
Noncompliance maxillary molar distalization with the First ... · appliance, Keles slider,...
13
ONLINE ONLY Noncompliance maxillary molar distalization with the First Class Appliance: A randomized controlled trial Moschos A. Papadopoulos, a Aristides B. Melkos, b and Athanasios E. Athanasiou c Thessaloniki and Evosmos, Greece Introduction: The aim of this study was to evaluate the treatment effects of the First Class Appliance (FCA) (Leone, Firenze, Italy) used for the distalization of maxillary first molars in patients with Class II malocclusion and mixed dentition. Methods: According to the results of the power analysis for sample size calculation, 32 consecutive patients with bilateral Class II molar relationships were initially included in the study. After appli- cation of the inclusion and exclusion criteria, 26 patients remained for the final evaluation. They were random- ized into 2 groups: treatment group (n 5 15) and untreated control group (n 5 11). Lateral cephalograms and dental casts were obtained before and immediately after distalization for the treatment group, and initially and approximately 22 weeks later for the control group. Statistical evaluation of the variables included the mixed 2-way analysis of variance at P \0.05. The method error was also estimated. Results: The mean treatment period to achieve a full Class I molar relationship was 17.2 weeks. Analysis of the data showed significant distalization of the maxillary first molars produced by the FCA (mean: 4.00 mm) when compared with the untreated group (mean: 0.95 mm). The rate of molar movement was 1.00 mm per month, which, however, was associated with distal tipping of the first molars (8.56 ) and anchorage loss of the anterior dental unit in terms of overjet increase (0.68 mm), and mesial movement (1.86 mm) and inclination (1.85 ) of the first premolars or first deciduous molars. The maxillary first molars also moved buccally (1.37 mm), but no significant distal rotation occurred. Conclusions: The FCA is an efficient noncompliance appliance to distalize molars in the mixed dentition without distal rotations. However, these movements are associated with distal molar tipping and anchorage loss of the anterior teeth. (Am J Orthod Dentofacial Orthop 2010;137:586.e1-586.e13) A common strategy to treat Class II malocclu- sions by a nonextraction protocol is to initially distalize the maxillary molars to create a Class I relationship. Various concepts, biomechanics, and ap- pliances have been routinely used, including extraoral traction, removable appliances with springs, and Class II intermaxillary elastics. 1-6 Since the patients’ compliance is a presupposition for the effectiveness of these modalities, the development and use of techniques and appliances that minimize the need for patient cooperation provides a reliable and more predictable treatment alternative. 7 The category of non- compliance mechanics includes a variety of intramaxil- lary appliances such as Jones jig, distal jet, pendulum appliance, Keles slider, repelling magnets, compressed coil springs, molar distalizing bows, and orthodontic implants or miniscrew implants. 7-21 Noncompliance distalization methods, however, are not problem free. They have some undesirable side ef- fects that diminish their clinical effectiveness, including anchorage loss (posterior: distal molar crown tipping or distal rotation of molar crowns; anterior: mesial move- ment and proclination of the maxillary anterior teeth). These side effects can vary among the different tech- niques and appliances, but they are always associated with maxillary molar distalization. 11 Open-coil springs combined with various noncom- pliance appliances have been used for a long time to distalize maxillary molars. 13,17,22-24 The First Class Appliance (FCA) (Leone, Firenze, Italy) was recently introduced for unilateral or bilateral noncompliance distalization of the maxillary molars. 25-27 Until now, a Associate professor and program coordinator, Department of Orthodontics, School of Dentistry, Aristotle University of Thessaloniki, Thessaloniki, Greece. b Private practice limited to orthodontics, Evosmos, Greece. c Professor and head, Department of Orthodontics, School of Dentistry, Aristotle University of Thessaloniki, Thessaloniki, Greece. The authors report no commercial, proprietary, or financial interest in the products or companies described in this article. Reprint requests to: Moschos A. Papadopoulos, Department of Orthodontics, School of Dentistry, Aristotle University of Thessaloniki, GR-54124 Thessalo- niki, Greece; e-mail, [email protected]. Submitted, July 2009; revised and accepted, October 2009. 0889-5406/$36.00 Copyright Ó 2010 by the American Association of Orthodontists. doi:10.1016/j.ajodo.2009.10.033 586.e1
Transcript of Noncompliance maxillary molar distalization with the First ... · appliance, Keles slider,...
ONLINE ONLY
Noncompliance maxillary molar distalizationwith the First Class Appliance: A randomizedcontrolled trial
Moschos A. Papadopoulos,a Aristides B. Melkos,b and Athanasios E. Athanasiouc
Thessaloniki and Evosmos, Greece
Introduction: The aim of this study was to evaluate the treatment effects of the First Class Appliance (FCA)(Leone, Firenze, Italy) used for the distalization of maxillary first molars in patients with Class II malocclusionand mixed dentition. Methods: According to the results of the power analysis for sample size calculation, 32consecutive patients with bilateral Class II molar relationships were initially included in the study. After appli-cation of the inclusion and exclusion criteria, 26 patients remained for the final evaluation. They were random-ized into 2 groups: treatment group (n 5 15) and untreated control group (n 5 11). Lateral cephalograms anddental casts were obtained before and immediately after distalization for the treatment group, and initially andapproximately 22 weeks later for the control group. Statistical evaluation of the variables included the mixed2-way analysis of variance at P \0.05. The method error was also estimated. Results: The mean treatmentperiod to achieve a full Class I molar relationship was 17.2 weeks. Analysis of the data showed significantdistalization of the maxillary first molars produced by the FCA (mean: 4.00 mm) when compared with theuntreated group (mean: 0.95 mm). The rate of molar movement was 1.00 mm per month, which, however,was associated with distal tipping of the first molars (8.56�) and anchorage loss of the anterior dental unitin terms of overjet increase (0.68 mm), and mesial movement (1.86 mm) and inclination (1.85�) of the firstpremolars or first deciduous molars. The maxillary first molars also moved buccally (1.37 mm), but nosignificant distal rotation occurred. Conclusions: The FCA is an efficient noncompliance appliance to distalizemolars in the mixed dentition without distal rotations. However, these movements are associated withdistal molar tipping and anchorage loss of the anterior teeth. (Am J Orthod Dentofacial Orthop2010;137:586.e1-586.e13)
Acommon strategy to treat Class II malocclu-
sions by a nonextraction protocol is to initiallydistalize the maxillary molars to create a Class
I relationship. Various concepts, biomechanics, and ap-pliances have been routinely used, including extraoraltraction, removable appliances with springs, and ClassII intermaxillary elastics.1-6 Since the patients’compliance is a presupposition for the effectiveness ofthese modalities, the development and use oftechniques and appliances that minimize the need for
aAssociate professor and program coordinator, Department of Orthodontics,
School of Dentistry, Aristotle University of Thessaloniki, Thessaloniki, Greece.bPrivate practice limited to orthodontics, Evosmos, Greece.cProfessor and head, Department of Orthodontics, School of Dentistry, Aristotle
University of Thessaloniki, Thessaloniki, Greece.
The authors report no commercial, proprietary, or financial interest in the
products or companies described in this article.
Reprint requests to: Moschos A. Papadopoulos, Department of Orthodontics,
School of Dentistry, Aristotle University of Thessaloniki, GR-54124 Thessalo-
niki, Greece; e-mail, [email protected].
Submitted, July 2009; revised and accepted, October 2009.
0889-5406/$36.00
Copyright � 2010 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2009.10.033
patient cooperation provides a reliable and morepredictable treatment alternative.7 The category of non-compliance mechanics includes a variety of intramaxil-lary appliances such as Jones jig, distal jet, pendulumappliance, Keles slider, repelling magnets, compressedcoil springs, molar distalizing bows, and orthodonticimplants or miniscrew implants.7-21
Noncompliance distalization methods, however, arenot problem free. They have some undesirable side ef-fects that diminish their clinical effectiveness, includinganchorage loss (posterior: distal molar crown tipping ordistal rotation of molar crowns; anterior: mesial move-ment and proclination of the maxillary anterior teeth).These side effects can vary among the different tech-niques and appliances, but they are always associatedwith maxillary molar distalization.11
Open-coil springs combined with various noncom-pliance appliances have been used for a long time todistalize maxillary molars.13,17,22-24 The First ClassAppliance (FCA) (Leone, Firenze, Italy) was recentlyintroduced for unilateral or bilateral noncompliancedistalization of the maxillary molars.25-27 Until now,
586.e1
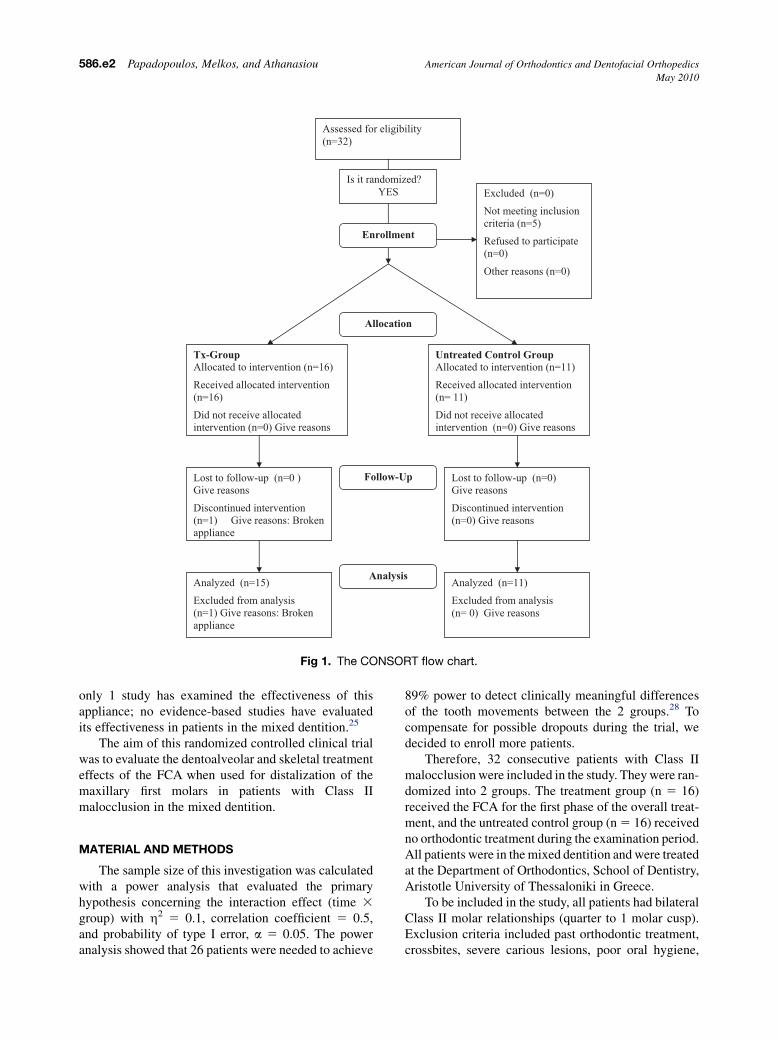
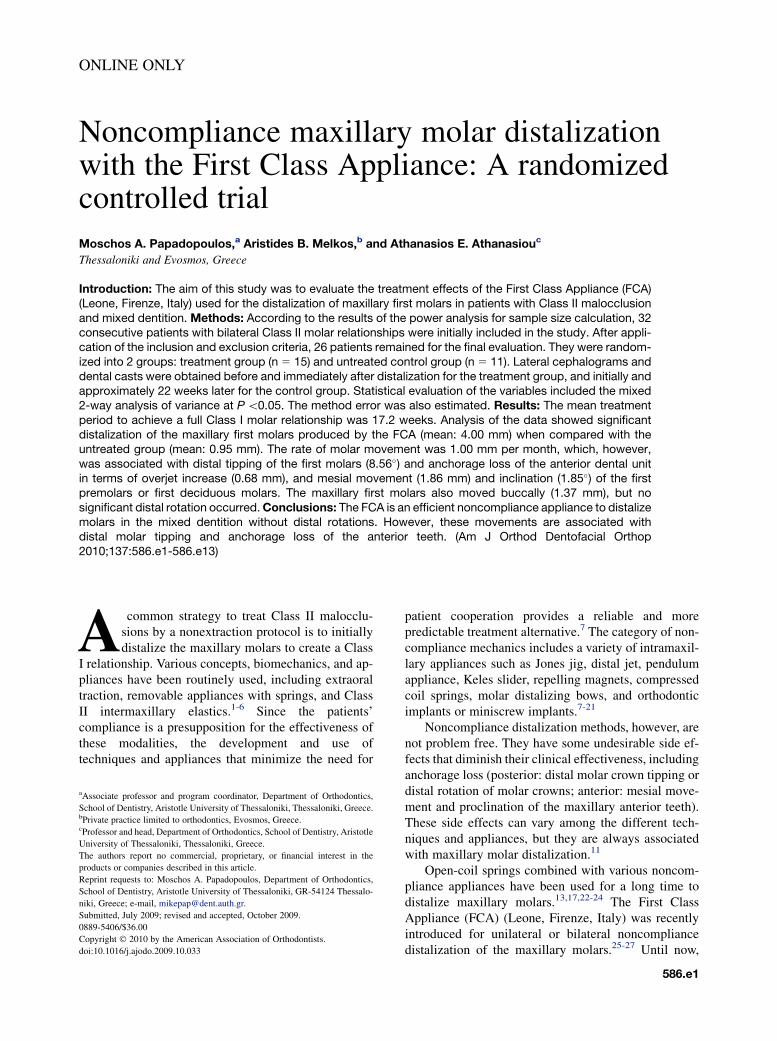
Fig 1. The CONSORT flow chart.
586.e2 Papadopoulos, Melkos, and Athanasiou American Journal of Orthodontics and Dentofacial Orthopedics
May 2010
only 1 study has examined the effectiveness of thisappliance; no evidence-based studies have evaluatedits effectiveness in patients in the mixed dentition.25
The aim of this randomized controlled clinical trialwas to evaluate the dentoalveolar and skeletal treatmenteffects of the FCA when used for distalization of themaxillary first molars in patients with Class IImalocclusion in the mixed dentition.
MATERIAL AND METHODS
The sample size of this investigation was calculatedwith a power analysis that evaluated the primaryhypothesis concerning the interaction effect (time 3
group) with h2 5 0.1, correlation coefficient 5 0.5,and probability of type I error, a 5 0.05. The poweranalysis showed that 26 patients were needed to achieve
89% power to detect clinically meaningful differencesof the tooth movements between the 2 groups.28 Tocompensate for possible dropouts during the trial, wedecided to enroll more patients.
Therefore, 32 consecutive patients with Class IImalocclusion were included in the study. They were ran-domized into 2 groups. The treatment group (n 5 16)received the FCA for the first phase of the overall treat-ment, and the untreated control group (n 5 16) receivedno orthodontic treatment during the examination period.All patients were in the mixed dentition and were treatedat the Department of Orthodontics, School of Dentistry,Aristotle University of Thessaloniki in Greece.
To be included in the study, all patients had bilateralClass II molar relationships (quarter to 1 molar cusp).Exclusion criteria included past orthodontic treatment,crossbites, severe carious lesions, poor oral hygiene,
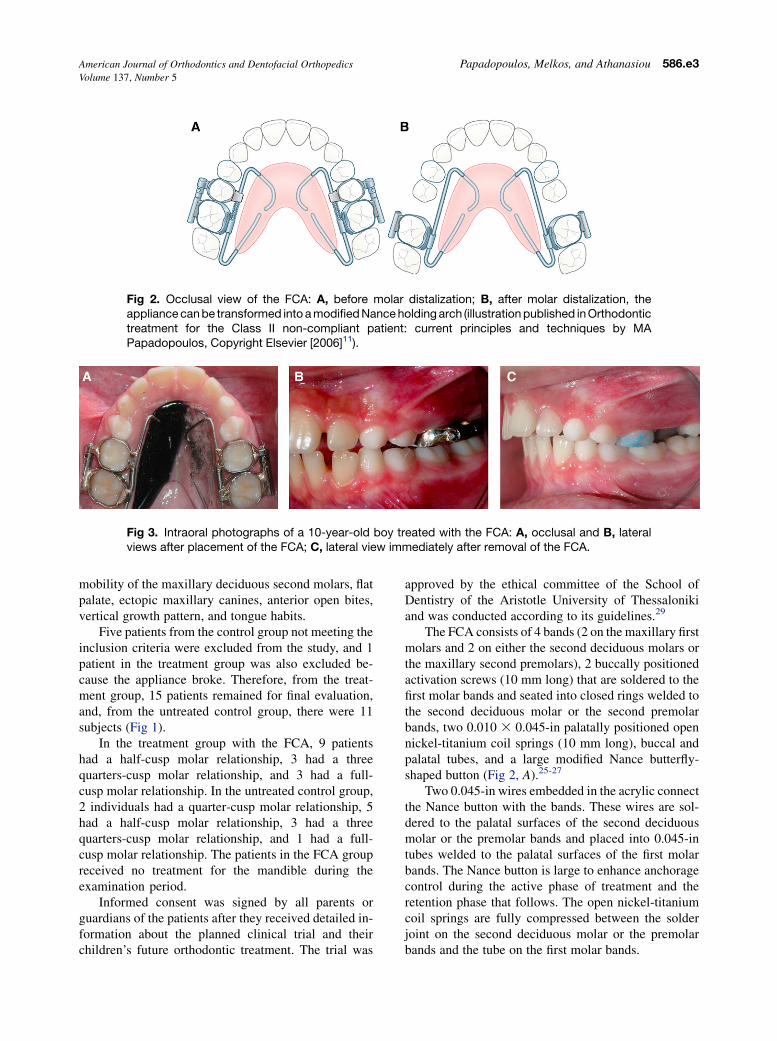
Fig 2. Occlusal view of the FCA: A, before molar distalization; B, after molar distalization, theappliance can be transformed into a modified Nance holding arch (illustration published in Orthodontictreatment for the Class II non-compliant patient: current principles and techniques by MAPapadopoulos, Copyright Elsevier [2006]11).
Fig 3. Intraoral photographs of a 10-year-old boy treated with the FCA: A, occlusal and B, lateralviews after placement of the FCA; C, lateral view immediately after removal of the FCA.
American Journal of Orthodontics and Dentofacial Orthopedics Papadopoulos, Melkos, and Athanasiou 586.e3Volume 137, Number 5
mobility of the maxillary deciduous second molars, flatpalate, ectopic maxillary canines, anterior open bites,vertical growth pattern, and tongue habits.
Five patients from the control group not meeting theinclusion criteria were excluded from the study, and 1patient in the treatment group was also excluded be-cause the appliance broke. Therefore, from the treat-ment group, 15 patients remained for final evaluation,and, from the untreated control group, there were 11subjects (Fig 1).
In the treatment group with the FCA, 9 patientshad a half-cusp molar relationship, 3 had a threequarters-cusp molar relationship, and 3 had a full-cusp molar relationship. In the untreated control group,2 individuals had a quarter-cusp molar relationship, 5had a half-cusp molar relationship, 3 had a threequarters-cusp molar relationship, and 1 had a full-cusp molar relationship. The patients in the FCA groupreceived no treatment for the mandible during theexamination period.
Informed consent was signed by all parents orguardians of the patients after they received detailed in-formation about the planned clinical trial and theirchildren’s future orthodontic treatment. The trial was
approved by the ethical committee of the School ofDentistry of the Aristotle University of Thessalonikiand was conducted according to its guidelines.29
The FCA consists of 4 bands (2 on the maxillary firstmolars and 2 on either the second deciduous molars orthe maxillary second premolars), 2 buccally positionedactivation screws (10 mm long) that are soldered to thefirst molar bands and seated into closed rings welded tothe second deciduous molar or the second premolarbands, two 0.010 3 0.045-in palatally positioned opennickel-titanium coil springs (10 mm long), buccal andpalatal tubes, and a large modified Nance butterfly-shaped button (Fig 2, A).25-27
Two 0.045-in wires embedded in the acrylic connectthe Nance button with the bands. These wires are sol-dered to the palatal surfaces of the second deciduousmolar or the premolar bands and placed into 0.045-intubes welded to the palatal surfaces of the first molarbands. The Nance button is large to enhance anchoragecontrol during the active phase of treatment and theretention phase that follows. The open nickel-titaniumcoil springs are fully compressed between the solderjoint on the second deciduous molar or the premolarbands and the tube on the first molar bands.
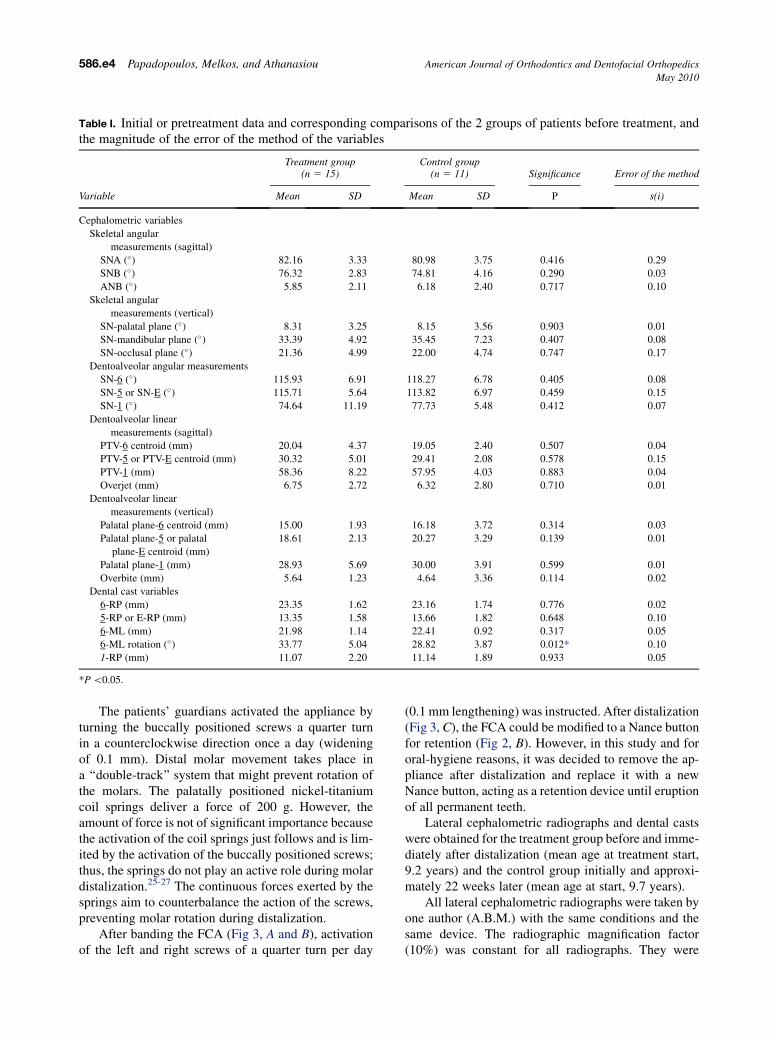
Table I. Initial or pretreatment data and corresponding comparisons of the 2 groups of patients before treatment, andthe magnitude of the error of the method of the variables
Variable
Treatment group(n 5 15)
Control group(n 5 11) Significance Error of the method
Mean SD Mean SD P s(i)
Cephalometric variables
Skeletal angular
measurements (sagittal)
SNA (�) 82.16 3.33 80.98 3.75 0.416 0.29
SNB (�) 76.32 2.83 74.81 4.16 0.290 0.03
ANB (�) 5.85 2.11 6.18 2.40 0.717 0.10
Skeletal angular
measurements (vertical)
SN-palatal plane (�) 8.31 3.25 8.15 3.56 0.903 0.01
SN-mandibular plane (�) 33.39 4.92 35.45 7.23 0.407 0.08
SN-occlusal plane (�) 21.36 4.99 22.00 4.74 0.747 0.17
Dentoalveolar angular measurements
SN-6 (�) 115.93 6.91 118.27 6.78 0.405 0.08
SN-5 or SN-E (�) 115.71 5.64 113.82 6.97 0.459 0.15
SN-1 (�) 74.64 11.19 77.73 5.48 0.412 0.07
Dentoalveolar linear
measurements (sagittal)
PTV-6 centroid (mm) 20.04 4.37 19.05 2.40 0.507 0.04
PTV-5 or PTV-E centroid (mm) 30.32 5.01 29.41 2.08 0.578 0.15
PTV-1 (mm) 58.36 8.22 57.95 4.03 0.883 0.04
Overjet (mm) 6.75 2.72 6.32 2.80 0.710 0.01
Dentoalveolar linear
measurements (vertical)
Palatal plane-6 centroid (mm) 15.00 1.93 16.18 3.72 0.314 0.03
Palatal plane-5 or palatal
plane-E centroid (mm)
18.61 2.13 20.27 3.29 0.139 0.01
Palatal plane-1 (mm) 28.93 5.69 30.00 3.91 0.599 0.01
Overbite (mm) 5.64 1.23 4.64 3.36 0.114 0.02
Dental cast variables
6-RP (mm) 23.35 1.62 23.16 1.74 0.776 0.02
5-RP or E-RP (mm) 13.35 1.58 13.66 1.82 0.648 0.10
6-ML (mm) 21.98 1.14 22.41 0.92 0.317 0.05
6-ML rotation (�) 33.77 5.04 28.82 3.87 0.012* 0.10
1-RP (mm) 11.07 2.20 11.14 1.89 0.933 0.05
*P \0.05.
586.e4 Papadopoulos, Melkos, and Athanasiou American Journal of Orthodontics and Dentofacial Orthopedics
May 2010
The patients’ guardians activated the appliance byturning the buccally positioned screws a quarter turnin a counterclockwise direction once a day (wideningof 0.1 mm). Distal molar movement takes place ina ‘‘double-track’’ system that might prevent rotation ofthe molars. The palatally positioned nickel-titaniumcoil springs deliver a force of 200 g. However, theamount of force is not of significant importance becausethe activation of the coil springs just follows and is lim-ited by the activation of the buccally positioned screws;thus, the springs do not play an active role during molardistalization.25-27 The continuous forces exerted by thesprings aim to counterbalance the action of the screws,preventing molar rotation during distalization.
After banding the FCA (Fig 3, A and B), activationof the left and right screws of a quarter turn per day
(0.1 mm lengthening) was instructed. After distalization(Fig 3, C), the FCA could be modified to a Nance buttonfor retention (Fig 2, B). However, in this study and fororal-hygiene reasons, it was decided to remove the ap-pliance after distalization and replace it with a newNance button, acting as a retention device until eruptionof all permanent teeth.
Lateral cephalometric radiographs and dental castswere obtained for the treatment group before and imme-diately after distalization (mean age at treatment start,9.2 years) and the control group initially and approxi-mately 22 weeks later (mean age at start, 9.7 years).
All lateral cephalometric radiographs were taken byone author (A.B.M.) with the same conditions and thesame device. The radiographic magnification factor(10%) was constant for all radiographs. They were
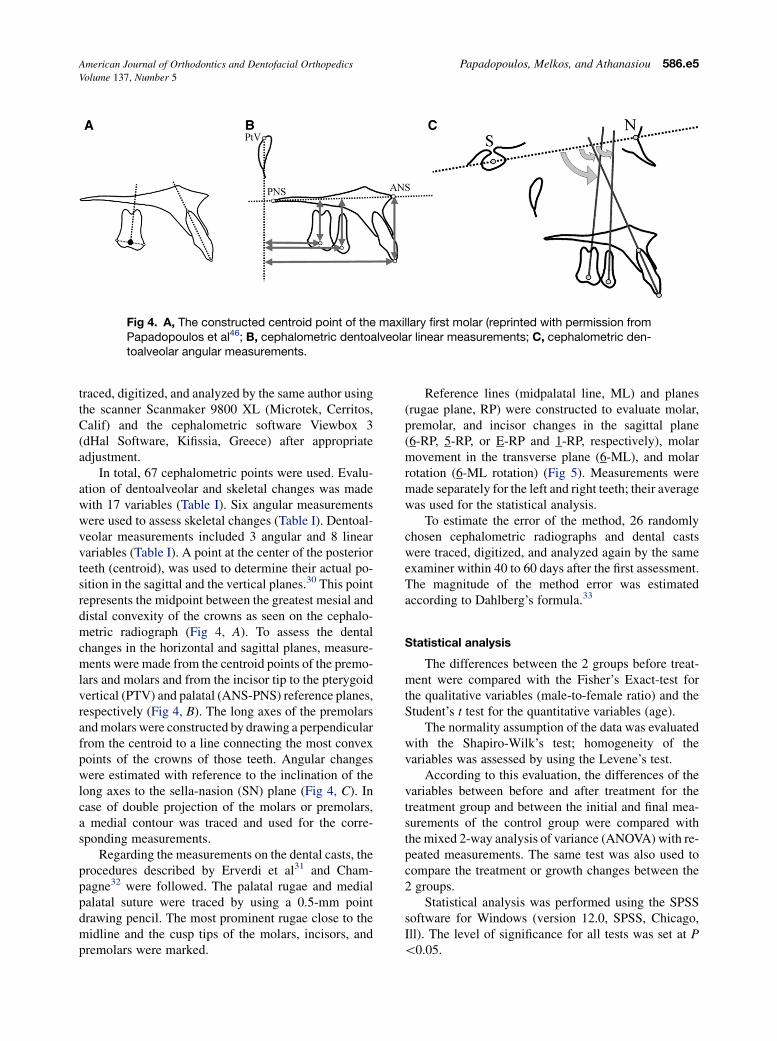
Fig 4. A, The constructed centroid point of the maxillary first molar (reprinted with permission fromPapadopoulos et al46; B, cephalometric dentoalveolar linear measurements; C, cephalometric den-toalveolar angular measurements.
American Journal of Orthodontics and Dentofacial Orthopedics Papadopoulos, Melkos, and Athanasiou 586.e5Volume 137, Number 5
traced, digitized, and analyzed by the same author usingthe scanner Scanmaker 9800 XL (Microtek, Cerritos,Calif) and the cephalometric software Viewbox 3(dHal Software, Kifissia, Greece) after appropriateadjustment.
In total, 67 cephalometric points were used. Evalu-ation of dentoalveolar and skeletal changes was madewith 17 variables (Table I). Six angular measurementswere used to assess skeletal changes (Table I). Dentoal-veolar measurements included 3 angular and 8 linearvariables (Table I). A point at the center of the posteriorteeth (centroid), was used to determine their actual po-sition in the sagittal and the vertical planes.30 This pointrepresents the midpoint between the greatest mesial anddistal convexity of the crowns as seen on the cephalo-metric radiograph (Fig 4, A). To assess the dentalchanges in the horizontal and sagittal planes, measure-ments were made from the centroid points of the premo-lars and molars and from the incisor tip to the pterygoidvertical (PTV) and palatal (ANS-PNS) reference planes,respectively (Fig 4, B). The long axes of the premolarsand molars were constructed by drawing a perpendicularfrom the centroid to a line connecting the most convexpoints of the crowns of those teeth. Angular changeswere estimated with reference to the inclination of thelong axes to the sella-nasion (SN) plane (Fig 4, C). Incase of double projection of the molars or premolars,a medial contour was traced and used for the corre-sponding measurements.
Regarding the measurements on the dental casts, theprocedures described by Erverdi et al31 and Cham-pagne32 were followed. The palatal rugae and medialpalatal suture were traced by using a 0.5-mm pointdrawing pencil. The most prominent rugae close to themidline and the cusp tips of the molars, incisors, andpremolars were marked.
Reference lines (midpalatal line, ML) and planes(rugae plane, RP) were constructed to evaluate molar,premolar, and incisor changes in the sagittal plane(6-RP, 5-RP, or E-RP and 1-RP, respectively), molarmovement in the transverse plane (6-ML), and molarrotation (6-ML rotation) (Fig 5). Measurements weremade separately for the left and right teeth; their averagewas used for the statistical analysis.
To estimate the error of the method, 26 randomlychosen cephalometric radiographs and dental castswere traced, digitized, and analyzed again by the sameexaminer within 40 to 60 days after the first assessment.The magnitude of the method error was estimatedaccording to Dahlberg’s formula.33
Statistical analysis
The differences between the 2 groups before treat-ment were compared with the Fisher’s Exact-test forthe qualitative variables (male-to-female ratio) and theStudent’s t test for the quantitative variables (age).
The normality assumption of the data was evaluatedwith the Shapiro-Wilk’s test; homogeneity of thevariables was assessed by using the Levene’s test.
According to this evaluation, the differences of thevariables between before and after treatment for thetreatment group and between the initial and final mea-surements of the control group were compared withthe mixed 2-way analysis of variance (ANOVA) with re-peated measurements. The same test was also used tocompare the treatment or growth changes between the2 groups.
Statistical analysis was performed using the SPSSsoftware for Windows (version 12.0, SPSS, Chicago,Ill). The level of significance for all tests was set at P\0.05.
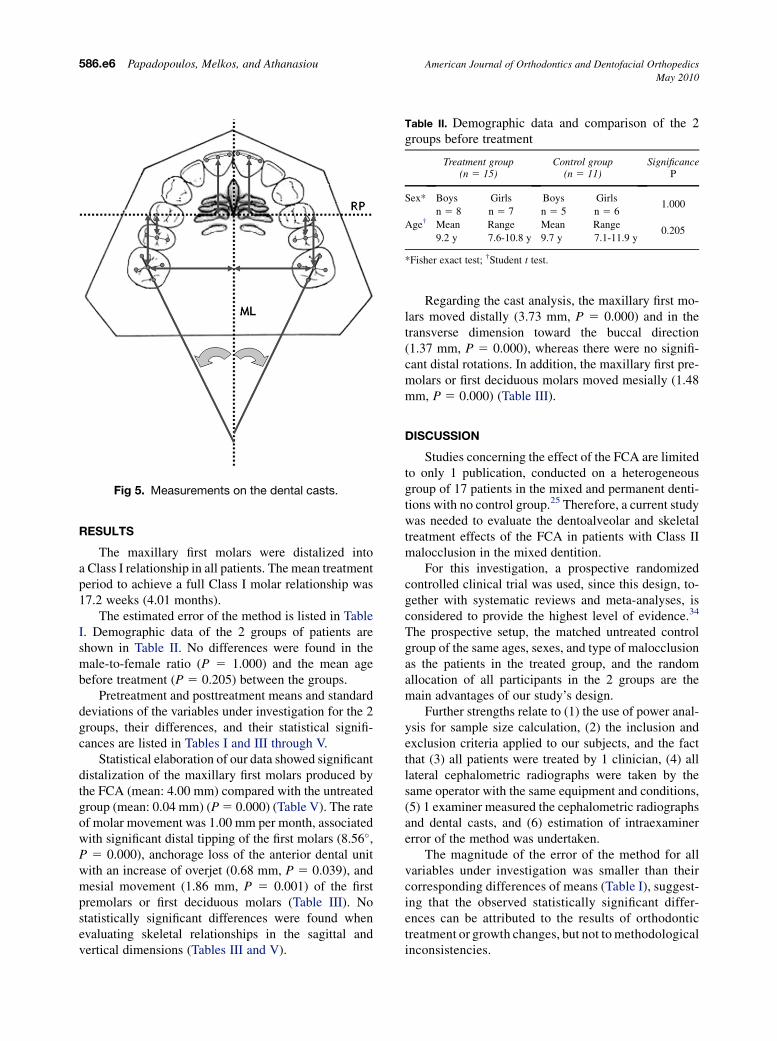
Fig 5. Measurements on the dental casts.
Table II. Demographic data and comparison of the 2groups before treatment
Treatment group(n 5 15)
Control group(n 5 11)
SignificanceP
Sex* Boys Girls Boys Girls
n 5 8 n 5 7 n 5 5 n 5 61.000
Age† Mean Range Mean Range
9.2 y 7.6-10.8 y 9.7 y 7.1-11.9 y0.205
*Fisher exact test; †Student t test.
586.e6 Papadopoulos, Melkos, and Athanasiou American Journal of Orthodontics and Dentofacial Orthopedics
May 2010
RESULTS
The maxillary first molars were distalized intoa Class I relationship in all patients. The mean treatmentperiod to achieve a full Class I molar relationship was17.2 weeks (4.01 months).
The estimated error of the method is listed in TableI. Demographic data of the 2 groups of patients areshown in Table II. No differences were found in themale-to-female ratio (P 5 1.000) and the mean agebefore treatment (P 5 0.205) between the groups.
Pretreatment and posttreatment means and standarddeviations of the variables under investigation for the 2groups, their differences, and their statistical signifi-cances are listed in Tables I and III through V.
Statistical elaboration of our data showed significantdistalization of the maxillary first molars produced bythe FCA (mean: 4.00 mm) compared with the untreatedgroup (mean: 0.04 mm) (P 5 0.000) (Table V). The rateof molar movement was 1.00 mm per month, associatedwith significant distal tipping of the first molars (8.56�,P 5 0.000), anchorage loss of the anterior dental unitwith an increase of overjet (0.68 mm, P 5 0.039), andmesial movement (1.86 mm, P 5 0.001) of the firstpremolars or first deciduous molars (Table III). Nostatistically significant differences were found whenevaluating skeletal relationships in the sagittal andvertical dimensions (Tables III and V).
Regarding the cast analysis, the maxillary first mo-lars moved distally (3.73 mm, P 5 0.000) and in thetransverse dimension toward the buccal direction(1.37 mm, P 5 0.000), whereas there were no signifi-cant distal rotations. In addition, the maxillary first pre-molars or first deciduous molars moved mesially (1.48mm, P 5 0.000) (Table III).
DISCUSSION
Studies concerning the effect of the FCA are limitedto only 1 publication, conducted on a heterogeneousgroup of 17 patients in the mixed and permanent denti-tions with no control group.25 Therefore, a current studywas needed to evaluate the dentoalveolar and skeletaltreatment effects of the FCA in patients with Class IImalocclusion in the mixed dentition.
For this investigation, a prospective randomizedcontrolled clinical trial was used, since this design, to-gether with systematic reviews and meta-analyses, isconsidered to provide the highest level of evidence.34
The prospective setup, the matched untreated controlgroup of the same ages, sexes, and type of malocclusionas the patients in the treated group, and the randomallocation of all participants in the 2 groups are themain advantages of our study’s design.
Further strengths relate to (1) the use of power anal-ysis for sample size calculation, (2) the inclusion andexclusion criteria applied to our subjects, and the factthat (3) all patients were treated by 1 clinician, (4) alllateral cephalometric radiographs were taken by thesame operator with the same equipment and conditions,(5) 1 examiner measured the cephalometric radiographsand dental casts, and (6) estimation of intraexaminererror of the method was undertaken.
The magnitude of the error of the method for allvariables under investigation was smaller than theircorresponding differences of means (Table I), suggest-ing that the observed statistically significant differ-ences can be attributed to the results of orthodontictreatment or growth changes, but not to methodologicalinconsistencies.
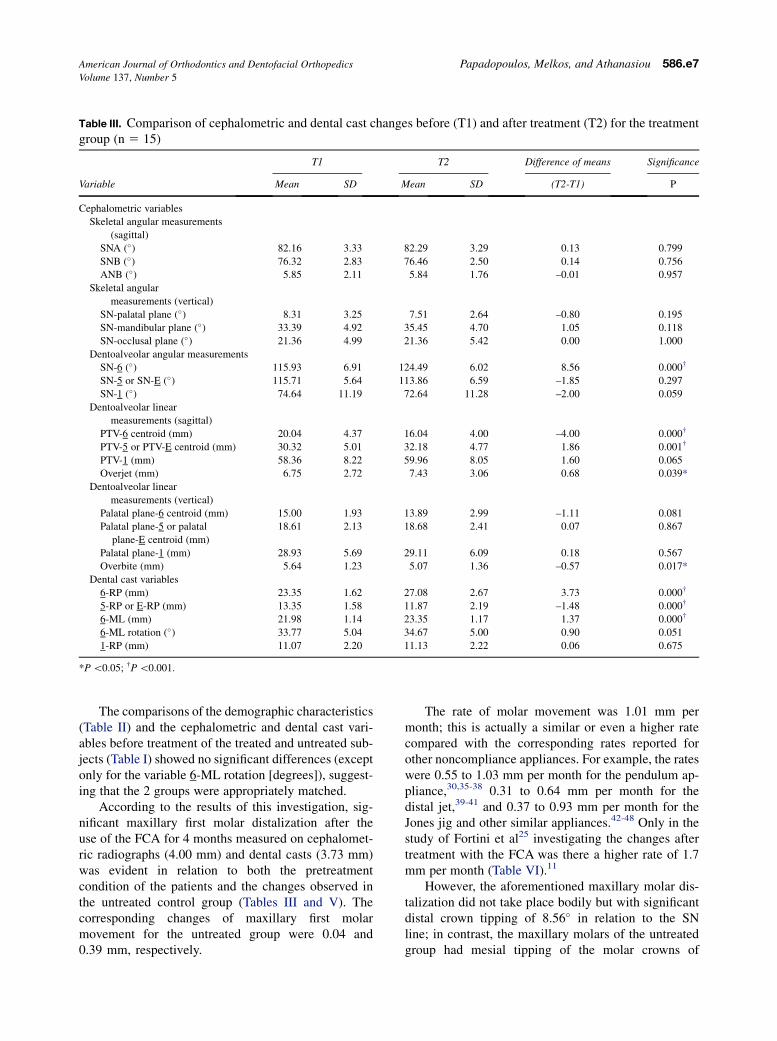
Table III. Comparison of cephalometric and dental cast changes before (T1) and after treatment (T2) for the treatmentgroup (n 5 15)
Variable
T1 T2 Difference of means Significance
Mean SD Mean SD (T2-T1) P
Cephalometric variables
Skeletal angular measurements
(sagittal)
SNA (�) 82.16 3.33 82.29 3.29 0.13 0.799
SNB (�) 76.32 2.83 76.46 2.50 0.14 0.756
ANB (�) 5.85 2.11 5.84 1.76 –0.01 0.957
Skeletal angular
measurements (vertical)
SN-palatal plane (�) 8.31 3.25 7.51 2.64 –0.80 0.195
SN-mandibular plane (�) 33.39 4.92 35.45 4.70 1.05 0.118
SN-occlusal plane (�) 21.36 4.99 21.36 5.42 0.00 1.000
Dentoalveolar angular measurements
SN-6 (�) 115.93 6.91 124.49 6.02 8.56 0.000†
SN-5 or SN-E (�) 115.71 5.64 113.86 6.59 –1.85 0.297
SN-1 (�) 74.64 11.19 72.64 11.28 –2.00 0.059
Dentoalveolar linear
measurements (sagittal)
PTV-6 centroid (mm) 20.04 4.37 16.04 4.00 –4.00 0.000†
PTV-5 or PTV-E centroid (mm) 30.32 5.01 32.18 4.77 1.86 0.001†
PTV-1 (mm) 58.36 8.22 59.96 8.05 1.60 0.065
Overjet (mm) 6.75 2.72 7.43 3.06 0.68 0.039*
Dentoalveolar linear
measurements (vertical)
Palatal plane-6 centroid (mm) 15.00 1.93 13.89 2.99 –1.11 0.081
Palatal plane-5 or palatal
plane-E centroid (mm)
18.61 2.13 18.68 2.41 0.07 0.867
Palatal plane-1 (mm) 28.93 5.69 29.11 6.09 0.18 0.567
Overbite (mm) 5.64 1.23 5.07 1.36 –0.57 0.017*
Dental cast variables
6-RP (mm) 23.35 1.62 27.08 2.67 3.73 0.000†
5-RP or E-RP (mm) 13.35 1.58 11.87 2.19 –1.48 0.000†
6-ML (mm) 21.98 1.14 23.35 1.17 1.37 0.000†
6-ML rotation (�) 33.77 5.04 34.67 5.00 0.90 0.051
1-RP (mm) 11.07 2.20 11.13 2.22 0.06 0.675
*P \0.05; †P \0.001.
American Journal of Orthodontics and Dentofacial Orthopedics Papadopoulos, Melkos, and Athanasiou 586.e7Volume 137, Number 5
The comparisons of the demographic characteristics(Table II) and the cephalometric and dental cast vari-ables before treatment of the treated and untreated sub-jects (Table I) showed no significant differences (exceptonly for the variable 6-ML rotation [degrees]), suggest-ing that the 2 groups were appropriately matched.
According to the results of this investigation, sig-nificant maxillary first molar distalization after theuse of the FCA for 4 months measured on cephalomet-ric radiographs (4.00 mm) and dental casts (3.73 mm)was evident in relation to both the pretreatmentcondition of the patients and the changes observed inthe untreated control group (Tables III and V). Thecorresponding changes of maxillary first molarmovement for the untreated group were 0.04 and0.39 mm, respectively.
The rate of molar movement was 1.01 mm permonth; this is actually a similar or even a higher ratecompared with the corresponding rates reported forother noncompliance appliances. For example, the rateswere 0.55 to 1.03 mm per month for the pendulum ap-pliance,30,35-38 0.31 to 0.64 mm per month for thedistal jet,39-41 and 0.37 to 0.93 mm per month for theJones jig and other similar appliances.42-48 Only in thestudy of Fortini et al25 investigating the changes aftertreatment with the FCA was there a higher rate of 1.7mm per month (Table VI).11
However, the aforementioned maxillary molar dis-talization did not take place bodily but with significantdistal crown tipping of 8.56� in relation to the SNline; in contrast, the maxillary molars of the untreatedgroup had mesial tipping of the molar crowns of
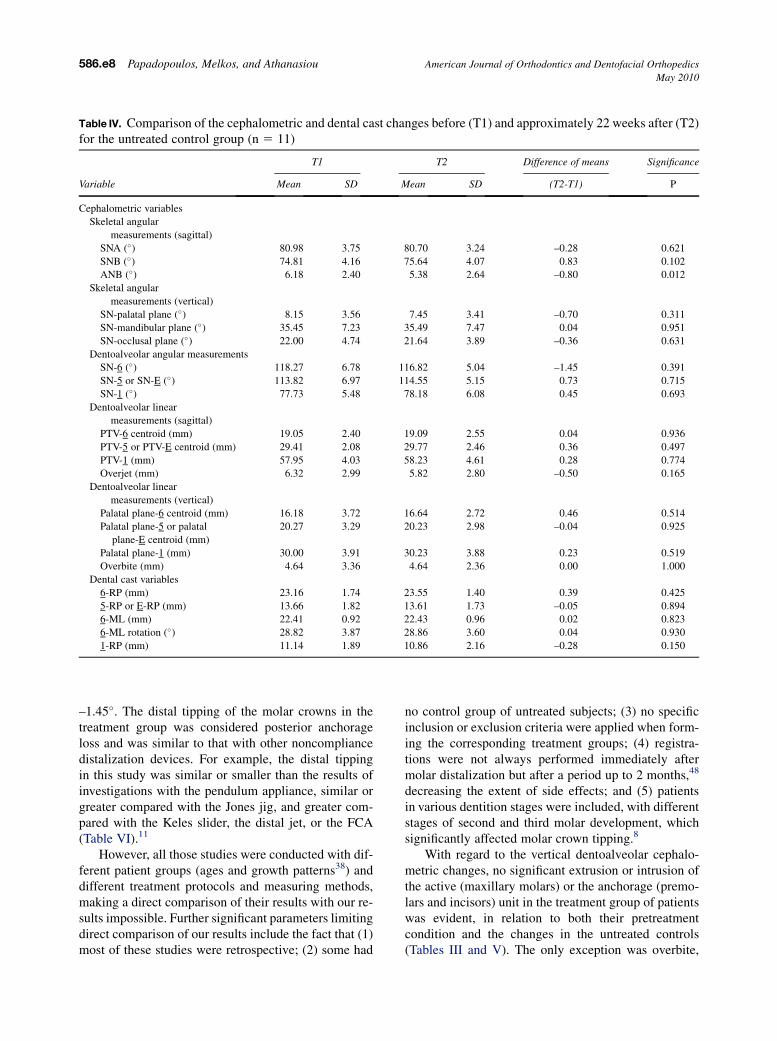
Table IV. Comparison of the cephalometric and dental cast changes before (T1) and approximately 22 weeks after (T2)for the untreated control group (n 5 11)
Variable
T1 T2 Difference of means Significance
Mean SD Mean SD (T2-T1) P
Cephalometric variables
Skeletal angular
measurements (sagittal)
SNA (�) 80.98 3.75 80.70 3.24 –0.28 0.621
SNB (�) 74.81 4.16 75.64 4.07 0.83 0.102
ANB (�) 6.18 2.40 5.38 2.64 –0.80 0.012
Skeletal angular
measurements (vertical)
SN-palatal plane (�) 8.15 3.56 7.45 3.41 –0.70 0.311
SN-mandibular plane (�) 35.45 7.23 35.49 7.47 0.04 0.951
SN-occlusal plane (�) 22.00 4.74 21.64 3.89 –0.36 0.631
Dentoalveolar angular measurements
SN-6 (�) 118.27 6.78 116.82 5.04 –1.45 0.391
SN-5 or SN-E (�) 113.82 6.97 114.55 5.15 0.73 0.715
SN-1 (�) 77.73 5.48 78.18 6.08 0.45 0.693
Dentoalveolar linear
measurements (sagittal)
PTV-6 centroid (mm) 19.05 2.40 19.09 2.55 0.04 0.936
PTV-5 or PTV-E centroid (mm) 29.41 2.08 29.77 2.46 0.36 0.497
PTV-1 (mm) 57.95 4.03 58.23 4.61 0.28 0.774
Overjet (mm) 6.32 2.99 5.82 2.80 –0.50 0.165
Dentoalveolar linear
measurements (vertical)
Palatal plane-6 centroid (mm) 16.18 3.72 16.64 2.72 0.46 0.514
Palatal plane-5 or palatal
plane-E centroid (mm)
20.27 3.29 20.23 2.98 –0.04 0.925
Palatal plane-1 (mm) 30.00 3.91 30.23 3.88 0.23 0.519
Overbite (mm) 4.64 3.36 4.64 2.36 0.00 1.000
Dental cast variables
6-RP (mm) 23.16 1.74 23.55 1.40 0.39 0.425
5-RP or E-RP (mm) 13.66 1.82 13.61 1.73 –0.05 0.894
6-ML (mm) 22.41 0.92 22.43 0.96 0.02 0.823
6-ML rotation (�) 28.82 3.87 28.86 3.60 0.04 0.930
1-RP (mm) 11.14 1.89 10.86 2.16 –0.28 0.150
586.e8 Papadopoulos, Melkos, and Athanasiou American Journal of Orthodontics and Dentofacial Orthopedics
May 2010
–1.45�. The distal tipping of the molar crowns in thetreatment group was considered posterior anchorageloss and was similar to that with other noncompliancedistalization devices. For example, the distal tippingin this study was similar or smaller than the results ofinvestigations with the pendulum appliance, similar orgreater compared with the Jones jig, and greater com-pared with the Keles slider, the distal jet, or the FCA(Table VI).11
However, all those studies were conducted with dif-ferent patient groups (ages and growth patterns38) anddifferent treatment protocols and measuring methods,making a direct comparison of their results with our re-sults impossible. Further significant parameters limitingdirect comparison of our results include the fact that (1)most of these studies were retrospective; (2) some had
no control group of untreated subjects; (3) no specificinclusion or exclusion criteria were applied when form-ing the corresponding treatment groups; (4) registra-tions were not always performed immediately aftermolar distalization but after a period up to 2 months,48
decreasing the extent of side effects; and (5) patientsin various dentition stages were included, with differentstages of second and third molar development, whichsignificantly affected molar crown tipping.8
With regard to the vertical dentoalveolar cephalo-metric changes, no significant extrusion or intrusion ofthe active (maxillary molars) or the anchorage (premo-lars and incisors) unit in the treatment group of patientswas evident, in relation to both their pretreatmentcondition and the changes in the untreated controls(Tables III and V). The only exception was overbite,
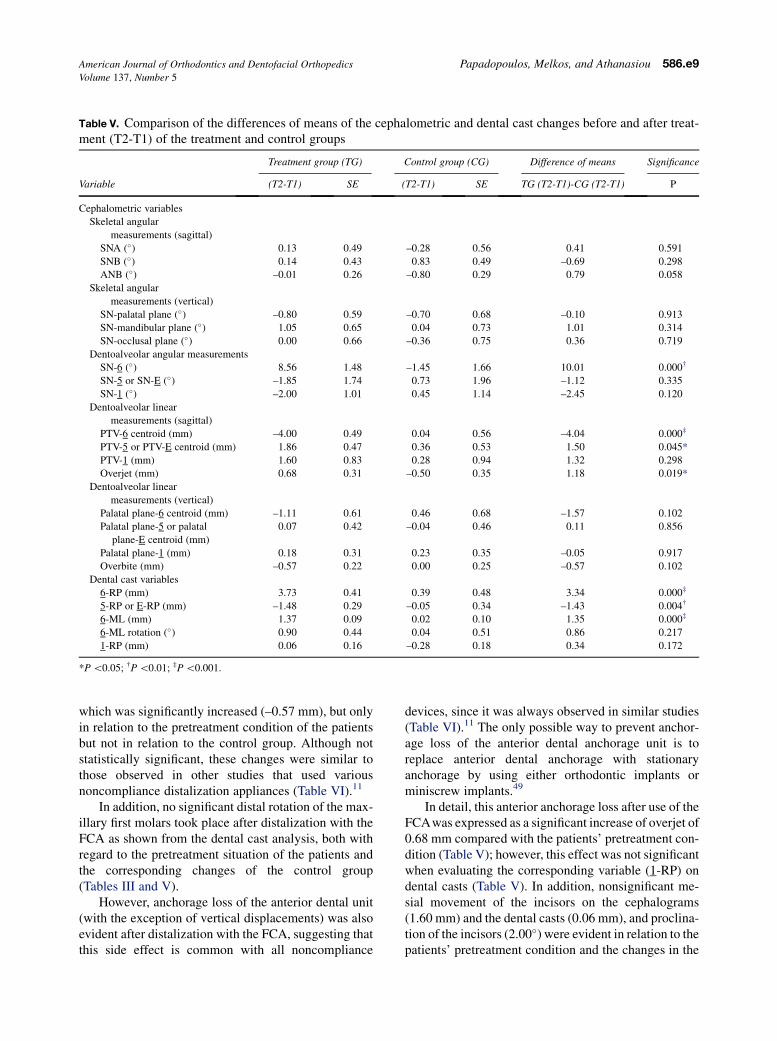
Table V. Comparison of the differences of means of the cephalometric and dental cast changes before and after treat-ment (T2-T1) of the treatment and control groups
Variable
Treatment group (TG) Control group (CG) Difference of means Significance
(T2-T1) SE (T2-T1) SE TG (T2-T1)-CG (T2-T1) P
Cephalometric variables
Skeletal angular
measurements (sagittal)
SNA (�) 0.13 0.49 –0.28 0.56 0.41 0.591
SNB (�) 0.14 0.43 0.83 0.49 –0.69 0.298
ANB (�) –0.01 0.26 –0.80 0.29 0.79 0.058
Skeletal angular
measurements (vertical)
SN-palatal plane (�) –0.80 0.59 –0.70 0.68 –0.10 0.913
SN-mandibular plane (�) 1.05 0.65 0.04 0.73 1.01 0.314
SN-occlusal plane (�) 0.00 0.66 –0.36 0.75 0.36 0.719
Dentoalveolar angular measurements
SN-6 (�) 8.56 1.48 –1.45 1.66 10.01 0.000†
SN-5 or SN-E (�) –1.85 1.74 0.73 1.96 –1.12 0.335
SN-1 (�) –2.00 1.01 0.45 1.14 –2.45 0.120
Dentoalveolar linear
measurements (sagittal)
PTV-6 centroid (mm) –4.00 0.49 0.04 0.56 –4.04 0.000‡
PTV-5 or PTV-E centroid (mm) 1.86 0.47 0.36 0.53 1.50 0.045*
PTV-1 (mm) 1.60 0.83 0.28 0.94 1.32 0.298
Overjet (mm) 0.68 0.31 –0.50 0.35 1.18 0.019*
Dentoalveolar linear
measurements (vertical)
Palatal plane-6 centroid (mm) –1.11 0.61 0.46 0.68 –1.57 0.102
Palatal plane-5 or palatal
plane-E centroid (mm)
0.07 0.42 –0.04 0.46 0.11 0.856
Palatal plane-1 (mm) 0.18 0.31 0.23 0.35 –0.05 0.917
Overbite (mm) –0.57 0.22 0.00 0.25 –0.57 0.102
Dental cast variables
6-RP (mm) 3.73 0.41 0.39 0.48 3.34 0.000‡
5-RP or E-RP (mm) –1.48 0.29 –0.05 0.34 –1.43 0.004†
6-ML (mm) 1.37 0.09 0.02 0.10 1.35 0.000‡
6-ML rotation (�) 0.90 0.44 0.04 0.51 0.86 0.217
1-RP (mm) 0.06 0.16 –0.28 0.18 0.34 0.172
*P \0.05; †P \0.01; ‡P \0.001.
American Journal of Orthodontics and Dentofacial Orthopedics Papadopoulos, Melkos, and Athanasiou 586.e9Volume 137, Number 5
which was significantly increased (–0.57 mm), but onlyin relation to the pretreatment condition of the patientsbut not in relation to the control group. Although notstatistically significant, these changes were similar tothose observed in other studies that used variousnoncompliance distalization appliances (Table VI).11
In addition, no significant distal rotation of the max-illary first molars took place after distalization with theFCA as shown from the dental cast analysis, both withregard to the pretreatment situation of the patients andthe corresponding changes of the control group(Tables III and V).
However, anchorage loss of the anterior dental unit(with the exception of vertical displacements) was alsoevident after distalization with the FCA, suggesting thatthis side effect is common with all noncompliance
devices, since it was always observed in similar studies(Table VI).11 The only possible way to prevent anchor-age loss of the anterior dental anchorage unit is toreplace anterior dental anchorage with stationaryanchorage by using either orthodontic implants orminiscrew implants.49
In detail, this anterior anchorage loss after use of theFCAwas expressed as a significant increase of overjet of0.68 mm compared with the patients’ pretreatment con-dition (Table V); however, this effect was not significantwhen evaluating the corresponding variable (1-RP) ondental casts (Table V). In addition, nonsignificant me-sial movement of the incisors on the cephalograms(1.60 mm) and the dental casts (0.06 mm), and proclina-tion of the incisors (2.00�) were evident in relation to thepatients’ pretreatment condition and the changes in the
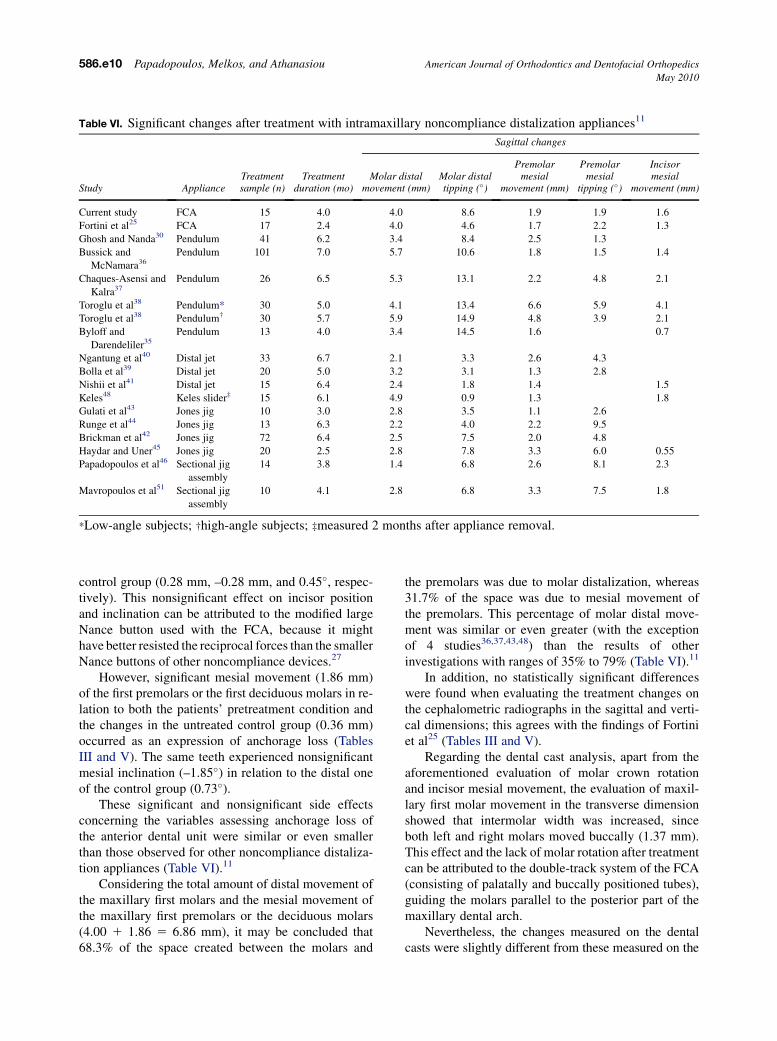
Table VI. Significant changes after treatment with intramaxillary noncompliance distalization appliances11
Study Appliance
Sagittal changes
Treatmentsample (n)
Treatmentduration (mo)
Molar distalmovement (mm)
Molar distaltipping (�)
Premolarmesial
movement (mm)
Premolarmesial
tipping (�)
Incisormesial
movement (mm)
Current study FCA 15 4.0 4.0 8.6 1.9 1.9 1.6
Fortini et al25 FCA 17 2.4 4.0 4.6 1.7 2.2 1.3
Ghosh and Nanda30 Pendulum 41 6.2 3.4 8.4 2.5 1.3
Bussick and
McNamara36Pendulum 101 7.0 5.7 10.6 1.8 1.5 1.4
Chaques-Asensi and
Kalra37Pendulum 26 6.5 5.3 13.1 2.2 4.8 2.1
Toroglu et al38 Pendulum* 30 5.0 4.1 13.4 6.6 5.9 4.1
Toroglu et al38 Pendulum† 30 5.7 5.9 14.9 4.8 3.9 2.1
Byloff and
Darendeliler35Pendulum 13 4.0 3.4 14.5 1.6 0.7
Ngantung et al40 Distal jet 33 6.7 2.1 3.3 2.6 4.3
Bolla et al39 Distal jet 20 5.0 3.2 3.1 1.3 2.8
Nishii et al41 Distal jet 15 6.4 2.4 1.8 1.4 1.5
Keles48 Keles slider‡ 15 6.1 4.9 0.9 1.3 1.8
Gulati et al43 Jones jig 10 3.0 2.8 3.5 1.1 2.6
Runge et al44 Jones jig 13 6.3 2.2 4.0 2.2 9.5
Brickman et al42 Jones jig 72 6.4 2.5 7.5 2.0 4.8
Haydar and Uner45 Jones jig 20 2.5 2.8 7.8 3.3 6.0 0.55
Papadopoulos et al46 Sectional jig
assembly
14 3.8 1.4 6.8 2.6 8.1 2.3
Mavropoulos et al51 Sectional jig
assembly
10 4.1 2.8 6.8 3.3 7.5 1.8
*Low-angle subjects; †high-angle subjects; ‡measured 2 months after appliance removal.
586.e10 Papadopoulos, Melkos, and Athanasiou American Journal of Orthodontics and Dentofacial Orthopedics
May 2010
control group (0.28 mm, –0.28 mm, and 0.45�, respec-tively). This nonsignificant effect on incisor positionand inclination can be attributed to the modified largeNance button used with the FCA, because it mighthave better resisted the reciprocal forces than the smallerNance buttons of other noncompliance devices.27
However, significant mesial movement (1.86 mm)of the first premolars or the first deciduous molars in re-lation to both the patients’ pretreatment condition andthe changes in the untreated control group (0.36 mm)occurred as an expression of anchorage loss (TablesIII and V). The same teeth experienced nonsignificantmesial inclination (–1.85�) in relation to the distal oneof the control group (0.73�).
These significant and nonsignificant side effectsconcerning the variables assessing anchorage loss ofthe anterior dental unit were similar or even smallerthan those observed for other noncompliance distaliza-tion appliances (Table VI).11
Considering the total amount of distal movement ofthe maxillary first molars and the mesial movement ofthe maxillary first premolars or the deciduous molars(4.00 1 1.86 5 6.86 mm), it may be concluded that68.3% of the space created between the molars and
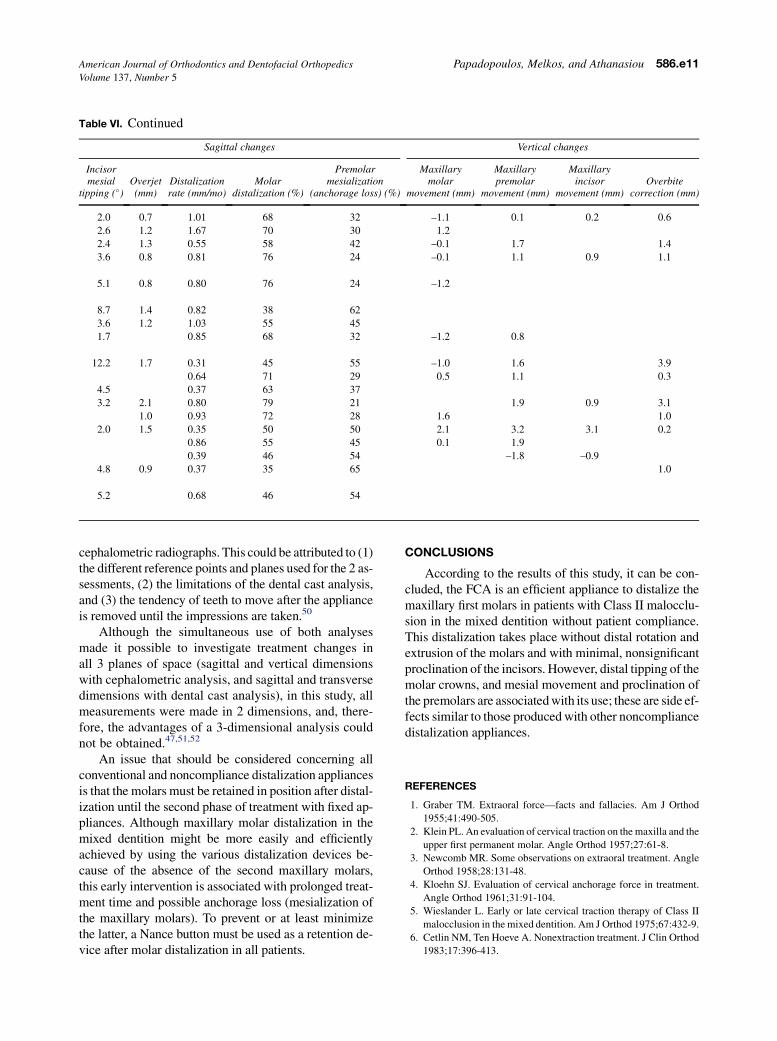
the premolars was due to molar distalization, whereas31.7% of the space was due to mesial movement ofthe premolars. This percentage of molar distal move-ment was similar or even greater (with the exceptionof 4 studies36,37,43,48) than the results of otherinvestigations with ranges of 35% to 79% (Table VI).11
In addition, no statistically significant differenceswere found when evaluating the treatment changes onthe cephalometric radiographs in the sagittal and verti-cal dimensions; this agrees with the findings of Fortiniet al25 (Tables III and V).
Regarding the dental cast analysis, apart from theaforementioned evaluation of molar crown rotationand incisor mesial movement, the evaluation of maxil-lary first molar movement in the transverse dimensionshowed that intermolar width was increased, sinceboth left and right molars moved buccally (1.37 mm).This effect and the lack of molar rotation after treatmentcan be attributed to the double-track system of the FCA(consisting of palatally and buccally positioned tubes),guiding the molars parallel to the posterior part of themaxillary dental arch.
Nevertheless, the changes measured on the dentalcasts were slightly different from these measured on the
Sagittal changes Vertical changes
Incisormesial
tipping (�)Overjet(mm)
Distalizationrate (mm/mo)
Molardistalization (%)
Premolarmesialization
(anchorage loss) (%)
Maxillarymolar
movement (mm)
Maxillarypremolar
movement (mm)
Maxillaryincisor
movement (mm)Overbite
correction (mm)
2.0 0.7 1.01 68 32 –1.1 0.1 0.2 0.6
2.6 1.2 1.67 70 30 1.2
2.4 1.3 0.55 58 42 –0.1 1.7 1.4
3.6 0.8 0.81 76 24 –0.1 1.1 0.9 1.1
5.1 0.8 0.80 76 24 –1.2
8.7 1.4 0.82 38 62
3.6 1.2 1.03 55 45
1.7 0.85 68 32 –1.2 0.8
12.2 1.7 0.31 45 55 –1.0 1.6 3.9
0.64 71 29 0.5 1.1 0.3
4.5 0.37 63 37
3.2 2.1 0.80 79 21 1.9 0.9 3.1
1.0 0.93 72 28 1.6 1.0
2.0 1.5 0.35 50 50 2.1 3.2 3.1 0.2
0.86 55 45 0.1 1.9
0.39 46 54 –1.8 –0.9
4.8 0.9 0.37 35 65 1.0
5.2 0.68 46 54
Table VI. Continued
American Journal of Orthodontics and Dentofacial Orthopedics Papadopoulos, Melkos, and Athanasiou 586.e11Volume 137, Number 5
cephalometric radiographs. This could be attributed to (1)the different reference points and planes used for the 2 as-sessments, (2) the limitations of the dental cast analysis,and (3) the tendency of teeth to move after the applianceis removed until the impressions are taken.50
Although the simultaneous use of both analysesmade it possible to investigate treatment changes inall 3 planes of space (sagittal and vertical dimensionswith cephalometric analysis, and sagittal and transversedimensions with dental cast analysis), in this study, allmeasurements were made in 2 dimensions, and, there-fore, the advantages of a 3-dimensional analysis couldnot be obtained.47,51,52
An issue that should be considered concerning allconventional and noncompliance distalization appliancesis that the molars must be retained in position after distal-ization until the second phase of treatment with fixed ap-pliances. Although maxillary molar distalization in themixed dentition might be more easily and efficientlyachieved by using the various distalization devices be-cause of the absence of the second maxillary molars,this early intervention is associated with prolonged treat-ment time and possible anchorage loss (mesialization ofthe maxillary molars). To prevent or at least minimizethe latter, a Nance button must be used as a retention de-vice after molar distalization in all patients.
CONCLUSIONS
According to the results of this study, it can be con-cluded, the FCA is an efficient appliance to distalize themaxillary first molars in patients with Class II malocclu-sion in the mixed dentition without patient compliance.This distalization takes place without distal rotation andextrusion of the molars and with minimal, nonsignificantproclination of the incisors. However, distal tipping of themolar crowns, and mesial movement and proclination ofthe premolars are associated with its use; these are side ef-fects similar to those produced with other noncompliancedistalization appliances.
REFERENCES
1. Graber TM. Extraoral force—facts and fallacies. Am J Orthod
1955;41:490-505.
2. Klein PL. An evaluation of cervical traction on the maxilla and the
upper first permanent molar. Angle Orthod 1957;27:61-8.
3. Newcomb MR. Some observations on extraoral treatment. Angle
Orthod 1958;28:131-48.
4. Kloehn SJ. Evaluation of cervical anchorage force in treatment.
Angle Orthod 1961;31:91-104.
5. Wieslander L. Early or late cervical traction therapy of Class II
malocclusion in the mixed dentition. Am J Orthod 1975;67:432-9.
6. Cetlin NM, Ten Hoeve A. Nonextraction treatment. J Clin Orthod
1983;17:396-413.
586.e12 Papadopoulos, Melkos, and Athanasiou American Journal of Orthodontics and Dentofacial Orthopedics
May 2010
7. Papadopoulos MA. Non-compliance distalization: a monograph
on the clinical management and effectiveness of a jig assembly
in Class II malocclusion orthodontic treatment. Thessaloniki,
Greece: Phototypotiki; 2005.
8. Kinzinger GS, Fritz UB, Sander FG, Diedrich PR. Efficiency of
a pendulum appliance for molar distalization related to second
and third molar eruption stage. Am J Orthod Dentofacial Orthop
2004;125:8-23.
9. Kinzinger G, Fritz U, Diedrich P. Combined therapy with pendu-
lum and lingual arch appliances in the early mixed dentition.
J Orofac Orthop 2003;64:201-13.
10. Kinzinger G, Fuhrmann R, Gross U, Diedrich P. Modified pendu-
lum appliance including distal screw and uprighting activation for
non-compliance therapy of Class II malocclusion in children and
adolescents. J Orofac Orthop 2000;61:175-90.
11. Papadopoulos MA. Clinical efficacy of the non-compliance
appliances used for Class II orthodontic correction. In:
Papadopoulos MA, editor. Orthodontic treatment for the Class
II non-compliant patient: current principles and techniques. Edin-
burgh, United Kingdom: Elsevier, Mosby; 2006. p. 367-87.
12. Bondemark L, Kurol J. Distalization of maxillary first and second
molars simultaneously with repelling magnets. Eur J Orthod
1992;14:264-72.
13. Gianelly AA, Bednar J, Dietz VS. Japanese NiTi coils used to
move molars distally. Am J Orthod Dentofacial Orthop 1991;99.
564–546.
14. Gianelly AA, Vaitas AS, Thomas WM. The use of magnets to
move molars distally. Am J Orthod Dentofacial Orthop 1989;
96:161-7.
15. McSherry PF, Bradley H. Class II correction-reducing patient
compliance: a review of the available techniques. J Orthod
2000;27:219-25.
16. Jeckel N, Rakosi T. Molar distalization by intra-oral force appli-
cation. Eur J Orthod 1991;13:43-6.
17. Jones RD, White JM. Rapid Class II molar correction with an
open-coil jig. J Clin Orthod 1992;26:661-4.
18. Papadopoulos MA. Simultaneous distalization of maxillary first
and second molars by means of superelastic NiTi coils. Hell
Orthod Rev 1998;1:71-6.
19. Fritz U, Ehmer A, Diedrich P. Clinical suitability of titanium mi-
croscrews for orthodontic anchorage—preliminary experiences.
J Orofac Orthop 2004;65:410-8.
20. Locatelli R, Bednar J, Dietz V, Giannelly AA. Molar distalization
with superelastic NiTi wire. J Clin Orthod 1992;26:66-72.
21. Sugawara J, Daimaruya T, Umemori M, Nagasaka H, Takahashi I,
Kawamura H, et al. Distal movement of mandibular molars in
adult patients with the skeletal anchorage system. Am J Orthod
Dentofacial Orthop 2004;125:130-8.
22. Carano A, Testa M. The distal jet for upper molar distalization.
J Clin Orthod 1996;30:374-80.
23. Puente M. Class II correction with an edgewise-modified Nance
appliance. J Clin Orthod 1997;31:178-82.
24. Reiner TJ. Modified Nance appliance for unilateral molar distal-
ization. J Clin Orthod 1992;26:402-4.
25. Fortini A, Lupoli M, Giuntoli F, Franchi L. Dentoskeletal effects
induced by rapid molar distalization with the first class appliance.
Am J Orthod Dentofacial Orthop 2004;125:697-705.
26. Fortini A, Lupoli M, Parri M. The first class appliance for rapid
molar distalization. J Clin Orthod 1999;33:322-8.
27. Fortini A, Franchi F. The first class appliance. In:
Papadopoulos MA, editor. Orthodontic treatment for the Class
II non-compliant patient: current principles and techniques. Edin-
burgh, United Kingdom: Elsevier, Mosby; 2006. p. 309-29.
28. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible
statistical power analysis program for the social, behavioral, and
biomedical sciences. Behav Res Methods 2007;39:175-91.
29. World Medical Association Declaration of Helsinki. Ethical prin-
ciples for medical research involving human subjects. Available
at: http://www.wma.net/e/policy/pdf/17c.pdf. Accessed October
27, 2008.
30. Ghosh J, Nanda RS. Evaluation of an intraoral maxillary molar
distalization technique. Am J Orthod Dentofacial Orthop 1996;
110:639-46.
31. Erverdi N, Koyuturk O, Kucukkeles N. Nickel-titanium coil
springs and repelling magnets: a comparison of two different
intra-oral molar distalization techniques. Br J Orthod 1997;24:
47-53.
32. Champagne M. Reliability of measurements from photocopies of
study models. J Clin Orthod 1992;26:648-50.
33. Dahlberg G. Statistical methods for medical and biological
students. New York: Interscience Publications; 1940.
34. Papadopoulos MA. Meta-analysis in evidence-based orthodon-
tics. Orthod Craniofac Res 2003;6:112-26.
35. Byloff FK, Darendeliler MA. Distal molar movement using the
pendulum appliance. Part 1: clinical and radiological evaluation.
Angle Orthod 1997;67:249-60.
36. Bussick TJ, McNamara JA. Dentoalveolar and skeletal changes
associated with the pendulum appliance. Am J Orthod Dentofacial
Orthop 2000;117:333-43.
37. Chaques-Asensi J, Kalra V. Effects of the pendulum appliance on
the dentofacial complex. J Clin Orthod 2001;35:254-7.
38. Toroglu MS, Uzel I, Cam OY, Hancioglu ZB. Cephalometric eval-
uation of the effects of pendulum appliance on various vertical
growth patterns and of the changes during short-term stabiliza-
tion. Clin Orthod Res 2001;4:15-27.
39. Bolla E, Muratore F, Carano A, Bowman J. Evaluation of maxil-
lary molar distalization with the distal jet: a comparison with other
contemporary methods. Angle Orthod 2002;72:481-94.
40. Ngantung V, Nanda RS, Bowman SJ. Posttreatment evaluation of
the distal jet appliance. Am J Orthod Dentofacial Orthop 2001;
120:178-85.
41. Nishii Y, Katada H, Yamaguchi H. Three-dimensional evaluation
of the distal jet appliance. World J Orthod 2002;3:321-7.
42. Brickman CD, Sinha PK, Nanda RS. Evaluation of the Jones jig
appliance for distal molar movement. Am J Orthod Dentofacial
Orthop 2000;120:526-34.
43. Gulati S, Kharbanda OP, Prakash H. Dental and skeletal changes
after intraoral molar distalization with sectional jig assembly. Am
J Orthod Dentofacial Orthop 1998;114:319-27.
44. Runge ME, Martin JT, Bukai F. Analysis of rapid molar distal
movement without patient cooperation. Am J Orthod Dentofacial
Orthop 1999;115:153-7.
45. Haydar S, Uner O. Comparison of Jones jig molar distalization ap-
pliance with extraoral traction. Am J Orthod Dentofacial Orthop
2000;117:49-53.
46. Papadopoulos MA, Mavropoulos A, Karamouzos A. Cephalomet-
ric changes following simultaneous first and second maxillary
molar distalization using a non-compliance intraoral appliance.
J Orofac Orthop 2004;65:123-36.
47. Mavropoulos A, Karamouzos A, Kiliaridis S, Papadopoulos MA.
Efficiency of noncompliance simoultaneous first and second
upper molar distalization: a three-dimensional tooth movement
analysis. Angle Orthod 2005;75:468-75.
48. Keles A. Maxillary unilateral molar distalization with sliding
mechanics: a preliminary investigation. Eur J Orthod 2001;23:
507-15.

American Journal of Orthodontics and Dentofacial Orthopedics Papadopoulos, Melkos, and Athanasiou 586.e13Volume 137, Number 5
49. Papadopoulos MA. Orthodontic treatment of Class II malocclu-
sion with miniscrew implants. Am J Orthod Dentofacial Orthop
2008;134:604.e1-16.
50. Fuziy A, Rodrigues de Almeida R, Janson G, Angelieri F,
Pinzan A. Sagittal, vertical, and transverse changes conse-
quent to maxillary molar distalization with the pendulum
appliance. Am J Orthod Dentofacial Orthop 2006;130:
502-10.
51. Mavropoulos A, Sayinsu K, Allaf F, Kiliaridis S,
Papadopoulos MA, Keles AO. Noncompliance unilateral maxil-
lary molar distalization: a three-dimensional tooth movement
analysis. Angle Orthod 2006;76:382-7.
52. Papadopoulos MA, Christou PK, Christou PK, Athanasiou AE,
Boettcher P, Zeilhofer HF, et al. Three-dimensional craniofacial
reconstruction imaging. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2002;93:382-93.


















