
NHS Trust STAR - SECAmb STAR Summer 10 Low.pdf · In this edition of STAR we’ve received praise...
16
THE MAGAZINE FOR SECAmb STAFF SUMMER 2010 STAR Spotlight on... Meet the team Make Ready (PAGE 3) (PAGE 5 - 7) (PAGE 11 - 13) Emergency Preparedness and HART HART Technician Chris Treves South East Coast Ambulance Service NHS Trust
Transcript of NHS Trust STAR - SECAmb STAR Summer 10 Low.pdf · In this edition of STAR we’ve received praise...

THE MAGAZINE FOR SECAmb STAFF
SUMMER 2010STAR
Spotlight on... Meet the team Make Ready
(PAGE 3) (PAGE 5 - 7) (PAGE 11 - 13)
Emergency Preparedness and HART
HART Technician Chris Treves
South East Coast Ambulance ServiceNHS Trust
This ISSUEIssue 7 / SUMMER 2010 Staff Topics, Awareness and Recognition
Icon KeyHot Potato
Important issues to you
CPDDeveloping
your skills
Hands upWe could have
done better
We’re ListeningShowing we are trying to change
2
STAR
IntranetRead more
on the intranet
Large print and other versions available from Evey on 01273 897811.
Bee-line Positively
buzzing
FC Foundation
Council
Product group from well-managedforests and other controlled sourceswww.fsc.org Cert no. TT-COC-002754© 1996 Forest Stewardship Concil
Product group from well-managedforests and other controlled sourceswww.fsc.org Cert no. TT-COC-002754© 1996 Forest Stewardship Concil
Product group from well-managedforests and other controlled sourceswww.fsc.org Cert no. TT-COC-002754© 1996 Forest Stewardship Concil
Your SECAmb, your callSummer is sadly coming to an end, and a busy summer it has been. The SECAmb journey has moved on a pace over the last few months since the last edition of STAR.
We have seen the first stage of the new CAD implementation with Coxheath EDC going live in July, and Banstead will be next in early October. Well done to all involved as the first stage was a great success.
We have also progressed to the next stage of our foundation trust application and have submitted our bid to the Secretary of State for approval. Our business plan was praised at the Board readiness stage (where the Strategic Health Authority Board met with our Trust Board and grilled us on our future plans) as one of the most robust they have seen.
We’ve also done a lot of work around clinical audit including rolling out the clinical performance indicator (CPI) crib sheets to emphasise the importance of recording the excellent care we give in the patient clinical record (PCR). It is data collected on PCRs that is used to measure our clinical effectiveness so correct recording of data is vital to ensure the excellent care you all provide is recognised. We are also working hard to stream-line how we co-ordinate the communication of clinical information (see the clinical column on page 4), to ensure that we are providing you with the right information and right tools to help you in your jobs.
In this edition of STAR we’ve received praise from a member of London Ambulance Service for the excellent care we gave his mother – great to see that the work we do is also recognised by
our peers in other services. Well done.
Paul Sutton - Chief Executive
Thanks to the editorial team: Karen Lavender , Tony Brooks, Hazel Wilks, Louise Hutchinson and Victoria Burtenshaw, and to all those who contributed to this edition.
Excellence in leadership and development (03) Spotlight on
Improving access and outcomes (04) Clinical column (05) Meet the team – Emergency Preparedness and HART
Improved satisfaction and experience for everyone (08) A truly lovely letter(08) Skilled care in unusual circumstances (09) Dunkers and a cuppa all round! (10) Beemail makes it easier than even to say thank you
Proud to work for (11) A Prince’s Trust Secondment (13) Caption competition
Improving performance, reducing variation (13) The story so far... Make Ready within SECAmb
Using resources effectively (16) RANT
Message from the (temporary!) EditorCongratulations to Evey on the birth of her daughter Rosalie recently – Mum and baby are both doing well! Whilst Evey is off on maternity leave, I will be acting as the temporary Editor of STAR, so please do continue to send through any ideas for articles, letters or RANTs to be included, to [email protected] . I will be delighted to receive them! Remember, it’s your magazine and we really want to include topics that are relevant to you, so please let us know and happy reading!Janine Compton, Editor - STAR

3
During my final technician exam my two and a half year old daughter was diagnosed with a rare childhood cancer called Nuroblastoma and was given a week to live. Molly received high dose chemotherapy, an operation to remove a large tumour from her right kidney, followed by more chemo, radiotherapy and a trial drug called Retinoic acid (a vitamin A derivative). I am pleased to say that Molly, now aged seven, is doing great and has just had her three year clear result! This experience helps me provide support and understanding to cancer patients I come into contact with out on the road and has made me keen to learn more about patient care and the human anatomy.
Whilst applying for the paramedic degree course I saw the HART Technician Operative role advertised. The possibility of further patient care in the hot zone really appealed to me.
With my family, I watched a DVD about HART and asked what they thought about me applying for the role. We wanted to know more about the role and family support, so, armed with lots of questions I listened to HART Manager Mathew England’s speech about the role of HART at one of the HART road shows.
I took a second DVD home which provided personal accounts of people who have applied for a HART role and how challenging they found it. This DVD paid off; not only did it help me apply for the HART role, it reassured my family.
I submitted my application, was shortlisted and asked to sit a competency based interview asking me questions about jobs I had been involved in. I was then asked to attend a PCA (physical competency assessment) test. I knew this would be a challenge as it involves carrying 35kgs over 1800m. Sounds relatively easy until you add into the mix a stair climb, descents, rain, wind and cold, obstacles to overcome whilst dragging a 70kg dummy followed by a manual dexterity test whilst crouching! No pressure! Other tests on the day included a blackout tunnel crawl, a ladder climb with competence test, being lowered down, and all in a day’s work! We all experienced some nerves but the team’s efforts were great. Having successfully completed the PCA test I was ready for training.
The first part of the training was a challenging two week Breathing Apparatus (BA) course with Sussex Fire and Rescue. In a smoke and heat filled building whilst in BA and with no visibility we had to deal with a casualty and stretcher them to safety. Despite heavy snow during this part of it, the course was fun!
We were then given police training as a civil responder (CR1). This was an interesting two day course and gained us confidence in the use of a different type of respirator, and the PPE that goes with it.
Two courses and successful completion of tests led to a three week residential Incident Response Unit (IRU) course. This course incorporated ambulance skills, trauma care, BA use, CR1 use, patient care, and every bit of kit we could need for any eventuality. Despite the weekly tests this was good fun and interesting throughout.
The courses challenged us all in different ways, but we all remained focused on the job and outcome that that was to be achieved. We also have a better understanding of how HART will fit in to the NHS, and how we will be able to help and assist crews out on jobs everyday. With the additional training and equipment we will have we can all offer the best possible outcome for the patients. I still hope to get on to a paramedic course to help me progress within HART. And with continued family and friend support I am proud to be a HART Technician Operative.
HART is funded by the government under the EP for the next two years; from there on the local primary care trust will commission HART within the Ambulance contract. HART teams across England are busy and have already dealt with a wide range of incidents. HARTs work will involve RTCs, train incidents, working at heights, confined spaces, swift water rescue, smoke filled and other toxic environments. In addition to this HART will respond to 999 calls in two adapted single response vehicles. HART will also provide support to other emergency services such as the police, fire rescue and some specialist services. South East Coast HART team will also be able to respond to national and potentially international requests for mutual aide.
HART Technician Chris TrevesSpotlight
on –I joined the ambulance service over five years ago and have worked in
healthcare for over 15 years now. I’ve been keen and enthusiastic in any
job I’ve entered and I’m always willing to learn.
Excellence in leadership and development

Improving access and outcomes
4
We realise it’s been frustrating for some staff, that clinical updates have come through to you via different sources, with well meaning and informed clinical experts in the Trust and outside, giving different guidance as to which of these should be adhered to. The questions you have asked are should you be following JRCALC guidelines and picking up amendments to the same off your own backs? Is this part of your HPC registration duty? Or should you wait for these to be approved by SECAmb’s MAG? Or follow guidance in the bulletin and in team briefing folders? Or even taking advice from clinical champions, such as Stroke champions, or CHD champions?
Since we do have all these methods of communicating changes in clinical practice, undoubtedly it has been a bit of a minefield. The advice you have been given during key skills training has been to follow JRCALC. JRCALC is, by definition, for guidance, although it is generally well respected and authoritative, it is however, up to local trusts to adopt what they feel is appropriate. The situation has also been further complicated by the delay in approval for the latest version of the new JRCALC guidelines, but these are now in preparation.
Now that we have the team briefing folder, we will be able to provide you with accurate updates that will either sanction the adoption of JRCALC or UKRC updates or supersede them. This information will also be reflected in key skills updates.
However the good news is, since the introduction of the team briefing folder and the clinical instruction, we are able to keep a handle on this important roll out of information. In a nutshell, any clinical updates from JRCALC have to also be agreed by SECAmb’s Medical Advisory Group and appropriate cascade training carried out before
staff are able to practice.
Therefore the stroke/TIA guidelines, which have been agreed, have been communicated via clinical instructions and, prior to the introduction of these, bulletin articles, but such updates as Oxygen administration, sickle cell update on sub cut morphine and patients’ own buccal midazolam have not, although this is under review.
To clear up the confusion on a number of issues raised recently, we have begun to issue clinical instructions highlighting which guidelines to follow for the following:
• Administering of sub cut morphine to sickle cell patients
• Administering of patients’ own buccal midazolam
• Administering of Aspirin if a patient is on Warfarin and is having a barn door STEMI AMI
• Following the latest UKRC anaphylaxis guidelines in place of JRCALC 2006
We are also starting to develop clinical management plans, relating to specific patient conditions, which will help to provide clarity for staff around exactly what clinical care should be provided in each case.
And remember, if you have any clinical questions that you are unable to get a clear answer for you can always email [email protected]
Andy, Kath and Jane
This column is a joint communication from Director of Professional Standards and Innovations Professor Andy Newton, Medical Director Jane Pateman and Director of Workforce Development & Chief Nurse Kath Start. The purpose is to provide you with the bottom line on clinical updates, JRCALC and SECAmb’s Medical Advisory Group (MAG).
Clinical columnthe final word on clinical updates
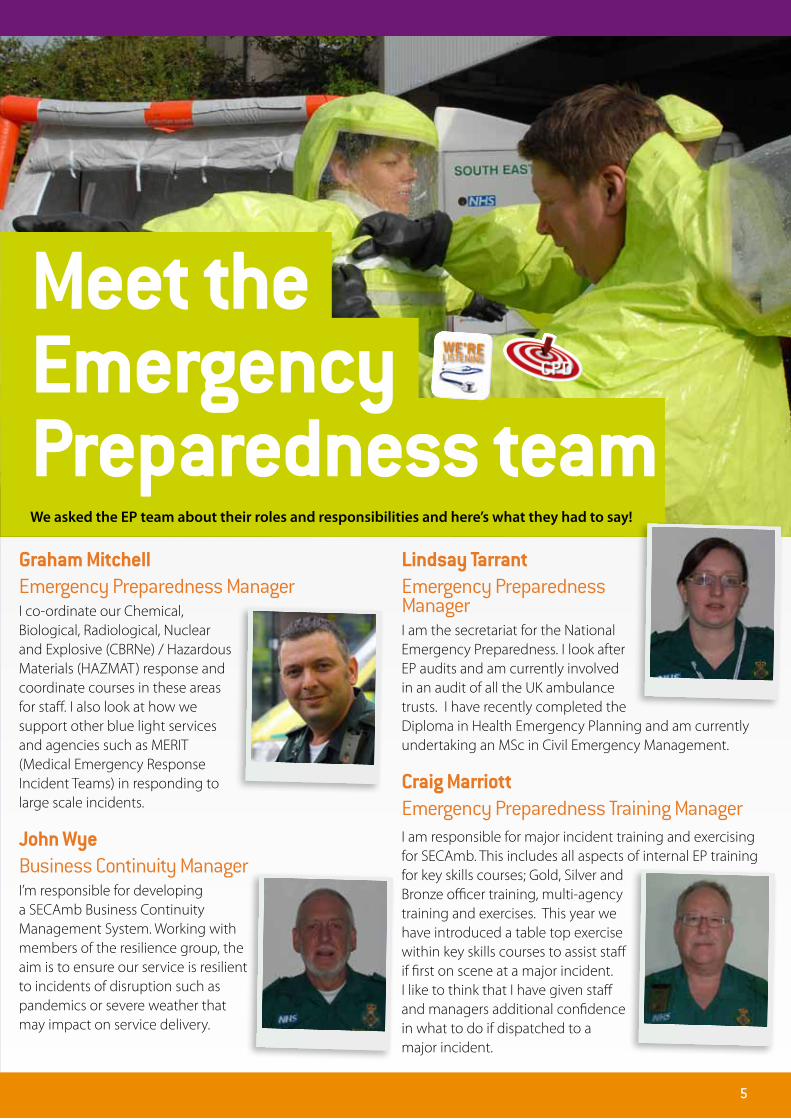
Graham Mitchell Emergency Preparedness ManagerI co-ordinate our Chemical, Biological, Radiological, Nuclear and Explosive (CBRNe) / Hazardous Materials (HAZMAT) response and coordinate courses in these areas for staff. I also look at how we support other blue light services and agencies such as MERIT (Medical Emergency Response Incident Teams) in responding to large scale incidents.
John Wye Business Continuity ManagerI’m responsible for developing a SECAmb Business Continuity Management System. Working with members of the resilience group, the aim is to ensure our service is resilient to incidents of disruption such as pandemics or severe weather that may impact on service delivery.
Lindsay Tarrant
Emergency Preparedness ManagerI am the secretariat for the National Emergency Preparedness. I look after EP audits and am currently involved in an audit of all the UK ambulance trusts. I have recently completed the Diploma in Health Emergency Planning and am currently undertaking an MSc in Civil Emergency Management.
Craig Marriott Emergency Preparedness Training ManagerI am responsible for major incident training and exercising for SECAmb. This includes all aspects of internal EP training for key skills courses; Gold, Silver and Bronze officer training, multi-agency training and exercises. This year we have introduced a table top exercise within key skills courses to assist staff if first on scene at a major incident. I like to think that I have given staff and managers additional confidence in what to do if dispatched to a major incident.
Meet the Emergency Preparedness teamWe asked the EP team about their roles and responsibilities and here’s what they had to say!
5
6
Improving access and outcomes
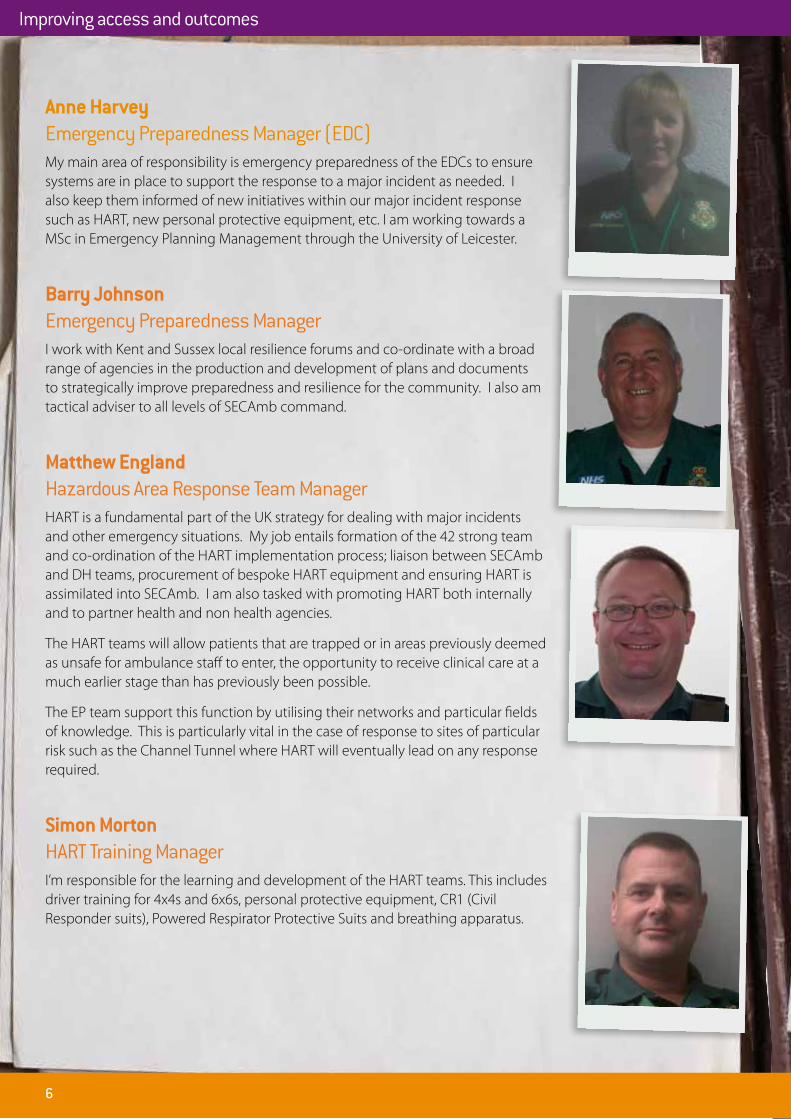
Anne Harvey Emergency Preparedness Manager (EDC)
My main area of responsibility is emergency preparedness of the EDCs to ensure systems are in place to support the response to a major incident as needed. I also keep them informed of new initiatives within our major incident response such as HART, new personal protective equipment, etc. I am working towards a MSc in Emergency Planning Management through the University of Leicester.
Barry Johnson Emergency Preparedness ManagerI work with Kent and Sussex local resilience forums and co-ordinate with a broad range of agencies in the production and development of plans and documents to strategically improve preparedness and resilience for the community. I also am tactical adviser to all levels of SECAmb command.
Matthew England Hazardous Area Response Team ManagerHART is a fundamental part of the UK strategy for dealing with major incidents and other emergency situations. My job entails formation of the 42 strong team and co-ordination of the HART implementation process; liaison between SECAmb and DH teams, procurement of bespoke HART equipment and ensuring HART is assimilated into SECAmb. I am also tasked with promoting HART both internally and to partner health and non health agencies.
The HART teams will allow patients that are trapped or in areas previously deemed as unsafe for ambulance staff to enter, the opportunity to receive clinical care at a much earlier stage than has previously been possible.
The EP team support this function by utilising their networks and particular fields of knowledge. This is particularly vital in the case of response to sites of particular risk such as the Channel Tunnel where HART will eventually lead on any response required.
Simon Morton HART Training ManagerI’m responsible for the learning and development of the HART teams. This includes driver training for 4x4s and 6x6s, personal protective equipment, CR1 (Civil Responder suits), Powered Respirator Protective Suits and breathing apparatus.

Jon Amos Emergency Preparedness ManagerMy role is in three parts to co-ordinate a new public events strategy for the Trust, ensure that public events across our patch have sufficient medical provision and that we attend when needed. Also on our Olympic research and planning. And finally I support the HART project, particularly around procurement of specialist equipment.
John HopkinsHART/ CBRN Command InstructorI joined the National NHS HART project as an instructor in 2008 on secondment. I am currently on a job share with SECAmb to assist with the development of HART as well as working on the National HART Project at Winterbourne Gunner.
Rory Collinge HART Project Support/AdministratorI support the delivery of the HART project in all aspects. I am involved in ensuring the procurement of equipment and courses, recording the progress of the HART team, and ensuring that the various parts of the project are delivered on time.
Andy ParrHead of Emergency PreparednessI head up our Emergency Preparedness Team and represent SECAmb at the Local and Regional Resilience Forums. I sit on the EP Board and am the lead for the policy and procedures work stream. I link with the Department of Health providing co-ordination for the National Capability Mass Casualty Equipment Vehicles, emergency dressings packs at main transport hubs and the development of Ambulance Maritime Incident Response Teams as part of the HART project. HART is a new and cutting edge initiative and an exciting new challenge for our team.
I still regularly respond to patients and firmly believe that the patient is at the heart of everything we do.The creation of SECAmb provided EP with a unique opportunity to modernise and professionalise the function. There is an active move towards the role of our EP Team to become world class expert advisers across the four generic areas of resilience Risk – Readiness – Response – Recovery. In the future all staff involved with EP must hold a professional qualification to become an ‘EP practitioner’. Many of the team members are currently following an academic course of study which will result in each one gaining a Masters or equivalent in their chosen subject area.
A team to be proud of!
7

8
Hello Michael,
I so hope you get this. It’s just a little note to say
thank you to you. Well a huge thank you in fact. Since
that Tuesday I’ve often thought what a different sort
of day it could have been and how mine and my
family’s life would have been turned upside down if
it weren’t for you.
I know you said it was your job and I know there are a
million guys doing it. But you are our one in a million.
Apart from saving Mum, you showed such care and
kindness and it will never be forgotten. Don’t ever
change – you’re bloody lovely! You take care and
truly, from the bottom of my heart, thank you.
Kind regards,
Sarah
This wonderful thank you came in a card to Michael
Jones, a Technician in Bognor Regis. Michael helped
Sarah’s Mum when she suffered an allergic reaction.
You really made an impression Michael, and a real
difference. Great work.
A truly lovely letter
From: Mr WSubject: Thank you Date: 11 June
Please could you pass on my deepest thanks to all involved in helping me after I collapsed at Lewes Victoria Hospital’s Minor Injury Unit on Saturday 5th June 2010.
Although I am not really aware of what actually happened after I collapsed, I have heard much from my girlfriend about your staff. I understand I presented your staff with an unusual situation which they may not have dealt with before. Despite this they clearly undertook their job with professionalism and skill.
I am very grateful for their help and I really appreciated the paramedic visiting me the following day at RSCH’s Acute Care Ward and for explaining some of what happened. Please pass on my thanks to all those concerned.
The great crew faced with this ‘unusual situation’ were Brighton’s David Miles (Paramedic) and Joseph Romaine (Technician). And the situation? Adder bites. Not something we see every day! Well done.
Skilled care in unusual circumstances
Improved satisfaction and experience for everyone

From: Mr HSubject: Thank you Date: 29 April
On the 16th April, my mum collapsed with her BP in her boots. I can’t express my thanks enough that the Crew who attended were so professional and kind. Mum couldn’t stop praising them. She was discharged the next day, although unfortunately it appears some brain/neuro problems were missed: and she collapsed with left-sided weakness/FAST Positive that Tuesday (20th April). Once again, she was treated wonderfully and, again, I’m so very grateful.
In both instances, your staff delivered an excellent level of service which freed our minds to focus on Mum rather than her care. Mum was discharged yesterday, with some residual weakness from CVA, but is generally much improved. Fortunately, she’s still fit enough to bake so her invitation to ‘ginger dunkers and a cuppa’ remains for any of the Staff/Crews who might be passing! Thank you.
Wonderful work by our teams on both occasions. Thank yous go out to: Lanre Madarikan (ECO) and Emily Paul (Dispatcher) in Lewes EDC; Anne Myhill (Technician), Marian Bowell (Paramedic) and Nick Bath (CTL) in Bognor; Steve Andrews (COM), Ronnie Redstone (Technician) and Zana Gall (Paramedic) in Chichester; and Charlotte Wood (ECO) and Hannah Culver (Dispatcher) in Lewes EDC.
Dunkers and a cuppa all round!
9
Skilled care in unusual circumstances

10
Beemail makes it easier than ever to say thank you
As always, here are some of the best messages taken from the bee-line!
Date left By Thanking For
2 April Tamsin Harwood Technician Rye
Dave Cook PTS/CFRHastings
I am continually impressed with your skill and level of care when community responding. Often we turn up after you at jobs to find the paperwork started and obs being undertaken in a systematic and thorough way. We don’t recognise or commend each other in this job very much and I think it sometimes gets missed. So credit where credit is due, just wanted to let you know!
3 May Godstone Ambulance station
John Kempton Community ResponderOxted
Yesterday John wasn’t on duty and EDC rang him on the off chance that he could respond. He was at a friend’s Confirmation and he dropped everything and responded. We think that he needs a thank you for all the good work he does. From all of us.
27 May Stuart Ward CTL Bognor
Ken Brown and Graeme Pidgeon PTSBognor
Ken and Graeme were first on scene to a two car head-on incident with four casualties. They dealt admirably with the incident until the first A/E crew arrived and then continued to work effortlessly as if it was something they dealt with everyday. How this incident was handled reflects well on all the Ambulance staff that attended: S Offer, D Croucher, A Webster (Chichester A/E), and D Skidmore and P Lawrence (Bognor A/E).
7 June Kirsty Lane CTL Tongham
Farnborough Technicians Dave Wallace and Richard Baker
Dave and Richard deserve praise for the professionalism and team work that they showed at a recent resus. They responded to a gentleman who was suffering with chest pain, who then collapsed and went into cardiac respiratory arrest. On my arrival he had a weak pulse and by the time we arrived at hospital he had return of spontaneous respiration and circulation. I have no doubt that this gentleman’s survival was down to the fast actions and quick thinking of the crew; they were a pleasure to work with.
8 June Lucy James CTLSittingbourne
Crystal McDonaghDispatcher Coxheath EDC
Thank you for your exceptional communication skills with crew on a cardiac arrest, constantly keeping the crew updated and informed, followed by genuine care and concern for the crew’s welfare after the job. This made such a difference and did not go unnoticed. Thank you!
14 June Andrew Anderson Technician Chichester
Peter Jones ECSW Worthing
Thanks to Peter for a great day when we worked together at Haywards Heath. Peter was very competent and confident: he has obviously gained significantly from the mentoring he has received on the STV at Worthing and he has good clinical ability himself.
20 June Nigel Brown DDM Lewes EDC
Sam Huguenot Dispatcher Lewes EDC
Chichester crew c/s 109 would like to thank you for looking after them today: they say you were ‘fantastic’! Well done, it is always nice to receive praise from our operational colleagues. Keep up the good work!
The new Bee-line email address (Beemail!) is proving popular, so much so that we’ve devoted more space to your thank you messages than usual in this edition of STAR. Keep them coming!
Improved satisfaction and experience for everyone
Create a buzz -call the bee-line01622 740317

11
Proud to work for
A Prince’s Trust SecondmentI began my secondment on 4 January with ‘Plantation’ at Guildford YMCA to assist a full time Prince’s Trust team leader, Nick Bragger, on a 12 week TEAM programme. Plantation has been running the Prince’s Trust programme in Surrey for the last seven years, but this was the first time they had used an outside agency. This was also the first time someone from the ambulance service was involved. So, I was full of excitement, good ideas and nerves.
The programme is a framework developed over many years by the Prince’s Trust which is given to local associations such as the YMCA to deliver. The following extract from literature they use in their recruitment process captures the essence of what they are trying to achieve:
“The Prince’s Trust Team is a challenging 12 week programme that helps troubled young people, between the ages of 16-25, to develop the confidence, motivation and skills to turn untapped potential into success. It is completely free and runs from Monday to Friday each week. It is often intense and demanding. One day you might be designing a community fundraising strategy, another day might mean enduring the elements in the wilderness of Dartmoor. By nature it stretches all those involved - mentally and physically. The focus of each week is
different and, if you go the full distance, you will feel inspired to keep achieving. A Prince’s Trust Team is rewarding like nothing else.”
Young people were referred to us from various sources - Connexions, job centres, key workers and youth justice officers. These young people are all mainly described as NEET (Not in Education Employment or Training) through either poor qualifications from school, disruptive behaviour or drug/alcohol misuse. I was involved in the interview process for the 12 young people and chose who I thought would benefit most.
After our first two weeks of team building and getting to know each other, we headed for Brockenhurst in the New Forest for our residential week. We used qualified adventure instructors and I was lucky enough to be able to sit back and enjoy watching my team getting very wet and muddy but, more importantly, gain confidence and boost their self-esteem. Activities included canoeing, rock climbing, abseiling, night navigations and problem solving. The team ended the week on the last day with a final team challenge to ‘save an agent from her captors’. This mission was successful... and carried out with a lot of shouting and running through mud! The week really showed the team what teamwork is all about.
Morris MacKenzie tells us about his experience working with a group of 12 young people on a YMCA project at Guildford...
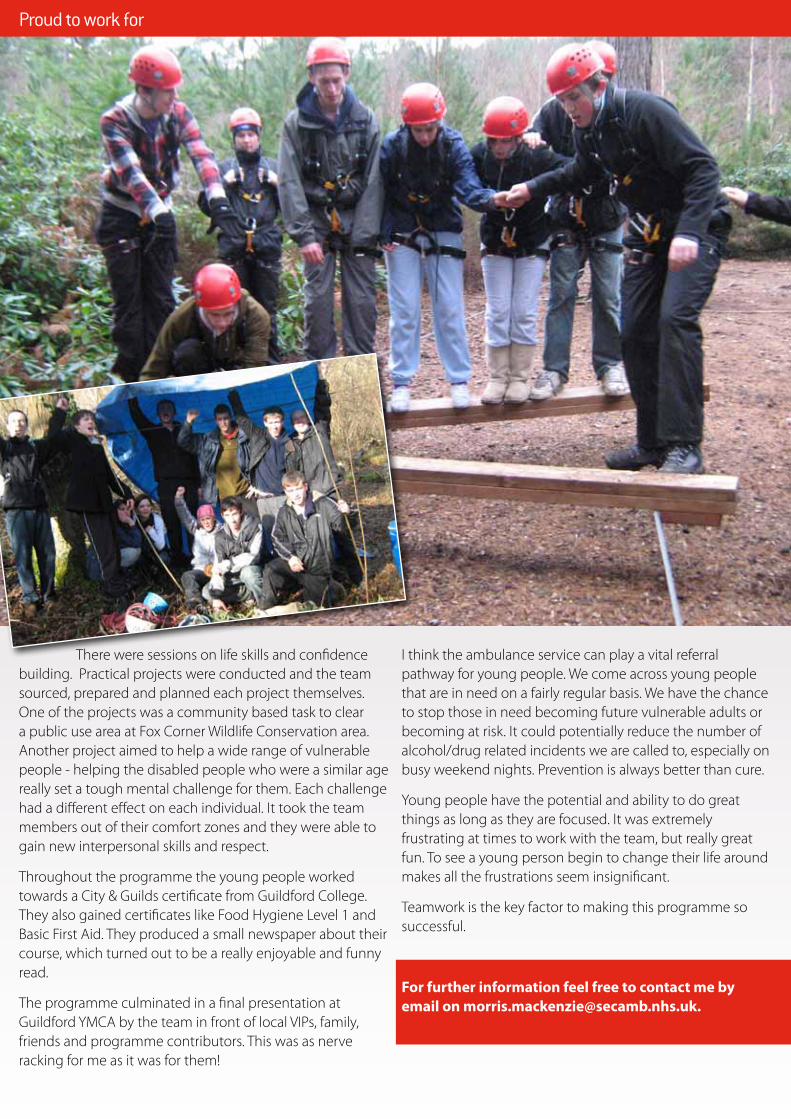
There were sessions on life skills and confidence building. Practical projects were conducted and the team sourced, prepared and planned each project themselves. One of the projects was a community based task to clear a public use area at Fox Corner Wildlife Conservation area. Another project aimed to help a wide range of vulnerable people - helping the disabled people who were a similar age really set a tough mental challenge for them. Each challenge had a different effect on each individual. It took the team members out of their comfort zones and they were able to gain new interpersonal skills and respect.
Throughout the programme the young people worked towards a City & Guilds certificate from Guildford College. They also gained certificates like Food Hygiene Level 1 and Basic First Aid. They produced a small newspaper about their course, which turned out to be a really enjoyable and funny read.
The programme culminated in a final presentation at Guildford YMCA by the team in front of local VIPs, family, friends and programme contributors. This was as nerve racking for me as it was for them!
I think the ambulance service can play a vital referral pathway for young people. We come across young people that are in need on a fairly regular basis. We have the chance to stop those in need becoming future vulnerable adults or becoming at risk. It could potentially reduce the number of alcohol/drug related incidents we are called to, especially on busy weekend nights. Prevention is always better than cure.
Young people have the potential and ability to do great things as long as they are focused. It was extremely frustrating at times to work with the team, but really great fun. To see a young person begin to change their life around makes all the frustrations seem insignificant.
Teamwork is the key factor to making this programme so successful.
For further information feel free to contact me by email on [email protected].
12
Proud to work for
The winning caption came from Technician Paul Nelms from Walton ambulance station; the caption: “See that gap down there, that’s where your lunch went back in the old days”. Well done Paul – you get a £15 voucher courtesy of Health and Wellbeing (the new name for Welfare).
Caption Competition
This next one was taken by Hazel Wilks, a member of the STAR editorial team, at a street party.
As always, email your captions to [email protected] by 5.30pm on 18 September 2010 and we’ll give you a couple of weeks to vote for a winner!
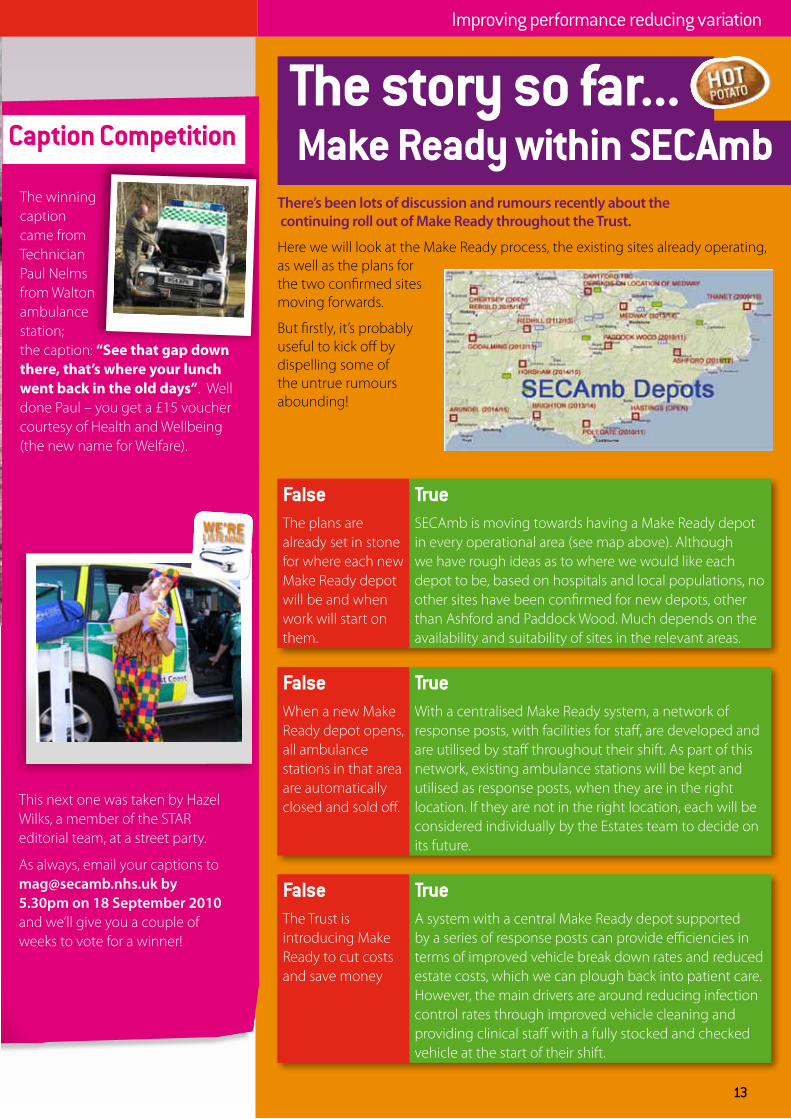
There’s been lots of discussion and rumours recently about the continuing roll out of Make Ready throughout the Trust.
Here we will look at the Make Ready process, the existing sites already operating, as well as the plans for the two confirmed sites moving forwards.
But firstly, it’s probably useful to kick off by dispelling some of the untrue rumours abounding!
FalseThe plans are already set in stone for where each new Make Ready depot will be and when work will start on them.
TrueSECAmb is moving towards having a Make Ready depot in every operational area (see map above). Although we have rough ideas as to where we would like each depot to be, based on hospitals and local populations, no other sites have been confirmed for new depots, other than Ashford and Paddock Wood. Much depends on the availability and suitability of sites in the relevant areas.
FalseWhen a new Make Ready depot opens, all ambulance stations in that area are automatically closed and sold off.
TrueWith a centralised Make Ready system, a network of response posts, with facilities for staff, are developed and are utilised by staff throughout their shift. As part of this network, existing ambulance stations will be kept and utilised as response posts, when they are in the right location. If they are not in the right location, each will be considered individually by the Estates team to decide on its future.
FalseThe Trust is introducing Make Ready to cut costs and save money
TrueA system with a central Make Ready depot supported by a series of response posts can provide efficiencies in terms of improved vehicle break down rates and reduced estate costs, which we can plough back into patient care. However, the main drivers are around reducing infection control rates through improved vehicle cleaning and providing clinical staff with a fully stocked and checked vehicle at the start of their shift.
13
The story so far... Make Ready within SECAmb
Improving performance reducing variation

14
The story so far... Make Ready within SECAmb
Improving performance reducing variationImproving performance reducing variation
The Trust has already introduced Make Ready in three ODAs throughout SECAmb, centred on: • Chertsey • Hastings • Thanet This approach has utilised the existing Trust sites at the above locations and converted the ambulance stations into Make Ready depots, working on a “hub and spoke” approach with crews from existing stations feeding into the Make Ready depot.
Feedback from staff working in these three areas has been overwhelmingly positive, with many of those who were initially sceptical now converted to the Make Ready way!
In the pipeline...The two sites currently being developed, at Paddock Wood and Ashford, will be the first “central reporting” depots within SECAmb. This will see purpose built depots created, supported by a network of response posts.
Why are we moving to centralised
Make Ready? Why not develop more “hub and spoke” sites like Hastings, Thanet and Chertsey? Or have mini Make Readys at each ambulance station?One of the main reasons is the lack of suitable sites to convert. But there are a number of other reasons why the Trust Board has chosen to move to centralised Make Ready, including:
• Increased numbers of staff based at a depot provide far greater flexibility and opportunities than smaller numbers of staff based at individual stations. This is especially important in terms of developing new rotas, allowing for a range of shift lengths and flexible working options, as well as improving our clinical governance and team working.
• The location and condition of our existing estate. Many of our existing ambulance stations are located in the wrong places to best respond to our patients, as well as expensive to maintain and up-grade
• The logistics involved at providing support services (cleaning and re-stocking of vehicles and checking and servicing of the vehicles) would make it simply impossible to provide these locally!
Why are both of the first new Make Ready depots in Kent?This isn’t part of a set plan (see above), more about the particular circumstances in these two areas.
With the building of a new hospital at Pembury and the planned re-development of the Kent & Sussex Hospital site at Tunbridge Wells, we urgently needed to find a new site for the current ambulance station located on the hospital site at Tunbridge Wells. With a site becoming available at Paddock Wood, it meant plans could move forwards for the new depot and provide staff with a new base in the area, closer to the new hospital.
We also needed to quickly set up a base for the first HART team in Kent and it made sense to make this a combined Make Ready/HART base,
How will a centralised Make Ready depot affect me and my working live?
• I will be able to pick up a clean, fully stocked and checked vehicle at the start of my shift.• I won’t have to worry that a vital piece of kit may be missing or that there won’t be enough fuel in
the vehicle• I may have a longer journey into work than currently, depending on where I live (although it could
also be less!). The implications of changing base are largely covered by Agenda for Change, although everything will be discussed with staff side representatives and via the Joint Partnership Forum
• Being part of a much larger team will provide new possibilities in terms of opportunities to work more flexibly (A range of rota options are currently being developed, which will provide different shift lengths, as well as the potential for flexible working options like term-time working or a rota comprising only nights. Rota planning like this is just not possible with a number of small stations as you need a large number of staff to provide the flexibility).
• During my shift, I will be able to take my break at one of the response posts with facilities in the area.
15
rather than two separate projects. The site in Ashford is well located strategically, in the centre of the ODA and close to the main hospital, with good transport links to key sites like the ports at Dover and Folkestone and the Channel Tunnel.
Paddock Wood The proposed depot for the Weald ODA will be located at Paddock Wood and will support staff currently working out of:
• Crowborough
• Tonbridge
• Tunbridge Wells
• Maidstone
• Cranbrook
• Sevenoaks
We are awaiting the final planning permission at the moment, which will allow building work to start.
Ashford The new Make Ready depot at Ashford, covering East Kent ODA, will also serve as the base for SECAmb’s first Hazardous Area Response Team (HART). As well as the HART team, the new depot will support staff currently working out of:
• Dover
• Folkestone
• Lydd
• Ashford
The Trust Board has given the go ahead for the purchase of the land and planning permission has also been submitted for this site. If permission is approved, work could start in Autumn 2010.
How to find out more?Over the coming months, there will be:
• Special bulletins/bulletin articles
• A series of station engagement sessions (at all the stations affected), with the opportunity to find out more about the new depot, the
process involved, etc. Dates for these are being arranged currently and will be circulated asap.
• Make Ready Champions – members of staff at each station affected, who will be able to keep local staff updated on the project, answer questions as well as feed back any questions and / or concerns that local staff may have
• Further articles in STAR
• Dedicated e-mail address – [email protected]; [email protected] or [email protected] - if you have a query, please e-mail these addresses as appropriate
We understand that these changes may be unsettling for some staff and we are fully committed to working with staff to ensure that the changes are implemented as smoothly as possible for everyone.

16
Reaction Against Non Truths! - IR1s for missed meal breaks RANT!
At a recent meeting of the FT champs they raised an issue about clinical risk to patients as a result of missed meal breaks – staff being too tired to perform at their best.
The issue is that staff feel that these IR1s ought to be receiving the same level of feedback as those submitted for any other reason.
So, if this is a RANT, where’s the non truth here?
These particular IR1s are not processed in the same way as other IR1s but they are, we can assure you, being seen by the right people!
What are we doing with this information?The IR1 system of reporting such incidents was requested by the Meal Break Working Group (MBWG) as this was the most robust system of reporting/recording in the Trust. They are still verified by Clinical Operations Managers (COMs) and if there is a risk to patients, this is investigated. They are also loaded to DATIX.
A breakdown of numbers by station and by area is discussed at the MBWG meetings, which includes staff-side representatives. This helps provide us with information where
the CAD has been unable to record missed meal breaks (as reported in the meal break communication circulated to all operational staff on 8 June 2010).
This information is then used to identify training issues within the EDCs – patterns emerge and we can see who is managing the meal break policy and who is not. We also use the information to report against the KPIs set out for each segment of the meal break window i.e. 30% within the first hour.
What happens next?
Whilst we are working hard to address issues raised we recognise that we have not published information to the bulletin as promised. We are instead circulating this information only to the staff that are affected by the interim A&E meal break policy. The interim policy will only work if we all work together. If you have any ideas on how the meal break policy would work better within the agreed parameters (i.e. non-disturbable and unpaid unless you opt out and within a four hour window) email [email protected].
End of RANT!
Using resources effectively
Next issue out Autumn 2010


















