![Norfolk southern [norfolk and western] zone 8 (2015)](https://static.fdocuments.us/doc/165x107/5886974c1a28abf6158b76af/norfolk-southern-norfolk-and-western-zone-8-2015.jpg)
Norfolk Needs Assessment Toolbox - NPHNF England - 2002

of 24
-
Upload
publichealthbydesign -
Category
Documents
-
view
213 -
download
0
Transcript of Norfolk Needs Assessment Toolbox - NPHNF England - 2002
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
1/24
1
The Norfolk Needs Assessment Tool Box
Version 2
April 2002
Produced under the auspices of the Norfolk Public Health Nurses Forum
Comments and requests for further copies (electronic or paper format):
Dr Peter BramblebyDirector of Public Health
Norwich Primary Care TrustSt Andrews HouseThorpe St AndrewNorwich NR7 0HT
Tel: 01603 307206Fax: 01603 307104
e-mail: [email protected]
mailto:[email protected]:[email protected] -
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
2/24
2
The Norfolk Needs Assessment Tool BoxVersion 2
Contents
Read items marked*for rapid scan of main messages
1. Introduction
1.1 About this Tool Box 31.2 About the Norfolk Nurses Public Health Forum 3
1.3 What is Needs Assessment? Definitions 5*1.4 Lessons from elephants 61.5 When is needs assessment used? 7
2. Practical techniques
2.1 What techniques are available to assess needs? 9
2.2 How to do a population needs assessment 11*(What are the needs of our population?)
2.3 How to address a problem-solving needs assessment 12*(Do we need this?)
2.4 How to prioritise a list of needs 14(Economic considerations)
3. Epidemiological considerations
3.1 Denominators 153.2 Rates 163.3 Standardisation 17
4. The difference between need, demand and supply 19*(Needs assessment as part of demand management)
5. References and further reading 23
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
3/24
3
1. Introduction.
1.1 About this Tool Box
This tool box has been produced in response to requests for help from avariety of sources from within the NHS and outside.
Some people want to do their own needs assessments but dont know whereto start. Others have been asked to give a perspective on some-one elsesassessment but dont know what its all about.
Please use it as a resource. It can be read from start to finish to give acomprehensive overview, or just dipped into for its ideas, definitions andtheoretical frameworks.
It began its development under the auspices of the Norfolk Public HealthNurses Forum, and had a predominantly health needs focus, but has sincebeen discussed with Social Services and various other statutory and voluntaryorganisations and is intended to be a resource for any caring agency. Theapproach and techniques should apply in most situations where the needs ofgroups of people are being reviewed.
Perhaps the most important concept is that of needs addressment a newterm invented by the Norfolk Public Health Nurses Forum. The process ofassessing needs should never be divorced from addressing them, either withnew resources or redeploying existing resources
1.2 About the Norfolk Nurses Public Health Forum
Following an inaugural meeting on 25 June 1999 it was agreed that a forumwould be set up one that would continue to meet on a regular basis. It isconvened by the Director of Nursing and Quality at Norwich Primary CareTrust but covers the whole of Norfolk. Its remit is to:
Help implement the national agenda for developing the public health roleof nurses
Raise the confidence and competence of nurse members on boards ofPrimary Care Trusts
Provide a focus for sharing experience, learning and peer support. Provide a link with the Public Health specialists.
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
4/24
4
Nurses Forums initial views on the advantages of needs assessment:-
bring together people who dont often work together
more co-operation better team work shared information and understanding provide a forum for the public and professionals to get together break down professional barriers allow bottom-up priorities to emerge break down paternalistic and professional dominance so that issues of
local public relevance can surface a first step in community development a useful management tool for review of services, fairer distribution and
better use of resources identify and plug gaps encourage the broadest view of health and well-being (not just a bio-
medical disease model) introduce the rigour of evidence-based planning to service development improve services on the ground improve the quality of data collection as data are seen to be used to
greater effect allow people to see the needs in their patch in a wider, comparative
context
Nurses Forums initial views on how to go about needs assessment:-
it is necessary to formulate clear questions before embarking time of participants is a scarce resource that should not be wasted project management discipline is required to prevent drift academic rigour should apply: assessments need to stand up to scrutiny,
especially where changes are brought about contributors might find participation intimidating, so openness and
tolerance of inexperience should also apply needs assessments should be seen to make a difference
information gleaned and gaps identified should be recorded and shared sothat learning takes place specialist public health may be needed, for example with comparative
data, but grass-roots input is almost always needed. there are immediate and continuing training needs in this field (one reason
for producing this tool kit!)
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
5/24
5
1.3 Definitions
Needcan be said to exist when people couldbenefit from some sort of intervention that their liveswould be measurably improved if this gap was filled.
The only distinction between a health need, health careneed, social need, educational need and so on, is theway in which the question is phrased and the means bywhich it is remedied. These needs frequently overlap andit is usually unhelpful to be too restrictive at the outset ofan assessment. Narrower focus can be introduced lateronce the parameters are clearer.
Needs assessmentis the process ofidentifying both the nature and scale of needs asdefined above. Its purpose is to tease out gaps and
priorities. Sometimes this is in absolute terms, as in:How many people need this? or Do we need this?.Sometimes it is in relative terms, as in: What are ourcommunitys needs relative to the rest of Norfolk?, orWhich three needs should we address first?.
The themes of measurability and ability to benefit arecentral to the process.
Needs assessment deals with populations, and aims to:- be objective, systematic and valid involve the population served include a range of key informants, particularly those
with special interest and expertise in the subject use a number of agencies and methods of collection come up with recommendations for change
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
6/24
6
1.4 Lessons from elephants
(Skip this section if you do not find allegories helpful!)
Rather like an elephant, a need is easier to describe than define, buteveryone knows one when they meet one. Or do they?
There is a story from the Far East of three blind men in the forest whoencounter an elephant. The first has put his arms round a leg and calls outCareful Ive just walked into a tree! The second has hold of the tail andsays to his friends Yes, and someones left a rope hanging down!. But thethird feels the trunk and shouts out No! Its a snake! Run for it!. The point ofthis story is that need is a multi-faceted thing, and is viewed differently by
different people at different times. In general it is better to explore it in severalways in order to build up a more complete picture than to rely on a singletechnique or just one perspective.
In another story, a sculptor, famous for his detailed carvings of elephants, wasasked how he went about it. Easy, he said, I just take a block of stone andchip off anything that doesnt look like an elephant!. But thats the skill. Inthe case of needs assessment, its the ability to approach a wealth of data andsee the elephant hidden within the stone.
Question: How do you eat an elephant?
Answer: A bite at a time!Moral: Complex tasks like needs assessments have to be broken down
into bite-sized chunks.Corollary: Complex electronic databases have to be broken down into
byte-size chunks!
Do not be over-elaborate. If it looks like an elephant, walks like an elephantand sounds like an elephant it probably is an elephant. Do not fall into theparalysis by analysis trap and do not let a needs assessment become astalling exercise or a substitute for action.
Dont let your needs assessment exercise become like an elephant withconstipation ie, three months of intense straining, followed by a loud report,after which the whole lot is dropped!
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
7/24
7
1.5 When is Needs Assessment useful?
1.5.1 Taking the initiative, scanning the whole population, setting the agenda:as in these questions:
What are the top five health care needs of our practice population, orof our Primary Care Trust?
What factors do our population believe affect their health or well-beingadversely?
What are the major inequalities in health or well-being across ourcounty?
What are the top three social care priorities for our senior citizens? What are the health and educational needs of children in care? Given our current budget for coronary heart disease, could we deploy
it to better effect?.
This is horizon-scanning stuff. The initiative is taken by the needs assessorsand the answers will set in train new lines of work. It helps to set the agendaand sort out priorities from a very long list when one is are starting fromscratch and doesnt know where to begin. It tends to be deliberately wide inits scope, and usually looks forrelative importance amongst a range ofpossible needs.
1.5.2 Responding to a specific proposal or demand:as in the questions:
Do we need to use this new drug in our hospital? Do we need another health visitor in our practice, or social worker on
our discharge ward? Do we need to introduce a screening programme for a specific
disease? Should we suspend a particular service because it is no longer
needed?
It is often forced upon planners in response to a direct request for a newservice or some external pressure. It is very focused in its remit and tends to
look at a single drug, surgical technique, screening programme, service,specialist input, disease or client group.
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
8/24
8
1.5.3 Needs Addressment.
This is a new term, coined by the Nurses Forum. Just as in clinical practiceone tries never to request a test on a patient unless the result will affect theclinical management, so in needs assessment one would not embark on a
project unless there is some prior commitment to act on the findings.
Needs assessment can be time-consuming and expensive, and it raisesexpectations. It involves the scientific disciplines of
- epidemiology (to identify the nature and scale of the problems) and- economic appraisal (to identify cost and savings, benefits and
disbenefits of doing different things and doing things differently).
There must be some clear end in mind, and action must follow, otherwise theneeds assessment will be futile and the engagement of others will be harder
to secure next time around.
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
9/24
9
2. Practical techniques
2.1 What techniques are available to assess needs?
Broadly, there are three techniques:1. Analysis of routinely held data2. Acquisition of information from local informed sources3. Surveys of those who live in the area or use the services
2.1.1 Routinely available data at national or local level, such as:
census-based population statistics (numbers of people, age profiles,housing tenure, car ownership, self-reported limiting illness, etc),
births and deaths statistics, data on current resource allocation money, staff and facilities and
future expectations data held by local authorities, benefits agencies, police hospital utilisation data held by health authorities data held by general practices, now rapidly getting easier to access, such
as disease registers, community contacts, prescribing.
These have the advantage of being fairly readily available and pre-digested(e.g. rates and comparative information calculated as in the national publichealth common data set, Health Authority annual report of the Director ofPublic Health, reports from Housing, Voluntary Agencies, Education, Policeand Social Services, and PCG profiles). They allow comparisons between the
locality of interest and similar localities elsewhere.
This aspect of a needs assessment is often best handled by data analystswho have access to large databases and experience in dealing withspreadsheets.
Remember: routinely available comparative data are almost alwaysuseful, but very seldom sufficient on their own to complete a needsassessment. There is no substitute for up to date information, drawndirectly from the people affected, couched in their own terms (seebelow).
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
10/24
10
2.1.2 Rapid participatory appraisal(focus groups, key informants or health forums).
One of the fastest and most useful techniques is participatory appraisal.Here, a group of local informants such as health workers, social workers,
patient support groups, teachers, police, clergy, womens groups, communityhealth councils, elected members of local government and so on can gettogether and give rapid opinions of what the needs and gaps are. Healthforums that exist in most Primary Care Trust areas are a good example. Mostprimary care groups have experience in drawing on their input. Focus groups,perhaps convened on an ad hoc basis for a single issue, are a similarconcept.
2.1.3 Surveys of the population
The third approach is to conduct a survey by post, telephone or interview -
and simply ask a random sample of the population what their views are. Thiscan be done in a structured, semi-structured, or totally open format. It cancontain open questions about what they feel the health needs are, or directthem to specific areas that the assessor wants to explore. Surveys are also away of getting reaction to a health needs assessment that has already beenconducted, to validate its findings and see if the respondents can spot gaps.
In choosing a sample of the population for a survey, care must be taken thatthey are a representative cross-section so as not to introduce bias. It helps ifthe sample is truly random, and it also useful to know the characteristics ofany non-responders just in case the views of an important sub-group havebeen omitted.
A number of statutory and voluntary caring agencies conduct periodic surveysor market research. It makes sense to pool effort, pool resources and poolresults. Local strategic partnerships are one such forum, led by localauthorities, and as they get off the ground they should be used to fulladvantage.
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
11/24
11
2.2 How to do a population needs assessment(What are the needs of?
1 Formulate a clear question, or questions, that your needs assessmentwill address. Rather than just asking open questions about what might
be done in an imaginary ideal world, it is often better to phrase aquestion along these lines: Given our present level of resources (money,people, facilities, partners), and what we can reasonably expect in thenext few years, are there better ways of aligning them with what ourpopulation needs?
2 Check the question, or questions, with the people who commissionedthe assessment and who will act on the findings
3 If its a big project, convene a project group; agree the tasks, timetableand administrative support.
4 Check to see if anyone has done something similar, from which you
could learn, either locally or from a literature review5 Discuss the project with the Public Health Department at the HealthAuthority they will be able to help you design your needs assessmentand may be able to provide the comparative data from routine sourcesthat are part of the assessmentor put you in touch with others who can.
6 Identify routine data sources that might help (taking advice from PublicHealth Department, University, information department of local trust,local authority, police, etc). This might shed light on the questions beingaddressed and provide comparative information about other localities toput the findings into context.
7 Think of informed local sources forparticipatory appraisal, either
something like a health forum that already exists, or a new focus groupconvened specifically to address the question.
8 Think of a representative sample of the local population who could beapproached for a population survey.
9 Consider testing your methodology with a pilot, especially if you aretreading new ground.
10 Go for it! Local flavour and local participation are the greatest strengths!11 Validate your assessment and draft recommendations by feeding back
to the people who contributed and the people who are affected bychange.
12 Agree the priorities and gaps you have identified, at Board level in the
participating organisations, and start addressing them!13 Registeryour project with the HImP partnership so that others can tap
into your experience. This is also an important record to ensurestandards, openness and corporate governance.
14 Conduct a de-brief or washing-up session with your group to see if,with hindsight, it could be handled even better in future.
15 Depending on the importance and generalisability of your assessment,considerpublishing your findings in a peer-reviewed journal.
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
12/24
12
2.3 How to address a problem-solving needs assessment(Do we need a .)
(Note: this section was drafted from a health care perspective, but is probablyapplicable in other types of need, such as social care and education.)
Most of this resource pack deals with pro-active population-based needsassessments, but situations can arise often prompted by a local provider ofservices when the question is: Do we need a new member of staff, orbuilding, or major piece of equipment, or screening programme, orexpensive new medicineand so on? In the case of new medicines there isan established policy for handling these at primary care level, in secondarycare trusts (Drugs and Therapeutics Committees) and whole-county level(Therapeutic Advisory Committee), but for others the decision-making processand checklist for scrutiny are less well established at present.
The following list (all beginning with E for convenience) may be helpful.
Epidemiology What is the nature and scale of the problem in our area, forwhich this innovation offers a solution?Can we estimate the prevalence (existing cases) andincidence (new cases)? Note: with a new service there maybe a temporary prevalence pool to mop up, followed by adifferent steady state when new cases balance those beingcured or dying.What are the likely demographic trends over time?
Effectiveness What is the quality of the evidence of effectiveness?Has there been a head-to-head comparison with currentpractice, rather than just placebo, and what is currentpractice in our patch?Can the research evidence be extrapolated to our area?How many people will benefit? (numbers needed to treat)What are the likely benefits, eg longer life, improved quality oflife, better experience of care, or improved efficiency?What are the adverse effects of the intervention, and howmany people will be expected to have them? (numbers
needed to harm.)
Economics What are the added costs of the new intervention in our area,if any, over what we do at present?Are there savings - do they release money, staff, facilities?Where and when do costs and savings fall?Do we judge that the overall added benefit is in proportion tothe overall added cost?How do the benefits of using resources in this way comparewith other ways of using the same amount of resource?Is there some other, perhaps unrelated, area of activity in
which we should now disengage?
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
13/24
13
Expectations What, if anything, do we know about what local patients andprofessionals want? Note: if there is little outside pressure,especially from the public, there is less chance of the issuegetting priority. This is not a defence of prioritising bydecibels but a reminder that commissioners need to show
that they are responsive to local needs and wishes.
Equity How well does this proposal fit with the current HealthImprovement Programme or Service and FinancialFramework, and do they need to be re-negotiated?Are we satisfied that we are maintaining a fair distribution ofresources between care groups and providers?Will the new initiative increase or reduce inequalities?
Education How will we raise awareness of the changes?Is staff training required in any of the collaborating
organisations?Who will compile the guidelines for staff, patients and carers?Is this such a significant change that a major publicitycampaign or public consultation is called for?
Execution How do we make it all happen?Are shared care protocols needed?What does the patient pathway look like now, and can weenshrine that in a new long-term service agreement?
Evaluation How will we know if it is all working according to plan?What programmes of clinical audit, contract monitoring andreporting do we need to establish?
Adapted and expanded from:
Best L, Stevens A, Colin-Jones D: Rapid and responsive health technology assessment: thedevelopment and evaluation process in the South and West region of England. J Clin. Effect., Vol 2, No2, 1997, 51-6
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
14/24
14
2.4 How to prioritise a list of needs
This is the domain of Economics the discipline that deals with scarcity andchoice. In some specific clinical areas, such as cancer or stroke, there arevalidated instruments (sets of questions) for assessing the outcomes of
treatment, but comparing between different types of need is always difficult.There has been expansion in the department of health economics at UEA -(try Ric Fordham at UEA 01603 593543). Meanwhile, even though we oftenfall back on qualitative judgements, we should still be systematic and openabout the reasons for our decisions.
Look at the numbers of people who will receive the new service ortreatment
Estimate the numbers who are likely to benefit (may be all those receivingthe new service, but depends on the evidence about the particularintervention)
If it is an intervention with possible adverse effects (eg false positives in ascreening test or dangerous side effects from a new medicine), estimatethe possible scale of harm
Look at the kinds of effects being generated, for example:
length of life
quality of life
relief of pressure on carers
improved efficiency of service
improved conditions for staff
benefits for other caring agencies (eg invest in health care to reduce
pressure on social care) Look at the magnitude of that effect (By how long is life extended? By how
much is quality of life enhanced?)
Look at the duration of that effect: a few months? a few years?
Look at all the costs (not just cash, but travel time, time off work, etc) andthe savings too. Dont just focus on the caring agencies, think of thepatients and families too. Ask for the help of a health economist if thescale of the changes warrant this
Having looked at all these factors, try to prioritise those which give thegreatest health gain ie, combination of length and quality of life and
then look at relative costs and affordability. Do this in a qualitative way,when quantitative ways are impractical. Try to make it clear what thereasoning is.
Remember: data on costs and outcomes can only ever be estimates;certain vulnerable groups may need a protected (or weighted) share ofresources; national priorities and imperatives have to be accommodated; itis justifiable to adjust the priority list so long as the reasons are clearlystated and the final decision taken in open forum.
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
15/24
15
3. Epidemiological considerations
3.1 Denominators
Remember studying fractions at school? The number on top is the numeratorand the number on the bottom is the denominator.
Now think of needs assessments.
The number of needy people identified is the numerator. The populationfrom which they are drawn is the denominator. Deciding on the relevantpopulation to act as the denominator can be difficult.
Take a Primary Care Trust (PCT) for example.
Its population could be taken as the people registered with the practices thatmake up the PCT, wherever they live, or those who are resident within thePCT boundary drawn on a map, whether they are registered with practices inthat area or not.
We know about practice populations broken down into age and sex groups, sowe can calculate rates (another term for fractions) for the needs and NHSactivity that goes on in those practices. For example, we could look atnumbers of health visitors attached to each practice per 100 children agedunder 5 years in the practice, or per 100 low birth weight babies born in theprevious year. In this example we are relating provision of a service (healthvisiting) to indicators of need (pre-school children and vulnerable new-borns).
But suppose we were looking at house ownership, or unemployment, or socialdeprivation (which is based on replies to the ten-yearly national census) in thePCT area. This information is not routinely available from GP records. In thissituation we might use resident, as opposed to registered, population. Insteadof GP practices being the building blocks which add up to a PCT total, wecould look at electoral wards or post-codes falling within the geographical
boundary of the PCT. The difference between registered and residentpopulation in PCTs in Norfolk is +6.7% to 1.9%.
The practical relevance of this for needs assessments at the level of primarycare or community services is the selection of a population that suits the dataavailable and suits the purposes of the study being conducted.
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
16/24
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
17/24
17
3.2 Standardisation
A technique for getting around the problem of making comparisons betweenpopulations that have different structures (typically in relation to age and sex)is to standardise them so as to compare on a like-for-like basis.
There are two approaches to standardisation: direct and indirect.
Direct standardisation. In this technique a standard population is chosen,such as the UK population or (increasingly frequently) an imaginaryEuropean Standard Population (ESP, see below). Direct standardisationagainst the ESP is easy if you know the age-specific rates in your ownpopulation broken down in the 5-year age bands used in the ESP. Simplymultiply each age-specific rate by the number of people in the same age band
on the ESP table, and add up the totals to give an ESP-standardised rate.Obviously, since this was an imaginary population the actual figure isrelatively meaningless, but compared with other ESP-standardised rates it isinstantly meaningful because differences in rates cannot be due to age or sex.Direct standardisation is most useful when wishing to make directcomparisons between populations with different age or sex structures.
The European Standard Population (ESP)
The ESP is widely used to compute directly age-standardised rates. The samepopulation is used for males, females or all persons.
Age Group European Standard Population0 1,6001-4 6,4005-9 7,00010-14 7,00015-19 7,00020-24 7,00025-29 7,00030-34 7,00035-39 7,000
40-44 7,00045-49 7,00050-54 7,00055-59 6,00060-64 5,00065-69 4,00070-74 3,00075-79 2,00080-84 1,00085+ 1,000Total 100,000
Source: 1991 World Health Annual of Statistics based on J Waterhouse et al (eds). Cancer Incidencein Five Continents, Lyon, IARC, 1976 (Vol. 3, p 456)
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
18/24
18
Indirect standardisation. This is useful in making comparisons in ratesbetween one population (such as Norfolk) and a real standard population(such as the UK). Its most familiar use is in the standardised mortality ratio(SMR), but it applies equally to standardised illness ratios, standardised
hospital admission ratios, or other such events.
To perform an indirect age standardisation you need to know the age-specific(and sex-specific too if you wish) rates in the standard population. Multiplythese by numbers of people in each of those age bands in your studypopulation. The total of all of these gives you an expected number of events ie the number you would expect if standard rates applied in your population.But you may well have observed a different number in reality. If theobserved events are divided by the expected events and multiplied by 100,it gives the standardised ratio. The figure you get is instantly meaningful. If itis greater than 100 then the events are occurring at a higher rate in your studypopulation than the standard population, and if less than 100 then at a lowerrate. Differences in age (and sex) structures of the two populations havebeen taken out of consideration.
Statistical significance. Some published sources, such as the PCG profilesproduced in 2000 for Norfolk and the national Public Health Common DataSet, give 95% confidence intervals for SMRs. This gives a range within whichyou can be 95% certain that the true value lies. It is particularly helpful insmaller populations where the reliability of the estimate is weaker. A 95%confidence interval, eg 102-134, gives the lower and higher value of the range
within which the true SMR is likely to lie. In this example even the lowestestimate is above 100 so the SMR can be said to be statistically significantlyhigher than 100. If the 95% confidence interval for an SMR was 87-98 thatwould be statistically significantly lower than 100 because even the highestestimate is below 100. If the 95% confidence interval for an SMR was 85-105that would not be statistically significant because the figure 100 falls within therange.
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
19/24
19
4. The difference between need, demand andsupply
Need (the ability to benefit in some measurable way) is not the same as
demand (what patients ask for) and different again from supply (what is onoffer for them). To illustrate the differences the following schematicpresentation relating to secondary care (hospital) services may be helpful.
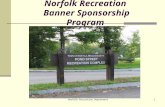
Have a look at diagram 1 (representing where we are now) and diagram 2(where we aspire to get to in an ideal system). These are schematic, and notdrawn to scale, but as a general framework they are pretty robust. Diagram 1appeared in NHS guidance back in 19911.
Diagram 1Need, Demand and Supply for secondary health care the present.
Diagram 2
Need, demand and supply for secondary health care the objective
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
20/24
20
In these diagrams: Need is the ability to achieve a measurable change in health status as a
result of a secondary health care intervention. Technological advancespush back the boundaries of need for example, before there were
effective coronary artery re-vascularisation procedures the NHS did nothave to assess the need, but now it does. Need can also be definedarbitrarily for local circumstances for example most health authoritieshave decreed that tattoo removal is not a legitimate NHS need.
Demand is seen here from the hospital perspective, ie what the GP isreferring the patient to hospital for (for those who have been through thesieve of General Practice) or the patients who self-refer (eg via casualty).
Supply represents what is provided by way of hospital services (iecapacity).
Note, from diagram 2, that a better overlap between all three istheoretically possible without new resources.
If we look at each of the numbered areas in diagram 1 in turn we can teaseout the components of the problem and begin to see some solutions. Theultimate objective of demand management is to get a better overlap betweenneed and supply.
Zone 1: Supply that is neither demanded nor needed.This is spare capacity, wastage and inefficiency. Think of drugs thrown awayunused, cottage hospitals only three-quarters full or excessive numbers of
specialist registrars in obstetrics and gynaecology. This Zone has beensqueezed hard over many years, but largely on a Trust by Trust basis. Theremay still be scope for a whole-system approach that enables further waste tobe excluded. This frees up resources for covering more of the need. It wouldnot mean taking resources out of the system but re-deploying them.
Zone 2: Demand that is not a need, and therefore not supplied.This represents silt in the system that can clog up the machinery. It is, in part,what NHS Direct was set up to address. Practice charters, patient education,information and campaigns all have a role in mitigating this problem in primarycare before it translates into an inappropriate demand on secondary care
(think of the milder end of the tonsillectomy demand). At Trust level it can bedifficult to turn away inappropriate demand because patient and GPexpectation are, by that stage, very high. That, together with the fact thatservice agreements and targets are skewed towards rewarding interventionand not refusal, means some patients move on to Zone 3.
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
21/24
21
Zone 3: Demand that is met even though it is not strictly needed.This is a waste of scarce resources. Think of the milder cases of glue ear thatproceed to surgery where watchful waiting would be more appropriate.Tightening up the local criteria for referral and thresholds for intervention, orrewarding appropriate clinical management rather than activity per se, are
ways to free up resources here. Taking Zones 1 and 3 together gives the totalarea of current provision that is not addressing true need. It represents theprincipal hunting ground for disinvestment and re-deployment of resources(such as staff, theatre sessions or finance). It requires considerable effort inpublic information and education.
Zone 4: Demand that fulfils criteria of need but is not yet met.This zone equates with the waiting list for admissions after the patients havebeen assessed in the outpatient clinic. There is such intense managerial andpolitical pressure to address this group that it is easy to concentrate onnothing else to lose sight of the bigger picture and miss the whole-system
approach. Note that a hospitals outpatient waiting list contains a mixture ofZone 2 and 3 patients all of whom have expressed a demand but are notnecessarily in need.
Zone 5: Unmet need, not brought to medical attention.An important but neglected part of demand management is generating newdemand where it ought to be greater. Think of a 54-year-old man, a life-longsmoker with a family history of heart attacks, who has not come forward forhealth screening. Now look closely at practices within PCTs that haveunexplained low referral rates. Remember that the objective of demandmanagement is not to curtail demand per se but to get a better fit betweenneed and supply. This is where needs assessment links up with demandmanagement.
Zone 6: Services that are supplied to meet need without prior demandby the patient. Do we ever meet needs without them being demanded? An unusual conceptat first glance, but think of cancer screening, childhood immunisation, healthpromotion and well-person clinics. This is where the Health Service goes intoproactive mode. It is a major plank in the strategy to get need and supply tooverlap better. Go get them!
Zone 7: Needs that have been demanded and met.This is the ideal situation. In reality, the scale should show this to be a verysubstantial box. We tend to forget just how good a population coverage wedo achieve in the NHS. This is the ideal situation, and the closestapproximation to diagram 2, which is our aspiration.
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
22/24
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
23/24
23
5. References and further reading
1 Hooper J and Longworth P. Health Needs Assessment in PrimaryHealth Care A workbook for primary health care teams. DoHResource Pack, ring-binder format. Sept 1997
Available free on request from: Health Literature Line: 0800 555777
A potentially useful resource for team development, but follows a fairlyrigid sequential set of steps and requires several hours to complete.Not a book to dip into, but a valuable primer for individuals and teamswith time for training. (See also new version, reference 13 below)
2 Rowley J and Bhuhi J. Participatory Needs Assessment: apractical approach in partnerships between local residents and
professionals. Public Health Medicine 1999; 1:27-30
London-based. Strong on public participation. Broad brush scanningtype of approach to tease out environmental, social, economic andpolitical determinants of quality of life.
3 UK Health For All. What is Community Health needs Assessment a Protocol? UK HFA Network, 1993
Community-development orientated approach, long-term perspective.
4 Shanks J, Kheraj S, Fish S. Better ways of assessing healthneeds in primary care. BMJ 1995; 310: 480-1
Short, punchy leader in the BMJ recommended.
5 Murray SA, et al. Listening to local voices: adapting rapidappraisal to assess health and social needs in general practice.BMJ 1994; 308: 698-700
One of the key references in this field recommended.
6 Murray SA, Graham LJC. Practice based health needsassessment: use of four methods in a small neighbourhood. BMJ1995; 310: 1443-8
Highly recommended. Sets out the methods which are used in thisNorfolk resource pack.
7 Wright J, Williams R, Wilkinson JR. Development and importanceof health needs assessment. Br Med J 1998: 316; 1310-3.
First in a series of 6 weekly articles (two more follow below) in the BMJwhich covered the topic.
-
8/14/2019 Norfolk Needs Assessment Toolbox - NPHNF England - 2002
24/24
8 Stevens A, Gillam S. Needs assessment: from theory to practice.Br Med J 1998; 316: 1488-52
9 Wilkinson JR, Murray SA. Assessment in primary care: practicalissues and possible approaches. Br Med J 1998: 316; 1524-8
10 Balding J, Foot G, Regis D. The assessment of health needs atthe community level. Schools Health Education Unit, Exeter 1991.
Sets out the groundbreaking, and still market-leading, needsassessment service in schools. This unit conducts schools surveysand has a wealth of comparative data going back for several years.
11 Health Needs Assessment and the cycle of change (chapter) in:Public Health Practice Resource Pack. DoH 1999, pp 41-44(Copies available from: Strategic Development, DoH - 01908 844584or from www.doh.gov.uk/publichealth.htm
An excellent overview of public health practice. Essential reading forall nurses who practice in the community.
12 Picken C, St Leger S. Assessing Health Needs using the LifeCycle Framework. OUP. 1993
Used by Sarah Kember and team in the schools needs assessment.
13 Harris A. Needs to know a guide to needs assessment forprimary care. Churchill Livingstone. 1997
14 Hooper J, Longworth P. Health Needs assessment workbook.HDA. 2002 Available from: Health Development Agency, PO Box90, Wetherby, Yorkshire LS23 7EX
15 NHSE. Public Health Resource Pack. Out of print, but available
from www.doh.gov.uk/publichealth.htm
16 Pencheon D et al (eds). Oxford Handbook of Public HealthPractice. OUP. 2001
http://www.doh.gov.uk/publichealth.htmhttp://www.doh.gov.uk/publichealth.htm