NEWER ANTIPLATELETS
52
NEWER ANTIPLATELETS JOURNAL REVIEW Dr RAJESH K F
description
NEWER ANTIPLATELETS. JOURNAL REVIEW Dr RAJESH K F. Adenosine diphosphate (ADP) plays a key role in the genesis of physiological platelet-rich hemostatic plugs and of pathological arterial thrombi. T ransduction of ADP signal involves interaction with 2 platelet receptors - PowerPoint PPT Presentation
Transcript of NEWER ANTIPLATELETS

NEWER ANTIPLATELETSJOURNAL REVIEW
Dr RAJESH K F

Adenosine diphosphate (ADP) plays a key role in the genesis of physiological platelet-rich hemostatic plugs and of pathological arterial thrombi

Transduction of ADP signal involves interaction with 2 platelet receptors
Gq-coupled P2Y1 receptor and Gi-coupled P2Y12 receptor
Concomitant activation of both Gq and Gi pathways by ADP elicit normal platelet aggregation
P2Y1

Prasugrel
Rapid and consistent inhibitory effects on platelet aggregation than clopidogrel
Distinct chemical structure permits conversion to its active metabolite with less dependence on CYP enzymes than clopidogrel

Different metabolism Appearance of active metabolite
in circulation within 15 min Reaches max plasma
concentration at 30 min Higher mean area under
concentration-time curve of active metabolite of prasugrel 60 mg than that of clopidogrel 600 mg

Faster and greater mean inhibition of P2Y12-dependent platelet function after 60-mg LD and 10-mg maintenance dose than after a 300- or 600-mg LD and 75- or 150-mg maintenance dose of clopidogrel
No influence of CYP genotype on its pharmacokinetics and pharmacodynamics
Lower interindividual variability in inhibition of P2Y12 Low prevalence of subjects who display resistance to
prasugrel

TRITON TIMI 38
Randomized, double-blind, parallel-group, multinational trial
Evaluated 13 608 high-risk patients with ACS who required PCI
Patients randomized to receive 60-mg prasugrel followed by 10 mg/d or a 300-mg clopidogrel followed by 75 mg/d for 6 to 15 months

Prasugrel associated with Fewer ischemic events (HR, 0.81;
95% CI, 0.73 to 0.90; P<0.001) Significant reductions in Rates of MI (9.7% for clopidogrel
vs. 7.4% for prasugrel; P<0.001), Urgent TVR(3.7% vs. 2.5%;
P<0.001) Stent thrombosis (2.4% vs. 1.1%;
P<0.001)

Major bleeding observed in 2.4% of prasugrel and in 1.8% of clopidogrel (hazard ratio, 1.32; 95% CI, 1.03 to 1.68; P = 0.03)
Rate of life-threatening bleeding (1.4% vs. 0.9%;P= 0.01)
Nonfatal bleeding (1.1% vs. 0.9%; HR, 1.25; P = 0.23)
Fatal bleeding (0.4% vs. 0.1%; P = 0.002)

Posthoc analysis 3 subgroups appeared to have
less net clinical benefit(≥75 yrs and <60 kg) or greater harm(previous CVA)
More effective antithrombotic drug than clopidogrel in patients with diabetes mellitus, STEMI, coronary stents, or recurrent cardiovascular events on treatment
DIABETIC SUBGROUP

CV death, MI, or stroke0
10
20
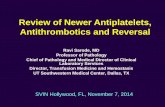
TRILOGY ACS
• At 30 months, among patients <75 years of age:
• CV death, MI, or stroke: 13.9% of the prasugrel group vs. 16.0% of the clopidogrel group (HR = 0.91, p = 0.21)
• All-cause death: 7.8% vs. 8.1% (HR = 0.96, p = 0.63 )
• Non-CABG TIMI major bleeding: 2.1% vs. 1.5% (HR = 1.31, p = 0.27)
• Outcomes were similar in the overall population, including the elderly
Trial design: NSTE-ACS patients <75 years of age selected for medical management without PCI (n = 7,243) were randomized to prasugrel 10 mg daily vs. clopidogrel 75 mg daily. Patients ≥75 years of age (n = 2,083) were randomized to prasugrel 5 mg daily vs. clopidogrel 75 mg daily.
Results
Conclusions• Among medically treated patients with NSTE-
ACS, prasugrel did not reduce adverse outcomes compared with clopidogrel
• Major bleeding was similar between groups
Roe MT, et al. N Engl J Med 2012;367:1297-1309
(p = 0.21)
Prasugrel
% 13.916.0
Clopidogrel


PRINCIPLE – TIMI 44 Comparison with Higher Dose Clopidogrel
P<0.0001 for each
IPA (%; 20 mM ADP)
Hours 14 Days
IPA (%; 20 mM ADP)P<0.0001
Prasugrel 10 mg
Clopidogrel 150 mg
Wiviott et al Circ 2007 (In Press)
N=201
Prasugrel 60 mg
Clopidogrel 600 mg

CANGRELOR
Belongs to family of analogs of ATP Display high affinity for P2Y12
receptor Potent inhibitor of ADP-induced
aggregation of human washed platelets (PIC509.4 with 30 mol/L ADP)
Does not require conversion to an active metabolite
Immediately active after IV infusion Half-life of 3 to 6 minutes

IV infusion well tolerated in healthy volunteers Result in dose-dependent inhibition of ADP-induced
platelet aggregation at doses up to 4 microg/kg/min At highest dose 3.2- and 2.9-fold increase in bleeding
time in men and women, respectively Short half-life result in rapid reversal of both
platelet-inhibitory effect and effect on bleeding time Reverse within 20 minutes after cessation of infusion
Clinical Pharmacology


Double-blind randomized trial in PCI 2-part phase II study Assessed safety and pharmacodynamics in PCI First part of study enrolled 200 patients undergoing
PCI Randomized to 18- to 24-hour IV infusion of placebo
or to 1, 2, or 4 microg/kg/min cangrelor in addition to aspirin and heparin before procedure
Greenbaum AB, Grines CL, Bittl JA, Becker RC, Kereiakes DJ, Gilchrist IC, Clegg J, Stankowski JE, Grogan DR, Harrington RA, Emanuelsson H,Weaver WD. Initial experience with an intravenous P2Y12 platelet receptor antagonist in patients undergoing percutaneous coronary intervention:results from a 2-part, phase II, multicenter, randomized, placeboand active-controlled trial. Am Heart J. 006;151:689.e1– 689.e10.

Second part of study 199 patients Randomized to receive either
cangrelor (4 microg / kg/ min1) or abciximab before PCI
Incidence of combined major and minor bleeding - not significant difference
After termination of infusion platelet aggregation returned to baseline values much faster in cangrelor treated group
5.7%
2.1%
5.4%
1.0%
Death, MI,revascularization
Major bleed (TIMI criteria)
Abciximab (N=94)Cangrelor (N=105)
10 DAY EVENTS

Safety, Tolerability and Effect on Patency in Acute MI Angiographic trial Assessed safety and efficacy of cangrelor as an adjunct to tpa in 92
patients with AMI All patients were treated with aspirin and heparin Randomized to cangrelor alone (280micro g/min), full-dose tpa alone, or
cangrelor 35, 140, or 280micro g/min in conjunction with half-dose tpa Combination of cangrelor and half-dose tpa resulted in 60-min coronary
patency similar to that of full-dose tpa alone (55% versus 50%; PNS) and greater patency than with cangrelor alone (55% versus 18%; P0.05)
Bleeding and adverse clinical events were comparable across groups
STEP-AMI

Study directly compared effects of clopidogrel and cangrelor administration in patients with IHD
Cangrelor (2 and 4micro g/mL/min) almost completely inhibited 10 mol/L ADP induced platelet aggregation
4 to 7 days of clopidogrel treatment resulted in only 60% inhibition
Storey RF, Wilcox RG, Heptinstall S. Comparison of the pharmacodynamic effects of the platelet ADP receptor antagonists clopidogrel and AR-C69931MX in patients with ischaemic heart disease. Platelets. 2002;13:407– 413.

CHAMPION PCI
Comparing Treatment With Cangrelor (With Usual Care) to Usual Care, in Subjects Who Require PCI
N=8877

Clopidogrel maintenance (at the discretion of the physician)
Subjects who require PCI (with or without stent)1:1 randomization to main treatment groups
Double blind, double dummy
Cangrelor bolus (30 µg/kg) &
infusion (4 µg/kg/min)
Clopidogrel capsules(600 mg)
Placebo capsules
(to match)
Placebo bolus & infusion
(to match)++
Subjects
IndexProcedure
Endpoints
Subjects who require PCIStudy drug infusion: for at least 2 hours or the duration
of the procedure, whichever is longer
Clopidogrel capsules(600 mg)
Placebo capsules(to match)
At 48 hours after randomization—• 1° efficacy endpoint: composite incidence of all-cause mortality, MI, and IDR• 2° efficacy endpoint: incidence of individual components, stroke & abrupt vessel closure• Safety endpoints: hemorrhage and transfusion• Safety: AEs/SAEs

Cangrelor not superior to 600 mg clopidogrel in moderate to high risk patients undergoing PCI
Using standard methods cangrelor appears to be non-inferior to 600 mg clopidogrel
Platelet function testing - cangrelor provides very rapid ADP blockade and did not interfere with post PCI clopidogrel effect

Efficacy Endpoints at 48 hours
*mITT= modified intent to treat population (patients with PCI and study drug)
Cangrelor ClopidogrelEfficacy mITT* (N=3897) (N=3871) OR (95% CI) P Value
Death/MI/IDR 7.5% 7.1% 1.05 (0.88, 1.24) 0.59(primary endpoint)MI 7.1% 6.6% 1.09 (0.91, 1.29) 0.36
IDR 0.3% 0.6% 0.56 (0.28, 1.11) 0.10
All-cause mortality 0.2% 0.1% 1.59 (0.52, 4.87) 0.42
Stent thrombosis 0.2% 0.3% 0.63 (0.25, 1.63) 0.34
Stroke 0.2% 0.2% 0.85 (0.29, 2.54) 0.77
Q-wave MI 0.1% 0.3% 0.40 (0.12, 1.27) 0.12
Death/Q-wave MI/ 0.6% 0.9% 0.67 (0.39, 1.14) 0.14IDRDeath/Q-wave MI/ 0.5% 0.6% 0.78 (0.42, 1.44) 0.42Stent thrombosis
0.1 1 10Cangrelor
BetterClopidogrel
(600 mg) Better

Increase in ACUITY minor and GUSTO mild bleeding with cangrelor though no increase in the need for blood transfusion

CHAMPION PLATFORM

Efficacy Endpoints at 48 Hours
Efficacy mITT*(SA/UA/NSTEMI)
CangrelorN=2654
ComparatorN=2641
OR [95% CI] P value
Death/MI/IDR** 7.0% 8.0% 0.87 (0.71,1.07) 0.17
MI 6.7% 7.2% 0.92 (0.74,1.13) 0.42
Non QMI** 6.5% 6.9% 0.94 (0.76,1.16) 0.55
QMI 0.2% 0.3% 0.50 (0.15,1.65) 0.25
IDR 0.7% 0.9% 0.79 (0.43,1.44) 0.44
Stent Thrombosis 0.2% 0.6% 0.31 (0.11,0.85) 0.02
Death 0.2% 0.7% 0.33 (0.13,0.83) 0.02
Death/QMI/IDR 0.9% 1.6% 0.55 (0.33,0.93) 0.02
Cangrelor Better5.02.01.00.2 0.5
Comparator (placebo) Better
* *Primary Analysis ** mITT= modified intent to treat population (patients with PCI and study drug), QMI= Q-wave myocardial infarction

Difference in primary endpoint not statistically significant
Lower rates of stent thrombosis, mortality

No significant effect on transfusions, even in high risk subgroups
Groin hematomas increased, not unexpected versus placebo

CHAMPION PHOENIX
Randomized, double-blind, double-dummy, superiority
Primary efficacy endpoint: Death/MI/IDR/ST at 48 hours
Key secondary endpoint: Stent Thrombosis at 48 hours
Efficacy endpoints also examined at 30 days
Primary safety endpoint: GUSTO Severe Bleeding at 48 hours

Primary Efficacy Outcomes at 48 Hours, MITT
Cangrelor(N=5472)
Clopidogrel(N=5470) OR (95% CI) P-value
Primary Analysis Adjusted1
Death/MI/IDR/ST 257/5470 (4.7%)
322/5469 (5.9%)
0.78 (0.66, 0.93) 0.005
1. The logistic model was adjusted for baseline status and clopidogrel dose. P value of 0.006 shown on the KM curve is log rank p value.
Secondary Efficacy Outcomes at 48 Hours, MITTStent thrombosis (keysecondary endpoint)
46/5470 (0.8%)
74/5469 (1.4%)
0.62 (0.43,0.90) 0.01
MI 207/5470 (3.8) 255/5469 (4.7) 0.80 (0.67,0.97) 0.02
Q-wave MI 11/5470 (0.2) 18/5469 (0.3) 0.61 (0.29,1.29) 0.19
IDR 28/5470 (0.5) 38/5469 ( 0.7) 0.74 (0.45,1.20) 0.22
Death 18/5470 (0.3) 18/5469 (0.3) 1.00 (0.52,1.92) >0.99
CV Death 18/5470 (0.3) 18/5469 (0.3) 1.00 (0.52,1.92) >0.99
Bhatt DL, Stone GW, Mahaffey KW, et al…. Harrington RA. NEJM 2013 at www.nejm.org

IV cangrelor significantly (p=0.005) reduced composite of death, MI, ischemia-driven revascularization, or stent thrombosis at 48 hours, with a 22% odds reduction
key secondary endpoint of stent thrombosis significantly reduced with 38% odds reduction
Benefit sustained through 30 days

No excess in severe bleeding or transfusions
Intravenous cangrelor may be an attractive option across the full spectrum of PCI, including stable angina, NSTEMI, and STEMI.

BRIDGE STUDY
To evaluate the use of cangrelor, an IV, reversible P2Y12 platelet inhibitor, for bridging thienopyridine-treated patients to CABG
Stage II Randomized, Double-Blind, Placebo-Controlled

Bridging strategy to CABG after thienopyridine discontinuation Cangrelor (at 0.75 µg/kg/min) achieves levels of platelet inhibition
known to be associated with a low risk of thrombotic events Without increased risk of bleeding before or during CABG,
although with a numerical increase in minor pre-CABG bleeding Independent of prior thienopyridine dose & time of discontinuation Consistent pharmaocdynamic effect during IV infusion Rapid offset after IV discontinuation prior to surgery No increased incidence of adverse events (e.g. dyspnea) or
laboratory abnormalities despite extended dosing

Not a prodrug; does not require metabolic activation Rapid onset of inhibitory effect on P2Y12 receptor Greater inhibition of platelet aggregation than clopidogrel Degree of inhibition reflects plasma concentration Faster offset of effect than clopidogrel Functional recovery of all circulating platelets Displays no significant affinity for other P2 receptors P2Y12 receptor is targeted by ticagrelor via noncompetitive
mechanism suggesting existence of an independent receptor binding site
TICAGRELOR

Dose-Finding Investigative Study to Assess the Pharmakodynamic Effects in Atherosclerotic Disease
Comparison of Ticagrelor With Clopidogrel Randomized, double-blind, parallel-group dose-finding
study 200 stable atherosclerotic outpatients on treatment with
aspirin 75 to 100 mg once daily Received ticagrelor (50, 100, or 200 mg BID or 400 mg
QD) or clopidogrel 75 mg once daily for 28 days
DISPERSE TRIAL

Ticagrelor (100 or 200 mg BID or 400 mg QD) inhibited platelet aggregation more rapidly and effectively and with less variability than clopidogrel after both first dose and 28 days of therapy
Only 1 major, nonfatal hemorrhage occurred in ticagrelor 400 mg QD group Moderate and minor bleeding events - dose related (from 29% to 51%) in
ticagrelor and 32% in clopidogrel Other adverse events- dyspnea,dizziness, headache, and hematuria Dyspnea-dose related(10%-50mg BID, 16% - 200 mg BID and 20% - 400
mg QD) None of dyspnea was serious None associated with congestive heart failure or bronchospasm.

Compared safety of ticagrelor with clopidogrel 990 patients NSTEMI treated with aspirin and standard therapy for
ACS Randomly assigned ticagrelor 90 mg BID or 180 mg
BID and clopidogrel (300-mg LD 75-mg QD MD) for up to 12 weeks
Statistically significant difference in major bleedings
DISPERSE-2 study

Posthoc analysis Continuous ECG- asymptomatic ventricular pauses 2.5
seconds were more common with ticagrelor 180 mg BID Dyspnea frequently with ticagrelor Clinical impact appeared low, with few cases being
considered serious or leading to discontinuation of treatment
Pathogenesis of dyspnea is unclear Hypothesis - may be mediated by adenosine

Ticagrelor inhibition of platelet aggregation-dose dependent
Both doses achieved greater inhibition than clopidogrel
Ticagrelor produced further suppression of platelet aggregation in patients who were currently receiving clopidogrel
SUBSTUDY OF DISPERSE-2
Storey RF, Husted S, Harrington RA, Heptinstall S, Wilcox RG, Peters G,Wickens M, Emanuelsson H, Gurbel P, Grande P, Cannon CP. Inhibition of platelet aggregation by AZD6140, a reversible oral P2Y12 receptor antagonist, compared with clopidogrel in patients with acute coronary syndromes. J Am Coll Cardiol. 2007;50:1852–1856.

PLATO
Platelet Inhibition and Patient Outcomes
Phase III randomized, double-blind, parallel group efficacy and safety study
Ticagrelor (180-mg LD 90-mg BID MD) compared with clopidogrel (300- to 600-mg LD 75-mg daily MD) for prevention of MACEs in patients with NSTEMI or STEMI
65% of enrolled patients underwent PCI

After 12 months of follow-up primary end point (a composite of vascular death,MI or stroke) - 9.8% in ticagrelor compared with 11.7% in patients receiving clopidogrel

Major efficacy endpoints
All patients*Ticagrelor(n=9,333)
Clopidogrel(n=9,291)
HR for (95% CI) p value†
Primary objective, n (%) CV death + MI + stroke 864 (9.8) 1,014 (11.7) 0.84 (0.77–0.92) <0.001
Secondary objectives, n (%) Total death + MI + stroke CV death + MI + stroke + ischaemia + TIA + arterial thrombotic events Myocardial infarction CV death Stroke
901 (10.2)
1,290 (14.6)
504 (5.8)353 (4.0)125 (1.5)
1,065 (12.3)
1,456 (16.7)
593 (6.9)442 (5.1)106 (1.3)
0.84 (0.77–0.92)
0.88 (0.81–0.95)
0.84 (0.75–0.95) 0.79 (0.69–0.91)1.17 (0.91–1.52)
<0.001
<0.001
0.005 0.001 0.22
Total death 399 (4.5) 506 (5.9) 0.78 (0.69–0.89) <0.001
The percentages are K-M estimates of the rate of the endpoint at 12 months.

Stent thrombosis
Ticagrelor(n=5,640)
Clopidogrel (n=5,649)
HR (95% CI) p value
Stent thrombosis, n (%)
Definite
Probable or definite
Possible, probable, definite
71 (1.3)
118 (2.1)
155 (2.8)
106 (1.9)
158 (2.8)
202 (3.6)
0.67 (0.50–0.91)
0.75 (0.59–0.95)
0.77 (0.62–0.95)
0.009
0.02
0.01
(evaluated in patients with any stent during the study)
*Time-at-risk is calculated from first stent insertion in the study or date of randomisation

Higher incidence of TIMI major non–CABG related bleeding in ticagrelor (2.8%)compared with clopidogrel (2.2%;P0.03)
Incidence of TIMI major CABG related bleeding - similar
High incidence of CABG-related bleeding in both groups (446 of 931 [47.9%] in ticagrelor versus 476 of 968 [49.2%] in clopidogrel) incidence of total bleeding not significantly different

PLATO - Dyspnoea
All patientsTicagrelor(n=9,235)
Clopidogrel(n=9,186)
p value*
Dyspnoea, % Any With discontinuation of study treatment
13.80.9
7.80.1
<0.001<0.001
*p values were calculated using Fischer’s exact test

Direct-acting, reversible P2Y12 inhibitor Can be administered both intravenously and orally Terminal half-life of 12 hours Complete inhibition of P2Y12-dependent ADP induced
platelet aggregation was observed at the 20-mg dose.
ELINOGREL

Early Rapid Reversal of Platelet Thrombosis With Intravenous PRT060128 Before PCI to Optimize Reperfusion in Acute MI
Phase II clinical trial Randomized trial evaluating the safety and tolerability of
adjunctive antiplatelet therapy with intravenous elinogrel (10, 20, 40, and 60 mg) before PCI in patients with STEMI
Results showed that incidence of bleeding events was infrequent and appeared to be similar in patients treated with all doses of elinogrel and in placebo
ERASE-MI
ERASE-MI, published in the December 2009 issue of the American Heart JournalDr Jeffrey Berger (Duke Clinical Research Institute, Durham, NC).

Phase 2 Safety and Efficacy Study Evaluate use of both intravenous and oral formulations Multicenter, randomized, double-blind, triple-
dummy,clopidogrel-controlled study of intravenous and oral elinogrel compared with clopidogrel in non urgent (including elective) PCI
After CAG randomized to clopidogrel or 1 of 3 doses of elinogrel
Study designed to understand clinical efficacy, biological activity, tolerability, and safety nonurgent PCI
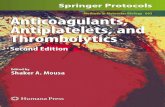
INNOVATE-PCI

ischemic0
3
6• No TIMI major bleeds in any group• Numerical increase in access bleeds requiring
medical attention with higher doses of elinogrel compared with clopidogrel
• Death, MI, stroke, or revascularization: approximately 2.8% of the elinogrel 150 mg group, 4% of the elinogrel 100 mg group, and 1.5% of the clopidogrel group (p = NS)
• Dyspnea: 12.1%, 15.4%, and 4.3%
INNOVATE PCITrial design: Patients undergoing nonurgent PCI were randomized to one of four groups prior to PCI: 1) elinogrel 80 mg IV, then 150 mg oral twice daily (n = 207); 2) elinogrel 80 mg IV, then 100 mg oral twice daily (n = 201); 3) elinogrel 80 mg IV, then 50 mg oral twice daily; or 4) clopidogrel 300-600 mg, then 75 mg daily (n = 208).
Results
Conclusions• Among patients undergoing nonurgent PCI, the use
of elinogrel is feasible • Access site bleeds were numerically higher with
increasing doses of elinogrel • Similar to ticagrelor, dyspnea was more common
with study drug
Presented by Dr. Sunil Raul at ESC 2010
(p = NS)
Elinogrel 150 mg
Elinogrel 100 mg
%
Death, MI, stroke, or revascularization
2.8
4.0
1.5
Clopidogrel

THANK U