New strategies in the work-up of chronic coronary syndromes€¦ · Focal CAD Diffuse CAD...
63
New strategies in the work-up of chronic coronary syndromes Carlos Collet Bortone MD, PhD Interventional Cardiologist Cardiovascular Center OLV-Aalst, Belgium
Transcript of New strategies in the work-up of chronic coronary syndromes€¦ · Focal CAD Diffuse CAD...

New strategies in the work-up of chronic coronary syndromes
Carlos Collet Bortone MD, PhDInterventional Cardiologist
Cardiovascular Center OLV-Aalst, Belgium

Introduction
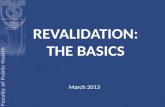
• The current understanding of the pathophysiology of coronary
artery disease relies on the potential adverse effect of myocardial
ischemia.

log
Haz
ard
Rat
io
01
23
45
% Ischemic Myocardium0 12.5% 25% 32.5% 50%
Medical Rx*
Revasc*
*p<0.001
N=10,627 no known CAD
146 Cardiac Deaths
Hachamovitch Circulation 2003;107:2900-2907.
Observational study: Revascularization was associated with lower risk of
cardiac death only in those with >10% ischemia on perfusion imaging

Ischemia
Angio-Based
Invasive physiology
Symptoms
Non-invasive
Test
FFR
iFR
Pd/Pa
RFR
dPR
DFR
2020

Introduction
• The current understanding of the pathophysiology of coronary
artery disease relies on the potential adverse effect of myocardial
ischemia.
• No clear evidence supporting the benefit of revascularization in
terms of hard clinical endpoints namely myocardial infarction
and death.
1. Tonino P et al. FAME NEJM (2009) 360:213-24

COURAGE 10 years FU
Sedlis SP et al. NEJM 2015

0%
5%
10%
15%
20%
25%
30%
0 1 2 3 4 5
Cu
mu
lati
ve I
ncid
en
ce (
%)
Follow-up (years)
CON
INV
Adjusted Hazard Ratio = 0.93 (0.80, 1.08), p-value = 0.34
Subjects at Risk
CON 2591 2431 1907 1300 733 293
INV 2588 2364 1908 1291 730 271
ISCHEMIA Primary OutcomeCV Death, MI, hospitalization for UA, HF or resuscitated cardiac arrest
15.5%
13.3%

Introduction
• The current understanding of the pathophysiology of coronaryartery disease relies on the potential adverse effect of myocardialischemia.
• No clear evidence supporting the benefit of revascularization interms of hard clinical endpoints namely myocardial infarctionand death.
• Patients selection based on functional non-invasive methods wasunable to identify which patients may benefit fromrevascularization using percutaneous based therapies.
Sedlis SP et al. NEJM 2015

Introduction
• Patient selection for PCI using FFR, epicardial vessel level metrichas been associated with improved clinical outcomes. 1
2. Xaplanteris et al. FAME 2 NEJM 2018
1. Tonino P et al. FAME NEJM 2009

Fractional Flow Reserve in MVD
Tonino P et al. FAME NEJM (2009) 360:213-24
RR 0.72 (95% CI 0.54 -0.96), p=0.02

Introduction
• Patient selection using FFR at the vessel level is associated withimproved clinical outcomes. 1
• FFR-guided PCI strategy was associated with a significantlylower rate of MACE than medical therapy alone. 2
2. Xaplanteris et al. FAME 2 NEJM 2018
1. Tonino P et al. FAME NEJM 2009

PCI vs. OMT in patients with FFR ≤ 0.80
Xaplanteris et al. NEJM 2018

Introduction
• Patient selection using FFR at the vessel level is associated withimproved clinical outcomes. 1
• FFR-guided PCI strategy was associated with a significantlylower rate of MACE than medical therapy alone. 2
• Randomized controlled trials have confirmed clinical benefit ofinvasive functional assessment for decision-making aboutrevascularization in patients with chronic coronary syndromes.
2. Xaplanteris et al. FAME 2 NEJM 2018
1. Tonino P et al. FAME NEJM 2009

Revascularization in patients with multivessel CAD
c With documented ischaemia or a haemodynamically relevant lesion defined by FFR ≤0.80 or iwFR ≤0.89, or >90% stenosis in a major coronary vessel.
ESC/EACTS Guidelines 2018

Improving outcomes in patients undergoing PCI

Effective therapies PCI
Thin strut biodegradable
or biocompatible
polymer
Physiology guided-PCI
IVUS/OCT for sizing and
optimisation
DAPT, PCSK9…

PCI Patient Selection
Focal CAD Diffuse CAD
Microvascular CAD Others
The current approach is limited in differentiating CAD endotypes

Personalised approach
Focal CAD Diffuse CAD
Microvascular CAD Others
PCIOMTCABG
OMTRevalidation
Tailored MT

Personalised approach
Goal = Complete “functional” myocardial revascularization
Focal CAD Diffuse CAD
Epicardial Coronary Artery Disease

Incomplete anatomical revascularisation: Residual SYNTAX score (RSS)
Farooq et al. Circulation 2013

Impact of residual angiographic disease after functionally complete revascularisation
Kobayashi et al. JACC 2016 RSS Residual SYNTAX score

Choi et al. JACC Cardiovasc Interv. 2018
Clinical Implication of Functional Incomplete Revascularization

Clinical risk factors: age, sex, HTN, DLP, DM, PMI, prior revasc, and ACS
3-vessel FFR performed after PCI Residual functional SYNTAX score (rFSS) defined as rSS in vessels with
FFR ≤0.80)
Risk scores 2 years clinical outcomes in 358 pts
Choi et al. JACC Cardiovasc Interv. 2018

How often do we achieve functional revascularisation
after PCI?

Toth et al. Circ Cardiovasc Interv. 2017.
Clinical outcomes stratified by FFR Post-PCI in the FAME trial
One-third of the vessel remained with FFR <0.88

Jeremias A et al. JACC Card Interv 2020
Post PCI iFR

Case # 17 Case # 5
Pullback vs. single FFR
Confidential information Cardiovascular Center OLV Aalst

FFR
FFR
gra
die
nt
0.78
Motorized FFR with n=12800 values
FFR 0.78
Male, 51 years old. Post PCI for RCA (STEMI, 2 month ago). BMI 31.8kg/m2. CrCl 152ml/min (Cr 0.75 mg/dL). LVEF 60%. Elective PCI for LAD
Focal Functional CAD
Length(mm)

FFR
FFR
gra
die
nt
0.78
ΔFFR lesion = 0.19 units
PCI DES 3.0 x 23 mm
Focal Functional CAD
Length(mm)

FFR
FFR
gra
die
nt
0.88
Focal Functional CAD Post-PCI
Length(mm)

0.78
FFR
FFR
gra
die
nt
Length(mm)
Male, 61 years old. Hypertension, Hyperlipidemia. BMI 27.7kg/m2. CrCl 115ml/min (Cr 0.86 mg/dL). LVEF 60%. Stable typical chest pain.
Motorized FFR with n=12500 values
Diffuse Functional CAD

0.78FFR
FFR
gra
die
nt
ΔFFR = 0.10
PCI DES 3.5 x 33 mm
Diffuse Functional CAD
Length(mm)

0.80
FFR
FFR
gra
die
nt
Diffuse Functional CAD Post-PCI
Length(mm)

PCI in Focal and Difusse CAD
Pre PCI Post PCI
Functional Focal CAD
Functional Diffuse CAD

Refining patient selection and predicting functional
revascularisation

PPG index calculation
PPGindex =Maximal PPG over 20 mm
Vessel FFR gradient
Length with functional disease
Vessel length+( )1-
2
PPGindex = Magnitude of pressure drop
Extent of functional CAD
Confidential information Cardiovascular Center OLV Aalst

PPG index calculation
PPGindex =Maximal PPG over 20 mm
Vessel FFR gradient
Length with functional disease
Vessel length+( )1-
2
PPGindex = Magnitude of pressure drop
Extent of functional CAD
Confidential information Cardiovascular Center OLV Aalst

PPG index calculation
PPGindex =Maximal PPG over 20 mm
Vessel FFR gradient
Length with functional disease
Vessel length+( )1-
2
PPGindex = Magnitude of pressure drop
Extent of functional CAD
Confidential information Cardiovascular Center OLV Aalst

PPGindex =Maximal PPG over 20 mm
Vessel FFR gradient
Length with functional disease
Vessel length+
Maximal PPG over 20 mm: Maximum FFR gradient over 20 mm.
Vessel FFR: Difference between FFR values obtained at the ostium of the
vessel and the most distal anatomical location.
Length with functional disease: Length of coronary artery in millimetres
with FFR drop ≥0.0015 FFR units.
Vessel length: Length from the ostium to the most distal pressure wire
location.
( )1-
2
PPG index calculation

Functional Patterns of CAD
Confidential information Cardiovascular Center OLV Aalst
PPGindex 0.86PPGindex 0.45PPGindex 0.28
Focal CADCombined CADDiffuse CAD
Collet et al. JACC 2019 in press

Epicardial Resistance and PCI
PPGindex 0.95 Post-PCI FFR 0.97
PPGindex 0.36 Post-PCI FFR 0.83
Pre PCI
Pre PCI Post PCI
Post PCI
Foca
l CA
DD
iffu
se C
AD
17%
12% 9%
0.4%
Reduction of epicaldial resistance
97%
Reduction of epicaldial resistance
23%

Epicardial Resistance and PCI
PPGindex 0.95 Post-PCI FFR 0.97
PPGindex 0.36 Post-PCI FFR 0.83
Pre PCI
Pre PCI Post PCI
Post PCI
Foca
l CA
DD
iffu
se C
AD
17%
12% 9%
0.4%
Reduction of epicaldial resistance
97%
Reduction of epicaldial resistance
23%

PPG index and post-PCI FFR
PPG Index and FFR post PCI
N = 53
Slope = 0.21
Intercept = 0.76
r = 0.69 (95%CI 0.51 to 0.81)
P < 0.001
PPG Index and Functional Gain
N = 53
Adjusted R2 = 0.72 (95%CI 0.50
to 0.86)
P < 0.001
Mizukami T, Collet C et al. Under revision

iFR Pullback
Kikuta JACC Intv2018


Stent
Collet et al. Nature Reviews 2018.
Baseline LM PCI Mid LAD PCI Mid + distal LAD PCI
FFRCT Revascularization Planner in MVD

Macro-circulation Macro and Micro-circulation

Patel MR et al. N Engl J Med. 2010.
398,9
78 p
atients
Noninvasive testing 83.9%
Diagnostic Yield of Elective Coronary Angiography

Macro-circulation Macro and Micro-circulation

Methods to diagnose MVD
Non-invasive Invasive
Thermodilution
Doppler
Spasm provocation test
PET/SPECT
Doppler LAD
MRI
CT Perfusion

0
10
20
30
40
50
60
70
80
90
100Invasive-CFR Invasive-IMR Non-Invasive
Prevalence of Microvascular Dysfucntion
Pro
po
rtio
n (
%)

Prevalence of Microvascular Dysfunction 47% (CI 95% 34 to 59%)
Comprising 14073 patients included in 24 studies undergoing invasive and
non-invasive assessment
I2 99.5%
4,22
4,11
4,18
4,16
4,17
4,15
4,17
4,22
4,2
3,99
4,14
4,16
4,12
4,22
4,11
4,15
4,22
4,22
4,23
4,22
4,18
4,17
4,18
4,1
Collet et al. Under revision

14% of the screened patients had moderate to severe
ischemia and NOCAD
Approx. 40% of the patients in the invasive arm remained
symptomatic (diffuse disease?, MVD?)

Prevalence of Microvascular Dysfunction
Lee et al. Circulation 2015.

PET derived CRF and MBF
Gupta A et al. Circulation. 2017 Dec 12;136(24):2325-2336.
CFR independent predictor of cardiovascular mortality

CMD PathwaysMicrovascular Dysfunction
Macrovascular Dysfunction
Non-endothelium dependentCFR in response to adenosine
< 2.5
Change in coronary artery diameter in response to
nitroglycerine < 20%
Endothelium dependentChange in CBF in response to
acetylcholine < 50%
Change in coronary artery diameter in response to
acetylcholine ≤ 0%
Coronary spasmChest pain + ECG change + Change in coronary artery diameter
in response to acetylcholine < 90%

Methods to diagnose MVD
Bolus thermodilution Continuous thermodilution
Index of Microvascular Resistance Absolute Microvascular Resistance and Flow

Ford TJ et al. JACC 2018

Ford TJ et al. JACC 2018


Conclusions
• The evaluation of patients with chronic coronary syndromes is
advancing to better identify patients that benefit from
revascularization.
• For patients considered for PCI, the characterization of the
pattern of CAD (PPG index) predicts functional complete
revascularization.
• The evaluation of the microvascular compartment can further
personalise medical management and improve symptoms.

Conclusions
An epicardial ‘luminogram’ as tool to diagnose, decide
upon and treat CAD is sub-optimal. A functional
evaluation of both epicardial and microvascular
compartments is required to understand identify disease
endotypes and individualize therapies.