Nitric oxide donors and implantation ROWAA A. MOSTAFA MD, FRCOG
33
Nitric oxide Nitric oxide donors and donors and implantation implantation ROWAA A. MOSTAFA ROWAA A. MOSTAFA MD, FRCOG MD, FRCOG
description
Nitric oxide donors and implantation ROWAA A. MOSTAFA MD, FRCOG. Implantation is a progressive process in which the embryo has to appose and attach itself to the maternal endometrium , and invade it. This process involves 2 sides: - PowerPoint PPT Presentation
Transcript of Nitric oxide donors and implantation ROWAA A. MOSTAFA MD, FRCOG

Nitric oxide donors and Nitric oxide donors and implantationimplantation
ROWAA A. MOSTAFA ROWAA A. MOSTAFA
MD, FRCOGMD, FRCOG
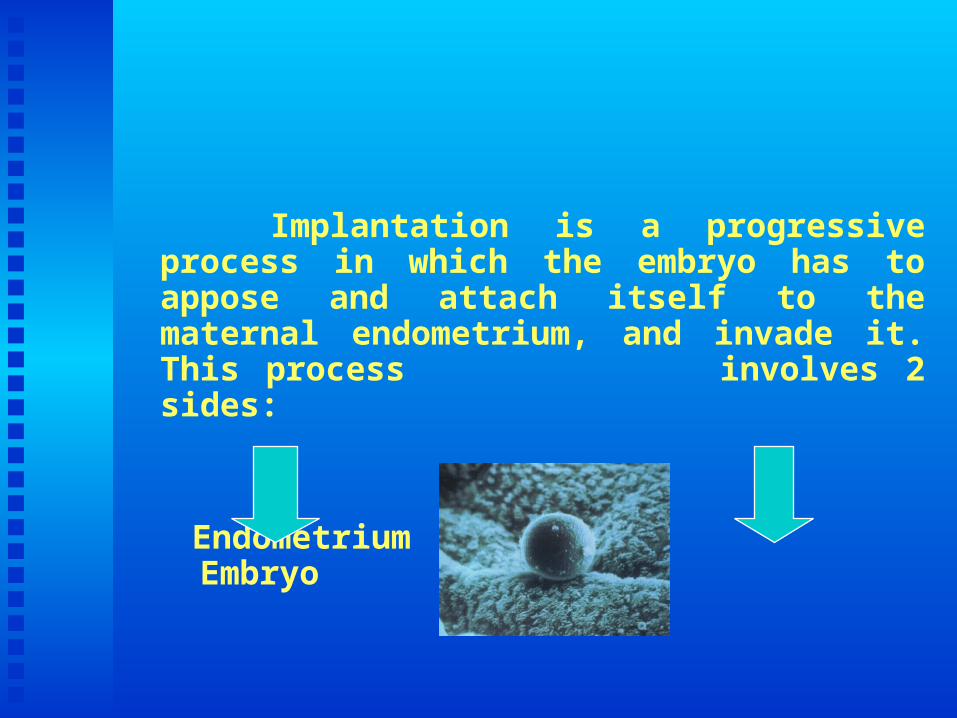
Implantation is a progressive process in which the embryo has to appose and attach itself to the maternal endometrium, and invade it. This process involves 2 sides:
Endometrium Embryo

Since the introduction of IVF ,there has been substantial improvement of all IVF steps. However, the endpoint, which is to improve implantation and pregnancy rates after transferring adequate number of embryos remains below expectations.

The main reason for this disappointing result is the quality of the endometrial factor that is affected during COH . . The fundamental question is : could implantation be improved in ART, therefore increasing the pregnancy rates in IVF/ ICSI cycles?

Adjuvant medical therapies to improve implantation
Several medical therapies were tried as adjuvants with Several medical therapies were tried as adjuvants with progesterone to increase endometrial receptivity and progesterone to increase endometrial receptivity and improve implantation after ET.improve implantation after ET.
Aspirin.Aspirin. Ascorbic acid .Ascorbic acid . Vitamin E.Vitamin E. Corticosteroids.Corticosteroids. Heparin.Heparin.
Luteal E2 supplementation.Luteal E2 supplementation. Nitric oxide donors.Nitric oxide donors.

Nitric oxide donors
NO donors are compounds capable of releasing free NO donors are compounds capable of releasing free NO in vivo. NO in vivo.
Several observations were behind the trials of using Several observations were behind the trials of using nitric oxide donors in ART in attempt to improve nitric oxide donors in ART in attempt to improve endometrial receptivity and implantation.endometrial receptivity and implantation.
These observations include
No acts as a relaxant of blood vessels and smooth muscles of uterus.No acts as a relaxant of blood vessels and smooth muscles of uterus. No inhibits platelets aggregation.No inhibits platelets aggregation. NOS reaches peak levels in the endometrium during implantation NOS reaches peak levels in the endometrium during implantation
window in natural cycle.window in natural cycle.
Adequate uterine perfusion is an important factor in uterine receptivity. Adequate uterine perfusion is an important factor in uterine receptivity. Various studies showed that high resistance to uterine blood flow at Various studies showed that high resistance to uterine blood flow at HCG time or at ET is correlated with poor outcome. HCG time or at ET is correlated with poor outcome. Using Doppler Using Doppler ultrasonography,ultrasonography, GoswamyGoswamy and Steptoe, 1988and Steptoe, 1988 reported a high reported a high incidence of poor uterine perfusion in women with repeated failed incidence of poor uterine perfusion in women with repeated failed IVF trials. They postulated that sub-optimal uterine blood flow IVF trials. They postulated that sub-optimal uterine blood flow could possibly be an independent factor of infertility.could possibly be an independent factor of infertility.
Types of NO donors:Types of NO donors: Organic:Organic:
* Isosorbide mononitrate (ISMN).* Isosorbide mononitrate (ISMN).
* Isosorbide dinitrate (ISDN).* Isosorbide dinitrate (ISDN).
* Isosorbide trinitrate (ISTN).* Isosorbide trinitrate (ISTN).
* Nitroglycerine.* Nitroglycerine. Non organic:Non organic:
* Nicorandial. * Molsidomine.* Nicorandial. * Molsidomine.

A study was carried to A study was carried to assess the effect of assess the effect of nitric oxide donor on uterine blood nitric oxide donor on uterine blood flow , endometrial receptivityflow , endometrial receptivity and and implantation in IVF/ICSIimplantation in IVF/ICSI . A better . A better understanding of implantation is understanding of implantation is essential for further improvement of essential for further improvement of success rates in assisted conception success rates in assisted conception treatment cyclestreatment cycles
Subjects and Methods
The present study was conducted in Fertility IVFIVF center center in the period from September 2006 to May 2008. Forty women whom ICSI was indicated for male factor ( oligo-asthenosprmia) were selected for this study. Their ages ranged from 25 to 35 year. . There were no other indications for ICSI in all participating women. Cases of PCOD were not included.
The subjects received the long protocol of controlled ovarian hyper-stimulation using GnRH analogue decapeptyl 0.1 mg; Ferring and HMG , 75 IU FSH and LH; Menogon ,Ferring 2-3 amp /day.
HCG ,pregnyl; Organon 10 000 IU was given by IMI when ≥ 3 follicles with a mean diameter of 18 mm or more were seen. Oocytes retrieval was done 36 hours later followed by ICSI. Each woman had ET of 2 or 3 good quality embryos on day 3 after oocytes retrieval. Cases with only one embryo available for transfer and /or no grade A embryos, were not included.


Luteal phase support was undertaken with progesterone vaginal pessaries ( Cyclogest 400mg daily) starting on the day of oocytes retrieval and for 2 weeks after embryo transfer. Measurement of B-HCG was done after 2 weeks and if it is positive, transvaginal ultrasound scan is done 2 weeks later to assess the pregnancy.

The subjects were divided randomly into 2 groups after embryo transfer.
Group I:Group I: 20 women received nitric oxide donors in the form of nitroglycerin skin patch(Nitroderm 5mg/24 hours)(Nitroderm 5mg/24 hours) Novartis pharma S.A.E; Basles Switzerland. The patch releases transdermal propanetriol trinitrate. The patches were used for 2 weeks.
Group II:Group II: the other 20 women did not receive this treatment.this treatment.

Nitroderm TTs is a flat Nitroderm TTs is a flat multilayer system designed multilayer system designed to deliver nitroglycerin to deliver nitroglycerin continuously through a continuously through a release a release membrane release a release membrane following application to the following application to the skin. The active substance skin. The active substance penetrates the skin and thus penetrates the skin and thus becomes directly becomes directly bioavailable to the systemic bioavailable to the systemic circulation . circulation .
Three Nitroderm skin patches are available: Three Nitroderm skin patches are available: TTS 5, TTS 10 and TTS 15. The figures TTS 5, TTS 10 and TTS 15. The figures denote the nominal amount of nitroglycerin denote the nominal amount of nitroglycerin in mg delivered by the system in 24 hours. in mg delivered by the system in 24 hours. The rate of release is 20-25 ug/cm2. hr. The rate of release is 20-25 ug/cm2. hr. TTS 5 was used in the current study.TTS 5 was used in the current study.
Uterine artery doppler blood flow assessment was done for all women on the day of HCGon the day of HCG administration and one week laterone week later. The. The pulsatility index (PI)pulsatility index (PI) was used for this purpose.
PI = PI = peak systolic- end diastolicpeak systolic- end diastolic mean velocity for the entire cardiac cyclemean velocity for the entire cardiac cycle
Transvainal probe 5 MHz of Color doppler ultrasonography (Digital GAIA , Sonace 8800, Medison; S.Korea ) machine was used. All scans were done by experienced operators and almost in the same time of the day to avoid diurnal variation in the uterine blood flow.

Transvaginal pelvic scanning was first performed and the morphology of the uterus and ovaries was explored. Color flow mapping and pulsed Doppler measurements were performed to the uterine artery on both sides. Blood flow velocity waveforms were obtained and quantitated by the calculation of pulsatility index (PI).



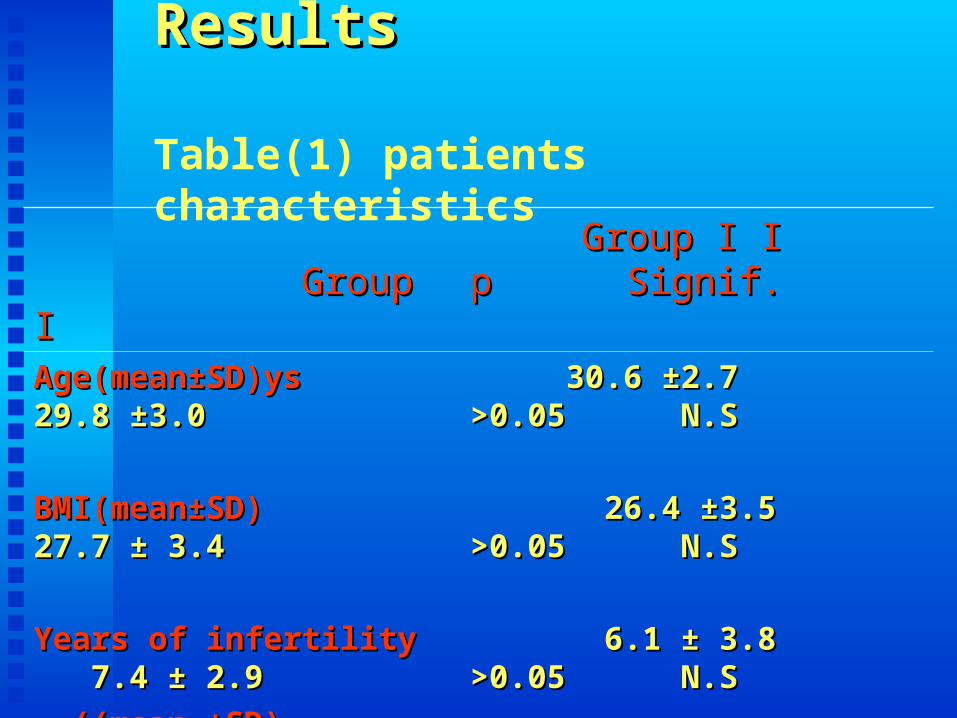
ResultsResults
Table(1) patients characteristics Group I Group I
Group I I p Signif. Group I I p Signif.
Age(mean±SD)ys Age(mean±SD)ys 29.8 ±3.029.8 ±3.0
BMI(mean±SD) BMI(mean±SD) 27.7 ± 3.427.7 ± 3.4
Years of infertility Years of infertility 7.4 ± 2.97.4 ± 2.9
((mean ±SD)((mean ±SD)
30.6 ±2.7 >0.05 N.S30.6 ±2.7 >0.05 N.S
26.4 ±3.5 >0.05 N.S26.4 ±3.5 >0.05 N.S
6.1 ± 3.8 >0.05 N.S6.1 ± 3.8 >0.05 N.S

Table (2) characteristics of treatment cycles
Group I Group II P Signif.Group I Group II P Signif.
(mean) (mean)(mean) (mean)HMG ampoulesHMG ampoules
HMG daysHMG days
Retrieved oocytes Retrieved oocytes
Fertilized oocytesFertilized oocytes
Fertilization rateFertilization rate
Transferred embryosTransferred embryos
34.5±3.2 37.8 ±4.1 >0.05 N.S 34.5±3.2 37.8 ±4.1 >0.05 N.S
11.4±2.3 12.5±3.8 >0.05 N.S11.4±2.3 12.5±3.8 >0.05 N.S
7.4 ±2.2 8.7±3.1 >0.05 N.S7.4 ±2.2 8.7±3.1 >0.05 N.S
5.9±1.3 6.1±1.0 > 0.05 N.S5.9±1.3 6.1±1.0 > 0.05 N.S
79.7±5.3% 73.1±4.8% >0.05 N.S79.7±5.3% 73.1±4.8% >0.05 N.S
2.1± 0.5 2.5 ± 0.2 >0.05 N.S2.1± 0.5 2.5 ± 0.2 >0.05 N.S
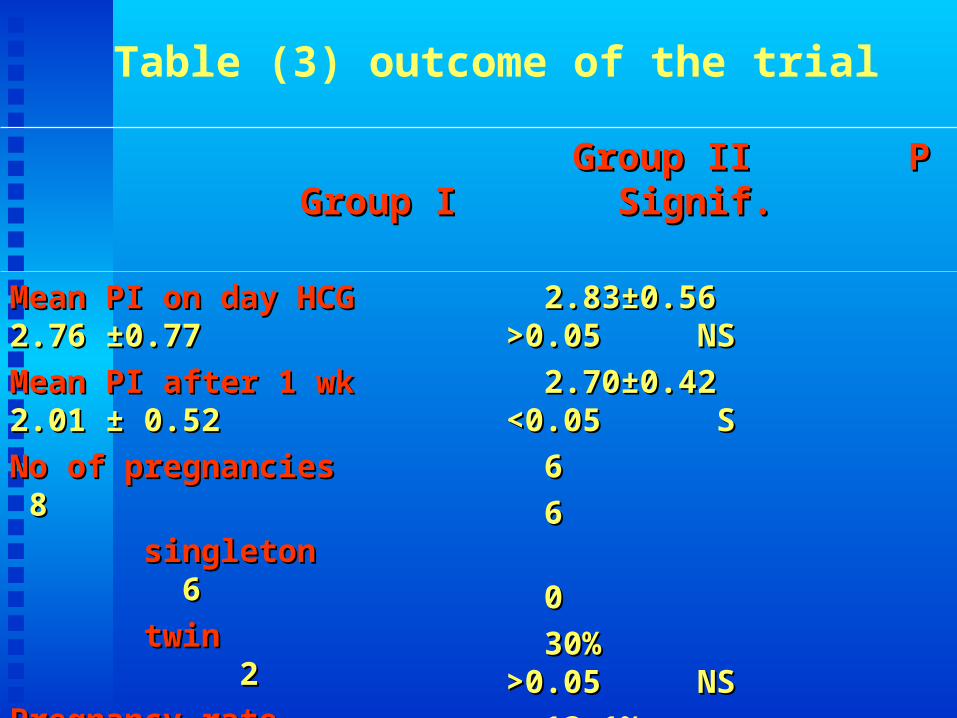
Table (3) outcome of the trial
Group I Group I
Group II P Signif.Group II P Signif.
Mean PI on day HCGMean PI on day HCG 2.76 ±0.77 2.76 ±0.77
Mean PI after 1 wkMean PI after 1 wk 2.01 ± 0.52 2.01 ± 0.52
No of pregnanciesNo of pregnancies 88
singletonsingleton 6 6
twintwin 2 2
Pregnancy ratePregnancy rate 40% 40%
Implantation rateImplantation rate 21.7 % 21.7 %
2.83±0.56 >0.05 NS2.83±0.56 >0.05 NS
2.70±0.42 <0.05 S2.70±0.42 <0.05 S
6 6
6 6
00
30% >0.05 NS30% >0.05 NS
13.1% <0.05 S13.1% <0.05 S
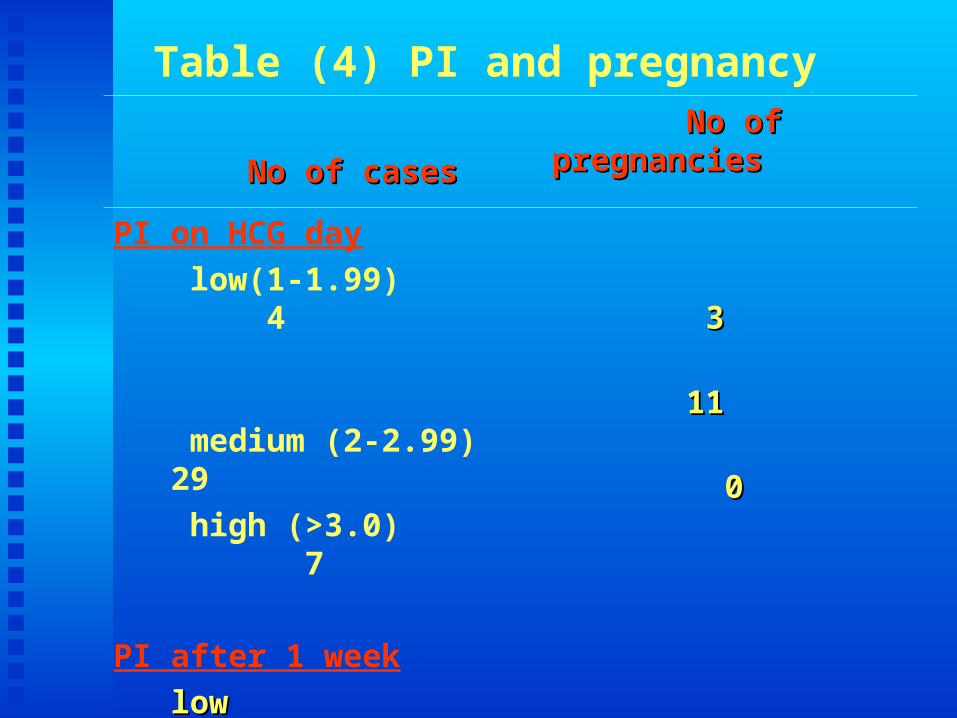
Table (4) PI and pregnancy
No of casesNo of cases No of pregnanciesNo of pregnancies
PI on HCG day
low(1-1.99) 4
medium (2-2.99) 29
high (>3.0) 7
PI after 1 week
low 7 low 7
medium 30medium 30
high 3 high 3
33
1111
00
55
99
00

ConclusionsConclusions
Implantation process constitutes the limiting Implantation process constitutes the limiting factor to increase pregnancy rates in ART.factor to increase pregnancy rates in ART.
Optimal uterine perfusion is an important Optimal uterine perfusion is an important factor for uterine receptivity and consequently factor for uterine receptivity and consequently successful implantation.successful implantation.
Nitric oxide donors may hove a role in Nitric oxide donors may hove a role in optimizing uterine blood flow and perfusion. optimizing uterine blood flow and perfusion. Their use may improve implantation which can Their use may improve implantation which can increase pregnancy rate in ART treatment increase pregnancy rate in ART treatment cycles.cycles.