173
study had diagnoses related to a neuromuscular dysfunction (n=45, 43.7%). This group
included children with Cerebral Palsy (n=18), Down Syndrome (n=6), Athrogryposis
(n=4), Myelodysplasia (n=4), a Muscular Dystrophy related diagnosis including Spinal
Muscular Atrophy (n=10) and others (n=3) that cannot be specifically named to maintain
participant confidentiality. Respiratory dysfunction was the primary diagnosis for 22.3%
(n=23); about half of these children had Bronchopulmonary Dysplasia (n=10). Digestive
dysfunction was the primary diagnosis for 16.5% (n=17) of children including Short
Bowel Syndrome (n=3). Other primary diagnoses that were less common included
circulatory dysfunction (n=6, 5.8%), Cystic Fibrosis (n=6, 5.8%), metabolic dysfunction
(n=4, 3.9%) and renal dysfunction (n=2, 1.9%). Cystic Fibrosis was left as a separate
diagnostic category due to the fact that this disease includes multiple system (respiratory
and digestive) involvement. There were three children in foster care for whom HIPAA
releases for a chart review could not be obtained due to county custody regulations. The
main diagnosis was determined based upon the type of technology used, the recruitment
site responsible for identifying the child and the information that was permitted to be
shared with the investigator however specific information regarding preterm birth or the
presence of a genetic disorder could not be obtained.
Children required a variety of technologies and were categorized into levels of
technology dependence based on the OTA (1987) designation for groups: Group 1
mechanical ventilation (n=18, 17.5%), Group 2 intravenous medications or nutritional
substances (n=9, 8.7%) and Group 3 respiratory or nutritional support (n=76, 73.8%) as
displayed in Table 4.3. A majority of children required one type of technology (n=51,
49.5%), 23.3% required two (n=24), 14.6% required three types of technology (n=15)
however some children required up to four types of technology simultaneously (n=13,

174
12.6%) as shown in Table 4.4. Table 4.5 provides a description of the types of
technologies required by the children. Most required some type of feeding tube; either a
nasogastric tube (n=2, 1.9%) or a gastrostomy tube (n=89, 86.4%). Others required
oxygen at least on an as needed basis (n=44, 42.7%) via nasal cannula or face mask
(n=18), trach collar (n=24), or continuous positive airway pressure (n=2) (Table 4.5).
Table 4.4. Number of Technologies Used
Number of Technologies
Used
n %
1 51 49.5 2 24 23.3 3 15 14.6 4 13 12.6
Table 4.5. Descriptive Statistics – Type of Technology Used (N=103) Variable n % Nasogastric Tube Feeding with 2 1.9 without 101 18.1 Gastrostomy Tube Feeding with 89 86.4 without 14 13.6 Intravenous Infusion with 10 9.7 without 93 90.3 Oxygen with 44 42.7 without 59 57.3 Continuous Positive Airway Pressure with 4 3.9 without 99 96.1 Tracheostomy Tube with 32 31.1 without 71 68.9 Mechanical Ventilator with 18 17.5 without 85 82.5 Note: May use more than one type of technology simultaneously.

175
A total of 31.1% had a tracheostomy tube (n=32), 17.5% required mechanical ventilation
(n=18) and 3.9% used continuous positive airway pressure (n=4). Of the 9.7% (n=10)
with intravenous infusions 6 received intermittent infusions and 1 received continuous
infusion of medications while 3 received intravenous infusions of total parenteral
nutrition.
Description of Study Variables
The independent variables in this study included the child’s severity of illness
(functional status, level of technology dependence), mother’s depressive symptoms,
efforts at normalization and family functioning. Covariates included age of the child,
duration of caregiving, amount of home health care nursing, family income and race. The
outcome variable (family functioning/normalization) differed depending upon the
Table 4.6. Means, Standard Deviations, Ranges and Skew for Major Study Variable (N=103)
Variable Mean SD Possible Ranges
Actual Ranges
Skew
Age of Child (months)
78.86 53.13 3 – 203 7 – 202 .46
Duration of Caregiving (months)
57.06 44.92 2 – 203 2 – 161 .64
Home Health Care Nursing (hours/week)
41.23 43.89 0 – 168 0 – 144 .60
Functional Status 21.47 4.03 0 – 28 11 – 28 -.83 Depressive Symptoms 14.07 11.05 0 – 60 0 – 54 .94 Normalization (millimeters)
385.89 190.5 0 – 1000 45 – 900 -1.37
Family Functioning 35.25 20.58 0 – 150 0 – 114 1.02
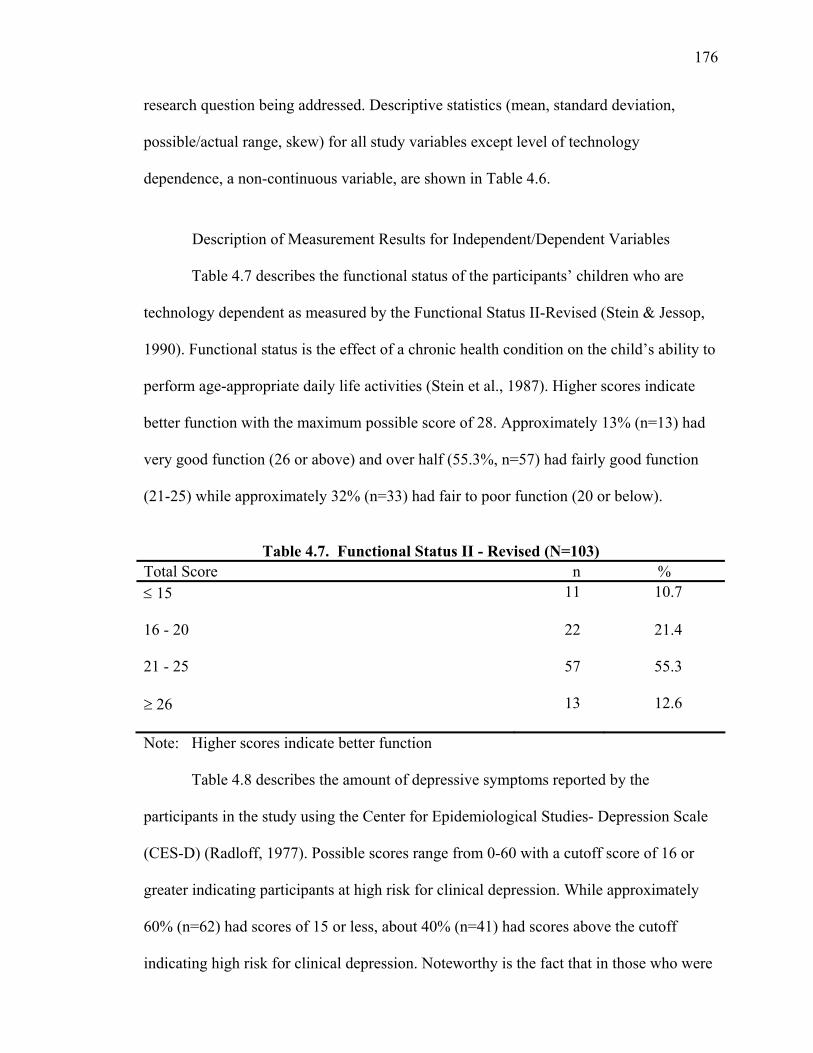
176
research question being addressed. Descriptive statistics (mean, standard deviation,
possible/actual range, skew) for all study variables except level of technology
dependence, a non-continuous variable, are shown in Table 4.6.
Description of Measurement Results for Independent/Dependent Variables
Table 4.7 describes the functional status of the participants’ children who are
technology dependent as measured by the Functional Status II-Revised (Stein & Jessop,
1990). Functional status is the effect of a chronic health condition on the child’s ability to
perform age-appropriate daily life activities (Stein et al., 1987). Higher scores indicate
better function with the maximum possible score of 28. Approximately 13% (n=13) had
very good function (26 or above) and over half (55.3%, n=57) had fairly good function
(21-25) while approximately 32% (n=33) had fair to poor function (20 or below).
Table 4.7. Functional Status II - Revised (N=103)
Total Score n % 15 11 10.7
16 - 20 22 21.4 21 - 25 57 55.3
26 13 12.6 Note: Higher scores indicate better function
Table 4.8 describes the amount of depressive symptoms reported by the
participants in the study using the Center for Epidemiological Studies- Depression Scale
(CES-D) (Radloff, 1977). Possible scores range from 0-60 with a cutoff score of 16 or
greater indicating participants at high risk for clinical depression. While approximately
60% (n=62) had scores of 15 or less, about 40% (n=41) had scores above the cutoff
indicating high risk for clinical depression. Noteworthy is the fact that in those who were

177
above the cutoff the majority had scores equal to or greater than 21 (24.3%) indicating a
very high risk for clinical depression. The CES-D was scored while mothers were
completing other questionnaires. Mothers who scored equal to or greater than 16 were
informed that their score was high and were directed to discuss this with their primary
health care provider. They were also given an IRB approved resource information sheet
with the telephone number for 24 hour crisis information as well as a telephone number
for assistance with access to mental health care services or resources for themselves, their
child or other family members. Mothers who scored 23 or above on the CES-D were
screened for suicide risk as mandated by the IRB as previously described. None of the
mothers screened indicated a risk for suicide therefore none required emergency
intervention.
Table 4.8. Depressive Symptoms. Center for Epidemiological Studies – Depression
Scale (CES-D) (N=103) Total Score n %
15 62 60.2 16 – 20 16 15.5
21 25 24.3 Note: A cutoff of 16 is used to identify those at high risk for clinical depression.
Table 4.9 describes the amount of normalization efforts used by families as
measured by the “Actual Effect of Chronic Physical Disorder on the Family”, a subscale
of the Normalization Scale (Murphy & Gottlieb, 1992). Normalization includes,
“adjusting the environment to provide normal life experiences that will meet the child’s
evolving social, physical, intellectual and emotional needs” (Murphy, 1994, p. 10) while
at the same time managing family life and activities so that they can lead as close to a
“normal” family life as possible (Murphy, 1994). This Visual Analog Scale (VAS) has

178
potential scores from 0-1000; higher scores indicate greater use of normalization. There
was fairly even distribution of scores with 27.2 % (n=28) having very low normalization
efforts and 15.5% (n=16) had very high normalization efforts.
Table 4.9. Normalization Scale. “Actual Effect of Chronic Physical Disorder on the
Family” Subscale (N=103) Total Score n %
250 28 27.2 251 – 350 19 18.4 351 – 450 21 20.4 451 – 550 19 18.5
551 16 15.5 Note: Higher scores indicate greater use of normalization.
Table 4.10 describes results from the Feetham Family Functioning Survey (FFFS)
that measures family functioning (Roberts & Feetham, 1982). This instrument measures
the parent’s perception and level of satisfaction with relationships between the family and
individuals, the family and subsystems and between the family and the community.
Scores indicate the discrepancy between how much there is now and how much there
should be of a particular activity or function with possible scores ranging from 0-150.
Higher scores indicate greater dissatisfaction with family functioning; poorer family
functioning. There was a fairly equal amount of distribution across all categories however
almost half of the participants had scores from 21-40 indicating they were somewhat
satisfied with family functioning. Approximately 23% (n=24) had scores equal to or less
than 20 indicating that they were for very satisfied with family functioning while 10%
(n=10) were very dissatisfied with family functioning. The majority of mothers (45%,

179
n=45) indicated they were somewhat satisfied with family functioning and about 21%
(n=22) were somewhat dissatisfied.
Table 4.10. Feetham Family Functioning Survey (N=103) Total Discrepancy Score n %
20 24 23.3 21 - 40 45 43.7 41 - 60 22 21.4
61 10 9.7 missing 2 1.9 Note: Higher scores indicate greater dissatisfaction with family functioning (poorer
family functioning).
Description of Caregiving Variables
Table 4.11 describes two important covariables examined in this study; the duration of
caregiving and the amount of home health care nursing the children received. The
duration of caregiving is defined as the period of time the mother had been caring for the
child since he/she had been discharged from the hospital dependent on technology. The
duration of caregiving for this study ranged from 2 to 161 months (M 57.06, SD 44.92)
and included a fairly even distribution of participants in each of the categories: 17.5%
(n=18) 12 months or less, 22.3% (n=23) 13-35 months, 24.3% (n=25) 36-71 months,
22.3% (n=23) 72-107 months and 13.5% (n=14) had a caregiving duration of equal to or
greater than 108 months. The amount of home health care nursing the children received
ranged from 0-144 hours per week (M 41.23, SD 43.89). A large proportion of children
in the study did not receive any home health care nursing (n=38, 36.8%), however, 20.3%
(n=21) received 1-40 hours, 16.5% (n=17) received 41-80 hours, 23.3% (n=24) received
80-120 hours and 2.9% (n=3) received 121 or more hours per week.

180
Table 4.11. Descriptive Statistics – Caregiving Variables (N=103) Variable n % Duration of Caregiving (total months) 12 months 18 17.5 13 – 35 months 23 22.3 36 – 71 months 25 24.3 72 – 107 months 23 22.3 108 months 14 13.5 Home Health Care Nursing (total hours / week) None 38 36.8 1 – 40 21 20.3 41 – 80 17 16.5 81 – 120 24 23.3 121 3 2.9
Preliminary Data Analysis
Preliminary analysis of all study variables included frequencies and descriptive
statistics. Data cleaning was performed and the assumptions of multiple regression and
Analysis of Variance (ANOVA) were examined.
Missing data was handled using individual mean substitution. On the CES-D, data
were missing completely at random for 4 participants; therefore, the mean score for the
missing item was imputed. For the “Actual Effect of the Chronic Physical Disorder on
the Family” subscale, those mothers who only had one child left item 6 blank because it
asked how much their child’s condition affected their other children’s activities. This
missing data was handled by summing the scores on items answered, determining the
mean for those items then multiplying by the total number of items on the scale (10
items). On the Feetham Family Functioning Scale those mothers who did not have

181
partner/spouse involvement in their lives were reluctant to answer those questions despite
the fact that the directions indicate if there is no spouse/partner they are to answer the
questions based on how much they want the functions met. This missing data was
handled by summing the scores on items answered, determining the mean for those items
then multiplying by the total number of items on the scale (25 items).
Testing Assumptions for Multiple Regression
Correlation and hierarchical multiple regression were the primary methods of
analysis for this study. The assumptions for multiple regression were examined prior to
testing for statistical significance to prevent violation of assumptions that would
confound statistical conclusion validity. The primary assumptions for correlation and
multiple regression included:
1) Normality. For this assumption to be met the distribution of the variables must
follow a normal curve for adequate variance. This assumption was tested by
examining the frequency distribution and histogram with a superimposed normal
curve for all continuous study variables. Furthermore, while some of the variables
did have a slight skew as shown in Table 4.6, none were skewed greater than +/-3,
which would indicate a non-normal distribution (Tabachnick & Fidell, 2001). In
addition, the P-P probability plots were examined to compare observed to
expected residuals. The Normalization subscale and amount of home health care
nursing hours showed the most deviation between the observed and the expected
observations. The Central Limit Theorem proposes however that with a large
sample size such as in this study (n=103), the sampling distribution of means is

182
normally distributed therefore the assumption of normality for this study was met
(Tabachnick & Fidell, 2001).
2) Linearity. The assumption of linearity requires that the association of X
(independent variable) and Y (dependent variable) must be linear and when
graphed follow a straight line (Tabachnick & Fidell, 2001). This assumption was
tested by analyzing the partial regression scatter-plots for each of the continuous
study variables. The partial plots option assesses the effect of each independent
variable on the dependent variable controlling for all of the other independent
variables. It was determined that normalization, family income and functional
status were non-linear therefore the variables were squared to overcome the
violation of non-linearity. Since no differences in results were noted, the original
(non-squared) variable was used to maintain a more parsimonious model.
3) Homoscedasticity. This assumption requires that the distribution of a Y score
should have approximately an equal score on X. Homoscedasticity was tested by
examining the constant error variance and plotting the Studentized Deleted
Residuals (Y axis ) against the Standard Predicted value (X axis) and ascertaining
that residuals are in an even, random scatter around the zero line. According to
Fox (1991), a problematic non-constant error indicating violation of this
assumption is higher than a 3:1 ratio of highest to lowest error variance. This
assumption was not violated for any of the study variables.
4) Independence of Observations. This assumption requires that independent
observations were collected; there are no nested data or data collected at multiple
time points on the same participant. Because this was a cross-sectional study this
assumption was not violated. This assumption was tested by examining that one

183
residual is not influenced by the other residuals and determining that the Durbin
Watson statistic is not>2.5 or<1.5. There was no violation of this assumption; the
Dubin Watson statistic did not exceed 2.0 for any of the regression analyses.
5) Zero Mean for Residuals. This assumption requires that the mean value of the
error term for standardized residuals is zero and the standard deviation is one.
This assumption was met as determined by output from SPSS output of all
multiple regression analyses.
Secondary Regression Assumptions:
1) Absence of Measurement Error. All instruments were administered to mothers
in a consistent fashion by the investigator. Instruments demonstrated acceptable
reliability as evidenced by Cronbach’s alpha coeffients of .77-.92 in Table 3.1.
2) Absence of Multicollinearity. This assumption requires that independent
variables not be highly correlated >. 80. The highest correlation in this study (.73)
was between the variables child’s age and duration of caregiving.
Multicollinearity was also determined by examining that the tolerance was not
equal to or <.20. The lowest tolerance was noted to be duration of caregiving
(.433) which is still acceptable therefore this assumption was met.
3) Absence of Influential Data Points. This assumption examines if all cases exert
approximately the same influence on the regression coefficients. This assumption
was tested by examining that the Cook’s D is not equal to or >1.0. In this study
although there were two cases that were considered outliers (high discrepancy
scores on the Feetham Family Functioning Survey) none of the regression
analyses had a Cook’s D greater than .24; this assumption was not violated.

184
Research Questions and Hypothesis Testing
Research Question 1a. What are the relationships of mother’s depressive
symptoms, child’s severity of illness (functional severity and level of technology
dependence) and normalization efforts, with family functioning in families with a child
who is technology dependent? 1b. Do these relationships hold after adjusting for length
of caregiving duration, amount of home health care nursing hours, race, family income
and age of the child who is dependent on technology?
More depressive symptoms, greater severity of illness and less normalization
effort were hypothesized to be related to poorer family functioning while controlling for
length of caregiving duration, amount of home health care nursing hours, race, family
income and age of the child who is dependent on technology. A Pearson product moment
correlation coefficient matrix comprising all study variables and covariates (Table 4.12)
was examined to determine if any significant relationships existed. The assumptions of
normal distribution and level of measurement were met. The value of statistical
significance was set at alpha .05.
Table 4.12. Correlations Among Study Variables (N=103) Variable Age Race Inc. Dur. HHC Dep. Norm. Fam. FS TD1 TD2 Age 1.000 Race .175 1.000 Inc .074 .360** 1.000 Dur .733** .145 .149 1.000 HHC .220* -.055 -.097 .236* 1.000 Dep .087 .080 -.224* .114 -.002 1.000 Norm .017 -.247* .044 -.068 -.126 -.453** 1.000 Fam .105 .049 -.090 .085 .034 .608** -.348** 1.000 FS -.108 .001 .087 -.020 -.002 -.239* .375** -.168 1.000 TD1 .120 .094 -.107 .191 -.417** .023 -.035 .099 .055 1.000 TD2 .202* .023 -.099 -.257** -.075 .079 -.131 .132 -.010 .142 1.000

185
Note: Inc = Income; Dur = Duration of caregiving; HHC = Total home health care nursing hours; Dep = Depressive symptoms; Norm = normalization; Fam = Family Functioning; FS = Functional Status; TD1 = Ventilator dummy code;
TD2 = IV dummy code *p .05, **p .01 (2 – tailed)
Child’s Age.
As shown in Table 4.12 there were significant positive correlations between the
child’s age and duration of caregiving as well as amount of home health care nursing
hours. The older the child, the longer the duration of caregiving (r= .733, p<.01) and the
greater the number of home health care nursing hours required per week (r= .220, p<.05).
Additionally, age was significantly correlated in a positive direction with level of
technology dependence (r= .202, p<.05). The older the child, the more likely they were to
be classified as OTA (1987) Group 2 (intravenous medications or nutrition) than Group 1
(ventilators) or Group 3 (respiratory/nutritional support).
Race.
For purposes of the analysis, race was coded as 1=Caucasian (non-Hispanic) and
0=all others (Hispanic ethnicity, African American, Asian, Bi-racial). Mothers who
identified themselves as Caucasian of Hispanic ethnicity were grouped with the other
racial groups due to cultural differences with mothers in the Caucasian, non-Hispanic
group; many were immigrants and English was their second language. There was a
significant positive correlation between race and income (r= .360, p<.01); Caucasian,
non-Hispanic mothers reported significantly higher incomes than the other mothers in the
study. There was a significant negative correlation between race and normalization (r= -
.247, p<.05). Mothers who were of Hispanic ethnicity, African American, Asian, or Bi-

186
racial had higher scores on the Normalization Subscale indicating greater normalization
efforts.
Income
A mother’s reported total family income was significantly correlated in a positive
direction with race (r= .360, p<.01) as noted above. There was also a significant negative
correlation of income with depressive symptoms (r= -.224, p<.05). Mothers with higher
total family incomes reported fewer depressive symptoms.
Duration of Caregiving
There was a significant positive correlation between duration of caregiving, and
both a child’s age and the amount of home health care nursing the child received per
week. The older the child the longer the duration of care (r= .733, p<.01). Also, the
longer the duration of care the greater the amount of home health care nursing the child
received per week (r= .236, p<.05). Duration of caregiving also had a significant positive
correlation with the level of technology dependence for the intravenous group compared
to all others (r= .257, p<.01) but not for the ventilator group. Children with a longer
duration of care were more likely to be classified as Group 2 (intravenous medications or
nutrition) than Group 1 (ventilators) or Group 3 (respiratory/nutritional support).
Amount of Home Health Care Nursing
There was a significant positive correlation between amount of home health care
nursing and duration of caregiving and the child’s age as noted above. Amount of home
health care nursing was also significantly correlated in a positive direction with level of
technology dependence (r= .417, p<.01). Children with a greater amount of home health
care nursing were more likely to be classified as OTA (1987) Group 1 (mechanical

187
ventilation) than Group 2 (intravenous medications/nutrition) or Group 3
(respiratory/nutritional support).
Depressive Symptoms
There was a significant negative correlation between depressive symptoms and
income as noted above (r= -.224, p<.05). Additionally, there were significant negative
correlations between depressive symptoms and normalization efforts as well as the
child’s functional status. Mothers who reported a greater number of depressive symptoms
had lower scores on the Normalization subscale indicating less use of normalization (r= -
.453, p<.01) and had children with poorer scores on the Functional Status II-Revised
indicating poorer function (r= -.239, p<.05). There was a very strong significant positive
correlation between depressive symptoms and family functioning (r= .608, p<.01).
Mothers who reported a greater number of depressive symptoms had a higher
discrepancy score indicating poorer family functioning.
Normalization
There was a significant negative correlation between normalization and race (r= -
.247, p<.05) as well as depressive symptoms (r= -.453, p<.01) as noted above. Mothers of
non-Caucasian race or Hispanic ethnicity with fewer depressive symptoms reported
greater use of normalization. There was also a significant negative correlation between
normalization and family functioning (r= -.348, p<.01). Mothers who reported greater use
of normalization had lower discrepancy scores indicating better family functioning.
Additionally, functional status had a significant positive correlation with normalization
(r= .375, p<.01). Mothers who reported greater use of normalization had children with
better function.

188
Family Functioning
There was a strong significant positive correlation between family functioning
and depressive symptoms (r= .608, p<.01) as noted above. Mothers with a higher
discrepancy score indicating poorer family functioning reported a greater number of
depressive symptoms. Additionally there was a significant negative correlation between
family functioning and normalization (r= -.348, p<.01). Mothers with lower discrepancy
scores indicating better family functioning reported greater use of normalization.
Functional Status
There was a significant negative correlation between the child’s functional status
and depressive symptoms (r= -.239, p<.05) as noted above. Mothers with children who
had higher functional status scores indicating better function reported fewer depressive
symptoms. Additionally, there was a significant positive correlation between the child’s
functional status and normalization efforts (r= .375, p<.01) as noted above. The higher
the child’s functional status score indicating better function the greater the use of
normalization efforts.
Level of Technology Dependence
In order for the categorical variable of level of technology dependence to be
included in the multiple regression analysis, two dummy variables were created to
represent the three levels of technology dependence (OTA Groups 1-3). Variable Tech.
Dependent 1= Group 1 (ventilators) versus all others and Tech Dependent 2= Group 2
(intravenous medications/nutrition) versus all others. There were significant positive
correlations between level of technology dependence OTA (1987) Group 2 and duration
of caregiving (r= .257, p<.01) as well as child’s age (r= .202, p<.05). Children who were
older and had a longer duration of care, more likely they were to be classified as OTA

189
(1987) Group 2 (intravenous medications or nutrition) than Groups 1 or 2. Children who
were classified as Group 1 (ventilators) had a significantly greater number of home health
care nursing hours per week (r=.417, p<.01).
Regression Analysis – Family Functioning
A hierarchical multiple regression analysis was conducted to examine the
significance of the research hypotheses. Assumptions of normality, linearity,
homoscedasticity, independence, zero mean for residuals as well as absence of
measurement error, multicollinearity and influential data points were met.
For research question one, family functioning was regressed on mother’s
depressive symptoms, child’s severity of illness (functional severity and level of
technology dependence) and normalization efforts. As shown in Table 4.13 Model A,
depressive symptoms, child’s severity of illness and normalization accounted for 36.3%
of the adjusted variance in family functioning and achieved statistical significance (F=
12.172, p<.001). The only independent variable in the regression equation noted to be
significant according to the standardized beta was depressive symptoms ( = .56,
p=<.001). After all covariates (length of caregiving duration, amount of home health care
nursing hours, race, family income and age of the child who is dependent on technology)
were included in the regression model (Table 4.13 Model B) the adjusted variance
decreased slightly to 34.9%. Depressive symptoms continued to be the only significant
variable as indicated by the standardized beta ( = .585, p=<.001).
To address the hypothesis: “More depressive symptoms, greater severity of illness
and less normalization effort are related to poorer family functioning while controlling
for length of caregiving duration, amount of home health care nursing hours, race, family

190
income and age of the child who is dependent on technology” the hierarchical regression
equation in Table 4.13 Model B was examined. There was a significant finding in relation
to depressive symptoms and family functioning in the direction proposed ( = .585,
p=<.001) therefore this portion of the hypothesis was supported. On the contrary, there
was no significant influence of severity of illness (functional status, level of technology
dependence) and normalization on family functioning therefore this portion of the
hypothesis was not supported.
Table 4.13. Summary of Regression Analysis for Family Functioning (N=99) Predictor Variable Model A Model B B B Constant 22.974 19.636 Normalization -.010 -.094 -.015 -.136 Functional Status -.001 .000 .115 .022 Depressive Symptoms 1.057 .560*** 1.103 .585*** Tech. Dependent: Ventilator 4.259 .078 5.774 .105 Tech. Dependent: IV 6.274 .087 7.211 .100 Race -4.826 -.100 Age of Child .059 .150 Duration of Caregiving -.060 -.132 Home Healthcare Nursing -.001 -.003 Family Income 1.867 .120 R2 .396 .415 Adjusted R2 .363 .349 F 12.172*** 6.243*** ***p .001

191
In conclusion, the only variable in this regression equation that was significantly
related to family functioning was mother’s depressive symptoms; greater depressive
symptoms were related to poorer family functioning.
Research Question 2. Are there differences in a) family functioning and b)
normalization efforts and c) mother’s level of depressive symptoms based on the child’s
level of technology dependence (3 levels)?
Testing Assumptions for Analysis of Variance (ANOVA)
The following assumptions were examined prior to the ANOVA testing:
1) Instruments at Proper Level of Measurement. The instruments used to
determine the dependent variables (family functioning, normalization, depressive
symptoms) were continuous, interval level measurements and the independent variable (3
levels of technology dependence) was categorical with a minimum of two groups. This
assumption was met.
2) Normality. The variable residuals were examined using a histogram and
probability plot as previously discussed. The data assumed a normal distribution.
Additionally, with a large sample size such as in this study (N=103) the Central Limit
Theorem assumes normal distribution. This assumption was met.
3) Mutually Exclusive Groups. Levels of technology dependence were mutually
exclusive groups as determined by the OTA (1987) rubric therefore this assumption was
met.
4) Equality of Variances. This assumption was examined by determining the
Levene statistic. The Levene statistic was non-significant for each ANOVA meaning
equal groups were assumed. Since there were fewer than 20 participants (Tabachnick &

192
Fidell, 2001) in two of the three groups, the Welch F-ratio and the Brown-Forsythe F-
ratio, more robust tests of equality of means were used (Fields, 2005).
5) Linearity. This assumption was tested by analyzing the partial regression
scatter-plots for each of the continuous study variables. The partial plots option assesses
the effect of each independent variable on the dependent variable controlling for all of the
other independent variables. It was determined that normalization was non-linear
therefore the variables were squared to overcome the violation of non-linearity. Since no
differences in results were noted, the original (non-squared) variable was used to
maintain a more parsimonious model.
6) Absence of Outliers. This assumption was tested by examining that the Cook’s
D for each of the dependent variables are not equal to or >1.0. This assumption was met.
Tests of Significance
Although each of the dependent variables (family functioning, normalization,
depressive symptoms) were correlated >.30 with one another, they were not correlated
>.30 with the independent variable (level of technology dependence). Individual
ANOVAs were performed for each of the dependent variables and results are shown in
Table 4.14.
Results on Table 4.14 include the means, standard deviations, ANOVA F
Statistic, Welch F Statistic and Brown-Forsythe F Statistic for ANOVA tests of each of
the dependent variables. The ANOVA tests examined if the between group differences
were greater than the within group differences. The F test was used to determine
significance at the .05 level. The F test for each of the dependent variables; family
functioning (F= 1.589, p= .208), normalization (F= 1.749, p= .362) and depressive
symptoms (F= .377, p= .687) was found to be non-significant. The Welch and the

193
Brown-Forsythe Statistical tests for equality of means, alternative robust F-ratio
formulas, were employed to evaluate differences between the group means (Fields,
2005). Both the Welch F and the Brown-Forsythe F tests were non-significant for each of
the dependent variables indicating that there were no significant differences between the
levels of technology dependence (OTA Groups 1-3) for family functioning,
normalization and depressive symptoms (Table 4.14).
A Multiple Analysis of Variance (MANOVA) was performed with all three of the
dependent variables (family functioning, normalization, depressive symptoms) to reveal
differences not shown in separate ANOVAs and also to overcome any overall inflated
Type I error (Mertler & Vannatta, 2005; Tabachnick & Fidell, 2001). The result of the
Box’s Test was non-significant therefore, equal variances were assumed. Results from
the MANOVA were as follows: Wilk’s Lambda .959, F=.679, p=.667. Therefore, results
from the MANOVA were insignificant as well; there were no significant differences in
the means between the groups (level of technology dependence) for family functioning,
efforts at normalization and level of depressive symptoms.

194
Table 4.14. Means, Standard Deviations and One-Way Analysis of Variance (ANOVA) for Three Levels of Technology Dependence and Three Dependent Variables
ANOVA Welch Brown-Forsythe Variable Group 1 Mechanical Ventilators
n=18
Group2 IV Nutrition and/or Meds.
n=9
Group 3 Resp/Nutrition
Support n=76
F
Statistic
p value
Statistic
p value
X SD X SD X SD Family Functioning 39.76 13.95 43.89 31.74 33.19 20.09 1.589ns 1.548 p=.240ns 1.130 p=.352ns
(df2, 98) Normalization 371.28 158.70 305.67 130.39 398.86 202.90 1.028ns 1.749 p=.198ns 1.586 p=.218ns
(df2, 100) Depressive Symptoms 14.61 9.94 16.89 10.11 13.61 11.47 .377ns .421 p=.662ns .445 p=.645ns
(df2, 100) Note: ns = non-significant

195
Research Question 3. Do a mother’s depressive symptoms have a mediating effect
on the relationship between the child’s severity of illness (functional status) and (a)
normalization and (b) family functioning in mothers with a child who is technology
dependent?
The assumptions for multiple regression were met as previously discussed in
research question one: normality, linearity, homoscedasticity, independence, zero mean
for residuals as well as absence of measurement error, multicollinearity and influential
data points. Results of the Pearson r product-moment correlations were also examined
(Table 4.12). Additionally, the following assumptions for mediator testing were
examined prior to proceeding: 1) there is a significant direct effect of the independent
variable (functional status) on the dependent variable (normalization, family functioning)
and 2) there is no measurement error in the mediator- depressive symptoms (Baron &
Kenney, 1986; Bennett, 2000). Both of these assumptions were met.
Mediation Testing
A variable functions as a mediator when variation in an independent variable
account for variations in the proposed mediator (path a), variations in the mediator
account for significant variations in the dependent variable (path b) and finally when the
previous paths (paths a and b) are controlled, there is no longer a significant relationship
between the independent variable and the dependent variable (path c). The strongest
evidence of mediation is when this path is zero (Baron & Kenny, 1986).
Based on the study model, (Figure 1.2) the mediating effect of depressive
symptoms between the child’s functional status and normalization as well as family
functioning were examined. To test if depressive symptoms mediated the relationship

196
between child’s functional status and normalization or family functioning three steps of
regression were used. If the mediating effect was present the following needed to occur:
(1) the independent variable (child’s functional status) is a significant predictor of the
mediator (depressive symptoms) as indicated by a significant F test (alpha .05), (2) the
independent variable (child’s functional status) is a significant predictor of the dependent
variable (normalization or family functioning) as indicated by a significant F test (alpha
.05), (3) the relationship between the independent variable and the dependent variable is
reduced when the mediator (depressive symptoms) is added, that is, there is a significant
drop in the -weight or the -weight for the independent variable becomes non-
significant.
Table 4.15. Mediating Effect of Depressive Symptoms between Functional Status and Normalization (N=103)
Variable Normalization Model A
Normalization Model B
B B Constant 5.406 192.214 Functional Status 17.725 .375*** 13.373 .283** Depressive Symptoms -6.638 -.385*** R2 .141 .281 Adjusted R2 .132 .266 R2 Change .134 ** p .01, ***p .001


198
and accounted for 13.2% of variance in normalization. After the mediator (depressive
symptoms) was entered, the adjusted R square increased to 26.6% (Table 4.15 Model B).
Therefore, after depressive symptoms was added the incremental R squared change was
13.4%.
A test for mediation effect of depressive symptoms between functional status and
family functioning was conducted using the assumptions and techniques described above.
The Pearson’s product moment correlation table (Table 4.12) was examined and it was
determined that functional status was not significantly correlated with family functioning
therefore depressive symptoms could not be a mediator between functional status and
family functioning. Table 4.16 and Figure 4.2 represent the test for mediation steps
followed.
Table 4.16. Mediating Effect of Depressive Symptoms between Functional Status and Family Functioning (N=101)
Variable Family Functioning Model A
Family Functioning Model B
B B Constant 53.781 21.373 Functional Status -.864 -.168 -.107 -.021 Depressive Symptoms 1.128 .603*** R2 .028 .371 Adjusted R2 .018 .358 R2 Change .340 *** p .001



201
Table 4.18. Mediating Effect of Normalization between Depressive Symptoms and
Family Functioning (N=101) Variable Family Functioning
Model A Family Functioning
Model B B B Constant 18.944 24.292 Depressive Symptoms 1.138 .608*** 1.056 .564*** Normalization -.011 -.100 R2 .370 .378 Adjusted R2 .364 .366 R2 Change .002 *** p .001
A test for mediation effect of normalization between depressive symptoms and
family functioning was conducted. The Pearson’s product-moment correlation matrix was
examined (Table 4.12) and it was determined that all three variables were significantly
correlated therefore mediation testing could proceed. Three conditions to test for a
mediating effect of normalization between functional status and family functioning were
as follows (Table 4.18, Figure 4.4): (1) the mothers depressive symptoms had a
significant relationship with normalization ( = -.453, p = <.001) that is an increased
number of depressive symptoms was related to less use of normalization, (2) on the
second regression, depressive symptoms explained 36.4% of the variance in family
functioning, increased depressive symptoms was related with higher family functioning
discrepancy score ( = .608, p= <.001) indicating poorer family functioning and the
equation was significant (Baron & Kenney, 1986) (Table 4.18 Model B). (3) when both
depressive symptoms and normalization were entered together the -weight for
depressive symptoms decreased ( = .564, p= <.001) however the level of significance


203
Research Question 5a. What are the relationships among mother’s depressive
symptoms, child’s severity of illness (functional status, level of technology dependence),
family functioning on normalization efforts in families with a child who is technology
dependent? 5b. Do these relationships hold after adjusting for length of caregiving
duration, amount of home health care nursing hours, race, family income and age of the
child who is dependent on technology?
Less depressive symptoms and severity of illness, Caucasian (non-Hispanic race),
longer caregiving duration, greater amount of home health care nursing hours and a
younger child were hypothesized to be significantly related to greater efforts at
normalization while controlling for length of caregiving duration, amount of home health
care nursing hours, race, family income and age of the child who is dependent on
technology.
A Pearson’s product moment correlation coefficient matrix comprising all study
variables and covariates (Table 4.12) was examined to determine if any significant
relationships existed. The assumptions of normal distribution and level of measurement
were met. The value of statistical significance was set at alpha .05.
Multiple Regression Analysis - Normalization
A hierarchical multiple regression analysis was conducted to examine the
significance of the research hypotheses. Assumptions of normality, linearity,
homoscedasticity, independence, zero mean for residuals as well as absence of
measurement error, multicollinearity and influential data points were met. Normalization
was regressed on mother’s depressive symptoms, child’s severity of illness (functional

204
Table 4.19. Summary of Regression Analysis for Normalization (N=99) Predictor Variable Model A Model B B B Constant 224.801 240.903 Family Functioning -1.013 -.112 -1.242 -.137 Functional Status 12.928 .275** 14.629 .312*** Depressive Symptoms -4.944 -.289* -4.204 -.246* Tech. Dependent: Ventilator -31.183 -.063 16.070 .034 Tech. Dependent: IV -66.959 -.103 -87.049 -.134 Race -133.185 -.305** Age of Child 1.177 .330** Duration of Caregiving -.511 -.122 Home Healthcare Nursing -.825 -.193* Family Income 4.917 .035 R2 .284 .410 Adjusted R2 .246 .343 F 7.381*** 6.111*** *p< .05 **p< .01 ***p .001 status and level of technology dependence) and family functioning. As shown in Table
4.19 Model A, depressive symptoms, child’s functional status and family functioning
accounted for 24.6% of the adjusted variance in normalization and achieved statistical
significance (F= 7.381, p<.001). Two independent variables in the regression equation
were significant: depressive symptoms ( = -.289, p=<.05) and functional status of the
child ( = .275, p=<.01). After all covariates (length of caregiving duration, amount of

205
home health care nursing hours, race, family income and age of the child who is
dependent on technology) were included, the adjusted variance of the regression model
(Table 4.19 Model B) increased to 34.3% with a R square change of 12.6%. Depressive
symptoms remained a significant variable in the equation however the addition of the
covariates caused the standardized beta to drop ( = -.246, p= .030). Functional status
continued to be significant and the standardized beta increased with the addition of the
covariates ( = .312, p= .001). Three covariates added to the explained variance in the
regression model (Table 4.19 Model B); amount of home health care nursing ( = -.193,
p= <.05), child’s age ( = .330, p= <.01) and race ( = -.305, p= .001).
To address the hypothesis: “Less depressive symptoms and severity of illness,
Caucasian (non-Hispanic ethnicity), longer caregiving duration, greater amount of home
health care nursing hours and a younger child are significantly related to greater efforts at
normalization while controlling for length of caregiving duration, amount of home health
care nursing hours, race, family income and age of the child who is dependent on
technology” the hierarchical multiple regression equation in Table 4.19 Model B was
examined. There was a significant finding in relation to depressive symptoms ( = -.246,
p= <.05) as well as functional status ( = .312, p= .001) and normalization in the direction
proposed therefore these hypotheses was supported. On the contrary, level for technology
dependence was not significantly related to normalization efforts in the direction
proposed for either Group 1 ( = .034, p= .739) or Group 2 ( = -.134, p= .139) as
compared to Group 3 therefore the hypothesis regarding severity of illness was only
partially supported. Better functional status but not level of technology dependence was
significantly related to greater normalization efforts. Caucasian (Non-Hispanic) race was

206
not significantly related to greater efforts at normalization. The opposite was true;
Hispanic ethnicity and other races were significantly related to greater efforts at
normalization in this study ( = -.305, p= .001). This hypothesis was not supported.
Duration of caregiving was not significantly related to greater efforts at normalization
( = -.122, p= .341). This hypothesis was not supported. The amount of home health care
nursing hours was significantly related to efforts at normalization but contrary to the
hypothesis, decreased amount of home health care nursing hours was significantly related
to greater efforts at normalization ( = -.193, p= <.05). This hypothesis was not
supported. The age of the child was significantly related to efforts at normalization but
contrary to the hypothesis, older age of the child was significantly related to greater
efforts at normalization ( = .330, p= .009). This hypothesis was not supported.
Therefore the variables that were significantly related with greater normalization
efforts include: better functional status, less depressive symptoms, Non-Caucasian race or
Hispanic ethnicity, less home health care nursing hours and older age of the child who is
technology dependent.

207
CHAPTER FIVE - DISCUSSION
Introduction
Few quantitative studies have examined the impact of a child who is technology
dependent on their families yielding little evidence to guide delivery of care for this
population. This study explores how families (n=103) manage the challenges of caring
for a child who is technology dependent at home following discharge from the hospital.
This chapter includes a summary of the study findings, significance for nursing research
and practice as well as an interpretation of the findings based on prior empirical and
theoretical literature. Limitations of the study are discussed and future research
recommendations, based on study findings, are suggested.
Summary
This study examined how families respond to and manage the special challenges
of children who are technology dependent after they have been discharged from the
hospital to home. Participants of this study included 103 mothers who cared for their
children aged 7 months-16 years who are technology dependent at home for a minimum
of 2 months. The purpose of this study was to examine the relationship between
child/maternal factors (child’s functional status, level of technology dependence,
mother’s depressive symptoms, length of caregiving duration, amount of home health
care nursing hours, race, family income and age of the child) and (a) family functioning
as well as (b) normalization in families with a child who is technology dependent.
Additionally, this study examined whether there are differences in family functioning,

208
normalization and depressive symptoms based upon the child’s level of technology
dependence (Group 1 mechanical ventilation, Group 2 intravenous nutrition/medication,
Group 3 respiratory/nutritional support) using the Office of Technology Assessment
(1987) rubric. The orienting frameworks for this study were the Family Management
Style Framework by Knafl and Deatrick (2003) and Paterson’s “Shifting Perspectives
Model of Chronic Illness” (2001).
Convenience sampling was used to recruit mothers (n=103) primarily from
Rainbow Babies and Children’s Hospital (RB&C), a large children’s hospital in
Cleveland, Ohio from July 2007-November 2008. A majority of mothers lived in the
Northeastern Ohio area; a few were recruited from bordering states served by the tertiary
care hospital. The number of participants in the study was adequate based upon an a
priori power analysis that included the effect size, alpha and power of greater than .80 to
decrease the chance of a Type II error. Face-to-face interviews were conducted in the
RB&C outpatient clinics or in a private place of the mother’s choosing. In addition to a
demographic questionnaire five instruments were included in the data collection
interview: the Functional Status II-Revised (Stein & Jessop, 1990), Level of Technology
Dependency Questionnaire, the Center for Epidemiological Studies-Depression Scale
(Radloff, 1977), “Actual Effect of a Chronic Physical Disorder on the Family” subscale
of the Normalization Scale (Murphy & Gottlieb, 1992) and the Feetham Family
Functioning Survey (Roberts & Feetham, 1982).
Statistical analyses were performed to answer the research questions. A Pearson
product-moment correlation matrix was developed to evaluate the relationship between
the variables. Normalization, family functioning and depressive symptoms were all

209
significantly correlated with one another. Additionally, functional status was significantly
correlated with normalization and depressive symptoms; income with depressive
symptoms and race with normalization. Hierarchical Multiple Regression analyses were
used to evaluate the percentage of explained variance as well as the relationship of
independent variables and covariates with the outcome variables family functioning and
normalization. Additionally, mediating effects of normalization on family functioning as
well as mediating effects of mother’s depressive symptoms on normalization and family
functioning were examined using multiple regression analyses. Analysis of Variance
(ANOVA) was performed to examine differences in normalization efforts, family
functioning and mother’s depressive symptoms based on the child’s level of technology
dependence.
Findings from this study indicate that mothers of children who are technology
dependent are at high risk for psychological distress that can affect overall family
functioning. A mother’s depressive symptoms was the only significant predictor of
family functioning while controlling for covariates (length of caregiving duration,
amount of home health care nursing hours, race, family income and age of the child who
is dependent on technology) in Hierarchical Multiple Regression analysis; greater number
of depressive symptoms was related to poorer family functioning. Using Hierarchical
Multiple Regression Analysis, several independent variables/covariates were found to be
significant predictors of greater normalization efforts: better child’s functional status, less
depressive symptoms, fewer home health care nursing hours per week, an older child and
Non-Caucasian race or Hispanic ethnicity. ANOVA analyses indicate there were no
statistical differences in normalization efforts, family functioning and mother’s

210
depressive symptoms based on the child’s level of technology dependence. Statistical
analyses for mediation (Baron & Kenney, 1986) revealed that depressive symptoms are a
mediator between the child’s functional status and normalization.
Findings
Characteristics of Participants
Statistical analyses of mother’s individual characteristics showed that while the
average age of the mothers was 38 years old (range 21-66 years) there was a wide age
variation; approximately 10% were 51 years or older. The majority of mothers were
Caucasian, non-Hispanic (73%) however the percentage of minority participants modeled
the demographics of Northeastern Ohio. Mothers possessed a wide variation of
educational backgrounds; the majority (68.9%) had at least a partial college education.
Most participants (85.4%) were the biological mother of the child but a surprising finding
was the number of adoptive/foster mothers and grandmothers who cared for these
children. All of the adoptive and foster mothers had full knowledge that the child was
technology dependent and had multiple special health care needs prior to establishing the
caretaking relationship. A majority of mothers were married (70.9%). About half of the
participants (50.5%) had a yearly total family income that was $60,000 or less however
19.4% earned $80,001 or more and 11.6% had incomes less than the federal poverty level
for a family of four. Almost half of participants (45.6%) were not employed outside the
home while 27.2% worked 40 hours or more per week. No data were collected in this
study regarding employment status prior to caring for the child who was technology
dependent however. Many mothers who were not employed outside of the home

211
indicated that this was their full time job; coordinating care, performing multiple care
tasks and transporting their child to a variety of health care and therapy appointments.
Characteristics of Participant’s Children
The mean age of the children was 6.58 years (range 7 months-16.6 years);
approximately half were age 5 years or less (47.6%); a finding consistent with the
literature. According to Houtrow, Kim and Newacheck (2008), children with special
health care needs ages 5 years or less had 3.6 times the hospital days and 100 times more
home health care days as their peers with the highest decile of these children accounting
for 74% of medical expenditures for this age group. Undoubtedly, the highest decile
group referred to are those children who are technology dependent. There were an equal
number of each gender. Only one article was found that described the demographics and
characteristics of children who are technology dependent in England (Kirk, 2008); none
were found that described this population in the United States. Most of the available
literature described children with special health care needs in general.
About half (49.5%) of the children had a primary diagnosis that was due to a
genetic disorder and 27.1% were born preterm at 36 weeks or less. The largest percentage
of children had diagnoses related to neuromuscular dysfunction (43.7%) or respiratory
dysfunction (22.3%).
A majority of children (73.8%) were categorized as belonging to OTA (1987)
Group 3 and required respiratory or nutritional support such as oxygen, feeding tube or a
tracheostomy while others were categorized as Group 1 (17.5%) requiring mechanical
ventilation or Group 2 (8.7%) requiring intravenous medications or nutritional
substances. This finding is characteristic of the population of these children as fewer

212
children require mechanical ventilation or intravenous medications/nutrition. About half
required one type of technology (49.5%) however some children (12.6%) required up to
four types of technology simultaneously. Almost all (88.7%) of the children had either a
nasogastric tube (1.9%) or gastrostomy tube (86.4%). Other frequently required
technologies included oxygen or a tracheostomy tube. A total of 42.7% required oxygen
on at least an as-needed basis via nasal cannula, face mask, trach collar, continuous
positive airway pressure and 31.1% required a tracheostomy tube. Less frequently
required technologies were mechanical ventilators (17.5%) or intravenous
medication/nutritional substances (9.7%).
Caregiving Variables
The average caregiving duration was 57 months (range 2-161 months) and
included a fairly even distribution in each of the categories (Table 4.6). This data points
to the fact that many of these children do remain dependent on technology for significant
periods of time. The high level of care required by these children over the long term can
be taxing on the mother’s mental health and consequently family functioning. The
average amount of home health care nursing that the children received was 41.23 hours
per week (range 0-144) however; a large proportion of children (36.8%) did not receive
any home health care nursing (Table 4.6). Therefore, while some mothers received
respite others were not as fortunate either because they were unable to find qualified
nursing help or they were not eligible to receive such services due to insurance or had
been denied enrollment in the state funded Medicaid waiver program. Children who
received the greatest number of home health care nursing hours were those children who
were categorized as Group 1 (mechanical ventilators) and Group 2 (intravenous

213
medications/nutritional substances). These children often required more frequent and
complex care and treatments and therefore were often enrolled in the Medicaid waiver
program.
Depressive Symptoms
Mothers in this study reported higher levels of depressive symptoms compared to
the general population (Radloff, 1977) as measured by the CES-D. In this study, 39.8%
of mothers scored at or above 16 (cutoff established indicating risk for clinical
depression) on the CES-D as compared to 21% of the general population (Radloff, 1977)
and up to 45% in previous studies of mothers of children who are technology dependent
(Kuster & Badr, 2006; Miles et al., 1999). The mean CES-D score of 14.07 (SD 11.05)
for women in this study was similar to previous findings in studies of mothers with
children who are technology dependent where mean scores ranged from 13.6-15.5
(Heyman et al., 2004; Kuster & Badr, 2006; Miles et al., 1999). While prior studies
indicated the percentage of mothers who scored 16 or greater on the CES-D, none
indicated the percentage that scored above a more critical level of 21 or greater (Myers &
Weissman, 1980). In this study, 15.5% scored 16-20 while 24.3% scored equal to or
greater than 21 on the CES-D indicating a higher risk for clinical depression. Therefore,
women in this study were identified as at risk for clinical depression at approximately
double the rate of the general population (21% vs. 40%). Clearly, a large proportion of
these mothers are at risk for clinical depression and many (24%) are at a significant risk
due to their very high levels of depressive symptoms.

214
Depressive Symptoms and Severity of Illness
Correlational analysis revealed that depressive symptoms had a significant
negative correlation with the child’s functional status which is consistent with prior
studies of children with chronic illness (Silver et al., 1998; Silver et al., 1995; Frankel &
Wamboldt, 1998; Lustig et al., 1996; Weiss & Chen, 2002). On the contrary, other
researchers did not find a relationship between depressive symptoms and severity of
illness however standardized instruments were not used to measure severity of illness
(Affleck, 1987; Miles et al., 1999; Thompson et al., 1993).
While functional status was significantly correlated with a mother’s depressive
symptoms, findings from this study, both Pearson Product-Moment Correlations and
ANOVA, indicate that the level of technology dependence was not. Mothers of children
with mechanical ventilation or intravenous medications/nutrition did not have a greater
number of depressive symptoms as compared to mothers of children with respiratory or
nutritional support. This is consistent with findings from previous studies (Fleming et al.,
1994) and may be due in part to the mother’s perception and definition of the situation.
What may seem overwhelming and tragic to one mother regarding treatment and care for
her child may be viewed as manageable to another.
Depressive Symptoms and Family Income
A mother’s depressive symptoms had a significant negative correlation with
family income which is consistent with prior research (Canning et al., 1996; Drotar et al.,
1997; Shore et al., 2002). Lower family income was related to a mother’s increased
depressive symptoms. Income however was not a significant predictor of normalization
or family functioning in the multiple regression analyses.

215
Depressive Symptoms and Family Functioning
In this study, depressive symptoms had a strong positive correlation with family
functioning; greater number of depressive symptoms was related to a higher family
functioning discrepancy score indicating poorer family functioning. Furthermore,
hierarchical multiple regression analysis indicated (Figure 5.1) that a mother’s level of
depressive symptoms was the only significant predictor ( = .585, p=<.001) of family
functioning while controlling for the child’s severity of illness (functional status, level of
technology dependence), normalization efforts as well as the covariates (caregiving
duration, amount of home health care nursing hours, race, family income and child’s
age). A mother’s level of depressive symptoms therefore accounted for 34.9% (F=6.243,
p<.001) of the variance in family functioning (Table 4.10).
This study’s findings regarding a strong relationship between depressive
symptoms and family functioning is consistent with previous research (Frankel &
Wamboldt, 1998; Ireys and Silver, 1996; Kuster et al., 2006). Past research indicates that
decreased satisfaction with family relationships, an indicator of family functioning, is
significantly related to greater depressive symptoms (Shore et al., 2002; Weiss & Chen,
2002). Frankel and Wamboldt (1998) found that the Psychiatric Symptom Index
predicted 39% of the variance in the Impact On Family Scale, a measure of family
functioning. The researchers propose that how a child’s illness interferes with and
impacts a family is determined by the psychological health of the primary parent
caretaker. The psychological health of the parent is in turn affected by family functioning
and the child’s functional status (Frankel & Wamboldt, 1998). Ireys and Silver (1996)
also found that family functioning accounted for a large percentage of variance on a

216
mental health measure (p=<.001) even after controlling for other variables. Therefore, a
mother’s psychological state, particularly the amount of depressive symptoms, plays a
significant role in how a family with a child who is technology dependent functions.
Age
Race
Amt. ofHHC Nsg
NormalizationR2 = .34
.585 ***-.2
46 *
FamilyFunctioning
R2 = .35
Mother'sDepressiveSymptoms
Child'sSeverity of
Illness
.312 ***.330 **
-.305 **
-.193 *
-.239
*
* p< .05 **p<.01 ***p<.001
Figure 5.1. Study Model for Normalization and Family Functioning in
Families with a Child who is Technology Dependent
Depressive Symptoms and Normalization Efforts
Depressive symptoms also had a strong negative correlation with normalization
efforts in this study; mothers with greater depressive symptoms made fewer
normalization efforts (Figure 5.1). Normalization efforts and depressive symptoms of
mothers have not been measured together to date in any previous study. Past research

217
regarding caregivers of children who are technology dependent has indicated a significant
level of depressive symptoms. Some of the depressive symptoms such as sleep
disturbances or inability to concentrate could affect performance of complex
technological procedures (Smith, 1999) and consequently compromise the care of her
child who is technology dependent as well as any typically developing siblings in the
household. Additionally, depressive symptoms can influence a mother’s definition of the
situation, one of the major components of normalization (Knafl & Deatrick, 2003).
Therefore, a mother’s psychological state plays an important role in normalization efforts
that can promote the integration of the child who is technology dependent and the care
required into the family and family life.
In conclusion, a mother’s depressive symptoms have a significant influence on a
family’s functioning and are a major predictor of how much a family is affected by the
child’s chronic illness and dependence on technology. Additionally, depressive
symptoms significantly affect a mother’s normalization efforts.
Normalization
Normalization had a significant negative correlation with race, depressive
symptoms and family functioning as well as a significant positive correlation with the
child’s functional status. Non-Hispanic, Caucasian mothers, greater depressive
symptoms, poorer family functioning and a child’s poorer functional status were all
significantly related with less normalization efforts (Figure 5.1). Greater normalization
indicates greater integration of the child and his/her care into every day family life and is
viewed as a desirable goal for families of children with chronic illness (Knafl & Deatrick,
2003).

218
Normalization and Race
In this study, normalization was significantly correlated with race; mothers who
were of Hispanic ethnicity, African American, Asian or Biracial had significantly greater
efforts at normalization. There have been few previous studies regarding normalization
but to date none have found a relationship between race and normalization (Knafl et al.,
1996). One quantitative study regarding normalization did not specifically examine the
relationship between race and normalization (Murphy, 1994). Many of the studies were
qualitative with small samples and did not describe the ethnicity of participants and in
those that did, the majority was Caucasian.
Normalization and Child’s Age
Normalization and child’s age was significantly correlated in this study.
Participants with older children used greater normalization efforts. This is contrary to
previous studies. Knafl and Deatrick (2006) stated that one of the barriers to
normalization in children with chronic illness was older age of the child; parents had a
greater difficulty with normalization efforts particularly if the child was an adolescent.
Qualitative studies that examined normalization efforts with children who are technology
dependent (Carnevale et al., 2006; Judson, 2004; Lee, 1996; Morse et al., 2000; Rehm &
Bradley, 2005) did not examine the effect of a child’s age on normalization efforts.
Normalization and Depressive Symptoms
Normalization also had a significant negative correlation with depressive
symptoms; mothers in this study with increased depressive symptoms used less
normalization efforts. According to Clark et al. (1999), depression, and even sub-clinical

219
depressive symptoms, are associated with significant impairment in psychosocial and
physical functioning and well being and could therefore affect normalization.
Furthermore, depressive symptoms can influence a mother’s definition of the situation,
one of the major components of normalization (Knafl & Deatrick, 2003). Having a
negative view of the situation could thus influence and lessen the amount of
normalization effort. No previous research has specifically examined the relationship
between a parent’s normalization efforts and their own psychological well-being.
Normalization and Family Functioning
Normalization also had a significant negative relationship with family
functioning; greater normalization efforts were related to lower family functioning
discrepancy scores indicating better family functioning. Knafl and Zoeller (2000) also
found that parents with greater normalization efforts had better family functioning. The
researcher hypothesized that with greater normalization efforts families identify illness
management strategies that help with family functioning (Knafl & Zoeller, 2000).
Greater normalization efforts have been found to be related to greater flexibility in
carrying out treatments so that the illness care is incorporated into family routines thus
improving family functioning (Gallo & Knafl, 1998; Knafl & Deatrick, 2002; Knafl &
Gilliss, 2002; Thorne et al., 1997; Wilson et al., 1998). Additionally, care for the child
who is technology dependent, if fit around other family activities, will facilitate family
functioning. Families learn “tricks of the trade” to facilitate this process of flexibility
(Gallo & Knafl, 1998) and routinization of the treatment regimen (Knafl & Gilliss, 2002).
Rules were broken to deliver safe care but yet “normalize” childhood by giving
experiences similar to other children while at the same time maintaining family

220
functioning (Wilson et al., 1998). Families who used less normalization effort in previous
studies were noted to have difficulties related to strictly adhering to the treatment
regimen, saw the treatment regimen as the focus of family life and a burden that made
their family different from other families (Knafl & Deatrick, 2002). Therefore, families
who incorporated flexibility in adherence to medical regimen used greater normalization
efforts which consequently led to improved family functioning.
Normalization and Severity of Illness
In this study, both functional status and level of technology dependence were
included in measurement of the concept, severity of illness. Only functional status was
found to have a significant correlation with normalization; greater normalization efforts
were related to better functional status. This is consistent with previous qualitative study
findings (Dashiff, 1993; Knafl & Deatrick, 2002). Additionally, Lee (1996) found that
mothers reported increased normalization efforts with their child’s decreased dependency
on technology, ie. less dependent on oxygen.
Components of the illness that have been found to interfere with and hinder
normalization efforts in children with chronic conditions include illness control,
uncertainty or unpredictability of the illness (Cohen, 1993; Haase & Rostad, 1994;
O’Brien, 2001) and visibility of the condition (Murphy, 1994). Knafl & Deatrick (2002)
found that with exacerbations and flare-ups of the child’s disease, there was dissolution
of normalization even in parents who described themselves as competent and confident
caregivers and managers of the illness. The illness exacerbation made the illness
management burdensome and the focus of family life; as in Paterson’s Model of Shifting
Perspectives (2001), brought the disease to the foreground. Conversely, as the illness

221
improved or became better controlled, parents shifted to normalization in their family life
and increased their normalization efforts. While the illness was in remission or was well
controlled, the illness management was taken for granted and became part of the family
routine thus normalizing efforts were increased (Knafl & Deatrick, 2002).
Researchers who studied families with children who were technology dependent
also noted a link between increased severity of illness and decreased normalization
efforts. In a qualitative study of families with ventilator dependent children, Carnevale et
al. (2006) found that normalization efforts were undermined by the unpredictability of the
child’s condition that was complicated and at times overwhelming. All of the families
devoted significant effort toward normalizing the experience by creating routines so that
their lives would resemble that of “normal” families.
Rehm and Bradley (2005), on the contrary, state that based on their qualitative
study, families with children who are technology dependent and developmentally delayed
do not meet the established attributes of normalization. Most notable was the conclusion
that the “normalcy lens” in these families was impossible. The researchers propose that
since the child’s condition required constant vigilance and frequent skilled intervention,
parents felt that they needed to continuously prioritize the care of the child and strove for
stability for all family members but did not see life as “normal”. Additionally, due to the
fragility of the child’s condition, particularly since they were both technology dependent
and developmentally delayed, parents were not able to modify the treatment regimen very
much nor were they able to count on a predictable routine that would aid in normalization
efforts. Due to the visibility of equipment and appearance of the child, parents felt

222
conspicuous in public and frequently experienced distress due to discrimination (Rehm &
Bradley, 2005).
Families of children who are technology dependent experienced many limits in
their routines and activities related to the child’s chronic condition. The equipment, time
required for treatments and care, the need for trained caregivers all affected normalization
efforts as well as the child’s ability to participate in normal childhood and family
experiences and socialization with peers (O’Brien & Wegner, 2002). The reliance on
technology also affected daily activities due to the time and planning required even for a
simple outing. Therefore, families of children who have poorer functional status,
particularly children who are technology dependent with poor functional status, have
more difficulty with normalization.
Hierarchical Multiple Regression Analysis of Normalization
Two independent variables in the regression equation were significant: depressive
symptoms and functional status of the child explained about 25% of the variance in
normalization. These findings are consistent with past research as discussed above;
depressive symptoms and functional status of the child are predictors of normalization
efforts. Following the addition of the covariates (length of caregiving duration, amount of
home health care nursing hours, race, family income and age of the child who is
dependent on technology) on the second step of the regression analysis, the amount of
explained variance increased to 34.3%. Three covariates were significant and added to
the explained variance; amount of home health care nursing, child’s age, and race. Less
home health care nursing hours, older child and those who identified themselves as
African-American, Asian, Bi-racial or of Hispanic ethnicity were significantly related

223
with increased normalization efforts. The remaining variance that has not been explained
in the regression model could be due to strain experienced by these mothers that may
hinder normalization efforts or as Rehm and Bradley (2005) suggest, the presence of
developmental delay. Additionally, as Knafl and Deatrick (2003) indicate, mutuality
between both mother and father regarding management strategies helps promote
normalization while increased conflict decreases normalization efforts.
With regard to the home health care nursing hours, those children who require
more hours are those children who have a poorer functional status and more complex care
needs such as ventilators and intravenous medications/nutrition. Therefore, there are two
plausible explanations for the relationship between amount of home health care nursing
hours and normalization. One possibility is that it is actually the functional status of the
child and complexity of care needs that determine the amount of nursing hours; children
with more complex care needs qualify for more hours. It can then be proposed that it is
the functional status and not necessarily the home health care nursing hours that exert the
greatest influence on normalization efforts.
Another explanation for the relationship between nursing hours and normalization
is that an increased amount of nursing hours is disruptive to the family routine and limits
the amount of normalization efforts. Past research presents conflicting results regarding
the use of home health care nursing with children who are technology dependent. Nurses
in the home were seen as supportive yet disruptive (Wang & Barnard, 2004) as their
presence affected privacy and family dynamics (Obrien et al., 2002) such as marital,
sibling and parental relationships (Murphy, 1997). Knafl and Deatrick (2002) noted that
the major barrier to normalization is parental conflict and not illness management

224
because the continual tension keeps the illness a focus of family life. Furthermore, lack
of consistent, high quality nursing care contributed to family disorganization (Tommet,
2003). Interestingly, while children with ventilators (Group 1) required more home health
care nursing hours than children with intravenous medications/nutrition (Group 2) or
respiratory/nutritional support (Group 3) there were no significant differences between
groups in normalization efforts. To date, no previous studies have been found that
examined amount of home health care nursing hours and normalization efforts.
The findings from the model regarding contributors to normalization suggest that
families with older children who are technology dependent have significantly greater
normalization efforts. This finding is contrary to previous studies as noted above.
Races/ethnicity other than Caucasian, Non-Hispanic was noted to have greater
normalization efforts in this study. While no past research has examined the relationship
between race and normalization, the literature suggests that African American caregivers
are resilient despite the negative effects of caregiving and displayed higher levels of
resourcefulness in the face of adversity (Gonzalez, 1997; Zauszniewski & Wykle, 1994).
These findings from past studies help to illuminate possible reasons for differences in
normalization efforts between Caucasian, Non-Hispanic mothers and other racial/ethnic
groups.
Normalization, while not an entirely new concept has only been measured
quantitatively in one previous study (Murphy, 1994). According to Knafl and Deatrick
(2002), a family’s definition of the situation influences management behaviors; both of
these, then, ultimately affect normalization efforts. In this study, the child’s functional
status and mother’s depressive symptoms were the most important predictors of

225
normalization efforts. This is consistent with previous literature that complexity of care is
related to how much families are able to normalize particularly if the child’s condition is
fragile and unpredictable (Carnevale et al., 2006). Parents are thus unable to establish a
routine, a key component of normalization. Furthermore, a child’s functional status will
determine how much a family’s lifestyle may be limited particularly if there is little room
for flexibility with treatments and management behaviors; an important component of
normalization. Additionally, a mother’s response to the child who is technology
dependent is shaped by their definition of the situation. Increased depressive symptoms
experienced by a mother and actual severity of illness affect their definition of the
situation thus management behaviors and consequently normalization.
Contrary to previous studies, older age of the child was related to increased
normalization efforts. Others proposed that with increasing age there is increased
pressure for conformity to peer groups. This did not appear to be the case in this study of
children who are technology dependent. Mothers were well aware of their child’s
differences from other children but sought to include them in as many age appropriate
activities as possible including attending school with a ventilator, intravenous
medications and feeding tubes and attending sporting events, camps and including them
on family vacations.
As an adjunct to this study, a qualitative question was posed. Many mothers
described how they problem-solved how to transport their child and their equipment and
supplies to appointments, family outings and vacations. Others described various
organizational strategies such as charts, notebooks and computer spread sheets to keep
track of the child’s supplies, physicians, therapists, surgeries, treatments, medications and

226
appointments. All of these activities point to management strategies employed by
mothers that were a part of their normalization efforts. An interesting finding was that
mothers who scored low on normalization efforts were unable to name an example of
how they were able to problem solve to continue living a “normal family life”; rather,
they discussed how the child’s condition was an obstacle or a barrier to being able to
carry on a normal family life.
Family Functioning
Family Functioning was significantly correlated with only two variables in this
study: mother’s depressive symptoms and normalization efforts. The relationship of both
of these predictors to family functioning was discussed above.
Hierarchical Multiple Regression Analysis osf Family Functioning
Interestingly, in contrast to normalization that had a number of predictors,
depressive symptoms was the sole predictor of family functioning in the regression
equation and accounted for a large proportion of explained variance (34.9%) even after
the addition of covariates (length of caregiving duration, amount of home health care
nursing hours, race, family income and age of the child who is dependent on technology).
Greater number of depressive symptoms was related to poorer family functioning.
Similar to past research, those mothers with greater depressive symptoms reported that
their child’s condition and technology dependence was disruptive and had a major impact
on family life, more specifically family functioning. The findings from the hierarchical
multiple regression analyses for family functioning suggest that a mother’s depressive
symptoms influence the mother’s perception of the illness or “definition of situation” as

227
proposed by Knafl and Deatrick’s (2003) Family Management Style Model and
consequently affect family functioning and helps to explain how families develop the
“normalcy lens”.
Results from this study also validate Paterson’s (2001) Shifting Perspectives
Model of Chronic Illness. A mother’s perception of reality is how the mother interprets
and responds to the illness. When a mother has “wellness in the foreground” the child is
seen as well or “normal” even if numerous technologies and treatments are necessary for
the child. This is not a distortion of reality or denial of the child’s fragile condition, but
rather a revision of what is “normal”. The goal of normalization is to allow the child who
is technology dependent to be integrated into the family and not to be the central focus.
This was evident in several cases when the mother scored high in normalization efforts.
Although normalization was significantly correlated with family functioning it was not a
significant predictor of family functioning in this analysis.
In summary, findings from the hierarchical multiple regression analyses for
normalization and family functioning suggest that a mother’s depressive symptoms and a
child’s functional status strongly influence the mother’s “definition of situation” and play
an important role in perception of the impact of the illness on normalization efforts and
family functioning. Since Group 3 (Respiratory/Nutritional Support) was such a large
group further analysis was performed to divide the children into two groups; children
with/without tracheostomies. The results from the ANOVA analysis with 4 groups (levels
of technology dependence) continued to show no difference for amount of depressive
symptoms. Therefore, results from ANOVA testing help to substantiate that the type of
technology the child uses (ventilator, intravenous medications/nutrition,

228
respiratory/nutritional support) is not a significant predictor of family functioning,
normalization efforts or a mother’s depressive symptoms.
Mediator Testing
Four separate analyses were performed in research questions 3-4 to test if
depressive symptoms and normalization functioned as mediators in this study. Mediators
help to give additional information regarding how or why variables are strongly
associated (Baron & Kenney, 1986) and show a process. Using mediation analysis
techniques as described by Baron and Kenney (1986), only a mother’s depressive
symptoms were found to have partial mediation effects between a child’s functional
status and normalization. Poorer functional status and greater depressive symptoms were
related to fewer normalization efforts. In hierarchical multiple regression of
normalization, the predictor variable, functional status, had the strongest, most significant
influence on the outcome variable, normalization (p=<.001) due to the presence of
depressive symptoms as a mediator. While no quantitative data could be found regarding
the mediation effects of depressive symptoms between functional status and
normalization, many researchers have described the significant relationship of a child’s
severity of illness, particularly functional status to a parent’s depressive symptoms
(Canning, et al., 1996; Lustig, et al., 1996; Silver et al., 1998; Silver et al., 1995; Frankel
& Wamboldt, 1998; Lustig et al., 1996; Weiss & Chen, 2002). Furthermore, increased
severity of illness has been linked to decreased normalization efforts particularly when
the illness is poorly controlled, the illness symptoms are unpredictable or with illness
exacerbations (Carnevale et al., 2006; Cohen, 1993; Dashiff, 1993; Haase & Rostad,
1994; Knafl & Deatrick, 2002; Lee, 1996; O’Brien, 2001). Therefore, this study finding

229
helps to explain the strong correlation between a child’s functional status and
normalization efforts; a mother’s depressive symptoms act as a mediator to help
strengthen the relationship.
While normalization was significantly correlated with family functioning it did
not perform as a mediator in the analysis. However, it is possible that with a larger
sample size normalization would be a significant predictor of family functioning.
Normalization would then possibly serve as a mediator between depressive symptoms
and family functioning.
Instruments
Overall, the instruments chosen for this study performed well and had acceptable
instrument reliability (Table 3.1). A Cronbach alpha coefficient analysis for the CES-D
excluded four participants due to missing data on one of the questions. The data was
missing totally at random on four different questions. After the mean score for each of the
missing items was imputed and the data re-analyzed the Cronbach alpha (.92) did not
change. Mothers did not voice any difficulty with completing this instrument.
The Cronbach alpha for the Normalization subscale was computed with only 81
participants because one item of the subscale (item 6) queried mothers regarding effect of
the technology dependent child on siblings. Therefore, mothers with only one child left
this VAS question blank. Reliability with 81 participants was .83. When the instrument
was reanalyzed with Item 6 deleted, the alpha was .78 with 99 participants. Some
mothers voiced concerns regarding the wording of a few of the items. Many indicated
that they did not care for the wording in item 5 “How much of a hassle does your child’s
medical treatment create for your family’s daily routine?” Mothers questioned the use of

230
the word “hassle” and found it too strong of a word. Most stated that they see their child’s
treatment as part of their responsibility as parents and not a hassle or bother. Some of the
mothers stated that they found completing the questionnaire helpful because it helped
them to reflect on their situation and gain insight.
The Feetham Family Functioning Scale (FFFS) was more problematic because
mothers without a spouse/partner left those items blank even though the instructions
regarding spouse/partner indicated that they were to answer the questions based on how
much they wanted the functions met. Most stated they did not care to complete those
items because they saw them as non-applicable. The Cronbach alpha was .86, however,
34 participants had missing data primarily on the spouse/partner questions. When this
scale was re-analyzed with spouse items removed, the alpha was .81 for 80 participants.
Additionally, since there was a fair amount of missing data on the FFFS, data was
imputed as discussed earlier in Chapter 4. Therefore, to assure statistical conclusion
validity, the hierarchical multiple regression analysis was re-run using only those
participants with no missing data. The results were the same; depressive symptoms were
the sole predictor of family functioning and the level of significance for the equation
remained the same. While the FFFS has good reliability and validity and has been used in
many previous studies of children with chronic conditions, it is problematic with mothers
who have no spouse/partner involvement due to missing data.
The Functional Status II-R had a Cronbach alpha of .76. Since this instrument was
administered by the investigator only two had missing data. These missing data were due
to errors in omitting questions that should have been asked in Part 2 of the instrument.
Mothers did not express any difficulty with completing this instrument. The first item on

231
the scale that queried mothers about their child’s eating was problematic however. This
item asked if their child ate well. Although almost 90% of the children had a feeding tube
many of the mothers answered that their children ate well most of the time. For
consistency sake, mothers were then asked to think about whether they ate well by
mouth, not if the tube feeding sessions went well.
Study Limitations
The study had methodological and sampling limitations. Generalizability of the
study is limited because of the convenience sample. While there was diversity in regards
to race/ethnicity, education, income, and marital status, the sample was primarily
comprised of married, Caucasian, Non-Hispanic mothers from suburban, Northeastern
Ohio with at least a partial college education who were recruited from a large tertiary
children’s hospital. Therefore, study results should be interpreted with caution for other
groups. Recruitment from a variety of sites such as a large county hospital in the area that
cares for a large population of children who receive public assistance would have added
to the diversity in terms of family income, inner city residence as well as race/ethnicity.
Since the sample was voluntary, it may be less representative of the general
population of mothers. However, most mothers who met inclusion criteria were invited to
participate therefore; this study had a good sampling of the population of mothers with
children who are technology dependent in the Northeast Ohio area. A vast majority of the
participants were eager to share their story and intrigued that someone would be
interested to hear about their life with a child who is technology dependent. Mothers who
declined to participate in the study primarily stated that they were too busy; overwhelmed
with all of their responsibilities caring for their families. These refusals occurred despite

232
the offer of flexible interview times and locations. These mothers would have added
greater understanding of this population because they may have had more challenges with
family functioning and normalization, particularly organization, thus they felt
overwhelmed.
Third, since the sample was cross-sectional it is difficult to assess the study
variables over time. The investigator is currently conducting a 12-month follow-up study
of participants to overcome this limitation.
Another limitation of the study was the amount of missing data on the Feetham
Family Functioning Survey. This limitation was mitigated by imputation of data using a
statistical calculation based on data available. Further analysis using only participants
with complete data on this instrument helped to validate use of this statistical technique;
there were no differences in statistical results or conclusions.
A fifth limitation is that only one subscale of the Normalization Scale, the “Actual
Effect of the Chronic Physical Disorder on the Family” (Murphy & Gottlieb, 1992), was
used in this study to measure normalization. Since this study was to include children ages
3 months to 16 years, many items on the other subscales were found to be not applicable.
This subscale however had the highest Cronbach alpha reliability (.84) and the highest
Eigenvalue (7.0) making it the most representative of the concept of normalization.
Additionally, since this instrument has only been used in one previous study by the
scale’s creator, results should be interpreted with caution. Missing data on one of the
items related to siblings was discussed above.

233
Study Implications
Clinical Implications
The results from this study increase nursing knowledge regarding the impact of
the child who is technology dependent on their families and provides evidence for
improved delivery of care for this population. Study findings indicate that mothers of
children who are technology dependent are at high risk for psychological distress that can
affect overall family functioning. Greater depressive symptoms and less use of
normalization were found to be significantly associated with poorer family functioning.
Findings from this study provide evidence that managing the demanding care regimens
and coordinating the many services typically required by these children while still
maintaining a “normal” family life is difficult for many families.
It is of paramount importance that the complex issues these families face be
addressed by a multidisciplinary team and an effective intervention employed to facilitate
family functioning thereby bolstering the child’s optimal growth and development. Past
research indicates that maintaining the mental health of caregivers and positive family
functioning affect the child’s growth and development (Miles et al., 1999). Findings from
this study revealed that 35% of the variance in family functioning was explained solely
by the level of depressive symptoms, underscoring the impact of such symptoms.
Therefore, an intervention that targets a mother’s psychological distress, a key concern in
this population, is vitally necessary.
Study findings support the need for all health care providers working with
families of children who are technology dependent to be vigilant to objectively assess the
level of depressive symptoms in the primary caregivers of these children. Noteworthy is

234
the fact that during the course of data collection the investigator had no indication of the
high level of depressive symptoms in some participants during the interview. Mothers
with a high level of depressive symptoms often would appear very “upbeat and together”
for the investigator as well as their child’s health care providers. The level of depressive
symptoms was only evident after the CES-D instrument had been scored and the findings
discussed with the mother. It could be proposed that mothers wanted to appear composed
so that there would be no question as to her ability to adequately care for her child.
Mothers indicated that the availability of and financial resources for mental health
support services are sorely lacking. Many stated that when they did find a mental health
provider the provider was overwhelmed by the magnitude of the situation the mother
presented and was of little assistance or guidance. Some indicated that they were unable
to continue attending mental health care sessions due to lack of financial resources to do
so. Furthermore, complicating a mother’s access to mental health care is the fact that she
often has limited time or respite care for her child to attend such sessions. Therefore, the
availability of and referral to mental health care providers who are familiar with the
complex situations these mothers face and who would provide flexibility as far as time
and location for mental health care sessions would greatly benefit this population by
enhancing family functioning and in the long term promote the child’s growth and
development.
When the access to mental health care is delayed or unavailable, all health care
providers can help to make a big difference for the mental health of mothers by simply
asking how things are going at home caring for a child who is technology dependent
while trying to maintain a “normal” family life. Many mothers indicated that no one else

235
had genuinely been interested in what the experience is like. Frequently mothers stated,
“they just don’t get it”-referring to the fact that it is difficult to explain the experience of
caring for a child who is technology dependent to family and friends or even health care
providers. Mothers would greatly benefit from the opportunity to have a discussion with
health care providers. The mothers invest substantial amounts of time and effort in the
care of their child that is often unrecognized by family, friends and at times even health
care providers. Simple words of encouragement to mothers from health care providers
such as “you are doing an amazing job caring for your child…” can be of great benefit as
was witnessed by the investigator.
Many indicated that while they were taught the techniques and procedures for
their child’s equipment, treatments and medical care prior to discharge from the hospital
no one discussed with them how to practically apply it and make it work at home in their
family situation. Basically they felt as if they were “left to figure it out on your own”.
Very few had a resource person to contact following discharge when questions arose.
While normalization efforts were not a significant predictor of family functioning,
perhaps in part due to the sample size, normalization was significantly correlated with
family functioning: better family functioning was associated with more normalization
efforts. Therefore, health care providers could assist families and perhaps help to enhance
family functioning by providing education regarding normalization efforts particularly
prior to a child’s discharge from the hospital to home. Normalization efforts includes the
development of management techniques such as organizational strategies; charts,
notebooks to help keep track of the child’s supplies, physicians, therapists, surgeries,
treatments, medications and appointments. Also, health care providers could educate

236
caregivers regarding how to deliver safe care and treatments to the child while
concomitantly providing information regarding flexibility that would allow them to live
as “normal” of a family life as possible. Additionally, health care providers could assist
with tips and techniques of how to transport the child and their equipment and supplies to
appointments, family outings and vacations. While more research needs to be done these
are some of the many management strategies that health care providers could teach
families that might help to bolster a family’s normalization efforts and in the long term
positively enhancing family functioning.
Theory Implications
Results from this study helped to support the models upon which it was based:
The Family Management Style Framework (Knafl &Deatrick, 2003) and Paterson’s
(2001) Shifting Perspectives of Chronic Illness Model. Findings suggest that a mother’s
depressive symptoms influence her perception of the illness or “definition of the illness”,
thereby affecting family functioning as suggested by Knafl and Deatrick (2003).
Additionally, these findings help to explain how families develop the “normalcy lens”
and what factors might hinder the process of normalization, primarily the child’s poor
functional status and the mother’s high level of depressive symptoms.
The findings support Paterson’s (2001) Shifting Perspectives Model of Chronic
Illness which suggests that a mother’s perception of reality will dictate how she interprets
her situation and consequently responds to the child’s condition. Thus, when a mother
has “wellness in the foreground”, the child is seen as “normal” despite the number of
technologies or treatments necessary. As Knafl and Deatrick (2003) suggest in their
description of normalization attributes, this is not a denial of the child’s condition or

237
distortion of reality, but instead a revision of what is “normal”. On the other hand, in the
case of children with poorer functional status, or who are experiencing an illness
exacerbation, mothers often had “illness in the foreground”, and therefore had decreased
normalization efforts.
Policy Implications
Findings from this study indicate the need for review of current policy regarding
families of children who are technology dependent. There is an urgent need to address
resources allocated to help families continue to care for their child who is technology
dependent at home. These resources include family mental health support systems that
need to be put in place prior to the child’s discharge home. As evidenced in this study, it
is a formidable task to care for these children, particularly when there are no supports
available that address mental health. The goal of such supports might be for family
members to have preventive mental health treatment available before discharge home. At
least it should be available by the home health care nurse or be assessed. Such preventive
support and/or treatment would help to potentially avoid mental health crises that would
negatively affect family functioning and the health of the child.
Another resource that policy change would need to address is establishment of a
qualified respite care system for families. Respite requires individuals who are
knowledgeable and capable of caring for the needs of these children. Almost half of the
families did not have any nursing care. For those who did receive nursing care, a number
indicated that some of the nurses assigned to them were not adequately prepared to care
for their child. These mothers often felt they could not leave their child with others
because they did not have adequate knowledge or training to be able to safely care for

238
their child and had experienced negative consequences as a result. Some mothers
indicated, even tearfully, that none of their family members were willing to watch their
child even for a few hours due to fear of the equipment or that they would not be able to
appropriately handle an emergency should one arise.
On a federal level, the government needs to comprehensively examine the current
state of funding for these children. Research into best practices that would
comprehensively care for these children and their families while being fiscally
responsible is of paramount importance. This is of particular interest at this point in
history due to the economic concerns of this country. Children who are technology
dependent while small in number are responsible for a large percentage of the health care
expenditures for children. Families are often willing to care for these children but need to
be given the resources to do so in the form of respite care, mental health support and
financial compensation for the caregiving parent who has often given up gainful
employment. Development of a comprehensive program will in the long term be fiscally
responsible and prudent approach as it will decrease duplication of services, provide
coordination of services and address health care needs promptly to decrease hospital
readmission rates.
At a state level, mechanisms need to be put into place to adequately assess
children who are technology dependent and in need of placement on a Medicaid waiver
program that would provide financial assistance to fund much needed respite care,
medications and equipment as well as transportation equipment. Some mothers have
suffered permanent back injuries due to lack of funds for lifts that would help with
transporting and moving their children.

239
At a local level, pediatric tertiary care centers would be able to serve this
population more effectively with a comprehensive, interdisciplinary team approach.
Members of the team include health care professionals from a variety of specialties as
well as home care agencies and durable medical equipment companies. Holistic care for
the child and family such as the hospice care model would be important to explore.
Important members of the team include the care coordinator that would act as a liaison
between the family and other members of the team and a mental health care professional
with experience dealing with the issues these families face on a daily basis.
Recommendations for Future Research
Findings from this study point to the need for further research regarding families
of children who are technology dependent. Future research of this population of children
and their families should include longitudinal, quantitative studies. Few quantitative
studies have been done of these children and their families particularly studies that have
longitudinally examined family functioning or how families try to provide as normal a
family life as possible for children who are technology dependent. Furthermore, little
information exists regarding the impact of a child’s technology dependence on their
siblings or family finances. A 12 month follow-up study of the participants from this
study is currently underway to help to address these gaps.
Although mothers were chosen as participants for this study, little has been done
to examine the perspective of fathers with children who are technology dependent. Some
of the spouse/partners of the study participants expressed interest in being able to provide
their views regarding the experience. Having the perspective of both parents would yield
helpful evidence regarding family functioning.

240
This study provides foundational evidence to develop and design interventions
that will address the needs of this population. While the sample did include diversity in
terms of race/ethnicity, purposive recruitment of minority families would greatly enhance
the generalizability of the findings. The study results indicate that mothers with a high
level of depressive symptoms are at risk for poorer family functioning and decreased
normalization efforts that consequently place the child as well as their typically
developing siblings at risk for deleterious effects on their growth and development.
Further descriptive, correlational studies need to be done to look at factors correlated with
increased depressive symptoms so that risk factors could be identified. Additionally,
interventions that will target the mother’s psychological distress, a key concern in this
population, are essential. Of paramount importance are mental health resource
interventions. The goal of such interventions is to help the mother to reframe her
situation; put life in perspective and celebrate the positive thereby fostering personal
growth.
Future research with larger sample sizes should investigate the relationship of
normalization and family functioning. Given the correlation of these variables,
interventions that may offer assistance with normalization efforts may ultimately assist
with family functioning. Such normalization strategies include teaching of organizational
skills such as helping to establish a routine and schedule for care and treatments,
assistance with prioritizing, time management, and flexibility. Other intervention
suggestions include on-line support groups in lieu of in-person support groups due to
time constraints and limited respite as well as a web site with resource information.

241
Future research should include development of a measurement tool for severity of
illness for children who are technology dependent. While the FSII-Revised instrument
did capture functional status it did not capture the variation of time required for care and
treatment, the number of care needs or the level of acuity for these children thus it did not
seem to capture the true severity of illness. Also, a tool other than the OTA (1987) rubric
that would capture the level of technology dependence would be helpful for future
quantitative studies.
Other recommendations for future research include a randomized, prospective
experimental study of families upon discharge from the hospital for the first time with
and without an intervention protocol that would include intense discharge teaching and
preparation as well as normalization promotion activities and support. Families in the
treatment group would be taught how to balance daily life with the technology to keep
the child stable and healthy while concomitantly maintaining effective and positive
family functioning and ensuring the child who is technology dependent has a childhood.
Finally, the holistic delivery of care that is an essential part of the hospice model
shows great promise for families of children who are technology dependent. This model
includes supports for the spiritual, instrumental and physical needs of patients and their
families. Future research should investigate an intervention using this model of care for
families with children who are technology dependent.
Conclusions
This descriptive, correlational study examined how 103 families respond to and
manage the special challenges of children who are technology dependent after they have

242
been discharged from the hospital to home. This is the first quantitative study to examine
both family functioning and normalization efforts of these families.
Findings from this study support past research; a large percentage of mothers of
children who are technology dependent have a significant amount of psychological
distress. A total of 40% of mothers who were participants in this study had a level of
depressive symptoms above the established cutoff point of 16 on the CES-D, indicating a
risk for clinical depression (Radloff, 1977). Furthermore, a total of 24% of mothers had
levels indicating a very high risk for clinical depression (Myers & Weissman, 1980)
(Table 4.8).
A critical new finding of this study is that a mother’s level of depressive
symptoms has a very significant affect on overall family functioning in this population.
Hierarchical Multiple Regression analysis revealed that a mother’s depressive symptoms
was the only significant predictor of family functioning while controlling for covariates
(length of caregiving duration, amount of home health care hours, race, family income
and age of the child who is technology dependent); greater number of depressive
symptoms was related to poorer family functioning.
Other significant findings from this study are related to normalization efforts,
level of technology dependence and depressive symptoms as a mediator variable. Several
independent variables/covariates were found to be significant predictors of greater
normalization efforts: better child’s functional status, less depressive symptoms, fewer
home health care nursing hours, an older child and Non-Caucasian race or Hispanic
ethnicity. This finding is important empirical evidence because it is the first time that
normalization has been quantitatively analyzed to determine correlates and predictors.

243
Results from the ANOVA analyses indicate there were no statistical differences in
normalization efforts, family functioning and mothers’ depressive symptoms based on the
child’s level of technology dependence (OTA, 1987 Group 1: mechanical ventilation,
Group 2: intravenous medications/nutritional substances, Group 3: respiratory or
nutritional support). These findings are consistent with the few quantitative studies that
have examined outcomes based on level of technology dependency (Fleming et al., 1994;
Leonard et al., 1993), however improved methodology to capture level of technology
dependence and severity of illness may help to assess for significant differences of these
groups in future studies.
Statistical analyses for mediation (Baron & Kenney, 1986) reveal that depressive
symptoms are a partial mediator between a child’s functional status and normalization.
Normalization was not found to be a mediator between a child’s functional status or a
mother’s depressive symptoms and family functioning. While normalization was
significantly correlated with family functioning it was not a significant predictor of
family functioning in multiple regression analysis.
This work provides important empirical evidence for the design of interventions
to assist families caring for this vulnerable and growing population of children at home. It
is of paramount importance that the complex issues these families face be addressed by a
multidisciplinary team and an effective intervention employed to facilitate family
functioning thereby bolstering the child’s optimal growth and development. The
implementation of an effective intervention that will target the level of psychological
distress experienced by these mothers is an important beginning step in this process.

244
APPENDICES
Appendix A Functional Status II (Revised)

245

246
Appendix B Level of Technology Dependency Questionnaire
Participant’s ID #____________ Child’s OTA Group Level:________
Types of Technology
0=No, 1= Yes
a Nasogastric tube feeding
b Gastrostomy tube feeding
c Intermittent intravenous infusion
d Continuous intravenous infusion
e Intravenous infusion of total parenteral nutrition
f Oxygen via nasal cannula
g Oxygen via tracheostomy collar
h
Oxygen via continuous positive airway pressure (CPAP)
i
Continuous positive airway pressure (CPAP) without oxygen
j Tracheostomy tube
k Mechanical ventilator
l Other

247
Appendix C Normalization Scale
Instructions: Please think about your child and your family over the last two months. For each question, you are asked to rate the frequency with which your child or family has believed something or done something by placing a slash (l) to cut the line somewhere between the two extremes labeled A LOT or A LITTLE- at the place that best corresponds to the answer that fits best for your child and family. For example, if you feel that the question describes your child/family a lot over the past two months, you should place the slash (l) at the A LOT end of the line. If you believe that the question sort of describes your child/family, you should place the slash (l) somewhere between the two extremes-closer to the A LITTLE end if it only partly describes your child/family and closer to the A LOT end if it pretty much describes your family. If the question hardly describes your child/family at all, you place your slash (l) at the A LITTLE end of the line.
Please remember-there are no right or wrong (nor good nor bad) answers. You know what best describes your situation.
1. If your child did not have this chronic condition, how different would your family be
compared to what it is like now?
a lot --------------------------------------------------------------------- a little
2. If your child did not have this chronic condition, how different would your child be
compared to what she/he is like now?
a lot --------------------------------------------------------------------- a little
3. How much of your family’s daily activities have to be planned around your child’s
needs?
a lot --------------------------------------------------------------------- a little
4. How much are your activities with your spouse/partner or other adults affected by your
child’s condition?
a lot --------------------------------------------------------------------- a little

248
5. How much of a hassle does your child’s medical treatment create for your family’s
daily routine?
a lot --------------------------------------------------------------------- a little
6. If you have more than one child: How much are your children’s activities affected by
your child’s condition?
a lot --------------------------------------------------------------------- a little
7. How much does your child’s condition affect your family life?
a lot --------------------------------------------------------------------- a little
8. How much do other people treat your family like they treat other families?
a lot --------------------------------------------------------------------- a little
9. How much does a child with a condition like your child’s need to be treated differently
because of the condition?
a lot --------------------------------------------------------------------- a little
10. How reluctant are other people to include your family in some activity because of
your child’s condition?
a lot --------------------------------------------------------------------- a little

249
Appendix D Center for Epidemiological Studies- Depression (CES-D)
ID#
Instructions for Questions: Below is a list of the ways you might have felt or behaved. Which of the following statements best describes how often you felt or behaved this way DURING THE PAST WEEK. 0. Rarely or None of the Time (Less than 1 Day) 1. Some or a Little of the Time (1 – 2 Days) 2. Occasionally or a Moderate Amount of Time (3 - 4 Days) 3. Most or All of the time (5 - 7 Days) DURING THE PAST WEEK……… SCORE
1. I was bothered by things that usually don’t bother me. 0 1 2 3
2. I did not feel like eating; my appetite was poor. 0 1 2 3
3. I felt that I could not shake off the blues even with help from my family or friends.
0 1 2 3
4. I felt that I was just as good as other people. 0 1 2 3
5. I had trouble keeping my mind on what I was doing. 0 1 2 3
6. I felt depressed. 0 1 2 3
7. I felt that everything I did was an effort. 0 1 2 3
8. I felt hopeful about the future. 0 1 2 3
9. I thought my life had been a failure. 0 1 2 3
10. I felt fearful. 0 1 2 3
11. My sleep was restless. 0 1 2 3
12. I was happy. 0 1 2 3
13. I talked less than usual. 0 1 2 3
14. I felt lonely. 0 1 2 3
15. People were unfriendly. 0 1 2 3
16. I enjoyed life. 0 1 2 3
17. I had crying spells. 0 1 2 3
18. I felt sad. 0 1 2 3
19. I felt that people dislike me. 0 1 2 3
20. I could not get “going”. 0 1 2 3

250
Appendix E Feetham Family Functioning Survey (FFFS)
In this survey you are asked to rate activities (functions) that occur in your family and with family members. For each family function you are asked to answer three questions: How much is there now? How much should there be? How important is this to you? Please answer all three questions for each family function by circling the number with represents how your feel now about the family function. The term spouse refers to your husband or wife or the person who assumes the functions of a spouse/partner. If you do not have a person in the spouse/partner role, answer the questions based on how much you want the functions met. Please try to answer all items. Please mark you answer by circling the number Little Much
1. The amount of discussion with your friends regarding your concerns and problems.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
2. The amount of discussion with your relatives regarding your concerns and problems (do not include your spouse/partner).
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
3. The amount of time you spend with your spouse/partner.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
4. The amount of discussion of your concerns and problems with your spouse/partner.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
5. The amount of time you spend with your neighbors.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
6. The amount of time you spend in

251
leisure/recreational activities. a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
7. The amount of help from your spouse/partner with family tasks such as care of children, house repairs, household chores, etc.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
8. The amount of help from relatives with family tasks such as care of children, house repairs, household chores, etc.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
9. The amount of time with health professionals (doctors, nurses, social workers, etc.)
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
10. The amount of help from your friends with family tasks such as care of children, house repairs, household chores, etc.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
If you do not have a child(ren) please indicate here and skip questions 11, 12 and 13.
Children Yes No
11. The number of problems with your child(ren).
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
12. The amount of time you spend with your child(ren).
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
Do you have a child(ren) in school?
Child in school
Yes No If No, please skip question # 13
13. The amount of time your child(ren) miss

252
school. a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
14. The number of disagreements with your spouse/partner.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
15. The amount of time you are ill. a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
16. The amount of time you spend doing housework (cooking, cleaning, washing, yard work, etc.).
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
17. The amount of time you miss work (including housework).
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
18. The amount of time your spouse/partner misses work (including housework).
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
19. The amount of emotional support from friends.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
20. The amount of emotional support from relatives.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
21. The amount of emotional support from your spouse/partner.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
22. The amount of time your work routine is

253
disrupted (including housework). a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
23. The amount of time your spouse’s/partner’s work routine is disrupted (including housework).
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
24. The amount of satisfaction with your marriage (relationship with spouse/partner).
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
25. The amount of satisfaction with the sexual relations with your spouse/partner.
a. How much is there now? b. How much should there be? c. How important is this to you?
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
26. What is most helpful to you now?
27. What is least helpful to you now?

254
Appendix F Demographic Questionnaire
1. Age of child (in months)_____: Date of Birth _______; Today’s Date_______
2. Gender of child:
1=Male
2=Female
3. Mother’s age:______
4. Mother’s relationship to the child:
1=biological mother 4=step mother
2=adoptive mother 5=grandmother
3=foster mother
5. Marital status:
1=single, never married 4=separated
2=single, living with partner 5=widowed
3=married 6=divorced
6. Education:
1=less than 7th grade 7=associate’s college degree
2=completed 8th grade 8=baccalaureate degree
3=partial high school 9=partial graduate school
4=high school graduate 10=master’s degree
5=technical/vocational program graduate 11=doctoral degree
6=partial college 12=other

255
7. Race/ethnicity:
1=Latino or Hispanic 4=Asian
2=African-American 5=Native American
3=White, Non-Hispanic 6=Bi-racial
8. Total number living in household:
Number of adults_____
Number of children_____
9. Mother’s employment status:
0=not employed outside the home
1=employed outside the home
10. Number of hours employed per week:______
11. Yearly family income:
0=equal or less than $20,000
1=$20,000-40,000
2=$40,001-60,000
3=$60,001-80,000
4=>$80,001
12. Duration of caregiving (in months)_______:
Date began caregiving_________
Today’s date____________
13. Number of home health care nursing hours:
Number of RN hours__________
Number of LPN hours_________

256
14. Current Address with Zip Code:
________________________________________________ ________________________________________________
15. Current Phone Number:
(Home)___________________ (Cell)__________________ 16. Name, Address, Phone Number of Two Family Members/Friends who will know your whereabouts should you move. You may be contacted about a long term study in the future about how you and your child are doing and what changes have occurred. a. ______________________________________________ ________________________________________________ ________________________________________________ ________________________________________________
b. ______________________________________________ ________________________________________________ ________________________________________________ ________________________________________________

257
Appendix G Introductory Letter
July 1, 2008 Hello! My name is Valerie Toly and I am a doctoral student at the Frances Payne Bolton School of Nursing, Case Western Reserve University. I have had over 20 years experience as a pediatric nurse. Because you are a female caregiver for a child who has special technology needs you have been identified as a potential participant for a research study. The study has been approved by University Hospitals of Cleveland/Rainbow Babies & Children’s Hospital Institutional Review Board. This research study looks at how families manage the care of their child with special technology needs after he/she is discharged from the hospital. I would like to know if you would be willing to answer some questions regarding your experiences of caring for your child with special technology needs. You will be compensated for your time and inconvenience. I can arrange to meet you when you come for your child’s next clinic visit. Participation in this research study is voluntary. Your care would not be affected in any way by your decision regarding participation in this study. The goal of this study is to explore what helps families to best manage the care of their child with special technology needs after they are discharged from the hospital to home. This is also your chance to discuss your thoughts and feelings related to caring for your child. You may contact me at to hear more about the study and to arrange an interview time. I know that you are very busy caring for your child so if I do not hear from you I’ll try giving you a call in about 2 weeks. Thank you for your kind consideration. I look forward to hearing from you soon! Sincerely, Valerie Toly, PhD(c), RN, CPNP Instructor of Nursing

258
Appendix H Telephone Script for Recruitment
Families with Children who are Technology Dependent Valerie Boebel Toly, PhD(c), RN, CPNP
PhD Student at the FPB School of Nursing, CWRU
My name is Valerie Toly and I am a doctoral student at the Frances Payne Bolton School of Nursing, Case Western Reserve University. I sent you a letter a couple of weeks ago that described a research study. This research study looks at how families manage the care of their child with special technology needs after he/she is discharged from the hospital. I would like to know if you would be willing to answer some questions regarding your experiences of caring for your child with special technology needs. I can arrange to meet you when you come for your child’s next clinic visit. Participation in this research study is voluntary and I can go over more details about the study when we meet. Your care would not be affected in any way by your decision regarding participation in this study.

259
Appendix I Resources for Mental Health
Resources for Mental Health Care
This information is provided for participants of the research study regarding families of children with special technology needs. Symptoms of psychological distress should be discussed with your primary care physician. Other resources in the Greater Cleveland area that can provide immediate assistance include: Cuyahoga County 24-Hour Mental Health Crisis Information and Referral Hotline Phone: (216) 623-6888 United Way Services of Greater Cleveland First Call for Help Phone: 211 or (216) 436-2000

260
Appendix J
Consent Form

261

262

263
Appendix K HIPPA Release Form

264

265
REFERENCES
Affleck, G., Tennen, H., Pfeiffer, C., Fifield, J., & Rowe, J. (1987). Downward
comparison and coping with serious medical problems. American Journal of Orthopsychiatry, 57(4), 570-578.
Affleck, G., Tennen, H., Rowe, J., & Higgins, P. (1990). Mothers remembrances of
newborn intensive care: A predictive study. Journal of Pediatric Psychology, 15, 67-81.
Alexander, E., Rennick, J. E., Carnevale, F., & Davis, M. (2002). Daily struggles: Living
with long-term childhood technology dependence. Canadian Journal of Nursing Research, 34(4), 7-14.
Allen, N. L., Simone, J. A., & Wingenbach, G. F. (1994). Families with a ventilator-
assisted child: Transitional issues. Journal of Perinatology, 14(1), 48-55. Baron, R., & Kenny, D. (1986). The moderator-mediator variable distinction in social
psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173-1182.
Baumann, S. L. (2000). Family nursing: Theory-anemic, nursing theory-deprived.
Nursing Science Quarterly, 13(4), 285-290. Bennett, J. (2000). Mediator and moderator variables in nursing research: Conceptual and
statistical differences. Research in Nursing and Health, 23, 415-420. Biegel, D., Sales, E., & Schulz, R. (1991). Family caregiving in chronic illness. Newbury
Park, CA: Sage Publications. Boland, D. L., & Sims, S. L. (1996). Family care giving at home as a solitary journey.
Image Journal of Nursing Scholarship, 28(1), 55-58. Bronfenbrenner, U. (1993). The ecology of cognitve development: Research models and
fugitive findings. In R. H. Wozniak & K. W. Fischer (Eds.), Development in context: Acting and thinking in specific environments (pp. 3-44). Hillsdale, NJ: Lawrence Erlbaum Associates, Publishers.
Buescher, P., Whitmire, J. T., Brunssen, S., & Kluttz-Hile, C. (2006). Children who are
medically fragile in North Carolina: Using Medicaid data to estimate prevalence and medial care costs in 2004. Maternal Child Health Journal, 10, 461-466.
Bull, M. (1992). Managing the transition from hospital to home. Qualitative Health
Research, 2(1), 27-41.

266
Burke, S., Harrison, M., Kauffman, E., & Wong, C. (2001). Effects of stress-point intervention with families of repeatedly hospitalized children. Journal of Family Nursing, 7, 128-158.
Burns, N., & Grove, S. (1997). The practice of nursing research: Conduct, critique, and
utilization (3rd Edition). Philadelphia, PA: W. B. Saunders Company. Canning, R. D., Harris, E. S., & Kelleher, K. J. (1996). Factors predicting distress among
caregivers to children with chronic medical conditions. Journal of Pediatric Psychology, 21(5), 735-749.
Carnevale, F. A., Alexander, E., Davis, M., Rennick, J., & Troini, R. (2006). Daily living
with distress and enrichment: The moral experience of families with ventilator-assisted children at home. Pediatrics, 117(1), e48-60.
Case-Smith, J. (2004). Parenting a child with a chronic medical condition. American
Journal of Occupational Therapy, 58(5), 551-560. Cavanagh, E. (1999). Maintaining a childhood: A phenomenological study of family
experiences providing home care for chronically ill, technology-dependent children., Unpublished doctoral dissertation, University of Washington.
Chernoff, R. G., List, D. G., DeVet, K. A., & Ireys, H. T. (2001). Maternal reports of
raising children with chronic illnesses: The prevalence of positive thinking. Ambulatory Pediatrics, 1(2), 104-107.
Chisholm, J. (2000). The context, content and consequences of mothering a child with
disabilities. Axone, 22(2), 22-28. Clark, D., Beck, A., & Alford, B. (1999). Scientific foundations of cognitive theory and
therapy of depression. New York: John Wiley & Sons, Inc. Clarke-Steffen, L. (1997). Reconstructing reality: Family strategies for managing
childhood cancer. Journal of Pediatric Nursing, 12(5), 278-287. Clawson, J. A. (1996). A child with chronic illness and the process of family adaptation.
Journal of Pediatric Nursing, 11(1), 52-61. Clements, D. B., Copeland, L. G., & Loftus, M. (1990). Critical times for families with a
chronically ill child. Pediatric Nursing, 16(2), 157-161, 224. Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ: L.
Erlbaum & Associates. Cohen, J. (1992). A power primer. Psychological Bulletin, 112, 155-159.

267
Cohen, M. H. (1993). The unknown and the unknowable--managing sustained uncertainty. Western Journal of Nursing Research, 15(1), 77-96.
Cohen, M. H. (1999). The technology-dependent child and the socially marginalized
family: A provisional framework. Qualitative Health Research, 9(5), 654-668. Dadds, M. R., Stein, R. E., & Silver, E. J. (1995). The role of maternal psychological
adjustment in the measurement of children's functional status. Journal of Pediatric Psychology, 20(4), 527-544.
Dashiff, C. J. (1993). Parents' perceptions of diabetes in adolescent daughters and its
impact on the family. Journal of Pediatric Nursing, 8(6), 361-369. Deatrick, J. A., & Knafl, K. A. (1990). Management behaviors: Day-to-day adjustments
to childhood chronic conditions. Journal of Pediatric Nursing, 5(1), 15-22. Deatrick, J. A., Knafl, K. A., & Murphy-Moore, C. (1999). Clarifying the concept of
normalization. Image Journal of Nursing Scholarship, 31(3), 209-214. Deatrick, J., Knafl, K., & Walsh, M. (1988). The process of parenting a child with a
disability: Normalization through accommodations. Journal of Advanced Nursing, 13, 15-21.
Deatrick, J. A., Thibodeaux, A. G., Mooney, K., Schmus, C., Pollack, R., & Davey, B. H.
(2006). Family management style framework: A new tool with potential to assess families who have children with brain tumors. Journal of Pediatric Oncology Nursing, 23(1), 19-27.
Dickstein, S. (2002). Family routines and rituals--the importance of family functioning:
Comment on the special section. Journal of Family Psychology, 16(4), 441-444. Dodgson, J., Garwick, A., Blozis, S., Patterson, J., Bennett, F., & Blum, R. (2000).
Uncertainty in childhood chronic conditions and family distress in families of young children. Journal of Family Nursing, 6, 252-266.
Donnelly, E. (1994). Parents of children with asthma: An examination of family
hardiness, family stressors, and family functioning. Journal of Pediatric Nursing, 9(6), 398-408.
Drotar, D. (1997). Relating parent and family functioning to the psychological adjustment
of children with chronic health conditions: What have we learned? What do we need to know? Journal of Pediatric Psychology, 22(2), 149-165.
Drotar, D., Agle, D. P., Eckl, C. L., & Thompson, P. A. (1997). Correlates of
psychological distress among mothers of children and adolescents with hemophilia and hiv infection. Journal of Pediatric Psychology, 22(1), 1-14.

268
Elfert, H., Anderson, J., Lai, M. (1991). Parents’ perceptions of children with chronic illness: A study of immigrant Chinese families. Journal of Pediatric Nursing, 6, 114-120.
Farmer, J. E., Marien, W. E., Clark, M. J., Sherman, A., & Selva, T. J. (2004). Primary
care supports for children with chronic health conditions: Identifying and predicting unmet family needs. Journal of Pediatric Psychology, 29(5), 355-367.
Fields, A. (2005). Discovering statistics using SPSS. London: Sage. Fleming, J., Challela, M., Eland, J., Hornick, R., Johnson, P., Martinson, I., Dativio, D.,
Nokes, K., Riddle, I., Steele, N. et al. (1994). Impact on the family of children who are technology dependent and cared for in the home. Pediatric Nursing, 20(4), 379-388.
Foreman, M. (1997). Measuring cognitive status. In S. Olsen & M. Frank-Stromborg
(Ed.), Instruments for clinical health-care research. (2nd Edition ). Boston: Jones and Bartlett Publishers.
Fox, J. (1991). Regression diagnostic series: Quantitative applications in social sciences,
number 79. Newbury Park, CA: Sage. Frankel, K., & Wamboldt, M. Z. (1998). Chronic childhood illness and maternal mental
health--why should we care? The Journal of Asthma, 35(8), 621-630. Gallo, A. M., & Knafl, K. A. (1998). Parents' reports of "tricks of the trade" for managing
childhood chronic illness. Journal of the Society of Pediatric Nurses, 3(3), 93-100.
Gennaro, S., Brooten, D., Roncoli, M., & Kumar, S. (1993). Stress and health outcomes
among mothers of low-birth-weight infants. Western Journal of Nursing Research, 15, 97-113.
Glendinning, C., & Kirk, S. (2000). High-tech care: High-skilled parents. Paediatric
Nursing, 12(6), 25-27. Glendinning, C., Kirk, S., Guiffrida, A., & Lawton, D. (2001). Technology-dependent
children in the community: Definitions, numbers and costs. Child: Care, Health and Development, 27(4), 321-334.
Goldenberg, I., & Goldenberg, H. (1991). Family therapy: An overview (3rd Ed.). Pacific
Grove, CA: Brooks/Cole Publishing Company. Gonzalez, E. (1997). Resourcefulness, appraisals, and coping efforts of family caregivers.
Issues in Mental Health Nursing, 18, 209-227.

269
Gravelle, A. M. (1997). Caring for a child with a progressive illness during the complex chronic phase: Parents' experience of facing adversity. Journal of Advanced Nursing, 25(4), 738-745.
Grey, M., Knafl, K., & McCorkle, R. (2006). A framework for the study of self- and
family management of chronic conditions. Nursing Outlook, 54, 278-286. Guyer, B., MacDorman, M. F., Martin, J. A., Peters, K. D., & Strobino, D. M. (1998).
Annual summary of vital statistics-1997. Pediatrics, 102(6), 1333-1349. Haase, J. E., & Rostad, M. (1994). Experiences of completing cancer therapy: Children's
perspectives. Oncology Nursing Forum, 21(9), 1483-1492; discussion 1493-1484. Hatton, D. L., Canam, C., Thorne, S., & Hughes, A. M. (1995). Parents' perceptions of
caring for an infant or toddler with diabetes. Journal of Advanced Nursing, 22(3), 569-577.
Heaton, J., Noyes, J., Sloper, P., & Shah, R. (2005). Families' experiences of caring for
technology-dependent children: A temporal perspective. Health and Social Care in the Community, 13(5), 441-450.
Heyman, M. B., Harmatz, P., Acree, M., Wilson, L., Moskowitz, J. T., Ferrando, S., et al.
(2004). Economic and psychologic costs for maternal caregivers of gastrostomy-dependent children. Journal of Pediatrics, 145(4), 511-516.
Hock-Long, L. (1997). Pediatric home ventilator care: Family caregiver perspective.
Unpublished doctoral dissertation, University of Pennsylvania, Philadelphia. Houtrow, A., Kim, S., & Newacheck, P. (2008). Health care utilization, access, and
expenditures for infants and young children with special health care needs. Infants and Young Children, 21, 149-159.
Ireys, H. T., & Silver, E. J. (1996). Perception of the impact of a child's chronic illness:
Does it predict maternal mental health? Journal of Developmental and Behavioral Pediatrics, 17(2), 77-83.
Jackson Allen, P. (2004). The primary care provider and children with chronic
conditions. In P. Jackson Allen and J. A. Vessey (Ed.), Primary care of the child with a chronic condition (4th Edition, pp. 3-19). St. Louis, MO: Mosby.
Jerrett, M. D. (1994). Parents' experience of coming to know the care of a chronically ill
child. Journal of Advanced Nursing, 19(6), 1050-1056. Joachim, G., & Acorn, S. (2000). Living with chronic illness: The interface of stigma and
normalization. Canadian Journal of Nursing Research, 32(3), 37-48.

270
Johnson, B. S. (2000). Mothers' perceptions of parenting children with disabilities. MCN American Journal of Maternal Child Nursing, 25(3), 127-132.
Judson, L. (2004). Protective care: Mothering a child dependent on parenteral nutrition.
Journal of Family Nursing, 10, 93-120. Katz, S. & Krulik, T. (1999). Fathers of children with chronic illness: Do they differ from
fathers of healthy children? Journal of Family Nursing, 5, 292-315. Kiernan, B. S. (1995). Parents' perceptions of family functioning and parental coping in
families of chronically ill child dependent upon home intravenous therapy. Unpublished doctoral dissertation, University of Kentucky.
Kirk, S. (1998). Families' experiences of caring at home for a technology-dependent
child: A review of the literature. Child: Care, Health and Development, 24(2), 101-114.
Kirk, S. (2008). A profile of technology-assisted children and young people in north west
England. Paediatric Nursing, 20 (9), 18-20. Kirk, S., & Glendinning, C. (2004). Developing services to support parents caring for a
technology-dependent child at home. Child: Care, Health and Development, 30(3), 209-218; discussion 219.
Kirk, S., Glendinning, C., & Callery, P. (2005). Parent or nurse? The experience of being
the parent of a technology-dependent child. Journal of Advanced Nursing, 51(5), 456-464.
Knafl, K., & Zoeller, L. (2000). Childhood chronic illness: A comparison of mothers' and
fathers' experiences. Journal of Family Nursing, 6(3), 287-302. Knafl, K., Breitmayer, B., Gallo, A., & Zoeller, L. (1996). Family response to childhood
chronic illness: Description of management styles. Journal of Pediatric Nursing, 11(5), 315-326.
Knafl, K. A., & Deatrick, J. A. (1986). How families manage chronic conditions: An
analysis of the concept of normalization. Research in Nursing and Health, 9(3), 215-222.
Knafl, K. A., & Deatrick, J. A. (1990). Family management style: Concept analysis and
development. Journal of Pediatric Nursing, 5(1), 4-14. Knafl, K. A., & Deatrick, J. A. (2006). Family management style and the challenge of
moving from conceptualization to measurement. Journal of Pediatric Oncology Nursing, 23(1), 12-18.

271
Knafl, K., & Deatrick, J. (2003). Further refinement of the family management style framework. Journal of Family Nursing, 9, 232-256.
Knafl, K., & Deatrick, J. (2002a). The challenge of normalization for families of children
with chronic conditions. Pediatric Nursing, 28(1), 49-53, 56. Knafl, K., & Gilliss, C. (2002b). Families and chronic illness: A synthesis of current
research. Journal of Family Nursing, 8, 178-198. Kohlen, C., Beier, J., & Danzer, G. (2000). "they don't leave you on your own:" a
qualitative study of the home care of chronically ill children. Pediatric Nursing, 26(4), 364-371.
Kuster, P. A. (2002). Health outcomes of mothers caring for ventilator-assisted children
at home: The influence of social support, coping and community resources. Unpublished doctoral dissertation, UCLA, Los Angeles, CA.
Kuster, P. A., Badr, L. K., Chang, B. L., Wuerker, A. K., & Benjamin, A. E. (2004).
Factors influencing health promoting activities of mothers caring for ventilator-assisted children. Journal of Pediatric Nursing, 19(4), 276-287.
Lasky, P., Buckwalter, K., Whall, A., Lederman, R., Speer, J., McLane, A., King, J., &
White, M. (1985). Development of a research group: Developing an instrument for the assessment of family dynamics. Western Journal of Nursing Research, 7, 40-52.
Lee, D. A. (1996). Motherhood as usual: Two studies of african american women with
technology dependent infants. Unpublished doctoral dissertation, University of North Carolina at Chapel Hill.
Leonard, B. J., Brust, J. D., & Nelson, R. P. (1993). Parental distress: Caring for
medically fragile children at home. Journal of Pediatric Nursing, 8(1), 22-30. Lustig, J. L., Ireys, H. T., Sills, E. M., & Walsh, B. B. (1996). Mental health of mothers
of children with juvenile rheumatoid arthritis: Appraisal as a mediator. Journal of Pediatric Psychology, 21(5), 719-733.
Madigan, E. A., Youngblut, J., & Haruzivishe, C. (1999). Pediatric home healthcare:
Patients and providers. Home Healthcare Nurse, 17(11), 699-705. May, K. M. (1997). Searching for normalcy: Mothers' caregiving for low birth weight
infants. Pediatric Nursing, 23(1), 17-20. McCain, G. C. (1990). Family functioning 2 to 4 years after preterm birth. Journal of
Pediatric Nursing, 5(2), 97-104.

272
Mertler, C. & Vannata, R. (2005). Advanced and multivariate statistical methods: Practical application and interpretation (3rd Edition). Glendale, CA: Pyrczak Publishing.
Miles, M. S., Holditch-Davis, D., Burchinal, P., & Nelson, D. (1999). Distress and
growth outcomes in mothers of medically fragile infants. Nursing Research, 48(3), 129-140.
Miller, V. L., Rice, J. C., DeVoe, M., & Fos, P. J. (1998). An analysis of program and
family costs of case managed care for technology-dependent infants with bronchopulmonary dysplasia. Journal of Pediatric Nursing, 13(4), 244-251.
Mitchell, W., & Sloper, P. (2002). Information that informs rather than alienates families
with disabled children: Developing a model of good practice. Health and Social Care in the Community, 10(2), 74-81.
Morse, J. M., Wilson, S., & Penrod, J. (2000). Mothers and their disabled children:
Refining the concept of normalization. Health Care for Women International, 21(8), 659-676.
Murphy, F. (1994). Relationship between family use of normalization and psychosocial
adjustment in children with chronic physical disorders. Unpublished master’s thesis, McGill University, Montreal, Quebec, Canada.
Murphy, F. & Gottlieb, L. (1992). Normalization scale. Unpublished instrument. Murphy, K. E. (1997). Parenting a technology assisted infant: Coping with occupational
stress. Social Work in Health Care, 24(3-4), 113-126. Myers, J., & Weissman, M. (1980). Use of a self-report sympom scale to detect
depression in a community sample. American Journal of Psychiatry, 137, 1081-1083.
Neabel, B., Fothergill-Bourbonnais, F., & Dunning, J. (2000). Family assessment tools: A
review of the literature from 1978-1997. Heart & Lung, 29, 196-209. Neuss, J. (2004). Mothers as primary caregivers for their technology dependent child at
home: A qualitative study. Unpublished doctoral dissertation, New York University, New York, NY.
Newacheck, P. W., & Halfon, N. (1998). Prevalence and impact of disabling chronic
conditions in childhood. American Journal of Public Health, 88(4), 610-617. Newacheck, P. W., & Kim, S. E. (2005). A national profile of health care utilization and
expenditures for children with special health care needs. Archives in Pediatric & Adolescent Medicine, 159(1), 10-17.

273
Nickel, J. (2004). Personal communication regarding statistics on Ohio children who are
technology dependent. December 2, 2004, Cleveland, OH. O'Brien, M. E. (2001). Living in a house of cards: Family experiences with long-term
childhood technology dependence. Journal of Pediatric Nursing, 16(1), 13-22. O'Brien, M. E., & Wegner, C. B. (2002). Rearing the child who is technology dependent:
Perceptions of parents and home care nurses. Journal for Specialists in Pediatric Nursing, 7(1), 7-15.
Office of Technology Assessment. (1987). Technology-dependent children: Hospital care
vs. home care: A technical memorandum: Congress of the United States. Ostwald, S. K., Leonard, B., Choi, T., Keenan, J., Hepburn, K., & Aroskar, M. A. (1993).
Caregivers of frail elderly and medically fragile children: Perceptions of ability to continue to provide home health care. Home Health Care Service Quarterly, 14(1), 55-80.
Paquette, D., & Ryan, J. (2001, 7/12/2001). Bronfenbrenner's ecological systems theory.
Retrieved October, 2006 from URL: http://pt3.nl.edu/paquetteryanwebquest.pdf. Paterson, B. (2001). The shifting perspectives model of chronic illness. Journal of
Nursing Scholarship, 33, 21-26. Patterson, J. M., Leonard, B. J., & Titus, J. C. (1992). Home care for medically fragile
children: Impact on family health and well-being. Journal of Developmental and Behavioral Pediatrics, 13(4), 248-255.
Pelletier, L., Godin, G., Lepage, L., & Dussault, G. (1994). Social support received by
mothers of chronically ill children. Child: Care, Health and Development, 20(2), 115-131.
Radloff, L. S. (1977). The ces-d scale: A self-report depression scale for research in the
general population. Applied Psychological Measurement, 1, 385-401. Rehm, R. S., & Bradley, J. F. (2005). Normalization in families raising a child who is
medically fragile/technology dependent and developmentally delayed. Qualitative Health Research, 15(6), 807-820.
Rehm, R. S., & Franck, L. S. (2000). Long-term goals and normalization strategies of
children and families affected by hiv/aids. Advances in Nurs Science, 23(1), 69-82.
Roberts, C. S., & Feetham, S. L. (1982). Assessing family functioning across three areas
of relationships. Nursing Research, 31(4), 231-235.

274
Robinson, C. A. (1993). Managing life with a chronic condition: The story of
normalization. Qualitative Health Research, 3(1), 6-28. Sales, E., Greeno, C., Shear, M. K., & Anderson, C. (2004). Maternal caregiving strain as
a mediator in the relationship between child and mother mental health problems. Social Work Research, 28(4), 211-223.
Sandelowski, M. (1993). Toward a theory of technology dependency. Nursing Outlook,
41(1), 36-42. Santacroce, S. J., Deatrick, J. A., & Ledlie, S. W. (2002). Redefining treatment: How
biological mothers manage their children's treatment for perinatally acquired hiv. AIDS Care, 14(2), 247-260.
Scharer, K., & Dixon, D. M. (1989). Managing chronic illness: Parents with a ventilator--
dependent child. Journal of Pediatric Nursing, 4(4), 236-247. Shore, C. P., Austin, J. K., Huster, G. A., & Dunn, D. W. (2002). Identifying risk factors
for maternal depression in families of adolescents with epilepsy. Journal for Specialists in Pediatric Nursing, 7(2), 71-80.
Silver, E. J., Bauman, L. J., & Ireys, H. T. (1995). Relationships of self-esteem and
efficacy to psychological distress in mothers of children with chronic physical illnesses. Health Psychology, 14(4), 333-340.
Silver, E. J., Bauman, L. J., & Weiss, E. S. (1999). Perceived role restriction and
depressive symptoms in mothers of children with chronic health conditions. Journal of Developmental and Behavioral Pediatrics, 20(5), 362-369.
Silver, E. J., Westbrook, L. E., & Stein, R. E. (1998). Relationship of parental
psychological distress to consequences of chronic health conditions in children. Journal of Pediatric Psychology, 23(1), 5-15.
Smith, C. E. (1999). Caregiving effectiveness in families managing complex technology
at home: Replication of a model. Nursing Research, 48(120-128). Stanton, B. R. (1999). Does family functioning affect outcome in children with
neurological disorders? Pediatric Rehabilitation, 3(4), 193-199. Stein, R. E. (1992). Chronic physical disorders. Pediatrics in Review, 13(6), 224-229. Stein, R. E., Gortmaker, S. L., Perrin, E. C., Perrin, J. M., Pless, I. B., Walker, D. K., et
al. (1987). Severity of illness: Concepts and measurements. Lancet, 2(8574), 1506-1509.

275
Stein, R. E., & Jessop, D. J. (1990). Functional status ii(r). A measure of child health status. Medical Care, 28(11), 1041-1055.
Stephenson, C. (1999). Well-being of families with healthy and technology-assisted
infants in the home: A comparative study. Journal of Pediatric Nursing, 14(3), 164-176.
Sullivan-Bolyai, S., Knafl, K., Sadler, L., & Gilliss, C. (2004). Great expectations: A
position description for parents of caregivers: Part II. Pediatric Nursing, 30, 52-56.
Tabachnick, B. G. & Fidell, L. S. (2001). Using multivariate statistics (4th Edition).
Boston: Allyn & Bacon. Teague, B. R., Fleming, J. W., Castle, A., Kiernan, B. S., Lobo, M. L., Riggs, S., et al.
(1993). "high-tech" home care for children with chronic health conditions: A pilot study. Journal of Pediatric Nursing, 8(4), 226-232.
Thompson, R., Oehler, J., Catlett, A., & Johndrow, D. (1993). Maternal psychological
adjustment to the birth of an infant weighing 1,500 grms or less. Infant Behavior and Development, 16, 471-485.
Thorne, S., Paterson, B., Acorn, S., Canam, C., Joachim, G., & Jillings, C. (2002).
Chronic illness experience: Insights from a metastudy. Qualitative Health Research, 12(4), 437-452.
Thorne, S. E., & Paterson, B. L. (2000). Two decades of insider research: What we know
and don't know about chronic illness experience. Annual Review of Nursing Research, 18, 3-25.
Thorne, S. E., Radford, M. J., & McCormick, J. (1997). The multiple meanings of long-
term gastrostomy in children with severe disability. Journal of Pediatric Nursing, 12(2), 89-99.
Thyen, U., Kuhlthau, K., & Perrin, J. M. (1999). Employment, child care, and mental
health of mothers caring for children assisted by technology. Pediatrics, 103(6 Pt 1), 1235-1242.
Thyen, U., Terres, N. M., Yazdgerdi, S. R., & Perrin, J. M. (1998). Impact of long-term
care of children assisted by technology on maternal health. Journal of Developmental and Behavioral Pediatrics, 19(4), 273-282.
Toly, V. (2003). A concept analysis of family functioning. Unpublished manuscript, Case
Western Reserve University.

276
Tommet, P. A. (2003). Nurse-parent dialogue: Illuminating the evolving pattern of families with children who are medically fragile. Nursing Science Quarterly, 16(3), 239-246.
Torok, L. S. (2001). The lived experience of receiving and caring for a technology
dependent infant in the home. Unpublished doctoral dissertation, University of Cincinnati, Cincinnati, OH.
Von Bertlannffy, L. (1968). General systems theory: Foundation, development,
applications. New York: Braziller. Wallander, J. L., Varni, J. W., Babani, L., Banis, H. T., & Wilcox, K. T. (1989). Family
resources as resistance factors for psychological maladjustment in chronically ill and handicapped children. Journal of Pediatric Psychology, 14(2), 157-173.
Wang, K. W., & Barnard, A. (2004). Technology-dependent children and their families:
A review. Journal of Advanced Nursing, 45(1), 36-46. Weiss, S. J., & Chen, J. L. (2002). Factors influencing maternal mental health and family
functioning during the low birthweight infant's first year of life. Journal of Pediatric Nursing, 17(2), 114-125.
Wilson, S., Morse, J. M., & Penrod, J. (1998). Absolute involvement: The experience of
mothers of ventilator-dependent children. Health and Social Care in the Community, 6(4), 224-233.
Wright, L. & Leahey, M. (1994). Nurses and families: A guide to family assessment and
intervention (2nd ed.). Philadelphia: F. A. Davis. Young, J. B. (1995). Black families with a chronically disabled family member: A
framework for study. Association of Black Nurses Faculty Journal, 6(3), 68-73. Youngblut, J. M., Brennan, P. F., & Swegart, L. A. (1994). Families with medically
fragile children: An exploratory study. Pediatric Nursing, 20(5), 463-468. Zauszniewski, J., & Wykle, M. (1994). Racial differences in self-assessed health
problems, depressive cognitions, and learned resourcefulness. Journal of the National Black Nurses Association, 7, 3-14.