Noon conference: Intro to Toxicology
52
IM Board IM Board Prep Fun Prep Fun Toxicology Toxicology Kurt Kleinschmidt, MD, Kurt Kleinschmidt, MD, FACEP, FACMT FACEP, FACMT Professor of Professor of Emergency Medicine Emergency Medicine Division Chief & Division Chief & Program Director Program Director Medical Toxicology Medical Toxicology UTSW Medical Center UTSW Medical Center
-
Upload
katejohnpunag -
Category
Health & Medicine
-
view
217 -
download
0
Transcript of Noon conference: Intro to Toxicology

IM Board IM Board Prep FunPrep Fun
Toxicology Toxicology
Kurt Kleinschmidt, MD, Kurt Kleinschmidt, MD,
FACEP, FACMTFACEP, FACMT
Professor of Professor of
Emergency MedicineEmergency Medicine
Division Chief & Division Chief &
Program DirectorProgram Director
Medical ToxicologyMedical Toxicology
UTSW Medical CenterUTSW Medical Center

• Drug overdoseDrug overdose• Hazardous exposure to chemical productsHazardous exposure to chemical products
– Pesticides; heavy metals Pesticides; heavy metals – Household productsHousehold products– Toxic gasesToxic gases– Toxic alcoholsToxic alcohols– Other industrial chemicals Other industrial chemicals
• Drug Abuse management & MRO Drug Abuse management & MRO • EnvenomationsEnvenomations• Food-borne toxins, such as botulism; marine toxins Food-borne toxins, such as botulism; marine toxins
(e.g. paralytic shellfish toxin; ciguatoxin). (e.g. paralytic shellfish toxin; ciguatoxin). • Plants and mushrooms. Plants and mushrooms. • Independent medical examinations Independent medical examinations
Problems Evaluated By ToxicologistsProblems Evaluated By Toxicologists

Board CertificationBoard Certification
• American Board Medical Specialties RecognizedAmerican Board Medical Specialties Recognized• First ABMS exam 2000First ABMS exam 2000• Toxicology is a Dependent “Sub-Board”Toxicology is a Dependent “Sub-Board”
– Emergency Medicine (Administrative)Emergency Medicine (Administrative)– Preventive MedicinePreventive Medicine– PediatricsPediatrics
• Approximately 50 examinees every Approximately 50 examinees every otherother year year• Total Boarded < 400Total Boarded < 400

Which physicians can become Which physicians can become medical toxicologists?medical toxicologists?
• Emergency MedicineEmergency Medicine
• Preventive and Preventive and Occupational MedicineOccupational Medicine
• PediatricsPediatrics
• Internal MedicineInternal Medicine
• Family MedicineFamily Medicine
• PsychiatryPsychiatry
• NeurologyNeurology
> 50%> 50%
> 95%> 95%
North Texas Poison CenterNorth Texas Poison Center
Division of Toxicology ≠ Poison Center(But we do share much)

ToxidromesToxidromes
• Collection of symptoms characteristic for Collection of symptoms characteristic for specific agent groupsspecific agent groups
• Many different agents can cause “a” Many different agents can cause “a” toxidrometoxidrome
• Management of any one toxidrome…Management of any one toxidrome…
– Is the sameIs the same
– No matter the agentNo matter the agent

ToxidromesToxidromesSympathomimeticSympathomimetic Cocaine, Amphetamines, Cocaine, Amphetamines,
Decongestants, CaffeineDecongestants, Caffeine
AnticholinergicAnticholinergic 11stst-Generation antihistamines, -Generation antihistamines, Neuroleptics, Tricyclics Neuroleptics, Tricyclics
CholinergicCholinergic Carbamates, Carbamates, OrganophosphatesOrganophosphates
OpioidOpioid Codeine, Morphine, Codeine, Morphine, HydrocodoneHydrocodone
Sedative-HypnoticSedative-Hypnotic Benzos, Barbs, EthanolBenzos, Barbs, Ethanol
SerotonergicSerotonergic Too many to list…Too many to list…

AdrenalMedulla
EpiEpi NENE
NN
VasoconstrictionVasoconstriction↑↑ Urethral Urethral Sphincter ToneSphincter ToneMydriasisMydriasis
DiaphoresisDiaphoresis MM
α α
TachycardiaTachycardiaVasodilationVasodilationBronchodilationBronchodilationMetabolicMetabolic↓ ↓ K+K+↓ ↓ PO4PO4↓ ↓ pHpH↑↑ GlucoseGlucose↑↑ WBCWBC
ββNENE
NENE
NN
NNAChACh DDiarrhea iarrhea
UUrinationrinationMMiosisiosisBBronchospasmronchospasmBBronchorrhearonchorrheaEEmesismesisLLacrimationacrimationSSalivationalivation
NN
MMAChACh
AChACh
AChACh
AChACh
AChACh
ANSANSParsympatheticParsympatheticSympatheticSympathetic
AnticholinergicsAnticholinergicsHot as a hareHot as a hare HyperthermiaHyperthermia
Mad as a hatterMad as a hatter Delirium / AgitationDelirium / Agitation
Dry as a boneDry as a bone Skin; Muc Membranes DrySkin; Muc Membranes Dry
Red as a beetRed as a beet Skin flushedSkin flushed
TachycardiaTachycardia
Hypoactive Bowel SoundsHypoactive Bowel Sounds
Bladder Urine RetentionBladder Urine Retention
But which are the most
Sensitive?

Anticholinergic vs. SympathomimeticAnticholinergic vs. Sympathomimetic
SympathoSympatho Anti-CholAnti-Chol
HRHR ↑ ↑ ↑ ↑BPBP ↑ ↑ ↑ ↑PupilsPupils ↑ ↑ ↑ ↑MentalMental AgitatedAgitated AgitatedAgitated
BladderBladder Nml Nml Nml or Nml or ↑↑Bowel SoundsBowel Sounds NmlNml Nml or Nml or ↓↓SkinSkin WetWet Dry**Dry**

CholinergicsCholinergicsMuscarinicMuscarinic
““DUMBELS”DUMBELS”• DiarrheaDiarrhea• UrinationUrination• MiosisMiosis• BronchorrheaBronchorrhea• BronchospasmBronchospasm• EmesisEmesis• LacrimationLacrimation• SalivationSalivation
NicotinicNicotinic
““M, T, W, tH, F”M, T, W, tH, F”• MydriasisMydriasis• TremorTremor• WeakWeak• HypertensionHypertension• FasciculationsFasciculations
What agents affect these receptors?What agents affect these receptors?Organophosphates (Insecticides)Organophosphates (Insecticides)Carbamates (Insecticides)Carbamates (Insecticides)Nerve agentsNerve agents

OpioidOpioidThe ToxidromeThe Toxidrome
• Mental status depressedMental status depressed
• MiosisMiosis
• Respirations depressedRespirations depressed
Not always clear…Coingestants…Not always clear…Coingestants…Hypoxic Brain damage may already be presentHypoxic Brain damage may already be presentNarcan is a poor diagnostic toolNarcan is a poor diagnostic tool
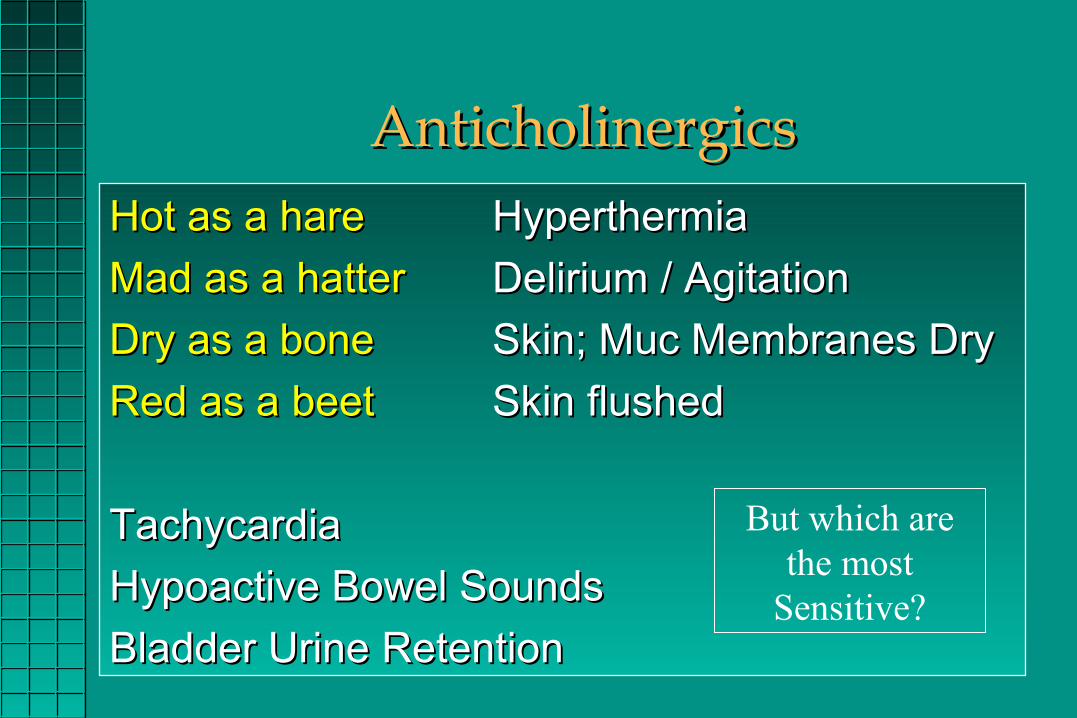
Serotonergic ExcessSerotonergic Excess
Class Drugs
AntidepressantsMonoamine oxidase inhibitors (MAOIs), TCAs, SSRIs, SNRIs, bupropion, nefazodone, trazodone mirtazapine
Opioids tramadol, meperidine, dextromethorphan
CNS stimulants MDMA, MDA, phentermine, methamphetamine, cocaine
5-HT1 agonists triptans
Psychedelics 5-Methoxy-diisopropyltryptamine, LSD

Serotonergic ExcessSerotonergic Excess
• ClinicalClinical– Tremor Tremor
– ↑ ↑ DTRs / ClonusDTRs / Clonus– TachycardiaTachycardia– Agitation or Agitation or
diaphoresisdiaphoresis• Differential DxDifferential Dx
– NMSNMS– LithiumLithium– SympathomimeticsSympathomimetics– Malignant HyperthermiaMalignant Hyperthermia
6 Acetaminophen Cases6 Acetaminophen CasesAll are 40 y/o Males who took 15 grams…All are 40 y/o Males who took 15 grams…
• 2 hrs before arrival2 hrs before arrival– One vomitingOne vomiting– One notOne not
• 8 hrs before arrival8 hrs before arrival– One vomitingOne vomiting– One notOne not
• 15 hrs before arrival15 hrs before arrival
– One vomitingOne vomiting– One notOne not
Start antidote before getting a level?Start antidote before getting a level?PO or IV?PO or IV?Duration of therapy?Duration of therapy?Role of repeat levels?Role of repeat levels?

Acetaminophen Case ContinuedAcetaminophen Case Continued
• 2 hrs before arrival2 hrs before arrival– One vomitingOne vomiting– One notOne not
• 8 hrs before arrival8 hrs before arrival– One vomitingOne vomiting– One notOne not
• 15 hrs before arrival15 hrs before arrival– One vomitingOne vomiting– One notOne not
Start antidote before getting a level?No
PO or IV?If toxic level, go IV
Duration of therapy?If IV, Bolus + 20 hours
Role of repeat levels?None
Start antidote before getting a level?Start antidote before getting a level?PO or IV?PO or IV?Duration of therapy?Duration of therapy?Role of repeat levels?Role of repeat levels?

Acetaminophen Case ContinuedAcetaminophen Case Continued
• 2 hrs before arrival2 hrs before arrival– One vomitingOne vomiting– One notOne not
• 8 hrs before arrival8 hrs before arrival– One vomitingOne vomiting– One notOne not
• 15 hrs before arrival15 hrs before arrival– One vomitingOne vomiting– One notOne not
Start antidote before getting a level?Yes
PO or IV?If Vomiting, go IV If Not Vomiting, go PO (?)
Duration of therapy?If IV, Bolus + 20 hours
If PO, typically 24-36 hrsRole of repeat levels?
None
Start antidote before getting a level?Start antidote before getting a level?PO or IV?PO or IV?Duration of therapy?Duration of therapy?Role of repeat levels?Role of repeat levels?

• If treated within 8 hrsIf treated within 8 hrs– No pts → Liver FailureNo pts → Liver Failure
– Some patients → HepatitisSome patients → Hepatitis
• Toxicity Defined – AST > 1000Toxicity Defined – AST > 1000

Acetaminophen Case ContinuedAcetaminophen Case Continued
• 2 hrs before arrival2 hrs before arrival– One vomitingOne vomiting– One notOne not
• 8 hrs before arrival8 hrs before arrival– One vomitingOne vomiting– One notOne not
• 15 hrs before arrival15 hrs before arrival– One vomitingOne vomiting– One notOne not
Start antidote before getting a level?Yes (?)
PO or IV?If Vomiting, go IV If Not Vomiting, go PO (?)
Duration of therapy?If IV, typically 36 hrs**
If PO, typically 36 hrsRole of repeat levels?
None
Start antidote before getting a level?Start antidote before getting a level?PO or IV?PO or IV?Duration of therapy?Duration of therapy?Role of repeat levels?Role of repeat levels?
Duration based upon LFTs. Note that Acetadote use is likely BEYOND 21 hours

Besides vomiting, conditions Besides vomiting, conditions where IV route is preferred?where IV route is preferred?
PregnancyPregnancyLiver FailureLiver Failure
Lets talk…BioavailabilityLets talk…Bioavailability

LithiumLithium• Your body thinks it is sodium…and treats it as suchYour body thinks it is sodium…and treats it as such• ClinicalClinical
– NeuromuscularNeuromuscular – tremor; ↑ DTRs (very sensitive) – tremor; ↑ DTRs (very sensitive)– Chronic Neuro Sequelae #1 Concern. Chronic Neuro Sequelae #1 Concern.
• Include cerebellar issues; memory deficits, NM weak, personality Include cerebellar issues; memory deficits, NM weak, personality change, tremors. change, tremors.
• DecontaminationDecontamination– Charcoal – No role (like all monovalent cations)Charcoal – No role (like all monovalent cations)– Whole Bowel Irrigation Whole Bowel Irrigation
• Fluids and Electrolytes - Key - Restore volume if there is depletion, Fluids and Electrolytes - Key - Restore volume if there is depletion, otherwise Lithium elimination is slowedotherwise Lithium elimination is slowed
• Dialysis - Dialysis - Ideal for dialysis - (1) small, (2) not protein bound, and (3) small Ideal for dialysis - (1) small, (2) not protein bound, and (3) small volume of distributionvolume of distribution; BUT…Li; BUT…Li++ is mainly intracellular and it diffuses slowly is mainly intracellular and it diffuses slowly across cell membranes (needs serial HD treatments)across cell membranes (needs serial HD treatments)– Indication - Severe neurotoxicity i.e. AMS, those with ARF, Level > 4.0 Indication - Severe neurotoxicity i.e. AMS, those with ARF, Level > 4.0
mEq/L (Acute) or 2.5 mEq/L (Chronic). mEq/L (Acute) or 2.5 mEq/L (Chronic).

Distribution Clinical MomentsDistribution Clinical MomentsLithiumLithium
• Normal Level: 0.6-1.2 mEq/LNormal Level: 0.6-1.2 mEq/L
• Which is clinically worse for a patient?Which is clinically worse for a patient?
– Level 4.2 mEq/LLevel 4.2 mEq/L
– Level 2.2 mEq/LLevel 2.2 mEq/L
It all depends…It all depends…Acute vs Chronic ExposureAcute vs Chronic ExposureAgent with slow distributionAgent with slow distribution

Distribution Clinical MomentsDistribution Clinical Moments - Lithium - Lithium
FastFast
SlowSlow
Stomach and IntestinesStomach and Intestines
Blood and Blood and some organs (Liver)some organs (Liver)
BrainBrain
AcuteAcute ChronicChronic
4.24.2 2.22.2
0.20.2 2.22.2
AbsorptionAbsorption
DistributionDistribution

Common SalicylatesCommon Salicylates
Alka-Seltzer
Alka-Seltzer
AnacinAnacin
ExcedrinExcedrin
Bismuth subsalicylate Bismuth subsalicylate (Pepto Bismol)(Pepto Bismol)
Cold Cold PreparationsPreparations
AspirinAspirin
KeratolyticKeratolyticAgentsAgents
Oil of Oil of WintergreenWintergreen

Clinical Signs and SymptomsClinical Signs and Symptoms
Salicylate Toxidrome (Acute)Salicylate Toxidrome (Acute)• Shortness of Breath (Hyperpnea, Tachypnea)Shortness of Breath (Hyperpnea, Tachypnea)• N/V & stomach upsetN/V & stomach upset• Tinnitus and/or Hearing changeTinnitus and/or Hearing change• DizzyDizzy• DiaphoresisDiaphoresis
My great clinical moment…My great clinical moment…
Can be easy to miss

More Clinical Signs and SymptomsMore Clinical Signs and Symptoms• CNSCNS
– AMS (Cerebral edema, Hypoglycemia)AMS (Cerebral edema, Hypoglycemia)– SeizuresSeizures
• HyperthermiaHyperthermia
• Non-Cardiogenic Pulmonary EdemaNon-Cardiogenic Pulmonary Edema
• Metabolic Acidosis & Resp AlkalosisMetabolic Acidosis & Resp Alkalosis
• CoagulopathyCoagulopathy
• Liver failureLiver failure
• Renal failureRenal failure
Multiorgan!Multiorgan!
Often confused with Sepsis Often confused with Sepsis and/or other conditionsand/or other conditions

LaboratoryLaboratory
• Anion-Gap Metabolic AcidosisAnion-Gap Metabolic Acidosis• Plasma Salicylate LevelsPlasma Salicylate Levels
– Serial levelsSerial levels – Useless without clinical courseUseless without clinical course
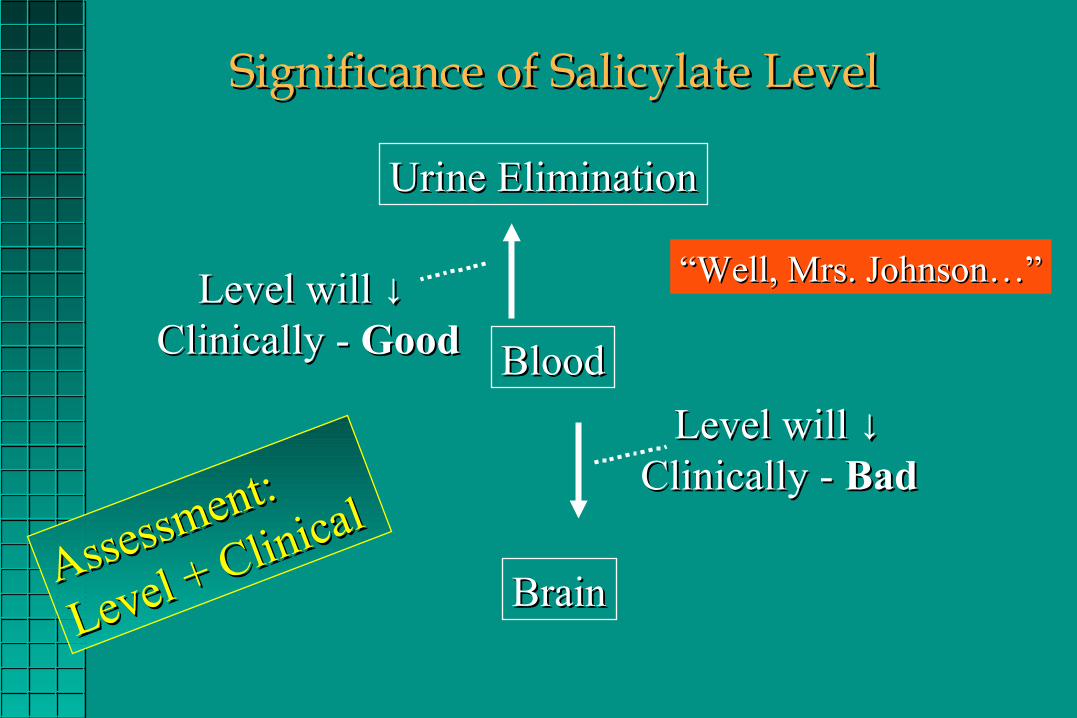
Significance of Salicylate LevelSignificance of Salicylate Level
Urine EliminationUrine Elimination
BloodBlood
BrainBrain
Level will Level will ↓↓ Clinically - Clinically - GoodGood
Level will Level will ↓↓Clinically - Clinically - BadBad
Assessment:
Assessment:
Level + Clinical
Level + Clinical
““Well, Mrs. Johnson…”Well, Mrs. Johnson…”
TreatmentTreatment
• Absorption:Absorption: CharcoalCharcoal → ↓ → ↓ AbsorptionAbsorption
• Distribution: Distribution: Not a targetNot a target
• Metabolism and EliminationMetabolism and Elimination
– Multidose Activated CharcoalMultidose Activated Charcoal
– Ion Trapping (Sodium Bicarbonate)Ion Trapping (Sodium Bicarbonate)
– HemodialysisHemodialysis

Ion TrappingIon Trapping
Brain BloodRenal Tubule
HA HA ↑ ↓↑ ↓
HH+ + + A+ A--
Diurese it outDiurese it out
HA HA ↑ ↓↑ ↓
HH+ + + A+ A--
HA HA ↑ ↓↑ ↓
HH+ + + A+ A--

Ion TrappingIon Trapping
Brain BloodRenal Tubule
HA HA ↑ ↑ ↓↓
HH+ + + A+ A--
Diurese it outDiurese it out
HA HA ↑↑ ↓ ↓
HH+ + + A+ A--
HA HA ↑↑ ↓ ↓
HH+ + + A+ A--
A weak acid in an alkaline environmentA weak acid in an alkaline environmentAlkalinize the urineAlkalinize the urine
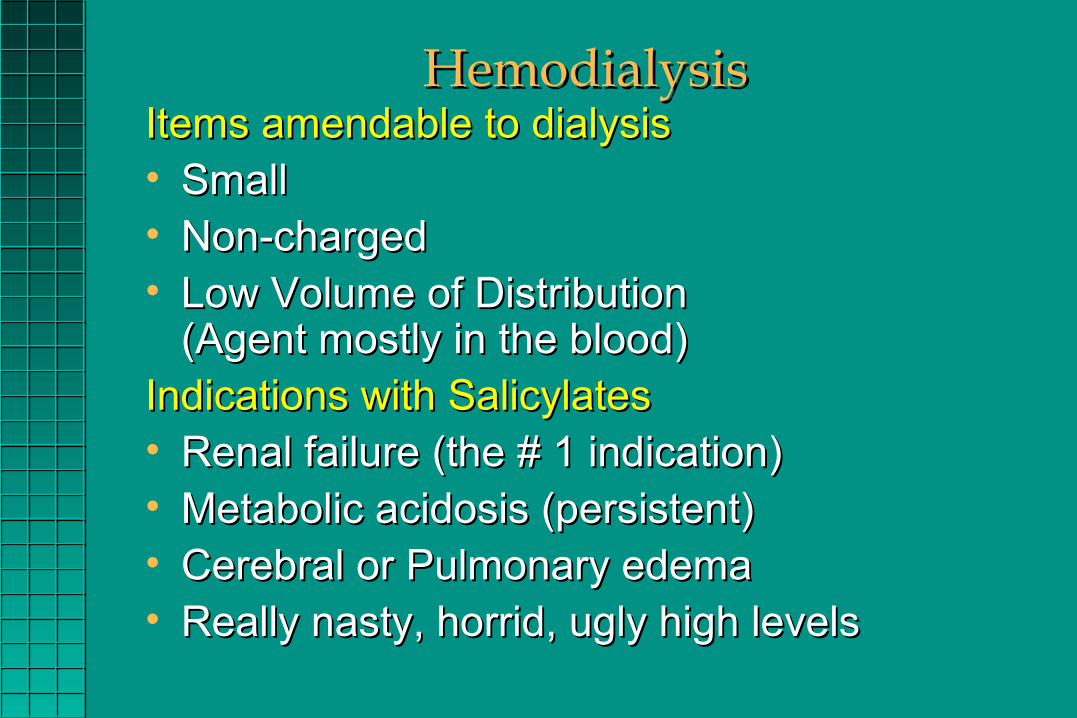
HemodialysisHemodialysisItems amendable to dialysisItems amendable to dialysis• SmallSmall• Non-chargedNon-charged• Low Volume of Distribution Low Volume of Distribution
(Agent mostly in the blood)(Agent mostly in the blood)Indications with SalicylatesIndications with Salicylates• Renal failure (the # 1 indication)Renal failure (the # 1 indication)• Metabolic acidosis (persistent)Metabolic acidosis (persistent)• Cerebral or Pulmonary edemaCerebral or Pulmonary edema• Really nasty, horrid, ugly high levelsReally nasty, horrid, ugly high levels
Pitfalls in Salicylate Management Pitfalls in Salicylate Management • Failure to be scaredFailure to be scared• Failure to know that symptoms Failure to know that symptoms
can be delayedcan be delayed• Ruling out toxicity using Ruling out toxicity using
serum level alone serum level alone • Failure to alkalinize the urine due Failure to alkalinize the urine due
to inadequate K+ levelto inadequate K+ level• Failure to Dialyze in the really Failure to Dialyze in the really
sick ones!!!!!!!!!!!!!!!!!!!!!!!!!sick ones!!!!!!!!!!!!!!!!!!!!!!!!!
Continue therapy until Continue therapy until symptoms are gonesymptoms are gone
• Sodium Bicarb Sodium Bicarb for Ion Trappingfor Ion Trapping
• Multiple Dose Multiple Dose Activated Activated
CharcoalCharcoal

CyanideCyanide• Cyanide Salts: Ingest Cyanide Salts: Ingest → → CN-salt + stomach Acid CN-salt + stomach Acid →→
HCN HCN →→ Absorbed Absorbed →→ Die Die• HCN Gas: HCN Gas: Inhale Inhale →→ Mucosal absorption Mucosal absorption →→ Die Die
Burn...Burn...Plastics (Polyacrylonitriles, Polyacrylamides)Plastics (Polyacrylonitriles, Polyacrylamides)Foam (Polyurethane)Foam (Polyurethane)Varnishes and Paints (Polyurethane)Varnishes and Paints (Polyurethane)Wool and SilkWool and Silk
FireFire
Smoke Smoke with with HCNHCN
Formed when combine an acid with the salt; thus keep pH high, no gas will be created

Cyanide PathophysiologyCyanide Pathophysiology
Binds ferric ion in Binds ferric ion in Cytochrome Cytochrome OxidaseOxidase
CNCNCyt a3++Cyt a3++Cyt a3+++Cyt a3+++
OO22 2H2H22OO
Oxidative Oxidative PhosphorylationPhosphorylation
X
X
Can NOT use OCan NOT use O22
CNSCNSLOCLOCSeizuresSeizures
Body Ischemia Body Ischemia Severe Met acidosisSevere Met acidosis

Cyanide DiagnosisCyanide Diagnosis
HistoryHistoryLaboratoryLaboratory• Cyanide LevelCyanide Level: : Back next weekBack next week• Lactate:Lactate: Back next hourBack next hour

Cyanide DiagnosisCyanide Diagnosis
Blood GasBlood Gas• Supporting CNSupporting CN
– Severe metabolic acidosis*****Severe metabolic acidosis*****– Arterial-venous OArterial-venous O22 gradient gradient ↓ ↓ (?) (?)
– Venous OVenous O22 ↑↑ (?) (?)
• Smoke “clouds” the picture Smoke “clouds” the picture – Hypoxia…Hypoxia… AsphyxiantsAsphyxiants Pulmonary irritants Pulmonary irritants
COCO CN CN – Lactate…Lactate… Hypoxia Hypoxia Hypoperfusion Hypoperfusion
Severe Met Acidosis (Tox Related)Inhibitors / Uncouples Oxid PhosphToxic Alcohols
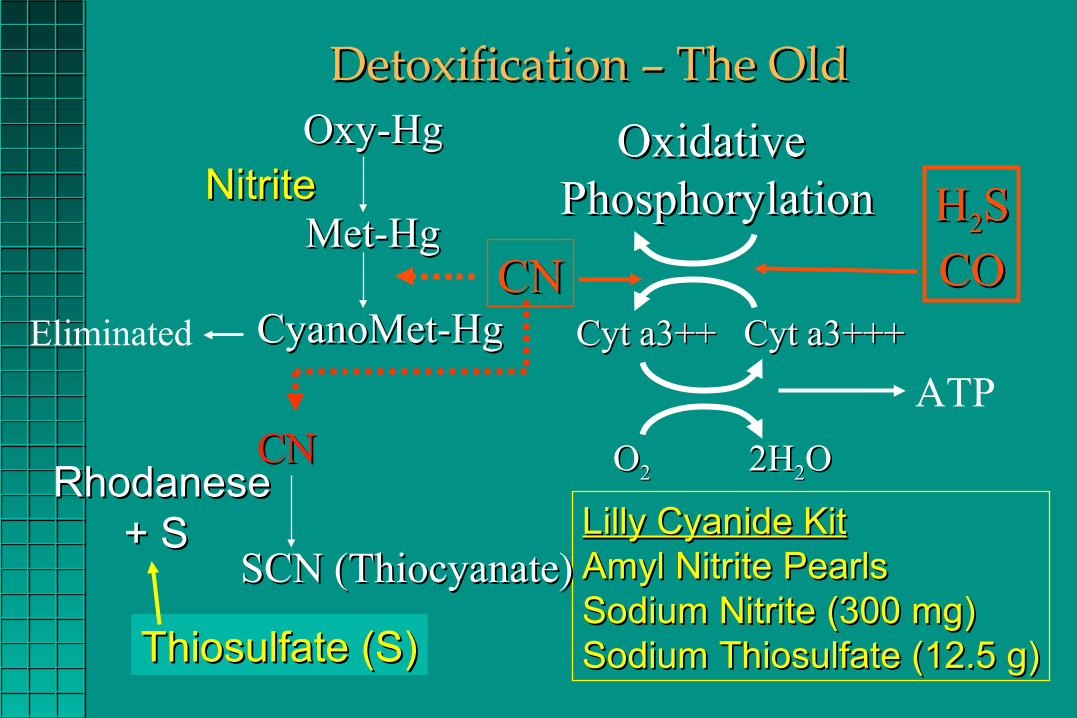
Detoxification – The OldDetoxification – The Old
CNCN
HH22SS
COCO
NitriteNitrite
Thiosulfate (S)Thiosulfate (S)
Lilly Cyanide KitLilly Cyanide KitAmyl Nitrite PearlsAmyl Nitrite PearlsSodium Nitrite (300 mg)Sodium Nitrite (300 mg)Sodium Thiosulfate (12.5 g)Sodium Thiosulfate (12.5 g)
Cyt a3++Cyt a3++ Cyt a3+++Cyt a3+++
OO22 2H2H22OO
Oxidative Oxidative PhosphorylationPhosphorylation
Oxy-HgOxy-Hg
Met-HgMet-Hg
CyanoMet-HgCyanoMet-Hg
CNCN RhodaneseRhodanese + S+ S
SCN (Thiocyanate)SCN (Thiocyanate)
Eliminated
ATP

NitritesNitritesSide Effects Side Effects
– Vasodilation Vasodilation →→ Hypotension Hypotension– MethemoglobinemiaMethemoglobinemia →→ ↓↓OO22 Carrying Capacity Carrying Capacity
• Create a “toxicity” to cure another “toxicity”Create a “toxicity” to cure another “toxicity”• Another issue in smoke inhalation setting Another issue in smoke inhalation setting
Carbon Monoxide also Carbon Monoxide also →→ “Dys-hemoglobinemia” “Dys-hemoglobinemia”
→→ ↓↓OO22 Carrying Capacity Carrying Capacity
Sodium Thiosulfate Sodium Thiosulfate is quite benignis quite benign
NormalHemoglobin

HydroxocobalaminHydroxocobalaminfor for
CyanideCyanide(CN)(CN)

Recycling of HydroxycobalaminRecycling of Hydroxycobalamin
CobalaminCobalamin
OHOH
CNCN
CNCN
CobalaminCobalamin OHOH--++ ++(Vitamin B(Vitamin B1212))
HH++
CNCN
CobalaminCobalamin ThiosulfateThiosulfate CobalaminCobalamin
OHOH
ThiocyanateThiocyanateRhodanaseRhodanaseHH22OO
++ ++++++(Vitamin B(Vitamin B1212))

Alcohols that in significant amounts Alcohols that in significant amounts typically cause specific end organ typically cause specific end organ damage if not managed appropriatelydamage if not managed appropriately
Toxic AlcoholsToxic AlcoholsDefinedDefined
These include:These include:
• Ethylene GlycolEthylene Glycol
• MethanolMethanol
Do NOT include:Do NOT include:
• IsopropanolIsopropanol
• EthanolEthanol

Alcohol DehydrogenaseAlcohol Dehydrogenase
Aldehyde DehydrogenaseAldehyde Dehydrogenase
Metabolism of Ethylene GlycolMetabolism of Ethylene Glycol
PyridoxinePyridoxine
ThiamineThiamine
GlycineGlycine
OxalateOxalate
FormateFormate
αα-Hydroxy- -Hydroxy- ββ-Ketoadipate-Ketoadipate
GlyoxylateGlyoxylate
Ethylene glycolEthylene glycol
GlycoaldehydeGlycoaldehyde
GlycolateGlycolate

FolateFolate
AlcoholAlcohol DehydrogenaseDehydrogenase
Metabolism of Metabolism of MethanolMethanolMethanolMethanol
FormaldehydeFormaldehyde
FormateFormate
COCO22 + H + H22OO

The IssuesThe Issues
• Ethylene GlycolEthylene Glycol ARFARF
• MethanolMethanol BlindnessBlindness
• IsopropanolIsopropanol Tummy upsetTummy upset
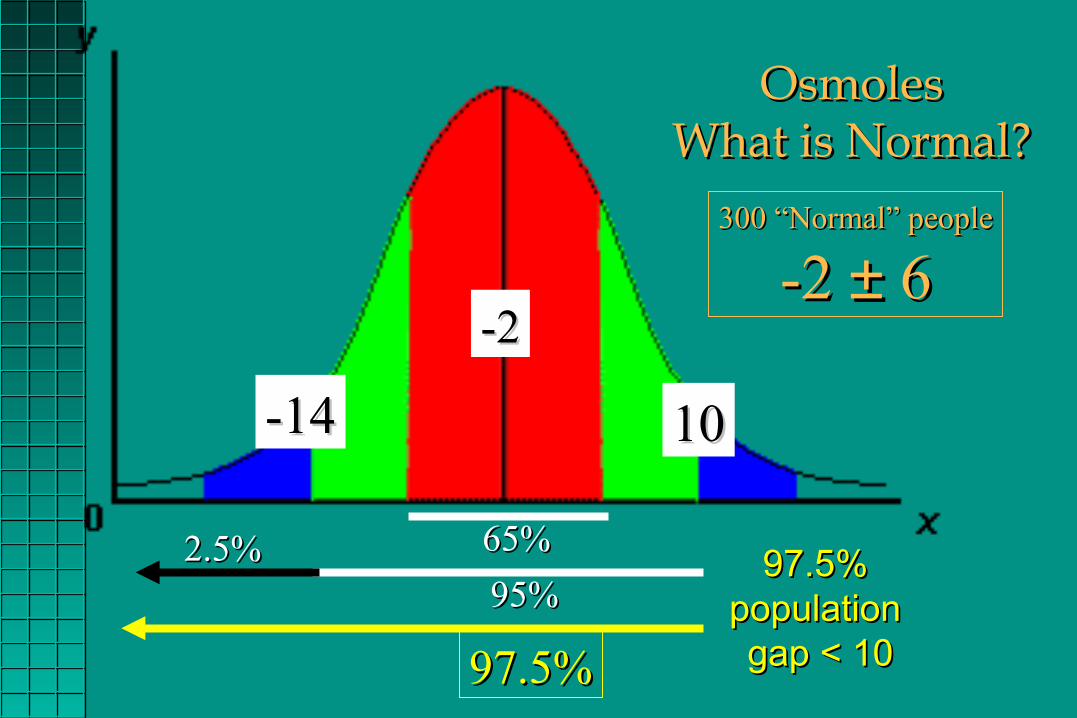
OsmolesOsmolesWhat is Normal?What is Normal?
65%65%
-2-2
300 “Normal” people300 “Normal” people
-2 -2 ±± 6 6
95%95%
1010-14-14
2.5%2.5%
97.5%97.5%
97.5% 97.5% population population gap < 10gap < 10

ManagementManagement
Ethylene GlycolEthylene Glycol
GlycoaldehydeGlycoaldehyde
MethanolMethanol
FormaldehydeFormaldehyde
Alcohol DehydrogenaseAlcohol Dehydrogenase
EthanolFomepizole

ManagementManagement Hemodialysis Hemodialysis
• SymptomaticSymptomatic
• Significant metabolic acidosis (?)Significant metabolic acidosis (?)
– pH < 7.1pH < 7.1
– One that can’t easily correct One that can’t easily correct
• Ethylene glycol or methanol levels Ethylene glycol or methanol levels
– > 25 mg/dL > 25 mg/dL
– > 50 mg/dL> 50 mg/dL
• Renal compromiseRenal compromise
?
Indications:
Symptomspresent
Often done Often done after symptoms after symptoms have begunhave begun

Sodium BicarbonateSodium Bicarbonate
For TCAs and Other For TCAs and Other Sodium Channel Blockers Sodium Channel Blockers
•It’s the It’s the sodiumsodium that counts that counts
•Boluses (Boli?) – the way to goBoluses (Boli?) – the way to go
•You follow your “efficacy” thru – QRS!!!You follow your “efficacy” thru – QRS!!!
•QRS corrects rapidly (minutes)QRS corrects rapidly (minutes)

• The big questions – Is there a correlation between…The big questions – Is there a correlation between…– QRS ≥ 100 ms & TCA concentration > 1000 ng/mLQRS ≥ 100 ms & TCA concentration > 1000 ng/mL
– Development of seizures or Development of seizures or ventricular dysrhythmias and ventricular dysrhythmias and • QRS ≥ 100 ms QRS ≥ 100 ms • TCA concentration > 1000 ng/mL TCA concentration > 1000 ng/mL
NEJM 1985313:474-9

Figure 1Figure 1Correlation between the Correlation between the max Limb Lead QRS max Limb Lead QRS Duration and the Duration and the Occurrence of Seizures of Occurrence of Seizures of Ventricular Arrhythmias.Ventricular Arrhythmias.Each circle denotes 1 of the Each circle denotes 1 of the 49 study patients.49 study patients.
Vs. Sodium Bicarbonate Vs. Sodium Bicarbonate with Salicylateswith Salicylates
• It’s the bicarbonate that countsIt’s the bicarbonate that counts
• Done as an infusion.Done as an infusion.
• You will cause hypokalemiaYou will cause hypokalemia
• You monitor “efficacy” via – urine pH You monitor “efficacy” via – urine pH (want it high to trap)(want it high to trap)



![TOXICOLOGY CENTRE SELF-ASSESSMENT DOCUMENT Assessment_Report... · toxicopathology, inorganic biogeochemistry [later changed to analytical toxicology], and contaminant fate ... Toxicology](https://static.fdocuments.us/doc/165x107/5b42ffd97f8b9ab15f8b94bd/toxicology-centre-self-assessment-document-assessmentreport-toxicopathology.jpg)