Non-Neoplastic Colon Disorders Randolph K Peterson, MD Department of Laboratory Medicine and...
54
Non-Neoplastic Colon Disorders Randolph K Peterson, MD Department of Laboratory Medicine and Pathology
-
Upload
hillary-ferguson -
Category
Documents
-
view
221 -
download
5
Transcript of Non-Neoplastic Colon Disorders Randolph K Peterson, MD Department of Laboratory Medicine and...

Non-Neoplastic Colon Disorders
Randolph K Peterson, MDDepartment of Laboratory Medicine
and Pathology
Colon Disorders: Review
• The colon is retroperitoneal for most of it’s length.
• Vascular supply:– Superior mesenteric artery: cecum, right colon,
transverse colon– Inferior mesenteric: descending colon, sigmoid
colon, proximal rectum– Hemorrhoidal branches of internal iliac: distal
rectum
Colon Disorders: Review (2)
• This vascular distribution produces “Watershed Areas,” at the points they meet:– Splenic Flexure– Rectum
• What this means is that during times of systemic ischemia/shock/hypovolemia/etc. these areas have a compromised vascular supply and may infarct!

Colon Disorders: Review (3)
• The colon has an intrinsic nervous supply: Auerbach’s plexus (within the muscularis), and Meissner’s plexus (submucosa).

Colon Disorders: Malformations
• Hirschsprung’s Disease– Failure of nueroblasts to migrate to the end of the
bowel: the distal portion is aganglionic.– ALWAYS involves the rectum (90% restricted to
rectum) and extends proximally to a varying degree.
– 80 % are male; 10 % have Down Syndrome; 4 % risk in siblings of affected individuals.
– Histo: no ganglion cells with patchy nerve hyperplasia in submucosa.
Colon Disorders: Malformations (2)
– Lack of peristalsis forms a functional obstruction– The distal portion dilates; “Megacolon.”– Surgical correction is required.• 5-10 % mortality rate due to electrolyte imbalances and
infection.
• Diverticula:– Outpouchings of Mucosa through a weakened
area of the muscularis– Symptomatic in only 20%

Colon Disorders: Malformations (3)
– Symptoms: abdominal discomfort and pain are variable. If inflamed/infected may fibrose, or form an abscess/perf/fistula.
• Hemorrhoids– Variceal dilations of the anal and perianal venous plexus– 5 % of population affected. Unusual under 30 except
for pregnant females.– Types:
• External: below anorectal line; inferior hemorrhoidal plexus• Internal: above; superior
Colon Disorders: Malformations (4)
• Angiodysplasia– Dilation and increased tortuosity of the submucosal
veins in the cecum and ascending colon.– Probably acquired.– May cause bleeding in elderly.
• Misc.:• Malrotation• Duplication• Imperforate anus

Colon Disorders: Inflammation
• Necrotizing Enterocolitis– Acute necrotizing inflammation of the small and large
intestine.– Affects INFANTS! Supossedly 10% of full term babies
(????). Most common in premies.– Peaks at 2-3 days of life following initiation of oral
feeding.– More common in formula fed babes.– Symptoms: Vary from mild tenderness to bleeding, perf.,
sepsis.– Most common in terminal Ilium, cecum, ascending colon.
Colon Disorders: InflammationInflammatory Bowel Disease
• Etiology: Unknown, Probably multifactorial• ?Genetic? (Families = 10x risk )– NOD2 = product of candidate gene at IBD1 locus on
chromosome 16– used by immune system cells to detect bacterial products
through activation of cytokines– Recently: IL23R mutation prevents cell from binding proinflammatory protein
INFLAMMATORY BOWEL DISEASE: ETIOLOGY (2)
• Infectious:– Virus: rota, EBV, CMV– Bacteria: Pseudomonas, M. Kansasii,
Chlamydia, Yersinia
• Current concept: Disease is product of overly-aggressive immune response to commensal bacteria in genetically predisposed person

INFLAMMATORY BOWEL DISEASE: ETIOLOGY (3)
• Immunologic:– Antibodies + immune complexes (1°? 2°?)– Cell-mediated: tissue lymphs (2°?)
• Other: vasculitis
IBD: CROHN DISEASE
• Chronic enteritis with recurrent acute
relapses
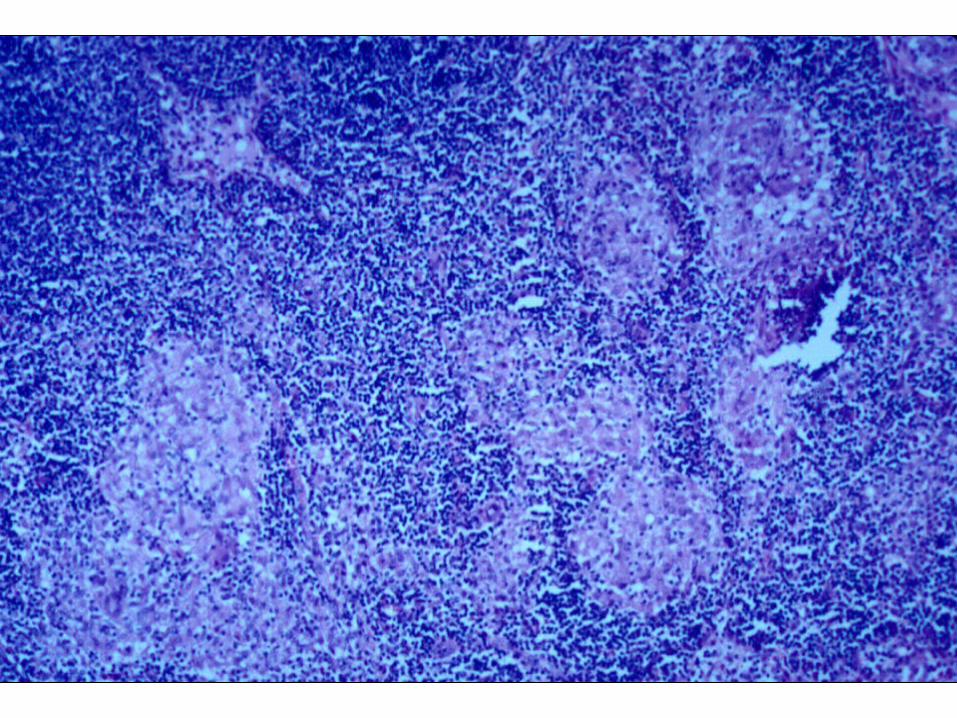
• Granulomatous inflammation
• Fibrosing
• Enteritis (any level)
• Idiopathic
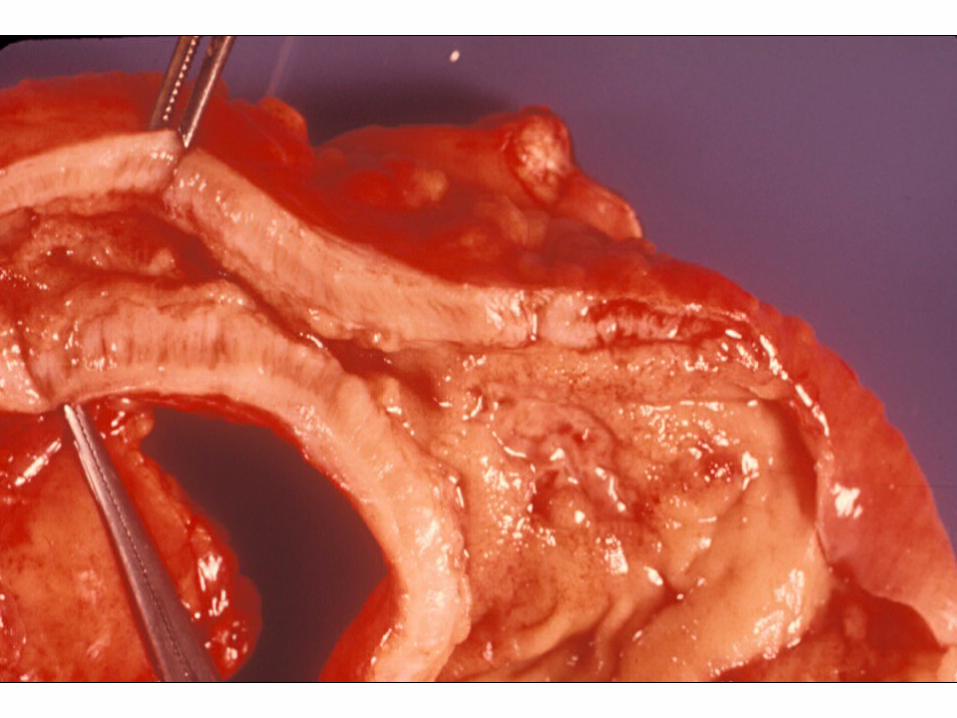
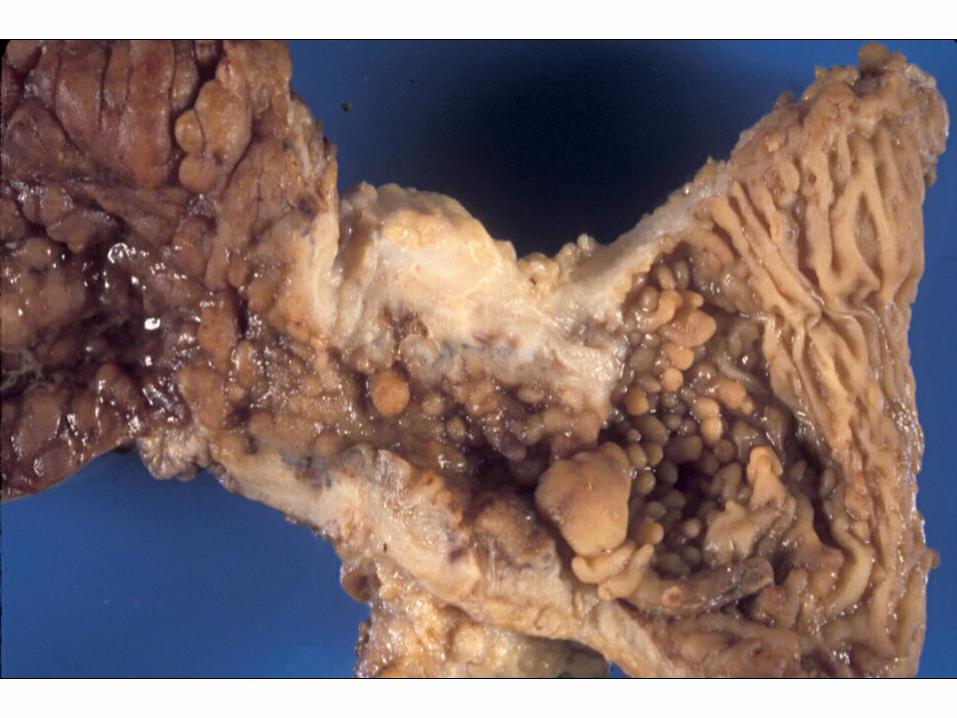
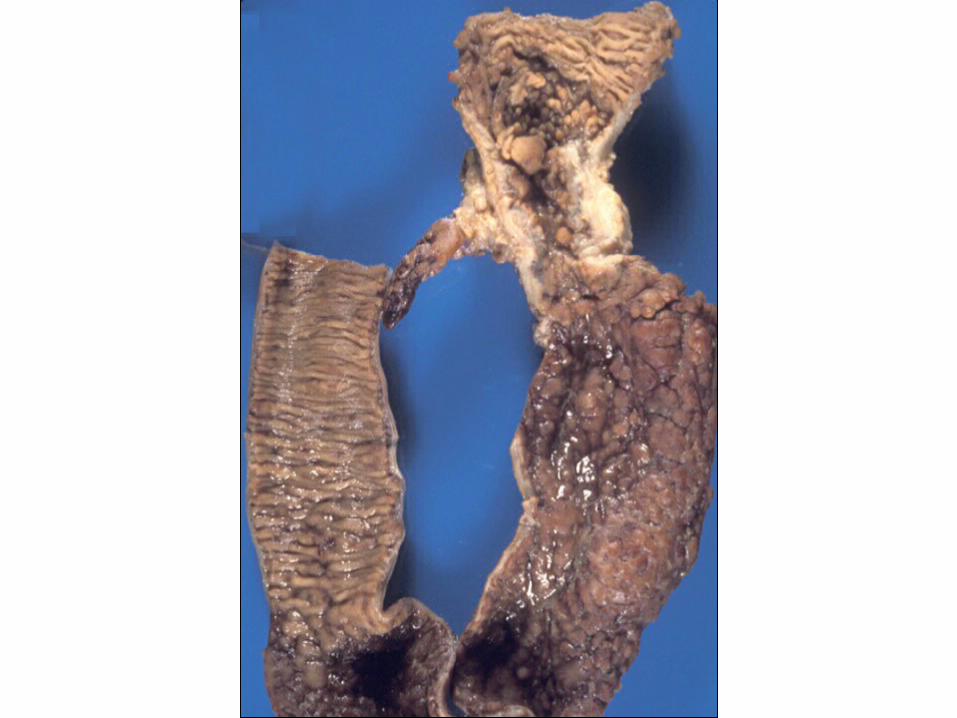
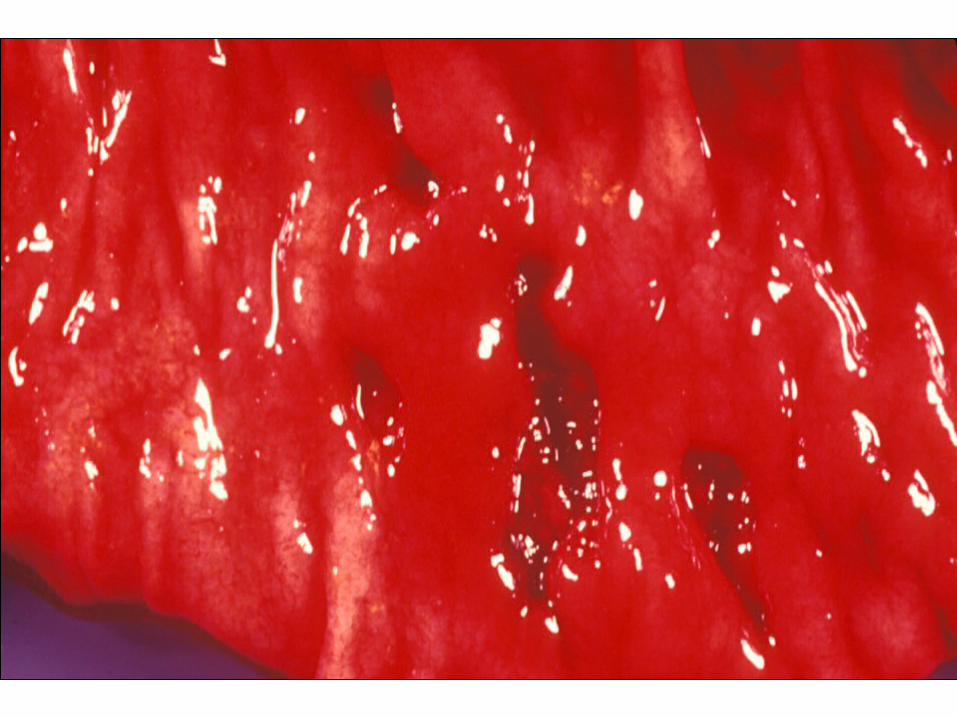
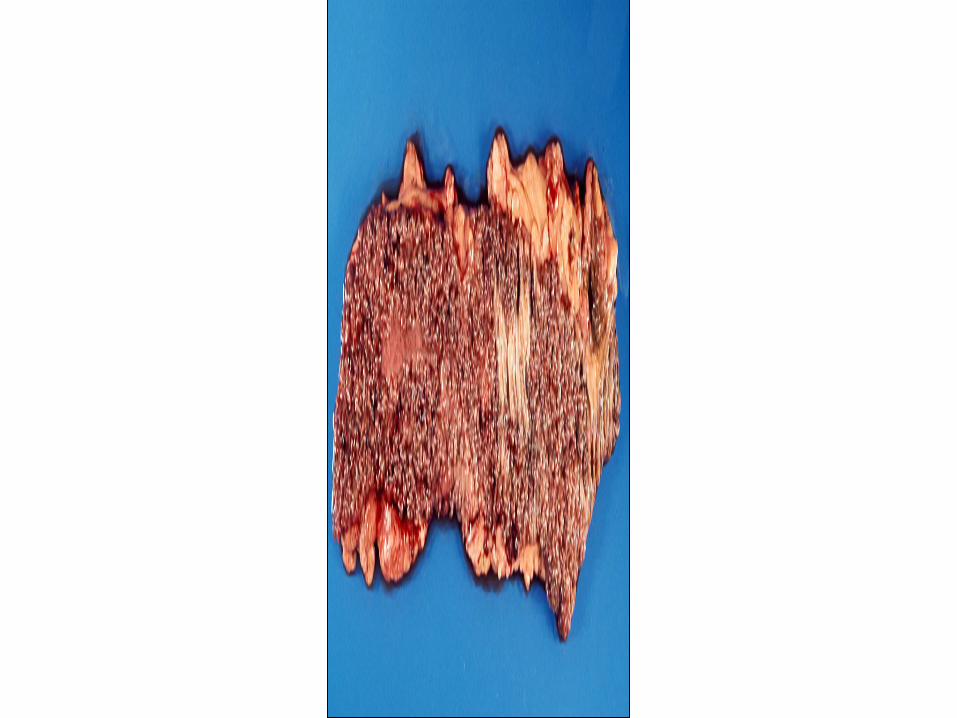
CROHN DISEASE: PATHOLOGY
• Transmural inflammation– wall thick, rigid, scarred
– granulomatous
– mucosal ulcers long, thin
• “Skip areas” common







CROHN DISEASE: LOCATION
• 40% ileum only
• 30% terminal ileum + colon
• 30% colon only


CROHN DISEASE: PATHOLOGY
• Transmural inflammation– wall thick, rigid, scarred
– granulomatous
– mucosal ulcers long, thin
• “Skip areas” common



CROHN DISEASE: COMPLICATIONS
• Stenosis• Fistulae (bowel, bladder, perineum)• Protein-losing enteropathy• Malabsorption• Systemic:– arthritis, uveitis, gallstones– cancer (local; distant) 3%

CROHN DISEASE: COMPLICATIONS
• Stenosis• Fistulae (bowel, bladder, perineum)• Protein-losing enteropathy• Malabsorption• Systemic:– arthritis, uveitis, gallstones– cancer (local; distant) 3%



CROHN DISEASE: COMPLICATIONS
• Stenosis• Fistulae (bowel, bladder, perineum)• Protein-losing enteropathy• Malabsorption• Systemic:– arthritis, uveitis, gallstones– cancer (local; distant) 3%

CROHN DISEASE: THERAPY (1)
• Reduce antigenic load:– anti-inflammatory agents:
• 5-aminosalicylates (mesalamine)• sulfasalazine• antibodies against tumor necrosis factor
(infliximab)—but serious side effects (activation of latent tb, lymphoma)
– total parenteral nutrition– surgical diversion
CROHN DISEASE: THERAPY (2)
• Immunosuppression:– Steroids (budesonide = local effect but minimal
systemic: rapid liver metabolize)– Immunosuppressives — azathioprine, methotrexate,
cyclosporine– T-cell apheresis– Anti-tumor necrosis factor alpha (TNF-a) monoclonal
antibody (cA2)—only for severe disease or fistulae. 60% improve.
• Other: fish oil diet; smoking ¯

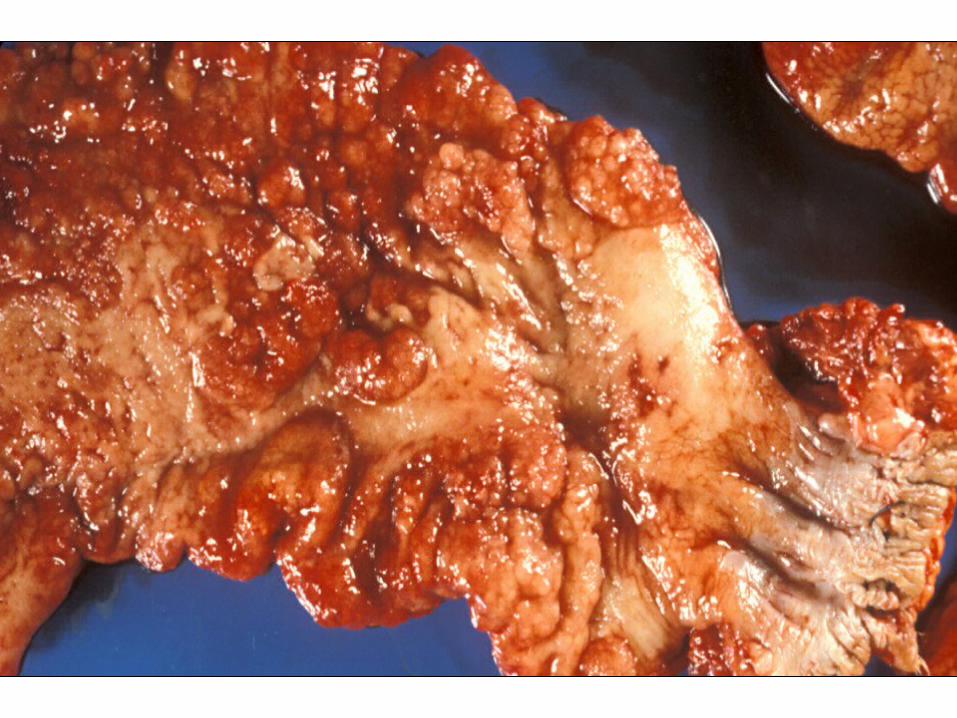
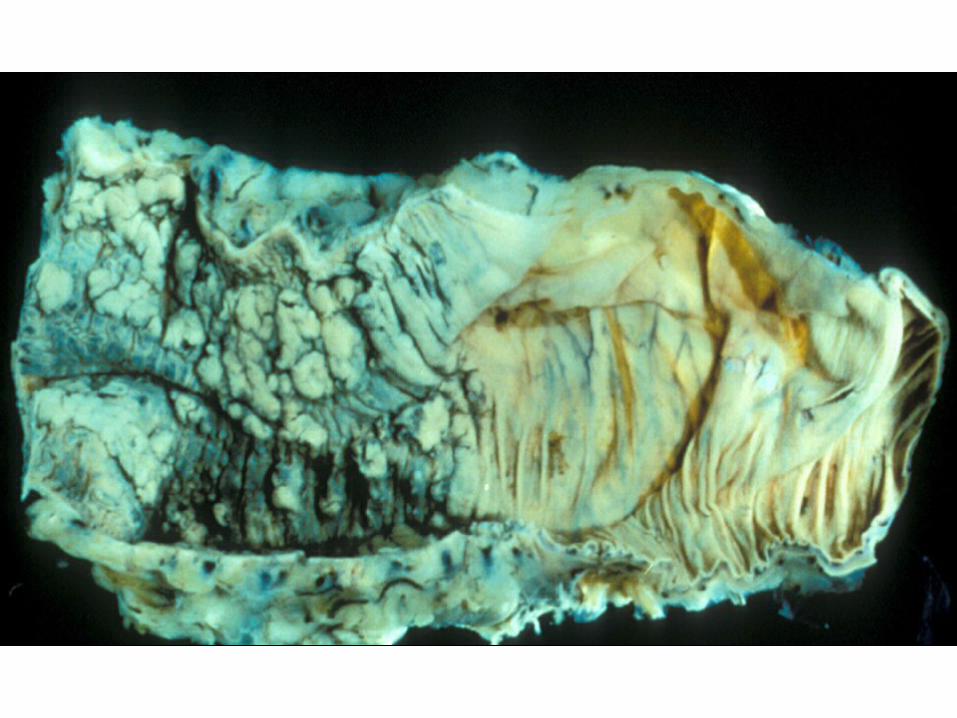
Ulcerative Colitis• Begins in rectum; progresses proximally• Limited to mucosa and submucosa• Nongranulomatous• No skip areas ("backwash ileitis")• Scarring mild• Ulcers: crypt abscess, irregular pseudopolyps• p-ANCA (peripheral-antineutrophile cytoplasmic
antibody) + 75% - 80% (only 8% in Crohn's)








Crohns UC
Site All of GI, extra GI Colon
Inflammation Granulomatous Non-granulomatous
Skip areas Present Absent
Wall Depth Full Thickness Mucosa
Fistula formation Yes No
Obstruction Yes No
Cancer 3% 30% +

CUC: COMPLICATIONS
• Stenosis: none• Fistulae: none• Protein-losing enteropathy: few• Malabsorption: rare• Systemic: primary sclerosing cholangitis
obstructive jaundice• Cancer: (duration & degree):
– 10 yrs <1%, 30 yrs 30%
• Toxic megacolon
CUC: COMPLICATIONS
• Stenosis: none• Fistulae: none• Protein-losing enteropathy: few• Malabsorption: rare• Systemic: as in Crohn disease, plus primary
sclerosing cholangitis obstructive jaundice• Cancer: (duration & degree):
– 10 yrs <1%, 30 yrs 30%
• Toxic megacolon

CUC: THERAPY
• Medical: – Sulfasalazine– Antigen-processing inhibitor (chloroquine)– Steroids– I.V. cyclosporine (T lymphs
• Surgical: colectomy with ileoanal anastomosis

Colon Disorders: InflammationNon IBD
• Ischemic Colitis– Most common in elderly in distal colon and
watershed areas.– Early: edema, hemorrhage– Late (Chronic): fibrosis, psuedomembranes,
psudopolyps• Infectious:– Acute self-limited Colitis• Numerous organisms.

Colon Disorders: InflammationNon IBD (2)
– Pseudomembranous Colitis• Caused by Clostridium difficile.• A pseudomembrane of fibrin and inflammatory cells• Most often involves the right colon• TEST for toxin in lab
– Other infections that may involve the colon: Amebic, TB, CMV, Cryptosporidiosis