
Nezam Afdhal, MD Michael Fried, MD Ira Jacobson, MD · COBAS® ®AmpliPrep/COBAS Taqman® HCV Test....
54
Accredited by: Sponsored by: Nezam Afdhal, MD Beth Israel Deaconess Medical Center Boston, MA Kim Brown, MD Henry Ford Hospital Detroit, MI Jordan Feld, MD Toronto Western Hospital Liver Center Toronto, Canada Michael Fried, MD University of North Carolina Chapel Hill, NC Ira Jacobson, MD Weill Cornell Medical College New York, NY Presented for attendees of the 63rd AASLD Annual Meeting (or The Liver Meeting ® ). This event/function is sponsored by Chronic Liver Disease Foundation and supported by Vertex Pharmaceuticals. This is not an official function/event of the American Association for the Study of Liver Diseases. Supported by:
Transcript of Nezam Afdhal, MD Michael Fried, MD Ira Jacobson, MD · COBAS® ®AmpliPrep/COBAS Taqman® HCV Test....

Accredited by: Sponsored by:
Nezam Afdhal, MD Beth Israel Deaconess
Medical Center
Boston, MA
Kim Brown, MD Henry Ford Hospital
Detroit, MI
Jordan Feld, MD Toronto Western
Hospital Liver Center
Toronto, Canada
Michael Fried, MD University of North Carolina
Chapel Hill, NC
Ira Jacobson, MD Weill Cornell Medical College
New York, NY
Presented for attendees of the 63rd AASLD Annual Meeting (or The Liver Meeting®).
This event/function is sponsored by Chronic Liver Disease Foundation and supported by Vertex Pharmaceuticals.
This is not an official function/event of the American Association for the Study of Liver Diseases.
Supported by:

Welcome
• Tonight’s News Program
– Field Report – Breaking News on New CDC Recommendations
• Michael Fried, MD
– Case #1 – Treat Now or Wait for Future Therapies
• Kim Brown, MD; Jordan Feld, MD
– Field Report – Breaking News on Real-World Clinical Data
• Ira Jacobson, MD
– Case #2 – Optimizing Outcomes with Current Treatments
• Kim Brown, MD; Jordan Feld, MD
– Press Conference: Late Breaking Data, Q&A

Glenn: Patient Characteristics
• 55 year old male
• Shift worker
• History/risk factors
– BMI=34
– Hypertension and dyslipidemia
– Moderate drinker/cigarette smoker
• Concomitant medications
– Simvastatin 20 mg/day
– Lisinopril 10 mg/day

Glenn: Baseline Labs
• Hemoglobin 15.6 g/dL
• Neutrophils 1400 cells/mm3
• Platelets 210,000 cells/mm3
• AST/ALT 55/75 IU/L
• Albumin 4.1 g/dL
• Bilirubin 0.7 mg/dL

Glenn: Disease Characteristics
• Treatment naïve
• Genotype 1a
• IL28B CC
• METAVIR F3
• BL viral load 1,300,000 IU/mL

ARS #1
• How would you manage this patient?
1. Continue to monitor patient but do not start treatment
2. Start patient on first generation protease inhibitor/PEG-IFN/RBV

Modeling of Liver Fibrosis in Chronic Hepatitis C
n=1157 Patients
0
1
2
3
4
0 10 20 30 40 50
F M
eta
vir
Years
Rapid progressors Intermediate progressors
Slow progressors
Poynard et al, Hepatology 1999
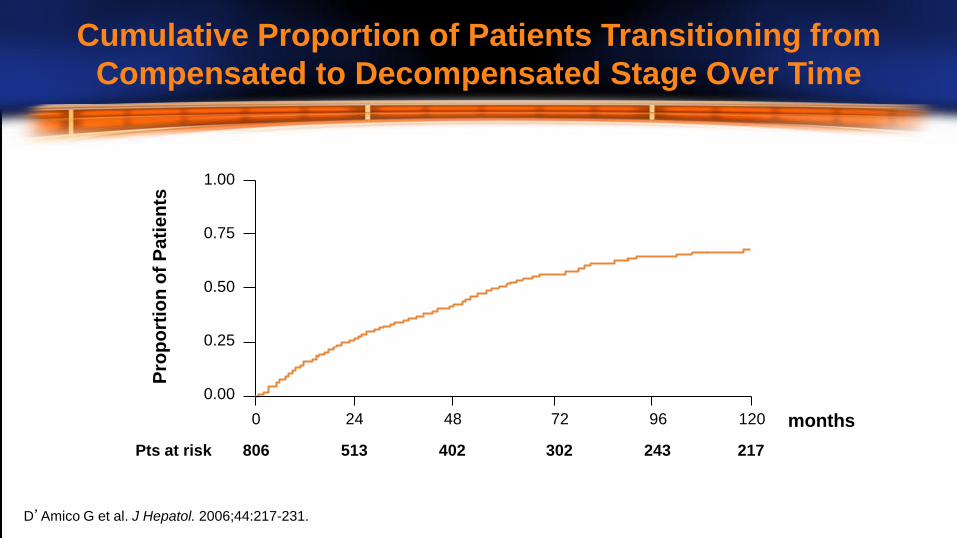
D’Amico G et al. J Hepatol. 2006;44:217-231.
Pro
po
rtio
n o
f P
ati
en
ts 1.00
0.75
0.50
0.25
0.00
Pts at risk 806 513 402 302 243 217
months 0 24 48 72 96 120
Cumulative Proportion of Patients Transitioning from
Compensated to Decompensated Stage Over Time

0%
20%
40%
60%
80%
100%
Non-responders (n=1452)
Relapsers (n=464) Sustained responders (n=1094)
36% 43%
86%
43% 36%
12% 21% 21%
2%
% o
f p
ati
en
ts
Improved Stabilized Worsened
*Necrosis and Inflammation.
Poynard et al. Gastroenterology, 2002;122:1303-1313.
Impact According to Response of 10 Different Treatment Regimens
on Evolution of Activity* in 3010 Patients with Paired Biopsies

Jacobson et al. EASL 2011
*T12PR = T+PR12 weeks, then PR12 or 36 weeks depending on eRVR status
**T8PR = T+PR8 weeks, then PR16 or 40 weeks depending on eRVR status
In Patients Tested for IL28B (%)
In All
ADVANCE
Patients
CC CT TT Total
T12PR* 90 71 73 78 75
T8PR** 87 58 59 67 69
PR 64 25 23 38 44
ADVANCE: IL28B Genotype Effect on
Telaprevir Therapy

SVR Rates in F1/2 vs F3/4 Naïve Patients
0
10
20
30
40
50
60
70
80
90
100
Boceprevir Telaprevir
F1/2
F3/4 76%
67% 67%
48% SV
R
Poordad F et al, NEJM, 2011; 364: 1195-1206
Jacobson IM et al, NEJM, 2011; 364: 2405-2416

OPTIMIZE Trial: Telaprevir BID vs TID
• PR + TVR 1125 mg BID versus 750 mg TID
• Response-guided therapy
• 740 patients
• 29% bridging fibrosis or cirrhosis
• 57% G1a, IL28B CC 29%
Buti M et al, Abstract LB-8, AASLD 2012

OPTIMIZE Trial: Results
0
20
40
60
80
100
RVR SVR
TVR 1125 mg BID
TVR 750 mg TID
(%)
69% 67%
74% 73%
Buti M et al, Abstract LB-8, AASLD 2012

Should Glenn Be Treated Now?
• F3 disease – risk of progression with waiting
• IL28B CC
• Potential BID option is attractive
• I would treat
• Multiple issues with current therapy
– Compliance – pill burden
– Co-morbidities
– Adverse effects
The Case for Waiting
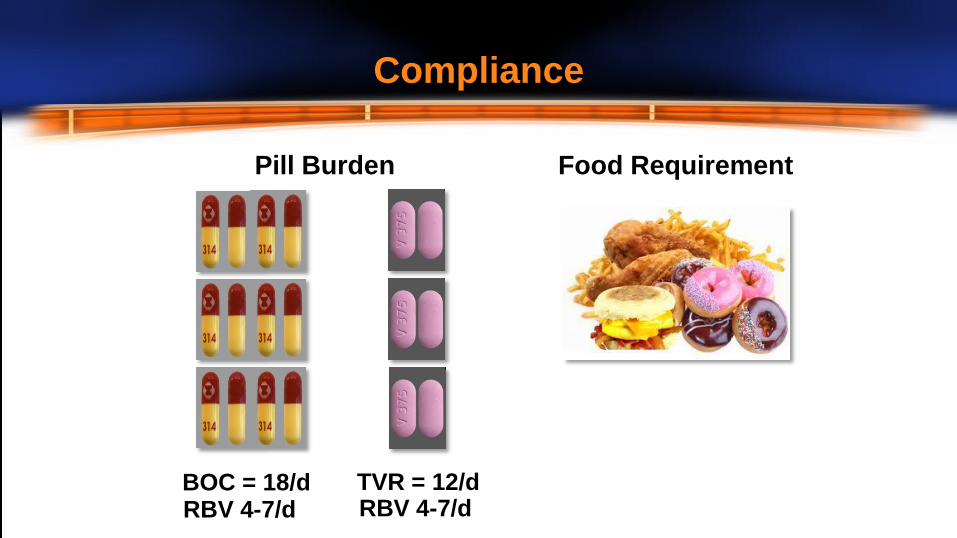
BOC = 18/d TVR = 12/d
Pill Burden Food Requirement
RBV 4-7/d RBV 4-7/d
Compliance

• Cardiac Risk Factors
– Hypertension, hyperlipidemia, smoker
• Pre Treatment
– DDI – Statin with TVR/BOC likely just stop it
• On Treatment
– Anemia management consider pre-treatment cardiac testing
Co-Morbidities

Drugs with the Potential to Interact with First Generation
Protease Inhibitors are Commonly Used by HCV Patients
Mayer et al, Abstract #136, AASLD 2012
Drug Name Percent Drug Name Percent
Zolpidem * 17.4 Diazepam 7.9
Codeine 16.0 Bupropion * 7.2
Prednisone 15.4 Trazodone 7.1
Tramadol * 14.3 Fluconazole 6.8
Citalopram 13.5 Sertraline 6.4
Fluticasone 13.1 Clarithromycin 6.1
Methylprednisolone 13 Sildenafil (Viagra) 5.4
Alprazolam * 11.8 Clonazepam 5.3
Amlodipine * 10.2 Simvastatin 5.2
Escitalopram * 8.1 Venlafaxine 5.0
* One of the 20 most frequently filled
• No clinically significant interactions
– Boceprevir
• Prednisone (abstract #1896)
• Omeprazole (abstract #1808)
• Ethinyl estrodiol/norethidrone (abstract #1901)
– Simeprevir (TMC-435)
• Cyclosporine/tacrolimus (abstract #80)
• Ethinyl estrodiol/norethidrone (abstract #773)
New Drug-Drug Interaction Data at AASLD
2012: HCV Protease Inhibitors

0
10
20
30
40
50
60
70
80
90
100
< 10 g/dL < 8.5 g/dL
BOC
PR
5/5 11/13 13/14
0
10
20
30
40
50
60
70
80
90
100
< 10 g/dL < 8.5 g/dL
TVR
PR
% o
f p
ati
en
ts
36%
17% 14%
5%
49%
28%
7% 3%
Anemia is a Known Side Effect with First
Generation Protease Inhibitor Based Therapies
% o
f p
ati
en
ts
Telaprevir (INCIVEK™) Prescribing Information. Vertex Pharmaceuticals Incorporated, Cambridge, MA. October, 2012.
Boceprevir (VICTRELIS™) Prescribing Information. Merck Sharp & Dohme Corp., Whitehouse Station, NJ, November 2012.

Future Options for Waiting? (Short-Term)
Simeprevir 150 mg OD x 12 wks + PR x 24-48
81
0
20
40
60
80
100
%
n/
N =
62/
77
50/
77
65
P=0.013
SVR
PILLAR (G1 Naïve)1
PR x 48
Faldaprevir 240 mg OD x 24 wks + PR x 24-48
83
%
n/
N =
118/
142
40/
71
56
P=0.001
SVR
SILEN C1 (G1 Naïve)2
PR x 48
93
57/
61
79
61/
77
SVR Met RGT
93
53/
57
87
124/
142
SVR Met RGT
2. Sulkowski et al. EASL 2011
0
20
40
60
80
100
1. Fried et al. AASLD 2011

Anemia with
Simeprevir + P/R1
Anemia with
Faldaprevir + P/R2
2. Sulkowski et al, EASL 2011
No Incremental Decline in Hemoglobin or
Neutrophils with Simeprevir or Faldaprevir
1. Jacobson et al, IDSA, 2012

Should Glenn Delay Treatment?
• IL28B CC ~80% chance of shortened therapy
- 80-90% chance of SVR
• F3 disease – risk of progression with waiting
• No clear issues with IFN
• Seems anxious and willing to be treated now
• I would suggest treatment

Glenn: On Treatment Response
• Glenn was started on TVR/PEG/RBV
• TW4 and TW12
– HCV RNA undetectable

ARS #2
• Which regimen should Glenn receive?
1. 12 weeks TVR/PEG/RBV
2. 12 weeks TVR/PEG/RBV + 12 weeks PEG/RBV
3. 12 weeks TVR/PEG/RBV + 24 weeks PEG/RBV
4. 12 weeks TVR/PEG/RBV + 36 weeks PEG/RBV
5. 24 weeks TVR/PEG/RBV

Recommended Treatment Duration
Treatment-Naïve and Prior Relapse Patients
HCV-RNA Triple Therapy
TVR/Peg-IFN/RBV
Dual Therapy
Peg-IFN/RBV
Total
Treatment
Duration
Undetectable at TW4 and
TW12
First 12 weeks Additional 12 weeks 24 weeks
Detectable (<1000 IU/mL)
at TW4 and/or TW12
First 12 weeks Additional 36 weeks 48 weeks
Telaprevir (INCIVEK™) Prescribing Information. Vertex Pharmaceuticals Incorporated, Cambridge, MA. October, 2012.

HCV-RNA Levels and Lab Assays
4/6 13/14
Assay Name LLOQ
Roche COBAS®
AmpliPrep/COBAS®
Taqman® HCV Test
43 IU/mL
Roche COBAS®
Taqman® HCV Test,
v2.0
25 IU/mL†
Abbott RealTime HCV
Assay 12 IU/mL
LLOQ Values for Various Assays*
*Package Inserts state the “the assay should have a lower limit of HCV-RNA
quantification ≤ 25 IU/mL and a limit of HCV-RNA detection of approximately
10-15 IU/mL. † Usually considered 25 IU/mL, but 23 IU/mL per FDA-approved label.
• “Undetectable” (or “target not
detected”) result is required for
assessing RGT eligibility
• Below LLOQ but still “detectable”
is not sufficient to shorten
therapy—ie, patient should
continue for full 48 wks
COBAS® AmpliPrep/COBAS® Taqman® HCV Test. Roche Molecular Diagnostics. Accessed July 19, 2011. Harrington PR, et al. Hepatology.
2012;55: 1046-1057. United States Food and Drug and Drug Administration (FDA), FDA Division of Antiviral Products; June 30, 2011.

• 45 year old African American female
• History/risk factors
– BMI=32
• CHC diagnosed in 2002
• Treated with Peg-IFN/RBV in 2007
– Tolerability issues: fatigue, anemia, neutropenia, alopecia,
anxiety, depression after 6 months (treated with paroxetine)
Jackie: Patient Characteristics

Jackie: Disease Characteristics
• Prior relapser (early virologic response)
• Genotype 1a
• IL28B CT
• METAVIR F1 in 2007
• BL viral load 18,000,000 IU/mL
Jackie: Baseline Labs
• Hemoglobin 12.1 g/dL
• Neutrophils 1300 cells/mm3
• Platelets 200,000 cells/mm3
• Serum creatinine 0.9 mg/dL
• AST/ALT 73/56 IU/L
• Albumin 4.1 g/dL
• Bilirubin 0.8 mg/dL
• INR 0.9

ARS #3
• Would you reassess stage of fibrosis before retreatment
and, if so, how?
1. No, I don’t believe it is necessary
2. Yes, I would re-biopsy the patient
3. Yes, I would use non-invasive test

ARS #4
• Which of the following statements is most accurate?
1. Jackie has a low likelihood of success because she is African
American and IL28B CT.
2. Jackie has a very high likelihood of success because she is a
prior relapser.
3. If restaging shows cirrhosis, Jackie has a very low chance of
success.
4. Treatment is contraindicated for Jackie since she developed
depression while on PEG/RBV.

86%
59%
32%22%
15%5%
0
20
40
60
80
100
REALIZE: SVR by Response to Previous
Peg-IFN/RBV Therapy
All Patients
%S
VR
All T12/PR48
Placebo/PR48
Relapsers Partial Responders Null Responders
Telaprevir (INCIVEK™) Prescribing Information. Vertex Pharmaceuticals Incorporated, Cambridge, MA. October, 2012.

72%
46%
31%
7%
0
20
40
60
80
100
%S
VR
BOC*
PR
Prior Relapsers Partial Responders
*Response Guided Therapy and 48 Week Arms Combined
150/208 16/51 53/115 2/29
RESPOND 2: SVR by Response to Previous
Peg-IFN/RBV Therapy
Boceprevir (VICTRELIS™) Prescribing Information. Merck Sharp & Dohme Corp., Whitehouse Station, NJ, November 2012.

Prior Response Trumps Other Pretreatment
Baseline Factors
• Ethnicity
• IL28B Genotype
• Baseline Viral Load
• Fibrosis Score
• G1 Subtype

Jackie: On Treatment Labs
Hemoglobin
(g/dL)
Neutrophil Count
(cells/mm3)
HCV RNA
(IU/mL)
Baseline 12.1 1300 18,000,000
TW2 11.0 1100 3,300
TW4 9.5 900 Undetectable

ARS #5
• How would you manage Jackie’s anemia?
1. No change to treatment
2. Add EPO
3. Reduce RBV from 1200 mg to 1000 mg
4. Reduce RBV from 1200 mg to 600 mg
5. Add EPO and reduce RBV (1200 to 600 mg)

82
72
10
82
71
10
0
10
20
30
40
50
60
70
80
90
100
EOT Response SVR Relapse
% o
f P
ati
en
ts
RBV DR Arm EPO Arm
203/
249 19/
196
178/
249
178/
251 205/
251 19/
197
Patients Randomized When
Hb <10 g/dL
Boceprevir: No Difference in SVR Rate in Anemic
Patients Undergoing RBV DR vs EPO Use
Adapted from Poordad F et al. Abstract 1419. Poster presented at the 47th Annual Meeting of the European Association for the Study of the
Liver. April 2012, Barcelona, Spain.

70
64
79
82 71
71 68
70
88
71
0
10
20
30
40
50
60
70
80
90
100
≤4 Wks >4-8 Wks >8-12 Wks >12-16Wks >16 Wks
SV
R (
%;
95
% C
I)
Timing of the Start of Anemia Management
RBV DR EPO Use
38/
54
39/
55
58/
90
60/
88
49/
62
47/
67
18/
22
15/
17
15/
21
17/
24
SVR Rates Did Not Vary with the
Start Time of Anemia Management
Poordad F et al, Abstract 154, AASLD 2012

Adapted from Sulkowski MS et al. Abstract 1162. Poster presented at the 47th Annual Meeting of the European Association for the
Study of the Liver. April 21, 2012, Barcelona, Spain.
0
10
20
30
40
50
60
70
80
90
Any Dose reduction Received ≤600 mg/day Received 800-1000 mg/day
Never reduced
T12PR
PR
74% 74% 75% 79%
47% 42%
54%
46%
SV
R, n
/N(%
)
RBV Dose Reductions
329/
446
291/
395
38/
51
346/
439
29/
62
16/
38
13/
24
134/
292
SVR Rates in Treatment Naïve Patients
by RBV Dose/Day

Jackie: On Treatment Labs
Hemoglobin
(g/dL)
Neutrophil Count
(cells/mm3)
HCV RNA
(IU/mL) Action
Baseline 12.1 1300 18,000,000
TW2 11.0 1100 3,300
TW4 9.5 900 Undetectable Decreased RBV
(1200 to 600 mg/day)
TW6 10.0 850 Undetectable
TW8 10.4 900 Undetectable
TW12 10.9 900 Undetectable Increased RBV
(600 to 800 mg/day)
TW16 11.5 1050 Undetectable Increased RBV
(800 to 1000 mg/day)

Jackie: Non-hematologic Adverse Events
How do you manage?
• Constitutional symptoms (fatigue, arthralgia)
• Mouth sores
• Rash
• Anorectal burning
• Depression

*12-week groups (G and H) were enrolled after 24-week groups (A, C, and E)
RBV: 1000-1200 mg/d, weight-based (GT1)
n = 41
n = 15
n = 14
SVR12 Week 24 SVR24
Follow-up
n = 41
n = 15
Follow-up
Follow-up
Follow-Up
SVR4 Week 12
Follow-Up
Group C: DCV 60 mg QD + SOF 400 mg QD
Group E: DCV 60 mg QD + SOF 400 mg QD + RBV
Group A: SOF 400 mg QD x 7d, then DCV 60 mg QD + SOF 400 mg QD
Group G: DCV 60 mg QD + SOF 400 mg QD
Group H: DCV 60 mg QD + SOF 400 mg QD + RBV
SVR4 SVR48
SVR48
Sulkowski MS et al, Abstract LB-2, AASLD 2012
LB-2: Daclatasvir (NS5A) +
Sofosbuvir (GS-7977, nuc) in GT1a/1b

20
SVR4
0
20
40
60
80
100
Week 4 SVR12
n = EOT
15 14 15
SVR24
C: DCV + SOF
A: SOF LI + DCV
E: DCV + SOF
+ RBV
87 93 73 % of patients
with HCV RNA
<LLOQ-TND
100 100 100 100 100 100 100 100 100 100 100
• Group A: 1 patient with detectable HCV RNA at PT Week 24: HCV RNA cleared 4 weeks later, sequence not
consistent with relapse
100
15 14 15 15 14 15 15 14 15 15 14 15
93
100 100 100 100 100 100 100 100 100 100 100 100 100
93
HC
V R
NA
< L
LO
Q (%
pa
tie
nts
)
Virologic Response is Maintained at PT Week 24
(GT1a/1b; 24-Week Treatment Groups)
Sulkowski MS et al, Abstract LB-2, AASLD 2012

0
20
40
60
80
100
SVR4
HC
V R
NA
< L
LO
Q
(% p
ati
en
ts)
Week 4
n =
EOT
G: DCV + SOF (12-wk)
H: DCV + SOF + RBV (12-wk)
% of patients
with HCV RNA
<LLOQ-TND
• Group G: 1 patient with missing HCV RNA at PT Week 4—patient achieved SVR12
• Group H: 1 patient with missing HCV RNA at PT Week 4—patient achieved SVR12; 1 patient with HCV RNA < LLOQ-TND at PT week 2 and HCV RNA = 54 IU/mL at PT week 4 (not confirmed)—patient achieved SVR12
100 95 100 100 98 95
78 76 100 100 98 95
41 41 41 41 41 41
Virologic Response During and After Treatment
12 Week Treatment Groups
Sulkowski MS et al, Abstract LB-2, AASLD 2012

LB-3: Daclatasvir (NS5A), Asunaprevir (PI), and
BMS-791325 (non-nuc)
• 32 treatment naïve, G1 patients w/o cirrhosis
• ASV 200 mg BID, DCV 60 mg QD, BMS-791325 75 mg
BID (part 2 with 150 mg BID)
• Patients randomized to 24 vs 12 weeks
• Majority of patients G1a and non-CC
• Most common AEs: headache, diarrhea, asthenia Everson G et al, Abstract LB-3, AASLD 2012

94%**
SV
R(%
)
* One d/c’ed early with HCV RNA<LLOQ
**One lost to follow up
Daclatasvir, Asunaprevir, and
BMS-791325 (non-nuc)
Everson G et al, Abstract LB-3, AASLD 2012
0
20
40
60
80
100
Week 12 (24 week group) SVR4 (12 wk group)
94%*
15/16 15/16
Abstract LB-1: ABT-450/r, ABT-267, ABT-333 +/- RBV in HCV
Genotype 1 Treatment Naïve Patients
• Randomized to treatment for 8, 12, or 24 weeks with:
– ABT-450/r (Protease inhibitor + ritonavir boost) combined with ABT-
267(NS5A inhibitor) +/- ABT-333 (Non-nuc polymerase inhibitor) +/-
Ribavirin
• Patient characteristics:
– Non-cirrhotic
– Genotype 1a = 66%
– IL28B non-CC= >90%
– N=438 naïve
– N=133 prior null responders
Kowdley KV et al, Abstract LB-1, AASLD 2012

0
20
40
60
80
100
Overall G1a G1b
+RBV
-RBV
% S
VR
Treatment Naive
% S
VR
Null Responders +RBV
0
10
20
30
40
50
60
70
80
90
100
Overall G1a G1b
+RBV
77/
79
52/
54
43/
52
25/
25
24/
25
69/
79 42/
45
25/
28
17/
17
97.5%
87.3%
96%
83%
100% 96% 93.3%
89%
100%
Abbott Press Release, Nov. 10, 2012, Kowdley KV et al, Abstract LB-1, AASLD 2012
LB-1: SVR12 Results

Zeuzem S et al, Abstract 232, AASLD 2012; Soriano V et al, Abstract 84, AASLD 2012
• Five arm study that evaluated different doses and durations in regimens
with faldaprevir (PI) and BI207127 (non-nuc) with or without RBV
– Durations: 16, 28 or 40 weeks
– BID vs TID
• Randomization was stratified by genotype (1a vs 1b) and IL28B
– 9% of patients had cirrhosis
• SVR12 ranged between 52% to 69% in RBV-containing arms and 39%
without RBV
– SVR in cirrhotics is 54%
• IL28B CC, genotype 1b and female gender were favorably associated with
SVR12
Abstract 232: Final Results of SOUND-C2 and
Predictors of Response

Sofosbuvir +RBV
Sofosbuvir + RBV
Sofosbuvir +RBV
Sofosbuvir +
RBV
Sofosbuvir +
RBV (800mg/d)
0 12 Weeks 8
Prior Null
GT 1
Naive
GT 1
Experienced
GT 2/3
Naive
GT 2/3
Naive
GT 2/3
SVR12
1/10 (10%)
21/25 (84%)
17/25 (68%)
16/25 (64%)
6/10 (60%)
SVR8
Gilead Press Release, Nov. 10, 2012
• Evaluate sofosbuvir
+RBV as single
agent treatment for
HCV
• Small phase IIb
exploratory study
• Non-cirrhotic
patients
• Well-tolerated
regimen
Abstract 229: Once Daily Sofosbuvir (GS-7977) Plus RBV in
Patients with HCV G1, 2, and 3: The ELECTRON Trial

Press Conference
Q&A

Conclusions
• More patients will be screened, diagnosed and referred
into HCV specialty practices as a result of new
recommendations
• Many of these patients are good candidates for
treatment today
• Treatment outcomes with current treatments can be
optimized with appropriate management/interventions
• The HCV pipeline is promising with potential new
treatment modalities in the near future

We thank… Vertex Pharmaceuticals
for the educational grant to support this activity
Accredited by: Sponsored by:
Presented for attendees of the 63rd AASLD Annual Meeting (or The Liver Meeting®).
This event/function is sponsored by Chronic Liver Disease Foundation and supported by Vertex
Pharmaceuticals.
This is not an official function/event of the American Association for the Study of Liver Diseases.
Supported by:


















