New Models of Care...New Models of Care Supporting General Practice through Community Pharmacy Garry...
65
New Models of Care Supporting General Practice through Community Pharmacy Garry Myers & James Roach Supported by a research grant from the National Pharmacy Association Garry Myers is Executive Partner in Jaunty Springs Medical Practice and is a practising community pharmacist operating community pharmacies in Sheffield & North Derbyshire. James Roach is Managing Director of Conclusio Ltd. Previously CEO Mid Essex CCG and Joint Health & Social Care Director Local Authority/NHS Wiltshire. EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL 1 Community Pharmacist Crispin Bliss delivering integrated care
Transcript of New Models of Care...New Models of Care Supporting General Practice through Community Pharmacy Garry...

New Models of Care Supporting General Practice through Community Pharmacy
Garry Myers & James Roach
Supported by a research grant from the National Pharmacy Association
Garry Myers is Executive Partner in Jaunty Springs Medical Practice and is a practising community pharmacist operating
community pharmacies in Sheffield & North Derbyshire.
James Roach is Managing Director of Conclusio Ltd. Previously CEO Mid Essex CCG and Joint Health & Social Care
Director Local Authority/NHS Wiltshire.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �1
Community Pharmacist Crispin Bliss delivering integrated care

Executive Summary Case for Change
Demand Outstripping Supply
• As the population has aged, it has become more dependent on health services. • An additional one million people over the age of 75 predicted in the next ten
years, according to the Secretary of State for Health & Social Care . 1
• Approximately 40% of the NHS budget is currently spent on care for older people, according to the Nuffield Trust, with this figure set to grow because of the increasing health demands of this group . 2
• The Nuffield Trust has highlighted that on the basis of recent projections from the Office of Budgetary Responsibility there will be a £30 billion gap between actual spending and what is required to effectively “stand still “ and meet the growth in demand by 2020. The NHS Five Year Forward View acknowledged this gap, and put in place a plan to deliver £22bn of efficiency savings by 2020 . 3
GP workforce under pressure
• In spite of an additional 5000 GPs being promised we have actually seen a net reduction of 1,300 FTEs in the number of GPs, with numbers of GPs in post - way below the Government’s own projections and targets , . 4 5
• The age demographic of Partners and Salaried GPs means more GPs are leaving the profession each year and a high number of GP practices are now closing (450 practices have closed since 2013 impacting 1.3m people) . There is growing 6
concern that the aspirations of the GP Forward View are diverging from the reality faced by clinicians and patients, urgent intervention is now required.
• Reducing number of trainees (more than 600 GP training vacancies across the country) and new entrants . 7
• A recent survey suggested that more doctors would prefer to be a locum or a salaried doctor rather than a GP partner and there has been an increase in the number of GPs reducing their weekly sessional commitments . 8
The potential of Community Pharmacy
Nationally, Community Pharmacy remains a resource that creates significant opportunity in terms of scale and clinical expertise and could provide a solution to the emerging financial, clinical and demand challenges in the NHS and social care in that : 9
• There are around 11,500 community pharmacies in England . 10
• Each pharmacy serves a catchment population of approximately 5,000 people.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �2

• It is widely quoted that 1.6m people walk into a pharmacy every day meaning that on average a pharmacy will deal with approximately 136 patients without an appointment every single day.
• Many of these pharmacies are open extended hours and many are open over 85 hours a week. In almost all cases, access to a pharmacy will be far easier than a GP.
New Models of Care - Community Pharmacy
The Prime Minister’s Challenge Fund in Sheffield
Funding was made available through the Prime Minister’s Challenge Fund (PMCF), for a 4-hour session of pharmacist time each week to support participating GP practices in Sheffield. The work programme of the pharmacist was intended to free up GP time and provide quality & service enhancement.
Jaunty Springs
Jaunty Springs Medical Centre is located at the heart of a post war housing estate in the suburbs of Sheffield. It has a list size of around 3,600 patients and its population is generally older than the Sheffield and England average.
Dedicated Community Pharmacy support time was provided by Basegreen Pharmacy to support and enhance the existing General Practice model. This practice has a formal Partnership Agreement in place between the Community Pharmacy, with the lead community pharmacist being a partner of the practice.
Jaunty Springs Integrated Care Model
Through IT integration and a formal Partnership Agreement between the Community Pharmacy and the General Practice, the Community Pharmacist was able to undertake appropriate consultations within the Community Pharmacy setting. Read/write access to the full GP Clinical Record enabled real time information sharing and allowed the community pharmacist to make full use of their training and knowledge as the NHS medicines expert.
Patients were proactively directed towards the pharmacy as a source of care, reducing demand on the practice, and improvements in the patient experience as they were able to be seen more quickly as the community pharmacist was more readily available.
The vast majority (67%) of pharmacist time was spent providing face to face direct consultation with patients, with the remaining 33% of time spent reviewing and updating patient care plans and pathways through the GP clinical system. The pharmacy team was
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �3

also working to enhance the ongoing safety and efficiency of Community Pharmacy services. Our evidence suggests that the activity undertaken in the Community Pharmacy setting reduces pressure and redirects demand away from the GP surgery.
Key Benefits to the Health System
Community pharmacy support for General Practice through this integrated approach can: • Create more capacity in primary care through a highly scalable model (9.45%). • Reduce average waiting times to be seen in a primary care setting, reducing
pressure on the whole GP team. Average waiting times at the practice were significantly lower than either the local or national average.
• Release GP time by utilising the expertise of the community pharmacist to deal with medicines related issues, e.g. drug availability problems.
• Support patients in taking their medicines - enhancing adherence. • Support quality and safety of prescribing within the practice. • Enhance patient outcomes, continuity and seamlessness of care between GP
Practice and Community Pharmacy - leading to better coordinated management of Long Term Conditions.
• Eliminate prescribing errors at source, and in real time by allowing the Community Pharmacist to access the full GP record.
• Increase support for frail elderly patients in their own home, and those residing in nursing homes on the Registered List.
• Support the best management and use of NHS resources through appropriate prescribing, improved adherence and reduced waste.
• Provide access to real time access to cost effective prescribing advice & support. • Change patient behaviour, making pharmacy first port of call for a range of
conditions. • Reduce A&E activity (-7.5%). • Utilise existing therapeutic relationships and a network of highly accessible
pharmacists.
Quantitative Benefits to the Health System
• More than 1,000 interventions were carried out by the Community Pharmacist during a 9 month period (36*4 hour sessions).
• From the pilot it was demonstrated that every 4 minutes of pharmacist time, saves approximately 2 minutes of GP time, whilst also improving quality. This finding is consistent with another recent study by Williams et al, which demonstrated the same ratio of GP time saved . 11
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �4

• For every day of dedicated Community Pharmacist support for General Practice, one whole session of GP clinical time is created, meaning an additional 25 patients can see their GP every week.
• There is enormous potential to scale this model as there are 11,500 community pharmacies in England. If every pharmacy were to provide just one day of clinical support to General Practice each week, it would release in excess of 18m GP appointments per year - the equivalent of 1,200 WTE GPs.
Key Conclusions
NHS England policy focuses on the role of the Clinical Pharmacist in General Practice. Pharmacists in General Practice alone are not the solution to the GP capacity crisis, current data shows that there is only one clinical pharmacist for every 30,000 patients.
The Jaunty Springs Integrated Care Model demonstrates that the Community Pharmacy team can provide care at scale, offering a cost effective alternative or supplement to the Clinical Pharmacists in GP Practice Programme. Furthermore, in our integrated model the whole Community Pharmacy team is responsible for a cohort of around 4,000 patients weighted for age and other characteristics, from the point of view of pharmacist access alone, this is nearly 8 times more accessible. Our model brings the additional benefits of utilising existing patient and professional relationships and breaking down silos within the health system, which combined have led to improved trust and confidence in the clinical input of the Community Pharmacy team.
Ready Reckoner: Impact of 1 day (8 hours) of dedicated Community Pharmacy Support for General Practice each week:
Jaunty Springs England
Interventions per annum (per day of Community Pharmacy support/ week)
3,062 interventions could be undertaken by the community pharmacy team.
35.2m interventions per annum based on one day of community pharmacy support per week (11,500 pharmacies).
GP Capacity Released
0.178 WTE GPs/practice 1,213 WTE GPs 9.45% of GP appointment capacity.
A&E attendances -7.5% 1.154m attendances saved annually
Care homes admissions
-20%
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �5

Operational integration between Community Pharmacy and General Practice can be delivered through existing IT capabilities, supported by a template Memorandum of Understanding to govern data sharing between Practices and Pharmacies. The Jaunty Springs Model has benefited from a formal Shared Care Agreement setting out the roles and responsibilities which underpin this shared care arrangement.
The opportunities are not only to release vital GP capacity, but also to enhance the safety, quality and efficiency of medicines taking across the health system. The Community Pharmacy network provides an opportunity to make real system change, and address policy priorities such as the need to reduce A&E attendances and hospital admissions from care homes. This new model of working has been credited with helping to save Jaunty Springs practice from closure, and could be adapted to work elsewhere in a highly scalable solution.
For further information please contact: [email protected]
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �6

Foreword This is not an academic research paper. Rather it is a summary report on, and in some ways the culmination of the experiences of myself and my Community Pharmacy team over the last 10 years since we entered into a partnership agreement at Jaunty Springs Health Centre. At the time, this arrangement was probably unique, and was triggered by the very real threat of closure of the Jaunty Springs Health Centre practice which in turn threatened the viability of our nearby Basegreen Pharmacy.
In the early stages of our collaboration we merely provided managerial & operational support to the practice. As the capabilities of SystmOne developed with the advent of mobile clinical systems access, it became possible to evolve and expand the scope of our support to eventually deliver a seamless & integrated clinical care model.
In this paper we examine the performance of the practice in several strategic areas, as well as the specific outputs from the Prime Minister’s Challenge Fund project in Sheffield. Due to the way that we work, it is particularly difficult to disentangle our integrated approach to show precisely what impact each part of the system has made. We have attempted to provide a flavour of our model, and to support this with as much information as we have available in an open and transparent sharing of information. We are certain that the practice would not be in as healthy position as it is today without the integration of the Community Pharmacy Team.
It should be noted that a form of legal, structural integration originally facilitated our ability to develop this model. However, in our experience it would be feasible for others to utilise a formal Shared Care Agreement to achieve similar results, without the need for legal or structural integration.
We set out to explore the potential to use Community Pharmacy differently - to explicitly support General Practice, and to provide better and more integrated care for patients.
• We have established that read-write access to GP Clinical Systems is already feasible within a Community Pharmacy setting, and adds significant value to both GP practice and pharmacy.
• The availability of routine access to the GP Clinical System is the key enabler to unlocking the potential of Community Pharmacy to deliver more advanced and holistic clinical care.
• Our advanced skill mix model uses the full capabilities of the whole of the Community Pharmacy team, and it does so in a way which utilises existing relationships with patients and GPs.
• We believe that our collaborative approach is more cost effective and ultimately preferable to the NHS England Clinical Pharmacists in General Practice model
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �7

because it does not require practices to take the risk of directly employing additional staff.
• We demonstrate as a prelude to reform of the Community Pharmacy Contractual Framework, that it is possible for pharmacies to work around funding incentives that reward prescription volume and procurement margin in order to support practices with the growing burden of primary care sustainability.
• Our experience tells us that the point of supply of medicines is the best opportunity to influence and manage patient behaviours in the context of Medicines Optimisation. This is entirely consistent with Hepler’s principles of Pharmaceutical Care . 12
• This is an integrated model of care which is readily scalable and deliverable right now.
This report details no service specifications, because there are none. Our modus operandi is integrated care because we believe that a holistic approach is the best for the patient, and in the long term for the Health Service. Through alignment of priorities, sharing of information and respect for the skills and clinical competence of the Community Pharmacy team, we work together almost as a single organisation with a single purpose.
Our journey can act as a roadmap for others who are ready and willing to rise to the challenge. The benefits are self-evident - working together in this way has contributed to making the practice not only sustainable, but in many ways flourishing, while the pharmacy enjoys the positive contribution it can make to patient care. At its simplest, Community Pharmacy access to the GP Clinical Record has saved 1-2 hours per day of GP time for our Practice. It is my view that this number is highly scalable, but requires a will from policymakers.
We urge policymakers to expand their thinking when it comes to the utilisation of Community Pharmacy to support General Practice. Alignment of funding and contractual mechanisms between GP and Pharmacy Contracts is a logical step forward. It is clear to me that a move towards a registration-based Pharmacy Contract cannot come soon enough, in order to release the latent potential of the Community Pharmacy network which sees more people every day than any other part of the National Health Service.
Finally, I would like to acknowledge the work of my team, to which this way of working is now second nature, their dedication and skill continues to change lives and improve outcomes. That is why I am so passionate to see our learning disseminated and replicated in other areas.
Garry Myers Managing Director; Shires Pharmacies Limited Executive Partner; Jaunty Springs Medical Practice. May 2018
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �8

Table of Contents
Executive Summary 2 Demand Outstripping Supply 2
GP workforce under pressure 2
The potential of Community Pharmacy 2
The Prime Minister’s Challenge Fund in Sheffield 3
Jaunty Springs 3
Jaunty Springs Integrated Care Model 3
Foreword 7
Section 1: Context 11 Demand versus supply in the NHS 11
General Practice workforce under pressure 11
General Practice Nursing Crisis 12
The potential of Community Pharmacy 13
The Prime Minister’s Challenge Fund in Sheffield 14
Jaunty Springs Integrated Care Model 15
National Pharmacy Association Innovation Programme 15
Section 2: Jaunty Springs Integrated Care Model 17 Summary of the Model 17
Key Opportunities 17
Clinical consultations 18
Clinical review and coordination 18
Developing effective working relationships with the GP practice 18
Outline of the service delivery model 19
Methodology 20
Section 3: Results & Evaluation 21 General Practice Capacity 22
Return on Investment 23
Access to a GP 24
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �9

Types of Intervention 25
Prime Minister’s Challenge Fund 26
A&E Attendance 26
Hospital Discharge 28
Patients in Care Homes 29
QoF Achievement 30
Demand Management 31
Patient Experience 32
Prescribing Costs & Quality 33
Use of Repeat Dispensing (eRD) 34
Other Prescribing Indicators 35
Primary Care Integration 36
Community Pharmacy Team 36
Patient Safety 37
Section 4: Conclusions & Recommendations 39 Key Findings 39
Potential Economic Benefits 39
Comparison with Clinical Pharmacists in General Practice Programme 40
Developing a new type of business model (mutuality) 42
Enabling IT Access to GP Clinical Software 43
Enhancing Safety & Quality 44
Contractual & Payment Mechanisms 44
Patient Perspective 45
Acknowledgements 60
Bibliography 62
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �10

Section 1: Context
Demand versus supply in the NHS
As the population has aged, it has become more dependent on health services. We have seen:
• An increase in the number of patients with multi-morbidities; the National Institute for Health Research estimates that two thirds of people over the age of 65 will be living with three or more Long Term Conditions by 2035 . 13
• An increase in the number of patients with moderate to severe frailty. • A significant decline in the number of elderly patients able to undertake one or
more self-help tasks. • An additional one million patients over the age of 65 predicted in the next ten
years.
The Nuffield Trust has highlighted that on the basis of recent projections from the Office of Budgetary Responsibility there will be a £30 billion gap between actual spending and what is required to effectively “stand still“ and meet the growth in demand.
The Five Year Forward View acknowledged the funding gap and put in place a plan in which the NHS would deliver £22 billion of efficiency savings by 2020.
General Practice workforce under pressure
The General Practice Forward View (NHSE, 2016) recognises some of the key issues in 14
efficiently and effectively managing the frontline demand and supply of healthcare in the UK. The rise in Long Term Conditions and the ageing population has impacted by increasing demand for Primary Care. GP & nurse consultations increased by an estimated 10.5% between 2007 - 2014 (Hobbs et al, 2016) and nurse consultations by 150% 15
between 1996-2008 . 16
There are significant reductions in the numbers entering General Practice as a career, and a high rate of turnover of those working in the profession . (Baird et al, 2016) In addition, 17
the GP workforce is ageing, with 50% of GPs reaching retirement age by 2020 in Somerset, Lincolnshire and Essex (iNews, 2017). The Government’s own research shows 18
that 39% of all GPs have a considerable/high intention of leaving patient care within the next five years, amongst GPs over 50 this number is 61% (Gibson et al, 2017). 19
The GP workforce 10-point plan (NHSE, 2015) acknowledged that GP practices were 20
recruiting pharmacists and laid out plans for a national pilot launching in 2015 with the first pharmacists working in General Practice on the pilot scheme by 2016. This scheme is
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �11

currently underway and evaluation taking place. The GPFV action plan confirms that this is seen as a long-term solution and sets out that by 2020 there will be 10,000 more medical professionals working in general practice with real term budget rises of up to 15% (NHSE, 2017).
Research shows that 27% of general practice appointments are avoidable. This equates to around 40 million appointments per year in England, and many of these people could have gone to their local pharmacy (NHSE, 2018). Currently, up to 18% of general 21
practice workload is taken up dealing with patients suffering from minor ailments at a cost of £2bn (Vibhu et al, 2013) . Meanwhile, a retrospective review demonstrated that 8% of 22
A&E attendances could be managed by community pharmacists (Family Practice, 2015). 23
Despite the Government’s promise of 5000 extra GPs overall by 2020, the actual number of GPs has fallen by more than 1000 (Pulse, 2018). The Secretary of State for Health has 24
admitted that he is struggling to fulfil this commitment (Mahase, 2018). 25
There has been a generalised increase in practice waiting times (with average waiting times as high as two weeks in some areas).
General Practice Nursing Crisis
The shortage of GPs nationally is exacerbated by the shortage of district nurses, community nurses and practice nurses across the country. A recent report commissioned by the Health Foundation in 2017 highlighted : 26
• Nationally there was a shortfall of 22,000 nurses specialising in caring for adult
patients (this is circa 10 % of the workforce). • By 2020 the shortage will be 38,000 nurses.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �12
Challenges Include: • The GP forward view projections not being met. In spite of an additional 5000
GPs being promised, we have actually seen a net reduction in the number of GPs, with numbers of GPs in post way below the Governments own projections and targets. Age demographic of partners and salaried GPs in certain parts of the country means more GPs are leaving the profession each year and a high number of GP practices are now closing
• Reducing number of trainees and new entrants. • Change in professional preferences; a recent survey suggested that more
doctors would prefer to be a locum or a salaried doctor rather than be a GP partner and there has been an increase in the number of GPs reducing their weekly sessional commitments.

• 49% of nurses currently in post don’t think there are sufficient staffing levels to enable them to do their job properly.
• The number of district nurses in England fell by almost half between 2000 and 2014 and fell by a further 15% between 2014 and 2016 for full time posts.
• Most regions have 1 in 5 posts unfilled. • Latest available data on recruitment show that the NHS filled one nurse job for around
every 7 posts advertised across England in the 3 months up to June 2017. All of this generates a tsunami effect with significant downstream pressure being placed on GP surgeries and A&E with the increased possibility of patient safety being compromised. The traditional contingencies for General Practice are now in short supply and this further supports the need to look at a more expansive primary care support model with community pharmacists at the centre. One of the aims of this report is to demonstrate that practical changes to the workforce model can free up GPs to focus on the care of the most complex patients and on diagnostics. Overall working in this way leads to a more holistic model of Shared Care.
But this requires a change in mind set and an open willingness to utilise the skills and experience of other clinical professionals such as a community pharmacist and at least sign up to the principle that...
The potential of Community Pharmacy
Nationally community pharmacy remains a resource that creates significant opportunity in terms of scale and clinical expertise and could provide a solution to the emerging financial, clinical and on-demand challenges for the NHS and social care. The New NHS Alliance wrote:
• There are nearly 11,500 community pharmacies in England. • Each pharmacy serves a catchment population of approximately 5,000 people. • It is widely quoted that 1.6m people walk into a pharmacy every day meaning that
on average a pharmacy may have 136 people that walk in without an appointment every single day.
• On average patients have 14 interventions /contacts with a community pharmacist per annum. The community pharmacy infrastructure is uniquely placed to work with general practice to free up capacity and develop a more sustainable model.
• Many of these pharmacies are open extended hours and many are open over 85 hours a week.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �13
Any patient who could be well managed by the community pharmacy team should be referred there to reduce practice workload, improve the patient experience and encourage positive patient behaviours towards
self-care and care management.

• Community pharmacists have the clinical competencies and skills to undertake more patient consultations.
• All pharmacists have significant clinical training within their degree course and pre-registration training. This is further developed in Community Pharmacy practice and through Continuing Professional Development.
• The NHS England Clinical Pharmacists in GP Practices Programme has recruited 60% of its pharmacists from Community Pharmacy.
• Virtually all community pharmacies have an area reserved for confidential conversations with people away from the main counter area. These private consultation rooms have been extensively used within the NHS England commissioned Medicines Use Review (MUR) and New Medicines Service (NMS).
• Pharmacies offer a competitive unit price per intervention and a considerable delivery scale given the wide distribution of pharmacies in neighbourhoods across the country.
The Prime Minister’s Challenge Fund in Sheffield
There has long been local recognition of the important role community pharmacies play in delivering primary health services in Sheffield, such as support in minor ailments, drug misuse, and smoking cessation.
As part of the Prime Ministers Challenge Fund programme (PMCF), funding was made available in Sheffield to fund a 4 hour session of Community Pharmacist time each week to support participating GP practices. The work programme of the pharmacist was intended to free up GP time and provide quality enhancement by including the following menu of tasks: repeat prescription management, discharge medicines processing and liaison across primary care, structured medication reviews, shared care monitoring requirements, supporting patients with long term conditions and complex medication issues, supporting patients in residential care. It should be noted that whilst 4 hours of sessional time was funded through the PMCF, this was in addition to the ongoing work of the Community Pharmacy team to support the GP practice at the Jaunty Springs site.
An evaluation of the scheme, published by Sheffield Hallam University in November 2016, found that having specialist input for medicines management was overall deemed to be a quality, as well as a time-releasing, innovation. 18,044 individual activities were carried out under the scheme between October 2015 and July 2016 . However, there 27
was a considerable variation in uptake by the practices. Only one fifth of practices were consistently high users – among which was the Jaunty Springs Medical Centre who fully utilised the opportunities associated with this programme. The evaluation found that the Primary Care Pharmacy Programme delivered the following benefits (Sheffield Hallam, 2016):
• Improved patient outcomes on long term medication. • Reduced prescribing spend.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �14

• Reduced medication related admissions/readmissions. • Released GP time. • Tested the benefits of working with more clinically focused community
pharmacists.
Jaunty Springs Integrated Care Model
Jaunty Springs Medical Centre is situated in the middle of a post war housing estate in the suburbs of Sheffield. Situated at the heart of its community, with a list size of around 3,600 patients and a population which is generally older than the Sheffield and England average, with 25.9% of patients aged 65 and over, compared to around 17% in England and 16% in Sheffield. Levels of deprivation are around the England average but life expectancy for both males and females is slightly lower than the England average.
Around two thirds of the practice’s patients have a long-standing health condition compared to around half in England and Sheffield. This difference seems to be driven by conditions such as chronic heart disease, heart failure, diabetes and COPD.
Dedicated Community Pharmacy support time was provided by Basegreen Pharmacy (operated by Shires Pharmacies Limited) to the GP practice to support and enhance the existing General Practice model. This practice had a formal Shared Care Agreement in place between the community pharmacy and the GP Partners, with the lead community pharmacist being a partner in the practice.
National Pharmacy Association Innovation Programme
This report was commissioned as part of the NPA’s Innovation Programme to examine the overall experience and service delivery model at Jaunty Springs Medical Practice.
The aims of the NPA Innovation Programme are to : • Improve access to General Practice and encourage new models for delivery of
primary care services. • Test a wider range of innovative ideas such as extended opening hours, more
ways for patients to access services, and new services to better support patients with complex needs.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �15
A notable feature of the Jaunty Springs integrated care model, is that the vast majority of the interventions were made from the Community
Pharmacy consultation room, rather than on the premises of the GP practice.

• Examine how community pharmacy can play an even stronger role at the heart of more integrated out-of-hospital services that delivers better heath outcomes, more personalised care, and excellent patient care.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �16

Section 2: Jaunty Springs Integrated Care Model
Summary of the Model
The core ethos of the Jaunty Springs Integrated Care Model is that any patient who could be managed in a community pharmacy should be referred there to reduce practice workload, improve the patient experience and encourage positive patient behaviours towards self care and care management.
The practice operates a formal Shared Care agreement with nearby Basegreen Pharmacy to provide care services from its Community Pharmacy premises. This is enabled by IT links to the practice, and dedicated time for the Community Pharmacist to provide support services to the practice.
Key Opportunities
• Creating more capacity for patients to be seen in primary care by a Community Pharmacist.
• Reduction in average waiting times to be seen in a primary care setting, made possible by the Community Pharmacist having the ability to book patients in and see them in the Community Pharmacy consulting room.
• Release GP time by a medicines expert (the community pharmacist) performing tasks that would ordinarily be carried out by GPs.
• Focused support for patients in taking their medication, enhancing adherence and optimising the benefits of the therapeutic regimen.
• Support General Practice prescribing with the provision of expertise from an aligned community pharmacist.
• Enhanced patient outcomes & continuity of care and coordinated management of long term conditions and increased support for frail elderly patients in their own home and those who reside in the one large nursing home that forms part of the GP Practices’ Registered List.
• Redefining and maximising the potential of the patient-pharmacist relationship.
• Support the best management and use of NHS resource through appropriate prescribing, improved adherence and reduction of waste.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �17

To this end, in partnership with the GP team, the Community Pharmacist was able to deliver a range of evidenced quality improvements as a consequence of the community pharmacist undertaking the following tasks:
Clinical consultations
• Booked consultations with patients – for the treatment of minor ailments and illnesses.
• Focused support and coordination for patients with long term conditions and complex medication needs, including case reviews, therapeutic drug monitoring and titration of doses.
• Supporting elderly patients by undertaking home visits and providing wider support to patients living in the large local nursing home.
• Delivering structured medication reviews with patients.
Clinical review and coordination
• Management, coordination and review of repeat prescriptions • Leading on the review and processing of discharge medicines and liaising with several
clinical teams from across the system in ensuring patients are supported to remain in their place of residence
• Ensuring evidence-based prescribing in the GP practice
Developing effective working relationships with the GP practice
Shared care arrangements were developed between General Practice and Community Pharmacy. This helped to improve operational and clinical links, as well as risk management between the General Practice and the Community Pharmacy.
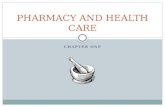
The vast majority of pharmacist time (67%) was spent providing face to face direct consultation with patients, with the remaining 33% of the time spent reviewing and updating patient care plans and pathways, through access to the GP clinical system. In all instances the Community Pharmacist was working with a Pharmacy Technician to ensure the ongoing safety and efficiency of the Pharmacy dispensing service. This is summarised in the Figure 1 below;
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �18
In each of these areas there was the added quality benefit associated with comprehensive review of the medication pathway by the community pharmacist and the ability to eliminate medication or prescribing errors at source through in-pharmacy read write access to GP clinical systems.

Outline of the service delivery model
• The Community Pharmacy had access to the Practice’s SystmOne from the Pharmacy consultation room, using an appropriately configured smart card and the existing Pharmacy N3 connection.
• The Community Pharmacist having such read/write access to the system is able to update the patient record in real time and share that information with the GP.
• In depth medicines data analysis led by the Community Pharmacist. • Patients were given the choice of healthcare professional in either the Practice or the
Community Pharmacy and this was significant in managing and reducing the demand being faced by the Practice.
• The full Community Pharmacy team consisted of 2 Community Pharmacists (1FTE, one of whom was an independent prescriber), 2 Dispensers, 1.5 WTE Accuracy Checking Technician and a Medicines Counter Assistant. Two Pharmacists and one Pharmacy Technician had access to the GP Clinical System.
• Pharmacists & Technicians were bound by surgery confidentiality agreements and were considered ‘part of the practice team’. This allowed them to access patient medical records for the purposes of their work for the surgery. Full sight of the patient medical record by the pharmacist enabled a more in-depth intervention informed by knowledge of condition(s), recent test results and medicines being prescribed. Access to the clinical record also enabled more efficient communication with GPs and pharmacists being able to communicate via the system using the ‘task’ facility.
• Patients were booked an appointment to see the Community Pharmacist using SystmOne.
• The Community Pharmacist referred back to the practice when: ▪ Clinical input of the GP was required. ▪ Patient required blood tests.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �19
Figure 1: Proportion of Community Pharmacist time during evaluation on different activities.
Patient pathway reviews via GP system33%
Patient facing medication & prescription management42%
Booked Community Pharmacy consultation25%

▪ Patient requires spirometry or wound care from Practice Nurses. ▪ Patient requires referral to the District Nurse. ▪ Appointment required with other members of the healthcare team.
Methodology
During the evaluation, Community Pharmacists recorded the amount of time they spent on each activity. Data was recored on the PharmOutcomes platform between 6/10/15 -1/7/16. The majority of interventions were carried out directly by the Community Pharmacist, but some activities were managed by other members of the pharmacy team: Pharmacy Technicians and Dispensers.
Due to the limitations of the data gathered for the PMCF evaluation, we have reviewed the effectiveness of the practice in a number of other key areas relating to medicines and clinical performance. Whilst we cannot claim a definitive causal link between the actions of the community pharmacy team, and the performance of the practice, it should be remembered that Jaunty Springs Medical Practice was threatened with closure before the formal partnership with the pharmacy was initiated.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �20
This model enabled the community pharmacist to support the practice from the community pharmacy and negating the need for physical co-location, structural integration and practice infrastructure investment.
Community Pharmacy/
Pharmacist
GP Surgery Admin Team -
Practice Manager or Reception.
GP Surgery Clinical Team -
GPs, Nurses, HCAs, Phlebotomist,
Medicines Management
Figure 2: Workflows between General Practice and Community Pharmacy setting.

Section 3: Results & Evaluation Data for the Financial Year 2016/17 was reviewed retrospectively to examine the effectiveness of the Jaunty Springs Integrated Care Model on a number of strategic indicators. Where possible the practice’s performance was measured against local and national comparators.
It was anticipated that additional pharmacy support at Jaunty Springs would provide the following benefits:
General Practice Capacity
• Free up GP time and create additional capacity for the Practice.
• Free up the GP to diagnose and manage more complex patients.
• Improve QoF performance for the Practice.
• Reduction in GP waiting list and average wait times.
• Optimising skills and knowledge of the wider Practice team. "
"
"
"
!
Demand Management
• Reduction in hospital admissions.
• Reduction in A&E attendances.
• Divert patients from the General Practice waiting list to appropriate consultation with the Community Pharmacist.
• Educate patients about the role and value of the expanded primary care team to produce long term behaviour change.
"
"
"
"
Patient Experience
• Improve the patient experience through reduced waiting times to see a healthcare professional.
• Improved experience by maximising the amount of time patients can spend with a healthcare professional.
• Improvements in patient safety through use of the Community Pharmacists & Pharmacy Technicians.
• Focused support for patients to get the best from their medicines. "
"
"
!
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �21

General Practice Capacity
As part of Prime Minister’s Challenge Fund activity in Sheffield, interventions made by community pharmacists were recorded. Data relating to Jaunty Springs was extracted by Pinnacle LLP. Key assumptions to support these calculations can be found in Appendix 2.
The pilot has demonstrated that it is possible to improve General Practice capacity through the use of dedicated Community Pharmacy support.
At a time when there are simply not enough GPs to meet the rising demands of the population, there appears to be a strong case for utilising the clinical skills and scalability of the Community Pharmacy network. If every Community Pharmacy were tasked and empowered to support General Practice as at Jaunty Springs, the capacity created could be of the order of 1,200 WTE GPs for every full day of Community Pharmacy support.
Jaunty Springs Pilot Data
Interventions per 4 hour ‘session’ 29.44
Interventions per 8 hour working day 58.88
Total number of interventions during pilot (36 x 4 hour sessions) 1060
Community Pharmacy time per intervention 8.15 minutes
GP time saving per intervention 4.03 minutes
Total GP time saved through Community Pharmacy intervention during pilot.
71.2 hours
Capacity released per full day (8 hours) of Community Pharmacy Support each week
GP hours saved 3.95 hours
Potential number of additional 9.4 minute GP appointments created each week
25.32
GP capacity released each week (WTEs) (1 FTE GP = 37.5 hours/wk) for each Community Pharmacy providing support
0.105
Appointments saved in England if all community pharmacies offer 8 hours of dedicated support for General Practice per week
15.141m
Potential appointments released per practice per year (6793 practices) 2,229
WTE GPs saved in England per annum per day of CP support 1,213
Potential increase in GP appointment capacity at an average practice 9.45%
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �22

Return on Investment
At a ratio of 2 minutes of Community Pharmacy Support time to save 1 minute of GP time this is a cost effective option to create additional capacity in General Practice. Funding for the pilot was £36/hour, and was ostensibly to cover the cost of locum backfill for community pharmacies.
Return on Investment calculation using the formula:
This shows that during the pilot a 106% Return on Investment was achieved versus the cost of the traditional GP-only model of care provision . 28
There were also additional economic benefits resulting from the integrated care model, resulting from direct drug cost savings, and potentially improvements to the quality of care & outcomes, as well as negating some of the consequential costs associated with delays to treatment, but these were not measured as part of the PMCF pilot, or as part of routine service monitoring at the practice. Bush et al found an ROI of £4.73 per pound invested, using the same methodology , these savings included consequential savings 29
such as drug costs which were not captured as part of the PMCF study. It is likely that a similar overall ROI could be achieved using the Jaunty Springs model, although more data capture may be warranted.
Jaunty Springs Pilot Economic Efficiency
Total value of GP time saved (71.2 hours * £150/hr Cost/hr of GMS) [9 months] (A)
£10,680
Total Cost of Community Pharmacy Support (inc data collection) PMCF pilot [9 months] (B)
£5,184
Net saving from pilot (value of GP time - total cost) [9 months] (A-B) £5,496
Cost per Intervention £4.89
Return on Investment 106%
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �23
Net Savings (A-B)
Costs (B)= Return on
Investment
It is likely that the true Return on Investment of the Jaunty Springs Integrated Care Model is many times the investment made, however with the limitations of this study mean that it is not possible to show the full impact of the Community Pharmacy Support on system costs.
Due to the IT link between Basegreen Pharmacy & Jaunty Springs practice, it was possible to provide these interventions from the Community Pharmacy premises, meaning that any future service would be deliverable without the need for locum backfill, which would potentially increase the ROI significantly.

Access to a GP
Typical waiting times for a non-urgent appointment at Jaunty Springs Medical Practice is 2 - 3 days. Many GP practices are now offering non-urgent appointments with waiting times in excess of two weeks, and with forecasts lengthening due to increased demand, and reducing numbers of GPs. This means that patients at the practice can be seen quicker when they need to be, enhancing not only clinical outcomes, but also the patient experience. Diverting demand to Community Pharmacy, and educating patients about the value & skills of the Community Pharmacy team can pay long term dividends for both patients and the health system: for patients the greater availability of on-demand access to a healthcare professional; and for the NHS and General Practice in particular both defrayed demand and cost.
GP trade publication Pulse, regularly runs a survey of its readers to understand current waiting times for non-urgent appointments. It shows that only around one quarter of practices were able to offer these types of appointments in under a week. The vast majority of patients are left waiting for longer than a week to see a GP. For working people in particular, there is an economic impact in terms of lost productivity, and income. It is in the interest of society and the wider economy for people’s health needs to be addressed in a timely fashion.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �24
GP appointment waiting times - present vs 12 month forecast
0%
10%
20%
30%
40%
Under 1 Week 1-2 weeks 2-3 weeks 3-4 weeks 4-5 weeks >5 weeks
2016 How long is the average waiting time for a non-urgent appointment at your practice? n=831
2016 How long do you predict the average waiting time for a non-urgent appointment at your practice will be in 12 months’ time? n=785
2017 Non-urgent appointments n=837
Jaunty Springs 2-3 days
Figure 3: Pulse Magazine GP Waiting Time Survey 2016 - 2017

Types of Intervention
During the PMCF pilot, the Community Pharmacist was involved in a range of interventions. The most common type of intervention was the provision of ad hoc advice to patients, GPs and other members of practice staff (71%, n= 787). The opportunity for staff and patients to ask the advice of the NHS medicines expert is invaluable to the practice as it helps to avoid the need for GP appointments, as well as helping to resolve problems quickly.
The next most frequent intervention (19%, n= 206) was the clinical re-authorisation of one or more medicines, this is an essential safety mechanism which is designed to check and challenge unnecessary prescribing. If the pharmacist did not undertake this activity it would require input from the GP to make the clinical decision to re-authorise the medicine.
Although other types of intervention occurred at a low frequency (1-3%) this reflects the more in-depth and time consuming nature of some of these activities, such as full clinical medicines reviews, or support for a discharge, which can require long consultations with patients. This activity can be extremely valuable in helping to resolve complex issues, saving the GP’s time, and adding value by focusing in on medicines related problems which can cause readmissions to hospital.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �25
1%
2%
1%
19%
2%
71%
3%
Medicines ReviewAd Hoc AdviceSupporting DischargePrescription Re-authorisationMedicines ReconciliationOther Clinical Activity Referral
Figure 4: Interventions during PMCF evaluation period by type.

Prime Minister’s Challenge Fund
During the 9 month Prime Minister's Challenge Fund period, Basegreen Pharmacy was funded to provide 36 sessions of clinical support to Jaunty Springs Medical Practice (1 x 4 hour session per week). Interventions were logged on the PharmOutcomes data collection platform.
It is important to note that although the Pharmacy was only funded to provide one session of clinical support each week, because of the extremely close working relationships between practice and pharmacy the actual amount of support, and interventions provided are much higher than the recorded figure. This reflects changes in patient and professional behaviours because of the new model of integrated care. Independent Prescribing was not considered an integral component to this model, but was considered an enhancement, as it magnified the impact of the effectiveness of the Community Pharmacy team, as a wider range of clinical workload could be managed by an individual with the prescribing skillset. It would also improve the ratio of Pharmacy Support to GP time saved from the current 2:1 ratio.
The Pharmacy was funded at a rate of £36/hour from the PMCF, including some recognition of the costs of data capture and recording. Total funding from the PMCF amounted to £5,184 for Basegreen Pharmacy during the evaluation period, resulting in a cost of £4.89 per intervention, NHS unit costs for other interventions using 2016/17 data are presented for comparison (Kent, 2018).
A&E Attendance
Given the financial and demand stresses on the acute healthcare system, primary care should be viewed as an opportunity to reduce active demand on Accident and Emergency Departments.
Data from the Jaunty Springs practice shows a very favourable performance compared to both the Sheffield and NHS England A&E attendance trends.
Comparative Intervention Costs
PMCF Pharmacist cost/intervention £4.89
Costs of Nurse-led telephone triage (2016/17) £6.10
Cost of GP-led telephone triage (2016/17) £14.60
Cost of GP Consultation inc Prescription (2016/17) £29.30
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �26

This performance has been delivered despite an above average number of frail elderly people under the care of Jaunty Springs Medical Practice, and despite a 3.9% growth in the number of people over the age of 65 on the practice list. The reduction in A&E attendances is greater than the small drop in the Registered List at the Practice, suggesting that improvements to the quality of care realised through the Practice’s service delivery model are having a real impact on the local health economy.
The potential cost savings to the health system if this performance can be replicated elsewhere are enormous. NHS Improvement’s Reference Costs for 2017 show that each A&E attendance costs £148.36 . A 7.5% reduction in A&E attendances could be worth 30
£231m to the taxpayer, based on 2016/17 figures.
2014 -2015 2016 - 2017 % change
Jaunty Springs 1,265 1,170 -7.5%
Sheffield Teaching Hospitals 144,748 147,640 2.0%
NHS England 19,556,781 20,866,411 6.7%
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �27
Figure 5: A&E Attendance rates at Jaunty Springs Practice over time
50
60
70
80
90
2013 Q4 2014 Q1 2014 Q2 2014 Q3 2014 Q4 2015 Q1 2015 Q2 2015 Q3
A&E Attendance rates Jaunty Springs Practice

Hospital Discharge
Community Pharmacists supported the discharge of patients from hospital by reviewing the patient’s medication requirements and coordinating care planning with other parts of the system. Not only did this help to smooth out the process, but it also helped to improve safety by eliminating prescribing errors at source. According to the National Patient Safety Agency in 2007, between 30% and 70% of patients can have either an error or an unintentional change to their medicines when care is transferred from one setting to another . This can cause impacts such as increased costs, worse care and 31
readmissions for patients. The Community Pharmacy team was not only involved in helping to support discharges, but also Medicines Reconciliation, to help improve patient safety by removing unnecessary or out of date medicines from patients medicines cabinets at home.
A recent study by Parekh et al showed that 37% (n=413) of older people discharged from five teaching hospitals in Southern England experienced medicines related harm post-discharge (556 events per 1000 discharges). 336 (81%) cases were serious and 214 (52%) were preventable. Four patients suffered fatal consequences as a result of medicines. Medicines related harm was responsible for 78 readmissions per 1000 discharges. The study estimates that medicines related harm costs the NHS around £396m per annum, of which £243m is preventable . Increasing the uptake of post-discharge Medicines Use 32
Reviews, or commissioning of a specialist service such as the Discharge Medication Review (DMR) service in Wales, could be potentially cost effective measures to help reduce preventable medicines related harm. The work at Jaunty Springs practice demonstrates the value of an integrated, longitudinal approach to medicines safety.
Community Pharmacies are generally open for longer hours than practices, they are well situated to help with discharge of patients which can happen at any time during the week. One of the limitations of NHS England’s Clinical Pharmacists in GP Practice Programme is that pharmacists are typically shared across several practices, or working on a part time basis, meaning that there can often be a delay between a patient being discharged and their medicines being reviewed by the pharmacist. In addition, Community Pharmacists and their teams have existing longitudinal relationships with patients, which can provide important context to clinical problems and potential solutions.
This pilot suggests that the Community Pharmacist was able to (a) make discharge more efficient as they were to more quickly translate changes made during the patient’s hospital stay onto their ongoing medication record; (b) were able to reduce the risk associated with transfer of care setting. Further quantitative data should be collected in future to measure these impacts both in terms of service and quality improvement, as well as financial savings.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �28

Patients in Care Homes
Evidence from a number of sources demonstrates that by focusing clinical support on patients over the age of 75, a reduction in demand on Urgent & Emergency Care can be achieved, which in turn leads to financial savings for the health system. Nursing Home residents registered at Jaunty Springs practice benefited from joint Medication Reviews undertaken by the Community Pharmacist & GP with the aim of:
NHS England has also reported that Vanguard projects have including Pharmacists in Care Homes, have produced solid results : 33
The work carried out by the Community Pharmacist at the Practice and in visits to the Care Home is very similar to that carried out by Pharmacists in Care Homes, and it is likely that similar impacts would be achieved by the Jaunty Springs model, although this was not directly measured as part of the Prime Minister’s Challenge Fund data collection, or by the practice as part of its internal audit and evaluation activity.
The value in using a Community Pharmacist to review these patients is that it is more joined up, meaning that actions can be followed through reliably to the end user, and enables longitudinal follow up with residents they will be involved in the care of for long periods of time. This potentially improves upon the NHS England Care Homes Pharmacist model which appears to follow a snapshot approach with the pharmacist shared by lots of different care homes, giving limited opportunity for follow up or longitudinal care.
• Reviewing patient’s medication needs.
• Providing nursing home residents with the appropriate level of clinical support and supervision for their care setting.
• Supporting and coordinating clinical aspects of patient discharge from hospital.
• Providing advice to care home staff.
NHS England Vanguards Jaunty Springs equivalent
Emergency Hospital Admissions -21%
Ambulance Call Outs -30%
Drug Cost Savings £125-£305/resident £3,250 to £7,930
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �29

QoF Achievement
Jaunty Springs Medical Practice out performs both the NHS Sheffield CCG and National average for QoF achievement. This is in part due to the clinical model which it employs, with GP capacity released through appropriate use of the wider primary care team.
Although the large improvement in QoF performance in 2015/16 pre-dates the Prime Minister’s Challenge Funding, the practice has been operating its formal relationship with Basegreen Pharmacy since 2008. The practice takes collective responsibility for QoF performance, and the pharmacy team in particular have taken direct responsibility for improving QoF performance.
While the exact causal relationship behind Jaunty Springs’ improved QoF performance is a matter for debate, it makes empirical sense that reducing demand on the practice, and its clinical staff by referring workload to the Community Pharmacy will create an environment where the Practice team can have more time to focus on areas such as QoF, therefore improving practice performance.
Detailed Disease Registers for Jaunty Springs Medical Practice versus local and national averages can be found in Appendix 2.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �30
Jaunty Springs QoF Performance
QoF
Poi
nts
490
500
510
520
530
540
2014/15 2015/16 2016/17
Jaunty SpringsNHS Sheffield CCG (average)NHS England (average)
Figure 6: QoF Performance - Jaunty Springs vs local & national averages

Demand Management
The Primary Care Foundation (Carson, 2009) reports that there are approximately 100m 34
same day appointments made each year. At that time this represented approximately one third of total General Practice capacity. Jaunty Springs Integrated Care Model saw practice staff making referrals directly to the Community Pharmacy for many different acute problems, such as:
• Coughs, colds and sore throats. • Exacerbations of Long Term Conditions, such as COPD. • Management of calls from nursing and residential care. • Management of medication problems and queries. • Management of drug shortages.
Evidence from the pilot has demonstrated the following outcomes for patients:
Outcome % of patients
Seen by Community Pharmacist with no need for onward referral or prescription.
85%
Referred to GP (including under shared care agreements). 5%
Patient managed in other ways e.g. “See, treat & complete” where prescriptions issued directly by Independent Prescriber.
10%
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �31
Case Study - Community Pharmacist Input into Practice QoF Activity
“My main area of work was upon disease registers for QOF and improving performance against QOF indicators. The surgery started out with 412 points and by the end of my time we had got it up to 470 out of 530 points. This involved checking that all suitable patients that met the criteria were on the correct registers. Often this would mean going through hospital letters and old consultations to correctly Read code for the original diagnosis“…
“As part of this I would also take part in various disease audits. I did these upon Atrial Fibrillation, Dementia, Cephalosporin and Quinolone prescribing, childhood Asthma, and DMARDS. So, through doing the audits I would link that in to work upon QOF since I would often be looking at a specific disease area and therefore the same patients. This would also then raise questions as far as some things that needed changing for best practice such as blood tests which would then require a change to the template the surgery used.”…
Crispin Bliss, Community Pharmacist Independent Prescriber

We believe that this service has helped to educate patients about how they can use the Community Pharmacy team, rather than attending a GP or A&E, this may help to limit “health seeking” behaviour in the long term.
In addition, NHS England estimates that between 5 and 8% of unplanned hospital admissions are due to medicines . Often the full course of prescribed medicines is not 35
taken because of failure to monitor and properly encourage and instruct patients. This, in turn imposes additional costs because conditions are not properly treated and become more serious (Frontier Economics, 2014). Integrating the accessibility of the Community 36
Pharmacist with the Practice’s systems has opened up opportunities to make things better and more convenient for patients. For example the ability to see the pharmacist during their longer opening hours, and for a wider range of conditions has meant patients being seen more quickly, reducing the costs of escalation associated with deteriorating health conditions.
Patient Experience
One of the key drivers for working differently at Jaunty Springs has been the desire to maintain good access for patients seeking healthcare advice and treatment. Patient surveys from the Practice were reviewed to understand patient’s feelings about the new model of service delivery. Common themes were identified:
Access:
Outcomes:
“This was a very quick and impressive service”.
“Useful to have access to evening appointments”.
“Really useful to have availability of appointments”.
“Really good to be able to come after work”.
“Extended opening hours are a big help as I work full time”.
“I was impressed at the speed I got my appointment today”.
“If I didn’t get this appointment and things persisted I would have gone to A&E”.
“I was booked to see the Community Pharmacist quickly, and was offered an appointment that day, otherwise I would have travelled to the hospital”.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �32

Anecdotally, patients were very happy to have a consultation with the local Community Pharmacy. A finding which is consistent with a University of Nottingham study into Community Pharmacy Independent Prescribers which reported “patients now actively seek out the CPIP as an alternative to the GP” (Mann et al).
Prescribing Costs & Quality
Jaunty Springs has one of the largest populations of elderly people across Sheffield. Whilst this has an adverse impact on total cost, when relative measures such as cost per ASTRO or Star PU is used, practice costs compare favourably with others across Sheffield. Figure 7 below shows the distribution of practices across Sheffield CCG by ASTRO PU, showing that Jaunty Springs prescribing costs are within the top quartile for efficiency (lowest costs per prescribing unit).
"
Due to the integrated nature of the Practice-Community Pharmacy relationship at Jaunty Springs Practice, there is a deep cultural and philosophical partnership when it comes to the use of medicines. This did not begin with the Prime Minister’s Challenge Fund, and it did not stop at the end of that pilot. The GPs routinely call upon the advice and expertise of the Community Pharmacy team to help them make prescribing not only cheaper, but also better and safer.
In a number of key prescribing performance indicators the Practice is performing well versus its local contemporaries. It is our belief that this is at least in part due to the deep cultural and professional integration between the Practice and the Pharmacy, but we cannot prove this categorically without further academic evaluation.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �33
Figure 7: Prescribing Costs per ASTRO PU NHS Sheffield CCG

Use of Repeat Dispensing (eRD)
Electronic Repeat Dispensing offers a different mechanism to allow patients on regular, long term medicines to obtain their medicines without having to reorder from the practice each time. With eRD a repeatable electronic prescription is created and can be accessed from the nominated pharmacy either at set intervals, or on demand. This reduces the administrative burden associated with repeat prescription management for practices. Pharmacies are required to ask questions of the patient when they collect the medicine to make sure that they still need it, and that nothing else has changed with their pharmacotherapy. The pharmacy has the responsibility to reduce waste of medicines.
The Department of Health & Social Care has agreed with the General Practitioners Committee of the British Medical Association (GPC) to a target of 25% of repeat prescriptions to be managed through eRD. Jaunty Springs performance is already well in excess of this level, twice the Sheffield average, and four times the NHS England average.
In 2002 it was estimated that as much as 80% of repeat prescriptions could be suitable for electronic Repeat Dispensing, which could save as much as 2.7m hours of GP and Practice admin time . At Jaunty Springs high use of eRD is enabling staff to focus on 37
other areas of activity such as QoF and direct clinical care.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �34
0
10
20
30
40
Jaunty Springs NHS Sheffield CCG NHS England
Precentage of eRD items
National Target
Figure 8: Uptake of electronic Repeat Dispensing.

Other Prescribing Indicators
Antibiotic Prescribing
Given the increasing prevalence of antibiotic resistant infections, all healthcare professionals have a duty to reduce unnecessary use of antibiotics. In the elderly the use of broad spectrum antibiotics can also have serious adverse effects, such as the spread of infections such as C.difficile. The practice has managed to reduce its rate of antibiotic use, and is in the top third of practices in Sheffield CCG for this measure. The close relationship between the Practice and the Community Pharmacy team means that the pharmacist can frequently intervene to ensure that antibiotic therapy is both indicated and safe. Jaunty Springs managed to reduce antibiotic prescribing rates by 3.6% during the evaluation period versus the previous year, this is one of the largest drops in the Sheffield area.
Measure Jaunty Springs Relative Performance
Analgesic Prescribing 7.6% reduction Well above Sheffield average
Antidepressant Prescribing Rate
3.9% increase Smaller increase than Sheffield average
Pregabalin Cost Changes 1.2% increase Increase in costs below Sheffield average
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �35
Antibacterial Prescribing Rate / STAR PU
0
0.085
0.17
0.255
0.34
2015 Q1 2015 Q3 2016 Q1 2016 Q3 2017 Q1 2017 Q3
Jaunty SpringsSheffieldEngland

Primary Care Integration
Working together in this model has brought many unforeseen benefits to both the Practice and the Pharmacy, such as improving the way that Medicines Use Reviews (MURs) work alongside health checks for the elderly. The GP and the Community Pharmacist have been able in some instances to conduct joint reviews, allowing them to produce and implement a truly integrated care plan. By improving this communication all parties believe that the effectiveness of care has been improved, with significant additional value being created for an MUR.
Another example of how the Community Pharmacist has been able to support the GP to prescribe effectively is through the management of drug shortages. Real time information sharing has helped to smooth care pathways and make the patient journey more efficient, as well as saving the GP time, this has helped to minimise the cost implications for the practice.
Community Pharmacy Team
During the pilot, 70% of activity was undertaken directly by the Community Pharmacist, with 30% undertaken by the supporting Pharmacy Technicians (under the supervision of the pharmacist). In the clear majority of cases, patients received face to face advice and support.
The typical division of labour across the Jaunty Springs model is shown below:
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �36
GP
Community Pharmacist
Pharmacy Technicians
Dispensers/Support staff
Diagnosis, treatment, complex care.
Treatment, routine care & minor illness triage.
Medicines reconciliation, support for discharge, dispensing.
Supply of medicines, Over The Counter medicines.
Figure 11: Workforce roles and responsibilities.

This division of labour has helped patients to be able to spend more time with their healthcare professional, with typical appointments with the Community Pharmacist lasting on average 30 minutes. This has allowed the pharmacist to take a more structure and in-depth approach to reviewing the patient.
The PMCF pilot has demonstrated the value of the advanced skill mix employed by the Community Pharmacy team at Basegreen pharmacy. The pharmacy uses a ‘Maximum Facilitation’ model where all staff are trained to the highest level, and all tasks are delegated down to the most suitable level. This operating model does not require any changes to legislation, although many pharmacy owners have disinvested from employing and training Pharmacy Technicians due to cost, which could be a barrier to some.
Patient Safety
The routine presence of the Community Pharmacy Team as part of the extended practice team has brought safety benefits to patients. Many of the interventions captured as part of the Prime Minister’s Challenge Fund related to the safety of ongoing repeat prescriptions. Activities such as medicines reconciliation, where the Pharmacy team compares the medicines that the patient has at home, versus their current repeat prescription, help to avoid the risk of inadvertent errors. Helping to upskill patients with additional education and information as as result of Medication Reviews, or longer individual consultations helps to reduce the risk of unintentional errors.
We have already referred to the importance of handover between care settings at admission and discharge - the Community Pharmacy team is well placed to help with the transfer of information, which was easily affected by their access to the full GP clinical system. This helped to eliminate errors with prescriptions at source. No data was examined about relative error rates at Jaunty Springs practice versus other similar practices or local comparators, but this would be worthy of further evaluation.
Safety is not just about one measure, but about the accumulation of marginal gains from lots of different activity. In this respect the Jaunty Springs Integrated Care Model should be considered a success as it has built medication safety into the culture of the practice. It is not easy to measure this improvement, but the commitment to safety is easy to observe in a holistic sense: reduced A&E admissions, reduced hospital admissions for Care Homes residents, good quality prescribing indicators, integration between GP and Pharmacy teams.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �37

EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �38
Case Study: Crispin Bliss, Community Pharmacist Independent Prescriber
I was running my regular anticoagulation clinic, and my patient arrived. I noticed immediately that his skin was slightly yellow, a symptom of jaundice. We discussed when this symptom had started, and he confirmed that it had come on pretty quickly 2 weeks earlier, when his brother pointed it out to him. The patient thought nothing more of it because the discolouration had faded and he hadn’t felt unwell.
I booked the patient in for a full set of blood tests the following day, and the receptionist managed to book him a same day appointment with the GP at my request.
The patient was given an urgent 2 Week Wait referral and a scan was organised.
We are awaiting the further developments, but the jaundice has continued to develop and the patient has been feeling quite lethargic recently.
This recent example really underlines how I can make a difference clinically to my patients, and how our model of integrated care can improve patient care.

Section 4: Conclusions & Recommendations
Key Findings
Potential Economic Benefits
In Summary:
• Integrated Care Model can free General Practice capacity by more than 10% per day of Community Pharmacy Support.
• Improved QoF performance for the Practice.
• Low GP waiting list and average wait times.
• Reduced number of hospital admissions compared to local and national trends.
• Reduced number of A&E attendances.
• Divert patients to Community Pharmacy, reduce demand on Practice.
• Improve patient safety through holistic medicines management.
• Strong prescribing performance against key targets.
• Harness longitudinal patient relationships & knowledge of Community Pharmacy teams.
• Key enablers: 1. Formal Shared Care Agreement between Practice & Community Pharmacy providing structure to working relationship. 2. Access to GP Clinical Software.
In Summary:
• Create equivalent of 1,200 WTE GPs per day of Community Pharmacy Support.
• Create an additional 17.73m GP appointments per year per day of Community Pharmacy Support.
• Reduce A&E attendances by up to 7.5% annually.
• Reduce hospital admissions from care homes by 21% annually.
• Reduced Practice operating & infrastructure costs.
• Reduce costs associated with patient safety incidents.
• Reduce costs associated with delays to treatment & lost productivity.
• Reduce costs associated with Clinical Pharmacists in General Practice Programme.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �39

Comparison with Clinical Pharmacists in General Practice Programme
In 2015 NHS England launched the first wave of it’s Clinical Pharmacists in General Practice Programme (CPGPP), which sought to embed pharmacy knowledge within General Practice teams. It was recognised that utilising the skills of Pharmacists & Pharmacy Technicians to improve the use of medicines within Practices would help to improve outcomes with medicines, and would provide a vital boon to General Practice at a time when numbers of GPs was falling and expectations & demands of the public were rising.
The current deployment of CPGPP suggests that there is one Clinical Pharmacist for a population of around 30,000 people. Added to this there was a significant training and development programme, as well as evaluation which further reduced the availability of those pharmacists who were already in post. In reality this means that even by 2020 when the CPGPPP model is fully deployed, there will only be on average of one day of pharmacist support for each practice (c7000 patients) each week. It is difficult to see how this scale of activity and manpower can have a significant impact on the seismic pressures facing General Practice.
In many ways the Jaunty Springs model is the natural evolution of CPGPP in that proof of concept that Community Pharmacy teams can handle caseload and therefore reduce pressure on overstretched GPs. The Jaunty Springs integrated model takes this programme forward to demonstrate that those pharmacists do not need to be physically co-located with GPs.
The Jaunty Springs model operates at a much more realistic scale, with the Basegreen Pharmacy team supporting a Weighted Registered Population of around 4,000 patients. Extending this model to more of the 11,500 Community Pharmacies in England provides a scalable solution which could have a dramatic impact on GP workload. In addition, there are potential economic benefits to this model over the NHS England CPGPP model, in that practices and the NHS end up bearing the cost of higher Professional Indemnity Premiums as a result of siting pharmacists within the practice, and also the cost of NHS Superannuation which is not insignificant. The ability to access and write to GP Clinical Software means that it is not even necessary for the Community Pharmacist to even leave the pharmacy, which makes the cost of this model substantially cheaper than the CPGPP model.
We recognise that the impact of the Community Pharmacist was improved to an extent by their ability to prescribe and alter drug therapy as a result of Independent Prescriber status. Any expansion of this model should consider this a very important enabler not only to advanced practice, but also a larger impact on GP capacity. NHS Scotland has just announced that it will be funding Community Pharmacists to undertake Independent Prescribing training, in a move which is highly resonant with our experience . Another 38
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �40

critical enabler was the IT infrastructure as discussed, and the formal Shared Care Agreement, which will be discussed in greater detail later in this report.
As there was no need for physical co-location of the pharmacist, the Jaunty Springs Integrated Care model would not put further pressure on the primary care estate within General Practice, which is already struggling to cope with the demands which are being placed upon it.
Research for the National Pharmacy Association shows that the public question the logic of concentrating more activity within GP Practices, as they are seen as a bottleneck and already operating at full capacity. Indeed, the logic of asking patients to go to their Community Pharmacy as their first port of call, is well understood and adopted. In some respects the CPGPP model flies in the face of this logic and public understanding. Empowering Community Pharmacy teams to deal with a wider range of conditions and activities as we propose supports the Pharmacy First message, and helps to stop patients from needing to contact or access their GP Practice. By utilising Community Pharmacists, who are already regarded as trusted, and as the most accessible NHS healthcare professional the NHS would be able to rely on the existing relationships between patients and their pharmacies/pharmacists, rather than seeking to create new relationships under the CPGPP. Our evaluation demonstrates that it is possible to achieve changes in patient and public behaviour to reduce ‘health seeking’ behaviour.
For GP Contractors, the appeal of the CPGPP is limited as it provides only a proportion of funding on a declining scale over three years before eventually stopping altogether. This leaves GP businesses with additional liability in terms of Employers National Insurance, Superannuation and Indemnity Insurance. These additional liabilities may have stopped some practices from examining closer working with Pharmacists. Avery has questioned the longevity of the NHS England CPGPP approach, arguing that unless the funding formula is changed the scheme may fail . Under the Jaunty Springs model, these costs 39
all sit with the Community Pharmacy provider, who is able to provide the professional knowledge & skills of the pharmacist at a marginal cost.
To reiterate we believe that the CPGPP model has been a helpful development which has proven the value and effectiveness of pharmacists in helping to reduce workload on hard-pressed GPs. But we believe that our evaluation shows that it is possible to achieve many of those benefits from an existing workforce, operating from the Community Pharmacy setting, making it ultimately cheaper and more scalable as a solution which could have a dramatic impact on GP sustainability.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �41

Developing a new type of business model (mutuality)
Community Pharmacies supporting General Practice can create a “win-win” situation for all parties, and could provide a critical opportunity given the demand on primary care. The Jaunty Springs - Basegreen Pharmacy partnership could be best described by Figure 12 below:
"
The key enabler for the Jaunty Springs model of care has been the formal Practice Agreement between the Practice & the Community Pharmacy provider. This agreement formalises the relationship and gives it status and credibility in business, financial and clinical terms. Critically the establishment of the governance framework means that no formal structural or legal integration is required, making this model both feasible and highly scalable.
The agreement:
• Outlines the core role of the Community Pharmacist.
• Defines the construct of the Practice team.
• Confirms and formalises the Shared Care arrangements that is in place between the Community Pharmacy and the GP.
• Protects the clinical freedoms of each clinical professional.
• Manages conflicts of interest.
• Demonstrates in practical terms how the Community Pharmacist can support the GP to deliver their obligations under the PMS/GMS contract.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �42

The Shared Care Agreement should evolve to cover emerging issues such as data quality, and Prescription Direction. It may also benefit in providing clarity about Shared Care roles with respect to diagnostics and treatment initiation, to make clear where accountability rests. New legislation such as the General Data Protection Regulations (GDPR) should be reviewed to understand the implications for data sharing across organisations which happens under the Jaunty Springs Integrated Care Model.
There is a clear opportunity for national organisations to work together to produce a template Memorandum of Understanding which Practices & Community Pharmacy providers could use to explore an Integrated Care Model.
Enabling IT Access to GP Clinical Software
It must be remembered that while GPs host and curate the patient’s electronic health record, ultimate ownership of this data rests with the patient themselves. The formal Shared Care Agreement between the Practice and the Pharmacy has helped to create a governance framework to allow the Community Pharmacy team to access the full GP-held record.
All pharmacies have access to an NHS N3 Connection, and would be technically able to access the GP system provided that the necessary hardware and software was in place. The Jaunty Springs model demonstrates that through the use of a relatively inexpensive laptop with the GP software installed, it is possible for Community Pharmacies to fulfil a much wider remit in helping to reduce demand on GP practices. The ability for the Community Pharmacy to remotely access the GP clinical record, and to write to them, has helped to avoid the need for structural integration, or costly physical co-location. Although it is true that GP practices within each locality may use different GP systems, most CCGs have ‘Systems of Choice’ in place, which should limit the number of different GP systems which pharmacies would have to access. Neither GP practices or Community Pharmacies have the luxury of waiting until technical solutions to system interoperability are resolved, our approach is rooted in a pragmatism which is already delivering results for patients and organisations. It should also be noted that CCG Medicines Management teams already have the ability to remotely access GP systems.
The programme has also demonstrated that Community Pharmacy teams are able to use GP held records appropriately, and in the patient’s best interests. This has enhanced not only the patient’s care, but also the holistic safety of the system when it comes to the use and management of medicines. Dr Richard Vautrey, Chair of the BMA General Practitioners Committee (GPC) recently called for a workforce strategy across Primary Care, which should included greater involvement of Pharmacists “working in, or linked to practices and surgeries”.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �43

There is an opportunity for national organisations to work together to help produce a template Shared Care Agreement which will cover aspects of information sharing.
Enhancing Safety & Quality
The Secretary of State for Health has recently spoken about the need to reduce and eliminate the 700 preventable medicines-related deaths each year which happen in the NHS . 40
The longstanding integration between Practice & Community Pharmacy at Jaunty Springs has had significant impacts on prescribing quality, costs and outcomes. We have demonstrated that an integrated approach helps to reduce prescribing errors at source, particularly when patients move to and from hospital or managed care settings.
Interventions made by the lead Community Pharmacist have for example resulted in improvements in the dosing for an anticoagulant (rivaroxaban), as he is now able to accurately adjust dosing now that he has access to the GP clinical system as he can now calculate the patient’s renal function.
Data from the Prime Minister’s Challenge Fund showed that more than 700 interventions were made in a 9 month period to give ad hoc advice and support to patients and members of staff. We shouldn’t underestimate the importance of these spontaneous conversations which help to embed the expertise of the pharmacist as the NHS medicines expert, firmly in the minds of clinicians and patients. This can only help to improve safety in the long run. The Community Pharmacist has helped to take some of the administrative and workload burden off the GPs in the practice which has helped to keep those GPs available as and when patients need them. This has meant shorter waiting times for appointments which in turn means faster treatment and fewer consequential costs associated with delays, or time off work.
GPs are spending more time with patients, and patients are spending more time with the Community Pharmacist talking to them about medicines, which leads to a virtuous circle of health improvement.
Contractual & Payment Mechanisms
The Jaunty Springs Integrated Care model has demonstrated the value of both working together, and working differently. Despite a small amount of funding from the Prime Minister’s Challenge Fund in 2016/17, there has been no formal recognition of the investment made by Basegreen Pharmacy to operate this model. The organisations have naturally come together to work in this way because they believe it is the right thing to
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �44

do for patients. This alignment has been critical to building the trust and understanding required to work in such a radically different way.
The national contracts for both Community Pharmacy and General Practice should in the future, reflect the value created when the two professions work together. Our experience has shown that it is possible for Community Pharmacy providers to operate against the incentives created by the current contract which is almost entirely driven by prescription volume, and purchase margin. We would recommend that greater consideration is given to exploring alternate payment and contractual mechanisms which underpin closer working relationships for the benefit of patients. In time the Community Pharmacy Contractual Framework (CPCF) should be completely re-designed and recommissioned to ensure complete alignment of Community Pharmacy funding drivers with those of both Practices and the wider NHS. This requires the abandonment of the existing volume & margin driven CPCF funding model.
The Pharmacy Integration Fund should consider supporting the training of more Community Pharmacists as Independent Prescribers, as they have recently announced in Scotland. It should also consider how it can be deployed to help more pharmacies to work as we have with their GP practices, as this is a win-win-win-win for the GP, Pharmacy, NHS and patient.
Patient Perspective
When healthcare services are designed we need to put ourselves in the position of the patient to understand what the services 'looks and feels like’. As a result of the model operated by Jaunty Springs Practice patients experienced a number of quantitative and qualitative benefits.
• Improved access for those patients who urgently need to see the doctor, patients were also given the option of seeing a Community Pharmacist.
• Able to see a highly competent clinical professional in a Community Pharmacy setting.
• Freeing up GPs to diagnose and manage complex healthcare needs.
• Average waiting times below the national average. Typically 2-3 days as opposed to 2 weeks in some areas for a non-urgent appointment.
• Patients with chronic health needs were seen by the most appropriate healthcare professional, who had the time and the information at their disposal to provide high quality care and appropriate medication support.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �45

• Supported patients in understanding and managing their condition and keeping them independent - giving them more control over their treatment and health.
• Working in partnership with patients to help maximise the benefits from their therapeutic regimen.
• Educating patients about the benefits of appropriately accessing a Community Pharmacist to support self care.
• Seamless care for patients because of the integration of pharmacy and GP providers. This means less ‘bouncing’ between provider for the patient and hopefully solving the patient’s need first time.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �46

Recommendations
Key: BMA - British Medical Association DHSC - Department of Health & Social Care GPhC - General Pharmaceutical Council NHSE - NHS England NPA - National Pharmacy Association PSNC - Pharmaceutical Services Negotiating Committee RCGP - Royal College of General Practitioners RPS - Royal Pharmaceutical Society of Great Britain
Reference Recommendation Organisations
1.1 National organisations to work together to produce template Share Care Agreements to underpin operational and clinical partnership working.
BMA, NPA, RPS, RCGP, PSNC.
1.2 National organisations to work together to facilitate routine access to GP Clinical Software for Community Pharmacies, subject to appropriate governance.
BMA, PSNC, RPS, GPhC, GMC, RCGP.
1.3 National organisations to work together to develop a joint strategy and service model for Primary Care.
NPA, PSNC, BMA, RCGP.
2.1 Pharmacy Integration Fund to explore Jaunty Springs Integrated Care model as an alternative to the Clinical Pharmacists in General Practice Programme.
DHSC, NHSE.
2.2 Pharmacy Integration Fund to support more Community Pharmacists to become Independent Prescribers.
DHSC, NHSE.
3 Consideration be given to a new contract and funding model for Community Pharmacy to support General Practice as per Jaunty Springs Integrated Care model.
DHSC, PSNC, NHSE.
4 Further consideration be given towards the impact of the Jaunty Springs Integrated Care model on patient safety.
Academia.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �47

Conclusions
At face value it might be difficult to understand what is special about Jaunty Springs and its deep & fruitful partnership with its local Community Pharmacy. In many ways it has been impossible to understand where the Practice stops and the Pharmacy begins in order to write this evaluation. This probably sums up the cultural, philosophical and practical integration better than anything.
The Community Pharmacy and the Practice act as though it was one organisation, but without having to either physically co-locate or structurally integrate. It has done this through the deployment of a team approach, underpinned by IT links which add value to both the Pharmacy and to the Practice’s day to day operation, for the benefits of patients. A formal agreement exists to help describe the roles and responsibilities of each partner in the provision of care: this helps to avoid conflict and duplication of effort.
Our review of the data shows that through a highly integrated and holistic approach towards patient care and medicines management, it is possible to provide not only better care, but also to create a lot more capacity. We have striven to talk about this in terms of the opportunity it creates to increase timely access to healthcare, rather than talking about this as an opportunity to provide cost savings. At a time when demand for healthcare is rising due to an ageing and ailing population, and we are seeing a fall in GP numbers due to the demographics of the profession and changing career structures for younger doctors; we believe the time is ripe to do something different.
The concept of Clinical Pharmacists in General Practice is not a new one, but it has been the only model that NHS England has actively pursued for the last 3 years. Yet the model comes with a number of intrinsic limitations, most notably its ability to provide a readily scalable solution to the GP capacity crisis today. The Jaunty Springs Integrated Care Model provides an opportunity to build upon the successful elements of the Clinical Pharmacists programme, by utilising the network of 11,500 Community Pharmacies to deliver a scalable, timely and effective solution. In evaluating this model we have shown that there are clear opportunities not only to create capacity, but to improve quality and holistic patient care at the same time. g
No legislative changes are required to enable scaling of this model. The digital infrastructure exists for Community Pharmacy teams to access GP Clinical Software, but this requires a policy commitment to encourage rapid deployment.
We urge decision makers to visit Jaunty Springs to experience the power of our collective team approach, to understand that we have blurred the lines between providers in the interests of patients, and it is working. The passion and commitment of everyone involved in this project has been clear throughout, we want to bring this approach to other Practices so that they and their patients can benefit from working differently.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �48

Appendix One: Jaunty Springs Integrated Care Model - Testimonial from the Lead Community Pharmacist“When I was doing my work on acute prescriptions I would also make changes to patient’s medication based upon hospital discharges, clinic letters and prescribe new medication based upon these and set it up upon repeat prescribing where necessary. I would also do prescriptions based upon outpatient prescriptions that the patients brought in that hadn’t been collected from hospital.”
“Also during this time, I telephoned over a 100 patients to try and book them in for asthma or COPD reviews as we had found that patients had a habit of ignoring the many recall letters sent to them for reviews so I thought a more direct approach might illicit a better response. As part of this I also did asthma and COPD reviews, performing spirometry where necessary and if the patient was able. I did 11 asthma reviews and 7 COPD reviews during this time”
“My work upon acute prescribing probably saved the GP’s on average 1-2 hours a day. I calculated I sorted out 276 items, did 36 medication reviews, 57 sets of repeat dispensing prescriptions and 6 home visits and 2 lots of telephone advice.”
In undertaking the evaluation, we reviewed a number a number of patient pathways and case examples with a summary provided below of the level of support provided by the Community Pharmacist. These patient insights have been provided by the community pharmacists themselves and are displayed in the form of a relevant quote in each section.
Managing chronic disease
“A patient came in to see me who was struggling to use her salbutamol inhaler and asthma symptoms were worsening rather than sending the patient to the surgery I was able to give her an Easi-breathe inhaler which she was able to use and get her asthma symptoms under control.”
Enhancing safety through appropriate prescribing
“A patient that had repeat dispensing for warfarin that had been recently discharged from hospital upon rivaroxaban came to collect his repeat dispensing unfortunately the patients medication hadn't been updated but because I could access the surgery system I could check the discharge and remove the warfarin and stop it on the repeat dispensing.”
“On a few occasions whilst doing TTOs we have found that the list of discharge medication and changes do not agree with stated changes and current medication thus
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �49

resulting in checks with the patient or hospital ward to ensure the patient had the correct medication.”
Improving quality and reducing clinical risk
“I have also picked up in reviews that patients have dropped off hospital follow up lists like ophthalmology patients where their last consultant letter states they should be seen again in 6 months but a year later has not received an appointment.”
Providing enhanced clinical support to care homes
“The community pharmacist and the lead GP went to the local nursing home and reviewed all patients in partnership with the nursing staff to review medication where necessary. In addition to this we were able to discuss possible improvements in the medication regimes for these patients in the latter stages of dementia. During this we made multiple changes, most of them being de-prescribing based upon the Frailty Index.”
Enhancing care for patients with COPD
“Another patient I realised through review of his medication was having a lot of antibiotics for chest infections but wasn’t on the optimum medication for his COPD. I therefore decided to introduce the patient to a Symbicort inhaler alongside the tiotropium and salbutamol the patient was using. It is early days as the patient had another exacerbation soon after starting but hopefully this will improve his breathing.”
Providing enhanced support to the frail elderly
“One lady had just moved into accommodation within the surgery catchment area. I went out and did a medication review in her home and found out that her Rheumatoid Arthritis was a major problem meaning she struggled to undo bottle tops and use a standard blister pack. So following this I was able to better advise her on use of her medication and set up a NOMAD that was suitable for her so that she could continue to live independently without carers.”
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �50

Appendix 2: Additional Data
Jaunty Springs QoF Disease Registers
Jaunty Springs NHS Sheffield CCG NHS England2014/1
52015/1
62016/1
7%
change2014/1
52015/1
62016/1
7%
change2014/1
52015/1
62016/1
7%
change
Atrial Fibrillation
106 106 123 16.0 100,22 10,178 11,242 12.2 926,551 965,145 1,065,569 15.0
CHD 203 201 216 6.4 21,091 20,729 2,101 0.0 1,843,813 1,802,916 1,829,777 -0.8
Heart Failure
72 74 79 9.7 5,565 6,028 6,394 14.9 410,783 426,737 457,974 11.5
Hypertension 695 677 669 -3.7 76,282 76,190 76,879 0.8 7,833,779 7,786,738 8,028,077 2.5
Stroke 137 134 136 -0.7 11,905 11,800 11,904 0.0 981,836 979,809 1,013,462 3.2
Asthma 229 232 237 3.5 36,965 36,478 37,523 1.5 3,402,437 335,189 3,444,218 1.2
COPD 125 133 137 9.6 11,775 11,989 12,225 3.8 1,034,578 1,044,006 1,087,908 5.2
Kidney Disease
266 254 238 -10.5 21,455 20,432 19,990 -6.8 1,859,963 1,834,448 1,885,665 1.4
Diabetes 258 262 268 3.9 29,513 30,070 30,827 4.5 2,913,538 2,972,408 3,116,399 7.0
Dementia 61 63 63 3.3 4,871 5,026 5,059 3.9 419,073 428,343 443,839 5.9
Depression 275 299 325 18.2 38,830 41,706 45,603 17.4 3,305,363 3,695,035 4,187,797 26.7
Mental Health
22 22 26 18.2 5,113 5,223 5,510 7.8 500,451 507,183 534,431 6.8
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �51

Key Assumptions to Support Calculations
*Irving et al, 2017 . 41
**Information Services Division, 2013 .42
England Population 55 million
Number of Community Pharmacies in England (CPs) 11500
Population per English Pharmacy 4783
Average Practice List Size (2018 GMS) 8096
Number of English Practices 6793
Working days per annum (weekdays only) 260
Average length of GP appointment* 9.37 minutes
Standardised Practice GP appointments/week/1000 patients** 56
PMCF Pilot Data
JS Interventions per 4 hour session 29.44
JS Interventions per 8 hour working day 58.88
JS Total Interventions 1060
JS Total mins of GP time saved 4271
JS GP time saved/intervention 4.03 mins
Savings Calculations
GP Hours saved per full day of CP support 3.95 hours
Unit cost per hour of GMS time (2017) £150
Each WTE CP team saves (full time support 260 days*8 hours) £154,207 pa
If all CPs in England operate this model 5 days/week (gross) £1.8 bn***
Savings per English Practice (1.7 CPs per practice) £261,042 pa
***This calculation is for illustrative purposes and assumes that all pharmacies provide full time support for General Practice.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �52

Appendix 3 -Comparing the Clinical Pharmacist in General Practice Model with the Community Pharmacy Alternative. Stated limitation of the Clinical pharmacist model
Limitations of the Clinical Pharmacist in General Practice Model
How this model adds value
• Recruitment was challenging due to limited supply of Independent
Prescribing pharmacists in community pharmacy.
• Recruitment of Community
Pharmacist Independent Prescribers to the available posts
was more challenging than anticipated
✓ We have demonstrated that a successful model can be put in
place without absolute dependence on the independent prescriber model.
✓ There is an existing community pharmacy workforce in place
(11,500 community pharmacies in place nationally) which can add value now supporting the General
Practice from the Community Pharmacy
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �53

• Induction is vital to the success of
the scheme. This induction needs to be provided by senior GPs however there is simply not
the not time, capacity or staff base to support this. As
evidenced this has created barriers to implementation
• There is also a view that a period
of clinical shadowing would add value, but again this is time and
capacity constrained
✓ More effective provided from the
community pharmacy consulting room with appropriate IT links to the GP Practice.
✓ This model can be provided without a significant draw on the
capacity of the GP practice, does not require structural integration or physical co –location, can be
delivered within the existing skill base and competencies of the
community pharmacist and the wider support team within the community pharmacy and does
not require changes to the current law on supervision.
On the basis of current recruitment levels, there will be on average one WTE clinical pharmacist for every 30,000 patients.
The Jaunty Springs model draws on the existing accessibility and presence of the community pharmacy and on average supports a ratio of 1 community pharmacist per 4000 weighted patients. i.e. almost 8 times more accessible.
• Limited number of direct patient consultations
✓ In any one day the community pharmacist in this model would
have circa 50-60 face to face interactions with the patient in
addition to dispensing, prescribing and wider patient support
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �54

• Clinical Pharmacists worked for
varying hours in each practice, between one and four days per week. As such the model did not
provide consistent support to the GP Practice and as such its impact
was variable
✓ Community pharmacists in this
model were able to provide consistent support to the General Practice during the working week
and provide additional services during evenings and weekends
which further reduced pressure on General Practice whether it was the next working day or working
week.
✓ As the patient examples in the
report demonstrate, continued care coordination in this regard had a positive impact on patients
with long term conditions
• For patients to access the
services, skills and expertise provided by the clinical pharmacist they would still need
to attend or book through general practice. Whilst in some
regards this increased capacity it would not change patient behavior or support the
redirection of non-urgent traffic away from the GP surgery.
✓ Key to reducing demand in
General Practice and Urgent Care is to change patient behaviour in relation to accessing different
points in the health system and encouraging patients to
understand their own condition better and in time self-manage.
✓ This model achieves that by (a)
directing them to the community pharmacy for an appointment (b)
providing an opportunity to see the community pharmacist (c) develop an already enduring
relationship with the patient which adds value to the patient
and free up the GP to diagnose and manage the more complex patients on their list.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �55

Comparing stated benefits
Clinical Pharmacists in General Practice (CPIP ) Model Perceived Benefits
The Benefits of this Community Pharmacy Model
• As soon as they are in post, CPIPs can undertake medication reviews and respond to prescription
queries which immediately release GP capacity and thereby
saving money for the practice.
✓ Community Pharmacists are and can provide this service at a far greater scale away from the
practice.
• Through a scaffolded mentoring
process CPIPs can begin chronic disease reviews in the early stages (within the first 6 months)
of the role and be in a position to undertake them independently
thereafter
✓ Evidence in this report suggests
that with sufficient access to the practice system and an effective working relationship with the
general practice. Community pharmacists can provide focused
support for patients with chronic conditions in the community pharmacy. This does not require
significant input or mentoring from the GP.
• This work releases further capacity and also generates income through the Quality and
Outcomes (QOF) scheme. Practices can focus chronic
disease work around local demand and respond to strategic needs
✓ As evidence from this report demonstrates the approach has clearly demonstrated that
additional practice income through QOF can be delivered by
this model.
✓ There is a higher return on investment from this type of
general practice community pharmacy engagement.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �56

• This work releases capacity,
improves service and can have a significant impact on preventing readmissions
• Therefore, saving NHS spend in both primary and secondary care.
The evidence collected clearly demonstrates the ways in which the work of the CPIP releases
capacity for GPs and nurses. Improving Capacity was a clear
driver for the stakeholders in the scheme. The evidence supports the concept those CPIPs can have
a positive impact on the current supply-demand issues in general
practice.
✓ Similar benefits were delivered in
the Sheffield wide service;
• Saved time of 2 WTE GPs
• Saving of circa £300,000 in
staffing costs
• Reduced A&E attendances by 7.5
% (Jaunty Springs only)
• Provided circa 18,000 interactions in community pharmacy
• Positive feedback from patients and professionals
These benefits have been delivered without the need for structural or physical integration.
Unlike the NHSE GP Practice Pharmacist Programme practices do not have to take on additional NIC or Superannuation liabilities.
Using IT integration, future costs of providing support to the Practice would not require locum pharmacist backfill.
This approach would therefore be more cost-effective than the NHSE employed approach for both practices and for the Health System as a whole.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �57

• Through this programme, clinical
pharmacists can provide high quality holistic care to patients.
✓ Similar benefits can be evidenced
through this model and this is reflected
in terms of evidence from case reviews,
patient and professional feedback.
✓ The community pharmacists in this
model also helped to support and
coordinate patients discharge form
hospital in relation to review and
organisation of the discharge medicines
and on-going care support. This has
added additional value in terms of
eliminating errors at source and ensuring
that patients are on the most
appropriate and, via real time access to
drug cost & supply information, cost-
effective medications and that their care
is coordinated moving forward.
✓ This as the evidence suggests will save
money for the wider NHS in terms of
direct costs of medication and also
ensuring that a wider range of patients
are supported and are independent in
their own communities.
✓ Community Pharmacists are better
positioned to enable longitudinal care
coordination and case management in a
range of settings. This is because
Community Pharmacy teams already
have relationships with their patients
which is further developed by this
model. This type of patient – community
pharmacist relationship is key in ensuring
that patients with long terms conditions
or frail elderly patients receive
comprehensive care at the point of
need. This is as distinct from the GP
Practice model currently favoured by
NHS England where part time
Pharmacists with little prior local
experience tend to be allocated to
practices
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �58

Perceived capacity Benefits of Clinical Pharmacists in General Practice
Community Pharmacy Model
• Medication reviews were conducted by CPIPs from day 1 releasing capacity from GPs.
✓ Delivered 5+ days a week
• CPIPs visits to care homes and domiciliary environments represent a significant release of practice capacity.
✓ Yes, structured and in partnership
with GPs.
• Prescription queries, both from patients and other staff, quickly become the responsibility of the CPIP improving capacity for other staff.
✓ Provided from the community
pharmacy in real time every day.
✓ Yes, and facilitated through access to
the GP practice system.
• Chronic disease management can be delivered by CPIPs including medication reviews and adherence and condition monitoring.
✓ Achieved through direct community
pharmacist consultation with patient
(evidenced).
• CPIPs can be actively directed to follow the strategic direction of local practice needs in terms of condition management and prescribing.
✓ Can be achieved through community
pharmacy support model.
• CPIPs positively contribute to discharge management and provide a strong link between primary and secondary care and the domiciliary or care home environment(s).
✓ In this model the community
pharmacist reviews all discharge
letters, and this has reduced the
likelihood of complication and errors
and ensures patient has the most
appropriate care plan in place to
meet their needs
• CPIPs can manage acute care consultations and provide a useful back up to others offering these appointments, especially as demand fluctuates.
✓ Provided from the community
pharmacy in real time every day.
✓ Yes, and facilitated through access to
the GP practice system.
• Patients recognise the benefits on primary care capacity and are happy to have ease of access to a clinician.
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �59

Acknowledgements The original suggestion of a form of structural integration as a means of effectively saving both the Practice & Community Pharmacy from the threat of closure, came in the first instance from my close friend and longtime inter-professional collaborator Dr Richard Oliver, who is a GP in Sheffield. So, it is only right that in the first instance I should offer my thanks to Richard for his friendly advice & support throughout this whole journey.
It is however also the case that none of this would have been possible at all without the professionalism, vision and forbearance of the two original GP partners to our Partnership arrangement: Dr’s Alison Fox & Deirdre Hendra who have since retired from General Practice. My thanks to them both.
In the intervening period we have also been really privileged to have worked with an absolutely exemplary and dedicated practice team of GP’s, Practice Nurses and Receptionists and I would like to pay tribute to them all, particularly Dr’s Graham Collins & Jill Freeman.
This report is however mainly concerned with the work of our Community Pharmacy team and how they have helped to improve the operational sustainability and quality of Primary Care services delivery, via our integrated care model, to patients served by Jaunty Springs Medical Practice and Basegreen Pharmacy. This endeavour has been delivered in the face of the extreme capacity and funding crisis which is now engulfing General Practice and Community Pharmacy in England. In this regard therefore, I would offer a sincere note of thanks to the Community Pharmacy team: Crispin & Tariq (our Pharmacists), Tracy and Nicola (our ACT’s) and our dispensers and counter assistants Nicola, Paula, Zoe & Alison.
I would also like to offer additional extra special thanks to; Crispin in his capacity as our Superintendent Pharmacist and Community Pharmacy clinical development lead for his leadership, together with his clinical and technical excellence; To Tracy in her undoubtedly unique role as combined Pharmacy and Practice manager; And to Bev, Corinne & Barbara, our administrative support team. My thanks to all of them for their unstinting dedication, professionalism and sheer hard work since 2008. Their efforts have made this entire project not only possible but also a seemingly ground-breaking success.
Turning to the report’s actual compilation I would like to offer my thanks to Gary Warner at Pinnacle Health for extracting & providing the PharmOutcomes PMCF data specific to Basegreen Pharmacy, Sheffield.
I would also like to thank my co-author James Roach & his health economist colleague Jeremy Hopper for their assistance in writing, developing and working with me to refine
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �60

and finalise this report which turned all our experiences, thoughts, ideas and raw data into what you have in front of you today. My thanks also to all the team at the NPA for their advice, support, editing and formatting skills provided throughout the whole report writing process.
On a personal note I would also like to thank my close personal friends & professional colleagues Gary Warner, Mike Hewitson & Mark Burdon for their encouragement and advice during the preparation of the report.
Finally, and most importantly, I would like to place on record my appreciation of and express my love and thanks to my wife, fellow Community Pharmacist & Co-Director Anna for her love & support throughout the period following the commencement of this project of ours in 2008.
Garry Myers Managing Director; Shires Pharmacies Limited Executive Partner; Jaunty Springs Medical Practice.
May 2018
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �61

Bibliography
Hunt, J. (2018). Peston on Sunday, 25/3/18. 1
Robineau, D. (2018). Ageing Britain: two-fifths of NHS budget is spent on over-65s. [online] the Guardian. 2
Available at: https://www.theguardian.com/society/2016/feb/01/ageing-britain-two-fifths-nhs-budget-
spent-over-65s [Accessed 27 May 2018].
! NHS England (2018). NHS Five Year Forward View Next Steps. [online] England.nhs.uk. Available at: 3
https://www.england.nhs.uk/five-year-forward-view/next-steps-on-the-nhs-five-year-forward-view/the-nhs-
in-2017/ [Accessed 28 May 2018].
Health & Social Care Information Centre (2016). General and Personal Medical Services, England. [online] 4
HSCIC. Available at: https://files.digital.nhs.uk/publicationimport/pub20xxx/pub20503/nhs-staf-2005-2015-
gene-prac-rep.pdf [Accessed 12 Jun. 2018].
Health & Social Care Information Centre (2017). General and Personal Medical Services, England. 5
Provisional Experimental Statistics. [online] HSCIC. Available at: https://files.digital.nhs.uk/pdf/a/r/
general_and_personal_medical_services__england_provisional_september_2017.pdf [Accessed 12 Jun.
2018].
Wickware, C. (2018). Revealed: 450 GP surgeries have closed in the last five years. [online] Pulse Today. 6
Available at: http://www.pulsetoday.co.uk/news/hot-topics/stop-practice-closures/revealed-450-gp-
surgeries-have-closed-in-the-last-five-years/20036793.article [Accessed 30 May 2018].
British Medical Association (2017). General Practice in the UK - background briefing. BMA.7
! Wickware, C. (2018). NHS has lost 1,000 GPs since Jeremy Hunt set workforce target. [online] Pulse 8
Today. Available at: http://www.pulsetoday.co.uk/news/gp-topics/employment/nhs-has-lost-1000-gps-
since-jeremy-hunt-set-workforce-target/20036703.article [Accessed 28 May 2018].
New NHS Alliance (n.d.). Supporting the Development of Community Pharmacy Practice within Primary 9
Care. [online] New NHS Alliance. Available at: https://www.nhsalliance.org/wp-content/uploads/2016/06/
Supporting-the-Development-of-Community-Pharmacy-Practice-within-Primary-Care-NEW-LOGO.pdf
[Accessed 29 May 2018].
! General Pharmaceutical Statistics. (2018). 2007/8 to 2016/17. [online] NHS Digital. Available at: https://10
files.digital.nhs.uk/publication/h/j/gen-pharm-eng-201617-rep.pdf [Accessed 28 May 2018].
Williams, S., Hayes, J. and Brad, L. (2018). Clinical pharmacists in general practice: a necessity not a 11
luxury?. British Journal of General Practice, 68(667), pp.85-85.
Hepler, C. (2010). Pharmaceutical Care Principles and Processes. [online] University of Florida. Available 12
at: http://file.cop.ufl.edu/pop/hepler/apha/PhC_Principles_and_Processes.pdf [Accessed 15 Jun. 2018].
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �62

! Kingston, A., Robinson, L., Booth, H., Knapp, M. and Jagger, C. (2018). Projections of multi-morbidity in 13
the older population in England to 2035: estimates from the Population Ageing and Care Simulation
(PACSim) model. Age and Ageing, [online] 47(3), pp.374-380. Available at: https://academic.oup.com/
ageing/article/47/3/374/4815738 [Accessed 28 May 2018].
! NHS England (2016). General Practice Forward View. [online] NHS England. Available at: https://14
www.england.nhs.uk/wp-content/uploads/2016/04/gpfv.pdf [Accessed 29 May 2018].
! Hobbs, F., Bankhead, C., Mukhtar, T., Stevens, S., Perera-Salazar, R., Holt, T. and Salisbury, C. (2016). 15
Clinical workload in UK primary care: a retrospective analysis of 100 million consultations in England, 2007–
14. The Lancet, 387(10035), pp.2323-2330.
General Medical Council (2016). The state of medical education and practice in the UK. [online] GMC. 16
Available at: https://www.gmc-uk.org/-/media/documents/
SOMEP_2016_Full_Report_Lo_Res.pdf_68139324.pdf [Accessed 12 Jun. 2018].
! Baird, B., Charles, A., Honeyman, M., Maguire, D. and Das, P. (2016). Understanding pressures in 17
general practice. [online] The Kings Fund. Available at: https://www.kingsfund.org.uk/sites/default/files/
field/field_publication_file/Understanding-GP-pressures-Kings-Fund-May-2016.pdf [Accessed 29 May
2018].
! Milmo, C., Day, A., Mort, D., Burn, C., Kitchen, R., Lynch, P., Fishwick, B., Bradfield, P. and Punshon, D. 18
(2017). Revealed: NHS faces GP recruitment crisis as 40% of doctors approach retirement. [online] iNews.
Available at: https://inews.co.uk/nhs/revealed-nhs-gp-recruitment-crisis-40-approach-retirement/ [Accessed
29 May 2018].
Gibson, J., Sutton, M., Spooner, S. and Checkland, K. (2017). Ninth National GP Worklife Survey 2017. 19
[online] Manchester: PruComm. Available at: http://blogs.lshtm.ac.uk/prucomm/files/2018/05/Ninth-
National-GP-Worklife-Survey.pdf [Accessed 11 Jun. 2018].
! NHS England & British Medical Association (2015). GP Workforce 10 Point Plan. [online] NHSE & BMA. 20
Available at: https://www.bma.org.uk/collective-voice/committees/general-practitioners-committee/gpc-
current-issues/workforce-10-point-plan [Accessed 29 May 2018].
NHS England. Stay Well Pharmacy Campaign Briefing. February 2018.21
Paudyal, V., Watson, M., Sach, T., Porteous, T., Bond, C., Wright, D., Cleland, J., Barton, G. and Holland, 22
R. (2013). Are pharmacy-based minor ailment schemes a substitute for other service providers?. British
Journal of General Practice, 63(612), pp.472-481.
Bednall, R. (2003). Identification of patients attending Accident and Emergency who may be suitable for 23
treatment by a pharmacist. Family Practice, [online] 20(1), pp.54-57. Available at: https://
www.ncbi.nlm.nih.gov/pubmed/12509371.
Kaffash, J. (2018). GP numbers decrease by more than 1,000 over past year. [online] Pulse Today. 24
Available at: http://www.pulsetoday.co.uk/news/gp-topics/employment/gp-numbers-decrease-by-more-
than-1000-over-past-year/20035705.article [Accessed 28 May 2018].
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �63

Mahase, E. (2018). Jeremy Hunt admits he is ‘struggling to deliver’ 5,000 GPs by 2020. [online] Pulse 25
Today. Available at: http://www.pulsetoday.co.uk/news/gp-topics/employment/jeremy-hunt-admits-he-is-
struggling-to-deliver-5000-gps-by-2020/20036846.article [Accessed 11 Jun. 2018].
Buchan, J., Seccombe, I., Gershlick, B. and Charlesworth, A. (2017). In Short Supply: Pay Policy and 26
Nurse Numbers. [online] The Health Foundation. Available at: http://reader.health.org.uk/InShortSupply
[Accessed 29 May 2018].
Sheffield Hallam University (2016). Evaluation of the Sheffield Enhanced Primary Care Programme. 27
[online] Sheffield Hallam University. Available at: http://www.primarycaresheffield.org.uk/wp-content/
uploads/2017/05/Evaluation-SEPCP-Final_Report_v13_3.pdf [Accessed 29 May 2018].
Dx.doi.org. (2018). Unit Costs of Health and Social Care 2017 - Kent Academic Repository. [online] 28
Available at: http://dx.doi.org/10.22024/UniKent/01.02/65559 [Accessed 15 Jun. 2018].
Bush, J., Langley, C., Jenkins, D., Johal, J. and Huckerby, C. (2017). Clinical pharmacists in general 29
practice: an initial evaluation of activity in one English primary care organisation. International Journal of
Pharmacy Practice.
NHS England. National Schedule of Reference Costs 2016/17. https://improvement.nhs.uk/documents/30
1973/2_-_National_schedule_of_reference_costs_-_the_main_schedule.xlsx Accessed 31/5/18.
National Patient Safety Agency and National Institute for Health and Clinical Excellence. (2007). Technical 31
safety solutions, medicines reconciliation..
Parekh, N., Ali, K., Stevenson, J., Davies, J., Schiff, R., Van der Cammen, T., Harchowal, J., Raftery, J. and 32
Rajkumar, C. (2018). Incidence and cost of medication harm in older adults following hospital discharge: a
multicentre prospective study in the UK. British Journal of Clinical Pharmacology.
NHS England (2018). NHS England » Care home pharmacists to help cut overmedication and 33
unnecessary hospital stays for frail older patients. [online] England.nhs.uk. Available at: https://
www.england.nhs.uk/2018/03/care-home-pharmacists-to-help-cut-over-medication-and-unnecessary-
hospital-stays-for-frail-older-patients/ [Accessed 30 May 2018].
Primary Care Foundation (2009). Urgent Care - A practical guide to transforming same day care in 34
General Practice. [online] Primary Care Foundation. Available at: http://www.primarycarefoundation.co.uk/
images/PrimaryCareFoundation/Downloading_Reports/Reports_and_Articles/Urgent_Care_Centres/
Urgent_Care_May_09.pdf [Accessed 30 May 2018].
Mann, C., Anderson, C., Waring, J., Avery, T. and Boyd, M. (2017). "GP Pharmacy Transformation 35
project” Community Pharmacist Independent Prescribers (CPIPs) working in patient facing roles in Primary
Care. Independent Evaluation Report. [online] Nottingham: University of Nottingham. Available at: https://
www.nottingham.ac.uk/pharmacy/research/divisions/pharmacy-practice-and-policy/documents/gpptp-final-
report.pdf [Accessed 29 May 2018].
Frontier Economics (2014). Exploring the costs of unsafe care in the NHS. [online] Frontier Economics. 36
Available at: https://www.frontier-economics.com/documents/2014/10/exploring-the-costs-of-unsafe-care-
in-the-nhs-frontier-report-2-2-2-2.pdf [Accessed 29 May 2018].
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �64

Department of Health & Social Care (2012). Improving the Use of Medicines For Better Outcomes and 37
Reduce Waste: An Action Plan/. [online] Department of Health & Social Care. Available at: https://
www.gov.uk/government/uploads/system/uploads/attachment_data/file/212837/Improving-the-use-of-
medicines-for-better-outcomes-and-reduced-waste-An-action-plan.pdf [Accessed 31 May 2018].
Chief Medical Officer Directorate, NHS Scotland (2018). COMMUNITY PHARMACIST SUPPLEMENTARY 38
AND INDEPENDENT PRESCRIBING CLINICS: FUNDING ARRANGEMENTS FOR 2018-19. Edinburgh.
Avery, A. (2017). Pharmacists working in general practice: can they help tackle the current workload 39
crisis?. British Journal of General Practice, 67(662), pp.390-391.
BBC News. (2018). 'Drug errors cause appalling harm'. [online] Available at: http://www.bbc.co.uk/news/40
health-43161929 [Accessed 31 May 2018].
Irving, G., Neves, A., Dambha-Miller, H., Oishi, A., Tagashira, H., Verho, A. and Holden, J. (2018). 41
International variations in primary care physician consultation time: a systematic review of 67 countries.
NHS Scotland (2013). Practice Team Information. Annual Update 2012/13. [online] Information Services 42
Division, NHS Scotland. Available at: https://www.isdscotland.org/Health-Topics/General-Practice/
Publications/2013-10-29/2013-10-29-PTI-Report.pdf [Accessed 25 Jun. 2018].
EVALUATION OF JAUNTY SPRINGS INTEGRATED CARE MODEL �65