New insights into symptoms and neurocircuit function of anorexia nervosa

of 12
Transcript of New insights into symptoms and neurocircuit function of anorexia nervosa
-
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
1/12
Anrxia nra (AN), a dirdr f nknwn ati-gy, i charactrizd by rtrictd ating and a rnt- prit f thinn (BOX 1). AN i piby tht hgn f a pychiatric dirdr. Thri a narrw rang f ag f nt (ary adcnc),trtypic prntatin f ypt and cr, andrati gndr pcificity1. Indiida with AN ha ang-yntnic ritanc t ating and a pwrf pr-it f wight , yt ar paradxicay prccpidwith fd and ating rita t th pint f bin.Indiida ha a ditrtd bdy iag and, n whnaciatd, tnd t th a fat, xpr dniaf bing ndrwight and cpiy r-xrci.Thy ar ftn ritant t tratnt and ack inightrgarding th rin f th dica cnqncf th dirdr.
Tw typ f ating-ratd bhair ar n in AN
(BOX 1). Rtricting-typ anrxic wight pry byditing witht bing ating r prging. Bing-ating/prging-typ anrxic a rtrict thir fd intakt wight, bt ha a pridic diinhibitin frtraint and ngag in bing ating and/r prging ad indiida with biia nra (BN). Cnidringthat tranitin btwn yndr ccr in any, itha bn argd that AN and BN har rik andiabiity factr2,3. Hwr, thi Riw fc nrtricting-typ AN.
Athgh AN i charactrizd a an ating dirdr,it rain nknwn whthr thr i a priary di-trbanc f apptiti pathway, r whthr ditrbd
apptit i cndary t thr phnna, ch aanxity r bina prccpatin with wight gain.Thr ha bn cnidrab intrt in th r f thhypthaa in fd and wight rgatin in AN,athgh it rain ncrtain whthr hypthaaicatratin ar a ca r a cnqnc f th yp-t. Thi Riw fc n anthr prpcti. Thati, athgh th hypthaa i an iprtant rgatrf fd intak and bdy wight, thr i iitd idncthat hypthaaic pptid ha a r in th atigyf AN. Hwr, tdi in ania and hathy hanar ading t a nw ndrtanding f rapping n-ra pathway that cntribt t th datin f rwardand tin in rpn t apptiti tii. Ginth prbab ink btwn fding bhair and affc-ti prc in AN, th nra btrat ndryingth prc ar ptntia candidat rgin fr ndr-
tanding th pathphyigy f thi in. Thi Riwintgrat finding fr pharacgica, bhairaand nriaging tdi that cntribt t th ndr-tanding f apptit rgatin, rward, nrtranittrand nrcircit that ar aciatd with AN.
State and trait
Whn anrihd and aciatd, indiida withAN ha widprad and r atratin f brain andpriphra-rgan fnctin; hwr, it i ncar whthrth chang ar th ca r th cnqnc f a-ntritin and wight . Thrfr, t ndrtand thatigy and cr f in f AN, it i f t diid
*Eating Disorder Treatment &
Research Program,
Department of Psychiatry,
University of California, San
Diego, La Jolla Village
Professional Center, 8950
Villa La Jolla Drive, Suite
C-207, La Jolla, California
92037, USA.Psychiatry & Neurobiology
and Anatomy, University of
Rochester Medical Center,601 Elmwood Avenue,
Rochester, New York 14642,
USA.Laboratory of Biological
Dynamics and Theoretical
Medicine, Department
of Psychiatry, University of
California, San Diego, 8939
Villa La Jolla Dr. Suite 200,
La Jolla, California 92037-
0985, USA.
Correspondence to W.H.K.
e-mail: [email protected]
doi:10.1038/nrn2682
Published online 15 July
New insights into symptomsand neurocircuit functionof anorexia nervosaWalter H. Kaye*, Julie L. Fudge and Martin Paulus
Abstract | Individuals with anorexia nervosa have a relentless preoccupation with dieting and
weight loss that results in severe emaciation and sometimes death. It is controversial whether
such symptoms are secondary to psychosocial influences, are a consequence of obsessionsand anxiety or reflect a primary disturbance of brain appetitive circuits. New brain imaging
technology provides insights into ventral and dorsal neural circuit dysfunction perhaps
related to altered serotonin and dopamine metabolism that contributes to the puzzling
symptoms found in people with eating disorders. For example, altered insula activity could
explain interoceptive dysfunction, and altered striatal activity might shed light on altered
reward modulation in people with anorexia nervosa.
R E V I E W S
NATuRe RevIeWs |NeuroscieNce volume 10 | AuGusT 2009 |573
2009 Macmillan Publishers Limited. All rights reserved
mailto:[email protected]:[email protected] -
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
2/12
Interoception
The sensing and integrating of
afferent proprioceptive and
visceroceptive information,
resulting in feeling the inner
state of the body, which is
important for allocating
attention, evaluating context
and planning actions.
th nrbigica atratin int tw catgri. Firt,thr t b prrbid, gnticay-dtrind traitatratin that cntribt t a nrabiity t dpAN. scnd, thr ar tat atratin cndary tantritin that ight tain th in, and pr-hap accrat th t-f-cntr pira that rt inr aciatin and th hight rtaity rat f anypychiatric dirdr.
Trait-related alterations. larg-ca cnity-badtwin tdi ha hwn that 50% t 80% f th ari-anc in AN and BN can b accntd fr by gnticfactr35. Th gntic nrabiity t ating dirdright b xprd a a diff phntyp f cntinbhaira trait, a ggtd by idnc f ignificanthritabiity f dirdrd ating attitd, wight prc-cpatin, diatifactin with wight and hap, ditaryrtraint, bing ating and f-indcd iting68, andf ignificant faiiaity f bthrhd fr f atingdirdr2,9.
Cnidrab idnc ha ggtd that chid-
hd tprant and prnaity trait can ad ta prdipitin t dp AN dring adcnc.Rcnt tdi1012 dcrib ngati tinaity, haraidanc, prfctini, inhibitin, dri fr thinn,atrd interoceptive awarn and bi-cpiprnaity trait a chidhd prdiping factrthat prcd th nt f an ating dirdr (FIG. 1)and that prit aftr rcry ( bw). stdi ggtthat th trait ar hritab, can b prnt in naffctdfaiy br and ar indpndnt f bdy wight13,priding frthr idnc that thy cnfr iabiity tth dpnt f AN.
State-related alterations. staratin and aciatinha prfnd ffct n th fnctining f th brainand thr rgan yt. Thy ca nrchicaditrbanc that cd xaggrat prrbid trait14,adding ypt that aintain r accrat th di-a prc (FIG. 1). Fr xap, bjct with AN haa rdcd brain 15, an atrd tabi infrnta, cingat, tpra and parita rgin16, and argrin t pr-pbrta gnada fnctin17. Th fact
that ch ditrbanc tnd t nraiz aftr wightrtratin ggt that thy ar a cnqnc rathrthan a ca f AN.
It i iky that any f th taratin-drin nd-crin and tabic chang that rt fr AN arcpnatry and attpt t cnr nrgy r ti-at hngr and fding18. Fr xap, bjct with ANha atrd cncntratin19 f nrpptid Y (NPY),ptin, crtictrpin-raing hrn (CRH), ch-cytkinin, bta-ndrphin and pancratic pypptid.It i iprtant t nt that ch atratinar iky tca atratin in d, cgniti fnctin, ipcntr and atnic and hrna yt20, whichindicat that thy ight cntribt t th bhairaypt aciatd with th i tat. Fr xap,intracrbrntricar CRH adinitratin in xpri-nta ania prdc any f th phyigicaand bhaira chang aciatd with AN, incd-ing hypthaaic hypgnadi, atrd tinaity,dcrad xa actiity, hypractiity and dcradfding bhair21. Thrfr, it can b argd that
cndary chang in pptid cncntratin cantain AN bhair (FIGS 1,2) by driing a dir frr diting and wight . mrr, antritin-aciatd atratin xaggrat tina dyrga-tin, cnitnt with th any indiida with ANthat t Dsm-Iv (Diagntic and statitica manaf mnta Dirdr, frth ditin) critria1 fr ajrdprin, bi cpi dirdr (oCD) rthr anxity dirdr22,23.
Do symptoms in individuals with AN reflect trait orstate?Th difficty in ditingihing chang that ard t trait fr th that ar ratd t tat in td-i f bjct with AN ha bn a ajr cnfnd inth rarch f thi dirdr. Prpcti, ngitdinatdi ar diffict gin th yng ag f ptntiabjct, th rarity f th dirdr and th any yarf fw-p rqird. An atrnati tratgy i t tdyindiida wh ha rcrd fr AN, th aidingth cnfnding infnc f antritin and wight n bigica yt. Thr i prnty n agrd-pn dfinitin f rcry fr AN, bt r rarchdfin it a haing a tab and hathy bdy wight frnth r yar, with tab ntritin, rati abncf ditary abnraiti and, in fa,nra n-tratin. Athgh th prc f rcry fr ANi pry ndrtd and, in t ca, prtractd,
apprxiaty 50% t 70% f affctd indiida wintay attain cpt r drat rtin fth in, athgh thi ight nt ccr nti thirary t id 202426. stdi ha dcribd tpra-nt and charactr trait that ti prit aftr ng-trrcry fr AN, ch a ngati tinaity, haraidanc, prfctini, dir fr thinn and idditary prccpatin. It i pib that ch pritntypt ar car cad by chrnic antritin.Hwr, th fact that ch bhair24,27,28 ar iiart th dcribd fr chidrn wh wi dp AN1012arg that thy rfct ndrying trait that cntribtt th pathgni f thi dirdr.
Box 1 | DSM-IV, diagnostic criteria for anorexia nervosa1
Refusaltomaintainbodyweightatoraboveaminimallynormalweightforageand
height(forexample,weightlossleadingtomaintenanceofbodyweightlessthan85%ofthatexpected;orfailuretomakeexpectedweightgainduringperiodofgrowth,
leadingtobodyweightlessthan85%ofthatexpected.)
Intensefearofgainingweightorbecomingfat,eventhoughunderweight.
Disturbanceinthewayinwhichonesbodyweightorshapeisexperienced,undue
influenceofbodyweightorshapeonself-evaluation,ordenialoftheseriousnessof
thecurrentlowbodyweight.
Inpostmenarchealfemales,amenorrhea(thatis,theabsenceofatleastthree
consecutivemenstrualcycles).
Therearetwotypesofanorexianervosa:1.Restrictingtype,inwhichthepersonhas
notregularlyengagedinbinge-eatingorpurgingbehaviour;2.Binge-eating/purging
type,inwhichthepersonhasregularlyengagedinbinge-eatingorpurgingbehaviour
(thatis,self-inducedvomitingorthemisuseoflaxatives,diureticsorenemas).
R E V I E W S
574 | AuGusT 2009 | volume 10 www.nat.m/w/n
2009 Macmillan Publishers Limited. All rights reserved
-
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
3/12
Traits
Negative emotionPerfectionismDrive for thinnessIncreased interoceptive awarenessObsessive-compulsive personality
Puberty
Brain developmentHormonesStressCultural factors
Dieting
Weight loss
Neurobiologicalchanges
Denial, rigidity,anxiety, depression,obsessionality
Chronic illness(3050%)
Recovery(5070%)
Childhood
Adolescence
Adulthood
Neurobiology and behaviour
Cn crbid bhair typica f bth rcrdand i AN indiida ar ftn xprd in cncrt.Th incd inhibitin, anxity, dprin and b-inaity, and pzzing ypt ch a bdy iagditrtin, prfctini, and anhdnia. Th bha-ir cd b ncdd in ibic and cgniti circitknwn t dat and intgrat nrna prcthat ar ratd t apptit, tinaity and cgniticntr. Tw nrcircit that ha bn dcribdbad n iaging, nrphyigica and in td-i29,30 ight b f particar ranc t ndrtand-
ing bhair in AN. A ntra (ibic) nrcircitthat incd th aygdaa, ina, ntra triatand ntra rgin f th antrir cingat crtx(ACC) and th rbitfrnta crtx (oFC) t biprtant fr idntifying th tina ignificancf tii and fr gnrating an affcti rpn t thtii29,30. A dra (cgniti) nrcircit i thghtt dat cti attntin, panning and ffrtfrgatin f affcti tat, and incd th hippca-p, dra rgin f th ACC, dratra prfrntacrtx (DlPFC), parita crtx and thr rgin29,30.Indd, arir brain iaging tdi ha hwn thatbjct wh ha rcrd fr AN ha atrd
actiity in frnta, antrir cingat and paritargin3133 sra intigatr ha prpd thatdyrgatin f th tw circit cntribt t rapychiatric dirdr incding ajr dprin, anxi-ty dirdr and oCD. It i pib that abrrant fnc-tin f th circit ca atrd tin rgatin rbinaity bt that th car bai f th dy-fnctin diffr btwn dirdr30. Indd, th nr-bigica ditrbanc in pp with ating dirdray diffr fr th fnd in pp with dprin,anxity r oCD. Fr xap, th binding ptntia fth rtnin (5-HT) rcptr 1A (5-HT
1A) i dcrad
in bjct with dprin34, a w a in pp withcia phbia35 and panic dirdr36, whrait tnd tb incrad in pp with ating dirdr3740.
Thi Riw fc n th finding drid frra iaging tchngi. stdi ing pitrniin tgraphy (PeT) brain iaging and ratdtchngi ha ad 5-HT and dpain (DA)nrtranittr yt in bjct with AN and inth wh ha rcrd.scnd, rcnt fnctinamRI (fmRI) tdi ha bgn t hd ight n atrdactiity in intrcnnctd brain rgin f th indi-
ida. Tgthr th tdi prid nw inightint nrbigica ditrbanc that charactriz thidady dirdr.
Serotonin function in AN. Th 5-HT yt ha bnintniy tdid in pp with AN a cnidrabidnc ggt that thi nrtranittr ytcd pay a part in ypt ch a nhancd ati-ty41, ip cntr42,43 and d44,45. Indd, thr ich idnc f abnra fnctina actiity f th5-HT yt in bjct with AN46,47(FIG. 2). Fr xap,in ndrwight and anrihd indiida ffr-ing fr AN th crbrpina fid (CsF) ha rdcdant f 5-hydrxyindactic acid (5-HIAA) which i th ajr brain tabit f 5-HT and ithght t rfct xtracar 5-HT cncntratin48.By cntrat, 5-HT tabit wr atd in thCsF f bjct wh had rcrd fr AN.
It i iprtant t nt that th 5-HT yt in14 r r rcptr, and intract withany thrnrtranittr and c. ony a fw f thcpnnt can crrnty b ard in vivo inhan. sti, iaging tdi f 5-HT fnctina acti-ity ar f; athgh th cpxity f 5-HT circitcannt b fy cidatd in han, ch iaging td-
i can charactriz ptntia tat and trait diffrncbtwn indiida with AN and hathy cntr, bd t d ratinhip f 5-HT actiity t bhairand prid nw inight n ptntiay r ffctitratnt targt. In fact, brain iaging tdi cnit-nty hw that, whn cpard with hathy bjct,indiida with r haing rcrd fr ating di-rdr ha atd and diinihd binding ptntiafr ptynaptic 5-HT
1Arcptr and5-HT
2Arcptr,
rpctiy3740,4951. stdi f indiida with r ha-ing rcrd fr AN tnd t prdc iiar find-ing, pprting th ntin that thr ar trait-ratdatratin f 5-HT fnctin in AN.
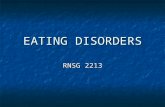
Figure 1 | T tm an nmngy anxa na. Childhood
personality and temperament traits, which contribute to a vulnerability for developing
anorexia nervosa (AN), become intensified during adolescence as a consequence of the
effects of multiple factors, such as puberty and gonadal steroids, development, stress
and culture. Individuals with AN find that dieting reduces, and eating enhances
dysphoric mood. But with chronic dieting and weight loss, there are neurobiological
changes which increase denial, rigidity and obsessions, as well as depression and anxiety,
so that individuals often enter a downward spiral. Although 50% or more of individuals
with AN recover by their early to mid20s, a significant proportion of subjects develop a
chronic illness or die.
R E V I E W S
NATuRe RevIeWs |NeuroscieNce volume 10 | AuGusT 2009 |575
2009 Macmillan Publishers Limited. All rights reserved
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3350&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3350&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3356&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3356&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3356&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3356&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3350&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSum -
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
4/12
Dieting
Dysphoric mood
CRH-endorphin
Dysphoric mood
Weight loss
5 10 15 20 25 30 35Novelty seeking
[11C]WAY100635BP
orbitalcortex
10 14 18 22 26 30
0.8
1.0
1.2
1.4
1.6
1.8
2.0
[18F]altamserinBP
orbitofrontalcorte
x
0
11
10
9
8
7
6
5
4
3
5 10 15 20 2 5 30
Harm avoidance
[11C]WAY100635BP
mesialtemporalcortex
+
+
+
+
+
5-HT1A receptor
5HT2A receptor
Normal
AN trait
5-HT overdrive
Dysphoric mood Error detection Inhibition
5-HT production 5HT1A levels
5-HT 5-HT
1A
, 5-HT2A
bindingForced
eating
Harm avoidance
Continuedstarvation
a
b
1
2
3
4
5
6
7
Restrictive eating
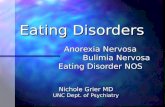
Figure 2 | T tnn na ntn n anxa na. It is well known that people with anorexia nervosa
(AN) enter a vicious cycle, whereby malnutrition and weight loss drive the desire for further restricted eating and emaciation.
Evidence suggests that, compared with healthy individuals (a), individuals who are vulnerable to developing an eating
disorder might have a trait for increased extracellular serotonin (5HT) concentrations 68 and an imbalance in postsynaptic
5HT1A
and 5HT2A
receptor activity3740,4951 (b), which together might contribute to increased satiety and an anxious,
harmavoidant temperament. Gonadal steroid changes during menarche or stress related to adolescent individuationissues might further alter activity of the 5HT system and so exacerbate this temperament, resulting in a chronic dysphoric
state. It is important to note that foodmood relationships in AN are very different from those in healthy controls. That is,
palatable foods in healthy subjects are associated with pleasure, and starvation is aversive. By contrast, palatable foods
seem to be anxiogenic in AN, and starvation reduces dysphoric mood. In subjects with AN, starvation and weight loss result
in reduced levels of 5HIAA in the cerebrospinal fluid (CSF)74 (and inferentially reduced extracellular 5HT concentrations)
but exaggerated 5HT1A
receptor binding in limbic and cognitive cortical regions39. Starvationinduced reductions of
extracelluar 5HT levels might result in reduced stimulation of postsynaptic 5HT1A
and 5HT2A
receptors, and thus
decreased dysphoric symptoms. However, when individuals with AN are forced to eat, the resulting increase in extracellular
5HT levels, and thus stimulation of postsynaptic 5HT1A
and 5HT2A
receptors, increases dysphoric mood, which makes
eating and weight gain aversive. Alternatively, if subjects with AN continue to starve, anorexigenic signals related to
neuropeptide disturbances (for example, increased corticotropinreleasing hormone (CRH)21 and reduced endorphin166)might drive further food restriction and changes in behaviour and cognition, which thus promotes AN symptoms.
Scatterplots reproduced, with permission, from REF. 39 (2007) American Medical Association and REF. 40 (2005) Elsevier.
R E V I E W S
576 | AuGusT 2009 | volume 10 www.nat.m/w/n
2009 Macmillan Publishers Limited. All rights reserved
-
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
5/12
mrr, iaging tdi prid inight int hwditrbd 5-HT fnctin i ratd t dyphric din AN52,53. That i, PeT iaging tdi hw trikingand cnitnt piti crratin btwn th bind-ing ptntia f bth 5-HT
1Aand 5-HT
2Arcptr
and har aidanc a tifactd tpranttrait54 that cntain nt f anxity, inhibitin, andinfxibiity. stdi in ania and hathy hanpprt th pibiity that 5-HT
1Aand 5-HT
2Arcptr
actiity ha a r in anxity5558. It i iprtant t ntthat thr i high c-caizatin (80%) f th 5-HT
2A
and 5-HT1A
ptynaptic rcptr in th rdnt frntacrtx59 and thr crtica rgin60. Thrgh intrn-rn, thy diat, rpctiy, dirct hyprparizingand dparizing actin f 5-HT n prfrnta n-rn that prjct t crtica and bcrtica ara61,62.Intractin btwn 5-HT
1Aand 5-HT
2Arcptr
in th dia prfrnta crtx (PFC) and ratdrgin t dat anxity, attntina fnctin-ing63, ipiity and cpi prratin62, andxpratin f nw nirnnt64. It rain t b
dtrind whthr th ibaanc btwn nhancd5-HT
1Aand diinihd 5-HT
2Arcptr binding ptn-
tia cntribt t ch ypt in indiida withating dirdr.
Implications for satiety and the benefit of starvation. Iti thght that, in indiida with AN, ditary rtraintrdc anxity, whra ating tiat dyphricd53,65,66. I atrd 5-HT fnctin th ink btwnrtrictd fding bhair and anxity in bjctffring fr AN? It i w-knwn that carbhydratintak incra xtracar 5-HT cncntratin inth brain thrgh cpx tabic ffct n tryp-tphan, th ain acid prcrr f 5-HT53,67. W pr-p that, bth prrbidy and aftr rcry frAN, a nra ant f fd ingtin i aciatdwith xaggratd xtracar brain 5-HT crtin68.Thi i cnitnt with incrad CsF 5-HIAA inpp wh ha rcrd fr AN68. Incrad 5-HTcncntratin inhibit apptit, prhap thrgh acti-
atin f5-HT2C
rcptr69; hwr, 5-HT2C
rcp-tr binding ha nt bn ard by iaging tdiin indiida with AN. Incrad 5-HT
1Abinding
ptntia i pitiy aciatd with har aidancin bjct wh ha rcrd fr AN40 (FIG. 2), andnhancd anxity and har aidanc ar trait thatar prnt prrbidy and prit aftr rcry fr
AN. It i thrfr pib that carbhydrat-indcdincra in xtracar 5-HT dri anxity andhar aidanc thrgh tiatin f 5-HT
1Arcp-
tr (FIG. 2), ffring a ptntia xpanatin fr fd-ing-ratd dyphric d in AN. By cntrat, whnindiida with AN tar, xtracar 5-HT cn-cntratin ight diinih, rting in a brif rpitfr dyphric d. stdi in ania and hathyhan hw that bth a rtrictd dit (which ignifi-canty wr paa tryptphan) and xprintayrdcd tryptphan dptin dcra 5-HT ynthiin th brain67,70,71. Indd, anrihd and aciatdindiida with AN ha rdcd paa tryptphan
aaiabiity72,73 and rdcd CsF 5-HIAA 74.Iprtanty, xprinta anipatin that rdcth f tryptphan in th brain dcra anxityin bth i and rcrd AN bjct53. Hwr, tar-
atin in AN t b aciatd with a cpna-try incra in ptynaptic 5-HT
1Arcptr binding
ptntia39. mrr, 5-HT2A
rcptr binding i pi-tiy ratd t har aidanc in bjct ffringfr AN. Thrfr, whn indiida with AN arfrcd t at (FIG. 2), it i iky that thy ha a ratiincra in xtracar 5-HT cncntratin in thbrain, ading t an xaggratin f dyphric d.Th, indiida with AN ight pr taratinin an attpt t aid th dyphric cnqnc fating and cnqnty pira t f cntr.
Dopamine and reward processing in AN. Pp withAN ftn xrci cpiy, ar anhdnic andactic, and find itt in if that i rwarding aidfr th prit f wight 1. sch tprantprit, in a r dt fr, aftr rcry24,75,
indicating that th charactritic ar trait rathrthan bing tat ratd.DA dyfnctin, particaryin triata circit, ight cntribt t atrd rwardand affct, dciin-aking and xcti cntr, aw a trtypic tr nt and dcradfd ingtin in bjct with AN76. eidnc thatth DA yt i ind in AN incd rdcdCsF f DA tabit in bth i indiida andth haing rcrd fr AN77, fnctina DA D2rcptr (DRD2) gn pyrphi in bjct withAN78 and ipaird ia dicriinatin arning 79,which i thght t rfct DA-ignaing fnctin, inindiida with AN. A PeT tdy fnd that bjctwh rcrd fr AN had incrad D2/D3 rcp-tr (DRD3) binding in th ntra triat76, a rginthat dat rpn t rward tii80,81. Thicd indicat incrad D2/D3 dniti, dcradxtracar DA, r bth, in indiida wh rcrdfr AN. In additin, D2/D3 rcptr binding in thdra cadatdra ptan crratd pitiywith har aidanc in bjct wh had rcrdfr AN76.
T dtrin whthr indiida wh ha rc-rd fr AN ha fndantay diffrnt rpnt rward cpard with hathy cntr, an nt-ratd fmRI tdy xaind th bd xygn -dpndnt (BolD) igna whi participant prfrd
a ip chic and fdback tak82. Th tak waadaptd fr a w-charactrizd ging-gaprtc83 that i knwn t actiat th ntra triatand bgna ACC, with cntr participant hwingdiffrntia actiity in th ara in rpn t pitiand ngati ntary fdback. In th bjct whhad rcrd fr AN actiity in th bgna ACCand it ntra triata targt wa iiar dring pi-ti and ngati fdback82, ggting that indiid-a with AN ha a circit-bad abnraity dringthi ip tak and ight ha difficty dicriinat-ing btwn piti and ngati fdback. Aniatdi hw that DA ha a r in th prcing f
R E V I E W S
NATuRe RevIeWs |NeuroscieNce volume 10 | AuGusT 2009 |577
2009 Macmillan Publishers Limited. All rights reserved
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3358&ordinalpos=2&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3358&ordinalpos=2&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=1813&ordinalpos=9&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=1814&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=1814&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=1813&ordinalpos=9&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3358&ordinalpos=2&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSum -
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
6/12
Hedonic
A sensation related to or
characterized by pleasure
tiatina apct t tii in th ntra triat:DA dat th infnc f ibic inpt n tri-ata actiity30,80,81 and i thght t thrby diat thbinding fhedonic aatin f tii t bjct ract (wanting rpn)84. Th ntra triata rpnin bjct wh had rcrd fr AN82 ight rfct afair t apprpriaty bind, dat r dicriinatrpn t aint tii. Th data pprt th p-ibiity that indiida wh ha rcrd fr ANight ha an ipaird abiity t idntify th tinaignificanc f tii30, which cd b iprtant inndrtanding why it i diffict t tiat th tngag in tratnt r apprciat th cnqnc fthir bhair85.
mrr, th wn wh had rcrd fr ANhad xaggratd actiatin in th cadatdra tria-t and in th cgniti crtica rgin that prjct tthi ara, pcificay th DlPFC and th parita cr-tx82. Th cadat nc i actiatd by tak in whichthr i bth a prcid cnnctin btwn actinand tc, and ncrtainty abt whthr th
actin wi ad t th dird tc86. many f thwn indicatd an attpt at tratgic (a ppdt hdnic) rpn t ipr th rati f win t, which prhap cntribtd t th gratr actia-tin f thi rgin. In th abnc f apprpriat rwardprcing thrgh ntra-triata/DA path, indiidawh ha rcrd fr AN ight fc n a dtaidtratgy rathr than th ra itatin87. Fr anthrprpcti, cntr wn apprpriaty id in thnt. That i, thy raizd thy had t ak a gand thn d n t th nxt tak. By cntrat, bjctwith AN tnd t xaggratdy and biy wrryabt th cnqnc f thir bhair kingfr r whn thr ar nn and ar ry cn-crnd abt aking itak. A rcnt fmRI iagingtdy, ing a t hifting tak, hwd ratiy iiarfinding in indiida with AN88, nay hypactia-tin in th ntra antrir cingat-triat-thaaicp, with prdinant actiatin f frntparitantwrk. Tgthr th data ggt that indiid-a with AN ight b ab t prciy dataffcti rpn t idiaty aint tii btha incrad actiity in nrcircit cncrnd withpanning and cnqnc.
Serotonindopamine interactions. D intractinbtwn 5-HT and DA yt cntribt t ypt
in AN? It ha bn pcatd that 5-HT i th crciabtrat f an ari tiatina yt whichight pp a DA-ratd apptiti yt89,90. Indd,tdi f ania hw that 5-HT
2Crcptr tnicay
inhibit DA nrn91,92. A PeT tdy in bjct thathad rcrd fr ating dirdr fnd piti cr-ratin btwn 5-HT tranprtr and D2/D3 rcp-tr binding in th ntra triat and dra cadat(u. F. Bair and W.H.K.,npbihd bratin).Fr anthr prpcti, tdi ggt that 5-HTha a r in actin chic by cntring th ticaf dayd rward thrgh diffrntia ffct n n-tra and dra triata circit93,94. Thi i cnitnt with
idnc that rdcd and incrad 5-HT actiity araciatd with ipi, aggri bhair andbhaira inhibitin, rpctiy43,93,95. Cnidrdtgthr, indiida with AN ight ha a trait twardan ibaanc btwn 5-HT and DA pathway, whichcd ha a r in an atrd intractin btwn
ntra and dra nrcircit.Dpit cnidrab idnc f 5-HT abnr-
aiti, indiida with AN hw itt rpn, intr f iprnt f d r rdctin f crating dirdr ypt, whn tratd with ctirtnin r-ptak inhibitr (ssRI)96. Th fficacyf ssRI i dpndnt n nrna ra f 5-HT 97,and 5-HT ra in trn rt in dnitizatin fth 5-HT
1Arcptr98. It i pib that atd acti-
ity f 5-HT1A
rcptr in th raph nc f bjctwith AN (FIG. 2) rt in rdcd 5-HT nrna firing,and th dcrad xtracar 5-HT 74, cnit-nt with th rdcd CsF 5-HIAA fnd in thindiida. Thrfr, it i pib that ssRI ar ntffcti in indiida with AN bca ssRI wd
nt ha ch ffct if ynaptic 5-HT ar dptdby antritin. Priinary data rai th pibiitythat anzapin (Zyprxa; ei liy) which ha ffctn bth DA and 5-HT rcptr and piby thratypica antipychtic ight b f fr incraingwight gain and rdcing anxity and binaityin AN99.
Neurocircuitry of appetite
Hw can indiida with AN rtrict thir fd intakry day, aintain a w wight fr any yar andti di f taratin, whn t pp trg-g t a fw pnd? Apptit i a cpx incn-ti tiatina dri and i thght t dpnd nintrratd pychbigica factr incding fdrwarding prprti, an indiida htaticnd and th cgniti abiity t far atrnati (tating) bhair100102. Apptit i cary ditrbd inbjct with AN: thy diik high-fat fd103,104, dnt find cr ari whn atiatd and fai t ratfd a piti whn hngry105,106. Th rpntnd nt t chang fwing wight rgain and, antd ab, thr i idnc that ditary rtraintrdc anxity and that ating rt in dyphricd in indiida with AN53,65,66. Th cpx fdcnatry ypt f ating dirdr ar ra-tiy niq and ha a trtypic and rnt
xprin, pprting th pibiity that thy rfct abrrant fnctin f nra circit ind inrgating ating bhair.
Athgh a wt-tat prcptin tak d nt ttth cpxity f fd chic107, it can b d in brainiaging tdi t actiat brain ara ind in app-tit rgatin.swt-tat prcptin (FIG. 3) i priph-ray diatd by tng rcptr108 thrgh a nrayt cniting f crania nr, th nc tractitarii, and thaaic ntrptrir dia nc,t th priary gtatry crtx, which in han c-pri th frnta prc and th antrir ina109113.Th antrir ina and aciatd gtatry crtx
R E V I E W S
578 | AuGusT 2009 | volume 10 www.nat.m/w/n
2009 Macmillan Publishers Limited. All rights reserved
-
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
7/12
Planning futureconsequences
Reward
Workingmemory
Bodyspace
Incentive learning(flexible)
Conflictmonitoring
Interoceptiveawareness
Affectiverelevance
DLPFCParietalcortex
ACC
Spinal cord
Chemoreceptorsof the tongue
Sensory input
C
P
OFC
Amygdala
Thalamictaste centre
NTSMedulla
Brainstem
Gustatorycortex
Anteriorinsula
Visceroception
A sensation originating from
the internal organs.
Proprioception
A sensation originating from
the joints and the
subcutaneous tissues.
rpnd t th tat and phyica prprti f fd, anday a rpnd t it rwarding prprti114117.
othr rgin cpriing th ntra nrcircitntind ab ar intrcnnctd with th ina(FIG. 3), incding th aygdaa, th ntra ACC andth oFC. Th ACC i inkd t hypthaaic and brain-t pathway that diat atnic and icra cn-tr118,119. Th prgna ACC i ipicatd in cnfict
nitring and dtct ing nprdictd tc tgid bqnt bhair80,120122. Th oFC i a-ciatd with fxib rpn t changing tii: itrpnd t th anticipatd ngati (r piti) af xtrna tii and fxiby atr rpn bad nchanging incnti a f a ti123126. Th ant-rir ina, ACC and oFC a innrat a brad rginf th rtra ntra triat, in which bhairarprtir ar cptd bad n th inpt. Thintrcnnctd rgin f th ntra nrcircit payan iprtant part in dtrining htatic app-titi nd (FIG. 3). Indd, brain iaging tdi hacnitnty hwn that fd dpriatin (cpardt haing bn fd) in hathy indiida actiat thina and th oFC117,127130. Crtica rgin incdd inth dra nrcircit ch a th DlPFC, th pari-ta crtx and th ptrir inar rgin diatcgniti fnctin ch a panning and qncing.Th rgin nd inpt t r dratra part fth triat, bt a ight intrfac and rap with
ntra triata ara131,132. Tgthr, th inpt ar
thght t dat th triata actiity that ndrith apprach r aidanc f fd.
Adinitring cr r watr t bjct whha rcrd fr AN rt in a rdcd BolDrpn in th ina, ACC and triat a cpardwith cntr bjct133. In hathy cntr, f-ratingf paantn f th gar tat crratd pitiywith th BolD rpn in th ina, th ACC and th
ntra and dra ptan133. Cnitnt with th idathat th abiity t prci a paatab tat i fndan-tay atrd in AN, indiida wh had rcrd frAN faid t hw any ratinhip btwn actiity inth rgin and f-rating f th paantn f thcr tat. Th finding ar pprtd by thrbrain iaging tdi in which th bratin f fdpictr by ndrwight bjct with AN d t atrdactiity in th ina, th oFC, th ia tpra andparita crtx and th ACC134138. mrr, th atrdactiity in th prgna ACC and dia prfrn-ta crtx pritd aftr rcry33. Atrd actiityin th antrir ina, it visceroceptive and propriocep-tive affrnt, and it ffrnt t th oFC, th ACC,th aygdaa and th ntra triat ight ndri thatratin fnd in bjct with AN in inking nry-hdnic xprinc t th tiatina cpnntf rward139.
A central role for the anterior insula?Th antririna i crciay ind in intrcpti prc-ing140142. Intrcptin incd a rang f natinbynd tat, incding th prcptin f pain, t-pratr, itch, tick, na tch, c tnin, airhngr, tach pH and inttina tnin. Intgratinf th intrna fing prid an intgratd n fth phyigica cnditin f th ntir bdy143 and icrcia fr th intantiatin f th f bca it pr-
id th ink btwn cgniti and affcti prcand th crrnt bdy tat140142,144,145.
It i thght that atrd intrcpti awarn ightb a prcipitating and rinfrcing factr in AN10,146148.
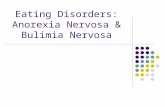
Figure 3 | cta-tata atway wt a n tat. Chemoreceptors on the
tongue detect a sweet taste. The signal is then transmitted through brainstem and
thalamic taste centres to the primary gustatory cortex, which lies adjacent to and is
densely interconnected with the anterior insula. The anterior insula is an integral part of
a ventral (limbic) neurocircuit through its connections with the amygdala, the anterior
cingulate cortex (ACC) and the orbitofrontal cortex (OFC). Afferents from the corticalstructures involved in the ventral neurocircuit (anterior insula and interconnected limbic
cortices) are directed to the ventral striatum, whereas cortical structures involved in
cognitive strategies (forming a dorsal neurocircuit) send inputs to the dorsolateral
striatum. Therefore, the sensory aspects of taste are primarily an insula phenomenon,
whereas higher cortical areas modulate pleasure, motivation and cognitive aspects of
taste. These aspects are then integrated, resulting in an eat or do not eat decision.
Coding the awareness of pleasant sensation from the taste experience via the anterior
insula might be altered in subjects with anorexia nervosa, tipping the balance of striatal
processes away from normal, automatic reward responses mediated by the ventral
striatum and towards a more strategic approach mediated by the dorsal striatum. The
figure links each cortical structure with arrows, indicating that all cortical structures
project to striatum in a topographic manner.DLPFC, dorsolateral prefrontal cortex; NTS,
nucleus tractus solitarii.
R E V I E W S
NATuRe RevIeWs |NeuroscieNce volume 10 | AuGusT 2009 |579
2009 Macmillan Publishers Limited. All rights reserved
-
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
8/12
C
P
C
P
Foodpresentation
Foodpresentation
Interoceptivesignals
Interoceptivesignals
Amygdala
DLPFC
Anterior insulaParietalcortex
Posteriorinsula
Positivevaluation
Negativevaluation
Top-downmodulatoryinfluence
Approach foodEat food
Dont approach foodAvoid food in the future
Short-term Long-term Short-term Long-term
Consequences Consequences
Satisfyinghunger
Stayingthin
Healthy Anorexia nervosa Th r f th antrir ina in intgrating intrcp-ti infratin and th atrd ina actiity that habn fnd in indiida with AN ( arir) pprtth ida that thy ight ffr fr a fndantay andphyigicay atrd n f f149. Indd, any f thypt f AN, ch a ditrtd bdy iag, ack frcgnitin f th ypt f antritin (fr xap,a fair t apprpriaty rpnd t hngr) and diin-ihd tiatin t chang, cd b ratd t ditrbdintrcpti awarn. In particar, thr ight b aqaitati chang in th way that pcific intrcptiinfratin i prcd. Fr xap, indiida withAN ight xprinc an ari icra natin whnxpd t fd r fd-ratd tii. Thi xprincight fndantay atr th rward-ratd prprtif fd and rt in a bia tward ngati tinaity.mrr, th ari intrcpti xprinc aciatdwith fd ight triggr tp-dwn datry prcaid at anticipating and iniizing th xpr tfd tii (har aidanc), which ad t incradanticipatry prcing aid t rdc th xpr t
th ariy ad ti. Thrfr, indiida withAN ight xhibit attnatd rpn t th idiatrward-ratd igna f fd (rdcing hngr) bt hwincrad rpn t th ng-tr rward-igna a-ciatd with th ga f wight rdctin r thr idacgniti cntrct. Finay, th antrir ina ha bnipicatd in rik prdictin rrr150, ggting thatipairnt in ina fnctin ight ad t anaattitd in a cntxt f ncrtainty and th cntribtt har aidanc.
Thrfr, gin th prinnt atratin in inaactiity in indiida with AN, n ight pcat thatthy xprinc an atrd nitiity t r intgratin fintrna bdy igna. spcificay, th prjctin f thantrir ina t th antrir cingat ay datth dgr t which cgniti cntr i ngagd t atrbhair tward pr dciin aking that d ntbr th htatic wight baanc bt intadrt in prgri wight .
A neurocircuitry of appetite regulation in AN. Badn th ab prc and aciatd brain ara, wcan bgin t ab a nra yt prcingd f AN (FIG. 4). spcificay, tp-dwn (crtica)apificatin f anticipatry igna ratd t fdr tii aciatd with atity igna (intgratdwithin th ina)cd triggr bhaira tratgifr aiding xpr t fd. Th anticipatry int-rcpti tii ar aciatd with an ari bdytat that rb apct f th phyigica tatf th bdy aftr fding. Thi abnra rpn tfd anticipatin ight fnctin a a arning ig-na t frthr incra aidanc bhair, that i,t ngag in actiiti aid at iniizing xpr tfd. spcificay, tii that prdict fd intak, cha dipay f fd r fd , cd gnrat abdy prdictin rrr, rting fr cparing thcrrnt bdy tat with th anticipatd bdy tat (frxap, fing atiatd) aftr fding. Thi prdictinrrr wd gnrat a tiatina r apprach igna
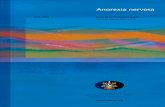
Figure 4 | ima baan btwn ntt an wa ng. We
propose that subjects with anorexia nervosa (AN) experience a strong conflict between
the biological need for food and the acquired aversive association with food. In healthy
individuals, the presentation of foodrelated stimuli is associated with ascending
interoceptive afferents that converge on the anterior insula, which processes
staterelated positive or negative valuation of these signals. In individuals with AN this
interoceptive information is biased towards the negative or aversive properties of food.
As a consequence, topdown, cortical circuits (dotted box) are engaged to resolve theconflict between the need for food and the aversive interoceptive evaluation,
processed in the anterior insula. Thus, topdown modulatory circuits are overengaged
in people with AN, which emerges on a symptomatic level as high anticipatory
reactivity, behavioural rigidity and excessive worry about future events. On a biological
level, these dysfunctions are implemented in a neural system consisting of the
ascending interoceptive pathways, the insular cortex, the amygdala and the anterior
cingulate cortex (not shown). This information converges in the striatum, which receives
inputs from the anterior insula (for the integrated bottomup information) and the
prefrontal cortex (for the topdown modulation relating to cognitive control circuits).
The excessive topdown cognitive control in subjects with AN in response to
interoceptive stimuli alters the striatal responses, shifting the behavioural event horizon
towards satisfying longterm goals (avoiding food, getting thin) rather than shortterm
goals (eating food).
R E V I E W S
580 | AuGusT 2009 | volume 10 www.nat.m/w/n
2009 Macmillan Publishers Limited. All rights reserved
-
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
9/12
in hathy indiida bt ight ad t an aidancigna in AN.
Th dra and ntra nrcircit dcribd ariright b ind in th prc: Th ACC, n fth prjctin ara f th inar crtx, i iprtantin prcing th cnfict btwn aaiab bhairand tc, fr xap, ha I at thi cak and at-ify y hngr nw r ha I nt at thi cak and taythin?151. Th oFC, anthr prjctin ara f th ant-rir inar crtx152, can dynaicay adjt rward
aatin bad n th crrnt bdy tat f th indi-ida153. Th DPlFC can witch btwn cptingbhaira prgra bad n th rrr igna itrci fr th ACC154.
Athgh w d nt prp hr that AN i an ina-pcific dirdr, w pcat that an atrd inarpn t fd-ratd tii i an iprtant cp-nnt f thi dirdr. If thi i indd th ca, n wdnd t dtrin whthr ina-pcific intrntin,ch a nitizatin r habitatin f intrcpti ni-tiity thrgh ra-ti nitring f th inar crtx
actiatin, ight hp. mrr, cptatina dch a th that ha bn prpd fr addictin155ight prid a thrtica apprach t bttr ndrtandth cpx pathgy f thi dirdr.
Within th frawrk f th ntra and dranrcircit dcribd arir, thr ar a ptn-tia xpanatin fr thr cr cpnnt f cinicadyfnctin in AN. Ngati affct ch a anxityand har aidanc and anhdnia cd b ratdt difficti in accraty cding r intgrating pi-ti and ngati tin within ntra triata cir-cit.Thr i cnidrab rap btwn circitthat dat tinaity and th rwarding apctf fd cnptin156. Fd i parab in hathyindiida bt fding i anxignic in indiida withAN, and taratin ight r t rdc dyphricd tat. Th nrbigic chani rpni-b fr ch bhair rain t b cidatd, bt it ipib that an nhancnt f 5-HT-ratd aritiatin, and/r diinihd DA-ratd apptitidri89,90 cntribt t th bhair.
Finay, it i pib that prfctini and b-ina prnaity trait ar ratd t xaggratd cgni-ti cntr by th DlPFC. Th DlPFC ight dpxci inhibitry actiity t dapn infratinprcing thrgh rward pathway157. Atrnatiy,incrad actiatin f cgniti pathway ight c-
pnat fr priary dficit in ibic fnctin: whnthr ar dficit in tina rgatin, rdpnd-nc pn cgniti r i a ranab tratgy ff-anagnt158. Th inabiity t fw n gt(r hart) that i, ak ffcti f intrcp-ti infratin i ipaird in indiida with AN.mrr, thr i a car hift away fr aing i-diat tc t th aciatd with dayd r ng-tr tc. Thi bhair i at cptyppit t that brd in indiida with ach rbtanc ab159 and i cnitnt with th bra-tin that indiida with AN ha w crbidity withdrg and ach dirdr160.
Conclusions and future directions
W prp that atic, atnic and icra infr-atin i abrranty prcd in pp wh ar -nrab t dping AN. Brain chang aciatdwith pbrty ight frthr chang th prc.Fr xap, rbita and dratra prfrnta crtxrgin dp graty dring and aftr pbrty161, andincrad actiity f th crtica ara ight b a caf th xci wrry, prfctini and tratgizingin pp with AN. It i pib that in bjct withAN, hypractiity f cgniti ntwrk in th dranrcircit (fr xap, DlPFC t dra triat)dirct tiatd actin whn th abiity f th ntratriata pathway t dirct r atatic r intititiatd rpn i ipaird. Anthr pibiity ithat in indiida with AN (thrwi adqat) ibic-triata infratin prcing in th ntra circit i ttrngy inhibitd by cnrging inpt fr cgnitidain ch a th DlPFC and th parita crtx.
It i pib that ch trait-ratd ditrbanc arratd t atrd nain nrna datin that
prdat th nt f AN and cntribt t prrbidtprant and prnaity ypt. spcificay,ditrbanc in th 5-HT yt cntribt t a nr-abiity fr rtrictd ating, bhaira inhibitin anda bia tward anxity and rrr prdictin, whraditrbanc in th DA yt cntribt t an atrdrpn t rward. sra factr ight act n th
nrabiiti t ca th nt f AN in adcnc.Firt, pbrty-ratd fa gnada trid r ag-ratd chang ight xacrbat 5-HT and DA ytdyrgatin. scnd, tr and/r ctra and ci-ta prr ight cntribt by incraing anxiand bina tprant. Indiida find thatrtricting fd intak i pwrfy rinfrcing bcait prid a tprary rpit fr dyphric d.Pp with AN ntr a ici cyc which cdaccnt fr th chrnicity f thi dirdr bcaating xaggrat, whra fd rfa rdc, ananxi d.
Th tprant and prnaity trait that ightcrat a nrabiity t dp AN ight a ha apiti apct. Th trait incd attntin t dtai,cncrn abt cnqnc and a dri t accpihand ccd. It i r cinica xprinc that anyindiida wh rcr fr AN d w in if. It itpting t pcat that th abiity t pan ahad, cn-tr ip, and aid har ight ha had highy
adapti a fr anctr wh id in nirnntwhr fd ppi wr cntraind by ng pridf cd wathr (fr xap, wrry in Jy abt fdppi in Janary). Adcnc i a ti f tranitin:indiida a th crity f thir h nirnntand t arn t baanc idiat and ng-trnd and ga t achi indpndnc158. Fr chindiida, arning t fxiby intract with and atrcpx and ixd ctra and cita ag andprr and cp with tr, ight b diffict andrwhing, which cd xacrbat pib ndr-ying trait f har aidanc and a dir t achiprfctin.
R E V I E W S
NATuRe RevIeWs |NeuroscieNce volume 10 | AuGusT 2009 |581
2009 Macmillan Publishers Limited. All rights reserved
-
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
10/12
AN ha th hight rtaity rat f any pychi-atric dirdr. It i xpni t trat and w ha
inadqat thrapi. It i crcia t ndrtand thnrbigic cntribtin and thir intractinwith th nirnnt, in rdr t dp r ffc-ti thrapi. Thrfr, ftr iaging tdi hdfc n charactrizing nra circit, thir fnctin
and thir ratinhip t bhair in indiida withAN. Gntic tdi ight hd ight n th cpx
intractin f c within th nra circit.Finay, prpcti and ngitdina tdi hdfc n idntifying th nrbigic trait andxtrna factr (BOX 2) that crat a cptibiity frdping AN.
Box 2 | From vulnerability to illness the complex aetiology of anorexia nervosa
Anorexianervosa(AN)isthoughttobeadisorderofcomplexaetiology,inwhichgenetic,biological,psychologicaland
socioculturalfactors,andinteractionsbetweenthem,seemtocontributesignificantlytosusceptibility10,11,158,162.Because
nosinglefactorhasbeenshowntobeeithernecessaryorsufficientforcausinganorexianervosa,amultifactorial
thresholdmodelmightbemostappropriate(forareviewseeREF. 158).Typically,ANbeginswitharestrictivedietand
weightlossduringteenageyears,whichprogressestoanout-of-controlspiral(FIG. 1).Therefore,individualsmightcross
athresholdinwhichapremorbidtemperament,interactingwithstressand/orpsychosocialfactors,progressestoan
illnesswithimpairedinsightandapowerful,obsessivepreoccupationwithdietingandweightloss.Adolescenceisatimeofprofoundbiological,psychologicalandsocioculturalchange,anditdemandsaconsiderabledegreeofflexibilityto
successfullymanagethetransitionintoadulthood.Psychologically,changemightchallengetheperfectionism,harm
avoidanceandrigidityofthoseatriskofANandthusfuelanunderlyingvulnerability.Thebiologicalchangesof
adolescenceorpubertymightalsoincreasetheriskofonsetofeatingdisorders.Thispossibilityissupportedbytwin
studies163whichimpliedthatpubertymighthavearoleinactivatingthegeneticpredispositionforeatingdisorder
symptoms.Moreover,thebiologicalchangesassociatedwithadolescencedifferbetweenmalesandfemales,which
couldexplainthesexualdimorphismofAN.Forexample,menarcheisassociated158witharapidchangeinbody
compositionandneuropeptidesmodulatingmetabolism.Littleisknownaboutwhethertheriseinoestrogenlevels
associatedwithpubertyinfemalesiscontributorytoAN,butitcouldaffectneuromodulatorysystemssuchas
serotonin164orneuropeptides165thataffectfeeding,emotionalityandotherbehaviours.
1. American Psychiatric Association. Diagnostic and
Statistical Manual of Mental Disorders 4th edn
(American Psychiatric Association, Washington, DC
1994).
2. Lilenfeld, L. R. et al. A controlled family study of
anorexia nervosa and bulimia nervosa: psychiatric
disorders in first-degree relatives and effects of proband
comorbidity.Arch.Gen.Psychiatry55, 603610
(1998).
3. Walters, E. E. & Kendler, K. S. Anorexia nervosa andanorexic-like syndromes in a population-based female
twin sample.Am. J. Psychiatry152, 6471 (1995).
4. Berrettini, W. Genetics of psychiatric disease.Annu.
Rev.Med.51, 465479 (2000).
5. Bulik, C. et al. Prevalence, heritability and prospective
risk factors for anorexia nervosa.Arch. Gen.
Psychiatry63, 305312 (2006).
6. Wade, T., Martin, N. G. & Tiggemann, M. Genetic and
environmental risk factors for the weight and shape
concerns characteristic of bulimia nervosa. Psychol.
Med.28, 761771 (1998).
7. Rutherford, J., McGuffin, P., Katz, R. J. & Murray, R. M.
Genetic influences on eating attitudes in a normal
female twin population. Psychol.Med.23, 425436.
8. Bulik, C., Slof-Opt Landt M, van Furth, E. & Sullivan, P.
The genetics of anorexia nervosa.Ann.Rev.Nutr.27,
263275 (2007).
9. Strober, M., Freeman, R., Lampert, C., Diamond, J. &
Kaye, W. Controlled family study of anorexia nervosa
and bulimia nervosa: evidence of shared liability andtransmission of partial syndromes.Am.J.Psychiatry
157, 393401.
10. Lilenfeld, L., Wonderlich, S., Riso, L. P., Crosby, R. &
Mitchell, J. Eating disorders and personality: a
methodological and empirical review. Clin.Psychol.Rev.26, 299320 (2006).
This paper, which reviews the relationship between
personality and eating disorders, shows that negative
emotionality, perfectionism, drive for thinness, poor
interoceptive awareness, ineffectiveness and obses-
sive-compulsive personality traits are probable
predisposing factors for AN and BN.
11. Stice, E. Risk and maintenance factors for eating
pathology: a meta-analytic review. Psychopharm. Bull.
128, 825848 (2002).
12. Anderluh, M. B., Tchanturia, K., Rabe-Hesketh, S. &
Treasure, J. Childhood obsessive-compulsive
personalitiy traits in adult women with eating
disorders: defining a broader eating disorder
phenotype.Am.J.Psychiatry. 160, 242247 (2003).
One of the first studies to find that childhood traits
reflecting obsessive-compulsive personality seem
to be important risk factors for the development of
eating disorders. Such traits may represent
markers of a broader phenotype for a specific
subgroup of patients with AN.
13. Bulik, C. et al. Genetic epidemiology, endophenotypes,
and eating disorder classification. Int. J. Eat. Disord.40, S52S60 (2007).
14. Pollice, C., Kaye, W. H., Greeno, C. G. & Weltzin, T. E.
Relationship of depression, anxiety, and obsessionality
to state of illness in anorexia nervosa. Int.J.Eat.
Disord.21, 367376 (1997).
15. Katzman, D. K. et al. Cerebral gray matter and white
matter volume deficits in adolescent girls with
anorexia nervosa.J.Pediat.129, 794803 (1996).
16. Kaye, W., Wagner, A., Frank, G., U. F. Review of brain
imaging in anorexia and bulimia nervosa inAnnual
Review of Eating Disorders, Part 2 (eds Wonderlich,
S., Mitchell, J., De Zwann, M. & Steiger, H.) 113130
(Radcliffe Publishing Ltd, Abingdon UK, 2006).
17. Boyar, R. K. et al. Anorexia nervosa. Immaturity of the
24-hour luteinizing hormone secretory pattern.N. Engl. J. Med.291, 861865 (1974).
18. Schwartz, M. W., Woods, S. C., Porte, D. Jr, Seeley,
R. J. & Baskin, D. G. Central nervous system control of
food intake. Nature404, 661671 (2000).
19. Inui, A. Eating behavior in anorexia nervosaanexcess of both orexigenic and anorexigenic signalling?
Mol.Psychiatry. 6, 620624 (2001).
20. Jimerson, D., Wolfe, B. Psychobiology of eating
disorders inAnnual Review of Eating Disorders, Part 2
(eds Wonderlich, S., Mitchell, J., De Zwann, M. &
Steiger, H.) 115 (Radcliffe Publishing Ltd, Abingdon
UK, 2006).
21. Kaye, W. H. et al. Elevated cerebrospinal fluid levels of
immunoreactive corticotropin-releasing hormone in
anorexia nervosa: relation to state of nutrition,
adrenal function, and intensity of depression.J.Clin.
Endocrinol.Metab.64, 203208 (1987).
22. Godart, N. et al. Comorbidity studies of eating
disorders and mood disorders. Critical review of the
literature.J. Affect. Disord.97, 3749 (2007).
23. Kaye, W. et al. Comorbidity of anxiety disorders with
anorexia and bulimia nervosa.Am.J.Psychiatry161,
22152221 (2004).
24. Wagner, A. et al. Personality traits after recovery from
eating disorders: do subtypes differ? Int.J.Eat.
Disord.39, 276284 (2006).
25. Steinhausen, H. C. The outcome of anorexia nervosa
in the 20th century.Am. J. Psychiatry159,
12841293 (2002).
26. Strober, M., Freeman, R. & Morrell, W. The long-term
course of severe anorexia nervosa in adolescents:
survival analysis of recovery, relapse, and outcome
predictors over 1015 years in a prospective study.Int.J.Eat. Disord.22, 339360 (1997).
27. Casper, R. C. Personality features of women with good
outcome from restricting anorexia nervosa.
Psychosom. Med.52,156170 (1990).
28. Srinivasagam, N. M. et al. Persistent perfectionism,
symmetry, and exactness after long-term recovery
from anorexia nervosa.Am.J.Psychiatry 152,
16301634 (1995).
29. Phillips, M., Drevets, W. R. & Rauch, S. L. Neurobiology
of emotion perception II: implications for major
psychiatric disorders Biol.Psych.54, 515528 (2003).
30. Phillips, M., Drevets, W. R., Rauch S. L. & Lane, R.
Neurobiology of emotion perception I: The neural
basis of normal emotion perception Biol.Psych.54,
504514 (2003).
References 29 and 30 provide an outstanding
synthesis of neural processes underlying emotional
perception, as well as how distinct patterns of
structural and functional abnormalities in neural
systems important for emotion processing areassociated with specific symptoms of schizophrenia
and bipolar and major depressive disorder.
31. Gordon, I., Lask, B., Bryant-Waugh, R., Christie, D. &
Timimi, S. Childhood-onset anorexia nervosa: towards
identifying a biological substrate. Int.J. Eat.Disord.
22, 159165 (1997).
32. Rastam, M. et al. Regional cerebral blood flow in
weight-restored anorexia nervosa: a preliminary
study. Dev.Med.Child.Neurol.43, 239242 (2001).
33. Uher, R. et al. Recovery and chronicity in anorexia
nervosa: brain activity associated with differential
outcomes. Biol.Psychiatry54, 934942 (2003).
One of the first neuroimaging studies to identify
neural correlates of food stimuli that underlie trait
and state characteristics of AN.
34. Drevets, W. R. et al. Serotonin-1A receptor imaging in
recurrent depression: replication and literature review.
Nucl.Med.Biol.34, 865877 (2007).
R E V I E W S
582 | AuGusT 2009 | volume 10 www.nat.m/w/n
2009 Macmillan Publishers Limited. All rights reserved
-
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
11/12
35. Lanzenberger, R. et al. Reduced serotonin-1A receptor
binding in social anxiety disorder. Biol.Psychiatry61,
10811089 (2007).
36. Neumeister, A. et al. Reduced serotinin type 1A
receptor
binding in panic disorder.J.Neurosci.24, 589591
(2004).
37. Tiihonen, J. et al. Brain serotonin 1A receptor binding in
bulimia nervosa. Biol.Psychiatry55, 871873 (2004).
38. Galusca, B. et al. Organic background of restrictive-
type anorexia nervosa suggested by increased
serotonin1A
receptor binding in right frontotemporal
cortex of both lean and recovered patients: [
18
F]MPPFPET scan study. Biol.Psychiatry64, 10091013 (2008).
39. Bailer, U. F. et al. Exaggerated 5-HT1A
but normal
5-HT2A
receptor activity in individuals ill with anorexia
nervosa. Biol.Psychiatry61, 10901099 (2007).
40. Bailer, U. F. et al. Altered brain serotonin 5-HT1A
receptor binding after recovery from anorexia nervosa
measured by positron emission tomography and
[Carbonyl11C]WAY-100635.Arch.Gen.Psychiatry62,
10321041 (2005).
41. Simansky, K. J. Serotonergic control of the
organization of feeding and satiety. Behav.BrainRes.
73, 3742 (1996).
42. Soubrie, P. Reconciling the role of central serotonin
neurons in human and animal behavior. Beh.Brain
Sci.9, 319364 (1986).
43. Fairbanks, L., Melega, W., Jorgensen, M., Kaplan, J. &
McGuire, M. Social impulsivity inversely associated
with CSF 5-HIAA and fluoxetine exposure in vermet
monkeys. Neuropsychopharmacology24, 370378
(2001).
44. Lesch, K., Merschdorf, U. Impulsivity, aggression, and
serotonin: a molecular psychobiological perspective.
Behav.Sci.Law185,581604 (2000).
45. Mann, J. J. Role of the serotonergic system in the
pathogenesis of major depression and suicidal behavior.
Neuropsychopharmacology21, S99S105 (1999).
46. Brewerton, T. D., Brandt, H. A., Lessem, M. D.,
Murphy, D. L., Jimerson, D. C. Serotonin in eating
disorders in Serotonin in Major Psychiatric Disorders
(Progress in Psychiatry). (eds Coccaro, E. F. & Murphy,
D. L.) 155184 (American Psychiatric Press,
Washington DC, 1990) .
47. Kaye, W. H., Frank, G., Bailer, U. F. & Henry, S.
Neurobiology of anorexia nervosa: clinical implications
of alterations of the function of serotonin and other
neuronal systems. Int.J.Eat. Disord.37, S15S19
(2005).
48. Stanley, M., Traskman-Bendz, L. & Dorovini-Zis, K.
Correlations between aminergic metabolites
simultaneously obtained from human CSF and brain.
LifeSci.37, 12791286 (1985).49. Frank, G. K. et al. Reduced 5-HT2A receptor binding
after recovery from anorexia nervosa. Biol.Psychiatry
52, 896906 (2002).
50. Bailer, U. F. et al. Altered 5-HT2A
receptor binding after
recovery from bulimia-type anorexia nervosa:
relationships to harm avoidance and drive for thinness.
Neuropsychopharmacology 29, 11431155 (2004).
51. Audenaert, K. et al. Decreased 5-HT2a
receptor
binding in patients with anorexia nervosa.J.Nucl.
Med.44, 163169 (2003).
52. Frank, G. K. et al. Altered response to meta-
chlorophenylpiperazine in anorexia nervosa: support
for a persistent alteration of serotonin activity after
short-term weight restoration. Int.J.Eat. Disord.30,
5768 (2001).
53. Kaye, W. H. et al. Anxiolytic effects of acute
tryptophan depletion in anorexia nervosa. Int.J.Eat.
Disord.33, 257267 (2003).
54. Cloninger, C. R., Przybeck, T. R., Svrakic, D. M.,
Wetzel, R. D. in The temperament and characterinventory (TCI): a guide to its development and use .
(Center for Psychobiology of Personality, Washington
University, St Louis, Missouri, USA, 1994).
55. File, S. E., Kenny, P. J. & Cheeta, S. The role of the
dorsal hippocampal serotonergic and cholinergic
systems in the modulation of anxiety. Pharmacol.
Biochem.Behav.66, 6572 (2000).
56. Tauscher, J. et al. Inverse relationship between
serotonin 5-HT1A
receptor binding and anxiety: a [11C]
WAY-100635 PET investigation in healthy volunteers.
Am.J.Psychiatry158,13261328 (2001).
57. Weisstaub, N. et al. Cortical 5-HT2A receptor signaling
modulates anxiety-like behaviors in mice. Science
313, 536540 (2006).
58. Moresco, F. M. et al.In vivo serotonin 5HT2A
receptor
binding and personality traits in healthy subjects: A
positron emission tomography study. NeuroImage17,
14701478 (2002).
59. Amargos-Bosch, M. et al. Co-expression and in vivo
interaction of serotonin1A
and serotonin2A
receptors in
pyramidal neurons of prefrontal cortex. Cereb. Cortex
14, 281299 (2004).
60. Varnas, K., Halldin, C. & Hall, H. Autoradiographic
distribution of serotonin transporters and receptor
subtypes in human brain. Hum.Brain Mapp. 22,
246260 (2004).
61. Santana, N., Bortolozzi, A., Serrats, J., Mengod, G. &
Artigas, F. Expression of serotoinin1A
and serotonin2A
receptor in pyramidal and GABAergic neurons of the
rat prefrontal cortex. Cereb. Cortex. 14, 11001109(2004).
62. Carli, M., Baviera, M., Invernizzi, R. & Balducci, C.
Dissociable contribution of 5-HT1A and 5-HT2A
receptors in the medial prefrontal cortex to different
aspects of executive control such as impulsivity and
compulsive perseveration in rats
Neuropsychopharmacology31, 757767 (2006).
63. Winstanley, C. A. et al. Intra-prefrontal 8-OH-DPAT
and M100907 improve visuospatial attention and
decrease impulsivity on the five-choice serial reaction
time task in rats. Psypchopharmacology(Berl.)167,
304314 (2003).
64. Krebs-Thomson, K. & Geyer, M. A. Evidence for a
functional interaction between 5-HT1A
and 5-HT2A
receptors in rats. Psychopharmacology(Berl.)140,
6974 (1998).
65. Strober, M. Family-genetic perspectives on anorexia
nervosa and bulimia nervosa. in Eating Disorders and
Obesity - A Comprehensive Handbook (eds Brownell,
K. & Fairburn, C.) 212218 (The Guilford Press, New
York,1995).
66. Vitousek, K. & Manke, F. Personality variables and
disorders in anorexia nervosa and bulimia nervosa.
J. Abnorm.Psychol.103,137147 (1994).
67. Fernstrom, J. D. & Wurtman, R. J. Brain serotonin
content: physiological regulation by plasma neutral
amino acids. Science178, 414416 (1972).
68. Kaye, W. H., Gwirtsman, H. E., George, D. T. & Ebert,
M. H. Altered serotonin activity in anorexia nervosa
after long-term weight restoration. Does elevated
cerebrospinal fluid 5-hydroxyindoleacetic acid level
correlate with rigid and obsessive behavior?Arch.
Gen.Psychiatry48, 556562 (1991).
69. Simansky, K. J. et al. A 5-HT2C
agonist elicits
hyperactivity and oral dyskinesia with hypophagia in
rabbits. Physiol.Behav.82, 97107 (2004).
70. Young, S. N. & Gauthier, S. Effect of tryptophan
administration on tryptophan, 5- hydroxyindoleacetic
acid and indoleacetic acid in human lumbar and
cisternal cerebrospinal fluid.J. Neurol. Neurosurg.
Psychiatry44, 323327 (1981).71. Anderson, I. M., Parry-Billings, M., Newsholme, E. A.,
Fairburn, C. G. & Cowen, P. J. Dieting reduces plasma
tryptophan and alters brain 5-HT function in women.
Psychol.Med.20, 785791 (1990).
72. Schweiger, U., Warnhoff, M., Pahl, J. & Pirke, K. M.
Effects of carbohydrate and protein meals on plasma
large neutral amino acids, glucose, and insulin
plasma levels of anorectic patients. Metabolism35,
938943 (1986).
73. Attia, E., Wolk, S., Cooper, T., Glasofer, D. & Walsh, B.
Plasma tryptophan during weight restoration in
patients with anorexia nervosa. Biol.Psychiatry57,
674678 (2005).
74. Kaye, W. H., Gwirtsman, H. E., George, D. T.,
Jimerson, D. C. & Ebert, M. H. CSF 5-HIAA
concentrations in anorexia nervosa: reduced values
in underweight subjects normalize after weight gain.
Biol.Psychiatry23, 102105 (1988).
75. Klump, K. et al. Personality characteristics of women
before and after recovery from an eating disorder.Psych. Med.34,14071418 (2004).
76. Frank, G. et al. Increased dopamine D2/D3 receptor
binding after recovery from anorexia nervosa
measured by positron emission tomography and
[11C]raclopride. Biol.Psychiatry58, 908912
(2005).
77. Kaye, W. H., Frank, G. K. & McConaha, C. Altered
dopamine activity after recovery from restricting-type
anorexia nervosa. Neuropsychopharmacology21,
503506 (1999).
78. Bergen, A. et al. Association of multiple DRD2
polymorphisms with anorexia nervosa.
Neuropsychopharmacology30,17031710 (2005).
79. Lawrence, A. Impaired visual discrimination learning in
anorexia nervosa.Appetite20, 8589 (2003).
80. Montague, R., Hyman, S. & Cohen, J. Computational
roles for dopamine in behavioural control. Nature
431, 760767 (2004).
81. Schultz, W. Neural coding of basic reward terms of
animal learning theory, game theory, microeconomics
and behavioural ecology. Science14, 139147 (2004).
This is an excellent summary of the new approach
proposed by Schultz and others as to the function
of dopamine in learning and reward. Specifically, it
implicates dopamine as a key learning signal that
functions to alter relative preferences among
available choices.
82. Wagner, A. et al. Altered reward processing in women
recovered from anorexia nervosa.Am.J.Psych.
164,18421849 (2007).83. Delgado, M., Nystrom, L., Fissel, C., Noll, D. & Fiez, J.
Tracking the hemodynamic responses to reward and
punishment in the striatum.J.Neurophysiol. 84,
30723077 (2000).
84. Berridge, K. & Robinson, T. What is the role of
dopamine in reward: hedonic impact, reward learning,
or incentive salience? BrainRes.28, 309369 (1998).
85. Halmi, K. et al. Predictors of treatment acceptance
and completion in anorexia nervosa.Arch.Gen.
Psychiatry62, 776781 (2005).
86. Tricomi, E. M., Delgado, M. R. & Fiez, J. A. Modulation
of caudate activity by action contingency. Neuron41,
281292 (2004).
87. Lopez, C. et al. An examination of the concept of
central coherence in women with anorexia nervosa.
Int.J.Eat.Disord.41, 143152 (2008).
88. Zastrow, A. et al. Neural correlates of impaired
cognitive-behavioral flexibility in anorexia nervosa.Am.J.Psychiatry166, 608616 (2009).
This paper shows that impaired behavioural response
shifting in AN is associated with hypoactivation in the
ventral anterior cingulate-striato-thalamic loop that is
involved in motivation-related behaviour. By contrast,
subjects with AN have predominant activation of
frontoparietal networks that is indicative of effortful
and supervisory cognitive control during task
performance.
89. Daw, N. D., Kakade, S. & Dayan, P. Opponent
interactions between serotonin and dopamine. Neural
Networks15, 603616 (2002).
90. Cools, R., Roberts, A. & Robbins, T. Serotoninergic
regulation of emotional and behavioural control
processes. TrendsCogn.Sci.12, 3140 (2008).
91. De Deurwaerdere, P., Navailles, S., Berg, K., Clarke, W.
& Spampinato, U. Constitutive activity of the
serotonin2C receptor inhibits in vivo dopamine release
in the rat striatum and nucleus accumbens.J.
Neurosci.24, 32353241 (2004).
92. Di Matteo, V., Di Giovanni, G., Di Mascio, M. &
Esposito, E. Biochemical and electrophysiological
evidence that RO 600175 inhibits mesolimbicdopaminergic function through serotonin
2Creceptors.
BrainRes.865, 8590 (2000).
93. Schweighofer, N., Tanaka, S. & Doya, K. Serotonin and
the evaluation of future rewards: theory, experiments,
and possible neural mechanisms.Ann.NYAcad.Sci.
1104, 289300 (2007).
94. McClure, S., Laibson, D., Loewenstein, G. & Cohen, J.
Separate neural systems value immediate and delayed
monetary rewards. Science306, 503507 (2004).
A study in which the authors propose that two
competing systems, that is, the prefrontal cortex
and the subcortical striatum, underlie the
computation of the immediate and delayed value.
95. Westergaard, G. et al. Physiological correlates of
aggression and impulsivity in free-ranging female
primates. Neuropsychopharmacology28,
10451055 (2003).
96. Attia, E., Schroeder, L. Pharmacologic treatment of
anorexia nervosa: where do we go from here? Int.J.
Eat.Disord.37, S60S63 (2005).97. Tollefson, G. D. Selective serotonin reuptake inhibitors.
in Textbook of Psychopharmacology. (Schatzberg,
A. F. & Nemeroff, C. B.) 161182 (American
Psychiatric Press, Inc. Washington DC,1995).
98. Blier P, de Montigny, C. Serotonin and drug-induced
therapeutic responses in major depression, obsessive-
compulsive and panic disorders.
Neuropsychopharmacology21, S91S98 (1999).
99. Bissada, H., Tasca, G. A., Barber, A. M. & Bradwejn, J.
Olanzapine in the treatment of low body weight and
obsessive thinking in women with anorexia nervosa: a
randomized, double-blind, placebo-controlled trial.
Am. J. Psych.165,12811288 (2008).
100. Elman, I., Borsook, D. & Lukas, S. E. Food intake and
reward mechanisms in patients with schizophrenia:
implications for metabolic disturbances and treatment
with second-generation antipsychotic agents.
Neuropsychopharmacology31, 20912120 (2006).
R E V I E W S
NATuRe RevIeWs |NeuroscieNce volume 10 | AuGusT 2009 |583
2009 Macmillan Publishers Limited. All rights reserved
-
8/14/2019 New insights into symptoms and neurocircuit function of anorexia nervosa
12/12
101. Kelley, A. E. Ventral striatal control of appetite
motivation: role in ingestive behavior and reward-related
learning. Neurosci. Biobehav. Rev.27, 765776 (2004).
102. Saper, C. B., Chou, T. C., Elmquist, J. K. The need to
feed: homeostatic and hedonic control of eating.
Neuron36:199211 (2002) .
103. Fernstrom, M. H., Weltzin, T. E., Neuberger, S.,
Srinivasagam, N. & Kaye, W. H. Twenty-four-hour food
intake in patients with anorexia nervosa and in healthy
control subjects. Biol.Psychiatry36, 696702 (1994).
104. Drewnowski, A., Pierce, B. & Halmi, K. A. Fat aversion
in eating disorders.Appetite10, 119131 (1988).105. Garfinkel, P., Moldofsky, H. & Garner, D. M. The
stability of perceptual disturbances in anorexia
nervosa. Psychol.Med.9, 703708 (1979).
106. Santel, S., Baving, L., Krauel, K., Mnte, T. & Rotte, M.
Hunger and satiety in anorexia nervosa: fMRI during
cognitive processing of food pictures. BrainRes.1114,
138148 (2006).
107. Small, D. Central gustatory processing in humans.Adv.
Otorhinolaryngol. 63, 191220 (2006).
108. Chandraskekar, J., Hoon, M., Ryba, N. & Zuker, C. The
receptors and cells for mammalian taste. Nature444,
288294 (2006).
109. Ogawa, H. Gustatory cortex of primates: anatomy and
physiology. Neurosci.Res.20, 113 (1994).
110. Scott, T. R., Yaxley, S., Sienkiewicz, Z. & Rolls, E.
Gustatory responses in the frontal opercular cortex of
the alert cynomolgus monkey.J.Neurophysiol. 56,
876890 (1986).
111. Yaxley, S., Rolls, E. & Sienkiewicz, Z. Gustatory
responses of single neurons in the insula of the macaque
monkey.J.Neurophysiol.63, 689700 (1990).
112. Faurion, A. et al. Human taste cortical areas studied
with functional magnetic resonance imaging: evidence
of functional lateralization related to handedness.
Neurosci.Lett.277, 189192 (1999).
113. Schoenfeld, M. et al. Functional magnetic resonance
tomography correlates of taste perception in the
human primary taste cortex. Neuroscience127,
347353 (2004).
114. ODoherty, J., Kringelbach, M. L., Rolls, E. T., Hornak,
J. & Andrews, C. Abstract reward and punishment
representations in the human orbitofrontal cortex.
NatureNeuroscience 4, 95102 (2001).
115. Schultz, W., Tremblay, L. & Hollerman, J. R. Reward
processing in primate orbitofrontal cortex and basal
ganglia. Cereb. Cortex10, 272284 (2000).
116. Small, D. Toward an understanding of the brain
substrates of reward in humans. Neuron22, 668671
(2002).
117. Small, D. M., Zatorre, R. J., Dagher, A., Evans, A. C. &
Jones-Gotman, M. Changes in brain activity related toeating chocolate: from pleasure to aversion. Brain
124,17201733 (2001).
118. Freedman, L. J., Insel, T. R. & Smith, Y. Subcortical
projections of area 25 (subgenual cortex) of the macaque
monkey.J. Comp. Neurol.421, 172188 (2000).
119. Ongur, D., An, X. & Price, J. Prefrontal cortical
projections to the hypothalamus in macaque monkeys.
J.Comp.Neurol.401, 480505 (1998).
120. Carter, C. S., Botvinick, M. M. & Cohen, J. D. The
contribution of the anterior cingulate cortex to
executive processes in cognition. Rev.Neurosci.10,
4957 (1999).
121. Critchley, H. D., Mathias, C. J. & Dolan, R. J. Neural
activity in the human brain relating to uncertainty and
arousal during anticipation. Neuron29, 537545
(2001).
122. Critchley, H. D. et al. Human cingulate cortex and
autonomic control: converging neuroimaging and
clinical evidence. Brain126, 21392152 (2003).
123. Furuyashiki, T., Holland, P. & Gallagher, M.Rat orbitofrontal cortex separately encodes response
and outcome information during performance of goal-
directed behavior.J.Neurosci.28, 51275138
(2008).
124. Gottfried, J., ODoherty, J. & Dolan, R. Encoding
predictive reward value in human amygdala and
orbitofrontal cortex. Science301, 11041107 (2003).
125. Hare, T. A., ODoherty, J., Camerer, C. F., Schultz, W. &
Rangel, A. Dissociating the role of the orbitofrontal
cortex and the striatum in the computation of goal
values and prediction errors.J.Neurosci.28,
56235630 (2008).
126. Roberts, A. Primate orbitofrontal cortex and adaptive
behaviour. TrendsCogn.Sci.10, 8390 (2006).
127. Tataranni, P. A. et al. Neuroanatomical correlates of
hunger and satiation in humans using positron
emission tomography. Proc.NatlAcad.Sci.USA96,
45694574 (1999).
128. Morris, J. S. & Dolan, R. J. Involvement of human
amygdala and orbitofrontal cortex in hunger-enhanced
memory for food stimuli.J.Neurosc. 21, 53045310
(2001).
129. Kringelbach, M. L., ODoherty, J., Rolls, E. & Andrews, C.
Activation of the human orbitofrontal cortex to a liquid
food stimulus is correlated with its subjective
pleasantness. Cereb. Cortex13, 10641071 (2003).
130. Uher, R., Treasure, J., Heining, M., Brammer, M. C. &
Campbell I. C. Cerebral processing of food-related
stimuli: effects of fasting and gender. Behav.Brain
Res.169, 111119 (2006).131. Chikama, M., McFarland, N., Amaral, D. H. & Haber
S. N. Insular cortical projections to functional regions
of the striatum correlate with cortical cytoarchitectonic
organization in the primate.J.Neurosci.17,
96869705 (1997).
132. Fudge, J., Breitbart, M., Danish, M. & Pannoni, V. Insular
and gustatory inputs to the caudal ventral striatum in
primates.J.Comp.Neurol.490,101118 (2005).
133. Wagner, A. et al. Altered insula response to a taste
stimulus in individuals recovered from restricting-type
anorexia nervosa. Neuropsychopharmacology33,
513523 (2008).
134. Ellison, Z. et al. Functional anatomy of calorie fear in
anorexia nervosa. Lancet 352,1192 (1998).
135. Gordon, C. M. et al. Neural substrates of anorexia
nervosa: a behavioral challenge study with positron
emission tomography.J.Pediatr.139, 5157 (2001).
136. Naruo, T. et al. Characteristic regional cerebral blood
flow patterns in anorexia nervosa patients with binge/
purge behavior.Am.J.Psychiatry157,15201522
(2000).
137. Nozoe, S. et al. Changes in regional cerebral blood
flow in patients with anorexia nervosa detected
through single photon emission tomography imaging.
Biol.Psychiatry34, 578580 (1993).
138. Uher, R. et al. Medial prefrontal cortex activity
associated with symptom provocation in eating
disorders.Am.J.Psychiatry. 161,12381246 (2004).
139. Devinsky, O., Morrell, M. J. & Vogt, B. A.
Contributions of anterior cingulate cortex to
behaviour. Brain118, 279306 (1995).
140. Critchley, H., Wiens, S., Rotshtein, P., Ohman, A. &
Dolan, R. Neural systems supporting interoceptive
awareness. NatureNeurosci.7, 189195 (2004).
One of the first neuroimaging studies to demonstrate
a direct association between interoceptive awareness
and perceived emotions. In a paradigm that asked
subjects to detect their heartbeat as accurately as
possible, activation of an interoceptive circuit
involving the anterior insula/frontal operculum (AI/FO)
was identified. AI/FO activation predicted accuracy inheartbeat detection, which in turn correlated with
indices of negative emotional experience.
141. Paulus, M. & Stein, M. B. An insular view of anxiety.
Biol.Psychiatry60, 383387 (2006).
142. Craig, A. How do you feel now? The anterior insula
and human awareness. NatureRev.Neurosci.10,
5970 (2008).
143. Craig, A. D. How do you feel? Interoception: the sense
of the physiological condition of the body. NatureRev.
Neurosci.3, 655666 (2002).
This paper reviews the afferent neural system in
non-human and human primates that represents all
aspects of the physiological condition of the physical
body. This system constitutes a representation of the
material me, and thus might provide a foundation for
subjective feelings, emotion and self-awareness.
144. Craig, A. Human feelings: why are some more aware
than others? TrendsCogn.Sci.8, 239241 (2004).
145. Damasio, A. et al. Subcortical and cortical brain
activity during the feeling of self-generated emotions.NatureNeurosci.3, 10491056 (2000).
146. Bruch, H. Perceptual and conceptual disturbances in
anorexia nervosa. Psychosom.Med.24, 187194
(1962).
147. Fassino, S., Piero, A., Gramaglia, C. & Abbate-Daga,
G. Clinical, psychopathological and personality
correlates of interoceptive awareness in anorexia
nervosa, bulimia nervosa and obesity.
Psychopathology37, 168174 (2004).
148. Garner, D. M., Olmstead, M. P. & Polivy, J.
Development and validation of a multidimensional
eating disorder inventory for anorexia and bulimia
nervosa. Int.J.Eat.Disord.2, 1534 (1983).
149. Pollatos, O. et al. Reduced perception of bodily signals
in anorexia nervosa. Eat.Behav.9, 381388 (2008).
150. Preuschoff, K., Quartz, S. & Bossaerts, P. Human
insula activation reflects risk prediction errors as well
as risk.J.Neurosci.28, 27452752 (2008).
This study uses an elegant design to disambiguate
the role of the insular cortex in risk-related
processing. In particular, the authors suggest that
the insula is important for both generating
prediction errors and risk (variance) related
processing.
151. Carter, C. S. et al. Parsing executive processes:
strategic vs. evaluative functions of the anterior
cingulate cortex. Proc. Natl Acad. Sci. USA97,
19441948 (2000).
152. Ongur, D. & Price, J. L. Organization of networks within
the orbital and medial prefrontal cortex of rats, monkeys,and humans. Cereb. Cortex10, 206219 (2000).
153. Rolls, E. T. The orbitofrontal cortex. Philos.Trans.R.
Soc.Lond. B Biol.Sci.351, 14331443 (1996).
154. Kerns, J. et al. Anterior cingulate conflict monitoring
and adjustments in control. Science303, 10231026
(2004).
155. Redish, A. Addiction as a computational process gone
awry. Science306, 19441947 (2004).
156.Volkow, N. D., Wise, R. A. How can drug addiction help
us understand obesity? NatureNeurosci.8, 555560
(2005).
157. Chambers, R., Taylor, J. & Potenza, M. Developmental
neurocircuitry of motivation in adolescence: a critical
period of addiction vulnerability.Am.J.Psych.160,
10411052 (2003).
158. Connan, F., Campbell, I., Katzman, M., Lightman, S. &
Treasure, J. A neurodevelopmental model for anorexia
nervosa. Physiol.Behav.79, 1324 (2003).
This excellent synthesis integrates genetic, biological,
cognitive and psychosocial factors, and interpersonal
stress, to generate a neurodevelopmental
hypothesis for the aetiology of AN.
159. Kirby, K., Petry, N. & Bickel, W. Heroin addicts have
higher discount rates for delayed rewards than
non-drug-using controls.J.Exp.Psychol.Gen.128,
7887 (1999).
160. Kaye, W., Wisniewski, L. Vulnerability to substance
abuse in eating disorders. NIDA Res.Monogr.159,
269311 (1996).
161. Huttenlocher, P. & Dabholkar, A. Regional differences
in synaptogenesis in human cerebral cortex.J.Comp.
Neurol.387, 167178 (1997).
162. Jacobi, C., Hayward C, de Zwaan, M., Kraemer, H. &
Agras, W. Coming to terms with risk factors for eating
disorders: application of risk terminology and suggestions
for a general taxonomy. Psych. Bull.130, 1965 (2004).
163. Klump, K., Burt, S., McGue, M. & Iacono, W. Changes
in genetic and environmental influences on disordered
eating across adolescence. A longitudinal twin study.
Arch.Gen.Psychiatry64, 14091415 (2007).
The authors of this study present data from the firstlongitudinal twin studies in eating disorders.
Findings highlight the transition from early to mid
adolescence as a crucial time for the emergence of a
genetic diathesis for disordered eating. The increase
in genetic effects during this developmental stage
corroborates previous research implicating puberty
in the genetic aetiology of eating disorders.
164. Rubinow, D. R., Schmidt, P. J. & Roca, C. A. Estrogen-
serotonin interactions: implications for affective
regulation. Biol.Psychiatry44, 839850.
165. Torpy, D. J., Papanicolaou, D. A. & Chrousos, G. P.
Sexual dismorphism of the human stress response
may be due to estradiol-mediated stimulation of
hypothalamic corticotropin-releasing hormone
synthesis.J.Clin.Endocrinol.Metab.82, 982 (1997).
166. Kaye, W. H. et al. Reduced cerebrospinal fluid levels of
immunoreactive pro- opiomelanocortin related
peptides (including beta-endorphin) in anorexia
nervosa. Life Sci.41, 21472155 (1987).
AcknowledgementsMuch of the research incorporated into this Review was sup-
ported for W.H.K. by the National Institute of Mental Health
(NIMH) (046001, 042984, 066122 and 001894) and the
Price Foundation, for J.L.F. by the NIMH (063291) and for
M.P. by the National Institute on Drug Abuse (016663,
018307 and 020687) and the Center of Excellence in Stress
and Mental Health.
DATABASESEntrez Gene:http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=gene
5HT1A
| 5HT2A
|DRD2 | DRD3
FURTHER INFORMATIONWalter H. Kayes homepage:http://eatingdisorders.ucsd.edu/
All liNks Are AcTive iN The oNliNe pdf
R E V I E W S
584 | AuGusT 2009 | volume 10 / /
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=genehttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=genehttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3350&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3350&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3356&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3356&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=1813&ordinalpos=9&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=1813&ordinalpos=9&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=1814&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=1814&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://eatingdisorders.ucsd.edu/http://eatingdisorders.ucsd.edu/http://eatingdisorders.ucsd.edu/http://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=1814&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=1813&ordinalpos=9&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3356&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=gene&Cmd=ShowDetailView&TermToSearch=3350&ordinalpos=1&itool=EntrezSystem2.PEntrez.Gene.Gene_ResultsPanel.Gene_RVDocSumhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=genehttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=gene