
Normal investigations ist
74
Are You Normal or if not Are You Very Unusual? Asymptomatic Scan Results, Pain Sources and Case Studies of Lumbar Spine, Cervical Spine, Shoulders and Knees Sean Dadswell 2015
-
Upload
sean-dadswell -
Category
Health & Medicine
-
view
70 -
download
0
Transcript of Normal investigations ist

Are You Normal or if not
Are You Very Unusual?
Asymptomatic Scan Results, Pain Sources and Case Studies of Lumbar Spine, Cervical Spine,
Shoulders and Knees
Sean Dadswell
2015

Introduction
How do you justify to patients not to get investigations done?
Do you know what scans of normal patients look like?
Pressure on investigation budgets?
GP ordering scans prior to arriving in Physio.
Have you ever been guilty of changing your practice because of a scan result that doesn’t correlate with what you have found clinically?
If you don’t know what’s normal how can you know what is abnormal?
Personal experience of back pain and subsequent MRI results.

Aims Identify different
investigation results for the Lumbar Spine, Neck, Shoulders and Knee in Asymptomatic patients.
Give clinicians an appreciation of the prevalence of different changes in normal patients in relation to demographic characteristics and activity levels etc
Discuss research/experimental relating to sources of pain in all mentioned areas and the presentation of this pain.
Case Studies of things that are unusual (just to confuse things).
Based on 40+ Journal articles
Draw your own conclusion
Dispel some myths

Magnetic Resonance Imaging of the Lumbar Spine in People Without Back Pain (Jensen et al 1994)
98 Pt’s no episode of back pain lasting >48 Hours and never had radicular symptoms.
50:48 male: female
Age 20-80 (Mean 42.8)
Recruited by flyer
27 symptomatic MRIs interspersed
Diagnosed as disc bulge, protrusion and extrusion


Results

Change Percentage of Asymptomatic Subjects
Normal all levels 38
Bulge at least 1 level 52
Protrusion 27
Extrusion 1
Abnormalities > 1 level 38
Schmorl’s Node 19
Annular Tear 14
Facet degeneration 8
Spondylosis 7
Stenosis (Central/Lateral) 7/7
Spondylolysthesis 7
Results cont

Most Abnormalities at L4/5 (30%) and L5/s1 (30%) Fewest L1/2 5% Prevalence of chages is significantly worse with age (P=
0.001) 67% of over 50’s had disc abnormalities at > 1 Level
compared to 27% under 50’s More Abnormalities in those who exercises than those
who are sedentary 16% compared to 4% (Small sample)
REMEMBER ALL COMPLETELY ASYMPTOMATIC
Conclusion: MRI results are COMPLETELY MEANINGLESS in isolation
Other Results of Note
Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations
(Brinjikji et al 2014)
Systematic review
33 Articles (1988-2014)
All subjects had never suffered any kind of back pain
No motor or neuro deficit, no trauma
Studies excluded if they did not specifically state pt’swere pain free

• With nearly 90% of 60+ year olds having disc degeneration and other changes then these could be considered age related changes rather than pathological changes
• As >50% of asymptomatic 30-39 year olds having disc degeneration then it may suggest that changes on MRI are incidental and not causative.

67 Pt Never suffered rom LBP or Sciatica (age 20-80)
Interpreted by 3 neurologist all blinded to Symptoms
Scans of Asymptomatic patients mixed with those of 33 symptomatic patients
Interestingly only 60% of scans had total agreement of all 3 neurologist but 99% had 2 or more (? Questions findings)
(Right: MRI 33 Year old man never had back pain)
Abnormal MRI Scans of the Lumbar Spine in Asymptomatic Subjects (Boden et al 1990)

Finding Age 20-39 40-59 60+
Herniated Disc 21% 22% 36%
Spinal Stenosis 1% 0% 21%
Results:
• Most disc herniations at L4/5 (35%) and L5/s1 (45%)
• In context: 1 in 4 normal patients will have abnormal MRI findings at any age!!!!
• Would you use a clinical test that was this inaccurate
• Author suggests to perform surgery based on an MRI alone would be a DISASTER!!!!!

75Year old man with bilat thigh pain for 3 years
Pain mainly getting up from chair
Severe loss PKB 90 degs bilat which progressed to 120 degs with stretching
Failed to progress pain so asked for MRI
ESP not seen many L2/3 disc bulge/stenosis so felt unlikelydiscussed with radiologist who suggested MRI
MRI showed L2/3 central stenosis
Asquier et al 1996 had only 100 pt to major hospital in france in 10 years with femoral neuralgia
Found L2/3 8%, L3/4 35% and L4/5 40%
Quick Case study to highlight higher Lsp involvement.

Loughnan et al 2002
Epidural analgesia and backache: An RCT comparison of IM Meperidine for analgesia during labour.
611 Mothers
310 received IM Meperidine
301 received epidural
Follow up at 6/12 with 85% follow up completed
Results:
Common Myth: I’ve had back pain since I had an epidural when I was pregnant!!
Epidural IM Meperidine
Any Back Pain 48% 50%
New Episode 29% 28%

Common Myth: Surgery doesn’t help Chronic LBP!!
Fritzell et al 2002
CLBP and Fusion: A Comparison of 3 Surgical Techniques: A Prospective Multicenter Randomised Study from The Swedish Lumbar Spine Study Group
Compared 3 progressively extensive spinal fusion techniques
294 Patients with at least 2 years therapy resistant LBP (Mean 8 Years pain)
All had L4/5 or L5/S1 spondylosis diagnosed on radiology
4 Groups (1 non surgical and 3 surgical all n=70-75)
Off work for mean of 3 years
Age 25-65

201 followed up for 6,12 and 24 Months
All treatment groups improved compared to control
P score reduced average 6.5 to 4.5/10 (P=0.0001)
Oswestry 47.5 to 36 (P=0.0001)
35% back to work across all treatment groups
60-68% reported “better” or “Much better” post Rx
In the 3 groups the complications increased from 6% to 31% with increased fixation.
Results

Congenital Vascular Malformations Present in 10% Autopsys and 14 % of over 60’s Only cause problem when they cause spinal cord
compression, hypertrophied bone, epidural hemorrhage or compression fracture.
Case 1: 54 year old progressive LL weakness over 1 year could ony
walk few steps with a walker +ve babinski Pain below mid chest CT showed T4 compression Rx Arterial Embolization (No Help) Scerlosing Ethanol 2 injections 10/52 apart Resolve symptoms in 6/12 back to work as ward sister
Common Abnormal Findings: Hemanginomas

Case 2:
64 Year old 3/12 HO Progressive LL weakness
Walking less than 6m
Weak prox leg muscles
MRI T12 compression
CT Hemanginoma
Same Rx of ethanol injections 10/52 apart
In 6 weeks walking 2 miles day
5/12 later MRI showed no compression

Biomechanics of back pain (Adams 2004)
Research well established re innervation of spine
Dorsal Rami of each spinal nerve divides into 3 and different parts supply Facets, interspinus ligs and muscles, skin, erector spinae and multifidus
End plates have spinal nerve so have potential to produce pain
Disc innervation (in health patients) is only in external few mm’s of nerve. Anybody know why?
Sources of Lumbar Spine Pain

Disc innervation controversial but possibly related to health discs having significant pressure through more central part of disc and less through outermost part.
Lack of hydrostatic pressure allows capillary formation which are required for neural infiltration.
Mechanism of pain from degenerative is that loss of structure reduces discs weight bearing properties and as pressure reduces more nerves can infiltrate discs (similar process to tendinopathy?)
Further evidence discussed that predisposition to back pain is genetic more than environmental based on twin studies
Mentions that 30% of chronic LBP comes from SI joint??? (Based on spurious claims and only related to pain below L5/S1)

Landmark paper in 80’s (would not be allowed now)
193 surgeries done with only local anesthetic then surgeon mechanically compressed various structures and pt described pain
All patients had been diagnosed with LBP with or with out leg pain due to disc bulge of stenosis
The Tissue Origin of Sciatic & Back Pain (Kuslich et Al 1991)
Structure Some pain Reproduced pain Site pain
Involved nerve 99% 90% Gluts leg foot
Normal nerve 11% 9% Gluts leg
Annulus of disc 73% 23% Back
Vert end plate 61% 9% Back
Facet 30% 3% Back

Normal Nerves generally no pain except sustained compression
Scar tissue from previous surgery usually asymptomatic unless compressing nerve
Annulus LBP side consistent and never gave leg pain although there was some buttock pain (1/3 v.tender, 1/3 tender, 1/3 no pain)
Facets took greater force to elicit any pain and always back pain (Remember sample)
Interesting findings from a study that wouldn’t get approved today!

120 Pts Chronic pain (>6/12) (Age 18-90)
No neural deficit
All failed conservative management
3 Stages to experiment
Evaluation of the Relative Contributions of Various Structures in Chronic LBP (Manchikanti et al 2001)
2 x Facet Injections
SI injectionProvocative Discography
Transforaminalinjection
Results: • 40% Facet joint pain• 26% Discogenic pain• 2% SI joint pain• 13% Nerve root
Bear in mind pt’s with LBP onlyDifficult thing to Ax but seem to have ried to limit flaws

500 pt’s age 18-90
P >6/12 (mean 83-106 months depending on area)
No radicular pain
Failed conservative management
Each had 2 injections of short and long lasting anaesthetic only +ve if both injections worked.
Results: (64-72% had bilateral involvement)
Prevalence of facet pain in Chronic Spinal Pain In Csp, Tsp and Lsp (Manchikanti et al, 2004)
Part of spine Facets Percentage
Cervical 140/212 55%
Thoracic 30/72 42%
Lumbar 124/397 31%


Case Study: Melanoma
67 Year old lady
HO 6/12 LBP followed by 2/12 of intermittent Claudication
Diagnosed as osteoporotic on X ray
Rx Meds and Physio => no Change
MRI = Epidural mass presumed to be hypertrophy of lig flavum
Even though pt had tumourremoved 13 years previous
Planned to fuse spine
Dark mass found during surgery found to be malignant melanoma
Bone scan revealed increase bone uptake L3 and SI Jt
Had radio and immunotherapy
All Clear 12/12 later
Apparently usual to miss these on MRI



497 Asymptomatic pt’s
Even spread 10 to >60
No Current or previous neck pain requiring medical intervention
Clear criteria for size and shape of abnormality
Results
MRI of Cervical Intervertebral Discs in Asymptomatic Subjects (Matsumoto et al 1998)
Abnomality 20’s 40’s >60
Disc Degeneration 15% 40% 87%
Post bulge 8% 18% 25%
Ant bulges 2% 8% 18%
Foraminal Stenosis 2% 5% 14%
50 Discs had posterior bulge with spinal cord compression mainly over 40’s


105 Asypt from 18-90
No previous neck pain
No Rheumatologic history
Not the best study in terms of report in but good images
Results
Evaluation of Age Related Changes in Cervical Spine in Saudi Arabian Adult Population: Using CT Scan Images (Hassan et al
2014)
18-35 years 36-55 56-90
Normal 20/35 3/35 1/35
Abnormal 15/35 32/35 34/35




63 Pts age 20-73
No Neck, shoulder or Radcular pain
37 Symptomatic scans interspersed
Multiple pothologies looked for (Spurs, < disc hieght, disc bulges, foraminal stenosis and cord impingement)
Catergories of mild/mod/severe and important/not important
Results:
Prevalence of cervical Spine MRI Pathology in AsymtpomaticIndividuals (Faubel 1990)
Abnormality <40 >40
Major Abnormality 14% 28%
Herniated disc 10% 5%
Foraminal Stenosis 4% 20%
Disc Degeneration 25% 57%
Cord Abnormalities 9% 1%
Highlights dangers of ordering surgery based solely on MRI

Longitudinal study (Although does not report difference in symptoms over time??)
Subjects 26 No Pain 40 sypmtoms of neck and/or sh pain for > 6 months
Age 17-19 then 24-26 Scanned 7 years apart
Not very high quality study but does highlight that changes on MRI are equally prevalent in young people when comparing symptomatic and asymptomatic subjects
MRI Changes of Cervical Spine in Asymptomatic and Symptomatic Young Adults (Siivola et al including Dr
Vanharanta 2002)
Change No Pain Pain
Disc Degeneration 11/15 9/16
Annular Tear 10 8
Disc Protrusion 13 11
Disc Herniation 0 4 (? Relevant)
No Findings 2 4

68 Consectutive patients
Chronic Pain >3/12 secondary toy RTA (54/12 mean)
Only 25% Normal Activity
34% off work because of pain
Given 3 injections one short lasting, one longer astinganasthetic and 1 placebo
Results:
Over 60% of Chronic neck pain could originate from facets
Most common levels C2/3 and 5/6
Sources of Neck PainChronic Cervical Zygapophyseal Joint Pain After Whiplash: Placebo
Controlled Prevalance Study (Lord et al 1996)
Type of pain +ve response -ve response
Headache 11 11
Neck pain 20 21

56 Pt’s Post Traumatic neck pain
Underwent provocative discography and facet joint blocks
Results:
Concludes that discography or Facet blocks not sufficient alone
Also discs and facets often pain generators following trauma
On The Nature of Neck Pain, Discography and Cervical Zygapophyseal Joint Blocks (Bogduk & Aprill 1993)
Structures involved Percentage
Disc alone 20%
Facet alone 23%
Disc and Facet 17%
No Segmental involvement 17%

170 pt’s (Although only 149 completed) with neck pain and/or radiculopathy
Age 15-83 (Mean 49)
No Duration of symptoms
Agreement between 3 radiologists
Results:
C4/5 level most commonly involved
TB Most Common Lsp
Cervical Spine MRI Findings in Patients Presenting with Neck Pain and Radiculopathy (Okedayo et al 2014)
Change Percentage
Normal 14%
Spondylosis alone 35%
Prolapse alone 10%
Spondylosis with Disc prolapse 33%
TB 3%

9 Health subjects
No previous neck pain
Electrical Stimulation of Medial Branch of Cervical posterior rami
Fluoroscopic guidance
Author appreciates that in chronic or severe neck pain referral patterns may vary due to central sensitisation/hypersensitivity
Electrcial Stimulation Induced Cervical Medial Branch Referral Patterns (Windor et al 2003)

2 Different studies referral patterns

51 Consecutively enrolled subjects
No Shoulder pain in each shoulder
Analyzed 3 Ultrasonographers
Age 40-70
96% Patients had an abnormality
Even when symptoms are present US results should be viewed with caution
Ultrasound of the Shoulder: Asymptomatic Findings in Men (Girish et al 2011)
Problem Percentage
Bursal Thickening 78
AC joint OA 65
Supraspinatus Tendinosis 39
Subscapularis Tendinosis 25
Partial Thickness tear 22
Labral Abnormalities 14
Calcification 4
Long Head Biceps prblem 4

96 Asymptomatic Shoulders
Exclusions no sh or neck pain or functional limitations
Age 19-88
Mixture of sedentary and active people in over 60’s Group
Abnormal Findings on MRI of Asymptomatic Shoulders (Sheret al 1995)
Problem Percentage
Any tear 34
Full thickness 15
Partial thickness 20
Over 60’s FTT 28
Over 60’s PTT 26
40-60 Any Tear 28
19-39 Any Tear 3

66% No tear
All problems increased with age
65% had evidence of AC joint OA
Other study cited reports that as long as Posterior cuff not damaged then it can still function

Chinese Study
644 out of 3117 members of the same village
Age 20-87 (Mean 69)
2:1 female to male
No one had ever had surgery
The Asymptomatic sh’s had never had sh pain
Symptomatic shoulders had pain at the time of the study
Prevalence of Symptomatic and Asymptomatic Rotator Cuff Tears in the General Population (Minagawa et al 2013)

Results:
In >50years old 50:50 ratio of Sympt: Asympt
In >60 years 2:1 Asymp: Sympt
Cuff tears significantly higher in manual laborers (38% forest workers)
Problem Total Symptomatic Asymptomatic
Full Thickness Tear 147 (22%) 35% 65%

Shoulder pain in 7-36% of general public 3rd most common MSK problem 94 Cases upper limb pain Exclusions of neck pain or previous multiple sh problems Diagnosis agreed on by 2 blinded Practitioners based on
tests including, apprehension, H&K, lift off Xrays, US Some patients had MRI and Arthroscopy Diagnostic injections were performed to confirm diagnosis
of AC jt pain, impingement and calcific tendinosis Pts were asked to map pain and rate intensity Young pt’s genereally diagnosed as instability (Mean age
34) Calcific tendinosis (Mean age 46 years) GH OA (Mean 69)
Sources of Pain in the ShoulderPain Mapping for Common Shoulder Disorders (Bayam et al
2011)

Severity pain worst in GH jt OA
Least variation in Ac jt distribution
Weak correlation between pain intensity and area
Interestingly no mention of frozen shoulder
Pain mapping in shoulder

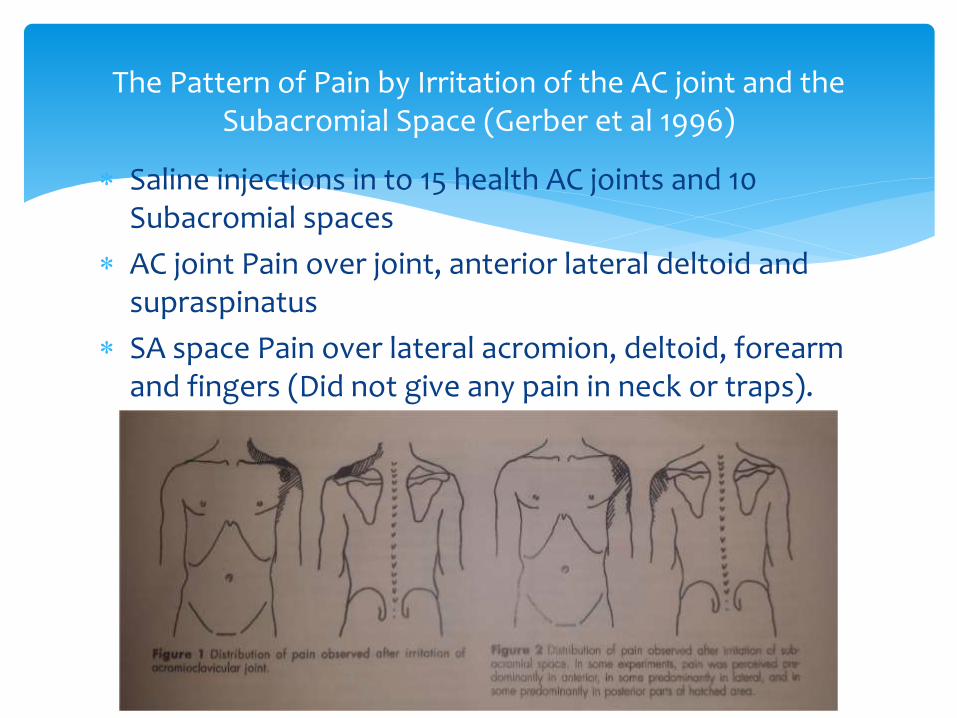
Saline injections in to 15 health AC joints and 10 Subacromial spaces
AC joint Pain over joint, anterior lateral deltoid and supraspinatus
SA space Pain over lateral acromion, deltoid, forearm and fingers (Did not give any pain in neck or traps).
The Pattern of Pain by Irritation of the AC joint and the Subacromial Space (Gerber et al 1996)

Testing Scarf test whilst pain was present only increased pain in 13% of patients
Direct pressure to coracoid process reproduced AC jtpain in 87% of patients
Did not test after subacromial injection as movement seemed very limited so could not get to start positions

Systematic Review of 53 trials
Not limited to MSK but included trials Sh OA, Spinal surgery 6 studies, General OA 4 Studies, Plantar Callosities
Results:
72% of surgery resulted in improvements in both placebo and surgical groups
Only 49% of studies reported superior outcomes for Rx group
Rx effects were generally small
Use of Placebo Controls in Evaluation of Surgery (Wartolowska et al 2014)

5 Cases where shoulder joint malignancy diagnosis was delayed secondary being treated as frozen shoulder
Tumours are uncommon
Clinical history can be identical to frozen shoulder
Arthroscopic distention are strictly contraindicated with local oncological process is present
Can result in treatment being a limb preserving resection to a forequarter amputation
All 5 cases had prolonged conservative management and hydrodylation
2 had arthroscopic surgery
Lessons Learnt from the Painful Shoulder; Case series of Malignant Shoulder Girdle Tumours Misdiagnosed as Frozen
Shoulder (Quan et al 2005)

6 Year Old lady
18/12 HO worsening shoulder stiffness
Initially Rx with oral painkillers and steroid inj (No Help)
Then Hydrodylation (No improvement)
MRI showed large permeative tumour in scap
Case 1

42 Year old man
Sudden onset sh pain due to work
Originally diagnosed as Rot cuff tendinopathy and SAI
Had Physio and arthroscopic release (No Help)
2/12 later reduced ROM so hydrodylation (Worsened)
X ray Showed destructive lesion
Course of Chemo and en bloc resection
Case 2


50 Year old woman 6/12 HO episodic shoulder pain
Xray initially NAD
SAI injection
Arthroscopic distention
MUA
Arthroscopic debridment and acromioplasty
Lots of synovitis during arthroscopy which her symptoms were put down to
Xray 2 years after onset diagnosed large lesion in glenoid cartiledge
En bloc resection of tumour
Case 3

A initial X-ray B repeat X-ray

Other cases one initially responded to injection and distension but stiffness returned and ended up with palliative care
Last one had previous HO tumour, had arthroscopy and diagnosed rot cuff tendinopathy, repeat Xrayafter 1 year and showed destruction of glenoid and coracoid
10% of Xrays will be normal
2% of patients referred for MUA had chest wall tumours
Misdiagnosis has grave consequences
Should Xray be routine for frozen sh?
Further Ix if pain and restriction persist or are atypical

100 Pt’s age 18-73
45 Pts with traumatic HO pain
Ref by orthopadic surgeons, Rheumatologist, GP and general Surgery
Pt had Unilat knee pain and had never missed work or sport because of other knee
Results:
Patients with Suspected Meniscal Tears: Prevalance of Abnormalities Seen on MRI of 100 Symptomatic and 100
Contralateral Asymptomatic Knees (Zanetti 2003)
Type of Tear Symptomatic Asymptomatic
Any tear 57% 36%
Medial 50% 34%
Lateral 16% 8%

All patients with out meniscal tear on symptomatic side had normal Asymptomatic side
Prevalence of tears on Asymptomatic side in patients with symptoms was 63%
In this paper 57% clinically suspected Meniscal tears were confirmed on MRI
Very high prevalence in opposite knee
May be medial collateral more relevant and mimic meniscus
88% of those referred to the study were done so by Ortho Consultants
Problem Symptomatic Asymptomatic
Collat lig Abnormality 53% 6% (P=0.001)
Percapsular oedema 64% 12% (P=0.001)
Bone Marrow Oedema 36% 3% (P=0.001)
Necrosis or fracture 11% 0% (P0.001)
Pericapsular soft tissue abnormalities most common finding 62% (? Clinical relevant?)
Bone Oedema/Bruie very common 35%

14 NBA players (both knees)
Age 20-36
Include pt’s with previous knee injuries, 1 MCL tear and 1 meniscectomy
Results
25 knees (89%) had one or more abormalities
Only 3 knee no abnormalities
All players had something wrong with at least one knee
Jt effusion in30%
Patella tendinosis 40%
Not representative but highlights need to consider hobbies
Abnormal Findings on Knee MRI in Asymptomatic NBA Players (Walczak et al 2008)


220 knees with Asymptomatic OA
30 Bakers Cysts detected none of which were painful
The Reliability of Clinical Exam for Detecting Bakers Cysts in Asymptomatic Fossa (Akgul et al 2013)

320 Elite Athletes (Cricket, netball, basket ball and Australian rules) All Asymptomatic
27 non athletes (Controls)
Results:
22% athletes (Have Hydroechoic area) 4% Controls
30% Males 15% Females
32% Basketball Players 9% Other athletes
Patella Tendon ultrasound in Asymptomatic Active Athletes Reveals Hydroechoic Regions: A Study of 320 Tendons (Cook
et al 1998)

26 Basketball players (8 Male 18 Female)
2 Compatition days 1 year apart
All patients were asymptomatic at first competition
10 Pt’s had abnormalities at first competition
42 no abnormalities
Results:
3 of 10 (30%) subjects developed jumpers knee
3 of 42 (7%) controls developed jumpers knee
At follow up 1 year later 60% still had adnormalities
Prospective Imaging Study of Asymptomatic Patella Tendinopathy in Young Basketball Players (Cook et al 2000)

243 Subjects
90 Controls (No Knee pain No OA on Xray)
59 Knee pain
32 Asymptomatic but OA on Xray
62 Symptomatic OA confirmed on Xray
Results:
Sources of Knee PainSynovial Pathology Detected on Ultrasound Correlates With the Severity of Radiographic Knee OA More Than Symptoms
(Hall et al 2004)
Problem Controls Knee pain Asympt OA Sympt OA
Effusion 28% 19 81 92
Synovial hypertrophy
8 7 40 82
Bakers Cyst 12 9 21 39
Infrapat bursitis 0 6 0 8

Significantly higher effusion and synovitis in Symptomatic OA group compared to Asympt and controls
Pain correlated weakly but significantly with amount of synovitis
Synovitis not necessarily inflammatory but may give mechanical pain

401 patients with OA on Xray
351 with pain
50 with no pain
Mean age 67
Results:
Bone Marrow Lesions in 77.5% pts with pain compared 30% asymptomatic knees
Large lesions almost exclusively in painful knees (36%:2%)
However size of lesion does not correlate with severity pain
The Association of Bone Marrow Lesons with Pain in Knee OA (Felson et al 2001)

535 Pts (subset of larger study)
Sample 50-79
Mix of OA or at risk ie obese, previous knee pain etc
Only 454 included due to loss data
Found amount of synovitis strongly correlates with severity of pain measured with 2 different pain measures
Relation of Synovitis to Knee Pain Using Contrast Enhanced MRI (Baker et al 2010)

25 pts of 667 people with tumors referred to and ortho dept had previously been diagnosed with sports injuries
All had invasive procedures for intraarticularproblems
18 men 7 women
Age 15-55 (Mean 27)
21 Disagnosed as meniscus tear
1 ACL, 1 Patfem pain, 1 Synovial Cyst, 1 Synovitis
None MRI prior to surgery which would have diagnosed tumors
Tumors About the Knee Misdiagnosed as Athletic Injuries (Muscolo et al 2009)

Delayed diagnosis affected 6/11 pt’s with benign tumor as initially could have been treated with cureltage but had to be resected
9/14 malignant pts might have been treated differently as 8 could have been treated with intraarticular resection and 1 with extraarticularresection
Instead 3 had extra articular resection and 6 had amputation

Always consider clinical findings when evaluating scan results
Always consider that scan result findings may be incidental
Ensure you are aware of what are normal values/finding when ordering an investigation
Conclusions


















