NICU Enteral Guideline for the Use of an Exclusive Human ... · As with all feeding guidelines,...
19
1 NICU Enteral Guideline For the Use Of An Exclusive Human Milk Diet (EHMD) in Infants < 1250 g Birth Weight Andi Markell RD, LD Housekeeping Items Presentation will be available on-demand http://www.prolacta.com/webinars/feeding-guideline 1 2 3 4 Turn up your speaker volume or dial in Submit your questions throughout the presentation Leave us feedback and suggestions 2 DISCLAIMER: This presentation is intended to provide a guideline for healthcare providers in the use of an Exclusive Human Milk Diet in infants ≤1250 g birth weight. The information within is the collective opinion of the Nutrition Advisory Committee, a committee sponsored by Prolacta Bioscience. As with all feeding guidelines, appropriate medical judgement should be exercised. Be sure to review your clinical experience and outcomes around the management of nutrition in very low-birth-weight infants.
Transcript of NICU Enteral Guideline for the Use of an Exclusive Human ... · As with all feeding guidelines,...

1
NICU Enteral Guideline
For the Use Of An Exclusive Human Milk Diet (EHMD)
in Infants < 1250 g Birth Weight
Andi Markell RD, LD
Housekeeping Items
Presentation will be available on-demand http://www.prolacta.com/webinars/feeding-guideline1
2
3
4
Turn up your speaker volume or dial in
Submit your questions throughout the presentation
Leave us feedback and suggestions
2
DISCLAIMER: This presentation is intended to provide a guideline for healthcare providers in the use of an Exclusive Human Milk Diet in infants ≤1250 g birth weight. The information within is the collective opinion of the Nutrition Advisory Committee, a committee sponsored by Prolacta Bioscience. As with all feeding guidelines, appropriate medical judgement should be exercised. Be sure to review your clinical experience and outcomes around the management of nutrition in very low-birth-weight infants.
chong
Typewritten Text

2
EDUCATION Bachelor of Science in Nutrition and Food Management, Focus: Dietetics
NATIONAL CERTIFICATIONS Commission on Dietetic Registration, 2000 - present Oregon Board of Examiners of Licensed Dietitians, 2001 – present
PUBLICATIONS Decreasing necrotizing enterocolitis and gastrointestinal bleeding in the neonatal intensive care unit. ICAN Infant Child Adolescent Nutr 2014; 6 (2):86 - 93.
Computer Programming: Quality and Safety for Neonatal Parenteral Nutrition Orders. Nutr Clin Pract 2013. 28, 515.
Decreasing Necrotizing Enterocolitis and Gastrointestinal Bleeding in the NICU: An Evaluation of the Use of Donor Human Milk and Exclusive Human Milk Diets in Infants < 1500 Grams Birth Weight. PAS; 2013. Washington D.C.
Neonatal Parenteral Nutrition Containing Calcium Chloride and Sodium Phosphate: Mineral Intake and Aluminum Content. Infant, Child, & Adolescent Nutrition. 2012. 4 (3), 137-142.
Andi Markell, RD, LD
3
• Introduce the Nutrition AdvisoryCommittee (NAC)
• Discuss the clinical significance ofan Exclusive Human Milk Diet(EHMD)
• Review the 2016 NAC NICUEnteral Guidelines for the use of anEHMD for < 1250 g babies
4
Agenda

3
5
NAC Members
The Nutrition Advisory Committee is comprised of leading registered dietitians from around the country. Their mission is to provide neonatal intensive care units (NICUs) with clinical expertise, research, insights, and guidance on premature infant nutrition. They also serve as a resource to fellow clinicians for education and support around the growing use of an exclusive human milk diet for extremely premature infants.
The NAC is committed to sharing ideas and evidence-based practices with others who are also dedicated to providing the best care for their patients.
The NAC is sponsored by Prolacta Bioscience.
Our Mission
6

4
7
Exclusive Human Milk Diet (EHMD)
MOM/BBM
Human Milk-Based Modulars
Human Milk-Based
Fortifier
8
Feeding Guideline

5
9
Calorie/Protein Goals
Calorie/Protein Goals • 110-130 kcal/kg, 3.5-4.5 g/kg of protein(1)
• Calories and protein should be based on nutritional assessment
1. Koletzko B, et al., Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines. Basel, Switzerland: Karger; 2014. World Review of Nutrition and Dietetics. Vol 110.
10
Calorie/Protein Goals
* < 1 kg** 1-1.5 kg *** 1-1.8 kg
Nutrient Koletzko 2014 AAP 2014 ESPGHAN 2010
Calories Kcal/kg
110-130 105-130 130-150* 110-130**
110-135
Protein g/kg
3.5-4.5 3.5-4.0 3.8-4.4* 3.4-4.2**
4-4.5* 3.5-4***
• Koletzko B, et al., Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines. Basel, Switzerland: Karger; 2014. World Review of Nutrition and Dietetics. Vol 110.
• Kleinman, Ronald E., and Frank R. Greer. “Pediatric Nutrition.” AAP Books (2013).• Agostoni, Carlo, et al. "Enteral nutrient supply for preterm infants: commentary from the European Society of Paediatric Gastroenterology,
Hepatology and Nutrition Committee on Nutrition." Journal of pediatric gastroenterology and nutrition 50.1 (2010): 85-91.

6
11
Initiation of Feeds
Initiation of Feeds • Initiate feeds on day of birth or as soon as possible(1,2)
• Use Mom’s own Milk (MOM) or Banked Breast Milk(BBM)(3)
1. Koletzko B, et al., Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines. Basel, Switzerland: Karger; 2014. World Review of Nutrition and Dietetics. Vol 110.
2. Kleinman, Ronald E., and Frank R. Greer. “Pediatric Nutrition.” AAP Books (2013).3. Eidelman, Arthur I., et al. “Breastfeeding and the use of human milk.” Pediatrics 129.3 (2012): e827-e841.
• Start as soon as possible after birth(1,2)
– Benefits:• Decreased incidence of indirect hyperbilirubinemia, cholestatic
jaundice, metabolic bone disease, nosocomial sepsis, and oxygenneeds
• Increased levels of gastrin and other enteric hormones
• Decreased days to full feeds
• Increased weight gain and head growth
• Decreased length of stay
12
Initiation of Feeds Advantage
1. Koletzko B, et al., Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines. Basel, Switzerland: Karger; 2014. World Review of Nutrition and Dietetics. Vol 110.
2. Kleinman, Ronald E., and Frank R. Greer. “Pediatric Nutrition.” AAP Books (2013)

7
– Disadvantage (none):(1,2)
• Studies show no increased incidence of NEC among preterminfants receiving trophic feeds
• Absence of enteral feeds leads to GI mucosal atrophy anddysfunction
• Delaying introduction of enteral feedings significantly increasesthe time to establish full enteral feedings and therefore PN needsand associated morbidities
13
Initiation of Feeds Disadvantage
1. Koletzko B, et al., Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines. Basel, Switzerland: Karger; 2014. World Review of Nutrition and Dietetics. Vol 110.
2. Kleinman, Ronald E., and Frank R. Greer. “Pediatric Nutrition.” AAP Books (2013)
“Human milk from the preterm infant’s mother is the enteral feeding of choice”(2)
14
Initiation of Feeds Benefits of HM
HM Components(2) HM Benefits(1)
• Immunologic and antimicrobial
• Hormones
• Enzymes
• Decrease LOS • Decreased hospital readmission• Improved feeding tolerance• Decrease need for PN• Improved mother infant bonding• Reduction of severity of ROP• Higher long term
neurodevelopmental scores• Lower risk for later metabolic
syndrome1. Koletzko B, et al., Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines. Basel, Switzerland: Karger; 2014. World Review
of Nutrition and Dietetics. Vol 110.2. Kleinman, Ronald E., and Frank R. Greer. “Pediatric Nutrition.” AAP Books (2013)

8
“If MOM is unavailable…pasteurized donor milk should be used”
15
TABLE 3* Recommendations on Breastfeeding Management for Preterm Infants
1. All preterm infants should receive human milk.
• Human milk should be fortified, with protein, minerals, and vitamins to ensure optimal nutrient intake for infants
weighing <1500 g at birth.
• Pasteurized donor human milk, appropriately fortified, should be used if mother’s own milk is unavailable or its use is
contraindicated.
2. Methods and training protocols for manual and mechanical milk expression must be available to mothers.
3. Neonatal intensive care units should possess evidence-based protocols for collection, storage, and labeling of human
milk.
4. Neonatal intensive care units should prevent the misadministration of human milk
(http://www.cdc.gov/breastfeeding/recommendations/other_mothers_milk.htm).
5. There are no data to support routinely culturing human milk for bacterial or other organisms.
3. AAP 2015 HM Statement American Academy of Pediatrics. Breastfeeding and the Use of Human Milk
Initiation of Feeds Pasteurized Donor Milk
16
Clinical Benefits Potential Clinical
Benefits Concerns
• Protection against NEC
• Enhanced feeding tolerance
• Long-term health benefits
• Enhanced immunity• HMO• LCPUFA
• Slow growth• Optimize
fortification
• Alterations in nutritional/biologicalquality
• Arslanoglu, Sertac, et al. "Donor human milk in preterm infant feeding: evidence and recommendations.” Journal of perinatal medicine 38.4 (2010): 347-351.
Initiation of Feeds Pasteurized Donor Milk

9
17
Lost Biological active milk components
Preserved Biological active milk components
• sIgA • Total IgA• Lactoferrin• Lysozyme• Lymphocytes• Lipase • Alkaline phosphatase • Cytokines• Some growth factors
• Oligosaccharides• Vitamin A • Vitamin D• Vitamin E• Lactose• LCPUFA • Epidermal growth factor
• Arslanoglu, Sertac, et al. "Donor human milk in preterm infant feeding: evidence and recommendations.” Journal of perinatal medicine 38.4 (2010): 347-351.
Initiation of Feeds Pasteurized Donor Milk
18
Advancement of Feeds
Advancement of Feeds • Feeding Protocol recommended(1,2)
• 10-35 mL/kg advancement(1)
1. Koletzko B, et al., Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines. Basel, Switzerland: Karger; 2014. World Review of Nutrition and Dietetics. Vol 110.
2. Kleinman, Ronald E., and Frank R. Greer. “Pediatric Nutrition.” AAP Books (2013)

10
19
Advancement of Feeds Standardized Feeding Protocol
Benefits Possible Components
• Earlier full enteralfeeding
• Reduction in neonatalmorbidities
1. Establish criteria2. Desired milk (MOM/BBM)3. Trophic volume of feeds
(1-25 mL/kg/day) for 3-5 days(2)
4. Daily advances (10-35 mL/kg)(1)
5. Include fortification as part of the feeding protocol6. Establish stopping criteria
1. Koletzko B, et al., Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines. Basel, Switzerland: Karger; 2014. World Review of Nutrition and Dietetics. Vol 110.
2. Kleinman, Ronald E., and Frank R. Greer. “Pediatric Nutrition.” AAP Books (2013)
20
Initiation of Fortification
Initiation of Fortification • Initiate fortification before 100 mL/kg(1)
• Prolact+ 4 H2MF for lower volume fortification• Ex 40-60 mL/kg
• Prolact+ 6 H2MF for higher volume fortification• Ex 80-100 mL/kg
• Avoid fortification and advancement on the same day• Wait to make changes in fortification until tolerance
shown
1. Koletzko B, et al., Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines. Basel, Switzerland: Karger; 2014. World Review of Nutrition and Dietetics. Vol 110.

11
21
Initiation of Fortification Feeding Progression
Day Feed Volume
Day 1 Initiate feeds 10 ml/kg
Day 2-3 Trophic feeds 10 ml/kg
Day 4-6 Advancement 20 ml/kg
Day 7 Prolact+4 40 ml/kg (no advance)
Day 8-13 Advance 20 ml/kg
Day 14 Prolact+6 130 ml/kg (no advance)
Day 15 Advance 20 ml/kg
Day 16 Protocol end 160 ml/kg
22
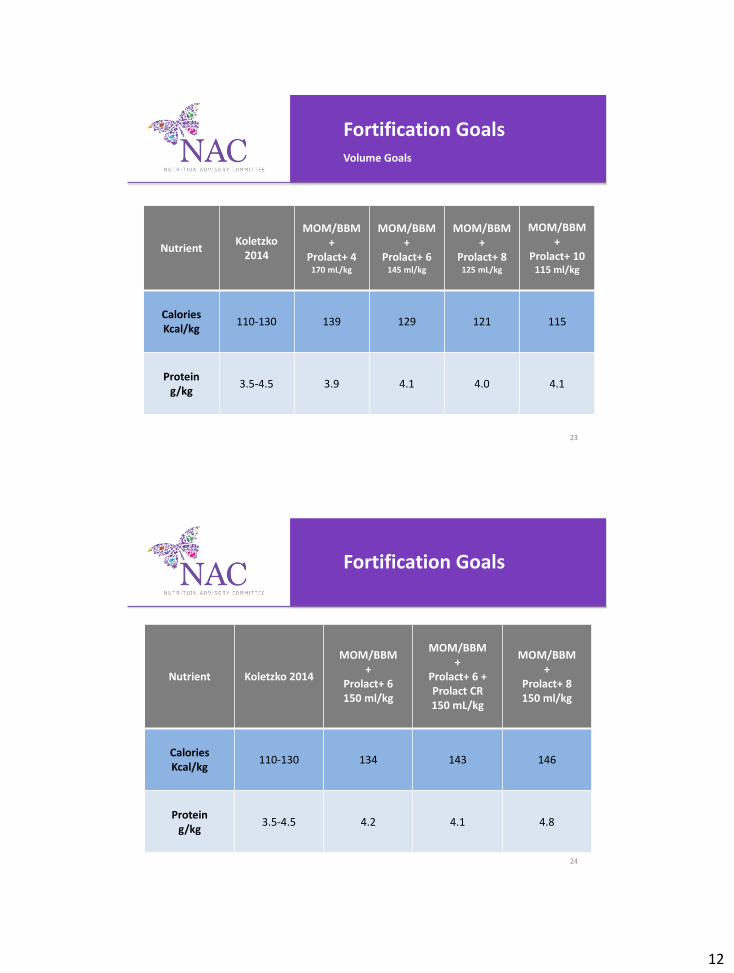
Fortification Goals
Fortification Goals • Fortification goals to meet protein and caloric goals> 170 mL/kg: MOM/BBM with Prolact+ 4 H2MF > 145 mL/kg: MOM/BBM with Prolact+ 6 H2MF > 125 mL/kg: MOM/BBM with Prolact+ 8 H2MF < 125 mL/kg: MOM/BBM with Prolact+ 10 H2MF
• Further increase in concentration may be needed to meet growth goals
• Do not add non-human milk-based modulars to EHMD• Prolact CR®
• 4 mL Prolact CR with 100 mL MOM/BBM if growthgoals not met in 3-7 days
• Prolact CR can also be mixed as 4 mL of Prolact CRwith 96 mL of MOM/BBM
12
23
Nutrient Koletzko
2014
MOM/BBM +
Prolact+ 4 170 mL/kg
MOM/BBM +
Prolact+ 6 145 ml/kg
MOM/BBM +
Prolact+ 8 125 mL/kg
MOM/BBM +
Prolact+ 10 115 ml/kg
Calories Kcal/kg
110-130 139 129 121 115
Protein g/kg
3.5-4.5 3.9 4.1 4.0 4.1
Fortification Goals Volume Goals
24
Nutrient Koletzko 2014
MOM/BBM +
Prolact+ 6 150 ml/kg
MOM/BBM +
Prolact+ 6 + Prolact CR 150 mL/kg
MOM/BBM +
Prolact+ 8 150 ml/kg
Calories Kcal/kg
110-130 134 143 146
Protein g/kg
3.5-4.5 4.2 4.1 4.8
Fortification Goals

13
25
Vitamins & Iron
Vitamins & Iron • 1 mL MVI without Fe• Fe 2-3 mg/kg(1)
• Consider splitting dose twice a day for tolerance
1. Koletzko B, et. al, ed. Nutritional Care of Preterm Infants: Scientific Basis and Practical Guidelines. Basel, Switzerland: Karger; 2014. World Review of Nutrition and Dietetics. Vol 110.
26
Vitamins & Fe
Koletzko 2014 (kg/d) 1 ml Poly-Vi-Sol
Vitamin A, IU 400-1,100 750
Vitamin D, IU 400-1,000 400
Vitamin E, IU 2.2-11 5
Vitamin C, mg 11-46 35
Thiamin, mg 0.14-0.30 0.5
Riboflavin, mg 0.2-0.4 0.6
Niacin, mg 0.38-5.50 8
Vitamin B6, mg 0.045-0.300 0.4
Vitamin B12, mcg 0.10-0.77 2
Iron, mg 2-3
• 1 mL Poly-Vi-Sol adds +160 mOsmo/kg water, recommended to add 0.5 ml BID
• 1 mL Fer-In-Sol adds +55 mOsmol/kg water
https://www.meadjohnson.com/pediatrics/us-en/product-information/products/vitamins/enfamil-poly-vi-sol-drops#nutrients https://www.meadjohnson.com/pediatrics/us-en/product-information/products/vitamins/enfamil-fer-in-sol-iron-supplement#osmolality

14
27
Growth Goals
Growth Goals • Weight: 15-20 g/kg(4)
• Length: > 0.9 cm/wk(4)
• OFC: > 0.9 cm/wk(4)
4. Groh-Wargo, Sharon, Melody Thompson, and Janice Hovasi Cox. Academy of Nutrition and Dietetics Pocket Guide to Neonatal Nutrition. SecondEdition Pediatric Nutrition Dietetic Practice Group, 2016.
• Weight gain, measured daily,
assessed as an average over one week• Often linked with neurodevelopmental outcome
• May be effected by clinical picture
• Length, measured weekly• Preferred method is with two people using a length board
• OFC, measured weekly• Measured with a tape measure
• Can be effected by micro/macrocephaly
28
Growth Goals
4. Groh-Wargo, Sharon, Melody Thompson, and Janice Hovasi Cox. Academy of Nutrition and Dietetics Pocket Guide to Neonatal Nutrition. SecondEdition Pediatric Nutrition Dietetic Practice Group, 2016.

15
29
Transition off EHMD
Transition off EHMD • Consider using an EHMD until 34 weeks postmenstrual age• Consider transition off Prolact+ H2MF® over
three daysExample of feeding transition • Day one: 6 of 8 feeds as Prolact+ H2MF• Day two: 4 of 8 feeds as Prolact+ H2MF• Day three: 2 of 8 feeds as Prolact+ H2MF• Day four: Transition complete
EHMD until 34 weeks post menstrual age
• Early studies using an EHMD diet reported the last case ofNEC at 34 weeks
• AAP recommends using MOM/BBM for premature infants
• Transitioning at 34 weeks gives time to test tolerance of newfortification
30
Transition off EHMD

16
Example transition off EHMD
8 feeds per day
31
Transition off EHMD
Feed (q 3 hours)
1 2 3 4 5 6 7 8
Day 1 CMB H2MF H2MF H2MF CMB H2MF H2MF H2MF
Day 2 CMB H2MF CMB H2MF CMB H2MF CMB H2MF
Day 3 CMB CMB CMB H2MF CMB CMB CMB H2MF
Day 4 CMB CMB CMB CMB CMB CMB CMB CMB
• Introduce the Nutrition AdvisoryCommittee (NAC)
• Discuss an Exclusive Human MilkDiet (EHMD)
• Review the 2016 NAC NICUEnteral Guidelines for the use of anEHMD for < 1250 g babies
32
Review

17
NAC March 2016 33
34
Q&A

3/30/2016
18
• Calorie/Protein goals– Koletzko, Berthold, Brenda Poindexter, and Ricardo Uauy. "Nutritional care of preterm
infants." Ann Nutr Metab 64.3-4 (Koletzko, Berthold, Brenda Poindexter, and Ricardo Uauy. "Nutritional care of preterm infants." Ann Nutr Metab 64.3-4 (2014): 183-342.
35
References
• Initiation of Feeds– Kleinman, Ronald E., and Frank R. Greer. "Pediatric Nutrition." AAP Books(2014).
• McClure, R. J., and S. J. Newell. "Randomised controlled trial of trophic feeding and gut motility." Archives of Disease in Childhood-Fetal and Neonatal Edition 80.1 (1999): F54-F58.
• Schanler, Richard J., et al. "Feeding strategies for premature infants: randomized trial of gastrointestinal primingand tube-feeding method."Pediatrics 103.2 (1999): 434-439.
• Schanler, Richard J., et al. "Randomized trial of donor human milk versus preterm formula as substitutes for mothers' own milk in the feeding of extremely premature infants." Pediatrics 116.2 (2005): 400-406.
– Koletzko, Berthold, Brenda Poindexter, and Ricardo Uauy. "Nutritional care of preterminfants." Ann Nutr Metab 64.3-4 (Koletzko, Berthold, Brenda Poindexter, and Ricardo Uauy. "Nutritional care of preterm infants." Ann Nutr Metab 64.3-4 (2014): 183-342.
• Flidel-Rimon, O., et al. "Early enteral feeding and nosocomial sepsis in very low birthweight infants." Archives of Disease in Childhood-Fetal and Neonatal Edition 89.4 (2004): F289-F292.
• Rochow, Niels, et al. "A nutritional program to improve outcome of very low birth weight infants." Clinical nutrition 31.1 (2012): 124-131.
• Dunn, L., et al. "Beneficial effects of early hypocaloric enteral feeding on neonatal gastrointesting function: Preliminary report of a randomized trial."The Journal of pediatrics 112.4 (1988): 622-629.
• Bombell, Sarah, and William McGuire. "Early trophic feeding for very low birth weight infants." Cochrane Database Syst Rev 3 (2009).
• Dsilna, Ann, et al. "Continuous feeding promotes gastrointestinal tolerance and growth in very low birth weightinfants." The Journal of pediatrics 147.1 (2005): 43-49.
36
References

3/30/2016
19
• Initiation of Feeds – Koletzko, Berthold, Brenda Poindexter, and Ricardo Uauy. "Nutritional care of preterm
infants." Ann Nutr Metab 64.3-4 (2014): 183-342. • Patole, S. K., and N. De Klerk. "Impact of standardised feeding regimens on incidence of neonatal necrotising
enterocolitis: a systematic review and meta-analysis of observational studies." Archives of Disease in Childhood-Fetal and Neonatal Edition 90.2 (2005): F147-F151.
– Kleinman, Ronald E., and Frank R. Greer. "Pediatric Nutrition." AAP Books(2014). • McCallie, K. R., et al. "Improved outcomes with a standardized feeding protocol for very low birth weight
infants." Journal of Perinatology 31 (2011): S61-S67.
• Wiedmeier, Susan E., et al. "Center differences in NEC within one health-care system may depend on feeding protocol." American journal of perinatology 25.1 (2008): 5-11.
– Eidelman, Arthur I., et al. "Breastfeeding and the use of human milk."Pediatrics 129.3 (2012): e827-e841.
– Arslanoglu, Sertac, et al. "Donor human milk in preterm infant feeding: evidence and recommendations." Journal of perinatal medicine 38.4 (2010): 347-351.
37
References
• Initiation of fortification – Koletzko, Berthold, Brenda Poindexter, and Ricardo Uauy. "Nutritional care of preterm
infants." Ann Nutr Metab 64.3-4 (2014): 183-342.
• Vitamins & Iron – Koletzko, Berthold, Brenda Poindexter, and Ricardo Uauy. "Nutritional care of preterm
infants." Ann Nutr Metab 64.3-4 (2014): 183-342.
• Growth Goals – Groh-Wargo, Sharon, Melody Thompson, and Janice Hovasi Cox. AND Pocket guide to
neonatal nutrition. American Dietetic Associati, 2016.
• Transition off EHMD – Sullivan, Sandra, et al. "An exclusively human milk-based diet is associated with a lower
rate of necrotizing enterocolitis than a diet of human milk and bovine milk-based products." The Journal of pediatrics 156.4 (2010): 562-567.
38
References