Niyada. Orbital hematoma - Ophthalmologist consultation -Orbital massage,Off packing -Manitol 1-2...
56
niyada
-
Upload
ashlie-tate -
Category
Documents
-
view
217 -
download
0
Transcript of Niyada. Orbital hematoma - Ophthalmologist consultation -Orbital massage,Off packing -Manitol 1-2...

niyada
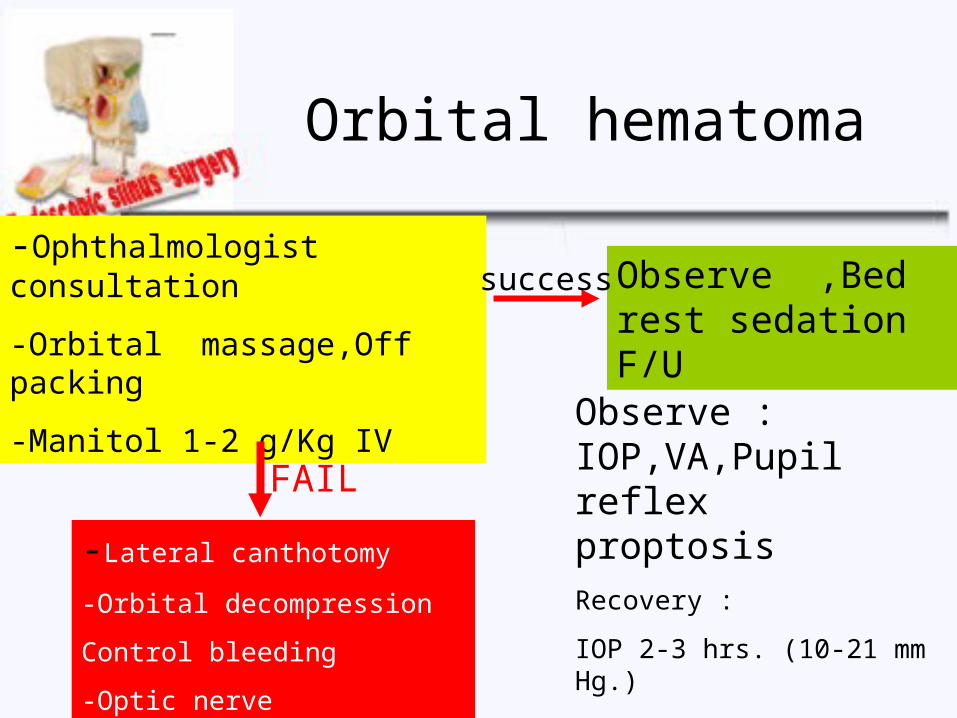
Orbital hematoma
-Ophthalmologist consultation
-Orbital massage,Off packing
-Manitol 1-2 g/Kg IV
-Lateral canthotomy
-Orbital decompression
Control bleeding
-Optic nerve decompression
Observe ,Bed rest sedation F/U
success
FAIL
Observe : IOP,VA,Pupil reflex proptosisRecovery :
IOP 2-3 hrs. (10-21 mm Hg.)
Light perception within 24 hrs.
Pupillary reflex : 24-48 hrs.

Prevention
• Pre-op CT scan evaluate unusual orbit anatomy
• Both eyes should be include in surgical field
• Preferred LA due to pain response
• Identify ant. ethmoidal artery that locate on posterior to ant. wall of EB

Prevention
• Palpate and compress the orbit when suspected LP injury

Blindness
• Temporary : transient increase IOP
• Permanent : directed optic nerve injury and prolonged IOP (60-90 min.)
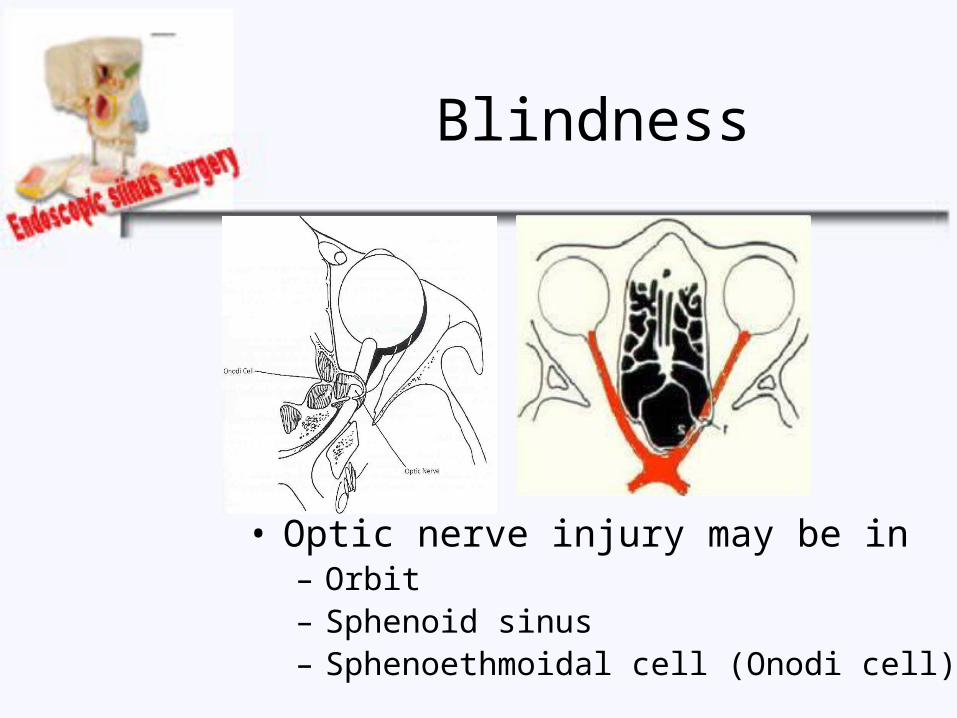
Blindness
• Optic nerve injury may be in – Orbit– Sphenoid sinus – Sphenoethmoidal cell (Onodi cell)

Blindness
• Optic canal– 98% at superolateral of sphenoid sinus – 4-12% bony dehiscence– 78% bony covering <0.5 mm. thickness– 65% of the optic nerve in Asians was present i
n the posterior ethmoid

Blindness
• Symptoms & signs– Severe pain– Acute VA drop– Pupil dilate and not react to light– Orbital hemorrhage

Blindness
• Treatment as orbital hemorrhage– Ophthalmologic consultation– Remove nasal packing– Systemic steroid (controversy)
• Dexamethasone 1 mg/kg then 0.5 mg/kg q 6 hr
– Optic nerve decompression if failure to conservation
Prevention
• Beware Intraoperation – Post. ethmoid sinus– Sphenoid sinus– Onodi cell
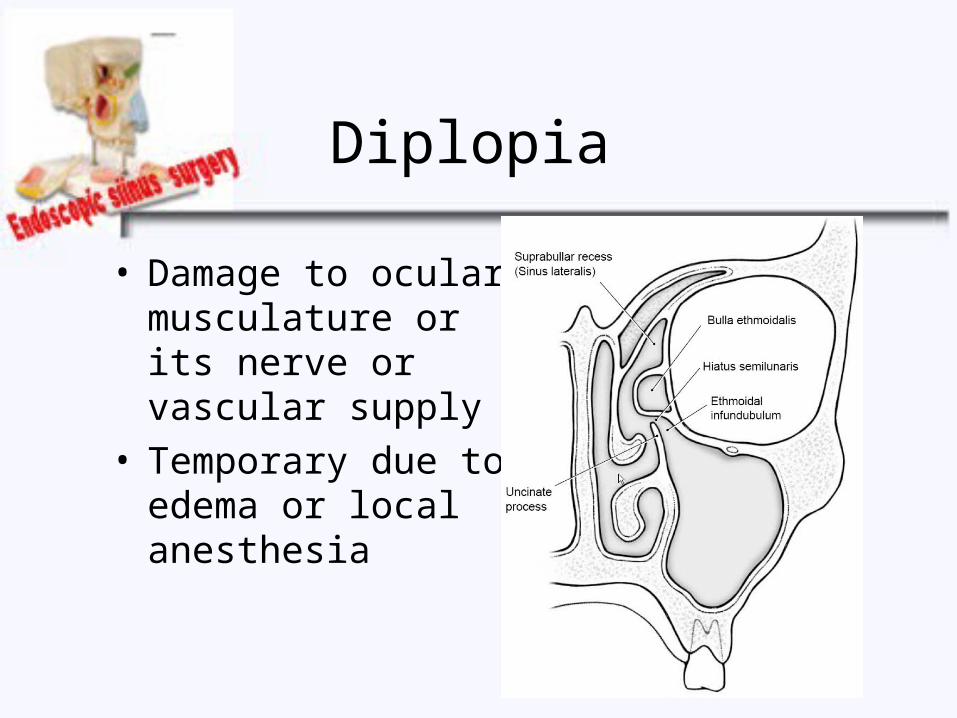
Diplopia
• Damage to ocular musculature or its nerve or vascular supply
• Temporary due to edema or local anesthesia
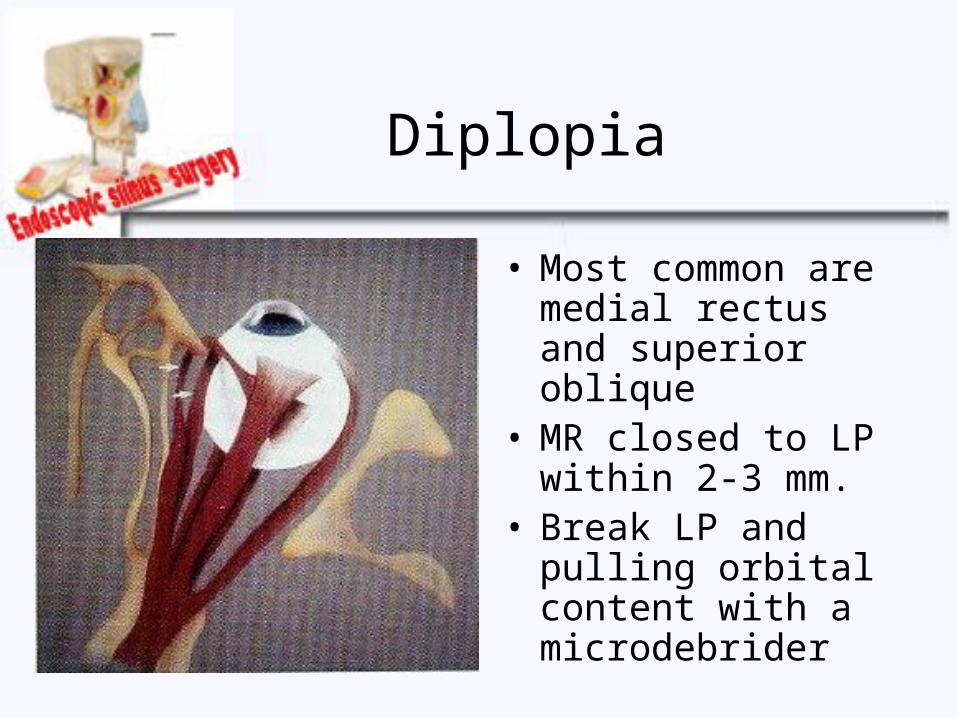
• Most common are medial rectus and superior oblique
• MR closed to LP within 2-3 mm.
• Break LP and pulling orbital content with a microdebrider
Diplopia


• Symptoms & Signs• Significant pain• Diplopia • Limitation of eye movement• Subconjunctival hemorrhage at medial side • Force duction test
Diplopia
Diplopia
• Urgent MRI evaluate muscle damage
• Immediate repair by ophthalmologist
• Poor prognosis
• Prevent as orbital hematoma

Nasolacrimal duct injury
• Cause– Over opening of ant. edge of the maxillary sinus ostium
• Post-op epiphora immediately or 1-2 wk. post-op• Occult injury about 15%

Nasolacrimal duct injury
• DCR in symptomatic patient
DCR : Dacryocystorhinostomy

Prevention
• Not performed anterior to ant. margin of MT
• Bone covering NLD is harder

Prevention
• Agger nasi cell is closed to lacrimal sac

Subcutaneous emphysema
• Small fracture of LP• Positive pressure via mask ventilation• Cough, vomit, or blow nose• Periorbital subcutaneous crepitation• Spontaneous resolve in 7-10 days

Intracranial complications

Intracranial complications
• CSF fistula (most common)• Meningitis • Brain abscess• ICH• Brain injury• Pneumocephalus

CSF fistula
• Incidence : 1 in every 200 to 500 cases
• Risk factors– Performed under GA
due to loss of pain at skull base
– Revision case– Extensive disease

CSF fistula
• Danger areas– Fovea ethmoidalis– Cribiform plate

CSF fistula
• Danger areas– Roof of ethmoid
and sphenoid– Area posterior to
ant. ethmoidal artery
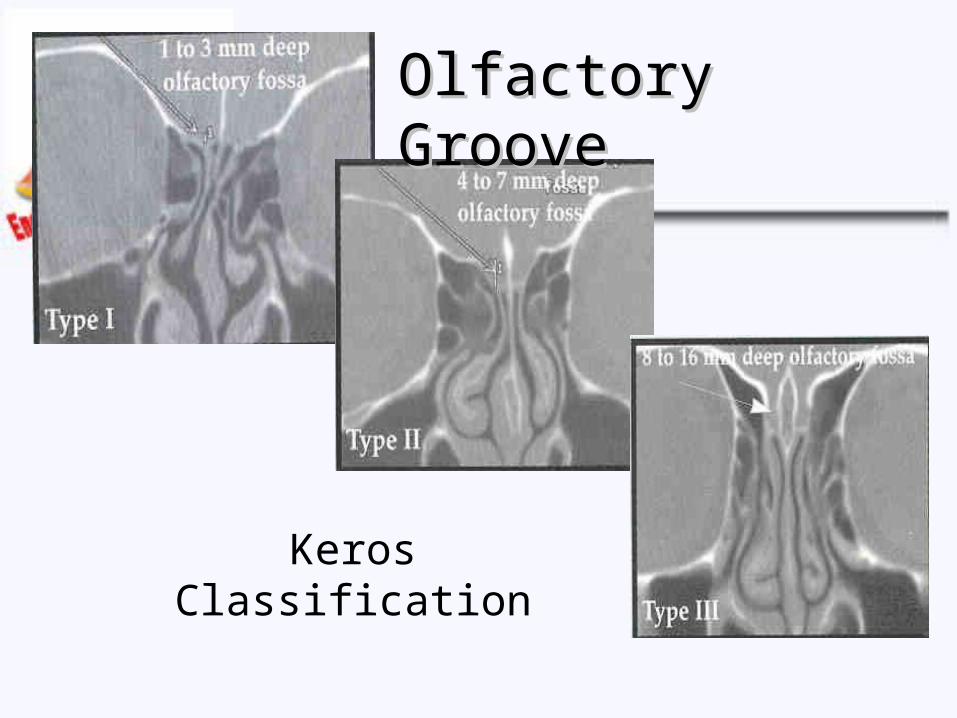
Olfactory GrooveOlfactory Groove
Keros Classification
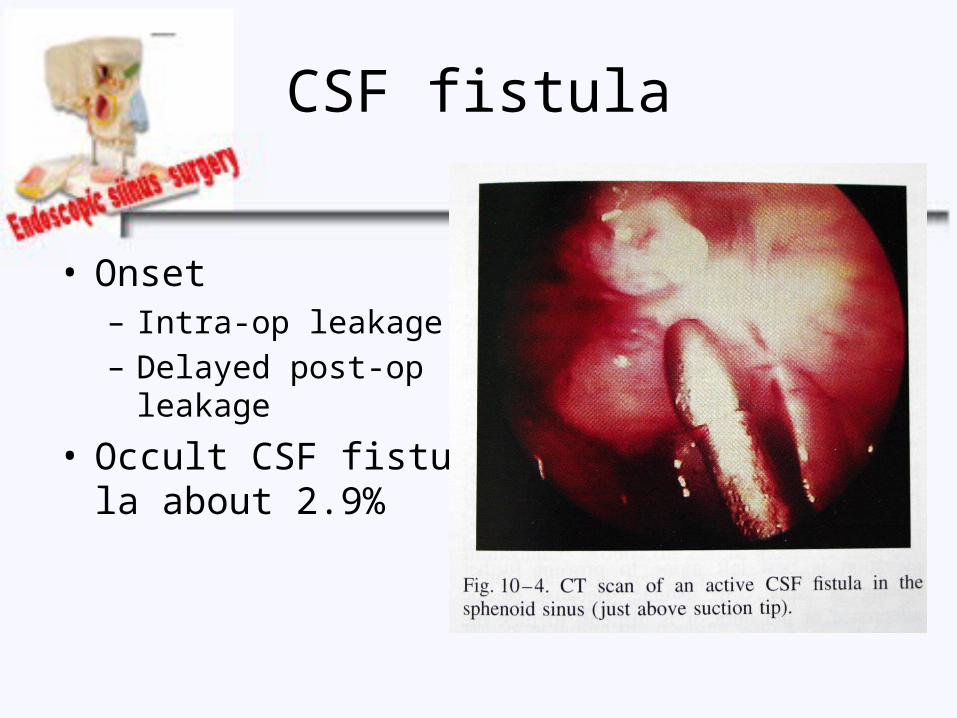
CSF fistula
• Onset – Intra-op leakage– Delayed post-op
leakage
• Occult CSF fistula about 2.9%

Intra-op leakage
• Diagnosis– Washout sign– Compress bilateral IJN
10-12 sec.
(Queckenstedt-stookey test)

Intra-op leakage
• IT fluorescine– Most popular– No FDA approved– 0.1 ml. of 10% fluorescine
(IV prep.) + 10 ml. of CSF– Infused slowly >30 min.– Grand Mal seizure : dose
related complication

Treatment
• Repaired immediately– Soft tissue patch : nasal mucosa, temporalis
fascia, fat, muscle, or dermal graft– Bone or cartilage bridge– Fibrin glue
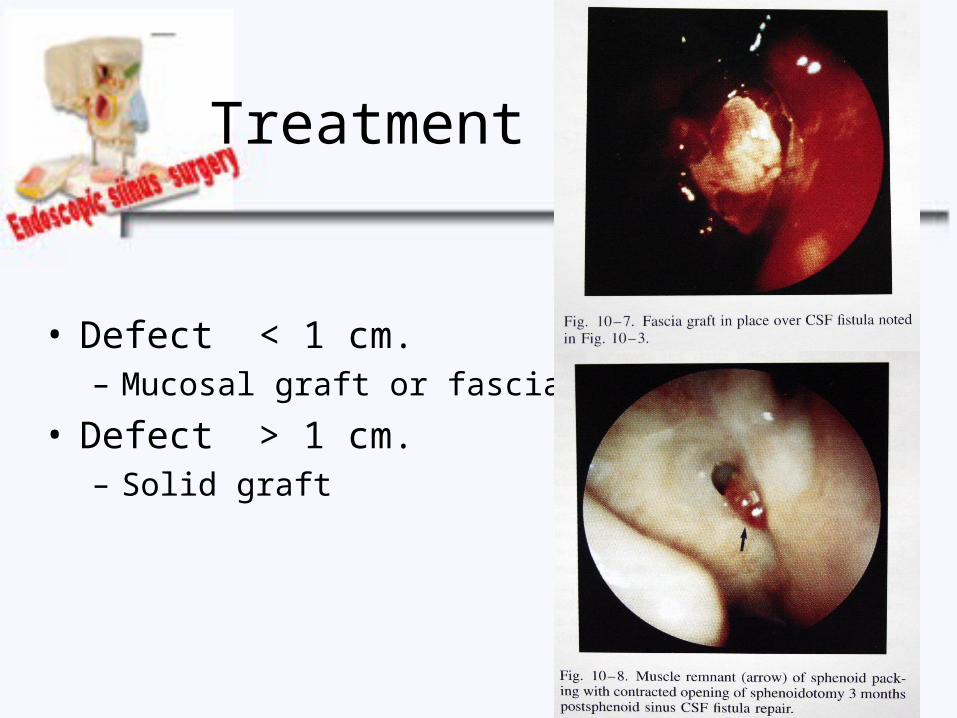
Treatment
• Defect < 1 cm. – Mucosal graft or fascia
• Defect > 1 cm.– Solid graft

Delayed post-op leakage
• Diagnosis
– Days, weeks, months, or years after procedure
– Clear intermittent rhinorrhea
– Associated lean forward position
Delayed post-op leakage
• Diagnosis– Hyposmia or headache– Halo sign : clear ring , central bloody spot– Endoscopic exam
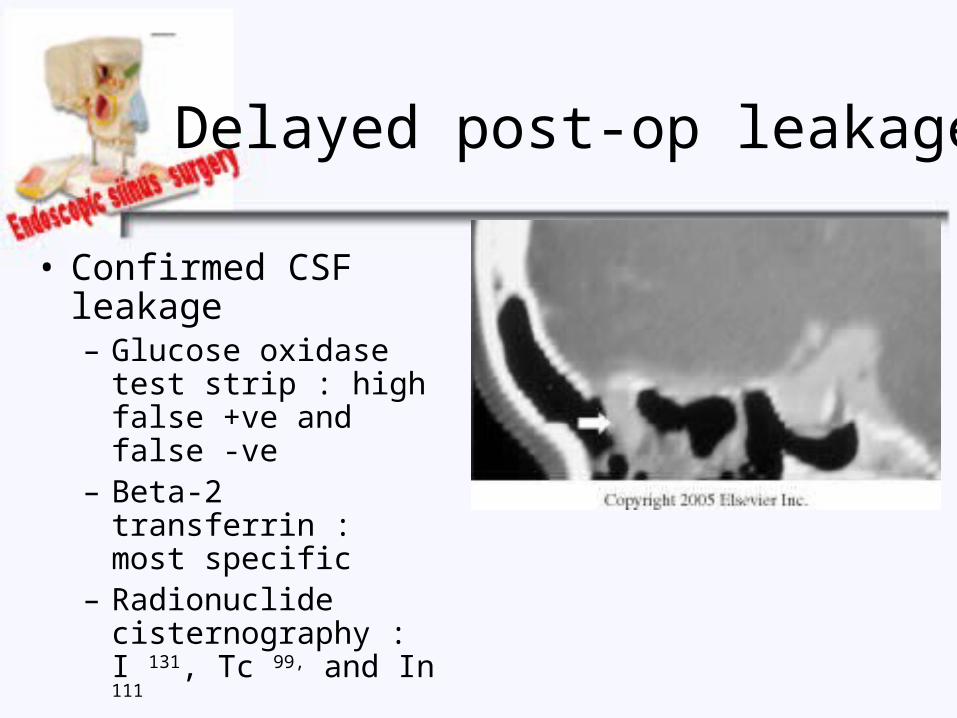
Delayed post-op leakage
• Confirmed CSF leakage– Glucose oxidase test
strip : high false +ve and false -ve
– Beta-2 transferrin : most specific
– Radionuclide cisternography : I 131, Tc 99, and In 111

Delayed post-op leakage
• Locate leakage site – Endoscopic exam– High resolution CT– IT fluorescein– CT cisternography
(metrizamide)– MR cisternography T2-
weighted with fat suppression
Treatment
• Small leakage often close spontaneously
• Conservative for 1-2 wk.
• Surgery when unresponsive
• Mostly need surgical intervention

Conservative treatment
• Strict bed rest
• Head elevation
• Stool softener
• Avoid cough, sneezing, nose blowing, and straining
• Lumbar drainage

Lumbar drainage
• Draining rate = 5-10 ml/hr
• Complication – Pneumocephalus : low ICP– Meningitis
• Prophylaxis ATB in case of sinusitis• Unwarranted prophylaxis ATB in traumatic case
• ATB prevent cellulitis at puncture site

Surgical treatment
• Transcranial approach
• Extracranial approach– Trans-sinus external approach– Endoscopic transnasal approach

Transcranial approach
• Craniotomy
• Tissue graft + fibrin glue– Fascia lata– Muscle plugs– Pedicle galeal flap

Transcranial approach
• Advantage– Multiple areas– Identify leakage site– Associated intracranial problem
• Disadvantage– Morbidity & mortality– Prolong hospital stay– Limited sphenoid sinus approach
Transcranial approach
• Morbidity– Brain compression – Hematoma– Seizure– Anosmia

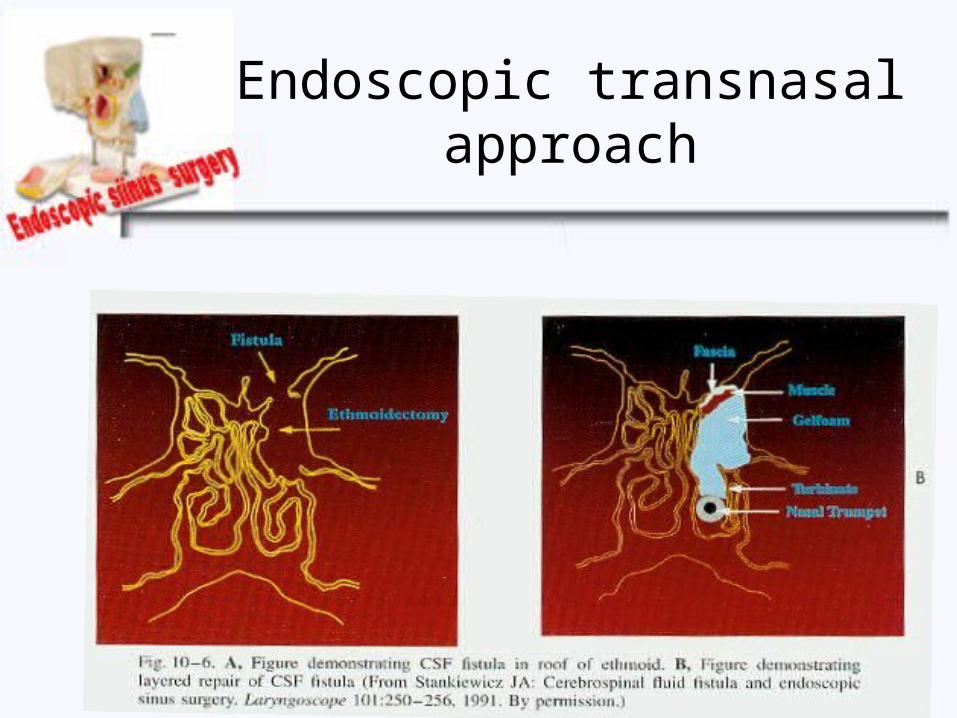
Endoscopic transnasal approach
• Advantage – Excellent visualization– Well tolerated– Excellent outcome (85-90%)
Endoscopic transnasal approach
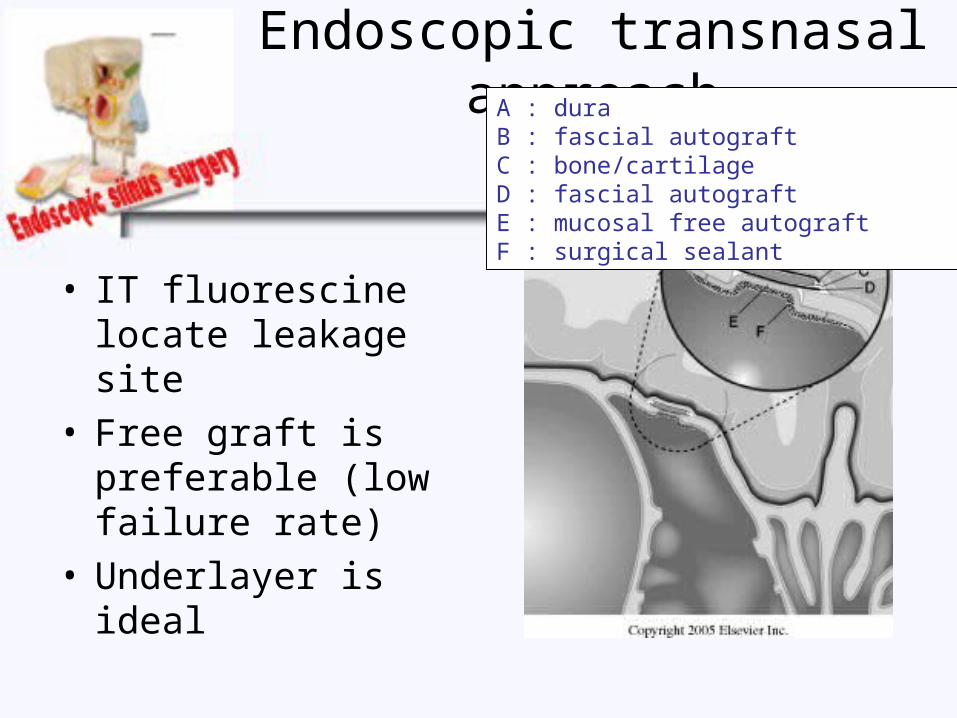
• IT fluorescine locate leakage site
• Free graft is preferable (low failure rate)
• Underlayer is ideal
A : duraB : fascial autograftC : bone/cartilageD : fascial autograftE : mucosal free autograftF : surgical sealant

Endoscopic transnasal approach
• Mucosal graft should never placed intracranially (intracranial mucocele)
• Nasal packing – Absorbable packing is placed adjacent the
graft– Non-absorbable packing support beneath
• Excellent access to ethmoid roof, cribiform plate, and sphenoid sinus
Endoscopic transnasal approach

Endoscopic transnasal approach
• Post-op care– Bed rest – Anti -staphylococcal ATB– Monitor intracranial complication in first 24 hr.– CSF drainage continued for 4-5 days– Avoid strenuous activity, sneezing, and cough
for 6 wks.
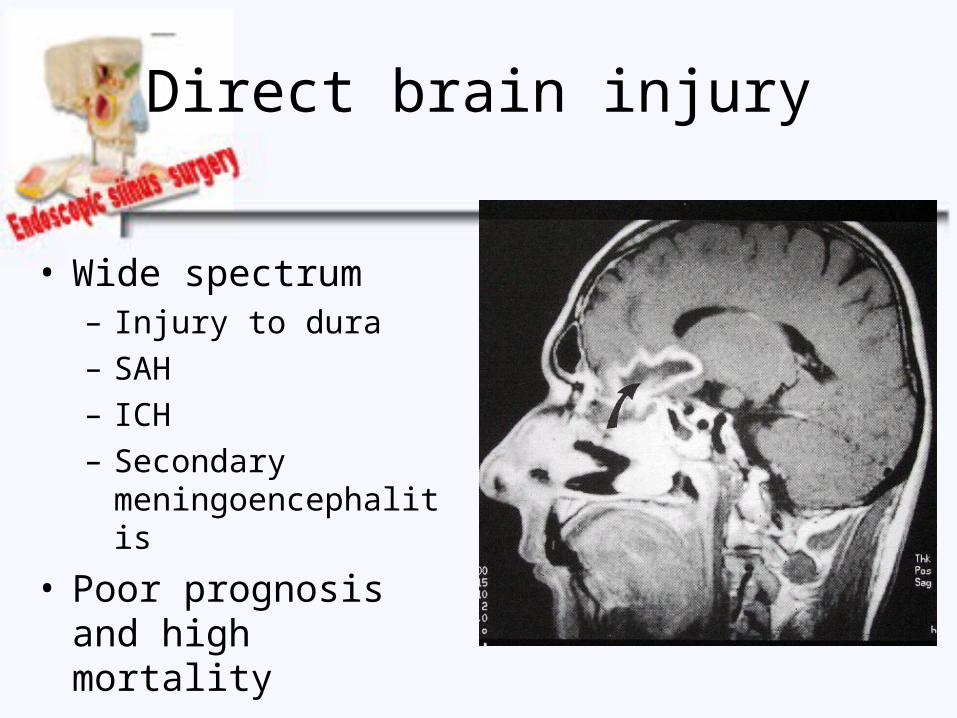
Direct brain injury
• Wide spectrum– Injury to dura– SAH– ICH– Secondary
meningoencephalitis
• Poor prognosis and high mortality
Direct brain injury
• Frontal lobe is common site
• Treatment – Immediate rhinological closure– Consult neurosurgeon
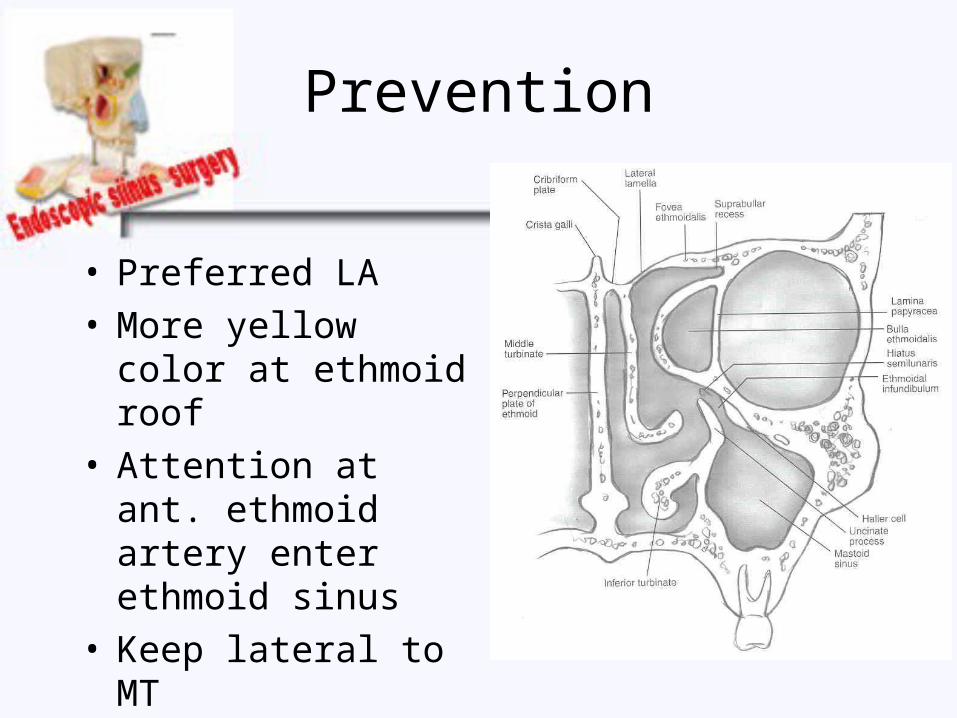
Prevention
• Preferred LA • More yellow color at
ethmoid roof• Attention at ant.
ethmoid artery enter ethmoid sinus
• Keep lateral to MT

Synechiae
• Incidence : 1.2-8%• 15-20% symptomatic
and need treatment• Location : raw surface
between middle turbinate and lateral nasal
• Treatment : lysis synechiae and silastis spacer for 4 wks.

• Prevention – Minimal injury to surrounded mucosa– Preserve mucosa of MT– Serial post-op cleanning– Silastic stent
Synechiae

Other complications
• Asthma exacerbation– Usually occur in LA
• Infection– Sinus surgery + septorhinoplasty risk to
severe infection
• Mucocele – Long term sequelae

Conclusion
• Prevention is the best
• Pre-op assessment and decision to operate
• Knowledge of anatomy relationship and its variation
• Informed about complication to the patient
Conclusion
• Adequate training
• CT-scan
• Expose the eye during surgery
• Do not blind dissection
• Early detection and treatment