Newsletter_2010-9
17
www.scai.org www.seconds-count.org September/October 2010 The Society for Cardiovascular Angiography and Interventions I nterventionalists hope that patients and physicians will soon have a wider range of choices for the treatment of carotid artery stenosis, following publication of the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST) in the New England Journal of Medicine in late May. The trial found carotid artery stenting (CAS) to be equally safe and effective as carotid endarterectomy (CEA) for prevention of stroke, all-cause death, and myocardial infarction in patients at average surgical risk for CEA. Experts say it has the potential to shift the focus of treatment decisions from which procedure is covered by health insurers to which is best for each patient. “CREST teaches us that for average-risk patients, the patient and physician should be able to choose between carotid stenting and endarterectomy,” said SCAI President-Elect Christopher J. White, M.D., FSCAI, a professor of medicine and system chairman for cardiovascular diseases at The John Ochsner Heart & Vascular Institute in New Orleans. “We now have equipoise. One is not better than the other.” L. Nelson “Nick” Hopkins, III, M.D., who performs both CEA and CAS, agrees. “What’s compelling is that the overall results for stroke, death, and myocardial infarction were incredibly good in both arms of the study,” said Dr. Hopkins, a professor and chairman of neurosurgery and a professor of radiology at State University of New York at Buffalo. “We now have the largest randomized trial ever done comparing carotid stenting and endarterectomy, and it really shows equivalence between these two procedures.” CREST Raises Hopes of Expanded Coverage for Carotid Stenting (continued on page 9) IN THIS ISSUE: An Important Message from SCAI’s President! See page 2 SCAI Committees Revitalized: New Members, New Leaders, New Opportunities Highly calcified, critical right internal carotid artery stenosis (CAS) in an 80-year-old male who had recently experienced a transient ischemic attack. (A) Subtracted, selective right internal carotid artery stenosis prior to angioplasty and stenting using distal embolic protection. (B) After dilation with a 4mm/4cm angioplasty balloon; the distal filter is clearly identified. (C) After the procedure has been completed and the filter removed. (Images courtesy David Jessup, M.D., FSCAI.) A B C K eeping things fresh, building on innovative ideas, seizing exciting opportunities while retaining the expertise and involvement of long-time volunteers. That’s the idea behind this summer’s update of SCAI’s committees. The result is new groups all across the Society’s committee structure, including many new faces, new chairs and co-chairs at the helm of many of the committees, and countless new opportunities for every SCAI member to get involved in their Society. “A membership organization is only as strong as its members,” said SCAI President Larry S. Dean, M.D., FSCAI. “We want to draw on the talents, knowledge, and experience of every single one of our members.” There are new faces throughout SCAI’s almost two dozen committees, each of which typically has a chair, co-chair, and at least nine core committee members. “We looked for members — either newcomers or seasoned committee participants — who would be a good match for each committee,” explained Immediate (continued on page 5)
-
Upload
scai-publications -
Category
Documents
-
view
214 -
download
0
description
IN THIS ISSUE: www.scai.org www.seconds-count.org September/October 2010 September/October 2010 An Important Message from SCAI’s President! See page 2 (continued on page 9) (continued on page 5) The Society for Cardiovascular Angiography and Interventions The Society for Cardiovascular Angiography and InterventionsTheSocietyforCardiovascularAngiographyandInterventions
Transcript of Newsletter_2010-9

www.scai.org www.seconds-count.org September/October 2010
The Society for Cardiovascular Angiography and Interventions
Interventionalists hope that patients and physicians will soon have a wider range of choices for the
treatment of carotid artery stenosis, following publication of the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST) in the New England Journal of Medicine in late May. The trial found carotid artery stenting (CAS) to be equally safe and effective as carotid endarterectomy (CEA) for prevention of stroke, all-cause death, and myocardial infarction in patients at average surgical risk for CEA. Experts say it has the potential to shift the focus of treatment decisions from which procedure is covered by health insurers to which is best for each patient.
“CREST teaches us that for average-risk patients, the patient and physician should be able to choose between carotid stenting and endarterectomy,” said SCAI President-Elect Christopher J. White, M.D., FSCAI, a professor of medicine and system chairman for cardiovascular diseases at The John Ochsner Heart & Vascular Institute in New Orleans. “We now have equipoise. One is not better than the other.”
L. Nelson “Nick” Hopkins, III, M.D., who performs both CEA and CAS, agrees. “What’s compelling is that the overall results for
stroke, death, and myocardial infarction were incredibly good in both arms of the study,” said Dr. Hopkins, a professor and chairman of neurosurgery and a professor of radiology at State University of New York at Buffalo. “We now have the largest randomized trial ever done comparing carotid stenting and endarterectomy, and it really shows equivalence between these two procedures.”
CREST Raises Hopes of Expanded Coverage for Carotid Stenting
(continued on page 9)
September/October 2010
The Society for Cardiovascular Angiography and InterventionsThe Society for Cardiovascular Angiography and Interventions
CREST Raises Hopes of Expanded Coverage for Carotid Stenting
IN THIS ISSUE: An Important Message from
SCAI’s President! See page 2
SCAI Committees Revitalized: New Members, New Leaders, New Opportunities
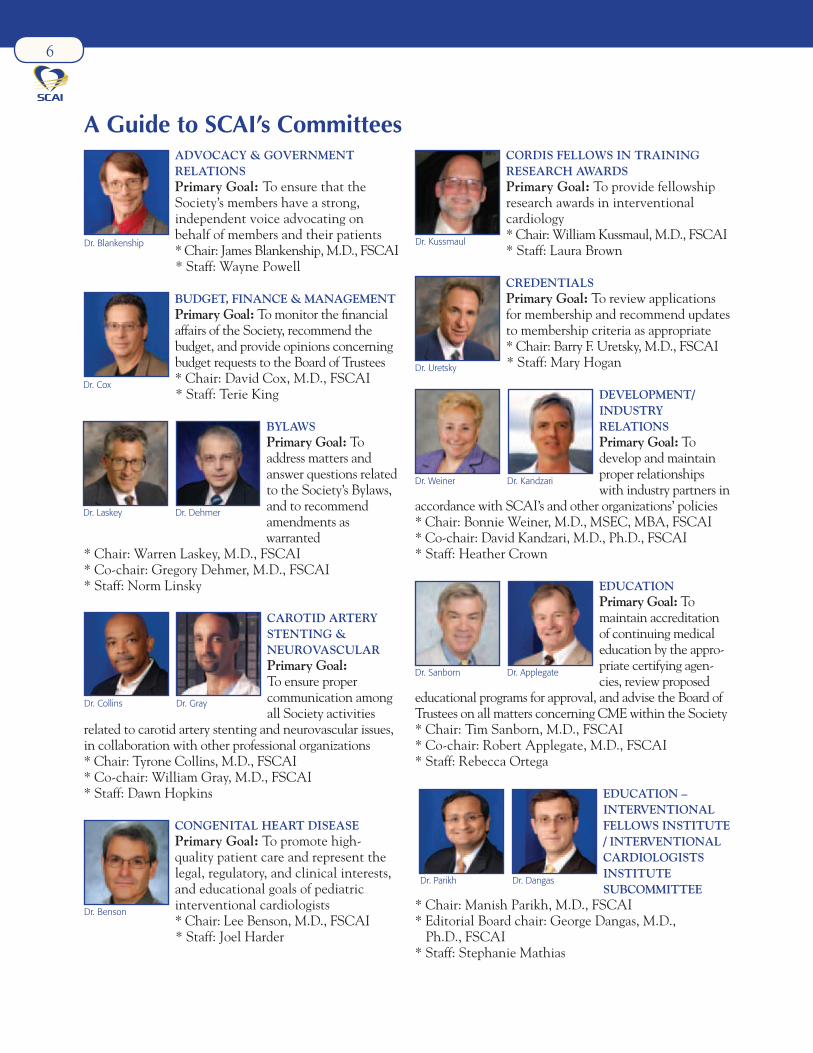
Highly calcifi ed, critical right internal carotid artery stenosis (CAS) in an 80-year-old male who had recently experienced a transient ischemic attack. (A) Subtracted, selective right internal carotid artery stenosis prior to angioplasty and stenting using distal embolic protection. (B) After dilation with a 4mm/4cm angioplasty balloon; the distal fi lter is clearly identifi ed. (C) After the procedure has been completed and the fi lter removed. (Images courtesy David Jessup, M.D., FSCAI.)
A B C
Keeping things fresh, building on innovative ideas, seizing exciting opportunities while retaining the expertise and involvement of long-time volunteers.
That’s the idea behind this summer’s update of SCAI’s committees. The result is new groups all across the Society’s committee structure, including many new faces, new chairs and co-chairs at the helm of many of the committees, and countless new opportunities for every SCAI member to get involved in their Society.
“A membership organization is only as strong as its members,” said SCAI President Larry S. Dean, M.D., FSCAI. “We want to draw on the talents, knowledge, and experience of every single one of our members.”
There are new faces throughout SCAI’s almost two dozen committees, each of which typically has a chair, co-chair, and at least nine core committee members. “We looked for members — either newcomers or seasoned committee participants — who would be a good match for each committee,” explained Immediate
(continued on page 5)

2
Dear Colleagues,As follow-up to my recent message
focused on the developments in Maryland impacting interventional cardiology, I am writing to provide SCAI members with an update on SCAI’s ongoing involvement on the issue.
Allegations by Maryland healthcare legislators pertaining to the possible inappropriate use of coronary stent
placement in patients have been made public. State offi cials are making plans to move forward with legislative action, and journalists have suggested patients have been placed at risk by inappropriate stent placement. The specific cases are under ongoing investigation by Maryland healthcare officials, thus SCAI cannot comment on them.
However, as I noted in my last communication, SCAI is aggressively addressing the challenges these allegations engender. These challenges include potential confusion and mistrust among some patients and their families as to the effectiveness of PCI; inconsistency of the current methods of peer review and a critical need for better methods moving forward; and the need to convince Maryland and other states to obtain accurate, valid outcomes-based data (rather than deeply fl awed cost-based Medicare data) to make conclusions or guide legislation. Given the potential for a ripple-effect beyond Maryland on these issues, SCAI is proactively addressing ways to reassure patients and legislators.
It is more important than ever for us to work to inform policymakers, journalists and, most importantly, Maryland’s citizens about how interventional cardiologists deliver quality, appropriate, guidelines-driven care for thousands of patients with cardiovascular disease. Concurrently, we must demonstrate as a profession full transparency to legislators and an ability to provide a strong peer review process with independent oversight.
This is an opportunity for us to share with the public the standards and processes our profession has established and constantly improves to support delivery of optimal care, and to identify and correct problems either with process or with specifi c healthcare providers.
To be clear, we cannot comment on the interventional cardiologists in question, nor do we defend inappropriate use or overuse in interventional cardiology. The goal and intent of SCAI’s involvement in this issue is consistent with all of our activities: to promote and improve
education and quality standards in interventional cardiology as a means to providing the best in patient care.
Last week, Maryland officials issued a report suggesting “legislative and programmatic changes” that would enhance state agencies’ authority to address any inappropriate use of procedures. Representatives from SCAI, ACC and ACE (Accreditation for Cardiovascular Excellence) met with top Maryland offi cials just two days after the report was issued. The meeting was very positive and encouraging. State representatives indicated a desire to work with our organizations to develop potential solutions for maintaining quality in the state’s hospitals. In fact, the state has recognized our profession’s track record for promoting and improving quality at the professional level. I feel confi dent that we will have a collaborative role in developing standards and processes for appropriate oversight.
Our communications team has also been working closely with Maryland media to balance their ongoing coverage of this local issue. The team has successfully arranged interviews for myself, ACC President Dr. Ralph Brindis and others. We will continue this work to ensure the media and the public are aware of our efforts surrounding quality improvement, including the appropriateness criteria guidelines for PCI, peer-review guidelines and ACE accreditation.
SCAI leadership takes this situation seriously. Our efforts will continue to ensure the voice of quality in our profession is heard by key stakeholders in Maryland and elsewhere. We will continue to keep you informed on our ongoing efforts.
As always, your feedback is appreciated. You can reach me at [email protected]. In addition, I invite you to contact the following SCAI members involved with the Society’s efforts in this regard, at [email protected].
• Dr. Charles Chambers: SCAI PR Committee Chair Dr. Mark Turco: SCAI’s representative on the state committee addressing this issue
• Dr. Bonnie Weiner: ACE chief medical offi cer n
Sincerely,
Larry S. Dean, M.D., FSCAIPresident, SCAI
SCAI Responds to Developments Impacting Interventional Cardiology
Larry S. Dean, M.D., FSCAI
President’s Message

Larry S. Dean, M.D., FSCAI, PresidentChristopher J. White, M.D., FSCAI, President-Elect
Steven R. Bailey, M.D., FSCAI, Immediate Past President J. Jeffrey Marshall, M.D., FSCAI, Vice President
Carl L. Tommaso, M.D., FSCAI, TreasurerTheodore Bass, M.D., FSCAI, Secretary
Morton Kern, M.D., FSCAI, Editor-in-Chief_______________________________________________________________
SCAI News & HighlightsispublishedbyTheSocietyforCardiovascularAngiographyandInterventions
2400NStreet,NW,Suite500,Washington,DC20037Phone800-992-7224;Fax202-689-7224
www.SCAI.org;www.Seconds-Count.org;www.SCAI-WIN.org;[email protected]
TrusteesAlexander Abizaid, M.D., FSCAI
Lee N. Benson, M.D., FSCAIJeffrey Cavendish, M.D., FSCAITyrone J. Collins, M.D., FSCAIAnthony Farah, M.D., FSCAI
Runlin Gao, M.D., FSCAIJames A. Goldstein, M.D., FSCAI
James Hermiller, M.D, FSCAIThomas Jones, M.D., FSCAIUpendra Kaul, M.D., FSCAI
Clifford Kavinsky, M.D., Ph.D., FSCAIAhmed Magdy, M.D., FSCAIRoxana Mehran, M.D., FSCAIIssam D. Moussa, M.D., FSCAI
Kimberly A. Skelding, M.D., FSCAI
Corrado Tamburino, M.D., FSCAI Zoltan G. Turi, M.D., FSCAI
TrusteesforLifeFrank J. Hildner, M.D., FSCAI
William C. Sheldon, M.D., FSCAI
StaffNorm Linsky
Executive DirectorKerry O’Boyle Curtis
Senior Director for Education, Meetings, & Communications
Wayne PowellSenior Director for Advocacy
& Guidelines
Rick HenegarDirector of Meetings
Kathy Boyd David Communications Director
Mary HoganMembership Manager
Terie KingCPA, Director of Finance
& AccountingBea Reyes
Director of Operations
touch three Design and Production
Imaging Zone Printing
ISTANBUL,TURKEYOCTOBER 22-24, 2010
REGISTERNOW!
The Society for CardiovascularAngiography and Interventions www.SCAI.org/GIS
Where the World of INTERVENTIONAL CARDIOLOGY Meets
in collaboration withSCAI GLOBAL INTERVENTIONAL SUMMIT
TURKISHSOCIETY OF CARDIOLOGY
GIS-RegNow-HalfPg.indd 1 6/15/2010 8:45:19 AM

Past President Steven R. Bailey, M.D., FSCAI. “We want to give as many people as possible a chance to share their expertise and their experience as they work to advance the mission of the Society that represents them.”
One example is James Dwyer, M.D., FSCAI, who now chairs the e-SCAI Committee along with co-chair Michael Ragosta, M.D., FSCAI. “SCAI has done a lot for me over the years,” said Dr. Dwyer. “I thought it was just time for me to give something back.”
Dr. Dwyer plans to draw on his background in medical journalism to help SCAI take advantage of new opportunities in social media and other tools. “The electronic world is not the future; it’s now,” he said. The committee hopes to work with the Seconds-Count.org Editorial Board to expand the resources available on the patient education site, explore applications for the smart phones, and find ways to get information out quickly to physicians, the public, and the media when controversies arise.
For Lee Benson, M.D., FSCAI, chair of the Congenital Heart Disease Committee, one goal is to get as many pediatric/adult congenital interventional cardiologists participating in the committee as possible. Achieving that goal, he said, will help the committee achieve its other goals of enhancing the group’s website, establishing a Listserv, and developing a “home” within the committee for those interventional cardiologists who care for patients with congenital heart disease.
In other cases, such as the Transradial Committee, the committee itself is new. “People interested in the transradial approach have come together in subcommittees of other committees off and on for many years,” said Kimberly A. Skelding, M.D., FSCAI, who is chairing the committee alongside co-chair Samir Pancholy, M.D., FSCAI. “We decided to formalize it and try to get all the experts in the field in one place so we can have a unified effort.”
On the Transradial Working Group’s agenda are a white paper and continuing education initiatives aimed at both fellows just learning the approach and those who want to enhance their existing skills. The group’s ultimate goal is to make the transradial approach as common in the United States as it is abroad.
Another transformed committee focuses on quality
improvement (QI). “It’s important to support the organization that represents what we do,” explained Chair Steven Yakubov, M.D, FSCAI, who has teamed up with co-chairs Matthew Price, M.D., FSCAI, and H. Vernon Anderson, M.D., FSCAI, to launch a series of initiatives in continuous quality improvement. “This is our opportunity to improve the way practice is done and
to have our voice heard, both in the clinical community and in the political community.”
Among other things, the QI Committee plans to develop ways for catheterization labs to implement quality measures that can be shared from program to program, said Dr. Yakubov. “The end goal is always enhanced patient safety.”
“Whether you’ve never been directly involved in the Society’s committees, or have been volunteering for decades, there are opportunities for you to help,” stressed Dr. Dean. He urges every SCAI member to peruse SCAI’s Guide to the Committees on pages 6–9 of this newsletter.
“Based on interests expressed by members as well as our knowledge of individuals’ backgrounds and interests, we’ve invited a number of members to serve as chairs, co-chairs, or voting members of each committee,” said Dr. Bailey. “These members have the important charge of keeping the committees focused and moving forward.”
Drs. Dean and Bailey are both quick to remind members of SCAI’s unique open-door policy for most committees. “You don’t have to have an appointment to be actively engaged in the committees of your choice,” stressed Dr. Bailey. “All SCAI members in good standing are encouraged to attend meetings of just about every committee. And every committee welcomes input, whether you want to devote yourself to an existing project or have an idea for a brand-new one.”
The common consensus of the committee chairs and co-chairs new to SCAI and not-so-new is that everyone has a lot more to contribute than they may realize. After taking a look at SCAI’s Guide to the Committees in this newsletter, send an email expressing your interests to [email protected]. Before you know it, you’ll be connected with the best people to get you started. n
Committees (cont’d from pg 1)
“Whether you’ve never been directly involved in the Society’s committees, or have been volunteering for decades, there are opportunities for you to help.” — Larry S. Dean, M.D., FSCAI
5
6
ADVOCACY & GOVERNMENT RELATIONSPrimary Goal: To ensure that the Society’s members have a strong, independent voice advocating on behalf of members and their patients* Chair: James Blankenship, M.D., FSCAI
* Staff: Wayne Powell
BUDGET, FINANCE & MANAGEMENTPrimary Goal: To monitor the financial affairs of the Society, recommend the budget, and provide opinions concerning budget requests to the Board of Trustees * Chair: David Cox, M.D., FSCAI * Staff: Terie King
BYLAWSPrimary Goal: To address matters and answer questions related to the Society’s Bylaws, and to recommend amendments as
warranted* Chair: Warren Laskey, M.D., FSCAI* Co-chair: Gregory Dehmer, M.D., FSCAI* Staff: Norm Linsky
CAROTID ARTERY STENTING & NEUROVASCULARPrimary Goal: To ensure proper communication among all Society activities
related to carotid artery stenting and neurovascular issues, in collaboration with other professional organizations* Chair: Tyrone Collins, M.D., FSCAI* Co-chair: William Gray, M.D., FSCAI* Staff: Dawn Hopkins
CONGENITAL HEART DISEASEPrimary Goal: To promote high-quality patient care and represent the legal, regulatory, and clinical interests, and educational goals of pediatric interventional cardiologists* Chair: Lee Benson, M.D., FSCAI
* Staff: Joel Harder
CORDIS FELLOWS IN TRAINING RESEARCH AWARDSPrimary Goal: To provide fellowship research awards in interventional cardiology* Chair: William Kussmaul, M.D., FSCAI* Staff: Laura Brown
CREDENTIALSPrimary Goal: To review applications for membership and recommend updates to membership criteria as appropriate* Chair: Barry F. Uretsky, M.D., FSCAI * Staff: Mary Hogan
DEVELOPMENT/INDUSTRY RELATIONSPrimary Goal: To develop and maintain proper relationships with industry partners in
accordance with SCAI’s and other organizations’ policies* Chair: Bonnie Weiner, M.D., MSEC, MBA, FSCAI* Co-chair: David Kandzari, M.D., Ph.D., FSCAI* Staff: Heather Crown
EDUCATIONPrimary Goal: To maintain accreditation of continuing medical education by the appro-priate certifying agen-cies, review proposed
educational programs for approval, and advise the Board of Trustees on all matters concerning CME within the Society* Chair: Tim Sanborn, M.D., FSCAI* Co-chair: Robert Applegate, M.D., FSCAI* Staff: Rebecca Ortega
EDUCATION – INTERVENTIONAL FELLOWS INSTITUTE / INTERVENTIONAL CARDIOLOGISTS INSTITUTE SUBCOMMITTEE
* Chair: Manish Parikh, M.D., FSCAI* Editorial Board chair: George Dangas, M.D., Ph.D., FSCAI* Staff: Stephanie Mathias
A Guide to SCAI’s Committees
Dr. Blankenship
Dr. Cox
Dr. Laskey Dr. Dehmer
Dr. Collins Dr. Gray
Dr. Benson
Dr. Kussmaul
Dr. Uretsky
Dr. Weiner Dr. Kandzari
Dr. Sanborn Dr. Applegate
Dr. Parikh Dr. Dangas

EMERGING LEADERSHIP MENTORINGPrimary Goal: To foster comprehensive mentoring relationships between senior interventionalists and future leaders* Chair: Srihari S. Naidu, M.D., FSCAI* Staff: Laura Brown
eSCAIPrimary Goal: To assist the Society in applying the latest information technologies to the Society’s many educational programs and
to ensure the Society’s web-based offerings fully meet the needs of members and other audiences* Chair: James Dwyer, M.D., FSCAI* Co-chair: Michael Ragosta, M.D., FSCAI* Staff: Eric Grammer
ETHICSPrimary Goal: To develop, update, and oversee enforcement of the Society’s code of ethics and related policies
* Chair: Joseph Babb, M.D., FSCAI* Co-chair: Warren Laskey, M.D., FSCAI* Staff: Norm Linsky
INTERNATIONAL PROGRAMS & MEMBERSHIP
Primary Goal: To develop and foster SCAI’s close, productive, and respectful partnerships with interventional organizations and working groups worldwide on issues in interventional cardiology of global interest, including, but not limited to, professional education, guidelines, and leadership* Chair: Theodore Bass, M.D., FSCAI* Co-chairs: Ashok Seth, M.D., FSCAI, and Ziyad M. Hijazi, M.D., MPH, FSCAI* Staff: Stephanie Mathias
INTERVENTIONAL CAREER DEVELOPMENTPrimary Goal: To provide resources and a forum for early-career in-terventionalists in order
to assist them during the formative stages of their careers* Chair: Paul Sorajja, M.D., FSCAI* Co-chair: Paul McMullan, M.D., FSCAI* Staff: Laura Brown
INTERVENTIONAL FELLOWS-IN-TRAINING GRANT PROGRAMPrimary Goal: To solicit training grant applications from U.S.
ACGME-accredited interventional cardiology programs; review applications in an impartial, fair manner; and set up mechanisms to receive and review reports about proper use of the resulting grants* Chair: Joseph Babb, M.D., FSCAI* Co-chair: Barry F. Uretsky, M.D., FSCAI* Staff: Laura Brown
INTERVENTIONAL TRAINING STANDARDS & DIRECTORS
Primary Goal: To develop and update relevant training standards and to provide a forum for training directors to share information and communication regarding training programs issues, policies and practices* Chair: Tarek Helmy, M.D., FSCAI* Co-chairs: Michael Lim, M.D., FSCAI, and John P. Reilly, M.D., FSCAI* Staff: Sheila Agyman
KNOW WHAT COUNTS SUBCOMMITTEEPrimary Goal: To develop regional education/awareness programs for patients, healthcare providers, and policymakers, and to encourage dialogue about topics affecting optimal
cardiovascular care and outcomes* Chair: Anthony Farah, M.D., FSCAI* Staff: Kathy Boyd David
7
(continued on page 8)
Dr. Dwyer Dr. Ragosta
Dr. Babb Dr. Laskey
Dr. Bass Dr. Seth Dr. Hijazi
Dr. Helmy Dr. Lim Dr. Reilly
Dr. Babb Dr. Uretsky
Dr. SorajjaDr. Naidu Dr. McMullan
Dr. Farah

8
SCAI Committees (cont’d from pg 7)
LAB SURVEYPrimary Goal: To serve as a resource for physicians and administrators, provid-ing comprehensive, independent outside review services for cardiac catheterization laboratories regarding all aspects of labo-ratory function, including facilities, equip-
ment, personnel, policies, procedures, and quality assurance* Chair: Charles Chambers, M.D., FSCAI* Staff: Laura Brown
MULTISPECIALTY OCCUPATIONAL HEALTH GROUPPrimary Goal: In coordination with other societies, to develop recommen-dations for the reduction of occupa-tional safety risks in the cath lab* Chair: James Goldstein, M.D., FSCAI
* Staff: Wayne Powell
NOMINATINGPrimary Goal: To prepare lists of nominees for consideration to become Trustees and Offi cers of the Society
* Chair: Ziyad M. Hijazi, M.D., MPH, FSCAI* Co-chair: Steven R. Bailey, M.D., FSCAI* Staff: Norm Linsky
PERIPHERAL VASCULAR DISEASEPrimary Goal: To ensure proper communi-cation among all Society activities related to pe-ripheral vascular disease,
in collaboration with other professional organizations* Chair: Bruce Gray, D.O., FSCAI* Co-chair: Michael Jaff, D.O.* Staff: Dawn Hopkins
PROGRAMPrimary Goal: To plan the scientifi c program for the SCAI Annual Scientifi c Sessions and present these plans to the Board of Trustees, and to maintain docu-mentation for continu-ing medical education* Co-chairs (adult program): Christopher J. White, M.D.,
FSCAI, and James Hermiller, M.D., FSCAI* Co-chairs (pediatric): Frank Ing, M.D., FSCAI, and Daniel Levi, M.D., FSCAI* Staff: Rick Henegar and Kerry Curtis
PUBLIC RELATIONSPrimary Goal: To inform and educate media, the public, and non-interventional healthcare providers about the important
role of invasive/interventional cardiology in optimal cardiovascular care and outcomes; and to expand SCAI’s visibility and credibility among these audiences * Chair: Charles Chambers, M.D., FSCAI* Co-chair: John P. Reilly, M.D., FSCAI* Staff: Kathy Boyd David
PUBLICATIONSPrimary Goal: To promote optimal patient care through educational, policy, and clinical/scientifi c docu-ments that refl ect the
current state-of-the-science in interventional cardiology* Chair: Issam Moussa, M.D., FSCAI* Co-chair: Charanjit S. Rihal, M.D., FSCAI* Staff: Joel Harder
Dr. Hijazi Dr. Bailey
Dr. Gray Dr. Jaff
Dr. White Dr. Hermiller
Dr. Ing Dr. Levi
Dr. Chambers Dr. Reilly
Dr. Moussa Dr. Rihal
Dr. Chambers
Dr. Goldstein

9
QUALITY IMPROVEMENT
Primary Goal: To provide guidance and recommendations for development of the Society’s policies and positions related to healthcare quality improvement initiatives, with emphasis on quality measures, public reporting of quality measures, pay-for-performance initiatives, interventional cardiology standards development, and radiation issues* Chair: Steven Yakubov, M.D., FSCAI* Co-chairs: Matthew Price, M.D., FSCAI, and H. Vernon Anderson, M.D., FSCAI* Staff: Joel Harder
SECONDS-COUNT.ORG EDITORIAL BOARDPrimary Goal: To develop SCAI’s patient/public education website into the preeminent online resource for
cardiovascular patients, their families, and the public* Chair: Mark A. Turco, M.D., FSCAI* Co-chair: Dennis Kim, M.D., Ph.D., FSCAI* Staff: Kathy Boyd David
SIMULATIONPrimary Goal: To partner with other interested societies in developing standards for applying medical simulation technology to professional education programs of the highest quality and relevance
* Chair: John Messenger, M.D., FSCAI* Staff: Georgina Lopez-Cruz
STRUCTURAL HEART DISEASE COUNCIL
Primary Goal: To provide a forum for structural heart disease specialists to collaborate on issues facing cardiovascular specialists who treat structural heart disease so that patients receive optimal care * Chairs: Ziyad M. Hijazi, M.D., MPH, FSCAI, and Ted Feldman, M.D., FSCAI* Co-chair: Carlos Ruiz, M.D., Ph.D., FSCAI* Staff: Joel Harder
TRANSRADIAL WORKING GROUP* Chair: Kimberly A. Skelding, M.D., FSCAI* Co-chair: Samir Pancholy, M.D., FSCAI* Staff: Georgina Lopez-
Cruz
WOMEN IN INNOVATIONS
Primary Goal: To foster professional development, education, collaboration, and research by and on behalf of women in interventional cardiology and their patients* Chair: Roxana Mehran, M.D., FSCAI* Co-chairs: Bonnie Weiner, M.D., MSEC, MBA, FSCAI, and Alaide Chieffo, M.D., FSCAI* Staff: Rebecca Ortega n
Advocates hope that CREST will not only cement the role of CAS in the treatment of average-risk patients, but also prompt health insurers to ease restrictive coverage policies in patients at high surgical risk. For that to happen, the CREST data will have to convince policymakers at the Centers for Medicare and Medicaid Services (CMS) to reconsider a recent ruling.
In September 2009, CMS declined to expand coverage for CAS in high-risk patients even after release of what many consider compelling data on CAS in over 8,000 patients from three large registries. Instead the federal
agency affirmed its restriction of Medicare coverage to patients at high risk for CEA who have symptomatic carotid artery stenosis of more than 70 percent, provided the procedure is performed using an embolic protection device and stents approved by the Food and Drug Administration. In high-risk patients with a symptomatic stenosis between 50 and 70 percent, and in those who are asymptomatic but have a significant stenosis, CAS is covered only if performed as part of a clinical trial.
Existing rules put many patients in a bind. “I have Medicare patients in my clinic every week who have to choose between
Carotid Stenting (cont’d from pg 1)
(continued on page 10)
Dr. Yakubov Dr. Price Dr. Anderson
Dr. Turco Dr. Kim
Dr. Messenger
Dr. Hijazi Dr. Feldman Dr. Ruiz
Dr. Mehran Dr. Weiner Dr. Chieffo
Dr. Skelding Dr. Pancholy

1010
paying out of pocket for carotid artery stenting or having surgery,” Dr. White said. “They don’t want the risk or morbidity of surgery but they don’t qualify for a clinical trial, so Medicare won’t pay. They’re afraid they’re going to have a stroke if they can’t have a stent. It’s brutal. It’s not the way we should be treating Medicare patients.”
In CREST, investigators recruited just over 2,500 patients with symptomatic and asymptomatic moderate-to-severe carotid artery stenosis. Patients were randomly assigned to CEA or CAS and followed-up for a median of 2.5 years. The study found no signifi cant difference between the two procedures in the estimated 4-year combined rate of stroke, myocardial infarction, or death from any cause (7.2 percent for CAS and 6.8 percent for CEA). Peri-procedural rates of myocardial infarction were lower with CAS, while minor rates of stroke were higher. When major (disabling) strokes were considered, there was no difference between surgery and stenting.
The CREST results are in contrast to those of three recent European trials—and therein lies a valuable lesson about physician training and experience, observers say. The Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis (EVA-3S) found surgery to be superior to stenting. The Stent-Supported Percutaneous Angioplasty of the Carotid Artery versus Endarterectomy (SPACE) study could not prove the non-inferiority of stenting, although there was no difference in 30-day stroke and death rates. The International Carotid Stenting Study (ICSS) found more minor strokes with stenting than for surgery, although the primary endpoint of the trial, major stroke and death, was not different between CEA and CAS.
But there’s more to the data than meets the eye. The key to good results with procedures such as CEA and CAS is operator experience and training, Dr. White said. “In their urgency to rapidly enroll patients, the European trials appeared to cut some corners and allowed very inexperienced CAS operators to enroll patients in a randomized clinical trial, while the surgeons were experienced
in CEA. Allowing CAS operators who required proctoring to enroll patients and perform CAS seems to have placed stenting at a disadvantage.”
Dr. White pointed out that in ICSS, two inexperienced CAS sites were responsible for fi ve major strokes in 11 treated patients, accounting for one-third of all the major stroke complications.
By comparison, credentialing requirements for operators performing CAS were much more rigorous in CREST. The trial featured a lead-in phase that enabled all operators to develop and demonstrate a high level of skill before being allowed to perform CAS in the main trial. None of the European trials had a lead-in phase
to ensure that inexperienced sites could perform the procedure as well as more experienced sites. And SPACE investigators recently published data showing that their most inexperienced CAS sites produced significantly worse results than experienced CAS sites.
“Experience is very, very important in any technology, but especially when you’re dealing with the carotid artery and there’s a risk of stroke,” Dr. Hopkins said.
Over the years, interventionalists have also learned which patients are good candidates for CAS, and which are not. Contraindications to CAS include severe peri-lesional tortuosity, calcifi ed lesions, and a complex aortic arch (Type III arch). Over the last decade, the numbers of patients undergoing CEA at SUNY Buffalo has plummeted, Dr. Hopkins said, but recently surgery is making a comeback as his team becomes more selective about which patients should have CAS.
“In our weekly conferences, we’re always looking at the aortic arch and lesion morphology,” Dr. Hopkins said. “The question isn’t, ‘Can we stent this?’—we can stent almost anything—it’s ‘Should we stent this?’ If the patient needs the artery fi xed, which is the best operation, stent or surgery, for this particular patient?”
CREST and other studies have also raised a red flag about patient age as a selection criterion. In CREST, patients under the age of 70 did better with CAS than surgery, whereas those 70 and older did better with surgery. However, since older patients tend to have more atherosclerotic disease, more tortuous vessels, and greater arch complexity, the key may lie in careful patient selection, rather than a restriction on the age of patients who undergo carotid stenting.
“Age drops out as a meaningful criterion if patient selection is adequate,” Dr. Hopkins said. “A 90-year-old with good anatomy can be a perfectly good candidate for carotid artery stenting.”
There have been several large series of elderly patients who have had excellent results with CAS when treated by experienced operators who carefully selected their patients, Dr. White noted.
As CMS and private health insurers mull the CREST results, interventionalists hope a decision favoring expanded reimbursement for CAS will be announced by year’s end. In the meantime, new CAS results using proximal embolic protection devices suggest the safety of CAS continues to improve, with 30-day combined rates of stroke and death in neighborhood of 3 percent for symptomatic patients and less than 1 percent for asymptomatic patients.
“Proximal protection devices have the potential to drive complication rates to historically low levels that not even surgery can achieve,” Dr. White said. “It’s a very exciting development.” n
Carotid Stenting (cont’d from pg 9)
Christopher J. White, M.D., FSCAI
L. Nelson Hopkins, III, M.D.

11
This summer, SCAI leaders traveled to Capitol Hill, where they visited more than a dozen elected officials and delivered important messages about
legislative efforts that have the potential to limit the ability of interventional cardiologists to deliver high-quality specialty care to patients. The goal was to provide legislators insights from the front lines of interventional cardiology about how current legislation could directly affect the treatment of Medicare patients, unfairly penalize interventional cardiologists for patient hospital readmissions, and put Medicare reimbursement decisions in the hands of appointees.
SCAI President Larry S. Dean, M.D., FSCAI, SCAI President-Elect Christopher J. White, M.D., FSCAI, and Immediate Past Advocacy Committee Chairs Joseph D. Babb, M.D., FSCAI, and Mark A. Turco, M.D., FSCAI, went to Washington, DC, as part of an event organized by the Alliance of Specialty Medicine, a non-partisan advocacy group of which SCAI is a member. The Alliance, which focuses on the development of federal healthcare policy for specialty medicine associations, brought in over 50 specialty physicians from around the United States to talk with their elected representatives about the realities of specialty medicine practice and the potential effects of legislation on patient care.
“It was an opportunity for us to have face time with the elected representatives to discuss the issues that are of great concern—not all the issues, but some of the major concerns of our membership,” said Dr. Dean.
“While the legislators in general were somewhat noncommittal in the run-up to the November elections, the overall reception was positive and the Representatives seemed willing to reconsider legislative positions based on new information,” said Dr. Babb.
“Frankly, I felt good about how we were received,” said Dr. White. “I kept reminding myself that these were professionals whose job is to listen. But we were not talking to a wall. When talking to them, it was clear every single one of them understood what we were saying.”
The two-day event began with a crash course in healthcare issues of central importance to specialty medicine. Speakers included Dr. Mark McClellan, former head of the Centers for Medicare and Medicaid Services and the Food and Drug Administration; Dr. Robert Berenson, the current Vice-Chair of the Medicare Payment Advisory Commission; and patient advocate and former
House majority whip Tony Coelho. Several Congressional members also addressed the group, including Senators John McCain (R-AZ) and Tom Coburn, MD (R-OK) and Congressional Representatives Pete Stark (D-CA-13), Phil Roe, MD (R-TN-1), and Zack Space (D-OH-18).
The first day was also a day of honing the key issues each participating physician would deliver to the Congressional members from his or her own state. SCAI’s expert advocacy staff facilitated the interviews and prepared SCAI leaders for maximal effectiveness once in those interviews. Drs. Dean, White, Babb, and Turco spoke with more than 15 legislators and legislative staff.
The emphasis for SCAI leaders was on making sure that interventional cardiologists not be legislated out of practicing medicine for the best benefit of patients. “It wasn’t an effort to say that primary care isn’t important, but rather that specialty care is just as important,” explained Dr. Babb.
Battling the SGR“At the time we were there, the biggest issue was the
sustainable growth rate formula,” said Dr. Dean. “The SGR formula is long outdated, and everyone we talked to agreed it should be changed.”
On June 24, Congress passed an act as a stopgap measure that was retroactive to June 1. This act prevents the SGR from taking effect for six months, reverses the planned 21 percent fee cut, and boosts fees by 2.2 percent.
SCAI is pleased to have this fix, but the bigger problem remains, as it has since 1998, when the SGR was enacted, said Dr. Babb. “Each year, advocacy groups, including SCAI, convince Congress that implementing the cuts will have damaging effects for patients and physicians. Congress has often applied temporary fixes, but it has never
Advocacy & Guidelines
SCAI Leaders Voice Concerns of Interventional Cardiologists on Capitol Hill
(continued on page 12)
SCAI leaders joined the Alliance of Specialty Medicine for meetings on Capitol Hill.

12
addressed the long-term need for a formula that works,” he explained.
Fighting the IPABSCAI members also pushed legislators to repeal
the Independent Payment Advisory Board (IPAB), a provision in the healthcare reform law that will make reimbursement decisions the purview of an independent board, not Congress.
“If the IPAB is not repealed, these appointed officials will be looking at what is appropriate to be reimbursed and what is not,” said Dr. Dean. “Although Congress will have a small degree of oversight, it is going to be very difficult to overturn any decisions made by this independent board.”
Improving Quality Metrics, Including ReadmissionsThe third key message delivered as part of the Alliance
“fly-in” was that the newly enacted quality improvement provisions of the reform law could measure the wrong things and unfairly penalize skilled interventional cardiologists.
“We expressed our serious concern about the quality metrics, namely that they’ve picked things they can measure, but they haven’t picked things that will make things better,” said Dr. White.
As the legislation currently reads, an interventional cardiologist could be financially penalized for patient hospital readmissions within 30 days of an interventional procedure. The data collected would not distinguish between a patient readmitted for cardiovascular complications and one who is admitted, for example, for a twisted knee. Dr. Babb used the example of the twisted knee in his visits with legislators.
“With every person we visited, you could see the light of understanding in their eyes…I think they all got that. I think focusing on the knee example was helpful. I think they were enlightened by that simple kind of real-life example,” said Dr. Babb.
For more information on SCAI’s advocacy efforts, and how you can participate, visit www.SCAI.org, or email [email protected]. n
This month SCAI published a first-of-its-kind core curriculum consensus document for the treatment of structural heart disease. An introduction to SCAI’s
Structural Heart Disease Council, structural heart disease core curriculum, and results of a survey of physicians and training directors on structural heart disease procedures were published simultaneously in Catheterization and Cardiovascular Interventions and JACC Cardiovascular Interventions.
The structural heart disease core curriculum, endorsed by the American College of Cardiology Foundation and written by interventional specialists from multiple regions, defines training and credentialing requirements along with program standards for practitioners who perform interventional structural heart disease procedures. The evolution of interventional treatments for structural and congenital heart disease has occurred rapidly during the past 10 years, and interventional therapies are increasingly helping patients who previously had to undergo open-heart surgery, or who could not be treated at all. With such rapid advancement, SCAI identified a need – confirmed by the survey results – for uniformity across structural heart disease training programs as well as specific credentials and standards for practitioners who treat structural heart disease with interventional techniques. Currently, a lack of comprehensive training programs prohibits many practitioners from treating structural heart disease, according to the SCAI survey of 107 U.S.-based interventional cardiologists.
“The primary goal of the core curriculum is to provide patients with the highest level of care and treatment available,” said Carlos Ruiz, M.D., Ph.D., FSCAI, professor of pediatrics and medicine and director of the Division of Congenital and Structural Heart Disease at Lenox Hill Heart and Vascular Institute of New York, and lead author of the core curriculum. “The core curriculum will serve training centers and practitioners dedicated to growing their knowledge and skill base for structural heart disease interventions and provide a forum to discuss the latest treatment advancements for structural heart disease to advance and improve patient care.”
The core curriculum outlines specific training recommendations and skill requirements for certification as a structural heart disease practitioner, including:• Superb basic catheterization skills with the ability to
achieve unusual types of vascular access and manipulate various catheters, balloons and other devices
• The ability to competently handle potential complications resulting from interventional treatment
• A knowledge base and interventional skills for a variety of complex structural heart diseases, including appropriate device selection, imaging needs, stenting techniques, managing complications and acute and long-term post-procedural care
SCAI Publishes Structural Heart Disease Core Curriculum — Defining Training Requirements, Program Standards
Carlos Ruiz, M.D., Ph.D., FSCAI
Capitol Hill (cont’d from pg 11)

13
In October, SCAI will release Peripheral Vascular Disease Online, the newest addition to the Society’s menu of online educational offerings.
Feedback from SCAI’s membership has consistently ranked educational opportunities in peripheral vascular disease as a primary interest. This program will ensure interventional cardiologists have access to current information on this challenging area of medicine.
Under the leadership of Course Director and SCAI President-Elect Christopher J. White, M.D., FSCAI, Peripheral Vascular Disease Online will feature online lectures prepared by one of the most renowned leaders in the field.
“The course is designed for all physicians, regardless of their background in PVD,” said Dr. White. “By providing information on basic as well as advanced aspects of PVD, we are able to offer a course that is just as useful to experts as it is to physicians just getting into this area.”
Ideal for physicians interested in learning the background, potential complications, and treatment options for peripheral vascular disease, Peripheral Vascular Disease Online will feature 13 modules that operate as
“As s t ructural heart d i sease procedures advance and become increasingly common, it is essential that practitioners acquire the right set of skills and knowledge base,” sa id SCAI Past Pres ident Ted Feldman, M.D., FSCAI, director of cardiac catheterization at Evanston Northwestern Healthcare in Evanston, IL, and chair of the Structural Heart
Disease Council. “Patient care will benefit from those who acquire the skills and training outlined in the core curriculum document.”
Additionally, specific guidelines for adequate structural heart disease training centers include:• A structural heart center composed of integrated and
dedicated faculty members from various specialties, including anesthesiology, pediatrics, surgery and radiology, among others
• Staff and faculty dedicated to mentorship • Sufficient patient volume with a variety of patient
case levels• Hybrid procedure rooms, sophisticated imaging
equipment and simulation technology• Formal didactic sessions, ongoing mentorship
opportunities, weekly medical-surgical structural
heart disease conferences, inpatient and outpatient consultation services and clinical follow-up“SCAI is dedicated to advancing
the treatment of structural heart disease and providing our patients with the best treatments and technologies available to treat their disease,” said SCAI Past President Ziyad M. Hijazi, M.D., MPH, FSCAI, director of Congenital and Structural Heart Disease, Rush University Medical Center, co-author of the core curriculum, and chair of the Structural Heart Disease Council. “It was critical for SCAI to take the lead to define this core set of program and credentialing standards for practitioners as a way to ultimately provide better and more standardized care to our patients.”
Moving forward, SCAI’s Structural Heart Disease Council will work to increase awareness of structural heart disease therapies as treatment options while advocating for patients’ improved access to interventional therapies. The Council also hopes to increase the opportunities for mentorship and career advancement in structural heart disease–related fields, and partner with organizations that promote the use of interventional structural heart disease therapies.
To view the full survey results, visit www.SCAI.org or contact Joel Harder at [email protected] n
Ted Feldman, M.D., FSCAI
Ziyad M. Hijazi, M.D., MPH, FSCAI
SCAI to Launch Online Course on Peripheral Vascular Disease
(continued on page 14)
Education

14
an online textbook of information. Each module will include a slide presentation as well as a full narration by the author. Navigating through presentations will be easy due to several key features, including expanded search capabilities that will allow physicians to search for key terms and phrases within the text and audio to quickly target information. And, because the full curriculum will operate on a Flash system, users will experience fast load-times on high-speed Internet connections.
“Providing this information in an online course format is ideal,” added Dr. White. “All of this information is available 24 hours a day, seven days a week, so physicians can fit in a module on their own schedule.”
The curriculum covers a wide breadth of topics covering all aspects of PVD, including:
• Acute Limb Ischemia• Critical Limb Ischemia• Claudication• Aorto-Iliac Intervention• Femoro-Popliteal Intervention• Below-Knee Intervention• Abdominal Aortic Aneurysm• Chronic Mesenteric Artery Ischemia• Renal Artery Stenosis• Innominate and Subclavian Artery Stenosis• Vertebral Artery Stenosis• Carotid Artery Stenosis• Deep Venous Thrombosis/ PE• Dialysis Access• Intracranial Artery Stenosis
“Physicians have questions about every area of PVD, and we kept that fact in mind while designing this curriculum,” explained Dr. White. “The topics covered will provide an excellent overview of the basics, but the course also tackles some of the more complicated issues. This kind of versatile curriculum will appeal to every physician who is looking for education on PVD.”
While practicing physicians will find Peripheral Vascular Disease Online useful for both continued education and review, fellows-in-training will also reap the benefits of this resource. “Fellows-in-training have specifically requested access to PVD education, and we hope this course will become a great resource for training programs as well as individuals,” said Dr. White.
Expansions of the course are already planned, including the addition of assessment questions that will allow physicians to test their knowledge after reviewing a module. SCAI plans to provide CME credit for the program starting in 2011.
Peripheral Vascular Disease Online will be available to SCAI members for $495, a $100 discount from the $595 fee for non-members. Fellows-in-training will have access to the course for $200. Beginning in October, the course will be available at www.scai.org/pvdonline.
Peripheral Vascular Disease Online is provided through an educational grant provided by Cook Medical. For more information about the course or to register, contact SCAI’s online education manager, Stephanie Mathias, at [email protected] or 800-922-7224. n
Peripheral Vascular Disease Online (cont’d from pg 13)
As a result of the growing partnership
between SCAI and the community-based patient support group Mended Hearts , i n t e r v e n t i o n a l cardiologists now have a new resource for helping many of their patients. Life After the Cath Lab: A Guide to Recovery, a packet of information
that explains cardiac catheterization procedures and answers questions about recovery and secondary prevention. The materials were unveiled this May, at the Mended Hearts
annual meeting during a special session aimed at dramatically expanding the Cath Patient Outreach Program.
Through the Cath Patient Outreach Program, Mended Hearts’ trained and accredited volunteers visit new cardiac catheterization patients and their families to offer support, reassurance, and insights from their own experiences as heart disease survivors. Mended Hearts volunteers have been providing the same service to bypass patients since the 1950s, but until recently only a few of Mended Hearts’ many chapters have ventured into cath lab waiting rooms.
Life After the Cath Lab: A Guide to Recovery was developed by Mended Hearts, with input from SCAI, so the volunteer-visitors would have an information-packed “leave-behind” to place in the hands of patients who may have just learned they have cardiovascular disease. A Spanish version will be available in the fall. Both the English and Spanish versions were made possible as a result of educational grant support from AstraZeneca.
Mended Hearts and SCAI Unveil New Patient Education Resource
One of several helpful brochures inside the Life After the Cath Lab patient education packets

15
SCAI mailed one copy of Life After the Cath Lab: A Guide to Recovery to each member practicing in North America. The goal was to make members more aware of the Cath Patient Outreach Program and how they can support Mended Hearts visiting in their hospitals: 1. Start by visiting www.mendedhearts.org to see if
there’s a Mended Hearts chapter in your area. If there is, contact the chapter president or visiting chairperson to see about setting up a cath lab visiting program at your hospital.
2. Spread the word among your cath lab colleagues and staff about the value of this program.
3. Urge your patients and their families to attend Mended Hearts chapter meetings. “Interventional cardiologists should welcome this
opportunity with open arms,” says J. Jeffrey Marshall, M.D., FSCAI, who has worked with the Mended Hearts chapter at the Northeast Georgia Heart Center to support cath patient visits. “This is a great opportunity for our patients to be educated by somebody who has actually had these procedures and been highly trained to communicate educational objectives. Working with Mended Hearts volunteers has become part of my practice.”
For more information, read the SCAI News & Highlights article announcing the partnership at www.scai.org/mendedhearts or visit www.mendedhearts.org. n
J. Jeffrey Marshall, M.D., FSCAI
A panel of expert cardiologists at this year’s SCAI Scientific Sessions shared their insights
on the challenges and tough questions facing early-career interventional cardiologists, especially in light of today’s uncertain healthcare environment. Hosted by SCAI’s Interventional Career Development Committee (ICDC), this year’s “Early-Career Sessions” featured a
morning of talks on topics such as finding the best career opportunities, the economics of practice, and recognizing opportunities for continued growth and development in the field.
Finding a Good Fit“For many new interventional cardiologists, finding
the right job is more daunting than the challenges of fellowship training,” said panelist Peter L. Duffy, M.D., MMM, FSCAI.
“Take some time to organize your thoughts,” he advised the group. “It will help you zero in on what you want and how to get it.”
He suggested listing all the variables on a spreadsheet, for example, minimum compensation, call schedule, time off for vacation and continuing education, time to partnership, buy-in to partnership, and tail coverage. Next, put the items in order of importance with “must haves” and “deal breakers” at the top of the list.
Dr. Duffy also recommended gaining a detailed
understanding of the financial structure and governance of any group you consider. Ask about its compensation model, culture, and goals for the future, and compare that information to the items on your spreadsheet.
“Many physicians are moving away from individual or small group practices to larger group/hospital-based employment,” said Dr. Duffy. He explained that in theory, hospital-based jobs offer fewer administrative responsibilities, increased benefits, more stable job security, and increased flexibility in terms of call schedules. “But if a high level of autonomy is one of your deal breakers,” Dr. Duffy continued, “an individual or small group practice may still be the best choice for you.”
Making Yourself MarketableThe panel also addressed why it is so difficult to find a
job right now. Even with an aging population, Dr. Duffy said there is some evidence that the job market for new interventionalists is shrinking.
He explained that though the projected demand for interventional therapy will continue to grow over time, practices are under stress from decreased reimbursement rates and uncertainties about ongoing healthcare reform efforts. “These issues make it difficult for established groups to predict future needs, and, therefore, more reluctant to commit to new interventional physicians,” said Dr. Duffy.
Joseph D. Babb, M.D., FSCAI, offered another explanation: many older cardiologists are delaying retirement, presumably due to the recent economic downturn, thus limiting turnover within the job pool. He
Early CareerEarly-Career Sessions Offer Guidance for Challenges AheadBy Anand Prasad, M.D., FSCAI
Anand Prasad, M.D., FSCAI
(continued on page 16)

16
Q: Is reimbursement available for services performed within the context of a clinical trial?
A: Certainly, if required conditions are met. In 2000, President Clinton issued an Executive Memorandum directing Medicare to cover
the routine healthcare costs of beneficiaries in clinical trials. In response, CMS issued a National Coverage Determination (NCD) implementing this directive. All routine costs of qualifying clinical costs are covered under the Medicare program, as well as reasonable and necessary items and services used to diagnose and treat complications arising from participation in all clinical trials. Some states and commercial insurance carriers have elected to follow in CMS’s footsteps and support coverage of routine costs associated with a patient’s participation within a clinical trial.
The NCD issued by CMS defines routine costs of a clinical trial as being all items and services that are otherwise generally available to Medicare beneficiaries (i.e., there exists a benefit category, it is not statutorily excluded, and there is not a national non-coverage
decision) that are provided in either the experimental or the control arms of a clinical trial, including:
• Items or services that are typically provided absent a clinical trial (e.g., conventional care);
• Items or services required solely for the provision of the investigational item or service (e.g., administration of a non-covered chemotherapeutic agent), the clinically appropriate monitoring of the effects of the item or service, or the prevention of complications; and
• Items or services needed for reasonable and necessary care arising from the provision of an investigational item or service—in particular for the diagnosis or treatment of complications.
CMS does NOT consider the following “routine costs” and will not cover, the following:
• The investigational item or service itself, unless otherwise covered outside of the clinical trial;
• Items and services provided solely to satisfy data
Clinical Trials and Reimbursement
suggested learning new skills. “While PCI volumes have leveled off recently, there are still avenues of growth in the peripheral, carotid, and ASD closure arenas,” said Dr. Babb. “The versatility you gain from adding to your skill set could buffer losses of PCI volume, particularly as reimbursement rates undoubtedly continue to decrease.”
Keeping an Eye on the FutureDavid R. Holmes, M.D., FACC, FSCAI, recommended
that, after landing a job, early-career interventionalists continue to monitor developments in their field. “In addition to the challenges of building a practice, understanding the intricacies of billing and reimbursement, and honing and develop interventional skills, early-career interventional cardiologists face many of the same challenges faced by all interventional cardiologists.”
One of those challenges is the perception, and in rare cases the reality, of overutilization of interventional therapy. “As healthcare reform continues, utilization of expensive services will be scrutinized more and more,” said Dr. Holmes. “Because politicians and the media may not understand the complex clinical issues faced by physicians when treating individual patients in this healthcare environment, abuse of therapies by a small number of individuals can have a profound impact on all cardiologists and our patients.”
“Cutting reimbursement for invasive therapies in response to overutilization may result in denying access to effective treatments and diminishing the quality of care,” said Dr. Holmes. “It will be more important than ever for the next generation of interventional cardiologists to continue doing what is best for their patients, with each intervention backed by clear clinical justification.”
Panelists agreed that the challenges faced by early-career interventionalists are great but the demand for their skills remains high. “With baby boomers getting older, and the rising rates of obesity and diabetes—interventional cardiologists have the opportunity to remain at the forefront of the emerging healthcare system,” said Dr. Holmes. “But it will require a commitment on our part to educate the public about heart and vascular disease and remain active in the reform process.”
Find more information on navigating early-career challenges at http://www.scai.org/Careers/Stories.aspx. If you are interested in joining ICDC or finding out how you can get more involved, send an email to [email protected]. n
Dr. Anand Prasad is an Assistant Clinical Professor of Medicine at the University of California, San Diego, and an active member of SCAI’s Interventional Career Development Committee.
Coding Q&A
Early-Career Sessions (cont’d from pg 15)

17
collection and analysis needs that are not used in the direct clinical management of the patient (e.g., monthly CT scans for a condition usually requiring only a single scan); and
• Items and services customarily provided by the research sponsors free of charge for any enrollee in the trial.
To qualify for Medicare coverage of routine costs, a clinical trial must meet the following three requirements:
1. The subject or purpose of the trial must be the evaluation of an item or service that falls within a Medicare benefit category (e.g., physicians’ service, durable medical equipment, diagnostic test) and is not statutorily excluded from coverage (e.g., cosmetic surgery, hearing aids).
2. The trial must not be designed exclusively to test toxicity or pathophysiology; it must have therapeutic intent.
3. The trials of therapeutic interventions must enroll patients with diagnosed disease rather than healthy volunteers. Trials of diagnostic interventions may enroll healthy patients in order to have a proper control group.
Additionally, to qualify a clinical trial for Medicare coverage of routine costs, the clinical trial should have the following characteristics:
1. The principal purpose of the trial is to test whether the intervention potentially improves the participants’ health outcomes;
2. The trial is well-supported by available scientific and medical information or it is intended to clarify or establish the health outcomes of interventions already in common clinical use;
3. The trial does not unjustifiably duplicate existing studies;
4. The trial design is appropriate to answer the research question being asked in the trial;
5. The trial is sponsored by a credible organization or individual capable of executing the proposed trial successfully;
6. The trial is in compliance with federal regulations relating to the protection of human subjects; and
7. All aspects of the trial are conducted according to the appropriate standards of scientific integrity.
NCDR®
The NCDR®, an initiative of the American College of Cardiology Foundation®, began in 1997 to help health care provider groups and institutions respond to increasing requirements to document their processes and outcomes of care in the cath lab setting.
For more information about the NCDR, please visit www.ncdr.org.
Today, more than 2,300 hospitals nationwide participate in the NCDR’s six registries, making it the United States’ preeminent cardiovascular data repository.
Encompassing both hospital-based registries and one practice-based program, the NCDR provides evidence-based quality improvement solutions for cardiologists and other medical professionals who are committed to mea-surement, improvement, and excellence in cardiovascular care. In addition to facility-level benefits, physicians can also use their NCDR participation to meet MOC recertifica-tion requirements.
The NCDR is made up of the following five hospital-based registries:• ACTIONRegistry®-GWTG™ for acute coronary
syndrome patients• CARERegistry® for carotid artery revascularization and
endarterectomy procedures
• CathPCIRegistry® for cardiac catheterization and percutaneous coronary intervention procedures
• ICDRegistry™ for implantable cardioverter defibrillator procedures
• IMPACTRegistry™ for adult and pediatric congenital heart conditions (launching this fall)
And one practice-based registry:• PINNACLERegistry™ for coronary artery disease,
hypertension, heart failure and atrial fibrillation in the outpatient setting
The NCDR is proud to work with SCAI, a valued partner in the development and ongoing advancement of the CathPCI Registry, CARE Registry and IMPACT Registry. Support from partners like SCAI provides perspective and knowledge from medical experts throughout the cardiovas-cular community, benefiting the NCDR, its registries and participating facilities.
(continued on page 18)

18
The NCD finds that clinical trials that “have been deemed by AHRQ, in consultation with the other agencies represented on the multi-agency panel to be highly likely to have the above-listed seven desirable characteristics of clinical trials” are automatically qualifi ed to receive Medicare coverage of their routine costs. Clinical trials that are deemed to be automatically qualifi ed are:
1. Trials funded by NIH, CDC, AHRQ, CMS, DOD, and VA;
2. Trials supported by centers or cooperative groups funded by the NIH, CDC, AHRQ, CMS, DOD, and VA;
3. Trials conducted under an investigational new drug application (IND) reviewed by the FDA; and
4. Drug trials that are exempt from having an IND under 21 CFR 312.2(b)(1). These will be deemed automatically qualifi ed until the qualifying criteria are developed and the certifi cation process is in place. At that time the principal investigators of these trials must certify that the trials meet the qualifying criteria in order to maintain Medicare coverage of routine costs. This certifi cation process will only affect the future status of the trial and will not be used to retroactively change the earlier deemed status.
Clinical trials that meet the qualifying criteria will receive Medicare coverage of routine costs after the trial’s lead principal investigator certifi es that the trial meets the criteria and the investigator enrolls the trial in a Medicare clinical trials registry, currently under development. The principal investigators of automatically qualifi ed trials do not need to certify that the trials meet the qualifying criteria, but also must enroll the trials in the Medicare clinical trials registry for administrative purposes, once the registry is established.
Providers who participate in an IDE trial and anticipate fi ling Medicare claims must notify their local Medicare contractor. The following information must be furnished prior to submission of a claim for payment:
• A copy of the FDA-approval letter provided to the sponsor or manufacturer of the device. The approved IDE code number must be on the letter;
• The name of the device (both trade, common or usual, and classifi cation name);
• Any action taken to conform to any applicable IDE special controls;
• A narrative description of the device suffi cient to make a payment determination;
• A statement indicating how the device is similar to and/or different from other comparable products;
• Indication of whether the device will be billed on an inpatient or outpatient claim;
• A brief summary of the study design or a copy of the actual trial protocol; and
• The provider’s protocol for obtaining informed consents for benefi ciaries participating in the clinical trial.
Each individual claim for routine costs provided within the context of a qualifying clinical trial must include the IDE number obtained from the manufacturer supplying the device or from the FDA. The FDA issues an IDE number that corresponds to each FDA-approved device that has been granted an investigational device exemption. Additionally, modifi er –Q0 must be appended to all CPT codes used to report the routine costs and the diagnosis code V70.7 must be presented as the secondary diagnosis:
-Q0 Investigational clinical service provided in a clinical research study that is an approved clinical research study V70.7 Examination of participant in clinical trial
For information regarding the IDE trial approval process, see the FDA Web page, http://www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/default.htm
For information on state specific regulations pertaining to coverage for routine clinical trial costs, see the National Cancer Institute Web site, http://www.cancer.gov/clinicaltrials/developments/laws-about-clinical-trial-costs
For more information regarding CMS’ National Coverage Determination for Clinical Trials, see https://www.cms.gov/ClinicalTrialPolicies/ n
Please note: SCAI is committed to making every reasonable effort to provide accurate information regarding the use of CPT®, and the rules and regulations set forth by CMS for the Medicare program. However, this information is subject to change by CMS and does not dictate coverage and reimbursement policy as determined by local Medicare contractors or any other payor. SCAI assumes no liability, legal, fi nancial, or otherwise, for physicians or other entities who utilize this information in a manner inconsistent with the policies of any payors or Medicare carriers with which the physician or other entity has a contractual obligation. CPT codes and their descriptors are copyright 2009 by the American Medical Association.
Clinical Trials and Reimbursement (cont’d from pg 17)

![[XLS]servicioscompartidos.uniandes.edu.co · Web view2 4 6 9 6 9 6 9 6 9 6 9 9 9 9 9 9 7 9 9 9 9 9 7 9 7 9 7 9 4 6 9 9 9 9 9 4 6 9 4 6 9 4 6 9 4 6 9 6 9 4 6 9 9 9 9 9 4 6 9 9 9 9](https://static.fdocuments.us/doc/165x107/5be14b3a09d3f232098d2967/xls-web-view2-4-6-9-6-9-6-9-6-9-6-9-9-9-9-9-9-7-9-9-9-9-9-7-9-7-9-7-9-4-6.jpg)
















