NONPRESCRIPTION NICOTINE REPLACEMENT THERAPY. is the chief, single, avoidable cause of death in our...
65
NONPRESCRIPTION NICOTINE REPLACEMENT THERAPY
-
Upload
shonda-watts -
Category
Documents
-
view
214 -
download
0
Transcript of NONPRESCRIPTION NICOTINE REPLACEMENT THERAPY. is the chief, single, avoidable cause of death in our...

NONPRESCRIPTION NICOTINEREPLACEMENT THERAPY
is the chief, single, avoidable cause of death
in our society and the most important public health issue of our time.”
C. Everett Koop, M.D., former U.S. Surgeon General
“CIGARETTE SMOKING…
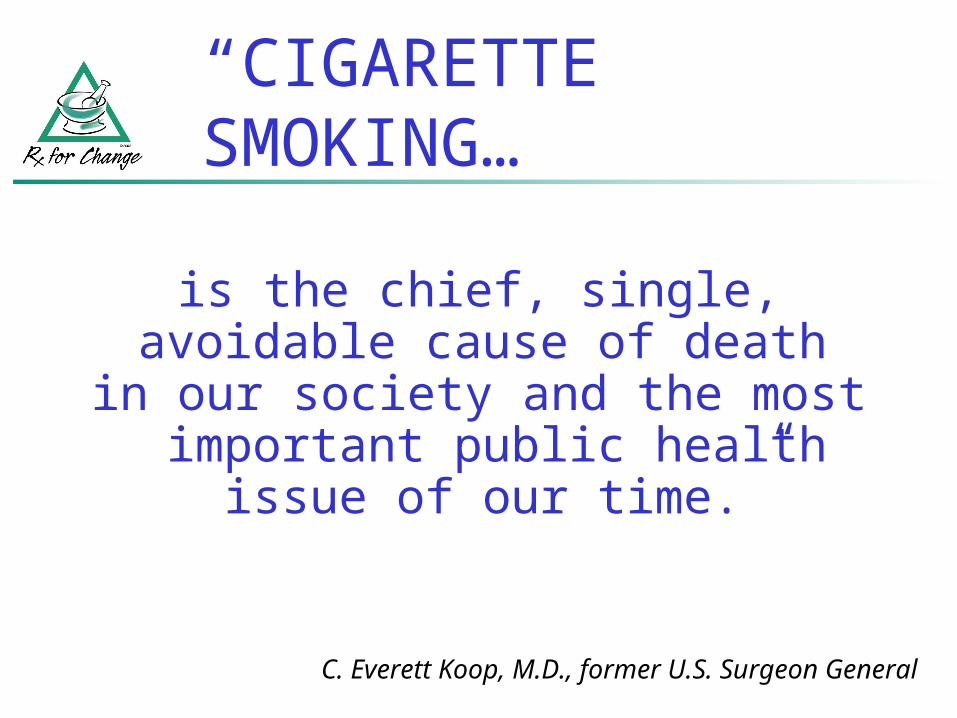
Adapted from NCI Smoking and Tobacco Control Monograph 8, 1997, p. 13. Data from U.S. Department of Agriculture.
Reprinted with permission. Thun et al. Oncogene 2002;21:7307–7325.
0
2
4
6
8
10
12
14
1880 1890 1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000
Year
Po
un
ds
of
tob
ac
co
pe
r c
ap
ita
Cigarettes
Cigars
Chewing tobacco
Snuff
Pipe/roll your own
ADULT PER CAPITA CONSUMPTION OF TOBACCO, 1880-2000
All forms of tobacco
are harmful
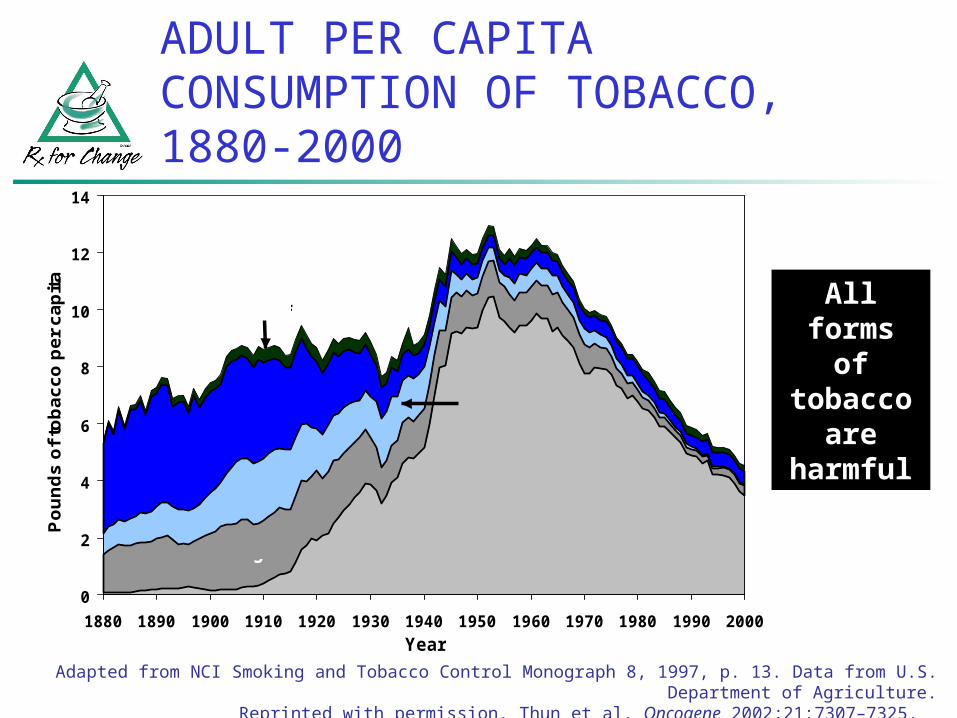
TRENDS in ADULT SMOKING, by SEX—U.S., 1955–2002
Trends in cigarette current smoking among persons aged 18 or older, by sex
0
10
20
30
40
50
60
1955 1959 1963 1967 1971 1975 1979 1983 1987 1991 1995 1999
Year
Graph provided by the Centers for Disease Control and Prevention. 1955 Current Population Survey; 1965–2001 NHIS. Estimates since 1992 include some-day smoking.
Male
Female
Perc
en
t
25.2%
20.0%
70% want to quit70% want to quit
22.5% of adults are
current smokers
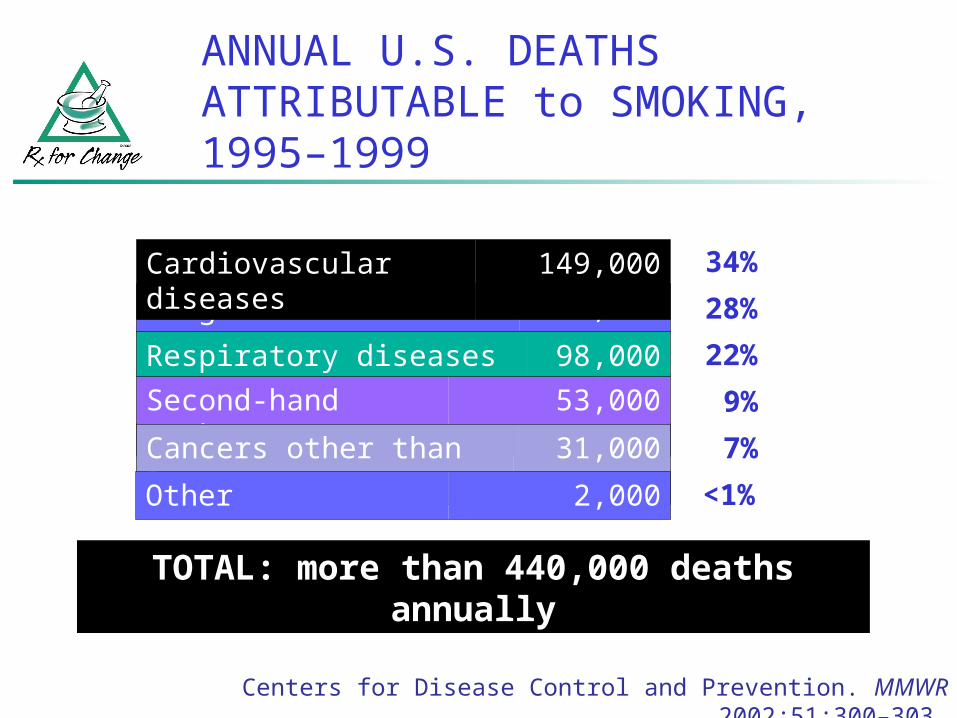
ANNUAL U.S. DEATHS ATTRIBUTABLE to SMOKING, 1995–1999
Centers for Disease Control and Prevention. MMWR 2002;51:300–303.
Second-hand smoke 53,000
Respiratory diseases 98,000
Cancers other than lung 31,000
Lung cancer 125,000
Cardiovascular diseases 149,000
Other 2,000
34%
28%
22%
9%
7%
<1%
TOTAL: more than 440,000 deaths annually
2004 REPORT of the SURGEON GENERAL
Smoking harms nearly every organ of the body, causing many diseases and reducing the health of smokers in general.
Quitting smoking has immediate as well as long-term benefits, reducing risks for diseases caused by smoking and improving health in general.
Smoking cigarettes with lower machine-measured yields of tar and nicotine provides no clear benefit to health.
Numerous diseases are caused by smoking.U.S. Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General, 2004.
FOUR MAJOR CONCLUSIONS
HEALTH CONSEQUENCES of SMOKING
Cancers Lung Laryngeal, pharyngeal, oral
cavity, esophagus Pancreatic Bladder and kidney Cervical and endometrial Gastric Acute myeloid leukemia
Reduce fertility in women, poor pregnancy outcomes, low birth weight babies, sudden infant death syndrome
Cardiovascular diseases Subclinical atherosclerosis Coronary heart disease Stroke Abdominal aortic aneurysm
Respiratory diseases Acute respiratory illnesses,
e.g., pneumonia Chronic respiratory
diseases, e.g., COPD
Cataract
Periodontitis
U.S. Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General, 2004.

CAUSALLY ASSOCIATED HEALTH RISKS of SECOND-HAND SMOKE
Developmental effects Fetal growth retardation, SIDS
Carcinogenic effects Lung cancer, nasal sinus cancer
Cardiovascular effects Heart disease mortality, acute and chronic CHD morbidity
Respiratory effects Children: acute lower respiratory tract infections,
asthma induction and exacerbation, chronic respiratory symptoms, middle ear infections
Adults: eye and nasal irritation
National Cancer Institute. Health Effects of Exposure to Environmental Tobacco Smoke: The Report of the California Environmental Protection
Agency, 1999.
EVEN A LITTLE SECOND-
HAND SMOKE IS
DANGEROUS

SMOKE-FREE WORKPLACE LAWS
Smoke-free offices, restaurants, and bars:Delaware, California, Connecticut, Maine, Massachusetts, New York, Rhode Island Smoke-free offices and restaurants: Florida, Idaho, Vermont, UtahSmoke-free offices: Maryland
Exposure to second-hand smoke increases the risk of myocardial
infarction.

ANNUAL SMOKING-ATTRIBUTABLE ECONOMIC COSTS—U.S., 1995–1999
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85
Annual lost productivity
costs (1995–1999)
Medical expenditures
(1998)
Billions of dollars
Men, $55.4 billion
Ambulatory care, $27.2 billion
Prescription
drugs, $6.4
billion
Women, $26.5 billion
Nursing home,
$19.4 billion
Other care, $5.4 billion
Centers for Disease Control and Prevention. MMWR 2002;51:300–303.
Hospital care, $17.1 billion
Societal costs: $7.18 per pack
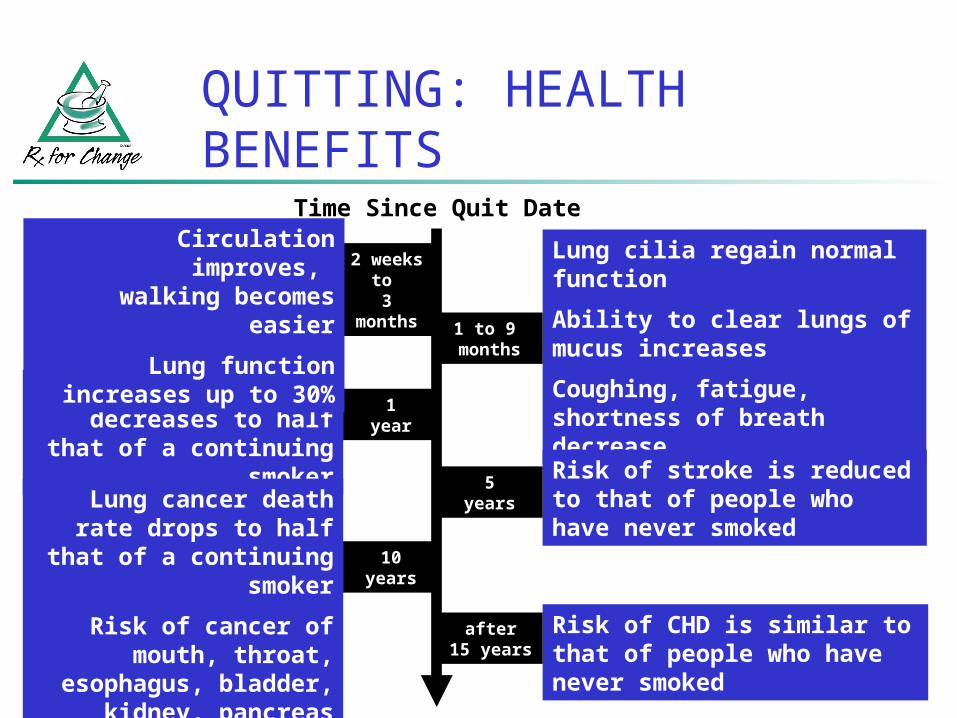
QUITTING: HEALTH BENEFITS
Lung cilia regain normal function
Ability to clear lungs of mucus increases
Coughing, fatigue, shortness of breath decrease
Excess risk of CHD decreases to half that of a
continuing smokerRisk of stroke is reduced to that of people who have never smoked
Lung cancer death rate drops to half that of a
continuing smoker
Risk of cancer of mouth, throat, esophagus,
bladder, kidney, pancreas decrease
Risk of CHD is similar to that of people who have never smoked
2 weeks to
3 months
1 to 9 months
1year
5years
10years
after15 years
Time Since Quit Date Circulation improves,
walking becomes easier
Lung function increases up to 30%

Released June 2000
Sponsored by the AHRQ (Agency for Healthcare Research and Quality) of the USPHS (US Public Heath Service) with:
CDC (Centers for Disease Control) NCI (National Cancer Institute) NIDA (National Institute for Drug
Addiction) NHLBI (National Heart Lung & Blood
Institute) RWJF (Robert Wood Johnson Foundation)
http://www.surgeongeneral.gov/tobacco/
CLINICAL PRACTICE GUIDELINE for TREATING TOBACCO USE and DEPENDENCE

ASK
ADVISE
ASSESS
ASSIST
ARRANGE
The 5 A’s
The 5 A’s (cont’d)
Ask about tobacco use “Do you ever smoke or use any type of tobacco?”
“I take time to ask all of my patients about tobacco use—because it’s important.”
ASK
The 5 A’s (cont’d)
tobacco users to quit (clear, strong, personalized, sensitive) “It’s important that you quit as soon as possible,
and I can help you.”
“I realize that quitting is difficult. It is the most important thing you can do to protect your health now and in the future. I have training to help my patients quit, and when you are ready, I will work with you to design a specialized treatment plan.”
ADVISE
The 5 A’s (cont’d)
Assess readiness to make a quit attemptASSESS
Assist with the quit attemptASSIST

Arrange follow-up careARRANGE
The 5 A’s (cont’d)
Number of sessions
Estimated quit rate*
0 to 1 12.4%
2 to 3 16.3%
4 to 8 20.9%
More than 8 24.7%* 5 months (or more)
postcessation
Fiore et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, 2000.
PROVIDE ASSISTANCE THROUGHOUT THE QUIT PROVIDE ASSISTANCE THROUGHOUT THE QUIT ATTEMPTATTEMPT

THE 5 A’s: REVIEW
ASK about tobacco USE
ADVISE tobacco users to QUIT
ASSESS readiness to make a QUIT attempt
ASSIST with the QUIT ATTEMPT
ARRANGE FOLLOW-UP care
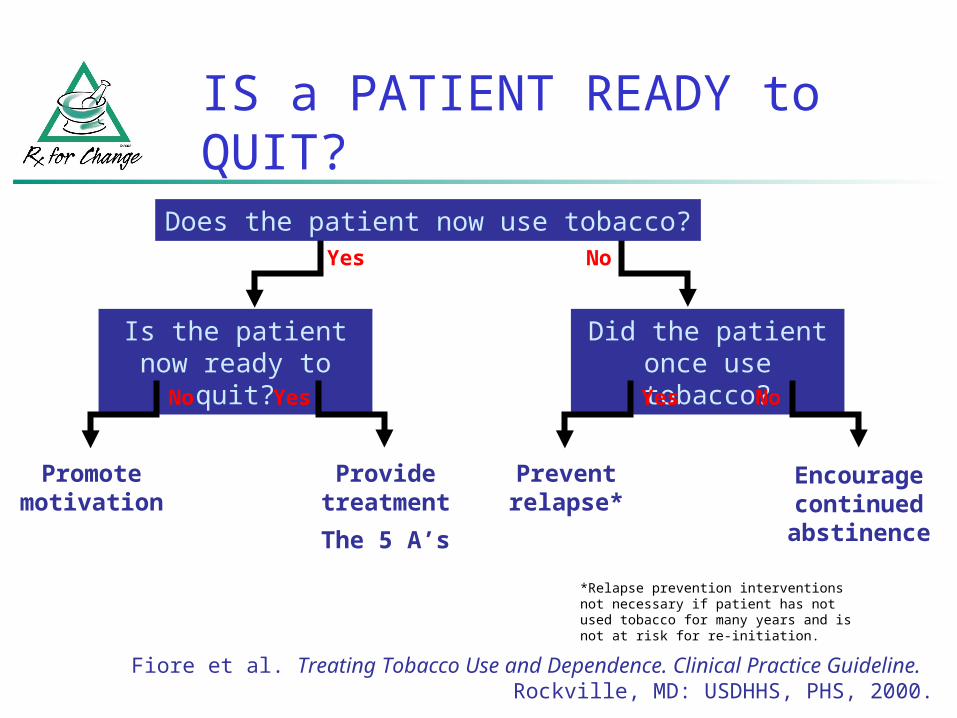
IS a PATIENT READY to QUIT?Does the patient now use tobacco?
Is the patient now ready to quit?
Provide treatment
The 5 A’s
Promote motivation
Yes
YesNo
Did the patient once use tobacco?
Prevent relapse*
Encourage continued abstinence
Yes
No
No
*Relapse prevention interventions not necessary if patient has not used tobacco for many years and is not at risk for re-initiation.
Fiore et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, 2000.
PHARMACOTHERAPY
“All patients attempting to quit should be encouraged to use effective pharmacotherapies for cessation except in the
presence of special circumstances.”
Fiore et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, 2000.

PHARMACOLOGIC METHODS:
FIRST-LINE THERAPIES
Two general classes of FDA-approved drugs for cessation:
1. Nicotine replacement therapy
Nicotine gum, patch, lozenge, nasal spray, inhaler
2. Psychotropics
Sustained-release bupropion
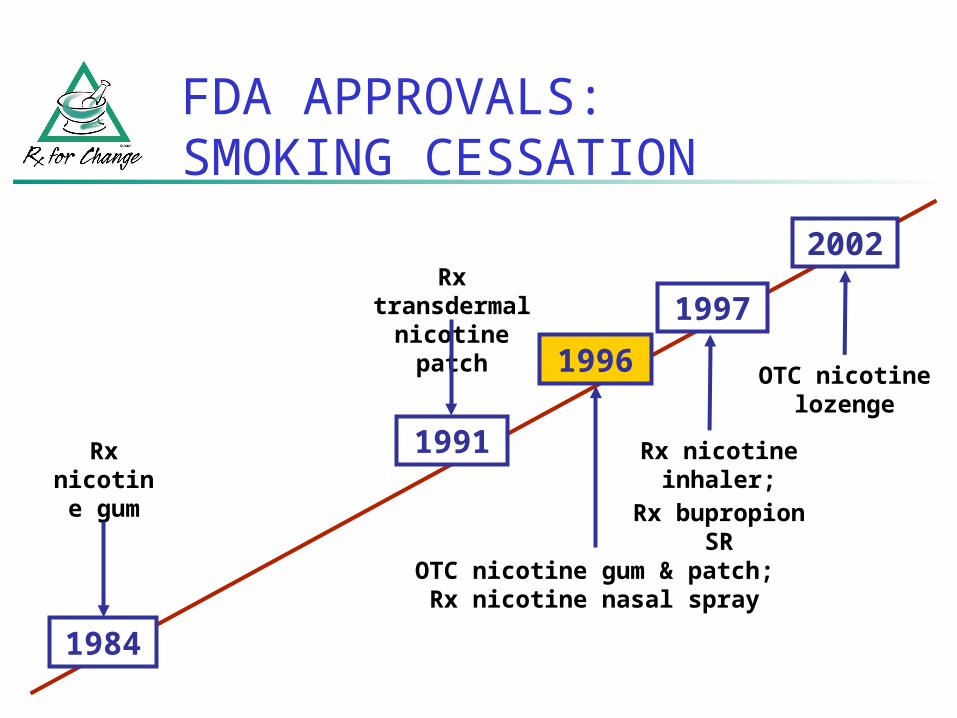
FDA APPROVALS: SMOKING CESSATION
1984
Rx nicotine
gum
1991
Rx transdermal
nicotine patch1996
OTC nicotine gum & patch;Rx nicotine nasal spray
1997
Rx nicotine inhaler;
Rx bupropion SR
2002
OTC nicotine lozenge
NRT: RATIONALE for USE
Reduces physical withdrawal from nicotine
Allows patient to focus on behavioral and psychological aspects of tobacco cessation
IMPROVES SUCCESS RATESIMPROVES SUCCESS RATES

Anger/irritability
Anxiety
Cravings
Difficulty concentrating
Hunger/weight gain
Impatience
Restlessness
Drowsiness
Fatigue
Impaired task performance
Nervousness
Sleep disturbances
SYMPTOMS of NICOTINE WITHDRAWAL
Hughes et al. Arch Gen Psychiatry 1991;48:52–59.
Polacrilex Gum Nicorette (OTC) Generic nicotine gum
(OTC)
Lozenge Commit (OTC)
Transdermal Patches Nicoderm CQ (OTC) Nicotrol (OTC) Generic nicotine patches
(OTC, Rx)
Nasal Spray Nicotrol NS (Rx)
Inhaler Nicotrol (Rx)
NRT: PRODUCTS

PLASMA NICOTINE CONCENTRATIONS for NICOTINE-CONTAINING PRODUCTS
0
5
10
15
20
25
1/0/1900 1/10/1900 1/20/1900 1/30/1900 2/9/1900 2/19/1900 2/29/1900
Pla
sma
nic
oti
ne
(mcg
/L)
Cigarette
Moist snuff
Nasal spray
Inhaler
Lozenge (2mg)
Gum (2mg)
Patch
0 10 20 30 40 50 60
Time (minutes)
Cigarette
Moist snuff

NRT: PRECAUTIONS
Patients with underlying cardiovascular disease
Recent myocardial infarction
Life-threatening arrhythmias
Severe or worsening angina
NRT: PRECAUTIONS (cont’d)
Patients with other underlying conditions
Active temporomandibular joint disease (gum only)
Pregnancy
Lactation
Minimum age for FDA-approved NRT use: 18 years

NICOTINE GUM: Nicorette; generic (GlaxoSmithKline; Watson Labs)
Approved for Rx use in 1984; OTC in 1996
Resin complex Nicotine Polacrilin
Sugar-free chewing gum base
Buffering agents to enhance buccal absorption of nicotine
Available: 2 mg, 4 mg; regular, mint, orange

NICOTINE GUM: DOSING
Dosage based on current smoking patterns:If patient smokes Recommended
strength
25 cigarettes/day 4 mg
<25 cigarettes/day 2 mg
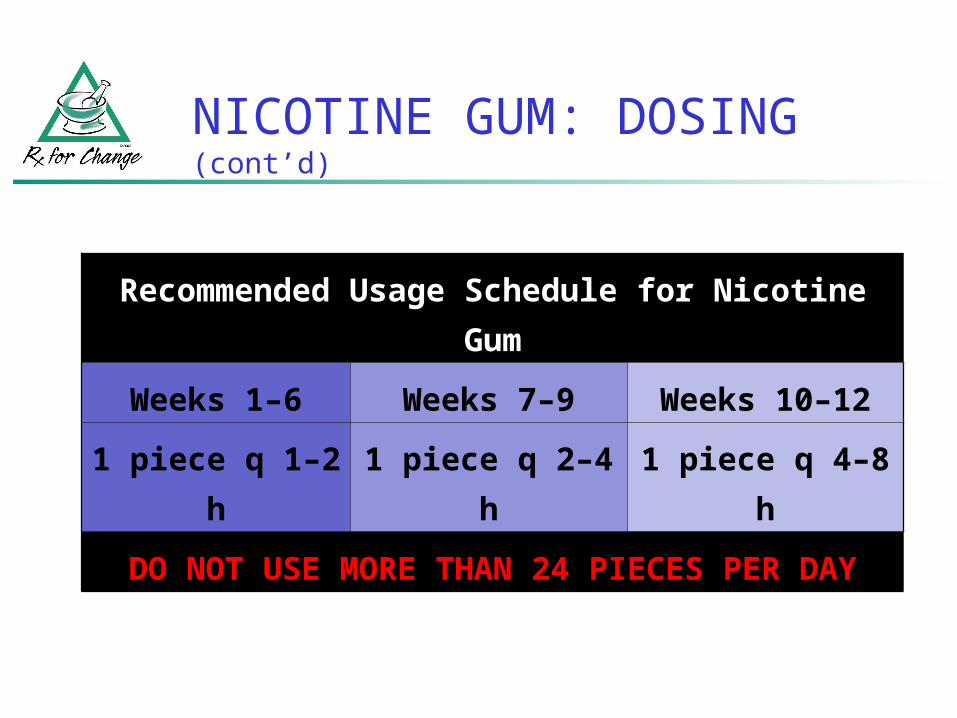
NICOTINE GUM: DOSING (cont’d)
Recommended Usage Schedule for Nicotine
Gum
Weeks 1–6 Weeks 7–9 Weeks 10–12
1 piece q 1–2
h
1 piece q 2–4
h
1 piece q 4–8
h
DO NOT USE MORE THAN 24 PIECES PER
DAY
NICOTINE GUM:
DIRECTIONS for USE
Use gum according to recommended dosing schedule (to decrease cravings & withdrawal symptoms)
Chew each piece very slowly several times
Stop chewing at first sign of peppery, minty, or citrus taste or of slight tingling in mouth (~15 chews, but varies)
“Park” gum between cheek & gum (to allow absorption of nicotine across buccal mucosa)
NICOTINE GUM:
DIRECTIONS for USE (cont’d)
Resume slow chewing when taste or tingle fades
When taste or tingle returns, stop and park gum in different place in mouth
Repeat chew/park steps until most of the nicotine is gone (taste or tingle does not return; generally 30 minutes)

NICOTINE GUM:
CHEWING TECHNIQUE SUMMARY
Park
Stop chewing at first sign of peppery, minty, or citrus taste or tingle
Chew slowly
Chew again when the taste or tingle fades

NICOTINE GUM:GRADUAL REDUCTION of DOSE
Recommended strategies for discontinuing use of nicotine gum:
Chew gum for 10–15 minutes instead of 30 minutes
Chew each piece for more than 30 minutes but reduce the number of pieces used daily
Substitute ordinary chewing gum for nicotine gum

NICOTINE GUM: ADDITIONAL PATIENT EDUCATION
To improve chances of quitting, use at least nine pieces of gum daily
The effectiveness of nicotine gum may be reduced by some foods and beverages:
Coffee Juices Wine Soft drinks
Do NOT eat or drink for 15 minutes BEFORE or while using nicotine gum.

NICOTINE GUM:ADD’L PATIENT EDUCATION (cont’d)
Chewing gum will not provide same rapid satisfaction that smoking provides
Chewing gum too rapidly can cause excessive release of nicotine, resulting in Lightheadedness Nausea/vomiting Irritation of throat and mouth Hiccups Indigestion

NICOTINE GUM:ADD’L PATIENT EDUCATION (cont’d)
Side effects of nicotine gum include Mouth soreness Hiccups Dyspepsia Jaw muscle ache
Nicotine gum may stick to dental work Discontinue use if excessive sticking or damage
to dental work occurs

NICOTINE GUM: SUMMARY
DISADVANTAGES Gum chewing may not
be socially acceptable. Gum is difficult to use
with dentures. Patients must use
proper chewing technique to minimize adverse effects.
ADVANTAGES Gum use may
satisfy oral cravings.
Gum use may delay weight gain.
Patients can titrate therapy to manage withdrawal symptoms.

NICOTINE LOZENGECommit (GlaxoSmithKline)
Approved for OTC use in 2002
Nicotine polacrilex formulation
Delivers ~25% more nicotine than equivalent gum dose
Available: 2 mg, 4 mg

NICOTINE LOZENGE: DOSING
Dosage based on the “time to first cigarette” (TTFC) as an indicator of nicotine addiction.
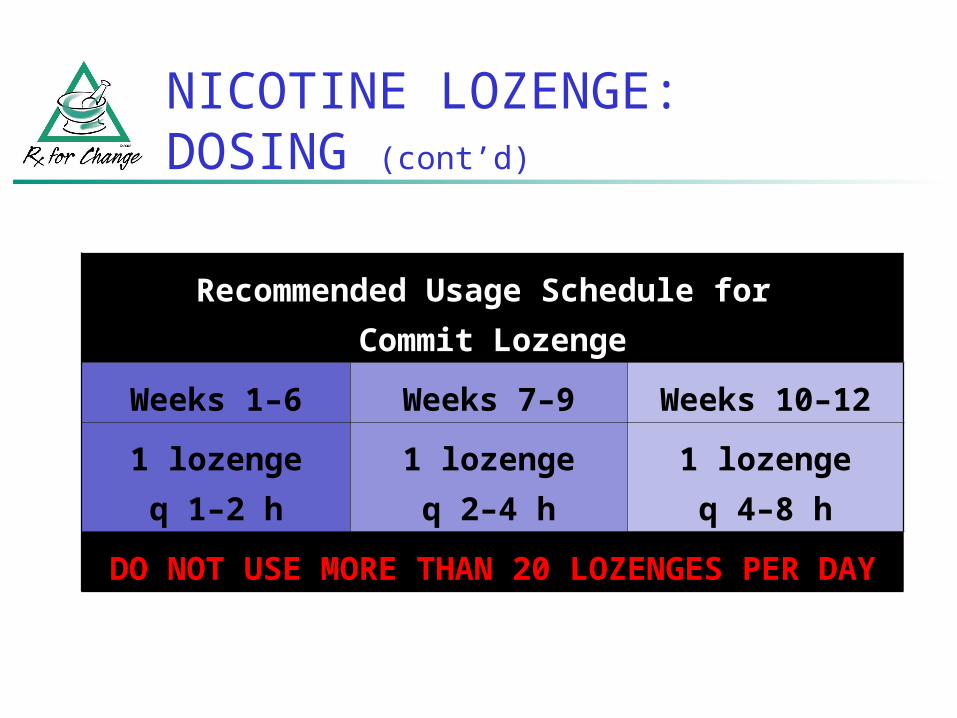
NICOTINE LOZENGE: DOSING (cont’d)
Recommended Usage Schedule for
Commit Lozenge
Weeks 1–6 Weeks 7–9 Weeks 10–12
1 lozenge
q 1–2 h
1 lozenge
q 2–4 h
1 lozenge
q 4–8 h
DO NOT USE MORE THAN 20 LOZENGES PER
DAY

NICOTINE LOZENGE:
DIRECTIONS for USE (cont’d)
Do not chew or swallow the lozenge
Occasionally rotate the lozenge to different areas of the mouth
Lozenge will completely dissolve in about 2030 minutes

NICOTINE LOZENGE: ADDITIONAL PATIENT EDUCATION
To improve chances of quitting, use at least nine lozenges daily during the first 6 weeks
The lozenge will not provide same rapid satisfaction that smoking provides
The effectiveness of nicotine lozenge may be reduced by some foods and beverages:
Coffee Juices Wine Soft drinks
Do NOT eat or drink for 15 minutes BEFORE or while using nicotine
lozenge.
NICOTINE LOZENGE:ADD’L PATIENT EDUCATION (cont’d)
Side effects of nicotine lozenge include Nausea Hiccups Cough Heartburn Headache Flatulence Insomnia
NICOTINE LOZENGE: SUMMARY
DISADVANTAGES Gastrointestinal side
effects (nausea, hiccups, and heartburn) may be bothersome.
ADVANTAGES Lozenge use may
satisfy oral cravings.
The lozenge is easy to use and conceal.
Patients can titrate therapy to manage withdrawal symptoms.
TRANSDERMAL NICOTINE PATCH
Approved for Rx use in 1991; OTC in 1996
Current products include Nicoderm CQ PatchOTC (GlaxoSmithKline) Nicotrol PatchOTC (Pharmacia) Generic ProductsRx, OTC
TRANSDERMAL NICOTINE PATCH Nicotine is well absorbed across the
skin
Delivery to systemic circulation avoids hepatic first-pass metabolism
Plasma nicotine levels are lower, fluctuate less than with smoking Relieve nicotine withdrawal
Low potential for dependence (compared to rapid delivery systems)

TRANSDERMAL NICOTINE PATCH:PREPARATION COMPARISON
Product Nicotrol Nicoderm CQ
Generics
Nicotine delivery 16 hours 24 hours 24 hours
Availability
5 mg patch
10 mg patch
15 mg patch
7 mg patch
14 mg patch
21 mg patch
7 mg patch
14 mg patch
21 mg patch
11 mg patch
22 mg patch

TRANSDERMAL NICOTINE PATCH: DOSING
Product Light Smoker Heavy SmokerNicotrol 10 cigarettes/day
Not indicated>10 cigarettes/dayStep 1 (15 mg x 6 weeks)Step 2 (10 mg x 2 weeks)Step 3 (5 mg x 2 weeks)
Nicoderm CQ 10 cigarettes/dayStep 2 (14 mg x 6 weeks)Step 3 (7 mg x 2 weeks)
>10 cigarettes/dayStep 1 (21 mg x 6 weeks)Step 2 (14 mg x 2 weeks)Step 3 (7 mg x 2 weeks)
Generic (formerly Habitrol)
10 cigarettes/dayStep 2 (14 mg x 6 weeks)Step 3 (7 mg x 2 weeks)
>10 cigarettes/dayStep 1 (21 mg x 4 weeks)Step 2 (14 mg x 2 weeks)Step 3 (7 mg x 2 weeks)
Generic (formerly ProStep)
15 cigarettes/day11 mg x 6 weeks
>15 cigarettes/day22 mg x 6 weeks

TRANSDERMAL NICOTINE PATCH:DIRECTIONS for USE
Choose an area of skin on the upper body or the upper outer part of the arm
Make sure the skin is clean, dry, and hairless
Hair will interfere with application of the patch
Do not shave; this may irritate the skin
TRANSDERMAL NICOTINE PATCH:DIRECTIONS for USE (cont’d)
Do not apply patch to skin that is inflamed, burned, or irritated in any way (these conditions may alter nicotine absorption)
Apply patch to a different area each day
The same area should not be used again for at least 1 week

TRANSDERMAL NICOTINE PATCH:DIRECTIONS for USE (cont’d)
Remove patch from protective pouch

TRANSDERMAL NICOTINE PATCH:DIRECTIONS for USE (cont’d)
Peel off half of the backing from the patch
TRANSDERMAL NICOTINE PATCH:DIRECTIONS for USE (cont’d)
Apply adhesive side of patch to the skin
Peel off remaining protective covering
Press firmly with palm of hand for 10 seconds
Make sure the patch sticks well to skin, especially around the edges

TRANSDERMAL NICOTINE PATCH:DIRECTIONS for USE (cont’d)
Wash hands (nicotine on hands can get into eyes or nose and cause stinging or redness)
Do not leave the patch on skin for more than 16 hours (Nicotrol) or 24 hours (Nicoderm, generic patches—doing so may lead to skin irritation
Adhesive remaining on skin may be removed with rubbing alcohol or acetone
Dispose of a used patch by folding onto itself, completely covering the adhesive area
TRANSDERMAL NICOTINE PATCH:ADDITIONAL PATIENT EDUCATION
Water will not harm the nicotine patch if it is applied correctly; patients may bathe, swim, shower, or exercise while wearing the patch
Do not cut patches to adjust dose Nicotine will evaporate rapidly Patch will be rendered useless
Keep new and used patches out of the reach of children and pets

TRANSDERMAL NICOTINE PATCH:ADD’L PATIENT EDUCATION (cont’d)
Side effects to expect in first hour: Mild itching Burning Tingling
After patch removal, the skin may appear red for the next 24 hours
If skin stays red more than 4 days or swells, or if a rash appears, contact health care provider; do not put on a new patch

TRANSDERMAL NICOTINE PATCH:ADD’L PATIENT EDUCATION (cont’d)
Additional possible side effects: Vivid dreams or sleep disturbances Headache Local skin reactions (erythema, burning,
pruritus) Usually caused by adhesive Up to 50% of patients experience this reaction Incidence may be higher with 24-hour products Less than 5% of patients discontinue therapy Avoid use in patients with dermatologic conditions
(e.g., psoriasis, eczema, atopic dermatitis)

TRANSDERMAL NICOTINE PATCH: SUMMARY
DISADVANTAGES Patients cannot titrate
the dose. Allergic reactions to
adhesive may occur. 16-hr patch may lead to
morning nicotine cravings.
Patients with dermatologic conditions should not use the patch.
ADVANTAGES The patch
provides consistent nicotine levels.
The patch is easy to use and conceal.
Fewer compliance issues are associated with the patch.

LONG-TERM (6 month) QUIT RATES for AVAILABLE CESSATION MEDICATIONS
0
5
10
15
20
25
30
Nicotine gum Nicotine patch Nicotinelozenge
Nicotine nasalspray
Nicotineinhaler
Bupropion
Active drugPlacebo
Data adapted from Silagy et al. Cochrane Database Syst Rev, 2002 and Hughes et al., Cochrane Database Syst Rev, 2000
Per
cen
t q
uit 19.7
14.4
11.5
8.4
17.2
8.9
23.9
11.8
17.1
9.1
19.3
10.2

COMBINATION NRT
Long-acting formulation (patch) Produces relatively constant levels of
nicotine
PLUS
Short-acting formulation (gum, lozenge, inhaler, nasal spray) Allows for acute dose titration as needed
for withdrawal symptomsReserve for patients unable to quit using monotherapy.
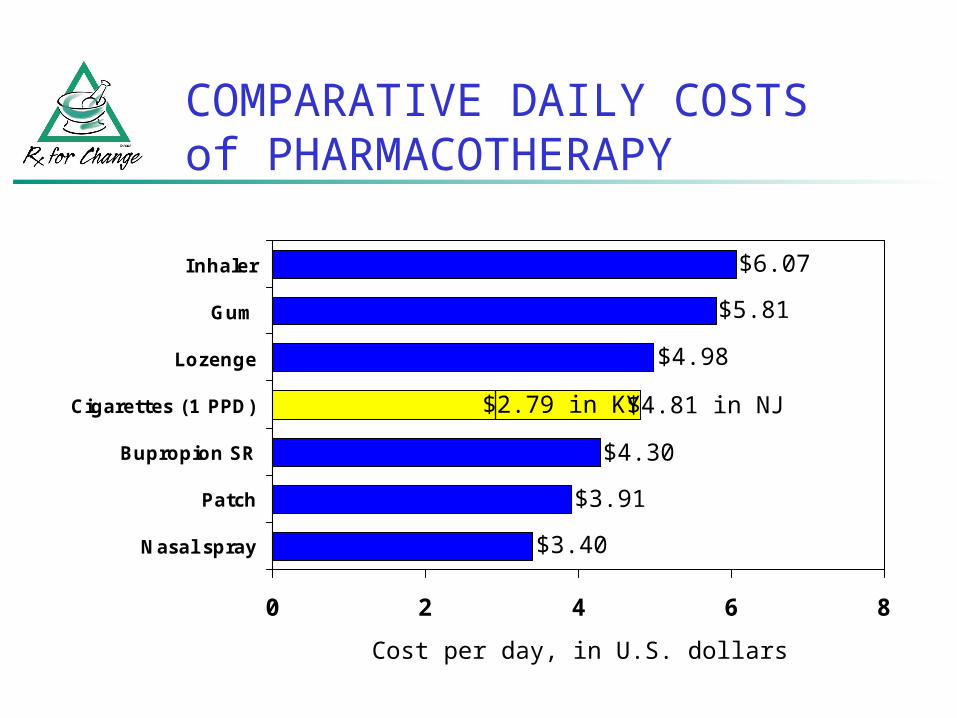
COMPARATIVE DAILY COSTS of PHARMACOTHERAPY
Cost per day, in U.S. dollars
0 2 4 6 8
Nasal spray
Patch
Bupropion SR
Cigarettes (1 PPD)
Lozenge
Gum
Inhaler
$2.79 in KY $4.81 in NJ
$6.07
$5.81
$4.98
$4.30
$3.91
$3.40

The RESPONSIBILITY of HEALTH PROFESSIONALS
It is inconsistent
to provide health care and
—at the same time—
remain silent (or inactive)
about a major health risk.
TOBACCO CESSATION is an important component of
THERAPY.
DR. GRO HARLEM BRUNTLAND,
DIRECTOR-GENERAL of the WHO:
“If we do not act decisively, a hundred years from now our grandchildren and their children will look back and seriously question how people claiming to be committed to public health and social justice allowed the tobacco epidemic to unfold unchecked.”
US Department of Health and Human Services. Women and Smoking: A Report of the Surgeon General. Washington, DC: Public Health Service, 2001.