NEW EMPLOYEE CHECKLIST - Swaggart Brothers · NEW EMPLOYEE CHECKLIST. ... HRM-FRM-1202 Rev/Date:...
22
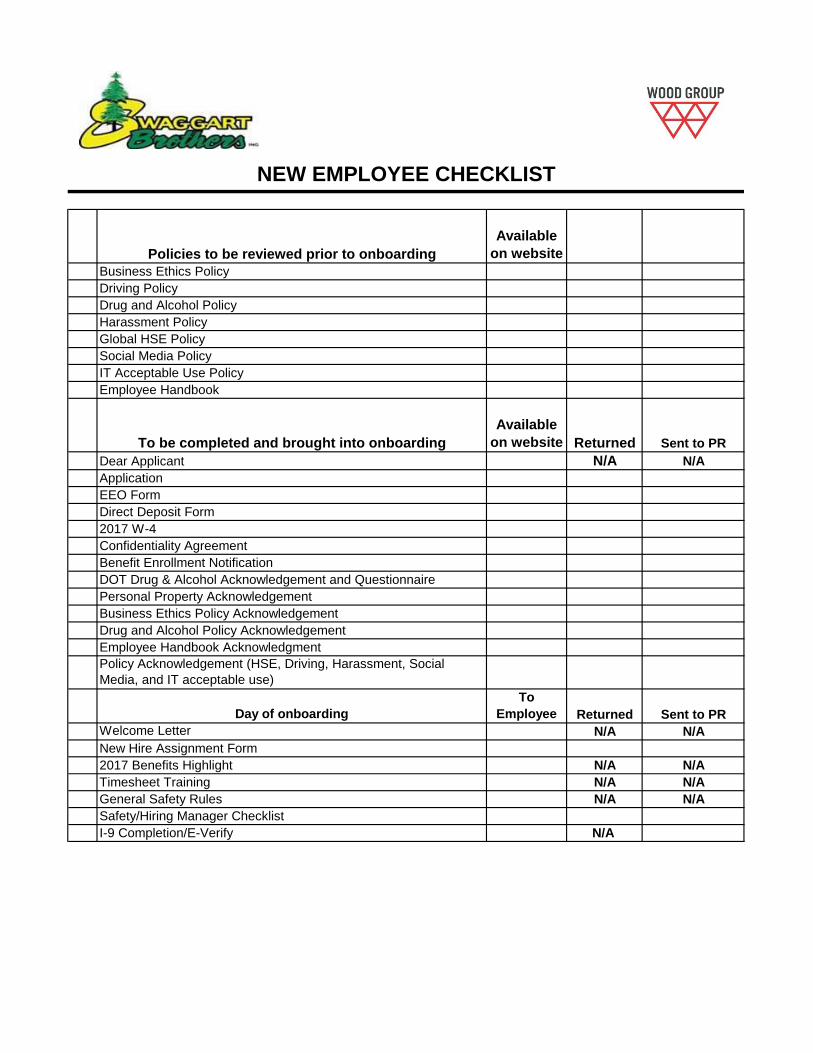
Policies to be reviewed prior to onboarding Available on website Business Ethics Policy Driving Policy Drug and Alcohol Policy Harassment Policy Global HSE Policy Social Media Policy IT Acceptable Use Policy Employee Handbook To be completed and brought into onboarding Available on website Returned Sent to PR Dear Applicant N/A N/A Application EEO Form Direct Deposit Form 2017 W-4 Confidentiality Agreement Benefit Enrollment Notification DOT Drug & Alcohol Acknowledgement and Questionnaire Personal Property Acknowledgement Business Ethics Policy Acknowledgement Drug and Alcohol Policy Acknowledgement Employee Handbook Acknowledgment Policy Acknowledgement (HSE, Driving, Harassment, Social Media, and IT acceptable use) Day of onboarding To Employee Returned Sent to PR Welcome Letter N/A N/A New Hire Assignment Form 2017 Benefits Highlight N/A N/A Timesheet Training N/A N/A General Safety Rules N/A N/A Safety/Hiring Manager Checklist I-9 Completion/E-Verify N/A NEW EMPLOYEE CHECKLIST
Transcript of NEW EMPLOYEE CHECKLIST - Swaggart Brothers · NEW EMPLOYEE CHECKLIST. ... HRM-FRM-1202 Rev/Date:...
Policies to be reviewed prior to onboarding
Available
on website
Business Ethics Policy
Driving Policy
Drug and Alcohol Policy
Harassment Policy
Global HSE Policy
Social Media Policy
IT Acceptable Use Policy
Employee Handbook
To be completed and brought into onboarding
Available
on website Returned Sent to PR
Dear Applicant N/A N/A
Application
EEO Form
Direct Deposit Form
2017 W-4
Confidentiality Agreement
Benefit Enrollment Notification
DOT Drug & Alcohol Acknowledgement and Questionnaire
Personal Property Acknowledgement
Business Ethics Policy Acknowledgement
Drug and Alcohol Policy Acknowledgement
Employee Handbook Acknowledgment
Policy Acknowledgement (HSE, Driving, Harassment, Social
Media, and IT acceptable use)
Day of onboarding
To
Employee Returned Sent to PR
Welcome Letter N/A N/A
New Hire Assignment Form
2017 Benefits Highlight N/A N/A
Timesheet Training N/A N/A
General Safety Rules N/A N/A
Safety/Hiring Manager Checklist
I-9 Completion/E-Verify N/A
NEW EMPLOYEE CHECKLIST
Dear Applicant:
Thank you for your interest in Swaggart Brothers, a division of Wood Group PSN. Attached you will find
the necessary forms that you must complete and bring with you to the office on the first day of hire.
You will not be permitted to start work unless you complete these forms before your start date.
Also, please click on the following link (http://www.swaggartbrothers.com/swaggart/wp-
content/uploads/2012/12/New-Hire-Policies-and-Handbooks.pdf) to read the related WGPSN policies
prior to your start date. The corresponding Acknowledgement Forms are included in this new hire
package and will need to be completed along with the rest of your paperwork.
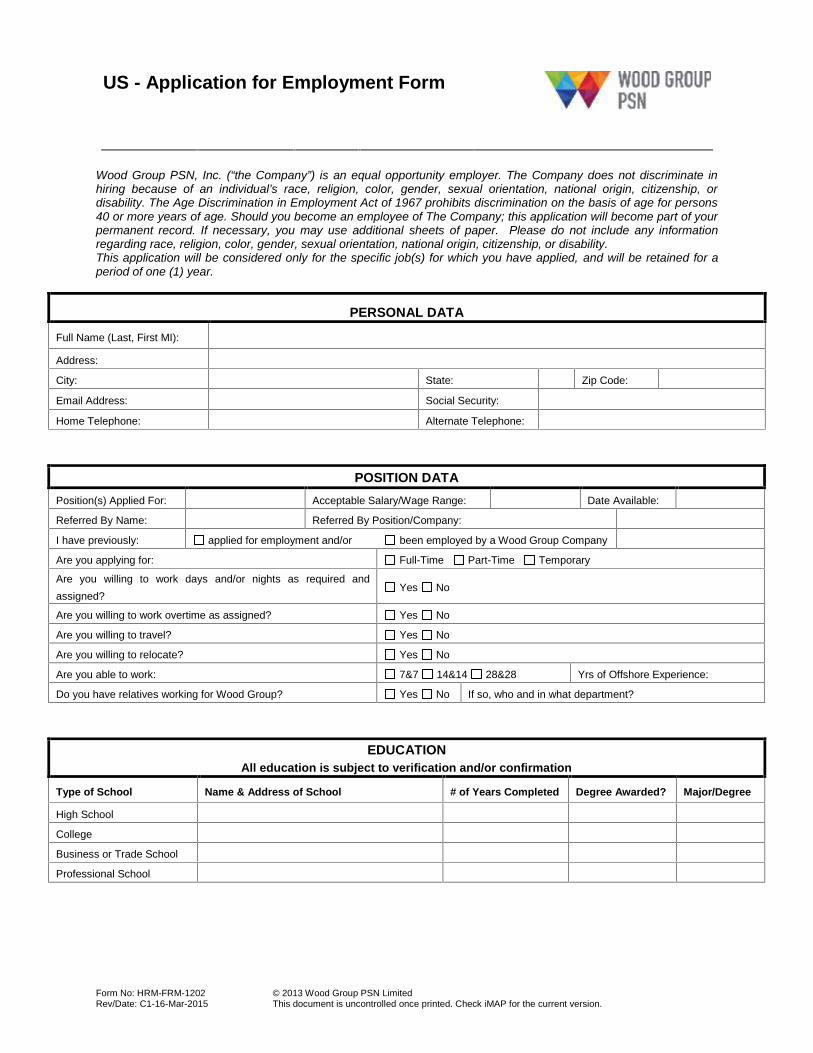
US - Application for Employment Form
Form No: HRM-FRM-1202Rev/Date: C1-16-Mar-2015
© 2013 Wood Group PSN LimitedThis document is uncontrolled once printed. Check iMAP for the current version.
Wood Group PSN, Inc. (“the Company”) is an equal opportunity employer. The Company does not discriminate inhiring because of an individual’s race, religion, color, gender, sexual orientation, national origin, citizenship, ordisability. The Age Discrimination in Employment Act of 1967 prohibits discrimination on the basis of age for persons40 or more years of age. Should you become an employee of The Company; this application will become part of yourpermanent record. If necessary, you may use additional sheets of paper. Please do not include any informationregarding race, religion, color, gender, sexual orientation, national origin, citizenship, or disability.This application will be considered only for the specific job(s) for which you have applied, and will be retained for aperiod of one (1) year.
PERSONAL DATA
Full Name (Last, First MI):
Address:
City: State: Zip Code:
Email Address: Social Security:
Home Telephone: Alternate Telephone:
POSITION DATAPosition(s) Applied For: Acceptable Salary/Wage Range: Date Available:
Referred By Name: Referred By Position/Company:
I have previously: applied for employment and/or been employed by a Wood Group Company
Are you applying for: Full-Time Part-Time Temporary
Are you willing to work days and/or nights as required andassigned?
Yes No
Are you willing to work overtime as assigned? Yes No
Are you willing to travel? Yes No
Are you willing to relocate? Yes No
Are you able to work: 7&7 14&14 28&28 Yrs of Offshore Experience:
Do you have relatives working for Wood Group? Yes No If so, who and in what department?
EDUCATIONAll education is subject to verification and/or confirmation
Type of School Name & Address of School # of Years Completed Degree Awarded? Major/Degree
High School
College
Business or Trade School
Professional School
US - Application for Employment Form
Form No: HRM-FRM-1202Rev/Date: C1-16-Mar-2015
© 2013 Wood Group PSN LimitedThis document is uncontrolled once printed. Check iMAP for the current version.
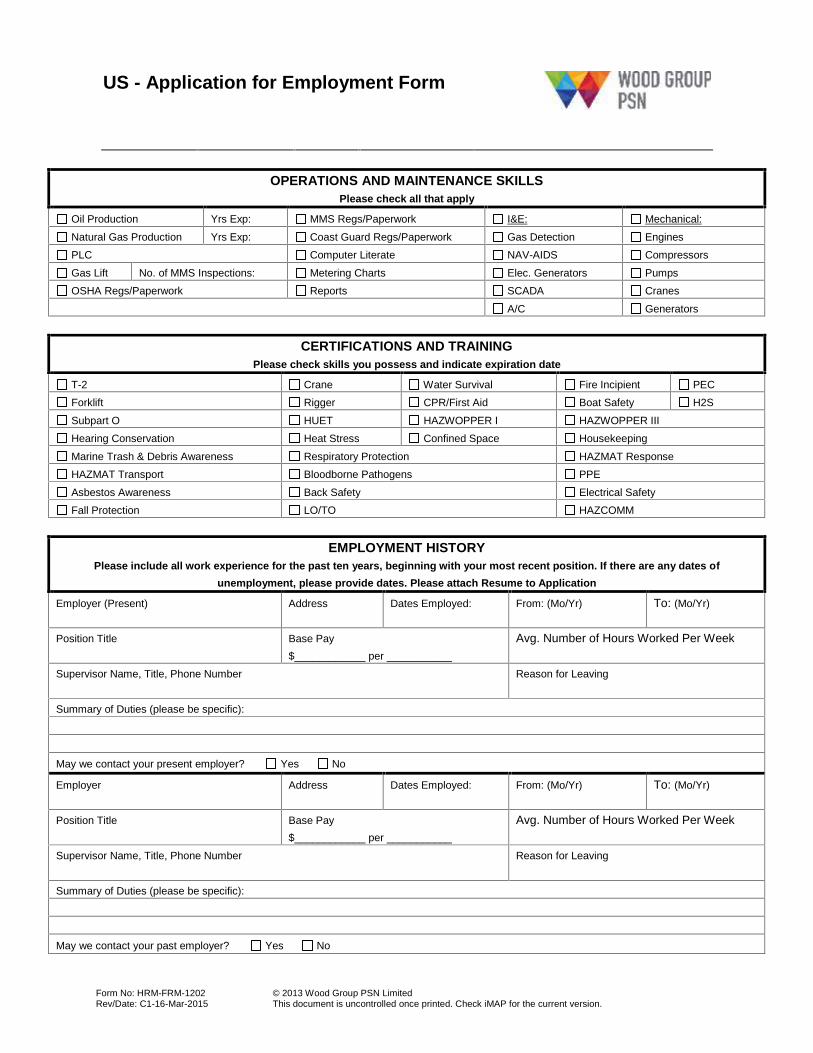
OPERATIONS AND MAINTENANCE SKILLSPlease check all that apply
Oil Production Yrs Exp: MMS Regs/Paperwork I&E: Mechanical:
Natural Gas Production Yrs Exp: Coast Guard Regs/Paperwork Gas Detection Engines
PLC Computer Literate NAV-AIDS Compressors
Gas Lift No. of MMS Inspections: Metering Charts Elec. Generators Pumps
OSHA Regs/Paperwork Reports SCADA Cranes
A/C Generators
CERTIFICATIONS AND TRAININGPlease check skills you possess and indicate expiration date
T-2 Crane Water Survival Fire Incipient PEC
Forklift Rigger CPR/First Aid Boat Safety H2S
Subpart O HUET HAZWOPPER I HAZWOPPER III
Hearing Conservation Heat Stress Confined Space Housekeeping
Marine Trash & Debris Awareness Respiratory Protection HAZMAT Response
HAZMAT Transport Bloodborne Pathogens PPE
Asbestos Awareness Back Safety Electrical Safety
Fall Protection LO/TO HAZCOMM
EMPLOYMENT HISTORYPlease include all work experience for the past ten years, beginning with your most recent position. If there are any dates of
unemployment, please provide dates. Please attach Resume to Application
Employer (Present) Address Dates Employed: From: (Mo/Yr) To: (Mo/Yr)
Position Title Base Pay$____________ per ___________
Avg. Number of Hours Worked Per Week
Supervisor Name, Title, Phone Number Reason for Leaving
Summary of Duties (please be specific):
May we contact your present employer? Yes No
Employer Address Dates Employed: From: (Mo/Yr) To: (Mo/Yr)
Position Title Base Pay$____________ per ___________
Avg. Number of Hours Worked Per Week
Supervisor Name, Title, Phone Number Reason for Leaving
Summary of Duties (please be specific):
May we contact your past employer? Yes No
US - Application for Employment Form
Form No: HRM-FRM-1202Rev/Date: C1-16-Mar-2015
© 2013 Wood Group PSN LimitedThis document is uncontrolled once printed. Check iMAP for the current version.
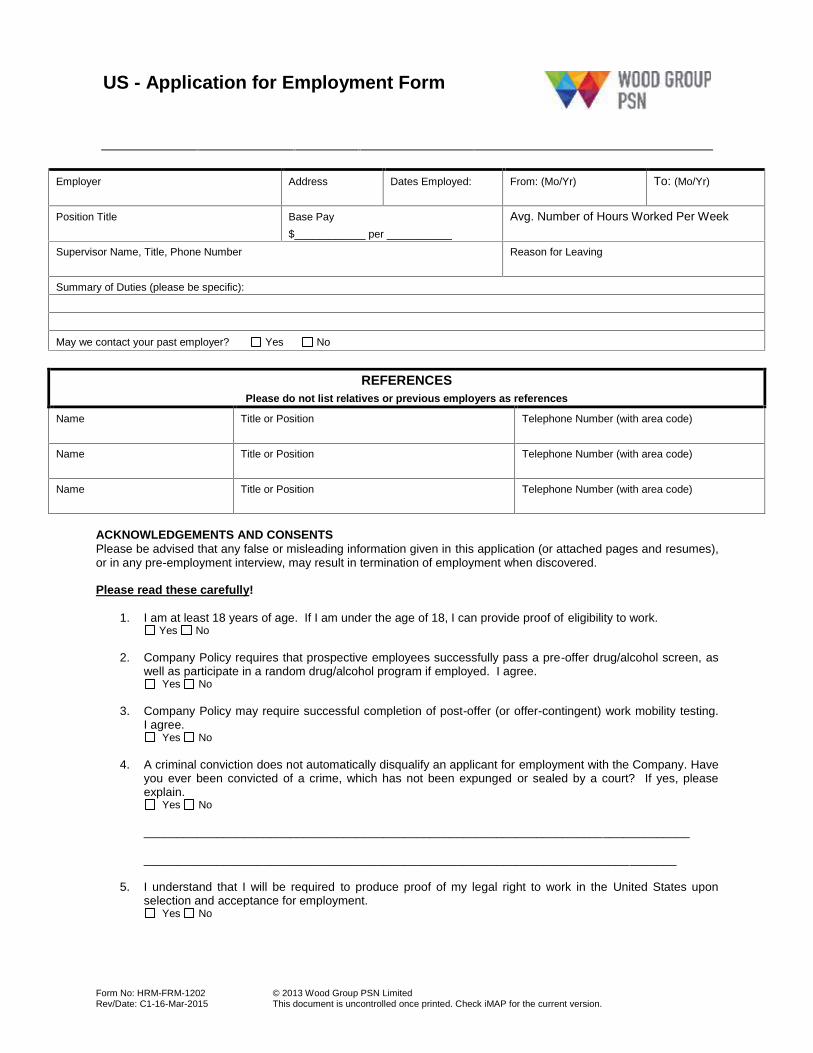
Employer Address Dates Employed: From: (Mo/Yr) To: (Mo/Yr)
Position Title Base Pay$____________ per ___________
Avg. Number of Hours Worked Per Week
Supervisor Name, Title, Phone Number Reason for Leaving
Summary of Duties (please be specific):
May we contact your past employer? Yes No
REFERENCESPlease do not list relatives or previous employers as references
Name Title or Position Telephone Number (with area code)
Name Title or Position Telephone Number (with area code)
Name Title or Position Telephone Number (with area code)
ACKNOWLEDGEMENTS AND CONSENTSPlease be advised that any false or misleading information given in this application (or attached pages and resumes),or in any pre-employment interview, may result in termination of employment when discovered.
Please read these carefully!
1. I am at least 18 years of age. If I am under the age of 18, I can provide proof of eligibility to work.Yes No
2. Company Policy requires that prospective employees successfully pass a pre-offer drug/alcohol screen, aswell as participate in a random drug/alcohol program if employed. I agree.
Yes No
3. Company Policy may require successful completion of post-offer (or offer-contingent) work mobility testing.I agree.
Yes No
4. A criminal conviction does not automatically disqualify an applicant for employment with the Company. Haveyou ever been convicted of a crime, which has not been expunged or sealed by a court? If yes, pleaseexplain.
Yes No
__________________________________________________________________________________
________________________________________________________________________________
5. I understand that I will be required to produce proof of my legal right to work in the United States uponselection and acceptance for employment.
Yes No
US - Application for Employment Form
Form No: HRM-FRM-1202Rev/Date: C1-16-Mar-2015
© 2013 Wood Group PSN LimitedThis document is uncontrolled once printed. Check iMAP for the current version.
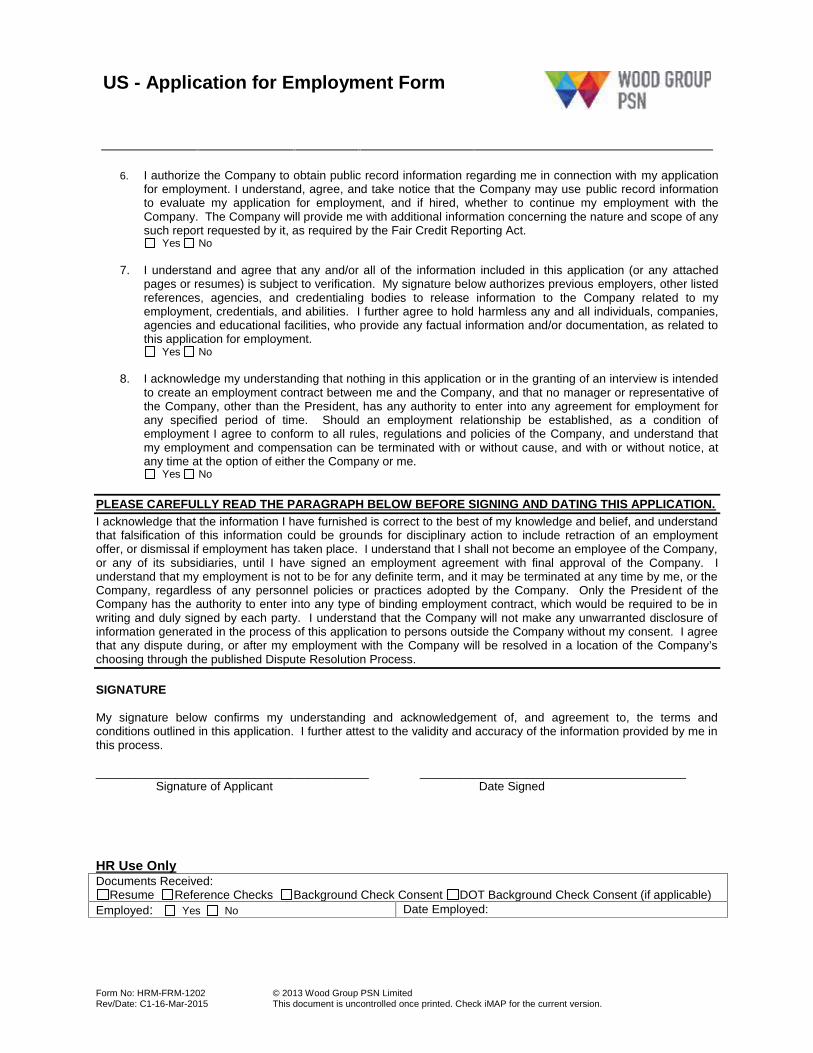
6. I authorize the Company to obtain public record information regarding me in connection with my applicationfor employment. I understand, agree, and take notice that the Company may use public record informationto evaluate my application for employment, and if hired, whether to continue my employment with theCompany. The Company will provide me with additional information concerning the nature and scope of anysuch report requested by it, as required by the Fair Credit Reporting Act.
Yes No
7. I understand and agree that any and/or all of the information included in this application (or any attachedpages or resumes) is subject to verification. My signature below authorizes previous employers, other listedreferences, agencies, and credentialing bodies to release information to the Company related to myemployment, credentials, and abilities. I further agree to hold harmless any and all individuals, companies,agencies and educational facilities, who provide any factual information and/or documentation, as related tothis application for employment.
Yes No
8. I acknowledge my understanding that nothing in this application or in the granting of an interview is intendedto create an employment contract between me and the Company, and that no manager or representative ofthe Company, other than the President, has any authority to enter into any agreement for employment forany specified period of time. Should an employment relationship be established, as a condition ofemployment I agree to conform to all rules, regulations and policies of the Company, and understand thatmy employment and compensation can be terminated with or without cause, and with or without notice, atany time at the option of either the Company or me.
Yes No
PLEASE CAREFULLY READ THE PARAGRAPH BELOW BEFORE SIGNING AND DATING THIS APPLICATION.I acknowledge that the information I have furnished is correct to the best of my knowledge and belief, and understandthat falsification of this information could be grounds for disciplinary action to include retraction of an employmentoffer, or dismissal if employment has taken place. I understand that I shall not become an employee of the Company,or any of its subsidiaries, until I have signed an employment agreement with final approval of the Company. Iunderstand that my employment is not to be for any definite term, and it may be terminated at any time by me, or theCompany, regardless of any personnel policies or practices adopted by the Company. Only the President of theCompany has the authority to enter into any type of binding employment contract, which would be required to be inwriting and duly signed by each party. I understand that the Company will not make any unwarranted disclosure ofinformation generated in the process of this application to persons outside the Company without my consent. I agreethat any dispute during, or after my employment with the Company will be resolved in a location of the Company’schoosing through the published Dispute Resolution Process.
SIGNATURE
My signature below confirms my understanding and acknowledgement of, and agreement to, the terms andconditions outlined in this application. I further attest to the validity and accuracy of the information provided by me inthis process.
_________________________________________ ________________________________________Signature of Applicant Date Signed
HR Use OnlyDocuments Received:
Resume Reference Checks Background Check Consent DOT Background Check Consent (if applicable)Employed: Yes No Date Employed:
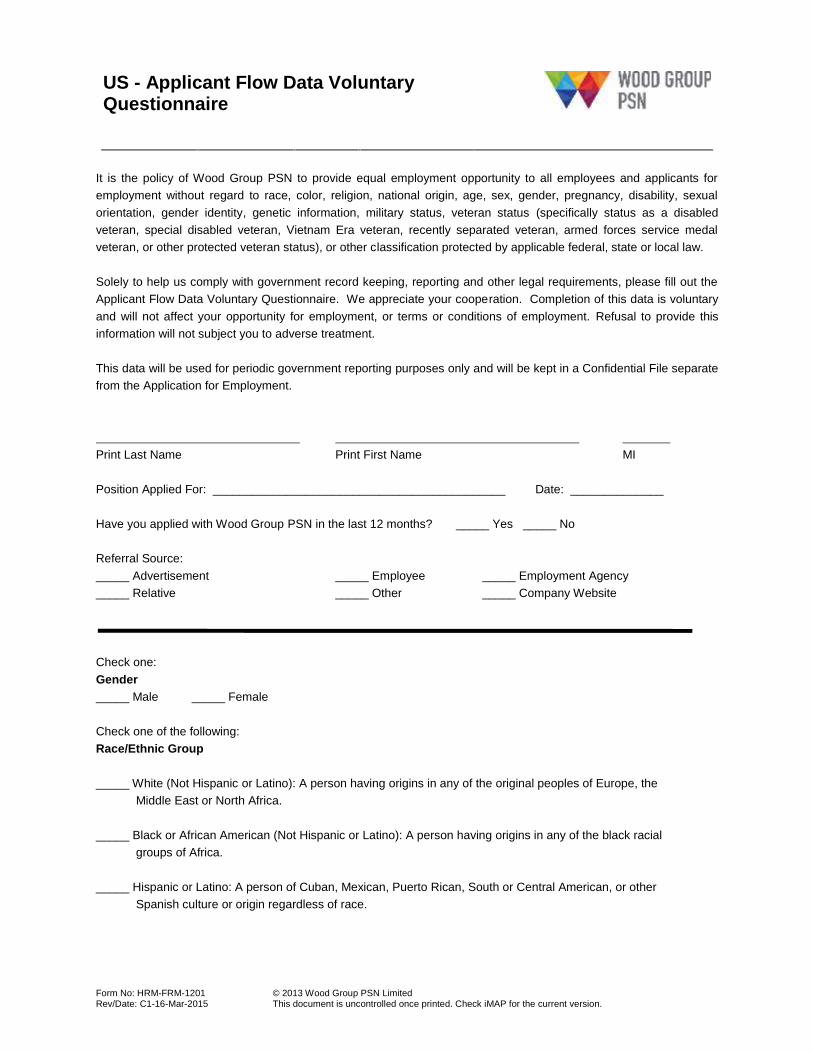
US - Applicant Flow Data VoluntaryQuestionnaire
Form No: HRM-FRM-1201Rev/Date: C1-16-Mar-2015
© 2013 Wood Group PSN LimitedThis document is uncontrolled once printed. Check iMAP for the current version.
It is the policy of Wood Group PSN to provide equal employment opportunity to all employees and applicants foremployment without regard to race, color, religion, national origin, age, sex, gender, pregnancy, disability, sexualorientation, gender identity, genetic information, military status, veteran status (specifically status as a disabledveteran, special disabled veteran, Vietnam Era veteran, recently separated veteran, armed forces service medalveteran, or other protected veteran status), or other classification protected by applicable federal, state or local law.
Solely to help us comply with government record keeping, reporting and other legal requirements, please fill out theApplicant Flow Data Voluntary Questionnaire. We appreciate your cooperation. Completion of this data is voluntaryand will not affect your opportunity for employment, or terms or conditions of employment. Refusal to provide thisinformation will not subject you to adverse treatment.
This data will be used for periodic government reporting purposes only and will be kept in a Confidential File separatefrom the Application for Employment.
Print Last Name Print First Name MI
Position Applied For: ____________________________________________ Date: ______________
Have you applied with Wood Group PSN in the last 12 months? _____ Yes _____ No
Referral Source:_____ Advertisement _____ Employee _____ Employment Agency_____ Relative _____ Other _____ Company Website
Check one:Gender_____ Male _____ Female
Check one of the following:Race/Ethnic Group
_____ White (Not Hispanic or Latino): A person having origins in any of the original peoples of Europe, theMiddle East or North Africa.
_____ Black or African American (Not Hispanic or Latino): A person having origins in any of the black racialgroups of Africa.
_____ Hispanic or Latino: A person of Cuban, Mexican, Puerto Rican, South or Central American, or otherSpanish culture or origin regardless of race.
US - Applicant Flow Data VoluntaryQuestionnaire
Form No: HRM-FRM-1201Rev/Date: C1-16-Mar-2015
© 2013 Wood Group PSN LimitedThis document is uncontrolled once printed. Check iMAP for the current version.
_____ Asian or Pacific Islander (Not Hispanic or Latino): A person having origins in any of the original peoples ofthe Far East, Southeast Asia or the Indian Subcontinent, including, for example, Cambodia, China, India,Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand and Vietnam.
_____ American Indian or Alaskan Native (Not Hispanic or Latino): A person having origins in any of the originalpeoples of North and South America (including Central America) and who maintains tribal affiliation orcommunity attachment.
_____ Two or more races (Not Hispanic or Latino): All persons who identify with more than one of the above fiveraces.
Check if any of the following are applicable:
_____ Vietnam Era Veteran: A person who served on active duty for a period of more than 180 days, any part ofwhich occurred between 8/5/64 and 5/7/75, and was discharged or released there from with other than adishonorable discharge or for a service connected disability.
_____ Disabled Veteran: A person entitled to disability compensation under laws administered by the VeteransAdministration for disability rated at 30% or more, or a person whose discharge or release from activeduty as a result of a disability which was incurred or aggravated in the line of duty.
_____ Disabled Individual: A person who has a mental or physical impairment that substantially limits one ormore major life activities, who has a record of such impairment, or who is regarded as having such animpairment.
Employee Payroll Direct Deposit Enrollment/Change Form
I hereby authorize Swaggart Brothers, Inc. to initiate credit entries into my account(s) listed below. Also, I hereby grant Swaggart Brothers, Inc. the right to correct any such electronic funds transfer resulting from erroneous overpayment by debiting my account to the extent of such overpayment. No more than three accounts may be designated. The initial setup and any changes to my direct deposit may be subject to a bank verification process. Therefore, the actual direct deposit of monies may not take place for 1 to 2 pay periods. It is my responsibility to verify that funds have been deposited as I have directed. The Company is not responsible for any banking fees incurred as a result of this agreement.
This authorization is to remain in full force and effect until the Company has received written notification from me of its termination in such time and such manner as to afford the Company and Depository a reasonable opportunity to act upon it.
Employee Name (Printed): Employee ID:
Employee Address:
Employee Phone #:
Employee Signature: Date:
Account Information (New/Change/Cancel)
Make sure to indicate what kind of account, along with the amount to be deposited, if less than your total net paycheck. Even if you are making changes to an existing account, you must indicate the bank name, routing and account number, so we can verify with your current information.
YOU MUST INCLUDE A COPY OF A VOIDED CHECK
1. Bank Name/City/Sate: New Change to Existing Cancel
Routing/Transit #: Account Number:
Checking Savings
I wish to deposit: $ or Entire Net Amount or Remaining Net Amount
2. Bank Name/City/Sate: New Change to Existing Cancel
Routing/Transit #: Account Number:
Checking Savings
I wish to deposit: $ or Entire Net Amount or Remaining Net Amount
3. Bank Name/City/Sate: New Change to Existing Cancel
Routing/Transit #: Account Number:
Checking Savings
I wish to deposit: $ or Entire Net Amount or Remaining Net Amount
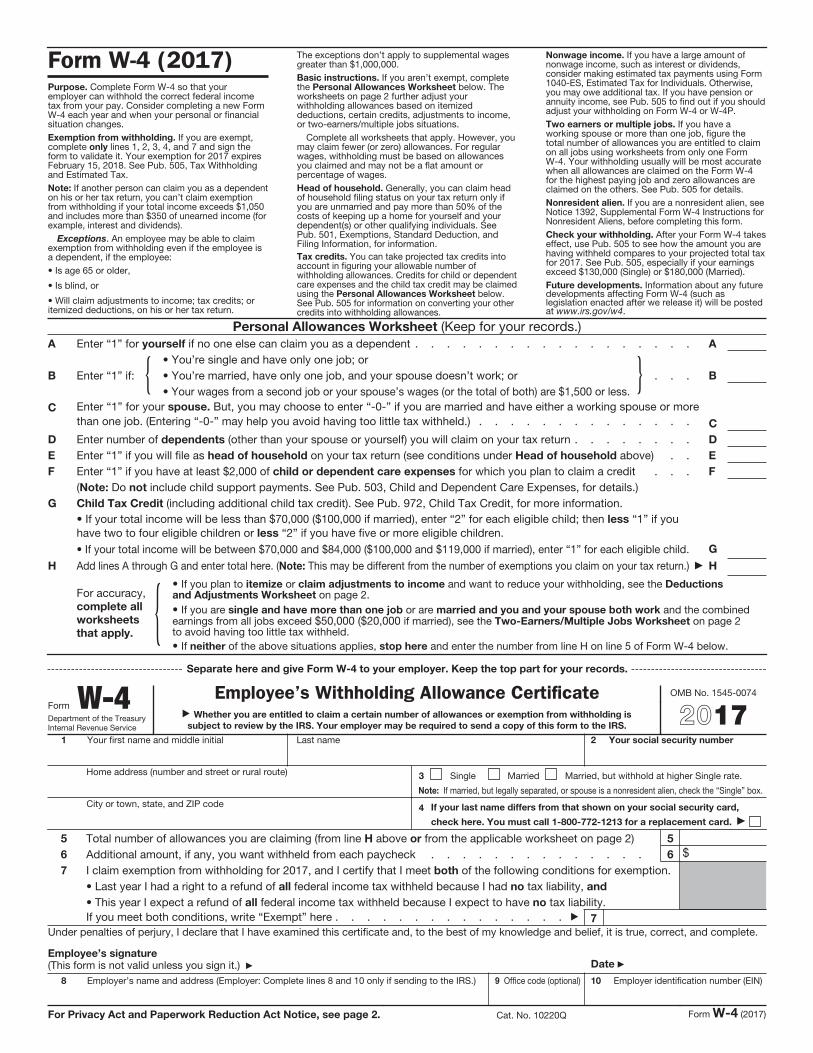
Form W-4 (2017)Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial situation changes.
Exemption from withholding. If you are exempt, complete only lines 1, 2, 3, 4, and 7 and sign the form to validate it. Your exemption for 2017 expires February 15, 2018. See Pub. 505, Tax Withholding and Estimated Tax.
Note: If another person can claim you as a dependent on his or her tax return, you can’t claim exemption from withholding if your total income exceeds $1,050 and includes more than $350 of unearned income (for example, interest and dividends).
Exceptions. An employee may be able to claim exemption from withholding even if the employee is a dependent, if the employee:
• Is age 65 or older,
• Is blind, or
• Will claim adjustments to income; tax credits; or itemized deductions, on his or her tax return.
The exceptions don’t apply to supplemental wages greater than $1,000,000.
Basic instructions. If you aren’t exempt, complete the Personal Allowances Worksheet below. The worksheets on page 2 further adjust your withholding allowances based on itemized deductions, certain credits, adjustments to income, or two-earners/multiple jobs situations.
Complete all worksheets that apply. However, you may claim fewer (or zero) allowances. For regular wages, withholding must be based on allowances you claimed and may not be a flat amount or percentage of wages.
Head of household. Generally, you can claim head of household filing status on your tax return only if you are unmarried and pay more than 50% of the costs of keeping up a home for yourself and your dependent(s) or other qualifying individuals. See Pub. 501, Exemptions, Standard Deduction, and Filing Information, for information.
Tax credits. You can take projected tax credits into account in figuring your allowable number of withholding allowances. Credits for child or dependent care expenses and the child tax credit may be claimed using the Personal Allowances Worksheet below. See Pub. 505 for information on converting your other credits into withholding allowances.
Nonwage income. If you have a large amount of nonwage income, such as interest or dividends, consider making estimated tax payments using Form 1040-ES, Estimated Tax for Individuals. Otherwise, you may owe additional tax. If you have pension or annuity income, see Pub. 505 to find out if you should adjust your withholding on Form W-4 or W-4P.
Two earners or multiple jobs. If you have a working spouse or more than one job, figure the total number of allowances you are entitled to claim on all jobs using worksheets from only one Form W-4. Your withholding usually will be most accurate when all allowances are claimed on the Form W-4 for the highest paying job and zero allowances are claimed on the others. See Pub. 505 for details.
Nonresident alien. If you are a nonresident alien, see Notice 1392, Supplemental Form W-4 Instructions for Nonresident Aliens, before completing this form.
Check your withholding. After your Form W-4 takes effect, use Pub. 505 to see how the amount you are having withheld compares to your projected total tax for 2017. See Pub. 505, especially if your earnings exceed $130,000 (Single) or $180,000 (Married).
Future developments. Information about any future developments affecting Form W-4 (such as legislation enacted after we release it) will be posted at www.irs.gov/w4.
Personal Allowances Worksheet (Keep for your records.)A Enter “1” for yourself if no one else can claim you as a dependent . . . . . . . . . . . . . . . . . . A
B Enter “1” if: {• You’re single and have only one job; or
• You’re married, have only one job, and your spouse doesn’t work; or . . .
• Your wages from a second job or your spouse’s wages (or the total of both) are $1,500 or less.} B
C Enter “1” for your spouse. But, you may choose to enter “-0-” if you are married and have either a working spouse or more
than one job. (Entering “-0-” may help you avoid having too little tax withheld.) . . . . . . . . . . . . . . C
D Enter number of dependents (other than your spouse or yourself) you will claim on your tax return . . . . . . . . D
E Enter “1” if you will file as head of household on your tax return (see conditions under Head of household above) . . E
F Enter “1” if you have at least $2,000 of child or dependent care expenses for which you plan to claim a credit . . . F
(Note: Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.)
G Child Tax Credit (including additional child tax credit). See Pub. 972, Child Tax Credit, for more information.
• If your total income will be less than $70,000 ($100,000 if married), enter “2” for each eligible child; then less “1” if you have two to four eligible children or less “2” if you have five or more eligible children.
• If your total income will be between $70,000 and $84,000 ($100,000 and $119,000 if married), enter “1” for each eligible child. G
H Add lines A through G and enter total here. (Note: This may be different from the number of exemptions you claim on your tax return.) H
For accuracy, complete all worksheets that apply. {
• If you plan to itemize or claim adjustments to income and want to reduce your withholding, see the Deductions and Adjustments Worksheet on page 2.
• If you are single and have more than one job or are married and you and your spouse both work and the combined earnings from all jobs exceed $50,000 ($20,000 if married), see the Two-Earners/Multiple Jobs Worksheet on page 2 to avoid having too little tax withheld.
• If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below.
Separate here and give Form W-4 to your employer. Keep the top part for your records.
Form W-4Department of the Treasury Internal Revenue Service
Employee’s Withholding Allowance Certificate Whether you are entitled to claim a certain number of allowances or exemption from withholding is
subject to review by the IRS. Your employer may be required to send a copy of this form to the IRS.
OMB No. 1545-0074
20171 Your first name and middle initial Last name
Home address (number and street or rural route)
City or town, state, and ZIP code
2 Your social security number
3 Single Married Married, but withhold at higher Single rate.
Note: If married, but legally separated, or spouse is a nonresident alien, check the “Single” box.
4 If your last name differs from that shown on your social security card,
check here. You must call 1-800-772-1213 for a replacement card.
5 Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2) 5
6 Additional amount, if any, you want withheld from each paycheck . . . . . . . . . . . . . . 6 $
7 I claim exemption from withholding for 2017, and I certify that I meet both of the following conditions for exemption.
• Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and
• This year I expect a refund of all federal income tax withheld because I expect to have no tax liability.
If you meet both conditions, write “Exempt” here . . . . . . . . . . . . . . . 7
Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete.
Employee’s signature (This form is not valid unless you sign it.) Date
8 Employer’s name and address (Employer: Complete lines 8 and 10 only if sending to the IRS.) 9 Office code (optional) 10 Employer identification number (EIN)
For Privacy Act and Paperwork Reduction Act Notice, see page 2. Cat. No. 10220Q Form W-4 (2017)
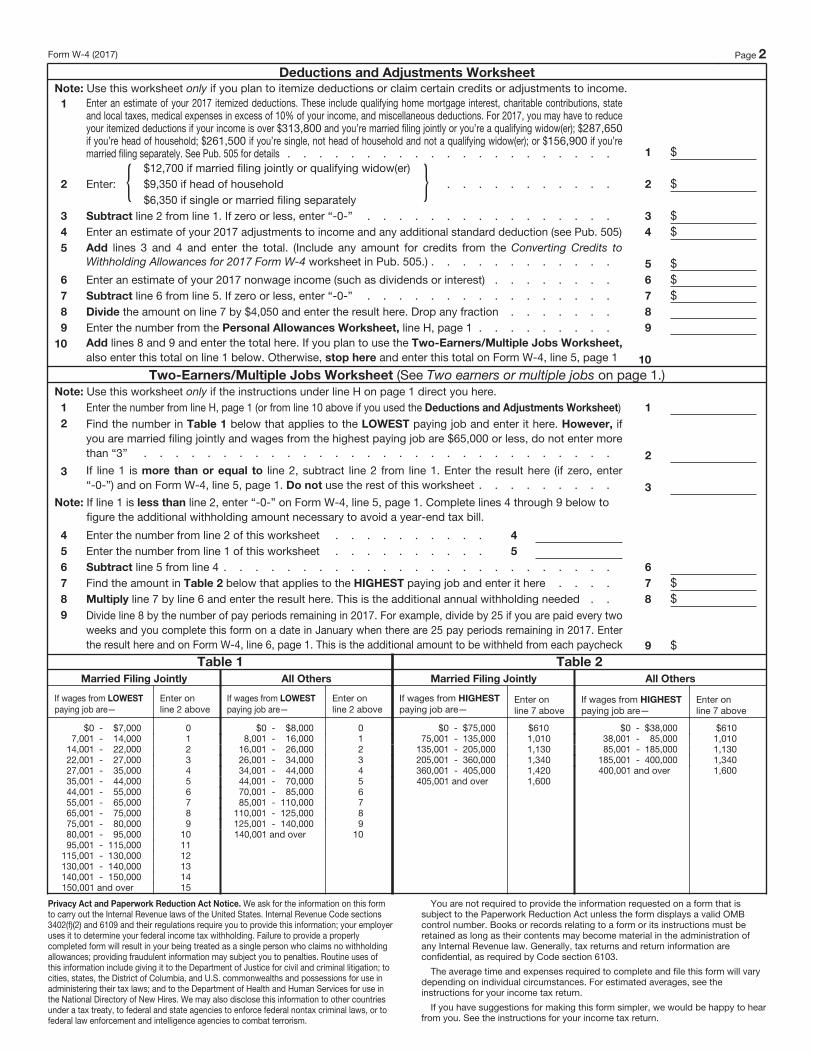
Form W-4 (2017) Page 2
Deductions and Adjustments WorksheetNote: Use this worksheet only if you plan to itemize deductions or claim certain credits or adjustments to income.
1 Enter an estimate of your 2017 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state and local taxes, medical expenses in excess of 10% of your income, and miscellaneous deductions. For 2017, you may have to reduce your itemized deductions if your income is over $313,800 and you’re married filing jointly or you’re a qualifying widow(er); $287,650 if you’re head of household; $261,500 if you’re single, not head of household and not a qualifying widow(er); or $156,900 if you’re married filing separately. See Pub. 505 for details . . . . . . . . . . . . . . . . . . . . . 1 $
2 Enter: {$12,700 if married filing jointly or qualifying widow(er)
$9,350 if head of household . . . . . . . . . . .
$6,350 if single or married filing separately} 2 $
3 Subtract line 2 from line 1. If zero or less, enter “-0-” . . . . . . . . . . . . . . . . 3 $
4 Enter an estimate of your 2017 adjustments to income and any additional standard deduction (see Pub. 505) 4 $
5 Add lines 3 and 4 and enter the total. (Include any amount for credits from the Converting Credits to
Withholding Allowances for 2017 Form W-4 worksheet in Pub. 505.) . . . . . . . . . . . . 5 $
6 Enter an estimate of your 2017 nonwage income (such as dividends or interest) . . . . . . . . 6 $
7 Subtract line 6 from line 5. If zero or less, enter “-0-” . . . . . . . . . . . . . . . . 7 $
8 Divide the amount on line 7 by $4,050 and enter the result here. Drop any fraction . . . . . . . 8
9 Enter the number from the Personal Allowances Worksheet, line H, page 1 . . . . . . . . . 9
10 Add lines 8 and 9 and enter the total here. If you plan to use the Two-Earners/Multiple Jobs Worksheet,
also enter this total on line 1 below. Otherwise, stop here and enter this total on Form W-4, line 5, page 1 10
Two-Earners/Multiple Jobs Worksheet (See Two earners or multiple jobs on page 1.)Note: Use this worksheet only if the instructions under line H on page 1 direct you here.
1 Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet) 1
2 Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if
you are married filing jointly and wages from the highest paying job are $65,000 or less, do not enter more
than “3” . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
3 If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter
“-0-”) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet . . . . . . . . . 3
Note: If line 1 is less than line 2, enter “-0-” on Form W-4, line 5, page 1. Complete lines 4 through 9 below to
figure the additional withholding amount necessary to avoid a year-end tax bill.
4 Enter the number from line 2 of this worksheet . . . . . . . . . . 4
5 Enter the number from line 1 of this worksheet . . . . . . . . . . 5
6 Subtract line 5 from line 4 . . . . . . . . . . . . . . . . . . . . . . . . . 6
7 Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here . . . . 7 $
8 Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed . . 8 $
9 Divide line 8 by the number of pay periods remaining in 2017. For example, divide by 25 if you are paid every two
weeks and you complete this form on a date in January when there are 25 pay periods remaining in 2017. Enter
the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck 9 $
Table 1
Married Filing Jointly
If wages from LOWEST paying job are—
Enter on line 2 above
$0 - $7,000 07,001 - 14,000 1
14,001 - 22,000 222,001 - 27,000 327,001 - 35,000 435,001 - 44,000 544,001 - 55,000 655,001 - 65,000 765,001 - 75,000 875,001 - 80,000 980,001 - 95,000 10
95,001 - 115,000 11115,001 - 130,000 12130,001 - 140,000 13140,001 - 150,000 14150,001 and over 15
All Others
If wages from LOWEST paying job are—
Enter on line 2 above
$0 - $8,000 08,001 - 16,000 1
16,001 - 26,000 226,001 - 34,000 334,001 - 44,000 444,001 - 70,000 570,001 - 85,000 685,001 - 110,000 7
110,001 - 125,000 8125,001 - 140,000 9140,001 and over 10
Table 2
Married Filing Jointly
If wages from HIGHEST paying job are—
Enter on line 7 above
$0 - $75,000 $61075,001 - 135,000 1,010
135,001 - 205,000 1,130205,001 - 360,000 1,340360,001 - 405,000 1,420405,001 and over 1,600
All Others
If wages from HIGHEST paying job are—
Enter on line 7 above
$0 - $38,000 $61038,001 - 85,000 1,01085,001 - 185,000 1,130
185,001 - 400,000 1,340400,001 and over 1,600
Privacy Act and Paperwork Reduction Act Notice. We ask for the information on this form to carry out the Internal Revenue laws of the United States. Internal Revenue Code sections 3402(f)(2) and 6109 and their regulations require you to provide this information; your employer uses it to determine your federal income tax withholding. Failure to provide a properly completed form will result in your being treated as a single person who claims no withholding allowances; providing fraudulent information may subject you to penalties. Routine uses of this information include giving it to the Department of Justice for civil and criminal litigation; to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws; and to the Department of Health and Human Services for use in the National Directory of New Hires. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism.
You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by Code section 6103.
The average time and expenses required to complete and file this form will vary depending on individual circumstances. For estimated averages, see the instructions for your income tax return.
If you have suggestions for making this form simpler, we would be happy to hear from you. See the instructions for your income tax return.
CONFIDENTIALITY
AGREEMENT This agreement is made between Wood Group PSN, Inc., its affiliates and subsidiaries (collectively, “Wood Group
Production Services Network”) and __________________________.
(employee’s name)
YOU UNDERSTAND AND ACKNOWLEDGE THE FOLLOWING FACTS:
You are employed by Wood Group PSN, Inc., in both your training and in doing the job, you may come in contact with confidential information that Wood Group PSN, Inc., owns and needs to protect. Wood Group PSN, Inc., does business worldwide. “Confidential information” means any data or information which is valuable to Wood Group PSN, Inc., and not generally known to competitors of Wood Group PSN, Inc., or other outsiders. This includes customer and client data, product specifications, production techniques, personnel records, personal matters, payroll data, financial data, sales and marketing activity and plans, trade secrets, and proprietary information. The unauthorized disclosure of confidential information, during employment or after termination, may cause irreparable injury to the Company or its customers. YOU AGREE not to use or communicate confidential information outside of your work for Wood Group PSN, Inc., you may not make any copies of that information for yourself or take it away from Wood Group PSN, Inc., except when specifically authorized to do so by your supervisor for brief periods to do your work. You may not keep or give away any of that information after you stop working for Wood Group PSN, Inc., and must return it to Wood Group PSN, Inc., with or without demand. If you work elsewhere, you will not communicate or use any confidential information in that work.
______________________________
Date
______________________________ ______________________________
Employee’s Signature Print Name (Full Legal Name)
Document No: Revision 0 Page 1 of 2
Wood Group Hiring Package
Title: Benefits Notification Effective Date: 01/01/2017
Benefit Notification: Wood Group has medical, life, dental and vision benefits available to employees beginning the 1st of the month following 60 days of full time service. The company also offers a 401(k) plan that is available to employees upon hire. Please visit usbenefits.woodgroup.net or call 1-844-260-3602 for more information on Health Benefits and www.empower-retirement.com/participant or call 1-888-411-4015 for information on the Retirement Benefit Plan. Wood Group will be sending Benefit information to your home address. PLEASE BE ADVISED YOU MUST LOG ON AND ENROLL FOR HEALTH AND WELFARE BENEFITS WITHIN 31 DAYS OF HIRE. I understand that it is my responsibility to sign up for Health Benefits within 31 days from hire. I also understand that these Benefits will begin the 1
st of the month following 60 days of full time
service. If I do not elect to enroll within 31 days I understand that I am waiving my right to participate in the benefit plan until the next eligibility period/open enrollment. ________________________________ Print Employee Name ________________________________ _________________ Signature Date Notification de Beneficios: Wood Group tiene médicos, vida, dental y beneficios de visión disponibles para empleados comenzando el día 1 del mes tras 60 días de servicio de tiempo completo. La compañía también ofrece un plan 401 (k) que está disponible para empleados en alquiler. Por favor visite usbenefits.woodgroup.net o llamar 1-844-260-3602 para obtener más información en cuanto a sus opciones de cobertura y www.empower-retirement.com/participant o llama 1-888-411-4015 para obtener información sobre el plan de beneficios de jubilación/retiro. Wood Group enviara información detallada sobre Beneficios a la dirección de su residencia. Le advertimos que debe iniciar la sesión e inscribirse para beneficios de salud y el bienestar dentro de los 31 días de alquiler. Entiendo que es mi responsabilidad el solicitar beneficios para la salud dentro de los 31 días del alquiler. También entiendo que estos beneficios iniciarán el día 1 del mes siguiente a 60 días de servicio de tiempo completo. Si no decide de inscribirse dentro de 31 días entiendo que estoy renunciando a mi derecho a participar en el plan de beneficios hasta la siguiente inscripción período abierto de elegibilidad. ______________________________________
Escribe el Nombre de Empleado ______________________________________ ___________________
Firma de Empleado Fecha
Document No: Revision 0 Page 2 of 2
Wood Group Hiring Package
Title: Benefits Notification Effective Date: 01/01/2017
EMPLOYEE KEEP THIS PAGE Health & Welfare Benefits contact: usbenefits.woodgroup.net 844-260-3602 Retirement Savings Plan contact: www.empower-retirement.com/participant 888-411-4015
US DOT Drug & Alcohol Authorizationand Questionnaire Form
Applicant Authorization to Release DOT Drug /Alcohol Test Results
To be completed by Applicant
I, ____________________________________, as the Applicant, understand that as a condition of hire with Wood GroupPSN, Inc. (WGPSN), I must consent to the release of the results of all DOT mandated drug and/or alcohol tests –including refusals to test – from all companies for which I worked in a DOT safety-sensitive position, or for which I took aDOT pre-employment drug test during the previous three (3) years.Below I have listed my current and/or past company for which I worked, or was pre-employment tested, during the pastthree years. I hereby authorize the company listed below to furnish, to WGPSN, the following information concerning myDOT drug and alcohol tests: (1) all DOT alcohol test results of 0.04 or greater; (2) all positive DOT drug test results; (3) allinstances in which I refused to submit to any DOT drug and/or DOT alcohol test (refusals include adulterated and/orsubstituted tests); (4) other violations of DOT drug and alcohol testing regulations; and (5) documentation of successfulcompletion of DOT return-to-duty requirements, including follow-up testing, as a result of a violation of DOT drug andalcohol regulations.
Previous Employer Name City & State Business Phone(+ area code)
Employment DatesMonth/Year
From:To:
This form must be completed for each employer, additional forms will be provided if necessary.
Applicant Certification: I have read and fully understand this authorization to release my previous drug and alcohol testresults and any non-negative test records to WGPSN. In signing below, I certify that all of the information I have furnishedon this form is true and complete, and that I have identified all of the companies for which I have worked in a DOT safety-sensitive position, or was DOT pre-employment tested by, during the previous three years. I also understand that I amresponsible for all costs associated with any pending Substance Abuse Professional assessment, recommendations,education and treatment, including costs involving return-to-duty testing and follow-up testing yet to be completed.
Check this box if you have NOT performed DOT functions in the past 3 years.
____________________________ _____________________________ ______________Signature of Applicant Social Security Number Date
To be completed by Previous Employer
In accordance with 49 CFR Part 40.25, WGPSN is required to obtain (and as a previous employer you are required torelease) information concerning the above named Applicant’s past DOT drug and alcohol test results within the last twoyears (FMCSA 3 years) – including refusals to test. Please complete the following:
Yes No 1. Any DOT alcohol test results of 0.04 or greater during the previous two years?Yes No 2. Any DOT positive drug test results during the previous two years?Yes No 3. Refusal to submit to a DOT required drug / alcohol test? (incl. adulterated or substituted specimens)Yes No 4. Other violations of DOT drug and alcohol testing regulations?Yes No 5. Did a previous employer report a drug/alcohol rule violation to you in the past two years?Yes No 6. If “yes” for any of the above items, did the employee complete the return-to-duty process?
7. Check this box if your company and/or the applicant was NOT subject to DOT regulations.
Note: If “yes” for item 5, you must provide the previous employer’s report. If “yes” for item 6, you must also transmit theappropriate return-to-duty documentation (e.g., SAP report(s), follow-up testing record).
_____________________________ ___________________________ _______________Previous Employer’s Company Name Name of Person Completing Form Date
FAX COMPLETED FORM TO: (713) 456-2930
US DOT Drug & Alcohol Authorizationand Questionnaire Form
APPLICANT QUESTIONAIRE REGARDING PREVIOUS DRUG & ALCOHOL TESTING INFORMATION
APPLICANT: PLEASE CHECK YES OR NO IN RESPONSE TO THE FOLLOWING QUESTIONS ASREQUIRED BY U.S. DEPARTMENT OF TRANSPORTATION REGULATIONS (49 CFR PART 40)FOR THE PAST THREE YEARS:
1. Have you been employed in a safety sensitive position by a DOT regulated employer in the past threeyears?
Yes No
2. Have you had any DOT required alcohol tests with a result of 0.04 or higher alcohol concentration?Yes No
3. Have you had any verified positive DOT required drug tests?Yes No
4. Have you refused to be tested (including having a verified adulterated or substituted drug test result)?Yes No
5. Have you had any other violation of a DOT agency drug or alcohol testing regulation?Yes No
6. Were there any situations in which you tested positive on a pre-employment test for a DOT employerthat did not hire you?
Yes No
7. Were there any situations in which you refused to submit (including any adulterated or substitutedfindings) to a pre-employment test for a DOT employer that did not hire you?
Yes No
I certify that my responses to the above questions are true:
Applicant’s Signature: Date: _______
Printed Name: SSN: ________
Background Check Questionnaire
Revision 0 Page 1 of 1
Hiring Package
Title: Personal Property Acknowledgement Form Effective Date: 03/01/2016
EMPLOYEE PERSONAL PROPERTY ACKNOWLEDGEMENT AND AGREEMENT
You are responsible for the safekeeping and security of all your personally owned tools and property. Personal tools and property are not to be stored in Swaggart Brothers supplied trailers, tool boxes, vehicles or equipment. It is your responsibility to inventory and maintain accountability for your personally owned tools and property at all times.
The undersigned, their successors and assigns, hereby forever completely release and discharge
Swaggart Brothers, its subsidiary companies, related entities and its Insurers for any and all claims,
damages, and liabilities resulting in any way from stolen employee owned tools or personal property.
Executed this the day of , 20 .
Employee Name (Please Print)
Employee Signature
24 Wood Group INT/B/1.4 May 2016
Business Ethics Policy
Receipt and Acknowledgement
I acknowledge that I have read and understood the Wood Group Business Ethics Policy.
I understand that each Wood Group employee, member of the Board of Directors, contractor and consultant and representatives, intermediaries and agents retained by Wood Group are responsible for knowing and adhering to the principles and standards of the Business Ethics Policy.
Signature:
Print name:
Strategic Business Unit:
Title:
Location:
Date:
The Wood Group Business Ethics Policy is available online in nine languages via the Wood Group intranet (www.woodgroup.net) or the Wood Group website (www.woodgroup.com).
“ Please sign this form and return it to Human Resources in hard copy or by email. ”
US - Drug and Alcohol PolicyAcknowledgement and Consent Form
Form No: HRM-FRM-1176Rev/Date: C1-10-Apr-2014
© 2013 Wood Group PSN LimitedThis document is uncontrolled once printed. Check iMAP for the current version.
ACKNOWLEDGEMENT & CONSENT
I hereby acknowledge that I have been provided a copy of the US Drug and Alcohol Policy. Iunderstand that disciplinary action, up to and including termination, will result if I violate this Policy.
Employee Signature Date
Employee Printed Name Employee ID/Last 4 Digits of SSN
I hereby consent to and authorize the disclosure by collecting and testing agents, MRO’s and othersinvolved in the drug and alcohol testing procedures under this policy, of alcohol and drug test resultsand related information, to WGPSN and its agents.
I hereby also consent to disclosure by WGPSN and its agents, including, but not limited to, anycollecting and testing agencies, of the test results identified above and any related information to anyclients/customers of WGPSN and their authorized agents, assignees, or representatives.
I hereby also consent to the release of the results of all drug and/or alcohol tests – including refusalsto test – from all companies, including WGPSN clients/customers, while employed by WGPSN. Ihereby authorize those companies to furnish, to WGPSN, the following information concerning mydrug and alcohol tests: (1) all alcohol test results of 0.04 or greater; (2) all positive drug test results;(3) all instances in which I refused to submit to any drug and/or alcohol test (refusals includeadulterated and/or substituted tests); (4) other violations of drug and alcohol testing regulations.
Employee Signature Date
Employee Printed Name Employee ID/Last 4 Digits of SSN
US - Drug and Alcohol PolicyAcknowledgement and Consent Form
Form No: HRM-FRM-1176Rev/Date: C1-10-Apr-2014
© 2013 Wood Group PSN LimitedThis document is uncontrolled once printed. Check iMAP for the current version.
Revision History
Revision Date Details of ChangesC1 10-Apr-2014 Issued for use to replace legacy Wood Group PSN Drug and Alcohol Policy
Acknowledgement & Consent Form – BEH115 (Appendix J)
1.0 PurposeThis form must be completed by all WGPSN employee’s acknowledging they have been provided a copy of the USDrug and Alcohol Policy as well as providing consent for release of drug and/or alcohol test results.
2.0 ScopeThis document applies to all US WGPSN personnel.
3.0 Glossary of Terms3.1 References
HRM-POL-1114 US Drug and Alcohol Policy
Note: These references are subject to change. Utilise the iMAP search engine for the latest applicable references.
3.2 Abbreviations
MRO Medical Review Officer
WGPSN Wood Group PSN
3.3 Terminology
Personnel — any of the Company’s employees, agents, independent contractors or subcontractors’ employeesworking on behalf of the Company.
4.0 Roles & ResponsibilitiesIt is the employee’s responsibility to read and understand the entire US Drug and Alcohol Policy. Employeeunderstands the disciplinary action, up to and including termination, will result if they violate the policy.
Wood Group PSN U.S. Employee Handbook Revision: C3 Acknowledgement Page 1 of 1
Employee Acknowledgement of Receipt and Understanding I acknowledge that I have received a copy and/or have received access to an electronic copy of the Wood Group PSN Employee Handbook, revision C3. I understand it contains important information about the Company’s general personnel policies and about my privileges and obligations as an employee. I further understand and acknowledge that I am governed by the contents of the Employee Handbook and I agree to read and familiarize myself with and comply with the policies contained in it. I also understand that if there is any policy or provision in the Handbook that I do not understand, I will seek clarification from my Manager/Supervisor or a member of the P&O team. I understand that Wood Group PSN is an "at will" employer (unless prohibited by state or other jurisdictional law) and as such employment with Wood Group PSN is not for a fixed term or definite period and may be terminated at the will of either party, with or without cause, and without prior notice. No Manager/Supervisor or other representative of the Company (except the President) has the authority to enter into any agreement for employment for any specified period of time, or to make any agreement contrary to Wood Group PSN’s at-will employment status. I also understand that the Company may change, rescind or add to any of the policies, benefits or practices described in the Employee Handbook, except the Employment-at-Will Policy in its sole and absolute discretion, with or without prior notice. I also understand that the Company will advise employees from time to time of material changes to the policies, benefits, or practices described in the Employee Handbook. Furthermore, I understand that this Handbook states Wood Group PSN’s policies and practices in effect on the date of publication. I understand that nothing contained in the Handbook may be construed as creating a promise of future benefits, entitlement, or a binding contract with Wood Group PSN. I also understand that these policies and procedures are continually evaluated and may be amended, modified or terminated at any time.
Employee Printed Name:
Employee Signature:
Date:
Policy AcknowledgementI hereby acknowledge that I have been provided with a copy of the following Wood Group PSN, Inc.policies,
Global HSE Policy (Global)
Driving Policy (Global)
Harassment Policy (Global)
IT acceptable use Policy (Global)
Social Media Policy (Global)
I understand that disciplinary action, up to and including termination, will result if I violate any of thesepolicies.
______________________________ ______________________________Employee – Printed Name Employee – Signature
______________________________Date