
NEWSLETTERsouthstaffsldc.com/South_Staffs_LDC/LPN_files/DENTAL LPN newslett… · of this...
8
Chairman's Report The Dental LPN in Shropshire and Stafford- shire is now well established. It has been a vehicle to bring issues to the attention of other dental stakeholders as well as the Area Team. The membership of the net- work took sometime to establish, but now that it is fully populated and there have also been 2 full meetings of the network, it is clear to see that all the membership is working well and taking part in the discus- sions that are occurring around the table. This kind of network of dental stakeholders has never existed before and it is hearten- ing to see that passions do run high when members are talking about improving the oral health of our local population. The Dental LPN must be effective by dem- onstrating achievements in: • High quality care • Reducing service variation • Reducing inequalities We can only achieve these laudable aims by putting aside differences and working together to achieve a common goal. Col- laborative discussion has been the main focus during meetings. Trying to allow an open and frank discussion with full partici- pation while at the same time trying to keep to a strict agenda has been a challenge. But it has allowed some much needed debate on the future direction of dental services and helped to identify good practice in some areas that can then be rolled out across the whole region. Each member of the LPN is there to be a voice for that particular stakeholder group. For each member to be effective it is imperative that they form smaller networks of individuals from their groups, so that information can be distributed out quickly and that they can gather opinion on whatever issues that may be relevant at the time. It is only then that the net- work can be truly inclusive and honestly reflect the views of all those concerned. Everyone should look at the back page of this newsletter and identify who is their member on the network. They should contact their member to canvas opinion and to generate debate. Only then can current issues be identified and raised by their respective member at the network meetings. We have already made huge strides in raising the profile of dentistry locally. Without the wider membership actively participating it cannot work effectively. There needs to be a loud and persistent dental voice in local decision making. The Dental LPN for Shropshire and Staf- fordshire is YOUR LPN. Be a part of it! “Knowing is not enough; we must apply. Willing is not enough, we must do.” Leonardo da Vinci Date—May 2014 Newsletter—Issue 3 “Working together to improve oral health” Inside this issue: Charity Run, Peer review groups 2 Sheesha Smoking 3 South Staffs LDC open meeting 4 Smile month, Dates for your diary 5 Inappropriate Orthodontic Referrals 6 Upcoming dental courses 6 Pictorial guide to Orthodontic Referrals 7 Contact details, Dental LPN member list 8 Please let us know of any email addresses that should be added to the mailing list for this newsletter. (Contact details on the back page) Visit our new website - http://www.england.nhs.uk/mids-east/mids-east-3/ss-at/dental-lpn/ NEWSLETTER DENTAL LPN—SHROPSHIRE AND STAFFORDSHIRE
Transcript of NEWSLETTERsouthstaffsldc.com/South_Staffs_LDC/LPN_files/DENTAL LPN newslett… · of this...
Chairman's Report
The Dental LPN in Shropshire and Stafford-shire is now well established. It has been a vehicle to bring issues to the attention of other dental stakeholders as well as the Area Team. The membership of the net-work took sometime to establish, but now that it is fully populated and there have also been 2 full meetings of the network, it is clear to see that all the membership is working well and taking part in the discus-sions that are occurring around the table. This kind of network of dental stakeholders has never existed before and it is hearten-ing to see that passions do run high when members are talking about improving the oral health of our local population.
The Dental LPN must be effective by dem-onstrating achievements in:
• High quality care
• Reducing service variation
• Reducing inequalities
We can only achieve these laudable aims by putting aside differences and working together to achieve a common goal. Col-laborative discussion has been the main focus during meetings. Trying to allow an open and frank discussion with full partici-pation while at the same time trying to keep to a strict agenda has been a challenge. But it has allowed some much needed debate on the future direction of dental services and helped to identify good practice in some areas that can then be rolled out
across the whole region.
Each member of the LPN is there to be a voice for that particular stakeholder group. For each member to be effective it is imperative that they form smaller networks of individuals from their groups, so that information can be distributed out quickly and that they can gather opinion on whatever issues that may be relevant at the time. It is only then that the net-work can be truly inclusive and honestly reflect the views of all those concerned.
Everyone should look at the back page of this newsletter and identify who is their member on the network. They should contact their member to canvas opinion and to generate debate. Only then can current issues be identified and raised by their respective member at the network meetings.
We have already made huge strides in raising the profile of dentistry locally. Without the wider membership actively participating it cannot work effectively. There needs to be a loud and persistent dental voice in local decision making. The Dental LPN for Shropshire and Staf-fordshire is YOUR LPN. Be a part of it!
“Knowing is not enough; we must apply. Willing is not enough, we must do.” Leonardo da Vinci
Date—May 2014 Newsletter—Issue 3
“Working together
to improve oral
health”
Inside this issue:
Charity Run, Peer review groups 2
Sheesha Smoking 3
South Staffs LDC open meeting 4
Smile month, Dates for your diary 5
Inappropriate Orthodontic Referrals 6
Upcoming dental courses 6
Pictorial guide to Orthodontic Referrals 7
Contact details, Dental LPN member list 8
Please let us know of any email addresses that should be added to the mailing
list for this newsletter. (Contact details on the back page)
Visit our new website -
http://www.england.nhs.uk/mids-east/mids-east-3/ss-at/dental-lpn/
NEWSLETTER
DENTAL LPN—SHROPSHIRE AND STAFFORDSHIRE

Page 2 NEWSLETTER—ISSUE 3
Tony Ahmed (current chair of the Dental LPN) took part in a 10k charity run on 4th May 2014 to raise money for Great Ormand Street Chil-dren's Hospital. Over 1400 runners made up of people from all over the country signed up to take part in the 30th “Mercy for Mankind” Charity Run. Tony’s run raised over £500. The run which took place at Batter-sea Park in London raised money for numerous other charities as well.
If anyone else wants to advertise a local dental event or achievement, please see contact details on the back page.
Peer review groups for DCPs and dentists
Natalie Preece who is taking overall responsibility. Her contact details are -
The dentists peer review group in Telford is operated by Kuldip Ghakal who is one of the general dental practice advisors for the Area Team. His contact de-tails are - [email protected]
These groups can be a really useful forum, especially for the smaller practices so that members can meet and share ideas, but also learn about good practice and what is happening locally in their region.
An issue that was raised at the last LPN meet-ing on 30th April was the lack of support for DCPs in the region. Specifically the lack of fo-rums where DCPs could get together to share good practice and meet other like minded pro-fessionals.
Having spoken to the members of the network, it became apparent that there are already peer review groups set up around the region, but they just have not been publicised well.
Angela Mayhew who is the course tutor for Tel-ford and Burton has given me the contact details for the peer groups she has set up. As you can see there is a dental nurse group in Telford and Burton - the Telford group is well established and the Burton group has newly started. There is a hygiene/therapist group which has not yet fully got off the ground but the opportu-nity for new members to join may be a welcome catalyst. There is also an established dentist peer group in Telford .
The contact at the moment is Angela Mayhew for the Dental Nurses group at both Telford and Burton—[email protected]
The contact for the Hygiene /therapist group is
Charity Run raises £500
Page 3 NEWSLETTER—ISSUE 3
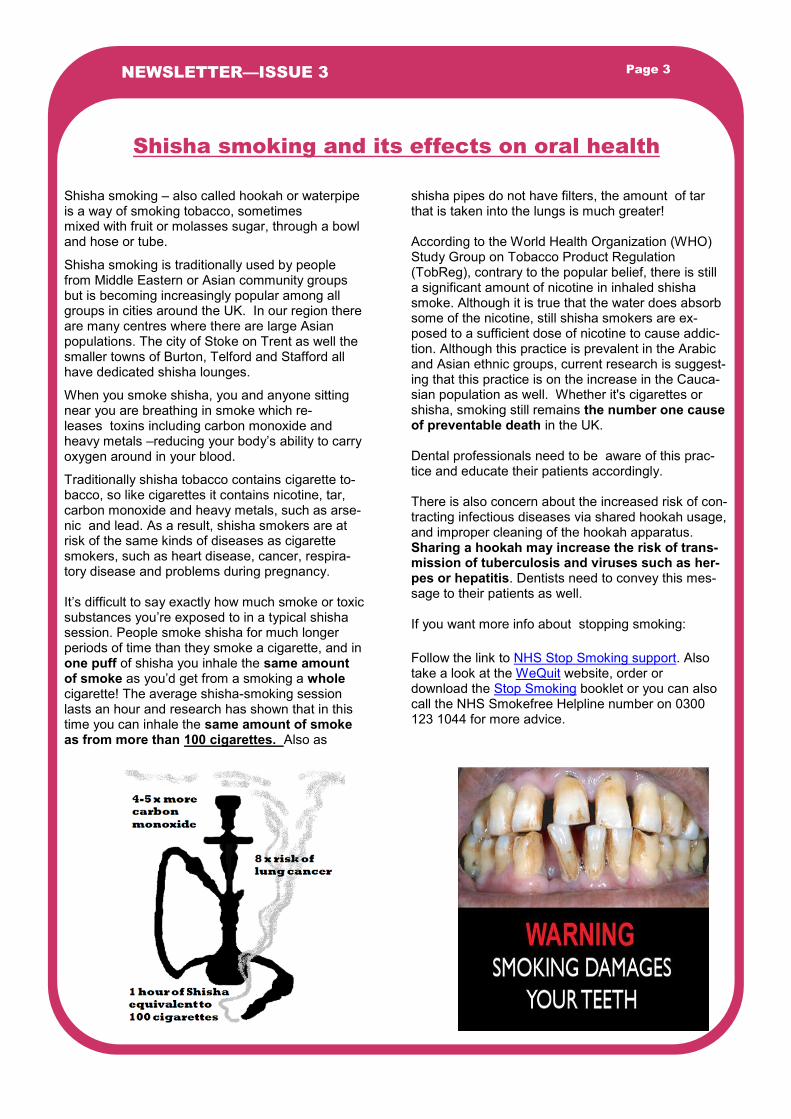
shisha pipes do not have filters, the amount of tar that is taken into the lungs is much greater! According to the World Health Organization (WHO) Study Group on Tobacco Product Regulation (TobReg), contrary to the popular belief, there is still a significant amount of nicotine in inhaled shisha smoke. Although it is true that the water does absorb some of the nicotine, still shisha smokers are ex-posed to a sufficient dose of nicotine to cause addic-tion. Although this practice is prevalent in the Arabic and Asian ethnic groups, current research is suggest-ing that this practice is on the increase in the Cauca-sian population as well. Whether it's cigarettes or shisha, smoking still remains the number one cause of preventable death in the UK. Dental professionals need to be aware of this prac-tice and educate their patients accordingly. There is also concern about the increased risk of con-tracting infectious diseases via shared hookah usage, and improper cleaning of the hookah apparatus. Sharing a hookah may increase the risk of trans-mission of tuberculosis and viruses such as her-pes or hepatitis. Dentists need to convey this mes-sage to their patients as well. If you want more info about stopping smoking:
Follow the link to NHS Stop Smoking support. Also take a look at the WeQuit website, order or download the Stop Smoking booklet or you can also call the NHS Smokefree Helpline number on 0300 123 1044 for more advice.
Shisha smoking – also called hookah or waterpipe is a way of smoking tobacco, sometimes mixed with fruit or molasses sugar, through a bowl and hose or tube.
Shisha smoking is traditionally used by people from Middle Eastern or Asian community groups but is becoming increasingly popular among all groups in cities around the UK. In our region there are many centres where there are large Asian populations. The city of Stoke on Trent as well the smaller towns of Burton, Telford and Stafford all have dedicated shisha lounges.
When you smoke shisha, you and anyone sitting near you are breathing in smoke which re-leases toxins including carbon monoxide and heavy metals –reducing your body’s ability to carry oxygen around in your blood.
Traditionally shisha tobacco contains cigarette to-bacco, so like cigarettes it contains nicotine, tar, carbon monoxide and heavy metals, such as arse-nic and lead. As a result, shisha smokers are at risk of the same kinds of diseases as cigarette smokers, such as heart disease, cancer, respira-tory disease and problems during pregnancy. It’s difficult to say exactly how much smoke or toxic substances you’re exposed to in a typical shisha session. People smoke shisha for much longer periods of time than they smoke a cigarette, and in one puff of shisha you inhale the same amount of smoke as you’d get from a smoking a whole cigarette! The average shisha-smoking session lasts an hour and research has shown that in this time you can inhale the same amount of smoke as from more than 100 cigarettes. Also as
Shisha smoking and its effects on oral health

Page 5 NEWSLETTER—ISSUE 3
The National Smile Month campaign, which kicks off on 19 May and runs until 19 June, is a brilliant way to engage with members of the general public in the hope you will better their oral health. It’s crucial to further oral health improvements that as many people as possible take the lead and deliver the messages promoted during the campaign. Taking part in National Smile Month is easy. It doesn’t necessarily involve lots of time or money, just the passion to make a difference and help promote oral health in your community. Visit and register your in-terest at
http://www.nationalsmilemonth.org and spread the word!
Dates for your diary
19th May-19th June—Smile month
4th June - Staffordshire dental forum—Stafford PGMC
2nd July— Dental LPN meeting—Area Team, Rugeley.
3rd July—BDA Stoke and Stafford “ Endodontics—an update on recent advances for GDPs”
17th September—Mouth Cancer awareness day
( this is not an exhaustive list, if any member wants to add to this list, please use the contact email for Jo Athersmith on the back page)
Page 6 NEWSLETTER—ISSUE 3
A concern to both providers and consumers of orthodontic treatment is the length of new patient consultation waiting lists. A possible reason for the excessive length of these lists could be un-necessary referral of patients. NHS orthodontic treatment, like all other areas of NHS dental care, underwent changes with the introduction of the new NHS dental contract in 2006. Orthodontic treatment was restricted to those patients with the most severe malocclusions as defined by the In-dex of Orthodontic Treatment Need (IOTN). In order for the new system to work successfully, it follows that dentists referring patients for ortho-dontic treatment should be familiar with the IOTN and its use.
Studies have shown that this clearly not the case
1,2. Having spoken to local consultants and
specialist orthodontic practitioners around Shrop-shire and Staffordshire, it is clear that GDPs are still not routinely using the Index to assess their patients and some had not even heard of it! It is understandable that some might have graduated in a country where the IOTN was not routinely used however, the Index was developed over 30 years ago and it has received considerable world-wide publicity and is used in many countries.
There is a tendency to consider orthodontics to be a subject that should only be taught at the postgraduate level. Although it is not possible to train a dental student to be competent to under-take orthodontic treatment when he or she quali-fies, all dentists should be competent in the diag-nosis of malocclusion and appropriate referral. It looks like there is still considerable work to do to achieve this aim.
With this in mind the British Orthodontic Associa-
tion issued some guidelines to make orthodontic refer-rals easier for the GDP. They are based on the IOTN philosophy, but do not rely on the individual scoring system. Please see the pictorial guide opposite.
By working closely with dentists, providers in primary and secondary care can develop robust and transpar-ent care pathways improving access to orthodontic care. Which includes the use of referral guidelines to ensure patients are referred to the most appropriate provider with minimal delay. This will negate the need for intermediate triaging of referrals and all the unnec-essary cost and delay this would incur. They should not be prescriptive or take away referring practitioners’ or patients’ choice where they access a specialist opinion. They should also not be used to limit or pre-vent referral for a specialist opinion, which remains a fundamental patient right. Therefore written guidelines should be accompanied by education and support for referring practitioners including lectures and courses, and regular reminders particularly for those practices which find it difficult to change their referral practice.
With this in mind all practitioners should regularly up-date their knowledge on IOTN and orthodontic refer-ral guidelines in their region. Please access the CPD courses that are provided by the Deanery to enhance your knowledge! See below for the latest courses.
(Courses run by HEE West Midlands)
Inappropriate Orthodontic Referrals
Stafford—
10th June – GDPs Orthodontics When to refer , when not to refer
8th July—Cross Infection and Control for the Den-tal team
Shrewsbury—
6th June—Current Ethical and Law based issues affecting the Dental Team
18th June—Medical Emergencies and Basic First Aid
1. Orthodontic referral behaviour of West Sussex dentists. Jackson OA, Cunningham SJ, Moles DR, Clark JR. Br Dent J. 2009 Nov 14; 207(9):E18; discussion 430-1. Epub 2009 Nov 6.
2. Do dentists refer orthodontic patients inappropriately? O’Brien KD, McComb JL, Fox N, Bearn D, Wright J. Br Dent J 1996;181(4):132-136.
Stoke—
18th June—Restorative Dentistry and the older patient
9th July—Ethics for the Dental Team
Telford—
2nd June—Mental Capacity and Consent!
25th June—Specification 21st Century Management Competencies
PLEASE PRESS THE CTRL KEY AND CLICK
TO FOLLOW TO THE RELEVANT WEBPAGE.
Upcoming dental courses run by HEE West Midlands
Page 7 NEWSLETTER—ISSUE 3
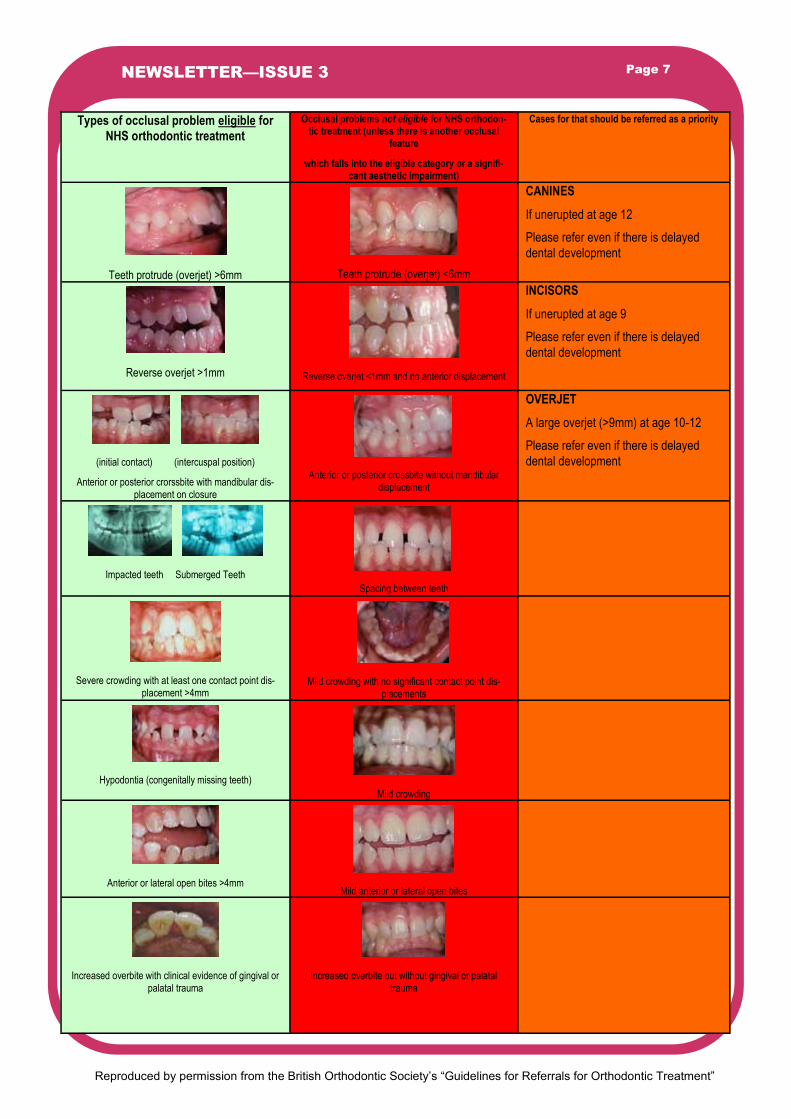
Types of occlusal problem eligible for NHS orthodontic treatment
Occlusal problems not eligible for NHS orthodon-tic treatment (unless there is another occlusal
feature which falls into the eligible category or a signifi-
cant aesthetic impairment)
Cases for that should be referred as a priority
Teeth protrude (overjet) >6mm
Teeth protrude (overjet) <6mm
CANINES
If unerupted at age 12
Please refer even if there is delayed
dental development
Reverse overjet >1mm
Reverse overjet <1mm and no anterior displacement
INCISORS
If unerupted at age 9
Please refer even if there is delayed
dental development
(initial contact) (intercuspal position)
Anterior or posterior crorssbite with mandibular dis-placement on closure
Anterior or posterior crossbite without mandibular displacement
OVERJET
A large overjet (>9mm) at age 10-12
Please refer even if there is delayed
dental development
Impacted teeth Submerged Teeth
Spacing between teeth
Severe crowding with at least one contact point dis-placement >4mm
Mild crowding with no significant contact point dis-placements
Hypodontia (congenitally missing teeth)
Mild crowding
Anterior or lateral open bites >4mm
Mild anterior or lateral open bites
Increased overbite with clinical evidence of gingival or palatal trauma
Increased overbite but without gingival or palatal trauma
Reproduced by permission from the British Orthodontic Society’s “Guidelines for Referrals for Orthodontic Treatment”
Community Dental Services officer – Richard Beck
Local Dental Committee representative—Adam Morby
Primary care orthodontic GDP – Graeme Manzie / Philip
Barton
2 GDP representatives—Harj Basra / Saleem Mulla
Dental Care Professional representative—Trudy Green
Health Education England representative – Karen Elley /
Jane Davies-Slowik
Admin and secretarial
Joanne Athersmith [email protected]
Lucy Jones [email protected]
Chair – Nadeem Ahmed (Tony)
Consultant in DPH – Kate Taylor- Weetman
GDPA – Frank Hollinshead
Primary Care Lead and deputy chair— Darrell Jackson
Patient representative – Mike Dixon – Community Health
Voice
Orthodontic Consultant in secondary care – John Scholey
Maxillofacial Consultant in secondary care—Tim Malins /
Daya Gahir
Restorative consultant in secondary care –
David Newsum / Stephen Brindley
LPN member contact details
If anybody has anything that they would like to include in future newsletters please can they forward it to Joanne Athersmith [email protected] . If anyone knows anybody that has been missed off the mailing list or would like someone to be added onto the mailing list then please can they also contact Joanne Athersmith.
Please share this newsletter with all members of the dental team. The purpose of the newsletter is to be as inclusive as possible and to be an easy way to communicate important information out to all dental stakeholders in Shropshire and Staffordshire.
Page 8 NEWSLETTER—ISSUE 3


















